Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
OHSS nasıl önlenebilir ?
Dr.Engin Oral İ.Ü. Cerrahpaşa Tıp Fakültesi Kadın Hastalıkları ve Doğum Anabilim Dalı Reprodüktif Endokrinoloji Bilim Dalı

2
OUTLINE Introduction Primary risk factors (due to patient characteristics) Secondary risk factors (appearent during COH) Primary prevention (before starting HMG/FSH) Secondary prevention (after starting HMG/FSH and before HCG administration) Conclusion
 Secondary prevention (after starting HMG/FSH and before HCG administration) Conclusion.")
4
Ovarian hyperstimulation syndrome (Pubmed)
n : citations (802 Severe OHSS)
")
5
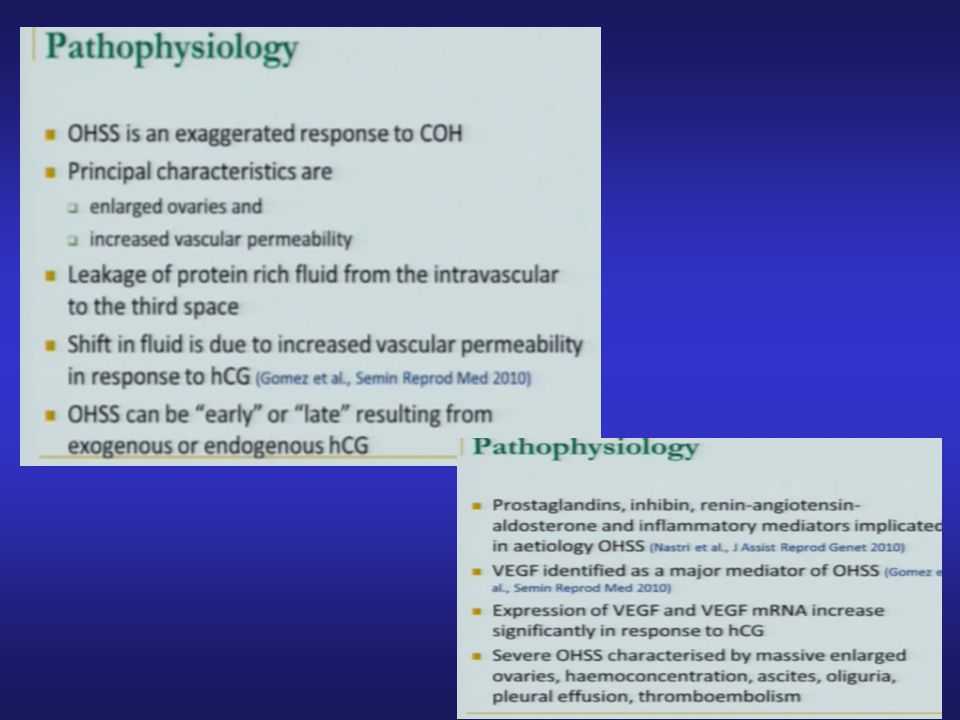
Early onset (early OHSS) up to 9 days after oocyte retrieval related to excessive ovarian response
Late onset (late OHSS) 10 days after oocyte retrieval induced by endogenously produced hCG after implantation
 10 days after oocyte retrieval induced by endogenously produced hCG after implantation.")
7
Ovarian VEGF Production (Basic&Clinical Studies)
Capillary permeability Angiogenesis Endothelial cell proliferation

8
OHSS-insidans ciddi OHSS insidansı %1 8-23% 5- 7% 0.08-1 20-33% 3-6%
Hafif OHSS Orta derecede OHSS Ciddi OHSS ovulasyon indüksiyonu (Gonadotropin) 8-23% 5- 7% 0.08-1 IVF 20-33% 3-6% 0.1-2% ciddi OHSS insidansı %1 CC-OHSS riski % 13.5 mild sporadik moderate ve severe
 8-23% 5- 7% IVF % 3-6% 0.1-2% ciddi OHSS insidansı %1. CC-OHSS riski. % 13.5 mild. sporadik moderate ve severe.")
11
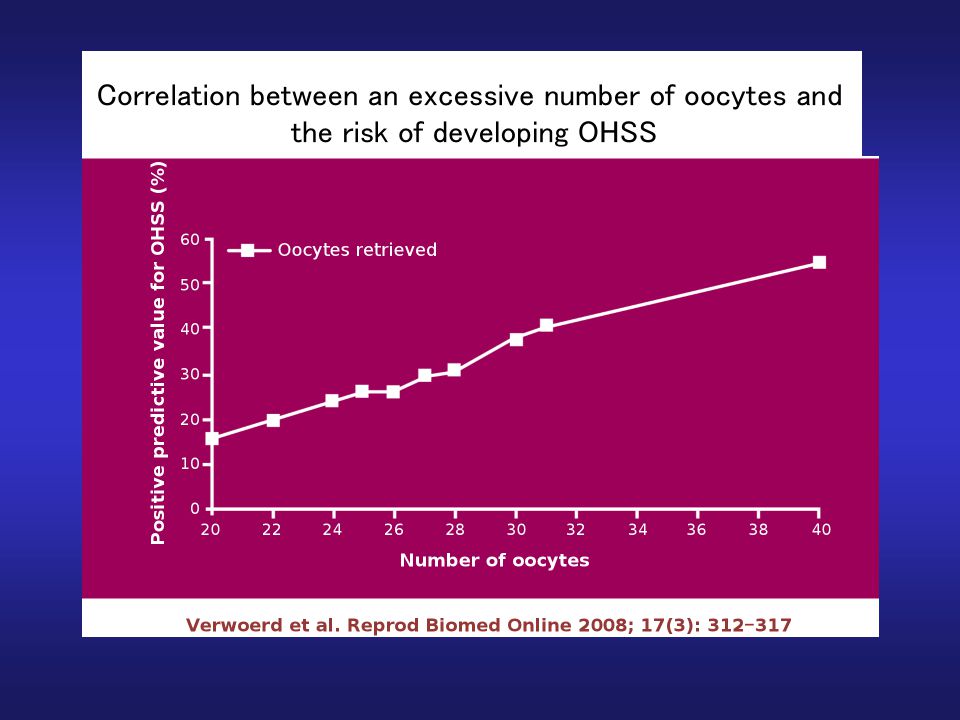
OHSS nin büyük bir kısmı önceden tahmin edilemeyen sikluslarda olabilirken , önceden yüksek risk olarak görüp ciddi –OHSS beklenilen olgular klinik pratikte yaklaşık:%20

12
the PRIMARY PREVENTION
The best treatment is the PRIMARY PREVENTION OHSS

13
Preventing Strategies
Identification of risk factors Monitoring ovulation USG & E2 Gold Standard

14
OHSS – prevention Identification of women at risk
Young age (<35yrs) Low body weight Polycystic ovary syndrome (PCOS). Polycystic appearance of ovaries by sonography Higher doses of exogenous gonadotrophins High absolute or rapidly rising E2 levels Number of oocytes Large number of follicles (small and intermediate size) Previous OHSS history Pregnancy (Multiple) hCG for luteal support GnRH agonist Egg donors AMH AFC, ovarian volume genetic predisposition
 Low body weight. Polycystic ovary syndrome (PCOS). Polycystic appearance of ovaries by sonography. Higher doses of exogenous gonadotrophins. High absolute or rapidly rising E2 levels. Number of oocytes. Large number of follicles (small and intermediate size) Previous OHSS history. Pregnancy (Multiple) hCG for luteal support. GnRH agonist. Egg donors. AMH. AFC, ovarian volume. genetic predisposition.")
15
OHSS-Allerji İmmünolojik hassasiyeti olan kişilerde (hipersensitivite veya alerjiler) OHSS daha fazla görülebilir. Prospektif kohort bir çalışma**, ağır OHSS gelişen hastalarda (n=18/428), kontrollere göre, istatistiki olarak anlamlı derecede yüksek allerji prevalansı görülmüştür (%56 versus %21). ** Enskog A, Henriksson M, Unander M, Nilsson L, Brannstrom M: Prospective study of the clinical and laboratory parameters of patients in whom ovarian hyperstimulation syndrome developed during controlled ovarian hyperstimulation for in vitro fertilization. Fertil Steril 1999, 71:808–814.
, kontrollere göre, istatistiki olarak anlamlı derecede yüksek allerji prevalansı görülmüştür (%56 versus %21). ** Enskog A, Henriksson M, Unander M, Nilsson L, Brannstrom M: Prospective study of the clinical and laboratory parameters of patients in whom ovarian hyperstimulation syndrome developed during controlled ovarian hyperstimulation for in vitro fertilization. Fertil Steril 1999, 71:808–814.")
16
Primary risk factors Variables Young age Low BMI History of OHSS PCOS
High antral follicle count High AMH level Genetic predisposition Others

17
OR : 6.8 (CI 95%: 4.9 – 9.6)
")
18
PCO pattern to predict OHSS

19
Primary risk factors AFC, only (excessive response)
Author N (cycle) Cut-off Sensitivity Specificity Ng et al, 2000 128 9 14 0.60 0.20 0.71 0.94 Van Rooij et al, 2002 114 0.92 0.63 Elder-Geva et al, 2005 56 0.33 Kwee et al, 2008 110 10 12 16 18 0.88 0.81 0.50 0.31 0.80 0.89 0.96 0.98 Aflatoonian et al, 2009 159 Overall (Buer SL, 2010) 0.82
 Cut-off. Sensitivity. Specificity. Ng et al, Van Rooij et al, Elder-Geva et al, Kwee et al, Aflatoonian et al, Overall (Buer SL, 2010)")
20
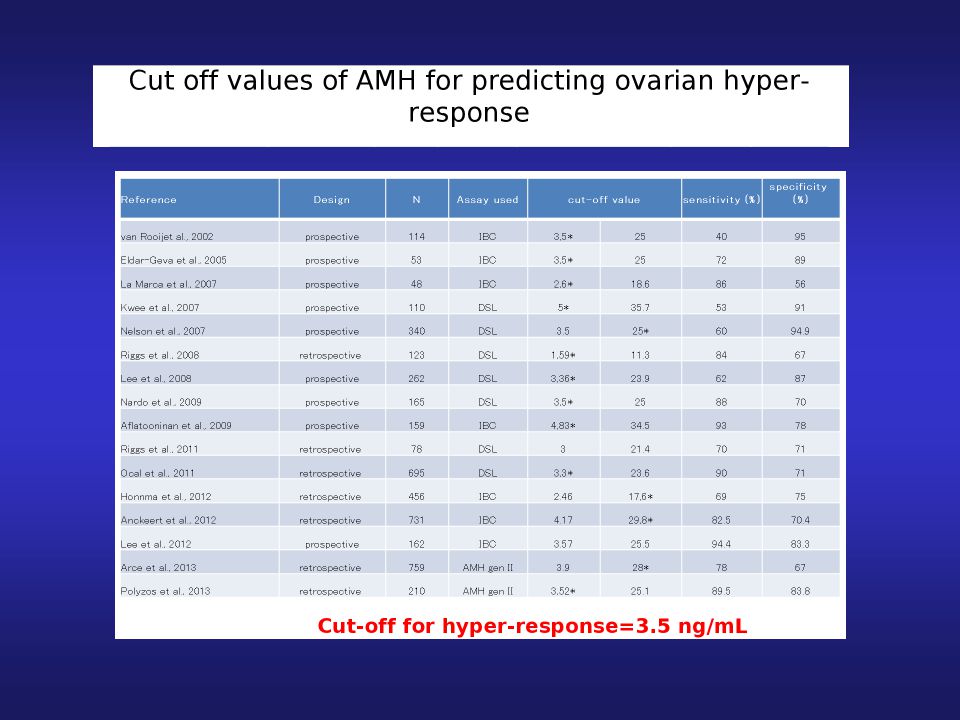
AMH- OHSS From La Marca et al. HRU 2011

22
OHSS OLAN 41 olgu vs OHSS OLMAYAN 41 olgu
OHSS OLAN OLGULARDA FSH (p < 0.0001) DÜŞÜK ; LH (p = 0.049 ) , AFS (p < 0.0001) , AMH (p < 0.0001) YÜKSEK inhibin B (p = 0.112) ve östradiol (p = 0.706) FARK YOK OHSS’ yi öngörmede AMH (AUC = 0.87) >> AFS (AUC = 0.74) AMH 3.3 ng/mL; duyarlılık %90,özgüllük %71,PPD %61,NPD %94. AFS > duyarlılık %78,özgüllük %65,PPD %52, NPD %86
 DÜŞÜK ; LH (p = ) , AFS (p < ) , AMH (p < ) YÜKSEK. inhibin B (p = 0.112) ve östradiol (p = 0.706) FARK YOK. OHSS’ yi öngörmede. AMH (AUC = 0.87) >> AFS (AUC = 0.74) AMH 3.3 ng/mL; duyarlılık %90,özgüllük %71,PPD %61,NPD %94. AFS >8 duyarlılık %78,özgüllük %65,PPD %52, NPD %86.")
23
background: Anti-Mullerian hormone (AMH) is a marker of ovarian reserve status and represents a good predictor of ovarian response to ovarian hyperstimulation. The aim of this study was to assess the accuracy of AMH and antral follicle count (AFC) as predictors of an excessive response in IVF/ICSI treatment. methods: A systematic review and meta-analysis of the existing literature was performed. Studies were included if 2 × 2 tables for the outcome excessive response in IVF patients in relation to AMH/AFC could be constructed. Using a bivariate meta-analytic model, both summary point estimates for sensitivity and specificity were calculated, as well as summary ROC curves. Clinical value was analysed by calculating post-test probabilities of excessive response at optimal cut-off levels, as well as the corresponding abnormal test rates. results: Nine studies reporting on AMH and five reporting on AFC were found. Summary estimates of sensitivity and specificity for AMH were 82 and 76%, respectively, and 82 and 80%, respectively, for AFC. Comparison of the summary estimates and ROC curves for AMH and AFC showed no statistical difference. Abnormal test rates for AMH and AFC amounted to 14 and 16%, respectively, at cut-off levels where test performance is optimal [likelihood ratio for a positive result (LR + ).8], with a post-test probability of +70%. conclusions: Both AMH and AFC are accurate predictors of excessive response to ovarian hyperstimulation. Moreover, both tests appear to have clinical value. This opens ways to explore the potential of individualized FSH dose regimens based on ovarian reserve testing.
 as predictors. of an excessive response in IVF/ICSI treatment. methods: A systematic review and meta-analysis of the existing literature was performed. Studies were included if 2 × 2 tables for the. outcome excessive response in IVF patients in relation to AMH/AFC could be constructed. Using a bivariate meta-analytic model, both. summary point estimates for sensitivity and specificity were calculated, as well as summary ROC curves. Clinical value was analysed by calculating. post-test probabilities of excessive response at optimal cut-off levels, as well as the corresponding abnormal test rates. results: Nine studies reporting on AMH and five reporting on AFC were found. Summary estimates of sensitivity and specificity for AMH. were 82 and 76%, respectively, and 82 and 80%, respectively, for AFC. Comparison of the summary estimates and ROC curves for AMH and. AFC showed no statistical difference. Abnormal test rates for AMH and AFC amounted to 14 and 16%, respectively, at cut-off levels where. test performance is optimal [likelihood ratio for a positive result (LR + ).8], with a post-test probability of +70%. conclusions: Both AMH and AFC are accurate predictors of excessive response to ovarian hyperstimulation. Moreover, both tests. appear to have clinical value. This opens ways to explore the potential of individualized FSH dose regimens based on ovarian reserve testing.")
24
SECONDARY risk factors
Variables (During COH) E2 (absolute level or rate) No. of follicle No. of oocytes retrieved Combination Others
 E2 (absolute level or rate) No. of follicle. No. of oocytes retrieved. Combination. Others.")
25
SECONDARY risk factors E2
Mean E2 levels are higher in patients who develop OHSS. A large overlap between the two groups. Less reliable in GnRH antagonist cycles. Valuable particularly in very high levels. Level of E2 (pg / ml) Rate of OHSS (%) 3500 3500 – 5999 1.5 6000 38 Delvigne A, RBM Online, 2009, 19: 8 – 13. Papanikolaou EG et al, F&S, 2006, 85: 112 – 20. Asch RH, et al, HR, 1991, 6: 1395 – 9.
 Rate of OHSS (%) – Delvigne A, RBM Online, 2009, 19: 8 – 13. Papanikolaou EG et al, F&S, 2006, 85: 112 – 20. Asch RH, et al, HR, 1991, 6: 1395 – 9.")
28
OHSS-Ön Bulgular Abdominal ağrı Kilo alımı Karın çevresinde artış
Sişkinlik Gaz sikayetleri İstahsızlık Bulantı Engin bey şuan ki Halim bu durumda gerçekten patlamak üzereyim:(Ne zaman geçecek dersiniz,asla ne gündüz ne geceleri uyku uyuyamıyorum,ne sağa ne solo dönebiliyorum,bir nebze olsun rahatlatıcı birşey yokmudur yapılabilecek?

29
OHSS ÖNLEME STRATEJİLERİ
Siklus iptali “Coasting” yaklaşımı Düşük doz Gn kullanımı- mild stimülasyon Ovülasyon tetiklemesine farklı ajanlar kullanmak (GnRh-agonist) HCG dozunun azaltılması IV human albumin veya hidroksiasetil starch Dopamin agonistleri Tüm embriyoları dondurmak /sayısını Erken follikul aspirasyonu Luteal faz desteği için HCG yerine P verilmesi Laparaskopik ovarian drilling IVM Diğer farmakolojik ajanlar (Metformin, ASA vs.)
 HCG dozunun azaltılması. IV human albumin veya hidroksiasetil starch. Dopamin agonistleri. Tüm embriyoları dondurmak /sayısını Erken follikul aspirasyonu. Luteal faz desteği için HCG yerine P verilmesi. Laparaskopik ovarian drilling. IVM. Diğer farmakolojik ajanlar (Metformin, ASA vs.)")
30
OHSS önlenebilir mi? Non-IVF siklüsleri
Düşük doz step-up protokol: Amaç monofolliküler gelişmedir. Bu protokolde obes olgularda iptal sayısı artmış olmakla birlikte, çoğul gebelikler ve OHSS insidansı düşmüştür. Hiperinsülinemik-PCOS olguları normoinsülinemik-PCOS olgularından daha çok OHSS riski altındadır.

31
Insulin resistance to predict OHSS in PCOS
Normo-insulinaemic (n = 21) Hyper-insulinaemic (n = 31) P value Mean total dose of HMG ± SD (IU) 1395 ± 472 1507 ± 727 NS Mean dose/BMI ± SD (IU/BMI) 57.7 ± 18.7 54 ± 18 Ovulation rate (n/cycle) 85.7 % (18/21) 83.8% (26/31) OHSS rate 23.8 % (5/21) 64.5 % (20/31) <0.05 * Pregnancy rate 28.5 % (6/21) 16% (5/31) Abortions (n/pregnancies) 16.6 % (1/6) 20% (1/5) Felghesu et al. JCEM 82: 644, 1997
 Hyper-insulinaemic. (n = 31) P value. Mean total dose of HMG ± SD (IU) 1395 ± ± 727. NS. Mean dose/BMI ± SD (IU/BMI) 57.7 ± ± 18. Ovulation rate. (n/cycle) 85.7 % (18/21) 83.8% (26/31) OHSS rate % (5/21) 64.5 % (20/31) <0.05 * Pregnancy rate % (6/21) 16% (5/31) Abortions. (n/pregnancies) 16.6 % (1/6) 20% (1/5) Felghesu et al. JCEM 82: 644,")
32
PRIMARY PREVENTION Variables FSH dose individualizing
Mild / minimal stimulation The way of pituitary suppresion (agonist / antagonist) Avoidance of hCG for LPS IVM Insulin-sensitizing agents
 Avoidance of hCG for LPS. IVM. Insulin-sensitizing agents.")
33
FSH versus HMG to prevent OHSS
Nugent et al, Cochrane Database: Issue 1, 2009

35
GnRHa v/s antagonists to prevent OHSS, 2009
Al-Inany et al, Cochrane Database: Issue 1, 2009

36
GnR a v/s antagonists to prevent OHSS, 2011
Al-Inany et al, Cochrane Database Syst Rev 11;(5):CD001750, 2011 36
:CD001750,")
37
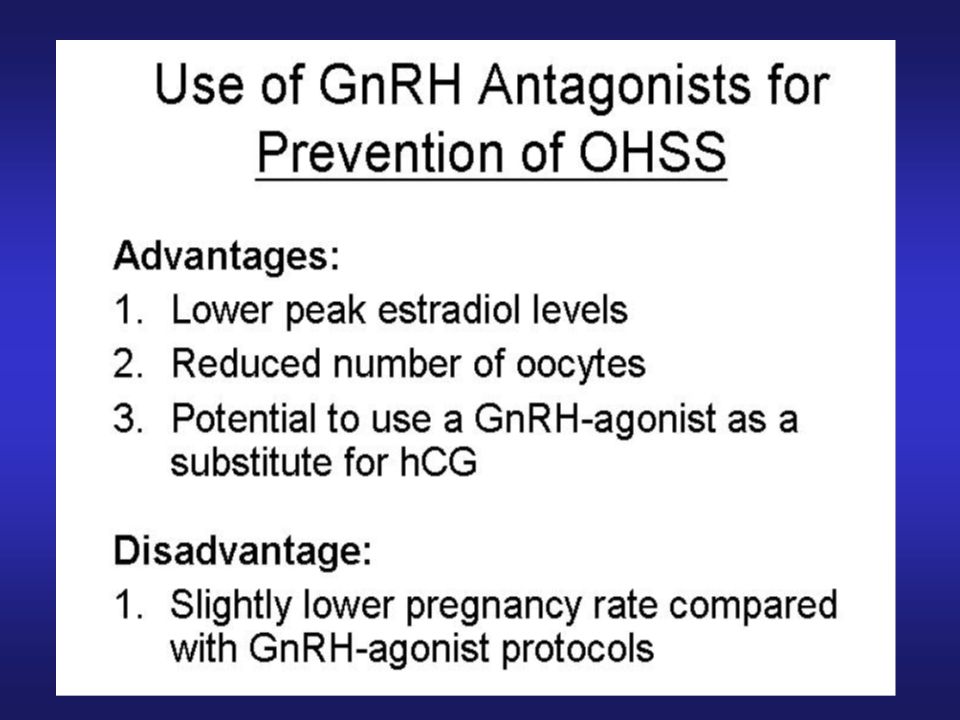
PRIMARY PREVENTION GnRH antagonist protocols
OR (95 CI%) in antagonist cycles Risk of OHSS 0.50 (0.37 – 0.66) Cancellation or coasting due to high risk to develop OHSS 0.53 (0.36 – 0.78) Al-Inany HG et al, HRU, 2011, 17(4), 435
 in antagonist cycles. Risk of OHSS (0.37 – 0.66) Cancellation or coasting due to high risk to develop OHSS (0.36 – 0.78) Al-Inany HG et al, HRU, 2011, 17(4), 435.")
38
OHSS önlenebilir mi? Metformin Cochrane 2009
Metformin : hiperinsulinemi ↓↓ ve hiperandrojenemi ↓↓ Metformin YÜT öncesi veya sonrasında Gebelik oranı aynı OR:0.71 (95% CI 0.39 to 1.28)NS Canlı Doğum aynı OR:0.77( 95% CI )NS OHSS↓↓ PKOS +metformin OR 0.27 (95% CI ). Metformin treatment before and during IVF or ICSI in women with polycystic ovary syndrome.(Tso L et al.2009)
NS. Canlı Doğum aynı OR:0.77( 95% CI )NS. OHSS↓↓ PKOS +metformin OR 0.27 (95% CI ). Metformin treatment before and during IVF or ICSI in women with polycystic ovary syndrome.(Tso L et al.2009)")
39
IVF-ICSI Sikluslarında Gn-Metformin BJOG-2013
10 RKÇ- 845 PCOS Gebelik (OR:1.20 CI: ) ve canlı doğum (OR:1.69 CI: ) oranlarına etkisi yok Metformin dozu, kullanım süresi ve ne zaman kesildiğinin önemi yok OHSS riskini azaltıyor. OR:0.27 CI: Abortus oranını azaltıyor: OR:0.50 CI: İmplantasyon oranlarını arttırıyor: OR 1.42 CI:
 ve canlı doğum (OR:1.69 CI: ) oranlarına etkisi yok. Metformin dozu, kullanım süresi ve ne zaman kesildiğinin önemi yok. OHSS riskini azaltıyor. OR:0.27 CI: Abortus oranını azaltıyor: OR:0.50 CI: İmplantasyon oranlarını arttırıyor: OR 1.42 CI:")
40
SECONDARY PREVENTION Variables
Coasting Reducing hCG dose Cryopreservation of embryos Cycle cancellation Alternative agents for triggering Albumin and starch Dopamine agonists Others Unilateral follicle aspiration before HCG Laparoscopic ovarian electro-cautery

41
Önlem Stratejileri Siklus iptali: OHSS, hCG ile ilişkilidir.
hCG, VEGF üretimini tetikler ve bu en önemli medyatörüdür. OHSS önlemede hCG triggerinin iptali en etkin yöntemdir. Ancak masraflı ve psikolojik olarak güçtür. Sadece yüksek OHSS riski olan veya siklus kontrolü tamamen kaybedilmiş hastalarda tercih edilmelidir.

43
Antagonist sikluslarında analog ile tetikleme
Ovulasyon agonistin flare-up etkisi ile tetiklenir : 0,2 mg triptorelin 0,5 mg buserelin 1-2 mg leuprolide acetat

44
P:0.05 favors lower risk after hCG
GnRH agonist for triggering final oocyte maturation in the GnRH antagonist ovarian hyperstimulation protocol: a systematic review and meta-analysis P<0.03 favors hCG P:0.05 favors lower risk after hCG Triggering final oocyte maturation with GnRH agonist during ovarian stimulation is feasible when inhibition of premature LH surge is performed with GnRH antagonists, and we aimed to systematically collate evidence on the clinical efficacy of GnRH agonist triggering in patients undergoing assisted reproduction in GnRH antagonist protocols. Twenty-three publications were identified by a comprehensive literature search that included PubMed, Embase and the Cochrane Library. Three publications out of 23 fulfilled the inclusion criteria for meta-analysis, which were (i) prospective, randomized controlled study design; (ii) stimulation with gonadotropins for induction of multifollicular development; (iii) suppression of endogenous LH by a GnRH antagonist; (iv) triggering of final oocyte maturation with GnRH agonist; (v) control group randomized to receive HCG for final oocyte maturation and (vi) any means of luteal phase support other than HCG. The participants were normoovulatory women undergoing IVF. The outcomes assessed were clinical pregnancy per randomized patient; number of oocytes retrieved; proportion of metaphase II oocytes; fertilization rate; embryo quality score; first trimester abortion rate; ovarian hyperstimulation syndrome (OHSS) incidence. Results are presented as combined standardized differences of the mean and combined odds ratios, as appropriate, with 95% confidence intervals. No significant difference was found for the number of oocytes retrieved (–0.94,–0.33–0.14), proportion of metaphase II oocytes (–0.03,–0.58–0.52), fertilization rate (0.15,–0.09–0.38) or embryo quality score (0.05,–0.18–0.29). No OHSS occurred in two of the studies, whereas in one study OHSS incidence was not reported. Thus from the available data, no conclusion can be drawn as regards OHSS incidence after GnRH agonist triggering. In comparison to HCG, GnRH agonist administration is associated with a significantly reduced likelihood of achieving a clinical pregnancy (0.21, 0.05–0.84;P=0.03). The odds of first trimester pregnancy loss is increased after GnRH agonist triggering; however, the confidence interval crosses unity (11.51,0.95–138.98; P=0.05). In conclusion, the use of GnRH agonist to trigger final oocyte maturation in IVF, where inhibition of premature LH surge is achieved with GnRH antagonists, yields a number of oocytes capable to undergo fertilization and subsequent embryonic cleavage, which is comparable to that achieved with HCG. However, the likelihood of an ongoing clinical pregnancy after GnRH agonist triggering is significantly lower as compared to standard HCG treatment. G.Griesinger, 2005
 prospective, randomized controlled study design; (ii) stimulation with gonadotropins for induction of multifollicular. development; (iii) suppression of endogenous LH by a GnRH antagonist; (iv) triggering of final oocyte maturation. with GnRH agonist; (v) control group randomized to receive HCG for final oocyte maturation and (vi) any means of. luteal phase support other than HCG. The participants were normoovulatory women undergoing IVF. The outcomes. assessed were clinical pregnancy per randomized patient; number of oocytes retrieved; proportion of metaphase II. oocytes; fertilization rate; embryo quality score; first trimester abortion rate; ovarian hyperstimulation syndrome. (OHSS) incidence. Results are presented as combined standardized differences of the mean and combined odds. ratios, as appropriate, with 95% confidence intervals. No significant difference was found for the number of oocytes. retrieved (–0.94,–0.33–0.14), proportion of metaphase II oocytes (–0.03,–0.58–0.52), fertilization rate (0.15,–0.09–0.38) or embryo quality score (0.05,–0.18–0.29). No OHSS occurred in two of the studies, whereas in one study OHSS incidence. was not reported. Thus from the available data, no conclusion can be drawn as regards OHSS incidence after. GnRH agonist triggering. In comparison to HCG, GnRH agonist administration is associated with a significantly. reduced likelihood of achieving a clinical pregnancy (0.21, 0.05–0.84;P=0.03). The odds of first trimester pregnancy. loss is increased after GnRH agonist triggering; however, the confidence interval crosses unity (11.51,0.95–138.98; P=0.05). In conclusion, the use of GnRH agonist to trigger final oocyte maturation in IVF, where inhibition of premature. LH surge is achieved with GnRH antagonists, yields a number of oocytes capable to undergo fertilization and subsequent. embryonic cleavage, which is comparable to that achieved with HCG. However, the likelihood of an ongoing. clinical pregnancy after GnRH agonist triggering is significantly lower as compared to standard HCG treatment. G.Griesinger,")
45
GnRH agonist for triggering final oocyte maturation in patients at risk of ovarian hyperstimulation syndrome: still a controversy S. Kol, 2008

46
GnRH agonists to trigger ovulation (8 RCTs Fresh ET, 3 RCTS donors)
OHSS incidence per randomised woman OR = 0.10 (95% CI = 0.01 to 0.82) * GnRH agonist versus HCG (LBR) OR = 0.44 (95% CI = 0.29 to 0.68) * GnRH agonist versus HCG (OPR) OR = 0.45 (95% CI = 0.31 to 0.65) * Youssef et al, Cochrane Database Syst Rev 10;(11):CD008046, 2010 46
 * GnRH agonist versus HCG (LBR) OR = 0.44 (95% CI = 0.29 to 0.68) * GnRH agonist versus HCG (OPR) OR = 0.45 (95% CI = 0.31 to 0.65) * Youssef et al, Cochrane Database Syst Rev 10;(11):CD008046,")
47
HCG veya GnRH Agonistleri Cochrane Data, 2011
OVULASYON TETİKLEMESİNDE HCG YERİNE GNRH AGONİSTLERİ KULLANIMI, CİDDİ OHSS RİSKİ DIŞINDA KULLANILMAMALIDIR. GNRH AGONİSTLERİ KULLANIMI İLE DAHA DÜŞÜK GEBELİK VE YÜKSEK DÜŞÜK ORANLARI ELDE EDİLMEKTEDİR.

50
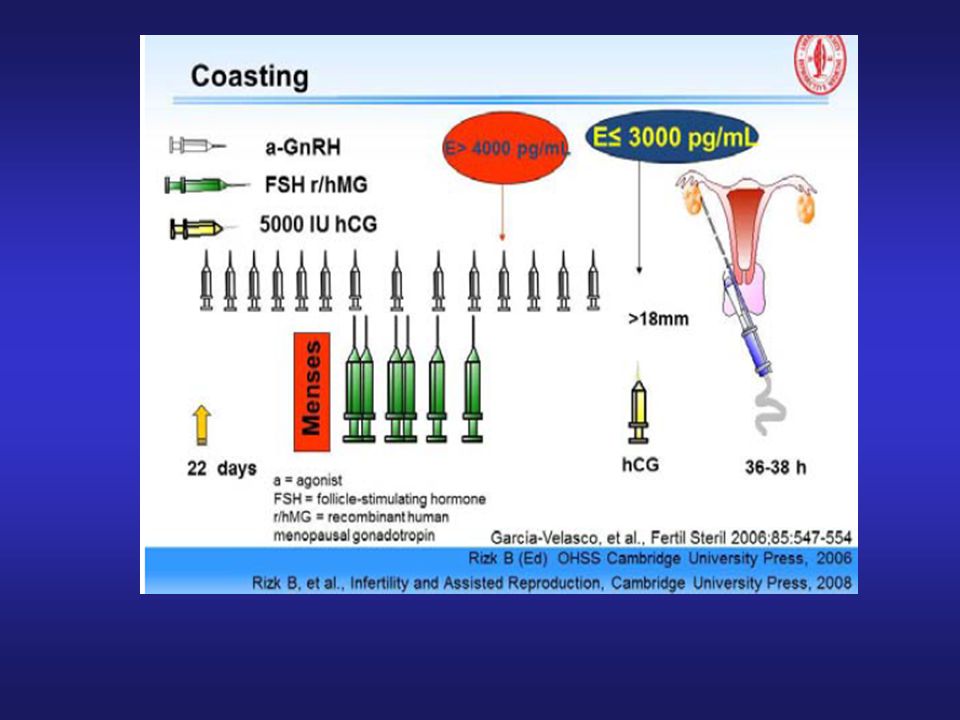
Önlem Stratejileri Coasting (gonadotropinleri geri çekmek)
Eksojen gonadotropinleri keserek, hCG triggerini hastanın E2 seviyesi daha güvenli bir aralığa indikten sonra kullanılır (genelde 3000 pg/nL). GnRH agonistine devam edilir. Apoptoz ve atreziye daha dirençli büyük foliküller, FSH seviyesi düşerken büyümeye devam ederler. 3-4 günden fazla uygulamanın gebelik ve implantasyon oranını düşürdüğü araştırmalarda belirtilmiştir Taze embriyo transferine olanak tanır OHSS insidansını azaltsa da tamamen elimine etmez Ani E2 düşmesi gebelik prognozu açısından kötü E2 düzeyi hala arttmaya devam ediyorsa coasting bir işe yaramaz
. GnRH agonistine devam edilir. Apoptoz ve atreziye daha dirençli büyük foliküller, FSH seviyesi düşerken büyümeye devam ederler. 3-4 günden fazla uygulamanın gebelik ve implantasyon oranını düşürdüğü araştırmalarda belirtilmiştir. Taze embriyo transferine olanak tanır. OHSS insidansını azaltsa da tamamen elimine etmez. Ani E2 düşmesi gebelik prognozu açısından kötü. E2 düzeyi hala arttmaya devam ediyorsa coasting bir işe yaramaz.")
52
García-Velasco, 2006

53
Coasting to prevent OHSS (Cochrane)
Incidence of OHSS OR = 0.53 (95% CI = 0.23 to 1.23) Live birth rate OR = 0.48 (95% CI = 0.14 to 1.62) Clinical pregnancy rate OR = 0.69 (95% CI = 0.44 to 1.08) Oocytes retrieved OR = (95% CI to -3.37) * D’Angelo et al, Cochrane Database Syst Rev 15;(6):CD002811, 2011
 Live birth rate. OR = 0.48 (95% CI = 0.14 to 1.62) Clinical pregnancy rate. OR = 0.69 (95% CI = 0.44 to 1.08) Oocytes retrieved. OR = (95% CI to -3.37) * D’Angelo et al, Cochrane Database Syst Rev 15;(6):CD002811,")
54
Coasting (withholding gonadotrophins) for preventing ovarian hyperstimulation syndrome
There was no evidence to suggest a benefit of using coasting to prevent OHSS compared with no coasting or other interventions.

55
rhCG ile ovulasyonun tetiklenmesi
Metaanaliz (Al-Inany et al., 2005) n=747 OHSS: rHCG vs üriner HCG (%3,3 vs %1,9) Fark yok 500μg rHCG vs 250μg OHSS: 3,4 vs 1,1
 n=747. OHSS: rHCG vs üriner HCG (%3,3 vs %1,9) Fark yok. 500μg rHCG vs 250μg. OHSS: 3,4 vs 1,1.")
56
OHSS Önlenmesinde HCG Doz Azaltılması
OHSS önlenmesinde düşük doz HCG etkilidir, Düşük doz HCG; Oosit kalitesini, Embryo sayı ve kalitesini, Klinik gebelik oranlarını bozmamaktadır. Kashyap S, Seminars in Reproductive Medicine, 2010

57
REDUCING THE hCG DOSE Cornell protocol E2 (pmol/ml) uHCG dose (IU)
≥ Coasting or cancellation 7000 – 3300 – 4000 4000 – 7000 5000 4000 10.000

58
OHSS önlenebilir mi? Albumin:
Plasma onkotik basıncını artırarak ekstravasküler alana sıvı geçişini engeller. Kapiller permeabiliteyi arttıran sitokinlere bağlanır 50gr albumin 15dk içinde 800ml sıvıyı intravasküler alana çeker 18 ciddi OHSS gelişme riskindeki olgu için 1 olgu da önleme sağlanabilmektedir. (2002) Uygulamada: OPU da 50 gr Albumin iv yada 50 gr+500 cc SF de dilüe olunarak verilebilinir. Yan etkileri: Bulantı,kusma,ateş,allerjik reaksiyon,Anaflaktik şok,Virus geçişi
 Uygulamada: OPU da 50 gr Albumin iv yada 50 gr+500 cc SF de dilüe olunarak verilebilinir. Yan etkileri: Bulantı,kusma,ateş,allerjik reaksiyon,Anaflaktik şok,Virus geçişi.")
60
OHSS önlenebilir mi? Proflaktik Hydroxyetil starch (HES):
İntravasküler hacmi ve onkotik basıncı artırır. Serum yarı ömrü 10saat Trombosit agregasyonunu engeller 1000 ml solüsyon OPU günü iv verilir (2 saatde) ve 48 saat sonra 500ml daha uygulanır. Ciddi OHSS de fark olmamasına karşı , Orta derecede OHSS azalma olmaktadır, Albumin ve plasebodan daha etkindir. Avantajı: enfeksiyon riski yok, albuminden daha ucuz
 ve 48 saat sonra 500ml daha uygulanır. Ciddi OHSS de fark olmamasına karşı , Orta derecede OHSS azalma olmaktadır, Albumin ve plasebodan daha etkindir. Avantajı: enfeksiyon riski yok, albuminden daha ucuz.")
61
SECONDARY PREVENTION ALBUMIN AND STARCH
Type of treatment No. Of trials OR of OHSS Human albumin 8 0.67 (0.45 – 0.99) Hydroxyethyl starch 3 0.12 (0.04 – 0.40) Youssef MAFM, Cochrane review, 2011.
 Hydroxyethyl starch (0.04 – 0.40) Youssef MAFM, Cochrane review,")
62
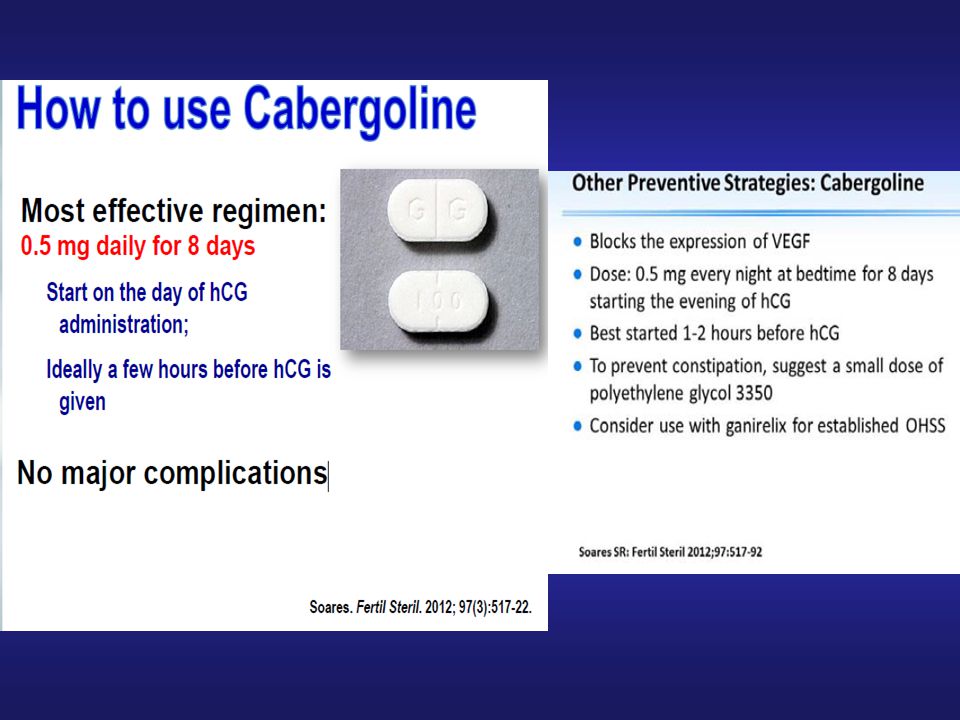
OHSS önlenebilir mi? Dopamin-agonist(Cabergoline):
hCG trigger gününden itibaren cabergolin gibi bir dopamin agonisti kullanımının OHSS insidansını azalltığı gözlemlenmiştir. Buna sebep hCG’ye cevap esnasındaki VEGFR-2 fosforilasyonunun önlenmesi olabilir. FDA kategori B Yan etki :Hpt, ergo deriveleri hipersensitivitesi Erken başlangıçlı OHSS de önemli azalma var Geç başlangıçlı OHSS de önemli farklılık yok.

63
Cabergoline for preventing ovarian hyperstimulation syndrome
Cabergoline for preventing ovarian hyperstimulation syndrome Tang H, Hunter T, Hu Y, Zhai SD, Sheng X, Hart RJ. ÇALIŞMA 230 OLGU ORAL CABERGOLİNE mg /GÜN VS PLASEBO OHSS ↓ ↓cabergoline grubunda (OR 0.40, 95% CI ) Orta OHSS ↓cabergoline grubunda (OR 0.38, 95% CI ) Ancak şiddetli OHSS aynı (OR 0.77, 95% CI ) ns Klinik gebelik aynı (OR 0.94, 95% CI 0.56 to 1.59) ns Abortus oranı aynı (OR 0.31, 95% CI 0.03 to 3.07) ns
 Orta OHSS ↓cabergoline grubunda (OR 0.38, 95% CI ) Ancak şiddetli OHSS aynı (OR 0.77, 95% CI ) ns. Klinik gebelik aynı (OR 0.94, 95% CI 0.56 to 1.59) ns. Abortus oranı aynı (OR 0.31, 95% CI 0.03 to 3.07) ns.")
65
Cabergoline reduces the occurrence of moderate-severe OHSS (RR 0
Cabergoline reduces the occurrence of moderate-severe OHSS (RR 0.38, 95% CI 0.29–0.51, 7 studies, 858 women) . Cabergoline is unlikely to have a clinically relevant negative impact on clinical pregnancy or on the number of retrieved oocytes. However, we are still uncertain of its impact on live birth, miscarriage, and congenital abnormalities. Objective: To evaluate the efficacy and safety of using cabergoline for reducing the risk of ovarian hyperstimulation syndrome (OHSS). Design: Systematic review and meta-analysis of randomized clinical trials (RCTs). Patients: Women submitted to controlled ovarian stimulation (COS) for assisted reproduction. Interventions: Cabergoline. Setting: Fertility centers. Main outcome measures: Moderate-severe OHSS, live birth, clinical pregnancy, number of retrieved oocytes, miscarriage, congenital abnormalities. Comparisons were performed with the use of risk ratios (RRs) or mean differences (MDs) and their respective 95% confidence intervals (CIs). Result(s): Eight RCTs were considered to be eligible; data from seven studies could be extracted and included in the meta-analysis. Cabergoline reduces the risk of moderate-severe OHSS (RR 0.38, 95% CI 0.29–0.51, 7 studies, 858 women) and probably has no clinically relevant negative impact on clinical pregnancy (RR 1.02, 95% CI 0.78–1.34, 4 studies, 561 women) or on the number of retrieved oocytes (MD 1.15, 95% CI 0.76 to 3.07, 5 studies, 628 women). However, our estimates were imprecise for distinguishing between substantial harm, no effect, and substantial benefit considering live birth (RR 1.03, 95% CI 0.71–1.48, 1 study, 200 women), and miscarriage (RR 0.69, 95% CI 0.27 to 1.76, 3 studies, 194 pregnant women). No studies reported congenital abnormalities. Conclusion(s): Cabergoline reduces the occurrence of moderate-severe OHSS. Cabergoline is unlikely to have a clinically relevant negative impact on clinical pregnancy or on the number of retrieved oocytes. However, we are still uncertain of its impact on live birth, miscarriage, and congenital abnormalities. (Fertil Steril 2013
 . Cabergoline is unlikely to have a clinically relevant negative impact on clinical pregnancy or on the number of retrieved oocytes. However, we are still uncertain of its impact on live birth, miscarriage, and congenital abnormalities. Objective: To evaluate the efficacy and safety of using cabergoline for reducing the risk of ovarian hyperstimulation syndrome (OHSS). Design: Systematic review and meta-analysis of randomized clinical trials (RCTs). Patients: Women submitted to controlled ovarian stimulation (COS) for assisted reproduction. Interventions: Cabergoline. Setting: Fertility centers. Main outcome measures: Moderate-severe OHSS, live birth, clinical pregnancy, number of retrieved oocytes, miscarriage, congenital. abnormalities. Comparisons were performed with the use of risk ratios (RRs) or mean differences (MDs) and their respective 95% confidence intervals (CIs). Result(s): Eight RCTs were considered to be eligible; data from seven studies could be extracted and included in the meta-analysis. Cabergoline reduces the risk of moderate-severe OHSS (RR 0.38, 95% CI 0.29–0.51, 7 studies, 858 women) and probably has no. clinically relevant negative impact on clinical pregnancy (RR 1.02, 95% CI 0.78–1.34, 4 studies, 561 women) or on the number of. retrieved oocytes (MD 1.15, 95% CI 0.76 to 3.07, 5 studies, 628 women). However, our estimates were imprecise for distinguishing. between substantial harm, no effect, and substantial benefit considering live birth (RR 1.03, 95% CI 0.71–1.48, 1 study, 200. women), and miscarriage (RR 0.69, 95% CI 0.27 to 1.76, 3 studies, 194 pregnant women). No studies reported congenital abnormalities. Conclusion(s): Cabergoline reduces the occurrence of moderate-severe OHSS. Cabergoline is unlikely to have a clinically relevant. negative impact on clinical pregnancy or on the number of retrieved oocytes. However, we. are still uncertain of its impact on live birth, miscarriage, and congenital abnormalities. (Fertil Steril")
66
OHSS önlenebilir mi? LUTEAL FAZ DESTEĞİ :PROGESTERON
YÜKSEK DOZ İNTRAMÜSKÜLER PROGESTERON OHSS ANTİÖSTROJENİK ETKİ PRORENİN GİBİ OVARYAN HORMONLARIN İNHİBİSYONU ALDOSTERON ANTAGONİSTİ

67
Long GnRH agonist protokol alan yüksek riskli hastalara GnRH antagonist uygulaması
E2 de hızlı düşüş Şiddetli OHSS de azalma Devam eden gebelik 51.8 %. Gustofson et al 2006, Aboulghar et al., 2007 ANTAGONİST KULLANIMI COASTING KADAR ETKİN

68
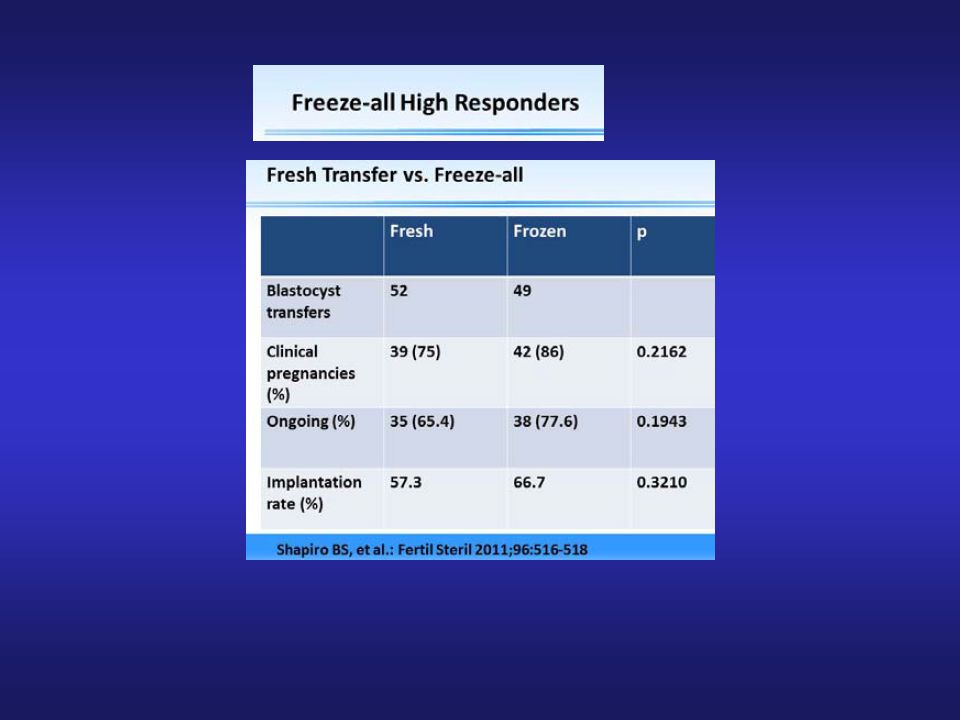
Tüm Embriyoları Dondurmak
Erken OHSS’ i engellemez Geç OHSS’yi engeller.

71
(Remington 1997) LOD OHSS riski olmadan unifoliküler gelişim için alternatif bir tedavidir OHSS’ yi önleme konusunda IVF sikluslarında rutin kullanımı için data yetersiz Sağlıklı over dokusuna da zarar verilmesi, postoperatif adezyon gelişimi nedeni ile kullanımı sınırlı Farquar,2004,Mathur,2007

74
Gebelik-OHSS Gebe kalınan sikluslarda OHSS daha fazla (2-5 kat)
Gebe kalınan sikluslarda OHSS şiddeti daha fazla OHSS sikluslarında multiple gebelik %

75
FINAL REMARKS Primary risk factor Secondary risk factor
Primary prevention Secondary prevention AFC E2 + no. of follicle Metformin Alternative triggering AMH GnRH antagonist Dopamine agonists History Mild /minimal stimulation HES Cryopreservation

Benzer bir sunumlar