Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
MEME KORUYUCU CERRAHİ ve CERRAHİ SINIR
Doç. Dr. Mehmet Ali Gülçelik

2
Tüm kanser cerrahisi içinde hiçbir başka yöntem Meme Koruyucu Cerrahi kadar yüksek derecede kanıt düzeyine sahip değildir. Morrow M. Expert Rev Anticancer Ther. 2008

3
TANIM Primer meme tümörünün, güvenli bir sağlam sınır sağlayacak şekilde komşu meme dokusuyla birlikte çıkartılması olarak tanımlanabilir. Lumpektomi Sektör rezeksiyonu AD/SLN+RT Kadrantektomi Lumpektomi fisher Quadrenektomi veronosi Sektör rezeksiyonu Quad-lump. Arasında Aspergen et al tarafından ortaya atılmış. İskandinav ve bazı avrupa ülkelerinde kullanılıyor. Wide rezeksiyon sektör rezeksiyonuna benzemekte

4
NEDEN MEME KORUYUCU CERRAHİ ?
Mastektomi ile eşdeğer sağkalım ve yerel yineleme oranları elde etmek koşuluyla; DAHA İYİ KOZMETİK SONUÇ

5
6 tane randomize çalışma evre 1-2, mastektomi/ mkc
RT cGy, Sadece NSABP çaşımasında boost yok

6
National cancer int çalışmasında lokal başarısızlık fazla fakat sadece gross tümör çıkartılmış,
patolojik olarak cerrahi sınır kontrol edilmemiş. EORTC %81 hasta T2 ve bunların %48 ü mikroskopik olarak pozitif. MKC sonrası lokal yineleme olan hastaların büyük kısmı salvage mastektomi ile tdv edilmiş Bunlarında 5 yıllık sağkalımı % 70 civarında Mastektomide burada görüldüğü gibi lokla yinelemede garanti bir yüntem değil, bunlarda da göğüs duvarı yinelemeside yaklaşık % 4-14

7
Her iki tip tedavide 20 yıllık genel ve hastalıksız sağ kalımda herhengi bir sağkalım farkı yok.

8
MKC de yerel yinelemelerin çoğu ipsilateral memede farklı kadranlarda oluşan yeni primer karsinomalardır. Gerçek yerel yinelemeler mastektomi grubu ile eşittir (10 vs 8). Ancak YY oranları ne olursa olsun iki gruptaki genel sağkalım ve hastalıksız sağkalım oranları eşittir. RT’e bağlı spontan kot kırıkları, geçici perikardit (sola ışın alanlar) ve memede yapı bozukluğu gibi komplikasyonların oranı (%2-5) düşüktür. Lokal nüks mastektomi %6,2 Lokal nüks MRM %5,9
 ve memede yapı bozukluğu gibi komplikasyonların oranı (%2-5) düşüktür. Lokal nüks mastektomi %6,2. Lokal nüks MRM %5,9.")
9
Yorum Randomize çalışmalar ve meta analizleri sağkalımın aynı olduğu kanıtlandığına göre, MKC grubunda ki görece yüksek yerel yinelemeler gerekçe gösterilerek meme kanserinin tedavisinde mastektominin standart tedavi yaklaşımı olması gerektiği ileri sürülemez.

10
MKC Ölçülebilir Sonuçları
Sağkalım Yerel yineleme Kozmezis Hasta tatmini (Yaşam kalitesi)
")
11
MKC / MASTEKTOMİ Sağkalım aynıdır
Yerel yineleme oranları kabul edilebilir orandadır Hayat kalitesinde artış Al-Ghazal et al. Eur J Cancer 2000; 36: 1938–43. Moyer A. Health Psychol 1997; 16: 284–98. Pusic A et al. Plast Reconstr Surg 1999; 104: 1325–33. Vücut imajını algılamada üstünlük Curran D et al. Eur J Cancer 1998; 34: 307–14. Arora NK et al. Cancer 2001; 92: 1288–98. Janni W et al Ann Surg Oncol 2001; 8: 542–8. Rowland JH et al. J Natl Cancer Inst 2000; 92: 1422–9.

12
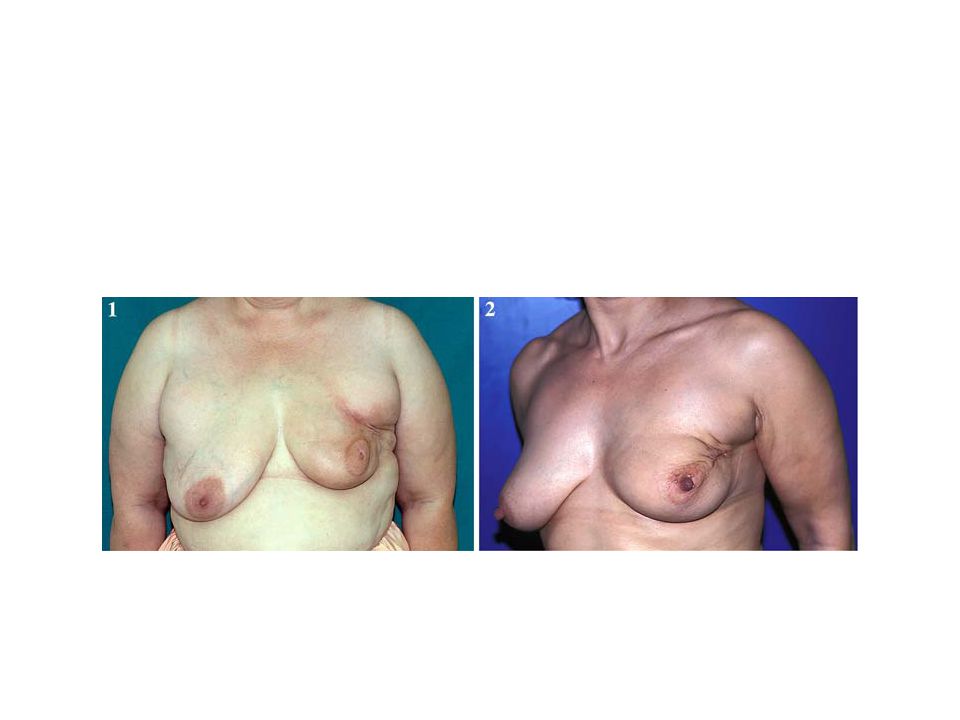
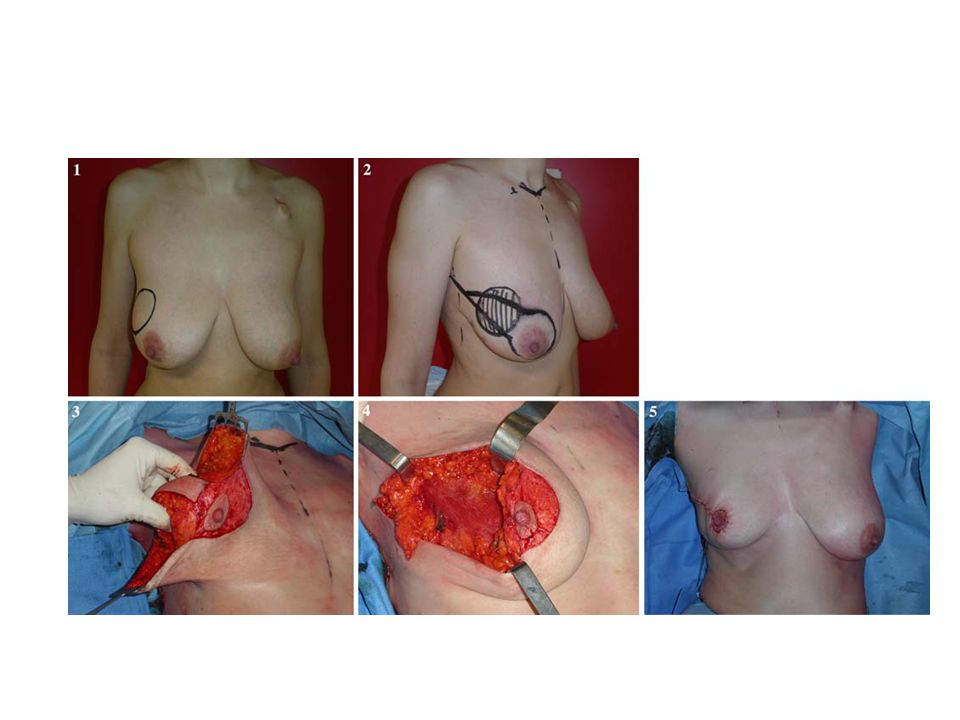
MKC SONRASI KOZMEZİS MKC’nin ana kuralı onkolojik prensiplerden taviz verilmeden en iyi kozmetik sonucun elde edilmesidir.

16
MKC SONRASI KOZMEZİS Meme koruyucu cerrahi sonrası deformitelerin büyük kısmının skar kontraktürü ve lokal glandüler defekt nedeniyle olduğu bilinmektedir. Cerrahi işlem yüzeyel skar ve volüm defektlerine Radyoterapi meme dokusu içerisinde telenjektazi ve fibrotik değişikliğe neden olur.

17
Hasta Seçimi ve Değerlendirme
Öykü ve fizik muayene Mammografi Spesmenden (biyopsi) elde edilen histolojik parametreler Hastanın istem ve beklentileri
 elde edilen histolojik parametreler. Hastanın istem ve beklentileri.")
18
Öykü RT alıp almadığı Kollajen vasküler hastalık İmplant varlığı
Gebelik Metastaz düşündüren semptom

19
Fizik muayene Tümör çapı ve lokalizasyonu Cilt fiksasyonu
Tümör /meme oranı Multipl tümör olasılığı Aksiller ve supraklaviküler nodal durum Lokal ileri tümör bulgusu Meme başı değişikliği Karşı meme ve aksillanın değerlendirilmesi

20
Mammografi Hastalığın yaygınlığı Karşı memenin değerlendirilmesi
Tümör çapı ölçümü, Multisentrisite ve multifokalite mamografi ve usg ile hastaların %95 nin MKC ye uygunluğu saptanabilir.* Multisentrisite ve multifokalite açısından MRG yararlı; standardizasyon problemi yüksek yalancı pozitiflik saptanan lezyonların biyopsisindeki zorluklar nedeniyle seçilmiş olgularda kullanılabilir *Morrow M et al.Surgery 2002; 118:621-26

21
Meme Kanserinde MRG Potansiyel Faydaları
MKC seçiminde gelişme MKC’den mastektomiye geçişte Tümör yaygınlıgını tespitte gelişme reeksizyon oranında Senkron kontralateral meme tümörü tespiti Lokal nüksde azalma

22
MRG planlanmamış mastektomi oranını azaltmakta mı?
% MKC Mastektomi Yazar sayı MRG(-) MRG(+) p Bleicher, 2008 290 5.9 3.8 NS Penzel, 2008 355 5.1 3.5
 MRG(+) p. Bleicher, NS. Penzel,")
23
MRG pozitif cerrahi sınır oranını azaltmakta mı?
% Pozitif sınır Yazar sayı MRG (-) MRG (+) p Bleicher, 2008 290 24 22 NS Penzel, 2008 355 19 14 Schiller, 2008 730 18 Hwang, 2009 472 12
 MRG (+) p. Bleicher, NS. Penzel, Schiller, Hwang,")
24
BU KONULAR HAKKINDA HASTA BİLGİLENDİRİLMELİ
Hastanın tercihi Uzak sağkalım Yerel yineleme olasılığı ve neye yol açacağı Kozmetik sonuç, seksüel uyum, ve fonksiyonel sonuçlar BU KONULAR HAKKINDA HASTA BİLGİLENDİRİLMELİ

25
Karara yardımcı yöntemler
Hastaların tedavi seçeneklerini değerlendirmesi ve hasta hekim ilişkisini standardize etmede önemli katkıları olduğu kabul edilmektedir. 2007 yılında 123 çalışmayı kapsayan bir meta analiz yayınlandı* Karar ve yardımcı yöntemi kullananlarda diğerlerine kıyasla %25 daha fazla MKC tercihi (RR 1.25; %95 CI ) Ortaya konmuştur *Waliee J.F. Et al. J Clin Oncol (9); Decision aids and breast cancer: do they influence choice for surgery and knowledge of treatment options? Waljee JF, Rogers MA, Alderman AK. Section of General Surgery and Section of Plastic Surgery, Department of Surgery, University of Michigan, Ann Arbor, MI, USA. PURPOSE: To describe the effect of decision aids on the choice for surgery and knowledge of surgical therapy among women with early-stage breast cancer. METHODS: A systematic review was conducted between years 1966 to 2006 of all studies designed to assess the effect of decision aids on surgical therapy. MEDLINE, EMBASE, Cumulative Index to Nursing and Allied Health (CINAHL), the Cochrane Network, HAPI databases, and bibliographies were searched. Of the 123 studies screened, 11 studies met criteria. Meta-analyses were performed to assess the pooled relative risk for surgical choice and the pooled mean difference in patient knowledge. RESULTS: Results from randomized controlled trials indicated that women who used a decision aid were 25% more likely to choose breast-conserving surgery over mastectomy (risk ratio, 1.25; 95% CI, 1.11 to 1.40). Decision aids significantly increased patient knowledge by 24% (P = .024). The data also suggested that decision aids decreased decisional conflict and increased satisfaction with the decision-making process. Decision aids were well received by surgeons and patients, facilitated patients' desire for shared decision making, and were feasible to implement into practice. CONCLUSION: Decision aids are important adjuncts for counseling women with early-stage breast cancer. Their use increases the likelihood that women will choose breast-conserving surgery, and enhances patient knowledge of treatment options.
 Ortaya konmuştur. *Waliee J.F. Et al. J Clin Oncol (9); Decision aids and breast cancer: do they influence choice for surgery and knowledge of treatment options Waljee JF, Rogers MA, Alderman AK. Section of General Surgery and Section of Plastic Surgery, Department of Surgery, University of Michigan, Ann Arbor, MI, USA. PURPOSE: To describe the effect of decision aids on the choice for surgery and knowledge of surgical therapy among women with early-stage breast cancer. METHODS: A systematic review was conducted between years 1966 to 2006 of all studies designed to assess the effect of decision aids on surgical therapy. MEDLINE, EMBASE, Cumulative Index to Nursing and Allied Health (CINAHL), the Cochrane Network, HAPI databases, and bibliographies were searched. Of the 123 studies screened, 11 studies met criteria. Meta-analyses were performed to assess the pooled relative risk for surgical choice and the pooled mean difference in patient knowledge. RESULTS: Results from randomized controlled trials indicated that women who used a decision aid were 25% more likely to choose breast-conserving surgery over mastectomy (risk ratio, 1.25; 95% CI, 1.11 to 1.40). Decision aids significantly increased patient knowledge by 24% (P = .024). The data also suggested that decision aids decreased decisional conflict and increased satisfaction with the decision-making process. Decision aids were well received by surgeons and patients, facilitated patients desire for shared decision making, and were feasible to implement into practice. CONCLUSION: Decision aids are important adjuncts for counseling women with early-stage breast cancer. Their use increases the likelihood that women will choose breast-conserving surgery, and enhances patient knowledge of treatment options.")
26
Tedavi Seçimini Etkileyebilecek Patolojik Özellikler
Sub tipler arasında fark yok Histolojik tip Grad Tümör nekrozu LVI Nodal durum EIK Yüksek gradda YY artıyor ancak yeterli kanıt yok 5 yılda YY risk artışı %10-15 MST aksine MKC+RT’de nod(+) hastalarda YY farkı yok
 hastalarda YY farkı yok.")
27
EİK EIK erken evre meme kanserlerinin yaklaşık %20 sinde görülür.
10 yılda % oranında memede YY’e yol açabilir. Ancak bunlar arasında negatif cerrahi sınır sağlanırsa bu oranlar düşmektedir Bu nedenle (-) CS elde edilebiliyorsa MKC kontrendike değildir Tümör kitlesinin ve komşu meme dokusunun %25 ve daha fazla intraduktal karsinoma içermesi
 CS elde edilebiliyorsa MKC kontrendike değildir. Tümör kitlesinin ve komşu meme dokusunun %25 ve daha fazla intraduktal karsinoma içermesi.")
28
Mutlak Kontrendikasyonlar
Multisentrisite Gebelik Göğüs bölgesine daha önce uygulanmış RT İnatçı CS (+) liği
 liği.")
29
Cerrahi sınır <2 cm.lik tümörde 2-cm.lik marjinde %26 intraduktal,
%12 invaziv, <2 cm.lik tümörde 2-4 cm.lik marjinde %5 intraduktal, %5 invaziv kanser, <4cm.lik tümörde 2-cm.lik marjinde %28 intraduktal, %14 invaziv, <4cm.lik tümörde 2-4-cm.lik marjinde %4 intraduktal, %7 invaziv kanser saptanır. Residüel odakların %53’ü 2-cm.lik marjinde bulunur. Holland R. Cancer 56; , 1985. Vaidya JS. Br J Cancer 74; 820-4, 1996.

30
Negatif cerrahi sınır memede rezüdü tümör olmadığı anlamına gelmez
Multifocality of “Localized” Breast Cancer NSABP B06 4 cm 2 cm 43% 20% NSABP cerrahi sınırı boyada tümör olmaması olarak European institute of oncology 1mm olarak kabul ediyor. 1999 peterson et al. focal mikroskopik pozitiflik(1 veya 2 fokal mikroskopik pozitiflik) CS negatif olanlar la aynı. Cancer Sep 1;56(5): Links Histologic multifocality of Tis, T1-2 breast carcinomas. Implications for clinical trials of breast-conserving surgery. Holland R, Veling SH, Mravunac M, Hendriks JH. Breast cancer multifocality was studied in mastectomy specimens by correlated specimen radiography and histologic techniques. The patients chosen for study were comparable to those eligible for breast-conserving surgical therapy. Two study groups, one with 282 invasive cancers (T1-2) and the other with 32 intraductal cancers, were selected from a group of 399 consecutive cases by omitting patients who were clearly, or very probably, not candidates for breast-conserving surgical therapy according to current trial criteria. Omitted patients included those with clinically and/or radiologically multifocal cancers and patients with tumor extension into the chest wall or skin (7%). Also excluded were the so-called diffuse invasive cancers (8%), the clinically and radiologically occult tumors (3%), and the invasive cancers larger than 5 cm (3%). Of the 282 invasive cancers, 105 (37%) showed no tumor foci in the mastectomy specimen around the reference mass. In 56 (20%) tumor foci were present within 2 cm, and in 121 (43%) tumor was found more than 2 cm from the reference tumor. In 75 (27%) the tumor foci beyond 2 cm were histologically noninvasive cancers, and in 46 cases (16%) they contained invasive cancers as well. A comparison between the group with reference tumors less than 2 cm and the group with reference tumors more than 2 cm in size showed no significant difference between the groups in terms of presence or absence of tumor foci or distance of tumor foci from the reference tumor. If the 264 invasive cancers in this series that were 4 cm or less in diameter had been removed with a margin of 3 to 4 cm, 7% to 9% of the patients would have had invasive cancer left in the remaining breast tissue, and 4% to 9% would have had foci of noninvasive cancer left in the remaining breast tissue. On the basis of the data on the distribution of tumor at different distances from the reference tumor, the current study estimates the expected rates of local recurrences after breast-conserving surgical procedures relative to the extensiveness of the excision. The possible impact of postoperative local radiation therapy on the rates of expected local recurrence is discussed. Cumulative Incidence of Recurrence (%) %37 Years after Surgery Holland, 1985 Fisher B, NEJM 2002;347:1233
 CS negatif olanlar la aynı. Cancer Sep 1;56(5): Links. Histologic multifocality of Tis, T1-2 breast carcinomas. Implications for clinical trials of breast-conserving surgery. Holland R, Veling SH, Mravunac M, Hendriks JH. Breast cancer multifocality was studied in mastectomy specimens by correlated specimen radiography and histologic techniques. The patients chosen for study were comparable to those eligible for breast-conserving surgical therapy. Two study groups, one with 282 invasive cancers (T1-2) and the other with 32 intraductal cancers, were selected from a group of 399 consecutive cases by omitting patients who were clearly, or very probably, not candidates for breast-conserving surgical therapy according to current trial criteria. Omitted patients included those with clinically and/or radiologically multifocal cancers and patients with tumor extension into the chest wall or skin (7%). Also excluded were the so-called diffuse invasive cancers (8%), the clinically and radiologically occult tumors (3%), and the invasive cancers larger than 5 cm (3%). Of the 282 invasive cancers, 105 (37%) showed no tumor foci in the mastectomy specimen around the reference mass. In 56 (20%) tumor foci were present within 2 cm, and in 121 (43%) tumor was found more than 2 cm from the reference tumor. In 75 (27%) the tumor foci beyond 2 cm were histologically noninvasive cancers, and in 46 cases (16%) they contained invasive cancers as well. A comparison between the group with reference tumors less than 2 cm and the group with reference tumors more than 2 cm in size showed no significant difference between the groups in terms of presence or absence of tumor foci or distance of tumor foci from the reference tumor. If the 264 invasive cancers in this series that were 4 cm or less in diameter had been removed with a margin of 3 to 4 cm, 7% to 9% of the patients would have had invasive cancer left in the remaining breast tissue, and 4% to 9% would have had foci of noninvasive cancer left in the remaining breast tissue. On the basis of the data on the distribution of tumor at different distances from the reference tumor, the current study estimates the expected rates of local recurrences after breast-conserving surgical procedures relative to the extensiveness of the excision. The possible impact of postoperative local radiation therapy on the rates of expected local recurrence is discussed. Cumulative Incidence of. Recurrence (%) %37. Years after Surgery. Holland, Fisher B, NEJM 2002;347:1233.")
31
Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Early Breast Cancer Trialist’ Collaborative Group (EBCTCG) Lancet 2005; 366: Bu çalışmalar göstermektedir ki RT lokal nüksü %70 oranında azaltmakta Tek kollu prospektif bir çalışmada joint center for radiation therapy; pT1N0, EIC yok, LVI yok, marjin en az 1 cm 86 ay takip lokal rekürens %23 (Lim M, Nixon AJ, Gelman R, et al. A prospective study of conservative surgery alone without radiotherapy in selected patients with stage 1 breast cancer . Breast Cancer Res Treat 1999;57:34.) EBCTCG Update in 2006
 EBCTCG Update in")
32
Çalışma Hasta sayısı Takip yıl RT (+) (% yineleme) RT (-) NSABP B-06 1140 12 10 35 Milano III 576 5.4 21.7 Uppsala Breast Cancer Study Group 371 8 8.5 24 Ontario Cancer Institute 837 11 Scottish Cancer Trial 585 5.8 24.5

34
Yeterli Cerrahi sınır? NSABP cerrahi sınırı boyada tümör olmaması
%46 %35 %35 %30 %28 NSABP cerrahi sınırı boyada tümör olmaması European institute of oncology 1mm Taghian Ann Surg 2005 Morrow, 2007

35
Cerrahi sınır ölçümünde kesin kurallar yoktur
örneklemede, standart teknik yok J Am Coll Surg Apr;204(4): Links Perpendicular inked versus tangential shaved margins in breast-conserving surgery: does the method matter? Wright MJ, Park J, Fey JV, Park A, O'Neill A, Tan LK, Borgen PI, Cody HS 3rd, Van Zee KJ, King TA. Breast Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, NY, USA. BACKGROUND: In breast-conserving surgery (BCS), the method of margin assessment and the definition of a negative margin vary widely. The purpose of this study was to compare the incidence of positive margins and rates of reexcision between two methods of margin assessment at a single institution. STUDY DESIGN: In July 2004, our protocol for margin evaluation changed from perpendicular inked margins (Group A, n=263) to tangential shaved margins (Group B, n=261). In Group A, margins were classified as positive, close, and negative. Margins designated as "close" were further defined as: < or = 1 mm, < or = 2 mm, and < or =3 mm. In Group B, shaved margins (by definition 2 to 3 mm) were reported as positive or negative. RESULTS: The rate of reported "positive" margins was significantly higher in Group B: 127 of 261 (49%) versus 42 of 263 (16%), p < But when patients with "positive, close, or both" kinds of margins were combined in Group A, there was no significant difference between the two techniques. Although the shaved margin was 2- to 3-mm thick, the rate of reexcision in Group B was significantly higher when compared with that in patients with "positive, close, or both" < or =3 mm margins in Group A (75% versus 52%, p < 0.001). The likelihood of finding residual disease remained the same (27% versus 32%, p=NS). CONCLUSIONS: The tangential shaved-margin technique results in a higher proportion of reported positive margins and limits the ability of the surgeon to discriminate among patients with close margins, resulting in a higher rate of reexcision. The fact that many, but not all, patients with positive or close margins in both groups underwent reexcision emphasizes the role of surgical judgment in this setting. Longer followup is required to determine equivalency in rates of local recurrence between these two methods of margin assessment. PMID: [PubMed - indexed for MEDLINE] Traşlanmış n = 261 % 49 pozitif boyalı n = 263 % 16 pozitif Wright MJ, JACS 2007;204:541
: Links. Perpendicular inked versus tangential shaved margins in breast-conserving surgery: does the method matter Wright MJ, Park J, Fey JV, Park A, O Neill A, Tan LK, Borgen PI, Cody HS 3rd, Van Zee KJ, King TA. Breast Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, NY, USA. BACKGROUND: In breast-conserving surgery (BCS), the method of margin assessment and the definition of a negative margin vary widely. The purpose of this study was to compare the incidence of positive margins and rates of reexcision between two methods of margin assessment at a single institution. STUDY DESIGN: In July 2004, our protocol for margin evaluation changed from perpendicular inked margins (Group A, n=263) to tangential shaved margins (Group B, n=261). In Group A, margins were classified as positive, close, and negative. Margins designated as close were further defined as: < or = 1 mm, < or = 2 mm, and < or =3 mm. In Group B, shaved margins (by definition 2 to 3 mm) were reported as positive or negative. RESULTS: The rate of reported positive margins was significantly higher in Group B: 127 of 261 (49%) versus 42 of 263 (16%), p < But when patients with positive, close, or both kinds of margins were combined in Group A, there was no significant difference between the two techniques. Although the shaved margin was 2- to 3-mm thick, the rate of reexcision in Group B was significantly higher when compared with that in patients with positive, close, or both < or =3 mm margins in Group A (75% versus 52%, p < 0.001). The likelihood of finding residual disease remained the same (27% versus 32%, p=NS). CONCLUSIONS: The tangential shaved-margin technique results in a higher proportion of reported positive margins and limits the ability of the surgeon to discriminate among patients with close margins, resulting in a higher rate of reexcision. The fact that many, but not all, patients with positive or close margins in both groups underwent reexcision emphasizes the role of surgical judgment in this setting. Longer followup is required to determine equivalency in rates of local recurrence between these two methods of margin assessment. PMID: [PubMed - indexed for MEDLINE] Traşlanmış. n = 261. % 49 pozitif. boyalı n = 263. % 16 pozitif. Wright MJ, JACS 2007;204:541.")
36
Bütün sınırlar eşit değildir
Anterior sınır < 1mm Posterior sınır < 1mm

37
Negative Margins: Factors to Consider
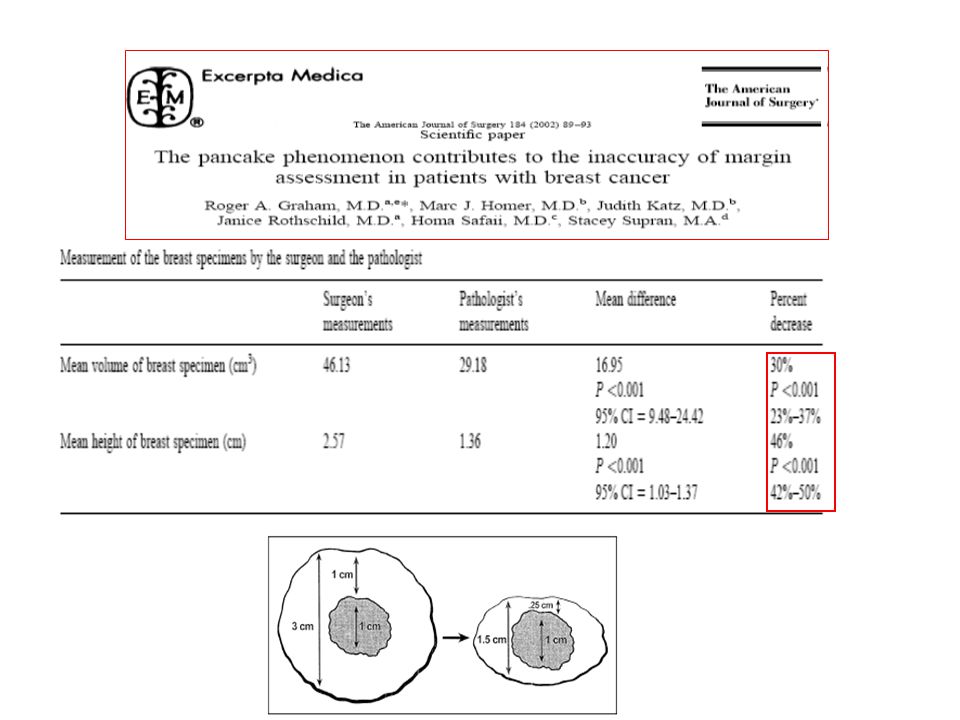
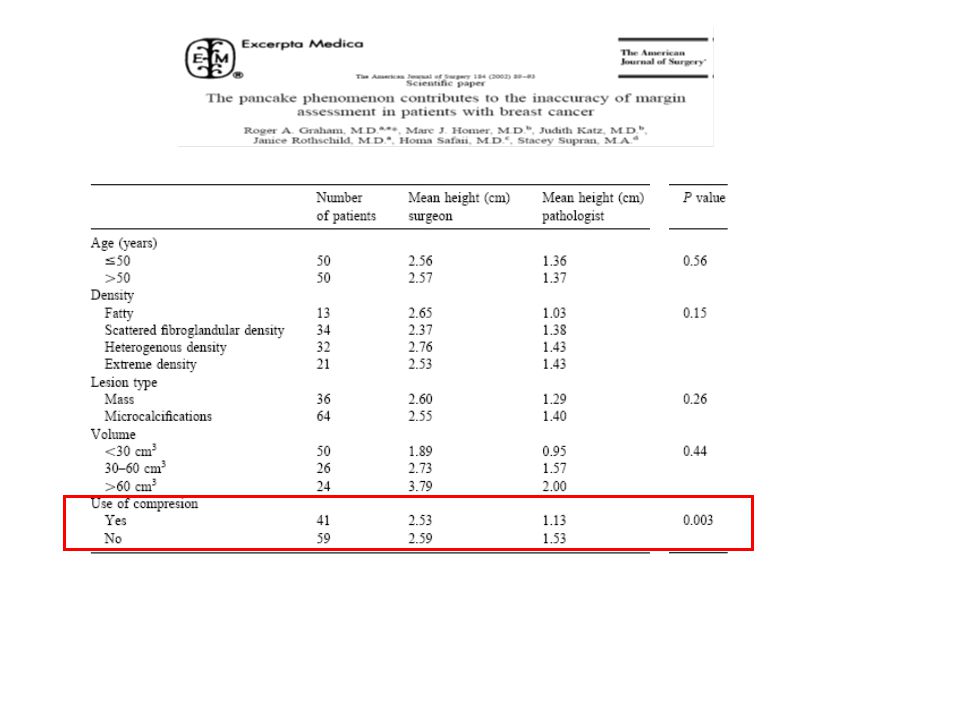
Specimen processing makes anterior and posterior margin distances irrelevant n = 100 Mean Height (cm) By surgeon 2.6 ( ) By pathologist 1.4 ( ) Independent of age, lesion type, breast density Compression devices ▲54% vs ▲41% without (p = .003) ▲46% BACKGROUND: To determine the effect on margin evaluation for patients with breast cancer, we prospectively quantified the "flattening" of the breast specimen after surgical removal. METHODS: The volume and height of 100 consecutive breast biopsy specimens were recorded independently by the operating surgeon and the pathologist. Five factors were analyzed that were thought to contribute to changes in specimen dimensions: patient age, breast tissue density, mammographic lesion type, specimen size, and the use of compression during specimen radiography. RESULTS: After surgical removal, mean volume and height of the breast specimens decreased from 46 cm(3) to 29 cm(3) (30%) and from 2.6 cm to 1.4 cm (46%), respectively. Flattening of the breast specimens occurred in all subgroups studied. CONCLUSIONS: Breast specimens are flattened after surgical removal, losing almost 50% of their original height. This "pancake" phenomenon has important implications for the accuracy of margin analysis. Graham RA, Am J Surg 2002;184:89
 By surgeon 2.6 ( ) By pathologist 1.4 ( ) Independent of age, lesion type, breast density. Compression devices ▲54% vs ▲41% without (p = .003) ▲46% BACKGROUND: To determine the effect on margin evaluation for patients with breast cancer, we prospectively quantified the flattening of the breast specimen after surgical removal. METHODS: The volume and height of 100 consecutive breast biopsy specimens were recorded independently by the operating surgeon and the pathologist. Five factors were analyzed that were thought to contribute to changes in specimen dimensions: patient age, breast tissue density, mammographic lesion type, specimen size, and the use of compression during specimen radiography. RESULTS: After surgical removal, mean volume and height of the breast specimens decreased from 46 cm(3) to 29 cm(3) (30%) and from 2.6 cm to 1.4 cm (46%), respectively. Flattening of the breast specimens occurred in all subgroups studied. CONCLUSIONS: Breast specimens are flattened after surgical removal, losing almost 50% of their original height. This pancake phenomenon has important implications for the accuracy of margin analysis. Graham RA, Am J Surg 2002;184:89.")
40
Negatif cerrahi sınırın önemi
CS (# çalışma) Hasta sayısı Ort. Takip ay Lokal yineleme (-) (+) Pos:neg (9) 5138 91 5.6 15.8 >1 mm (5) 1375 82 2.6 17.4 >2 mm (8) 5282 92 5.3 11.9 % Singletary E, 2002
 Hasta. sayısı. Ort. Takip. ay. Lokal yineleme. (-) (+) Pos:neg (9) >1 mm (5) >2 mm (8) % Singletary E,")
41
Yakın cerrahi sınır önemli mi?
% İMTN Yazar n takip yıl Neg Yakın 1mm Park 340 8y 7 Gage 5y 2 3 2mm Touboul 438 10y 6 Obedian 984 10 Freedman 1262 12 Wazer 234 3mm Pittinger 161 4y Int J Radiat Oncol Biol Phys Jul 15;44(5): Freedman G A negative margin (> 2 mm) identifies patients with a very low risk of IBTR (7% at 10 years) after conservative surgery and radiation. Patients with a close margin (< or = 2 mm) are at an equal or greater risk of IBTR as with a positive margin, especially following a reexcision. A margin involved by DCIS or invasive tumor has the same increased risk of IBTR. A reexcision of an initially close or positive margin that results in a negative final margin reduces the risk of IBTR to that of an initially negative margin. A close or positive margin is associated with an increased risk of IBTR even in patients who are EIC-negative or receiving higher boost doses of radiation. The median time to IBTR is delayed; however, the CI is not significantly decreased by adjuvant systemic therapy in patients with close or positive margins-the 5 year results in these patients underestimate their ultimate risk of recurrence. Importance of margin status in outcome of breast-conserving surgery for carcinoma. Pittinger TP, Maronian NC, Poulter CA, Peacock JL. Department of Surgery, University of Rochester School of Medicine and Dentistry, N.Y. BACKGROUND. The importance of margin status in breast-conserving therapy (BCT) for breast cancer remains unclear. We reviewed our experience with BCT to determine the risk of local recurrence as a function of margin status. METHODS. Stages I and II breast cancers treated with BCT between 1985 and 1990 were reviewed. Two hundred eleven patients were classified based on initial margin status: negative (more than 3 mm), close (3 mm or less), positive, or unknown. The incidence of reexcision and residual tumor is reported in each group. Patients with 36 months or more of follow-up (n = 183) were also stratified by final margin to examine rates of local recurrence and distant recurrence. RESULTS. Residual carcinoma was found in 0%, 24%, 44%, and 48% of the negative, close, positive, and unknown initial margin groups, respectively. The local recurrence rate was equivalent by Fisher exact test in patients with negative and close final margins (3%). The negative and close groups were not different by chi-squared analysis in terms of T stage, estrogen receptor status, and nodal status. CONCLUSIONS. Although one fourth of patients with close margins have residual tumor, recurrence rates are similar to those with negative margins. Reexcision of close margins is not necessary in patients who undergo BCT for carcinoma
: Freedman G. A negative margin (> 2 mm) identifies patients with a very low risk of IBTR (7% at 10 years) after conservative surgery and radiation. Patients with a close margin (< or = 2 mm) are at an equal or greater risk of IBTR as with a positive margin, especially following a reexcision. A margin involved by DCIS or invasive tumor has the same increased risk of IBTR. A reexcision of an initially close or positive margin that results in a negative final margin reduces the risk of IBTR to that of an initially negative margin. A close or positive margin is associated with an increased risk of IBTR even in patients who are EIC-negative or receiving higher boost doses of radiation. The median time to IBTR is delayed; however, the CI is not significantly decreased by adjuvant systemic therapy in patients with close or positive margins-the 5 year results in these patients underestimate their ultimate risk of recurrence. Importance of margin status in outcome of breast-conserving surgery for carcinoma. Pittinger TP, Maronian NC, Poulter CA, Peacock JL. Department of Surgery, University of Rochester School of Medicine and Dentistry, N.Y. BACKGROUND. The importance of margin status in breast-conserving therapy (BCT) for breast cancer remains unclear. We reviewed our experience with BCT to determine the risk of local recurrence as a function of margin status. METHODS. Stages I and II breast cancers treated with BCT between 1985 and 1990 were reviewed. Two hundred eleven patients were classified based on initial margin status: negative (more than 3 mm), close (3 mm or less), positive, or unknown. The incidence of reexcision and residual tumor is reported in each group. Patients with 36 months or more of follow-up (n = 183) were also stratified by final margin to examine rates of local recurrence and distant recurrence. RESULTS. Residual carcinoma was found in 0%, 24%, 44%, and 48% of the negative, close, positive, and unknown initial margin groups, respectively. The local recurrence rate was equivalent by Fisher exact test in patients with negative and close final margins (3%). The negative and close groups were not different by chi-squared analysis in terms of T stage, estrogen receptor status, and nodal status. CONCLUSIONS. Although one fourth of patients with close margins have residual tumor, recurrence rates are similar to those with negative margins. Reexcision of close margins is not necessary in patients who undergo BCT for carcinoma.")
42
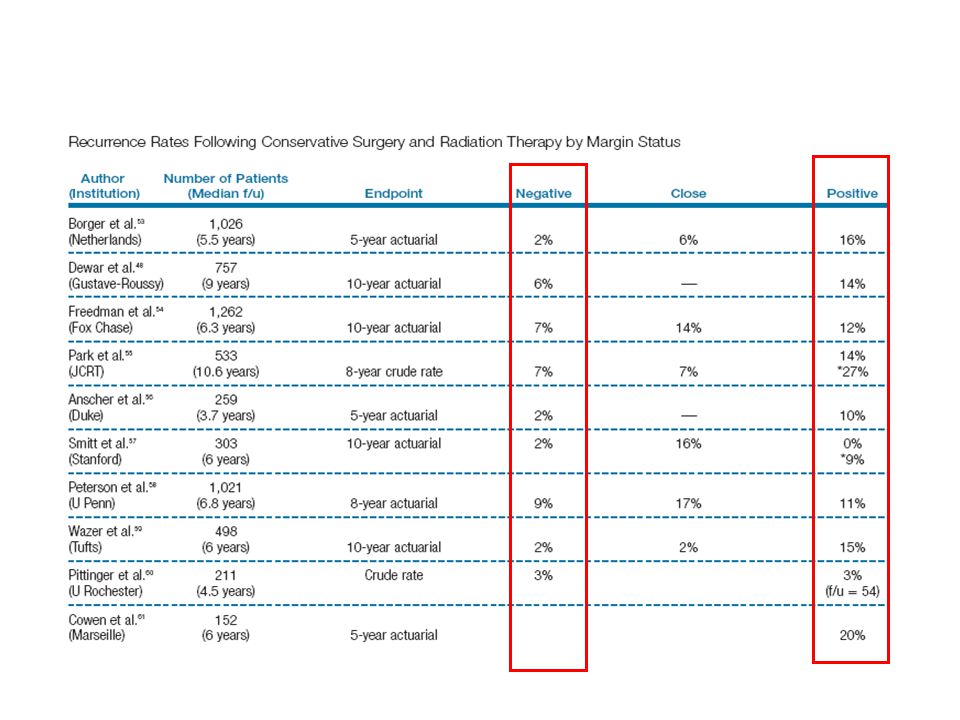
Sayı Sonlanım Negatif Yakın Pozitif
Borger et al 1,026 5y %2 %5 %16 Dewar et al 757 10y %6 %8 Anscher et al 259 Santiago et al 937 %9 %25 Wazer et al 498 %15 Pittinger et al 211 %3 Haffty, Obedian 984 %18 Yakın cerrahi daha çok öncelik KT tedavisi verilip RT geciktirilenlerde önemli Wazer, smith, freedman makalelerinde 2mm ve yakın cerrahi sınır: Lokal nüksler yakın ve pozitif ile aynı, Wazerin 6 yıl sonraki başka çalışmasında yakın ve negatif cerrahi sınır arasında fark yok Santiago, CS 2mm yakın negatif fark yok Smitt, CS 2mm yakın negatif fark yok Anscher, boyada tm var yok Park 1mm , yakın negatif fark yok

43
Hasta sayısı Süre (ay) Lokal nüks Negatif Pozitif
%3 %5 %2

44
Cerrahi sınır (+) CS kabul edilemez (2-3 kat daha fazla YY) *
Cerrahi sınır (-) 5 yıllık YY %2-6 Cerrahi sınır (+) 5 yıllık YY %11-26 Cerrahi sınır yakın 5 yıllık YY %2-8 Tümörün sağlam sınıra mesafesi konusunda görüş birliği yok 34 çalışmada 1,2,3 veya 5 mm verilmiş 1 mm, 2 mm, 3mm ve “mikroskopik” CS (-)’ lerde YY farkı yok* Singletary E. Advanced Therapy of Breast Disease 2nd Edition Singletary E. Am J Surg, 2002 Luini A, Breast CancerRes Treat, 2009
 5 yıllık YY %2-6. Cerrahi sınır (+) 5 yıllık YY % Cerrahi sınır yakın 5 yıllık YY %2-8. Tümörün sağlam sınıra mesafesi konusunda görüş birliği yok. 34 çalışmada 1,2,3 veya 5 mm verilmiş. 1 mm, 2 mm, 3mm ve mikroskopik CS (-)’ lerde YY farkı yok* Singletary E. Advanced Therapy of Breast Disease 2nd Edition. Singletary E. Am J Surg, Luini A, Breast CancerRes Treat,")
45
Yerel Yineleme Cerrahi sınır Tümör biyolojisi Tedavi

46
Tümör biyolojisi ve Yerel Yineleme
% 5-yıl LR 95% CI ER/PR Pos, HER2 Neg 0.8 ER/PR Pos, HER2 Pos 1.5 0.2-10 ER/PR Neg, HER2 Pos* 8.4 2.2-30 ER/PR Neg, HER2 Neg 7.1 J Clin Oncol May 10;26(14): Epub 2008 Apr 14. Links Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. Nguyen PL, Taghian AG, Katz MS, Niemierko A, Abi Raad RF, Boon WL, Bellon JR, Wong JS, Smith BL, Harris JR. Department of Radiation Oncology, Massachusetts General Hospital, Boston, MA, USA. PURPOSE: To determine whether breast cancer subtype is associated with outcome after breast-conserving therapy (BCT) consisting of lumpectomy and radiation therapy. PATIENTS AND METHODS: We studied 793 consecutive patients with invasive breast cancer who received BCT from July 1998 to December Among them, 97% had pathologically negative margins of resection, and 90% received adjuvant systemic therapy. No patient received adjuvant trastuzumab. Receptor status was used to approximate subtype: estrogen receptor (ER) or progesterone receptor (PR) positive and human epidermal growth factor receptor 2 negative = luminal A; ER+ or PR+ and HER-2+ = luminal B; ER-and PR -and HER-2+ = HER-2; and ER-and PR -and HER-2-= basal. Competing risks methodology was used to analyze time to local recurrence and distant metastases. RESULTS: Median follow-up was 70 months. The overall 5-year cumulative incidence of local recurrence was 1.8% (95% CI, 1.0 to 3.1); 0.8% (0.3, 2.2) for luminal A, 1.5% (0.2, 10) for luminal B, 8.4% (2.2, 30) for HER-2, and 7.1% (3.0, 16) for basal. On multivariable analysis (MVA) with luminal A as baseline, HER-2 (adjusted hazard ratio [AHR] = 9.2; 95% CI, 1.6 to 51; P = .012) and basal (AHR = 7.1; 95% CI, 1.6 to 31; P = .009) subtypes were associated with increased local recurrence. On MVA, luminal B (AHR = 2.9; 95% CI, 1.3 to 6.5; P = .007) and basal (AHR = 2.3; 95% CI, 1.1 to 5.2; P = .035) were associated with increased distant metastases. CONCLUSION: Overall, the 5-year local recurrence rate after BCT was low, but varied by subtype as approximated using ER, PR, and HER-2 status. Local recurrence was particularly low for the luminal A subtype, but was less than 10% at 5 years for all subtypes. Although further follow-up is needed, these results may be useful in counseling patients about their anticipated outcome after BCT. *Adjuvan trastuzumab almamış Nguyen PL. JCO 2008;26;2373.
: Epub 2008 Apr 14. Links. Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence after breast-conserving therapy. Nguyen PL, Taghian AG, Katz MS, Niemierko A, Abi Raad RF, Boon WL, Bellon JR, Wong JS, Smith BL, Harris JR. Department of Radiation Oncology, Massachusetts General Hospital, Boston, MA, USA. PURPOSE: To determine whether breast cancer subtype is associated with outcome after breast-conserving therapy (BCT) consisting of lumpectomy and radiation therapy. PATIENTS AND METHODS: We studied 793 consecutive patients with invasive breast cancer who received BCT from July 1998 to December Among them, 97% had pathologically negative margins of resection, and 90% received adjuvant systemic therapy. No patient received adjuvant trastuzumab. Receptor status was used to approximate subtype: estrogen receptor (ER) or progesterone receptor (PR) positive and human epidermal growth factor receptor 2 negative = luminal A; ER+ or PR+ and HER-2+ = luminal B; ER-and PR -and HER-2+ = HER-2; and ER-and PR -and HER-2-= basal. Competing risks methodology was used to analyze time to local recurrence and distant metastases. RESULTS: Median follow-up was 70 months. The overall 5-year cumulative incidence of local recurrence was 1.8% (95% CI, 1.0 to 3.1); 0.8% (0.3, 2.2) for luminal A, 1.5% (0.2, 10) for luminal B, 8.4% (2.2, 30) for HER-2, and 7.1% (3.0, 16) for basal. On multivariable analysis (MVA) with luminal A as baseline, HER-2 (adjusted hazard ratio [AHR] = 9.2; 95% CI, 1.6 to 51; P = .012) and basal (AHR = 7.1; 95% CI, 1.6 to 31; P = .009) subtypes were associated with increased local recurrence. On MVA, luminal B (AHR = 2.9; 95% CI, 1.3 to 6.5; P = .007) and basal (AHR = 2.3; 95% CI, 1.1 to 5.2; P = .035) were associated with increased distant metastases. CONCLUSION: Overall, the 5-year local recurrence rate after BCT was low, but varied by subtype as approximated using ER, PR, and HER-2 status. Local recurrence was particularly low for the luminal A subtype, but was less than 10% at 5 years for all subtypes. Although further follow-up is needed, these results may be useful in counseling patients about their anticipated outcome after BCT. *Adjuvan trastuzumab almamış. Nguyen PL. JCO 2008;26;2373.")
47
11. Ref Approximately 22% of patients in the initial Fox
Chase Cancer Center study had positive or unknown margins, a finding known to be associated with LR,

52
MKC sonrası lokal yineleme :
Uygun olmayan hasta seçimi Yetersiz cerrahi Yetersiz RT Biyolojik agresif tümör *ACR Practice Guideline *Luini A et al, Breast Cancer Res Treat 2009

53
ÇIKARIMLAR Her meme kanseri (özellikle Evre I-II) MKC adayıdır
Doğru hasta seçiminde bulunmak Hastaya göre doğru cerrahi yöntemin uygulamak Negatif cerrahi sınırları sağlamak En iyi kozmetik sonuçları elde etmek

Benzer bir sunumlar






>")













 ve Meme Başı Koruyucu Mastektomi(MBKM)>")

