Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Romatoid Artriti Nasıl Tanırız?
Doç. Dr. Salih PAY GATA Romatoloji BD 9. Ulusal İç Hastalıkları Kongresi 06 Eylül 2007

2
Tanım Romatoid artrit;
Periferik diathrodial (sinoviyal) eklemleri simetrik olarak tutan klinik bulguları ve seyri hastadan hastaya değişkenlik gösteren kıkırdak tahribatı ve kemik erozyonları ile eklem harabiyeti ve deformasyonu oluşturabilen çoğunlukla RF’nin pozitif bulunduğu eklem dışı bulguların eşlik ettiği kronik iltihabi eklem hastalığıdır. periferik simetrik poliartrit heterojen, sendrom? erozif, deforman seropozitif sistemik inflamatuvar, artrit
 eklemleri simetrik olarak tutan. klinik bulguları ve seyri hastadan hastaya değişkenlik gösteren. kıkırdak tahribatı ve kemik erozyonları ile eklem harabiyeti ve deformasyonu oluşturabilen. çoğunlukla RF’nin pozitif bulunduğu. eklem dışı bulguların eşlik ettiği. kronik iltihabi eklem hastalığıdır. periferik simetrik poliartrit. heterojen, sendrom erozif, deforman. seropozitif. sistemik. inflamatuvar, artrit.")
3
Sık tutulan eklemler

4
Romatoid artritin tanısı
Klinik başlangıç noktası: 2 veya daha fazla eklemde, 6 haftadan uzun süren artrit (şişlik ve efüzyon)
")
5
Romatoid artritin tanısı
Klinik başlangıç noktası: 2 veya daha fazla eklemde, 6 haftadan uzun süren artrit (şişlik ve efüzyon) Sinsi, poliartiküler tutulum ağrı, tutukluk ve şişlik, sabah tutukluğu Öncelikle MKF, PİF, 1.İP, EB ve MTF tutulumu
 Sinsi, poliartiküler tutulum ağrı, tutukluk ve şişlik, sabah tutukluğu. Öncelikle MKF, PİF, 1.İP, EB ve MTF tutulumu.")
6
Romatoid artritin tanısı
Klinik başlangıç noktası: 2 veya daha fazla eklemde, 6 haftadan uzun süren artrit (şişlik ve efüzyon) Sinsi, poliartiküler tutulum ağrı, tutukluk ve şişlik, sabah tutukluğu Öncelikle MKF, PİF, 1.İP, EB ve MTF tutulumu Akut poliartrit; miyalji, yorgunluk, ateş, kilo kaybı, depresyon Palindromik romatizma; 2-3 saat-gün arası, migratuvar artrit Kr.monoartrit; diz, omuz, kalça, el ve ayak bileği travma öyküsü Eklem dışı; genel ağrı, tutukluk, KTS, kilo kaybı, serozit, episklerit, vaskülit
 Sinsi, poliartiküler tutulum ağrı, tutukluk ve şişlik, sabah tutukluğu. Öncelikle MKF, PİF, 1.İP, EB ve MTF tutulumu. Akut poliartrit; miyalji, yorgunluk, ateş, kilo kaybı, depresyon. Palindromik romatizma; 2-3 saat-gün arası, migratuvar artrit. Kr.monoartrit; diz, omuz, kalça, el ve ayak bileği travma öyküsü. Eklem dışı; genel ağrı, tutukluk, KTS, kilo kaybı, serozit, episklerit, vaskülit.")
7
Romatoid artritin tanısı
Klinik başlangıç noktası: 2 veya daha fazla eklemde, 6 haftadan uzun süren artrit (şişlik ve efüzyon) Diğer klinik bulgular Laboratuar bulguları
 Diğer klinik bulgular. Laboratuar bulguları.")
8
Romatoid artritin tanısı
Klinik başlangıç noktası: 2 veya daha fazla eklemde, 6 haftadan uzun süren artrit (şişlik ve efüzyon) Diğer klinik bulgular Laboratuar bulguları Etkilenen eklemlerin sayısı ve dağılımı, Sabah tutukluğu, Eklem dışı bulgular Radyoloji: Düz grafiler, US, MRG Sinovit, Erozyon Kemik iliği ödemi Akut faz yanıtı; CRP ve ESR Seroloji; RF ve anti-CCP
 Diğer klinik bulgular. Laboratuar bulguları. Etkilenen eklemlerin. sayısı ve dağılımı, Sabah tutukluğu, Eklem dışı bulgular. Radyoloji: Düz. grafiler, US, MRG. Sinovit, Erozyon. Kemik iliği ödemi. Akut faz yanıtı; CRP ve ESR. Seroloji; RF ve anti-CCP.")
9
Romatoid artritin tanısı Ayırıcı tanıya giren hastalıkların
Klinik başlangıç noktası: 2 veya daha fazla eklemde, 6 haftadan uzun süren artrit (şişlik ve efüzyon) Diğer klinik bulgular Laboratuar bulguları Etkilenen eklemlerin sayısı ve dağılımı, Sabah tutukluğu, Eklem dışı bulgular Seroloji; RF ve anti-CCP Akut faz yanıtı; CRP ve ESR Radyoloji: Düz grafiler, US, MRG Sinovit, Erozyon Kemik iliği ödemi Ayırıcı tanıya giren hastalıkların gözden geçirilmesi Romatoid artrit
 Diğer klinik bulgular. Laboratuar bulguları. Etkilenen eklemlerin. sayısı ve dağılımı, Sabah tutukluğu, Eklem dışı bulgular. Seroloji; RF ve anti-CCP. Akut faz yanıtı; CRP ve ESR. Radyoloji: Düz. grafiler, US, MRG. Sinovit, Erozyon. Kemik iliği ödemi. Ayırıcı tanıya giren hastalıkların. gözden geçirilmesi. Romatoid artrit.")
10
Romatoid artritin tanısı
Klinik başlangıç noktası: 2 veya daha fazla eklemde, 6 haftadan uzun süren artrit (şişlik ve efüzyon) Diğer klinik bulgular Laboratuar bulguları Etkilenen eklemlerin sayısı ve dağılımı, Sabah tutukluğu, Eklem dışı bulgular Seroloji; RF ve anti-CCP Akut faz yanıtı; CRP ve ESR Radyoloji: Düz grafiler, US, MRG Sinovit, Erozyon Kemik iliği ödemi Ayırıcı tanıya giren hastalıkların gözden geçirilmesi Romatoid artrit Eklem harabiyeti ve fonksiyon kaybı yönünden kötü prognoz belirteçlerinin aranması
 Diğer klinik bulgular. Laboratuar bulguları. Etkilenen eklemlerin. sayısı ve dağılımı, Sabah tutukluğu, Eklem dışı bulgular. Seroloji; RF ve anti-CCP. Akut faz yanıtı; CRP ve ESR. Radyoloji: Düz. grafiler, US, MRG. Sinovit, Erozyon. Kemik iliği ödemi. Ayırıcı tanıya giren hastalıkların. gözden geçirilmesi. Romatoid artrit. Eklem harabiyeti ve fonksiyon kaybı yönünden. kötü prognoz belirteçlerinin aranması.")
11
El ve parmak deformiteleri

12
Parmak deformiteleri Kuğu boynu deformitesi Düğme iliği deformitesi

13
Sistemik bulguları

14
Tanımlar Erken sinovit Erken artrit Çok erken iltihabi artrit
Erken iltihabi poliartrit İdyopatik poliartrit Çok erken romatoid artrit Erken romatoid artrit

15
Erken Sinovit & RA Erken Sinovit Erken RA Yerleşik RA
İlerleyici eklem hasarı Sinoviyal inflamasyonun başlaması Klinik semptomların ortaya çıkması p53 mutasyonları(?) Otoimmün yantın başlaması Tak, PP Best Practice and Res Clin Rheum 2001
 Otoimmün. yantın. başlaması. Tak, PP Best Practice and Res Clin Rheum")
16
Erken Poliartritin Değerlendirilmesinde Sorunlar
NSAİİ cevabı çok iyi, tam tedavi olduğu sanılabilir RA klinik bulguları non-spesifik Kendine sınırlı artrit te sınıflandırma kriterlerini doldurabilir Tek önemli fark RA’nın kronik olması Laboratuar testleri ve radyoloji negatif olabilir Akut faz %60, radyoloji %70 normal ve RF %70 negatif OA ile birlikte olduğunda, radyoloji yanıltabilir Quinn MA ve ark Rheumatology 2003

17
Erken Poliartrit: Hangi Hasta Uzmana Gönderilmeli
Eklem şişliği olanlar MKF ve MTF tutulumu NSAİİ’ iyi yanıt verenler Simetrik tutulumu olanlar Aile öyküsü pozitif olanlar Belirgin sabah tutukluğu olanlar 6-12 haftadan uzun süren poliartrit? DMARD Quinn MA ve ark Rheumatology 2003

18
Arthritis in three joint groups or more is the most diagnostic variable obtained from physical examination. Compression pain of metacarpophalangeal (MCP) and metatarsophalangeal (MTP) joints is specific for persistent arthritis but is not sensitive. Subcutaneous nodules are very uncommon in early RA and therefore have no diagnostic value. Sabah tutkluğu 58/76

20
Hueber W ve ark. Clin Exp Rheum 2003
Erken RA: Tanı Antikor Spesifisite (%) Sensitivite (%) AKA AFA Anti-RA Anti-Sa *Anti-CCP Anti-hFibA Anti--enolaz AKA: Antikeratin Antikor, Anti-hFibA: Antihuman fibrinojen peptid A, AFA: Anti-filagrin Antikor, Anti-CCP: Anti-cyclic citrullinated peptide Hueber W ve ark. Clin Exp Rheum 2003
 Sensitivite (%) AKA AFA Anti-RA Anti-Sa *Anti-CCP Anti-hFibA Anti--enolaz AKA: Antikeratin Antikor, Anti-hFibA: Antihuman fibrinojen peptid A, AFA: Anti-filagrin Antikor, Anti-CCP: Anti-cyclic citrullinated peptide. Hueber W ve ark. Clin Exp Rheum")
22
The specificity of the anti-CCP ELISA was 96%, which is significantly higher than that of the IgM RF ELISA (91% specificity; PZ0.016). The IgM RF ELISA and the anti-CCP ELISA both had moderate sensitivity: 54 and 48% (PZ0.36), respectively. Table 2 also displays the predictive values of both tests and their combinations, employing optimal cut-off values. For the combination ‘CCP or RF’, at least one of the two tests should be positive for a positive test result, and for the combination ‘CCP and RF’, both tests should be positive for a positive test result. The prevalence of RA, or pretest probability, was 31%. The positive predictive value (PPV) of the anti-CCP ELISA (84%) was higher than that of the IgM RF ELISA (74%); however, the difference was not statistically significant (PZ0.14). The negative predictive value (NPV) was 81% for both ELISAs.
, respectively. Table 2 also displays the predictive values of both tests and their combinations, employing optimal cut-off values. For the combination ‘CCP or RF’, at least one of the two tests should be positive for a positive test result, and for the combination ‘CCP and RF’, both tests should be positive for a positive test result. The prevalence of RA, or pretest probability, was 31%. The positive predictive value (PPV) of the anti-CCP ELISA (84%) was higher than that of the IgM RF ELISA (74%); however, the difference was not statistically significant (PZ0.14). The negative predictive value (NPV) was 81% for both ELISAs..")
23
The diagnostic characteristics of SE and DQRA, used to discriminate between self-limiting and persistent arthritis at 2-year follow-up, are shown in Table 3. SE homozygosity and DQRA homozygosity both have a high specificity and a low sensitivity. SE heterozygosity and DQRA heterozygosity both have a low specificity and a moderate sensitivity. Overall, the diagnostic value of the genetic typing is not good enough to be of practical importance. When the results of the genetic typing were added to the prediction model (consisting of seven clinical variables) in the logistic regression analysis, only the presence of DQRA homozygosity contributed independently to an increase in its predictive value. The discriminative ability of the prediction model with the DQRA test was, however, not significantly better than without the DQRA test.9

24
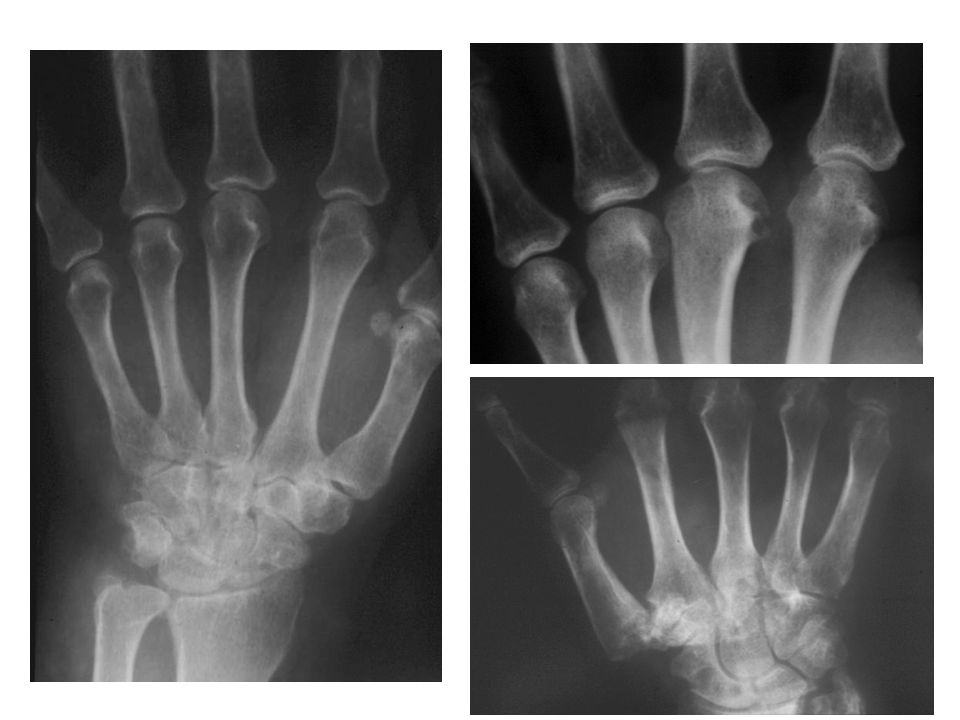
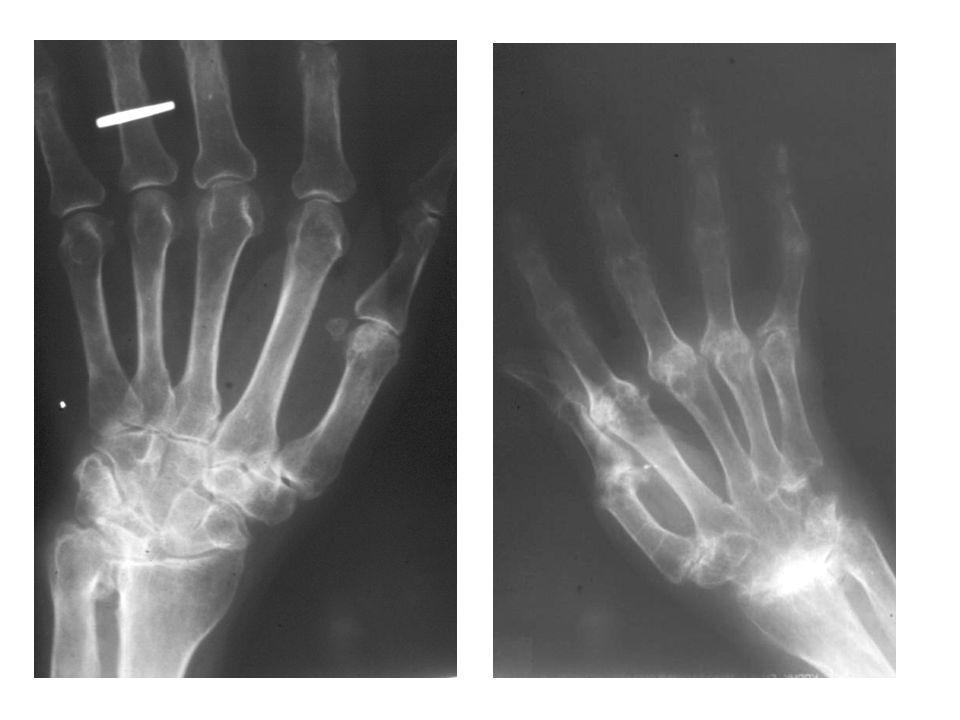
Erken RA: Tanı İki önemli bulgusu vardır:
Eklem aralığında daralma: kıkırdak harabiyeti Kemik erozyonları: kemik yıkımı Diğerleri, Yumuşak doku şişliği, Periartiküler osteoporoz, Subluksasyonlar, Sekonder osteoartroz

28
The diagnostic characteristics of X-rays of hands and feet when used to discriminate between self-limiting and persistent arthritis are shown in Table 4. The diagnostic value of X-rays of the feet is slightly higher than that of X-rays of the hands. The combination of X-rays of hands and feet is most diagnostic. The presence of erosions on X-rays of hands and/or feet has a high specificity but a low sensitivity in discriminating between self-limiting and persistent arthritis. In a recent study of 149 early arthritis patients, the ability of radiographic erosions at the hands or feet to predict the clinical diagnosis of RA after 2 years of follow-up was described.48 As shown in Table 4, the diagnostic characteristics of erosions on X-rays of hands or feet in this study are comparable with the results from the Leiden early arthritis clinic. Erosions at the feet had a higher specificity than erosions at the hands. Combining hand and foot radiographs improved diagnostic performance.

29
Erozyon Figure 1. Conventional X-ray, MRI and US in a patient with early RA. (a) X-rays of hands and feet (the displayed image shows the second to fifth metacarpophalangeal joints) show no erosions. Coronal (b) and axial (c) T1-weighted spin echo MRI scans show a bone erosion at the radial aspect of the second metacarpal head (arrow). US in the longitudinal (d) and transverse (e) planes of the radial aspect of the second metacarpal head demonstrates the same bone erosion as shown on MRI.
 X-rays of hands and feet (the displayed image shows the second to fifth metacarpophalangeal joints) show no erosions. Coronal (b) and axial (c) T1-weighted spin echo MRI scans show a bone erosion at the radial aspect of the second metacarpal head (arrow). US in the longitudinal (d) and transverse (e) planes of the radial aspect of the second metacarpal. head demonstrates the same bone erosion as shown on MRI.")
30
Sinovit

31
Sinovit Fig. 1a–d Transverse T1-weighted MR imaging pre- and postgadolinium (Gd-DTPA) through the MCP joints and wrist in a patient with RA. a Pre-Gd-DTPA and b post-Gd-DTPA in the same axial section through the MCP joints. The thickened enhancing synovium is clearly shown surrounding the joints and the flexor tendons (arrowheads).Some non-enhancing joint fluid is seen within the ring MCP joint (arrow). c Pre-Gd-DTPA and d post-Gd-DTPA in the same axial section through the wrist. Enhancing synovitis is seen at the distal radio-ulnar joint (arrowheads) and surrounding the flexor tendons. Non-enhancing fluid is also seen (arrow). Further synovitis is seen surrounding the extensor carpi ulnaris tendon, a common site for synovitis in RA (black arrowhead) RKMÖ RKMS
 through the MCP joints and wrist in a patient with RA. a Pre-Gd-DTPA and b post-Gd-DTPA in the same axial section through the MCP joints. The thickened enhancing synovium is clearly shown surrounding the joints and the flexor tendons (arrowheads).Some non-enhancing joint fluid is seen within the ring MCP joint (arrow). c Pre-Gd-DTPA and d post-Gd-DTPA in the same axial section through the wrist. Enhancing synovitis is seen at the distal radio-ulnar joint (arrowheads) and surrounding the flexor tendons. Non-enhancing fluid is also seen (arrow). Further synovitis is seen surrounding the extensor carpi ulnaris tendon, a common site for synovitis in RA (black arrowhead) RKMÖ. RKMS.")
32
Sinovit Sinovit

33
Sinovit

34
Kemik iliği ödemi RKMÖ RKMS
MRI scans from a 65 year old female rheumatoid arthritis patient with disease duration of one year. (a) Coronal T1 weighted image of the dominant wrist with reduced signal indicating florid bone oedema involving the entire lunate bone (circle). (b) Equivalent image following the injection of contrast (gadolinium diethylenetriamine pentaacetic acid (GdDPTA)) shows very bright signal within the lunate, suggesting the presence of vascularized tissue (slice does not exactly correspond with pre-GdDPTA image). (c) Axial T2w image with bright signal confirming bone oedema at the lunate. RKMÖ RKMS
 Coronal T1 weighted image of the dominant wrist with reduced signal indicating florid bone oedema involving the entire lunate bone (circle). (b) Equivalent image following the injection of contrast (gadolinium diethylenetriamine pentaacetic acid (GdDPTA)) shows very bright signal within the lunate, suggesting the presence of vascularized tissue (slice does not exactly correspond with pre-GdDPTA image). (c) Axial T2w image with bright signal confirming bone oedema at the lunate. RKMÖ. RKMS.")
35
Potential role of bone marrow-derived stem cells in trafficking to the subchondral bone and synovial membrane in rheumatoid arthritis joints, resulting in a subchondral cellular infiltrate (seen as bone oedema on MRI) followed by erosion. (a) CD34+ stem cells from bone marrow express high levels of NFkB, which leads to unusual sensitivity to TNFα. (b) Stem cells differentiate into fibroblast-like cells and travel via the circulation to synovial membrane to become type B synoviocytes - here they mediate formation of erosions via production of proinflammatory cytokines and matrix metalloproteinases [23,25]. (c) Stem cells may also traffic to the subchondral bone marrow where they differentiate into mesenchymal cells. These cells could then travel via bony canals from bone marrow to synovium [29] to excite an inflammatory response. (d) Alternatively, stem cells could travel to subchondral bone and at this site could mediate an inflammatory response via T/B cell interactions associated with angiogenesis [26] and osteoclast activation. This could lead to erosions originating from inside the bone, directed outwards towards joint surface [14]. (e) Coronal T2 weighted MRI scan of the wrist in early rheumatoid arthritis reveals bone oedema at the bases of the 2nd and 3rd metacarpals and adjacent regions of trapezoid and capitate carpal bones. Small intraosseous erosions are also apparent.
 followed by erosion. (a) CD34+ stem cells from bone marrow express. high levels of NFkB, which leads to unusual sensitivity to TNFα. (b) Stem cells differentiate into fibroblast-like cells and travel via the circulation to. synovial membrane to become type B synoviocytes - here they mediate formation of erosions via production of proinflammatory cytokines and. matrix metalloproteinases [23,25]. (c) Stem cells may also traffic to the subchondral bone marrow where they differentiate into mesenchymal cells. These cells could then travel via bony canals from bone marrow to synovium [29] to excite an inflammatory response. (d) Alternatively, stem cells could travel to subchondral bone and at this site could mediate an inflammatory response via T/B cell interactions associated with angiogenesis [26] and osteoclast activation. This could lead to erosions originating from inside the bone, directed outwards towards joint surface [14]. (e) Coronal T2 weighted MRI scan of the wrist in early rheumatoid arthritis reveals bone oedema at the bases of the 2nd and 3rd metacarpals and adjacent regions of trapezoid and capitate carpal bones. Small intraosseous erosions are also apparent.")
36
ACR 1987 Klasifikasyon Kriterleri
Eklem ve eklem çevresinde en az bir saat süren sabah tutukluğu, Doktor tarafından gözlenen ve en az 6 hafta süren üç veya daha fazla eklem bölgesinde artrit ; PİF, MKF, EB, dirsek, diz, AB, MTF El eklemlerinde en az 6 hafta süren (EB, MKF veya PİF) artrit Simetrik artrit Romatoid nodul Romatoid faktör pozitifliği Radyolojik değişiklikler; El ve EB AP grafilerinde erozyon ve kistik görünüm veren dekalsifakasyonlar
 artrit. Simetrik artrit. Romatoid nodul. Romatoid faktör pozitifliği. Radyolojik değişiklikler; El ve EB AP grafilerinde erozyon ve. kistik görünüm veren dekalsifakasyonlar.")
37
Poliartrit: Ayırıcı Tanı
İnflamatuar artritler Romatoid artrit Postviral artrit Psoriyatik artrit Reaktif artrit Ankilozan spondilit Enteropatik artrit Poliartiküler gut Kalsiyum pirofosfat artriti Bağ dokusu hastalıkları Sistemik lupus eritematozus Sjögren sendromu Dermatomiyozit/ polimiyozit Skleroderma Belirlenemyen bağ dokusu hastalığı Vaskülitler Behçet hastalığı Poliarteritis nodoza Ayırıcı tanıda önemli klinik tablolar Septik artrit Paraneoplastik sendrom Subakut bakteriyel endokardit Polimiyalji romatika İnflamtuar olmayan durumlar Osteoartrit Fibromiyalji Quinn MA ve ark Rheumatology 2003

39
Erken RA: Prognostik Faktörler
Otoantikorlar- RF/Anti-CCP Genetik faktörler- Paylaşılmış epitop Akut faz cevabı- CRP, ESR Cinsiyet- Kadın Görüntüleme- erozyon/kist (US/MRG/X-ray) Fonksiyonel bozukluk- HAQ Hastaların %60-70’ni değerlendirebilir Quinn MA ve ark Rheumatology 2003
 Fonksiyonel bozukluk- HAQ. Hastaların %60-70’ni değerlendirebilir. Quinn MA ve ark Rheumatology")
Benzer bir sunumlar