Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Endometriozisin Medikal Tedavisi
Dr. Moşe Benhabib Acıbadem İnternational Hospital

2
Definitions ‘The presence of endometrial-like tissue outside the uterus… induces a chronic, inflammatory reaction’1 ‘…found predominantly in women of reproductive age, from all ethnic and social groups’1 ‘…associated symptoms can impact on general physical, mental and social well-being’1 Reference Kennedy S, Bergqvist A, Chapron C et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005;20: Further information Endometriosis can be defined as: the presence of endometrium-like tissue (‘endometriotic lesions’) outside the uterus, which induces a chronic, inflammatory reaction [Kennedy et al, 2005]. Endometriosis affects women primarily during their reproductive years. The peak age for diagnosis is between 25 and 34 years; however, endometriosis is also increasingly diagnosed in adolescents. All ethnic and social groups of women are affected. The painful and long-lasting symptoms of endometriosis can have a profound impact on a woman’s quality of life, in terms of diminished well-being and self-esteem, as well as on employment and financial status. Kennedy S, Berggvist A, Chapron C et al. Hum Reprod 2005.
 outside the uterus, which induces a chronic, inflammatory reaction [Kennedy et al, 2005]. Endometriosis affects women primarily during their reproductive years. The peak age for diagnosis is between 25 and 34 years; however, endometriosis is also increasingly diagnosed in adolescents. All ethnic and social groups of women are affected. The painful and long-lasting symptoms of endometriosis can have a profound impact on a woman’s quality of life, in terms of diminished well-being and self-esteem, as well as on employment and financial status. Kennedy S, Berggvist A, Chapron C et al. Hum Reprod")
3
Critical Aspects of Pathogenesis
Endometrial-like cells attach to peritoneal tissue/other sites Cellular infiltration/invasion, involving angiogenesis Cellular proliferation Inflammation which can cause Nerve irritation Adhesions Individual variation References Mahutte NG, Kayisli U, Arici A. Endometriosis is an inflammatory disease. In: Endometriosis in Clinical Practice, ed. D. Olive. Taylor & Francis, 2005; pp.79–88. Fraser IS. Recognising, understanding and managing endometriosis. J Hum Reprod Sci 2008;1:56–64. Further information Endometriosis is believed to progress in a sequence of stages that commences with the attachment of endometrial-like cells and leads eventually to symptoms of pain and the development of adhesions. There is wide inter-individual variability in the progression of endometriosis, and little correlation exists between symptoms and the extent of lesions. Cellular proliferation – cyclical endometrial tissue growth in response to estrogen. Inflammation – inflammatory cell recruitment in response to inflammatory mediators. Adhesions – fibrosis and scar formation. Mahutte NG, Kayisli U, Arici A. Endometriosis in Clinical Practice. 2005; Fraser IS. J Hum Reprod Sci 2008.

4
Sites Commonly Affected
‘Extent of disease varies from a few, small lesions on otherwise normal pelvic organs to large, ovarian endometriotic cysts (endometriomas), and/or extensive fibrosis and adhesion formation causing marked distortion of pelvic anatomy’1 Pelvic cavity: Peritoneum, ovaries, pouch of Douglas, uterosacral ligaments Other sites: Vagina, bowel, bladder, ureters Rare sites: Lungs, brain Reference Kennedy S, Bergqvist A, Chapron C et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005;20:2698–2704. Further information Endometriosis is characterised by the growth of endometrial-like tissue (‘endometriotic lesions’) outside the uterus. The most commonly affected sites are regions in the pelvic cavity – including the peritoneum, ovaries, pouch of Douglas and uterosacral ligaments – although many other areas of the body may also be affected. The extent of disease varies considerably. Extensive growth of lesions may produce pain, heavy bleeding, adhesions and scarring, often damaging the fallopian tubes and ovaries and in many cases leading to infertility. Image usage rights For the period of 2 years, ending For global use. For use in PowerPoint (ppt) presentation only. Kennedy S, Berggvist A, Chapron C et al. Hum Reprod 2005.
, and/or extensive fibrosis and adhesion formation causing marked distortion of pelvic anatomy’1. Pelvic cavity: Peritoneum, ovaries, pouch of Douglas, uterosacral ligaments. Other sites: Vagina, bowel, bladder, ureters. Rare sites: Lungs, brain. Reference. Kennedy S, Bergqvist A, Chapron C et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005;20:2698–2704. Further information. Endometriosis is characterised by the growth of endometrial-like tissue (‘endometriotic lesions’) outside the uterus. The most commonly affected sites are regions in the pelvic cavity – including the peritoneum, ovaries, pouch of Douglas and uterosacral ligaments – although many other areas of the body may also be affected. The extent of disease varies considerably. Extensive growth of lesions may produce pain, heavy bleeding, adhesions and scarring, often damaging the fallopian tubes and ovaries and in many cases leading to infertility. Image usage rights For the period of 2 years, ending For global use. For use in PowerPoint (ppt) presentation only. Kennedy S, Berggvist A, Chapron C et al. Hum Reprod")
5
Risk Factors Pathophysiology unclear
Certain characteristics lead to increased/decreased risk Increased Risk Decreased Risk Increased exposure to endometrial material – short menstrual cycles, heavy/longer bleeding, early menarche, late menopause1,2 Increased number of live births1 Family history3 Longer duration of lactation1 Low exercise4-6 References Mounsey AL, Wilgus A, Slawson DC. Diagnosis and management of endometriosis: Am Fam Phys 2006;74:594–600. Missmer SA, Hankinson SE, Spiegelman D et al. Reproductive history and endometriosis among premenopausal women. Obstet Gynecol 2004;104:965–974. Bischoff F, Simpson JL. Genetic basis of endometriosis. Ann N Y Acad Sci 2004;1034:284–299. Eskenazi B, Warner ML. Epidemiology of endometriosis. Obstet Gynecol Clin North Am 1997;24:235–258. Cramer DW, Missmer SA. The epidemiology of endometriosis. Ann N Y Acad Sci 2002;955:11–22. Hediger ML, Hartnett HJ, Louis GM. Association of endometriosis with body size and figure. Fertil Steril 2005;84:1366–1374. Further information Although the pathophysiology of endometriosis remains unclear, women with certain characteristics are observed to be at increased risk of developing endometriosis. These characteristics include short menstrual cycles, heavy or long duration of menstrual flow, early menarche and late menopause. Genetic factors may also have an influence. For example, in one study, 5–7% of first-degree female relatives of patients with endometriosis were affected, compared to 1% or less of controls. Other factors, such as an increased number of live births, longer duration of lactation and certain lifestyle factors, may be associated with a decreased risk of developing endometriosis. Further investigation of these associations may help to characterise the pathophysiology of endometriosis. Mounsey AL et al. Am Fam Phys 2006; Missmer SAet al. Obstet Gynecol 2004; Bischoff F et al. Ann N Y Acad Sci 2004; Eskenazi B et al. Obstet Gynecol Clin North Am 1997; Cramer DW et al. Ann N Y Acad Sci 2002; Hediger ML et al. Fertil Steril 2005.

9
Diagnosis Diagnosis often delayed (average 8.3 years1) Suggestive
Typical clinical symptoms and signs (e.g. uterosacral nodularity)2,3 Diagnosis often delayed (average 8.3 years1) Suggestive Definitive Magnetic resonance imaging and ultrasound4 Laboratory tests currently fail to show predictive value5,6 New semi-quantitative procedures being assessed7 New techniques Laparoscopic visualisation – ideally with confirmatory histology1 References Kennedy S, Bergqvist A, Chapron C et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005;20:2698–2704. Mounsey AL, Wilgus A, Slawson DC. Diagnosis and management of endometriosis: Am Fam Phys 2006;74:594–600. Matorras R, Rodríguez F, Pijoan JI et al. Are there any clinical signs and symptoms that are related to endometriosis in infertile women? Am J Obstet Gynecol 1996;174:620–623. Bazot M, Daraï E. Sonography and MR imaging for the assessment of deep pelvic endometriosis. J Minim Invasive Gynecol 2005;12:178–185. Bedaiwy MA, Falcone T. Laboratory testing for endometriosis. Clin Chim Acta 2004;340:41–56. Matalliotakis IM, Goumenou AG, Mulayim N, Karkavitsas N, Koumantakis EE. High concentrations of the CA-125, CA 19-9 and CA 15-3 in the peritoneal fluid between patients with and without endometriosis. Arch Gynecol Obstet 2005;271:40–45. Fraser IS. Recognising, understanding and managing endometriosis. J Hum Reprod Sci 2008;1:56–64. Al-Jefout M, Dezarnaulds G, Cooper M et al. Diagnosis of endometriosis by detection of nerve fibres in an endometrial biopsy: a double blind study. Hum Reprod 2009;24:2972–2973. Hummelshoj L, Prentice A, Groothuis P. Update on endometriosis. Women's Health 2006;2:53–56. Further information A definitive diagnosis of endometriosis requires laparoscopy, ideally combined with histology, to identify the presence of endometriotic lesions. However, laparoscopic facilities are not universally available. Physicians and patients may also agree that it is not appropriate to perform this invasive procedure, with its associated risks, according to individual circumstances. In these situations, a physician may make a presumptive diagnosis based on the signs and symptoms alone. Laboratory tests have, to date, failed to show predictive value. In future, alternative techniques may offer a less invasive diagnosis than laparoscopy. Non-invasive imaging techniques such as MRI and ultrasound may assist in diagnosing certain forms of endometriosis. The detection of nerve fibres in biopsies of eutopic endometrium is recently reported to have a diagnostic accuracy similar to laparoscopy [Al-Jefout et al, 2009]. As a consequence of the difficulties in diagnosing endometriosis, there is commonly a delay between the first appearance of symptoms and a definitive diagnosis. An international survey reported that the average delay is 8.3 years [Hummelshoj et al, 2006]. Kennedy S, Bergqvist A, Chapron C, et al. Hum Reprod 2005; Mounsey AL, Wilgus A, Slawson DC. Am Fam Phys 2006; Matorras R, Rodríguez F, Pijoan JI, et al. Am J Obstet Gynecol 1996; Bazot et al. J Minim Invasive Gynecol 2005; Bedawy et al. Clin Chem Acta 2004; Matalliotakis et al. Arch Gynecol Obstet 2005; Fraser et al. J Hum Reprod Sci 2008. 9
2,3. Diagnosis often delayed. (average 8.3 years1) Suggestive. Definitive. Magnetic resonance imaging and ultrasound4. Laboratory tests currently fail to show predictive value5,6. New semi-quantitative procedures being assessed7. New. techniques. Laparoscopic visualisation – ideally with confirmatory histology1. References. Kennedy S, Bergqvist A, Chapron C et al. ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005;20:2698–2704. Mounsey AL, Wilgus A, Slawson DC. Diagnosis and management of endometriosis: Am Fam Phys 2006;74:594–600. Matorras R, Rodríguez F, Pijoan JI et al. Are there any clinical signs and symptoms that are related to endometriosis in infertile women Am J Obstet Gynecol 1996;174:620–623. Bazot M, Daraï E. Sonography and MR imaging for the assessment of deep pelvic endometriosis. J Minim Invasive Gynecol 2005;12:178–185. Bedaiwy MA, Falcone T. Laboratory testing for endometriosis. Clin Chim Acta 2004;340:41–56. Matalliotakis IM, Goumenou AG, Mulayim N, Karkavitsas N, Koumantakis EE. High concentrations of the CA-125, CA 19-9 and CA 15-3 in the peritoneal fluid between patients with and without endometriosis. Arch Gynecol Obstet 2005;271:40–45. Fraser IS. Recognising, understanding and managing endometriosis. J Hum Reprod Sci 2008;1:56–64. Al-Jefout M, Dezarnaulds G, Cooper M et al. Diagnosis of endometriosis by detection of nerve fibres in an endometrial biopsy: a double blind study. Hum Reprod 2009;24:2972–2973. Hummelshoj L, Prentice A, Groothuis P. Update on endometriosis. Women s Health 2006;2:53–56. Further information. A definitive diagnosis of endometriosis requires laparoscopy, ideally combined with histology, to identify the presence of endometriotic lesions. However, laparoscopic facilities are not universally available. Physicians and patients may also agree that it is not appropriate to perform this invasive procedure, with its associated risks, according to individual circumstances. In these situations, a physician may make a presumptive diagnosis based on the signs and symptoms alone. Laboratory tests have, to date, failed to show predictive value. In future, alternative techniques may offer a less invasive diagnosis than laparoscopy. Non-invasive imaging techniques such as MRI and ultrasound may assist in diagnosing certain forms of endometriosis. The detection of nerve fibres in biopsies of eutopic endometrium is recently reported to have a diagnostic accuracy similar to laparoscopy [Al-Jefout et al, 2009]. As a consequence of the difficulties in diagnosing endometriosis, there is commonly a delay between the first appearance of symptoms and a definitive diagnosis. An international survey reported that the average delay is 8.3 years [Hummelshoj et al, 2006]. Kennedy S, Bergqvist A, Chapron C, et al. Hum Reprod 2005; Mounsey AL, Wilgus A, Slawson DC. Am Fam Phys 2006; Matorras R, Rodríguez F, Pijoan JI, et al. Am J Obstet Gynecol 1996; Bazot et al. J Minim Invasive Gynecol 2005; Bedawy et al. Clin Chem Acta 2004; Matalliotakis et al. Arch Gynecol Obstet 2005; Fraser et al. J Hum Reprod Sci")
10
Endometriosis: Treatment Current Treatment Options

11
Surgical Therapy Aimed at removing endometrial implants and restoring fertility Efficacy reflects the skill of the surgeon Recurrence is common: 40–50% at 5 years1,2 References Mounsey AL, Wilgus A, Slawson DC. Diagnosis and management of endometriosis. Am Fam Phys 2006;74:594–600. Guo SW. Recurrence of endometriosis and its control. Hum Reprod Update 2009;15:441–461. Further information Surgery is a common treatment option. Surgical intervention involves excision or ablation of endometriotic lesions, the removal of endometriotic cysts and the division of adhesions, frequently combined with follow-up medical therapy. The success of surgical intervention reflects the skill of the practitioner, and recurrence of endometriosis is common (e.g. the 5-year recurrence rate is approximately 40–50%) [Guo 2009]. Mounsey AL, Wilgus A, Slawson DC. Am Fam Phys 2006; Guo SW. Hum Reprod Update 2009.
 [Guo 2009]. Mounsey AL, Wilgus A, Slawson DC. Am Fam Phys 2006; Guo SW. Hum Reprod Update")
12
Cerrahi Her 4 kadından yaklaşık 1’inde ilk ameliyattan sonra 4 yıl içinde ek cerrahi tedavi gerekir1 İlk ameliyatını genç yaşta olan kadınlarda yeniden operasyon riski artar2,3 Kadınların % 20-40’ı konservatif cerrahi sonrasi iyilesme belirtileri göstermez1 Lezyonlar tamamıyla eksize edilmeyebilir Endometrioma cerrahisinden dolayı over rezervinin zarar görmesi olasıdır2 Weir E, Mustard C, Cohen M, et al. Endometriosis: what is the risk of hospital admission, readmission, and major surgical intervention? J Minim Invasive Gynecol 2005;12:486-93 Cheong Y, Tay P, Luk F, et al. Laparoscopic surgery for endometriosis: how often do we need to re-operate? J Obstet Gynaecol 2008;28:82-5 Shakiba K, Bena JF, McGill KM, Minger J, Falcone T. Surgical treatment of endometriosis: a 7-year follow-up on the requirement for further surgery. Obstet Gynecol 2008;111:1285–1292. Abbott J, Hawe J, Hunter D, Holmes M, Finn P, Garry R. Laparoscopic excision of endometriosis: a randomized, placebo-controlled trial. Fertil Steril 2004;82:878–884. Johnson NP & Hummelsoj L. Hum Reprod (6): Leyland N, et al. J Obstet Gynaecol Can 2010;32(7 Suppl 2):S1–S32. Guo S-W. Hum. Reprod Update 2009;15(4):441–461.. Weir E et al. J Minim Invasive Gynecol 2005; 12: 486−93 Cheong Y et al. J Obstet Gynaecol 2008; 28: 82−85 Shakiba K et al. Obstet Gynecol 2008; 111: 1285–1292
: Leyland N, et al. J Obstet Gynaecol Can 2010;32(7 Suppl 2):S1–S32. Guo S-W. Hum. Reprod Update 2009;15(4):441–461.. Weir E et al. J Minim Invasive Gynecol 2005; 12: 486−93. Cheong Y et al. J Obstet Gynaecol 2008; 28: 82−85. Shakiba K et al. Obstet Gynecol 2008; 111: 1285–1292.")
13
Tedaviye yaklaşım Endometriozis hayat boyu tedavi planı gerektiren kronik bir hastalık olup; hedef, mümkün olduğunca tekrarlanan cerrahi müdahalelerden kaçınıp, medikal tedaviyi maksimum düzeyde kullanmaktır. Reference Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis. Fertil Steril 2008;90:(Suppl 3):S260–S269. Further information A recent review from the Practice Committee of the American Society for Reproductive Medicine included the clear-stated summary quoted above in relation to the treatment aims in endometriosis. Practice Committee of the American Society for Reproductive Medicine. Fertil Steril 2008. 13
:S260–S269. Further information. A recent review from the Practice Committee of the American Society for Reproductive Medicine included the clear-stated summary quoted above in relation to the treatment aims in endometriosis. Practice Committee of the American Society for Reproductive Medicine. Fertil Steril")
14
WES international consensus on endometriosis
Pelvik ağrıya erken ve etkin bir şekilde müdahale etmeyi önerir. “Pelvik ağrıya müdahale, endometriosisin cerrahi olarak kanıtı beklenmeksizin yapılmalı ve gecikmeye neden olunmamalıdır.” Further information: The World Endometriosis Society brought together experts from national and international endometriosis societies The views of women with endometriosis were also represented “The fundamental aim of gynaecologists treating endometriosis must be the definition of personalised, long-term, treatment strategies that take into consideration the individual woman’s point of view, as well as her priority for different outcomes.” The World Endometriosis Society (WES) initiated a process to bring together representatives of national and international, medical and non-medical societies with an interest in endometriosis with the aim of reaching a consensus on the management of endometriosis, in which the views of women with endometriosis were represented. This consensus advocates early, proactive management of pelvic pain and supports the use of both empirical and adjuvant medical therapy The consensus positions Visanne as a first-line medical treatment for endometriosis Although not an official guideline, this consensus is strongly supported by an extensive, experienced and well-respected group of key opinion leaders and representatives of medical societies from across our regions Many clinicians support empirical medical treatment of endometriosis prior to or in the absence laparoscopic confirmation Management of pelvic pain should not be delayed in order to obtain surgical confirmation of endometriosis NSAIDs, COCs and progestins such as medroxyprogesterone acetate, norethisterone or newer progestins such as dienogest should be considered for use as first-line empirical medical treatment. Johnson NP and Hummelsoj L. Hum Reprod 2013; 28(6): 1552–1568.
 initiated a process to bring together representatives of national and international, medical and non-medical societies with an interest in endometriosis with the aim of reaching a consensus on the management of endometriosis, in which the views of women with endometriosis were represented. This consensus advocates early, proactive management of pelvic pain and supports the use of both empirical and adjuvant medical therapy. The consensus positions Visanne as a first-line medical treatment for endometriosis. Although not an official guideline, this consensus is strongly supported by an extensive, experienced and well-respected group of key opinion leaders and representatives of medical societies from across our regions. Many clinicians support empirical medical treatment of endometriosis prior to or in the absence laparoscopic confirmation. Management of pelvic pain should not be delayed in order to obtain surgical confirmation of endometriosis. NSAIDs, COCs and progestins such as medroxyprogesterone acetate, norethisterone or newer progestins such as dienogest should be considered for use as first-line empirical medical treatment. Johnson NP and Hummelsoj L. Hum Reprod 2013; 28(6): 1552–1568.")
15
Growing support for empirical treatment
ESHRE Clinical guidelines WES International consensus statement Two key publications in 2013 advocate the use of initiating empirical medical treatment in the absence of laparoscopically confirmed diagnosis ESHRE=European Society of Human Reproduction and Embryology; WES=World Endometriosis Society. 15

16
Medikal Tedavi Progestinler Danazol Kombine oral kontraseptifler
GnRH agonistleri Levonorgestrel-IUD NSAI Aromatase inhibitörler Progesteron reseptör modülatörleri

17
İdeal endometriozis ilacı
Endometriozis odakları baskılanmalı - engellenmeli Semptomlar ortadan kalkmalı Yaşam kalitesini yükseltmeli Tedavi kesildikten sonrada etkisi devam etmeli (rekürensini engellemeli) Menstrüel siklus etkilenmemeli Yan etki profili kabul edilebilir olmalı, uzun süreli kullanıma uygun olmalı Gebe kalmak isteyen kadınlar için güvenli olmalı Ucuz olmalı
 Menstrüel siklus etkilenmemeli. Yan etki profili kabul edilebilir olmalı, uzun süreli kullanıma uygun olmalı. Gebe kalmak isteyen kadınlar için güvenli olmalı. Ucuz olmalı.")
18
Endometriosis: Treatment
Non-specific Therapies

19
Medical therapy – NSAIDs
In primary dysmenorrhea: NSAIDs have been shown to be effective compared to placebo1 But in endometriosis: NSAIDs show no clear benefit; limited data – only 1 RCT in 24 women2 Non-specific therapies – not approved in endometriosis Including non-steroidal anti-inflammatory drugs and combined oral contraceptives References Nothnick WB. The emerging use of aromatase inhibitors for endometriosis treatment. Reprod Biol Endocrinol. 2011;9:87. Kulak J, Jr., Fischer C, Komm B et al. Treatment with bazedoxifene, a selective estrogen receptor modulator, causes regression of endometriosis in a mouse model. Endocrinology. 2011; 152: Further information A range of medical therapies may be used in endometriosis. These medications can be categorized into: Specific therapies approved in the treatment of endometriosis – e.g. gonadotropin-releasing hormone (GnRH) agonists, danazol and certain progestins. Non-specific therapies that are not specifically approved in endometriosis or are used off-label – including non-steroidal anti-inflammatory drugs (NSAIDs) and combined oral contraceptives (COCs) Marjoribanks J et al. Cochrane Database Syst Rev 2010 Allen C et al. Cochrane Database Syst Rev 2009 19
 agonists, danazol and certain progestins. Non-specific therapies that are not specifically approved in endometriosis or are used off-label – including non-steroidal anti-inflammatory drugs (NSAIDs) and combined oral contraceptives (COCs) Marjoribanks J et al. Cochrane Database Syst Rev Allen C et al. Cochrane Database Syst Rev")
20
NSAIDs General, non-specific pain relief
Controlled trial data lacking1,2 No single NSAID shows superior efficacy1 Potential adverse effects in gastrointestinal tract1,2 Reference Allen C, Hopewell S, Prentice A. Non-steroidal anti-inflammatory drugs for pain in women with endometriosis. Cochrane Database Syst Rev 2005;4:CD Further information NSAIDs may provide general, non-specific pain relief in endometriosis. However, these agents are not approved in the management of endometriosis, controlled trial data to support their use are lacking, and there is no evidence to show whether any individual NSAID is more effective than another [Allen et al 2009]. A particular concern with the long-term use of NSAIDs is their well-known propensity to cause adverse effects in the gastrointestinal tract [Allen et al 2005]. NSAID, non-steroidal anti-inflammatory drug. Allen C, Hopewell S, Prentice A. Cochrane Database Syst Rev 2005; Kennedy S et al. Hum Reprod 2005.

21
Kombine Oral Kontraseptifler
Kombine oral kontraseptifler, endometriozisin tedavisindeki yerleri kanıtlanmamasına rağmen yaygın olarak kullanılmaktadır. RCT eksikliği Endometrioziste oral kontraseptiflerin östrojen komponentinin varlığı tedaviye tezat teşkil etmektedir. Estrogenik yan etkiler(bulantı, kilo alınımı, su retansiyonu, artmış tromboemboli riski)1 References Davis LJ, Kennedy SS, Moore J, Prentice A. Oral contraceptives for pain associated with endometriosis. Cochrane Database Syst Rev 2007;3:CD Crosignani P, Olive D, Bergqvist A, Luciano A. Advances in the management of endometriosis: an update for clinicians. Hum Reprod Update 2006;12:179–189. Further information Although COCs are widely used in clinical practice to treat the symptoms of endometriosis, these agents are not approved for this indication in most countries. There is a lack of clinical trial evidence to support the use of COCs in endometriosis, and treatment guidelines can therefore offer limited guidance on COC regimens. As a putative mode of action for hormonal therapies in endometriosis is via counteracting the effects of estrogen at the uterus, the inclusion of an estrogen in a medication may appear counter-productive. Debate also continues on whether the estrogen content of COCs may mask the development of the condition. COCs are associated with adverse events such as nausea, weight gain, and bloating and with increased thromboembolic risk. Davis LJ, Kennedy SS, Moore J et al. Cochrane Database Syst Rev 2007; Crosignani P, Olive D, Bergqvist A et al. Hum Reprod Update 2006.
1. References. Davis LJ, Kennedy SS, Moore J, Prentice A. Oral contraceptives for pain associated with endometriosis. Cochrane Database Syst Rev 2007;3:CD Crosignani P, Olive D, Bergqvist A, Luciano A. Advances in the management of endometriosis: an update for clinicians. Hum Reprod Update 2006;12:179–189. Further information. Although COCs are widely used in clinical practice to treat the symptoms of endometriosis, these agents are not approved for this indication in most countries. There is a lack of clinical trial evidence to support the use of COCs in endometriosis, and treatment guidelines can therefore offer limited guidance on COC regimens. As a putative mode of action for hormonal therapies in endometriosis is via counteracting the effects of estrogen at the uterus, the inclusion of an estrogen in a medication may appear counter-productive. Debate also continues on whether the estrogen content of COCs may mask the development of the condition. COCs are associated with adverse events such as nausea, weight gain, and bloating and with increased thromboembolic risk. Davis LJ, Kennedy SS, Moore J et al. Cochrane Database Syst Rev 2007; Crosignani P, Olive D, Bergqvist A et al. Hum Reprod Update")
22
Low-dose oral contraceptive pill for dysmenorrhea associated with endometriosis: a placebo-controlled, double-blind, randomized trial N: 100 Objective: To evaluate the efficacy of a low-dose oral contraceptive pill (OCP) for patients with dysmenorrhea associated with endometriosis. Design: A double-blind, randomized, placebo-controlled trial. Settings: Clinical trial sites in Japan. Patient(s): One hundred patients with dysmenorrhea associated with endometriosis. Most enrolled patients had radiologic evidence of endometriosis rather than surgical diagnosis. Intervention(s): Patients were randomly assigned to receive either monophasic OCP (ethinylestradiol plus norethisterone) or placebo. Participants used their usual pain medications as needed during the trial. Main Outcome Measure(s): After four cyclic treatments, we used a zero- to three-point verbal rating scale and a visual analogue scale to measure the severity of disability because of dysmenorrhea in daily life, and the patients’ use of analgesics. Result(s): Total dysmenorrhea scores assessed by the verbal rating scale were significantly decreased at the end of treatment in both groups. From the first cycle through the end of treatment, dysmenorrhea in the OCP group was significantly milder than in the placebo group. Nonmenstrual pelvic pain was present at baseline in 24.5% (12 of 49) of the OCP group and 34.0% (16 of 47) of the placebo group. The volume of endometrioma (larger than 3 cm in diameter) was significantly decreased in the OCP group, but not in the placebo group. No serious adverse events related to using OCPs occurred. Conclusion(s): The present study clearly demonstrated for the first time that OCPs could be used to effectively and safely treat pain associated with endometriosis. ( Tasuku Harada, 2008
 for patients with dysmenorrhea. associated with endometriosis. Design: A double-blind, randomized, placebo-controlled trial. Settings: Clinical trial sites in Japan. Patient(s): One hundred patients with dysmenorrhea associated with endometriosis. Most enrolled patients had. radiologic evidence of endometriosis rather than surgical diagnosis. Intervention(s): Patients were randomly assigned to receive either monophasic OCP (ethinylestradiol plus norethisterone) or placebo. Participants used their usual pain medications as needed during the trial. Main Outcome Measure(s): After four cyclic treatments, we used a zero- to three-point verbal rating scale and. a visual analogue scale to measure the severity of disability because of dysmenorrhea in daily life, and the patients’ use of analgesics. Result(s): Total dysmenorrhea scores assessed by the verbal rating scale were significantly decreased at the end of. treatment in both groups. From the first cycle through the end of treatment, dysmenorrhea in the OCP group was. significantly milder than in the placebo group. Nonmenstrual pelvic pain was present at baseline in 24.5% (12 of. 49) of the OCP group and 34.0% (16 of 47) of the placebo group. The volume of endometrioma (larger than 3 cm in. diameter) was significantly decreased in the OCP group, but not in the placebo group. No serious adverse events. related to using OCPs occurred. Conclusion(s): The present study clearly demonstrated for the first time that OCPs could be used to effectively and. safely treat pain associated with endometriosis. ( Tasuku Harada,")
23
Randomized trial of leuprolide versus continuous oral contraceptives in the treatment of endometriosis-associated pelvic pain (n: 47, 48 w) Objective: To compare the efficacy of leuprolide and continuous oral contraceptives in the treatment of endometriosis-associated pain. Design: Prospective, randomized, double-blind controlled trial. Setting: Academic medical centers in Rochester, New York, and Boston, Massachusetts. Patient(s): Forty-seven women with endometriosis-associated pelvic pain. Intervention(s): Forty-eight weeks of either depot leuprolide, mg IM every 12 weeks with hormonal add-back using norethindrone acetate 5 mg orally, daily; or a generic monophasic oral contraceptive (1 mg norethindrone þ 35 mg ethinyl estradiol) given daily. Main Outcome Measure(s): Biberoglu and Behrman (B&B) pain scores, numerical rating scores (NRS), Beck Depression Inventory (BDI), and Index of Sexual Satisfaction (ISS). Result(s): Based on enrollment of 47 women randomized to continuous oral contraceptives and to leuprolide, there were statistically significant declines in B&B, NRS, and BDI scores from baseline in both groups. There were no significant differences, however, in the extent of reduction in these measures between the groups. Conclusion(s): Leuprolide and continuous oral contraceptives appear to be equally effective in the treatment of endometriosis-associated pelvic pain. David S. Guzick, 2011
: Forty-seven women with endometriosis-associated pelvic pain. Intervention(s): Forty-eight weeks of either depot leuprolide, mg IM every 12 weeks with hormonal. add-back using norethindrone acetate 5 mg orally, daily; or a generic monophasic oral contraceptive (1 mg. norethindrone þ 35 mg ethinyl estradiol) given daily. Main Outcome Measure(s): Biberoglu and Behrman (B&B) pain scores, numerical rating scores (NRS), Beck. Depression Inventory (BDI), and Index of Sexual Satisfaction (ISS). Result(s): Based on enrollment of 47 women randomized to continuous oral contraceptives and to leuprolide, there. were statistically significant declines in B&B, NRS, and BDI scores from baseline in both groups. There were no. significant differences, however, in the extent of reduction in these measures between the groups. Conclusion(s): Leuprolide and continuous oral contraceptives appear to be equally effective in the treatment of. endometriosis-associated pelvic pain. David S. Guzick,")
24
Endometriosis: Treatment
Specific Therapies

25
Hormonal Therapy* GnRH agonists Progestins Androgens
(suppression of FSH/LH via desensitisation and down-regulation of pituitary GnRH receptors) Leuprolin Goserelin Buserelin Triptorelin Nafarelin Avorelin Progestins (suppression of FSH/LH, some have additional properties, e.g. anti-inflammatoric) MPA (oral/im/sc) Dydrogesterone Norethisterone Dienogest Gestrinone References Vercellini P, Somigliana E, Viganò P, Abbiati A, Daguati R, Crosignani PG. Endometriosis: current and future medical therapies. Best Pract Res Clin Obstet Gynaecol 2008;22: Mihalyi A, Simsa P, Mutinda KC, Meuleman C, Mwenda JM, D'Hooghe TM. Emerging drugs in endometriosis. Expert Opin Emerg Drugs 2006;11: Further information Here is a list of the hormonal therapies widely approved in the treatment of endometriosis. Androgens (suppression of FSH/LH, anti-estrogenic and hyperandrogenism) Danazol * Not all products available in all countries. FSH, follicle stimulating hormone; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone; MPA, medroxyprogesterone acetate Vercellini et al. Best Pract Res Clin Obstet Gynaecol 2008; Mihalyi et al. Expert Opin Emerg Drugs 2006. 25
 Leuprolin. Goserelin. Buserelin. Triptorelin. Nafarelin. Avorelin. Progestins. (suppression of FSH/LH, some have additional properties, e.g. anti-inflammatoric) MPA (oral/im/sc) Dydrogesterone. Norethisterone. Dienogest. Gestrinone. References. Vercellini P, Somigliana E, Viganò P, Abbiati A, Daguati R, Crosignani PG. Endometriosis: current and future medical therapies. Best Pract Res Clin Obstet Gynaecol 2008;22: Mihalyi A, Simsa P, Mutinda KC, Meuleman C, Mwenda JM, D Hooghe TM. Emerging drugs in endometriosis. Expert Opin Emerg Drugs 2006;11: Further information. Here is a list of the hormonal therapies widely approved in the treatment of endometriosis. Androgens. (suppression of FSH/LH, anti-estrogenic and hyperandrogenism) Danazol. * Not all products available in all countries. FSH, follicle stimulating hormone; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone; MPA, medroxyprogesterone acetate. Vercellini et al. Best Pract Res Clin Obstet Gynaecol 2008; Mihalyi et al. Expert Opin Emerg Drugs")
26
Endometriosis: Treatment
GnRH Agonists

27
. Effect of Gonadotropin-Releasing Hormone (GnRH) Agonists on Endometriosis
Figure 1. Effect of Gonadotropin-Releasing Hormone (GnRH) Agonists on Endometriosis. Endometriosis is maintained by estrogen, resulting from hypothalamic–pituitary stimulation of ovarian estrogen production. Endometriosis is also responsible for stimulation of many aspects of the immune system, the nervous system, and the endocrine system. GnRH agonists inhibit the secretion of follicle-stimulating hormone (FSH), preventing ovarian production of estrogen and creating a hypoestrogenic state. This inhibits the development, maintenance, and growth of endometriosis, which in turn alters the effect on the immune, nervous, and endocrine systems. The hypoestrogenemia also has direct effects on these systems, further altering their status from that seen in patients with active endometriosis.
 Agonists on Endometriosis. Endometriosis is maintained by estrogen, resulting. from hypothalamic–pituitary stimulation of ovarian estrogen. production. Endometriosis is also responsible. for stimulation of many aspects of the immune system, the nervous system, and the endocrine system. GnRH. agonists inhibit the secretion of follicle-stimulating. hormone (FSH), preventing ovarian production of estrogen. and creating a hypoestrogenic state. This inhibits. the development, maintenance, and growth of endometriosis, which in turn alters the effect on the. immune, nervous, and endocrine systems. The hypoestrogenemia. also has direct effects on these systems, further altering their status from that seen in patients. with active endometriosis.")
28
GnRH Agonists Considered ‘gold-standard’ treatment for endometriosis due to high efficacy in pain relief GnRH agonists promote atrophy of endometriotic lesions and induce amenorrhea Hypoestrogenic side-effects (e.g. hot flushes, vaginal dryness, loss of libido), including BMD decrease Limited to short-term use (6 months) in absence of ‘add-back’ therapy Caution in younger women not reached maximum BMD References Winkel CA, Scialli AR. Medical and surgical therapies for pain associated with endometriosis. J Women’s Health Gender-Based Med 2001;10:137–162. Sinaii N, Cleary SD, Younes N et al. Treatment utilization for endometriosis symptoms: a cross-sectional survey study of lifetime experience. Fertil Steril 2007;87:1277–1286. Crosignani P, Olive D, Bergqvist A, Luciano A. Advances in the management of endometriosis: an update for clinicians. Hum Reprod Update 2006;12:179–189. Mounsey AL, Wilgus A, Slawson DC. Diagnosis and management of endometriosis. Am Fam Phys 2006;74:594–600. Further information GnRH agonists are established as a gold-standard therapy for endometriosis because of their high efficacy in pain relief, but their use is limited by adverse effects. GnRH agonists promote atrophy of endometriotic lesions and induce amenorrhea by strongly reducing estrogen production, but these agents consequently may give rise to typical symptoms of estrogen deprivation (e.g. hot flushes, vaginal dryness, loss of libido). A particular safety concern with GnRH agonists is accelerated loss of bone mass due to the low estrogen levels, which elevates the risk for osteoporosis and limits the use of GnRH agonists to 6 months in the absence of add-back estrogen therapy. Although add-back therapy can prolong the duration of GnRH agonist therapy, this approach adds to the cost of therapy and the optimal regimens have not been established. In younger women who have not reached maximum bone density, the risk of bone mass loss requires particularly careful consideration before GnRH agonists are used. GnRH, gonadotropin-releasing hormone; BMD, bone mineral density. Winkel CA et al. J Women’s Health Gender-Based Med 2001; Sinaii N et al. Fertil Steril 2007; Crosignani P et al. Hum Reprod Update 2006; Mounsey AL et al. Am Fam Phys 2006.
, including BMD decrease. Limited to short-term use (6 months) in absence of ‘add-back’ therapy. Caution in younger women not reached maximum BMD. References. Winkel CA, Scialli AR. Medical and surgical therapies for pain associated with endometriosis. J Women’s Health Gender-Based Med 2001;10:137–162. Sinaii N, Cleary SD, Younes N et al. Treatment utilization for endometriosis symptoms: a cross-sectional survey study of lifetime experience. Fertil Steril 2007;87:1277–1286. Crosignani P, Olive D, Bergqvist A, Luciano A. Advances in the management of endometriosis: an update for clinicians. Hum Reprod Update 2006;12:179–189. Mounsey AL, Wilgus A, Slawson DC. Diagnosis and management of endometriosis. Am Fam Phys 2006;74:594–600. Further information. GnRH agonists are established as a gold-standard therapy for endometriosis because of their high efficacy in pain relief, but their use is limited by adverse effects. GnRH agonists promote atrophy of endometriotic lesions and induce amenorrhea by strongly reducing estrogen production, but these agents consequently may give rise to typical symptoms of estrogen deprivation (e.g. hot flushes, vaginal dryness, loss of libido). A particular safety concern with GnRH agonists is accelerated loss of bone mass due to the low estrogen levels, which elevates the risk for osteoporosis and limits the use of GnRH agonists to 6 months in the absence of add-back estrogen therapy. Although add-back therapy can prolong the duration of GnRH agonist therapy, this approach adds to the cost of therapy and the optimal regimens have not been established. In younger women who have not reached maximum bone density, the risk of bone mass loss requires particularly careful consideration before GnRH agonists are used. GnRH, gonadotropin-releasing hormone; BMD, bone mineral density. Winkel CA et al. J Women’s Health Gender-Based Med 2001; Sinaii N et al. Fertil Steril 2007; Crosignani P et al. Hum Reprod Update 2006; Mounsey AL et al. Am Fam Phys")
29
Estradiol Concentration (pg/mL)
Endometriosis Overview The Estrogen Threshold Hypothesis Percent of Maximal Response Stimulation of Endometriosis Lesions Therapeutic Window 100 Bone Loss Minimal 80 Bone Turnover Endometriosis Growth 60 40 Bone Loss Substantial Atrophy of Endometriosis Lesions 20 10 20 30 40 50 60 70 80 90 100 Estradiol Concentration (pg/mL) Barbieri (1992)
 Barbieri (1992)")
30
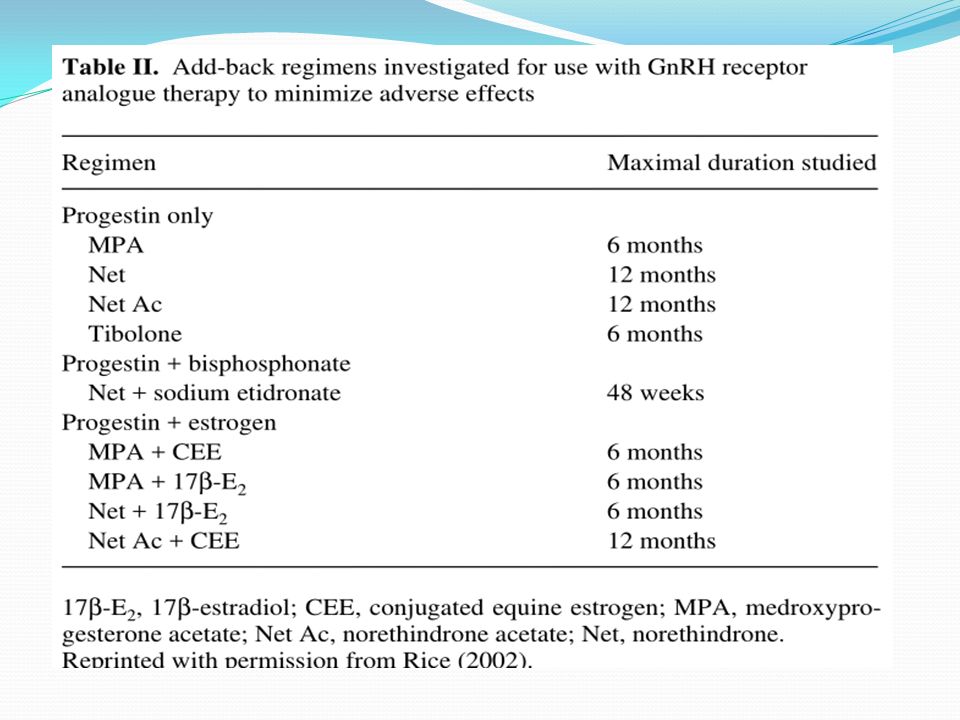
Add-Back Therapy Estrogens ± Progestins (Do not use OCP) Progestins
Progestins ± Bisphosphonate Tibolone GnRHa 3 mo No need for Add-back GnRHa 6 mo Add-back (Optional), Ca GnRHa > 6 mo or retreatment Mandatory Add-back, Ca, BMD, Lipids ?
, Ca. GnRHa > 6 mo or retreatment. Mandatory Add-back, Ca, BMD, Lipids")
32
Treatment with leuprolide acetate and hormonal add-back for up to 10 years in stage IV endometriosis patients with chronic pelvic pain (n: 5) This pilot study examined the effect of a low-dose E and pulsed progestogen hormone therapy (HT) regimen for add-back during long-term GnRH-agonist therapy on bone mineral density (BMD) in five patients with stage IV endometriosis. Bone mineral density was stable after initiation of HT for the entire follow-up period (up to 10 years). One patient stopped her treatment on two occasions to conceive and was successful each time with delivery of a normal baby. No patient had return of pelvic pain after HT add-back. (Fertil Steril 2006; 86:220 –2. ©2006 Mohamed A. Bedaiwy, 2006
 regimen. for add-back during long-term GnRH-agonist therapy on bone mineral density (BMD) in five patients with. stage IV endometriosis. Bone mineral density was stable after initiation of HT for the entire follow-up period. (up to 10 years). One patient stopped her treatment on two occasions to conceive and was successful each time. with delivery of a normal baby. No patient had return of pelvic pain after HT add-back. (Fertil Steril 2006; 86:220 –2. ©2006. Mohamed A. Bedaiwy,")
33
Gonadotropin-releasing hormone agonist and add-back therapy: what do the data show?
Effective add-back therapy should be initiated concomitantly with the GnRHa to minimize side effects. For the woman who requires retreatment with a GnRHa or whose therapy is anticipated to extend beyond 6 months, add-back should be considered mandatory Eric S. Surrey, 2010

34
Endometriosis: Treatment
Progestins

35
Endometriozis tedavisinde sentetik progesteron kullanımının temeli
Progestins Reduction of serum estrogen levels Decidualisation + atrophy of endometrial tissue Immunomodulatory effect Inhibition of matrix metalloproteinases References: Lazzeri L, Luisi S, Petraglia F. Progestins for the treatment of endometriosis: an update. J Endometriosis 2010; 2: Kappou D, Matalliotakis M, Matalliotakis I. Medical treatments for endometriosis. Minerva Ginecol. 2010;62: Crosignani P, Olive D, Bergqvist A, Luciano A. Advances in the management of endometriosis: an update for clinicians. Hum Reprod Update ;12:179–189. Anti-inflammatory effect Anti-angiogenic effect Lazzeri L, et al. J Endometriosis 2010;2:169–181; Kappou D, et al. Minerva Ginecol 2010;62:415–432; CrosignanI P, et al. Hum Reprod Update 2006;12:179–189

36
Mechanism of action of progestins in the treatment of endometriosis
Mechanism of action of progestins in the treatment of endometriosis. The cause of endometriosis may be implantation or metaplasia but the local reaction is the same: the implants grow and invade the tissue in their vicinity, causing inflammatory reactions. Progestins reduce the elevated activity of metalloproteinases and growth factors. The inflammatory reactions in and around the endometriotic implant are suppressed and, in addition, the peripheral estrogen levels are minimized via negative feedback to the hypothalamic–pituitary axis.

37
Endometriozisin medikal tedavisinde kullanılan progestinler
Oral yol Noretisteron asetat Didrogesteron MPA Dienogest İntramusküler yol Medroksiprogesteron asetat İntrauterin yol Levonorgestrel salgılayan RIA Implant Etonogestrel

38
Endometrioziste sentetik progesteron tedavisi

39
Dienogest:Farmakolojik Özellikler
Dienogest, 19-nortestosteron türevleri ile progesteron türevlerinin özelliklerini birleştiren bir progestindir 19-nortestosteron türevlerinin özellikleri Endometriyum üzerinde güçlü progestasyonel etki Yaklaşık 9-10 saatlik görece kısa plazma yarı ömrü >% 90 yüksek oral biyoyararlanım Progesteron türevlerinin özellikleri İyi tolere edilebilirlik Anti-androjenik etkiler Anti-proliferatif etkiler Görece düşük gonadotropin sekresyonu inhibisyonu CV ve metabolik sistem üzerine nötr etki References Oettel M, Carol W, Elger W. A 19-norprogestin without 17α-ethinyl group II: dienogest from a pharmacodynamic point of view. Drugs Today 1995:31:517–536. Sasagawa S, Shimizu Y, Kami H et al. Dienogest is a selective progesterone receptor agonist in transactivation analysis with potent oral endometrial activity due to its efficient pharmacokinetic profile. Steroids 2008;73:222–231. Further information Advantages that dienogest shares with other 19-nortestosterone derivatives include: a strong progestational effect on the endometrium, a relatively short plasma half-life of approximately 10 hours and high oral bioavailability >90%. The progesterone-like properties demonstrated by dienogest include a good tolerability profile, anti-androgenic activity and relatively moderate inhibition of gonadotropin secretion [Oettel et al, 1999; Sasagawa et al, 2008]. The anti-androgenic activity of dienogest is a significant characteristic. In contrast, many other progestins are characterised by adverse effects that are androgenic in nature. Additional double bond (Strong affinity to progesterone receptors) Cyanomethyl instead of an ethinyl group in the 17α position (Low interaction with hepatic proteins e.g Cytochrome P450) Oettel M et al. Drugs Today 1995; Sasagawa S et al. Steroids 2008. 39
 Cyanomethyl instead of an ethinyl group in the 17α position. (Low interaction with hepatic proteins e.g Cytochrome P450) Oettel M et al. Drugs Today 1995; Sasagawa S et al. Steroids")
40
Dienogest tedavisi sırasında istenmeyen ilaç reaksiyonlarının sıklığı (Toplu Analiz)
15 haftaya kadar uzayan dienogest tedavisi sırasında bildirilen istenmeyen ilaç reaksiyonları (İAR) Düşük sıklıkta ve Genellikle hafif-orta şiddettedirler, Genellikle ilk 3 ay içinde ortadan kalkarlar. En sık bildirilen İAR’ler Hastaların oranı Baş ağrısı %9.0 Memelerde hassasiyet %5.4 Depresif duygudurum %5.1 Akne Köhler G, et al. Int J Gynaecol Obstet 2010; 108: 21–25 Strowitzki T, et al. Eur J Obstet Gynecol Reprod Biol 2010 ;151: 193–198 Strowitzki T, et al. Hum Reprod 2010; 25: 633–641 Petraglia F, et al. Arch Gynecol Obstet 2012; 285(1): 167‒173
 Düşük sıklıkta ve. Genellikle hafif-orta şiddettedirler, Genellikle ilk 3 ay içinde ortadan kalkarlar. En sık bildirilen İAR’ler. Hastaların oranı. Baş ağrısı. %9.0. Memelerde hassasiyet. %5.4. Depresif duygudurum. %5.1. Akne. Köhler G, et al. Int J Gynaecol Obstet 2010; 108: 21–25. Strowitzki T, et al. Eur J Obstet Gynecol Reprod Biol 2010 ;151: 193–198. Strowitzki T, et al. Hum Reprod 2010; 25: 633–641. Petraglia F, et al. Arch Gynecol Obstet 2012; 285(1): 167‒173.")
41
Uzun süreli endometriozis tedavisinde dienogest deneyimleri
Tedaviden önce: hastaları kanamanın ilaç etkisinin yetersizliğine ait bir belirti olmadığı konusunda bilgilendirin Hastaların ~ %20’sinde ilk 3 ayda düzensiz kanama görülmektedir Siklusun ilk gününde başlanır Yüksek risk gruplarında, ilk 6 ya da 8 hafta 4 mg (off-label) dienogest ile iyi sonuç alınmaktadır (başlangıçtaki düzensiz kanama oranları daha düşük olmaktadır) Halen dienogest kullanmakta olan hastalar Atrofik (ince) endometriumdan kanama Kanamanın sorun yaratması halinde tedaviyi kesin ve 5 gün sonra yeniden başlatın Hastalar tek başına kanamadan çok, kanamaya ağrının eşlik etmesi durumunda endişe duymaktadır Hastaların, kanama paternindeki değişiklikler konusunda uyarılması önemlidir
 dienogest ile iyi sonuç alınmaktadır (başlangıçtaki düzensiz kanama oranları daha düşük olmaktadır) Halen dienogest kullanmakta olan hastalar. Atrofik (ince) endometriumdan kanama. Kanamanın sorun yaratması halinde tedaviyi kesin ve 5 gün sonra yeniden başlatın. Hastalar tek başına kanamadan çok, kanamaya ağrının eşlik etmesi durumunda endişe duymaktadır. Hastaların, kanama paternindeki değişiklikler konusunda uyarılması önemlidir.")
42
Depot MPA in Endometriosis
Depot MPA 150 mg intramuscularly investigated Lower dose formulation (104 mg, subcutaneously) approved in USA1 Effect on bone mineral density2 Black box warning: ‘Women who use depo-subQ provera 104 may lose significant bone mineral density’ ‘Bone loss is greater with increasing duration of use and may not be completely reversible’ Delay in resumption of ovulation at discontinuation2,3 References Crosignani PG, Luciano A, Ray A, Bergqvist A. Subcutaneous depot medroxyprogesterone acetate versus leuprolide acetate in the treatment of endometriosis-associated pain. Hum Reprod 2006b;21:248–256. Physician Information. depo-subQ provera 104 medroxyprogesterone acetate injectable suspension 104 mg/0.65 mL. Available at: (accessed January 2010). Vercellini P, Fedele L, Pietropaolo G, Frontino G, Somigliana E, Crosignani PG. Progestogens for endometriosis: forward to the past. Hum Reprod Update 2003;9:387–396. Further information Depot formulations of MPA are available, including depo-subQ provera 104, which has been approved recently for the treatment of endometriosis in the USA. With depot MPA, there is a concern that long-term use has an adverse impact on bone mineral density, while the delay in resumption of ovulation that follows discontinuation of therapy may be a contraindication to use in women who wish to conceive in the near future [Vercellini et al, 2003; Physician information 2009]. MPA, medroxyprogesterone acetate. Crosignani PG et al. Hum Reprod 2006; Physician information. 2009; Vercellini P et al. Hum Reprod Update 2003.
 approved in USA1. Effect on bone mineral density2. Black box warning: ‘Women who use depo-subQ provera 104 may lose significant bone mineral density’ ‘Bone loss is greater with increasing duration of use and may not be completely reversible’ Delay in resumption of ovulation at discontinuation2,3. References. Crosignani PG, Luciano A, Ray A, Bergqvist A. Subcutaneous depot medroxyprogesterone acetate versus leuprolide acetate in the treatment of endometriosis-associated pain. Hum Reprod 2006b;21:248–256. Physician Information. depo-subQ provera 104 medroxyprogesterone acetate injectable suspension 104 mg/0.65 mL. Available at: q=cache:pp1KgMPaQuoJ: (accessed January 2010). Vercellini P, Fedele L, Pietropaolo G, Frontino G, Somigliana E, Crosignani PG. Progestogens for endometriosis: forward to the past. Hum Reprod Update 2003;9:387–396. Further information. Depot formulations of MPA are available, including depo-subQ provera 104, which has been approved recently for the treatment of endometriosis in the USA. With depot MPA, there is a concern that long-term use has an adverse impact on bone mineral density, while the delay in resumption of ovulation that follows discontinuation of therapy may be a contraindication to use in women who wish to conceive in the near future [Vercellini et al, 2003; Physician information 2009]. MPA, medroxyprogesterone acetate. Crosignani PG et al. Hum Reprod 2006; Physician information. 2009; Vercellini P et al. Hum Reprod Update")
43
Depot MPA 150 mg: BMD Decline
Percentage change, spine BMD Controls Depot MPA Reference Clark MK, Sowers M, Levy B et al. Bone mineral density loss and recovery during 48 months in first-time users of depot medroxyprogesterone acetate. Fertil Steril 2006; 86:1466–1474. Further information The concern that depot MPA has an adverse impact on bone mineral density (BMD) has led to a black box warning from the Food and Drug Administration in the USA for 150 mg i.m. and 104 mg s.c. formulations. A study measuring hip and spine bone mineral density over 48 months in first-time users of depot MPA 150 mg for contraception identified substantial reductions in mean lumbar spinal BMD during treatment [Clark et al 2006]. Control patients received no hormonal treatment. After cessation of MPA treatment, recovery of BMD was prolonged. Months from baseline Label includes black box warning regarding bone mineral density BMD, bone mineral density. Modelled means and standard errors. Adapted from Clark MK, Sowers M, Levy B et al. Fertil Steril 2006. 43
 has led to a black box warning from the Food and Drug Administration in the USA for 150 mg i.m. and 104 mg s.c. formulations. A study measuring hip and spine bone mineral density over 48 months in first-time users of depot MPA 150 mg for contraception identified substantial reductions in mean lumbar spinal BMD during treatment [Clark et al 2006]. Control patients received no hormonal treatment. After cessation of MPA treatment, recovery of BMD was prolonged. Months from baseline. Label includes black box warning regarding bone mineral density. BMD, bone mineral density. Modelled means and standard errors. Adapted from Clark MK, Sowers M, Levy B et al. Fertil Steril")
44
Sadece progesteron içeren hormonal kontraseptif kullanımının endometriozisin primer önlenmesinde yeri var mıdır? Progestin kullanımı ile sağlanan terapötik amenore endometriozis yönetiminde faydalı bir yöntemdir. Endometriozis kronik ve rekürren bir hastalık olduğundan uzun süreli hormonal tedavinin uygulanması endometriozis olgularında tavsiye edilmektedir. Uzun süreli progestojen tedavisinin bir formu olan LNG-IUS, endometrial atrofiyi sağlayarak, apoptotik aktiviteyi arttırarak, antienflamatuar ve immunomodulator etkileri ile endometriozise bağlı şikayetlerin tedavisinde kesin etkilidir.

45
Revised guidelines, 2007 A The levonorgestrel intra-uterine system (LNG IUS) reduces endometriosis associated pain. Evidence Level 1a A systematic review identified two RCTs and three prospective observational studies, all involving small numbers and a heterogeneous group of patients (Varma et al., 2005). Nevertheless, the evidence suggests that the LNG IUS reduces endometriosis associated pain (Petta et al., 2005; Vercellini et al., 1999a) with symptom control maintained over 3 years (Lockhat et al., 2004; Lockhat et al., 2005).
. Nevertheless, the evidence suggests that the LNG IUS reduces endometriosis associated pain (Petta et al., 2005; Vercellini et al., 1999a) with symptom control maintained over 3 years (Lockhat et al., 2004; Lockhat et al., 2005).")
46
Progestinler Destek Dokümentasyonu, 2007 ESHRE
AFS skorları ve ağrıyı danazol ve GnRH analogları kadar azaltabildiği, daha düşük maliyetli olduğu ve yan etki insidansı danazol ve GnRH analoglarından daha düşük bulunduğu için endometriozis tedavisinde ilk seçenek olarak kabul edilebilirler. Vercellini. 1997

47
Endometriosis: Treatment
Danazol

48
Danazol Oral androgenic steroid
Derived from 17α-ethinyl testosterone Mechanism of action – induces amenorrhea via suppression of estrogen and progesterone Androgens (testosterone) first used to treat endometriosis in 1943 First use of danazol described in 1971 Use is limited by anabolic and androgenic side-effects References Olive DL, Pritts EA. Treatment of endometriosis. N Engl J Med 2001;345:266–275. Crosignani P, Olive D, Bergqvist A, Luciano A. Advances in the management of endometriosis: an update for clinicians. Hum Reprod Update 2006;12:179–189. Hirst JC. Favorable response of advanced endometriosis to testosterone proprionate therapy. Am J Obst Gynecol 1943;46:97–102. Greenblatt RB, Dmowski WP, Mahesh VB, Scholer HF.Clinical studies with an antigonadotropin - Danazol. Fertil Steril 1971;22:102. Winkel CA, Scialli AR. Medical and surgical therapies for pain associated with endometriosis. J Women’s Health Gender-Based Med 2001;10:137–162. Sinaii N, Cleary SD, Younes N et al. Treatment utilization for endometriosis symptoms: a cross-sectional survey study of lifetime experience. Fertil Steril 2007;87:1277–1286. Selak V, Farquhar C, Prentice A, Singla AA. Danazol for pelvic pain associated with endometriosis. Cochrane Database Syst Rev 2007;4:CD Further information Danazol is an androgenic steroid with efficacy in treating the symptoms of endometriosis, but its use is limited by the typical adverse effects of androgenic steroids on lipid metabolism and by unpleasant effects that include weight gain, edema, acne, vaginal dryness, hot flushes, oily skin, hirsutism and liver toxicity [Winkel & Scialli, 2001; Selak et al, 2007]. Because of these effects, danazol has largely been superseded by newer agents in many countries. Olive DL et al. N Engl J Med 2001; Crosignani P et al. Hum Reprod Update 2006; Hirst JC. Am J Obst Gynecol 1943; Greenblatt RB et al. Fertil Steril 1971; Winkel CA et al. J Women’s Health Gender-Based Med 2001; Sinaii N et al. Fertil Steril 2007.
 first used to treat endometriosis in First use of danazol described in Use is limited by anabolic and androgenic side-effects. References. Olive DL, Pritts EA. Treatment of endometriosis. N Engl J Med 2001;345:266–275. Crosignani P, Olive D, Bergqvist A, Luciano A. Advances in the management of endometriosis: an update for clinicians. Hum Reprod Update 2006;12:179–189. Hirst JC. Favorable response of advanced endometriosis to testosterone proprionate therapy. Am J Obst Gynecol 1943;46:97–102. Greenblatt RB, Dmowski WP, Mahesh VB, Scholer HF.Clinical studies with an antigonadotropin - Danazol. Fertil Steril 1971;22:102. Winkel CA, Scialli AR. Medical and surgical therapies for pain associated with endometriosis. J Women’s Health Gender-Based Med 2001;10:137–162. Sinaii N, Cleary SD, Younes N et al. Treatment utilization for endometriosis symptoms: a cross-sectional survey study of lifetime experience. Fertil Steril 2007;87:1277–1286. Selak V, Farquhar C, Prentice A, Singla AA. Danazol for pelvic pain associated with endometriosis. Cochrane Database Syst Rev 2007;4:CD Further information. Danazol is an androgenic steroid with efficacy in treating the symptoms of endometriosis, but its use is limited by the typical adverse effects of androgenic steroids on lipid metabolism and by unpleasant effects that include weight gain, edema, acne, vaginal dryness, hot flushes, oily skin, hirsutism and liver toxicity [Winkel & Scialli, 2001; Selak et al, 2007]. Because of these effects, danazol has largely been superseded by newer agents in many countries. Olive DL et al. N Engl J Med 2001; Crosignani P et al. Hum Reprod Update 2006; Hirst JC. Am J Obst Gynecol 1943; Greenblatt RB et al. Fertil Steril 1971; Winkel CA et al. J Women’s Health Gender-Based Med 2001; Sinaii N et al. Fertil Steril")
49
Danazol – side effects Due to hyperandrogenism and hypo-oestrogenemia
Weight gain Fluid retention Fatigue Nausea Acne Hirsutism Oily skin Muscle cramps Reduced libido Reduced breast size Emotional disturbances Atrophic vaginitis Hot flushes Hepatocellular damage Irreversible deepening of voice

51
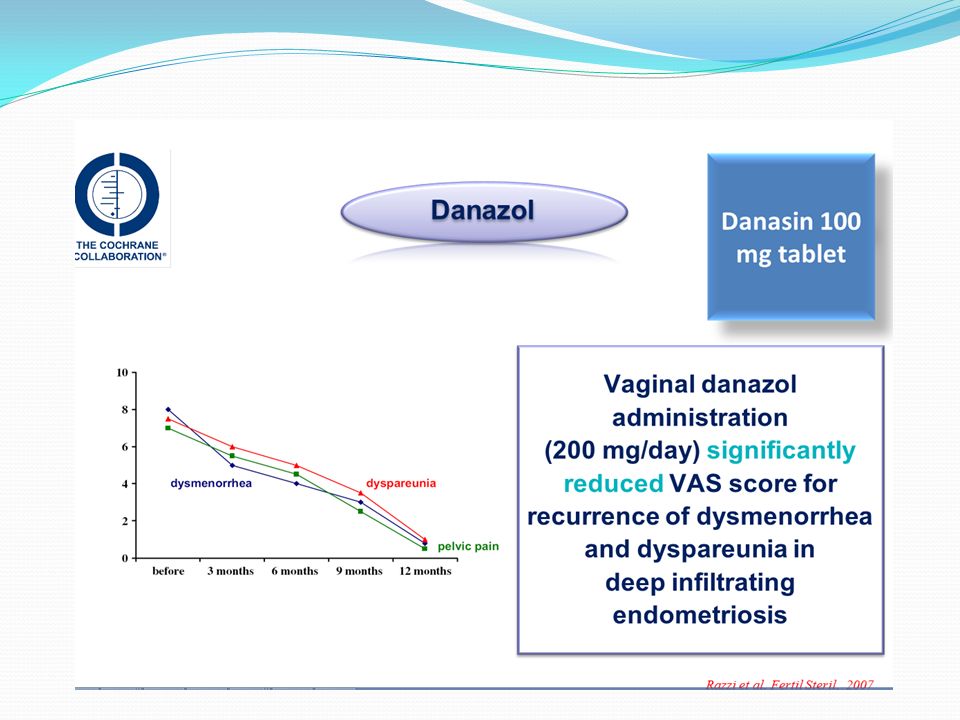
Vaginal danazol for the treatment of endometriosis-related pelvic pain (n: 21)
Vaginal danazol (200 mg) daily for 6 months. Sudhindra M. Bhattacharya, 2011
 daily for 6 months. Sudhindra M. Bhattacharya,")
52
Gestrinone Gestrinone is a 19-nortestosterone derivative with androgenic , antiprogestagenic, antiestrogenic, and antigonadotropic properties. Gestrinone causes cellular inactivation and degeneration of endometriotic implants but not their disappearance. Amenorrhea occurs in 50% to 100% of women and is dose dependent. The standard dose is 2,5mg twice a week. It acts centrally and peripherally to increase free testosterone and reduce sex hormone-binding globulin levels ( androgenic effect), reduce serum estradiol values to early follicular phase levels (antiestrogenic effect) , reduce mean LH levels, and obliterate the LH and follicle-stimulating hormone (FSH) surge (antigonadotropic effect).
, reduce serum estradiol values to early follicular phase levels (antiestrogenic effect) , reduce mean LH levels, and obliterate the LH and follicle-stimulating hormone (FSH) surge (antigonadotropic effect).")
53
Gestrinone The clinical side effects include nause, muscle cramps , and androgenic effects such as weight gain, acne, sebborrhea, and oily hair and skin. In a multicenter, randomized , double-blind study, gestrinone was as effective as GnRH for the treatment of pelvic pain associated with endometriosis, with fewer side effects and the added advantage of twice- weekly administration.

54
Endometriosis :alternative methods of medical treatment
GnRH antagonists Aromatase inhibitors Selective progesterone receptor modulators Anti-tumor necrosis factor-alfa Antiangiogenic factors

55
Elagolix a new GnRH Antagonist Drug
Oral GnRH Antagonists Elagolix a new GnRH Antagonist Drug

56
Nándor Ács, Chris O’Brien, Ping Jiang, Joshua Burke, Roland Jimenez,
Elizabeth Garner, Kristof Chwalisz

57
Treatment- related adverse events were generally mild to moderate in severity: headache, nausea, anxiety, hot flashes, BMD changes

58
These studies demonstrated that elagolix 150 mg reduces endometriosis-associated pain, partially suppresses estradiol and results in minimal changes in BMD. Elagolix is in clinical development as a potential treatment option for women with endometriosis. Bruce Carr, Linda Giudice, W.Paul Dmowski, Chris O’Brien, Ping Jiang, Joshua Burke, Roland Jimenez,Steven Hass, Mahesh Fuldeore, Kristof Chwalisz

59
Investigational agents for the treatment of endometriosis-associated pain
Figure 1. Investigational agents for the treatment of endometriosis-associated pain: mechanisms of aromatase inhibitors, anti-estrogens (selective estrogen receptor modulators) and selective progesterone receptor modulators. This schematic depicts the mechanisms of several new investigational agents for the treatment of endometriosis in relation to existing therapies in common use. GnRH analogues decrease the activity of endometrial implants by inhibiting the hypothalamic-pituitaryovarian (HPO) axis and blocking ovarian function, thereby greatly reducing systemic estrogen levels (inducing artificial menopause). Progestins both suppress HPO function and have antiproliferative effects directly on endometrial tissue (eutopic and endometriotic implants). The new agents attempt to more specifically target endometriotic implants. Aromatase P450, which is up-regulated in endometriotic implants, is a key enzyme in the biosynthesis of estrogen. Therefore, aromatase inhibitors decrease estrogen concentrations in the implants. Selective estrogen receptor modulators (SERMs) antagonize the effects of estrogen in the implants, thus reducing the growth and proliferation of implants. Selective progesterone receptor modulators (SPRMs), which can act as either agonists or antagonists of progesterone receptors in various tissues, have antiproliferative effects on endometrial growth (similar to progestins, but acting by differing mechanisms). However, SPRMs selectively suppress endometrial growth without inhibiting ovarian estrogen production. A, androstenedione; E1, estrone; E2, estradiol; E2–ER, estradiolbound estrogen receptors (Chwalisz et al., 2002; Olive, 2002; Viganò et al., 2003; Bulun et al., 2004)
 and selective progesterone receptor modulators. This schematic depicts the mechanisms of several new investigational agents for the treatment of. endometriosis in relation to existing therapies in common use. GnRH analogues decrease the activity of endometrial implants by inhibiting the hypothalamic-pituitaryovarian. (HPO) axis and blocking ovarian function, thereby greatly reducing systemic estrogen levels (inducing artificial menopause). Progestins both suppress HPO. function and have antiproliferative effects directly on endometrial tissue (eutopic and endometriotic implants). The new agents attempt to more specifically target. endometriotic implants. Aromatase P450, which is up-regulated in endometriotic implants, is a key enzyme in the biosynthesis of estrogen. Therefore, aromatase. inhibitors decrease estrogen concentrations in the implants. Selective estrogen receptor modulators (SERMs) antagonize the effects of estrogen in the implants, thus. reducing the growth and proliferation of implants. Selective progesterone receptor modulators (SPRMs), which can act as either agonists or antagonists of progesterone. receptors in various tissues, have antiproliferative effects on endometrial growth (similar to progestins, but acting by differing mechanisms). However, SPRMs selectively suppress endometrial growth without inhibiting ovarian estrogen production. A, androstenedione; E1, estrone; E2, estradiol; E2–ER, estradiolbound. estrogen receptors (Chwalisz et al., 2002; Olive, 2002; Viganò et al., 2003; Bulun et al., 2004)")
60
Aromatase inhibitors No clear evidence of their effectiveness for the treatment of pain related to endometriosis. Severe side effects (headaches, hot flashes, mood changes, muscle aches, breakthrough bleeding, change in BMD)and cost. ESHRE recommends the use of aromatase inhibitors associated to another hormonal treatment ( O.C. , progestogens, or GnRHa) only in women in whom all surgical and medical treatments have failed.
and cost. ESHRE recommends the use of aromatase inhibitors associated to another hormonal treatment ( O.C. , progestogens, or GnRHa) only in women in whom all surgical and medical treatments have failed.")
61
Selective progesterone receptor modulators
SPRMs exhibit both progesterone agonistic and antagonistic activities. İn the absence of progesterone, the SPRMs act like weak progestins. İn the presence of progesterone, they may also show weak antiprogestagenic properties in some tissues, particularly in the endometrium. This property justifies their use in the treatment of myomas and endometriosis. Mifepristone Ulipristal acetate

62
Anti-tumor necrosis factor-alfa
A feature of endometriotic tissue is inflammation. A nonhormanal alternative in endometriosis treatment could be modulating inflammation by means of TNF-alfa blocckers as currently used in other inflammatory diseases such as Crohn’s disease os rheumatoid arthritis. There is not enough evidence to recommend the use of anti-TNF-alfa drugs for the treatment of pain associated to endometriosis. which is mediated by the overproduction of prostaglandins, metalloproteinases, cytokines, and chemokines. Increased levels of acute inflammatory cytokines (interleukin-1beta, interleukin-6 and TNF) are detected in the peritoneal fluid of women whit endometriosis, and probably enhance the adhesion of shed endometrial-tissue fragments onto peritoneal surfaces.
 are detected in the peritoneal fluid of women whit endometriosis, and probably enhance the adhesion of shed endometrial-tissue fragments onto peritoneal surfaces.")
63
Antiangiogenic factors
Endometriosis is classified as an angiogenic disease. Several studies concentrate on antiangiogenic compounds as a promising therapy for endometriosis. The future in antiangiogenic therapy for endometriosis seems to be factors which blockade different pathways in the angiogenic cascade. The retrograde menstruation theory explains pathogenesis of endometriosis due to retrograde menstruation of endometrial tissue, rich in angiogenic growth factors, which implants in the peritoneum. The endometrium from patients with endometriosis reveals a higher angiogenic activity than the endometrium from healthy women, the same as is found in endometriotic lesions and peritoneal fluid from women with endometriosis.

64
Conclusion There is a need to find effective treatments that do not block ovarian function. Upcoming researches and controlled clinical trials should focus on these drugs, in order to establish if they are really effective in relieving pain without affecting fertility.

Benzer bir sunumlar