Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Morbid Obezite Cerrahisi Metabolik Cerrahi
Prof. Dr. Öge TAŞCILAR Genel Cerrahi AD.

2
Dünyada 2008 Obezite : 400 Milyon Fazla Kilolu : 1,4 milyar

3
İnsan Evrimi

4
Türkiye de obezite Erkeklerde %21.2, Kadınlarda ise % 41.5
19 yaş üstü obezite %30

5
Etiyoloji MULTİFAKTORİYEL Ailesel Genetik Cinsiyet (K>E)
Çevre ve Ortam Genetik Cinsiyet (K>E) Hastalıklar(end, psik) İlaçlar Psikolojik(Antidepresan ve rahatlama- Serotonin, Dopamin) Yemek-Ödül
 Hastalıklar(end, psik) İlaçlar. Psikolojik(Antidepresan ve rahatlama- Serotonin, Dopamin) Yemek-Ödül.")
6
Enerji Eşik Değeri Artışı ???
Uygunsuz Yağ depolanması ??? (Metabolik bozulma) Yılda 1 kilo almak için günlük 20 Kkalori fazla almak yeterli Leptin Reseptör Duyarsızlığı(deneysel)
 Yılda 1 kilo almak için günlük 20 Kkalori fazla almak yeterli. Leptin Reseptör Duyarsızlığı(deneysel)")
7
Amerika ve Kanada da çocuklar ebeveynlerinden (daha bilgisiz olacak) daha kısa yaşayacaklar
 daha kısa yaşayacaklar")
8
Ucuz kalori Rafine gıdalar(%80’i glukoz şurubu katkılı) İnsülinojenik ortam İnsülin=Yağ depolanması
333 Kcal 590 Kcal

9
Fizik Aktivite değişimi
1950 li yıllar 300 Kcal /saat 2000 li yıllar < 30 kcal /saat

10
Obezite sağlıklı olmayı engelleyen bir hastalıktır
Obezite kişinin sağlığını bozacak kadar vücutta yağ birikmesidir.

11
Vücut Kitle İndeksi (VKİ),(BMI)
Kilo ölçümü tekbaşına yağ fazlalığı anlamına gelmez (Profesyonel sporcular ). Herhangi bir VKİ de kadınların yağ oranı erkeklerden her zaman fazladır. Vücut Kitle İndeksi aşırı yağ dokusu değerlendirilmesi için “altın standart” dır. Vücut Kitle İndeksi= Ağırlık(kg)/Boy2(metre2) < = malnutrisyon = normal = aşırı kilolu 30 – = obez I (orta şiddette obezite) = obez II (ciddi obezite) > = obez III (morbid obezite)
. Herhangi bir VKİ de kadınların yağ oranı erkeklerden her zaman fazladır. Vücut Kitle İndeksi aşırı yağ dokusu değerlendirilmesi için altın standart dır. Vücut Kitle İndeksi= Ağırlık(kg)/Boy2(metre2) < 20 = malnutrisyon = normal = aşırı kilolu 30 – 34.9 = obez I (orta şiddette obezite) = obez II (ciddi obezite) > 40 = obez III (morbid obezite)")
12
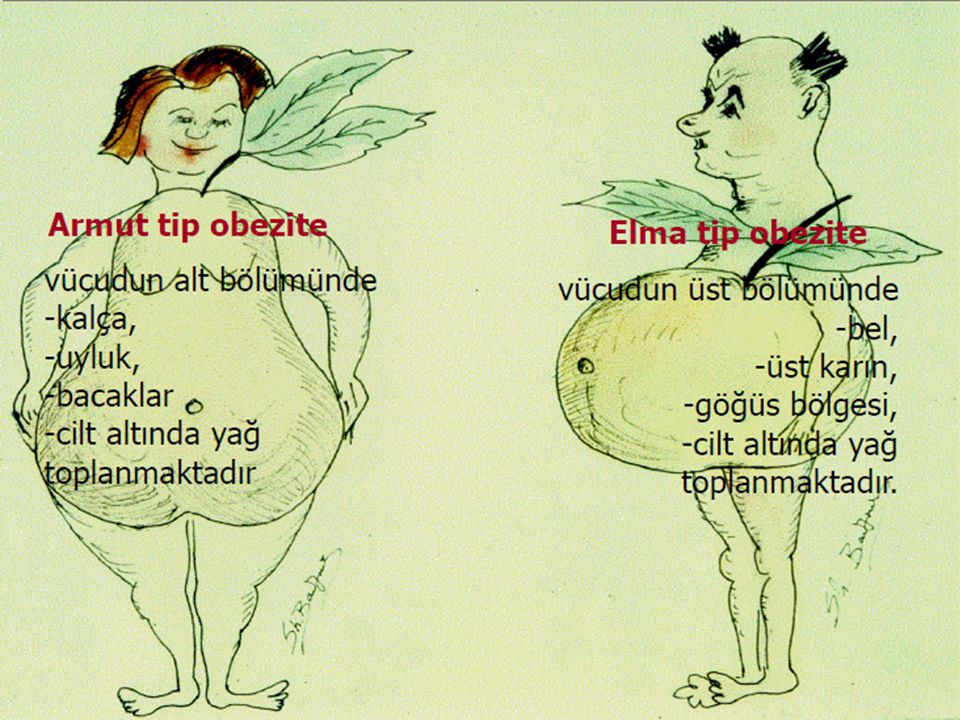
Vücut Yağ Dağılımı ve Santral Obezite
Vücut yağ dağılımı hastalık göstergesi olarak toplam yağ miktarından daha önemlidir. Vücut yağ dağılımı Ciltaltı yağ dokusu Viseral yağlar: Gövde organları etrafında depolanmış yağlar Viseral yağlarda artış (santral obezite) Kardiyovasküler hastalık Tip 2 DM (%92) Kanser artışa yol açar.
 Kardiyovasküler hastalık. Tip 2 DM (%92) Kanser artışa yol açar.")
14
SAĞLIK SORUNLARI • İnsülin direnci – Hiperinsülinemi • Tip 2 Diyabet
• Hipertansiyon • Koroner arter hastalığı • Hiperlipidemi – Hipertrigliseridemi • Metabolik sendrom • Safra kesesi hastalıkları • Bazı kanser türleri • Osteoartrit • Karaciğer yağlanması • Astım • Kas-iskelet sistemi problemleri

15
VKİ > 30 üzerinde morbidite ve mortalite dereceli olarak artmaktadır.
n = adults 14 yrs follow-up Calle, NEJM 1999;341:

16
Global Prevalence of Diabetes in 2000 and Projections for 2030
Global Increase 180 472 million! Millions of Cases of Diabetes in 2000 and Projections for 2030, with Projected Percent Changes. Data are from Wild et al.1 1 Wild S, Roglic G, Green A et. Al. Global prevalence of diabetes estimates for he year 2000 and projections for Diabetes Care 2004;27: P Hossain et al. N Engl J Med 2007;356: 16

17
Tip2 Diabet’in ana sebebi Obezite
IDF. Diabetes Atlas. Second Edition 2003

18
Around 55%of pts are NOT under control
Diabet Birçok yeni antidiabetik ajanlar Insulin pompaları Eğitim Özelleşmiş Diabet Merkezleri Around 55%of pts are NOT under control

19
Diabetik hastaların % 93’ünde glukoz, kolesterol and kan basıncı iyi KONTROL EDİLEMİYOR
Only 7% of adult diabetic patients from NHANES ( ) achieved: A1C <7% PA <130/80 mm Hg Total Cholesterol < 200 mg/dL Saydah SH et al. JAMA. 2004
 achieved: A1C <7% PA <130/80 mm Hg. Total Cholesterol < 200 mg/dL. Saydah SH et al. JAMA")
20
Mide Fundus bölgesinden 150 den fazla peptid salınıyor, (2014)
")
21
Ghrelin Diabetojenic ↑ GLUKOZ GHRELIN ↑ GH ↑ ACTH & Cortisol
↑ Epinephrine ↑ Glucagon? ↓ Adiponectin ↓ Insulin Action ↓ Insulin Secretion ↑ Food Intake Counter-regulatory Ghrelin Diabetojenic GHRELIN ↑ GLUKOZ DE Cummings

22
Yaşam Tarzı değişikliği
Obezite Tedavisi Medikal Tedavi 1. Diyet Tedavisi 2. Egzersiz Tedavisi 3. Davranış değişikliği tedavisi 4. Farmakolojik Tedavisi Cerrahi Tedavi Diyet Fizik Aktivite Yaşam Tarzı değişikliği İlaçlar Cerrahi Obesity treatment pyramid The clinical approach to obesity can be viewed as a pyramid consisting of several levels of therapeutic options. All patients should be involved in an effort to change their lifestyle behaviors to decrease energy intake and increase physical activity. Lifestyle modification also should be a component of all other levels of therapy. Pharmacotherapy can be a useful adjunctive measure for properly selected patients. Bariatric surgery is an option for patients with severe obesity, who have not responded to less-intensive interventions. The number of obese patients who require a specific level of treatment decreases as one moves up the pyramid.

23
Medikal Tedavi Medikal tedavi ile ortalama %10 oranında kilo kaybı oluşurken, hastaların %95’i 1-5 yıl içinde diyet öncesindeki kilolarına geri dönmektedirler. 17 yıllık süre içinde yapılan 3 büyük konsensus toplantısı sonucu; ”morbid obez hastalara uygulanan cerrahi dışı tedavilerin başarı şansı çok düşük”

24
CERRAHİ İÇİN HASTA SEÇİMİ
VKİ > 40 VKİ > 35 ve yandaş hastalık varlığı (HT, T2DM, Artrit) Cerrahi dışı yöntemlerle kilo verilememesi (>2 yıl süreyle) Gebe olmaması ve kilo verme sürecinde gebelik planlanmaması(1-2 yıl)
 Cerrahi dışı yöntemlerle kilo verilememesi (>2 yıl süreyle) Gebe olmaması ve kilo verme sürecinde gebelik planlanmaması(1-2 yıl)")
25
CERRAHİ TEDAVİNİN KESİN KONTRENDİKASYONLARI
Gastrointestinal sistemin enflamatuar hastalıkları Yüksek operatif risk Üst gastrointestinal sistem kanaması oluşturabilecek nedenler (varisler, telanjiektaziler) Hamilelik Alkol veya ilaç bağımlılığı Gastrointestinal sistem anomalileri (atrezi / stenoz) Aktif enfeksiyon varlığı Uyum sağlayamayacak hastalar Kullanılan materyallere reaksiyon gelişebilecek hastalar
 Hamilelik. Alkol veya ilaç bağımlılığı. Gastrointestinal sistem anomalileri (atrezi / stenoz) Aktif enfeksiyon varlığı. Uyum sağlayamayacak hastalar. Kullanılan materyallere reaksiyon gelişebilecek hastalar.")
26
NİÇİN AMELİYAT??

27
Adams et al. (2007) Mean Follow-up 7.1 years (total 18 years) Cases 7,925 (100% GBP), 84% female, 39.5 y, BMI 45.3 Controls 7,925 no bariatric surgery, 84% female, 39.3 y, BMI 46.7 % Deaths 2.7% cases, 4.1% controls % Death Reduction Unadjusted, 34% Adjusted, 40% Adams, et al. NEJM 2007;357:

28
Bariatric Surgery Reduces Mortality in Swedish Obese Subjects (n=2010 vs. 2037)
30% Reduction in All Cause Mortality Sjostrom L et al. NEJM 2007;357:741-52

29
Bariatric Surgery & Reduced Mortality (%)
Study Reference % Reduction MacDonald, KG. J Gastrointest Surg 1997;1: 88 Flum, DR. J Am Coll Surg 2004;199: 33 Christou, NV. Ann Surg 2004;240: 89 Sowemino, OA. Surg Obes Relat Dis 2007;3:73-77 63 Sjöström, L. NEJM 2007;357: 29 Adams. T. NEJM 2007;357: 40 Busetto, L. Surg Ob Rel Dis 2007;3: 60 Peeters, A. Ann Surg 2007;246: 72

30
Klinik Morbid Obezitede sadece Cerrahi uzun dönem etkili tedavidir (1991)
")
31
Bariatric Cerrahi ve Diabet ???
Eskiye Dönüş mü?....Keşif mi?

33
Ayarlanabilir Mide Kelepçesi

34
Laparoskopik Sleeve Gastrektomi

37
Biliopankreatik Diversiyon-Duodenal Switch

38
Diabet Üzerine Etkisi

40
Glukagon-Like Peptide-1
increases insulin secretion from the pancreas in a glucose-dependent manner. decreases glucagon secretion from the pancreas by engagement of a specific G protein-coupled receptor. increases insulin-sensitivity in both alpha cells and beta cells increases beta cells mass and insulin gene expression, post-translational processing and incretion. inhibits acid secretion and gastric emptying in the stomach. decreases food intake by increasing satiety in brain. promotes insulin sensitivity.

41
GLP1 Analogları Exenatide, Liraglutide, Dulaglutide
Dipeptidyl peptidase-4: Sitagliptin (DPP4 inhibitor) Liraglutide Glucose-dependent insulinotropic peptide
 Liraglutide. Glucose-dependent insulinotropic peptide.")
43
Gastrik Bypass Cerrahisi sonrası Vücut ağırlığı değişimi(uzun dönem)
20 40 60 80 100 (% of Excess Weight) Weight Loss Gastric bypass surgery results in sustained weight loss for most obese patients. This figure shows the results of a long-term evaluation of body weight in patients who had gastric bypass surgery [1]. In this study, maximum weight loss (70% of excess weight) occurred 2 years after surgery. Although patients regained some of their lost weight over time, a 50% weight loss, corresponding with a 15-point decrease in BMI, was maintained for 14 years. 1. Pories WJ, Swanson MS, MacDonald KG, et al. Who would have thought it? An operation proves to be the most effective therapy for adult onset diabetes mellitus. Ann Surg 1995;222: 2 4 6 8 10 12 14 Years After Surgery BMI (kg/m2): Pories et al. Ann Surg 1995;222:339.
 Weight Loss. Gastric bypass surgery results in sustained weight loss for most obese patients. This figure shows the results of a long-term evaluation of body weight in patients who had gastric bypass surgery [1]. In this study, maximum weight loss (70% of excess weight) occurred 2 years after surgery. Although patients regained some of their lost weight over time, a 50% weight loss, corresponding with a 15-point decrease in BMI, was maintained for 14 years. 1. Pories WJ, Swanson MS, MacDonald KG, et al. Who would have thought it An operation proves to be the most effective therapy for adult onset diabetes mellitus. Ann Surg 1995;222: Years After Surgery. BMI (kg/m2): Pories et al. Ann Surg 1995;222:339.")
44
Maintenance of weight loss after gastric bypass surgery

47
UK NICE Expedites Access to Bariatric Surgery in Diabetes
The new recommendations stress that individuals with a body mass index (BMI) of 35 kg/m2 or more who have recent-onset type 2 diabetes should be offered an expedited assessment for bariatric surgery. They also advise, for the first time, the consideration of bariatric surgery as a treatment option for those with a lower BMI of 30 to 35 kg/m2 and recent-onset diabetes.
 of 35 kg/m2 or more who have recent-onset type 2 diabetes should be offered an expedited assessment for bariatric surgery. They also advise, for the first time, the consideration of bariatric surgery as a treatment option for those with a lower BMI of 30 to 35 kg/m2 and recent-onset diabetes.")
48
UK May Lower BMI Threshold From 35 to 30 for Bariatric Surgery
The recent 3-year STAMPEDE results were some of the first to address use of bariatric surgery in a randomized fashion in obese diabetic patients with a BMI less than 35; those patients appeared to enjoy the same benefits as those with a BMI greater than 35.

49
STAMPEDE: Surgery reduces or eliminates need for diabetes meds
The Surgical Treatment and Medications Potentially Eradicate Diabetes Efficiently (STAMPEDE) study was reported by Dr Philip R Schauer (Cleveland Clinic, OH) as a late-breaking clinical trial today at the ACC meeting. Schauer and colleagues enrolled 150 obese patients (BMI 27–43 kg/m2) with uncontrolled type 2 diabetes and randomly assigned them to medical therapy, Roux-en-Y gastric bypass (RYGB), or sleeve gastrectomy. Mean age was 49 years, and mean HbA1c was 9.2%. The main study outcome of HbA1c <6.0% after 12 months of treatment was met by 12% of the medical-therapy group, 42% of the RYGB group (p=0.002 vs medical therapy), and 37% of the sleeve-gastrectomy group (p=0.008 vs medical therapy). Although glycemic control improved in all three groups, improvements were significantly greater in the surgical groups, as was weight loss and improvement in insulin resistance.
 study was reported by Dr Philip R Schauer (Cleveland Clinic, OH) as a late-breaking clinical trial today at the ACC meeting. Schauer and colleagues enrolled 150 obese patients (BMI 27–43 kg/m2) with uncontrolled type 2 diabetes and randomly assigned them to medical therapy, Roux-en-Y gastric bypass (RYGB), or sleeve gastrectomy. Mean age was 49 years, and mean HbA1c was 9.2%. The main study outcome of HbA1c <6.0% after 12 months of treatment was met by 12% of the medical-therapy group, 42% of the RYGB group (p=0.002 vs medical therapy), and 37% of the sleeve-gastrectomy group (p=0.008 vs medical therapy). Although glycemic control improved in all three groups, improvements were significantly greater in the surgical groups, as was weight loss and improvement in insulin resistance.")
50
The one exception to this is the International Diabetes Federation guidance, which last year changed to recommend that bariatric surgery could be considered as a reasonable treatment option in those with a BMI of 30 to 35 "if the patient has poorly controlled diabetes," Schauer noted.

51
An Unexpected Finding! The SOS study on mortality revealed a strong effect from cancer (control group, 47 deaths; surgery group, 29 deaths) The Utah study on mortality reported a 60% reduction in cancer deaths following bariatric surgery when compared to severely obese controls Sjöström, L. NEJM 2007;357: Adams et al. NEJM 2007;357:753

52
The Canadian Bariatric Five-Year Incidence of Overall Cancer Risk
Cohort Study Five-Year Incidence of Overall Cancer Risk Diagnosis: Cohort Bariatric Controls Relative Risk P-value N % Estimate 95% CI Any Cancer 21 2.0% 487 8.5% 0.22 0.14 0.35 0.001 78% Reduction in Overall Cancer Risk

53
The Canadian Bariatric Cohort Study
83% 68% (p=0.001) (p=0.063)
 (p=0.063)")
54
Komplikasyonlar(Erken)
Kanama-Kaçak Obstrüksiyon Pulmoner emboli Hipoglisemi Dehidratasyon

55
Komplikasyonlar(Geç)
Kilo verememe(kilo alma) Beslenme bozukluğu(malnütrisyon) Vitamin eksiklikleri Hipokalsemi Hiperparatiroidi
 Beslenme bozukluğu(malnütrisyon) Vitamin eksiklikleri. Hipokalsemi. Hiperparatiroidi.")
56
Bariatrik cerrahinin yan etkileri
Diare Kötü kokulu gaz çıkarma Kusma Yara enfeksiyonu Anal sorunlar Bypass enteriti Obstrüksiyon Protein malnütrisyonu Hipokalsemi Osteoporoz Parathormon Yüksekliği Vitamin A,B,D,E yetersizliği Safra taşı Böbrek taşı Karaciğer yetmezliği Anemi(Fe, VitB12) Alopesi Ödem Kemik ağrıları
 Alopesi. Ödem. Kemik ağrıları.")
58
YANDAŞ HASTALIKLARDA DÜZELME
Diabet (Tip2 DM) % 90 Lipid Profili düzelmesi % 90 Artroz % 50 Hipertansiyon % 85 Uyku apnesi % 80
 % 90. Lipid Profili düzelmesi % 90. Artroz % 50. Hipertansiyon % 85. Uyku apnesi % 80.")
59
Results: % Difference (based on mortality HR) Matched Groups
Cause of Death GBP Patients vs DL Applicants Total Mortality 40% decrease (p<0.001) All CVD 49% decrease (p<0.001) CAD 59% decrease (p=0.006) Heart Failure 41% decrease (p=0. 54) All Strokes 57% decrease (p=0.14) Diabetes 92% decrease (p=0.005) All Cancers 60% decrease (p<0.001) All Diseases 52% decrease (p<0.001) Adams, et al. NEJM 2007;357:
 All CVD. 49% decrease (p<0.001) CAD. 59% decrease (p=0.006) Heart Failure. 41% decrease (p=0. 54) All Strokes. 57% decrease (p=0.14) Diabetes. 92% decrease (p=0.005) All Cancers. 60% decrease (p<0.001) All Diseases. 52% decrease (p<0.001) Adams, et al. NEJM 2007;357:")
60
No relation between weight loss/gain and DM resolution
Delta BMI x A1c and FPG No relation between weight loss/gain and DM resolution FPG Delta BMI HAS NO IMPACT in the negative variation of A1c AND FPG from preop to 12 months

61
Kendi Vakalarım Açık Sleeve Gastrektomi 58 hasta
Lap Sleeve Gastrektomi 412 hasta Açık RNY Gastrik Bypass hasta Lap RNY Gastrik Bypass hasta Açık Duodenal switch hasta Lap Duodenal switch hasta Mortalite: 1 (Entübasyondan hemen sonra operasyona başlamadan anestezi altında anaflaktik şok, 2. gün) Kaçak: 1 hasta ( Geç kaçak, 21. gün cerrahi onarım)
 Kaçak: 1 hasta ( Geç kaçak, 21. gün cerrahi onarım)")
62
Bir yılda 75 kilo verdi - Hürriyet SAĞLIK -YAŞAM

63
55 yaş, BMI: 39, Tip2 Diabet, 100 Ü insülin kullanıyor idi
55 yaş, BMI: 39, Tip2 Diabet, 100 Ü insülin kullanıyor idi. RNY Gastrik Bypass Operasyondan 1 hafta sonradan itibaren 3 yıldır hiç ilaç kullanmıyor

64
BMI: 47 9. Ayında BMI: 26

65
Yeni Tedaviler Endoskopik yöntemler: Hastaların uyutularak veya sakinleştirici verilerek endoskop yardımıyla vücutlarında hiçbir kesi yapmadan uygulanan obezite tedavi yöntemleridir. Bu yöntemleri kendi aralarında birkaç gruba ayırabiliriz. A. Endosleeve yöntemi: Mide, onikiparmak barsağı ve ince barsağın içine emilimi önleyici plastik ince bir hortum konularak uygulanan bir yöntemdir. Henüz tam güvenilir klinik çalışmalar olmadığı için deneysel aşamadadır. B. Endoskopik zımba yöntemleri: Laparoskopik ameliyatlarda kullanılan zımbaların (stapler) benzeri cihazlarla hiçbir yer delinmeden midenin kesilerek küçültüldüğü yöntemlerdir. C. Endoskopik dikiş teknikleri : Birçok firma bu konuda çalışmaktadır. Ameliyat gerektirmeden endoskopik olarak mide hacmi küçültülebilmektedir.
 benzeri cihazlarla hiçbir yer delinmeden midenin kesilerek küçültüldüğü yöntemlerdir. C. Endoskopik dikiş teknikleri : Birçok firma bu konuda çalışmaktadır. Ameliyat gerektirmeden endoskopik olarak mide hacmi küçültülebilmektedir.")
Benzer bir sunumlar