Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
GEÇMİŞTEN GELECEĞE GONADOTROPİNLER VE SON TEDAVİ PROTOKOLLERİ
DOÇ. DR. ERAY ÇALIŞKAN ÖZGÜR HEKİM

2
TARİHÇE VE GELİŞİM

3
İnfertilite tedavisinin gelişimi
19th Century 18th 1960s 1970s 1980s 1990s 2000s 2010s İlk IVF— Kurbağa oositi İlk İnsan IUI Gonadların hipofiz tarafından uyarıldığına dair ilk kanıtlar HPO aksı İlk IVF bebeği Klinik kullanım için ilk gonadotropinler recFSH KOS için gebe at idrarı gonadotropini SFSs 17th Spermatozoa görülmesi insanPG IVF = in vitro fertilization; hPG = hypothalamic-pituitary-gonadal; COS = controlled ovarian stimulation; hPG = human pituitary gonadotropins; PMSG = pregnant mare serum gonadotropin; recFSH = recombinant human follicle-stimulating hormone; SFS = sustained follicle stimulant. Clarke. Hum Reprod. 2006;21:1645; Hayden. Eur J Endocrinol. 2008;(159 suppl 1):S17; Lunenfeld. Hum Reprod Update. 2004;10:453; Macklon et al. Endocr Rev. 2006;27: ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Fertil Steril. 2008;90:S13. Clarke GN. A.R.T. and history, Hum Reprod. 2006;21(7): ; Hayden C. GnRH analogues: applications in assisted reproductive techniques. Eur J Endocrinol. 2008;(159 suppl 1):S17-S25; Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Macklon NS, Stouffer RL, Giudice LC, Fauser BC. The science behind 25 years of ovarian stimulation for in vitro fertilization. Endocr Rev. 2006;27(2): ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Gonadotropin preparations: past, present, and future perspectives. Fertil Steril. 2008;90(5 suppl):S13-S20.
:S17; Lunenfeld. Hum Reprod Update. 2004;10:453; Macklon et al. Endocr Rev. 2006;27: ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Fertil Steril. 2008;90:S13. Clarke GN. A.R.T. and history, Hum Reprod. 2006;21(7): ; Hayden C. GnRH analogues: applications in assisted reproductive techniques. Eur J Endocrinol. 2008;(159 suppl 1):S17-S25; Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Macklon NS, Stouffer RL, Giudice LC, Fauser BC. The science behind 25 years of ovarian stimulation for in vitro fertilization. Endocr Rev. 2006;27(2): ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Gonadotropin preparations: past, present, and future perspectives. Fertil Steril. 2008;90(5 suppl):S13-S20.")
4
Gonadotropin Teorisinin İnfertilite Tedavisinde Önem Kazanması
Aschner (1912) Hipofizin gonad uyarısındaki rolnün kesinleşmesi Hipofizin başka beyin merkezleri tarafından kontrol edildiğinin ileri sürülmesi 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th Crowe et al (1910) Hipofizlerin overleri uyarması ile ilgili ilk deneysel kanıtlar Smith (1926) and Zondek (1926) “Gonadotropin teorisi” Although gonadotropin therapy is a critical part of the treatment of infertility today, considerable research was required before safe and effective treatments were available for clinical use. Evidence that the brain controls gonadal function and the growth cycle of ovarian follicles stems from partial pituitary ablation studies conducted by Crowe et al as early as 1910. In 1912, Aschner confirmed pituitary regulation of the gonads and proposed the idea that control of the pituitary itself was regulated by higher centers in the brain. Two independent groups discovered the “gonadotrophic principle,” the factor from the anterior pituitary that induced precocious sexual maturity when injected into immature animals. In subsequent studies, hypophysectomy of immature or adult animals resulted in failure to mature sexually or atrophy and loss of reproductive function, respectively, further supporting the role of the anterior pituitary in the regulation of the gonads. Crowe et al. Bull Johns Hopkins Hosp. 1910;21:127; Lunenfeld. Hum Reprod Update. 2004;10:453; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Fertil Steril. 2008;90:S13; Smith. Proc Soc Exp BiolMed. 1926;24:1311. Crowe SJ, Cushing H, Homans J. Experimental hypophysectomy. Bull Johns Hopkins Hosp. 1910;21: ; Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Gonadotropin preparations: past, present, and future perspectives. Fertil Steril. 2008;90(5 suppl):S13-S20; Smith PE. Hastening of development of female genital system by daily hemoplastic pituitary transplants. Proc Soc Exp BiolMed. 1926;24: 4
 Hipofizin gonad uyarısındaki rolnün kesinleşmesi. Hipofizin başka beyin merkezleri tarafından kontrol edildiğinin ileri sürülmesi. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. Crowe et al (1910) Hipofizlerin overleri uyarması ile ilgili ilk deneysel kanıtlar. Smith (1926) and Zondek (1926) Gonadotropin teorisi Although gonadotropin therapy is a critical part of the treatment of infertility today, considerable research was required before safe and effective treatments were available for clinical use. Evidence that the brain controls gonadal function and the growth cycle of ovarian follicles stems from partial pituitary ablation studies conducted by Crowe et al as early as In 1912, Aschner confirmed pituitary regulation of the gonads and proposed the idea that control of the pituitary itself was regulated by higher centers in the brain. Two independent groups discovered the gonadotrophic principle, the factor from the anterior pituitary that induced precocious sexual maturity when injected into immature animals. In subsequent studies, hypophysectomy of immature or adult animals resulted in failure to mature sexually or atrophy and loss of reproductive function, respectively, further supporting the role of the anterior pituitary in the regulation of the gonads. Crowe et al. Bull Johns Hopkins Hosp. 1910;21:127; Lunenfeld. Hum Reprod Update. 2004;10:453; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Fertil Steril. 2008;90:S13; Smith. Proc Soc Exp BiolMed. 1926;24:1311. Crowe SJ, Cushing H, Homans J. Experimental hypophysectomy. Bull Johns Hopkins Hosp. 1910;21: ; Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Gonadotropin preparations: past, present, and future perspectives. Fertil Steril. 2008;90(5 suppl):S13-S20; Smith PE. Hastening of development of female genital system by daily hemoplastic pituitary transplants. Proc Soc Exp BiolMed. 1926;24:")
5
Gonadotropinler Neredeyse Yüzyıl Önce Bulunmuştur
1929: Zondek Hipofizin overi uyaran iki hormon salgıladığını iddia etmiştir 1930: Zondek Postmenapozal kadınların kan ve idrarında gonadotropin olduğunu gözlemlemiştir Prolan A (FSH) Prolan B (LH) Gonadotropinlerin overler üzerindeki etkilerini tanımlamıştır Bernhard Zondek was the first to propose coordination of ovarian activity through what has come to be known as the hypothalamic-pituitary-ovarian (HPO) axis. A few years after the “gonadotrophic principle” was discovered, Zondek proposed the idea that 2 separate pituitary hormones (“Prolan A” and “Prolan B”) stimulate the gonads. Zondek also demonstrated that the blood and urine of postmenopausal women contained gonadotropins. He proposed roles for the gonadotropins that are very similar to our current understanding of the pituitary-gonadal relationship: Prolan A (follicle-stimulating hormone; FSH) stimulated follicular growth. Prolan A together with Prolan B (luteinizing hormone; LH) stimulated the secretion of “folliculin” (estrogen). Prolan B induced ovulation, the formation of the corpus luteum (CL), and the secretion of folliculin and “lutein” (progesterone). This illustration from Zondek represents the interaction of the hypothalamus, pituitary, ovaries, and endometrium. Zondek’s hypothesis that 2 separate gonadotropins acted on the gonads was confirmed in 1931 by Fevold et al with the extraction of 2 separate hormones from the pituitary. One of these hormones had follicle-stimulating properties. The other acted as a luteinizing factor. 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th LH = luteinizing hormone; FSH = follicle-stimulating hormone. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): 5
 Prolan B (LH) Gonadotropinlerin overler üzerindeki etkilerini tanımlamıştır. Bernhard Zondek was the first to propose coordination of ovarian activity through what has come to be known as the hypothalamic-pituitary-ovarian (HPO) axis. A few years after the gonadotrophic principle was discovered, Zondek proposed the idea that 2 separate pituitary hormones ( Prolan A and Prolan B ) stimulate the gonads. Zondek also demonstrated that the blood and urine of postmenopausal women contained gonadotropins. He proposed roles for the gonadotropins that are very similar to our current understanding of the pituitary-gonadal relationship: Prolan A (follicle-stimulating hormone; FSH) stimulated follicular growth. Prolan A together with Prolan B (luteinizing hormone; LH) stimulated the secretion of folliculin (estrogen). Prolan B induced ovulation, the formation of the corpus luteum (CL), and the secretion of folliculin and lutein (progesterone). This illustration from Zondek represents the interaction of the hypothalamus, pituitary, ovaries, and endometrium. Zondek’s hypothesis that 2 separate gonadotropins acted on the gonads was confirmed in 1931 by Fevold et al with the extraction of 2 separate hormones from the pituitary. One of these hormones had follicle-stimulating properties. The other acted as a luteinizing factor. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. LH = luteinizing hormone; FSH = follicle-stimulating hormone. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):")
6
İnfertilite Tedavisinin Klinik Kullanımında Gonadotropin Preparatlarının Markete Çıkması
1927: Gebelerin kan ve idrarında overleri uyarıcı maddenin bulunması (hCG) 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th 1931: Organon plasental ekstraktlardan «prolan B» isimli hipofiz hormonuna çok benzeyen bir maddeyi «overleri uyarmak için» üretmiştir : hCG ile klinik çalışmalar The availability of clinical preparations of gonadotropins for the treatment of infertility, generally through the stimulation of oocyte development on the follicles, began shortly after the discovery of the “gonadotrophic principle.” In 1927, Ascheim and Zondek demonstrated that blood and urine from pregnant women contained a gonad-stimulating substance (now known as human chorionic gonadotropin [hCG]), and clinical studies of this substance began in 1930. The first gonadotropin for clinical use was launched by Organon in 1931. This product was extracted from human placenta, had properties very similar to the pituitary hormone “Prolan B” (LH), and was to be used for “stimulation of the ovaries.” In 1940, purified urinary preparations of hCG become available for clinical use. Refinement of gonadotropin preparations for clinical use continued and will be discussed later in this presentation. 1940: İdrardan elde edilen hCG preparatlarının kullanımı hCG = human chorionic gonadotropin. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):
 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. 1931: Organon plasental ekstraktlardan «prolan B» isimli hipofiz hormonuna çok benzeyen bir maddeyi «overleri uyarmak için» üretmiştir : hCG ile klinik çalışmalar. The availability of clinical preparations of gonadotropins for the treatment of infertility, generally through the stimulation of oocyte development on the follicles, began shortly after the discovery of the gonadotrophic principle. In 1927, Ascheim and Zondek demonstrated that blood and urine from pregnant women contained a gonad-stimulating substance (now known as human chorionic gonadotropin [hCG]), and clinical studies of this substance began in The first gonadotropin for clinical use was launched by Organon in This product was extracted from human placenta, had properties very similar to the pituitary hormone Prolan B (LH), and was to be used for stimulation of the ovaries. In 1940, purified urinary preparations of hCG become available for clinical use. Refinement of gonadotropin preparations for clinical use continued and will be discussed later in this presentation. 1940: İdrardan elde edilen hCG preparatlarının kullanımı. hCG = human chorionic gonadotropin. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):")
7
Follikül Uyarımı İçin Gonadotropin Kullanımının Fikirsel Temelleri
1941: Mazer ve Ravetz Over uyarımı için gebe at idrarından üretilen gonadotropinlerin kullanımı hCG kullanarak ovülasyonun uyarılması “ Overlerin gonadotropinlere cevabı overlerin reseptivitesine, total doza, tedavi süresine bağımlıdır 1945: “Ideal Tedavi” – Hamblen et al Folliküler fazda at idrarından elde edilen gonadotropin kullanımı ve gün sonra hCG yapılması Sekretuvar endometriyum oluşmasına neden olmaktadır Planlı cinsel ilişki gebelik sağlayabilir A more methodical approach for the use of gonadotropins to stimulate follicular growth was developed. This “two-step approach” involved the use of gonadotropins, generally PMSG, to stimulate follicular growth, followed by the induction of final oocyte maturation by hCG. The approach was developed by Mazer and Ravetz in 1941. The authors also noted that the degree of ovarian response to the gonadotropins was dependent on several factors, including ovarian receptivity, total gonadotropin dose, and the duration of treatment. The results also indicated that excessive gonadotropin treatment could lead to overstimulation and ovarian pathology. Hamblen and co-workers were able to show that precise timing of hCG would lead to controlled ovulation as well as the development of a secretory endometrium, and that pregnancy could then often be established following planned coitus. As a result, Hamblen et al (1945) developed the “ideal treatment,” which included the administration of PMSG during the follicular phase, followed by hCG 12 to 18 days later. 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th PMSG = pregnant mare serum gonadotropin; hCG = human chorionic gonadotropin. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): 7
 developed the ideal treatment, which included the administration of PMSG during the follicular phase, followed by hCG 12 to 18 days later. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. PMSG = pregnant mare serum gonadotropin; hCG = human chorionic gonadotropin. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):")
8
Over Uyarılmasında Hayvan Hipofiz Ekstraktlarının Kullanımı
Hayvan hipofiz ekstraktları 1960’ların başına kadar overlerin uyarılması için kullanılmıştır 1956: Maddock et al Dışarıdan FSH kullanımının idrarda östrojen artışına yol açtığını bulmuştur Bazı hastalarda 7-10 cm’ye kadar büyümüş kistler bulunmuştur Kistlerde erken luteinizasyon değişiklikleri gösteren granüloza hücreleri gözlenmiştir 1959: Netter et al 1-3 ampul hayvan hipofiz ekstraktı kullanılarak idrarda inanılmaz östrojen artışları gözlenmiştir 1959: French Sosyal Güvenlik Sistemi Hayvan hipofiz ekstraktı kullanımını geri ödemeye almıştır Further study in the use of exogenous gonadotropins for the treatment of infertility demonstrated that, while these agents produced ovarian stimulation and increases in urinary estrogen, some “antihormones” were also produced after prolonged exposure to gonadotropins derived from animal sources. These “antihormones” or antibodies, generated against proteins (the gonadotropin hormones) derived from animal sources, could cause allergic responses as well as reduce efficacy of both exogenous and endogenous gonadotropins. This resulted in their eventual removal from the market. 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th FSH = follicle-stimulating hormone. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):
 derived from animal sources, could cause allergic responses as well as reduce efficacy of both exogenous and endogenous gonadotropins. This resulted in their eventual removal from the market. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. FSH = follicle-stimulating hormone. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):")
9
Ticari olarak İnsan Hipofizi Kaynaklı Gonadotropinlerin Üretilmesi
1958: Carl Gemzell insan hipofiz dokusundan gonadotropin elde etmiştir 1961: Buxton and Hermann liyofilize edilmiş insan hipofizinden alkol ile elde edilmiş FSH’yı test etmişlerdir İnsan hipofizi kaynaklı gonadotropinlerin bulunması ve infertilite tedavisinda başarı ile kullanılması İnsan hipofiz dokusundan elde edilen gonadotropinlerin market için yetersiz olduğu bulunmuş ve alternatif kaynaklar aranmaya başlanmıştır İnsan hipofizel gonadotropinlerinin kullanımından 20 yıl sonra iatrojenik Creutzfeld–Jakob hastalığı bulunmuştur Bu vakalar insan hipofizinden elde edilen gonadotropin kullanımı ile ilişkilendirilmiştir Bu olguların hiçbiri lisanslı ilaç şirketi ürünleri ile ilişkilendirilememişse de insan hipofizinden elde edilen gonadotropinin kullanımı yasaklanmış ilaçları marketten çekilmiştir In 1958, Carl Gemzell extracted gonadotropins from human pituitary tissue. This led to the development of commercially available gonadotropin preparations that were derived from human pituitary sources (human pituitary gonadotropin; hPG). In 1961, Buxton and Hermann tested an FSH preparation prepared by Merck & Co. from lyophilized human pituitaries with alcohol extraction. The clinical efficacy of hPG preparations was demonstrated, and hPG preparations were successfully used for the treatment of infertility from 1958 to However, it soon became apparent that the supply of human pituitary tissue would not meet the demand, so the search for alternative human sources of gonadotropins continued. About 20 years after the introduction of hPG, cases of iatrogenic Creutzfeld–Jakob disease (CJD) that were associated with the use of hPG or human pituitary growth hormone were discovered. None of the cases arose from the use of products registered by pharmaceutical companies, but were instead traced to the use of products produced by government agencies; nonetheless, hPG was withdrawn from the market. 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th hPG = human pituitary gonadotropins; FSH = follicle-stimulating hormone. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): 9
. In 1961, Buxton and Hermann tested an FSH preparation prepared by Merck & Co. from lyophilized human pituitaries with alcohol extraction. The clinical efficacy of hPG preparations was demonstrated, and hPG preparations were successfully used for the treatment of infertility from 1958 to However, it soon became apparent that the supply of human pituitary tissue would not meet the demand, so the search for alternative human sources of gonadotropins continued. About 20 years after the introduction of hPG, cases of iatrogenic Creutzfeld–Jakob disease (CJD) that were associated with the use of hPG or human pituitary growth hormone were discovered. None of the cases arose from the use of products registered by pharmaceutical companies, but were instead traced to the use of products produced by government agencies; nonetheless, hPG was withdrawn from the market. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. hPG = human pituitary gonadotropins; FSH = follicle-stimulating hormone. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):")
10
İnsn Menapozal Gonadotropinlerinin Hipofiz Ekstraktlarının Yerine Kullanımı
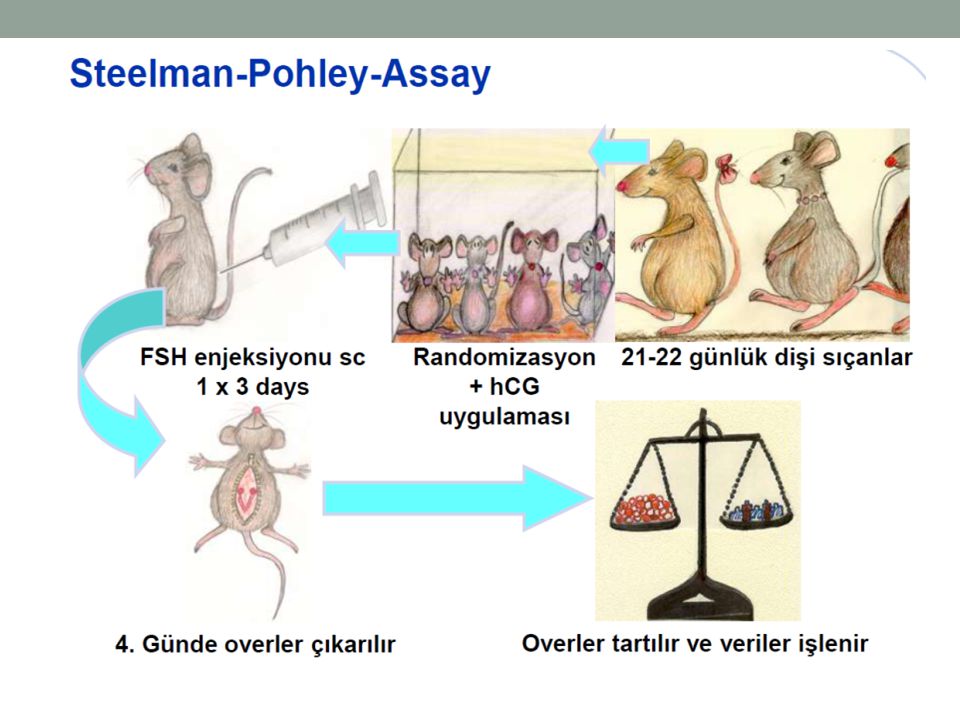
Büyük idrar havuzlarından izole edilip saflaştırılmıştır 1950: Pergonal 25 Klink kullanım için ilk hMG 1961: Lunenfeld et al Gebelikle sonuçlanan ilk başarılı ovülasyon indüksiyonunu tanımlamıştır 1953: Steelman and Pohley hMG içinde bulunan FSH miktarını belirlemek için altın standart bir ölçüm belirlemişlerdir 1965: hMG dozu standardize edilmiştir IU ölçümü kullanılmaya başlanmıştır 75 IU veya bir ampulde= 75 IU FSH + 75 IU LH One alternative to hPG is gonadotropins extracted from the urine of postmenopausal women (human menopausal gonadotropins; hMG). Human menopausal gonadotropins were (and still are today) extracted from the urine of postmenopausal women. In 1950, the first hMG preparation for clinical use, Pergonal 25, became available. Steelman and Pohley hold the distinction of developing the gold standard assay for detecting FSH/LH within hMG, an assay that is still in use today. It was not until 1965 that hMG dosing was standardized using International Units to describe the amount of active hormone. 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th hMG = human menopausal gonadotropin; FSH = follicle-stimulating hormone; IU = international unit; LH = luteinizing hormone. Lunenfeld. Hum Reprod Update. 2004;10:453; Steelman and Pohley. Endocrinology. 1953;53:604. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Steelman SL, Pohley FM. Assay of the follicle stimulating hormone based on the augmentation with human chorionic gonadotropin. Endocrinology. 1953;53(6): 10
. Human menopausal gonadotropins were (and still are today) extracted from the urine of postmenopausal women. In 1950, the first hMG preparation for clinical use, Pergonal 25, became available. Steelman and Pohley hold the distinction of developing the gold standard assay for detecting FSH/LH within hMG, an assay that is still in use today. It was not until 1965 that hMG dosing was standardized using International Units to describe the amount of active hormone. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. hMG = human menopausal gonadotropin; FSH = follicle-stimulating hormone; IU = international unit; LH = luteinizing hormone. Lunenfeld. Hum Reprod Update. 2004;10:453; Steelman and Pohley. Endocrinology. 1953;53:604. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Steelman SL, Pohley FM. Assay of the follicle stimulating hormone based on the augmentation with human chorionic gonadotropin. Endocrinology. 1953;53(6):")
11
İnsan Menapozal Gonadotropini Kullanımı Standardize Edilmiştir
1972: Cenevre de DSÖ bilimsel toplantısında İnfertil çiftlerin tanı ve tedavisinde yönergeler oluşturulmuştur Hipogonadotropik kadınlarda: hMG 150 – 225 IU/gün Anovulatuvar normogonadotropik kadınlarda: hMG 75 – 150 IU/gün 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th In 1972, the World Health Organization (WHO) convened a scientific group meeting in Geneva to develop guidelines for the diagnosis and management of infertile couples. The reported effective daily doses of 150 to 225 IU for hypogonadotrophic patients and 75 to 150 IU for anovulatory normogonadotrophic patients were established. These dosing standards are still applicable today. WHO = World Health Organization; hMG = human menopausal gonadotropin. Lunenfeld. Hum Reprod Update. 2004;10:453; World Health Organization. World Health Organization Technical Report. 1973; Series 514. World Health Organization, Geneva. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; World Health Organization. Agents stimulating gonadal function in the human. World Health Organization Technical Report. 1973; Series 514. World Health Organization, Geneva. 11
 convened a scientific group meeting in Geneva to develop guidelines for the diagnosis and management of infertile couples. The reported effective daily doses of 150 to 225 IU for hypogonadotrophic patients and 75 to 150 IU for anovulatory normogonadotrophic patients were established. These dosing standards are still applicable today. WHO = World Health Organization; hMG = human menopausal gonadotropin. Lunenfeld. Hum Reprod Update. 2004;10:453; World Health Organization. World Health Organization Technical Report. 1973; Series 514. World Health Organization, Geneva. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; World Health Organization. Agents stimulating gonadal function in the human. World Health Organization Technical Report. 1973; Series 514. World Health Organization, Geneva. 11.")
12
Dünyada İnsan Menapozal Gonadotropini Kullanımı Artmıştır
İlk idrar toplama merkezleri Hollanda, ispanya, israil, italya 600 kadının idrarı Yıllık üretimde kullanılan idrar miktarı 120,000 litre Günümüzde idrar toplama merkezleri Avrupa, Kore, Çin, Hindistan, Güney Amerika 600,000 kadının idrarı Yıllık üretimde kullanılan idrar 120,000,000 litre The original urine donors were postmenopausal nuns living in select convents throughout Europe. However, as the demand for hMG has increased, the number of women participating in the process has increased considerably and includes women from several continents. 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): 12
:")
13
Üriner FSH ve LH’nın ayrı ayrı üretimi
İmmünolojik tekniklerin gelişmesi ile üriner FH ve LH’nın ayrı ayrı üretilmesi mümkün olmuştur Bu durum biyolojik olarak minimal LH aktivitesi olan saflaştırılmış FSH üretimini sağlamıştır İmmünolojik teknolojide seçici olarak FSH bağlayan monoklonal antikorların geliştirilmesi ile hMG içinden FSH yı ayıklayabilen bir üretim doğmuştur FSH-HP FSH-HP nın seçici FSH aktivitesi artıştır Bu durum KOS protokollerinin gözden geçirilmesine düşük dozlu tedavilerin veya OHSS’yi önleyebilecek küçük doz artışlarının yapılabilmesini sağlamıştır The need for individualized treatment regimens required the development of separate preparations of FSH and LH. Although multiple modifications to urinary extraction techniques were required, new developments in immunologic techniques allowed the separation of urinary LH and FSH. This resulted in a biological FSH that has only minimal LH activity. This product, Metrodin, contained 150 IU of FSH and only 1 IU of LH per mg of protein. Further refinement of immunotechnology allowed the development of monoclonal antibodies that could be used to selectively bind FSH from urinary hMG, resulting in a highly purified FSH (FSH-HP), commercially available as Metrodin-HP. FSH-HP has increased specific FSH activity. Allows refinement of COS protocols, including low-dose regimens or increments to reduce the possibility of ovarian hyperstimulation. 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th LH = luteinizing hormone; FSH = follicle-stimulating hormone; hMG = human menopausal gonadotropin; FSH-HP = highly purified FSH; COS = controlled ovarian stimulation. Lunenfeld. Hum Reprod Update. 2004;10:453; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Fertil Steril. 2008;90:S13. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Gonadotropin preparations: past, present, and future perspectives. Fertil Steril. 2008;90(5 suppl):S13-S20. 13
, commercially available as Metrodin-HP. FSH-HP has increased specific FSH activity. Allows refinement of COS protocols, including low-dose regimens or increments to reduce the possibility of ovarian hyperstimulation. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. LH = luteinizing hormone; FSH = follicle-stimulating hormone; hMG = human menopausal gonadotropin; FSH-HP = highly purified FSH; COS = controlled ovarian stimulation. Lunenfeld. Hum Reprod Update. 2004;10:453; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Fertil Steril. 2008;90:S13. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6): ; Practice Committee of American Society for Reproductive Medicine, Birmingham, Alabama. Gonadotropin preparations: past, present, and future perspectives. Fertil Steril. 2008;90(5 suppl):S13-S")
14
RecFSH: Bir sonraki gelişme
Farmakodinamik profili doğal insan FSH’sı ile benzer FSH üretimi için memeli hücre dizileri kullanılmıştır Çin hamsterinin over hücresi dizileri Yabancı DNA transfeksiyonu kolay FSH için gerekli glikoprotein sentezi kapasitesi var Vektör klonları ile transfer edilen FSH genlerini kodlayıp okuyabiliyor LH aktivitesi yok İzohormon profili doğal hipofiz FSH’sı ile benzer Yabancı protein içermeyen FSH Proteinin kaynağı üretimde takip ve tespit edilebiliyor Dayanıklılığı yüksek 2010: Uzun süreli FSH uyarıcısı Avrupa’da kullanım onayı almıştır Advances in recombinant DNA technology, including the cloning of the FSH gene, meant that this gene could be inserted into a host cell (Chinese hamster ovary [CHO] cell lines) for the purpose of the production of an FSH compound with an isohormone profile nearly identical to that of pituitary FSH. Because the genes inserted into the host are specific for only the subunits of FSH, the resulting protein has no LH bioactivity. The profile of this recombinant FSH (recFSH) is very similar to that of natural human FSH from urinary and pituitary sources. ÇHO hücreleri 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th recFSH = recombinant follicle-stimulating hormone; DNA = Deoxyribonucleic acid; CHO = Chinese hamster ovary; LH = luteinizing hormone; SFS = sustained follicle stimulant. Galway et al. Endocrinology. 1990;127:93; Olijve et al. Mol Hum Reprod. 1996;2:371. Galway AB, Hsueh AJ, Keene JL, Yamoto M, Fauser BC, Boime I. In vitro and in vivo bioactivity of recombinant human follicle-stimulating hormone and partially deglycosylated variants secreted by transfected eukaryotic cell lines. Endocrinology. 1990;127(1):93-100; Olijve W, de Boer W, Mulders JW, van Wezenbeek PM. Molecular biology and biochemistry of human recombinant follicle stimulating hormone (Puregon). Mol Hum Reprod. 1996;2(5): 14
 for the purpose of the production of an FSH compound with an isohormone profile nearly identical to that of pituitary FSH. Because the genes inserted into the host are specific for only the subunits of FSH, the resulting protein has no LH bioactivity. The profile of this recombinant FSH (recFSH) is very similar to that of natural human FSH from urinary and pituitary sources. ÇHO hücreleri. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. recFSH = recombinant follicle-stimulating hormone; DNA = Deoxyribonucleic acid; CHO = Chinese hamster ovary; LH = luteinizing hormone; SFS = sustained follicle stimulant. Galway et al. Endocrinology. 1990;127:93; Olijve et al. Mol Hum Reprod. 1996;2:371. Galway AB, Hsueh AJ, Keene JL, Yamoto M, Fauser BC, Boime I. In vitro and in vivo bioactivity of recombinant human follicle-stimulating hormone and partially deglycosylated variants secreted by transfected eukaryotic cell lines. Endocrinology. 1990;127(1):93-100; Olijve W, de Boer W, Mulders JW, van Wezenbeek PM. Molecular biology and biochemistry of human recombinant follicle stimulating hormone (Puregon). Mol Hum Reprod. 1996;2(5):")
15
GnRH Agonist ve Antagonistlerinin Geliştirilip Onaylanması
1971: GnRH izole edilmiş yapısı çözülmüştür 1-2 amino asiti değiştirilmiş GnRH agonistleri üretilmiştir 1978: GnRH kullanımından sonra over fonksiyonlarında geçici artış «alevlenme etkisi» bulunmuştur 1980lerin başı: GnRH agonistleri KOS sırasında prematür LH artışını önlemede kullanılmaya başlanmıştır 1980lerin sonu: GnRH agonistlerinin kullanımı IVF de standart olmuştur : GnRH antagonistleri FDA tarafından onaylanmıştır GnRH antagonistleri endojen gonadotropin uyarımını hemen önlemekte kesildiklerinde endojen salgı hemen başlamaktadır. In 1971, GnRH was isolated and its structure elucidated. Clinically safe GnRH agonists with 1 or 2 amino acid substitutions were developed. The “flare response,” a transient increase in gonadal function followed by pituitary downregulation after repeated administration of GnRH agonists, was discovered in 1978. In the early 1980s, GnRH agonists began to be used to prevent premature LH rises during COS. By the late 1980s they were part of standard IVF practice, since the use of GnRH agonists resulted in significantly better outcomes, with reduced cancellations and some scheduling flexibility. The first use of GnRH agonists in IVF treatment cycles involved the “long downregulation” protocol. A number of researchers have tried to shorten the duration of GnRH agonist administration by beginning on day 2 of menses, with gonadotropin administration beginning the following day. Clinical trials comparing the long and short GnRH agonist protocols resulted in similar efficacy. Clinically useful GnRH antagonists, which induce an immediate suppression of endogenous gonadotropin secretion and result in rapid recovery upon discontinuation, took much longer to reach the market (2001). 1910s 1920s 1930s 1940s 1950s 18th Century 17th 1960s 1970s 1980s 1990s 2000s 2010s 19th GnRH = gonadotropin releasing hormone; LH = luteinizing hormone; COS = controlled ovarian stimulation; IVF = in vitro fertilization. Hayden. Eur J Endocrinol. 2008;159(suppl 1):S17; Macklon et al. Endocr Rev. 2006;27:170. Hayden C. GnRH analogues: applications in assisted reproductive techniques. Eur J Endocrinol. 2008;159 (suppl 1):S17-S25; Macklon NS, Stouffer RL, Giudice LC, Fauser BC. The science behind 25 years of ovarian stimulation for in vitro fertilization. Endocr Rev. 2006;27(2): 15
. 1910s. 1920s. 1930s. 1940s. 1950s. 18th. Century. 17th. 1960s. 1970s. 1980s. 1990s. 2000s. 2010s. 19th. GnRH = gonadotropin releasing hormone; LH = luteinizing hormone; COS = controlled ovarian stimulation; IVF = in vitro fertilization. Hayden. Eur J Endocrinol. 2008;159(suppl 1):S17; Macklon et al. Endocr Rev. 2006;27:170. Hayden C. GnRH analogues: applications in assisted reproductive techniques. Eur J Endocrinol. 2008;159 (suppl 1):S17-S25; Macklon NS, Stouffer RL, Giudice LC, Fauser BC. The science behind 25 years of ovarian stimulation for in vitro fertilization. Endocr Rev. 2006;27(2):")
16
Gonadotropinlerin Klink Kullanımındaki Köşe Taşları
Uzun etkili FSH GnRH antagonistleri GnRH agonistleri recFSH FSH-HP u-FSH Hipofiz FSH u-hMG Saflık ve Özgül Aktivite Domuz FSH hCG PMSG 1930s 1950 1980 1995 2003 2010 CJhastalığı This slide reviews the main milestones in the development of gonadotropins and GnRH analogues for clinical use. As purity and specificity have increased through the use of human-derived and recombinant gonadotropins, the potential for local reactions and side effects has decreased while safety, efficiency, and efficacy have increased. Research in this area continues. Güvenlik Verimlilik Etkinlik Antikorlar Lokal, sistemik reaksiyonlar PMSG = pregnant mare serum gonadotropin; FSH = follicle-stimulating hormone; hCG = human chorionic gonadotropin; u-hMG = urinary human menopausal gonadotropin; u-FSH = urinary human FSH; GnRH = gonadotropin releasing hormone; FSH-HP = highly purified FSH; recFSH = recombinant human FSH; SFS = sustained follicle stimulant. Lunenfeld. Hum Reprod Update. 2004;10:453. Lunenfeld B. Historical perspectives in gonadotrophin therapy. Hum Reprod Update. 2004;10(6):
:")
17
Over Uyarılmasında Gelecek
AMH/AF sayısı GnRH Agonist Uyarımı Hepsini Dondurma Implantasyon Yenidoğan sağlığı OHSS Zayıf Cevap Hasta Yükü AMH = Anti-Müllerian hormone; AFC = antral follicle count; GnRH = gonadotropin releasing hormone; OHSS = ovarian hyperstimulation syndrome. Practice Committee of Society for Assisted Reproductive Technology. Fertil Steril. 2012;97:835–842; Ferraretti Hum Reprod. 2011;26:1616–1624; Andersen et al. Hum Reprod. 2009;24:1267–1287; Umranikar et al. Eur J Obstet Gynecol Reprod Biol. 2013;170:299–304. 17

18
MOLEKÜLER YAPI VE FARMAKOLOJİ

19
Glikoprotein Hormonlar
LH FSH Alfa subunit ayı 92 aa hCG TSH

20
Non-kovalent bağla birleşmiş, 2 farklı amino asit zincirinden (α ve β subunitleri) oluşan gliko-protein hormondur α ALT ÜNİTE: 92 amino asitten oluşur ve Asn-52 ile Asn-78 amino asitlerine bağlı 2 karbohidrat eki içerir Toplam 4 aspargin içeren glikolizasyon bölgesi mevcut

21
β ALT ÜNİTE: 111 aminoasitten oluşur ve Asn-7 ile Asn-24 aminoasitlerine bağlı 2 karbohidrat eki içerir Toplam 4 aspargin içeren glikolizasyon bölgesi mevcut

22
İnsan FSH’sı nedir? FSH molekülü farklı birçok izoform yapıda bulunur: mikroheterojenite karbohidrat yapılarındaki farklılıktan kaynaklanır Karbohidrat yapıları FSH’nın yarı ömrünü belirleme açısından önemlidir ve dolayısı ile de in-vivo biyolojik aktivitesini belirlemede rol oynar

23
Follikül Stimulan Hormon (FSH)
Yarı ömrü dakika Sialik asid rezidüsü arttıkça, reseptör affinitesi azalır, dolaşımda daha uzun süre kalır

24
α LH β 121 aa hCG 145 aa

25
Gonadotropinlerin Peptid Kompozisyonu
LH ve HCG %81 oranında benzerlik gösterir Yarı ömür LH dakika hCG 24 saat

26
Yüksek oranda purifiye
GONADOTROPİNLER ÜRİNER hMG Menotropinler Üriner FSH Yüksek oranda purifiye Üriner hCG REKOMBİNANT Rekombinant FSH Rekombinant hCG Rekombinant LH Corifollitropin

27
İnsan Menapozal Gonadotropini

28
Human Menapozal Gonadotropini
Postmenapozal kadınların idrarından elde edilir İlk preparatlar %5 saf ve farklı oranlarda FSH, LH ve hCG içerirdi 75 IU FSH + 75 IU LH hMG’deki LH benzeri etki esas olarak hCG içeriğinden kaynaklanır hCG, LH-benzeri etki gösterir

29
ÜRİNER FSH Poliklonal antikorlar ile LH’nın uzaklaştırılması ile saf üriner FSH Post-menapozal kadınların idrarından elde edilir Gonadotropinler ya antikor affinite kolonları ya da konvansiyonel kromotografi ile saflaştırılarak elde edilir

30
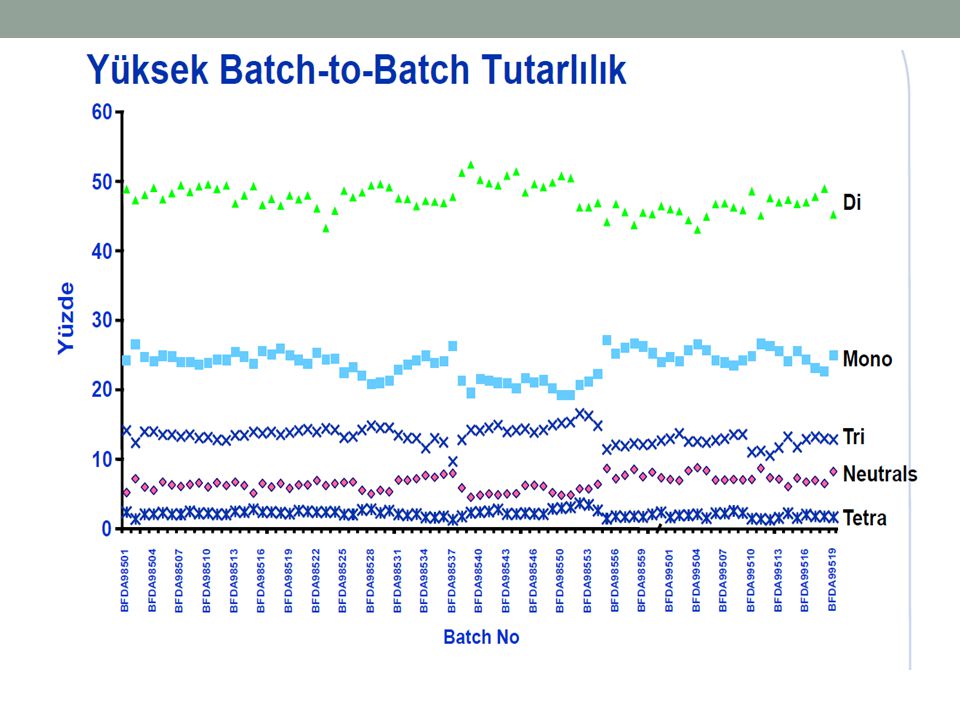
ÜRİNER FSH FSH’ya spesifik monoklonal antikorlar ile yüksek oranda purifiye (HP) üriner FSH HP-üriner FSH <0.1 IU LH <%5 üriner protein 10000 IU/mg spesifik FSH aktivitesi Subkutan uygulama Üretim serileri arası (Batch-to-batch) değişkenlikte azalma
 değişkenlikte. azalma.")
31
Rekombinant İnsan Gonadotropinleri

32
FSH’nın mikroheterojenitesi (İzoformlar)
Protein zincirlerine bağlı karbohidrat yapıları ve bunların sialik asit içerikleri farklı izoformları oluşturur Bu farklı formlar biyolojik yarı ömrü ve invivo aktivitedeki farklılığı belirler Daha bazik formlar daha çabuk elimine olur ve daha düşük invivo potense sahiptir Daha asidik formlar ise daha geç elimine olur ve daha yüksek invivo potense sahiptir

34
Mevcut 2 rekombinant preparat
Follitropin alfa Follitropin beta Her iki preparat ta FSH ile aynı Her ne kadar alfa ve beta olarak adlandırılsalar da aslında her ikisi de bir alfa ve bir beta glikoprotein zincir içerirler

35
Bu farklı glikoprotein zincirler elektrostatik ve hidrofobik kuvvetlerle non-kovalent bağ ile iki kompleks karbohidrat yapıya bağlanır Posttranslasyonel glikolizasyon işlemi ve saflaştırma işlemleri benzer değildir ve bu durum farklı sialik asid rezidü kompozisyonuna ve böylece farklı izoelektrik etkinliğe yol açar Ancak yapıdaki küçük farklılıklar klinik sonuçlar üzerine kanıtlanmış fark oluşturmamakta

37
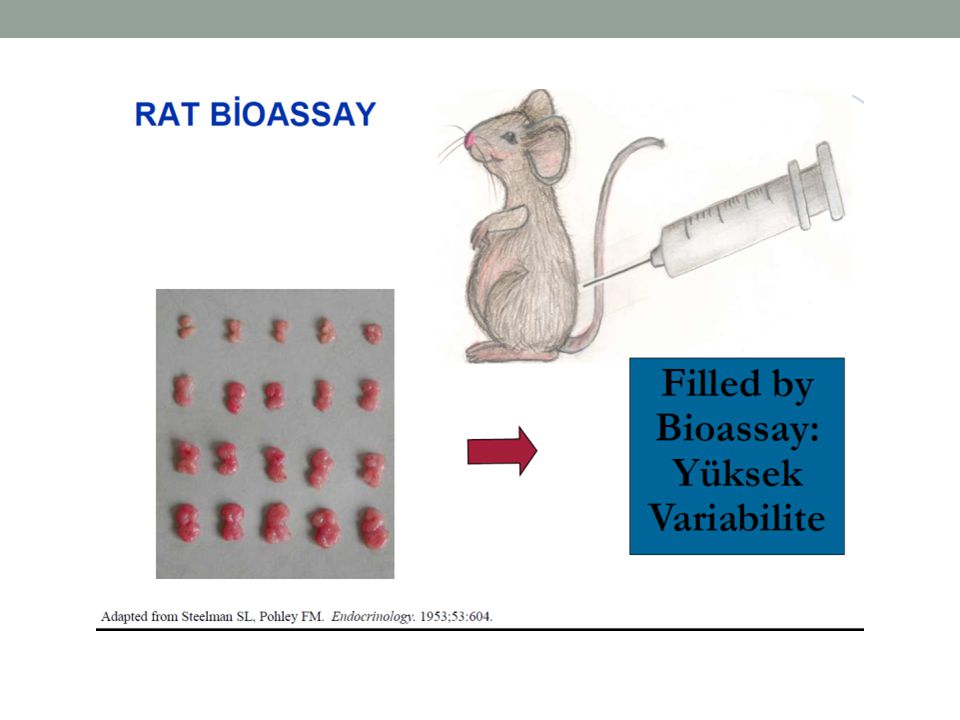
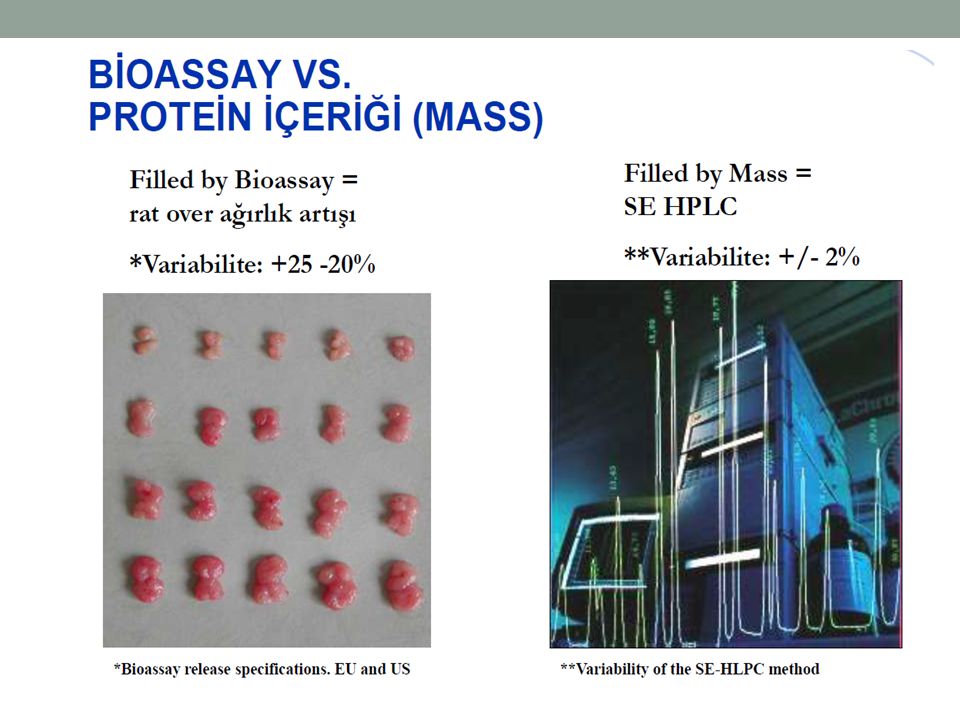
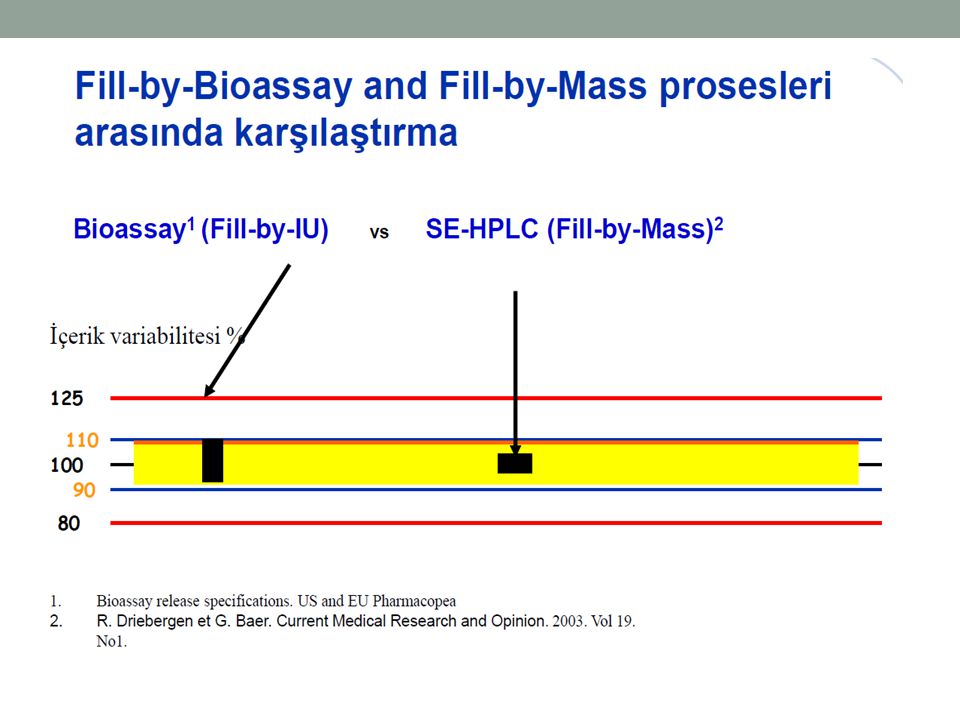
BİYOLOJİK AKTİVİTE Üriner kaynaklı FSH preparatlarının FSH içeriğinin aksine rekombinant FSH preparatları biolojik aktiviteleri yerine protein içeriklerine göre (µg cinsinden kütle) değerlendirilirler FSH içeren preparatların biolojik aktivitesi üretim aşamasında klasik Steelman-Pohley over bioassay ile doğrulanmaktadır
 değerlendirilirler. FSH içeren preparatların biolojik aktivitesi üretim aşamasında klasik Steelman-Pohley over bioassay ile doğrulanmaktadır.")
39
Fill-by-IU Prosesi Üriner preparatların hazırlanması için fazla miktarda idrar toplanması gerekli Preparatlar farklı içeriğe ve protein kontaminasyonuna sahipler Aktif proteinin kütle ile ölçülmesi anlamsız

40
Fill-by-IU Prosesi Bu nedenle biyofarmasötik endüstrisinde geleneksel standard gonadotropinleri (ve diğer ürünleri) INVIVO veya INVITRO BIOASSAY YÖNTEMLERİ (Fill-by-IU) kullanarak biyopotens ile ölçüp doldurmakta Bioassay yöntemleri aktif protein miktarını üretilen spesifik biyolojik yanıtı değerlendirerek ve international unit (IU) cinsinden işaretleyerek ölçmekte ve uluslararası kabul edilmiş standartlara göre etiketlemektedir
 kullanarak biyopotens ile ölçüp doldurmakta. Bioassay yöntemleri aktif protein miktarını üretilen spesifik biyolojik yanıtı değerlendirerek ve international unit (IU) cinsinden işaretleyerek ölçmekte ve uluslararası kabul edilmiş standartlara göre etiketlemektedir.")
41
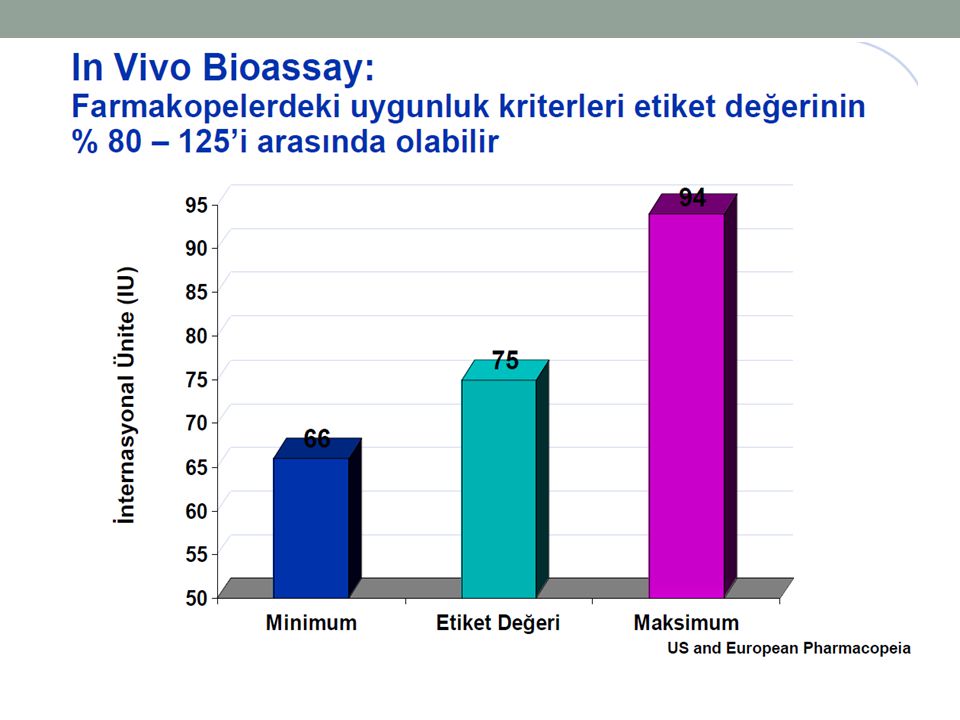
Fill-by-IU Prosesi Üretilen hammadde üzerindeki bioassay test sonuçları aktif proteinin ampul ve flakonlara istenilen bioaktivite miktarı ile doldurulmasına izin verir Sonuçta, Farmakopelere göre etiketlenen etkinlik miktarı % aralığındırda olmak zorunda

44
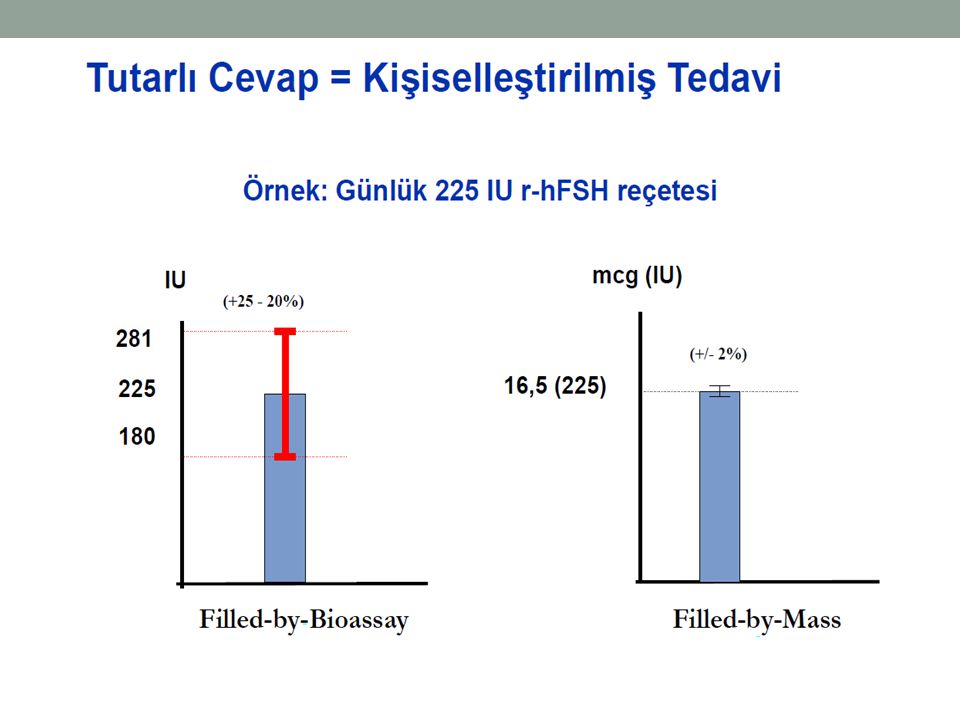
FİLL-BY-MASS Hem folitropin alfa hem de beta formulasyonları kütle-ile-dolum (fill-by-mass) yöntemi ile değerlendirilmekte Steelman-Pohley Assay ile 75 IU FSH = 5.0 ve 5.5 µg fill-by-mass ürüne denk gelmekte Rekombinant FSH ürünler: Pen-shaped devices Vialler halinde Tüm preparatlar liyofilize pudra olarak paketlenmiş cartridge ya da pen olarak hazırlanmış formulasyonları da mevcut

50
non-FSH insan proteini (%) İnsan Menapozal Gonadotropin İdrar 75
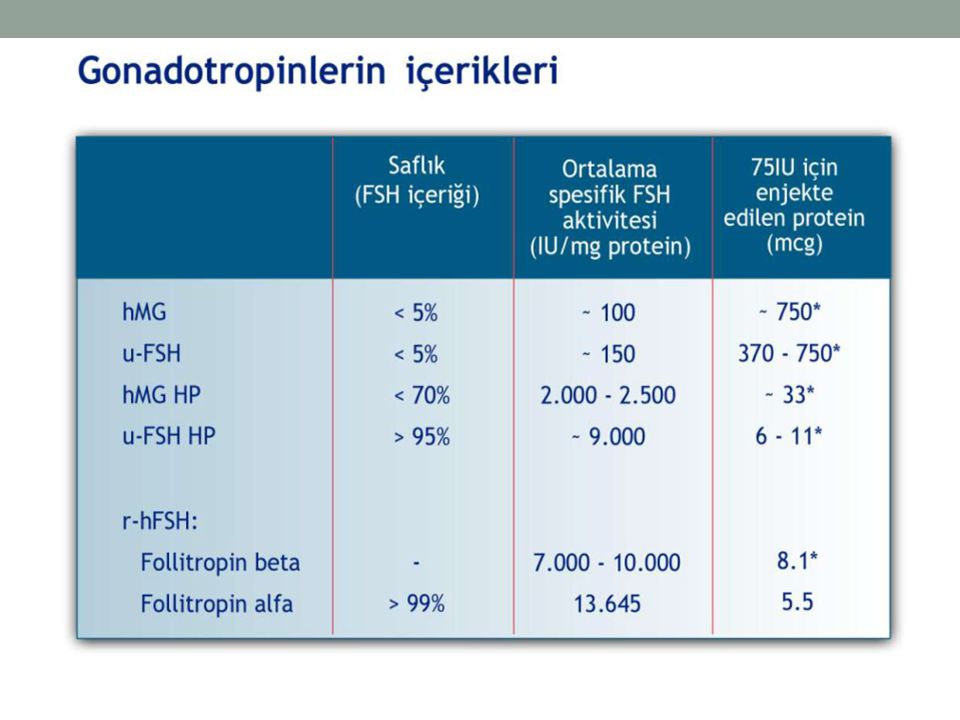
Preparat Kaynak FSH aktivitesi (IU/vial/ampul) LH aktivitesi Ko-purifiye non-FSH insan proteini (%) İnsan Menapozal Gonadotropin İdrar 75 >95 İdrar-kaynaklı FSH <0.7 Yüksek oranda pürifiye, idrar kaynaklı FSH 75-150 <0.001 <1 Rekombinant insan FSH Memeli hücreleri Yok Yeni formülasyon rekombinant insan FSH (filled by mass) 5.5µg (75IU) Gonadotropin preparatlarının içerikleri.
 LH aktivitesi. Ko-purifiye. non-FSH insan proteini (%) İnsan Menapozal Gonadotropin. İdrar. 75. >95. İdrar-kaynaklı FSH. <0.7. Yüksek oranda pürifiye, idrar kaynaklı FSH < <1. Rekombinant insan FSH. Memeli hücreleri. Yok. Yeni formülasyon rekombinant insan FSH (filled by mass) 5.5µg (75IU) Gonadotropin preparatlarının içerikleri.")
52
YÜKSEK ORANDA PÜRİFİYE ÜRİNER KAYNAKLI FSH
ASİDİK İZOFORMLAR (ürine hp-FSH) DAHA AZ ASİDİK İZOFORMLAR (Rekombinant) Yarılanma ömrü Daha uzun Daha kısa İn vivo biyopotens Yüksek Düşük İn vitro estradiol sekresyonu Foliküler eşik Yüksek seçicilik Düşük seçicilik Foliküler büyüme hızı Yavaş Hızlı
 DAHA AZ ASİDİK İZOFORMLAR (Rekombinant) Yarılanma ömrü. Daha uzun. Daha kısa. İn vivo biyopotens. Yüksek. Düşük. İn vitro estradiol sekresyonu. Foliküler eşik. Yüksek seçicilik. Düşük seçicilik. Foliküler büyüme hızı. Yavaş. Hızlı.")
53
REKOMBİNANT LH Rekombinant LH preparatları 1993 yılından itibaren 75 IU enjektör halinde mevcut LH eksikliği olan özellikle hipogonadotropik hipogonadizm tanılı hastalarda ya da azalmış over rezervinde kullanılabilir

54
KORYONİK GONADOTROPİN
Foliküler matürasyonun son basamağını hızlandırmak amacıyla ve profaz I’deki (germinal vezikül basamağı) immatür oositi metafaz II’e ulaştırmak üzere mayotik maturasyonunu sağlamak üzere kullanılır Mayotik sürecin tamamlanması için gerekli süre ortalama 36 saat OPU işleminin gerçekleşmemesi halinde ortalama 4 saat sonra ovulasyon gerçekleşecektir
 immatür oositi metafaz II’e ulaştırmak üzere mayotik maturasyonunu sağlamak üzere kullanılır. Mayotik sürecin tamamlanması için gerekli süre ortalama 36 saat. OPU işleminin gerçekleşmemesi halinde ortalama 4 saat sonra ovulasyon gerçekleşecektir.")
55
KORYONİK GONADOTROPİN
Koryonik gonadotropin insan kaynaklı gebe kadınların idrarından (hCG) elde edilebilir ya da rekombinant teknoloji kullanılarak üretilebilir hCG preparatları IU 10000 IU Rekombinant µg ( IU)
 elde edilebilir ya da rekombinant teknoloji kullanılarak üretilebilir. hCG preparatları 5000 IU IU. Rekombinant 250 µg ( IU)")
56
ELONVA™ Korifollitropin Alfa
FERT /12 ELONVA™ Korifollitropin Alfa

57
t½ corifollitropin alfa = 69 h
Corifollitropin alfa is a Recombinant Hormone Subunits β Subunits Human FSH 92 aa 111 aa t½ Puregon = 30 h hCG 92 aa 145 aa 28aa Corifollitropin alfa is a recombinant glycoprotein that was created from the fusion of the β-subunit of FSH with a part of the β-subunit of human chorionic gonadotropin (hCG) called the carboxy-terminal peptide. The gonadotropic hormones include thyroid-stimulating hormone (TSH), FSH, luteinizing hormone (LH), and hCG. All of these glycoprotein hormones consist of 2 linked protein chains, which are called α- and β-subunits. They all have an identical α-subunit, which is 92 amino acids long, but each has a unique β-subunit. The number of amino acids in the β-subunit varies between the hormones, and the β-subunit is therefore responsible for the specific biological action of each hormone. The corifollitropin alfa molecule consists of The α-subunit, which is identical for all gonadotropins, and A hybrid β-subunit created through the fusion of the β-subunit of human FSH with the carboxy-terminal peptide of the β-subunit of hCG The carboxy-terminal peptide is a small peptide found on the β-subunit of the hCG molecule; it is not found on other gonadotropins, and it has a significant impact on the biological activity of corifollitropin alfa (increases the half-life of the molecule from ≈30 hours to ≈70 hours). These are the molecular details; the clinical details are next (what you will receive when it is delivered to your clinic). Corifollitropin alfa 92 aa 111 aa t½ corifollitropin alfa = 69 h FSH = follicle-stimulating hormone; aa = amino acids; t½ = half life. Strauss and Barbieri. Yen and Jaffe's Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management. 5th edition
 called the carboxy-terminal peptide. The gonadotropic hormones include thyroid-stimulating hormone (TSH), FSH, luteinizing hormone (LH), and hCG. All of these glycoprotein hormones consist of 2 linked protein chains, which are called α- and β-subunits. They all have an identical α-subunit, which is 92 amino acids long, but each has a unique β-subunit. The number of amino acids in the β-subunit varies between the hormones, and the β-subunit is therefore responsible for the specific biological action of each hormone. The corifollitropin alfa molecule consists of. The α-subunit, which is identical for all gonadotropins, and. A hybrid β-subunit created through the fusion of the β-subunit of human FSH with the carboxy-terminal peptide of the β-subunit of hCG. The carboxy-terminal peptide is a small peptide found on the β-subunit of the hCG molecule; it is not found on other gonadotropins, and it has a significant impact on the biological activity of corifollitropin alfa (increases the half-life of the molecule from ≈30 hours to ≈70 hours). These are the molecular details; the clinical details are next (what you will receive when it is delivered to your clinic). Corifollitropin alfa. 92 aa. 111 aa. t½ corifollitropin alfa = 69 h. FSH = follicle-stimulating hormone; aa = amino acids; t½ = half life. Strauss and Barbieri. Yen and Jaffe s Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management. 5th edition")
58
ARKA PLAN

59
IVF’de Tedaviden Ayrılma Nedenleri
“Aktif”: Doktorun önerisiyle. “Pasif”: Hastanın kararıyla. 59

60
IVF Tedavisi Neden Terk Ediliyor?
Olivius et al.1 Rajkhowa et al.2 Sebepler n % Psikolojik Yük 50 26 Kötü Prognoz 48 25 Spontan Gebelik 37 19 Boşanma 28 15 Fiziksel Yük 11 6 Ağır Hastalık 3 2 Diğer 7 Total 192 100 Sebepler % Psikolojik Stres 36 Diğer Nedenler 30 Finansman 23 Başarısızlık Genel Huzursuzluk <10 Tıbbi Nedenler

61
Konvansiyonel vs Hasta-Dostu Tedaviler
Konvansiyonel protokol GnRH agonisti + 2 embriyo rFSH Hasta dostu tedavi protokolü GnRH antagonisti + 1-2 embriyo rFSH 61

62
Hastaların Tedaviye Devam Oranları
100 95.9% Hasta Dostu Konvansiyonel 88.3% 90 93.7% 80 Devam Oranları (%) 78.6% 75.9% 70 60 P=0.034 1 2 3 Sikluslar Verberg et al. Hum Reprod. 2008;23:2050. 62 62
 78.6% 75.9% P= Sikluslar. Verberg et al. Hum Reprod. 2008;23:")
63
Enjeksiyon Sürecinde Hastaların Deneyimleri
%55 : IVF enjeksiyonları hayatımı olumsuz etkiledi. %31: Enjeksiyonlar nedeniyle günlük aktivitelerim etkilendi. %57 : Enjeksiyonları yaparken sorun yaşadım. %45 : Enjeksiyon hatası yaptım. %29 : Hata yaptığım halde doktoruma söylemedim. Huisman et al. Reprod Biomed Online. 2009;19:(suppl 2):5.
:5.")
64
Moleküler YapI

65
Korifollitropin Alfa’nın Oluşumu1–3
FSH α β Ala Ser CH/S Asn CH/S Ser Glu CH/S Asn CH/S Asn t½ rFSH ≈ 40 saat CH/S Asn t½ korifollitropin alfa = 69 saat Ser Ser Karboksi-terminal Peptid t1. Yen and Jaffe's Reproductive Endocrinology: Physiology, Pathophysiology, and Clinical Management. 5th edition. Saunders: 2004:36–37; 2. Puregon SmPC (Jan 2010 update); 3. Elonva SmPC (March 2010 update). hCG = human chorionic gonadotropin; FSH = follicle-stimulating hormone. 1. Fares FA et al. Proc Natl Acad Sci U S A. 1992;89:4304–4308; 2. Puregon SmPC (Jan 2010 update); 3. Elonva SmPC (March 2010 update).
; 3. Elonva SmPC (March 2010 update). hCG = human chorionic gonadotropin; FSH = follicle-stimulating hormone. 1. Fares FA et al. Proc Natl Acad Sci U S A. 1992;89:4304–4308; 2. Puregon SmPC (Jan 2010 update); 3. Elonva SmPC (March 2010 update).")
66
Farmakokİnetİk Özellİkler Doz Bulma ÇalIşmalarI

67
Doz Bulma Çalışmaları: Modellemenin Şematik Gösterimi1
Korifollitropin alfa dozu (Yalnız 1. gün) Farmakokinetik Folliküler Hacim (8. günde) Model 1 Model 3 Model 5 Model 2 Model 4 Üretim Üretim Siklus İptal Oranı Oosit Sayısı Modülatör İnhibin B + Model 4 Model 5 + Eliminasyon Eliminasyon rFSH dozu (8.günden sonra) Model 5 1-8. günler arası primer farmakokinetik 8. günden sonraki final cevap 1. Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87. PK = pharmacokinetic; rFSH = recombinant follicle-stimulating hormone; AUC = area under the curve. 1. de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87.
 Farmakokinetik. Folliküler Hacim. (8. günde) Model 1. Model 3. Model 5. Model 2. Model 4. Üretim. Üretim. Siklus İptal Oranı. Oosit Sayısı. Modülatör. İnhibin B. + Model 4. Model 5. + Eliminasyon. Eliminasyon. rFSH. dozu. (8.günden sonra) Model günler arası primer farmakokinetik. 8. günden sonraki final cevap. 1. Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87. PK = pharmacokinetic; rFSH = recombinant follicle-stimulating hormone; AUC = area under the curve. 1. de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87.")
68
Ovülasyon İndüksiyonu
7.5 µg yetersiz 15-60 µg aralığında doza bağımlı uyarım var Anovulatuvar ve sağlıklı kadınlarda farmakokinetik aynı Plazma konsantrasyonları endojen hormonal çevreden etkilenmiyor Seyhan A ve Ata B, Int J Women Health, 2011

69
IVF/ICSI: Siklus Başına İptal Oranları/Elde Edilen Oosit Sayıları ile Korifollitropin alfa Dozu İlişkisi1 Ağırlık >60 kg Ağırlık ≤60 kg Siklus Başına Elde Edilen Ort. Oosit Sayısı İptal Oranı Ağırlık >60 kg Ağırlık ≤60 kg Korifollitropin alfa (µg) Korifollitropin alfa (µg) 1. Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87. AUC = area under the curve; GnRH = gonadotropin-releasing hormone. 1. de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87.
 Korifollitropin alfa (µg) 1. Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87. AUC = area under the curve; GnRH = gonadotropin-releasing hormone. 1. de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87.")
70
> 60 kg olan hastalarda 100-µg’lık doz daha fazla siklus iptaline neden olabilir.1
Over cevabında azalma yok. ELONVA™ (korifollitropin alfa) Siklus iptaline sebep olabilecek yetersiz maruziyet: FSH aktivitesinin eşik altına düşmesi FSH Aktivitesia Eşik 1 2 3 4 5 6 7 8 9 10 Stimülasyon Günleri 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159. 1. de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87. 2. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159.
 Siklus iptaline sebep olabilecek yetersiz maruziyet: FSH aktivitesinin eşik altına düşmesi. FSH Aktivitesia. Eşik Stimülasyon Günleri. 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒ de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒ Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159.")
71
≤ 60 kg olan hastalarda 150-µg’lık doz aşırı stimülasyona neden olabilir.1
ELONVA™ (korifollitropin alfa) Maksimum Cevap Aşırı maruziyete, dolayısıyla aşırı stimülasyona neden olabilir. Maksimum etki; bundan ötesi daha iyi over cevabı sağlamaz. FSH Aktivitesia Eşik 1 2 3 4 5 6 7 8 9 10 Stimülasyon Günleri 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159. 1. de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87. 2. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159.
 Maksimum Cevap. Aşırı maruziyete, dolayısıyla aşırı stimülasyona neden olabilir. Maksimum etki; bundan ötesi daha iyi over cevabı sağlamaz. FSH Aktivitesia. Eşik Stimülasyon Günleri. 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒ de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒ Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159.")
72
Vücut Ağırlığına Göre İki Farklı Doz Şeması1
>60 kg ≤60 kg 150 µg 1 hafta boyunca devam follikül gelişimi Uygun Değil Aşırı maruziyete, dolayısıyla aşırı stimülasyona neden olabilir 100 µg, bu grup için yeterlidir. 100 µg Yetersiz maruziyet nedeniyle daha fazla siklus iptali olasılığı. Bu doz, over cevabını değiştirmez. («mild» stimülasyon söz konusu değil) 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159. FSH = follicle-stimulating hormone. 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159.
 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159. FSH = follicle-stimulating hormone. 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159.")
73
Eğri Altında Kalan Alan (AUC)
Faz III çalışmalarda 100-µg ve 150-µg ELONVA™’ya (korifollitropin alfa) benzer maruziyet1 Eğri Altında Kalan Alan (AUC) 100 µg 150 µg AUC, hng/mL 1500 1000 500 ≤60 kg >60 kg 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159. 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒159. 2. de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒87. 3. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. 4. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.
 benzer maruziyet1. Eğri Altında Kalan Alan (AUC) 100 µg. 150 µg. AUC, hng/mL ≤60 kg. >60 kg. 1. Ledger WL et al. Reprod Biomed Online. 2011;23:150‒ Ledger WL et al. Reprod Biomed Online. 2011;23:150‒ de Greef R et al. Clin Pharmacol Ther. 2010;88:79‒ Devroey P et al. Hum Reprod. 2009;24:3063‒ Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.")
74
Doğal Step-down Protokole Benzer Farmakokinetik Özellik
Korifollitropin alfa rFSH t½ korifollitropin alfa = 69 saat Tmax = 36–48 saat2 FSH Activity1 Terapötik eşik t½ rFSH ≈ 40 saat Tmax = 10–12 saat3 1 2 3 4 5 6 7 8 9 10 Stimülasyon Günleri 1. Fauser BC et al. Hum Reprod Update. 2009;15:309–321; 2. ELONVA™ (corifollitropin alfa) summary of product characteristics, 2010; 3. PUREGON® (rFSH) summary of product characteristics, 2010. rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. J Clin Endocrinol Metab. 2004;89:2062‒ Duijkers IJ et al. Hum Reprod. 2002;17:1987‒ Fauser BC et al. Hum Reprod Update. 2009;15:309– ELONVA™ (corifollitropin alfa) summary of product characteristics. N.V. Organon, a subsidiary of Merck & Co., Inc.; 2010.
 summary of product characteristics, 2010; 3. PUREGON® (rFSH) summary of product characteristics, rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. J Clin Endocrinol Metab. 2004;89:2062‒ Duijkers IJ et al. Hum Reprod. 2002;17:1987‒ Fauser BC et al. Hum Reprod Update. 2009;15:309– ELONVA™ (corifollitropin alfa) summary of product characteristics. N.V. Organon, a subsidiary of Merck & Co., Inc.;")
75
Faz III Klİnİk ÇalIşma ProgramI

76
ELONVA™(korifollitropin alfa) Faz III Klinik Çalışmalar
Engage1 Ensure2 Pursue3 Çalışma Kolları ELONVA 150 µg vs rFSH 200 IU/gün; > 60 kg kadınlar ELONVA 100 µg vs rFSH 150 IU/gün; ≤ 60 kg kadınlar ELONVA 150 µg vs rFSH 300 IU/gün; > 50 kg kadınlar Dizayn Çift-kör randomize kontrollü çalışma, tek siklus Hasta Sayısı (n) 1,506 396 1,390 Primer Sonlanım Noktası Devam eden gebelik oranı (ET sonrası >10. hafta) Elde edilen oosit sayısı Vital gebelik oranı (ET sonrası 4-5. hafta) Çalışma Merkezleri Avrupa 20, Kuzey Amerika 14 Avrupa 14, Asya 5 ABD 33 1. Devroey P et al. Hum Reprod. 2009;24:3063‒ Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76 3. Boostanfar et al. Presented at ASRM 2012, San Diego. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.
 1, ,390. Primer Sonlanım Noktası. Devam eden gebelik oranı (ET sonrası >10. hafta) Elde edilen oosit sayısı. Vital gebelik oranı (ET sonrası 4-5. hafta) Çalışma Merkezleri. Avrupa 20, Kuzey Amerika 14. Avrupa 14, Asya 5. ABD Devroey P et al. Hum Reprod. 2009;24:3063‒ Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76 3. Boostanfar et al. Presented at ASRM 2012, San Diego. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.")
77
Engage ÇalIşmasI

78
Engage Çalışması: Tedavi Rejimleri1
ELONVA ™ (korifollitropin alfa) (150 µg) Plasebo ELONVA GnRH antagonist (GANIRELIX® 0.25 mg/gün) 5. günden hCG gününe dek Stimülasyon günü 5 hCG günü: 3 follikül ≥17 mm Stimülasyon günü 8 Siklus günü 2–3 = Stimülasyon günü 1 Günlük rFSH (7 gün boyunca 200 IU) Araştırma Grubu Referans Grup Plasebo rFSH (doz ≤200 IU) IVF veya ICSI Luteal faz desteği 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. COS = controlled ovarian stimulation; FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection; hCG = human chorionic gonadotropin. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.
 (150 µg) Plasebo. ELONVA. GnRH antagonist (GANIRELIX® 0.25 mg/gün) 5. günden hCG gününe dek. Stimülasyon günü 5. hCG günü: 3 follikül ≥17 mm. Stimülasyon günü 8. Siklus günü 2–3 = Stimülasyon günü 1. Günlük rFSH. (7 gün boyunca 200 IU) Araştırma Grubu. Referans Grup. Plasebo rFSH. (doz ≤200 IU) IVF. veya. ICSI. Luteal. faz desteği. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. COS = controlled ovarian stimulation; FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection; hCG = human chorionic gonadotropin. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.")
79
Hasta Alım Kriterleri1 Dahil Edilme Hariç Bırakılma
Engage Hasta Alım Kriterleri1 Dahil Edilme IVF/ICSI için KOS endikasyonu Normal menstrüel siklus uzunluğu (24–35 gün) ≥18 ila ≤36 yaş >60 ila ≤90 kg ağırlık (VKİ ≥18 ila ≤32 kg/m2) Hariç Bırakılma Endokrin anormallik PKOS Bilinen düşük over cevabı veya cevap yokluğu OHSS öyküsü >20 bazal antral follikül 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection; FSH = follicle-stimulating hormone; OHSS = ovarian hyperstimulation syndrome. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.
 ≥18 ila ≤36 yaş. >60 ila ≤90 kg ağırlık (VKİ ≥18 ila ≤32 kg/m2) Hariç Bırakılma. Endokrin anormallik. PKOS. Bilinen düşük over cevabı veya cevap yokluğu. OHSS öyküsü. >20 bazal antral follikül. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection; FSH = follicle-stimulating hormone; OHSS = ovarian hyperstimulation syndrome. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.")
80
Ko-primer Sonlanım Noktası: Oositler1
Engage Ko-primer Sonlanım Noktası: Oositler1 ELONVA™ (korifollitropin alfa) 150 µg (n=756) rFSH 200 IU/gün (n=750) Fark, ANOVA (95% CI) Elde Edilen Oosit Sayısı, Ortalama (SD) 13.7 (8.2) 12.5 (6.7) 1.2a (0.5–1.9) MII evresindeki oositler (%) 78.9 77.4 a P=0.001. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. rFSH = recombinant follicle-stimulating hormone; MII = metaphase II. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.
 150 µg. (n=756) rFSH. 200 IU/gün. (n=750) Fark, ANOVA (95% CI) Elde Edilen Oosit Sayısı, Ortalama (SD) 13.7 (8.2) 12.5 (6.7) 1.2a (0.5–1.9) MII evresindeki oositler (%) a P= Devroey P et al. Hum Reprod. 2009;24:3063‒3072. rFSH = recombinant follicle-stimulating hormone; MII = metaphase II. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.")
81
Primer Sonlanım Noktası: Devam Eden Gebelik Oranı1
Engage Primer Sonlanım Noktası: Devam Eden Gebelik Oranı1 ITT Grubu Hastalar, % 38.9 38.1 ELONVA 150 µg (n=756) Transfer edilen embriyo sayısı: 1.7 rFSH 200 IU/gün (n=750) Transfer edilen embriyo sayısı: 1.7 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.
 Transfer edilen embriyo sayısı: 1.7. rFSH 200 IU/gün (n=750) Transfer edilen embriyo sayısı: Devroey P et al. Hum Reprod. 2009;24:3063‒3072. rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.")
82
hCG Kriterlerine Ulaşılan Günler1
Engage hCG Kriterlerine Ulaşılan Günler1 ™ Hastalar, % Stimülasyon Günü Hastaların 1/3’ünde ek rFSH’a ihtiyaç olmamıştır. 1. Fauser BC et al. Reprod Biomed Online. 2010;21:593‒601. hCG = human chorionic gonadotropin; rFSH = recombinant follicle-stimulating hormone. 1. Fauser BC et al. Reprod Biomed Online. 2010;21:593‒601. 2. Data on file, MSD. 3. Devroey P et al. Hum Reprod. 2009;24:3063‒3072.

83
Serum E2 Düzeyleri1 Serum E2 düzeyi, pmol/L Stimülasyon Günü 4,000
Engage Serum E2 Düzeyleri1 Serum E2 düzeyi, pmol/L Stimülasyon Günü 4,000 8,000 12,000 1 5 8 hCG ELONVA™ (korifollitropin alfa) 150 µg rFSH 200 IU/gün 1. Fauser BC et al. Reprod Biomed Online. 2010;21:593‒601. rFSH = recombinant follicle-stimulating hormone. 1. Fauser BC et al. Reprod Biomed Online. 2010;21:593‒601.
 150 µg. rFSH 200 IU/gün. 1. Fauser BC et al. Reprod Biomed Online. 2010;21:593‒601. rFSH = recombinant follicle-stimulating hormone. 1. Fauser BC et al. Reprod Biomed Online. 2010;21:593‒601.")
84
ELONVA™ (korifollitropin alfa)
Engage Advers Olaylar Hastalar (%) ELONVA™ (korifollitropin alfa) 150 µg (n=755) rFSH 200 IU/gün (n=751) Ciddi Advers Olay 37 (4.9) 37 (4.9) Advers Olay Total 481 (63.7) 459 (61.1) İlaç İlişkili 177 (23.4) 187 (24.9) Şiddetli 55 (7.3) 43 (5.7) AO Nedeniyle Tedavi Kesilmesi 16 (2.1) 3 (0.4) 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. SAE = serious adverse event; AE = adverse event; rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. 2. Data on file, MSD.
 ELONVA™ (korifollitropin alfa) 150 µg. (n=755) rFSH. 200 IU/gün. (n=751) Ciddi Advers Olay. 37 (4.9) 37 (4.9) Advers Olay. Total. 481 (63.7) 459 (61.1) İlaç İlişkili. 177 (23.4) 187 (24.9) Şiddetli. 55 (7.3) 43 (5.7) AO Nedeniyle Tedavi Kesilmesi. 16 (2.1) 3 (0.4) 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. SAE = serious adverse event; AE = adverse event; rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒ Data on file, MSD.")
85
ELONVA™ (korifollitropin alfa)
Engage OHSS Olguları Hastalar, % (n) OHSS Şiddeti ELONVA™ (korifollitropin alfa) 150 µg (n=755) rFSH 200 IU/gün (n=751) Hafif 2.9 (22) 3.6 (27) Orta 2.3 (17) 1.3 (10) Ciddi 1.9 (14) 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. OHSS = ovarian hyperstimulation syndrome; rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. 2. Data on file, MSD.
 OHSS Şiddeti. ELONVA™ (korifollitropin alfa) 150 µg. (n=755) rFSH. 200 IU/gün. (n=751) Hafif. 2.9 (22) 3.6 (27) Orta. 2.3 (17) 1.3 (10) Ciddi. 1.9 (14) 1. Devroey P et al. Hum Reprod. 2009;24:3063‒3072. OHSS = ovarian hyperstimulation syndrome; rFSH = recombinant follicle-stimulating hormone. 1. Devroey P et al. Hum Reprod. 2009;24:3063‒ Data on file, MSD.")
86
Ensure ÇalIşmasI

87
Ensure Çalışması: Tedavi Rejimleri1
ELONVA ™ (korifollitropin alfa) (100 µg) Plasebo ELONVA GnRH antagonist (GANIRELIX® 0.25 mg/gün) 5. günden hCG gününe dek Stimülasyon günü 5 hCG günü: 3 follikül ≥17 mm Stimülasyon günü 8 Siklus günü 2–3 = Stimülasyon günü 1 Günlük rFSH (7 gün boyunca 150 IU) Araştırma Grubu Referans Grup Plasebo rFSH (doz ≤200 IU) IVF veya ICSI Luteal faz desteği 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. COS = controlled ovarian stimulation; rFSH = recombinant follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection; hCG = human chorionic gonadotropin. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.
 (100 µg) Plasebo. ELONVA. GnRH antagonist (GANIRELIX® 0.25 mg/gün) 5. günden hCG gününe dek. Stimülasyon günü 5. hCG günü: 3 follikül ≥17 mm. Stimülasyon günü 8. Siklus günü 2–3 = Stimülasyon günü 1. Günlük rFSH. (7 gün boyunca 150 IU) Araştırma Grubu. Referans Grup. Plasebo rFSH. (doz ≤200 IU) IVF. veya. ICSI. Luteal. faz desteği. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. COS = controlled ovarian stimulation; rFSH = recombinant follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection; hCG = human chorionic gonadotropin. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.")
88
Hasta Alım Kriterleri1 Dahil Edilme IVF/ICSI için KOS endikasyonu
Ensure Hasta Alım Kriterleri1 Dahil Edilme IVF/ICSI için KOS endikasyonu Normal menstrüel siklus uzunluğu (24–35 gün) ≥18 ila ≤36 yaş ≤ 60 kg ağırlık (VKİ ≥18 ila ≤32 kg/m2) Hariç Bırakılma Endokrin anormali PKOS Bilinen düşük over cevabı veya cevap yokluğu OHSS öyküsü >20 bazal antral follikül 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. COS = controlled ovarian stimulation; FSH = follicle-stimulating hormone; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.
 ≥18 ila ≤36 yaş. ≤ 60 kg ağırlık (VKİ ≥18 ila ≤32 kg/m2) Hariç Bırakılma. Endokrin anormali. PKOS. Bilinen düşük over cevabı veya cevap yokluğu. OHSS öyküsü. >20 bazal antral follikül. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. COS = controlled ovarian stimulation; FSH = follicle-stimulating hormone; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.")
89
Primer Sonlanım Noktası: Oosit Sayısı1
Ensure Primer Sonlanım Noktası: Oosit Sayısı1 ELONVA™ (korifollitropin alfa) 100 µg (n=268) rFSH 150 IU/gün (n=128) Fark, ANOVA (95% CI) Elde Edilen Oosit Sayısı (SD) 13.3 (7.3) 10.6 (5.9) 2.5 (1.2–3.9) Oosit kalitesi ve MII oositlerin oranları benzerdir. . 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. rFSH = recombinant follicle-stimulating hormone; MII = metaphase II; ICSI = intracytoplasmic sperm injection. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.
 100 µg. (n=268) rFSH. 150 IU/gün. (n=128) Fark, ANOVA (95% CI) Elde Edilen Oosit Sayısı (SD) 13.3 (7.3) 10.6 (5.9) 2.5 (1.2–3.9) Oosit kalitesi ve MII oositlerin oranları benzerdir Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. rFSH = recombinant follicle-stimulating hormone; MII = metaphase II; ICSI = intracytoplasmic sperm injection. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76.")
90
Devam Eden Gebelik Oranları1
Ensure Devam Eden Gebelik Oranları1 ITT Grubu Hastalar, % 34.4 25.4 Transfer edilen embriyo sayısı: 1.8 Transfer edilen embriyo sayısı: 1.8 ELONVA™ (korifollitropin alfa) 100 µg (n=268) rFSH 150 IU/gün (n=128) 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. rFSH = recombinant follicle-stimulating hormone. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. 2. Data on file, MSD.
 100 µg (n=268) rFSH 150 IU/gün. (n=128) 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. rFSH = recombinant follicle-stimulating hormone. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒ Data on file, MSD.")
91
hCG Gününde Serum LH Düzeyleri
Ensure hCG Gününde Serum LH Düzeyleri ITT Grubu 10 ELONVA™ (korifollitropin alfa) 100 µg rFSH 150 IU/gün Serum LH Düzeyi, IU/L 5 1 3 5 8 hCG ET ET2 Günler LH = luteinizing hormone; rFSH = recombinant follicle-stimulating hormone; hCG = human chorionic gonadotropin. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. 2. Data on file, MSD.
 100 µg. rFSH 150 IU/gün. Serum LH Düzeyi, IU/L hCG. ET. ET2. Günler. LH = luteinizing hormone; rFSH = recombinant follicle-stimulating hormone; hCG = human chorionic gonadotropin. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒ Data on file, MSD.")
92
hCG Gününde Serum Progesteron Düzeyleri
Ensure hCG Gününde Serum Progesteron Düzeyleri ITT Grubu 6 1,000 ELONVA™ (korifollitropin alfa) 100 µg 900 rFSH 150 IU/gün 5 800 700 4 600 SerProgesteron Düzeyleri, nmol/L 3 500 400 2 300 200 1 100 1 3 5 8 hCG ET ET2 Günler rFSH = recombinant follicle-stimulating hormone; hCG = human chorionic gonadotropin; ET = embryo transfer. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. 2. Data on file, MSD.
 100 µg rFSH 150 IU/gün SerProgesteron Düzeyleri, nmol/L hCG. ET. ET2. Günler. rFSH = recombinant follicle-stimulating hormone; hCG = human chorionic gonadotropin; ET = embryo transfer. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒ Data on file, MSD.")
93
ELONVA® (korifollitropin alfa)
Ensure OHSS Olguları Hastalar, % OHSS Şiddeti ELONVA® (korifollitropin alfa) 100 µg (n=268) rFSH 150 IU/gün (n=129) Grade 1 (hafif) 3.4 3.1 Grade 2 (orta) 1.9 0.8 Grade 3 (ciddi) 1.5 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. OHSS = ovarian hyperstimulation syndrome. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. 2. Data on file, MSD.
 100 µg. (n=268) rFSH. 150 IU/gün. (n=129) Grade 1 (hafif) Grade 2 (orta) Grade 3 (ciddi) Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒76. OHSS = ovarian hyperstimulation syndrome. 1. Corifollitropin alfa Ensure Study Group. Reprod Biomed Online. 2010;21:66‒ Data on file, MSD.")
94
Pursue ÇalIşmasI

95
Pursue Çalışması: Tedavi Rejimleri
Araştırma Grubu Korifollitropin alfa 150 µg Plasebo rFSH (7 gün boyunca günde 300 IU) rFSH (follitropin beta) (günlük doz ≤ 300 IU) ET 3. günde 2 adet kaliteli embriyo Oosit eldesi IVF ICSI Referans Grup Plasebo Korifollitropin alfa GnRH antagonist (ganireliks, 0.25 mg/gün) 5. günden hCG gününe kadar Luteal faz desteği Crinone 8%, 90 mg/gün rFSH (follitropin beta) (7 gün boyunca günde 300 IU) rFSH (follitropin beta) (günlük doz ≤ 300 IU) Stimülasyon günü 1 (Siklus günü 2–3) günü 5 günü 8 rhCG (Ovidrel 250 µg) 3 follikül ≥ 17 mm olunca 95
 rFSH (follitropin beta) (günlük doz ≤ 300 IU) ET. 3. günde 2 adet kaliteli embriyo. Oosit eldesi. IVF. ICSI. Referans Grup. Plasebo. Korifollitropin alfa. GnRH antagonist (ganireliks, 0.25 mg/gün) 5. günden hCG gününe kadar. Luteal faz desteği. Crinone 8%, 90 mg/gün. rFSH (follitropin beta) (7 gün boyunca günde 300 IU) rFSH (follitropin beta) (günlük doz ≤ 300 IU) Stimülasyon. günü 1. (Siklus günü 2–3) günü 5. günü 8. rhCG (Ovidrel 250 µg) 3 follikül ≥ 17 mm olunca. 95.")
96
Hasta Alım Kriterleri Dahil Edilme Hariç Bırakma
IVF/ICSI için KOS endikasyonu ≥ 35 ila ≤ 42 yaş Ağırlık ≥ 50 kg, VKİ ≥ 18 ila ≤ 32 kg/m2 Normal menstrüel siklus uzunluğu (24–35 gün) Ejakülatuvar sperm varlığı Hariç Bırakma Endokrin anormali PKOS >20 bazal antral follikül (< 11 mm) Bilinen düşük over cevabı veya cevap yokluğu OHSS öyküsü FSH > 15.0 IU/L veya LH > 12.0 IU/L Sigara içme veya yakın zamanda bırakmış olma 96
 Ejakülatuvar sperm varlığı. Hariç Bırakma. Endokrin anormali. PKOS. >20 bazal antral follikül (< 11 mm) Bilinen düşük over cevabı veya cevap yokluğu. OHSS öyküsü. FSH > 15.0 IU/L veya LH > 12.0 IU/L. Sigara içme veya yakın zamanda bırakmış olma. 96.")
97
Elde Edilen Oositler Korifollitropin Alfa 150 µg rFSH 300 IU/gün Fark
ANOVA (95% CI) Teşebbüs Başına Ortalama (SD) n = 694 10.7 (7.2) n = 696 10.3 (6.8) 0.5 (–0.2 to 1.2) 97
 Teşebbüs Başına. Ortalama (SD) n = (7.2) n = (6.8) 0.5 (–0.2 to 1.2) 97.")
98
Primer Sonlanım Noktası: Devam eden Gebelik Oranları
Korifollitropin Alfa 150 µg rFSH 300 IU/gün Fark (95% CI) Siklus başına, % (n/N) 23.9 (166/694) 26.9 (187/696) –3.0 (–7.4 ila 1.4) ≤ 38 yaş 30.4 (122/401) 33.2 (134/404) > 38 yaş 15.0 (44/293) 18.2 (53/292) Embriyo transferi başına, % (n/N) 26.3 (166/632) 28.9 (187/647) –2.7 (–7.4 ila 2.0) 98
 Siklus başına, % (n/N) 23.9 (166/694) 26.9 (187/696) –3.0 (–7.4 ila 1.4) ≤ 38 yaş (122/401) 33.2 (134/404) > 38 yaş (44/293) 18.2 (53/292) Embriyo transferi başına, % (n/N) 26.3 (166/632) 28.9 (187/647) –2.7 (–7.4 ila 2.0) 98.")
99
≥ 1 Ciddi Advers Olay Yaşayan Hastalar
Korifollitropin Alfa 150 µg n = 692 rFSH 300 IU/gün n = 698 Ciddi AO , % (n) 0.4 (3) 2.6 (19) AO , % (n) 56.5 (391) 57.2 (399) İlaç ilişkili Şiddetli 20.5 (142) 2.3 (16) 18.5 (129) 3.9 (27) AO nedeniyle tedaviyi bırakma, % (n) 0.7 (5) 0.9 (6) 99
 0.4 (3) 2.6 (19) AO , % (n) 56.5 (391) 57.2 (399) İlaç ilişkili. Şiddetli (142) 2.3 (16) 18.5 (129) 3.9 (27) AO nedeniyle tedaviyi bırakma, % (n) 0.7 (5) 0.9 (6) 99.")
100
Korifollitropin Alfa 150 µg
OHSS Olguları Korifollitropin Alfa µg n = 692 rFSH 300 IU/gün n = 698 OHSS insidansı, n (%) Grade bilinmiyor 1 (0.1) Grade I (hafif) 7 (1.0) Grade II (orta) 5 (0.7) 4 (0.6) Grade III (ciddi) 6 (0.9) Total 12 (1.7) Ciddi AO olan OHSS Hospitalizasyon 2 (0.3) Grade II ve/veya III 10 (1.4) 100
 Grade bilinmiyor. 1 (0.1) Grade I (hafif) 7 (1.0) Grade II (orta) 5 (0.7) 4 (0.6) Grade III (ciddi) 6 (0.9) Total. 12 (1.7) Ciddi AO olan OHSS. Hospitalizasyon. 2 (0.3) Grade II ve/veya III. 10 (1.4) 100.")
101
Trust ÇalIşmasI

102
Trust Klinik Çalışması1
Dizayn Faz III, tekrarlayan siklus çalışması Birincil Amaç ELONVA™’nın (korifollitropin alfa) tekrarlayan KOS sikluslarında immünojenisitesinin ve güvenliliğinin gösterilmesi. Sonlanım Noktaları Korifollitropin alfaya yönelik antikor oluşumu AO ve ciddi AO’lar OHSS gelişimi Hipersensitivite Lokal tolerans 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208. COS = controlled ovarian stimulation; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.
 tekrarlayan KOS sikluslarında immünojenisitesinin ve güvenliliğinin gösterilmesi. Sonlanım Noktaları. Korifollitropin alfaya yönelik antikor oluşumu. AO ve ciddi AO’lar. OHSS gelişimi. Hipersensitivite. Lokal tolerans. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208. COS = controlled ovarian stimulation; IVF = in vitro fertilization; ICSI = intracytoplasmic sperm injection. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.")
103
Trust: 3 Siklusa Kadar Tedavi1
ELONVA™ (korifollitropin alfa) 150 µg hCG 7 gün FSH (günlük) ≤225 IU GnRH antagonist (0.25 mg/gün) 5 veya 6. günden hCG’ye kadar IVF ICSI Oosit eldesi ET (maks 3) Luteal Faz Desteği (vajinal P) Siklus Günü 2–3 = Stimülasyon Günü 1 Stimülasyon Günü 5 veya 6 Stimülasyon Günü 8 hCG 3 follikül ≥17 mm olunca 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208. 18-39 yaş, >60 kg rFSH = recombinant follicle-stimulating hormone; hCG = human chorionic gonadotropin. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.
 150 µg. hCG. 7 gün. FSH (günlük) ≤225 IU. GnRH antagonist (0.25 mg/gün) 5 veya 6. günden hCG’ye kadar. IVF. ICSI. Oosit eldesi. ET. (maks 3) Luteal Faz Desteği (vajinal P) Siklus Günü 2–3 = Stimülasyon Günü 1. Stimülasyon Günü 5 veya 6. Stimülasyon Günü 8. hCG 3 follikül ≥17 mm olunca. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒ yaş, >60 kg. rFSH = recombinant follicle-stimulating hormone; hCG = human chorionic gonadotropin. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.")
104
Antikor Testi Yapılan Hastalar Klinik Olarak Anlamlı İmmünojenisite
Trust İmmünojenisite1 ELONVA™ (korifollitropin alfa) Kullanan Hastalar Antikor Testi Yapılan Hastalar Klinik Olarak Anlamlı İmmünojenisite 1. Siklus 682 681 0.0 2. Siklus 375 372 3. Siklus 198 192 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.
 Kullanan Hastalar. Antikor Testi Yapılan Hastalar. Klinik Olarak Anlamlı İmmünojenisite. 1. Siklus Siklus Siklus Norman RJ et al. Hum Reprod. 2011;26:2200‒ Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.")
105
OHSS Olguları1 Hastalar, % WHO Kriterleri 1. siklus (n=682) 2. siklus
Trust OHSS Olguları1 Trust Hastalar, % WHO Kriterleri 1. siklus (n=682) 2. siklus (n=375) 3. siklus (n=198) Grade I (hafif) Grade II (orta) Grade III (ciddi) 1.8 0.9 0.8 0.5 0.0 Total 3.5 1.9 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208. 1. Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.
 2. siklus. (n=375) 3. siklus. (n=198) Grade I (hafif) Grade II (orta) Grade III (ciddi) Total Norman RJ et al. Hum Reprod. 2011;26:2200‒ Norman RJ et al. Hum Reprod. 2011;26:2200‒2208.")
106
RCT’lerin Metaanalizi
Corifollitropin-rFSH karşılaştırması Normal cevap veren hastalarda rFSH’ya alternatiftir MII oosit Korifollitropinde fazla 1.92 ( ) Embriyo sayısı benzer 1.36 (0.72-2) Fertilizasyon benzer Gebelik benzer OHSS OR: 1.27 ( ) Youssef MAM, Fertil Steril, 2012
 Embriyo sayısı benzer 1.36 (0.72-2) Fertilizasyon benzer. Gebelik benzer. OHSS OR: 1.27 ( ) Youssef MAM, Fertil Steril,")
109
hCG günü >17 matür oosit OHSS yi öngörebilir
Kestirim ≥ 19 follikül için Sens = 74.3% Spes = 75.2% 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 Sensitivite AUC = 0.779 n=2,439 hasta GnRH-antagonist protokolü 35 ağır OHSS (1.4%) PPD 4.1 % NPD 99.5 % MSD: checl abstract ESHRE 2012 information as reference, could the figure be redrawn? If all cases predicted at risk of severe OHSS had been cancelled or OHSS had been prevented, the incidence of OHSS can be lowered to <0.5% (=9 remaining cases) 1-Spesifisite Orta – ağır OHSS için en uygun kestirim değeri ≥17 follikül. Sensitivite=68.9% Spesifisite=66.7% AUC = PPV, 6.0% NPV, 98.6% Mannaerts et al., ESHRE oral 2012
 PPD 4.1 % NPD 99.5 % MSD: checl abstract ESHRE 2012 information as reference, could the figure be redrawn If all cases predicted at risk of severe OHSS had been cancelled or OHSS had been prevented, the incidence of OHSS can be lowered to <0.5% (=9 remaining cases) 1-Spesifisite. Orta – ağır OHSS için en uygun kestirim değeri ≥17 follikül. Sensitivite=68.9% Spesifisite=66.7% AUC = PPV, 6.0% NPV, 98.6% Mannaerts et al., ESHRE oral")
110
Beklenmedik bir aşırı cevap gelişirse..
hCG yerine GnRH agonist ile ovülasyon tetiklemesi Oosit toplamadan 1 saat sonra 1500 IU hCG ve taze embryo transferi Humaidan, Polyzos et al. Hum Reprod 2013 Tüm embriyoların dondurulması Devroey, Polyzos et al. Hum Reprod 2011

111
Kötü Cevaplı Hastada Korifollitropin
Değişken Korifollitropin n=43 Kısa GnRHa n=64 Yaş 37.9 39 Siklus iptali 14 (%32.6) 18 (%28.1) Embriyo transferi 23 (%53.5) 34 (%53.1) Siklus başına +hCG 11.7 10.9 ET başına + hCG 18.5 15.6 Siklus başına devam eden gebelik 7 6.3 ET başına devam eden gebelik 13 12 Polyzos NP, Fertil Steril, basımda
 18 (%28.1) Embriyo transferi. 23 (%53.5) 34 (%53.1) Siklus başına +hCG ET başına + hCG Siklus başına devam eden gebelik ET başına devam eden gebelik Polyzos NP, Fertil Steril, basımda.")
112
Follitropin Çalışmalarının Katkıları
Antagonist sikluslarında LH seviyeleri Progesterone artışına yol açsa da devam eden gebelik oranlarını etkilememektedir Hormon LH <25 LH 25-75 LH>75 p Stim 8. gün E2 2096 3162 3854 <0.05 P4 2.1 2.4 2.7 hCG günü 3354 4588 6092 P 3 3.2

114
YENİDOĞAN SONUÇLARI Korifollitropin (n=424) rFSH (370)
Majör malformasyon 17 (%4) 20 (%5.4) Minör malformasyon 52 (%12.3) 43 (%11.6) Tüm malformasyonlar 69 (%16.3) 63 (%17) OR 0.94 ( ) Faz II ve III çalışmalardan ek 806 canlı doğum anomali oranları benzer Bonduelle M, Hum Reprod, 2012
 20 (%5.4) Minör malformasyon. 52 (%12.3) 43 (%11.6) Tüm malformasyonlar. 69 (%16.3) 63 (%17) OR ( ) Faz II ve III çalışmalardan ek 806 canlı doğum anomali oranları benzer. Bonduelle M, Hum Reprod,")
115
ELONVA™ (korifollitropin alfa)
rFSH hCG 1 2 3 4 5 6 7 8 9 10 GnRH antagonisti COS = controlled ovarian stimulation; rFSH = recombinant follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; RCT = randomized controlled trial; IVF = in vitro fertilization; WMD = weighted mean difference. 1. ELONVA™ (corifollitropin alfa) summary of product characteristics. N.V. Organon, a subsidiary of Merck & Co., Inc.; Kolibianakis EM et al. Hum Reprod Update. 2006;12:651–671.
 summary of product characteristics. N.V. Organon, a subsidiary of Merck & Co., Inc.; Kolibianakis EM et al. Hum Reprod Update. 2006;12:651–671.")
Benzer bir sunumlar