Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Endometrioma : İnfertilite Açısından Güncel Yaklaşım
Doç. Dr. L. Cem Demirel Memorial Ataşehir Hastanesi IVF Departmanı TJOD Antalya

2
Hedefler Endometriomanın üreme fonksiyonlarına etkisinin değerlendirilmesi Endometrioma cerrahisinin over rezervi üzerine etkileri Farklı cerrahi yöntemlerin karşılaştırılması Endometrioması olan infertil hastada cerrahi – ART sonuçlarının karşılaştırması

3
Endometriotik kistin özelliklerine göre ovülasyonun olduğu taraf
Özellik sayı tutulmuş overde ovülasyon N. (%) p değeri Tüm kohort (31) Kistleri sayısı (35) ≥ (19) Kist çapı < 30 mm (34) ≥ 30 mm 25 9 (36) 0.162 Kist çapı datası yalnızca bir endometrioması olan kadınlardan elde edilen data Benaglia et al, HR 2009 xxxxxsedcrtfvgb jnkml,
 p değeri Tüm kohort (31) Kistleri sayısı (35) ≥ (19) Kist çapı < 30 mm (34) ≥ 30 mm 25 9 (36) Kist çapı datası yalnızca bir endometrioması olan kadınlardan elde edilen data. Benaglia et al, HR xxxxxsedcrtfvgb jnkml,")
4
Kist olan ve olmayan karşıt overdeki antral folikül sayımı
kist olan over kist olmayan over p Fonksiyonel kist (n:198) 8.5 ± ± Endometrioma (n:53) 7.5 ± ± Dermoid kist (n:14) ± ± Multiloküle kist (n: 8) 7.2 ± ± Almog et al, Fertil Steril 2010
 8.5 ± ± Endometrioma (n:53) 7.5 ± ± Dermoid kist (n:14) 11.9 ± ± Multiloküle kist (n: 8) 7.2 ± ± Almog et al, Fertil Steril")
5
Hwu et al, Reprod Biol Endocrinol, 2011
Opere edilmemiş tek taraflı ve çift taraflı endometriomaların over rezervine etkileri unilateral bilateral endometrioma grubu endometrioma grubu (n: 109) (n: 32) Ortalama serum AMH düzeyi (ng/mL) 2.45 ± ± 0.24 * * P < 0.05 Hwu et al, Reprod Biol Endocrinol, 2011
 (n: 32) Ortalama serum. AMH düzeyi (ng/mL) 2.45 ± ± 0.24 * * P < Hwu et al, Reprod Biol Endocrinol,")
6
Laparotomi ve laparoskopi ile çıkartılan over kistlerinde eksizyona istemsiz dahil olan over dokusunun karşılaştırılması Over kistinin tipi Laparoskopi Laparotomi (n = 150) (n = 110) Endometrioma 49 / 75 (% 65) 40 / 50 (% 80) Non-endometrioma 24 / 75 (% 32) 25 / 60 (%41) Alborzi et al, Fertil Steril 2009
 (n = 110) Endometrioma 49 / 75 (% 65) 40 / 50 (% 80) Non-endometrioma 24 / 75 (% 32) 25 / 60 (%41) Alborzi et al, Fertil Steril 2009")
7
Laparoskopik olarak eksize edilen ovarian endometriotik kistlerin histopatolojik analizi (48 kadında) parietal adezyon kistin orta over hilusunda bölgesi kısmı kist duvarı Doku kalınlığı (mm) 1.2 ± ± ± 0.6 Over dokusu varlığı Over dokusu 0.30 ± ± ± 0.36 kalınlığı (mm) Over dokusu A area around the site of parieatal adhesions,where the cyst invagination originates. B intermediate area corresponding to the largest cyst surface C perihilar area with incerased capsule thickness , adhesion, vascularization and follciluar content xxxxxsedcrtfvgb jnkml,
 1.2 ± ± ± 0.6 Over dokusu varlığı Over dokusu 0.30 ± ± ± 0.36 kalınlığı (mm) Over dokusu A area around the site of parieatal adhesions,where the cyst invagination originates. B intermediate area corresponding to the largest cyst surface. C perihilar area with incerased capsule thickness , adhesion, vascularization and follciluar content. xxxxxsedcrtfvgb jnkml,")
8
Hwu et al, Reprod Biol Endocrinol, 2011
Opere edilmemiş ve eksize edilmiş endometrioması olan kadınların ortalama serum AMH düzeylerinin (ng /mL) kontroller ile karşılaştırılması kontrol opere edilmemiş kistektomi p grubu endometrioma grubu geçirmiş grup (n:1323) (n:141) (n:147) < 30 yaş 3.94 ± ± ± 0.25 < yaş 3.31 ± ± ± 0.14 <.001 > 36 yaş 1.98 ± ± ± 0.07 <.001 Hwu et al, Reprod Biol Endocrinol, 2011
 kontroller ile karşılaştırılması. kontrol opere edilmemiş kistektomi p grubu endometrioma grubu geçirmiş grup (n:1323) (n:141) (n:147) < 30 yaş 3.94 ± ± ± 0.25 < yaş 3.31 ± ± ± 0.14 <.001 > 36 yaş 1.98 ± ± ± 0.07 <.001 Hwu et al, Reprod Biol Endocrinol,")
9
Horikawa et al, J Assist Reprod Genet 2008
Tek taraflı endometriomalarda cerrahi öncesi ve sonrası ovülasyon tarafı etkilenmiş gonad intakt gonad (%) (%) Cerrahi öncesi Cerrahi sonrası 17 83 Horikawa et al, J Assist Reprod Genet 2008
 (%) Cerrahi öncesi Cerrahi sonrası Horikawa et al, J Assist Reprod Genet")
10
Endometriomaların eksizyonunun ardından ciddi over hasarı oranı
Cerrahinin over hasarı yapma mekanizmaları: Kistektomi sırasında sağlıklı over dokusunun aynı anda çıkartılması Hemostaz için elektrokoagülasyonun kullanılmasının foliküler deplesyon yapması Lkal enflamatuar reaksiyon sonucu gonadal vaskülarizasyon kaybı ve over fibrozisi Busacca et al. (% 2.4 cerrahi sonrası over yetmezliği) highlighted that women operated on for bilateral ovarian endometriomas may be at increased risk of premature ovarian failure. In one recent publication (33), it was reported that 54% of endometrioma cyst walls excised by stripping techniques also contained recognizable ovarian tissue. The potential for loss of ovarian reserve is particularly high if significant bleeding is encountered during the cyst wall dissection or the endometrioma is very large. It has been shown that surgery for endometrioma is not free of complications because there is a risk of postsurgical ovarian failure of 2.4% (72) and a 30.4% risk of disease recurrence (73). It has been reported that removing ovarian cysts that have well-defined ovarian capsules (dermoids, serous, and mucinous cysts) resulted in some ovarian tissue being removed in 6% of cases (37). Conversely, a small rim of tissue containing primordial follicles is removed in more than 50% of endometriomas Benaglia et al, HR 2010 xxxxxsedcrtfvgb jnkml,
 highlighted that women operated on for bilateral ovarian endometriomas may be at increased risk of premature ovarian failure. In one recent publication (33), it was reported that 54% of endometrioma cyst walls excised by stripping techniques also contained recognizable ovarian tissue. The potential for loss of ovarian reserve is particularly high if significant bleeding is encountered during the cyst wall dissection or the endometrioma is very large. It has been shown that surgery for endometrioma is not free of complications because there is a risk of postsurgical ovarian failure of 2.4% (72) and a 30.4% risk of disease recurrence (73). It has been reported that removing ovarian cysts that have well-defined ovarian capsules (dermoids, serous, and mucinous cysts) resulted in some ovarian tissue being removed in 6% of cases (37). Conversely, a small rim of tissue containing primordial follicles is removed in more. than 50% of endometriomas. Benaglia et al, HR xxxxxsedcrtfvgb jnkml,")
11
Vaporisation / coagulation better
Excision better Ovarian endometriotik kistlerin vaporizasyonunu eksizyonu ile karşılaştıran çalışmaların dökümü. Diamonds represent odds ratio of pregnancies and horizontal lines % 95 Cıs. in general endometrioma vaporization is performed using bipolar current; in this latter case, the postoperative results in terms of recurrences and fertility have been far from satisfactory (7, 18, 19). Conversely, when recent studies compared cystectomy with CO2 laser vaporization, the recurrence and pregnancy rates were found to be comparable (8), but preservation of antral follicles appeared to be superior with the ablative procedure (9). A large majority of surgeons have abandoned ablative techniques in their surgical treatment of ovarian endometriomas after two randomized controlled trials showed better outcomes after cyst excision when compared with cyst ablation (7, 18, 19). These studies reported that cystectomy has a more positive impact on postoperative pregnancy rate and on both pain and endometrioma recurrences, when compared with cyst wall vaporization using bipolar coagulation. Although the trials were well conducted and their conclusions consistent, it is probable that the negative results observed with the ablation technique were related to the use of bipolar current, which is most likely responsible for a deeper thermal effect than results from plasma energy or a CO2 laser. Furthermore, it has been demonstrated that laser vaporization in the hands of an experienced surgeon is associated with good results both in terms of recurrence risk and pregnancy rate (13). Taking into consideration that cystectomy leads to the removal of follicles close to the ovarian hilus (3), Donnez et al. (17) recently advocated a combined technique of cystectomy and vaporization of the cyst wall using a CO2 laser when approaching the ovarian hilus. In recent months, two randomized controlled studies have considerably rehabilitated the ablative technique. Carmona et al. (8) reported the results of a 5-year follow-up study in women free of surgical antecedents who were managed for unilateral endometriomas by either cystectomy or CO2 laser vaporization. Although at 1 year after surgery the rate of cyst recurrences in women managed by vaporization was higher than for those managed by cystectomy, both recurrence and pregnancy rates were comparable at 5 years after surgery. A second trial, which compared the postoperative variations of AFC and levels of antim€ullerian hormone (AMH) in 20 women who had been managed by either cystectomy or CO2 laser vaporization for bilateral ovarian endometriomas, reported better outcomes for the ablative procedure (9). These new studies suggest that the poor results reported for endometrioma vaporization by teams using bipolar coagulation should not be extrapolated to other energies such as the CO2 laser. These trials should not, however, exclude women with previous ovarian surgery or bilateral endometriomas, as these are the patients who most require surgical procedures that can spare the ovarian parenchyma to a greater extent than offered by cystectomy. Vercellini, HR 2009 xxxxxsedcrtfvgb jnkml,
. Conversely, when recent studies compared cystectomy with CO2 laser vaporization, the recurrence and pregnancy rates were found to be comparable (8), but preservation of antral follicles appeared to be superior with the ablative procedure (9). A large majority of surgeons have abandoned ablative techniques in their surgical treatment of ovarian endometriomas after two randomized. controlled trials showed better outcomes after cyst excision when compared with cyst ablation (7, 18, 19). These studies reported. that cystectomy has a more positive impact on postoperative pregnancy rate and on both pain and endometrioma recurrences, when compared with cyst wall vaporization using bipolar coagulation. Although the trials were well conducted and their conclusions consistent, it is probable that the negative results observed with the ablation technique were related to the use of bipolar current, which is most likely responsible for a deeper. thermal effect than results from plasma energy or a CO2 laser. Furthermore, it has been demonstrated that laser vaporization in the hands of an experienced surgeon is associated with good results both in terms of recurrence risk and pregnancy rate (13). Taking into consideration that cystectomy leads to the removal of follicles close to the ovarian hilus (3), Donnez et al. (17) recently advocated a combined technique of cystectomy and vaporization of the cyst wall using a CO2 laser when approaching the ovarian. hilus. In recent months, two randomized controlled studies have considerably rehabilitated the ablative technique. Carmona et al. (8) reported. the results of a 5-year follow-up study in women free of surgical antecedents who were managed for unilateral endometriomas by either cystectomy or CO2 laser vaporization. Although at 1 year after surgery the rate of cyst recurrences in women managed by vaporization was higher than for those managed by cystectomy, both recurrence and pregnancy rates were comparable at 5 years after surgery. A second trial, which compared the postoperative variations. of AFC and levels of antim€ullerian hormone (AMH) in 20 women who had been managed by either cystectomy or CO2 laser vaporization for bilateral ovarian endometriomas, reported better outcomes for the ablative procedure (9). These new studies suggest that the poor results reported for endometrioma vaporization by teams using bipolar coagulation should not be extrapolated to other energies such as the CO2 laser. These trials should not, however, exclude women with previous ovarian surgery or bilateral endometriomas, as these are the patients who most require surgical procedures that can spare the ovarian parenchyma to a greater extent than offered by cystectomy. Vercellini, HR xxxxxsedcrtfvgb jnkml,")
12
eksizyon lazer vaporizasyon
Endometriotik kistlerin eksizyonu ya da lazer vaporizasyonu yapılan kadınlarda over rezerv markerlarının karşılaştırılması eksizyon lazer vaporizasyon (n:10) (n:10) baseline 6 ay baseline 6 ay sonra sonra Antral folikül sayısı 2.0 ± ± ± ±0.8* AMH (ng/mL) 3.9 ± ± 0.2* 4.5 ± ±0.6 * P < 0.05 Vaporization of the internal wall was performed using a CO2 laser at a power Density of 30 W/cm2. The use of GnRH agonists before surgery is controversial. We used them in the present study because this has been considered a standard practice when treating endometriomas with CO2 laser but not with cystectomy (12). In our experience, the effect of 2-month GnRH agonist treatment on endometrioma size preceding surgery is small and clinically irrelevant Tsolakidis, FS 2010 xxxxxsedcrtfvgb jnkml,
 (n:10) baseline 6 ay baseline 6 ay. sonra sonra. Antral folikül sayısı 2.0 ± ± ± ±0.8* AMH (ng/mL) 3.9 ± ± 0.2* 4.5 ± ±0.6. * P < Vaporization of the internal wall was performed using a CO2 laser at a power Density of 30 W/cm2. The use of GnRH agonists before surgery is controversial. We used them in the present study because this has been considered a standard practice when treating endometriomas with CO2 laser but not with cystectomy (12). In our experience, the effect of 2-month GnRH agonist treatment on endometrioma size preceding surgery is small and clinically irrelevant. Tsolakidis, FS xxxxxsedcrtfvgb jnkml,")
13
Bilateral endometriotik kistleri olan kadınlarda endometrioma eksizyonu ile koagülasyonun karşılaştırılması kistektomi koagülasyon p grubu grubu Bazal folikül sayımı Over hacmi Toplanan oositleri Mevcut histopatolojik, sonografik ve hormonal verilere bakarak, gonadal hasar için en önemli kritik faktörün pseudokapsülün eksizyonundan sonra hemostaz için aşırı koagülasyona bağlı oluşan termal nekrozdur Var, et al FS 2011 xxxxxsedcrtfvgb jnkml,

14
Bilateral over kistlerinin tedavisinin ardından 12
Bilateral over kistlerinin tedavisinin ardından 12. ay ultrasonografi değerlendirmesi Li et al, FS, 2009

15
removal of the endometrioma wall or ablative surgery that entails opening the endometrioma and destroying the internal cyst wall by laser vaporization or bipolar coagulation. The depth of vaporization is shallow, as only the glandular epithelium and subjacent stroma need to be vaporized. We previously demonstrated that ablative surgery (CO2 laser vaporization) does not impair ovarian function, as evidenced by a normal ovarian response to gonadotropins and similar pregnancy rates after IVF in women undergoing endometrioma surgery according to our technique and control patients without endometriosis (3). However, ablative surgery may prove difficult because of the thickness and hypervascularization Of the cyst wall. Recently, a Cochrane Review reported a higher rate of recurrence after ablative surgery than cystectomy (4). We describe a mixed technique of excisional and ablative surgery (Fig. 1). A large part of the endometrioma is first excised according to the cystectomy technique. The endometrial cyst is opened and washed out with irrigation fluid. After identifying the plane of cleavage between the cyst wall and ovarian tissue by applying opposite bimanual traction and countertraction with two grasping forceps, providing strong but nontraumatic force, the inner lining of the cyst is stripped from the normal ovarian tissue. If the excision provokes bleeding or the plane of cleavage is not clearly visible, the cystectomy is stopped because of the risk of removing normal ovarian tissue containing primordial, primary, and secondary follicles along with the endometrioma. Thus, when approaching the hilus, where the ovarian tissue is more functional and the plane of cleavage less visible, resection of the dissected tissue (partial cystectomy) is performed. The stripping technique allows removal of 80%–90% of the cyst. After this first step (partial cystectomy), CO2 laser (Lumenis, London, United Kingdom) is used to vaporize the remaining 10%–20% of the endometrioma close to the hilus. Care must be taken to vaporize all the residual cyst wall to avoid recurrence. At the end of the procedure, the ovary is not sutured. xxxxxsedcrtfvgb jnkml,
 does not impair ovarian function, as evidenced by a normal ovarian response to gonadotropins and similar pregnancy rates after IVF in women undergoing endometrioma surgery according to our technique and control. patients without endometriosis (3). However, ablative surgery may prove difficult because of the thickness and hypervascularization. Of the cyst wall. Recently, a Cochrane Review reported a higher rate of recurrence after ablative surgery than cystectomy (4). We describe a mixed technique of excisional and ablative surgery (Fig. 1). A large part of the endometrioma is first excised. according to the cystectomy technique. The endometrial cyst is opened and washed out with irrigation fluid. After identifying the plane of cleavage between the cyst wall and ovarian tissue by applying opposite bimanual traction and countertraction with two grasping forceps, providing strong but nontraumatic. force, the inner lining of the cyst is stripped from the normal ovarian tissue. If the excision provokes bleeding or the plane of cleavage is not clearly visible, the cystectomy is stopped because of the risk of removing normal ovarian tissue containing primordial, primary, and secondary follicles. along with the endometrioma. Thus, when approaching the hilus, where the ovarian tissue is more functional and the plane of cleavage less visible, resection of the dissected tissue (partial cystectomy) is performed. The stripping technique allows removal of 80%–90% of the cyst. After this first step (partial cystectomy), CO2 laser (Lumenis, London, United Kingdom) is used to vaporize the remaining 10%–20% of the endometrioma close to the hilus. Care must be taken to vaporize all the residual cyst wall to avoid recurrence. At the end of the procedure, the ovary is not sutured. xxxxxsedcrtfvgb jnkml,")
16
kombine teknik karşı taraf normal
Unilateral endometrioması olan kadınlarda cerrahiden 6 ay sonra over volümü ve AFC kombine teknik karşı taraf normal (n = 20) overler (n = 20) Over hacmi ± ± 3.91 AFC ± ± 1.6 Donnez et al, FS 2010 However, in a very recent Cochrane Review, Hart et al. (4) concluded that excisional surgery of endometriomas results in a more favorable outcome than drainage and ablation in terms of recurrence, pain symptoms, subsequent spontaneous pregnancy in previously subfertile women, and ovarian response to stimulation. This review was based on three randomized studies comparing the two approaches of cystectomy and ablation by bipolar coagulation (17–19). Unfortunately, all three studies failed to prospectively analyze the ovarian reserve after surgery. Although these were randomized studies, we believe it is not possible to draw accurate conclusions from them. First of all, the number of cases was small. Second, ablation was performed by bipolar coagulation, not by laser. While a bipolar current can probably be used for ablation, care should be taken to avoid thermal damage as well as insufficient ablation, which could explain the high rate of recurrence observed in the Cochrane series. Third, the experience of the surgeons involved differed according to the technique used, which may also account for the high recurrence rate observed after ablative surgery. Close to the ovarian hilus, ovarian tissue removed along the endometrioma wall contained primordial, primary, and secondary follicles in 69% of cases (12). In the light of all this evidence, we can conclude that cystectomy may be destructive for the ovary, whereas ablation may be incomplete, with a greater risk of recurrence. The combined approach therefore takes the best elements from both techniques, while avoiding the risks. Indeed, according to our present data, this new technique appears to combine the best results of the stripping technique in terms of recurrence outcomes, since most of the cyst wall is excised, and of the ablation technique, since the hilar area of the ovary is spared from surgical damage. Clearly, such modified approaches need to be fully investigated, and a multicenter randomized controlled study could be conducted in the future to validate our findings xxxxxsedcrtfvgb jnkml,
 overler (n = 20) Over hacmi 7.45 ± ± AFC 5.5 ± ± 1.6. Donnez et al, FS However, in a very recent Cochrane Review, Hart et al. (4) concluded that excisional surgery of endometriomas results in a more favorable outcome than drainage and ablation in terms of recurrence, pain symptoms, subsequent spontaneous pregnancy in previously subfertile women, and ovarian. response to stimulation. This review was based on three randomized studies comparing the two approaches of cystectomy. and ablation by bipolar coagulation (17–19). Unfortunately, all three studies failed to prospectively analyze the ovarian reserve after surgery. Although these were randomized studies, we believe it is not possible to draw accurate conclusions from them. First of all, the number of cases was small. Second, ablation was performed by bipolar coagulation, not by laser. While a bipolar. current can probably be used for ablation, care should be taken to avoid thermal damage as well as insufficient ablation, which could explain the high rate of recurrence observed in the Cochrane series. Third, the experience of the surgeons involved differed according to the technique used, which may also account for the high recurrence rate observed after ablative surgery. Close to the ovarian hilus, ovarian tissue removed along the endometrioma wall contained primordial, primary, and secondary follicles in 69% of cases (12). In the light of all this evidence, we can conclude that cystectomy. may be destructive for the ovary, whereas ablation may be incomplete, with a greater risk of recurrence. The combined approach therefore takes the best elements from both techniques, while avoiding the risks. Indeed, according to our present data, this new technique appears to combine the best results of the stripping technique in terms of recurrence outcomes, since most of the cyst wall is excised, and of the ablation technique, since the hilar area of the ovary is spared from surgical damage. Clearly, such modified approaches need to be fully investigated, and a multicenter randomized controlled study could be conducted in the future to validate our findings. xxxxxsedcrtfvgb jnkml,")
17
et al., 2003; Garcia-Velasco and Somigliana, 2009).
Surgery for ovarian endometriomas may also be a risk factor for the ovarian reserve. One study demonstrated that the number of follicles greater than 15 mm was significantly reduced in the operated ovary when compared with the contralateral ovary. Studies evaluating this outcome in women who underwent monolateral excision of endometriotic cysts generally documented a relevant reduction in follicular development in operated gonads when compared with contralateral intact ovaries The clinical relevance of this finding remains however debated (Gupta et al., 2006; Tsoumpou et al., 2009). Indeed, a recent metanalysis confirmed a reduced responsiveness to hyperstimulation in women with ovarian endometriosis but failed to detect a detrimental impact on the rate of treatment success. The Odds Ratio (OR) [95% Confidence Interval (CI)] for pregnancy was 1.07 (0.63–1.31) (Gupta et al., 2006). In fact, as mentioned earlier, a recent metanalysis on this point reported a decreased folliculogenesis in women with ovarian endometriomas but failed to document an impact on pregnancy rate (Gupta et al., 2006). Using pathological sections of the ovarian cortex surrounding ovarian benign neoplasms, Maneschi et al. (1993) found a reduced follicular number and activity antecedent to surgery in endometriomas when compared with teratomas or benign cystadenomas. Moreover, in unoperated women with unilateral disease, responsiveness to ovarian hyperstimulation is reduced in the affected gonad by about 25% (Somigliana et al., 2006) and spontaneous ovulation occurs more frequently in the intact gonad with a ratio of 2:1 (Horikawa et al., 2008; Benaglia et al., 2009). Second, surgery may also injure the ovarian reserve. Given the abovementioned cases of post-surgical ovarian failure occurring soon after the intervention for bilateral endometriomas (Busacca et al., 2006; Di Prospero and Micucci, 2009), this aspect appears to be of utmost importance. A potential deleterious mechanism of surgery is the accidental removal of a consistent amount of ovarian tissue during cystectomy Primordial follicles are found in more than 50% of the endometriomas removed, probably due to the presence of ‘pseudocapsule’ which is, in fact, invaginated ovarian cortex (Brosens et al., 1996). Finally, the damage inflicted by surgery may be due not only to stripping and removal of healthy ovarian tissue, but also to the local inflammation and/or vascular injury secondary to electrosurgical coagulation (Wu et al., 2003; Garcia-Velasco and Somigliana, 2009). In conclusion, severe ovarian damage may occur in gonads operated for ovarian endometriomas. Even if our results would need to be confirmed in an unselected population, they at least allow us to state that this event is not rare. At present, there is evidence supporting that this damage may both precede and follow surgery, but the relative importance of these two pathogenic mechanisms has yet to be fully clarified. This point is of utmost relevance since the demonstration that surgery may be mainly responsible for the damage would strongly caution against systematic surgical removal of these lesions. In particular, a more conservative attitude would have to be considered in women with bilateral cysts, in those with small asymptomatic lesions and in those selected for IVF. xxxxxsedcrtfvgb jnkml,
. Indeed, a recent metanalysis confirmed a reduced responsiveness to hyperstimulation in women with ovarian endometriosis but failed to detect a detrimental impact on the rate of treatment success. The Odds Ratio (OR) [95% Confidence Interval (CI)] for pregnancy was 1.07 (0.63–1.31) (Gupta et al., 2006). In fact, as mentioned earlier, a recent metanalysis on this point reported a decreased folliculogenesis. in women with ovarian endometriomas but failed to document an impact on pregnancy rate (Gupta et al., 2006). Using pathological sections of the ovarian cortex surrounding ovarian benign neoplasms, Maneschi et al. (1993) found a reduced follicular number and activity antecedent to surgery in endometriomas when compared with teratomas or benign cystadenomas. Moreover, in unoperated. women with unilateral disease, responsiveness to ovarian hyperstimulation is reduced in the affected gonad by about 25% (Somigliana et al., 2006) and spontaneous ovulation occurs more frequently in the intact gonad with a ratio of 2:1 (Horikawa et al., 2008; Benaglia et al., 2009). Second, surgery may also injure the ovarian reserve. Given the abovementioned cases of post-surgical ovarian failure occurring soon after the intervention for bilateral endometriomas (Busacca et al., 2006; Di Prospero and Micucci, 2009), this aspect appears to be of utmost importance. A potential deleterious mechanism of surgery is the accidental removal of a consistent amount of ovarian tissue during cystectomy. Primordial follicles are found in more than 50% of the endometriomas removed, probably due to the presence of ‘pseudocapsule’ which is, in fact, invaginated ovarian cortex (Brosens et al., 1996). Finally, the damage inflicted by surgery may be due not only to stripping and. removal of healthy ovarian tissue, but also to the local inflammation and/or vascular injury secondary to electrosurgical coagulation (Wu. et al., 2003; Garcia-Velasco and Somigliana, 2009). In conclusion, severe ovarian damage may occur in gonads operated for ovarian endometriomas. Even if our results would need to be confirmed. in an unselected population, they at least allow us to state that this event is not rare. At present, there is evidence supporting that this. damage may both precede and follow surgery, but the relative importance of these two pathogenic mechanisms has yet to be fully clarified. This point is of utmost relevance since the demonstration that surgery may be mainly responsible for the damage would strongly caution. against systematic surgical removal of these lesions. In particular, a more conservative attitude would have to be considered in women with bilateral cysts, in those with small asymptomatic lesions and in those selected for IVF. xxxxxsedcrtfvgb jnkml,")
18
Bilateral endometrioma
SomiglianaHR, 2008 Endometriomas are mostly monolateral. Both gonads are indeed affected only in 19–28% of cases. The contralateral intact ovary may adequately supply for the reduced function of the affected one. Women selected for IVF–ICSI cycles who previously underwent bilateral endometriomas cystectomy were matched (1:2) for age and study period with patients who did not undergo prior ovarian surgery. Women operated on for bilateral endometriotic ovarian cysts had a higher withdrawal rate for poor response (P < 0.001
 for age and study period with patients who did not undergo prior ovarian surgery. Women operated on for bilateral endometriotic ovarian cysts had a higher withdrawal rate for poor response (P <")
19
Bilateral endometrioma: Operasyon?
Patients were included in the study only if they underwent stripping of the endometrioma. ). In these patients, despite the use of higher doses of gonadotrophins, the number of follicles (P ), oocytes retrieved (P ) and embryos obtained (P ) were significantly lower.
. In these patients, despite the use of higher doses of gonadotrophins, the number of follicles (P ), oocytes retrieved (P ) and embryos obtained (P ) were significantly lower.")
20
Bilateral endometrioma: Operasyon?
The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P ) and the delivery rate per started cycle was 4% and 17%, respectively (P ). CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas. In line with our hypothesis, recent evidence suggests that women operated on for bilateral endometriotic ovarian cysts may be at risk of severe ovarian function impairment (Busacca et al., 2006; Esinler et al., 2006). In the present study, it was shown that the ovarian reserve of previously operated gonads is significantly damaged. Finally, our study showed that the chances of pregnancy are significantly lower in affected women. We indeed documented a three-fold reduction in the clinical pregnancy rate and a four-fold reduction in the delivery rate. Surgery may directly affect ovarian reserve. A potential deleterious mechanism is the accidental removal of a consistent amount of ovarian tissue during cystectomy (Muzii et al., 2002). A further mechanism thatmay be responsible for the reduced ovarian reserve is represented by the damage that may be inflicted on the ovarian stroma and vascularization by both surgery-related local inflammation and electrosurgical coagulation during haemostasis. Using pathological sections of the ovarian cortex surrounding ovarian endometriomas, Maneschi et al. (1993) found a reduced number of follicles antecedent to surgery, suggesting that the disease may per se damage the ovary. Moreover, the presence of unoperated endometrioma is associated with a reduced responsiveness to gonadotrophins in IVF–ICSI cycles (Somigliana et al., 2006b).
 and the delivery rate per started cycle was 4% and 17%, respectively (P ). CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas. In line with our hypothesis, recent evidence suggests that women operated on for bilateral endometriotic ovarian cysts. may be at risk of severe ovarian function impairment (Busacca et al., 2006; Esinler et al., 2006). In the present study, it was shown that the ovarian reserve of previously operated gonads is significantly damaged. Finally, our study showed that the chances of pregnancy are significantly lower in affected women. We indeed documented. a three-fold reduction in the clinical pregnancy rate and a four-fold reduction in the delivery rate. Surgery may directly affect ovarian reserve. A potential deleterious mechanism is the accidental removal of a consistent amount of ovarian tissue during cystectomy (Muzii et al., 2002). A further mechanism thatmay be responsible for the reduced ovarian reserve is represented. by the damage that may be inflicted on the ovarian stroma and vascularization by both surgery-related local inflammation and electrosurgical coagulation during haemostasis. Using pathological sections of the ovarian cortex surrounding ovarian endometriomas, Maneschi et al. (1993) found a reduced number of follicles antecedent to surgery, suggesting that the disease may per se damage the ovary. Moreover, the presence of unoperated endometrioma is associated with a reduced responsiveness to gonadotrophins in IVF–ICSI cycles (Somigliana et al., 2006b).")
21
Cerrahi sonrası rekürrens
Değişik yayınlarda % arası rekürrens . Ameliyattan sonra. Evers, Br J Clin Pract 1991 xxxxxsedcrtfvgb jnkml,

22
Rekürensi olan (siyah) ve olmayan (gri) kadınlarda, opere edilmiş ve karşı taraf intakt overlerdeki folikül sayıları Somigliana, AJOG 2011

23
Ovarian tutulum için cerrahi (ASRM stage III-IV)
The benefit of excision of ovarian endometriomas is difficult to define due to multiple confounding factors and methodological drawbacks in the considered studies. Excision of rectovaginal endometriosis is of doubtful value and associated with worrying morbidity. Although it has been suggested that surgical excision might increase the chance of spontaneous conception (32), it is unclear whether the benefits of surgery derive principally from treatment of the endometrioma or more generally from concomitant lysis of adhesions, ablation of peritoneal endometriosis, and chromopertubation. Very different outcomes have been reported in uncontrolled studies evaluating the impact of laparoscopic treatment of ovarian endometriotic cysts on post-operative reproductive performance. Pregnancy rates vary from 30% (Marrs, 1991) to 67% (Beretta et al., 1998), with an overall weighted mean of about 50% (Fig. 3). Moreover, exclusion from the analysis of subjects lost to follow-up may enflate the purported benefit of surgery, as drop-outs notoriously have a worse prognosis. Publication bias (surgeons with suboptimal outcomes may be less willing to submit their data and may be less likely to have them published). The number of women with uni- or bilateral cysts is rarely specified. When a unilateral endometrioma was present, the operated gonad could have been damaged and pregnancy achieved as a result of the function of contra-lateral adnexa. lack of an adequately generated control group impedes measurement of the difference between post-operative and background spontaneous pregnancy rates. Noticeably, only such a difference, and not the total conception rate, may be ascribed to surgery. Accordingly, the potential absolute benefit increase over background pregnancy rate 12 months after surgery in women with patent tubes could be hypothetically estimated to not greater than 25%. Based on this estimate, the NNT would be 4. Conservative surgery may be indicated in women with infertility and endometriotic ovarian cysts (stage III/IV) also because of the need for histological examination to rule out early ovarian cancer. However, patients must be informed that the effect of endometrioma excision on reproductive prognosis is poorly defined and that the chances of conception without surgery are currently unclear
, it is unclear whether. the benefits of surgery derive principally from treatment of the endometrioma or more generally from concomitant lysis of adhesions, ablation of peritoneal endometriosis, and chromopertubation. Very different outcomes have been reported in uncontrolled studies evaluating the impact of laparoscopic treatment of ovarian endometriotic. cysts on post-operative reproductive performance. Pregnancy rates vary from 30% (Marrs, 1991) to 67% (Beretta et al., 1998), with an overall weighted mean of about 50% (Fig. 3). Moreover, exclusion from the analysis of subjects lost to follow-up may enflate the purported benefit of surgery, as drop-outs notoriously have a worse prognosis. Publication bias (surgeons with suboptimal outcomes may be less willing to submit their data and may be less likely to have them published). The number of women with uni- or bilateral cysts is rarely specified. When a unilateral endometrioma was present, the operated gonad could have been damaged and pregnancy achieved as a result of the function of contra-lateral adnexa. lack of an adequately generated control group impedes measurement of the difference between post-operative and background spontaneous pregnancy rates. Noticeably, only such a difference, and not the total conception rate, may be ascribed to surgery. Accordingly, the potential absolute benefit increase over background pregnancy rate 12 months after surgery in women with patent tubes could be hypothetically estimated to not greater than 25%. Based on this estimate, the NNT would be 4. Conservative surgery may be indicated in women with infertility and endometriotic ovarian cysts (stage III/IV) also because of the need for histological examination to rule out early ovarian cancer. However, patients must be informed that the effect of endometrioma excision on reproductive prognosis is poorly defined and that the chances of conception without surgery are currently unclear.")
24
ESHRE Guidelines for Diagnosis and Treatment of Endometriosis
‘no RCT or meta-analysis are available to answer the question whether surgical excision of moderate – severe endometriosis enhances pregnancy rates’ The above data suggest that excision of rectovaginal plaques does not improve the likelihood of pregnancy nor reduces the time-to-conception in women with endometriosis-associated infertility. Excision of deep endometriotic implants is unlikely to influence the probability of conception to a major extent if their burial limits the inflammatory consequences on the pelvic environment. purported benefit of excision of rectovaginal plaques in infertile women reported by several authors (Fig. 5) may be attributed to treatment of co-existent peritoneal and ovarian endometriosis. In fact, the three different lesion types are very frequently associated (Somigliana et al., 2004, 2007). here is still a lack of randomized controlled trials that evaluate the effectiveness of laparoscopic surgery for severe endometriosis-associated infertility, many observational studies suggest that in women with stage III–IV endometriosis, without other identifiable infertility factors, conservative surgical treatment with laparoscopy may increase fertility
 may be attributed to. treatment of co-existent peritoneal and ovarian endometriosis. In fact, the three different lesion types are very frequently associated. (Somigliana et al., 2004, 2007). here is still a lack of randomized controlled trials that evaluate the effectiveness of laparoscopic surgery for severe endometriosis-associated infertility, many observational studies suggest that in women with stage III–IV endometriosis, without other identifiable infertility factors, conservative surgical treatment with laparoscopy may increase fertility.")
25
IVF öncesi endometrioma için cerrahi uygulamış kadınlar ile uygulanmamışların klinik sonuçlarını karşılaştıran meta-analiz Collectively the available data in the literature show that surgical management of endometriomas has no significant effect on IVF pregnancy rates and ovarian response to stimulation compared with no treatment. Randomized controlled trials are needed before producing best-practice recommendations on this topic It has been reported that removing ovarian cysts that have well-defined ovarian capsules (dermoids, serous, and mucinous cysts) resulted in some ovarian tissue being removed in 6% of cases (37). Conversely, a small rim of tissue containing primordial follicles is removed in more than 50% of endometriomas One needs to be cautious when attributing the diminished response of the postcystectomy ovaries solely to the surgical injury to the ovary. It has been shown that ovaries with endometriotic cysts already exhibited reduced number of follicles and vascular activity compared with other types of benign cysts (43, 67). Furthermore, it is difficult to identify the impact of an isolated endometrioma per se on the cycle outcome because the majority of cases are associated with concomitant peritoneal disease, which is another confounding variable. According to this theory, an endometrioma would be a pseudocyst the wall of which is the inverted ovarian cortex, and hence its removal might involve removal of normal ovarian tissue with possible adverse implications for future fertility. At present it is estimated that 10%–25% of all patients undergoing IVF are diagnosed with endometriosis, there is an increasing concern regarding the amount of ovarian tissue that may be inadvertently removed or damaged during surgery. We excluded studies in which women received any medical therapy for endometriosis before or after surgery and whenever the study group was treated by either aspiration of the endometriotic cyst or by oophorectomy There were no significant differences in pregnancy and clinical pregnancy rate per cycle between women who underwent surgery and those who received no treatment for endometrioma (OR for pregnancy rate per cycle 0.92 [95% CI 0.61, 1.38]; OR for clinical pregnancy rate per cycle 1.34 [95% CI 0.82, 2.20]) (Fig. 2A and B). No significant difference was shown in the number of embryos available for transfer between the surgery group and the control group (WMD 0.57 [95% CI 0.27, 1.41]) (Fig. 2C). Garcia-Velasco et al. (2004a) did not observe a significant difference between the pregnancy rate of 133 women who underwent surgery for endometriomas before IVF (25.4%) and that of 56 subjects who proceeded directly to IVF without prior endometriotic cyst removal (22.7%). A prompt reply came from Demirol et al. (2006), who reported the results of the first available RCT on this issue. A group of 99 patients with endometriomas scheduled for an ICSI cycle were allocated to conservative surgery before ICSI (n ¼ 49) or immediate ICSI without prior surgery (n ¼ 50). No significant differences were observed in fertilization (86 versus 88%), implantation (16.5 versus 18.5%) and pregnancy (34 versus 38%) rates. There is general agreement that an endometrioma with a diameter of .4 cm may create difficulties during oocyte retrieval, as the cyst may be punctured, with subsequent possible rupture, infection and follicular fluid contamination (Somigliana et al., 2006). the choice of a laparoscopy before ART is based essentially on physical considerations (i.e. İnterference with pick-up) more than on improvement of results. An if laparoscopic surgery in experienced hands does not improve ovarian function or enhance IVF outcomes, then why perform the surgery at all? Clearly, if in addition to infertility the endometrioma is associated with pain, then surgery is the best means by which to treat both problems simultaneously. Proceeding directly to COH in asymptomatic women with ovarian endometriomas might reduce the time to pregnancy, diminish patient costs, and avoid the potential complications of surgery. Alternatively, symptomatic women with ovarian endometriomas might be advised that conservative ovarian surgery does not impair IVF success rates. Tsoumpou et al, FS 2009 xxxxxsedcrtfvgb jnkml,
 resulted in some ovarian tissue being removed in 6% of cases (37). Conversely, a small rim of tissue containing primordial follicles is removed in more. than 50% of endometriomas. One needs to be cautious when attributing the diminished response of the postcystectomy ovaries solely to the surgical. injury to the ovary. It has been shown that ovaries with endometriotic cysts already exhibited reduced number of follicles. and vascular activity compared with other types of benign cysts (43, 67). Furthermore, it is difficult to identify the impact of an isolated endometrioma per se on the cycle outcome because the majority of cases are associated with concomitant. peritoneal disease, which is another confounding variable. According to this theory, an endometrioma would be a pseudocyst the wall of which is the inverted ovarian cortex, and hence its removal. might involve removal of normal ovarian tissue with possible adverse implications for future fertility. At present it is estimated that 10%–25% of all patients undergoing IVF are diagnosed with endometriosis, there is an increasing concern regarding the amount of ovarian tissue that may be inadvertently removed or damaged during surgery. We excluded studies in which women received any medical therapy for endometriosis before or after surgery and. whenever the study group was treated by either aspiration of the endometriotic cyst or by oophorectomy. There were no significant differences in pregnancy and clinical pregnancy rate per cycle between women who underwent surgery and those who. received no treatment for endometrioma (OR for pregnancy rate per cycle 0.92 [95% CI 0.61, 1.38]; OR for clinical pregnancy. rate per cycle 1.34 [95% CI 0.82, 2.20]) (Fig. 2A and B). No significant difference was shown in the number of embryos available for transfer between the surgery group and the control group (WMD 0.57 [95% CI 0.27, 1.41]) (Fig. 2C). Garcia-Velasco et al. (2004a) did not observe a significant difference between the pregnancy rate of 133 women who underwent surgery. for endometriomas before IVF (25.4%) and that of 56 subjects who proceeded directly to IVF without prior endometriotic cyst removal (22.7%). A prompt reply came from Demirol et al. (2006), who reported the results of the first available RCT on this issue. A group of 99 patients with endometriomas scheduled for an ICSI cycle were allocated to conservative surgery before ICSI (n ¼ 49) or immediate ICSI without prior surgery (n ¼ 50). No significant differences were observed in fertilization (86 versus 88%), implantation (16.5 versus 18.5%) and pregnancy (34 versus 38%) rates. There is general agreement that an endometrioma with a diameter of .4 cm may create difficulties during oocyte retrieval, as the cyst may be punctured, with subsequent possible rupture, infection and follicular fluid contamination (Somigliana et al., 2006). the choice of a laparoscopy before ART is based essentially on physical considerations (i.e. İnterference with pick-up) more than on improvement of results. An if laparoscopic surgery in experienced hands does not improve ovarian function or enhance IVF outcomes, then why perform the surgery at all Clearly, if in addition to infertility the endometrioma is associated with pain, then surgery is the best means by which to treat both problems simultaneously. Proceeding directly to COH in asymptomatic women with ovarian endometriomas might reduce the time to pregnancy, diminish patient costs, and avoid the potential complications of surgery. Alternatively, symptomatic women with ovarian endometriomas might be advised that conservative ovarian surgery does not impair IVF success rates. Tsoumpou et al, FS xxxxxsedcrtfvgb jnkml,")
26
Garcia Velasco ve Somigliana, HR 2009
IVF kararı alınan endometriomalı kadınlarda cerrahi için dikkate alınması gereken klinik değişkenler Özellik cerrahiyi destekleyen cerrahi yapmamayı destekleyen Endometriozis için yok ≥ 1 önceki müdehaleler Over rezervi intakt azalmış Ağrı semptomları mevcut yok Bilateralite monolateral hastalık bilateral hastalık Sonografik malignite mevcut yok bulguları Büyüme hızlı büyüme stabil Over rezervi serum markerlara veya önceki hiperstimülasyon sikluslarına bakarak. Sonografik maliginte bulguları: solid komponent, lokülarite, ekojenite, regülarite, duvar lokasyon ve peritoneal sıvının varlığı. Surgery should be performed only in the presences of a large endometrioma that interferes with oocyte collection and severe symptoms or when there is a suspicion of malignancy. ≥ 4 cm ise laparoskopik kistektomi: Histolojik tanı konfirmasyonu Enfeksiyon riskini azaltmak Folliküllere ulaşmayı kolaylaştırmak ? Clearly, if in addition to infertility the endometrioma is associated with pain, then surgery is the best means by which to treat both problems simultaneously. Garcia Velasco ve Somigliana, HR 2009 xxxxxsedcrtfvgb jnkml,

28
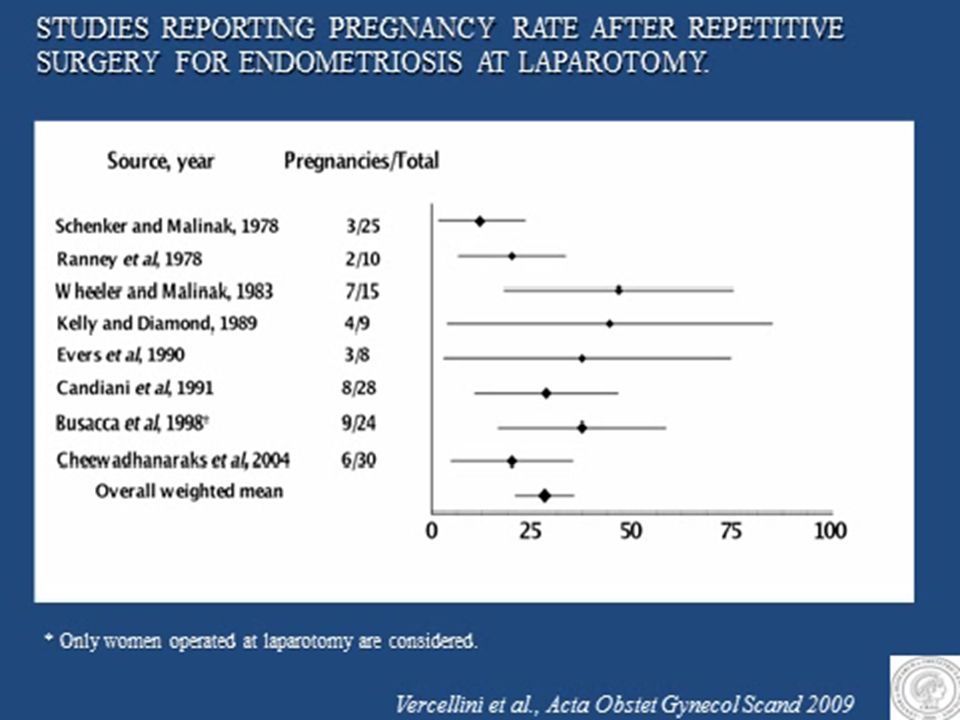
İnfertil kadında rekürren endometriozis için cerrahi
ASRM Practice Committee: Tekrar operasyon yerine IVF daha iyi bir seçenektir Very limited information is available on the effect of second-line surgery for recurrent endometriosis in infertile women. It is a common tenet that re-operations for endometriosis are technically more demanding and potentially more risky. In order to offer adequate counselling to patients, these drawbacks should be balanced by acceptable post-operative results. Based on the scanty available evidence, the effect of surgery appears smaller after second- compared with first-line surgery, and the potential absolute benefit increase in women with patent tubes and recurrent moderate to severe endometriosis is difficult to estimate but may be quite limited. According to the ASRM clinical guidelines, for infertile women who have moderate to severe endometriosis and have previously had one or more infertility operations, IVF-ET is often a better therapeutic option than another infertility operation (The Practice Committee of the American Society for Reproductive Medicine, 2004). However, data are so limited that drawing definitive conclusions seems inopportune. The final decision should be taken also considering the presence of pain symptoms and of large (.4 cm) endometriomas (Kennedy et al., 2005; Royal College of Obstetricians and Gynaecologists, 2006).
. However, data are so limited that drawing definitive. conclusions seems inopportune. The final decision should be taken also considering the presence of pain symptoms and of large. (.4 cm) endometriomas (Kennedy et al., 2005; Royal College of Obstetricians and Gynaecologists, 2006).")
29
Sonuçlar Ovarian endometriomalar over rezervinde azalmaya neden olmaktadır Eksizyonları over rezervine zararı daha da arttırmaktadır Bilateral endometriomaların hem cerrahi öncesi hem de sonrası gonad dokusuna etkileri daha da olumsuzdur Endometrioma cerrahisinde kaçınılması gerekenler: Perikapsüler stromal dokunun çıkartılması Pseudokapsülün hilar bölgesinin çıkartılması Aşırı koagülasyon

30
Sonuçlar Over rezervinin preoperatif serum AMH ile değerlendirilmesi postoperatif over yetmezliği riski altında olan kadınları belirleyecektir Foliküllere ulaşmayı etkilemeyecek ufak (<4 cm) asemptomatik endometriomalar IVF öncesi çıkartılmamalıdır Hastalığın uzun süreli yaklaşımında rekürrenslerin önlenmesinde oral kontraseptiflerin yeri vardır İleride gebe kalmayı planlayan ve ufak, şüpheli sonografik bulgular içermeyen kistleri olan kadınlarda hemen eksizyon mu yoksa gebelik arzu edilene dek OC ile tedavi mi daha uygundur ?
 asemptomatik endometriomalar IVF öncesi çıkartılmamalıdır. Hastalığın uzun süreli yaklaşımında rekürrenslerin önlenmesinde oral kontraseptiflerin yeri vardır. İleride gebe kalmayı planlayan ve ufak, şüpheli sonografik bulgular içermeyen kistleri olan kadınlarda hemen eksizyon mu yoksa gebelik arzu edilene dek OC ile tedavi mi daha uygundur")
Benzer bir sunumlar







>")











