Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
SANTRAL UYKU APNE SENDROMU
Doç. Dr. Remzi ALTIN Z.K.Ü Göğüs Hastalıkları Anabili Dalı

2
Tanım Santral Uyku Apne sendromu (CSA)
Uykuda santral solunum merkezinden solunum kaslarına giden uyarıların epizodlar halinde tam ya da kısmi azalması sonucunda meydana gelen bir hastalık grubu CSA is characterized by episodes of apnea or hypopnea related to loss of ventilatory output from the central respiratory generator in the brainstem to the respiratory pump. CSA’nin farklı klinik manifestasyonları (+)
")
3
Santral apne En az 10 sn süre ile solunum çabası olmaksızın hava akımında duraklama

5
Obstrüktif apnenin aksine; santral apne sırasında respiratuar drive’ın kesilmesine bağlı olarak solunum eforu yoktur. Bu iki apnenin birbirnden ayırt edilebilmesi için RIP ya da NP yöntemleri kullanılmalıdır. (oro nazal termistörler ile piezo elektrik kristal bantlarının santral apneyi tespit etmedeki duyarlılığı düşüktür) While the esophageal balloon is considered the gold standard to confirm reductions or absence of respiratory effort, central apneas appear to be adequately scored by plethysmographic measurement of chest wall and abdominal motion, a technique with reasonable reliability that is unlikely to misclassify a patient’s sleep-related breathing disorder. Cardiogenic oscillations noted in the airflow signal seen with a patent upper airway may further confirm that an apneic event is not obstructive.

6
Santral Uyku Apne “Santral / Obstrüktif Hipopne Tanım”
In the case of obstructive hypopneas, airflow decreases mainly as a consequence of upper airway obstruction, and therefore evidence of upper airway obstruction should be present, such as out of-phase thoraco-abdominal motion on RIP, or flow limitation on the nasal pressure signal. In the case of central hypopneas, airflow decreases mainly as a consequence of reduced respiratory drive, so that there should be no evidence of upper airway obstruction; thoraco-abdominal motion should be inphase, and there should be no evidence of flow-limitation on the nasal pressure signal. Although the ability of RIP and nasal pressure to distinguish between central and obstructive hypopneas has not been specifically addressed, both techniques have been validated against esophageal pressure as means of detecting airflow limitation. Consequently, both techniques can be used under most circumstance to distinguish central from obstructive apneas and hypopneas. Nevertheless, it is not always possible to distinguish central and obstructive hypopneas with these techniques. In such cases, esophageal pressure and diaphragmatic electromyogram can be used, but are invasive and require specialized equipment not available in most sleep laboratories. These techniques are not suitable for routine monitoring, but are usually reserved for research purposes. Kullanılan hipopne tanımları PSG raporunda belirtilmeli Ösafagal manometre, kalibre RIP ya da diafragmatik EMG kullanılmadan hipopne obstrüktif/santral/mikst olarak gruplandırılmamalıdır.

7
Santral Uyku Apne “Santral / Obstrüktif Hipopne Tanım”
Hipopnelerin büyük kısmı obstrüktif olarak skorlanır. Ancak, KY ya da stroke’lu hastalarda bu ayırımın yapılması önemlidir. However, when studying patients with cardiovascular diseases, especially those with HF and stroke, where CSA is much commoner than in the general population, distinguishing central from obstructive events assumes greater importance. Since, in the majority of patients with sleep apnea, most respiratory events are hypopneas, the determination of hypopnea type is also far more important in patients with cardiovascular diseases than in the general population. This is of practical importance, since in patients with HF, OSA is rapidly and completely reversed by continuous positive airway pressure (CPAP), whereas CSA responds more slowly and less completely to CPAP.
, whereas CSA responds more slowly and less completely to CPAP.")
8
Santral Hipopne Obstrüktif hipopne tanımı gibidir, ancak en belirgin fark; Özafagus basıncında fazla değişiklik YOK PTT’de belirgin azalma olması

9
TANI A + B + C: •A: Aşağıdakilerden en az birinin varlığı:
–Gündüz aşırıuyku hali –Gece sık arousal veya uyanma •B: Gece boyunca alınan PSG kayıtlarında uyku saati başına en az 5 santral tipte apne ve/veya hipopne saptanması(Santral apne-hipopne indeksi >5) •C: Santral tipte apne ve hipopnelerin sayısının tüm apne ve hipopnelerin %50’sini oluşturması
 •C: Santral tipte apne ve hipopnelerin sayısının tüm apne ve hipopnelerin %50’sini oluşturması.")
10
SANTRAL APNENİN SAPTANMASI
Tanıiçin tüm gece polisomnografi kaydı gereklidir Solunum eforunun değerlendirilmesi santral apne tanısında merkezi öneme sahiptir. Solunum eforu için altın standart özofagus basınçölçümüdür RIP (respiratory inductive plethysmography) solunum eforunun tayininde çoğunlukla yeterli olur. OBbstrüktif ve santral apnelerin bir arada bulunduğu durumlarda solunum olaylarının %50 den fazlasının santral olması santral uyku apne sendromu tanısI koydurur
 solunum eforunun tayininde çoğunlukla yeterli olur. OBbstrüktif ve santral apnelerin bir arada bulunduğu durumlarda solunum olaylarının %50 den fazlasının santral olması santral uyku apne sendromu tanısI koydurur.")
11
Apnenin Özofagus Balon Kateteri ile Saptanması

12
SANTRAL UYKU APNE SENDROMU PATOFİZYOLOJİ
1) Otomatik ya da Metabolik Kontrol; Kemoreseptörler Carotid arter & Aorta Medüller 2) Davranışsal Kontrol (yüksek kortikal merkezler); Konuşurken/yemek yerken ventilasyon kontrolü sağlanır Uyanıklık stimulusu 3) Mekanik Kontrol; Gerim & J reseptörleri NREM’de solunum tek başına kemoreseptörler ve vagal intrapulmoner reseptörlerce kontrol edilir. Solunum kaslarına giden nöronal outputun idamesinde kemoreseptörlerden gelen stimulusların uykuda solunumun devamının sağlanmasında kritik önemi (+) Unlike the heart, the respiratory muscles do not have a built-in pacemaker. These muscles receive impulses from the medulla from a region that has been called the respiratory center, respiratory oscillator, respiratory signal generator, and respiratory pacemaker. For breathing to change as physiologic conditions change, the respiratory center receives and responds to three general types of information: chemical information (from chemoreceptors responding to pH and to the partial pressures of oxygen [PaO2] and carbon dioxide [PaCO2]), mechanical information (from receptors in the lung and chest wall), and behavioral information (from higher cortical centers). These aspects of awake control also have an impact on the control of breathing during sleep. The major goal of the respiratory control system is homeostatis-that is, keeping blood gases in a tight range so that the metabolic functions of the body remain normal. Sleep is a time when the respiratory tranquility of resting wakefulness is replaced by marked respiratory variability due to changes in both the drive to the ventilatory pump muscles and the upper airway opening muscles. Breathing during wakefulness is controlled by several factors, including voluntary and behavioral elements, chemical factors (e.g., low oxygen levels, high carbon dioxide levels, and acidosis), and mechanical signals from the lung and chest wall. During sleep, there is loss of voluntary control and a decrease in the usual ventilatory response to both low oxygen and high carbon dioxide levels. Both hypoxemic and hypercapnic responses are most depressed in rapid eye movement (REM) sleep. * Ventilation is broadly controlled by both chemical/ metabolic stimuli (PaO2 and PaCO2) as well as neurobehavioral factors. The latter are prominent during wakefulness, and include stimuli from higher cortical centers related to daily living behaviors, such as phonation and deglutition as well as visual and auditory cues thought to contribute to an overall increase in tonic output from the cerebral cortex to the respiratory centers in the brainstem. During sleep, with loss of this neurobehavioral input, ventilation is driven by an automatic system which integrates afferent signals from peripheral (primarily sensing PaO2) and central (sensing PaCO2) chemoreceptors as well as vagally mediated feedback from lung and chest wall mechanoreceptors [7].
 Otomatik ya da Metabolik Kontrol; Kemoreseptörler. Carotid arter & Aorta. Medüller. 2) Davranışsal Kontrol (yüksek kortikal merkezler); Konuşurken/yemek yerken ventilasyon kontrolü sağlanır. Uyanıklık stimulusu. 3) Mekanik Kontrol; Gerim & J reseptörleri. NREM’de solunum tek başına kemoreseptörler ve vagal intrapulmoner reseptörlerce kontrol edilir. Solunum kaslarına giden nöronal outputun idamesinde kemoreseptörlerden gelen stimulusların uykuda solunumun devamının sağlanmasında kritik önemi (+) Unlike the heart, the respiratory muscles do not have a built-in pacemaker. These muscles receive impulses from the medulla from a region that has been called the respiratory center, respiratory oscillator, respiratory signal generator, and respiratory pacemaker. For breathing to change as physiologic conditions change, the respiratory center receives and responds to three general types of information: chemical information (from chemoreceptors responding to pH and to the partial pressures of oxygen [PaO2] and carbon dioxide [PaCO2]), mechanical information (from receptors in the lung and chest wall), and behavioral information (from higher cortical centers). These aspects of awake control also have an impact on the control of breathing during sleep. The major goal of the respiratory control system is homeostatis-that is, keeping blood gases in a tight range so that the metabolic functions of the body remain normal. Sleep is a time when the respiratory tranquility of resting wakefulness is replaced by marked respiratory variability due to changes in both the drive to the ventilatory pump muscles and the upper airway opening muscles. Breathing during wakefulness is controlled by several factors, including voluntary and behavioral elements, chemical factors (e.g., low oxygen levels, high carbon dioxide levels, and acidosis), and mechanical signals from the lung and chest wall. During sleep, there is loss of voluntary control and a decrease in the usual ventilatory response to both low oxygen and high carbon dioxide levels. Both hypoxemic and hypercapnic responses are most depressed in rapid eye movement (REM) sleep. * Ventilation is broadly controlled by both chemical/ metabolic stimuli (PaO2 and PaCO2) as well as neurobehavioral factors. The latter are prominent during wakefulness, and include stimuli from higher cortical centers related to daily living behaviors, such as phonation and deglutition as well as visual and auditory cues thought to contribute to an overall increase in tonic output from the cerebral cortex to the respiratory centers in the brainstem. During sleep, with loss of this neurobehavioral input, ventilation is driven by an automatic system which integrates afferent signals from peripheral (primarily sensing PaO2) and central (sensing PaCO2) chemoreceptors as well as vagally mediated feedback from lung and chest wall mechanoreceptors [7].")
13
Medullada; dorsal ve ventral nöronlardan çıkan afferent lifler; diafragma ve İK kaslara gider.
Medullada ayrıca pnömotaksik merkez de var; apnestik merkezi ve inspirasyonu inhibe eder. Hava yollarında gerim reseptörleri var; gerim reseptörleri akciğer inflasyonu ile stimüle olur ve inspirasyon sonlanır, ekspirasyon başlar solunum sayısı azalır. Slowly adapting pulmonary stretch receptors located in the airways with vagal afferents that are stimulated by increases in lung volume. For example, when functional residual capacity is raised or when lung volume is held at its end-inspiratory level, a reduction in respiratory frequency results primarily from prolongation of the expiratory period (inflation reflex of Hering–Breuer). A reduction in activity of these receptors with lung deflation stimulates inspiratory onset (deflation reflex) and may contribute to the tachypnea that accompanies atelectasis. • Rapidly adapting pulmonary stretch receptors concentrated near the carina and central bronchi, also with vagal afferents, are stimulated both mechanically and chemically to generate the cough reflex. • C-fiber endings attached to unmyelinated afferent fibers are found close to the pulmonary capillaries, where they have been called type J (juxtapulmonary capillary) receptors and are also present in the bronchi in proximity to the bronchial circulation. Both types of C-fiber endings are stimulated by endogenously produced substances, including histamine, some prostaglandins, bradykinin, and serotonin, and may have a role in conditions such as asthma, pulmonary venous congestion, and pulmonary embolism. C-fiber endings also are mechanically sensitive and can be activated by lung hyperinflation. • Musculoskeletal afferents stimulated by the stretching of skeletal muscle increase ventilation and may contribute to the initial hyperpnea of exercise.
. A reduction in activity of these receptors with lung deflation stimulates inspiratory onset (deflation reflex) and may contribute to the tachypnea that accompanies atelectasis. • Rapidly adapting pulmonary stretch receptors concentrated near the carina and central bronchi, also with vagal afferents, are stimulated both mechanically and chemically to generate the cough reflex. • C-fiber endings attached to unmyelinated afferent fibers are found close to the pulmonary capillaries, where they have been called type J (juxtapulmonary capillary) receptors and are also present in the bronchi in proximity to the bronchial circulation. Both types of C-fiber endings are stimulated by endogenously produced substances, including histamine, some prostaglandins, bradykinin, and serotonin, and may have a role in conditions such as asthma, pulmonary venous congestion, and pulmonary embolism. C-fiber endings also are mechanically sensitive and can be activated by lung hyperinflation. • Musculoskeletal afferents stimulated by the stretching of skeletal muscle increase ventilation and may contribute to the initial hyperpnea of exercise.")
14
PATOFİZYOLOJİ Uyku sırasında
İstemli (Davranışsal) kontrol ortadan kalkar Solunum merkezinin C02’a duyarlılığı azalır Uyku sırasında normal C02 düzeyinde hafif artış olur (~ 2-4 mmHg)
 kontrol ortadan kalkar. Solunum merkezinin C02’a duyarlılığı azalır. Uyku sırasında normal C02 düzeyinde hafif artış olur (~ 2-4 mmHg)")
15
PATOFİZYOLOJİ Uyku sırasında apne eşiği Uyanıklık Uyku PaC02 40 mmHg
Eşik PaC02 35 mmHg 41-42 mmHg

16
PATOFİZYOLOJİ Uyku sırasında faringeal hava yolu kollapsı, solunumu inhibe eden refleksleri başlatarak santral apneye yol açabilir

17
PATOFİZYOLOJİ-SONUÇ Ventilasyon UYKUDA multifaktöriyel olarak azalır.
SUAS’da ortaya çıkan santral apnelerin tek bir nedeni yoktur The reduction in ventilation associated with sleep appears to be multifactorial in origin. NREM sleep is associated with a twofold increase in upper airway resistance [9] which appears to be due in part to reduced neuromuscular input as demonstrated by electromyographic recordings of upper airway muscles. This reduction in neuromuscular control originates primarily from the tonic background, although decrements may be seen on phasic stimulation during inspiration [10]. These regional effects coupled with reductions in both the hypoxic and hypercapnic ventilatory response [8], result in modest hypoventilation associated with 2–4% reductions in oxyhemoglobin saturation and a 3–6mm Hg increase in the partial pressure of carbon dioxide [11, 12]. Further decrements in the ventilatory response occur during REM sleep [13], despite the return of behavioral cortical activity which is characterized by an irregular breathing pattern thought to be associated with dreaming. During both wakefulness and sleep, the most sensitive determinant of ventilation is PaCO2, the level of which is linearly related to minute ventilation. Thus, small changes in arterial CO2 tension actuate a change in ventilation. Oxygen tension also appears to play a role in the drive to breathe, but relatively large decrements (PaO2 60mm Hg) are required before an appreciable increase in minute ventilation is encountered (a hyperbolic response) [16]. Skatrud and Dempsey [17] were among the first to describe an apneic threshold, a PaCO2 level below which was frequently associated with central apnea during NREM sleep in healthy individuals. Hypoxia appears to promote apnea indirectly by stimulating ventilation with resultant hypocapnia sufficient to cross the apneic threshold [17].
 are required before an appreciable increase in minute ventilation is encountered (a hyperbolic response) [16]. Skatrud and Dempsey [17] were among the first to describe an apneic threshold, a PaCO2 level below which was frequently associated with central apnea during NREM sleep in healthy individuals. Hypoxia appears to promote apnea indirectly by stimulating ventilation with resultant hypocapnia sufficient to cross the apneic threshold [17].")
18
Santral Apne Mekanizmaları
CA’ler neden evre 1-2’de daha fazla ama REM’de daha az? Çünkü recp kemosensitivitesi daha az REM’de Artmış solunumsal Nöronal aktivitesi (+); solunum kontrolü metabolikten çok davranışsal kontrol altında Solunum drive’ı ve solunum kas aktivitesi daha az ve PC02 NREM’e göre daha yüksek Eckert DJ, et al. Central sleep apnea. Chest 2007; 131: 18
; solunum kontrolü metabolikten çok davranışsal kontrol altında. Solunum drive’ı ve solunum kas aktivitesi daha az ve PC02 NREM’e göre daha yüksek. Eckert DJ, et al. Central sleep apnea. Chest 2007; 131:")
19
EPİDEMİYOLOJİ CSA Apneik hastaların %5-10’nunda görülür
İnsidansı ~ %12 (araştırılan popülasyon belirleyici) Erkek hakimiyeti Orta-ileri yaş KY, stroke, DM’lu hastalarda CSA sıklığı daha fazla If abnormal nocturnal breathing is to be understood and recognized, it is important to determine how commonly central apneas occur in normal individuals. The reported frequency of disordered breathing, and in particular the individual patterns, varies depending on the population studied, the methods used for apnea detection, and the threshold used to define abnormalities.50 Carskadon and Dement found that 37.5% of all subjects over the age of 62 had apneas or hypopneas, and that most of the time, "when determinations were possible, apneas were primarily of central type." Other studies report an incidence of central sleep apnea of between 12% and 66%,depending on the population investigated. Lugaresi et al. stated that "central apneas lasting 5-15 sec may appear during light and REM sleep" in normal subjects.With these limitations in mind, a frequency of more than five central apneas per hour of sleep is generally considered abnormal. Although most research-based studies require a greater frequency of events for inclusion, a recent report from the American Academy of Sleep Medicine defined idiopathic central sleep apnea syndrome as the presence of five or more central apneas per hour of sleep in patients with an arterial PCO2 of less than 45 mm Hg who are either excessively sleepy during the day or have frequent nocturnal arousals or awakenings.This same report defined the Cheyne-Stokes respiration syndrome as the presence of at least three consecutive respiratory cycles, with a crescendo-decrescendo pattern and a cycle length near 60 seconds, in a patient with either congestive heart failure or cerebrovascular disease. In addition, these patients must have either five or more central apneas or hypopneas per hour of sleep or 10 consecutive minutes of crescendo-decrescendo breathing.5Thus, a standard now exists for defining these syndromes. In the four studies that specifically considered patients with symptomatic idiopathic central sleep apnea, no consistent epidemiologic trends emerge. Guilleminault et al.,1 White et al.,58 and Bradley et al.27 reported a strong male predominance; Roehrs et al.7 observed central apneas more commonly in women. No explanation can be offered for this discrepancy. All studies, however, noted this disorder to occur most commonly in middle-aged to older adult individuals, although a few younger patients have been reported. In the case of Cheyne-Stokes respiration, a number of reports suggest that patients with congestive heart failure, without obvious breathing abnormalities during the day, may have periodic breathing during sleep.59,60 One study suggests that 45% of patients with congestive heart failure (left ventricular ejection fraction of less than 40%) have more than 20 central apneas plus hypopneas per hour of sleep.61 Thus, Cheyne-Stokes respiration during sleep in patients with congestive heart failure is likely to be quite common. Santral uyku apne sendromu [central sleep apnea syndrome (CSAS)] ise, uykuda solunum bozuklukları spektrumu içerisinde, apneik hastaların %5-10’unda görülen, tüm apne ve hipopnelerin %50’den fazlasının santral tipte olması ile karakterize ve obstrüktif uyku apne sendromu (OSAS)’ndan belirgin farklılıkları bulunan bir hastalık tablosudur. Ancak çoğu zaman obstrüktif veya mikst tip uyku apnesi ile birlikte görülür (3). CAI> 20/sa ciddi olarak kabul edildiğinde < 65 yaş görülmrmiş, > 65y prevelansı %5
 Erkek hakimiyeti. Orta-ileri yaş. KY, stroke, DM’lu hastalarda CSA sıklığı daha fazla. If abnormal nocturnal breathing is to be understood and recognized, it is important to determine how commonly central apneas occur in normal individuals. The reported frequency of disordered breathing, and in particular the individual patterns, varies depending on the population studied, the methods used for apnea detection, and the threshold used to define abnormalities.50. Carskadon and Dement found that 37.5% of all subjects over the age of 62 had apneas or hypopneas, and that most of the time, when determinations were possible, apneas were primarily of central type. Other studies report an incidence of central sleep apnea of between 12% and 66%,depending on the population investigated. Lugaresi et al. stated that central apneas lasting 5-15 sec may appear during light and REM sleep in normal subjects.With these limitations in mind, a frequency of more than five central apneas per hour of sleep is generally considered abnormal. Although most research-based studies require a greater frequency of events for inclusion, a recent report from the American Academy of Sleep Medicine defined idiopathic central sleep apnea syndrome as the presence of five or more central apneas per hour of sleep in patients with an arterial PCO2 of less than 45 mm Hg who are either excessively sleepy during the day or have frequent nocturnal arousals or awakenings.This same report defined the Cheyne-Stokes respiration syndrome as the presence of at least three consecutive respiratory cycles, with a crescendo-decrescendo pattern and a cycle length near 60 seconds, in a patient with either congestive heart failure or cerebrovascular disease. In addition, these patients must have either five or more central apneas or hypopneas per hour of sleep or 10 consecutive minutes of crescendo-decrescendo breathing.5Thus, a standard now exists for defining these syndromes. In the four studies that specifically considered patients with symptomatic idiopathic central sleep apnea, no consistent epidemiologic trends emerge. Guilleminault et al.,1 White et al.,58 and Bradley et al.27 reported a strong male predominance; Roehrs et al.7 observed central apneas more commonly in women. No explanation can be offered for this discrepancy. All studies, however, noted this disorder to occur most commonly in middle-aged to older adult individuals, although a few younger patients have been reported. In the case of Cheyne-Stokes respiration, a number of reports suggest that patients with congestive heart failure, without obvious breathing abnormalities during the day, may have periodic breathing during sleep.59,60 One study suggests that 45% of patients with congestive heart failure (left ventricular ejection fraction of less than 40%) have more than 20 central apneas plus hypopneas per hour of sleep.61 Thus, Cheyne-Stokes respiration during sleep in patients with congestive heart failure is likely to be quite common. Santral uyku apne sendromu [central sleep apnea syndrome (CSAS)] ise, uykuda solunum bozuklukları spektrumu içerisinde, apneik hastaların %5-10’unda görülen, tüm apne ve hipopnelerin %50’den fazlasının santral tipte olması ile karakterize ve obstrüktif uyku apne sendromu (OSAS)’ndan belirgin farklılıkları bulunan bir hastalık tablosudur. Ancak çoğu zaman obstrüktif veya mikst tip uyku apnesi ile birlikte görülür (3). CAI> 20/sa ciddi olarak kabul edildiğinde < 65 yaş görülmrmiş, > 65y prevelansı %5.")
20
KLİNİK BULGULAR Semptom CSAS OSAS GAUH Değişken Var Rahatsız uyku
Horlama Noktürnal ND Sabah BA İnsomnia NOD PND, sık noktürnal arousal- awakenings (+) Horlama, GAUH, obezite nadir
 Horlama, GAUH, obezite nadir.")
21
KLİNİK SINIFLAMA (Uyanıklık CO2 Düzeylerine Göre)
Hiperkanik CSAS Hiperkapnik ventilatuar yanıt düşük Kronik Solunum kontrolü ya da solunum mekaniği bozuktur (uyku& uyanıklıkta) Normo-hipokapnik CSAS Hiperkapnik ventilatuar yanıt yüksek Solunum kontrolü instabilitesi Nonhiperkapnik formu daha sıktır. Horlama veya üst solunum yolu (ÜSY) obstrüksiyonu olmaksızın farklı mekanizmalarla oluşur. Disorders without hypercapnia, and importantly often associated with hypocapnia, include primary CSA syndrome, Cheyne-Stokes breathing pattern (also been referred to as periodic breathing) seen most commonly in the setting of heart failure (HF) or central neurologic disease, and high altitude periodic breathing (HAPB).
 Normo-hipokapnik CSAS. Hiperkapnik ventilatuar yanıt yüksek. Solunum kontrolü instabilitesi. Nonhiperkapnik formu daha sıktır. Horlama veya üst solunum yolu (ÜSY) obstrüksiyonu olmaksızın farklı mekanizmalarla oluşur. Disorders without hypercapnia, and importantly often associated with hypocapnia, include primary CSA syndrome, Cheyne-Stokes breathing pattern (also been referred to as periodic breathing) seen most commonly in the setting of heart failure (HF) or central neurologic disease, and high altitude periodic breathing (HAPB).")
22
KLİNİK SINIFLAMA Hiperkapnik CSAS; Nonhiperkapnik CSAS;
Santral solunum uyarısının bozulması Primer: Konjenital santral hipoventilasyon (PHOX2B) Sekonder: Ensefalit, beyinde tümör, infarkt, kanama, narkotik ve opioid ilaçlar, obezite-hipoventilasyon Solunum kaslarının etkin çalışmaması Kas hastalıkları: Myopatiler, myotonik distrofi, ALS, postpolio sendromu, myastenia gravis, MS Kifoskloyoz Nonhiperkapnik CSAS; Cheyne-stokes solunumu Kalp yetmezliği Yüksek irtifa Cerebrovasküler hastalıklar İdiyopatik santral uyku apne sendromu Diğer: Obtrüktif uyku apne sendromu, hipotiroidi, akromegali, fizyolojik (uyku başlangıcı, arousal sonrası, fazik REM) Solunum sisteminin asıl amacı hücrelere metabolizmalarına yetecek kadar oksijeni ulaştırıp, ortaya çıkan karbondioksitin atmosfere geri dönmesini sağlamaktır. Bu gaz alışverişinin çeşitli mekanizma ve nedenler ile bozulması yaşamsal fonksiyonları tehlikeye sokar. Bunlardan biri, alveoler hipoventilasyon yani alveollere giden gaz volümünde azalmadır. Alveoler hipoventilasyon karbondioksit retansiyonuna ve hiperkapniye yol açar. Hiperkapnik CSAS yeni sınıflamalarda “hipoventilasyon sendromları” içerisinde ele alınmaktadır.
 Sekonder: Ensefalit, beyinde tümör, infarkt, kanama, narkotik ve opioid ilaçlar, obezite-hipoventilasyon. Solunum kaslarının etkin çalışmaması. Kas hastalıkları: Myopatiler, myotonik distrofi, ALS, postpolio sendromu, myastenia gravis, MS. Kifoskloyoz. Nonhiperkapnik CSAS; Cheyne-stokes solunumu. Kalp yetmezliği. Yüksek irtifa. Cerebrovasküler hastalıklar. İdiyopatik santral uyku apne sendromu. Diğer: Obtrüktif uyku apne sendromu, hipotiroidi, akromegali, fizyolojik (uyku başlangıcı, arousal sonrası, fazik REM) Solunum sisteminin asıl amacı hücrelere metabolizmalarına yetecek kadar oksijeni ulaştırıp, ortaya çıkan karbondioksitin atmosfere geri dönmesini sağlamaktır. Bu gaz alışverişinin çeşitli mekanizma ve nedenler ile bozulması yaşamsal fonksiyonları tehlikeye sokar. Bunlardan biri, alveoler hipoventilasyon yani alveollere giden gaz volümünde azalmadır. Alveoler hipoventilasyon karbondioksit retansiyonuna ve hiperkapniye. yol açar. Hiperkapnik CSAS yeni sınıflamalarda hipoventilasyon sendromları içerisinde ele alınmaktadır.")
23
ICSD-2 2005 sınıflamasına göre Santral Uyku Apne Sendromları
II- Uykuda Solunum Bozuklukları Santral Uyku Apne Sendromları Obstrüktif Uyku Apne Sendromları Uyku ile ilişkili Hipventilasyon/Hipoksemi Sendromları Diğer Uykuda Solunum Bozuklukları, tanımlanmamış

24
ICSD-2 sınıflaması Santral Uyku Apne Sendromları
Primer Santral Uyku Apnesi Cheyne-Stokes Solunumuna bağlı Santral Uyku Apnesi Yüksek irtifada periyodik solunuma bağlı Santral Uyku Apnesi Cheyne-Stokes ya da Yüksek İrtifa dışındaki hastalıklara bağlı Santral Uyku Apnesi İlaçlara bağlı Santral Uyku Apnesi Çocukluk çağı (YENİDOĞAN) primer Santral Uyku Apnesi Central Sleep Apnea Syndromes Primary Central Sleep Apnea Other Central Sleep Apnea Due to Medical Condition Cheyne–Stokes Breathing Pattern High-Altitude Periodic Breathing Central Sleep Apnea Due to Medical Condition Not Cheyne–Stokes or High-Altitude Central Sleep Apnea Due to Drug or Substance Other Sleep-Related Breathing Disorder Due to Drug or Substance Primary Sleep Apnea of Infancy (formerly Primary Sleep Apnea of Newborn)
 primer Santral Uyku Apnesi. Central Sleep Apnea Syndromes. Primary Central Sleep Apnea. Other Central Sleep Apnea Due to Medical Condition. Cheyne–Stokes Breathing Pattern. High-Altitude Periodic Breathing. Central Sleep Apnea Due to Medical Condition Not Cheyne–Stokes or High-Altitude. Central Sleep Apnea Due to Drug or Substance. Other Sleep-Related Breathing Disorder Due to Drug or Substance. Primary Sleep Apnea of Infancy (formerly Primary Sleep Apnea of Newborn)")
25
Primer Santral Uyku Apnesi
Oldukça nadir, tüm SUAS hastaları%5 İdyopatik olarakta bilinir Orta-ileri yaş Herediter özellik KOAH ve nerömüsküler hastalık ile birliktelik

26
Primer Santral Uyku Apnesi
Solunum kontrolü instabil: PaCO2’e uyku ve uyanıklıkta anormal yanıt Artmış PaCO2 duyarlılığı sonucu PaCO2 apneik eşiğe yaklaşır Uykuda ani hiperventilasyon ile birlikte arousal olur ve bu durum ventilatuar instabiliteyi arttırır Cheyne stokes solunumda görülen arousal ve ventilasyondaki siklik değişim burada görülmez

27
Primer Santral Uyku Apnesi
Santral apneler tipik olarak NREM’de görülür Sık uyanma ile birlikte uykuda bölünmeler Gündüz aşırı uyku hali Bazen uykuya dalamama Sıklıkla uyanıklık PACO2 düşüktür

28
Primer Santral Apne Sendromu
1. Aşağıdakilerden en az biri olmalı - aşırı gündüz uykululuğu - uykuda sık arousal veya uyanıklıklar veya insomni yakınması - nefes darlığı ile uyanma 2. Polisomnografide uykunun her saatinde ortalama en az 5 santral apne varlığı 3. Bozukluk başka bir uyku bozukluğu, tıbbi veya nörolojik bozukluk veya ilaç ve madde kullanımı ile açıklanamamalı

29
Primer Santral Uyku Apnesi TEDAVİ
CO2 inhalasyonu CPAP Oksijen Asetazolamide

30
Cheyne-Stokes Solunumuna bağlı santral uyku apnesi

31
ICSD-2 sınıflaması Santral Uyku Apne Sendromu
Cheyne- Stokes Solunumu (CSR); 1818’de John Cheyne, sonra 1854’de William Stokes tarafından kalp ve/veya nörolojik hastalığı olanlarda tanımlanmış Periyodik bir solunum paterni Tidal volümün kreşendo- dekreşendo tarzında artıp azalması ve arada oluşan santral apneler ile karakterize CSR is a form of periodic breathing in which, according to the original description by Cheyne, the ventilatory period is characterized by a prolonged waxing waning pattern of tidal volume followed by central apnea or hypopnea. It is noteworthy that the patient in whom Cheyne first described this breathing disorder suffered from HF, atrial fibrillation, and a stroke, and undoubtedly had a low cardiac output and prolonged circulation time. CSA-CSR, an increasingly common form of SDB most often encountered in the setting of HF, is a breathing pattern characterized by crescendo-decrescendo tidal volumes with intervening central apneas. This waxing and waning pattern has also been referred to as periodic breathing. In contrast to OSA, where arousals typically occur with apnea termination, arousals from sleep in CSA-CSR tend to occur at the height of the hyperpneic phase following apnea. Considering this propensity for sleep disruption, it is not clear why daytime symptoms in CSA-CSR may not be as prominent as in OSA .CSA-CSR in HF has been associated with increased mortality .The severity of CSA is thought to be, to some extent, a reflection of underlying cardiac dysfunction, which could partially explain the mortality association.
; 1818’de John Cheyne, sonra 1854’de William Stokes tarafından kalp ve/veya nörolojik hastalığı olanlarda tanımlanmış. Periyodik bir solunum paterni. Tidal volümün kreşendo- dekreşendo tarzında artıp azalması ve arada oluşan santral apneler ile karakterize. CSR is a form of periodic breathing in which, according to the original description by Cheyne, the ventilatory period is characterized by a prolonged waxing waning pattern of tidal volume followed by central apnea or hypopnea. It is noteworthy that the patient in whom Cheyne first described this breathing disorder suffered from HF, atrial fibrillation, and a stroke, and undoubtedly had a low cardiac output and prolonged circulation time. CSA-CSR, an increasingly common form of SDB most often encountered in the setting of HF, is a breathing pattern characterized by crescendo-decrescendo tidal volumes with intervening central apneas. This waxing and waning pattern has also been referred to as periodic breathing. In contrast to OSA, where arousals typically occur with apnea termination, arousals from sleep in CSA-CSR tend to occur at the height of the hyperpneic phase following apnea. Considering this propensity for sleep disruption, it is not clear why daytime symptoms in CSA-CSR may not be as prominent as in OSA .CSA-CSR in HF has been associated with increased mortality .The severity of CSA is thought to be, to some extent, a reflection of underlying cardiac dysfunction, which could partially explain the mortality association.")
32
ICSD-2 sınıflaması Santral Uyku Apne Sendromu
Cheyne- Stokes Solunumu (CSR); The characteristic waxing and waning pattern of alternating apneas and hyperpneas in CSA-CSR is readily recognized on PSG. The cycle length, found to approximate 60 s, is significantly longer than those encountered in primary CSA ,and appears to correlate with circulatory delay. The 1999 Guidelines require 5 or more central apneas or hypopneas per hour of sleep as well as at least 10 consecutive minutes of cyclic crescendo and decrescendo changes in breathing amplitude. There are scant outcome data upon which to base severity criteria in CSA-CSR. Reported variables include the central apnea index ,the central AHI, and the quantity or percentage of sleep time with periodic breathing. Lanfranchi et al. found prognostic significance in the central AHI but not in the percentage of sleep time spent with periodic breathing. Son yayınlarda periyodik solunum prevalansının iskemik kalp hastalıklarında maksimum ejeksiyon fraksiyonu %40 olan ve optimal medikal tedavi alan hastalarda %45-50 olduğu bildirilmektedir. Erkeklerde kadınlara göre ve ileri yaşta daha sık görülür. CSR can be observed both during sleep and wakefulness, although it appears to be far more common during sleep. When it occurs during sleep, it is simply a form of CSA with a prolonged hyperpnea. When specifying the occurrence of CSR during sleep, we have used the term ‘‘Cheyne-Stokes respiration with central sleep apnea (CSR-CSA).’’ This term also connotes CSA in the presence of a low cardiac output state. In general, the use of the term ‘‘CSA’’ in patients with HF is synonymous with CSR or CSR-CSA.
; The characteristic waxing and waning pattern of alternating apneas and hyperpneas in CSA-CSR is readily recognized on PSG. The cycle length, found to approximate 60 s, is significantly longer than those encountered in primary CSA ,and appears to correlate with circulatory delay. The 1999 Guidelines require 5 or more central apneas or hypopneas per hour of sleep as well as at least 10 consecutive minutes of cyclic crescendo and decrescendo changes in breathing amplitude. There are scant outcome data upon which to base severity criteria in CSA-CSR. Reported variables include the central apnea index ,the central AHI, and the quantity or percentage of sleep time with periodic breathing. Lanfranchi et al. found prognostic significance in the central AHI but not in the percentage of sleep time spent with periodic breathing. Son yayınlarda periyodik solunum prevalansının iskemik kalp hastalıklarında maksimum ejeksiyon fraksiyonu %40 olan ve optimal medikal tedavi alan hastalarda %45-50 olduğu bildirilmektedir. Erkeklerde kadınlara göre ve ileri yaşta daha sık görülür. CSR can be observed both during sleep and wakefulness, although it appears to be far more common during sleep. When it occurs during sleep, it is simply a form of CSA with a prolonged hyperpnea. When specifying the occurrence of CSR during sleep, we have used the term ‘‘Cheyne-Stokes respiration with central sleep apnea (CSR-CSA).’’ This term also connotes CSA in the presence of a low cardiac output state. In general, the use of the term ‘‘CSA’’ in patients with HF is synonymous with CSR or CSR-CSA.")
33
Cheyne- Stokes Solunum Skorlanma***
Solunum amplitüdünde kreşendo ve dekreşendo gösteren en az 3 adet birbirini takip eden siklus bulunması ve aşağıdakilerden en az birinin olması 1) Uyku saati başına 5 ve üzerinde santral apne-hipopne olması 2) Kreşendo-dekreşendo siklusunun en az 10 dakikalık bir süre içinde izlenmesi
 Uyku saati başına 5 ve üzerinde santral apne-hipopne olması. 2) Kreşendo-dekreşendo siklusunun en az 10 dakikalık bir süre içinde izlenmesi.")
34
KKY’li olguların (EF<%40) %45-50’sinde
Erkeklerde ve ileri yaşta daha sık Uyku ve uyanıklıkta görülebilir Uykuda görüldüğünde CSR-CSA terimi kullanılır (düşük kardiyak output anlamına gelir)
")
35
CSR-CSA (+) olanlarda; EF daha düşük Kardiyak aritmi prevalansı yüksek
Prognoz kötü ve mortalite yüksek Cheyne-Stokes solunumu ve CSAS olan KKY’lilerde sol ventrikül ejeksiyon fraksiyonu daha düşük ve kardiyak aritmi prevalansı daha yüksektir. Prognoz daha kötü, mortalite daha yüksektir. CSS-CSAS’li KKY’lilerde mortalitenin yüksek olmasının nedeni santral uyku apnelerine bağlı olarak artmış sempatik aktivite, düşük kalp atımı, düşük barorefleks sensitivitesidir. Apneye bağlı hipoksi ve arousal, sempatik aktivite artışına yol açar. Sempatik aktivite artınca, dolaşımda katekolaminler artar ve bunlar kardiyotoksik etki yapar. Sonuçta kalp yetmezliği ağırlaşır, noktürnal kan basıncı artar, kardiyak iskemi oluşur ve mortalite yükselir

36
Kötü Prognoz ve Mortalite
Santral apnelere Artmış sempatik aktivite Düşük kalp atımı Düşük barorefleks sensitivitesi

37
SONUÇ KY ağırlaşır Noktürnal kan basıncı artar Kardiyak iskemi oluşur

38
ICSD-2 sınıflaması CSR-CSA
Polysomnographic recordings demonstrating differences in periodic breathing patterns between a patient with and without heart failure (HF). The upper panel shows a recording from a patient with idiopathic central sleep apnea (ICSA) during stage 2 sleep. Apnea length (AB) is 18 seconds, hyperpnea length (BD) is 7 seconds, and cycle length (AD) is 25 seconds. C represents the nadir of SaO2 (arterial oxygen saturation), detected by an oximeter placed on the ear in close proximity to the carotid body chemoreceptors. From the end of apnea (B) to the nadir in SaO2 (C) is the lung-to-ear circulation time (BC), which is 8 seconds and approximates lung-to carotid body circulation time. The lower panel is a recording from a patient with HF and Cheyne-Stokes respiration with central sleep apnea (CSR-CSA) during stage 2 sleep. Compared with the patient with ICSA, lung-to-ear circulation time (BC 5 26 s), hyperpnea (BD 5 46 s), and cycle lengths (AD 65 s) are substantially longer. However, apnea length (AB 5 21 s) is similar. In patients with HF and CSR, the periodic cycle duration averaged approximately 60 seconds, similar to that described by Cheyne, compared with only 35 seconds in patients with idiopathic CSA or high-altitude periodic breathing without HF (18, 28). Thus it is the presence of a prolonged hyperpnea with a waxing-waning pattern of tidal volume, and prolonged cycle duration, that distinguishes CSR from other forms of periodic breathing. Therefore, if the term ‘‘Cheyne-Stokes respiration’’ is to have any distinctive meaning, its use should be confined to periodic breathing in which the hyperpnea and cycle durations are prolonged. Since this pattern is characteristic of prolonged lung to chemoreceptor circulation time, it appears to be a manifestation of a low cardiac output as one would observe in patients with HF or bradyarrhythmias. CSR İdiopatik CSA HABD Periyodik siklus süresi 60 sn ~ 35 sn
. The upper panel shows a recording from a patient with idiopathic central sleep apnea (ICSA) during stage 2 sleep. Apnea length (AB) is 18 seconds, hyperpnea length (BD) is 7 seconds, and cycle length (AD) is 25 seconds. C represents the nadir of SaO2 (arterial oxygen saturation), detected by an oximeter placed on the ear in close proximity to the carotid body chemoreceptors. From the end of apnea (B) to the nadir in SaO2 (C) is the lung-to-ear circulation time (BC), which is 8 seconds and approximates lung-to carotid body circulation time. The lower panel is a recording from a patient with HF and Cheyne-Stokes respiration with central sleep apnea (CSR-CSA) during stage 2 sleep. Compared with the patient with ICSA, lung-to-ear circulation time (BC 5 26 s), hyperpnea (BD 5 46 s), and cycle lengths (AD 65 s) are substantially longer. However, apnea length (AB 5 21 s) is similar. In patients with HF and CSR, the periodic cycle duration averaged approximately 60 seconds, similar to that described by Cheyne, compared with only 35 seconds in patients with idiopathic CSA or high-altitude periodic breathing without HF (18, 28). Thus it is the presence of a prolonged hyperpnea with a waxing-waning pattern of tidal volume, and prolonged cycle duration, that distinguishes CSR from other forms of periodic breathing. Therefore, if the term ‘‘Cheyne-Stokes respiration’’ is to have any distinctive meaning, its use should be confined to periodic breathing in which the hyperpnea and cycle durations are prolonged. Since this pattern is characteristic of prolonged lung to chemoreceptor circulation time, it appears to be a manifestation of a low cardiac output as one would observe in patients with HF or bradyarrhythmias. CSR. İdiopatik CSA. HABD. Periyodik siklus süresi. 60 sn. ~ 35 sn.")
39
ICSD-2 sınıflaması CSR-CSA
The characteristic waxing and waning pattern of alternating apneas and hyperpneas in CSA-CSR is readily recognized on PSG (fig. 2). The cycle length, found to approximate 60 s, is significantly longer than those encountered in primary CSA [50], and appears to correlate with circulatory delay. The 1999 Guidelines require 5 or more central apneas or hypopneas per hour of sleep as well as at least 10 consecutive minutes of cyclic crescendo and decrescendo changes in breathing amplitude [1]. There are scant outcome data upon which to base severity criteria in CSA-CSR. Reported variables include the central apnea index [51], the central AHI, and the quantity or percentage of sleep time with periodic breathing [47]. Lanfranchi et al. [47] found prognostic significance in the central AHI but not in the percentage of sleep time spent with periodic breathing
. The cycle length, found to approximate 60 s, is significantly longer than those encountered in primary CSA [50], and appears to correlate with. circulatory delay. The 1999 Guidelines require 5 or more central apneas or hypopneas per hour of sleep as well as at least 10 consecutive minutes of cyclic crescendo and decrescendo changes in breathing amplitude [1]. There are scant outcome data upon which to base severity criteria in CSA-CSR. Reported variables include the central apnea index [51], the central AHI, and the quantity or percentage of sleep time with periodic breathing [47]. Lanfranchi et al. [47] found prognostic significance in the central AHI but not in the percentage of sleep time spent with periodic breathing.")
40
ICSD-2 sınıflaması CSR-CSA
It has subsequently been shown that the number of breaths in, and duration of, hyperpnea are directly proportional to the lung to peripheral chemoreceptor circulation time, and inversely proportional to cardiac output (18, 28, 29). In contrast, apnea duration bears no relation to circulation time or cardiac output.
. In contrast, apnea duration bears no relation to circulation time or cardiac output.")
41
ICSD-2 sınıflaması CSR-CSA
Klinik (Fragmente uyku) GAUH Yorgunluk
 GAUH. Yorgunluk.")
43
OSA VE SUAS ARASINDA BULGULAR AÇISINDAN FARKLAR

44
KALP YETMEZLİĞİ VE SANTRAL APNE İLİŞKİSİ

45
CSR-CSA için Risk Faktörleri
İleri yaş (>60) Erkek cinsiyet Uyanıklık hipokapnisi (≤38 mmHg) Yüksek PCWP Yüksek LV end-diastolik volümü Yüksek periferal ve santral kemoreseptör sensitivitesi Düşük LVEF
 Erkek cinsiyet. Uyanıklık hipokapnisi (≤38 mmHg) Yüksek PCWP. Yüksek LV end-diastolik volümü. Yüksek periferal ve santral kemoreseptör sensitivitesi. Düşük LVEF.")
46
CSR-CSA için Risk Faktörleri
KY’li hastaların bir kısmında CSR-CSA+OSA (+) OSA olarak başlar ve gecenin bitiminde CSA’ya shift olur [Sirkülasyon zamanı uzadıkça ve PaC02 düştükçe] In a small minority of patients with HF, OSA and CSR-CSA coexist. In one study, Tkacova and colleagues (75) demonstrated that in such patients, there was a shift from predominantly OSA at the beginning of the night to predominantly CSA at the end of the night. This shift in apnea type occurred in association with a prolongation of lung to peripheral chemoreceptor circulation time, a lengthening of hyperpnea and a fall in PaCO2 from the beginning to the end of the night. They concluded that the shift from predominantly OSA to CSR-CSA occurred in conjunction with an overnight deterioration of cardiac function. Since it has been shown that PaCO2 varies inversely with LV filling pressure, the implication was that OSA itself contributed to the deterioration of cardiac function, and that a rise in LV filling pressure contributed to the overnight decrease in PaCO2 that probably triggered CSR-CSA once PaCO2 fell below the apnea threshold. It has also been shown in patients with HF that the predominant type of sleep apnea can shift from obstructive to central in conjunction with an increase in circulation time and fall in nocturnal PaCO2, and vice versa over several months (76). These observations raise the possibility that in patients with HF, OSA and CSA can be part of a spectrum of periodic breathing whose predominant type can transform over time in response to alterations in cardiac function. Mechanisms involved in this transformation have not been identified, but may involve fluid displacement into and out of the upper airway and lungs, and alteration in chemosensitivity in relation to alteration in the severity of cardiac failure (40). 46
 OSA olarak başlar ve gecenin bitiminde CSA’ya shift olur [Sirkülasyon zamanı uzadıkça ve PaC02 düştükçe] In a small minority of patients with HF, OSA and CSR-CSA coexist. In one study, Tkacova and colleagues (75) demonstrated that in such patients, there was a shift from predominantly OSA at the beginning of the night to predominantly CSA at the end of the night. This shift in apnea type occurred in association with a prolongation of lung to peripheral chemoreceptor circulation time, a lengthening of hyperpnea and a fall in PaCO2 from the beginning to the end of the night. They concluded that the shift from predominantly OSA to CSR-CSA occurred in conjunction. with an overnight deterioration of cardiac function. Since it has been shown that PaCO2 varies inversely with LV filling pressure, the implication was that OSA itself contributed to the deterioration of cardiac function, and that a rise in LV filling pressure contributed to the overnight decrease in PaCO2 that probably triggered CSR-CSA once PaCO2 fell below the apnea threshold. It has also been shown in patients with HF that the predominant type of sleep apnea can shift from obstructive to central in conjunction with an increase in circulation time and fall in nocturnal. PaCO2, and vice versa over several months (76). These observations raise the possibility that in patients with HF, OSA and CSA can be part of a spectrum of periodic breathing whose predominant type can transform over time in response to alterations in cardiac function. Mechanisms involved in this transformation have not been identified, but may involve fluid displacement into and out of the upper airway and lungs, and alteration in chemosensitivity in relation to alteration in the severity of cardiac failure (40). 46.")
47
CSR-CSA’nın KV Etkileri
KY’li hastalarda PSG ile CSR-CSA %30-50 (+) CSR-CSA KY’ne sekonder olarak ortaya çıkar, ancak bir kez başladıktan sonra kısır bir döngüyle KV fonksiyonlarda kötüleşmeye neden olur. CSR-CSA; Basitçe bir sonuç mu? Sorunlu olan myokard üzerinde bağımsız patolojik etkileri mi var? Although CSR-CSA appears to arise secondary to HF, once initiated it may participate in a pathophysiologic vicious cycle that contributes to deterioration in cardiovascular function. However, currently debated is whether CSR-CSA is simply a reflection of severely compromised cardiac function with elevated LV filling pressure (35), or whether CSR-CSA exerts unique and independent pathologic effects on the failing myocardium. Regardless of its etiology, there is evidence that CSR-CSA may have detrimental physiologic effects on the failing heart.
 CSR-CSA KY’ne sekonder olarak ortaya çıkar, ancak bir kez başladıktan sonra kısır bir döngüyle KV fonksiyonlarda kötüleşmeye neden olur. CSR-CSA; Basitçe bir sonuç mu Sorunlu olan myokard üzerinde bağımsız patolojik etkileri mi var Although CSR-CSA appears to arise secondary to HF, once initiated it may participate in a pathophysiologic vicious cycle. that contributes to deterioration in cardiovascular function. However, currently debated is whether CSR-CSA is simply a. reflection of severely compromised cardiac function with elevated LV filling pressure (35), or whether CSR-CSA exerts unique. and independent pathologic effects on the failing myocardium. Regardless of its etiology, there is evidence that CSR-CSA. may have detrimental physiologic effects on the failing heart.")
48
EVET !!! Etyolojisinden bağımsız olarak KY’i üzerinde zararlı etkileri (+)
")
49
TEDAVİ I.Altta yatan kardiyak hastalığın optimal tedavisi
Diüretik (PCWP’nı azaltarak, met alkaloza !!!) ACE inhibitörleri (AHI ve NOD azaltır) Beta-blokör (sempatik aktivasyon) II- C02 inhalasyonu III- Oksijen tedavisi IV- Solunum stimülanları (Asetazolamid,teofilin,…) V- NIMV
 ACE inhibitörleri (AHI ve NOD azaltır) Beta-blokör (sempatik aktivasyon) II- C02 inhalasyonu. III- Oksijen tedavisi. IV- Solunum stimülanları (Asetazolamid,teofilin,…) V- NIMV.")
53
NONİNVAZİV MEKANİK VENTİLASYON TEDAVİSİ

54
CSR-CSA Tedavisinde NIMV
CPAP NOD SNA’da Naughton et al;Sempatik aktivitede azalma ile LVEF’da artmaya neden olduğu gösterilmiş. Ancak, CPAP’ın yararlı etkilerini nasıl gösterdiği tam olarak anlaşılamamıştır. Nasal CPAP has been shown to be an effective therapy for some patients with central sleep apnea.41,42 These patients probably fall into several groups. First, as stated previously, pharyngeal airway collapse or closure during sleep may initiate a reflex inhibition of ventilation in some patients and therefore a central apnea. With nasal CPAP, airway closure is prevented, and such apneas abolished. In obese, snoring patients in whom predominantly central apneas are observed, nasal CPAP may be an effective form of therapy. Second, an abstract suggests that CPAP may also be a viable form of therapy in idiopathic central sleep apnea.84 This efficacy was attributed primarily to a CPAP-induced increase in arterial PCO2. As a result, PCO2 was kept above the apnea threshold. Thus, some patients with central apnea may respond to CPAP, although the final role of this therapeutic modality in central apnea must await further investigation. CPAP has been shown to improve cardiovascular function in patients with heart failure who have central sleep apnea only when the treatment reduces the apnea–hypopnea index. Because CPAP does not attenuate central sleep apnea in patients with heart failure when the treatment is titrated over one night, we mandated a gradual upward-titration protocol. This resulted in a significant reduction in the apnea–hypopnea index, which was accompanied by an increase in nocturnal oxygen saturation that persisted for at least two years. Nonetheless, the reduction of 50 percent in the apnea–hypopnea index was less than had been achieved in previous trials with the use of similar upward titration and CPAP pressures, factors that may have contributed to the lack of a beneficial effect on clinical outcomes. Improvement in daytime LVEF may be due to several factors, including a reduction in cardiac sympathetic drive, left ventricular unloading resulting from an increase in intrathoracic pressure and reduced myocardial ischemia due to improvement in oxygen saturation.However, the increase of 2.2 percent in the LVEF was less than the increase of 7.7 percent observed in our first randomized trial. We attribute this difference to the higher initial LVEF (24.5 percent vs percent) and the greater proportion of patients receiving beta-blockers in the present trial (77 percent vs.<20 percent). Owing to the overlap in the effects of beta-blockade and CPAP on ventricular function, the potential for further improvement in the LVEF when CPAP is added may be limited. The high rate of use of beta-blockers may also have reduced the potential for a beneficial effect on clinical outcomes. One-night use of CPAP has been shown to eliminate central sleep apnea in 43% of the subjects with systolic heart failure.58 Typically, these CPAP-responsive patients had mild to moderate central sleep apnea, and the average AHI decreased from 36 to 4, with elimination of desaturation. An important observation was that the number of premature ventricular contractions, couplets, and ventricular tachycardias decreased. This effect was presumed to be due to decreased sympathetic activity because arousals decreased and saturation improved. Heart failure patients with severe central sleep apnea (57% of the patients) did not respond to CPAP, and use of CPAP had no significant effect on ventricular irritability in these patients.58 CPAP attenuated central sleep apnea and improved nocturnal oxygenation, left ventricular function, sympathetic nervous activity, and (at least initially) submaximal exercise performance. However, the CANPAP trial did not demonstrate a beneficial effect of CPAP on morbidity or mortality in these patients with central sleep apnea and heart failure. Ancak, CPAP’ın yararlı etkilerini nasıl gösterdiği tam olarak anlaşılamamıştır. Temel etkisi (primer) pre ve after loadu azaltmak (kalp çevresindeki basıncı arttırarak, transmural basıncı azaltır.) Ayrıca, plazma atriyal natriüretik peptid düzeyini düşürüp atrial duvar gerilimini önler. Tüm bu etkileriyle dispneyi düzeltir, yaşam kalitesini arttırır. Çalışmalar bir-üç aylık CPAP tedavisinin santral apne-hipopne indeksi (AHİ)’ni azalttığını, solunum sayısını düşürdüğünü, PaCO2’yi arttırdığını göstermiştir. KKY’lilerde santral uyku apnesine yol açan, uyku sırasında hiperventilasyonla birlikte hipokapnidir. Buna göre CPAP’ın solunumu düşürüp, PaCO2’yi apne eşiğinin üstüne kadar yükselttiği kabul edilebilir. Ayrıca CPAP, intratorasik basıncı arttırıp interstisyel sıvıyı ekstratorasik vasküler kompartımana çekerek pulmoner ödemi düzeltir. CPAP’la arousallar da azalır. PreLoad AfterLoad *Mortalite ? LVEF’da
 and the greater proportion of patients receiving beta-blockers in the present trial (77 percent vs.<20 percent). Owing to the overlap in the effects of beta-blockade and CPAP on ventricular function, the potential for further improvement in the LVEF when CPAP is added may be limited. The high rate of use of beta-blockers may also have reduced the potential for a beneficial effect on clinical outcomes. One-night use of CPAP has been shown to eliminate central sleep apnea in 43% of the subjects with systolic heart failure.58 Typically, these CPAP-responsive patients had mild to moderate central sleep apnea, and the average AHI decreased from 36 to 4, with elimination of desaturation. An important observation was that the number of premature ventricular contractions, couplets, and ventricular tachycardias decreased. This effect was presumed to be due to decreased sympathetic activity because arousals decreased and saturation improved. Heart failure patients with severe central sleep apnea (57% of the patients) did not respond to CPAP, and use of CPAP had no significant effect on ventricular irritability in these patients.58. CPAP attenuated central sleep apnea and improved nocturnal oxygenation, left ventricular function, sympathetic nervous activity, and (at least initially) submaximal exercise performance. However, the CANPAP trial did not demonstrate a beneficial effect of CPAP on morbidity or mortality in these patients with central sleep apnea and heart failure. Ancak, CPAP’ın yararlı etkilerini nasıl gösterdiği tam olarak anlaşılamamıştır. Temel etkisi (primer) pre ve after loadu azaltmak (kalp çevresindeki basıncı arttırarak, transmural basıncı azaltır.) Ayrıca, plazma atriyal natriüretik peptid düzeyini düşürüp atrial duvar gerilimini önler. Tüm bu etkileriyle dispneyi düzeltir, yaşam kalitesini arttırır. Çalışmalar bir-üç aylık CPAP tedavisinin santral apne-hipopne indeksi (AHİ)’ni azalttığını, solunum sayısını düşürdüğünü, PaCO2’yi arttırdığını göstermiştir. KKY’lilerde santral uyku apnesine yol açan, uyku sırasında hiperventilasyonla birlikte hipokapnidir. Buna göre CPAP’ın solunumu düşürüp, PaCO2’yi apne eşiğinin üstüne kadar yükselttiği kabul edilebilir. Ayrıca CPAP, intratorasik basıncı arttırıp interstisyel sıvıyı ekstratorasik vasküler kompartımana çekerek pulmoner ödemi düzeltir. CPAP’la arousallar da azalır. PreLoad. AfterLoad. *Mortalite LVEF’da.")
55
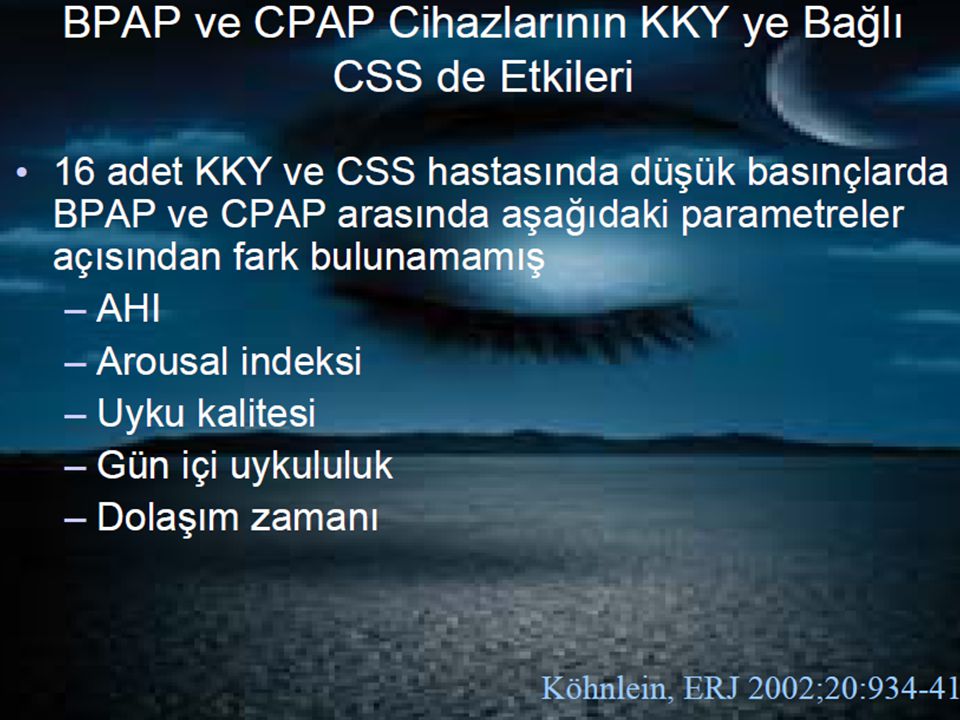
CSR-CSA NIMV CPAP çoğu CSR-CSA’ları önlemede yeterli Ø.
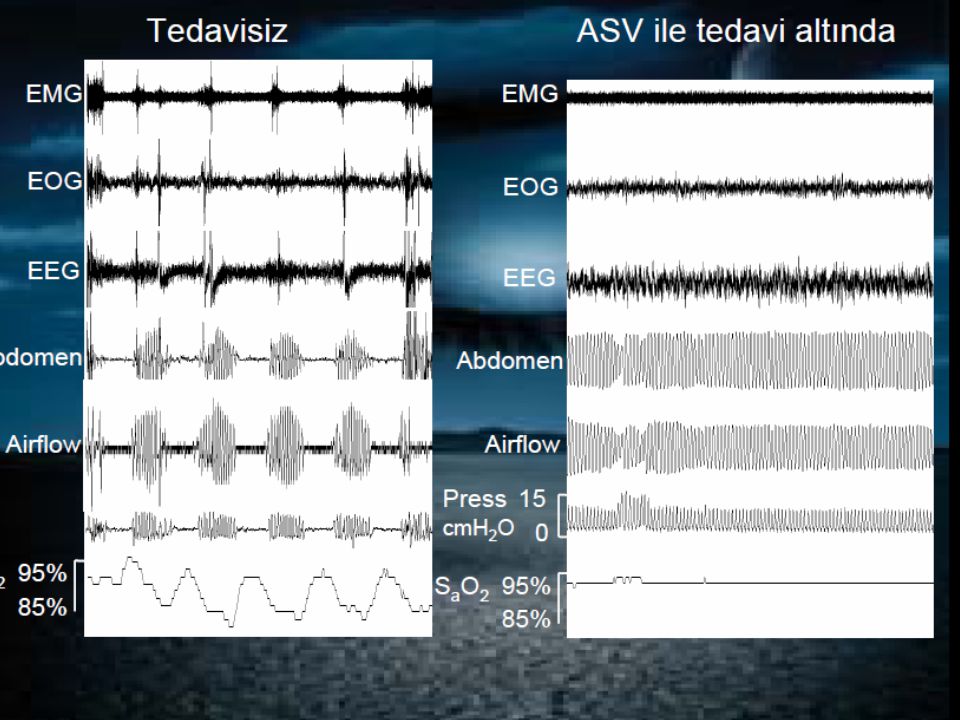
Diğer yöntemler kullanılmalı BiPAP ASV BiPAP ile ventilasyonun daha fazla arttırılması zaten hiperventile olan bu bireylerde hipokapnik alkaloz ile glottik kapanmaya neden olacaktır. Bu konuda BiPAP’ın daha yeni bir formu olan ASV’de flow jeneratörü ÜSY’daki obstrüktif olayları ortadan kaldırmaya titre edilen fiks bir end-ekspiratuar basınç üretir. İnspiratuar basınç desteği ise bir algoritmaya uygun olarak ventilasyonu; SON 3 DK İÇİNDEKİ bazal dakika ventilasyonunun yaklaşık olarak %80’ninde stabilize etmeyi amaçlayan bir şekilde değişir. Daha iyi sonuçları (+), uyum daha iyi. Adaptive servo-ventilation (ASV) utilizes an algorithm to analyze a patient’s ventilatory rhythm and estimates a minute ventilation with which to target support. While providing support during apneas and hypopneas, ASV is designed to avoid overventilation during the hyperpneic phase, promoting more uniform ventilation and reducing arousals from sleep. Previously available only outside of the U.S., the ASV mode recently received FDA approval and is targeted for U.S. distribution in ASV has been shown to effectively suppress CSA-CSR and may be preferred over CPAP by patients [51, 81]. A 1-month randomized trial comparing therapeutic ASV with subtherapeutic ASV showed significant improvements in daytime sleepiness and reductions in neurohormonal activity associated with active treatment in patients with stable HF and CSR-CSA [82]. A recent randomized crossover trial has demonstrated superiority of ASV over CPAP and NPPV in normalizing breathing and sleep parameters in patients with CSA syndromes with and without HF ASV, KY ve CSS olan hastaların tedavisinde son zamanlarda önerilen yeni bir NIMV tedavi modalitesidir. ASV, hedef ventilasyonu, hastaların son zamanlardaki ortalama ventilasyonunun % 90’ına eşit olarak ayarlar. Bu devamlı olarak güncellenen hedef, ASV’nin “adaptif” kısmıdır. ASV solunumdan solunuma, solunumsal desteği, hastaların ihtiyacına göre değişen miktarlarda verme kapasitesine sahiptir. CSS’nin kontrol altına alındığı kararlı durumda, düzleşmiş dalga formları kullanılarak, 5 cmH2O pozitif basıncın üzerine eklenen, 3 cmH2O basınç desteği verir. Küçük miktarlardaki pozitif basınç desteği; dispnenin, artmış önyükün ve pulmoner ödemin azaltılmasına yardım eder. Eğer hasta santral apne ya da hipopneye girerse, basıncın derecesi çok hızlı bir şekilde, solunum stabilize olana kadar (ya da ayarlanan maksimum 10 cmH2O’ya kadar) birkaç solunumda artırılır. Eğer hasta hiperpneye girerse ya da noktürnal solunum yeniden başlarsa, basıncın derecesi 3-4 solunumda azaltılır ve solunum stabilizasyonuna daha fazla yardım eder. Bu ASV’nin “servoventilasyon” kısmıdır. Özet olarak; ASV, ayarlanan bir solunum hızında, ekspiryum sonu pozitif basıncına ek olarak hastanın ihtiyacına göre (hiperpne-hipopne veya apnede olmasına göre) inspiryumda da uygun pozitif hava yolu basıncı vererek, CSS’ nu kontrol altına alır (77). Solunum stabilize olduktan sonra, ASV basıncın derecesini konforlu, minimum 3 cmH2O desteğe doğru, kademeli olarak azaltır ve böylece aşırı ventilasyon olasılığını azaltır. Basınç derecesinin otomatik olarak azaltılması önemlidir. Aşırı ventilasyon ve hipokapni vokal kord kapanmasına ve apnede artışa neden olur (77). ASV, KY olgularındaki uyku sırasında yaşanan santral apneleri, hipopneleri, arousalları, uyku bölünmelerini engelleyerek, aşırı yorgunluk ve uykululuk halini tedavi eder
, uyum daha iyi. Adaptive servo-ventilation (ASV) utilizes an algorithm to analyze a patient’s ventilatory rhythm and estimates a minute ventilation with which to target support. While providing support during apneas and hypopneas, ASV is designed to avoid overventilation during the hyperpneic. phase, promoting more uniform ventilation and reducing arousals from sleep. Previously available only outside of the U.S., the ASV mode recently received FDA approval and is targeted for U.S. distribution in ASV has been shown to effectively suppress CSA-CSR and may be preferred over CPAP by patients [51, 81]. A 1-month randomized trial comparing therapeutic ASV with subtherapeutic ASV showed significant improvements in daytime sleepiness and reductions in neurohormonal activity associated with active treatment in patients with stable HF and CSR-CSA [82]. A recent randomized crossover trial has demonstrated superiority of ASV over CPAP and NPPV in normalizing breathing. and sleep parameters in patients with CSA syndromes with and without HF. ASV, KY ve CSS olan hastaların tedavisinde son zamanlarda önerilen yeni bir NIMV tedavi modalitesidir. ASV, hedef ventilasyonu, hastaların son zamanlardaki ortalama ventilasyonunun % 90’ına eşit olarak ayarlar. Bu devamlı olarak güncellenen hedef, ASV’nin adaptif kısmıdır. ASV solunumdan solunuma, solunumsal desteği, hastaların ihtiyacına göre değişen miktarlarda verme kapasitesine sahiptir. CSS’nin kontrol altına alındığı kararlı durumda, düzleşmiş dalga formları kullanılarak, 5 cmH2O pozitif basıncın üzerine eklenen, 3 cmH2O basınç desteği verir. Küçük miktarlardaki pozitif basınç desteği; dispnenin, artmış önyükün ve pulmoner ödemin azaltılmasına yardım eder. Eğer hasta santral apne ya da hipopneye girerse, basıncın derecesi çok hızlı bir şekilde, solunum stabilize olana kadar (ya da ayarlanan maksimum 10 cmH2O’ya kadar) birkaç solunumda artırılır. Eğer hasta hiperpneye girerse ya da noktürnal solunum yeniden başlarsa, basıncın derecesi 3-4 solunumda azaltılır ve solunum stabilizasyonuna daha fazla yardım eder. Bu ASV’nin servoventilasyon kısmıdır. Özet olarak; ASV, ayarlanan bir solunum hızında, ekspiryum sonu pozitif basıncına ek olarak hastanın ihtiyacına göre (hiperpne-hipopne veya apnede olmasına göre) inspiryumda da uygun pozitif hava yolu basıncı vererek, CSS’ nu kontrol altına alır (77). Solunum stabilize olduktan sonra, ASV basıncın derecesini konforlu, minimum 3 cmH2O desteğe doğru, kademeli olarak azaltır ve böylece aşırı ventilasyon olasılığını azaltır. Basınç derecesinin otomatik. olarak azaltılması önemlidir. Aşırı ventilasyon ve hipokapni vokal kord kapanmasına ve apnede artışa neden olur (77). ASV, KY olgularındaki uyku sırasında yaşanan santral apneleri, hipopneleri, arousalları, uyku bölünmelerini engelleyerek, aşırı yorgunluk ve uykululuk halini tedavi eder.")
59
ASV vs CPAP AHI Üzerine % Etki C Philippe, M Stoïca-Herman, X Drouot et al. Heart 92:337-342, 2006

60
Yüksek irtifada periyodik solunuma bağlı santral uyku apnesi
7600 m ve üstünde sık Hipoksik ve hiperkapnik yanıtı yüksek bireyler TANI:En az 4000 m’ye çıkmış olmak ve SAI>5 ve siklus süresi12-34 sn arasında

61
Santral apne ve hiperpne periyotları ile karekterize
Santral tipte apnelerin ardından hiperpneik solunum gözlenir. Bu tip siklusların süresi genellikle 12 sn – 34 sn aralığında seyreder.

62
Yüksek irtifada periyodik solunuma bağlı santral uyku apnesi
Sık uyanma, uyku kalitesinde bozukluk ve boğulma hissi Aynı irtifada zamanla düzelir

63
Cheyne-Stokes dışında tıbbi durumlara bağlı santral uyku apnesi
1. Tıbbi bir bozukluğa ikincil 2. Cheyne-Stokes solunumunun özellikleri yoktur 3. Beyin sapı lezyonları, kardiyak ve renal bozukluklar sonucu gelişebilir

64
Medikal Sorunlara Bağlı Santral Uyku Apnesi
Shy-Drager sendromu (multipl santral sistem atrofisi) •Ailesel disotonomi, •Diabetes mellitusabağlıotonom nöropati •Poliomyelit •Tümör, infarkt, hemoraji veya ensefalit •Servikal kordotomi. •müsküler distrofi •myastenia gravis
 •Ailesel disotonomi, •Diabetes mellitusabağlıotonom nöropati. •Poliomyelit. •Tümör, infarkt, hemoraji veya ensefalit. •Servikal kordotomi. •müsküler distrofi. •myastenia gravis.")
65
İlaçlara bağlı santral uyku apne sendromu
Narkotikler ve Opiodler (codeine)*** Qubain (dijital) Cisapride V.s
*** Qubain (dijital) Cisapride. V.s.")
66
Top, A: An example of a patient receiving high-dose opioid medication for back pain experiencing repetitive central apneas as demonstrated by a lack of movement of respiratory effort bands (both abdominal and thoracic) with associated oxygen desaturations. Top, A: An example of a patient receiving high-dose opioid medication for back pain experiencing repetitive central apneas as demonstrated by a lack of movement of respiratory effort bands (both abdominal and thoracic) with associated oxygen desaturations. Bottom, B: Marked improvement in SDB following gradual dose reduction of opioid medication. Sao2 = arterial oxygen saturation Eckert D J et al. Chest 2007;131: ©2007 by American College of Chest Physicians
 with associated oxygen desaturations. Bottom, B: Marked improvement in SDB following gradual dose reduction of opioid medication. Sao2 = arterial oxygen saturation. Eckert D J et al. Chest 2007;131: ©2007 by American College of Chest Physicians.")
67
Çocukluk çağı primer santral uyku apnesi
REM evresinde apne/hipopnelerle karekterizedir Apneler obstrüktif, santral veya mikst tip olabilir Santral apneler kalp veya beyin (santral) nedenlidir Erken doğum sonrası doğan bebeklerde görülür ve çoğunlukla miks tip apnelerdir. Daha büyük çocuklarda santral tiptedir Apneler kısa sürelidir, 20 sn’i geçmez Bunlarda hipoksemi ve düşük kalp hızı saptanır. Buna bağlı bilinç yitimi olabilir Apnelerin beyin gelişim eksikliği veya medikal durumlara bağlı olduğu düşünülmektedir
 nedenlidir. Erken doğum sonrası doğan bebeklerde görülür ve çoğunlukla miks tip apnelerdir. Daha büyük çocuklarda santral tiptedir. Apneler kısa sürelidir, 20 sn’i geçmez. Bunlarda hipoksemi ve düşük kalp hızı saptanır. Buna bağlı bilinç yitimi olabilir. Apnelerin beyin gelişim eksikliği veya medikal durumlara bağlı olduğu düşünülmektedir.")
68
Santral Uyku Apnesi Ayırıcı Tanısı

69
TEŞEKKÜRLER

Benzer bir sunumlar













>")



>")


