Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

3
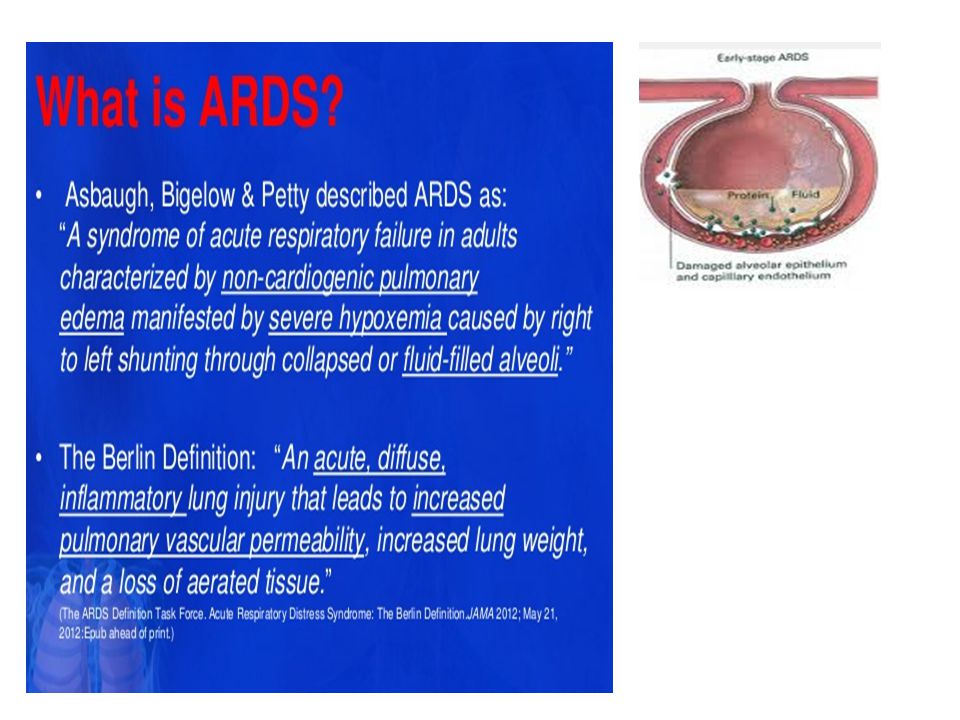
1 st described 1967 (Ashbaugh et al) Incidence 1.5 -7.5/ 100000 population 28 day mortality 25 – 30% 1 Diagnosis clinical
 Incidence / population 28 day mortality 25 – 30% 1 Diagnosis clinical")
7
Differential diagnosis LVF Fluid overload Mitral stenosis Lymphangitis carcinomatosis Interstitial lung disease Differential diagnosis LVF Fluid overload Mitral stenosis Lymphangitis carcinomatosis Interstitial lung disease

18
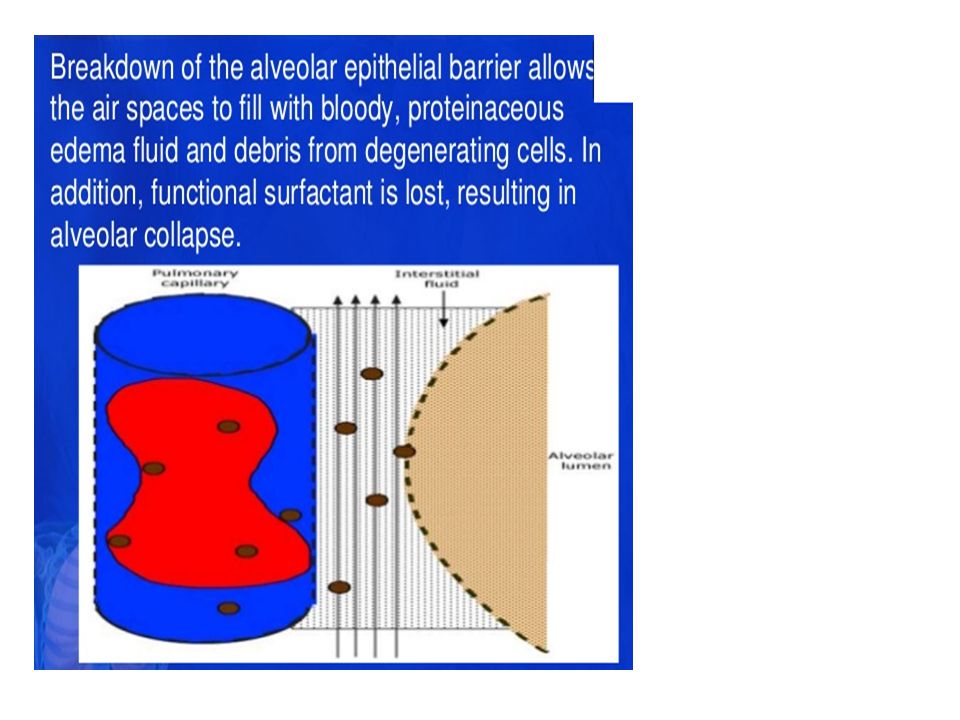
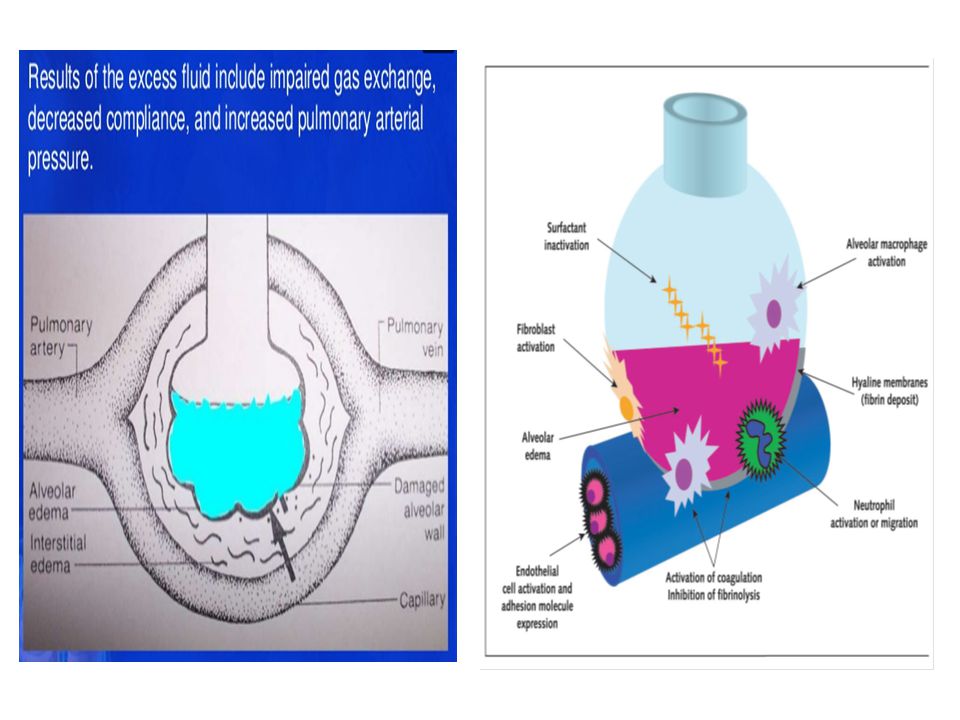
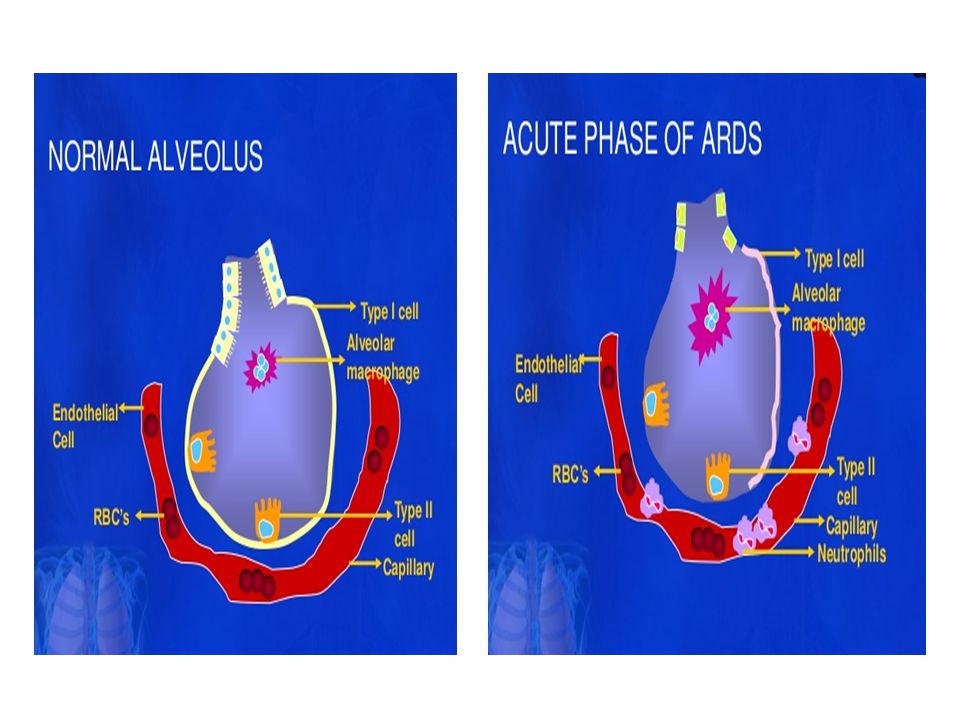
Alveolar Damage Capillary Damage Leakage Oedema Fluid Inflammatory Cellular Infiltrates V/Q Mismatch Atelectasis ↓Thoracic Compliance ↑Dead Space Hypoxic Vasoconstriction Hypoxia

24
Long Term Chronic Respiratory Disease Muscle Fatigue Muscle Wasting Weakness Long Term Chronic Respiratory Disease Muscle Fatigue Muscle Wasting Weakness

25
Symptoms and Signs + Rapid onset of profound dyspnea, usually 12–48 hours after the initiating event Labored breathing and tachypnea, with crackles on examination Marked hypoxemia refractory to supplemental oxygen Multiple-organ failure is seen in many patients

27
Differential Diagnosis Because ARDS is a syndrome, the concept of differential diagnosis applies only in considering the precipitating illness or injury Cardiogenic (hydrostatic) pulmonary edema Pneumonia Aspiration Diffuse alveolar hemorrhage Acute interstitial pneumonitis Acute eosinophilic pneumonia Acute hypersensitivity pneumonitis Cryptogenic organizing pneumonia Pulmonary contusion Drug-induced lung disease
 pulmonary edema Pneumonia Aspiration Diffuse alveolar hemorrhage Acute interstitial pneumonitis Acute eosinophilic pneumonia Acute hypersensitivity pneumonitis Cryptogenic organizing pneumonia Pulmonary contusion Drug-induced lung disease")
28
Diagnosis Laboratory Tests Tests to identify the systemic or pulmonary causes of ARDS are indicated Imaging Studies Chest radiograph shows diffuse or patchy bilateral opacities that rapidly become confluent Air bronchograms are seen in 80% of cases Features of heart failure (pleural effusions, cardiomegaly, venous engorgement in upper lung zones, indistinct blood vessels) are absent Diagnostic Procedures When indicated to exclude cardiogenic pulmonary edema, pulmonary artery catheterization will demonstrate pulmonary arterial wedge pressures ≤ 18 mm Hg
 are absent Diagnostic Procedures When indicated to exclude cardiogenic pulmonary edema, pulmonary artery catheterization will demonstrate pulmonary arterial wedge pressures ≤ 18 mm Hg")
37
Noninvasive sampling Trakeobronchial aspiration mini-bronkoalveolar lavage Mikroskobik analiz (Gram boyaması, sitoloji ) Mikrobiyolojik kültür Can be diagnostic for pnomonia, cancer, inflamatuar conditions
 Mikrobiyolojik kültür Can be diagnostic for pnomonia, cancer, inflamatuar conditions")
38
Fleksibl bronkoskopi Mikroskobik analiz ve mikrobiyolojik kültür Non invaziv tetkikler başarısız ise Non invaziv örnekleme mümkün olmuyor ise Havayollarında kırmızı taze kan, BAL sıvısında eritrosit artışı, hemosiderin-laden makrofajlar : diffüz alveolar hemoraji BAL sıvısında eozinofil sayısında artış : idiyopatik akut eozinofilik pnomoni Yiyecek partikülleri : aspirasyon pnomonisi

39
Ekokardiyografi Klinik ve BNP ile kardiyojenik pulmoner ödem tanısı dışlanamazsa transtorasik eko kullanılır Şiddetli aort yada mitral kapak disfonksiyonu Şiddetli diastolik disfonksiyon Sol ventrikül EF de belirgin azalma Kardiyojenik pulmoner ödemi destekler Bazı ARDS tetikleyicileri ( septik şok ) şiddetli kardiyomyopatiye yol açabilir ve ARDS ile birlikte bulunabilir [1,2]. 1 Bouhemad B, Crit Care Med 2009; 37:441. 2 Landesberg G, Eur Heart J 2012; 33:895.
![Ekokardiyografi Klinik ve BNP ile kardiyojenik pulmoner ödem tanısı dışlanamazsa transtorasik eko kullanılır Şiddetli aort yada mitral kapak disfonksiyonu Şiddetli diastolik disfonksiyon Sol ventrikül EF de belirgin azalma Kardiyojenik pulmoner ödemi destekler Bazı ARDS tetikleyicileri ( septik şok ) şiddetli kardiyomyopatiye yol açabilir ve ARDS ile birlikte bulunabilir [1,2].](http://images.slideplayer.biz.tr/13/4164035/slides/slide_39.jpg "1 Bouhemad B, Crit Care Med 2009; 37: Landesberg G, Eur Heart J 2012; 33:895..")
40
Akciğer biyopsisi Akut hipoksemik solunum yetersizliğinin diğer nedenleri dışlanamıyorsa cerrahi biyopsinin yeri vardır [1,2]. Major komplikasyon oranı %7 dir. Biyopsiye atfedilen ölüm yoktur. Komplikasyon oranı % 39 olmasına rağmen çoğu tolere edilmektedir (persistan hava kaçağı). Biyopsi sonucuna göre hastaların % 60 ına spesifik tedavi yapmak mümkün olmuştur. % 37 hastada gereksiz tedaviler kesilmiştir. Hedefev yönelik tedavi ve prognoz öngörüsü bakımından biyopsi gereklidir. Örnekler: Kriptojenik organize pnomoni Akut fungal infeksiyon Kronik interstisyen akciğer hastalşığı, vaskülitin alevlenmesi Dissemine kanser Patel SR, Chest 2004; 125:197. Papazian L, Anesthesiology 1998; 88:935.
![Akciğer biyopsisi Akut hipoksemik solunum yetersizliğinin diğer nedenleri dışlanamıyorsa cerrahi biyopsinin yeri vardır [1,2].](http://images.slideplayer.biz.tr/13/4164035/slides/slide_40.jpg "Major komplikasyon oranı %7 dir. Biyopsiye atfedilen ölüm yoktur. Komplikasyon oranı % 39 olmasına rağmen çoğu tolere edilmektedir (persistan hava kaçağı). Biyopsi sonucuna göre hastaların % 60 ına spesifik tedavi yapmak mümkün olmuştur. % 37 hastada gereksiz tedaviler kesilmiştir. Hedefev yönelik tedavi ve prognoz öngörüsü bakımından biyopsi gereklidir. Örnekler: Kriptojenik organize pnomoni Akut fungal infeksiyon Kronik interstisyen akciğer hastalşığı, vaskülitin alevlenmesi Dissemine kanser Patel SR, Chest 2004; 125:197. Papazian L, Anesthesiology 1998; 88:935..")
41
DIFFERENTIAL DIAGNOSIS Cardiogenic pulmonary edema is usually due to left ventricular systolic or diastolic dysfunction may also be due to fluid overload, severe hypertension, renal artery stenosis, or severe renal disease. Its presentation is nearly identical to ARDS except there may be evidence of cardiac dysfunction (S3 or S4 gallop, new or changed murmur), elevated right-sided filling pressures (elevated jugular venous pressure), related radiographic abnormalities (pulmonary venous congestion, Kerley B lines, cardiomegaly, and pleural effusions). Distinguishing cardiogenic pulmonary edema from ARDS can be aided by measurement of a BNP echocardiography, right heart catheterization.
, elevated right-sided filling pressures (elevated jugular venous pressure), related radiographic abnormalities (pulmonary venous congestion, Kerley B lines, cardiomegaly, and pleural effusions). Distinguishing cardiogenic pulmonary edema from ARDS can be aided by measurement of a BNP echocardiography, right heart catheterization..")
42
An acute exacerbation of idiopathic pulmonary fibrosis or other chronic interstitial lung diseases Like ARDS, the pathological findings are dominated by diffuse alveolar damage, but the prognosis is substantially worse. This diagnostic possibility is easily overlooked in patients whose underlying interstitial lung disease is unknown or mild or moderate in severity. The diagnosis is suggested by careful review of previous chest radiographic images, by discovery of subpleural reticulocytic changes intermixed with alveolar opacities on a chest CT scan obtained shortly after onset of ARDS, or by surgical lung biopsy

43
Diffuse alveolar hemorrhage May be associated with a large, otherwise unexplained drop in the hemoglobin concentration and hematocrit. While hemoptysis may be minimal or absent, bronchoscopy often reveals frothy bloody secretions throughout the airways and invariably detects an increasing amount of red blood cells in serial bronchoalveolar lavage specimens. The recovery of hemosiderin-laden macrophages from bronchoalveolar lavage fluid is strongly suggestive of diffuse alveolar hemorrhage.

44
Idiopathic acute eosinophilic pneumonia (IAEP) Occurs in previously healthy individuals and is characterized by cough, fever, dyspnea, and sometimes chest pain. Bronchoalveolar lavage specimens always contain a large number of eosinophils, typically 35 to 55 percent of all recovered cells. Peripheral eosinophil may or may not be present

45
Cryptogenic organizing pneumonia (COP) often mimics community-acquired pneumonia with an onset that is heralded by a flu-like illness with fever, malaise, fatigue, and cough. The most common features a persistent nonproductive cough, dyspnea with exertion, and weight loss. BAL usually contains a smaller proportion of macrophages and higher proportions of lymphocytes, neutrophils, and eosinophils than healthy patients. This "mixed pattern" of increased cellularity is thought to be characteristic of COP. The diagnosis is made by ruling out infectious causes of pneumonia and documenting typical pathologic changes in tissue obtained by open lung biopsy.

46
Acute interstitial pneumonia (Hamman-Rich syndrome) is a rare and fulminant form of diffuse lung injury that has a presentation similar to ARDS. Many people consider acute interstitial pneumonia a subset of idiopathic ARDS since its clinical manifestations are similar and both demonstrate diffuse alveolar damage on histopathology. The distinguishing characteristic is that ARDS is often associated with a known risk factor, whereas acute interstitial pneumonia is not.

47
Cancer can disseminate through the lungs so rapidly that the ensuing respiratory failure may be mistaken for ARDS. This is most often due to lymphoma or acute leukemia, but lymphangitic spread of solid tumors occasionally behaves this way. Cytological preparation of bronchoscopic specimens (eg, brushings, lavage) may reveal malignant cells.
 may reveal malignant cells..")
49
Treatment Medications Medications directed at the underlying cause of ARDS are indicated Intravascular volume should be maintained at the lowest level required to maintain adequate cardiac output Diuretics may be needed to reduce pulmonary capillary wedge pressure and improve oxygenation Cardiac output that falls when PEEP is used may be improved by reducing the level of PEEP or by the judicious use of inotropic drugs (eg, norepinephrine)norepinephrine Achieving supranormal oxygen delivery through the use of inotropes and blood transfusion is not clinically useful and may be harmful Sedatives, analgesics, and antipyretics may be used to decrease oxygen consumption Systemic corticosteroids have not been shown to reliably improve outcomes
norepinephrine Achieving supranormal oxygen delivery through the use of inotropes and blood transfusion is not clinically useful and may be harmful Sedatives, analgesics, and antipyretics may be used to decrease oxygen consumption Systemic corticosteroids have not been shown to reliably improve outcomes")
50
Therapeutic Procedures Intubation and mechanical ventilation are usually required to treat hypoxemia Use the lowest levels of PEEP and Fio 2 needed to maintain Pao 2 > 55 mm Hg (7.13 kPa) or the Sao 2 above 88% Mechanical ventilation with small tidal volumes (6 mL/kg of ideal body weight) has been shown to reduce mortality by 10% in a multicenter trial PEEP may be increased as long as cardiac output and oxygen delivery are not impaired and pulmonary pressures are not excessive Prone positioning may improve oxygenation in selected patients
 or the Sao 2 above 88% Mechanical ventilation with small tidal volumes (6 mL/kg of ideal body weight) has been shown to reduce mortality by 10% in a multicenter trial PEEP may be increased as long as cardiac output and oxygen delivery are not impaired and pulmonary pressures are not excessive Prone positioning may improve oxygenation in selected patients")
58
Supine Ventilation ± 40% lung volume under lung, especially patients with large hearts

59
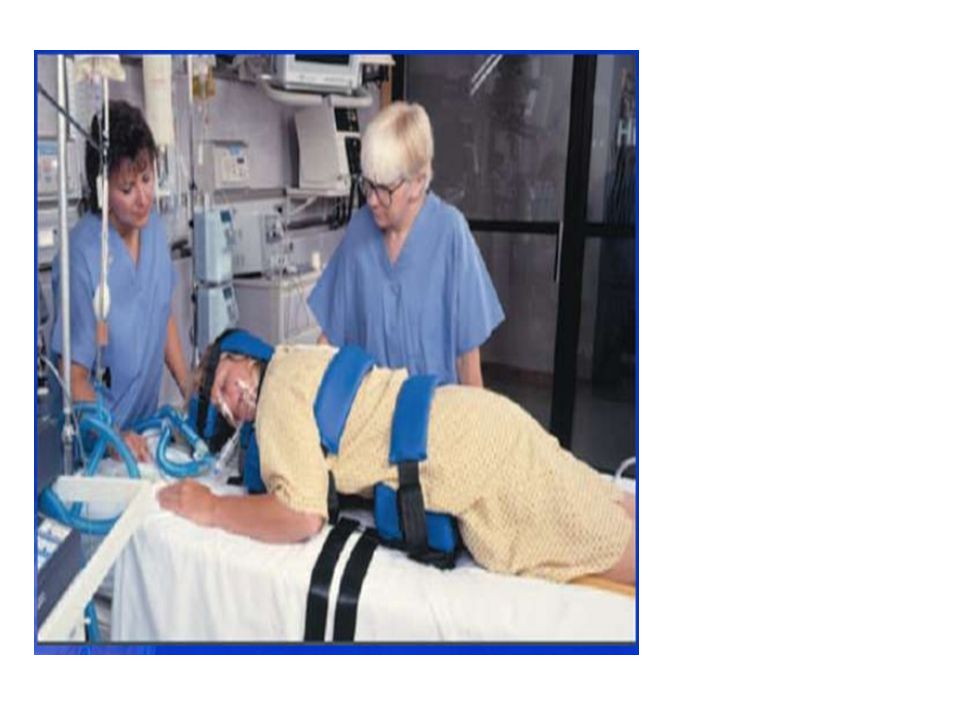
Prone Ventilation

62
Theoretical use to ↓inflammatory response associated with ARDS 2006 study No ↓60 day mortality (28.6% vs 29.2% p= 0.10) Use of steroids 14+ days post onset: ↑ mortality ↓ need for vasopressors ↑ ventilator and shock free days ↑ neuromuscular weakness Short term improvement in oxygenation
 Use of steroids 14+ days post onset: ↑ mortality ↓ need for vasopressors ↑ ventilator and shock free days ↑ neuromuscular weakness Short term improvement in oxygenation")
Benzer bir sunumlar

























>")
