Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
SEPSİS KILAVUZU : Ne değişti
Dr. Nahit Çakar Acıbadem Üniversitesi Acbadem Tıp Fakültesi Anesteziyoloji ve Reanimasyon Anabilimdalı o

2
SSK:Guidelines for Management of Severe Sepsis and Septic Shock
Sprung CL, Angus DC, Annane D, Carcillo JA, Deutschman CS, Gerlach H, Jaeschke R, Kleinpell RM, Machado FR, Opal S, Rubenfeld G, Sevransky J, Townsend SR, Dellinger RP. Dellinger RP et al. Crit Care Med. 2013;41: Dellinger RP et al. Intensive Care Med. 2013;39:

3
Başlangıç Resusitasyonu
Sepsisin oluşturduğu doku hipoperfüzyonu (başlangıç sıvı sınamasına rağmen sebat eden hipotansiyon veya laktat ≥4 mmol/L) varlığında protokollü sayısal ressusitasyon öneririz. Bu protokol hipoperfüzyon farkedildiğinde mümkün olan en erken dönemde başlanmalı YB gidişi beklememelidir. This recommendation has not changed from the 2008 version of the Surviving Sepsis Campaign (SSC) guidelines.
 varlığında protokollü sayısal ressusitasyon öneririz. Bu protokol hipoperfüzyon farkedildiğinde mümkün olan en erken dönemde başlanmalı YB gidişi beklememelidir. This recommendation has not changed from the 2008 version of the Surviving Sepsis Campaign (SSC) guidelines. ")
4
Başlangıç Resusitasyonu????
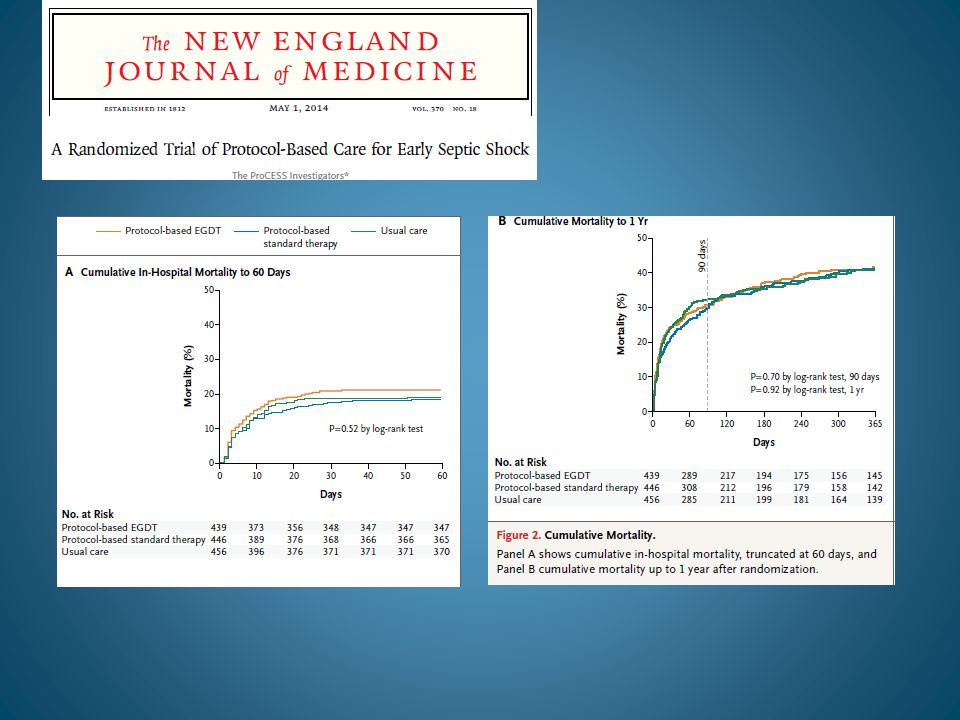
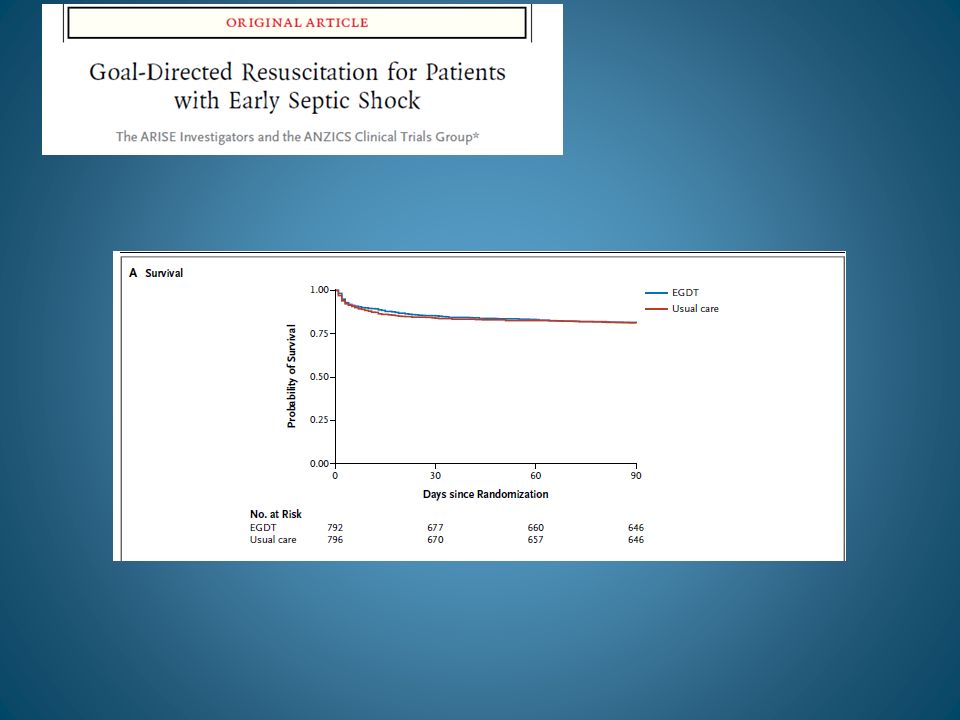
İlk 6 saat sepsise bağlı hipoperfüzyon ressusitasyon hedefleri aşağıdakilerin hepsini tedavi protokolünün bir parçası olarak içermelidir. (Grade 1C): SVB 8-12 mm Hg MAP≥65 mm Hg İdrar akımı≥0.5 mL/kg/saat SV (superior vena cava) veya mixed venöz oksijen saturasyonu sırası ile %70 veya %65 This recommendation has not changed from the 2008 version of the guidelines. We continue to include central venous pressure as a target, not in isolation but as part of the quantitative resuscitation protocol that has been tested in clinical trials. The SSC guidelines provide flexibility, allowing for quantitative, protocolized resuscitation implementation based upon the reality of available resources globally, including static or dynamic assessment of fluid responsiveness. Rivers E. N Engl J Med. 2001;345: PROCESS ve ARISE çalışmaları
: SVB 8-12 mm Hg. MAP≥65 mm Hg. İdrar akımı≥0.5 mL/kg/saat. SV (superior vena cava) veya mixed venöz oksijen saturasyonu sırası ile %70 veya %65. This recommendation has not changed from the 2008 version of the guidelines. We continue to include central venous pressure as a target, not in isolation but as part of the quantitative resuscitation protocol that has been tested in clinical trials. The SSC guidelines provide flexibility, allowing for quantitative, protocolized resuscitation implementation based upon the reality of available resources globally, including static or dynamic assessment of fluid responsiveness. Rivers E. N Engl J Med. 2001;345: PROCESS ve ARISE çalışmaları.")
7
Başlangıç Resusitasyonu
Doku hipoperfüzyon göstergesi olarak Laktat yüksek hastalarda ressusitasyonun hedefi mümkün olan en erken zamanda laktatı normalleştirmektir fikrini hatırlatırız (Grade 2C). For many years, physicians have been aware of the prognostic value of elevated lactate levels in ICU patients, even though mechanisms other than tissue hypoxia may contribute to that elevation. Recent randomized trials have provided evidence for the feasibility and prognostic value of increasing lactate clearance in patients with or without sepsis. Jones A. JAMA. 2010;303:739–746. Jansen TC. Am J Respir Crit Care Med ;182:752–761.
. For many years, physicians have been aware of the prognostic value of elevated lactate levels in ICU patients, even though mechanisms other than tissue hypoxia may contribute to that elevation. Recent randomized trials have provided evidence for the feasibility and prognostic value of increasing lactate clearance in patients with or without sepsis. Jones A. JAMA. 2010;303:739–746. Jansen TC. Am J Respir Crit Care Med. 2010;182:752–761.")
8
Sıvı Tedavisi Ağır sepsis ve septik şokun başlangıç sıvı ressusitasyonunda kristalloidlerin seçimini öneririz. (Grade 1B) Ağır sepsis ve septik şokta HES solusyonlarının kullanılmamasını öneririz. (Grade 1B) The absence of any clear benefit following the administration of colloid solutions compared to crystalloid solutions, together with the expense associated with colloid solutions, support a high-grade recommendation for the use of crystalloid solutions in the initial resuscitation of patients with severe sepsis and septic shock. It also supports a high-grade recommendation advising against the routine use of colloid solutions in the initial resuscitation of this patient group. These recommendations were based on information from multicenter trials [VISEP (Brunkhorst F. N Engl J Med. 2008;358: ), CRYSTMAS (Guidet B. Crit Care. 2012;16:R94), 6S (Perner A. N Engl J Med. 2012;367: ) and CHEST (Myburgh JA. N Engl J Med. 2012;367: )] and from a meta-analysis of 56 randomized trials (Perel P. Cochrane Database Syst Rev. 2011;(3):CD000567) that found evidence for survival benefit with colloids and increased risk for kidney injuries. These recommendations did not take into account the results from the more recently published CRISTAL trial (Annane D. JAMA. 2013;310: ), which found no evidence for survival differences at 28 days or for difference in the risk of renal failure between crystalloids and colloids, and suggested that colloid-treated patients may have more days alive and free of vasopressor and mechanical ventilation and a reduced risk of 90-day mortality. The U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMEA) have recently posted warnings about the risk associated with the use of starch solutions in critically ill patients (
 The absence of any clear benefit following the administration of colloid solutions compared to crystalloid solutions, together with the expense associated with colloid solutions, support a high-grade recommendation for the use of crystalloid solutions in the initial resuscitation of patients with severe sepsis and septic shock. It also supports a high-grade recommendation advising against the routine use of colloid solutions in the initial resuscitation of this patient group. These recommendations were based on information from multicenter trials [VISEP (Brunkhorst F. N Engl J Med. 2008;358: ), CRYSTMAS (Guidet B. Crit Care. 2012;16:R94), 6S (Perner A. N Engl J Med. 2012;367: ) and CHEST (Myburgh JA. N Engl J Med. 2012;367: )] and from a meta-analysis of 56 randomized trials (Perel P. Cochrane Database Syst Rev. 2011;(3):CD000567) that found evidence for survival benefit with colloids and increased risk for kidney injuries. These recommendations did not take into account the results from the more recently published CRISTAL trial (Annane D. JAMA. 2013;310: ), which found no evidence for survival differences at 28 days or for difference in the risk of renal failure between crystalloids and colloids, and suggested that colloid-treated patients may have more days alive and free of vasopressor and mechanical ventilation and a reduced risk of 90-day mortality. The U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMEA) have recently posted warnings about the risk associated with the use of starch solutions in critically ill patients ( curl=pages/news_and_events/news/2013/10/news_detail_ jsp&mid=WC0b01ac058004d5c1).")
9
Sıvı Tedavisi Ağır sepsis ve septik şokta hastalar tekrarlanan bolus kristalloid verilmesini gerektiriyorsa albumin kullanmayı hatırlatırız. (Grade 2C). This recommendation is new. Evidence available after 2008, in addition to the previously published SAFE trial (Finfer S. N Engl J Med. 2004;350: ), has provided new information about the benefit-to-risk ratio of albumin (Delaney AP. Crit Care Med. 2011;39: ). Also, as we were recommending against the use of starch solutions and bearing in mind that in some cases physicians may consider alternatives to crystalloids when repeating fluid resuscitation, we suggest that albumin can be considered as a second-line fluid therapy.
. This recommendation is new. Evidence available after 2008, in addition to the previously published SAFE trial (Finfer S. N Engl J Med. 2004;350: ), has provided new information about the benefit-to-risk ratio of albumin (Delaney AP. Crit Care Med. 2011;39: ). Also, as we were recommending against the use of starch solutions and bearing in mind that in some cases physicians may consider alternatives to crystalloids when repeating fluid resuscitation, we suggest that albumin can be considered as a second-line fluid therapy.")
10
Vazopressör tedavisi Vazopressör tedavisinin başlangıç hedefi (MAP) of 65 mm Hg öneririz. (Grade 1C) Birinci seçenek vazopressör olarak NE öneririz. (Grade 1B) The titration of norepinephrine to a MAP as low as 65 mm Hg has been shown to preserve tissue perfusion, and thus the recommendation is to maintain a MAP of 65 mm Hg. A recently completed multicenter trial that compared MAP targets of 65 mm Hg versus 85 mm Hg found no evidence for survival difference or tolerance. Information from 5 randomized trials (1993 patients with septic shock) comparing norepinephrine to dopamine did not support the routine use of dopamine in the management of septic shock. Indeed, the relative risk of short-term mortality was 0.91 (95% CI, 0.84 to 1.00; I2=0%) in favor of norepinephrine.
 The titration of norepinephrine to a MAP as low as 65 mm Hg has been shown to preserve tissue perfusion, and thus the recommendation is to maintain a MAP of 65 mm Hg. A recently completed multicenter trial that compared MAP targets of 65 mm Hg versus 85 mm Hg found no evidence for survival difference or tolerance. Information from 5 randomized trials (1993 patients with septic shock) comparing norepinephrine to dopamine did not support the routine use of dopamine in the management of septic shock. Indeed, the relative risk of short-term mortality was 0.91 (95% CI, 0.84 to 1.00; I2=0%) in favor of norepinephrine. ")
11
Vazopressör tedavisi Yeterli kan basıncını sürdürmek için ek ajan gerekirse epinefrin kullanılmasını (NE eklenmesini ve potansiyel olarak yerine kullanılmasını) öneririz. (Grade 2B) Although some human and animal studies suggest epinephrine has deleterious effects on splanchnic circulation and produces hyperlactemia, there is no clinical evidence that epinephrine results in worse outcomes, and it should be the first alternative to norepinephrine. This recommendation differs from that in the 2008 guidelines that stated: “We suggest that epinephrine, phenylephrine or vasopressin should not be administered as the initial vasopressor in septic shock (grade 2C).”
 öneririz. (Grade 2B) Although some human and animal studies suggest epinephrine has deleterious effects on splanchnic circulation and produces hyperlactemia, there is no clinical evidence that epinephrine results in worse outcomes, and it should be the first alternative to norepinephrine. This recommendation differs from that in the 2008 guidelines that stated: We suggest that epinephrine, phenylephrine or vasopressin should not be administered as the initial vasopressor in septic shock (grade 2C).")
12
Vazopressör tedavisi MAP artırmak veya NE dozunu azaltmak amacı ile vazopressin 0.03 unite/dk NE eklenebilir. Sepsis bağlı hipotansiyonda tek inisyal vazopressör olarak düşük doz vazopressin önerilmez ve ünte/dk dan yüksek dozlar kurtarma tedavisi (diğer vazopressörler ile yeterli MAP temin edilemez ise) için saklanmalıdır. This recommendation differs from that in the 2008 guidelines, which stated, "We suggest that epinephrine, phenylephrine, or vasopressin should not be administered as the initial vasopressor in septic shock (grade 2C). Vasopressin 0.03 units/minute may be added to norepinephrine subsequently with anticipation of an effect equivalent to that of norepinephrine alone."
 için saklanmalıdır. This recommendation differs from that in the 2008 guidelines, which stated, We suggest that epinephrine, phenylephrine, or vasopressin should not be administered as the initial vasopressor in septic shock (grade 2C). Vasopressin 0.03 units/minute may be added to norepinephrine subsequently with anticipation of an effect equivalent to that of norepinephrine alone.")
13
Vazopressör tedavisi
Dopamini NE alternatif olarak sadece seçilmiş hastalarda (düşük aritmi riski olan veya düşük kalp hızı olan) hatırlatırız. (Grade 2C) Fenilefrin aşağıdaki koşullar dışında önerilmez: NE ciddi aritmi oluşturursa CO yüksek olduğu bilinirken kan basıncı düşük sebat ederse Kombine inotrop/vazopressör ve düşük doz vazopressin MAP hedefini yakalamaz ise kurtarma tedavisi olarak . (Grade 1C) We believed that some physicians would like to consider using dopamine in very specific conditions when the side effects might be limited. As there was only one small trial of phenylephrine, a pure alpha-1 agonist, and other agents are available, the panel considered the restriction to the use of phenylephrine for highly selected patients who need an alternate treatment to norepinephrine.
 hatırlatırız. (Grade 2C) Fenilefrin aşağıdaki koşullar dışında önerilmez: NE ciddi aritmi oluşturursa. CO yüksek olduğu bilinirken kan basıncı düşük sebat ederse. Kombine inotrop/vazopressör ve düşük doz vazopressin MAP hedefini yakalamaz ise kurtarma tedavisi olarak . (Grade 1C) We believed that some physicians would like to consider using dopamine in very specific conditions when the side effects might be limited. As there was only one small trial of phenylephrine, a pure alpha-1 agonist, and other agents are available, the panel considered the restriction to the use of phenylephrine for highly selected patients who need an alternate treatment to norepinephrine. ")
14
İnotrop tedavisi Aşağıdakilerin varlığında 20 μg/kg/dk ulaşan dobutamin uygulanabilir veya kullanılıyorsa vazopressöre eklenmesini öneririz: Yüksek dolum basıncı ve düşük CO ile karakterize miyokard disfonksiyonunda veya Yeterli kan basıncı ve yeterli intravasküler volume rağmen devam eden hipoperfüzyon bulguları. (Grade 1C) CI belirlenen supranormal seviyelere arttırılması stratejisini red önerisinde bulunuyoruz. (Grade 1B) The panel considered it important that the introduction of dobutamine be only in case of demonstrable low cardiac output or tissue hypoperfusion where adequate filling pressures and mean arterial pressure are achieved. Owing to the increased risk of arrhythmias with high doses of dobutamine, we consider limiting dobutamine dosages to 20 µg/kg/min as the maximum dose.
 CI belirlenen supranormal seviyelere arttırılması stratejisini red önerisinde bulunuyoruz. (Grade 1B) The panel considered it important that the introduction of dobutamine be only in case of demonstrable low cardiac output or tissue hypoperfusion where adequate filling pressures and mean arterial pressure are achieved. Owing to the increased risk of arrhythmias with high doses of dobutamine, we consider limiting dobutamine dosages to 20 µg/kg/min as the maximum dose. ")
15
Sepsis için tarama ve performans geliştirme
Sepsisin erken tanınması ve erken sepsis tedavisi planının uygulamaya konulması açısından potansiyel olarak ciddi infekte hastaların ağır sepsis açısından rutin taramadan geçmelerini öneririz (Grade 1C). Ağır sepsiste hastaların sonucunu iyileştirme açısından performans iyileştirme çabaları yapılmalıdır (Ungraded). This is a new recommendation since 2008 because a number of clinical studies have verified that formal screening protocols for sepsis improve outcome (Jones et al. JAMA. 2010;303: ; Moore et al. J Trauma. 2009;66: ).
. Ağır sepsiste hastaların sonucunu iyileştirme açısından performans iyileştirme çabaları yapılmalıdır (Ungraded). This is a new recommendation since 2008 because a number of clinical studies have verified that formal screening protocols for sepsis improve outcome (Jones et al. JAMA. 2010;303: ; Moore et al. J Trauma. 2009;66: ).")
16
Tanı Kültür alınması antimikrobik tedavi başlangıcını belirgin geciktirmez ise (>45 dak) antimikrobik tedavi başlanmadan uygun kültürler alınmasını öneririz (Grade 1C). Neden olan organizmaların belirlenebilmesinin iyileştirilmesi için antimikrobik tedavi öncesi en az iki set kan kültürü (hem aerobik hemde anaerobik şişeler) alınmasını öneririz. Bunlardan en az biri perkutan alınmalı ve diğeri herbir vasküler yaklaşım aparatından alınabilir (yeterki aparat <48 saat önce takılmış olmasın) Kan kültürleri değişik anatomik bölgelerden aynı anda alınabilir. (Grade 1C). The underlined sections are new to the 2012 guidelines as ample evidence now exists to recommend these, rather than simple suggestions. (Memel L, Maki D. Ann Intern Med. 1993;119: ).
 antimikrobik tedavi başlanmadan uygun kültürler alınmasını öneririz (Grade 1C). Neden olan organizmaların belirlenebilmesinin iyileştirilmesi için antimikrobik tedavi öncesi en az iki set kan kültürü (hem aerobik hemde anaerobik şişeler) alınmasını öneririz. Bunlardan en az biri perkutan alınmalı ve diğeri herbir vasküler yaklaşım aparatından alınabilir (yeterki aparat <48 saat önce takılmış olmasın) Kan kültürleri değişik anatomik bölgelerden aynı anda alınabilir. (Grade 1C). The underlined sections are new to the 2012 guidelines as ample evidence now exists to recommend these, rather than simple suggestions. (Memel L, Maki D. Ann Intern Med. 1993;119: ).")
17
Tanı Potansiyel infeksiyon kaynağını doğrulamak üzere görüntüleme incelemeleri vakit kaybetmeden yapılmasını öneririz. Potansiyel infeksiyon kaynakları belirlendikçe, invazif girişimler dikkate alınarak ( örn: BT eşliğinde iğne aspirasyonu için transport kararı verildiğinde dikkatli bir koordinasyon ve agressif monitorizasyon) ile hasta transportu, yapılır bu bölgeler incelenir. Yatakbaşı incelemeler örneğin ultrason hasta transportuna gereksinimini ortadan kaldırır. (Ungraded). This recommendation was not graded in the 2012 guidelines as it is based on clinical experience and expert opinion rather than specific clinical trials.
 ile hasta transportu, yapılır bu bölgeler incelenir. Yatakbaşı incelemeler örneğin ultrason hasta transportuna gereksinimini ortadan kaldırır. (Ungraded). This recommendation was not graded in the 2012 guidelines as it is based on clinical experience and expert opinion rather than specific clinical trials.")
18
Tanı Antibiyotik başlamadan (Antibiyotik başlanmasını belirgin şekilde geciktirmeksizin) infeksiyon odağı olabilecek diğer bölgelerinde örneğin idrar, BOS, yara, solunum sekresyonları, veya diğer vucut sıvılarının kültürleri (tercihen uygun ise sayısal) alınmalıdır. (Grade 1C). İnvazif kandidiyazis infeksiyonun ayırıcı tanısında yer alıyorsa 1,3 β-D-glucan analizi (Grade 2B), mannan and anti-mannan antikor analizi (Grade 2C) yapılmasını hatırlatırız. The underlined recommendation on antigen detection systems for candidemia is new. It is based upon a number of clinical studies in neutropenic patients and a meta-analysis that included some ICU patients showing these assays, despite suboptimal sensitivity and specificity, allow for significantly faster diagnosis of invasive candidiasis and earlier intervention with antifungal agents. Early therapy for candida sepsis improves outcome (Alam et al. BMC Infect Dis. 2007;7:103; Sendid et al. Clin Vaccine Immunol. 2008;15: ).
 infeksiyon odağı olabilecek diğer bölgelerinde örneğin idrar, BOS, yara, solunum sekresyonları, veya diğer vucut sıvılarının kültürleri (tercihen uygun ise sayısal) alınmalıdır. (Grade 1C). İnvazif kandidiyazis infeksiyonun ayırıcı tanısında yer alıyorsa 1,3 β-D-glucan analizi (Grade 2B), mannan and anti-mannan antikor analizi (Grade 2C) yapılmasını hatırlatırız. The underlined recommendation on antigen detection systems for candidemia is new. It is based upon a number of clinical studies in neutropenic patients and a meta-analysis that included some ICU patients showing these assays, despite suboptimal sensitivity and specificity, allow for significantly faster diagnosis of invasive candidiasis and earlier intervention with antifungal agents. Early therapy for candida sepsis improves outcome (Alam et al. BMC Infect Dis. 2007;7:103; Sendid et al. Clin Vaccine Immunol. 2008;15: ).")
19
Antimikrobik tedavi Septik şokun (Grade 1B) ve ağır sepsisin (Grade 1C) tespitinin sonrası ilk saat içinde etkin intravenöz antimikrobik uygulanması tedavinin hedefi olmalıdır. Açıklama: Kanıtların ağırlığı ağır sepsis ve septik şok tanısını takiben derhal antibiyotik uygulanmasını desteklese de klinisyenin bu ideal durumu klinik pratikte elde etmede başarılı olma olasılığı bilimsel olarak araştırılmamıştır. The 1-hour recommendation for severe sepsis without septic shock was ungraded in the 2008 guidelines as some additional studies have suggested early intervention is an important prognostic indicator even without shock. There are fewer data here than in patients with septic shock. The next slide provides a summary of the evidence. The remark was added to clarify that the guidelines subcommittee acknowledges that this is a goal that may be difficult, if not impossible, to fully implement in all healthcare settings, busy emergency departments, and mass casualty settings, but should be the goal where possible.
 ve ağır sepsisin (Grade 1C) tespitinin sonrası ilk saat içinde etkin intravenöz antimikrobik uygulanması tedavinin hedefi olmalıdır. Açıklama: Kanıtların ağırlığı ağır sepsis ve septik şok tanısını takiben derhal antibiyotik uygulanmasını desteklese de klinisyenin bu ideal durumu klinik pratikte elde etmede başarılı olma olasılığı bilimsel olarak araştırılmamıştır. The 1-hour recommendation for severe sepsis without septic shock was ungraded in the 2008 guidelines as some additional studies have suggested early intervention is an important prognostic indicator even without shock. There are fewer data here than in patients with septic shock. The next slide provides a summary of the evidence. The remark was added to clarify that the guidelines subcommittee acknowledges that this is a goal that may be difficult, if not impossible, to fully implement in all healthcare settings, busy emergency departments, and mass casualty settings, but should be the goal where possible.")
20
Antimikrobik tedavi Başlangıç ampirik anti-infektif tedavinin olası patojenlere (bakteri ve/veya mantar veya viral) etkinliği olan ve sepsis kaynağı olduğu öngörülen dokulara yeterli konsantrasyonlarda penetre olan bir veya iki drog içermesi önerilir (Grade 1B). Antimikrobik rejim rezistans gelişimini önlemek, toksisiteyi azaltmak ve maliyeti düşürmek amacı ile potansiyel de-eskalasyon için her gün yeniden değerlendirilir (Grade 1B). These underlined changes from the 2008 guidelines were added to acknowledge that viral pathogens (e.g., influenza, hemorrhagic fever viruses) can cause sepsis on occasion and that antibiotic choices need to consider the levels of antibiotics achievable at the site of infection (cerebrospinal fluid, intracellular spaces, when appropriate) [Smith et al. Crit Care Med. 2010;38:41-51]. The de-escalation comment and the recommendation were upgraded to Grade 1B from the 2008 guidelines (Grade 1C) as evidence of reduced risk of antibiotic resistance can be accomplished by careful use and antibiotic stewardship to retain the activity of available antibiotics. Gao F et al. Crit Care. 2005;9:R764–R770 Schorr C. Crit Care Clin. 2009;25:857–867 Girardis M et al. Crit Care. 2009;13:R143 Pestaña D et al. J Trauma ;69:1282–1287 Berenholtz SM et al. Jt Comm J Qual Patient Safety. 2007;33:559–568 Masterton RG. Crit Care Clin. 2011;27:
 etkinliği olan ve sepsis kaynağı olduğu öngörülen dokulara yeterli konsantrasyonlarda penetre olan bir veya iki drog içermesi önerilir (Grade 1B). Antimikrobik rejim rezistans gelişimini önlemek, toksisiteyi azaltmak ve maliyeti düşürmek amacı ile potansiyel de-eskalasyon için her gün yeniden değerlendirilir (Grade 1B). These underlined changes from the 2008 guidelines were added to acknowledge that viral pathogens (e.g., influenza, hemorrhagic fever viruses) can cause sepsis on occasion and that antibiotic choices need to consider the levels of antibiotics achievable at the site of infection (cerebrospinal fluid, intracellular spaces, when appropriate) [Smith et al. Crit Care Med. 2010;38:41-51]. The de-escalation comment and the recommendation were upgraded to Grade 1B from the 2008 guidelines (Grade 1C) as evidence of reduced risk of antibiotic resistance can be accomplished by careful use and antibiotic stewardship to retain the activity of available antibiotics. Gao F et al. Crit Care. 2005;9:R764–R770. Schorr C. Crit Care Clin. 2009;25:857–867. Girardis M et al. Crit Care. 2009;13:R143. Pestaña D et al. J Trauma. 2010;69:1282–1287. Berenholtz SM et al. Jt Comm J Qual Patient Safety. 2007;33:559–568. Masterton RG. Crit Care Clin. 2011;27:")
21
Antimikrobik tedavi Düşük PCT seviyesi veya benzer biobelirteçlerin klinisyene sepsis olduğu düşünülen fakat daha sonra infeksiyonun hiçbir kanıtı bulunamayan hastalarda ampirik antibiyotikleri kesmede yardımcı olabileceğini hatırlatırız (Grade 2C). This is a new recommendation in the 2012 guidelines. Procalcitonin (or other biomarkers) has been studied in a number of trials as a guide to discontinue potentially unnecessary empirical antibiotics when the clinical situation is stabilized. The available data suggest that this might be useful in saving money and reducing antibiotic use (Heyland DK et al. Crit Care Med. 2011;39: ). However, the safety of this measure and the likelihood it can significantly reduce antibiotic resistance development of Clostridium difficile or other adverse events associated with continued antibiotic use remains to be demonstrated. Procalcitonin levels are not recommended as a biomarker for the diagnosis of sepsis.
. This is a new recommendation in the 2012 guidelines. Procalcitonin (or other biomarkers) has been studied in a number of trials as a guide to discontinue potentially unnecessary empirical antibiotics when the clinical situation is stabilized. The available data suggest that this might be useful in saving money and reducing antibiotic use (Heyland DK et al. Crit Care Med. 2011;39: ). However, the safety of this measure and the likelihood it can significantly reduce antibiotic resistance development of Clostridium difficile or other adverse events associated with continued antibiotic use remains to be demonstrated. Procalcitonin levels are not recommended as a biomarker for the diagnosis of sepsis.")
22
Antimikrobik tedavi Ampirik tedavi her hastanın mevcut hastalık durumun önergelerine göre ve lokal infeksiyon örüntülerine göre en olası patojenleri kapsamaya çalışmalıdır. Nötropenik ağır sepsis hastalarında ve Acinetobacter ve Pseudomonas spp. gibi tedavisi güç çoğul rezistan bakteri patojenler bulunan hastalarda ampirik tedavide kombinasyonu hatırlatırız (Grade 2B). (2008 Grade 2D) We upgraded the recommendation for neutropenia and for Pseudomonas spp. severe sepsis to 2B from 2D in the 2008 guidelines and added other difficult to treat pathogens such as Acinetobacter spp. in the 2012 guidelines. It has been repeatedly demonstrated that empiric therapy that does not cover these pathogens that are later found to be the cause of the infection is associated with significantly worse outcomes. However, much of this clinical data is not based on ICU patients with septic shock, and this indirectness of the data leads us to make it a suggestion (Grade 2) rather than a Grade 1 recommendation. The next two slides provide further supportive evidence of the value of empiric combination antibiotics in treating septic shock to assure that the infecting microorganism that caused septic shock is treated (Kumar et al. Crit Care Med. 2010;38: ; Micek ST et al. Antimicrob Agents Chemother. 2010;54: ).
. (2008 Grade 2D) We upgraded the recommendation for neutropenia and for Pseudomonas spp. severe sepsis to 2B from 2D in the 2008 guidelines and added other difficult to treat pathogens such as Acinetobacter spp. in the 2012 guidelines. It has been repeatedly demonstrated that empiric therapy that does not cover these pathogens that are later found to be the cause of the infection is associated with significantly worse outcomes. However, much of this clinical data is not based on ICU patients with septic shock, and this indirectness of the data leads us to make it a suggestion (Grade 2) rather than a Grade 1 recommendation. The next two slides provide further supportive evidence of the value of empiric combination antibiotics in treating septic shock to assure that the infecting microorganism that caused septic shock is treated (Kumar et al. Crit Care Med. 2010;38: ; Micek ST et al. Antimicrob Agents Chemother. 2010;54: ).")
23
Antimikrobik tedavi Solunum yetersizliği ile birlikte septik şoku bulunan hastalarda Pseudomonas aeruginosa bakteremisi için geniş spektrumlu -laktam ve aminoglikozid veya flurokinolon kombinasyon tedavisini hatırlatırız (Grade 2B). Benzer şekilde bakteremik Streptococcus pneumoniae infeksiyonları ile septik şoktaki hastalara β-laktam ve bir makrolid kombinasyonu hatırlatılır (Grade 2B). This recommendation relating to pneumococcal septic shock was added to the guidelines in keeping with a number of studies (see next slide for summary of evidence) suggesting improved outcomes for patients with septic shock when a macrolide is added to a beta-lactam in the early phase of treatment. The reasons for this apparent improved outcome in some, but not all, clinical studies are not clear but might relate to the anti-inflammatory actions attributable to macrolides or other mechanisms. It was decided to make this a suggestion until further clinical studies can support or refute this evidence.
. Benzer şekilde bakteremik Streptococcus pneumoniae infeksiyonları ile septik şoktaki hastalara β-laktam ve bir makrolid kombinasyonu hatırlatılır (Grade 2B). This recommendation relating to pneumococcal septic shock was added to the 2012 guidelines in keeping with a number of studies (see next slide for summary of evidence) suggesting improved outcomes for patients with septic shock when a macrolide is added to a beta-lactam in the early phase of treatment. The reasons for this apparent improved outcome in some, but not all, clinical studies are not clear but might relate to the anti-inflammatory actions attributable to macrolides or other mechanisms. It was decided to make this a suggestion until further clinical studies can support or refute this evidence.")
24
Antimikrobik tedavi Ağır sepsis hastalarında ampirik kombinasyon tedavisinin 3-5 günden uzun kullanılmamasını hatırlatırız. En uygun tek ajana deeskalasyon duyarlılık profili elde edildiğinde derhal yapılmalıdır (Grade 2B). (2008 Grade 2D) İstisnalar P. aeruginosa sepsisinde genel olarak kaçınılması gereken aminoglikozidlerin monoterapi olarak kullanılması ve uzun süreli kombinasyon antibiyotik tedavisi gerektiren bazı seçilmiş endokarditlerdir. The grade was increased from 2D in 2008 to 2B in 2012 as some new clinical data on early de-escalation of antibiotics suggest that this can be done safely. Exceptions exist to rapid conversion to monotherapy as indicated. Useful references include: Schorr C. Crit Care Clin. 2009;25:857–867 Girardis M. Crit Care. 2009;13:R143 Pestaña D. J Trauma. 2010;69:1282–1287 Berenholtz SM. Jt Comm J Qual Patient Saf. 2007;33:559–568 Black MD. Crit Care Med. 2012;40:1324–1328 Masterton RG. Crit Care Clin. 201;27:
. (2008 Grade 2D) İstisnalar P. aeruginosa sepsisinde genel olarak kaçınılması gereken aminoglikozidlerin monoterapi olarak kullanılması ve uzun süreli kombinasyon antibiyotik tedavisi gerektiren bazı seçilmiş endokarditlerdir. The grade was increased from 2D in 2008 to 2B in 2012 as some new clinical data on early de-escalation of antibiotics suggest that this can be done safely. Exceptions exist to rapid conversion to monotherapy as indicated. Useful references include: Schorr C. Crit Care Clin. 2009;25:857–867. Girardis M. Crit Care. 2009;13:R143. Pestaña D. J Trauma. 2010;69:1282–1287. Berenholtz SM. Jt Comm J Qual Patient Saf. 2007;33:559–568. Black MD. Crit Care Med. 2012;40:1324–1328. Masterton RG. Crit Care Clin. 201;27:")
25
Antimikrobik tedavi Antibiyotik tedavisi süresinin 7-10 gün olması hatırlatılır. Yavaş klinik cevabı olan hastalarda, drene edilemeyen infeksiyon odağı olanlarda, Staphylococcus aureus bakteremisinde, bazı fungal ve viral infeksiyonlarda, nötropeniyi içeren immun yetersizliklerde uzun süreli tedaviler gerekli olabilir (Grade 2C). The 2008 guidelines did not contain this recommendation. The committee wanted to clarify that certain specific indications for antibiotic therapy require more prolonged therapy than 7 to 10 days to avoid antibiotic failures and relapsing infections. Some of those situations are listed here and are provided as suggestions rather recommendations (Grade 2C).
. The 2008 guidelines did not contain this recommendation. The committee wanted to clarify that certain specific indications for antibiotic therapy require more prolonged therapy than 7 to 10 days to avoid antibiotic failures and relapsing infections. Some of those situations are listed here and are provided as suggestions rather recommendations (Grade 2C).")
26
Antimikrobik tedavi Viral orijinli ağır sepsis ve septik şok hastalarında antiviral tedavinin mümkün olan en erken sürede başlanmasını hatırlatırız (Grade 2C). Noninfeksiyöz nedenli olduğu belirlenen ciddi inflamatuar durumdaki hastalarda antimikrobik ajanların kullanılmamasını öneririz (Ungraded). These are new guideline statements following the events of the 2009 influenza pandemic when evidence rapidly accrued that early institution with antiviral therapy could be lifesaving in severe influenza. The second point was added to point out that antibiotics should be stopped as soon as possible after it is determined that an infectious disease is not causing the acute inflammatory state that was suspected to be due to sepsis. Preserving antibiotics until their use is warranted is important in ICU care and in medical care in general as part of antibiotic stewardship programs.
. Noninfeksiyöz nedenli olduğu belirlenen ciddi inflamatuar durumdaki hastalarda antimikrobik ajanların kullanılmamasını öneririz (Ungraded). These are new guideline statements following the events of the 2009 influenza pandemic when evidence rapidly accrued that early institution with antiviral therapy could be lifesaving in severe influenza. The second point was added to point out that antibiotics should be stopped as soon as possible after it is determined that an infectious disease is not causing the acute inflammatory state that was suspected to be due to sepsis. Preserving antibiotics until their use is warranted is important in ICU care and in medical care in general as part of antibiotic stewardship programs.")
27
Kaynak Kontrolü Acil kaynak kontrolü için değerlendirmek üzere infeksiyonun anatomik özgün teşhisi (örn: nekrotizan yumuşak doku infeksiyonu, peritonit, kolanjit, intestinal infarkt) aranmalı, yapılmalı veya dışlanmalı ve teşhis konulduktan sonra ilk 12 saat içinde kaynak kontrolü için gerekli müdahale yapılmasını öneririz (Grade 1C). Potansiyel infeksiyon kaynağı olarak infekte peripankreatik nekroz tespit edildiğinde nihai girişim viable ve nonviable dokular arasında demarkasyon hattı oluşuncaya kadar geciktirilir (Grade 2B). These recommendations and grade guidelines are comparable to those of 2008 except the time interval was lengthened for practical reasons to 12 hours versus the original 6-hour period. 2008 de ilk altı saat
 aranmalı, yapılmalı veya dışlanmalı ve teşhis konulduktan sonra ilk 12 saat içinde kaynak kontrolü için gerekli müdahale yapılmasını öneririz (Grade 1C). Potansiyel infeksiyon kaynağı olarak infekte peripankreatik nekroz tespit edildiğinde nihai girişim viable ve nonviable dokular arasında demarkasyon hattı oluşuncaya kadar geciktirilir (Grade 2B). These recommendations and grade guidelines are comparable to those of 2008 except the time interval was lengthened for practical reasons to 12 hours versus the original 6-hour period de ilk altı saat.")
28
Kaynak Kontrolü Ciddi septik hastada kaynak kontrolü gerektiğinde, en az fizyolojik hasar oluşturacak etkin girişim (örn: bir absenin cerrahi yerine perkütan drenajı) kullanılmasını öneririz (Ungraded). Eğer intravasküler erişim yolları ağır sepsis veya septik şokun olası kaynağı ise diğer bir vasküler erişim yolu oluşturulduğunda derhal çıkarılmalıdır (Ungraded). These recommendations were not graded as they were in the 2008 guidelines as they are primarily based upon common sense clinical observations and expert opinion rather than high-level clinical study evidence.
 kullanılmasını öneririz (Ungraded). Eğer intravasküler erişim yolları ağır sepsis veya septik şokun olası kaynağı ise diğer bir vasküler erişim yolu oluşturulduğunda derhal çıkarılmalıdır (Ungraded). These recommendations were not graded as they were in the 2008 guidelines as they are primarily based upon common sense clinical observations and expert opinion rather than high-level clinical study evidence.")
29
Selektif Dekontaminasyon
SOD ve SDD ventilatör ilişkili pnömoni (VAP) insidansını azaltmak metodu olarak yürürlüğe konulmasını ve araştırılmasını hatırlatırız. Bu infeksiyon kontrol yöntemi bu metodun etkin bulunduğu sağlık bakım yerleri ve bölgelerinde tesis edilmelidir (Grade 2B). Oral klorheksidin glukonatın orofarengeal dekontaminasyon formu olarak yoğun bakım hastalarında VAP riskini azaltmak için kullanılmasını hatırlatırız (Grade 2B). The 2008 guidelines did not make a selective digestive decontamination recommendation. Despite the ongoing controversy over its efficacy and impact on antibiotic resistance patterns, the committee agreed that it should be graded as much evidence now exists in the medical literature about this topic. We believe that this work deserves to be tested in long-term follow-up studies to determine its appropriate place in sepsis care in different regions of the world. Useful references include: Liberati A et al. Cochrane Collaboration. 2010;9:1–72 de Jonge E et al. Lancet. 2003;362:1011–1016 de Smet et al. N Engl J Med. 2009;360:20–31 Cuthbertson BH et al. Trials. 2010;11: de Smet AMGA et al. Lancet Infect Dis. 2011;11:372–380 Oostdijk EAN et al. Am J Respir Crit Care Med. 2010;181:452–457 Ochoa-Ardila ME et al. Intensive Care Med. 2011;37:1458–1465
 insidansını azaltmak metodu olarak yürürlüğe konulmasını ve araştırılmasını hatırlatırız. Bu infeksiyon kontrol yöntemi bu metodun etkin bulunduğu sağlık bakım yerleri ve bölgelerinde tesis edilmelidir (Grade 2B). Oral klorheksidin glukonatın orofarengeal dekontaminasyon formu olarak yoğun bakım hastalarında VAP riskini azaltmak için kullanılmasını hatırlatırız (Grade 2B). The 2008 guidelines did not make a selective digestive decontamination recommendation. Despite the ongoing controversy over its efficacy and impact on antibiotic resistance patterns, the committee agreed that it should be graded as much evidence now exists in the medical literature about this topic. We believe that this work deserves to be tested in long-term follow-up studies to determine its appropriate place in sepsis care in different regions of the world. Useful references include: Liberati A et al. Cochrane Collaboration. 2010;9:1–72. de Jonge E et al. Lancet. 2003;362:1011–1016. de Smet et al. N Engl J Med. 2009;360:20–31. Cuthbertson BH et al. Trials. 2010;11: de Smet AMGA et al. Lancet Infect Dis. 2011;11:372–380. Oostdijk EAN et al. Am J Respir Crit Care Med. 2010;181:452–457. Ochoa-Ardila ME et al. Intensive Care Med. 2011;37:1458–1465.")
30
Kortikosteroidler Eğer yeterli sıvı ressusitasyonu ve vazopresör tedavisi hemodinamik stabiliteyi sağlıyorsa erişkin septik şok hastalarında IV hidrokortizon tedavisinin kullanılmamasını hatırlatırız. Bu temin edilemez ise 200mg gün IV hidrokortizonu hatırlatırız (Grade 2C). The 2008 “positive“ formulation (“…only in patients…“) was reversed into a “negative“ phrasing according to the principle of “primum non nocere.“ As long as septic shock patients can be stabilized by volume and vasopressors, steroids should not be used. If this is not possible, thus raising the overall mortality risk, low-dose hydrocortisone could be used. According to some studies showing that lower doses may be advantageous, the daily dose should be limited to 200 mg. The 2012 guidelines no longer explicitly mention not using dexamethasone since all pertinent studies used hydrocortisone. The previous 2008 recommendation for not using high-dose steroids has been deleted as NOT using high-dose steroids for severe sepsis and septic shock is accepted as the “standard of care.”
. The 2008 positive formulation ( …only in patients… ) was reversed into a negative phrasing according to the principle of primum non nocere. As long as septic shock patients can be stabilized by volume and vasopressors, steroids should not be used. If this is not possible, thus raising the overall mortality risk, low-dose hydrocortisone could be used. According to some studies showing that lower doses may be advantageous, the daily dose should be limited to 200 mg. The 2012 guidelines no longer explicitly mention not using dexamethasone since all pertinent studies used hydrocortisone. The previous 2008 recommendation for not using high-dose steroids has been deleted as NOT using high-dose steroids for severe sepsis and septic shock is accepted as the standard of care.")
31
Kortikosteroidler Klinisyenlerin vazopressör gerekmediğinde steroid tedavisini azaltmalarını hatırlatırız (Grade 2D). Only minor amendments of the phrasing of the 2008 Guidelines. The crossover study by Keh et al (Am J Respir Crit Care Med. 2003;167: ) revealed a significant rebound phenomenon for hemodynamic as well as laboratory parameters after immediate interruption of hydrocortison infusion.
 revealed a significant rebound phenomenon for hemodynamic as well as laboratory parameters after immediate interruption of hydrocortison infusion. ")
32
Kortikosteroidler Kortikosteroidlerin şok bulunmayan sepsis tedavisinde uygulanmamasını öneririz (Grade 1D). Studies have shown that low-dose steroids seem to have a harmful effect, especially in patients without shock. In contrast to the 2008 guidelines, the 2012 document makes no explicit comment on other indications that may require steroid treatment (e.g., endocrine diseases), since this is assessed as “standard of care.“
, since this is assessed as standard of care. ")
33
Kortikosteroidler Düşük doz hidrokortizon verildiğinde tekrarlanan bolus injeksiyonlar yerine devamlı infuzyonun kullanılmasını hatırlatırız (Grade 2D). Some studies showed that hyperglycemia, a typical side effect after steroid boluses, is avoidable when a continuous infusion is used (Weber-Carstens et al. Intensive Care Med. 2007;33: ). However, there is no evidence that this has an impact on the patients‘ outcome (therefore a weak suggestion). Finally, the option of giving fludrocortisone is no longer mentioned because this was shown to have no effect on patient outcome (Annane et al. JAMA. 2010;303: ).
. Some studies showed that hyperglycemia, a typical side effect after steroid boluses, is avoidable when a continuous infusion is used (Weber-Carstens et al. Intensive Care Med. 2007;33: ). However, there is no evidence that this has an impact on the patients‘ outcome (therefore a weak suggestion). Finally, the option of giving fludrocortisone is no longer mentioned because this was shown to have no effect on patient outcome (Annane et al. JAMA. 2010;303: ).")
34
Kan ürünü verilmesi Doku hipoperfüzyonu çözüldükten sonra ve hafifletici sebepler (örn: miyokardial iskemi, ciddi hipoksemi, akut kanama, iskemik koroner arter hastalığı) yok ise hemoglobin konsantrasyonu 7 gr/dl altına düşerse yapılmasını ve hedef hemoglobin konsantrasyonunun 7-9 gr/dl olmasını erişkinler için öneririz (Grade 1B). Only minor changes of phrasing were made (“ischemic coronary artery disease“ instead of “cyanotic heart disease“). Lactic acidosis as an indication was deleted since this is now included in the section on initial resuscitation.
 yok ise hemoglobin konsantrasyonu 7 gr/dl altına düşerse yapılmasını ve hedef hemoglobin konsantrasyonunun 7-9 gr/dl olmasını erişkinler için öneririz (Grade 1B). Only minor changes of phrasing were made ( ischemic coronary artery disease instead of cyanotic heart disease ). Lactic acidosis as an indication was deleted since this is now included in the section on initial resuscitation.")
35
Kan ürünü verilmesi Ciddi sepsisle ilişkili aneminin spesifik tedavisinde eritropoetin kullanılmamasını öneririz (Grade 1B). (2008 de KBY hariç) The 2008 exclusion for patients with renal failure was removed, because new official warnings were issued by the U.S.Food and Drug Administration: In patients with chronic kidney disease, erythropoiesis-stimulating agents have been shown to increase the risk for serious adverse cardiovascular events. Hence, if these patients have severe sepsis, they should not receive erythropoietin.
 The 2008 exclusion for patients with renal failure was removed, because new official warnings were issued by the U.S.Food and Drug Administration: In patients with chronic kidney disease, erythropoiesis-stimulating agents have been shown to increase the risk for serious adverse cardiovascular events. Hence, if these patients have severe sepsis, they should not receive erythropoietin.")
36
Kan ürünü verilmesi Kanama veya planlı invazif girişim yoksa pıhtılaşma anormalliği gösteren laboratuar sonuçlarını düzeltmek için TDP kullanılmamasını hatırlatırız (Grade 2D). Ağır sepsis ve septik şoku tedavisi için antitrombin verilmemesini öneririz (Grade 1B). No changes made from the 2008 version.
. Ağır sepsis ve septik şoku tedavisi için antitrombin verilmemesini öneririz. (Grade 1B). No changes made from the 2008 version. ")
37
Kan ürünü verilmesi Ağır sepsis hastalarında belirgin kanama yok ise trombosit profilaktik olarak verilmesi için trombosit sayısı ≤10,000/mm3 (10 x 109/L) olmasını benzer şekilde eğer hastanın ciddi kanama riski varsa trombosit sayısı ≤20,000/mm3 (20 x 109/L) olmasını hatırlatırız Aktif kanama cerrahi veya invazif girişimler için daha yüksek trombosit sayısı (≥ 50,000/mm3 [50 x 109/L]) tavsiye edilir (Grade 2D). Only minor amendments were made to this 2008 guideline. There are no studies in septic patients, and these minor changes were included to avoid discrepancies with other guidelines.
 olmasını benzer şekilde eğer hastanın ciddi kanama riski varsa trombosit sayısı ≤20,000/mm3 (20 x 109/L) olmasını hatırlatırız Aktif kanama cerrahi veya invazif girişimler için daha yüksek trombosit sayısı. (≥ 50,000/mm3 [50 x 109/L]) tavsiye edilir (Grade 2D). Only minor amendments were made to this 2008 guideline. There are no studies in septic patients, and these minor changes were included to avoid discrepancies with other guidelines.")
38
Immunoglobulinler Öneri yok fakat seçim hakkı olarak:
IVIG’in toksik şokta rolü net değildir fakat çocuklardaki refraktuar toksik şok sendromunda düşünülebilir. Children are more prone to toxic shock than adults because of their lack of circulating antibodies to toxins. In refractory toxic shock syndrome, IVIG may be considered to reduce hyperinflammation.

39
Selenium Ağır sepsis tedavisinde iv selenyum kullanılmamasını öneririz (Grade 2C). Selenium was not included in the 2008 guidelines. Since then, several studies in ICU patients provided evidence that this substance may be beneficial. The clinical studies must be divided into two major groups: the first set of studies was performed to treat patients with existing severe sepsis, the second as a preventive measure to avoid development of infectious complications and organ dysfunction in critically ill patients.

40
rhAPC Dellinger et al Crit Care Med. 2013;41:580–637
In the 2008 SSC Guidelines, recombinant human activated protein C (rhAPC) was still mentioned as a suggested treatment option in patients with severe sepsis. This drug has since been withdrawn from the market and is no longer available, negating any need for a recommendation regarding its use. Dellinger et al Crit Care Med. 2013;41:580–637 Dellinger et al. Intensive Care Med. 2013;39:
 was still mentioned as a suggested treatment option in patients with severe sepsis. This drug has since been withdrawn from the market and is no longer available, negating any need for a recommendation regarding its use. Dellinger et al Crit Care Med. 2013;41:580–637. Dellinger et al. Intensive Care Med. 2013;39:")
41
SEPSİS’in İndüklediği ARDS’de yapay solunum
Sepsisin indüklediği ARDS’de klinisyenlerin 6 ml/kg (PBW) soluk hacmi hedeflemelerini öneririz (Grade 1A vs. 12 mL/kg). ARDS hastalarında plato basıncın ölçülmesini ve pasif olarak infle edilen akciğerde başlangıç plato basıncının üst sınırının ≤30 cm H2O olmasını öneririz (Grade 1B). The 2008 Surviving Sepsis Campaign guidelines recommended targeting a tidal volume of 6 mL/kg predicted body weight in patients with sepsis-induced acute lung injury. This recommendation has been continued in the 2012 guidelines, and is supported by the ARMA trial, which is described in the following slide. Because the ARMA trial combined a low tidal volume strategy with one of limiting plateau pressures ≤30 cm H2O, this recommendation has been added to the guidelines. Based on the recent update in the definition of ARDS, the terminology was changed to fit the new Berlin definition of ARDS, which will be described in a later slide (ARDS Definition Task Force et al. JAMA. 2012;307: ). Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:
 soluk hacmi hedeflemelerini öneririz (Grade 1A vs. 12 mL/kg). ARDS hastalarında plato basıncın ölçülmesini ve pasif olarak infle edilen akciğerde başlangıç plato basıncının üst sınırının ≤30 cm H2O olmasını öneririz (Grade 1B). The 2008 Surviving Sepsis Campaign guidelines recommended targeting a tidal volume of 6 mL/kg predicted body weight in patients with sepsis-induced acute lung injury. This recommendation has been continued in the 2012 guidelines, and is supported by the ARMA trial, which is described in the following slide. Because the ARMA trial combined a low tidal volume strategy with one of limiting plateau pressures ≤30 cm H2O, this recommendation has been added to the guidelines. Based on the recent update in the definition of ARDS, the terminology was changed to fit the new Berlin definition of ARDS, which will be described in a later slide (ARDS Definition Task Force et al. JAMA. 2012;307: ). Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:")
42
ARDS Berlin Tanımlaması
The Berlin definition replaces the previous American-European Consensus Conference definition of ALI and ARDS. Major changes to the definition include the addition of treatment variables, including the requirement for positive pressure, which can be delivered non-invasively in the mild ARDS group. The severity of hypoxemia based on the Pao2/Fio2 ratio will place patients into a mild, moderate, or severe category. Other changes include the requirement that the infiltrates occur in <1 week and that the respiratory failure not be entirely explained by cardiac failure or fluid overload. ARDS Definition Task Force et al. JAMA. 2012;307:

43
SEPSİS’in İndüklediği ARDS’de PEEP
Ekspirasyonun sonunda alveolar kollapsı (atelektotravma) önlemek için PEEP uygulanmasını öneririz. (Grade 1B). The 2008 guidelines recommended to keep positive end-expiratory pressure (PEEP) at a level to prevent alveolar collapse at end expiration. This recommendation is unchanged in Increased PEEP keeps lung units open to participate in gas exchange. A PEEP >5 cm H2O is often required to avoid lung collapse, and the majority of patients who are treated with a PEEP >5 cm H2O will have increased oxygen levels and increased lung aeration as shown by computed tomography. The best method to titrate PEEP remains unclear; options include either increasing by a protocolized approach or using a physiologic approach. Gattinoni et al. N Engl J Med. 2006;354:1775–1786
 önlemek için PEEP uygulanmasını öneririz. (Grade 1B). The 2008 guidelines recommended to keep positive end-expiratory pressure (PEEP) at a level to prevent alveolar collapse at end expiration. This recommendation is unchanged in Increased PEEP keeps lung units open to participate in gas exchange. A PEEP >5 cm H2O is often required to avoid lung collapse, and the majority of patients who are treated with a PEEP >5 cm H2O will have increased oxygen levels and increased lung aeration as shown by computed tomography. The best method to titrate PEEP remains unclear; options include either increasing by a protocolized approach or using a physiologic approach. Gattinoni et al. N Engl J Med. 2006;354:1775–1786.")
44
SEPSİS’in İndüklediği ARDS’de daha yüksek PEEP
Sepsisin indüklediği orta ve ciddi ARDS’de düşük PEEP temelli stratejiler yerine yüksek PEEP temelli stratejileri hatırlatırız (Grade 2C). This suggestion is new for the 2012 guidelines based on an individual patient data meta-analysis by Briel et al. In this review, patients with ARDS, but not ALI, had improved survival when treated with higher levels of PEEP than lower levels. The nomenclature has been changed to reflect the Berlin definition of ARDS. Briel et al. JAMA. 2010;303:
. This suggestion is new for the 2012 guidelines based on an individual patient data meta-analysis by Briel et al. In this review, patients with ARDS, but not ALI, had improved survival when treated with higher levels of PEEP than lower levels. The nomenclature has been changed to reflect the Berlin definition of ARDS. Briel et al. JAMA. 2010;303:")
45
Rekruitment Manevraları
Sepsis hastalarında ARDS’ye bağlı ciddi refraktör hipoksemide rekruitment manevralarını hatırlatırız (Grade 2C). This suggestion to use recruitment maneuvers in sepsis patients with severe refractory hypoxemia due to ARDS is new for 2012 and is based on the meta-analysis of Fan, which will be described in the following slide.
. This suggestion to use recruitment maneuvers in sepsis patients with severe refractory hypoxemia due to ARDS is new for 2012 and is based on the meta-analysis of Fan, which will be described in the following slide.")
46
SEPSİS’in İndüklediği ARDS’de Prone Pozisyon
Sepsisin indüklediği ARDS hastalarında Pao2/Fio2 oranı <100 mm Hg ise bu tür uygulamalarda tecrübe sahibi olan ünitelerde pron pozisyon uygulamasını hatırlatırız (Grade 2B). The 2008 guidelines suggested prone positioning in patients with profound hypoxemia. The 2012 guidelines changed the suggestion to grade 2B, based primarily on the meta-analysis of Sud et al, which will be described in the following slide. Sud et al. Intensive Care Med. 2010;36:
. The 2008 guidelines suggested prone positioning in patients with profound hypoxemia. The 2012 guidelines changed the suggestion to grade 2B, based primarily on the meta-analysis of Sud et al, which will be described in the following slide. Sud et al. Intensive Care Med. 2010;36:")
47
Pulmoner Arter Kateteri
Sepsisin indüklediği ARDS hastalarında pulmoner arter kateterinin rutin kullanılmamasını öneririz (Grade 1A). The 2008 Surviving Sepsis Campaign guidelines recommended against the routine use of pulmonary artery catheters for patients with ARDS. The recommendations for 2012 remain consistent against the use of pulmonary artery catheters in patients with sepsis-induced ARDS. Multiple studies across patient populations--including patients with ARDS, sepsis, and shock, and high-risk surgical patients--did not show improved outcomes with the use of a pulmonary artery catheter: Wheeler A. N Engl J Med. 2006;354: Richard C. JAMA. 2003:290: Sandham J. N Engl J Med. 2003;348:5-14 Harvey S. Lancet. 2005:366:
. The 2008 Surviving Sepsis Campaign guidelines recommended against the routine use of pulmonary artery catheters for patients with ARDS. The recommendations for 2012 remain consistent against the use of pulmonary artery catheters in patients with sepsis-induced ARDS. Multiple studies across patient populations--including patients with ARDS, sepsis, and shock, and high-risk surgical patients--did not show improved outcomes with the use of a pulmonary artery catheter: Wheeler A. N Engl J Med. 2006;354: Richard C. JAMA. 2003:290: Sandham J. N Engl J Med. 2003;348:5-14. Harvey S. Lancet. 2005:366: ")
48
Sepsisin indüklediği ARDS hastalarında Sıvı Yönetimi
Sepsisin indüklediği kesin olarak belirlenmiş ARDS hastalarında doku hipoperfüzyonunun kanıtı yoksa konservatif sıvı stratejisini öneririz (Grade 1C). The 2008 guidelines recommended a conservative fluid strategy for patients with ARDS who did not have evidence of tissue hypoperfusion. This recommendation has not changed for the 2012 guidelines. Wiedemann et al. N Engl J Med. 2006:354:
. The 2008 guidelines recommended a conservative fluid strategy for patients with ARDS who did not have evidence of tissue hypoperfusion. This recommendation has not changed for the 2012 guidelines. Wiedemann et al. N Engl J Med. 2006:354:")
49
Yatak başının yükseltilmesi
Aspirasyon riskini sınırlamak ve VAP gelişimini önlemek amacı ile yapay solunum uygulanan hastaların yatak başı derece yükseltilerek sürdürülmesini öneririz (Grade 1B). The 2008 Surviving Sepsis Campaign guidelines suggested elevation of the head of the bed in mechanically ventilated sepsis patients. The 2012 guidelines have recommended elevation of the head of the bed based on the widespread implementation of this goal as part of ventilator-associated pneumonia (VAP) prevention efforts.
. The 2008 Surviving Sepsis Campaign guidelines suggested elevation of the head of the bed in mechanically ventilated sepsis patients. The 2012 guidelines have recommended elevation of the head of the bed based on the widespread implementation of this goal as part of ventilator-associated pneumonia (VAP) prevention efforts.")
50
Yapay solunumdan ayırma
Ağır sepsisli ve yapay solunum uygulanan hastalarda weaning protokolu olmalı ve bu hastalarda aşağıdaki kriterlere uyduklarında a) uyandırılabilir b)hemodinamik olarak stabil ( vazopressör yok) c)potansiyel ciddiyet taşıyan yeni durum yok d)düşük ventilasyon ve end ekspirasyon basınç gereksinimi e)nazal kanül veya yüz maskesi ile uygulanabilecek düşük Fio2 gereksinimi ; düzenli olarak spontan solunum denemeleri uygulanarak yapay solunumdan ayırma olasılığı değerlendirilmelidir. Eğer ssd başarılı ise ekstubasyon düşünülmelidir önermelerinde bulunuruz (Grade 1A). The 2008 guidelines recommended use of a weaning protocol for patients with sepsis and respiratory failure. These recommendations are unchanged and are based on multiple studies supporting the use of spontaneous breathing trials (SBT) in patients with persistent respiratory failure, many of whom had sepsis. Esteban et al. N Engl J Med. 1995;332: Brochard et al. Am J Respir Crit Care Med. 1994;150: Ely et al. N Engl J Med. 1996;335: Kress et al. N Engl J Med. 2000;342: Girard et al. Lancet. 2008;371:
 uyandırılabilir b)hemodinamik olarak stabil ( vazopressör yok) c)potansiyel ciddiyet taşıyan yeni durum yok d)düşük ventilasyon ve end ekspirasyon basınç gereksinimi e)nazal kanül veya yüz maskesi ile uygulanabilecek düşük Fio2 gereksinimi ; düzenli olarak spontan solunum denemeleri uygulanarak yapay solunumdan ayırma olasılığı değerlendirilmelidir. Eğer ssd başarılı ise ekstubasyon düşünülmelidir önermelerinde bulunuruz (Grade 1A). The 2008 guidelines recommended use of a weaning protocol for patients with sepsis and respiratory failure. These recommendations are unchanged and are based on multiple studies supporting the use of spontaneous breathing trials (SBT) in patients with persistent respiratory failure, many of whom had sepsis. Esteban et al. N Engl J Med. 1995;332: Brochard et al. Am J Respir Crit Care Med. 1994;150: Ely et al. N Engl J Med. 1996;335: Kress et al. N Engl J Med. 2000;342: Girard et al. Lancet. 2008;371: ")
51
Glikoz kontrolü Kan glikoz yönetimine protokollü bir yaklaşım ile peşpeşe iki ölçümde kan glukoz seviyesi >180 mg/dL olduğunda insülin dozlarına başlanmasını öneririz. Bu protokollü yaklaşım hedef olarak üst glikoz seviyesi <110 mg/dL yerine <180 mg/dL hedeflemelidir (Grade 1A). The 2008 guidelines recommended intravenous insulin therapy to reduce blood glucose levels, targeting glucose levels to a range <150 mg/dL. The present recommendations have changed, recommending to commence insulin dosing with a trigger of blood glucose levels >180 mg/dL and targeting blood glucose <180 mg/dL (based on the Normoglycemia in Intensive Care Evaluation and Surviving Using Glucose Algorithm Regulation [NICE-SUGAR] study) rather than <110 mg/dL (based on the van den Berghe studies). NICE-SUGAR Investigators. N Engl J Med ;360:1283–1297 van den Berghe et al. N Engl J Med. 2001;345:1359–1367 Dellinger et al. Crit Care Med. 2013;41:580–637 Dellinger et al. Intensive Care Med. 2013;39: 51
. The 2008 guidelines recommended intravenous insulin therapy to reduce blood glucose levels, targeting glucose levels to a range <150 mg/dL. The present recommendations have changed, recommending to commence insulin dosing with a trigger of blood glucose levels >180 mg/dL and targeting blood glucose <180 mg/dL (based on the Normoglycemia in Intensive Care Evaluation and Surviving Using Glucose Algorithm Regulation [NICE-SUGAR] study) rather than <110 mg/dL (based on the van den Berghe studies). NICE-SUGAR Investigators. N Engl J Med. 2009;360:1283–1297. van den Berghe et al. N Engl J Med. 2001;345:1359–1367. Dellinger et al. Crit Care Med. 2013;41:580–637. Dellinger et al. Intensive Care Med. 2013;39:")
52
Glikoz kontrolü Kan glikoz değerleri ve insülin infüzyon hızları sabitleşesiye kadar 1-2 saatte bir kan glikoz değeri kontrolü monitorize edilmesi daha sonra 4 saatte bir kontrolü önerilir (Grade 1C). This slide notes the recommendation for frequency of glucose monitoring. This recommendation is basically unchanged from the 2008 guidelines. 52
. This slide notes the recommendation for frequency of glucose monitoring. This recommendation is basically unchanged from the 2008 guidelines. 52.")
53
Glikoz kontrolü Yatak başı testi ile edilen kapiller kanda glikoz seviyeleri dikkatle değerlendirilmelidir çünkü bazen arter veya plazma glikoz seviyelerini yanlış ölçebilir. (Ungraded). Factors that may affect the accuracy and reproducibility of point-of-care testing of capillary blood include the type and model of the device used, user expertise, and patient factors, including hematocrit (false elevation with anemia), Pao2, and drugs. 53
. Factors that may affect the accuracy and reproducibility of point-of-care testing of capillary blood include the type and model of the device used, user expertise, and patient factors, including hematocrit (false elevation with anemia), Pao2, and drugs. 53.")
54
Bikarbonat Tedavisi Hipoperfüzyon tarafından indüklenen pH ≥7.15 yapan laktik asidemi bulunan hastalarda hemodinamiği iyileştirmek veya vazopressör gereksinimi azaltmak için sodyum bikarbonat tedavisinin kullanılmamasını öneririz (Grade 2B). This recommendation has not changed from that in the 2008 Surviving Sepsis Campaign guidelines. 54
. This recommendation has not changed from that in the 2008 Surviving Sepsis Campaign guidelines. 54.")
55
Nutrisyon Ağır sepsis/septik şok tanısından sonra ilk 48 saat içinde tam açlık veya sadece iv glikoz yerine tolere edildiği sürece oral veya enteral beslenmenin yapılmasını hatırlatırız (Grade 2C). Early enteral nutrition has theoretical advantages in the integrity of gut mucosa and prevention of bacterial translocation and organ dysfunction, but also concerning is the risk of ischemia, mainly in hemodynamically unstable patients. Besides the insufficient evidence, the suggestion of benefit and absence of harm supports a weak recommendation that some enteral feeding is warranted. Marik and Zaloga. Crit Care Med ;29:2264–2270 Heyland et al. JPEN J Parenter Enteral Nutr. 2003;27: Doig et al. Intensive Care Med. 2009;35:2018–2027
. Early enteral nutrition has theoretical advantages in the integrity of gut mucosa and prevention of bacterial translocation and organ dysfunction, but also concerning is the risk of ischemia, mainly in hemodynamically unstable patients. Besides the insufficient evidence, the suggestion of benefit and absence of harm supports a weak recommendation that some enteral feeding is warranted. Marik and Zaloga. Crit Care Med. 2001;29:2264–2270. Heyland et al. JPEN J Parenter Enteral Nutr. 2003;27: Doig et al. Intensive Care Med. 2009;35:2018–2027.")
56
Nutrisyon İlk hafta tam kalorinin verildiği mecburi beslenmeden kaçınılmasını fakat düşük doz beslenmenin (örn: 500 kcal/gün) yapılmasını ve tolere edildikçe arttırılmasını hatırlatırız. (Grade 2B). Old and small studies, like those by Taylor et al and Ibrahim et al, comparing full caloric early enteral feeding to lower targets in the critically ill have produced inconclusive results. Recent studies with stronger methodological quality suggest no difference or even an advantage of underfeeding (60% to 70% of target) and trophic feeding (upper limit of 500 kcal) strategies over the enhanced strategy. Therefore, evidence is insufficient to support an early target of full caloric intake and, indeed, some possibility of harm exists. Thus, restrictive feeding is probably a better nutritional strategy in the first week of severe sepsis/septic shock. This upper limit for trophic feeding is a somewhat arbitrary number, but is based in part on the fact that the two recent studies used a range of 240−480 kcal. Underfeeding/trophic feeding strategies did not exclude advancing diet as tolerated in those who improved quickly. Taylor et al. Crit Care Med. 1999;27:2525–2531 Ibrahim et al. JPEN J Parenter Enteral Nutr. 2002;26:174–181 Arabi et al. Am J Clin Nutr. 2011;93:569–577 Rice et al. Crit Care Med. 2011;39:967–974 Rice et al. JAMA. 2012;137:795–803
 yapılmasını ve tolere edildikçe arttırılmasını hatırlatırız. (Grade 2B). Old and small studies, like those by Taylor et al and Ibrahim et al, comparing full caloric early enteral feeding to lower targets in the critically ill have produced inconclusive results. Recent studies with stronger methodological quality suggest no difference or even an advantage of underfeeding (60% to 70% of target) and trophic feeding (upper limit of 500 kcal) strategies over the enhanced strategy. Therefore, evidence is insufficient to support an early target of full caloric intake and, indeed, some possibility of harm exists. Thus, restrictive feeding is probably a better nutritional strategy in the first week of severe sepsis/septic shock. This upper limit for trophic feeding is a somewhat arbitrary number, but is based in part on the fact that the two recent studies used a range of 240−480 kcal. Underfeeding/trophic feeding strategies did not exclude advancing diet as tolerated in those who improved quickly. Taylor et al. Crit Care Med. 1999;27:2525–2531. Ibrahim et al. JPEN J Parenter Enteral Nutr. 2002;26:174–181. Arabi et al. Am J Clin Nutr. 2011;93:569–577. Rice et al. Crit Care Med. 2011;39:967–974. Rice et al. JAMA. 2012;137:795–803.")
57
Nutrisyon Tek başına veya enteral nutrisyon ile beraber TPN yerine iv glikoz ve enteral nutrisyon kullanmayı hatırlatırız (Grade 2B). Some form of parenteral nutrition has been compared to alternative feeding strategies (e.g., fasting or enteral nutrition) in well over 50 studies, although only one exclusively studied sepsis and several meta-analyses have been published. Of the papers listed here, two meta-analyses summarized comparisons of parenteral nutrition to fasting or intravenous glucose (Heyland, Braunschweig), and five looked at parenteral versus enteral nutrition (Heyland, Gramlich, Dhaliwal, Peter, Simpson), two of which attempted to explore the effect of early enteral nutrition (Peter, Simpson). No direct evidence supports the benefits or harm of parenteral nutrition in the first 48 hours of sepsis. Rather, the evidence is generated predominantly from surgical, burn, and trauma patients. None of the meta-analyses reports a mortality benefit with parenteral nutrition, although one suggested parenteral nutrition may be better than late introduction of enteral nutrition (Simpson). Several suggested that parenteral nutrition was associated with a higher incidence of infectious complications compared both to fasting or intravenous glucose and to enteral nutrition, while enteral feeding was associated with a higher rate of enteral complications (e.g., diarrhea) than parenteral nutrition. The use of parenteral nutrition to supplement enteral feeding was analyzed by Dhaliwal et al, who reported no benefit. Since then, the results of the Casaer study were reported (next slide). No study suggests the superiority of total parenteral nutrition over enteral alone. In fact, there is a suggestion that enteral nutrition may be superior to total parenteral vis-à-vis infectious complications and possibly a requirement for intensive care and organ support. Braunschweig et al. Am J Clin Nutr. 2001;74:534–542 Heyland et al. JPEN J Parenter Enteral Nutr. 2003;27:355–373 Gramlich et al. Nutrition. 2004;20:843–848 Dhaliwal et al. Intensive Care Med. 2004;30:1666–1671 Peter et al. Crit Care Med. 2005; 33:213–220 Simpson and Doig. Intensive Care Med. 2005;31:12–23 Casaer et al. N Engl J Med. 2011;365:506–517
 in well over 50 studies, although only one exclusively studied sepsis and several meta-analyses have been published. Of the papers listed here, two meta-analyses summarized comparisons of parenteral nutrition to fasting or intravenous glucose (Heyland, Braunschweig), and five looked at parenteral versus enteral nutrition (Heyland, Gramlich, Dhaliwal, Peter, Simpson), two of which attempted to explore the effect of early enteral nutrition (Peter, Simpson). No direct evidence supports the benefits or harm of parenteral nutrition in the first 48 hours of sepsis. Rather, the evidence is generated predominantly from surgical, burn, and trauma patients. None of the meta-analyses reports a mortality benefit with parenteral nutrition, although one suggested parenteral nutrition may be better than late introduction of enteral nutrition (Simpson). Several suggested that parenteral nutrition was associated with a higher incidence of infectious complications compared both to fasting or intravenous glucose and to enteral nutrition, while enteral feeding was associated with a higher rate of enteral complications (e.g., diarrhea) than parenteral nutrition. The use of parenteral nutrition to supplement enteral feeding was analyzed by Dhaliwal et al, who reported no benefit. Since then, the results of the Casaer study were reported (next slide). No study suggests the superiority of total parenteral nutrition over enteral alone. In fact, there is a suggestion that enteral nutrition may be superior to total parenteral vis-à-vis infectious complications and possibly a requirement for intensive care and organ support. Braunschweig et al. Am J Clin Nutr. 2001;74:534–542. Heyland et al. JPEN J Parenter Enteral Nutr. 2003;27:355–373. Gramlich et al. Nutrition. 2004;20:843–848. Dhaliwal et al. Intensive Care Med. 2004;30:1666–1671. Peter et al. Crit Care Med. 2005; 33:213–220. Simpson and Doig. Intensive Care Med. 2005;31:12–23. Casaer et al. N Engl J Med. 2011;365:506–517.")
58
Nutrisyon Ağır sepsis hastalarında özgün immunmodulatuar eklerin bulunmadığı beslenmenin kullanılmasını hatırlatırız (Grade 2C). Immune system function can be modified through alterations in the supply of certain nutrients, such as arginine, glutamine, or omega-3 fatty acids. Numerous studies have assessed whether the use of these agents as nutritional supplements can affect the course of critical illness, but few specifically addressed their early use in sepsis.

59
Glutamin Glutamin kullanılmamalıdır Mortaliteye etkisi yoktur
Bazı pozitif ikincil sonuçlar vardır (infeksiyon ve organ disfonksiyonunda azalama) Meta-analyses Heyland et al. JPEN. 2003;27:355 Jian et al. Zhonghua Shao Shang Za Zhi ;25:325 Avenell A et al. Proc Nutr Soc. 2006;65:236 Avenell A et al. Proc Nutr Soc. 2009;68:261 Novak et al. Crit Care Med. 2002;30:2022 Single Studies Fuentes-Orozco et al. Clin Nutr. 2004;23:13 Beale et al. Crit Care Med. 2008;36:131 Grau et al. Crit Care Med. 2011;39:1263 Wernerman et al. Acta Anaesthesiol Scand. 2011;55:812 Andrews et al. BMJ. 2011;342:d1542 Although a previous meta-analysis showed a reduction in mortality (Heyland 2003), four other meta-analyses did not (Novak, Avenell, Jiang, Avenell [slide 17]). Three well-designed studies also failed to show a mortality benefit in the primary analyses (Andrews, Grau, Wenerman)--but again, none focused specifically on septic patients. Two small studies on septic patients showed no benefit in mortality rates (Fuentes-Orozco, Beale) but a significant reduction in infectious complications and a faster recovery of organ dysfunction. Some previous individual studies and meta-analyses showed positive secondary outcomes, such as reduction in infectious morbidity and organ dysfunction. Beneficial effects were found mostly in trials using parenteral rather than enteral glutamine. However, well-sized studies could not demonstrate a reduction of infectious complications or organ dysfunction, even with parenteral glutamine (slide 18). After publication of the 2012 SSC guidelines, the REDOXS study was published and included more than 1,200 patients (slide 19).
 Meta-analyses. Heyland et al. JPEN. 2003;27:355. Jian et al. Zhonghua Shao Shang Za Zhi. 2009;25:325. Avenell A et al. Proc Nutr Soc. 2006;65:236. Avenell A et al. Proc Nutr Soc. 2009;68:261. Novak et al. Crit Care Med. 2002;30:2022. Single Studies. Fuentes-Orozco et al. Clin Nutr. 2004;23:13. Beale et al. Crit Care Med. 2008;36:131. Grau et al. Crit Care Med. 2011;39:1263. Wernerman et al. Acta Anaesthesiol Scand. 2011;55:812. Andrews et al. BMJ. 2011;342:d1542. Although a previous meta-analysis showed a reduction in mortality (Heyland 2003), four other meta-analyses did not (Novak, Avenell, Jiang, Avenell [slide 17]). Three well-designed studies also failed to show a mortality benefit in the primary analyses (Andrews, Grau, Wenerman)--but again, none focused specifically on septic patients. Two small studies on septic patients showed no benefit in mortality rates (Fuentes-Orozco, Beale) but a significant reduction in infectious complications and a faster recovery of organ dysfunction. Some previous individual studies and meta-analyses showed positive secondary outcomes, such as reduction in infectious morbidity and organ dysfunction. Beneficial effects were found mostly in trials using parenteral rather than enteral glutamine. However, well-sized studies could not demonstrate a reduction of infectious complications or organ dysfunction, even with parenteral glutamine (slide 18). After publication of the 2012 SSC guidelines, the REDOXS study was published and included more than 1,200 patients (slide 19).")
60
Omega-3 Yağ asitleri Omega-3 yağ asitleri kullanılmamalıdır.
Omega-6 zenginleştirilmiş dietlerin kontrol gruplarında yer aldığı daha önceki çalışmalar yarar göstermiştir Pontes-Arruda et al. Crit Care Med. 2006;34:2325 Gadek et al. Crit Care Med. 1999;27:1409 Singer et al. Crit Care Med. 2006;34:1033 Yeni çalışmalar yarar göstermemesinin yanında olası zarar göstermiştir Three early studies (Pontes-Arruda, Gadek, and Singer) were summarized in a meta-analysis that reported a significant mortality reduction, increased ventilator-free days, and reduced risk of new organ dysfunction. However, only one study was in septic patients, none was individually powered for mortality, and all three used a diet with high omega-6 lipid content in the control group, which is not the usual standard of care in the critically ill. Other studies using enteral (Rice, Stapleton, Grau-Carmona) or parenteral (Friesecke, Barbosa, Gupta) fish oil failed to confirm these positive findings in general critical illness or acute lung injury. Friesecke et al. Intensive Care Med. 2008;34:1411 Barbosa et al. Crit Care. 2010;14:R5 Gupta et al. Indian J Crit Care Med. 2011;15:108 Rice et al. JAMA. 2011; 306:1574 Stapleton et al. Crit Care Med. 2011;39:1655 Grau-Carmona et al. Clin Nutr. 2011;30:578
 were summarized in a meta-analysis that reported a significant mortality reduction, increased ventilator-free days, and reduced risk of new organ dysfunction. However, only one study was in septic patients, none was individually powered for mortality, and all three used a diet with high omega-6 lipid content in the control group, which is not the usual standard of care in the critically ill. Other studies using enteral (Rice, Stapleton, Grau-Carmona) or parenteral (Friesecke, Barbosa, Gupta) fish oil failed to confirm these positive findings in general critical illness or acute lung injury. Friesecke et al. Intensive Care Med. 2008;34:1411. Barbosa et al. Crit Care. 2010;14:R5. Gupta et al. Indian J Crit Care Med. 2011;15:108. Rice et al. JAMA. 2011; 306:1574. Stapleton et al. Crit Care Med. 2011;39:1655. Grau-Carmona et al. Clin Nutr. 2011;30:578.")
61
Renal Replasman Tedavisi
Ağır sepsis ve akut renal yetersizlikli hastalarda devamlı renal replasman tedavileri ve aralıklı hemodiyalizin eş olduğunu çünkü kısa dönem sağ kalımlarının benzer olduğunu hatırlatırız (Grade 2B). Hemodinamik olarak instabil hastalarda sıvı dengesinin yönetimini kolaylaştırmak devamlı renal replasman kullanılmasını hatırlatırız(Grade 2D). The 2008 Surviving Sepsis Campaign guidelines mirror the 2012 guidelines with the exception that the 2012 guidelines elected to add the qualifier that continuous renal replacement therapies and intermittent hemodialysis are equivalent in patients with severe sepsis and acute renal failure “because they achieve similar short-term survival rates.” Other bases for comparison do not provide ground for a different conclusion.
. Hemodinamik olarak instabil hastalarda sıvı dengesinin yönetimini kolaylaştırmak devamlı renal replasman kullanılmasını hatırlatırız(Grade 2D). The 2008 Surviving Sepsis Campaign guidelines mirror the 2012 guidelines with the exception that the 2012 guidelines elected to add the qualifier that continuous renal replacement therapies and intermittent hemodialysis are equivalent in patients with severe sepsis and acute renal failure because they achieve similar short-term survival rates. Other bases for comparison do not provide ground for a different conclusion.")
62
2008’de Grade 1A çalışmalarda infeksiyonu olan hasta az
VTE için profilaksi Ağır sepsisli hastaların VTE’i engellemek için günlük farmakoprofilaksi almalarını öneririz (Grade 1B). 2008’de Grade 1A çalışmalarda infeksiyonu olan hasta az VTE prophylaxis is generally effective in the acutely ill. Nine placebo-controlled randomized clinical trials (RCTs) and two meta-analyses support VTE prophylaxis in acutely ill patients. However, the evidence must be extrapolated to septic patients. Only 17% of patients in these studies had confirmed infection/sepsis. Therefore, the recommendation was downgraded from 1A to 1B. The complication rate of pharmacoprophylaxis is low, and the risk of not preventing a PE is high. Therefore, the strength of the recommendation was 1B.
. 2008’de Grade 1A çalışmalarda infeksiyonu olan hasta az. VTE prophylaxis is generally effective in the acutely ill. Nine placebo-controlled randomized clinical trials (RCTs) and two meta-analyses support VTE prophylaxis in acutely ill patients. However, the evidence must be extrapolated to septic patients. Only 17% of patients in these studies had confirmed infection/sepsis. Therefore, the recommendation was downgraded from 1A to 1B. The complication rate of pharmacoprophylaxis is low, and the risk of not preventing a PE is high. Therefore, the strength of the recommendation was 1B.")
63
VTE için profilaksi Biz VTE profilaksisi için günlük sc düşük molekül ağırlıklı heparin (LMWH) öneririz. Günde iki kez unfraksiyone heparine (UFH) göre (Grade 1B) Günde üç kez unfraksiyone heparine (UFH) göre (Grade 2C) This recommendation supplants the 2008 recommendation with an option for low-dose UFH administered twice or three times per day in addition to LMWH. The incidence of PE is lower in critically ill patients treated with LMWH compared to similar patients treated with UFH administered twice daily. There is no difference in the incidence of deep vein thromboses (DVTs) [PROTECT Investigators et al. Dalteparin versus unfractionated heparin in critically ill patients. N Engl J Med. 2011;364:1305–1314]. Therefore, use of LMWH over twice-daily UFH was graded 1B. Thrice-daily UFH is more effective than twice-daily UFH in a general population (GRADE A/B) (King CS et al. Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: A metaanalysis. Chest. 2007;131(2): ). No data compare twice-daily to thrice-daily UFH in critically ill/septic patients. Therefore, the need to extrapolate downgrades evidence to B. No data compare LMWH to UFH administered three times daily, further downgrading the evidence to C. Therefore, the use of LMWH is graded to 1B (vs twice-daily UFH) or 2C (vs thrice-daily UFH). The need for the most effective form of prophylaxis is profound. LMWHs are easier to give than UFH. The complication of bleeding risk is low. Therefore, the strength of the recommendation for the use of LMWH over twice-daily UFH is strong – 1B. The strength of recommendation for use of LMWH over thrice-daily UFH is not– 2C.
 göre (Grade 1B) Günde üç kez unfraksiyone heparine (UFH) göre (Grade 2C) This recommendation supplants the 2008 recommendation with an option for low-dose UFH administered twice or three times per day in addition to LMWH. The incidence of PE is lower in critically ill patients treated with LMWH compared to similar patients treated with UFH administered twice daily. There is no difference in the incidence of deep vein thromboses (DVTs) [PROTECT Investigators et al. Dalteparin versus unfractionated heparin in critically ill patients. N Engl J Med. 2011;364:1305–1314]. Therefore, use of LMWH over twice-daily UFH was graded 1B. Thrice-daily UFH is more effective than twice-daily UFH in a general population (GRADE A/B) (King CS et al. Twice vs three times daily heparin dosing for thromboembolism prophylaxis in the general medical population: A metaanalysis. Chest. 2007;131(2): ). No data compare twice-daily to thrice-daily UFH in critically ill/septic patients. Therefore, the need to extrapolate downgrades evidence to B. No data compare LMWH to UFH administered three times daily, further downgrading the evidence to C. Therefore, the use of LMWH is graded to 1B (vs twice-daily UFH) or 2C (vs thrice-daily UFH). The need for the most effective form of prophylaxis is profound. LMWHs are easier to give than UFH. The complication of bleeding risk is low. Therefore, the strength of the recommendation for the use of LMWH over twice-daily UFH is strong – 1B. The strength of recommendation for use of LMWH over thrice-daily UFH is not– 2C.")
64
Renal yetersizlik ve VTE profilaksi ilişkis 2008 de yok
VTE için profilaksi Eğer kreatinin klirensi <30 mL/dak ise dalteparin kullanılmasını (Grade 1A) veya renal metabolizma derecesi zayıf olan LMWH başka bir şekli kullanılmasını (Grade 2C) veya UFH kullanılmasını öneririz (Grade 1A). Reduced creatinine clearance was not addressed in the 2008 recommendations. Dalteparin has no bio-accumulation with creatinine clearance <30 mL/min, while UFH is not cleared by the kidney (Douketis J et al. Prophylaxis against deep vein thrombosis in critically ill patients with severe renal insufficiency with the low-molecular-weight heparin dalteparin: an assessment of safety and pharmacodynamics: the DIRECT study. Arch Intern Med. 2008;168: ). GRADE - A There are no data on other LMWHs. GRADE - C Lack of accumulation of either dalteparin or UFH in renal failure reduced the risk of significant bleeding. Other LMWHs may accumulate and increase the risk of bleeding, but accumulation has not been studied. Therefore, use of dalteparin or UFH is graded 1A and use of another LMWH is graded 2C. Renal yetersizlik ve VTE profilaksi ilişkis 2008 de yok
 veya renal metabolizma derecesi zayıf olan LMWH başka bir şekli kullanılmasını (Grade 2C) veya UFH kullanılmasını öneririz (Grade 1A). Reduced creatinine clearance was not addressed in the 2008 recommendations. Dalteparin has no bio-accumulation with creatinine clearance <30 mL/min, while UFH is not cleared by the kidney (Douketis J et al. Prophylaxis against deep vein thrombosis in critically ill patients with severe renal insufficiency with the low-molecular-weight heparin dalteparin: an assessment of safety and pharmacodynamics: the DIRECT study. Arch Intern Med. 2008;168: ). GRADE - A. There are no data on other LMWHs. GRADE - C. Lack of accumulation of either dalteparin or UFH in renal failure reduced the risk of significant bleeding. Other LMWHs may accumulate and increase the risk of bleeding, but accumulation has not been studied. Therefore, use of dalteparin or UFH is graded 1A and use of another LMWH is graded 2C. Renal yetersizlik ve VTE profilaksi ilişkis 2008 de yok.")
65
VTE için profilaksi Ağır sepsis hastalarının mümkün olduğunda farmakolojik tedavi ve aralıklı kompresyon cihazlarının kombinasyonu ile tedavi edilmelerini hatırlatırız (Grade 2C). (2008 1A) Studies were performed in patients who were not septic and not critically ill. The combination of pharmacological and mechanical prophylaxis is superior to either modality alone in preventing DVT. The combination of pharmacological and mechanical prophylaxis is superior to compression alone in preventing PE (Kakkos SK et al. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism in high-risk patients. Cochrane Database Syst Rev. 2008;4:CD005258). In a meta–analysis of 11 studies, including six RCTs, none of the included studies focused on septic or critically ill patients. Adding mechanical prophylaxis to pharmacoprophylaxis should not alter risk in any appreciable way, BUT… The data do not truly indicate a tangible outcome benefit with combined approach. Therefore, the recommendation was downgraded from 1A to 2C.
. (2008 1A) Studies were performed in patients who were not septic and not critically ill. The combination of pharmacological and mechanical prophylaxis is superior to either modality alone in preventing DVT. The combination of pharmacological and mechanical prophylaxis is superior to compression alone in preventing PE (Kakkos SK et al. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism in high-risk patients. Cochrane Database Syst Rev. 2008;4:CD005258). In a meta–analysis of 11 studies, including six RCTs, none of the included studies focused on septic or critically ill patients. Adding mechanical prophylaxis to pharmacoprophylaxis should not alter risk in any appreciable way, BUT… The data do not truly indicate a tangible outcome benefit with combined approach. Therefore, the recommendation was downgraded from 1A to 2C.")
66
VTE için profilaksi Heparine kontraendikasyonu bulunan septik hastalara farmakoprofilaksi uygulanmamasını öneririz (Grade 1B). (2 Bunun yerine eğer kontraendikasyon yok ise kademeli kompresyon çorapları, veya aralıklı kompresyon cihazları gibi mekanik profilaksi tedavisi uygulanmasını hatırlatırız (Grade 2C). Risk azaldığında farmakoprofilaksi başlanmasını hatırlatırız (Grade 2C). In some septic patients pharmacoprophylaxis is contraindicated, e.g., thrombocytopenia, severe coagulopathy, active bleeding, and recent intracerebral hemorrhage. This statement reflects common sense but is not truly supported by data. Mechanical prophylaxis is effective relative to nothing. Therefore, the first part of the recommendation was upgraded from 1C to 1B. The risk of VTE in septic patients is profound. Therefore, the first part of the recommendation was graded 1B. No high-quality study directly compares mechanical prophylaxis to pharmacoprophylaxis. Therefore, the second part of the recommendation was graded 2C.
. Risk azaldığında farmakoprofilaksi başlanmasını hatırlatırız (Grade 2C). In some septic patients pharmacoprophylaxis is contraindicated, e.g., thrombocytopenia, severe coagulopathy, active bleeding, and recent intracerebral hemorrhage. This statement reflects common sense but is not truly supported by data. Mechanical prophylaxis is effective relative to nothing. Therefore, the first part of the recommendation was upgraded from 1C to 1B. The risk of VTE in septic patients is profound. Therefore, the first part of the recommendation was graded 1B. No high-quality study directly compares mechanical prophylaxis to pharmacoprophylaxis. Therefore, the second part of the recommendation was graded 2C.")
67
Stres Ülser Profilaksisi
Kanama risk faktörü bulunan ağır sepsis/septik şok hastalarında H2 bloker veya proton pompa inhibitorleri kullanarak stres ülser profilaksisi öneririz (Grade 1B). Risk faktörleri bulunmayan hastaların profilaksi almamalarını hatırlatırız (Grade 2B). The 2004 and 2008 guidelines recognized the frequency of the problem and recommended prophylactic treatment. The 2008 guidelines started to take into account outcomes other than bleeding. Compared to the 2008 document, the 2012 recommendations are slightly weaker. First, the quality of evidence for the beneficial effect of SUP was decreased from high (A) to moderate (B); this was related to potential heterogeneity with effects possibly less/none among those fed enterally (Marik et al. Crit Care Med. 2010;38: ). The second issue requiring a difficult judgment by the panel was the recent increase in C. difficile infections and the potential increase of its prevalence by any SUP, especially using PPI (see next slides). C. difficile infection, which is associated with very low quality of evidence (QoE) in terms of its connection with SUP in the critically ill population, was judged not to be a critical outcome; hence, overall QoE remains moderate. Judging C. difficile infection as a critical outcome would change the overall QoE for SUP to low or very low and would likely result in a weak suggestion. This discussion took place and the final outcome required voting, the outcome of which was decided by only one vote. To further soften the recommendations, it is suggested that patients without risk factors (Cook et al. N Engl J Med. 1994;330: ) should not receive prophylaxis (considering the uncertainty about feeding, C. difficile infections, and VAP. The details of these considerations are presented on the next slides. 2008 Grade ….A dan 2012 Grade …..B Enteral beslenme gereksinimi azaltabilir, C. difficile infeksiyonu olasılığı
. Risk faktörleri bulunmayan hastaların profilaksi almamalarını hatırlatırız. (Grade 2B). The 2004 and 2008 guidelines recognized the frequency of the problem and recommended prophylactic treatment. The 2008 guidelines started to take into account outcomes other than bleeding. Compared to the 2008 document, the 2012 recommendations are slightly weaker. First, the quality of evidence for the beneficial effect of SUP was decreased from high (A) to moderate (B); this was related to potential heterogeneity with effects possibly less/none among those fed enterally (Marik et al. Crit Care Med. 2010;38: ). The second issue requiring a difficult judgment by the panel was the recent increase in C. difficile infections and the potential increase of its prevalence by any SUP, especially using PPI (see next slides). C. difficile infection, which is associated with very low quality of evidence (QoE) in terms of its connection with SUP in the critically ill population, was judged not to be a critical outcome; hence, overall QoE remains moderate. Judging C. difficile infection as a critical outcome would change the overall QoE for SUP to low or very low and would likely result in a weak suggestion. This discussion took place and the final outcome required voting, the outcome of which was decided by only one vote. To further soften the recommendations, it is suggested that patients without risk factors (Cook et al. N Engl J Med. 1994;330: ) should not receive prophylaxis (considering the uncertainty about feeding, C. difficile infections, and VAP. The details of these considerations are presented on the next slides Grade ….A dan 2012 Grade …..B. Enteral beslenme gereksinimi azaltabilir, C. difficile infeksiyonu olasılığı.")
68
Stress Ülser Profilaksisi
Stres ülser profilaksisi kullanıldığında H2 reseptör antagonistleri yerine proton pompa inhibitörleri kullanılmasını hatırlatırız (Grade 2C). The 2012 SSC guidelines suggested that once the decision to use SUP is made, PPI may be the preferred agent.
. The 2012 SSC guidelines suggested that once the decision to use SUP is made, PPI may be the preferred agent.")
69
Bakımın hedeflerini belirleme
Bakımın hedefleri ve prognozun hastalar ve yakınları ile konuşulmasını öneririz (Grade 1B). The first recommendation focuses on establishing goals of care and discussing prognosis with patients and families. Although the outcome of intensive care treatment in critically ill patients may be difficult to prognosticate accurately, establishing realistic treatment goals is important in promoting patient-centered care in the ICU (White DB et al. Med Decis Making. 2010;30:76-83). Since the 2008 Surviving Sepsis Campaign guidelines were published, a number of studies have identified the importance of discussing prognosis and setting realistic treatment goals. These studies have included several randomized clinical trials, many single-center observational studies, and synthesis literature reviews that have addressed the impact of family conferencing to discuss prognosis and goals (Evans LR et al. Am J Respir Crit Care Med. 2009;179:48-53; Machare Delgado E et al. Am J Hosp Palliat Care. 2009;26: ; Norton SA et al. Crit Care Med. 2007;35: ; Lee Char SJ et al. Am J Respir Crit Care Med. 2010;182; ).
. The first recommendation focuses on establishing goals of care and discussing prognosis with patients and families. Although the outcome of intensive care treatment in critically ill patients may be difficult to prognosticate accurately, establishing realistic treatment goals is important in promoting patient-centered care in the ICU (White DB et al. Med Decis Making. 2010;30:76-83). Since the 2008 Surviving Sepsis Campaign guidelines were published, a number of studies have identified the importance of discussing prognosis and setting realistic treatment goals. These studies have included several randomized clinical trials, many single-center observational studies, and synthesis literature reviews that have addressed the impact of family conferencing to discuss prognosis and goals (Evans LR et al. Am J Respir Crit Care Med. 2009;179:48-53; Machare Delgado E et al. Am J Hosp Palliat Care. 2009;26: ; Norton SA et al. Crit Care Med. 2007;35: ; Lee Char SJ et al. Am J Respir Crit Care Med. 2010;182; ).")
70
Bakımın hedeflerini belirleme
Uygun olduğunda bakımın hedeflerinin tedavi ve yaşam sonu bakım planlarında, kullanılan palyatif bakım prensiplerinde tüzel kişilik kazanmasını öneririz (Grade 1B). The second recommendation highlights that goals of care be incorporated into treatment plans and that end-of-life care planning utilizing palliative care principles be used. This recommendation is based on research that has demonstrated that the following actions can improve symptom management and patient comfort, and improve family communication: communication interventions with families; palliative care consultations; family care conferences; ethics consultations; proactive family meetings to discuss end-of-life decision making in the ICU; and integration of advanced care planning and palliative care focused on pain management, symptom control, and family support (Nelson JE et al. Crit Care Med. 2010;38: ; Machare Delgado E et al. Am J Hosp Palliat Care. 2009;4: ; Detering KM et al. BMJ. 2010;340:c1345; Curtis JR et al. Am J Respir Crit Care Med. 2008;178: ; Osborn TR et al. Am J Respir Crit Care Med. 2010;181:A6688; Quenot JP et al. Intensive Care Med. 2012;38: ; Stapleton RD et al. Crit Care Med. 2006;34: ).
. The second recommendation highlights that goals of care be incorporated into treatment plans and that end-of-life care planning utilizing palliative care principles be used. This recommendation is based on research that has demonstrated that the following actions can improve symptom management and patient comfort, and improve family communication: communication interventions with families; palliative care consultations; family care conferences; ethics consultations; proactive family meetings to discuss end-of-life decision making in the ICU; and integration of advanced care planning and palliative care focused on pain management, symptom control, and family support (Nelson JE et al. Crit Care Med. 2010;38: ; Machare Delgado E et al. Am J Hosp Palliat Care. 2009;4: ; Detering KM et al. BMJ. 2010;340:c1345; Curtis JR et al. Am J Respir Crit Care Med. 2008;178: ; Osborn TR et al. Am J Respir Crit Care Med. 2010;181:A6688; Quenot JP et al. Intensive Care Med. 2012;38: ; Stapleton RD et al. Crit Care Med. 2006;34: ).")
71
Bakımın hedeflerini belirleme
Bakımın hedefleri mümkün olan en kısa sürede yoğun bakıma girişin 72 saatini geçmeden tanımlanmasını hatırlatırız (Grade 2C). The third recommendation is that goals of care be addressed as early as feasible but no later than within 72 hours of ICU admission. This is consistent with research that has demonstrated that the use of proactive family care conferences to identify advanced directives and treatment goals early after ICU admission promotes communication and understanding between the patient’s family and the care team; improves family satisfaction; decreases stress, anxiety, and depression in surviving relatives; facilitates end-of-life decision making; and shortens length of stay for patients who die in the ICU (Bertolini G et al. Intensive Care Med. 2010;36: ; Davidson J et al. Crit Care Med. 2007;35: ; Detering KM et al. BMJ. 2010;340:c1345; Machare Delgado E et al. Am J Hosp Palliat Care. 2009;26: ; Lautretta A et al. N Engl J Med. 2007;356: ; Norton SA et al. Crit Care Med. 2007;35: ; Scheunemann LP et al. Chest. 2011;139: ).
. The third recommendation is that goals of care be addressed as early as feasible but no later than within 72 hours of ICU admission. This is consistent with research that has demonstrated that the use of proactive family care conferences to identify advanced directives and treatment goals early after ICU admission promotes communication and understanding between the patient’s family and the care team; improves family satisfaction; decreases stress, anxiety, and depression in surviving relatives; facilitates end-of-life decision making; and shortens length of stay for patients who die in the ICU (Bertolini G et al. Intensive Care Med. 2010;36: ; Davidson J et al. Crit Care Med. 2007;35: ; Detering KM et al. BMJ. 2010;340:c1345; Machare Delgado E et al. Am J Hosp Palliat Care. 2009;26: ; Lautretta A et al. N Engl J Med. 2007;356: ; Norton SA et al. Crit Care Med. 2007;35: ; Scheunemann LP et al. Chest. 2011;139: ).")
Benzer bir sunumlar