Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Prof. Dr. Metin ÖZKAN GATA Göğüs Hastalıkları
Exhale Nitrik Oksit Prof. Dr. Metin ÖZKAN GATA Göğüs Hastalıkları 1

2
Giriş 1987’ye kadar hava kirliliğinin bir komponenti
NO en çok çalışılan ekshale markır PubMed’de > 1500 yayın 1987’ye kadar hava kirliliğinin bir komponenti 1987’den sonra o güne kadar tanımlanmamış olan “endothelial-derived relaxing factor” Respiratuar sistemde: Vasküler ve bronşial tonusu regüle eder (dilatasyon) Siliyer epitelin koordineli çalışmasını sağlar Nörotransmitter (bronş duvarındaki “non-adrenerjik non-kolinerjik nöronlar) Sağlıklı veya hasta kişilerde Ekshale havada saptanabilir
 Siliyer epitelin koordineli çalışmasını sağlar. Nörotransmitter (bronş duvarındaki non-adrenerjik non-kolinerjik nöronlar) Sağlıklı veya hasta kişilerde Ekshale havada saptanabilir.")
3
NO Sentezi Exhaled Markers of Pulmonary Disease
KHARITONOV SA and BARNES PJ. Am J Respir Crit Care Med Vol 163. pp 1693–1722, 2001

5
Barnes PJ. NO or no NO in asthma.Thorax 1996;51:218-220

6
Yararlı etkileri İnsan hava yollarında NANC nöronal inhibitör yanıtla kolinerjik bronkokonstriksiyonu engeller. Kısa yarı ömrü nedeniyle inhalasyonu durumunda bronkodilatör etkisi beklendiği gibi değil. NOS inhibitörlerinin histamin ve bradikininin bronkokonstriktör etkilerini azaltması NO’nun koruyucu etkisini göstermekte

7
Yararlı etkileri Mukosiliyer klirensi regüle eder - NOS inhibitörleri hava yolu epitel hücrelerinde siliyer vuru frekansını azaltmakta. Düşük konsantrasyonlarda plazma eksudasyonunu azaltmakta. Bakteri, virüs ve parazitlere toksik etkili

8
Zararlı etkileri Inflamatuar yanıt – astımda hava yolu obstrüksiyonunda ve semptomlarda artış Vazodilatasyon – astmatik hava yollarında hiperemide artış Gevşek postkapiller venüllere kan akımında artış – hava yolu ödeminde artış Pulmoner damarlarda vazodilatasyon - V/Q dengesizliği Artmış mukus sekresyonu

9
Zararlı etkileri Astımdaki eozinofilik inflamasyon IL-4 ve IL-5 salgılayan Th2 hücrelerce regüle edilir. Th1 ise salgıladığı interferon gama ile Th2 hücrelerin proliferasyonunu baskılar. NO Th1’i inhibe ederek dolaylı yoldan Th2 lenfositlerin sekresyonunu artırarak inflamasyona katkıda bulunur

10
eNO (FeNO) İlk olarak 1991 yılında ppb seviyesinde chemiluminescence analizi ile saptandı Gustafsson LE et al. Biochem Biophys Res Commun 1991 Dec 16;181(2):852-7 FeNO ölçmenin yararları Kortikosteroid kullanmayan astım hastalarında doğru tanının konması Kronik öksürük ayırıcı tanısı Egzersize bağlı bronkokonstriksiyon-astım KOAH – astım ayrımı Astım, KOAH veya nonspesifik solunumsal semptomları olan olgularda uygun kortikosteroid yanıtının gösterilmesi Astım kontrolünün ve sürdürülmesinin sağlanması Astım atağının öngörülmesi Astım tedavisinin monitorizasyonu
: FeNO ölçmenin yararları. Kortikosteroid kullanmayan astım hastalarında doğru tanının konması. Kronik öksürük ayırıcı tanısı. Egzersize bağlı bronkokonstriksiyon-astım. KOAH – astım ayrımı. Astım, KOAH veya nonspesifik solunumsal semptomları olan olgularda uygun kortikosteroid yanıtının gösterilmesi. Astım kontrolünün ve sürdürülmesinin sağlanması. Astım atağının öngörülmesi. Astım tedavisinin monitorizasyonu.")
11
ATS/ERS FeNO ölçüm Klavuzu
NO düşük (< 5ppb) hava inhalasyonu Ekspratuar dirence karşı ekshalasyon ATS & ERS FeNO GUIDELINES Akım hızı 50 mL/s (1999 ATS statement) Oral alım x 2 saat önce Kafein alımı yok Bronkodilatör x 6 saat American Thoracic Society, European Respiratory Society. Am J Respir Crit Care Med. 2005;171(8):
 hava inhalasyonu. Ekspratuar dirence karşı ekshalasyon. ATS & ERS. FeNO GUIDELINES. Akım hızı 50 mL/s (1999 ATS statement) Oral alım x 2 saat önce. Kafein alımı yok. Bronkodilatör x 6 saat. American Thoracic Society, European Respiratory Society. Am J Respir Crit Care Med. 2005;171(8):")
12
EKSHALE NO ÖLÇÜMÜ online offline Ekspratuar akım (50ml/s)
Nazal NO kontaminasyonun önlenmesi (belli bir dirence karşı tek ekshalasyon)
")
13
Dirence karşı ekshalasyon ile yumuşak damağın kapanması ve nazal kontaminasyonun önlenmesi amaçlanmakta. Aynı anda CO2 ölçümü ekshale gazın kaynağını göstermekte eNO başlangıçta üst hava yollarında sentezlenen yüksek NO nedeniyle pik yapar ve daha sonra plato çizer Smith AD and Taylor DR. Current Opinion in Allergy and Clinical Immunology 2005, 5:49–56

14
FENO’nun akım hızı bağımlılığı
Silkoff et al., AJRCCM 1997 14

15
Ekshale NO Ölçümünü etkileyen faktörler
Farmakolojik Papaverin Oxymetazoline Sodium nitroprusside L-arginine ACE inhibitörleri (enalapril) Fizyolojik ve işlemsel Arginine alımı, nitrit/nitrat’dan zengin besinler Çevresel ve mesleksel Hava kirliliği (NO, ozon) Cep telefonlarını oluşturduğu elektromanyetik alan (nazal NO) Enfeksiyonlar Üst solunum yolu enfeksiyonları Farmakolojik Oxymetazoline NOS inhibitörleri Fizyolojik ve işlemsel Tekrarlanan spirometri Fiziksel egzersiz Menstrüel siklus Balgam varlığı Vucut ısı düşüşü Alışkanlık Sigara Alkol alımı
 Fizyolojik ve işlemsel. Arginine alımı, nitrit/nitrat’dan zengin besinler. Çevresel ve mesleksel. Hava kirliliği (NO, ozon) Cep telefonlarını oluşturduğu elektromanyetik alan (nazal NO) Enfeksiyonlar. Üst solunum yolu enfeksiyonları. Farmakolojik. Oxymetazoline. NOS inhibitörleri. Fizyolojik ve işlemsel. Tekrarlanan spirometri. Fiziksel egzersiz. Menstrüel siklus. Balgam varlığı. Vucut ısı düşüşü. Alışkanlık. Sigara. Alkol alımı.")
16
REFERANS DEĞERLER 1131 hiç sigara içmemiş sağlıklı denek
FENO oturur pozisyonda ölçülüyor (NIOX:Aerocrine AB; Sockholm, Sweden) Akım hızı 50 ml/s Tüm grupta FENO geometrik ortalaması 16.6 ppb (95% RI, 5.87 to 47.14) FENO nonatopiklerle karşılaştırıldığında atopiklerde daha yüksek saptanıyor; sırasıyla 18.8 ppb (95% RI, 6.03 to 58.74) 16.0 ppb (95% RI, 5.91 to 58.76). Benzer boy ve yaşta FENO cinsiyet farkı göstermiyor
 Akım hızı 50 ml/s. Tüm grupta FENO geometrik ortalaması 16.6 ppb (95% RI, 5.87 to 47.14) FENO nonatopiklerle karşılaştırıldığında atopiklerde daha yüksek saptanıyor; sırasıyla 18.8 ppb (95% RI, 6.03 to 58.74) 16.0 ppb (95% RI, 5.91 to 58.76). Benzer boy ve yaşta FENO cinsiyet farkı göstermiyor.")
17
Boy ve yaşa göre üst limitler 24.0 ile 54.0 ppb arasında değişiyor.
FENO boy ve yaşla değişiyor Boy ve yaşa göre üst limitler 24.0 ile 54.0 ppb arasında değişiyor.

18
Ekshale nitrik oksit için referans değerler (reveno çalışması)
Amaç erişkinlerde FENO referans değerlerini saptamak FENO sigara içmeyen normal spirometreli 204 sağlıklı kişide ölçülüyor Ana sonuç: erkek ve bayanlarda anlamlı fark. 50 ml/s akım hızında FENO erkeklerde 2.6 ile 28.8 ppb arasında, bayanlarda 1.6 ile 21.5 ppb arasında saptanıyor. Oliveri M et al. Respir Res. 2006;7:94.

19
Cinsiyet farkının eNO’ya etkisi N= 204 sağlıklı sigara içmeyen sağlıklı erişkin
FENO ppb Akım ml/s *p<0.01 **p<0.001 14 12 10 8 6 4 2 50 100 150 200 * ** male female FENO measured in 204 healthy non-smoking adults (age years) Significant differences observed in FENO levels between male and female Normal range of FENO: 2.6 to 28.8 ppb in men and 1.6 to 21.5 ppb in women The above study by Oliveri et al. was conducted to establish adult FENO reference values according to the international guidelines FENO was measured in 204 healthy, non-smoking adults with normal spirometry values using the on-line single-breath technique, and the results were analysed chemiluminescently Results: The main result of the study was the significant difference in FENO values between men and women, thus indicating that gender-based reference FENO values are necessary. The FENO levels obtained at expiratory flows of 50 ml/s ranged from 2.6 to 28.8 ppb in men, and from 1.6 to 21.5 ppb in women. Additionally, no association of FENO with age was observed among all adults in this study Oliveri M et al. Respir Res. 2006;7:94. * Reference: Olivieri M et al. Reference values for exhaled nitric oxide (reveno) study. Respir Res. 2006;7:94. 19
 Significant differences observed in FENO levels between male and female. Normal range of FENO: 2.6 to 28.8 ppb in men and 1.6 to 21.5 ppb in women. The above study by Oliveri et al. was conducted to establish adult FENO reference values according to the international guidelines. FENO was measured in 204 healthy, non-smoking adults with normal spirometry values using the on-line single-breath technique, and the results were analysed chemiluminescently. Results: The main result of the study was the significant difference in FENO values between men and women, thus indicating that gender-based reference FENO values are necessary. The FENO levels obtained at expiratory flows of 50 ml/s ranged from 2.6 to 28.8 ppb in men, and from 1.6 to 21.5 ppb in women. Additionally, no association of FENO with age was observed among all adults in this study. Oliveri M et al. Respir Res. 2006;7:94. * Reference: Olivieri M et al. Reference values for exhaled nitric oxide (reveno) study. Respir Res. 2006;7:")
20
Toplum çalışmalarında FENO için referans değerler ve üst limitler
FeNO çok değişken. Erişkinlerde, yaş – FENO ilişkisi çok açık değil. Çocuklarda, yaş – FENO arasında pozitif korelasyon Buchvald ve ark. FeNO’nun 15 ppb ile 25 ppb arasında değiştiğini ve her yıl için 1 ppb arttığını göstermişler Cinsiyet Akut ve kronik sigara içimi Üst solunum yolu enfeksiyonları Hashir Majid. Current Opinion in Pulmonary Medicine 2010, 16:42–47

21
Hava yolu hastalığı olan olgularda FENO değerlerinin yorumlanması
Düşük Normal Orta Yüksek Eozinophhilic inflammation Olası değil Var, hafif Ciddi oranda < 5ppb 5-25ppb 25-50ppb > 50ppb Olası: smoker Çocuk: PCD Kistik fibrozis Semptomatikse tanıyı gözden geçir. Asemptomatik ve tedavi altında ise: Hasta uyumlu Doz azaltılması? Klinik tabloya göre yorumlanmalı Semptomatik hastalarda muhtemelen antiinflamatuar tedaviye yanıt alınacak. Eğer ICS tedavisi alıyorsa kompliansda problem olabilir Allerjen yüklenmesini düşün, olası alevlenme Thorax 2006

22
eNO - Astım Yaygın olarak araştırılan belirteç.
Noninvaziv Tekrarlanabilir Hastalık aktivitesini gösteren diğer belirteçlerle korele Balgam eozinofil sayısı Hava yolu aşırı duyarlılığı Bronkodilatör yanıt Astım semptomları

23
Astım eNO artışı bir çok çalışmada gösterilmiştir.
Kharitonov SA. Lancet 1994;343:133–135 Persson MG. Lancet 1994;343:146–147.

24
Astım yönetiminde FENO ölçümünün yararlarının kanıt dereceleri
Kanıt derecesi Potansiyel uygulama Astımda FENO artışı 5 Tanı FENO’da steroid tedavisiyle azalma Monitorizasyon ve yanıt değerlendirmesi FENO’da diğer antiinflamatuar ilaçlarla (örn, lökotrien antagonistleri, anti-IgE) 2,3 FENO’da tedavi kesilince artma Komplians kontrolü FENO’nun eozinofilik inflamasyonla korelasyonu 2–3 İnflamatuar komponent monitorizasyonu FENO’nun diğer inflamatuar komponentlerle korelasyonu 0–1 FENO’nun ataklarda artışı 3 Atak değerlendirmesi FENO’nun atağın gelişini öngörmesi 1,2 Atak öngörüsü Astım kontrolü, QOL, sağlık harcamaları vs. konularda ilerleme sağlamak için NO inhibisyonuna yönelik tedaviler Uzun süreli kontrolün sağlanması Yeniden yapılanmanın, FEV1 düşüşünün vs. önlenmesinde FENO’nun hedeflenmesi Güzel bir düş Kısaltmalar: QOL yaşam kalitesi. Kanıt dereceleri: : 5: 10 yayın; 4: 6–9 yayın; 3: 3–5 yayın; 2: 1–2 yayın; 0: yayın yok. ATS Workshop Proceedings: Exhaled Nitric Oxide and Nitric Oxide Oxidative Metabolism in Exhaled Breath Condensate. Proc Am Thorac Soc Vol 3. pp 131–145, 2006
 2,3. FENO’da tedavi kesilince artma. Komplians kontrolü. FENO’nun eozinofilik inflamasyonla korelasyonu. 2–3. İnflamatuar komponent monitorizasyonu. FENO’nun diğer inflamatuar komponentlerle korelasyonu. 0–1. FENO’nun ataklarda artışı. 3. Atak değerlendirmesi. FENO’nun atağın gelişini öngörmesi. 1,2. Atak öngörüsü. Astım kontrolü, QOL, sağlık harcamaları vs. konularda ilerleme sağlamak için NO inhibisyonuna yönelik tedaviler. Uzun süreli kontrolün sağlanması. Yeniden yapılanmanın, FEV1 düşüşünün vs. önlenmesinde FENO’nun hedeflenmesi. Güzel bir düş. Kısaltmalar: QOL yaşam kalitesi. Kanıt dereceleri: : 5: 10 yayın; 4: 6–9 yayın; 3: 3–5 yayın; 2: 1–2 yayın; 0: yayın yok. ATS Workshop Proceedings: Exhaled Nitric Oxide and Nitric Oxide Oxidative Metabolism in Exhaled Breath Condensate. Proc Am Thorac Soc Vol 3. pp 131–145,")
25
Gelecekteki olası astımın öngörülmesi
eNO – astımın “subklinik” formlarının saptanması (normal akciğer fonksiyonları, negatif bronkodilatör testler ve artmış balgam eozinofilik katyonik protein konsantrasyonları) Hava yolu inflamasyonunun erken tanısı- kortikosteroidle tedavi – klinik olarak manifest astımın önlenmesi
 Hava yolu inflamasyonunun erken tanısı- kortikosteroidle tedavi – klinik olarak manifest astımın önlenmesi.")
26
Gelecekteki olası astımın öngörülmesi
Bu yüksek risk grubunda eNO ve PC20 testlerinin birleştirilmesi allerjik astımın saptanmasında daha spesifiktir. Bu durum Norveç’te 8000 erişkinle yapılan bir çalışmada incelendi. NO ölçümü bu tür geniş popülasyonların taranmasında maliyet etkin olabilir.

27
Eur Respir J 2000; 15: 849±855 Amaç: AHR ve eNO birlikte veya ayrı ayrı ölçüldüğünde astmatik ve sağlıklı kişileri ayırmada yararlı olabilir mi? 8,571 erişkin Polen, hayvan veya ev tozlarına maruz kaldığında astım semptomları tanımlayanların oranı %7.8 (şüpheli astım grubu) iken %56’sında astım veya allerjik semptom saptanmamış (kontrol grubu). Bu gruplardan sırasıyla 151 ve 213 erişkin allerji taraması, eNO ve metakolinle bronş provakasyon testlerine tabi tutulmuş.
 iken %56’sında astım veya allerjik semptom saptanmamış (kontrol grubu). Bu gruplardan sırasıyla 151 ve 213 erişkin allerji taraması, eNO ve metakolinle bronş provakasyon testlerine tabi tutulmuş.")
28
Eur Respir J 2000; 15: 849±855 Atopik ve nonatopiklerde eNO a) 131 astım şüphesi olan b) 187 kontrol. Geometrik ortalama: atopik astımlılar, 11.7 ppb; nonatopik astımlıar, 5.6 ppb; atopik kontrol vakaları, 6.4 ppb; nonatopik kontrol vakaları, 5.3 ppb.
 131 astım şüphesi olan b) 187 kontrol. Geometrik ortalama: atopik astımlılar, 11.7 ppb; nonatopik astımlıar, 5.6 ppb; atopik kontrol vakaları, 6.4 ppb; nonatopik kontrol vakaları, 5.3 ppb.")
29
Eur Respir J 2000; 15: 849±855 ENO ve DDR (dose response ratio to methacholine) pozitif korelasyon gösterdi. (r=0.41, p<0.001). ENO nonatopiklere göre atopiklerde anlamlı yüksek saptandı (sırasıyla 11.7 ppb ve 5.6 ppb, p<0.001). AHR pozitif olan ve atopisi olan olgularda en yüksek ENO elde edildi (14.2 ppb). Sonuç olarak; tek başına ENO ölçümü astım tanısı için toplum taramalarında yeterli değil, bunun AHR ile birlikte ölçülmesi allerjik astım tanısı için oldukça spesifiktir.
 pozitif korelasyon gösterdi. (r=0.41, p<0.001). ENO nonatopiklere göre atopiklerde anlamlı yüksek saptandı (sırasıyla 11.7 ppb ve 5.6 ppb, p<0.001). AHR pozitif olan ve atopisi olan olgularda en yüksek ENO elde edildi (14.2 ppb). Sonuç olarak; tek başına ENO ölçümü astım tanısı için toplum taramalarında yeterli değil, bunun AHR ile birlikte ölçülmesi allerjik astım tanısı için oldukça spesifiktir.")
30
Berry M et al. Eur. Respir J. 2005; 25: 986-991
Astımlı erişkinlerde alveoler NO: Distal akciğer inflamasyonunun kanıtı Berry M et al. Eur. Respir J. 2005; 25:

32
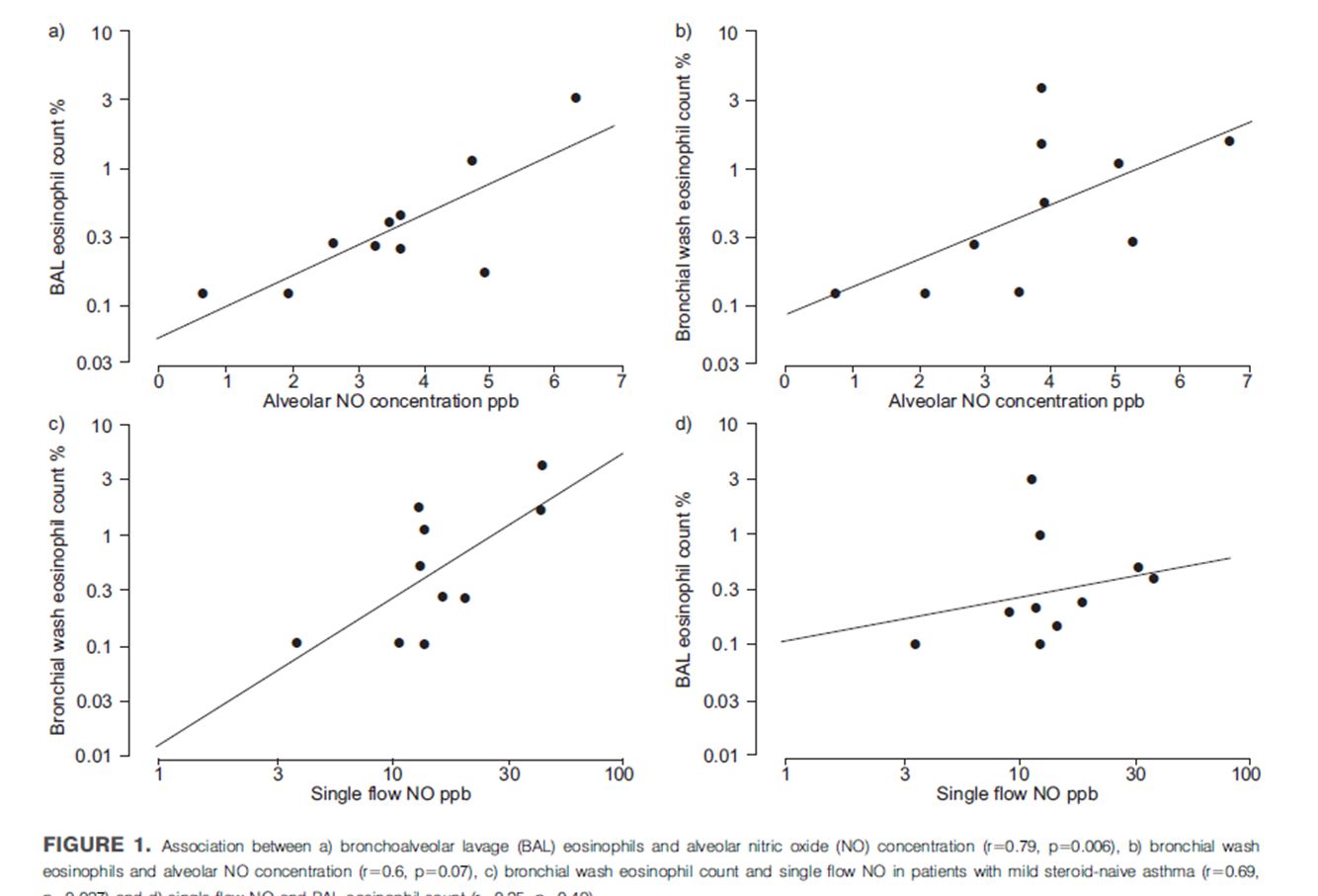
Astımlı erişkinlerde alveoler NO: Distal akciğer inflamasyonunun kanıtı
ENO, 10, 30, 50, 100 ve 200 mLs-1 akım hızlarında ölçümler yapıldı. CE=CWx(1-exp(-DNO/V))+CALVxexp(-DNO/V) Alveoler NO konsantrasyonu ppb Normal Hafif-orta asım Refrakter astım 20 15 10 5 *** NS Alveolar NO concentration was calculated for each patient using a nonlinear model described by SILKOFF et al. [5]. Briefly, exhaled NO and exhalation flow were used to resolve the following nonlinear equation CE~CW|(1{exp({DNO=V))zCALV|exp({DNO=V) ð1Þ In this equation, CE is the exhaled concentration of NO, CW is the airway wall concentration of NO, DNO is the diffusion constant for NO, V is the exhalation flow and CALV in the alveolar NO concentration. Maximal bronchial NO output was calculated using a linear method described by TSOUKIAS and GEORGE [4], where NO output is plotted against exhalation flow and the intercept recorded as the maximal bronchial NO output. Repeatability was assessed using intraclass correlation coefficient and SD of within subject SD. The current study by Berry et al. tested the hypothesis that alveolar NO concentration is a measure of inflammation in the distal lung (as reflected by BAL eosinophil count) and that increased alveolar NO concentration is a feature of refractory asthma. The authors also assessed the effect of 2 weeks of prednisolone (30 mg q.d.) on alveolar NO concentration. The study included patients who fulfilled the ATS criteria for refractory asthma (n=13), healthy volunteers (n=27) and those with mild to moderate asthma (n=25). Exhaled NO concentration was measured at 10, 30, 50, 100 and 200 mL s-1 using NIOX (Aerocrine, Stockholm, Sweden) analyzer in addition and prior to other measurements such as spirometry and methacholine PC20. Results: Alveolar NO concentration was both measurable and repeatable in patients with refractory asthma. A positive correlation was observed between alveolar NO concentration and BAL eosinophil count. Alveolar NO concentration was increased in patients with refractory asthma (7.1 ppb) compared with mild to moderate asthma (3.4 ppb) and normal controls (3.4ppb) and reduced by treatment with prednisolone. Conclusions: Distal lung inflammation is present in refractory asthma Alveolar NO is a potentially useful technique for investigating the role of distal lung inflammation in asthma and other airway diseases steroid naive sadece inhale steroid kullananlar oral ve inhaler steroid tedavisi Berry M et al. Eur. Respir J. 2005; 25: ***p,0.001; NS: Non-significant. Reference: 1. Berry M et al. Alveolar nitric oxide in adults with asthma: evidence of distal lung inflammation in refractory asthma. Eur Respir J. 2005; 25: 32
)+CALVxexp(-DNO/V) Alveoler NO konsantrasyonu ppb. Normal. Hafif-orta asım. Refrakter astım *** NS. Alveolar NO concentration was calculated for each patient. using a nonlinear model described by SILKOFF et al. [5]. Briefly, exhaled NO and exhalation flow were used to resolve the. following nonlinear equation. CE~CW|(1{exp({DNO=V))zCALV|exp({DNO=V) ð1Þ. In this equation, CE is the exhaled concentration of NO, CW is. the airway wall concentration of NO, DNO is the diffusion. constant for NO, V is the exhalation flow and CALV in the. alveolar NO concentration. Maximal bronchial NO output was. calculated using a linear method described by TSOUKIAS and. GEORGE [4], where NO output is plotted against exhalation. flow and the intercept recorded as the maximal bronchial NO. output. Repeatability was assessed using intraclass correlation. coefficient and SD of within subject SD. The current study by Berry et al. tested the hypothesis that alveolar NO concentration is a measure of inflammation in the distal lung (as reflected by BAL eosinophil count) and that increased alveolar NO concentration is a feature of refractory asthma. The authors also assessed the effect of 2 weeks of prednisolone (30 mg q.d.) on alveolar NO concentration. The study included patients who fulfilled the ATS criteria for refractory asthma (n=13), healthy volunteers (n=27) and those with mild to moderate asthma (n=25). Exhaled NO concentration was measured at 10, 30, 50, 100 and 200 mL s-1 using NIOX (Aerocrine, Stockholm, Sweden) analyzer in addition and prior to other measurements such as spirometry and methacholine PC20. Results: Alveolar NO concentration was both measurable and repeatable in patients with refractory asthma. A positive correlation was observed between alveolar NO concentration and BAL eosinophil count. Alveolar NO concentration was increased in patients with refractory asthma (7.1 ppb) compared with mild to moderate asthma (3.4 ppb) and normal controls (3.4ppb) and reduced by treatment with prednisolone. Conclusions: Distal lung inflammation is present in refractory asthma. Alveolar NO is a potentially useful technique for investigating the role of distal lung inflammation in asthma and other airway diseases. steroid naive sadece inhale steroid kullananlar oral ve inhaler steroid tedavisi. Berry M et al. Eur. Respir J. 2005; 25: ***p,0.001; NS: Non-significant. Reference: 1. Berry M et al. Alveolar nitric oxide in adults with asthma: evidence of distal lung inflammation in refractory asthma. Eur Respir J. 2005; 25:")
33
Olası astımı olan hastalarda FeNO, akciğer fonksiyon testlerinden üstün
FENO ROC özellikleri: Sensitivite %86 Specifite: %92 Akım hızı = 50 mL/s FENO ∆ Xre5%pred ∆ Rre5%pred 1-spesifite Sensitivite 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 10 ppb Receiver operating characteristics (ROC) of FENO and other lung function measures in discriminating children with probable asthma (n=21) and healthy controls (n=62) Percentage change from predicted baseline value: ?Rre5%pred, Resistance of the respiratory system ?Xre5%pred, Reactance of the respiratory system One key aspect of the potential utility of FENO would be the assessment of baseline lung function vis-à-vis existing diagnostic tools such as bronchodilator responsiveness to aide in early detection of children with probable asthma To that end, Malmberg et al studied 96 preschool children (aged 3.8 to 7.5 years) with asthmatic symptoms or history and 62 age-matched, healthy, non-atopic controls. FENO was measured with the standard online single exhalation technique, and baseline lung function and bronchodilator responsiveness were measured using impulse oscillometry. A cut point of 10 ppb was used The analysis of receiver operating characteristics (ROC) showed that FENO provided the best power for discriminating between children with probable asthma and healthy controls, with a sensitivity of 86% and specificity of 92% at the cut-off level of 1.5 standard deviations above predicted ROC curves evaluate the effectiveness of diagnostic tests. They are a graphical representation of any given test’s true-positive rate against its false-positive rate for different cut points of a diagnostic test. The slope of the tangent line at any given cut point provides the likelihood ratio for that value of the test and the area under the curve is a measure of accuracy for the given test The position of the cut point will determine the number of true positive, true negatives, false positives, and false negatives. We may wish to use different cut points for different clinical situations if we wish to minimize one of the erroneous types of test results. Sensitivity is a statistical measure of the degree to which a test correctly identifies a condition. The results of a screening test are compared to an absolute (gold standard); for example, for a medical test to determine if a person has a certain disease, the sensitivity to the disease is the probability that if the person has the disease, the test will be positive. Remember that 100% sensitivity means the test recognizes all sick people as sick Specificity is a statistical measure of how a diagnostic test correctly identifies the negative cases, or those cases that do not meet the condition under study. A 100% specificity means the test recognizes all healthy people as healthy Conclusion FENO is superior to baseline respiratory function and bronchodilator responsiveness in identifying preschool children with probable asthma. The results emphasize the presence of airway inflammation in the early stages of asthma, even in young children Malmberg LP et al. Thorax. 2003;58(6): Reference: Malmberg LP et al. Exhaled nitric oxide rather than lung function distinguishes preschool children with probable asthma. Thorax. 2003;58(6): 33
 of FENO and other lung function measures in discriminating children with probable asthma (n=21) and healthy controls (n=62) Percentage change from predicted baseline value: Rre5%pred, Resistance of the respiratory system. Xre5%pred, Reactance of the respiratory system. One key aspect of the potential utility of FENO would be the assessment of baseline lung function vis-à-vis existing diagnostic tools such as bronchodilator responsiveness to aide in early detection of children with probable asthma. To that end, Malmberg et al studied 96 preschool children (aged 3.8 to 7.5 years) with asthmatic symptoms or history and 62 age-matched, healthy, non-atopic controls. FENO was measured with the standard online single exhalation technique, and baseline lung function and bronchodilator responsiveness were measured using impulse oscillometry. A cut point of 10 ppb was used. The analysis of receiver operating characteristics (ROC) showed that FENO provided the best power for discriminating between children with probable asthma and healthy controls, with a sensitivity of 86% and specificity of 92% at the cut-off level of 1.5 standard deviations above predicted. ROC curves evaluate the effectiveness of diagnostic tests. They are a graphical representation of any given test’s true-positive rate against its false-positive rate for different cut points of a diagnostic test. The slope of the tangent line at any given cut point provides the likelihood ratio for that value of the test and the area under the curve is a measure of accuracy for the given test. The position of the cut point will determine the number of true positive, true negatives, false positives, and false negatives. We may wish to use different cut points for different clinical situations if we wish to minimize one of the erroneous types of test results. Sensitivity is a statistical measure of the degree to which a test correctly identifies a condition. The results of a screening test are compared to an absolute (gold standard); for example, for a medical test to determine if a person has a certain disease, the sensitivity to the disease is the probability that if the person has the disease, the test will be positive. Remember that 100% sensitivity means the test recognizes all sick people as sick. Specificity is a statistical measure of how a diagnostic test correctly identifies the negative cases, or those cases that do not meet the condition under study. A 100% specificity means the test recognizes all healthy people as healthy. Conclusion. FENO is superior to baseline respiratory function and bronchodilator responsiveness in identifying preschool children with probable asthma. The results emphasize the presence of airway inflammation in the early stages of asthma, even in young children. Malmberg LP et al. Thorax. 2003;58(6): Reference: Malmberg LP et al. Exhaled nitric oxide rather than lung function distinguishes preschool children with probable asthma. Thorax. 2003;58(6):")
34
Pozitif Predictif değer
Mevcut tanı testlerinin etkinlikleri Sensitivite Specifite Pozitif Predictif değer Negatif Predictif değer (%) Peak flow’da steroidle >%15 artış 24 100 69 Steroidle FEV1 artışı >%15 12 66 FEV1 < beklenenin %80’i 29 71 FEV1/FVC < %70 35 73 Balgam eozinofil sayısı > %3 86 88 80 92 FENO50 >20 ppb 79 70 Both FENO and sputum eosinophils have significantly higher diagnostic accuracy than lung function tests FENO provides the added advantage of being noninvasive and easy to perform “Best practice” for confirming the diagnosis of asthma is currently based on assessing abnormal airway physiology, using relatively simple and very common tests. In this article, Smith et al report the sensitivity, specificity, and positive and negative predictive values for commonly available diagnostic tests for asthma Both FENO and sputum eosinophils provided significantly higher degrees of diagnostic accuracy than did tests based on lung function (spirometry and peak flow recordings). Sensitivities for each of the conventional tests (0% to 47%) were lower than for FENO (88%) and sputum eosinophils (86%). Results of conventional tests based on lung function did not improve after a trial of steroid * Adapted from: Smith AD et al. Am J Respir Crit Care Med. 2004;169(4): Reference: Smith AD et al. Diagnosing asthma: comparisons between exhaled nitric oxide measurements and conventional tests. Am J Respir Crit Care Med. 2004;169(4): 34
 Peak flow’da steroidle >%15 artış Steroidle FEV1 artışı >% FEV1 < beklenenin %80’i FEV1/FVC < % Balgam eozinofil sayısı > % FENO50 >20 ppb Both FENO and sputum eosinophils have significantly higher diagnostic accuracy than lung function tests. FENO provides the added advantage of being noninvasive and easy to perform. Best practice for confirming the diagnosis of asthma is currently based on assessing abnormal airway physiology, using relatively simple and very common tests. In this article, Smith et al report the sensitivity, specificity, and positive and negative predictive values for commonly available diagnostic tests for asthma. Both FENO and sputum eosinophils provided significantly higher degrees of diagnostic accuracy than did tests based on lung function (spirometry and peak flow recordings). Sensitivities for each of the conventional tests (0% to 47%) were lower than for FENO (88%) and sputum eosinophils (86%). Results of conventional tests based on lung function did not improve after a trial of steroid. * Adapted from: Smith AD et al. Am J Respir Crit Care Med. 2004;169(4): Reference: Smith AD et al. Diagnosing asthma: comparisons between exhaled nitric oxide measurements and conventional tests. Am J Respir Crit Care Med. 2004;169(4):")
35
Atopi Atopi erişkinlerde eNO’yu etkiler mi?
Kısa etkili bronkodilatör ve inhale steroid ( mg/gün) alan 28 astımlı (ortalama FEV1 %85.7) Birinci gün: FEV1, eNO ve histamin challenge. İkinci gün: eNO, total IgE ve skin-prick test eNO ile total IgE arasında (r : 0.43, p = 0.02) ve pozitif cilt testlerinin sayısı arasında pozitif korelasyon (p = 0.002) saptanmış. eNO ve FEV1 veya PD20 arasında anlamlı korelasyon saptanmamış. eNO ile steroid kullanan veya kullanmayan gruplarda korelasyon saptanmış Buradan şu sonuç çıkarılabilir: astımlılarda artmış eNO ağırlıklı olarak atopi bulgusu oalarak değerlendirilebilir.
 alan 28 astımlı (ortalama FEV1 %85.7) Birinci gün: FEV1, eNO ve histamin challenge. İkinci gün: eNO, total IgE ve skin-prick test. eNO ile total IgE arasında (r : 0.43, p = 0.02) ve pozitif cilt testlerinin sayısı arasında pozitif korelasyon (p = 0.002) saptanmış. eNO ve FEV1 veya PD20 arasında anlamlı korelasyon saptanmamış. eNO ile steroid kullanan veya kullanmayan gruplarda korelasyon saptanmış. Buradan şu sonuç çıkarılabilir: astımlılarda artmış eNO ağırlıklı olarak atopi bulgusu oalarak değerlendirilebilir.")
37
Ekshale NO ile Eozinofilik hava yolu inflamasyonu arasındaki ilişki
1.00 Erkek Kadın 0.1 0.3 1 3 10 30 Ekshale NO konsantrasyonu (ppb) 100 P<.001 R = 0.52 8.3 ppb 0.75 0.50 Sensitivite Akım hızı: 250 ml/s Balgam eozinofil sayısı (%) 0.25 NO has potential advantages as a tool to monitor airway inflammation, although little is known about the relationship between exhaled NO and eosinophil airway inflammation and the factors that influence it. Berry et al attempted to define the relationship between exhaled NO and the sputum eosinophil count1 The authors found a significant positive relationship between exhaled NO and sputum eosinophil count (P<.001) and identified the exhaled NO concentration that best identified a sputum eosinophil count (>3%). In addition, the impact of several potential confounding factors was investigated in 566 consecutive patients with varying severity of asthma In a separate study, Jatakanon et al highlighted that there is consistency in assessment among all 3 noninvasive measures of airway inflammation (exhaled NO, AHR, and induced sputum analysis), thus confirming the reliability of using exhaled NO as an airway inflammation assessment tool2 Results and Conclusions There is a significant association between exhaled NO and sputum eosinophil count. The association is closer in nonsmokers An exhaled NO concentration of 8.3 ppb (250 ml/sec) identified a sputum eosinophil count of >3% with 71% sensitivity and 72% specificity Exhaled NO as a noninvasive measure of airway inflammation is as reliable as other methods of assessment 0.00 0.0 0.25 0.5 0.75 1.0 1-Specifite 100 eNO: 8.3 ppb (250 ml/sec) değerinde balgam eozinofil sayısı >%3 saptandığında sensitivite %71 ve spesifite %72 saptanmış. eNO noninvaziv bir yöntem olarak hava yolu inflamasyonunu değerlendirmede kullanılan diğer testler kadar değerli. Berry MA et al. Clin Exp Allergy. 2005;35(9): References: 1. Berry MA et al. The use of exhaled nitric oxide concentration to identify eosinophilic airway inflammation: an observational study in adults with asthma. Clin Exp Allergy. 2005;35(9): 2. Jatakanon A et al. An inhaled steroid improves markers of airway inflammation in patients with mild asthma. Eur Respir J. 1998;12(5): 37
 100. P<.001. R = ppb Sensitivite. Akım hızı: 250 ml/s. Balgam eozinofil sayısı (%) NO has potential advantages as a tool to monitor airway inflammation, although little is known about the relationship between exhaled NO and eosinophil airway inflammation and the factors that influence it. Berry et al attempted to define the relationship between exhaled NO and the sputum eosinophil count1. The authors found a significant positive relationship between exhaled NO and sputum eosinophil count (P<.001) and identified the exhaled NO concentration that best identified a sputum eosinophil count (>3%). In addition, the impact of several potential confounding factors was investigated in 566 consecutive patients with varying severity of asthma. In a separate study, Jatakanon et al highlighted that there is consistency in assessment among all 3 noninvasive measures of airway inflammation (exhaled NO, AHR, and induced sputum analysis), thus confirming the reliability of using exhaled NO as an airway inflammation assessment tool2. Results and Conclusions. There is a significant association between exhaled NO and sputum eosinophil count. The association is closer in nonsmokers. An exhaled NO concentration of 8.3 ppb (250 ml/sec) identified a sputum eosinophil count of >3% with 71% sensitivity and 72% specificity. Exhaled NO as a noninvasive measure of airway inflammation is as reliable as other methods of assessment Specifite eNO: 8.3 ppb (250 ml/sec) değerinde balgam eozinofil sayısı >%3 saptandığında sensitivite %71 ve spesifite %72 saptanmış. eNO noninvaziv bir yöntem olarak hava yolu inflamasyonunu değerlendirmede kullanılan diğer testler kadar değerli. Berry MA et al. Clin Exp Allergy. 2005;35(9): References: 1. Berry MA et al. The use of exhaled nitric oxide concentration to identify eosinophilic airway inflammation: an observational study in adults with asthma. Clin Exp Allergy. 2005;35(9): Jatakanon A et al. An inhaled steroid improves markers of airway inflammation in patients with mild asthma. Eur Respir J. 1998;12(5):")
38
Am J Respir Crit Care Med Vol 176. pp 231–237, 2007
Hipotez: kortikosteroid dozunun ayarlanması için FeNO’nun kullanılmasıyla daha etkili steroid tedavisi ve daha az atak sağlanabilir. Ölçümler ve sonuçlar: Tahmin edilen ortalama (SD) atak sıklığı FENO grubunda 0.33 (0.69) /hasta/yıl iken kontrol grubunda 0.42 (0.79) (ortalama fark %21; %95 güvenlik aralığı [CI], %57’ye 43; p 0.43). Çalışma sonundaki günlük inhale steroid dozu FENO grubunda daha düşük saptanmış (557 vs. 895 g; ort. fark 338 g; %95 CI, 640’a 37; p ).
 atak sıklığı FENO grubunda 0.33 (0.69) /hasta/yıl iken kontrol grubunda 0.42 (0.79) (ortalama fark %21; %95 güvenlik aralığı [CI], %57’ye 43; p 0.43). Çalışma sonundaki günlük inhale steroid dozu FENO grubunda daha düşük saptanmış (557 vs. 895 g; ort. fark 338 g; %95 CI, 640’a 37; p 0.028).")
39
GP: general practitioner;
JACS: Juniper asthma control questionnaire; PC20: methacholine challenge test; SPT: skin prick tests; Sputum: induced sputum differential cell count.

40
FENO grubu, dolu çember;kontrol grubu, açık çember.

41
Kümülatif atak sayıları Kontrol (kesik çizgil) ve FENO (koyu çizgi)
FENO 26ppb ve eozinofil %3 cutoff değerleri alındığında FENO grubunda eozifil saysının daha az saptandığı görülüyor FENO grubu, dolu çember;kontrol grubu, açık çember.

42
Fluticasone dose (mcg/day)
FENO ICS dozunu ayarlamada kullanılabilir Tek kör, plasebo-kontrollü çalışma. Düzenli inhale steroid kullanan 97 hastada doz ayarlaması geleneksel yöntemle veya FENO takibiyle iki fazlı olarak çalışıldı. Optimal doz ayarlandıktan sonra (Faz 1), hastalar 1 yıl takip edildi (Faz 2). Primer sonlanım: atak sıklığı; sekonder sonlanım: ortalama günlük inhale steroid dozu. 1.2 0.8 0.2 Atak oranları (hasta sayısı/y) 1.0 0.6 0.4 0.0 P=.27 P=.24 P=.91 Total Minor Major Ataklar End of phase 2 (final visit) 750 500 250 Fluticasone dose (mcg/day) 0.0 Study entry End of phase 1 (optimal dose) P=.36 P=.003 ICS dose adjusted using FENO measurements or conventional guidelines algorithm N=97 (12-75 years of age) randomized; FENO group (n=46), control group (n=48) FENO guided dose adjustments arrived at lower overall ICS doses One conceptual benefit of serial FENO measurements could be to aid and simplify the process of adjusting the dose of ICS asthma patients are receiving once good control has been established Smith et al studied the utility of FENO compared to a stepwise dose reduction approach in a single-blind, placebo-controlled trial of 97 patients with asthma who had been regularly receiving treatment with inhaled corticosteroids. Patients were randomly assigned to have their corticosteroid dose adjusted in a stepwise fashion, on the basis of either FENO measurements, or using an algorithm based on conventional guidelines. After the optimal dose was determined (phase 1), patients were followed up for 12 months (phase 2). The primary outcome was the frequency of exacerbations of asthma; the secondary outcome was the mean daily dose of inhaled corticosteroid At the end of the run-in period, patients began receiving 750 mcg of fluticasone per day. The dose was then adjusted at each visit according to each patient’s assigned algorithm. Patients who were taking less than 200 mcg of fluticasone per day (or the equivalent dose of budesonide or beclomethasone) at study entry began receiving 500 mcg per day. The dose could be increased to a maximum of 1000 mcg per day if the measured FENO was greater than 15 ppb or if asthma remained uncontrolled. If, during phase 2, after an upward adjustment, asthma was subsequently found to be controlled at 2 consecutive visits (ie, for 4 months), the dose of fluticasone was reduced by 1 step—but not below the optimal dose or to 0 mcg per day Results reveal a 45.6% non–statistically significant difference between the 2 groups in asthma exacerbation rates and cumulative total numbers of exacerbations as well as no significant difference in nighttime waking or use of bronchodilators among patients in the FENO group vs the control group There was a significant 40% reduction in ICS dose requirement using FENO measurements at a single cut point of 35 ppb, without any significant difference in the rate of asthma exacerbation By using FENO measurements, maintenance doses of ICS are significantly reduced without compromising asthma control Conclusions FENO is a simple, successful, and noninvasive tool to find the optimal ICS dose without compromising asthma control Compared with an algorithmic approach to ICS dose optimization, FENO-guided dose adjustment arrived at lower overall ICS doses, potentially minimizing long-term side effects from ICS therapy Kontrol grubu FENO grubu Akım hızı = 250 mL/s * Smith AD et al. N Eng J Med. 2005;352(21): Reference: Smith AD et al. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Eng J Med. 2005;352(21): 42
, hastalar 1 yıl takip edildi (Faz 2). Primer sonlanım: atak sıklığı; sekonder sonlanım: ortalama günlük inhale steroid dozu Atak oranları. (hasta sayısı/y) P=.27. P=.24. P=.91. Total. Minor. Major. Ataklar. End of phase 2. (final visit) Fluticasone dose (mcg/day) 0.0. Study entry. End of phase 1. (optimal dose) P=.36. P=.003. ICS dose adjusted using FENO measurements or conventional guidelines algorithm. N=97 (12-75 years of age) randomized; FENO group (n=46), control group (n=48) FENO guided dose adjustments arrived at lower overall ICS doses. One conceptual benefit of serial FENO measurements could be to aid and simplify the process of adjusting the dose of ICS asthma patients are receiving once good control has been established. Smith et al studied the utility of FENO compared to a stepwise dose reduction approach in a single-blind, placebo-controlled trial of 97 patients with asthma who had been regularly receiving treatment with inhaled corticosteroids. Patients were randomly assigned to have their corticosteroid dose adjusted in a stepwise fashion, on the basis of either FENO measurements, or using an algorithm based on conventional guidelines. After the optimal dose was determined (phase 1), patients were followed up for 12 months (phase 2). The primary outcome was the frequency of exacerbations of asthma; the secondary outcome was the mean daily dose of inhaled corticosteroid. At the end of the run-in period, patients began receiving 750 mcg of fluticasone per day. The dose was then adjusted at each visit according to each patient’s assigned algorithm. Patients who were taking less than 200 mcg of fluticasone per day (or the equivalent dose of budesonide or beclomethasone) at study entry began receiving 500 mcg per day. The dose could be increased to a maximum of 1000 mcg per day if the measured FENO was greater than 15 ppb or if asthma remained uncontrolled. If, during phase 2, after an upward adjustment, asthma was subsequently found to be controlled at 2 consecutive visits (ie, for 4 months), the dose of fluticasone was reduced by 1 step—but not below the optimal dose or to 0 mcg per day. Results reveal a 45.6% non–statistically significant difference between the 2 groups in asthma exacerbation rates and cumulative total numbers of exacerbations as well as no significant difference in nighttime waking or use of bronchodilators among patients in the FENO group vs the control group. There was a significant 40% reduction in ICS dose requirement using FENO measurements at a single cut point of 35 ppb, without any significant difference in the rate of asthma exacerbation. By using FENO measurements, maintenance doses of ICS are significantly reduced without compromising asthma control. Conclusions. FENO is a simple, successful, and noninvasive tool to find the optimal ICS dose without compromising asthma control. Compared with an algorithmic approach to ICS dose optimization, FENO-guided dose adjustment arrived at lower overall ICS doses, potentially minimizing long-term side effects from ICS therapy. Kontrol grubu. FENO grubu. Akım hızı = 250 mL/s. * Smith AD et al. N Eng J Med. 2005;352(21): Reference: Smith AD et al. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Eng J Med. 2005;352(21):")
43
40 çocuk (21 erkek) (ort.yaş 12.2)- ort. 400 mg budesonid veya eşiti.
FENO: steroid kesildikte -2, 0, 2, 4, 12 ve 24 hafta sonra Relaps tanımı: Ayda 1’den fazla atak veya En az iki hafta haftada 4 günden fazla beta agonist ihtiyacı duyma veya diurnal PEF değişkenliği >%20. 9 çocukta relaps FENO: 4 haftada relapsı göstermede en yüksek sensitivite (%71) ve spesifite (%93) 49 ppb FENOdeğerinde elde edildi.
 ve spesifite (%93) 49 ppb FENOdeğerinde elde edildi.")
44
FENO ICS kesildikten sonraki relapsın göstergesi olabilir FENO > 49 ppb değeri steroid kesildikten 4 hafta sonra astım relapsı yüksek olasılıkla göstermekte Sensitivite: 71% Specifite: 93% Sensitivite 1-Specifite 0.00 0.25 0.50 0.75 1.00 49 ppb FENO 58 FENO 49 FENO 24 FENO 7 Flow rate = 50 mL/s Pijnenburg MW et al. Thorax. 2005;60(3):
:")
45
ENO astımda KOAH’dan anlamlı oranda yüksek
Study included 46 patients (age>50 yrs) with fixed airflow obstruction and a history of asthma or COPD. Mean FENO levels in patients with asthma is 38 ppb as compared to 11 ppb for patients with COPD In this study Fabbri et al. investigated whether subjects with fixed airflow obstruction have distinct airway inflammation depending on their history of asthma or COPD. They examined a group of 46 consecutive patients presenting with fixed airflow obstruction (27 patients with COPD and 19 with asthma), and analyzed lung function, exhaled nitric oxide, high-resolution computed tomography (HRCT) scan of the chest, and airway pathology. Compared with the patients with a history of COPD, patients with a history of asthma had more eosinophils in peripheral blood, sputum, bronchoalveolar lavage, and airway mucosa. Patients with a history of asthma had a higher level of exhaled NO than those with a history of COPD (37.5 ± 9.2 ppb versus 11.1 ± 1.7 ppb; P<.01). (A) and (B): Photomicrographs showing bronchial biopsy specimens immunostained with anti–EG-2 (eosinophil cationic protein) from a patient with fixed airflow obstruction and a history of COPD (A) and from a patient with fixed airflow obstruction and a history of asthma (B). ** Fabbri LM et al. Am J Respir Crit Care Med ;167(3): Reference: Fabbri LM et al. Differences in airway inflammation in patients with fixed airflow obstruction due to asthma or chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2003;167(3): . 45
 with fixed airflow obstruction and a history of asthma or COPD. Mean FENO levels in patients with asthma is 38 ppb as compared to 11 ppb for patients with COPD. In this study Fabbri et al. investigated whether subjects with fixed airflow obstruction have distinct airway inflammation depending on their history of asthma or COPD. They examined a group of 46 consecutive patients presenting with fixed airflow obstruction (27 patients with COPD and 19 with asthma), and analyzed lung function, exhaled nitric oxide, high-resolution computed tomography (HRCT) scan of the chest, and airway pathology. Compared with the patients with a history of COPD, patients with a history of asthma had more eosinophils in peripheral blood, sputum, bronchoalveolar lavage, and airway mucosa. Patients with a history of asthma had a higher level of exhaled NO than those with a history of COPD (37.5 ± 9.2 ppb versus 11.1 ± 1.7 ppb; P<.01). (A) and (B): Photomicrographs showing bronchial biopsy. specimens immunostained with anti–EG-2 (eosinophil cationic protein) from a patient with fixed airflow obstruction and a history of COPD (A) and from a patient with fixed airflow obstruction and a history of. asthma (B). ** Fabbri LM et al. Am J Respir Crit Care Med. 2003;167(3): Reference: Fabbri LM et al. Differences in airway inflammation in patients with fixed airflow obstruction due to asthma or chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2003;167(3):")
46
KOAH ve eNO Astımdan düşük (sigara içen veya içmeyen) – normalden farklı değil Sigara içimi – eNOS downregulasyonu Artmış oksidatif stres nedeniyle NO’nun peroksinitrite dönüşerek harcanması unstabil KOAH – stabile göre yüksek NO

47
KOAH ve eNO Alevlenmelerde NO artışı
Pulmoner hipertansiyon – kor pulmonale – bozulmuş endotelial NO salınımı - düşük eNO Steroide iyi yanıt alınan KOAH hastalarında (muhtemelen eşlik eden astımı olan vakalar) artmış eNO. eNO hangi KAOH hastasının steroide yanıt vereceğini saptamada kullanılabilir
 artmış eNO. eNO hangi KAOH hastasının steroide yanıt vereceğini saptamada kullanılabilir.")
48
eNO in COPD Paredi P. Am J Respir Crit Care Med Vol 162. pp 369–373, 2000

49
Sigara - eNO Grup A steroid (-) sigara içmeyen astımlılar,
Grup B steroid (+) sigara içmeyen astımlılar, Grup C steroid (-) sigara içen astımlılar, Grup D sigara içmeyen sağlıklı gönüllüler Grup E sigara içen sağlıklı gönüllüler Anlamlı: * p , 0.05, ** p , 0.01, *** p , CHEST 1999; 116:59–64)
 sigara içmeyen astımlılar, Grup C steroid (-) sigara içen astımlılar, Grup D sigara içmeyen sağlıklı gönüllüler. Grup E sigara içen sağlıklı gönüllüler. Anlamlı: * p , 0.05, ** p , 0.01, *** p , CHEST 1999; 116:59–64)")
50
Sigara - eNO Grup A steroid (-) sigara içmeyen astımlılar, p , 0.05;
Grup B steroid (+) sigara içmeyen astımlılar; NS; Grup C steroid (-) sigara içen astımlılar; NS; CHEST 1999; 116:59–64)
 sigara içmeyen astımlılar; NS; Grup C steroid (-) sigara içen astımlılar; NS; CHEST 1999; 116:59–64)")
51
Linear regression between FENOpl : Plateau value of exhaled nitric oxide versus
A, sPAP : systolic pulmonary artery pressure (r= -0.63, p= 0.01). (B) TRP: tricuspid valve regurgitation pressure (r= -0.45, p <0.01). (C) RVwd :right ventricle wall dimension (r=0.59, p = < 0.05). Linear regression between FENOpl: plateau value of exhaled nitric oxide versus A, FEV1/FVC (r= 0.14, p= 0.5). B PaO2 (r= 0.24, p = 0.2). C DLCO (r = 0.02, p= 0.9). Am J Respir Crit Care Med Vol 162. pp 446–450, 2000
. (B) TRP: tricuspid valve regurgitation pressure. (r= -0.45, p <0.01). (C) RVwd :right ventricle wall dimension (r=0.59, p = < 0.05). Linear regression between FENOpl: plateau value of exhaled nitric oxide versus. A, FEV1/FVC (r= 0.14, p= 0.5). B PaO2 (r= 0.24, p = 0.2). C DLCO (r = 0.02, p= 0.9). Am J Respir Crit Care Med Vol 162. pp 446–450,")
52
Mohammed F. Exhaled nitric oxide in stable chronic obstructive pulmonary disease. Ann Thorac Med Apr–Jun; 4(2): 65–70 Linear regression analysis showing relationship between FEV1/FVC ratio and FENO levels in COPD subjects (r = −0.5855, P = ) Linear regression analysis showing relationship between FEV1/FVC ratio and FENO levels in healthy subjects (r = , P = )
 Linear regression analysis showing relationship between FEV1/FVC ratio and FENO levels in healthy subjects (r = , P = )")
53
PFTs Control n = 25 COPD n = 14 P value
FEV1 (Liters) ± ± FEV1/FVC ± ± FENO (ppb) ± ± PFTs COPD n = Asthma n=25 P value FEV1 (Liters) ± ± FEV1/FVC ± ± FENO (ppb) ± ± Linear regression analysis showing relationship between FEV1/FVC ratio and FENO levels in asthma subjects (r = −0.3076, P = ) Only steroid naïve patients Hb scavenging less effective colonization which stimulate NO synthase Ann Thorac Med Apr–Jun; 4(2): 65–70
 3.64 ± ± FEV1/FVC ± ± FENO (ppb) ± ± PFTs COPD n = 14 Asthma n=25 P value. FEV1 (Liters) 1.75 ± ± FEV1/FVC ± ± FENO (ppb) ± ± Linear regression analysis showing relationship between FEV1/FVC ratio and FENO levels in asthma subjects (r = −0.3076, P = ) Only steroid naïve patients. Hb scavenging less effective. colonization which stimulate NO synthase. Ann Thorac Med Apr–Jun; 4(2): 65–70.")
54
Am J Respir Crit Care Med Vol 162. pp 1773–1777, 2000

55
(r =0.7, p= 0.003). The vertical line represents 15-ppb cutoff value.
Am J Respir Crit Care Med Vol 162. pp 1773–1777, 2000 (r =0.7, p= 0.003). The vertical line represents 15-ppb cutoff value.
. The vertical line represents 15-ppb cutoff value.")
56
AM J RESPIR CRIT CARE MED 1998;157:998–1002.

57
AM J RESPIR CRIT CARE MED 1998;157:998–1002.

58
AM J RESPIR CRIT CARE MED 1998;157:998–1002.

59
Primer Siliyer Diskinezi (PCD)
Hava yollarında NO konsantrasyonunu düşürdüğü bilinen 3 durum mevcut: PCD, ilk olarak LUNDBERG ve ark. tanımlamış Kistik fibrozis (CF) Pulmoner hipertansiyonun eşlik ettiği sistemik skleroz NO’nun siliyer motilitenin regulasyonunda ve konak savunmasında rolü olduğu düşünülüyor.
 Pulmoner hipertansiyonun eşlik ettiği sistemik skleroz. NO’nun siliyer motilitenin regulasyonunda ve konak savunmasında rolü olduğu düşünülüyor.")
60
Eur Respir J 2003; 21: 43–47

61
Eur Respir J 1999; 13:

62
Kronik Öksürük Ayırıcı Tanısı ve FeNO
Chatkin JM et al. Am J Respir Crit Care Med. 1999;159(6): An increased level of exhaled NO may assist in the differential diagnosis of chronic cough. Patients with asthma and chronic cough and patients with a high cough frequency have higher exhaled NO levels than controls Accurate diagnosis of patients complaining of chronic cough is essential for the underlying disease to be treated correctly. In more than 90% of cases, symptoms are a result of smoking, postnasal drip, GERD, asthma, or COPD Chatkin et al investigated the value of exhaled NO in the assessment of chronic cough. Exhaled NO was measured in adults with chronic cough, known asthmatics, and healthy controls. Patients with chronic cough and asthma had significantly higher exhaled NO values than nonasthmatics with chronic cough or healthy controls. Using 30 ppb (at a flow of 45 mL/s) as the cut-off point for exhaled NO gave a sensitivity and specificity of 75% and 87%, respectively Levels of exhaled NO based on diagnostic category is shown in the figure here. The median FENO concentration was 16.7 ppb for the nonasthmatic (NA) group, whereas in the asthmatic (A) group, it was 75 ppb. The median FENO in the group of asthmatics with wheezing or dyspnea (WA) was 69.0 ppb and in the healthy control (C) group was 28.3 ppb Kronik öksürüklü Non-astmatikler Kronik öksürüklü astmatikler Wheezing veya dispneli Astmatikler Sağlıklı kontrol Reference: Chatkin JM et al. Exhaled nitric oxide as a noninvasive assessment of chronic cough. Am J Respir Crit Care Med. 1999;159(6): 62
: An increased level of exhaled NO may assist in the differential diagnosis of chronic cough. Patients with asthma and chronic cough and patients with a high cough frequency have higher exhaled NO levels than controls. Accurate diagnosis of patients complaining of chronic cough is essential for the underlying disease to be treated correctly. In more than 90% of cases, symptoms are a result of smoking, postnasal drip, GERD, asthma, or COPD. Chatkin et al investigated the value of exhaled NO in the assessment of chronic cough. Exhaled NO was measured in adults with chronic cough, known asthmatics, and healthy controls. Patients with chronic cough and asthma had significantly higher exhaled NO values than nonasthmatics with chronic cough or healthy controls. Using 30 ppb (at a flow of 45 mL/s) as the cut-off point for exhaled NO gave a sensitivity and specificity of 75% and 87%, respectively. Levels of exhaled NO based on diagnostic category is shown in the figure here. The median FENO concentration was 16.7 ppb for the nonasthmatic (NA) group, whereas in the asthmatic (A) group, it was 75 ppb. The median FENO in the group of asthmatics with wheezing or dyspnea (WA) was 69.0 ppb and in the healthy control (C) group was 28.3 ppb. Kronik öksürüklü Non-astmatikler. Kronik öksürüklü astmatikler. Wheezing veya dispneli Astmatikler. Sağlıklı. kontrol. Reference: Chatkin JM et al. Exhaled nitric oxide as a noninvasive assessment of chronic cough. Am J Respir Crit Care Med. 1999;159(6):")
63
GÖR - Astım 35 30 25 FENO (ppb) 20 15 10 5 P=.0001
Astım benzeri semptomları olan GÖR’lü çocuklar Allerjik Astımlı çocuklar FENO (ppb) 20 15 10 5 25 30 35 P=.0001 FENO levels are lower in allergic children with “asthma-like symptoms” and GERD (n=12) as compared to asthmatic children (n=20) FENO measured in the study population. The horizontal lines represent mean values. In gastro-esophageal (GER) reflux, micro-aspirations of gastric fluid may damage the epithelial surface of the airways, an important source of endogenous nitric oxide (NO) Silvestri et al conducted the present study to evaluate the possible influence of GER on fractional exhaled nitric oxide (FENO) release. They compared the FENO levels in 2 groups of atopic children: 20 children with mild asthma and responsive to standard anti-asthma pharmacologic therapy, and 12 children with GER and asthma-like symptoms Results: No significant differences in pulmonary function testing parameters (FEV1, FVC and FEF25-75%) were found between asthmatic children and GER children (P< 0.2). In contrast, FENO levels were higher in asthmatic children than in GER children (21.32 ppb (7.67) and 9.53 ppb (4.05); P=.0001) as illustrated in the figure The results of the study indicate that FENO levels are lower in allergic children with "asthma like symptoms" and GER as compared to asthmatic children Silvestri M et al. Respiration. 2004;71: Reference: Silvestri M et al. Correlations between exhaled nitric oxide levels and pH-metry data in asthmatics with gastro-oesophageal reflux. Respiration. 2004;7(4): 63
 P= FENO levels are lower in allergic children with asthma-like symptoms and GERD (n=12) as compared to asthmatic children (n=20) FENO measured in the study population. The horizontal lines represent mean values. In gastro-esophageal (GER) reflux, micro-aspirations of gastric fluid may damage the epithelial surface of the airways, an important source of endogenous nitric oxide (NO) Silvestri et al conducted the present study to evaluate the possible influence of GER on fractional exhaled nitric oxide (FENO) release. They compared the FENO levels in 2 groups of atopic children: 20 children with mild asthma and responsive to standard anti-asthma pharmacologic therapy, and 12 children with GER and asthma-like symptoms. Results: No significant differences in pulmonary function testing parameters (FEV1, FVC and FEF25-75%) were found between asthmatic children and GER children (P< 0.2). In contrast, FENO levels were higher in asthmatic children than in GER children (21.32 ppb (7.67) and 9.53 ppb (4.05); P=.0001) as illustrated in the figure. The results of the study indicate that FENO levels are lower in allergic children with asthma like symptoms and GER as compared to asthmatic children. Silvestri M et al. Respiration. 2004;71: Reference: Silvestri M et al. Correlations between exhaled nitric oxide levels and pH-metry data in asthmatics with gastro-oesophageal reflux. Respiration. 2004;7(4):")
64
15 hastada Pulmoner tutulum (%45.5)
İnflamatuar barsak hastalıklarındaki (İBH) pulmoner tutulumun gösterilmesinde FENO’nun değeri 33 sigara içmeyen İBH (25 ülseratif kolit [UC] ve 8 Crohn hastalığı [CD]) - Kortikosteroid kullanmıyorlar ve 25 sağlıklı kontrol 15 hastada Pulmoner tutulum (%45.5) FENO pulmoner tutulum olanlarda 32 ± 20 ppb; tutulum olmayanlarda 14 ± 8 ppb ve sağlıklı kontrol grubunda 8 ppb (P < 0.05). Ozyilmaz E, Yildirim B, Erbas G, Akten S, Oguzulgen İK, Tunc B, Tuncer C, Turktas H. Inflammatory bowel disease. Volume 16 Issue 4, Pages 670 - 676
 pulmoner tutulumun gösterilmesinde FENO’nun değeri. 33 sigara içmeyen İBH (25 ülseratif kolit [UC] ve 8 Crohn hastalığı [CD]) - Kortikosteroid kullanmıyorlar ve 25 sağlıklı kontrol. 15 hastada Pulmoner tutulum (%45.5) FENO pulmoner tutulum olanlarda 32 ± 20 ppb; tutulum olmayanlarda 14 ± 8 ppb ve sağlıklı kontrol grubunda 8 ppb (P < 0.05). Ozyilmaz E, Yildirim B, Erbas G, Akten S, Oguzulgen İK, Tunc B, Tuncer C, Turktas H. Inflammatory bowel disease. Volume 16 Issue 4, Pages")
65
Fig 1. Exhaled nitric oxide levels in 52 patients with sarcoidosis and
44 normal non-smoking controls. Exhaled nitric oxide levels in 12 atopic and 19 non-atopic patients with sarcoidosis.

66
Lung. 2001;179(4):
:")
67
Am. J. Respir. Cell Mol. Biol. Vol. 24, pp. 414–418, 2001
Immunohistochemical immunoreactivity for NOSIII antibody. (A) LAM smooth-muscle cells have diffuse moderate staining for NOSIII (L) similar to the adjacent bronchial smooth muscle (B) and endothelium (arrow) (Hematoxylin counterstain; original magnification, 320). (B) LAM smooth-muscle cells (L), bronchiolar smooth muscle (B), and endothelium of multiple vessels (arrows) have immunoreactivity to NOSIII (hematoxylin; original magnification, 340). (C) LAM smooth-muscle cells (L) and adjacent endothelium (arrow) have immunoreactivity to NOSIII (hematoxylin; original magnification, 3200).
 LAM smooth-muscle cells have diffuse moderate. staining for NOSIII (L) similar to the adjacent bronchial smooth. muscle (B) and endothelium (arrow) (Hematoxylin counterstain; original magnification, 320). (B) LAM smooth-muscle cells (L), bronchiolar smooth muscle (B), and endothelium of multiple vessels. (arrows) have immunoreactivity to NOSIII (hematoxylin; original magnification, 340). (C) LAM smooth-muscle cells (L) and adjacent endothelium (arrow) have immunoreactivity to. NOSIII (hematoxylin; original magnification, 3200).")
Benzer bir sunumlar









 HASTALARDA BRONŞİAL REMODELLİNG’İN İNDÜKTE BALGAMDA VASCULAR ENDOTHELIAL GROWTH FACTOR (VEGF) ÖLÇÜMÜ İLE DEĞERLENDİRİLMESİ.>")











