Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Özefagus Hastalıkları
Prof. Dr. Öge TAŞCILAR

2
Farinks ile mide arasında
Musküler, elastik, kontraktil tüp Uzunluk cm. Önce orta hat, sonra sağ, alt 1/3 sol Hiatustan geçip mide

3
Trake, troid, boyun damarları
D.Torasikus, aorta ile komşu 4 Bölüm Faringoözefagiayal Servikal Torakal Abdominal

4
Özefagus seyri boyunca 3 darlık:
Servikal(Krikoid kıkırdak altında) Torakal(Sol ana bronş ve aorta) Abdominal (D. Hiatus geçildiği yer AÖS).
 Torakal(Sol ana bronş ve aorta) Abdominal (D. Hiatus geçildiği yer AÖS).")
5
Mukoza Submukoza Muskularis Propria Seroza (sadece abdomende) İntraepitelyal Mukoza Epitel Bazal Membran Lamina Propria Muskularis Mukoza

6
Özefagus Motilite Bozuklukları
Akalazya Diffüz Özefagiyel Spazm Özefagus Divertikülleri Hiatal herni Gastroözefajiyel Reflü Hastalığı Barret Özefagus Özefagus Kanserleri

7
Semptom: Disfaji Regürjitasyon Retrosternal yangı Göğüs ağrısı

8
Achalasia Etiology and Pathophysiology
Peristalsis of lower two thirds of esophagus absent Impairment of neurons that innervate esophagus Unopposed contraction of LES LES pressure ↑ Incomplete relaxation of LES Obstruction occurs at/near diaphragm

9
Achalasia Fig. 42-9

10
Achalasia Clinical Manifestations
Gece regurjitasyon Aspirasyon Pnömoni Bronşit Akciğer abse

11
Achalasia Diagnostic Studies
Radiologic studies Manometric studies of lower esophagus Endoscopy

12
Achalasia Diagnostic Studies
Endoskopi Özefagus dilatasyonu Gıda retansiyonu Manometri AÖS basıncı yüksek(>25 mm Hg) Relaksasyon olmaması Aperistaltizm
 Relaksasyon olmaması. Aperistaltizm.")
13
Achalasia Komplikasyonlar: Respiratuar sistem en sık Pnömoni
Atelektazi, bronşit, abse Bronşektazi Hemoptizi Etrafa bası Premalign lezyon(%1-10)
")
14
Achalasia Treatment Drug therapy Symptomatic relief
Smooth muscle relaxants Uzun etkili nitratlar Ca channel blockers Nitrogliserin Botulinum toxin injection 1 to 2 years relief Symptomatic relief Semisoft diet Eating slowly Drinking with meals

15
Achalasia Treatment Endoscopic pneumatic dilation

16
Achalasia CERRAHİ ENDİKASYON Ciddi özefajit İnfant
Çok ilerlemiş, çok dilate, tortios Hasta cerrahi istiyorsa Takibi zor olgularda

17
Achalasia Surgical therapy Heller myotomy Özefagokardiyal myotomi

18
Diffüz Özefagus Spazmı
Ciddi disfaji, göğüs ağrısı. Anjinayı taklit edebilir. Stress ile artar. Birlikte psikosomatik ağrılar sıktır.

19
Diffüz Özefagus Spazmı
Tedavi: Drug therapy Uzun etkili nitratlar Ca channel blockers Nitrogliserin Botulinum toxin injection 1 to 2 years relief Balon dilatation

20
Diffüz Özefagus Spazmı
Cerrahi Tedavi: Medikal tedavi başarısız ise Epiprenik divertikül oluşmuş ise Cerrahi; Laparoskopik Özefagomyotomi

21
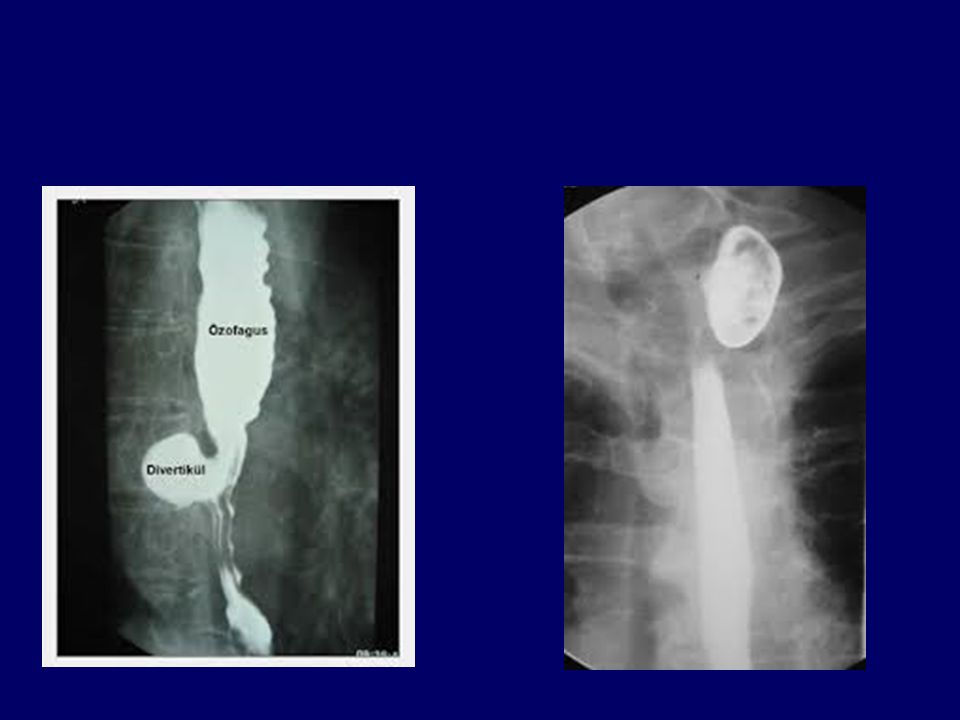
Esophageal Diverticula
Occur in three main areas Zenker’s diverticulum Most common location Traction diverticulum Near esophageal midpoint Epiphrenic diverticulum Above the LES

22
Sites for Occurrence of Esophageal Diverticula

24
Esophageal Diverticula Clinical Manifestations
Symptoms Dysphagia Regurgitation Chronic cough Aspiration Weight loss

25
Esophageal Diverticula Complications
Malnutrition Aspiration Perforation

26
Esophageal Diverticula Diagnostic Studies
Endoscopy Barium studies

27
Esophageal Diverticula
Surgery Zenker: Krikofaringeal myotomi >2 cm ise Divertikülektomi+Krikofaringeal myotomi

28
Hiatal Hernia Herniation of portion of the stomach into esophagus through an opening or hiatus in diaphragm

29
Hiatal Hernia Clinical Manifestations
May be asymptomatic Symptoms include Heartburn After meal or lying supine Dysphagia

30
Hiatal Hernia Diagnostic Studies
Barium swallow May show protrusion of gastric mucosa through esophageal hiatus Endoscopy Visualize lower esophagus Information on degree of inflammation or other problems

31
Hiatal Hernia Complications
GERD Esophagitis Hemorrhage from erosion Stenosis Ulcerations of herniated portion

32
Hiatal Hernia Complications
Strangulation of hernia Regurgitation with tracheal aspiration Increased risk of respiratory problems

33
THERAPY Lifestyle modifications Eliminate alcohol Stop smoking
Avoiding lifting/straining Weight reduction, if appropriate

34
Hiatal Hernia Surgical Therapy
Goals Reduce hernia Provide acceptable lower esophageal sphincter (LES) pressure Prevent movement of gastroesophageal junction
 pressure. Prevent movement of gastroesophageal junction.")
35
Hiatal Hernia Surgical Therapy
Laparoscopically performed Nissen and Toupet techniques are standard antireflux surgeries Thoracic or open abdominal approach used in select cases

36
Nissen Fundoplication
Fig. 42-5

37
GERH Mide içeriğinin distal özefagusa geçerek şikayet oluşturmasına denir. GERH 3 neden AÖS mekanik bozukluğu Yetersiz özefagus temizlenmesi İntragastrik basınç artışı

38
GERH-tanı Üst GIS grafi Anatomik yapının belirlenmesinde
Özefagus-kardiya diyafragma ilişkisi Endoskopi Diğer patolojilerin ekarte edilmesinde Özefajit tespitinde Özefagus manometri 24 saat özefagus pH testi

39
GERH Komplikasyonlar barret ülser kanama perforasyon striktür fibrozis

40
GERH-tedavi Medikal Tedavi: Pozisyon Beslenme AÖS basıncını artırmak
Mide asidini azaltmak Mide içi basıncı azaltmak Antiasit H2 blokör, PPI Metpamid, Sisaprid

41
GERH Cerrahi Tedavi Nissen Fundoplikasyon

42
Esophageal Cancer Adenocarcinomas Squamous cell

43
Esophageal Cancer Etiology and Pathophysiology
Risk factors Smoking Excessive alcohol intake Barrett’s esophagus Diets low in fruits and vegetables Plummer Wilson sendromu Lökoplaki Mantar toksinleri vb. Certain minerals and vitamins Exposure to lye, asbestos, and metal History of achalasia

44
Esophageal Cancer Etiology and Pathophysiology
Majority of tumors located in middle and lower portion of esophagus Malignant tumor Usually appears as ulcerated lesion Obstruction in later stages

45
Esophageal Cancer Clinical Manifestations
Progressive dysphagia is most common( Sıvı geçer katı geçmez) Initially with meat, then soft foods and liquids Pain develops late Substernal, epigastric, or back areas Weight loss Regurgitation of blood-flecked esophageal contents
 Initially with meat, then soft foods and liquids. Pain develops late. Substernal, epigastric, or back areas. Weight loss. Regurgitation of blood-flecked esophageal contents.")
46
Esophageal Cancer Diagnostic Studies
Endoscopy with biopsy Endoscopic ultrasonography (EUS) Barium swallow with fluoroscopy Computed tomography (CT) Magnetic resonance imaging (MRI) PET Bronchoscopic examination
 Barium swallow with fluoroscopy. Computed tomography (CT) Magnetic resonance imaging (MRI) PET. Bronchoscopic examination.")
47
Esophageal Cancer Complications
Hemorrhage Esophageal perforation with fistula formation Esophageal obstruction Metastasis Liver and lung common

48
Esophageal Cancer Surgical procedures Esophagectomy
Removal of part or all of the esophagus Esophagogastrostomy Resection of a portion of esophagus and anastomosis of remaining portion to stomach

49
Esophageal Cancer Endoscopic mucosal resection (EMR)
Removes superficial lesions Submucosal neoplasms

50
Not candidates for surgery(esp. Squamous carcinoma)
Radiation alone Combination chemoradiation

51
Chemoradiation Additional 69 patients were treated with the same combined therapy and were analyzed. Similar results were obtained Median survival : 17.2 months 3-year survival : 30% 5 yr survival :14%

52
NORMAL ESOPHAGUS Normal double contrast esophagram
(barium coating and air distention) Effervescent granules release air with ingestion. 52
 Effervescent granules release air. with ingestion. 52.")
53
PATHOLOGY/RADIOLOGY CORRELATION
image X ray image 53

54
ESOPHAGEAL CANCER Typical squamous cell carcinoma
Poor prognosis from local extension into critical mediastinal structures. (esophagus lacks a serosa) . 54
")
55
ESOPHAGEAL CANCER Distal malignancy may be adenocarcinoma
due to Barrett’s esophagus - dysplastic change caused by chronic reflux of gastric contents. 55

56
CT ESOPHAGEAL CANCER PET/CT CHEST CT

57
ESOPHAGEAL VARICES LINEAR TUBULAR FILLING DEFECTS represent distended veins from shunting due to cirrhosis and portal hypertension 57

58
CANDIDA ESOPHAGITIS Extensive NODULAR filling defects in the esophagus in an immunocompromised patient are typical for candida esophagitis. 58

59
ACHALASIA Distended esophagus with distal stricture
due to Achalasia - Failure of lower sphincter to relax – causing obstruction. Etiology is unknown. BIRD BEAK APPEARANCE Stricture due to cancer or reflux caused scarring have to be considered first. Barium filled esophagus 59

60
MALLORY-WEISS TEAR Esophagus shows a linear tear of mucosa of
distal esophagus due to vomiting with barium tracking into the wall. Full thickness tear or rupture (Boerhaave’s syndrome) can lead to mediastinitis and death. 60
 can lead to mediastinitis. and death. 60.")
61
HIATAL HERNIA NORMAL ESOPHAGUS
*Note distended distal esophagus with herniation of gastric fundus into chest through esophageal hiatus. DIAPHRAGM DIAPHRAGM 61

62
HIATAL HERNIA CXR FINDINGS L
Mass on chest X- ray posterior to heart may be a large hiatal hernia. 62

63
CT HIATAL HERNIA

64
SMALL BOWEL OBSTRUCTION
Ng tube ERECT Multiple Dilated Loops of Small Bowel with Air/Fluid Levels Present at Different Heights 64

65
SMALL BOWEL OBSTRUCTION

66
SMALL BOWEL OBSTRUCTION
String of Pearls Sign UPRIGHT

67
* PARTIAL SMALL BOWEL OBSTRUCTION
DILATED BOWEL * OBSTRUCTION ZONE OF TRANSITION NON DILATED BOWEL Proximal loops are dilated and distal loops are collapsed indicating an obstruction. 67

68
PROXIMAL DILATED BOWEL
CT- SMALL BOWEL OBSTRUCTION Proximal loops are dilated and distal loops are collapsed indicating an obstruction. Obstruction most likely due to adhesions in a patient with history of abdominal surgery ZONE OF TRANSISITON PROXIMAL DILATED BOWEL DISTAL NORMAL BOWEL 68

69
SM. BOWEL BARIUM STUDY HERNIA CT Note hernia in right lower quadrant on both exams accounting for obstruction. Hernia is likely cause if there is no history of prior surgery. 69

70
POST – OP ADYNAMIC ILEUS
COLON LARGE AND SMALL BOWEL SM. BOWEL SYMMETRIC dilatation of large and small bowel is seen normally as a post operative ileus. 70

71
POST – OP ADYNAMIC ILEUS
sutures Colon resection 71

72
CHROHN’S DISEASE normal
Narrowed distal ileum due to chronic inflammation is typical for Crohn’s disease. 72

73
APPENDICOLITH Occasionally a calculus (appendicolith) is seen as the source of appendicitis due to obstruction of the appendix and inflammation. 73

74
DISTENDED APPENDIX WITH LOCAL
ACUTE APPENDICITIS NORMAL DISTENDED APPENDIX WITH LOCAL INFLAMATION. 74

75
ABSCESS Catheter has been placed by radiologist using CT guidance draining abscess collection DRAINAGE 75

76
SPLENIC FLEXURE NORMAL COLON HEPATIC FLEXURE TRANSVERSE COLON DESENDING COLON ASCENDING COLON Normal air contrast barium enema (double contrast-air and barium per rectum) shows filling of colon with air and barium retrograde to the cecum with reflux into the terminal illeum TERMINAL ILEUM CECUM 76
 shows filling of colon with air and barium retrograde to the cecum with reflux into the terminal illeum. TERMINAL ILEUM. CECUM. 76.")
77
PEDUNCULATED COLON POLYP
(DESCENDING COLON) stalk on polyp--pedunculated 77
 stalk on polyp--pedunculated. 77.")
78
COLON POLYP Polyp on wall, sessile, without stalk is coated and outlined by barium 78

79
Distension extends to distal descending colon.
OBSTRUCTION Distension extends to distal descending colon. 79

80
COLON CANCER Barium enema showing an ”APPLE -CORE” constricting lesion with proximal dilatation of colon 80

81
COLON SIGMOID VOLVULUS “COFFEE BEAN SIGN”
Dilated coffee bean shaped sigmoid colon due to volvulus. “COFFEE BEAN SIGN” 81

82
Barium fills to point of obstruction and twist of sigmoid colon
SIGMOID VOLVULUS “BEAK SIGN” Barium fills to point of obstruction and twist of sigmoid colon 82

83
NECROTIZING ENTEROCOLITIS
#1 #2 Air in bowel wall is due to Necrotizing Enterocolits. #1- an infectious complication of premature infants. Air has tracked into the Portal Vein and is seen in #2. 83

84
CT - PNEUMATOSIS Air in the bowel wall Small tiny bubbles
in the wall bowel loop – Red arrows

85
Barium extends from lumen outward into diverticulum.
DIVERTICULOSIS Barium extends from lumen outward into diverticulum. 85

86
DIVERTICULITIS Extensive inflammation, wall thickening and spasm can simulate carcinoma with colonoscopy required to confirm. 86

87
DIVERTICULITIS Single arrow thickened LB; DBL arrow air in tic 87

88
DIVERTICULITIS Black arrow thickened bowel wall, white arrow air in tic

89
NORMAL SMA ARTERIOGRAM
Catheter is placed in superior mesenteric artery showing normal filling of small and large intestinal branches. 89

90
ABNORMAL SMA ARTERIOGRAM GI BLEED
Subtracted SMA arteriogram shows contrast collecting at site of active bleeding in Rt. lower quadrant. 90

91
Technetium-labeled RBC’S
NUCLEAR MEDICINE Technetium-labeled RBC’S Labeled red blood cells are imaged over 1 hour showing extravasation in Rt. colon steadily increasing indicating active bleeding. 91

92
AIR UNDER THE DIAPHRAGM
NORMAL GAS PATTERN AIR UNDER THE DIAPHRAGM Perforation of GI tract leads to pneumoperitoneum collecting subdiaphragmaticly on upright x-ray 92

93
ERECT AND DECUBITUS ABDOMEN FILMS SHOW FREE AIR UNDER THE DIAPHRAGM.
UPRIGHT ERECT AND DECUBITUS ABDOMEN FILMS SHOW FREE AIR UNDER THE DIAPHRAGM. DECUBITUS LEFT LATERAL DECUBITUS (left side dependent) shows air along liver margin. This is the preferred x-ray if the patient cannot stand. 93
 shows air along liver margin. This is the preferred x-ray if the patient cannot stand. 93.")
94
Rigler’s Sign – See both
sides of the bowel wall. Triangle Sign – Small triangles of air

95
Cupula – Continuous Diaphragm Sign
Rigler’s Sign – Double Wall Sign

97
Green Circle – Football Sign
Magenta – Continuous Diaphragm Sign Red – Falciform ligament Yellow – Double Wall Sign or Rigler’s Sign

98
CT – FREE AIR

99
CT – FREE AIR

Benzer bir sunumlar