Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Prof Dr Serhat Unal Hacettepe Üniversitesi Tıp Fakültesi Ankara
Erişkinlerde Aşılama Prof Dr Serhat Unal Hacettepe Üniversitesi Tıp Fakültesi Ankara ANTALYA HALK SAĞLIĞI MÜDÜRLÜĞÜ 1. AŞI SEMPOZYUMU 21 Mayıs 2014

2
Bir hastalık üzerine yöneldiğimde, hastalığa çare bulmayı düşünmem, onun yerine önlemenin yollarını düşünürüm. Louis Pasteur ( )
")
3
Aşılamada Genel Bakış Açısı
İnsanoğlunun çeşitli veba ve salgın hastalıklardan kendini kurtarmak için umutsuzca çabaladığı yüzyıllarla kıyaslandığında aşılamanın kısa bir geçmişi vardır. Daha sadece 20. yüzyılda geniş kitlelerin rutin aşılaması başlamıştır Görece gençliğine rağmen aşılama, Edward Jenner’den bu zamana 12 önemli hastalığı kontrol altına almıştır. Edward Jenner Louis Pasteur Susan L. Plotkin and Stanley A. Plotkin in Plotkin: Vaccines, 5th ed., Saunders 2008

4
Kontrol altına alınan 12 önemli hastalık
En azından dünyanın bir kısmı için: 1. Çiçek 2. Difteri 3. Tetanoz 4. Sarı Humma 5. Boğmaca 6. Haemophilus influenzae tip b 7. Poliomyelitis 8. Kızamık 9. Kabakulak 10. Kızamıkçık 11. Tifo 12. Kuduz Çiçek vakalarında tam eradikasyon hayaline ulaşılmıştır. Polio vakalarında da %99 azalma sağlanmıştır. Döküntüden yaklaşık 7 gün sonra tipik bir variola major vakası (Dünya Sağlık Örgütü Çiçek Tanıma kartlarından alınmıştır) Susan L. Plotkin and Stanley A. Plotkin in: Plotkin: Vaccines, 5th ed., Saunders 2008
 Susan L. Plotkin and Stanley A. Plotkin in: Plotkin: Vaccines, 5th ed., Saunders")
5
20.Yüzyıl yıllık morbidite†
20.yüzyıl ve günümüzde yıllık morbidite karşılaştırması: Aşılama ile önlenebilir Hastalıklar Hastalık 20.Yüzyıl yıllık morbidite† 2011 Bildirilen vakalar† † Azalma yüzdesi Çiçek 29,005 100% Difteri 21,053 Kızamık 530,217 212 > 99% Kabakulak 162,344 370 Boğmaca 200,752 15,216 92% Polio (paralitik) 16,316 Kızamıkçık 47,745 4 Konjenital Kızamıkçık Sendromu 152 Tetanoz 580 9 98% Haemophilus influenzae 20,000 8* †Kaynak: JAMA. 2007;298(18): † † Kaynak: CDC. MMWR January 6, 2012;60(51); (provisional 2011 data) * Haemophilus influenzae type b (Hib) < 5 years of age. An additional 14 cases of Hib are estimated to have occurred among the 237 reports of Hi (< 5 years of age) with unknown serotype.
 16,316. Kızamıkçık. 47, Konjenital Kızamıkçık Sendromu Tetanoz % Haemophilus influenzae. 20,000. 8* †Kaynak: JAMA. 2007;298(18): † † Kaynak: CDC. MMWR January 6, 2012;60(51); (provisional 2011 data) * Haemophilus influenzae type b (Hib) < 5 years of age. An additional 14 cases of Hib are estimated to have occurred among the 237 reports of Hi (< 5 years of age) with unknown serotype.")
8
Neden Aşılama? En etkin koruma Bağışıklık sistemini hedef alır
Gerçekten proaktif olan tek tedavi Hastalara bakan kişileri transmisyon için vektörlükten koruyabilir Advers reaksiyon insidansı düşük Vaccinations have proven to be an incredibly successful modality at prevention of disease. From a public health standpoint, only sanitation and clean water has exceeded its effectiveness at reducing disease. This is very well accepted for the pediatric population and in many cases a requirement for entry to public school. Vaccination remains the most cost effective tool in many adult infectious diseases as well, with some infections having been eradicated as a result of vaccination programs (I.e. Smallpox). Others, for all practical considerations, have ceased to be clinically threatening in the industrialized world because of virtual universal vaccination in children (I.e. mumps, rubella) Some infectious agents can mutate and change, or protective immunity wane with time. In these cases adult vaccination is required to prime the immune system against infection. Note that vaccination does not truly prevent infection at its earliest stages (I.e. mucosal invasion by influenza virus) but after vaccination the primed immune system is able to mount a swifter secondary response to the invading organisms, circumventing much of the pathology of infection. Even if successful at proliferating, infectious organisms in a vaccinated individual usually only cause attenuated illness, both in severity and length of symptoms. Due to the immune system being primed, vaccination remains the only true proactive defense against infection as all antibiotic and antiviral therapy requires detection of infection and implementation of therapy. This process is often inefficient in frail elderly due to the diminished symptoms and signs of infection from Immunosenescence. Vaccination is the only method by which the infection is immediately detected and the immune response put into action. Family, friends, and caregivers can all become infected with infections which can be transmitted to others, thus serving as vectors of transmission. Vaccination helps to reduce transmission rates by reducing the severity of infection and thus the number of invading organisms that may be passed onto another person. Finally, most vaccines are quite safe. Certainly the reduction in morbidity and mortality has far outweighed the adverse reactions due to vaccines.
. Others, for all practical considerations, have ceased to be clinically threatening in the industrialized world because of virtual universal vaccination in children (I.e. mumps, rubella) Some infectious agents can mutate and change, or protective immunity wane with time. In these cases adult vaccination is required to prime the immune system against infection. Note that vaccination does not truly prevent infection at its earliest stages (I.e. mucosal invasion by influenza virus) but after vaccination the primed immune system is able to mount a swifter secondary response to the invading organisms, circumventing much of the pathology of infection. Even if successful at proliferating, infectious organisms in a vaccinated individual usually only cause attenuated illness, both in severity and length of symptoms. Due to the immune system being primed, vaccination remains the only true proactive defense against infection as all antibiotic and antiviral therapy requires detection of infection and implementation of therapy. This process is often inefficient in frail elderly due to the diminished symptoms and signs of infection from Immunosenescence. Vaccination is the only method by which the infection is immediately detected and the immune response put into action. Family, friends, and caregivers can all become infected with infections which can be transmitted to others, thus serving as vectors of transmission. Vaccination helps to reduce transmission rates by reducing the severity of infection and thus the number of invading organisms that may be passed onto another person. Finally, most vaccines are quite safe. Certainly the reduction in morbidity and mortality has far outweighed the adverse reactions due to vaccines.")
9
Maliyet Etkinlik Aşıya harcanan her bir dolar Boğmaca DTP: $29
Kızamık/kabakulak/kızamıkçık: $21 Oral polio $6 Suçiçeği $5 Haemophilus influenza tip B: $2 Influenza: $31 daha az para harcanmasını sağlar Vaccinations are some of the most cost effective modalities used in medicine. Of the vaccines routinely recommended in childhood, several dollars are saved on treatment of the prevented disease for each dollar spent administering the vaccine. Considering these are universal recommendations, with no evaluation criteria if a vaccine is appropriate or not, this cost effectiveness is impressive. Other vaccines are recommended for specific populations and are clearly cost effective within those population parameters. Influenza virus vaccine and streptococcal pneumoniae vaccine in those > 65 yo are two examples which have proven not only efficacious at preventing disease, but cost effective at saving health care dollars expended on treating the diseases and secondary complications and rehabilitation that result. This cost effectiveness is despite many in this population having retired and not figuring lost work days into the calculation of savings. G Keusch, K Bart. Immunization Principles and Vaccine UseAnnals of Internal Medicine, 2002;137(4): ). Nichol, KL. Vaccine, 2003;21(16): )-The efficacy, effectiveness and cost-effectiveness of inactivated influenza virus vaccines. Harrison’s Principles of Internal Medicine. 15th Edition.
: ). Nichol, KL. Vaccine, 2003;21(16): )-The efficacy, effectiveness and cost-effectiveness of inactivated influenza virus vaccines. Harrison’s Principles of Internal Medicine. 15th Edition.")
10
Aşı ile ilişkili komplikasyonlar?
Ticari olarak mevcut olan aşılar güvenilirdir (Civa, thimerisol) Çoğu aşıdaki advers olaylar hafiftir Kol ağrısı yada hafif ateş Ciddi yan etkiler nadirdir 1/1000 ila1/1,000,000/doz Bazısı o kadar nadirdir ki risk tam olarak değerlendirilemez Aşıya bağlı istatistiksel ölüm riski o kadar nadirdşr ki değerlendirilmesi zordur yılları arasında VAERS’e (Aşı Advers Olay Bildirim Sistemi) bildirilen ölümlerden sadece birinin aşı ile ilgili olduğuna inanılmaktadır The Institute of Medicine (Tıp Enstitüsü) 1994 yılında aşıya bağlı ölüm riskini olağandışı düşük olarak bildirmiştir Occasionally the subject of vaccines causing a variety of health ailments. Little data exist to substantiate these claims. The Vaccine Adverse Event Reporting System is designed to record possible adverse events related to vaccines. While minor reactions are common (I.e. sore arm injection site or cold like symptoms including fever), almost no correlation has been shown between vaccines and serious adverse reactions or development of chronic illness. While experimental vaccines have had occurrances of serious side effects (a recent vaccine against Beta amaloid plaques developed to treat Alzheimer’s disease required halting of the trial due to a number of encephalitis deaths), clinically approved vaccines have proven quite safe. During one year of the influenza vaccine, it was shown to statistically increase the risk of Guillan-Barre very slightly (increased by 1 in a million). Conversely, protection from disease is easily demonstrated, making the benefit of vaccination far outweigh any known risk. Due to concerns over vaccine safety the Institute of Medicine reviewed safety data for commercially available vaccines. Their findings prompted them to declare vaccines available to the American public as ‘extraordinarily low’ as far as risk of death or serious complications. -CDC: Amerika Ulusal Bağışıklama Programı
 Çoğu aşıdaki advers olaylar hafiftir. Kol ağrısı yada hafif ateş. Ciddi yan etkiler nadirdir. 1/1000 ila1/1,000,000/doz. Bazısı o kadar nadirdir ki risk tam olarak değerlendirilemez. Aşıya bağlı istatistiksel ölüm riski o kadar nadirdşr ki değerlendirilmesi zordur yılları arasında VAERS’e (Aşı Advers Olay Bildirim Sistemi) bildirilen ölümlerden sadece birinin aşı ile ilgili olduğuna inanılmaktadır. The Institute of Medicine (Tıp Enstitüsü) 1994 yılında aşıya bağlı ölüm riskini olağandışı düşük olarak bildirmiştir. Occasionally the subject of vaccines causing a variety of health ailments. Little data exist to substantiate these claims. The Vaccine Adverse Event Reporting System is designed to record possible adverse events related to vaccines. While minor reactions are common (I.e. sore arm injection site or cold like symptoms including fever), almost no correlation has been shown between vaccines and serious adverse reactions or development of chronic illness. While experimental vaccines have had occurrances of serious side effects (a recent vaccine against Beta amaloid plaques developed to treat Alzheimer’s disease required halting of the trial due to a number of encephalitis deaths), clinically approved vaccines have proven quite safe. During one year of the influenza vaccine, it was shown to statistically increase the risk of Guillan-Barre very slightly (increased by 1 in a million). Conversely, protection from disease is easily demonstrated, making the benefit of vaccination far outweigh any known risk. Due to concerns over vaccine safety the Institute of Medicine reviewed safety data for commercially available vaccines. Their findings prompted them to declare vaccines available to the American public as ‘extraordinarily low’ as far as risk of death or serious complications. -CDC: Amerika Ulusal Bağışıklama Programı.")
11
Erişkin Bağışıklamasının Mantığı
Bebek, çocuk, adolesan bağışıklama programlarının başarısı üzerine kurulmuştur Yaşlanma: daha duyarlı. Artan antimikrobiyal direnci Erişkin aşılaması ile önlenebilir hastalıkların yükünün anlaşılması Erişkinlere yönelik yeni aşılar Eşdeğer ‘Erişkin Aşılama’ programının olmaması * *

12
Immunosenesens: Klinik Belirteçleri
İnfeksiyona bağışıklık yanıtın hızında ve büyüklüğünde azalma İnfeksiyona bağlı morbidite ve mortalitede artış İnfeksiyonun klinik olarak daha zor fark edilmesi Salgın infeksiyonlarda (influenza) tüm sebeplere bağlı mortalite riskinde artış Immunosenescence is not just an inability to fight off infection with aging. It is a dysfunction of immune processes overall. Infectious incidence is only one manifestation of this. Another common manifestation can be seen in the increased incidence in cancer as the immune system is less able to regulate its self/non-self recognition, allowing neoplasms that would have previously been destroyed to go undetected. Similarly, pro-inflammatory disease processes, such as arthritis or giant cell arteritis may result from recognizing self tissues as being non-self. The end result from an infectious standpoint is increased incidence of infection, increased morbidity and mortality, and increased secondary complications. Interestingly the symptoms and signs of infection may be attenuated or absent because of the diminished strength of the immune response. Immunosenescent individuals mount lower inflammatory levels of IL-1, IL-6, TNF-alpha, etc. Because these cytokines are what leads to manifestations of fever, waiting for a temperature of F may be too insensitive to detect infection. Other comorbidities also contribute to the difficulty at detecting infection. In frail, old patients, a high index of suspicion for infection is important. All cause mortality is increased epidemiologically during times of epidemic infection (such as influenza virus season) believed to be linked to increased inflammation destabilizing atherosclerotic plaques leading to thrombotic events. While proof of acute inflammation causing thrombotic events is not as strong as chronic inflammation, it is strongly suspected this is part of the mechanism leading to this increase in morbidity and mortality.
 tüm sebeplere bağlı mortalite riskinde artış. Immunosenescence is not just an inability to fight off infection with aging. It is a dysfunction of immune processes overall. Infectious incidence is only one manifestation of this. Another common manifestation can be seen in the increased incidence in cancer as the immune system is less able to regulate its self/non-self recognition, allowing neoplasms that would have previously been destroyed to go undetected. Similarly, pro-inflammatory disease processes, such as arthritis or giant cell arteritis may result from recognizing self tissues as being non-self. The end result from an infectious standpoint is increased incidence of infection, increased morbidity and mortality, and increased secondary complications. Interestingly the symptoms and signs of infection may be attenuated or absent because of the diminished strength of the immune response. Immunosenescent individuals mount lower inflammatory levels of IL-1, IL-6, TNF-alpha, etc. Because these cytokines are what leads to manifestations of fever, waiting for a temperature of F may be too insensitive to detect infection. Other comorbidities also contribute to the difficulty at detecting infection. In frail, old patients, a high index of suspicion for infection is important. All cause mortality is increased epidemiologically during times of epidemic infection (such as influenza virus season) believed to be linked to increased inflammation destabilizing atherosclerotic plaques leading to thrombotic events. While proof of acute inflammation causing thrombotic events is not as strong as chronic inflammation, it is strongly suspected this is part of the mechanism leading to this increase in morbidity and mortality.")
13
Aşı ile önlenebilir hastalıklardan erişkin kişi ölüm= 60,000
Neden Erişkin Aşılama? Aşı ile önlenebilir hastalıklardan erişkin kişi ölüm= 60,000 Çocuk ölümlerinden 200 kat daha fazla (300 çocuk ölümü). From: IOM, Calling the Shots: Immunization Finance Policies and Practices, 2000.
. From: IOM, Calling the Shots: Immunization Finance Policies and Practices,")
14
Erişkinleri etkileyebilecek Aşı ile önlenebilir hastalıklar: Öngörülen Yıllık Yük (US)a
Pneumokokal Hastalık1 Pnömoni nedenli 175,000 hastaneye yatış 50,000 bakteremi vakası 3,000–6,000 menenjit vakası Influenza2 >200,000 hastaneye yatış >50 yaş hastalar riskli grup yaklaşık 36,000 ölüm ilişkilendirilmiş komplikasyonlara bağlıdır Human Papillomavirus (HPV) Serviks kanseri nedenli ~3,700 ölüm 3 ~1.4 milyon yeni serviks displazi vakası8 1 milyon yeni genital siğil vakası4 Hepatit B 2006’da 4,713 akut semptomatik vaka bildirilmiş ve 46,000 yeni vaka olduğu tahmin edilmektedir5 Bildirilmiş vakalarda fatalite oranı 0.5% ila1%dir ve en yüksek de 60 yaş üstü hastalarda görülmüştür6 Herpes Zoster Yaklaşık 1 milyon yeni vaka7 US Erikinlerinin %90ınından fazlası zoster’e açıktır8 Hayatboyu risk yaklaşık %30dur9 Immunosenescence is not just an inability to fight off infection with aging. It is a dysfunction of immune processes overall. Infectious incidence is only one manifestation of this. Another common manifestation can be seen in the increased incidence in cancer as the immune system is less able to regulate its self/non-self recognition, allowing neoplasms that would have previously been destroyed to go undetected. Similarly, pro-inflammatory disease processes, such as arthritis or giant cell arteritis may result from recognizing self tissues as being non-self. The end result from an infectious standpoint is increased incidence of infection, increased morbidity and mortality, and increased secondary complications. Interestingly the symptoms and signs of infection may be attenuated or absent because of the diminished strength of the immune response. Immunosenescent individuals mount lower inflammatory levels of IL-1, IL-6, TNF-alpha, etc. Because these cytokines are what leads to manifestations of fever, waiting for a temperature of F may be too insensitive to detect infection. Other comorbidities also contribute to the difficulty at detecting infection. In frail, old patients, a high index of suspicion for infection is important. All cause mortality is increased epidemiologically during times of epidemic infection (such as influenza virus season) believed to be linked to increased inflammation destabilizing atherosclerotic plaques leading to thrombotic events. While proof of acute inflammation causing thrombotic events is not as strong as chronic inflammation, it is strongly suspected this is part of the mechanism leading to this increase in morbidity and mortality. aNumber of cases shown on the slide may also include persons <18 years of age 1. Centers for Disease Control and Prevention. In: Atkinson W et al. Epidemiology and Prevention of Vaccine-Preventable Diseases—The Pink Book. Pneumococcal Disease. 10th ed. Public Health Foundation; 2007:255– Nichol KL. Cleve Clin J Med. 2006;73:1009– American Cancer Society. Cancer Facts & Figures Atlanta, Ga: American Cancer Society; 2007:4. 4. Fleischer AB et al. Sex Transm Dis. 2001;28:643– Centers for Disease Control and Prevention. Surveillance for acute viral hepatitis — United States, MMWR. 2008;57(SS-2):1– CDC. MMWR. 2006;55(RR-16):1– Insinga RP et al. J Gen Intern Med. 2005;20:748– Gnann JW et al. N Engl J Med. 2002;347:340– Yawn, BP et al. Mayo Clin Proc. 2007;82(11):1341–1349.
 Serviks kanseri nedenli ~3,700 ölüm 3. ~1.4 milyon yeni serviks displazi vakası8. 1 milyon yeni genital siğil vakası4. Hepatit B. 2006’da 4,713 akut semptomatik vaka bildirilmiş ve 46,000 yeni vaka olduğu tahmin edilmektedir5. Bildirilmiş vakalarda fatalite oranı 0.5% ila1%dir ve en yüksek de 60 yaş üstü hastalarda görülmüştür6. Herpes Zoster. Yaklaşık 1 milyon yeni vaka7. US Erikinlerinin %90ınından fazlası zoster’e açıktır8. Hayatboyu risk yaklaşık %30dur9. Immunosenescence is not just an inability to fight off infection with aging. It is a dysfunction of immune processes overall. Infectious incidence is only one manifestation of this. Another common manifestation can be seen in the increased incidence in cancer as the immune system is less able to regulate its self/non-self recognition, allowing neoplasms that would have previously been destroyed to go undetected. Similarly, pro-inflammatory disease processes, such as arthritis or giant cell arteritis may result from recognizing self tissues as being non-self. The end result from an infectious standpoint is increased incidence of infection, increased morbidity and mortality, and increased secondary complications. Interestingly the symptoms and signs of infection may be attenuated or absent because of the diminished strength of the immune response. Immunosenescent individuals mount lower inflammatory levels of IL-1, IL-6, TNF-alpha, etc. Because these cytokines are what leads to manifestations of fever, waiting for a temperature of F may be too insensitive to detect infection. Other comorbidities also contribute to the difficulty at detecting infection. In frail, old patients, a high index of suspicion for infection is important. All cause mortality is increased epidemiologically during times of epidemic infection (such as influenza virus season) believed to be linked to increased inflammation destabilizing atherosclerotic plaques leading to thrombotic events. While proof of acute inflammation causing thrombotic events is not as strong as chronic inflammation, it is strongly suspected this is part of the mechanism leading to this increase in morbidity and mortality. aNumber of cases shown on the slide may also include persons <18 years of age. 1. Centers for Disease Control and Prevention. In: Atkinson W et al. Epidemiology and Prevention of Vaccine-Preventable Diseases—The Pink Book. Pneumococcal Disease. 10th ed. Public Health Foundation; 2007:255– Nichol KL. Cleve Clin J Med. 2006;73:1009– American Cancer Society. Cancer Facts & Figures Atlanta, Ga: American Cancer Society; 2007:4. 4. Fleischer AB et al. Sex Transm Dis. 2001;28:643– Centers for Disease Control and Prevention. Surveillance for acute viral hepatitis — United States, MMWR. 2008;57(SS-2):1– CDC. MMWR. 2006;55(RR-16):1– Insinga RP et al. J Gen Intern Med. 2005;20:748– Gnann JW et al. N Engl J Med. 2002;347:340– Yawn, BP et al. Mayo Clin Proc. 2007;82(11):1341–1349.")
16
Boğmaca Boğmaca aşısı ilk olarak 1914 yılında Amerika’da ruhsatlandırılmış ve 1918de difteri ve tetanoz toxoidleri ile kombine edilmiştir. 1940larda bebeklerde yaygın aşılamalar boğmaca vakalarında dramatik azalmalar sağlamıştır 1976’da tüm zamanların en düşük seviyesi olan 1000üzerinde vakaya düştü Edwards KM, DeckerM (2004) Pertussis vaccine. In: Plotkin SA, Orenstein WA, eds. Vaccines, Fourth edition. Philadelphia, United States: Saunders. Pp 471–528. Pertussis deaths–United States, 2000 (2002) MMWR Morb Mortal Wkly Rep 51: 616–618.
 Pertussis vaccine. In: Plotkin SA, Orenstein WA, eds. Vaccines, Fourth edition. Philadelphia, United States: Saunders. Pp 471–528. Pertussis deaths–United States, 2000 (2002) MMWR Morb Mortal Wkly Rep 51: 616–618.")
17
Tanı ile bildirilen Boğmaca Vakaları±, 1990-2010
±Data collection for PCR and Epi-Link began in 1995 Kaynak: CDC, National Notifiable Diseases Surveillance System and Supplemental Pertussis Surveillance System, 2010

19
Boğmaca Semptomları Neonatal apne +/- öksürük/whoop
Çocuklarda tipik semptomlar Adolesan ve erişkinlerdeki atipik semptomlar Paroksismal öksürük Hapşırık Öküsürük sonrası kusma Burun akması Inspiratuvar whoop Çok yüksek olmayan ateş Uzamış öksürük süresi (ortalama süre 36–48 gün) Özelliksiz öksürük Neonatal apne +/- öksürük/whoop Eğer çocuk büyükse/yetişkin USYE, Bronşit, sinüzit, astım gibi gözükebilir Eğer öksürük uzamışsa B. Pertussis3 olabileceğini düşün BIO/BOO/0016a/11 Cherry et al. Pediatr Infect Dis J 2005; 24(5 Suppl): S25–34; Brooks, Clover. J Am Board Fam Med 2006; 19: 603–11; 3. Wirsing von König et al. Lancet Infect Dis 2002; 2:744–50
 Özelliksiz öksürük. Neonatal apne +/- öksürük/whoop. Eğer çocuk büyükse/yetişkin USYE, Bronşit, sinüzit, astım gibi gözükebilir. Eğer öksürük uzamışsa B. Pertussis3 olabileceğini düşün. BIO/BOO/0016a/11. Cherry et al. Pediatr Infect Dis J 2005; 24(5 Suppl): S25–34; Brooks, Clover. J Am Board Fam Med 2006; 19: 603–11; 3. Wirsing von König et al. Lancet Infect Dis 2002; 2:744–50.")
20
Bir bebeğin yaşam mücadelesi

21
Korumacı Bağışıklama Stratejisi
Yeni anneler Aile bireyleri Bağışıklanmamış ya da tam bağışıklanması tamamlanmamış bebeklerin yakın temasında olanların Seçici İmmunizasyonu Sağlık Çalışanları Çocuk bakımında çalışanlarda Seçici İmmunizasyon

23
İnternet kaynakları CDC BoğmacaWeb sayfası
Hastalığa bakış, podcastler, aşı tavsiyeleri, örnek alma videoları vs. Ailelerle Aşı Konuşmaları CDC, AAP, ve AAFP tarafından hazırlanmışlardır

25
VZV aşıları Varisella - aşı öncesi ABD’de yılda 4 milyon vaka
% 90’dan fazlası çocuklar Yaklaşık hastaneye yatış 20 yaş altında yıllık ölüm Tek antijenli, MMR ile kombine MMRV

26
web.uct.ac.za/depts/mmi/jmoodie/vzv-clin.gif

27
Varicella Zoster Primer Enfeksiyon Sürecinde Latent Hale Gelir
Dorsal kök gangliyonu VZV duysal sinir boyunca dorsal kök gangliyonuna gider Omurilik Varisella döküntüsü Deri Viral latency is established during the primary varicella zoster virus (VZV) infection.1 The virus is transported from the infected dermal site to the dorsal root ganglion, where it lies dormant.1 There are 2 possible mechanisms for VZV transport to dorsal root ganglia:2 One mechanism involves retrograde axonal transport from infected cutaneous sites. The other mechanism involves direct hematogenous spread to the sensory ganglia. VZV most often remains dormant in dorsal root ganglia (thoracic and cervical nerves) and cranial nerve ganglia (trigeminal).2 1. Straus SE et al. In: Freedberg IM et al, eds. Fitzpatrick’s Dermatology in General Medicine. 5th ed. Vol 2. McGraw-Hill; 1999:2427–2450. 2. Silverstein S et al. In: Arvin AM et al, eds. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge, UK: Cambridge University Press; 2000:123–141. VZV dorsal kök gangliyonlarında latent olarak varlığını sürdürür VZV=varisella zoster virüsü. Image adapted from Johnson RW. Expert Rev Vaccines. 2010;9(3 Suppl):21–26. Straus SE et al. In: Freedberg IM et al, eds. Fitzpatrick’s Dermatology in General Medicine. 5th ed. Vol 2. McGraw-Hill; 1999:2427–2450.
 infection.1. The virus is transported from the infected dermal site to the dorsal root ganglion, where it lies dormant.1. There are 2 possible mechanisms for VZV transport to dorsal root ganglia:2. One mechanism involves retrograde axonal transport from infected cutaneous sites. The other mechanism involves direct hematogenous spread to the sensory ganglia. VZV most often remains dormant in dorsal root ganglia (thoracic and cervical nerves) and cranial nerve ganglia (trigeminal) Straus SE et al. In: Freedberg IM et al, eds. Fitzpatrick’s Dermatology in General Medicine. 5th ed. Vol 2. McGraw-Hill; 1999:2427– Silverstein S et al. In: Arvin AM et al, eds. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge, UK: Cambridge University Press; 2000:123–141. VZV dorsal kök gangliyonlarında latent olarak varlığını sürdürür. VZV=varisella zoster virüsü. Image adapted from Johnson RW. Expert Rev Vaccines. 2010;9(3 Suppl):21–26. Straus SE et al. In: Freedberg IM et al, eds. Fitzpatrick’s Dermatology in General Medicine. 5th ed. Vol 2. McGraw-Hill; 1999:2427–2450.")
28
Latent VZV Enfeksiyonunun Yeniden Aktifleşmesi Herpes Zosterin Klinik Tablolarıyla Sonuçlanır1–3
Akut fotofobi, ağrı, baş ağrısı, kırıklık Prodromal Faz Akut Faz Komplikasyonlar İyileşir Karakteristik dermatomal döküntü (tek taraflı), dokunmaya karşı duyarlılıkta değişiklik, ağrı, kaşıntı The presentation and subsequent resolution of zoster may not always be straightforward. The zoster rash is often preceded by several days of a prodromal phase that is characterized by pain that may range from tingling, itching, and burning to severe sharp, stabbing, or lancinating. Headache, photophobia, and malaise may also occur.1,2 Dermatomal pain and sensory abnormalities may precede development of the vesicular rash by 1 to 5 days.3 Forty percent of patients experience pain more than 4 days before the eruption of the characteristic vesicular rash.4 Prodromal pain may mimic several other conditions, such as pleurisy, early glaucoma, myocardial infarction, biliary or renal colic, or appendicitis. This may lead to misdiagnosis and inappropriate treatment.5 The zoster rash, itself, is generally limited to 1 or 2 unilateral dermatomes. Frequently reported symptoms include altered sensitivity to touch, pain provoked by slight stimuli, and unbearable itching.1,2 Lesions usually last 7 to 10 days and the rash fully heals within 2 to 4 weeks.2 Complications of zoster may include postherpetic neuralgia (PHN), scarring, bacterial superinfection, cranial and motor neuron palsies, visual impairment, and hearing loss.1,6 Although most complications will resolve over time, some patients are refractory to treatments and may suffer permanent impairment.1,2,7 1. Weaver BA. J Am Osteopath Assoc. 2009;109(6 suppl 2):S2–S6. 2. Harpaz R et al. MMWR. 2008;57(RR–5):1–30. 3. Gnann JW Jr, Whitley RJ. Herpes zoster. N Engl J Med. 2002;347:340–346. 4. Lycka BAS, Williamson D, Sibbald RG. Dermatologic aspects of herpes zoster. In: Watson CPN, Gershon AA, eds. Herpes Zoster and Postherpetic Neuralgia, 2nd Revised and Enlarged Edition. Vol 11. Amsterdam, The Netherlands: Elsevier Science BV; 2001:97–106. 5. Straus SE, Oxman MN. Varicella and herpes zoster. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s Dermatology in General Medicine. Vol 2. 5th ed. New York, NY: McGraw–Hill; 1999:2427–2450. 6. Oxman MN. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge University Press; 2000:246–275. 7. Watson CPN et al. Pain. 1991;46:195–199. Görülebilir veya görülmeyebilir; PHN yaygın bir komplikasyondur PHN=postherpetik nevralji; VZV=varisella zoster viüsü. 1. Oxman MN. In: Arvin AM et al, eds. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge, UK: Cambridge University Press; 2000:246– Harpaz R et al. MMWR. 2008;57(RR–5):1–30. 3. Weaver BA. J Am Osteopath Assoc. 2009;109(6 suppl 2):S2–S6.
, dokunmaya karşı duyarlılıkta değişiklik, ağrı, kaşıntı. The presentation and subsequent resolution of zoster may not always be straightforward. The zoster rash is often preceded by several days of a prodromal phase that is characterized by pain that may range from tingling, itching, and burning to severe sharp, stabbing, or lancinating. Headache, photophobia, and malaise may also occur.1,2. Dermatomal pain and sensory abnormalities may precede development of the vesicular rash by 1 to 5 days.3 Forty percent of patients experience pain more than 4 days before the eruption of the characteristic vesicular rash.4. Prodromal pain may mimic several other conditions, such as pleurisy, early glaucoma, myocardial infarction, biliary or renal colic, or appendicitis. This may lead to misdiagnosis and inappropriate treatment.5. The zoster rash, itself, is generally limited to 1 or 2 unilateral dermatomes. Frequently reported symptoms include altered sensitivity to touch, pain provoked by slight stimuli, and unbearable itching.1,2. Lesions usually last 7 to 10 days and the rash fully heals within 2 to 4 weeks.2. Complications of zoster may include postherpetic neuralgia (PHN), scarring, bacterial superinfection, cranial and motor neuron palsies, visual impairment, and hearing loss.1,6. Although most complications will resolve over time, some patients are refractory to treatments and may suffer permanent impairment.1,2,7. 1. Weaver BA. J Am Osteopath Assoc. 2009;109(6 suppl 2):S2–S6. 2. Harpaz R et al. MMWR. 2008;57(RR–5):1– Gnann JW Jr, Whitley RJ. Herpes zoster. N Engl J Med. 2002;347:340– Lycka BAS, Williamson D, Sibbald RG. Dermatologic aspects of herpes zoster. In: Watson CPN, Gershon AA, eds. Herpes Zoster and Postherpetic Neuralgia, 2nd Revised and Enlarged Edition. Vol 11. Amsterdam, The Netherlands: Elsevier Science BV; 2001:97– Straus SE, Oxman MN. Varicella and herpes zoster. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s Dermatology in General Medicine. Vol 2. 5th ed. New York, NY: McGraw–Hill; 1999:2427– Oxman MN. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge University Press; 2000:246– Watson CPN et al. Pain. 1991;46:195–199. Görülebilir veya görülmeyebilir; PHN yaygın bir komplikasyondur. PHN=postherpetik nevralji; VZV=varisella zoster viüsü. 1. Oxman MN. In: Arvin AM et al, eds. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge, UK: Cambridge University Press; 2000:246– Harpaz R et al. MMWR. 2008;57(RR–5):1– Weaver BA. J Am Osteopath Assoc. 2009;109(6 suppl 2):S2–S6.")
29
Herpes Zoster Riski Amerika Birleşik Devletleri’nde zoster riski yüksektir1 40 yaş ve üzeri yetişkinlerin yaklaşık %99.5’i, VZV-IgG (+) Zosterin insidansı ve şiddeti yaşla birlikte artar1,2 Batı ülkelerinde hayatın bir döneminde zona olma olasılığı % Benbernou A, Eur J Pain 2011; 15:1100-6 In the United States, about 99.5% of adults aged 40 years and older are at risk for zoster because they have had chickenpox.1 Although specific components of cell-mediated immunity have an important role in controlling the development of zoster, the exact triggers for reactivation of the virus are unknown. Thus, it is impossible to predict if and when someone will get zoster.1 Age is the most important risk factor for developing zoster. The incidence and severity of zoster increases with age.1,2 Of the estimated 1 million new cases per year,1,3 approximately 70% occur in adults 50 years of age and older.4 By 85 years of age, approximately 50% of individuals will have had zoster.1,5 According to the Centers for Disease Control and Prevention, the overall lifetime risk of developing zoster is approximately 1 in 3.1 1. Harpaz R et al. MMWR. 2008;57(RR–5):1–30. 2. Oxman MN et al. N Engl J Med. 2005;352:2271–2284. 3. Insinga RP et al. J Gen Intern Med. 2005;20:748–753. 4. Pappagallo M et al. CNS Drugs. 2003;17:771–780. 5. Schmader KE. Clin Infect Dis. 2001;32:1481–1486. CDC’ye göre yaklaşık olarak her 3 kişiden 1’inde yaşamlarının bir döneminde zoster gelişecektir1 CDC=Hastalık Kontrol ve Önleme Merkezleri; VZV=varisella zoster virüsü. 1. Harpaz R et al. MMWR. 2008;57(RR–5):1– Oxman MN et al. N Engl J Med. 2005;352:2271– Insinga RP et al. J Gen Intern Med. 2005;20:748– Pappagallo M et al. CNS Drugs. 2003;17:771– Schmader KE. Clin Infect Dis. 2001;32:1481–1486.
:1– Oxman MN et al. N Engl J Med. 2005;352:2271– Insinga RP et al. J Gen Intern Med. 2005;20:748– Pappagallo M et al. CNS Drugs. 2003;17:771– Schmader KE. Clin Infect Dis. 2001;32:1481–1486. CDC’ye göre yaklaşık olarak her 3 kişiden 1’inde yaşamlarının bir döneminde zoster gelişecektir1. CDC=Hastalık Kontrol ve Önleme Merkezleri; VZV=varisella zoster virüsü. 1. Harpaz R et al. MMWR. 2008;57(RR–5):1– Oxman MN et al. N Engl J Med. 2005;352:2271– Insinga RP et al. J Gen Intern Med. 2005;20:748– Pappagallo M et al. CNS Drugs. 2003;17:771– Schmader KE. Clin Infect Dis. 2001;32:1481–1486.")
30
2000 Yılında Yaş Grubuna göre Zoster İnsidansı
Vaka sayısı 1000 kişi-yıl başına orana Zoster Vakalarının Sayısı (n = 9,152) Oran/ 1000 Kişi-Yıl The number zoster cases increases with age, with the highest incidence occurring in individuals 50 years of age and older.1 1. Insinga RP et al. J Gen Intern Med. 2005;20:748–753. Yaş a2000 yılındaki A.B.D. nüfusu için yaşa spesifik oranlar Insinga RP et al. J Gen Intern Med. 2005;20:748–753.
 Oran/ 1000 Kişi-Yıl. The number zoster cases increases with age, with the highest incidence occurring in individuals 50 years of age and older Insinga RP et al. J Gen Intern Med. 2005;20:748–753. Yaş. a2000 yılındaki A.B.D. nüfusu için yaşa spesifik oranlar. Insinga RP et al. J Gen Intern Med. 2005;20:748–753.")
31
Zosterin Komplikasyonları
Nörolojik1,2 Postherpetik nevralji (PHN, en yaygın) Zosterli hastaların %10-%18’inde görülür Duyum kaybı, allodini (ağrılı olmayan uyarana ağrı yanıtı), kranyal ve motor nöron felçleri, meningoensefalit, işitme kaybı Oftalmik1,2 Oftalmik Herpes zoster (OHZ) Zosterli hastaların %10-%25’inde görülür Görme bozukluğu, ptozis (göz kapağı düşüklüğü), ağrı, yüzde skarlaşma Keratit OHZ’li hastaların yaklaşık üçte ikisinde görülür Deri tutulumları2 Skarlaşma, bakteri süperenfeksiyonu İç organların tutulumu (nadir)2 Hepatit, miyokardit, perikardit, artrit © Hemera Technologies/ AbleStock.com/ Jupiter Images. Gerçek hasta değildir. Complications of Zoster (continued) Postherpetic neuralgia (PHN) is a common complication of zoster.1,2 When PHN occurs, loss of sensation may occur within an affected dermatome, and other neurologic complications may include cranial and motor neuron palsies, encephalitis, and hearing loss.2 The risk for PHN in patients with zoster is about 10% to 18%.1 Ophthalmic involvement (herpes zoster ophthalmicus [HZO]), occurring in 10% to 25% of patients with zoster, may lead to visual loss, prolonged or permanent pain, and/or facial scarring. Keratitis also occurs in about two-thirds of patients with HZO.1 Cutaneous complications can occur with zoster and may include scarring and potential bacterial superinfection, usually with Staphylococcus aureus. Infections with group A beta hemolytic Streptococcus may occur in approximately 2% of patients with zoster.2 Potential visceral complications of zoster are rare, but may include hepatitis, myocarditis, pericarditis, and arthritis.2 1. Harpaz R et al. MMWR Morb Mortal Wkly Rep. 2008;57(RR-5):1–30. 2. Oxman MN. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge University Press; 2000:246–275. Pavan-Langston D. Ophthalmic zoster. In: Arvin AM, Gershon AA, eds. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge, UK: Cambridge University Press; 2000:276–298. İzinle basılmıştır. 1. Harpaz R et al. MMWR Morb Mortal Wkly Rep. 2008;57(RR-5):1–30. 2. Oxman MN. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge University Press; 2000:246–275.
 Zosterli hastaların %10-%18’inde görülür. Duyum kaybı, allodini (ağrılı olmayan uyarana ağrı yanıtı), kranyal ve motor nöron felçleri, meningoensefalit, işitme kaybı. Oftalmik1,2. Oftalmik Herpes zoster (OHZ) Zosterli hastaların %10-%25’inde görülür. Görme bozukluğu, ptozis (göz kapağı düşüklüğü), ağrı, yüzde skarlaşma. Keratit OHZ’li hastaların yaklaşık üçte ikisinde görülür. Deri tutulumları2. Skarlaşma, bakteri süperenfeksiyonu. İç organların tutulumu (nadir)2. Hepatit, miyokardit, perikardit, artrit. © Hemera Technologies/ AbleStock.com/ Jupiter Images. Gerçek hasta değildir. Complications of Zoster (continued) Postherpetic neuralgia (PHN) is a common complication of zoster.1,2 When PHN occurs, loss of sensation may occur within an affected dermatome, and other neurologic complications may include cranial and motor neuron palsies, encephalitis, and hearing loss.2 The risk for PHN in patients with zoster is about 10% to 18%.1. Ophthalmic involvement (herpes zoster ophthalmicus [HZO]), occurring in 10% to 25% of patients with zoster, may lead to visual loss, prolonged or permanent pain, and/or facial scarring. Keratitis also occurs in about two-thirds of patients with HZO.1. Cutaneous complications can occur with zoster and may include scarring and potential bacterial superinfection, usually with Staphylococcus aureus. Infections with group A beta hemolytic Streptococcus may occur in approximately 2% of patients with zoster.2. Potential visceral complications of zoster are rare, but may include hepatitis, myocarditis, pericarditis, and arthritis Harpaz R et al. MMWR Morb Mortal Wkly Rep. 2008;57(RR-5):1– Oxman MN. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge University Press; 2000:246–275. Pavan-Langston D. Ophthalmic zoster. In: Arvin AM, Gershon AA, eds. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge, UK: Cambridge University Press; 2000:276–298. İzinle basılmıştır. 1. Harpaz R et al. MMWR Morb Mortal Wkly Rep. 2008;57(RR-5):1– Oxman MN. Varicella-Zoster Virus: Virology and Clinical Management. Cambridge University Press; 2000:246–275.")
32
Antiviral tedavi İlk 72 saatte verilen antiviral tedavi – yeni lezyon oluşumunu azaltıyor, kurutlanmayı hızlandırıyor, viral saçılma süresini kısaltıyor. Cohen JI, N Engl J Med 2013;369: Ama meta-analizler PNH’e önemli etkisi olmadığını gösteriyor. Tyring SK, Arch Fam Med 2000;9:863-9.

33
Canlı Zoster Aşısı Kullanımına İlişkin ACIP Tavsiyeleri1
CDC’nin Bağışıklama Uygulamaları Danışma Komitesi’ne göre, Herpes zoster aşısı 60 yaş ve üzeri uygun nitelikteki tüm hastalara klinikte ilk karşılamada teklif edilmelidir. (Daha önce zona geçirenlere de verilebilir) Gebeler, primer ve akkiz immun yetmezliği olanlar veya jelatin, neomycin veya diğer aşı komponentlerine allerji öyküsü olanlara aşı verilmemeli Diğer koruyucu önlemlerle bağlantı kurulmalı ACIP Recommendations for Use of ZOSTAVAX® (Zoster Vaccine Live) These recommendations represent the ACIP’s statement on the use of a live attenuated vaccine for the prevention of herpes zoster and its sequelae.1 1 dose of zoster vaccine is recommended at first available clinical encounter for all persons aged ≥ 60 years who have no contraindications.1 ACIP-recommended strategies to promote zoster vaccination include1: “…linking delivery of zoster vaccine to delivery of other preventive-health interventions.” “Residents of nursing homes and other long-term–care facilities who are at least aged 60 years and without contraindications should be included in routine zoster vaccination activities.” 1.Harpaz R et al. MMWR Morb Mortal Wkly Rep. 2008;57(RR-5):1–30. ACIP = Bağışıklama Uygulamaları Danışma Komitesi 1. Centers for Disease Control and Prevention (CDC). Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2008;57(RR-5):1-30.
 Gebeler, primer ve akkiz immun yetmezliği olanlar veya jelatin, neomycin veya diğer aşı komponentlerine allerji öyküsü olanlara aşı verilmemeli. Diğer koruyucu önlemlerle bağlantı kurulmalı. ACIP Recommendations for Use of ZOSTAVAX® (Zoster Vaccine Live) These recommendations represent the ACIP’s statement on the use of a live attenuated vaccine for the prevention of herpes zoster and its sequelae.1. 1 dose of zoster vaccine is recommended at first available clinical encounter for all persons aged ≥ 60 years who have no contraindications.1. ACIP-recommended strategies to promote zoster vaccination include1: …linking delivery of zoster vaccine to delivery of other preventive-health interventions. Residents of nursing homes and other long-term–care facilities who are at least aged 60 years and without contraindications should be included in routine zoster vaccination activities. 1.Harpaz R et al. MMWR Morb Mortal Wkly Rep. 2008;57(RR-5):1–30. ACIP = Bağışıklama Uygulamaları Danışma Komitesi. 1. Centers for Disease Control and Prevention (CDC). Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2008;57(RR-5):1-30.")
34
Major Clinical Forms of Pneumococcal Disease
Invasive Noninvasive (Mucosal) Meningitis Bacteremia Pneumonia Acute Otitis Media Sinusitis Pneumococcal disease can be broadly grouped into categories of invasive disease and non ‐invasive (also termed “mucosal”) disease1 Non ‐invasive forms of disease may become invasive, eg, pneumonia when accompanied by bacteremia is considered invasive 2 Acute Respiratory Infections (Update September 2009). February 8, 2010. 2. CDC. Epidemiology and prevention of vaccine‐preventable diseases. 11th ed. 2009;217–230.
 Meningitis. Bacteremia. Pneumonia. Acute Otitis Media. Sinusitis. Pneumococcal disease can be broadly grouped into categories of invasive disease and non ‐invasive (also termed mucosal ) disease1. Non ‐invasive forms of disease may become invasive, eg, pneumonia when accompanied by bacteremia is considered invasive 2. Acute Respiratory Infections (Update September 2009). February 8, CDC. Epidemiology and prevention of vaccine‐preventable diseases. 11th ed. 2009;217–230.")
35
IPD’s in adults is largely bacteremia due to pneumonia
Distribution of clinical syndromes in IPD in the Netherlands (2004 ‐2006) Jansen et al. Vaccine 2009 ;27(17):2394 ‐401
 Jansen et al. Vaccine 2009 ;27(17):2394 ‐401.")
36
Burden of CAP: Overview
Annual incidence of CAP diagnosed in the community is 5–11 per adult population1 Between 22% and 42% of cases of CAP in adults are hospitalized1 Long-term mortality of adults aged ≥18 years with CAP is between 35.8% and 39.1% at 5 years (US and Canada)1 Case fatality rate of 4.5% in those aged 18–50 years (Portugal) to 47.2% in those aged 85 years and over (UK)2 19–31% of adult patients with CAP not back at work or not back to normal health by 6–8 weeks; 55% in the elderly3 Estimated costs of CAP in hospitalized patients From median $1,331 per case (Germany)4 to €1,586 (Italy)5 Only a few quality of life studies have been carried out in Europe:6 Dutch study found that 18 months after their diagnosis of CAP, patients had significantly lower scores on physical functioning and general health compared to matched controls Patients with co-morbidities had lower quality of life scores 1. Lim WS, et al. Thorax. 2009;64(Suppl III):iii1–iii55. doi: /thx Welte T, et al. Thorax doi: /thx 3. European Lung Foundation Bauer TT, et al. Chest. 2005;128;2238–2246. 5. De Negro R, et al. Monaldi Arch Chest Dis. 2002;57(1):3– Moussaoui R, et al. Chest. 2006;130;1165–1172. 36 36
1. Case fatality rate of 4.5% in those aged 18–50 years (Portugal) to 47.2% in those aged 85 years and over (UK)2. 19–31% of adult patients with CAP not back at work or not back to normal health by 6–8 weeks; 55% in the elderly3. Estimated costs of CAP in hospitalized patients. From median $1,331 per case (Germany)4 to €1,586 (Italy)5. Only a few quality of life studies have been carried out in Europe:6. Dutch study found that 18 months after their diagnosis of CAP, patients had significantly lower scores on physical functioning and general health compared to matched controls. Patients with co-morbidities had lower quality of life scores. 1. Lim WS, et al. Thorax. 2009;64(Suppl III):iii1–iii55. doi: /thx Welte T, et al. Thorax doi: /thx European Lung Foundation Bauer TT, et al. Chest. 2005;128;2238– De Negro R, et al. Monaldi Arch Chest Dis. 2002;57(1):3– Moussaoui R, et al. Chest. 2006;130;1165–")
37
Economic Burden of CAP in Europe
*Total costs of pneumonia in Europe are €10.1 billion each year Welte T, et al. Thorax Epub. (doi: /thx )
")
38
Pnomokok aşısı 19 yaş ve daha ileri yaşta immünkompromize (kronik böbrek yetmezliği, nefrotik sendrom), fonksiyonel yada anatomik asplenik olanlarda, BOS kaçağı olan veya kohlear implant takılanlarda tek doz PCV13 aşısının ardından 8 hafta sonra PPSV23 yapılmalıdır.
, fonksiyonel yada anatomik asplenik olanlarda, BOS kaçağı olan veya kohlear implant takılanlarda tek doz PCV13 aşısının ardından 8 hafta sonra PPSV23 yapılmalıdır.")
40
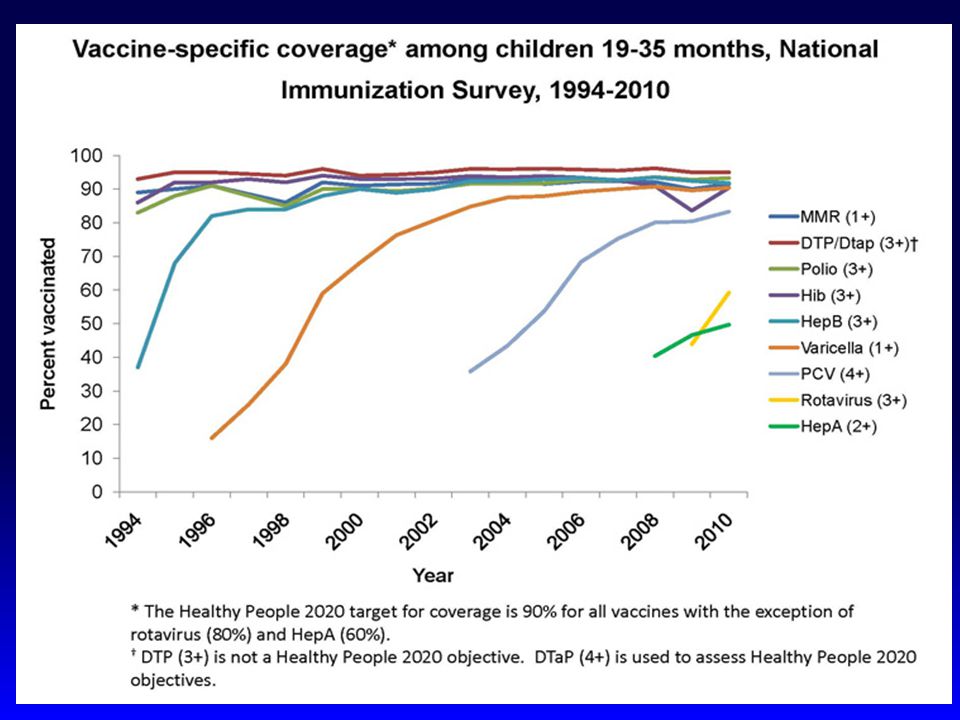
Erişkin Aşılanma Oranları, 2010
Estimated Vaccination Rates and Healthy People 2020 Goals (%) Goal1 Rate3 Pneumococcal Herpes Zoster Hepatitis B Rate2 Influenza a aGoal for persons 18 to 64 years of age. 1. US Department of Health and Human Services. healthypeople.gov/2020/topicsobjectives2020/pdfs/HP2020objectives.pdf. Accessed May 14, 2012. 2. Centers for Disease Control and Prevention (CDC). Final state specific influenza vaccination coverage estimates for the 2010–11 season—United States, National Immunization Survey and Behavioral Risk Factor Surveillance System, August 2010 through May cdc.gov/flu/professionals/vaccination/coverage_1011estimates.htm. Accessed April 13, 2012. 3. CDC. MMWR. 2012;61:61–80.
 Goal1. Rate3. Pneumococcal. Herpes Zoster. Hepatitis B. Rate2. Influenza. a. aGoal for persons 18 to 64 years of age. 1. US Department of Health and Human Services. healthypeople.gov/2020/topicsobjectives2020/pdfs/HP2020objectives.pdf. Accessed May 14, Centers for Disease Control and Prevention (CDC). Final state specific influenza vaccination coverage estimates for the 2010–11 season—United States, National Immunization Survey and Behavioral Risk Factor Surveillance System, August 2010 through May cdc.gov/flu/professionals/vaccination/coverage_1011estimates.htm. Accessed April 13, CDC. MMWR. 2012;61:61–80.")
41
Elisabeth E. Kanitza, et. al
Elisabeth E. Kanitza, et. al. Variation in adult vaccination policies across Europe: An overview from VENICE network on vaccine recommendations, funding and coverage Vaccine 30?(2012)
")
42
Cocuklu Çağı Aşılama Oranları 2002-2008 Türkiye
First 7 mo. *2006 yılından itibaren Kızamık aşısı yerine KKK aşısı ve 2008 yılından itibaren DBT aşısı yerine DaBT-IPV-Hib aşısı uygulanmaya başlanmıştır. 42 42

44
Türkiye’deki güncel kapsama
Türkiye’de ve pekçok ülkede erişkinlerde aşılamada kapsama hedefi yoktur TIHUD, Ege Bölgesi Çalışma Grubu

47
Sağlık Bakanlığı Erişkin Bağışıklama Kılavuzu, 2009

48
Türkiye’deki Pnömokok ve Influenza Aşılama Tavsiyeleri
Pnömokok aşısı1 2 yaşından büyük olup aşağıdakilerden birine sahip her bireyde; aspleni, dalak fonksiyon bozukluğunda, splenektomi (medikal, cerrahi, ve otosplenektomi) , Orak hücreli Anemi, immunsuppresif tedavi almış olmak, radyoterapi, organ transplantasyonu, HIV, tüm immun yetmezlikler, Kronik renal hastalıklar ve nefrotik sendrom, Kronik kalp hastalıkları, Astım dahil KOAH, Siroz dahil kronik karaciğer hastalıkları, diyabet, hemoglobinopatiler, kranyal defektler, santral sinir sistemi sıvı kaçakları dahil her hangi bir merabolik hastalık Influenza aşısı2 ≥ 65 yaş Kronik hastalığı olan çocuk ver eriişkinlerde Pulmoner (astım dahil) ve kardiyovasküler sistem renal, hepatik, hematolojik veya metabolik hastalıklar (diabetes mellitus) HIV infekte kişiler de dahil olmak üzere immun sistemi baskılanmış erişkin ve çocuklar ve immun sistem baskılayıcı ilaç kullananlar Uzun dönem aspirin tedavisi alan çocuk ve gençler(6 ay-18 yaş) Yaşlı bakımevi ve huzurevinde kalanlar Altta yatan hastalığı olan hastalar, kurum geri ödemesi için durumlarını bildirir sağlık raporu almalıdırlar yılı itibariyle katkı payı kaldırılmıştır. (Erişim tarihi )
 , Orak hücreli Anemi, immunsuppresif tedavi almış olmak, radyoterapi, organ transplantasyonu, HIV, tüm immun yetmezlikler, Kronik renal hastalıklar ve nefrotik sendrom, Kronik kalp hastalıkları, Astım dahil KOAH, Siroz dahil kronik karaciğer hastalıkları, diyabet, hemoglobinopatiler, kranyal defektler, santral sinir sistemi sıvı kaçakları dahil her hangi bir merabolik hastalık. Influenza aşısı2. ≥ 65 yaş. Kronik hastalığı olan çocuk ver eriişkinlerde. Pulmoner (astım dahil) ve kardiyovasküler sistem renal, hepatik, hematolojik veya metabolik hastalıklar (diabetes mellitus) HIV infekte kişiler de dahil olmak üzere immun sistemi baskılanmış erişkin ve çocuklar ve immun sistem baskılayıcı ilaç kullananlar. Uzun dönem aspirin tedavisi alan çocuk ve gençler(6 ay-18 yaş) Yaşlı bakımevi ve huzurevinde kalanlar. Altta yatan hastalığı olan hastalar, kurum geri ödemesi için durumlarını bildirir sağlık raporu almalıdırlar yılı itibariyle katkı payı kaldırılmıştır (Erişim tarihi )")
49
Pnömokok Aşısı - Antalya
Prospektif Çalışma Akdeniz Üniversitesi Tıp Fakültesi, Antalya 2383 Kişi ile yüz yüze görüşüldü. –Katılımcıların sadece % 10.7’si pnömokok aşısının farkında –Katılımcıların sadece % 0.9’u pnömokok aşısı yaptırmış •Doktor önerisi ile aşılanan % 68.2 •Kendi kendilerine veya çocuklarının önerisi ile aşılanan % 31.8 •Hastanede aşılanan % 45.4 •Aşıyı kendi cebinden karşılayan % 45.4 Özge Turhan ve ark. Kuwait Medical Journal 2010; 42 (2):
:")
50
18 yaş üzerinde aşılama TİHUD Kapadokya Projesi …… aşısı oldunuz mu?
Tetanoz Hepatit B Grip HPV Kuduz Diğer TİHUD Kapadokya Projesi

51
İç Hastalıkları Uzmanlık Öğrencilerinde erişkin aşılamasında düşük farkındalık
Tugba Akin Telli, Lale Ozisik, Mine Durusu Tanriover, Serhat Unal Hacettepe Universitesi Tıp Fakültesi

52
IM Residents in a Single University Hospital (n=74)
Only pneumococcus and influenza vaccines showed an increasing trend as the resident progresses through years. Self vaccination rates were also low during and after medical school: influenza 32.4%, tetanus 21.6%, hep B 71.6%, hep A 23%, measles 10.8%, MMR2.8%, dT 2.7%

53
Tugba Akin Telli, Burçin Halaçlı
Avrupa İç Hastalıkları Uzmanlık Öğrencilerinde erişkin aşılamasında farkındalık Tugba Akin Telli, Burçin Halaçlı

54
ESIM 2013 Residents (n=39)
")
55
Yaşlılarda pnömokok aşılama oranları: bir günlük bir eğitim programı ile hedef konulmasının etkileri Serhat Unal a, Mine Durusu Tanriover b Hacettepe Üniversitesi Tıp Fakültesi , Dahiliye Anabilim Dalı a Infeksiyon Bilim Dalı b Genel Dahiliye Bilim Dalı Ünal S, Durusu Tanrıöver M, Taş E, Güner İ, Çetin ÖY, Sayar İ. Pneumococcal vaccination coverage in the elderly population: before and after setting a target with a one-day educational program. FLORA 2014;19 (in press)
")
56
Müdahaleden önce belli gruplardaki eşlik eden hastalıklar ve aşılanma oranları

57
Seçilmiş aşılarda 65 yaş üzerinde aşılanma oranları
Aşılama n= (%) Tetanoz(son 10 yılda) 2.076 (2.6) Hepatit B 203 (0.3) Influenza (son bir yılda) (14) Pnömokok (son 5 yılda) 9.297 (11.6) * bir kişi birden fazla aşı ile aşılanmış olabilir
 Tetanoz(son 10 yılda) (2.6) Hepatit B. 203 (0.3) Influenza (son bir yılda) (14) Pnömokok (son 5 yılda) (11.6) * bir kişi birden fazla aşı ile aşılanmış olabilir.")
58
Pnömokok Aşısında artış > 65 y/o* Kasım 2011
6 Kat artış %60.2 %11.6 Yaşlılarda pnömokok aşılama oranları: bir günlük bir eğitim programı ile hedef konulmasının etkileri

59
Aşılanmamış olma nedenleri
* * * Hastanın beyanına göre

60
Erişkin Bağışıklanmasında Zorluklar: Pnömokok Aşısı, 2006, US
Aşılanmamada Tüketici kaynaklı sebepler Hekimlerin erişkinlerin neden aşılanmadığı konusunda açıklamaları Sağlıklı, ihtiyacı yok ~%60 Hasta sık ziyaret etmiyor %88 Doktor ihtiyacım olduğunu anlatmadı ~%58 Yan etkiler konusunda endişe %65 Yan etkiler ~%40 Bilgi eksikliği %73 Ne zaman yaptırmam gerektiğini bilmiyordum ~%25 İğne korkusu %71 Etkili olmayabilir ~%22 Etkin bir hatırlatma sistemi yok İğneden hoşlanmıyor ~%19 Yetersiz sigorta %68 Hastalık bulaşabilir ~%18 Farklı hekimler %62 Şu anki durumum kötüleşebilir ~%16 Aşı takviminin farkında değil %70 Sigortam kapsamıyor ~%15 Sağlıklı insanların ihtiyacı yok Aldığım ilaçlarla etkileşime girebilir Etkili değil Johnson DR, et al. Am J Med 2008;121:S28-S35

61
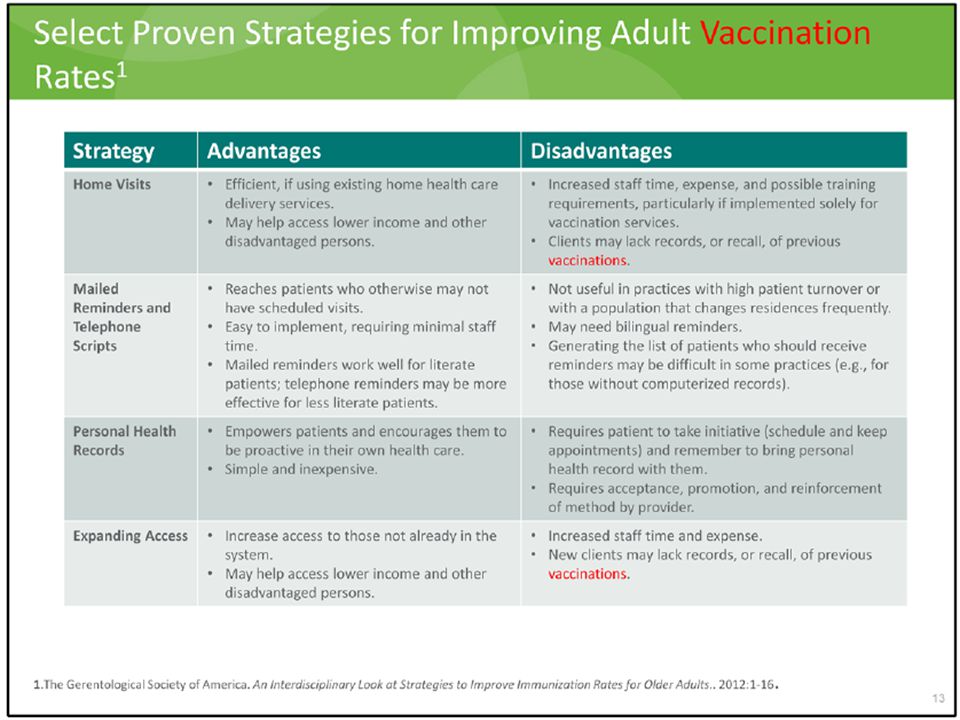
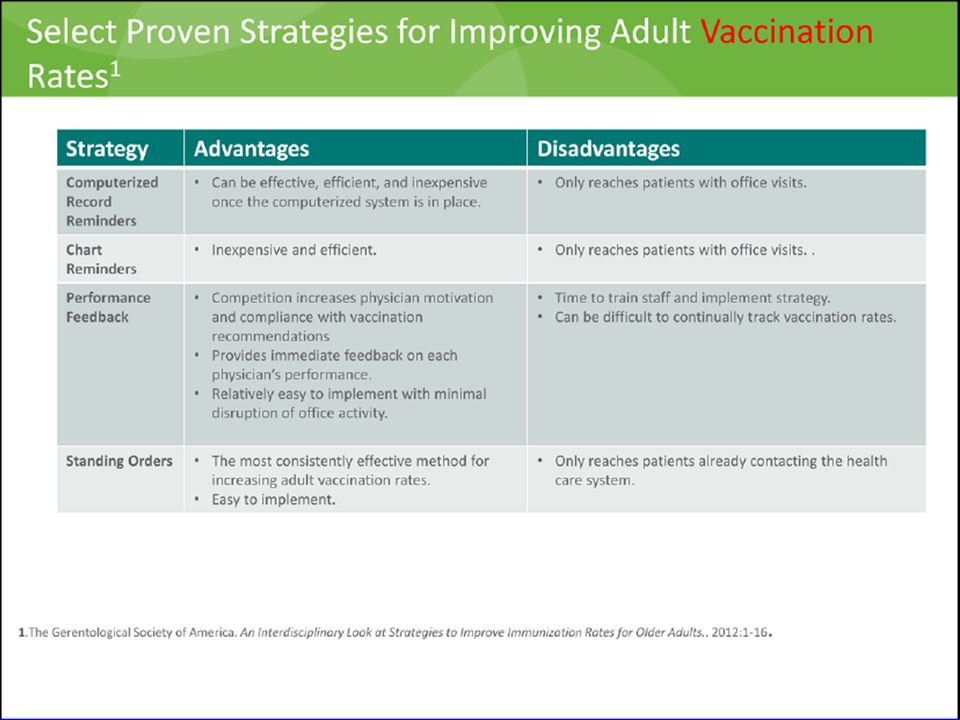
Stratejiler listesi Bekleyen siparişler Stratejiler listesi
Bilgisayarlı kayıt hatırlatıcılar Çizelge hatırlatıcılar Performans Geri Bildirimi Ev ziyaretleri Posta/telefon hatırlatmaları Sağlıkta genişletilmiş erişim Hasta eğitimi Kişisel Sağlık Kayıtları

64
Türkiye’de erişkinlerde tetanoz, difteri, boğmacı, kızamık seroprevalansı: Erişkin aşılaması için etkiler Mine Durusu Tanrıöver, Canan Aycan, Sibel Aşçıoğlu, Serhat Ünal Hacettepe Üniversitesi Tıp Fakültesi, Ankara Accepted for publication. Low seroprevalance of diphtheria, tetanus and pertussis in ambulatory adult patients: the need for lifelong vaccination. European Journal of Internal Medicine

65
Objektif Hastalar ve Metodlar Sonuçlar
Birincil amaç:erişkin ve yaşlılarda tetanoz, difteri, boğmaca ve kızamık seropozitifliğinin prevalansını araştırmak İkincil amaç: to determine the need for booster vaccination with regard to predefined cut off antibody levels. Hastalar ve Metodlar Mayıs-Aralık 2011 arasındaki erişkin ve yaşlı hastalar prospektif olarak dahil edldi. Demografik ve klinik veri: Tetanoz, difteri, boğmaca antitoksoid antikorları kan örneklemleri alındı. IgG ELISA ile belirlendi. Sonuçlar seropozitifliğe rapel ihtiyacı ve tavsiye edilen cut-off değerleri ile sağlanan korumaya göre değerlendirildi. Sonuçlar 1367 hastadan onam formu alındı kan örneklemi alındı Yaş ortalaması: 57.1 ± 15.8 (18-90) ve %68’i kadın Diyabet en sık görülen kronik hastalıktı (%23.5)
 ve %68’i kadın. Diyabet en sık görülen kronik hastalıktı (%23.5)")
66
Seropozitflik Rapel endikasyonu
Değişken Hasta sayısı(%) Tetanoz Korunma yok 899 (69) Korunma 404 (31) Difteri 849 (65.2) 454 (34.8) Kızamık 1177 (90.3) 126 (9.7) 16 (1.2) 1287 (98.8) Değişken Hasta sayısı(%) Tetanoz Aşı endike 1007 (77.3) Aşı endike değil 296 (22.7) Difteri 1256 (96.4) 47 (3.6) Kızamık 1177 (90.3) 126 (9.7) 24 (1.8) 1279 (98.2) Artan ilgi ve ulusal/uluslararası otoritelerin sürekli güncelledikleri kılavuzlara rağmen, erişkin aşılamasında kapsama çok düşüktür. Erişkin dönemdeki rapel aşılama ulusal/uluslararası otoritelerin kılavuzları doğrultusunda gereklidir.
 Tetanoz. Korunma yok. 899 (69) Korunma. 404 (31) Difteri. 849 (65.2) 454 (34.8) Kızamık (90.3) 126 (9.7) 16 (1.2) 1287 (98.8) Değişken. Hasta sayısı(%) Tetanoz. Aşı endike (77.3) Aşı endike değil. 296 (22.7) Difteri (96.4) 47 (3.6) Kızamık (90.3) 126 (9.7) 24 (1.8) 1279 (98.2) Artan ilgi ve ulusal/uluslararası otoritelerin sürekli güncelledikleri kılavuzlara rağmen, erişkin aşılamasında kapsama çok düşüktür. Erişkin dönemdeki rapel aşılama ulusal/uluslararası otoritelerin kılavuzları doğrultusunda gereklidir.")
67
“ADVICE” Avrupa Erişkin Aşı Kampanyası
Dr Lale Ozisik Dr Mine Durusu Tanrıover Dr Serhat Unal

68
Avrupada aşı ile önlenebilir hastalıkların epidemiyolojisi
Influenza Pnömokok Hepatit B Difteri-Boğmaca-Tetanoz

69
Avrupada genel erişkin aşı epidemiyolojisi
Sero-prevalans verisi Doktor farkındalık ve uyum verisi Hasta algı verisi

70
Kaynaklar/Linkler American Academy of Family Practice. Center for Disease Control. Morbidity Mortality Weekly Report. National Network for Immunization Information. Health Sentinel. Vaccine Adverse Event Reporting System. The Institute of Medicine.

Benzer bir sunumlar