Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Trizomi tarama testleri
Prof. Dr. Yalçın Kimya

2
Trizomi 21 riski Trizomi riski maternal yaş arttıkça artar, gebelik yaşı arttıkça azalır.

3
Maternal yaş>35 Üçlü test Dörtlü test %7.5 FPR, %30 saptama oranı
İkinci trimester tarama testi yaklaşık olarak 20 yıldan beri etkili bir şekilde kullanılmaktadır. Daha sonra dörtlü test buna eklenmiştir. 1990 yılında Nicolaides ve arkadaşları ilk trimesterde maternal yaş ve NT ile %5 yalancı pozitiflik ile Down sendromu olgularının %77’ini saptadıklarını bildirmişlerdir. RİSK >35 yaş amniosentez %47 saptama, %14 FPR 1 Down saptamak için 140 amniosentez 2 Down saptamak için 1 normal fetus kaybı Üçlü test %65 saptama, %5 FPR 1 saptama için 70 amniosentez 3 Down saptamak için 1 normal fetus kaybı

4
NT PAPP-A, Free Beta HCG NT, Free Beta HCG, PAPP-A
%5 FPR, %77 saptama oranı PAPP-A, Free Beta HCG %5 FPR, %60-65 saptama oranı NT, Free Beta HCG, PAPP-A %5 FPR, %80-90 saptama oranı Nicolaides, Krantz, 1996 1996 yılında Krants ve arkadaşları sadece PAPP-A ve Free beta HCG ölçümlerinin ilk trimesterde Down sendromunu %5 yalancı pozitiflik ile %60-65 saptadığını ortaya attılar.

5
İkili test (ilk trimester serum tarama) Kombine test
PAPP-A, Free beta HCG Kombine test NT, PAPP-A, Free beta HCG İkinci trimester dörtlü test AFP, beta HCG, uE, İnhibin A Bağımsız ardışık test Stepwise ardışık tarama Serum entegre test Tam entegre test Contingent tarama İlk kez 1988 yılında Wald ve arkadaşları tarafından üçlü tarama testi Down sendromunun taranmasında kullanıma sunulmuştur. Daha sonra kombine test gündeme gelmiştir. Bu gelişmeleri otomatik olarak hem ilk trimester hem de ikinci trimesterde test isteme pratiği izlemiştir. Ancak burada tahmin edilebileceği üzere yüksek oranda yalancı pozitiflik gündeme gelmiştir. Çıkış yolu aranmıştır. Bunlardan biri stepwise ardışık tarama denen yöntem olmuştur. Burada ilk trimesterde elde edilen parametreler ikinci trimester parametreleri ile (negatif olgularda) birleştirilmiştir. Bu yalancı pozitiflik oranlarında azalmaya neden olmuştur. daha sonra contingent tarama gündeme gelmiştir. Burada olgular sonuçlarına göre gruplandırılmışlardır. Çok riskli olan, orta ve az riskli olan diye. Orta gruba başka testler yapılarak invaziv girişime karar verilmektedir. Öncelikle Down sendromu tarama yöntemlerinin tanımlanması gereklidir. Yaygın olarak kullanlan yöntemler aşağıdaki gibi sıralanabilir. İkili test (ilk trimester serum tarama) PAPP-A, Free beta HCG Kombine test NT, PAPP-A, Free beta HCG İkinci trimester dörtlü test AFP, beta HCG, uE, İnhibin A Bağımsız ardışık test İlk trimester kombine test ve ikinci trimester dörtlü testin bağımsız olarak yapılması ve ikisi için e ayrı ayrı sonuç verilmesi Serum İntegrated test İlk trimesterde PAPP-A ölçülmesi, İkinci trimesterde dörtlü test sonucu hesaplanırken ilk trimesterde ölçülen PAPP-A’nın da hesaplamaya dahil edilmesi, olguya tek sonuç verilmesi (ilk trimesterde ölçüm yapılmasına rağmen sonuç verilmemesi) Full integrated test İlk trimesterde NT ve PAPP-A ölçülmesi, İkinci trimesterde dörtlü test sonucu hesaplanırken ilk trimesterde ölçülen NT ve PAPP-A’nın da hesaplamaya dahil edilmesi, olguya tek sonuç verilmesi (ilk trimesterde ölçüm yapılmasına rağmen sonuç verilmemesi) Table 1. Data on pregnancy and pediatric outcomes were obtained in 36,837 cases (97 percent). One hundred two approved ultrasonographers performed all nuchal-translucency evaluations. The ultrasonographer failed to obtain an adequate nuchaltranslucency image in 1727 cases (4.5 percent), and in a further 974 cases (2.6 percent) the images were rejected at central review. Adequate nuchaltranslucency measurements were therefore obtained in 35,332 cases (92.9 percent). Complete first- and second-trimester screening data were available for 33,459 unaffected pregnancies and 87 pregnancies affected by Down’s syndrome. There were 117 cases of Down’s syndrome in the population of 38,167 patients (38,033 enrolled patients plus 134 patients whose fetuses had cystic hygromas). Of the 117 cases of Down’s syndrome, 25 were in the cystic-hygroma subgroup and 92 occurred among the 38,033 pregnancies described in this report Stepwise da ilk trimesterde elde edilen tüm parametreler kullanılıyor NT dahil. Bu Fasterdeki stepwise ardışık. Muhtemelen farklı yerlerdeki stepwise ardışık tanımlamaları farklı olacak. AFP Alphafetoprotein uE3 Unconjugated oestriol hCG Human chorionic gonadotrophin Free β-hCG Free β human chorionic gonadotrophin PAPP-A Pregnancy associated plasma protein A NT Nuchal translucency: An ultrasound measurement of the width of an area of translucency at the back of the fetal neck early in pregnancy. Triple test Second-trimester test based on the measurement of AFP, uE3, and hCG (either total hCG or free β-hCG) together with maternal age. Quadruple test Second-trimester test based on the measurement of AFP, uE3, free β-hCG (or total hCG), and inhibin-A together with maternal age. Combined test First-trimester test based on combining nuchal translucency measurement with free β-hCG, PAPP-A and maternal age. Integrated test The integration of measurements performed at different times of pregnancy into a single test result. Unless otherwise qualified, ‘Integrated test’ refers to the integration of nuchal translucency measurement and PAPP-A in the first trimester with the Quadruple test markers in the second. Serum Integrated test A variant of the Integrated test without nuchal translucency (using PAPP-A in the first trimester and all or some of the quadruple test markers in the second trimester). Sequential screening Screening in which a first-trimester test is performed (for example, the Combined test) and the result interpreted immediately. If this is positive, a diagnostic test is offered, but if it is not positive, second-trimester serum markers are measured and the first-trimester markers reused to form an Integrated test. Contingent screening Screening in which a first-trimester test is used to triage the population of women screened into three groups: one group (high risk screen-positive) that is immediately offered a diagnostic test, a second group (screen-negative) that receives no further screening, and a third intermediate (or lower risk screen positive) group that has second-trimester markers measured and the first-trimester measurements reused to form an Integrated test.
 birleştirilmiştir. Bu yalancı pozitiflik oranlarında azalmaya neden olmuştur. daha sonra contingent tarama gündeme gelmiştir. Burada olgular sonuçlarına göre gruplandırılmışlardır. Çok riskli olan, orta ve az riskli olan diye. Orta gruba başka testler yapılarak invaziv girişime karar verilmektedir. Öncelikle Down sendromu tarama yöntemlerinin tanımlanması gereklidir. Yaygın olarak kullanlan yöntemler aşağıdaki gibi sıralanabilir. İkili test (ilk trimester serum tarama) PAPP-A, Free beta HCG. Kombine test. NT, PAPP-A, Free beta HCG. İkinci trimester dörtlü test. AFP, beta HCG, uE, İnhibin A. Bağımsız ardışık test. İlk trimester kombine test ve ikinci trimester dörtlü testin bağımsız olarak yapılması ve ikisi için e ayrı ayrı sonuç verilmesi. Serum İntegrated test. İlk trimesterde PAPP-A ölçülmesi, İkinci trimesterde dörtlü test sonucu hesaplanırken ilk trimesterde ölçülen PAPP-A’nın da hesaplamaya dahil edilmesi, olguya tek sonuç verilmesi (ilk trimesterde ölçüm yapılmasına rağmen sonuç verilmemesi) Full integrated test. İlk trimesterde NT ve PAPP-A ölçülmesi, İkinci trimesterde dörtlü test sonucu hesaplanırken ilk trimesterde ölçülen NT ve PAPP-A’nın da hesaplamaya dahil edilmesi, olguya tek sonuç verilmesi (ilk trimesterde ölçüm yapılmasına rağmen sonuç verilmemesi) Table 1. Data on pregnancy and pediatric outcomes. were obtained in 36,837 cases (97 percent). One. hundred two approved ultrasonographers performed. all nuchal-translucency evaluations. The ultrasonographer. failed to obtain an adequate nuchaltranslucency. image in 1727 cases (4.5 percent), and in a further 974 cases (2.6 percent) the images. were rejected at central review. Adequate nuchaltranslucency. measurements were therefore obtained. in 35,332 cases (92.9 percent). Complete. first- and second-trimester screening data were. available for 33,459 unaffected pregnancies and 87. pregnancies affected by Down’s syndrome. There. were 117 cases of Down’s syndrome in the population. of 38,167 patients (38,033 enrolled patients. plus 134 patients whose fetuses had cystic hygromas). Of the 117 cases of Down’s syndrome, 25. were in the cystic-hygroma subgroup and 92 occurred. among the 38,033 pregnancies described in. this report. Stepwise da ilk trimesterde elde edilen tüm parametreler kullanılıyor NT dahil. Bu Fasterdeki stepwise ardışık. Muhtemelen farklı yerlerdeki stepwise ardışık tanımlamaları farklı olacak. AFP Alphafetoprotein. uE3 Unconjugated oestriol. hCG Human chorionic gonadotrophin. Free β-hCG Free β human chorionic gonadotrophin. PAPP-A Pregnancy associated plasma protein A. NT Nuchal translucency: An ultrasound measurement of the width of an area of translucency at. the back of the fetal neck early in pregnancy. Triple test Second-trimester test based on the measurement of AFP, uE3, and hCG (either total hCG or. free β-hCG) together with maternal age. Quadruple test Second-trimester test based on the measurement of AFP, uE3, free β-hCG (or total hCG), and. inhibin-A together with maternal age. Combined test First-trimester test based on combining nuchal translucency measurement with free β-hCG, PAPP-A and maternal age. Integrated test The integration of measurements performed at different times of pregnancy into a single test. result. Unless otherwise qualified, ‘Integrated test’ refers to the integration of nuchal. translucency measurement and PAPP-A in the first trimester with the Quadruple test markers. in the second. Serum Integrated test A variant of the Integrated test without nuchal translucency (using PAPP-A in the first. trimester and all or some of the quadruple test markers in the second trimester). Sequential screening Screening in which a first-trimester test is performed (for example, the Combined test) and the. result interpreted immediately. If this is positive, a diagnostic test is offered, but if it is not. positive, second-trimester serum markers are measured and the first-trimester markers reused. to form an Integrated test. Contingent screening Screening in which a first-trimester test is used to triage the population of women screened. into three groups: one group (high risk screen-positive) that is immediately offered a. diagnostic test, a second group (screen-negative) that receives no further screening, and a third. intermediate (or lower risk screen positive) group that has second-trimester markers measured. and the first-trimester measurements reused to form an Integrated test.")
6
Kombine test (yaygın olarak ikili test olarak adlandırılmakta)
")
7
The optimal gestational age for measurement of fetal NT is weeks. The minimum fetal crown–rump length (CRL) should be 45 mm and the maximum 84 mm The reasons for selecting 11 weeks as the earliest gestation are: Screening necessitates the availability of a diagnostic test and chorionic villous sampling before this gestation is associated with transverse limb reduction defects Many major fetal abnormalities can be diagnosed at the NT scan, provided the minimum gestation is 11 weeks The reasons for selecting 13 weeks and 6 days as the upper limit are: To provide women with affected fetuses the option of 1st rather than 2nd trimester termination The incidence of abnormal accumulation of nuchal fluid in chromosomally abnormal fetuses decreases after 13 weeks The success rate for taking a measurement decreases after 13 weeks because the fetus becomes vertical making it more difficult to obtain the appropriate image

8
ABSTRACT 60 mm CRL nin eksik ya da fazla ölçülmesi saptama oranı ve yalancı pozitiflik oranını etkiler. Bu nedenle Hata yapmaktan kaçınmak gerekir. Objective To assess the repeatability of crown–rump length (CRL) measurement and examine the effect of its over- and underestimation on first-trimester combined screening. Methods Intra- and interoperator repeatability of CRL measurement at 11–13 weeks of gestation was assessed in 124 cases by two operators. Raw data were transformed into gestational age and intra- and interoperator repeatability was evaluated by within-operator standard deviation (SD) and the SD of differences in measurements between both operators. Modeling techniques were used to assess the impact of CRL measurement error on general population screening and on the operatorspecific screening performance. The impact of errors in CRL measurement were investigated by simulating fetal nuchal translucency (NT) measurements and multiple of the median (MoM) values for pregnancy-associated plasma protein A (PAPP-A) and free β-human chorionic gonadotropin (β-hCG) for euploid and trisomy 21 pregnancies at 12 weeks and 9 weeks of gestation, and adding to or subtracting from each CRL value up to 10 mm and recalculating patient-specific risks. Results Within-operator SD of the CRL measurement was 1.27 days of gestation. The SD of the differences in CRL measurement between operators was 1.37 days of gestation. Both intra- and interoperator 95% limits of agreement were around ±5 mm. In general populationbased screening, a CRL measurement error SD of 5 mm accounts for an estimated 5% of the SD of log MoM PAPP-A and less than 1% of the SD of log MoM free β-hCG. Modeling the effect of removing this measurement error on overall screening performance showed a minimal impact. For a risk cut-off of 1 in 100, the benefit in terms of overall screening performance would be an increase in detection rate of about 1% and a reduction in false-positive rate of less than 0.1%. With regard to the operator-specific screening performance, a consistent 5-mm underestimation of CRL reduces the detection rate from 84% to 79% and the false-positive rate from 2.4% to 1.2%.With a consistent 5-mm overestimation the rates would be 88% and 5.6%, respectively. Conclusion The impact of the interoperator variability in CRL measurement on patient-specific risk needs to be taken into account when interpreting first-trimester screening results. A systematic under- or overestimation of CRL should be avoided. Copyright 8
 measurement and examine the effect of. its over- and underestimation on first-trimester combined. screening. Methods Intra- and interoperator repeatability of CRL. measurement at 11–13 weeks of gestation was assessed. in 124 cases by two operators. Raw data were transformed. into gestational age and intra- and interoperator. repeatability was evaluated by within-operator standard. deviation (SD) and the SD of differences in measurements. between both operators. Modeling techniques were. used to assess the impact of CRL measurement error. on general population screening and on the operatorspecific. screening performance. The impact of errors in. CRL measurement were investigated by simulating fetal. nuchal translucency (NT) measurements and multiple. of the median (MoM) values for pregnancy-associated. plasma protein A (PAPP-A) and free β-human chorionic. gonadotropin (β-hCG) for euploid and trisomy 21 pregnancies at 12 weeks and 9 weeks of gestation, and adding to or subtracting from each CRL value. up to 10 mm and recalculating patient-specific risks. Results Within-operator SD of the CRL measurement. was 1.27 days of gestation. The SD of the differences in. CRL measurement between operators was 1.37 days of. gestation. Both intra- and interoperator 95% limits of. agreement were around ±5 mm. In general populationbased. screening, a CRL measurement error SD of 5 mm. accounts for an estimated 5% of the SD of log MoM. PAPP-A and less than 1% of the SD of log MoM free. β-hCG. Modeling the effect of removing this measurement. error on overall screening performance showed a. minimal impact. For a risk cut-off of 1 in 100, the benefit. in terms of overall screening performance would be an. increase in detection rate of about 1% and a reduction. in false-positive rate of less than 0.1%. With regard to. the operator-specific screening performance, a consistent. 5-mm underestimation of CRL reduces the detection rate. from 84% to 79% and the false-positive rate from 2.4% to 1.2%.With a consistent 5-mm overestimation the rates. would be 88% and 5.6%, respectively. Conclusion The impact of the interoperator variability. in CRL measurement on patient-specific risk needs to. be taken into account when interpreting first-trimester. screening results. A systematic under- or overestimation. of CRL should be avoided. Copyright 8.")
9
NT Mid sagital Baş ve toraks üst kısmı ekranı kaplamalı
Nötral pozisyon Baş spinal kord ile aynı hizada Amniotik membran ayırt edilmeli Görüntünün büyüklüğü fetal baş ve gögüs kafesinin üst kısmı tüm ekranı kaplayacak şekilde büyütülmelidir Fetüsün mid sagittal kesiti alınmalıdır Fetüs nötral pozisyonda, baş spinal kord ile ayni hizada olmalıdır. Eğer fetal boyun hiperekstansiyonda ise ölçüm yanlış olarak artmış ve boyun fleksiyonda ise yanlış olarak azalmıştır Fetal cilt ile amniyon zarının ayırt edilmesine dikkat edilmelidir

10
Kaliper amnios ile temas etmemeli En geniş yer Gain azaltılması
Saydamlıgın en genis oldugu bölge her zaman ölçülmelidir Cilt ve yumuşak doku arasındaki cilt altı sıvı (NT) servikal omurlar uzerinde en genis oldugu yerden ölçülmelidir. Artı seklindeki kaliperler NT kalınlığını tanımlayan beyaz cizgilerin hemen uzerine, cizgiden ayırt edilemeyecek şekilde yerlestirilmeli ve sıvı görünümünün üzerine kaliperler temas etmemelidir Görüntüyü büyütürken gain ayarını düşürmek (dondurulduktan önce veya sonra) önemlidir. Gain ayarının düşürülmesi ile NT çizgileri daha net belirir ve bu kaliperleri bulanık, net olmayan ve gerçekte olduğundan daha dar görünebilecek NT çizgileri üzerine yerleştirme hatasından koruyarak NT nin olduğundan küçük ölçülmesine engel olur Tarama sırasında birden fazla ölçüm alınmali ve tüm bu kriterlere uyan en büyük ölçüm veri tabanına kaydedilmelidir
 servikal omurlar uzerinde en genis oldugu yerden ölçülmelidir. Artı seklindeki kaliperler NT kalınlığını tanımlayan beyaz cizgilerin hemen uzerine, cizgiden ayırt edilemeyecek şekilde yerlestirilmeli ve sıvı görünümünün üzerine kaliperler temas etmemelidir. Görüntüyü büyütürken gain ayarını düşürmek (dondurulduktan önce veya sonra) önemlidir. Gain ayarının düşürülmesi ile NT çizgileri daha net belirir ve bu kaliperleri bulanık, net olmayan ve gerçekte olduğundan daha dar görünebilecek NT çizgileri üzerine yerleştirme hatasından koruyarak NT nin olduğundan küçük ölçülmesine engel olur. Tarama sırasında birden fazla ölçüm alınmali ve tüm bu kriterlere uyan en büyük ölçüm veri tabanına kaydedilmelidir.")
11
Burun kemiği ve yüz açısı
Doğru mid-sagital plan şöyle tanımlanır: Önde ekojenik burun ucu ve dikdörtgen şeklinde damak Merkezde saydam diensefalon Arkada nukal zar Başın çevrilmesi orta hattan yaklaşık 10 derece ile burun ucu görüntüden çıkar, zigomatik kemik görüntüye girer ki bu üstte nazal kemik ile altta damağın ön kısmı arasındaki ekojenik yapıdır Orta hattan daha da fazla yaklaşık 15 derece çevrildiğinde nazal kemik kaybolur ve damağın da birleşmesiyle zigomatik kemik genişler

12
Orta hattan sapma arttıkça NT daha az ölçülüyor
Orta hattan sapma arttıkça NT daha az ölçülüyor. Bu da saptama oranını azaltıyor. ABSTRACT Objective Screening for trisomy 21 by fetal nuchal translucency (NT) thickness at 11 to weeks’ gestation requires an appropriate examination of the NT. Errors in the assessment of NT may lead to an under- or overestimation of the NT and to incorrect patient-specific risks. In this study we aimed to examine the importance of the mid-sagittal section and whether the acquired plane of the head and face influences the measurement of the fetal NT thickness. Methods Sixty three-dimensional volumes of the fetal head and face in a mid-sagittal plane were acquired. NT thickness was firstly measured in the mid-sagittal plane according to the guidelines of The Fetal Medicine Foundation. The head was then rotated by steps of 5◦ up to 25◦ around themid-point of the biparietal diameter and occipitofrontal diameter and NT was measured again. All six NT measurements were taken by the same operator, Operator A, who on completion of the assessment of the 60 volumes repeated all the measurements. The whole process was then repeated by Operator B. Both operators were blinded to each others’ measurements. Results In the true mid-sagittal plane, the mean NT was 1.9 mm and it was above the expected median in 72.5% of the measurements. At a deviation of 15◦, mean NT was 1.5 mm, and 36.3% of the measurements were above the expected median. At a deviation of 25◦, mean NT was reduced to 1.3 mm and 17.9% of the measurements were above the expected median. Conclusion Fetal NT thickness is greatest in the midsagittal plane. Increasing deviation away from the midsagittal plane results in progressive underestimation of the fetal NT thickness and so to a corresponding underestimation of the patient-specific risk. Copyright 2010 ISUOG. Published by John Wiley & Sons, Ltd
 thickness at 11 to weeks’ gestation requires an appropriate examination of the NT. Errors in the assessment of NT may lead to an under- or. overestimation of the NT and to incorrect patient-specific. risks. In this study we aimed to examine the importance. of the mid-sagittal section and whether the acquired plane. of the head and face influences the measurement of the. fetal NT thickness. Methods Sixty three-dimensional volumes of the fetal. head and face in a mid-sagittal plane were acquired. NT thickness was firstly measured in the mid-sagittal. plane according to the guidelines of The Fetal Medicine. Foundation. The head was then rotated by steps of 5◦ up. to 25◦ around themid-point of the biparietal diameter and. occipitofrontal diameter and NT was measured again. All. six NT measurements were taken by the same operator, Operator A, who on completion of the assessment of the. 60 volumes repeated all the measurements. The whole. process was then repeated by Operator B. Both operators. were blinded to each others’ measurements. Results In the true mid-sagittal plane, the mean NT was. 1.9 mm and it was above the expected median in 72.5% of the measurements. At a deviation of 15◦, mean NT was. 1.5 mm, and 36.3% of the measurements were above the. expected median. At a deviation of 25◦, mean NT was. reduced to 1.3 mm and 17.9% of the measurements were. above the expected median. Conclusion Fetal NT thickness is greatest in the midsagittal. plane. Increasing deviation away from the midsagittal. plane results in progressive underestimation of. the fetal NT thickness and so to a corresponding. underestimation of the patient-specific risk. Copyright. 2010 ISUOG. Published by John Wiley & Sons, Ltd.")
13
Artmış NT Kromozomal anomali, fetal ölüm, major defekt Artmış NT
Sonuçları KROMOZOMAL DEFEKTLER Kromozomal defektlerin sıklığı NT’nin 5. ve 95. persantilinde olan olgularda %0.2’den NT’nin 6.5 mm’de veya daha fazla olanlarda %65’e kadar belirgin olarak artar Kromozomal olarak anormal grubun; yaklaşık %50’sini trizomi 21, %25’ini trizomi 18 veya 13, %10’unu Turner sendromu, %5’ini triploidi ve %10’unu da diğer kromozomal defektler oluşturur FETAL ÖLÜM Kromozomal olarak normal olan fetuslarda NT’nin persantil arasında olduğu olgularda %1 olan fetal ölüm oranı NT’nin 6.5 mm ve üzerine çıktığı olgularda %20’ye kadar ulaşan fetal ölüm sıklığı NT kalınlaşması ile artar Fetal olümlerin çoğu 20. haftadan önce olur ve bunlarda genellikle artmış NT ciddi hidropsa ilerler MAJOR DEFEKTLER Medikal ve/veya cerrahi tedavi gerektiren ya da mental geriliğe yol açan anomali major fetal anomali olarak tanımlanır Kromozomu normal olan fetuslarda NT’nin 95. persantilin altında olanlarda %1.5’den NT’nin persantilindekilerde %2.5’e ve NT’nin 6.5 mm ve üzerine çıktığı olgularda belirgin olarak artarak %45’e ulaşan major fetal anomali prevalansı NT kalınlığı ile artar Kromozomal anomali, fetal ölüm, major defekt

14
Artmış NT, sağlıklı doğum
Her ne kadar artmış NT kalınlığı anomaliler ve fetal ölümle ilişkili ise de bebeklerin büyük çoğunluğu canlı doğar ve normal gelişim gösterir Artmış NT tespit edildiğinde amaç problem olması muhtemel bebeklerle normal olan bebekleri mümkün olduğunca çabuk ve doğru olarak ayırt etmek olmalıdır

15
Nuchal Translucency Trizomi 21’li fetuslerin %75-80’inde
NT>95. persantil Maternal yaştan bağımsız NT’nin kalınlığı öploid fetüslerde BPM ile artar Trizomi 21’li fetüslerin %75-80’inde NT kalınlığı normal oranların 95. persentilin üzerindedir Trizomi 21’li fetüslerde NT kalınlığı ile anne yaşı arasında ilişki yoktur yani NT kalınlığı ve anne yaşı birbirinden bağımsızdır Kromozomal anomaliler için etkili bir ilk trimester tarama testi sağlamak için anne yaşı ile fetal NT birleştirebilinir Verilen bir CRL ölçümü için, her NT ölçümü bir “olasılık oranı” ifade eder ve bu oran, maternal yaş ve gestasyonel haftaya bağli olarak hesaplanan basal risk ile çarpılarak gebenin kromozomal anomalili fetüse sahip olma riski “yeni risk“ belirlenir NT arttıkça ‘Olasılık Oranı’ artar ve böylece ‘Yeni Risk’te artmış olur Aksine, NT küçüldükçe ‘Olasılık Oranı’ küçülür ve böylece ‘Yeni Risk’ azalır 20 yaşında NT kalınlığı artmış ölçülen bir kadının kromozomal anomalili fetuse sahip olma riski, 40 yaşında ki NT kalınlık ölçümü düşük olan bir kadına göre daha yüksektir

17
serbest ß-hCG PAPP-A Trizomi 21 2.0 0.5 Trizomi 18 0.2 Trizomi 13 0.3 0.4 Turner 1.2 Triploidi Diginik 0.1 Diandrik 9.0 0.7 Down sendromunu tararken %0.1 FPR artışı ile Trizomi 13 ve 18’in %95’i saptanıyor Birleşik tarama Diğer defektler Öploid gebeliklerde ortalama serbest ß-hCG 1.0 MoM ve PAPP-A 1.0 MoM’dir. Kromozomal defektlilerdeki değerler: serbest ß-hCGPAPP-ATrizomi Trizomi Trizomi Turner1.20.5Triploidi Diginik0.20.1 Diandrik9.00.7

18
Kalp atım hızı 5. hafta 110/dk 10. hafta 170/dk 14. hafta 150/dk
Normal gebelikte, FKH 5. gebelik haftasında yaklaşık 110 bpm’den 10. gebelik haftasında ise 170 bpm’e yükselir ve sonra tedricen 14. haftada 150 bpm’e düşer 5. hafta 110/dk 10. hafta 170/dk 14. hafta 150/dk

19
Trizomi 21’de FKH çok az artar ve olguların yaklaşık %15’de 95
Trizomi 21’de FKH çok az artar ve olguların yaklaşık %15’de 95. persentilin üzerindedir Trizomi 18’de FKH çok az yavaştır ve olguların %15’de 5. persentelin altındadır Trizomi 13 FKH önemli olarak artar ve olguların %85’de 95. persentelin üzerindedir FKH’nın eklenmesi ilk trimesterde kromozomal anomali tanısında birleşik biyokimyasal ve sonografik taramasında trizomi 21 ve 18 tanısına küçük bir katkı sağlarken, trizomi 13 tanısında önemli bir katkı sağlar Ek olarak, FKA nın değerlendirilmesiTrizomi 18 ve Trizomi 13 ayrımında önemlidir çünkü artmış fetal NT, azalmış serum s-βhcg ve PAPP-A bulguları her iki kromozomal anomalide de benzerlik gösterir, bu nedenle FKA ikisi arasında ayrımda önemlidir BACKGROUND: A beneficial consequence of screening for trisomy 21 is the early diagnosis of trisomies 18 and 13. Our objective was to examine the performance of first-trimester screening for trisomies 21, 18 and 13 by maternal age, fetal nuchal translucency (NT) thickness, fetal heart rate (FHR) and maternal serum-free b-hCG and pregnancyassociated plasma protein-A (PAPP-A). METHODS: Prospective screening for trisomy 21 by maternal age, fetal NT, free b-hCG and PAPP-A at 1110–1316 weeks in singleton pregnancies, including normal cases, 395 with trisomy 21, 122 with trisomy 18 and 61 with trisomy 13. Risk algorithms were developed for the calculation of patient-specific risks for each of the three trisomies based on maternal age, NT, FHR, free b-hCG and PAPP-A. Detection (DR) and false positive rates (FPR) were calculated and adjusted according to the maternal age distribution of pregnancies in England and Wales in 2000–2002. RESULTS: The DR and FPR were 90% and 3%, respectively, for trisomy 21, 91% and 0.2% for trisomy 18 and 87% and 0.2% for trisomy 13. When screen positivity was defined by an FPR of 3% on the risk for trisomy 21 in conjunction with an FPR of 0.2% on the maximum of the risks for trisomies 13 and 18, the overall FPR was 3.1% and the DRs of trisomies 21, 18 and 13 were 91%, 97% and 94%, respectively. CONCLUSIONS: As a side effect of first-trimester screening for trisomy 21, 95% of trisomy 13 and 18 fetuses can be detected with an 0.1% increase in the FPR.
 thickness, fetal heart rate (FHR) and maternal serum-free b-hCG and pregnancyassociated. plasma protein-A (PAPP-A). METHODS: Prospective screening for trisomy 21 by maternal age, fetal. NT, free b-hCG and PAPP-A at 1110–1316 weeks in singleton pregnancies, including normal cases, 395. with trisomy 21, 122 with trisomy 18 and 61 with trisomy 13. Risk algorithms were developed for the calculation. of patient-specific risks for each of the three trisomies based on maternal age, NT, FHR, free b-hCG and PAPP-A. Detection (DR) and false positive rates (FPR) were calculated and adjusted according to the maternal age distribution. of pregnancies in England and Wales in 2000–2002. RESULTS: The DR and FPR were 90% and 3%, respectively, for. trisomy 21, 91% and 0.2% for trisomy 18 and 87% and 0.2% for trisomy 13. When screen positivity was defined by an. FPR of 3% on the risk for trisomy 21 in conjunction with an FPR of 0.2% on the maximum of the risks for trisomies 13. and 18, the overall FPR was 3.1% and the DRs of trisomies 21, 18 and 13 were 91%, 97% and 94%, respectively. CONCLUSIONS: As a side effect of first-trimester screening for trisomy 21, 95% of trisomy 13 and 18 fetuses. can be detected with an 0.1% increase in the FPR.")
20
Burada değişik eşik değerlerde saptama ve FPR değişiklikleri çok çarpıcı
19614 ilk trimester kombine tarama değerlendirilmiş Bu slide ile eşik değer İkili test Kombine testin anlamları verilebilir.

21
Bu tablo ise beklenen ve gözlenen riski gösteriyor
Bu tablo ise beklenen ve gözlenen riski gösteriyor. Yaklaşık olarak benzer sonuçlar.

22
Trizomi 21 Trizomi 18 FPR %5 DR %83.3 DR %66.7
Am J Obstet Gynecol 2007;197:374.e1-374.e3 Trizomi 21 FPR %5 DR %83.3 Trizomi 18 DR %66.7

23
İkiz Dikorionik ikizlerde CRL ve NT bağımsız
Monokorionik ikizlerde ortalama NT Nicolaides, 2011 In twin pregnancies, effective screening for chromosomal abnormalities is provided by a combination of maternal age and fetal NT thickness (Pandya et al., 1995b; Sebire et al., 1996a, 1996b; Maymon et al., 2001). The performance of screening can be improved by the addition of maternal serum biochemistry, but appropriate adjustments are needed for chorionicity (Sepulveda, et al., 1996). In dichorionic twins at 11 to 13 weeks, the levels of maternal serum free β-hCG and PAPP-A are about twice as high as in singleton pregnancies, but in monochorionic twins the levels are lower than in dichorionic twins (Spencer and Nicolaides, 2000, 2003; Spencer et al., 2008; Linskens et al., 2009). In dichorionic twins, patient-specific risks for trisomy 21 are calculated for each fetus based on maternal age and fetal NT, and the detection rate (75–80%) and falsepositive rate (5% per fetus or 10% per pregnancy) are similar to those in singleton pregnancies (Sebire et al., 1996a). In the calculation of risk for trisomies, it has been assumed that in each pregnancy the measurements of NT for CRL between the two fetuses were independent of each other. However, recent evidence indicates that in euploid dichorionic twins, the measurements of NT in each twin pair are correlated and this correlation is not a simple reflection of the common effect of sonographers (Wøjdemann et al., 2006; Cuckle and Maymon, 2010; Wright et al., 2011). In screening in twins it is therefore necessary to take this correlation into account because it has a substantial impact on the estimated patient-specific risk for trisomies. First-trimester screening allows the possibility of earlier and therefore safer selective fetocide in cases where one fetus is euploid and the other is abnormal (Sebire et al., 1996b). An important advantage of screening by fetal NT is that when there is discordance for a chromosomal abnormality, the presence of a sonographically detectable marker helps to ensure the correct identification of the abnormal twin should the parents choose selective termination. In monochorionic twin pregnancies, the false-positive rate of NT screening is higher than in dichorionic twins, because increased NT in at least one of the fetuses is an early manifestation of twin-to-twin-transfusion syndrome, as well as a marker of chromosomal abnormalities (Sebire et al., 1997, 2000; Kagan et al., 2007). In the calculation of risk of trisomy 21, the NT of both fetuses should be measured and the average of the two should be considered (Vandecruys et al., 2005).
. The performance of screening can be improved. by the addition of maternal serum biochemistry, but. appropriate adjustments are needed for chorionicity. (Sepulveda, et al., 1996). In dichorionic twins at 11 to. 13 weeks, the levels of maternal serum free β-hCG and. PAPP-A are about twice as high as in singleton pregnancies, but in monochorionic twins the levels are lower. than in dichorionic twins (Spencer and Nicolaides, 2000, 2003; Spencer et al., 2008; Linskens et al., 2009). In dichorionic twins, patient-specific risks for trisomy. 21 are calculated for each fetus based on maternal age. and fetal NT, and the detection rate (75–80%) and falsepositive. rate (5% per fetus or 10% per pregnancy) are. similar to those in singleton pregnancies (Sebire et al., 1996a). In the calculation of risk for trisomies, it has. been assumed that in each pregnancy the measurements. of NT for CRL between the two fetuses were independent. of each other. However, recent evidence indicates. that in euploid dichorionic twins, the measurements of. NT in each twin pair are correlated and this correlation. is not a simple reflection of the common effect of sonographers. (Wøjdemann et al., 2006; Cuckle and Maymon, 2010; Wright et al., 2011). In screening in twins it is. therefore necessary to take this correlation into account. because it has a substantial impact on the estimated. patient-specific risk for trisomies. First-trimester screening. allows the possibility of earlier and therefore safer. selective fetocide in cases where one fetus is euploid and. the other is abnormal (Sebire et al., 1996b). An important. advantage of screening by fetal NT is that when. there is discordance for a chromosomal abnormality, the. presence of a sonographically detectable marker helps. to ensure the correct identification of the abnormal twin. should the parents choose selective termination. In monochorionic twin pregnancies, the false-positive. rate of NT screening is higher than in dichorionic twins, because increased NT in at least one of the fetuses is. an early manifestation of twin-to-twin-transfusion syndrome, as well as a marker of chromosomal abnormalities. (Sebire et al., 1997, 2000; Kagan et al., 2007). In. the calculation of risk of trisomy 21, the NT of both. fetuses should be measured and the average of the two. should be considered (Vandecruys et al., 2005).")
24
Ölçülebilir CRL ile ölü fetus PAPP-A 1.34 MOM DR %85’de %75’e düşer
Sadece NT ile tarama önerilmiş Objective To assess the impact of a vanishing twin on the levels of the biochemical markers used in the first trimester aneuploidy screening. Methods A retrospective analysis of free β-hCG and PAPP-A levels in 270 women with a normal singleton fetus with ultrasound evidence of a vanishing twin pregnancy. Marker levels (as MoM) were compared in three groups—76 women with a second empty gestational sac, 194 women with a second gestational sac containing a dead fetus with a measurable crown rump length (CRL), and 1360 matched singleton pregnancies. Results In women with a second empty gestational sac, the median free β-hCG and PAPP-A MoMs (0.968 and 1.040, respectively) were not significantly different from the 1.0 MoM in singleton pregnancies. In the group with a vanished twin with a measurable—CRL—there was a significantly increased median PAPP-A MoM (1.317) but the median free β-hCG MoM was not changed (1.024). Modelling this bias in PAPP-A MoM the detection rate for trisomy 21 would fall from 85 to 75%. Conclusion First trimester screening in the presence of a vanishing twin may lead to errors in risk estimation. In such circumstances it may be advisable to restrict screening to the use of nuchal translucency (NT) alone. Copyright 2010 John Wiley & Sons, Ltd. KEY WORDS: Down syndrome; prenatal screening; PAPP-A; free β-hCG; trisomy; vanishing twin INTRODUCTION First trimester screening which combines the ultrasound measurement of nuchal translucency (NT) with the biochemical measurement of maternal serum free β-hCG and PAPP-A is one of the most effective methods of screening for Down syndrome (trisomy 21) enabling detection rates of 90% to be achieved at false-positive rate of 5% or less (Spencer et al., 1999; Nicolaides et al., 2005). In addition this method of screening also identifies a large proportion of the other major aneuploidies such as trisomies 13 and 18 (Tul et al., 1999; Spencer et al., 2000b), triploidy (Spencer et al., 2000d), and various sex aneuploidies (Spencer et al., 2000a). A number of confounding factors are known to influence primarily the maternal serum biochemical markers. These include gestational age, maternal weight, ethnicity, smoking status, parity, mode of conception in vitro fertilisation (IVF), twin pregnancy, and chorionicity (Spencer, 2000, 2005; Spencer et al., 2000c,f, 2003, 2004, 2005a, 2008; Liao et al., 2001; Kagan et al., 2007, 2008). Most of these confounders have such a significant influence as to require correction for. Others such as diabetes, fetal sex, previous aneuploidy history, early vaginal bleeding (Cuckle et al., 2005; Cowans et al., *Correspondence to: K. Spencer, Clinical Biochemistry Department, King George Hospital, Barley Lane, Goodmayes IG3 8YB, UK. 2009; Spencer et al., 2000e, 2005b, 2009a 24
 were compared in three. groups—76 women with a second empty gestational sac, 194 women with a second gestational sac containing. a dead fetus with a measurable crown rump length (CRL), and 1360 matched singleton pregnancies. Results In women with a second empty gestational sac, the median free β-hCG and PAPP-A MoMs ( and 1.040, respectively) were not significantly different from the 1.0 MoM in singleton pregnancies. In the. group with a vanished twin with a measurable—CRL—there was a significantly increased median PAPP-A. MoM (1.317) but the median free β-hCG MoM was not changed (1.024). Modelling this bias in PAPP-A. MoM the detection rate for trisomy 21 would fall from 85 to 75%. Conclusion First trimester screening in the presence of a vanishing twin may lead to errors in risk estimation. In such circumstances it may be advisable to restrict screening to the use of nuchal translucency (NT) alone. Copyright 2010 John Wiley & Sons, Ltd. KEY WORDS: Down syndrome; prenatal screening; PAPP-A; free β-hCG; trisomy; vanishing twin. INTRODUCTION. First trimester screening which combines the ultrasound. measurement of nuchal translucency (NT) with the biochemical. measurement of maternal serum free β-hCG. and PAPP-A is one of the most effective methods of. screening for Down syndrome (trisomy 21) enabling. detection rates of 90% to be achieved at false-positive. rate of 5% or less (Spencer et al., 1999; Nicolaides et al., 2005). In addition this method of screening also identifies. a large proportion of the other major aneuploidies. such as trisomies 13 and 18 (Tul et al., 1999; Spencer. et al., 2000b), triploidy (Spencer et al., 2000d), and various. sex aneuploidies (Spencer et al., 2000a). A number of confounding factors are known to influence. primarily the maternal serum biochemical markers. These include gestational age, maternal weight, ethnicity, smoking status, parity, mode of conception in. vitro fertilisation (IVF), twin pregnancy, and chorionicity. (Spencer, 2000, 2005; Spencer et al., 2000c,f, 2003, 2004, 2005a, 2008; Liao et al., 2001; Kagan et al., 2007, 2008). Most of these confounders have such a significant. influence as to require correction for. Others such. as diabetes, fetal sex, previous aneuploidy history, early. vaginal bleeding (Cuckle et al., 2005; Cowans et al., *Correspondence to: K. Spencer, Clinical Biochemistry Department, King George Hospital, Barley Lane, Goodmayes IG3. 8YB, UK ; Spencer et al., 2000e, 2005b, 2009a. 24.")
25
First And Second Trimester Evaluation of Risk
Bu konudaki en önemli çalışmalardan biri FASTER çalışmasıdır. Bu çalışma yılları arasında ABD’de 15 merkezde yapılmış. First And Second Trimester Evaluation of Risk yılları arasında ABD’de 15 merkez

26
FASTER 36837 olgu 1727 olguda NT ölçülememiş (%4.5)
974 olgunun ölçümü kabul edilmemiş (%2.6) NT ölçüm başarısızlığı %7.1 Bu çalışmaya gör haftalarda NT ölçümü olguların %7.1’inde başarılamayacak kadar zor bir incelemedir. Bazı çalışmalarda ölçüm yapılamama sıklığı %0.5 olarak verilse de, ölçüm kalitesi yönünden değerlendirildiğinde, başarısızlık muhtemelen %7 olmalıdır. Table 1. Data on pregnancy and pediatric outcomes were obtained in 36,837 cases (97 percent). One hundred two approved ultrasonographers performed all nuchal-translucency evaluations. The ultrasonographer failed to obtain an adequate nuchaltranslucency image in 1727 cases (4.5 percent), and in a further 974 cases (2.6 percent) the images were rejected at central review. Adequate nuchaltranslucency measurements were therefore obtained in 35,332 cases (92.9 percent). Complete first- and second-trimester screening data were available for 33,459 unaffected pregnancies and 87 pregnancies affected by Down’s syndrome. There were 117 cases of Down’s syndrome in the population of 38,167 patients (38,033 enrolled patients plus 134 patients whose fetuses had cystic hygromas). Of the 117 cases of Down’s syndrome, 25 were in the cystic-hygroma subgroup and 92 occurred among the 38,033 pregnancies described in this report Ultrasonography for the measurement of nuchal translucency can be a difficult technique to perform consistently well, as evidenced by the 7 percent rate of failed or suboptimal imaging in our study. A recent U.S. study suggested a rate of failure to obtain an image of only 0.5 percent, but no data were provided on image quality. 5 However, the detection rate of Down’s syndrome by measurement of nuchal translucency appeared lower than in the present study (79 percent, at a 5 percent false positive rate). This suggests that quality assurance, as performed by us, may contribute to improved screening performance.
 NT ölçüm başarısızlığı %7.1. Bu çalışmaya gör haftalarda NT ölçümü olguların %7.1’inde başarılamayacak kadar zor bir incelemedir. Bazı çalışmalarda ölçüm yapılamama sıklığı %0.5 olarak verilse de, ölçüm kalitesi yönünden değerlendirildiğinde, başarısızlık muhtemelen %7 olmalıdır. Table 1. Data on pregnancy and pediatric outcomes. were obtained in 36,837 cases (97 percent). One. hundred two approved ultrasonographers performed. all nuchal-translucency evaluations. The ultrasonographer. failed to obtain an adequate nuchaltranslucency. image in 1727 cases (4.5 percent), and in a further 974 cases (2.6 percent) the images. were rejected at central review. Adequate nuchaltranslucency. measurements were therefore obtained. in 35,332 cases (92.9 percent). Complete. first- and second-trimester screening data were. available for 33,459 unaffected pregnancies and 87. pregnancies affected by Down’s syndrome. There. were 117 cases of Down’s syndrome in the population. of 38,167 patients (38,033 enrolled patients. plus 134 patients whose fetuses had cystic hygromas). Of the 117 cases of Down’s syndrome, 25. were in the cystic-hygroma subgroup and 92 occurred. among the 38,033 pregnancies described in. this report. Ultrasonography for the measurement of nuchal. translucency can be a difficult technique to perform. consistently well, as evidenced by the 7 percent rate. of failed or suboptimal imaging in our study. A recent. U.S. study suggested a rate of failure to obtain. an image of only 0.5 percent, but no data were provided. on image quality. 5. However, the detection rate. of Down’s syndrome by measurement of nuchal. translucency appeared lower than in the present. study (79 percent, at a 5 percent false positive rate). This suggests that quality assurance, as performed. by us, may contribute to improved screening performance.")
27
FASTER %5 yalancı pozitiflik ile saptama oranı Kombine %85 Üçlü %69
Dörtlü test %81 Serum entegre %86 Tam entegre %95 Tam entegre %1 yalancı pozitiflik ile %87 saptama Buradaki tabloda çeşitli yalancı pozitiflik oranlarındaki saptama oranları görülmekte. FASTER çalışmasına göre Down sendromu saptanmasında %5 yalancı pozitiflik ile %94 saptama oranın sahip olan full integre test en etkili test olarak görülmekte. Bu oranlar hesaplanırken septalı kistik higromalar hesaplamaya dahil edilmemişler. Kombine test 11. haftada yapılırsa, 2. trimester dörtlü teste göre daha yüksek saptama oranına sahip olarak görülmektedir. Ancak diğer haftalara kayarsa başarı dörtlü test ile benzerlik göstermektedir. İlk trimester taramanın gücü gebelik haftası ilerledikçe azalıyor All calculations take into account maternal age, according to the 1999 U.S. distribution of maternal age. 14 Cases of septated cystic hygroma are excluded from the analysis. The figures in parentheses are 95 percent confidence intervals surrounding the point estimates of screening performance. Confidence intervals are given at 11 weeks of gestation for the major tests that measure first-trimester markers; the 95 percent confidence intervals at 12 and 13 weeks are similar to those at 11 weeks in proportion to the point estimates. Confidence intervals are given for all tests that measure only second-trimester markers. † The serum-only test consists of measurement of pregnancy-associated plasma protein A (PAPP-A) and the free beta subunit of human chorionic gonadotropin (f b hCG). ‡ The combined test in the first trimester consists of measurement of nuchal translucency, PAPP-A, and f hCG. § The serum integrated test consists of measurement of PAPP-A in the first trimester and quadruple markers (alpha-fetoprotein, hCG, unconjugated estriol, and inhibin A) in the second trimester. ¶ The fully integrated test consists of measurement of nuchal translucency and PAPP-A in the first trimester and quadruple markers (alpha-fetoprotein, hCG, unconjugated estriol, and inhibin A) in the second trimester. The triple test in the second trimester consists of measurement of alpha-fetoprotein, hCG, and unconjugated estriol. ¿ The quadruple test consists of measurement of alpha-fetoprotein, hCG, unconjugated estriol, and inhibin A.
 and the free beta subunit of human chorionic gonadotropin (f. b. hCG). ‡ The combined test in the first trimester consists of measurement of nuchal translucency, PAPP-A, and f. hCG. § The serum integrated test consists of measurement of PAPP-A in the first trimester and quadruple markers (alpha-fetoprotein, hCG, unconjugated estriol, and inhibin A) in the second. trimester. ¶ The fully integrated test consists of measurement of nuchal translucency and PAPP-A in the first trimester and quadruple markers (alpha-fetoprotein, hCG, unconjugated estriol, and inhibin. A) in the second trimester. The triple test in the second trimester consists of measurement of alpha-fetoprotein, hCG, and unconjugated estriol. ¿ The quadruple test consists of measurement of alpha-fetoprotein, hCG, unconjugated estriol, and inhibin A.")
28
FASTER Bağımsız ardışık
Faster çalışması, Down sendromunun saptanmasında kullanılan testlerin gücünü gösteren önemli bir çalışmadır. Bu çalışmada olguya hem ilk trimester hemde ikinci trimester tarama testleri uygulanmıştır. Toplam 117 Down sendromlu olgunun saptandığı bu çalışmada testlerin ayrı ayrı Down sendromunu saptama güçleri aşağıdaki tabloda gösterildiği gibidir. Bu çalışmada ilk trimesterde elde olunan sonuçlar hasta ile paylaşılmamış. İkinci trimesterde test yapılması beklenmiştir. Surus ve faster çalışmalarının BUN çalışmasından en önemli farkları bu. background It is uncertain how best to screen pregnant women for the presence of fetal Down’s syndrome: to perform first-trimester screening, to perform second-trimester screening, or to use strategies incorporating measurements in both trimesters. methods Women with singleton pregnancies underwent first-trimester combined screening (measurement of nuchal translucency, pregnancy-associated plasma protein A [PAPP-A], and the free beta subunit of human chorionic gonadotropin at 10 weeks 3 days through 13 weeks 6 days of gestation) and second-trimester quadruple screening (measurement of alpha-fetoprotein, total human chorionic gonadotropin, unconjugated estriol, and inhibin A at 15 through 18 weeks of gestation). We compared the results of stepwise sequential screening (risk results provided after each test), fully integrated screening (single risk result provided), and serum integrated screening (identical to fully integrated screening, but without nuchal translucency). results First-trimester screening was performed in 38,167 patients; 117 had a fetus with Down’s syndrome. At a 5 percent false positive rate, the rates of detection of Down’s syndrome were as follows: with first-trimester combined screening, 87 percent, 85 percent, and 82 percent for measurements performed at 11, 12, and 13 weeks, respectively; with second-trimester quadruple screening, 81 percent; with stepwise sequential screening, 95 percent; with serum integrated screening, 88 percent; and with fully integrated screening with first-trimester measurements performed at 11 weeks, 96 percent. Paired comparisons found significant differences between the tests, except for the comparison between serum integrated screening and combined screening. conclusions First-trimester combined screening at 11 weeks of gestation is better than secondtrimester quadruple screening but at 13 weeks has results similar to second-trimester quadruple screening. Both stepwise sequential screening and fully integrated screening have high rates of detection of Down’s syndrome, with low false positive rates. Bağımsız ardışık
 and second-trimester quadruple screening (measurement. of alpha-fetoprotein, total human chorionic gonadotropin, unconjugated estriol, and inhibin A at 15 through 18 weeks of gestation). We compared the results of stepwise. sequential screening (risk results provided after each test), fully integrated screening. (single risk result provided), and serum integrated screening (identical to fully integrated. screening, but without nuchal translucency). results. First-trimester screening was performed in 38,167 patients; 117 had a fetus with Down’s. syndrome. At a 5 percent false positive rate, the rates of detection of Down’s syndrome. were as follows: with first-trimester combined screening, 87 percent, 85 percent, and. 82 percent for measurements performed at 11, 12, and 13 weeks, respectively; with. second-trimester quadruple screening, 81 percent; with stepwise sequential screening, 95 percent; with serum integrated screening, 88 percent; and with fully integrated. screening with first-trimester measurements performed at 11 weeks, 96 percent. Paired comparisons found significant differences between the tests, except for the. comparison between serum integrated screening and combined screening. conclusions. First-trimester combined screening at 11 weeks of gestation is better than secondtrimester. quadruple screening but at 13 weeks has results similar to second-trimester. quadruple screening. Both stepwise sequential screening and fully integrated screening. have high rates of detection of Down’s syndrome, with low false positive rates. Bağımsız ardışık.")
29
SURUSS (1995-2001),47507 olgu Serum Urine and Ultrasound Screening Study
İngiltere’de 24 Avustralya’da 1 merkez SURUSS çalışmasına 47,507 olgu alındı. Bu çalışma birinci ve ikinci trimesterde Down sendromu taramasının etkinliğini saptamak amacıyla günümüze kadar yapılmış olan en büyük çalışmadır. Çalışma yılları arasında İngiltere’de 24 Avustralya’da 1 olmak üzere toplam 25 merkezde yapılmıştır. Bu çalışmada olgularda hem 1. trimesterde hem de ikinci trimesterde inceleme yapılmıştır. Birinci trimester sonucu ne olursa olsun girişim yapılmamış ve ikinci trimester sonuçlarının alınması beklenmiştir.

30
Burada bir bilgisayar modeli kullanılmış
Burada bir bilgisayar modeli kullanılmış. SURUSS çalışmasının verileri kullanılarak etkilenen ve etkilenmeyen gebenin verileri varsayılmış. Değişik hesapra yapılarak %90 saptama oranında yalancı pozitiflikler verilmiş. İkinci trimesterde test yapılan ardışık testlerin sonuçlarını ilk trimesterdeki eşik değer yakından etkiler. Bu nedenele bu tabloda farklı eişk değer ve saptama oranlarındaki değerler sonrasında yapılan ardışık testlerin sonuçları canlandırılmış. Eğer başlangıçta yapılan kombine testin yalancı pozitiflik oranı düşük tutulursa Örneğin %0.5, overall yalancı pozitiflik oranı full integre teste çok yakın. Bunun tek avantajı down’lı olguların 2/3’ü bu evrede saptanıyor. Ancak olguların %99.5’i integre test için yollanıyor. Yani maliyet sorunu var. Eğer ilk trimesterdeki kombine testin FPR’İ %2’e ayarlanırda Down sendromluların 4/5’i bu evrede yakalanıyor (toplam saptama oranı %90’da sabit olarak düşünüyoruz), ancak yalancı pozitiflik oranı artıyor %2.15’e karşılık % Ardışık testin etkili olabilmesi için başlangıçta seçilen eşik değer, full integre testin aynı saptama oranındaki eşik değerinden (FPR’inden) daha aşağıda olmalıdır. Yani kabaca %2’nin altında olmalıdır. Öbür türlü toplam yalancı pozitifliğin artması ile maliyet ve amniosentez yapılan gebe sayısı belirgin olarak artmaktadır. Burada unutulmaması gereken şey sabit saptama oranı ile ne kadar az amniosentez yaparız. Tabi ki en önemli şeylerden biri de erken saptanan olguların sayısında artma. Birinci trimesterde yapılan tarama testinde düşük eşik değer kullanıldığı zaman (örneğin FPR 0.1, 0.5) olguların nerede ise tamamına yakınına (%99.5) ikinci trimester dörtlü test yapılıyor. Buradaki avantajlı nokta bu kadar düşük eşik değerde bile olguların (örneğin %0.1’de, %51’i) olguların önemli bir bölümü ilk trimesterde yakalanmakta. Bu slide insana şunu düşündürüyor. Her enstütü veya ülke kendisine sabit saptama oranı ile en avantajlı tarama yöntemini seçmeli. Bu slide ile ardışık taramanın sonuçları verilmiş. Bir sonraki slide’da ise contingent tarama sonuçları verilmiş. Objective To compare the Integrated test in three policies for prenatal Down syndrome screening: Integrated screening for all women, sequential screening (first-trimester tests allowing early completion of screening for high-risk pregnancies), and Contingent screening (early completion of screening for high- and low-risk pregnancies). Design and Methods Estimation of detection rates (DRs) and false-positive rates (FPRs) using Monte Carlo simulation and cost effectiveness for each method. Setting and Population Down syndrome affected and unaffected pregnancies studied in the Serum Urine and Ultrasound Screening Study (SURUSS). Results and Main Outcomes Integrated screening has the best screening performance. The performance of the other two policies approached that of Integrated screening as the first-trimester test FPR decreased. If the first-trimester FPR is set to 0.5% (risk ≥1 in 30) with an overall DR of 90%, sequential and contingent screening yield overall FPRs of 2.25% and 2.42%, respectively, and 66% of the affected pregnancies are detected by the first-trimester test. The Integrated test on all women yields an FPR of 2.15%. With sequential screening, 99.5% of women would proceed to an Integrated test, or 30% with contingent screening if those with first-trimester test risks of ≤1 in 2000 are classified screen-negative and receive no further testing. About 20% of affected pregnancies identified in the first trimester using sequential or contingent screening would have unnecessary terminations (they would miscarry before the early second trimester). Contingent screening is the most cost-effective if there is no alphafetoprotein screening for neural tube defects, otherwise Integrated screening is more cost-effective. Conclusions Integrated screening for all women is the simplest, most effective, and the safest policy. Contingent screening is the most complex with the lowest screening performance. Making an earlier diagnosis with sequential and contingent screening has adverse consequences that are sufficient to discourage their use. Copyright 2006 John Wiley & Sons, Ltd.
, ancak yalancı pozitiflik oranı artıyor %2.15’e karşılık % Ardışık testin etkili olabilmesi için başlangıçta seçilen eşik değer, full integre testin aynı saptama oranındaki eşik değerinden (FPR’inden) daha aşağıda olmalıdır. Yani kabaca %2’nin altında olmalıdır. Öbür türlü toplam yalancı pozitifliğin artması ile maliyet ve amniosentez yapılan gebe sayısı belirgin olarak artmaktadır. Burada unutulmaması gereken şey sabit saptama oranı ile ne kadar az amniosentez yaparız. Tabi ki en önemli şeylerden biri de erken saptanan olguların sayısında artma. Birinci trimesterde yapılan tarama testinde düşük eşik değer kullanıldığı zaman (örneğin FPR 0.1, 0.5) olguların nerede ise tamamına yakınına (%99.5) ikinci trimester dörtlü test yapılıyor. Buradaki avantajlı nokta bu kadar düşük eşik değerde bile olguların (örneğin %0.1’de, %51’i) olguların önemli bir bölümü ilk trimesterde yakalanmakta. Bu slide insana şunu düşündürüyor. Her enstütü veya ülke kendisine sabit saptama oranı ile en avantajlı tarama yöntemini seçmeli. Bu slide ile ardışık taramanın sonuçları verilmiş. Bir sonraki slide’da ise contingent tarama sonuçları verilmiş. Objective To compare the Integrated test in three policies for prenatal Down syndrome screening: Integrated. screening for all women, sequential screening (first-trimester tests allowing early completion of screening. for high-risk pregnancies), and Contingent screening (early completion of screening for high- and low-risk. pregnancies). Design and Methods Estimation of detection rates (DRs) and false-positive rates (FPRs) using Monte Carlo. simulation and cost effectiveness for each method. Setting and Population Down syndrome affected and unaffected pregnancies studied in the Serum Urine. and Ultrasound Screening Study (SURUSS). Results and Main Outcomes Integrated screening has the best screening performance. The performance. of the other two policies approached that of Integrated screening as the first-trimester test FPR decreased. If. the first-trimester FPR is set to 0.5% (risk ≥1 in 30) with an overall DR of 90%, sequential and contingent. screening yield overall FPRs of 2.25% and 2.42%, respectively, and 66% of the affected pregnancies are. detected by the first-trimester test. The Integrated test on all women yields an FPR of 2.15%. With sequential. screening, 99.5% of women would proceed to an Integrated test, or 30% with contingent screening if those. with first-trimester test risks of ≤1 in 2000 are classified screen-negative and receive no further testing. About. 20% of affected pregnancies identified in the first trimester using sequential or contingent screening would. have unnecessary terminations (they would miscarry before the early second trimester). Contingent screening. is the most cost-effective if there is no alphafetoprotein screening for neural tube defects, otherwise Integrated. screening is more cost-effective. Conclusions Integrated screening for all women is the simplest, most effective, and the safest policy. Contingent screening is the most complex with the lowest screening performance. Making an earlier diagnosis. with sequential and contingent screening has adverse consequences that are sufficient to discourage their use. Copyright 2006 John Wiley & Sons, Ltd.")
31
Saptama oranı aynı olmakla birlikte contingent taramada yalancı pozitiflik çok az.
Objective To compare the efficacy of combined, stepwise sequential, and contingent screening versus the integrated test in detecting fetal aneuploidies. Study design First trimester combined test, sequential second trimester, and contingent risks were retrospectively calculated for 7292 unselected pregnant women with singleton pregnancies who had received integrated screening. The first trimester testing was based on nuchal translucency, pregnancy-associated plasma protein-A, and free-beta-human chorionic gonadotrophin (free β-hCG) and the second trimester tests were alpha-fetoprotein, hCG, and unconjugated estriol. A second trimester risk of 1 : 250 defined a positive result for all protocols with the contingent protocol based on additional second trimester testing for those with risks between 1 : 30 and 1 : 1200. Results Among the population submitted for the integrated test, the detection rate was 19/21 (90%) for Down syndrome (DS) and 6/6 (100%) for Edwards syndrome (ES) and the DS false-positive rate (FPR) was 247/7271 (3.4%). Provision of the first trimester combined test alone would have resulted in a 17/21 (81%) detection rate for DS, that of 4/6 (67%) for ES and a DS FPR of 292/7271 (4.0%). The sequential and contingent approaches had the same final detection rates as the integrated test but potentially allowed a high proportion of the affected pregnancies to be detected in the first trimester. The lowest net DS FPR was seen with the contingent approach (2.6%) and using this protocol only 12.7% of women would have required second trimester testing. Conclusions Integrated, sequential, and contingent screenings are all more efficacious than the combined test. Overall, the contingent approach was the most efficient with a high-detection rate, the lowest FPR, and the least amount of testing. Copyright 2011 John Wiley & Sons, Ltd. KEY WORDS: maternal serum screening; Down syndrome; prenatal diagnosis; amniocentesis; genetic counselling 1/30-1/1200 Contingent gurupta olguların %12’si dörtlü teste gerek duymuş ve olguların %52’si ilk trimesterde saptanmış 31
 and the second trimester tests were. alpha-fetoprotein, hCG, and unconjugated estriol. A second trimester risk of 1 : 250 defined a positive result. for all protocols with the contingent protocol based on additional second trimester testing for those with risks. between 1 : 30 and 1 : Results Among the population submitted for the integrated test, the detection rate was 19/21 (90%) for Down. syndrome (DS) and 6/6 (100%) for Edwards syndrome (ES) and the DS false-positive rate (FPR) was 247/7271. (3.4%). Provision of the first trimester combined test alone would have resulted in a 17/21 (81%) detection rate. for DS, that of 4/6 (67%) for ES and a DS FPR of 292/7271 (4.0%). The sequential and contingent approaches. had the same final detection rates as the integrated test but potentially allowed a high proportion of the affected. pregnancies to be detected in the first trimester. The lowest net DS FPR was seen with the contingent approach. (2.6%) and using this protocol only 12.7% of women would have required second trimester testing. Conclusions Integrated, sequential, and contingent screenings are all more efficacious than the combined. test. Overall, the contingent approach was the most efficient with a high-detection rate, the lowest FPR, and. the least amount of testing. Copyright 2011 John Wiley & Sons, Ltd. KEY WORDS: maternal serum screening; Down syndrome; prenatal diagnosis; amniocentesis; genetic counselling. 1/30-1/1200. Contingent gurupta olguların %12’si dörtlü teste gerek duymuş ve olguların %52’si ilk trimesterde saptanmış. 31.")
32
Biyokimya farklı zamanda (iki basamaklı)
")
33
Trizomi 21’li gebeliklerde:
Serbest β-hCG düzeyi öploid gebeliklerden daha yüksektir ve aradaki farklılık 13. haftada, 11. haftadan daha fazladır Serum PAPP-A düzeyi, öploid gebeliklerden daha düşüktür ve ikisi arasındaki farklılık 11. haftada, 13. haftadan daha fazladır 11. haftadaki PAPP-A’nın normal gebeliklerden farklılığı, 13. haftada serbest β-hCG’nin farklılığından daha fazladır. Böylece, bütün olarak biyokimyasal tarama 11. haftada 13. haftadan daha iyi bir performansa sahiptir Birleşik tarama Trizomi 21’li gebeliklerde, normal gebelikler ile karşılaştırıldığında: Biyokimyasal değerlerdeki farklılık 11. haftada, 13. haftadan daha fazladır Fetal NT’deki farklılık 11. haftada 13. haftadan daha fazladır Bundan dolayı taramanın performansı 11. haftada 13. haftadan daha yüksektir Sigara içen kadınlar ve YÜT gebeliklerde PAPP-A düzeyi düşüktür ve bu da trizomi 21 riskinin artığına dair yanlış bir yorumlamaya ve önemli oranda yüksek yanlış pozitifliğe neden olur

34
%3 yalancı pozitiflikle NT 12. hafta PAPP-A ve beta HCG 12. hafta %86
886 trizomi 21 normal gebe , Çok merkezli çalışma %3 yalancı pozitiflikle NT 12. hafta PAPP-A ve beta HCG 12. hafta %86 PAPP-A ve beta HCG 9. hafta %90 PAPP-a 9, beta HCG 12 hafta %90 ABSTRACT Objective To establish an algorithm for first-trimester combined screening for trisomy 21 with biochemical testing from 7 to 14 weeks’ gestation and ultrasound testing at 11–13 weeks. Methods This was a multicenter study of 886 pregnancies with trisomy 21 and unaffected pregnancies with measurements of free β-human chorionic gonadotropin (β-hCG) and pregnancy-associated plasma protein-A (PAPP-A) at 7–14 weeks’ gestation. Multiple regression modeling of log-transformed marker values was used to produce log multiples of the median (MoM) values for PAPP-A and free β-hCG. The models included terms for the center attended and the machine used for biochemical analysis, gestational age, maternal racial origin, maternal weight, smoking status and method of conception. Bivariate Gaussian distributions were fitted to log MoM PAPP-A and log MoM free β-hCG in trisomy 21 and in unaffected pregnancies. In each case the patient-specific risk for trisomy 21 was estimated by multiplying the individual maternal agerelated risk with the likelihood ratio (LR) for fetal nuchal translucency (NT) according to the mixture model and the combined LR for maternal serum free β-hCG and PAPP-A. Estimates of detection rates for trisomy 21 and false-positive rates were calculated for combined screening with measurements of NT at 12 weeks together with measurements of free β-hCG and PAPP-A from 8 to 13 weeks. Results In trisomy 21 pregnancies the mean log MoM free β-hCG increased linearly with gestation between 7 and 14 weeks, whereas the relation between log MoM PAPP-A and gestation was fitted by a quadratic equation such that the maximum separation between trisomy 21 and unaffected pregnancies occurs at 9–10 weeks. At a false-positive rate of 3% the detection rate of combined screening at 12 weeks was 86% and this increased to 90% by biochemical testing at 9 weeks and ultrasound scanning at 12 weeks. The detection rate increased to 92% by measuring PAPP-A at 9 weeks and free β-hCG at the time of the scan at 12 weeks. Conclusion The performance of first-trimester biochemical screening for trisomy 21 is best at 9–10 weeks rather than at 7–8 or 11–14 weeks. Copyright 2010 ISUOG. Published by John Wiley & Sons, Ltd. 34
 and pregnancy-associated plasma protein-A. (PAPP-A) at 7–14 weeks’ gestation. Multiple regression. modeling of log-transformed marker values was used. to produce log multiples of the median (MoM) values. for PAPP-A and free β-hCG. The models included. terms for the center attended and the machine used. for biochemical analysis, gestational age, maternal. racial origin, maternal weight, smoking status and. method of conception. Bivariate Gaussian distributions. were fitted to log MoM PAPP-A and log MoM free. β-hCG in trisomy 21 and in unaffected pregnancies. In. each case the patient-specific risk for trisomy 21 was. estimated by multiplying the individual maternal agerelated. risk with the likelihood ratio (LR) for fetal nuchal. translucency (NT) according to the mixture model and. the combined LR for maternal serum free β-hCG and. PAPP-A. Estimates of detection rates for trisomy 21 and. false-positive rates were calculated for combined screening. with measurements of NT at 12 weeks together with. measurements of free β-hCG and PAPP-A from 8 to. 13 weeks. Results In trisomy 21 pregnancies the mean log MoM. free β-hCG increased linearly with gestation between 7. and 14 weeks, whereas the relation between log MoM. PAPP-A and gestation was fitted by a quadratic equation. such that the maximum separation between trisomy 21. and unaffected pregnancies occurs at 9–10 weeks. At a. false-positive rate of 3% the detection rate of combined. screening at 12 weeks was 86% and this increased to. 90% by biochemical testing at 9 weeks and ultrasound. scanning at 12 weeks. The detection rate increased to. 92% by measuring PAPP-A at 9 weeks and free β-hCG. at the time of the scan at 12 weeks. Conclusion The performance of first-trimester biochemical. screening for trisomy 21 is best at 9–10 weeks rather. than at 7–8 or 11–14 weeks. Copyright 2010 ISUOG. Published by John Wiley & Sons, Ltd. 34.")
35
En iyi sonuç PAPP-A’nın erken bakılması ile alınıyor
En iyi sonuç PAPP-A’nın erken bakılması ile alınıyor. Hem erken hem geç bakılması (biyokimyanın) sonuçları olumlu etkileyebilir diye yorum yapılmış. Data are given as % (95% CI). Protocol 1, pregnancy-associated plasma protein-A (PAPP-A) (late sample) + β-human chorionic gonadotropin (β-hCG) (late sample); Protocol 2, PAPP-A (early sample) + β-hCG (early sample); Protocol 3, PAPP-A (early sample) + β-hCG (late sample); Protocol 4, PAPP-A (early and late samples) + β-hCG (early and late samples). ABSTRACT Objective To prospectively evaluate the performance of first-trimester combined screening for trisomy 21 using the biochemical markers pregnancy-associated plasma protein-A (PAPP-A) and free beta-human chorionic gonadotropin (free β-hCG) obtained before and at the time of the nuchal translucency (NT) scan. Methods Three fetal medicine departments in Denmark participated in the study. Screening for trisomy 21 was set up as a two-step approach with blood sampling performed before the NT scan (early sample) and again at the time of the NT scan (late sample). PAPP-A and free β- hCG were measured on both the early and late samples. Age-standardized detection and false-positive rates for different screening protocols were calculated. Results Wecollected two blood samples in 27 pregnancies affected by trisomy 21 and in 3891 control pregnancies. The early samples were taken between gestational ages 8+0 and 13+6 weeks, and the late samples between 11+3 and 14+6 weeks. The median interval between the samples was 17 (range, 1–40) days. We found a significantly better estimated screening performance when using early sampling vs late sampling (P<0.05). With a risk cut-off of 1 in 100, at the time of the risk assessment the estimated detection and false-positive rates when using the early sample were 91% (95% CI, 81–98%) and 1.6% (95% CI, 1.3–2.0%), respectively. For fixed false-positive rates the highest detection rates were achieved using both blood samples. When comparing early sampling vs double sampling there was no significant difference in screening performance. Conclusion In combined first-trimester screening for trisomy 21, use of early sampling with measurement of PAPP-A and free β-hCG before the time of the NT scan can optimize screening performance. Using maternal serum markers obtained both before and at the time of the NT scan has the potential to further improve performance, but larger studies are needed to confirm this potential. Copyright 2012 ISUOG. Published by John Wiley & Sons, Ltd. G,G E,E E,G EG,EG 35
 sonuçları olumlu etkileyebilir diye yorum yapılmış. Data are given as % (95% CI). Protocol 1, pregnancy-associated. plasma protein-A (PAPP-A) (late sample) + β-human chorionic. gonadotropin (β-hCG) (late sample); Protocol 2, PAPP-A (early. sample) + β-hCG (early sample); Protocol 3, PAPP-A (early sample) + β-hCG (late sample); Protocol 4, PAPP-A (early and late samples) + β-hCG (early and late samples). ABSTRACT. Objective To prospectively evaluate the performance of. first-trimester combined screening for trisomy 21 using. the biochemical markers pregnancy-associated plasma. protein-A (PAPP-A) and free beta-human chorionic. gonadotropin (free β-hCG) obtained before and at the. time of the nuchal translucency (NT) scan. Methods Three fetal medicine departments in Denmark. participated in the study. Screening for trisomy 21 was set. up as a two-step approach with blood sampling performed. before the NT scan (early sample) and again at the. time of the NT scan (late sample). PAPP-A and free β- hCG were measured on both the early and late samples. Age-standardized detection and false-positive rates for. different screening protocols were calculated. Results Wecollected two blood samples in 27 pregnancies. affected by trisomy 21 and in 3891 control pregnancies. The early samples were taken between gestational ages. 8+0 and 13+6 weeks, and the late samples between and 14+6 weeks. The median interval between. the samples was 17 (range, 1–40) days. We found a. significantly better estimated screening performance when. using early sampling vs late sampling (P<0.05). With a. risk cut-off of 1 in 100, at the time of the risk assessment. the estimated detection and false-positive rates when using. the early sample were 91% (95% CI, 81–98%) and 1.6% (95% CI, 1.3–2.0%), respectively. For fixed false-positive. rates the highest detection rates were achieved using both. blood samples. When comparing early sampling vs double. sampling there was no significant difference in screening. performance. Conclusion In combined first-trimester screening for. trisomy 21, use of early sampling with measurement of. PAPP-A and free β-hCG before the time of the NT. scan can optimize screening performance. Using maternal. serum markers obtained both before and at the time. of the NT scan has the potential to further improve. performance, but larger studies are needed to confirm this. potential. Copyright 2012 ISUOG. Published by John. Wiley & Sons, Ltd. G,G. E,E. E,G. EG,EG. 35.")
36
Nazal kemik Burun kemiği
Fetal burun kemiğinin incelenmesinde gebelik haftada ve BPM’si mm arasında olmalıdır Görüntü fetal baş ve gögüs kafesi tüm ekranı kaplayacak şekilde büyütülmelidir Fetal profilin mid-sagital kesiti elde edilmelidir Ultrason probu burun yönüne paralel olmalı ve prob nazikçe burnun bir yanından diğer yanına eğilmelidir Bu kriterler tatmin edici bir şekilde elde edildiyse burun seviyesinde üç ayrı hat görülür: Üst hat cildi gösterir Alt hat ki üstteki ciltten daha kalın ve daha ekojeniktir, burun kemiğini gösterir Kemiğin önünde ve daha yüksek seviyedeki üçüncü hat ise burun ucunu gösterir Burun kemiği üstteki ciltten daha ekojenik ise mevcut olarak, değerlendirilir. Eğer görülemiyor veya ekojenitesi cilt ile aynı yada daha azsa yok olarak değerlendirilir

37
37 Nazal kemik yokluğu riski 23 kat artırıyor ABSTRACT
Objective To investigate the performance of firsttrimester screening for aneuploidies by including assessment of the fetal nasal bone in the combined test of maternal age, fetal nuchal translucency (NT) thickness, fetal heart rate (FHR) and serum free β-human chorionic gonadotropin (β-hCG) and pregnancy-associated plasma protein-A (PAPP-A). Methods Screening by the combined test was performed in singleton pregnancies, including with euploid fetuses, 122 with trisomy 21, 36 with trisomy 18, 20 with trisomy 13 and eight with Turner syndrome. In all cases the fetal nasal bone was assessed and classified as present or absent. We examined the performance of two screening strategies: firstly, assessment of the nasal bone in all patients and secondly, first-stage screening using the combined test in all patients followed by secondstage assessment of the nasal bone only in those with an intermediate risk of 1 in 51 to 1 in 1000 after the first stage. To validate the new risk algorithm we used a second independent dataset of fetuses, including 139 with trisomy 21. Results The nasal bone was absent in 2.6% of the euploid fetuses, 59.8% with trisomy 21, 52.8% with trisomy 18, 45.0% with trisomy 13 and in none of the fetuses with Turner syndrome. Respective figures for an absent nasal bone in the validation population, which contained fewer Black women, were 0.6%, 62.6%, 55.3%, 35.3% and 41.7%. In a screening policy based on maternal age, fetal NT, FHR, serum free β-hCG and PAPP-A, for a fixed risk cut-off of 1 : 100, the false-positive rate was 3.0%. The standardized detection rates were 91% for trisomy 21 and 100% for trisomy 18, trisomy 13 and Turner syndrome, respectively. Assessment of the nasal bone in all pregnancies reduced the false-positive rate to 2.5% without changing the detection rate. A detection rate of 93% was achieved with the two-stage strategy at a falsepositive rate of 2.4% in which it was necessary to assess the nasal bone in only 15% of the total population. In the validation dataset, screening by the combined test and using a risk cut-off of 1 : 100 detected 90% of the cases with trisomy 21 for a false-positive rate of 4%. Inclusion of the nasal bone increased the detection rate to 92% for a false-positive rate of 2.9%. Contingent screening detected 92% of cases for a false-positive rate of 2.9%. Conclusions Assessment of the fetal nasal bone improves the performance of first-trimester screening for trisomy 21. Copyright 2009 37
 thickness, fetal heart rate (FHR) and serum free β-human chorionic. gonadotropin (β-hCG) and pregnancy-associated plasma. protein-A (PAPP-A). Methods Screening by the combined test was performed. in singleton pregnancies, including with euploid. fetuses, 122 with trisomy 21, 36 with trisomy 18, 20. with trisomy 13 and eight with Turner syndrome. In all. cases the fetal nasal bone was assessed and classified as. present or absent. We examined the performance of two. screening strategies: firstly, assessment of the nasal bone. in all patients and secondly, first-stage screening using. the combined test in all patients followed by secondstage. assessment of the nasal bone only in those with. an intermediate risk of 1 in 51 to 1 in 1000 after the. first stage. To validate the new risk algorithm we used a. second independent dataset of fetuses, including. 139 with trisomy 21. Results The nasal bone was absent in 2.6% of the euploid. fetuses, 59.8% with trisomy 21, 52.8% with trisomy 18, 45.0% with trisomy 13 and in none of the fetuses with. Turner syndrome. Respective figures for an absent nasal. bone in the validation population, which contained fewer. Black women, were 0.6%, 62.6%, 55.3%, 35.3% and. 41.7%. In a screening policy based on maternal age, fetal. NT, FHR, serum free β-hCG and PAPP-A, for a fixed. risk cut-off of 1 : 100, the false-positive rate was 3.0%. The standardized detection rates were 91% for trisomy. 21 and 100% for trisomy 18, trisomy 13 and Turner. syndrome, respectively. Assessment of the nasal bone in. all pregnancies reduced the false-positive rate to 2.5% without changing the detection rate. A detection rate of. 93% was achieved with the two-stage strategy at a falsepositive. rate of 2.4% in which it was necessary to assess. the nasal bone in only 15% of the total population. In. the validation dataset, screening by the combined test and. using a risk cut-off of 1 : 100 detected 90% of the cases. with trisomy 21 for a false-positive rate of 4%. Inclusion. of the nasal bone increased the detection rate to 92% for a. false-positive rate of 2.9%. Contingent screening detected. 92% of cases for a false-positive rate of 2.9%. Conclusions Assessment of the fetal nasal bone improves. the performance of first-trimester screening for trisomy. 21. Copyright ")
38
Burada öncelikle contingent yaklaşımdan, ilk trimesterde saptanan Down sendromu olgularının oranından ve ne kadar olguya nazal kemik bakma gereksinimi bulunduğundan söz etmek gerekir.

39
Duktus venozus Pozitif veya yok (normal) Tersine dönmüş (anormal)
Hepatik ven kontaminasyonu Duktus venozusdaki kan akımı karakteristik dalga formuna sahiptir: Yüksek velositeye sahip ventriküler sistol (S-dalgası) ve diyastol (D-dalgası) Atriyal kasılma (a-dalgası) sırasında ileri akım Duktus venozustaki kan akımının kalitatif değerlendirilmesi a-dalgasının görünümü temel alınarak yapılır: Pozitif veya yok (normal) Tersine dönmüş (anormal) Dalga formu komşu venlerle kontamine olabilir eğer pulse Doppler örneklemesi : Geniş (1.0 mm daha fazla) ise Tam olarak duktus venozusun üzerine yerleştirilmemiş ise Tersine a-dalgası 11-13 haftalarda tersine a-dalgası fetüslerin yaklaşık %4’ünde bulunur Ters a-dalgası su durumlarda artış gösterir: Gebelik 13. haftadan ise 11. hafta ise Fetal nukal translusensi artmış ise Anne serum PAPP-A düzeyi düşük ise Anne siyah ırktansa Tersine a-dalgası şunlar için artmış riskle ilişkilidir: Kromozomal anomaliler Kardiyak defektler Fetal ölüm Tersine a-dalgası su patolojilerle iliskilidir: kromosomal anomaliler kardiak defektler fetal ölüm Ancak ters a-dalgasınin pozitif oldugu vakaların % 80 ‘i normal gebeliklerdir Umbilikal ven kontaminasyonu
 ve diyastol (D-dalgası) Atriyal kasılma (a-dalgası) sırasında ileri akım. Duktus venozustaki kan akımının kalitatif değerlendirilmesi a-dalgasının görünümü temel alınarak yapılır: Pozitif veya yok (normal) Tersine dönmüş (anormal) Dalga formu komşu venlerle kontamine olabilir eğer pulse Doppler örneklemesi : Geniş (1.0 mm daha fazla) ise. Tam olarak duktus venozusun üzerine yerleştirilmemiş ise. Tersine a-dalgası haftalarda tersine a-dalgası fetüslerin yaklaşık %4’ünde bulunur. Ters a-dalgası su durumlarda artış gösterir: Gebelik 13. haftadan ise 11. hafta ise. Fetal nukal translusensi artmış ise. Anne serum PAPP-A düzeyi düşük ise. Anne siyah ırktansa. Tersine a-dalgası şunlar için artmış riskle ilişkilidir: Kromozomal anomaliler. Kardiyak defektler. Fetal ölüm. Tersine a-dalgası su patolojilerle iliskilidir: kromosomal anomaliler. kardiak defektler. fetal ölüm. Ancak ters a-dalgasınin pozitif oldugu vakaların % 80 ‘i normal gebeliklerdir. Umbilikal ven kontaminasyonu.")
40
Ters A dalgası Euploid %3 Trizomi 21 %65 Trisomi 18 %55 Trisomi 13 %55
Duktus venozus akımı Tersine a-dalgası 11-13 haftada ters a-dalgası yaklaşık şu oranlarda bulunur: Euploid fetuslerde 3% trizomi 21li fetüslerde 65% trisomi 18li fetüslerde 55% trisomi 13lü fetüslerde 55%

41
Olguların %15’ine gerekiyor
Duktusta reverse akım ODDS ratio 22, taramaya eklenince %3 yalancı pozitiflik ile Down’lıların %96’sı saptanıyır. Ancak contingent ilede %96 saptanıyor. Üstelik yalancı pozitiflik %2.6 ve olguların sadece %15’ine duktus venozus bakılması gerekiyor. Anormal duktus venozus konjenital kalp hastalıklarını %11 sensitivite, %5.5 PPV ile gösteriyor. Contingent ile herkese bakmanın başarı oranı benzer. ABSTRACT Objectives To investigate the performance of firsttrimester screening for aneuploidies by including assessment of ductus venosus flow in the combined test ofmaternal age, fetal nuchal translucency thickness, fetal heart rate, and serum free β-human chorionic gonadotropin and pregnancy-associated plasma protein-A. Methods Screening by the combined test was performed in singleton pregnancies, including with euploid fetuses, 122 with trisomy 21, 36 with trisomy 18, 20 with trisomy 13 and eight with Turner syndrome. In all cases the a-wave in the fetal ductus venosus flow was assessed. We examined the performance of two screening strategies: first, assessment of the a-wave in all patients and, second, first-stage screening using the combined test in all patients followed by second-stage assessment of the a-wave only in those with an intermediate risk of one in 51 to one in 1000 after the first stage Results Reversed a-wave was observed in 3.2% of the euploid fetuses, and in 66.4%, 58.3%, 55.0% and 75.0% of fetuses with trisomies 21, 18 and 13 and Turner syndrome, respectively. Inclusion of ductus venosus flow in all pregnancies would detect 96%, 92%, 100% and 100% of trisomies 21, 18 and 13 and Turner syndrome, respectively, at a false-positive rate of 3%. The same detection rates were achieved with the two-stage strategy at a false-positive rate of 2.6%, in which it was necessary to assess the ductus venosus in only 15% of the total population. Conclusions Assessment of ductus venosu Olguların %15’ine gerekiyor 41

42
Triküspid Triküspit akımı
Triküspit akımın değerlendirilmesinde gebelik haftalarda ve BPM’si mm arasında olmalıdır Fetus hareketsiz olmalıdır Görüntü fetal toraks tüm ekranı kaplayacak şekilde büyütülmelidir Fetal kalbin apikal dört-odacık görüntüsü elde edilmelidir Renkli akım haritalaması (colour flow mapping) kullanılmamalıdır çünkü birinci trimesterde triküspit regürjitasyonu değerlendirilmesinde güvenilir değildir Pulse Doppler örneklemesi geniş olmalı ( mm) ve triküspit kapağı çaprazlayacak şekilde yerleştirilmelidir Insonasyon açısı ventriküler septum yönünden, akım yönüne doğru, 30 dereceden daha küçük olmalıdır Triküspit kapağın üç parçasından biri ya da birkaçında yetersizlik olabilir. Bu nedenle tüm kapağı değerlendirebilmek için örnekleme volümü kapak boyunca en az üç kez yerleştirilmelidir Sistol sırasında regürjitasyonsuz normal profil Hız 60 cm/s'den fazla olduğunda yaklaşık sistolün yarısında regürjitasyon
 kullanılmamalıdır çünkü birinci trimesterde triküspit regürjitasyonu değerlendirilmesinde güvenilir değildir. Pulse Doppler örneklemesi geniş olmalı ( mm) ve triküspit kapağı çaprazlayacak şekilde yerleştirilmelidir. Insonasyon açısı ventriküler septum yönünden, akım yönüne doğru, 30 dereceden daha küçük olmalıdır. Triküspit kapağın üç parçasından biri ya da birkaçında yetersizlik olabilir. Bu nedenle tüm kapağı değerlendirebilmek için örnekleme volümü kapak boyunca en az üç kez yerleştirilmelidir. Sistol sırasında regürjitasyonsuz normal profil. Hız 60 cm/s den fazla olduğunda yaklaşık sistolün yarısında regürjitasyon.")
43
Triküspid regurjitasyon
Euploid %1 Trizomi 21 %55 Trizomi 18 %30 Trizomi 13 %30 Triküspit akımı Triküspit regürjitasyonu 11-13 haftalarda triküspit regürjitasyonu yaklaşık aşağıdakiler gibi bulunur: Öploid fetüslerde %1 Trizomi 21'li fetüslerde %55 Trizomi 18'li fetüslerde %30 Trizomi 13'lü fetüslerde %30 Triküspit regurjitasyonu su durumlarda daha sıklıkla görülür eğer: Gebelik 13. haftadan ise 11. haftada ise Fetal nukal translusensi artmış ise

44
Olguların %15’ine gerekiyor
TR bulunması riski 62 kat artırıyor. Triküspid FPR, detection %3, 91’i, %3, 96 ya çıkarıyor. Aynı oran (%2.4, 96) contingent ile elde ediliyor ve olguların sadece %15’ine triküspid bakılıyor. For comparison, the last row gives the FPRs and detection rates of contingent screening whereby the tricuspid flow is assessed only in the subgroup with an intermediate risk. All percentages are standardized to the maternal age distribution of pregnancies in England and Wales in 2000–20028. ABSTRACT Objective To investigate the performance of firsttrimester screening for aneuploidies by including assessment of tricuspid blood flow in the combined test of maternal age, fetal nuchal translucency (NT) thickness, fetal heart rate (FHR) and serum free β-human chorionic gonadotropin (β-hCG) and pregnancy-associated plasma protein A (PAPP-A). Method Screening by the combined test was performed in singleton pregnancies, including with chromosomally normal fetuses or the delivery of a phenotypically normal baby (euploid group), 122 with trisomy 21, 36 with trisomy 18, 20 with trisomy 13 and eight with Turner syndrome. In all cases tricuspid flow was assessed to determine if there was tricuspid regurgitation. We examined the performance of two screening strategies: firstly, assessment of tricuspid flow in all patients and secondly, first-stage screening using the combined test in all patients followed by second-stage assessment of tricuspid flow only in those with an intermediate risk of 1 in 51 to 1 in 1000 after the first stage. Results Tricuspid regurgitation was observed in 0.9% of the euploid fetuses and 55.7%, 33.3% and 30% of the fetuses with trisomies 21, 18 and 13, respectively, and in 37.5% of those with Turner syndrome. In a screening policy based on maternal age, fetal NT, FHR, serum free β-hCG and PAPP-A, for a fixed false positive rate of 3% the standardized detection rates were 91% for trisomy 21 and 100% for trisomy 18, trisomy 13 and Turner syndrome. Assessment of tricuspid flow in all pregnancies would increase the detection rate of trisomy 21 to 96%, and the detection rates of trisomy 18, trisomy 13 and Turner syndrome would be 92%, 100% and 100%, respectively. The same detection rates were achieved with the two-stage strategy – inwhich it was necessary to assess tricuspid flow in only 15% of the total population – at a false positive rate of 2.4%. Conclusions Assessment of tricuspid flow improves the performance of first-trimester screening for trisomy 21. Copyright 2008 ISUOG. Published by John Wiley & Sons, Ltd. Olguların %15’ine gerekiyor 44
 contingent ile elde ediliyor ve olguların sadece %15’ine triküspid bakılıyor. For comparison, the last row gives the FPRs and detection rates of contingent screening whereby the tricuspid flow is assessed only in the. subgroup with an intermediate risk. All percentages are standardized to the maternal age distribution of pregnancies in England and Wales. in 2000– ABSTRACT. Objective To investigate the performance of firsttrimester. screening for aneuploidies by including assessment. of tricuspid blood flow in the combined test of. maternal age, fetal nuchal translucency (NT) thickness, fetal heart rate (FHR) and serum free β-human chorionic. gonadotropin (β-hCG) and pregnancy-associated plasma. protein A (PAPP-A). Method Screening by the combined test was performed. in singleton pregnancies, including with chromosomally. normal fetuses or the delivery of a phenotypically. normal baby (euploid group), 122 with trisomy 21, 36. with trisomy 18, 20 with trisomy 13 and eight with. Turner syndrome. In all cases tricuspid flow was assessed. to determine if there was tricuspid regurgitation. We. examined the performance of two screening strategies: firstly, assessment of tricuspid flow in all patients and secondly, first-stage screening using the combined test in all. patients followed by second-stage assessment of tricuspid. flow only in those with an intermediate risk of 1 in 51 to. 1 in 1000 after the first stage. Results Tricuspid regurgitation was observed in 0.9% of. the euploid fetuses and 55.7%, 33.3% and 30% of the. fetuses with trisomies 21, 18 and 13, respectively, and. in 37.5% of those with Turner syndrome. In a screening. policy based on maternal age, fetal NT, FHR, serum free. β-hCG and PAPP-A, for a fixed false positive rate of 3% the standardized detection rates were 91% for trisomy. 21 and 100% for trisomy 18, trisomy 13 and Turner. syndrome. Assessment of tricuspid flow in all pregnancies. would increase the detection rate of trisomy 21 to 96%, and the detection rates of trisomy 18, trisomy 13 and. Turner syndrome would be 92%, 100% and 100%, respectively. The same detection rates were achieved with. the two-stage strategy – inwhich it was necessary to assess. tricuspid flow in only 15% of the total population – at a. false positive rate of 2.4%. Conclusions Assessment of tricuspid flow improves the. performance of first-trimester screening for trisomy 21. Copyright 2008 ISUOG. Published by John Wiley & Sons, Ltd. Olguların %15’ine gerekiyor. 44.")
45
Facial açı Yüz açısı Fetal yüz açısı ölçümünde gebelik haftası ve BPM’si mm arasında olmalıdır Görüntü baş ve üst gögüs kafesi tüm ekranı kaplayacak şekilde büyütülmelidir Fetal profilin mid-sagital kesiti alınmalıdır Yüz açısı şunlar arasından ölçülmelidir: damağın üst yüzeyi boyunca uzanan çizgi ve önde maksilanın üst köşesinden geçen çizgi ile alnın dış yüzeyine uzanan hat. Bu hattı frontal kemik veya cilt altında gebeliğin bu döneminde genellikle açık olan metopic sutur altından uzanan ekojenik çizgi oluşturur

46
Öploid %5 Trizomi 21'li %45 Trizomi 18'li %55 Trizomi 13'lü %45 Down
ABSTRACT Saptama oranını %90’dan %94’e çıkarıyor. Veya %3 yalancı pozitiflik ile %85’den %92’ye çıkarıyor. Contingent ile %3 %91 olguların sadece %12’ine FMA bakılıyor. Objective Trisomy 21 is associated with a flat face, which can now be quantified by measurement of the frontomaxillary facial (FMF) angle. The aim of this study was to examine whether in trisomy 21 fetuses fetal nuchal translucency (NT) thickness and maternal serum free ß-human chorionic gonadotropin (ß-hCG) and pregnancyassociated plasma protein-A (PAPP-A) are independent of the FMF angle, and to estimate the performance of a first-trimester screening test for trisomy 21 that includes measurement of the FMF angle. Methods This was a prospective study in singleton pregnancies at to weeks of gestation in which three-dimensional volumes of the fetal head were obtained and measurement of the FMF angle performed immediately before fetal karyotyping by chorionic villus sampling (CVS). The women chose to have CVS after risk assessment by a combination of maternal age, fetal NT thickness and maternal serum free ß-hCG and PAPP-A. Regression analysis was used to examine the significance of the association within the euploid and within the trisomy 21 fetuses between the deviation from the normal median in FMF angle and the deviation in NT, free ßhCG and PAPP-A. We estimated the detection rate (DR) and false positive rate (FPR) of first-trimester screening for trisomy 21 by measuring the FMF angle in all cases and of an alternative policy in which first-stage screening is by fetal NT and maternal serum biochemistry in all patients, followed by second-stage assessment of FMF angle only in those with an intermediate risk (1 in 51 to 1 in 1000) after the first stage. Results The FMF angle was measured in 782 euploid and 108 trisomy 21 fetuses. In the euploid fetuses the mean FMF angle decreased linearly with CRL from 83.5◦ at a crown–rump length (CRL) of 45 mm to 76.4◦ at a CRL of 84 mm. In the euploid fetuses the mean delta FMF angle was 0.0 (SD, 4.264)◦ and the respective values in the trisomy 21 fetuses were (SD, 4.092)◦. Incorporating the FMF angle in first-trimester combined screening increased the estimated DR from 90 to 94% at an FPR of 5% and from 85 to 92% at an FPR of 3%. In two-stage screening it would be necessary to measure the FMF angle in 12% of cases and the DRs would be 93 and 91% at FPRs of 5 and 3%, respectively. Conclusions Measurement of the FMF angle improves the performance of first-trimester screening for trisomy 21. Copyright 2008 ISUOG. Published by John Wiley Down Euploid 46
 angle. The aim of this study was. to examine whether in trisomy 21 fetuses fetal nuchal. translucency (NT) thickness and maternal serum free. ß-human chorionic gonadotropin (ß-hCG) and pregnancyassociated. plasma protein-A (PAPP-A) are independent. of the FMF angle, and to estimate the performance of a. first-trimester screening test for trisomy 21 that includes. measurement of the FMF angle. Methods This was a prospective study in singleton. pregnancies at to weeks of gestation in. which three-dimensional volumes of the fetal head were. obtained and measurement of the FMF angle performed. immediately before fetal karyotyping by chorionic villus. sampling (CVS). The women chose to have CVS after risk. assessment by a combination of maternal age, fetal NT. thickness and maternal serum free ß-hCG and PAPP-A. Regression analysis was used to examine the significance. of the association within the euploid and within the. trisomy 21 fetuses between the deviation from the normal. median in FMF angle and the deviation in NT, free ßhCG. and PAPP-A. We estimated the detection rate (DR) and false positive rate (FPR) of first-trimester screening. for trisomy 21 by measuring the FMF angle in all. cases and of an alternative policy in which first-stage. screening is by fetal NT and maternal serum biochemistry. in all patients, followed by second-stage assessment of. FMF angle only in those with an intermediate risk. (1 in 51 to 1 in 1000) after the first stage. Results The FMF angle was measured in 782 euploid and. 108 trisomy 21 fetuses. In the euploid fetuses the mean. FMF angle decreased linearly with CRL from 83.5◦ at. a crown–rump length (CRL) of 45 mm to 76.4◦ at a. CRL of 84 mm. In the euploid fetuses the mean delta. FMF angle was 0.0 (SD, 4.264)◦ and the respective. values in the trisomy 21 fetuses were (SD, 4.092)◦. Incorporating the FMF angle in first-trimester combined. screening increased the estimated DR from 90 to 94% at. an FPR of 5% and from 85 to 92% at an FPR of 3%. In. two-stage screening it would be necessary to measure the. FMF angle in 12% of cases and the DRs would be 93 and. 91% at FPRs of 5 and 3%, respectively. Conclusions Measurement of the FMF angle improves. the performance of first-trimester screening for trisomy. 21. Copyright 2008 ISUOG. Published by John Wiley. Down. Euploid. 46.")
48
ABSTRACT Baştan sadeve NT ve nazal kemik. Down’ların %73’ünü saptıyor. Olguların sadece %21’ine biyokimya gerekiyor. Total saptama %90, FPR %2.6 Objectives This study was carried out to examine the performance of a contingent policy in first-trimester screening for trisomy 21, in which the estimated risk was first derived by a combination of maternal age, fetal nuchal translucency (NT) thickness, presence/absence of the nasal bone, blood flow in the ductus venosus or flow across the tricuspid valve, and biochemical testing was carried out only in those who were found to have an intermediate risk. We also examined the performance of a policy in which the estimated risk was first derived by a combination of maternal age and biochemical testing, and ultrasound examination was carried out only in those with an intermediate risk. Methods The data for this study were derived from prospective screening for trisomy 21 in singleton pregnancies, using, as markers, a combination of maternal age, fetal NT thickness and maternal-serum free β-human chorionic gonadotropin (β-hCG) and pregnancy- associated plasma protein-A (PAPP-A), in a onestop clinic for first-trimester assessment of risk at to weeks of gestation. Assessment of the fetal nasal bone, ductus venosus flow and tricuspid flow were also routinely performed by appropriately trained sonographers. The performance of different screening policies was examined. Results The study population consisted of pregnancies with a normal karyotype or delivery of a phenotypically normal baby (euploid group) and 122 cases of trisomy 21. The best performance was achieved by a contingent policy in which first-stage screening was based on maternal age, fetal NT thickness and either tricuspid valve or ductus venosus blood flow, followed by biochemical testing only those with an intermediate risk, of 1 in 51 to 1 in 1000 (which constituted about 20% of the total). The performance of contingent screening in which first-stage testing relies on biochemistry was poorer than when first-stage screening was performed by ultrasound examination because, in order to achieve the same detection rate, the false-positive rate was twice as high. Conclusion Effective first-trimester screening for trisomy 21 can be achieved by a contingent policy in which first-stage testing is based on ultrasound examination and second-stage biochemical testing is carried out in only 20% of the patients. Copyright 2010 ISUOG. Published by John Wiley & Sons, Ltd 48
 thickness, presence/absence of. the nasal bone, blood flow in the ductus venosus or flow. across the tricuspid valve, and biochemical testing was. carried out only in those who were found to have an. intermediate risk. We also examined the performance of. a policy in which the estimated risk was first derived by. a combination of maternal age and biochemical testing, and ultrasound examination was carried out only in those. with an intermediate risk. Methods The data for this study were derived from. prospective screening for trisomy 21 in singleton. pregnancies, using, as markers, a combination of. maternal age, fetal NT thickness and maternal-serum free. β-human chorionic gonadotropin (β-hCG) and pregnancy- associated plasma protein-A (PAPP-A), in a onestop. clinic for first-trimester assessment of risk at to weeks of gestation. Assessment of the fetal. nasal bone, ductus venosus flow and tricuspid flow. were also routinely performed by appropriately trained. sonographers. The performance of different screening. policies was examined. Results The study population consisted of pregnancies with a normal karyotype or delivery of a. phenotypically normal baby (euploid group) and 122. cases of trisomy 21. The best performance was achieved. by a contingent policy in which first-stage screening was. based on maternal age, fetal NT thickness and either. tricuspid valve or ductus venosus blood flow, followed by. biochemical testing only those with an intermediate risk, of 1 in 51 to 1 in 1000 (which constituted about 20% of the total). The performance of contingent screening. in which first-stage testing relies on biochemistry was. poorer than when first-stage screening was performed by. ultrasound examination because, in order to achieve the. same detection rate, the false-positive rate was twice as. high. Conclusion Effective first-trimester screening for trisomy. 21 can be achieved by a contingent policy in which. first-stage testing is based on ultrasound examination. and second-stage biochemical testing is carried out in. only 20% of the patients. Copyright 2010 ISUOG. Published by John Wiley & Sons, Ltd. 48.")
49
Figure 1 Axial view of fetal brain demonstrating lateral ventricles (dotted line) and choroid plexuses (*) in a euploid fetus (a) and in a fetus with trisomy 13 (b). In both fetuses the biparietal diameter was 24 mm. ABSTRACT Objective To examine the possible association between aneuploidies and fetal lateral cerebral ventriculomegaly in the first trimester of pregnancy. Methods Three-dimensional brain volumeswere acquired by transvaginal ultrasound examination at 11–13 weeks’ gestation in 410 euploid fetuses and 63 fetuses with trisomy 21, 34 with trisomy 18 and seven with trisomy 13. Lateral ventricles were assessed in a transverse view, just above the roof of the third ventricle and measurements of the areas of the lateral ventricles and choroid plexuses were obtained. The ratio between choroid plexus and lateral ventricle areas (CLR) was calculated. Measurements in aneuploid fetuses were compared to those in euploid fetuses. Results In euploid fetuses the lateral ventricle and choroid plexus areas increased, whereas the CLR decreased with fetal biparietal diameter. In fetuseswith trisomy 21, lateral ventricle and choroid plexus areas were smaller but CLR was not significantly different from that in euploid fetuses. In trisomy 18 and 13 fetuses, CLR was significantly smaller than in euploid fetuses. The CLR was below the 5th centile of normal range in 11 (32.4%) fetuses with trisomy 18 and in six (85.7%) with trisomy 13. Conclusion There is evidence of ventriculomegaly at 11–13 weeks’ gestation in most fetuses with trisomy 13 and one third of fetuses with trisomy 18. Copyright 2012 ISUOG. Published by John Wiley & Sons, Ltd.
 was calculated. Measurements. in aneuploid fetuses were compared to those in euploid. fetuses. Results In euploid fetuses the lateral ventricle and choroid. plexus areas increased, whereas the CLR decreased with. fetal biparietal diameter. In fetuseswith trisomy 21, lateral. ventricle and choroid plexus areas were smaller but CLR. was not significantly different from that in euploid fetuses. In trisomy 18 and 13 fetuses, CLR was significantly. smaller than in euploid fetuses. The CLR was below the. 5th centile of normal range in 11 (32.4%) fetuses with. trisomy 18 and in six (85.7%) with trisomy 13. Conclusion There is evidence of ventriculomegaly at. 11–13 weeks’ gestation in most fetuses with trisomy 13. and one third of fetuses with trisomy 18. Copyright 2012 ISUOG. Published by John Wiley & Sons, Ltd.")
50
Figure 3 (a) Doppler recording of ductus venosus flow (upper trace) and hepatic artery flow (lower trace) in a 12-week fetus with trisomy 21. The sample gate includes the ductus venosus and the hepatic artery, the waveforms of which are very clearly recorded in spite of no clear color Doppler visualization of the vessel. Note the high velocities. (b) Doppler recording with the sample gate including the ductus venosus only. The hepatic artery waveform can still be seen faintly in the upper channel. (c) Doppler recording with the sample gate moved slightly toward the fetal aorta to include only the hepatic artery waveform. ABSTRACT Objective Low-resistance hepatic artery (HA) flow has been reported in severely growth-restricted fetuses. The same finding has been incidentally observed in firsttrimester fetuses with enlarged nuchal translucency (NT). The aim of this study was to investigate HA flow in first-trimester fetuses. Methods Crown–rump length (CRL), NT, ductus venosus (DV) pulsatility index for veins (PIV) and HA pulsatility index (PI) were measured prospectively in fetuses at increased risk on first-trimester assessment for aneuploidy and in a control group of low-risk fetuses. Outcome of pregnancy was known in all cases. Independent sample t-test was used for intergroup comparison. Results NT, DV-PIV and HA-PI were measured prospectively in 59 fetuses. Thirty-four had an enlarged NT and underwent karyotyping, which was abnormal in 16 cases (trisomy 21, n = 12; trisomy 18, n = 3; 47,XXY, n = 1). Two pregnancies were terminated in view of fetal anomalies. In three other infants an abnormality was confirmed after birth (Noonan syndrome, unspecified genetic syndrome and cardiac defect). The remaining 13 fetuses with enlarged NT and the 25 with normal NT had an uneventful pregnancy outcome. HA-PI was significantly and inversely correlated with NT and DV-PIV. Mean HA-PI was significantly lower in fetuses with adverse outcome (chromosomal anomalies 1.60; chromosomally normal fetuses with adverse outcome 1.66) than in controls (2.03). Conclusions Low-resistance HA flow can be observed in first-trimester fetuses and, based on its association with adverse outcome, it can be regarded as an ominous sign. Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. While investigating ductus venosus (DV) flow in severely growth-restricted fetuses, a strong arterial signal can sometimes be recorded on the reverse channel. This signal arises from the hepatic artery (HA), a vessel situated in close proximity to the DV (Figure 1). From studies in second- and third-trimester growthrestricted fetuses it is known that the flow in this vessel increases in conditions of redistribution of the fetal circulation driven by hypoxemia1–3. This mechanism has been called the hepatic arterial buffer response (HABR)3. The underlying mechanism of the HABR is a compensatory one, aiming to maintain blood supply to the liver when there is increased shunting of umbilical venous blood through the DV. In postnatal life the HABR operates in conditions of reduced portal flow such as in anemia, hypovolemia or liver cirrhosis4–6. While investigating DV flow in first-trimester fetuses at increased risk of aneuploidy we incidentally observed that in particularly severe circumstances (hydrops, large nuchal translucency (NT)) a similarly strong arterial signal can be detected on the reverse channel of the DV Doppler flow spectrum7. The aim of this study was to prospectively investigate blood flow in this vessel and to attempt to understand the underlying pathophysiological mechanism of HABR in first-trimester fetuses.
 Doppler recording with the sample gate including the ductus venosus. only. The hepatic artery waveform can still be seen faintly in the upper channel. (c) Doppler recording with the sample gate moved slightly. toward the fetal aorta to include only the hepatic artery waveform. ABSTRACT. Objective Low-resistance hepatic artery (HA) flow has. been reported in severely growth-restricted fetuses. The. same finding has been incidentally observed in firsttrimester. fetuses with enlarged nuchal translucency (NT). The aim of this study was to investigate HA flow in. first-trimester fetuses. Methods Crown–rump length (CRL), NT, ductus venosus. (DV) pulsatility index for veins (PIV) and HA. pulsatility index (PI) were measured prospectively in. fetuses at increased risk on first-trimester assessment. for aneuploidy and in a control group of low-risk. fetuses. Outcome of pregnancy was known in all cases. Independent sample t-test was used for intergroup. comparison. Results NT, DV-PIV and HA-PI were measured prospectively. in 59 fetuses. Thirty-four had an enlarged NT and. underwent karyotyping, which was abnormal in 16 cases. (trisomy 21, n = 12; trisomy 18, n = 3; 47,XXY, n = 1). Two pregnancies were terminated in view of fetal anomalies. In three other infants an abnormality was confirmed. after birth (Noonan syndrome, unspecified genetic syndrome. and cardiac defect). The remaining 13 fetuses. with enlarged NT and the 25 with normal NT had an. uneventful pregnancy outcome. HA-PI was significantly. and inversely correlated with NT and DV-PIV. Mean. HA-PI was significantly lower in fetuses with adverse. outcome (chromosomal anomalies 1.60; chromosomally. normal fetuses with adverse outcome 1.66) than in. controls (2.03). Conclusions Low-resistance HA flow can be observed in. first-trimester fetuses and, based on its association with. adverse outcome, it can be regarded as an ominous sign. Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. While investigating ductus venosus (DV) flow in severely. growth-restricted fetuses, a strong arterial signal can. sometimes be recorded on the reverse channel. This. signal arises from the hepatic artery (HA), a vessel. situated in close proximity to the DV (Figure 1). From studies in second- and third-trimester growthrestricted. fetuses it is known that the flow in this vessel. increases in conditions of redistribution of the fetal. circulation driven by hypoxemia1–3. This mechanism. has been called the hepatic arterial buffer response. (HABR)3. The underlying mechanism of the HABR. is a compensatory one, aiming to maintain blood. supply to the liver when there is increased shunting of. umbilical venous blood through the DV. In postnatal. life the HABR operates in conditions of reduced. portal flow such as in anemia, hypovolemia or liver. cirrhosis4–6. While investigating DV flow in first-trimester fetuses. at increased risk of aneuploidy we incidentally observed. that in particularly severe circumstances (hydrops, large. nuchal translucency (NT)) a similarly strong arterial. signal can be detected on the reverse channel of the. DV Doppler flow spectrum7. The aim of this study. was to prospectively investigate blood flow in this. vessel and to attempt to understand the underlying. pathophysiological mechanism of HABR in first-trimester. fetuses.")
51
Figure 1 Cross-sectional view of the fetal mediastinum at the level of the three vessels and trachea view, showing measurement of the intrathoracic mediastinal diameter and, along the same line, the anteroposterior diameter of the fetal thymus in a normal fetus (a) and a fetus with trisomy 21 (b), which had a smaller thymic–thoracic ratio. Copyright ABSTRACT Objectives To assess thymic size expressed as the thymic–thoracic ratio (TT-ratio) in fetuses with trisomy 21, 18 or 13. Methods The TT-ratio, the quotient of the anteroposterior thymic and the intrathoracic mediastinal diameter, was measured in 65 trisomic fetuses between 15 and 36 weeks’ gestation, including 30 cases with trisomy 21, 19 with trisomy 18 and 16 with trisomy 13. In addition these 65 fetuses were divided into two groups, according to whether they showed growth that was appropriatefor- gestational age (AGA) (n=39) or intrauterine growth restriction (IUGR) (n=26). Measurements were compared with reference ranges from 302 normal fetuses. Results The TT-ratio was low in 27.7% (n=18) of the 65 fetuses with aneuploidy. In comparison to normal fetuses (mean TT-ratio, 0.44), those with trisomy 18 or 21 had a significantly smaller TT-ratio (mean, 0.38 (P<0.001) and 0.40 (P<0.05), respectively), while those with trisomy 13 did not (mean, 0.43). These values were not as low as those observed previously in fetuses with del.22q11, suggesting a mechanism involving accelerated thymic involution rather than primary thymic hypoplasia. Furthermore, the TT-ratio was significantly lower than normal in both AGA (P<0.05) and IUGR (P<0.001) fetuses. Conclusion Fetuses with trisomy 18 or 21, but not trisomy 13, have a small thymus, suggesting accelerated thymic involution in utero. IUGR may contribute to the reduced thymic size in trisomy 18 fetuses. Trisomy 21 fetuses seem to have additional factors leading to a small thymus which could be a possible confirmation of the reduced immune response observed in fetuses and neonates with Down syndrome. Copyright
 and a. fetus with trisomy 21 (b), which had a smaller thymic–thoracic ratio. Copyright. ABSTRACT. Objectives To assess thymic size expressed as the. thymic–thoracic ratio (TT-ratio) in fetuses with trisomy. 21, 18 or 13. Methods The TT-ratio, the quotient of the anteroposterior. thymic and the intrathoracic mediastinal diameter, was measured in 65 trisomic fetuses between 15 and. 36 weeks’ gestation, including 30 cases with trisomy 21, 19 with trisomy 18 and 16 with trisomy 13. In addition. these 65 fetuses were divided into two groups, according. to whether they showed growth that was appropriatefor- gestational age (AGA) (n=39) or intrauterine growth. restriction (IUGR) (n=26). Measurements were compared. with reference ranges from 302 normal fetuses. Results The TT-ratio was low in 27.7% (n=18) of the. 65 fetuses with aneuploidy. In comparison to normal. fetuses (mean TT-ratio, 0.44), those with trisomy 18. or 21 had a significantly smaller TT-ratio (mean, (P<0.001) and 0.40 (P<0.05), respectively), while those. with trisomy 13 did not (mean, 0.43). These values were. not as low as those observed previously in fetuses with. del.22q11, suggesting a mechanism involving accelerated. thymic involution rather than primary thymic hypoplasia. Furthermore, the TT-ratio was significantly lower than. normal in both AGA (P<0.05) and IUGR (P<0.001) fetuses. Conclusion Fetuses with trisomy 18 or 21, but not. trisomy 13, have a small thymus, suggesting accelerated. thymic involution in utero. IUGR may contribute to the. reduced thymic size in trisomy 18 fetuses. Trisomy 21. fetuses seem to have additional factors leading to a. small thymus which could be a possible confirmation. of the reduced immune response observed in fetuses. and neonates with Down syndrome. Copyright.")
52
Burada triküspid, nazal kemik veya duktus anlatılırken hepsine değil sadece birine bakılması önerilmiş.

53
Sonuç Gebe tarama yönteminin gücü hakkında bilgilendirilmeli
Uygulanacak tarama testinin seçilme nedeni anlatılmalı En düşük yalancı pozitiflik ile yüksek saptama düzeyi hedeflenmeli Belki de en önemli şey hitap edilen topluma tarama testlerinin amacı ve gücü hakkında doğru bilgi verilmesi.

54
Teşekkür ederim

Benzer bir sunumlar

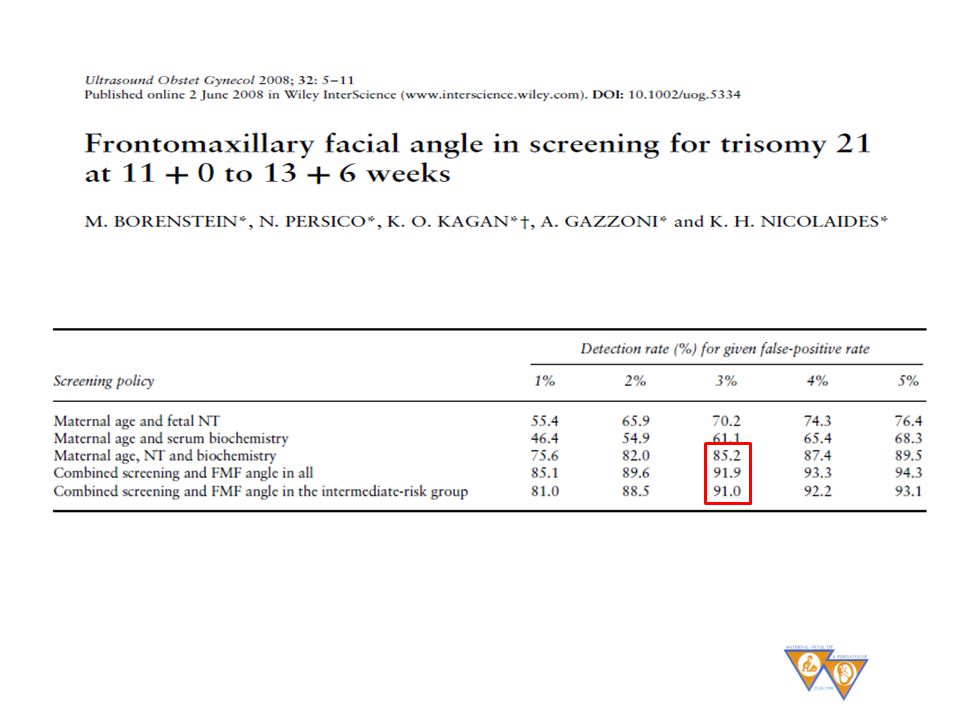


>")





>")










