Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Santral Sinir Sistemine Etkili İlaçlar
Sedatif-Hipnotikler Antipsikotikler (Nöroleptikler) Antidepresanlar Antiparkinson ilaçlar
 Antidepresanlar. Antiparkinson ilaçlar.")
2
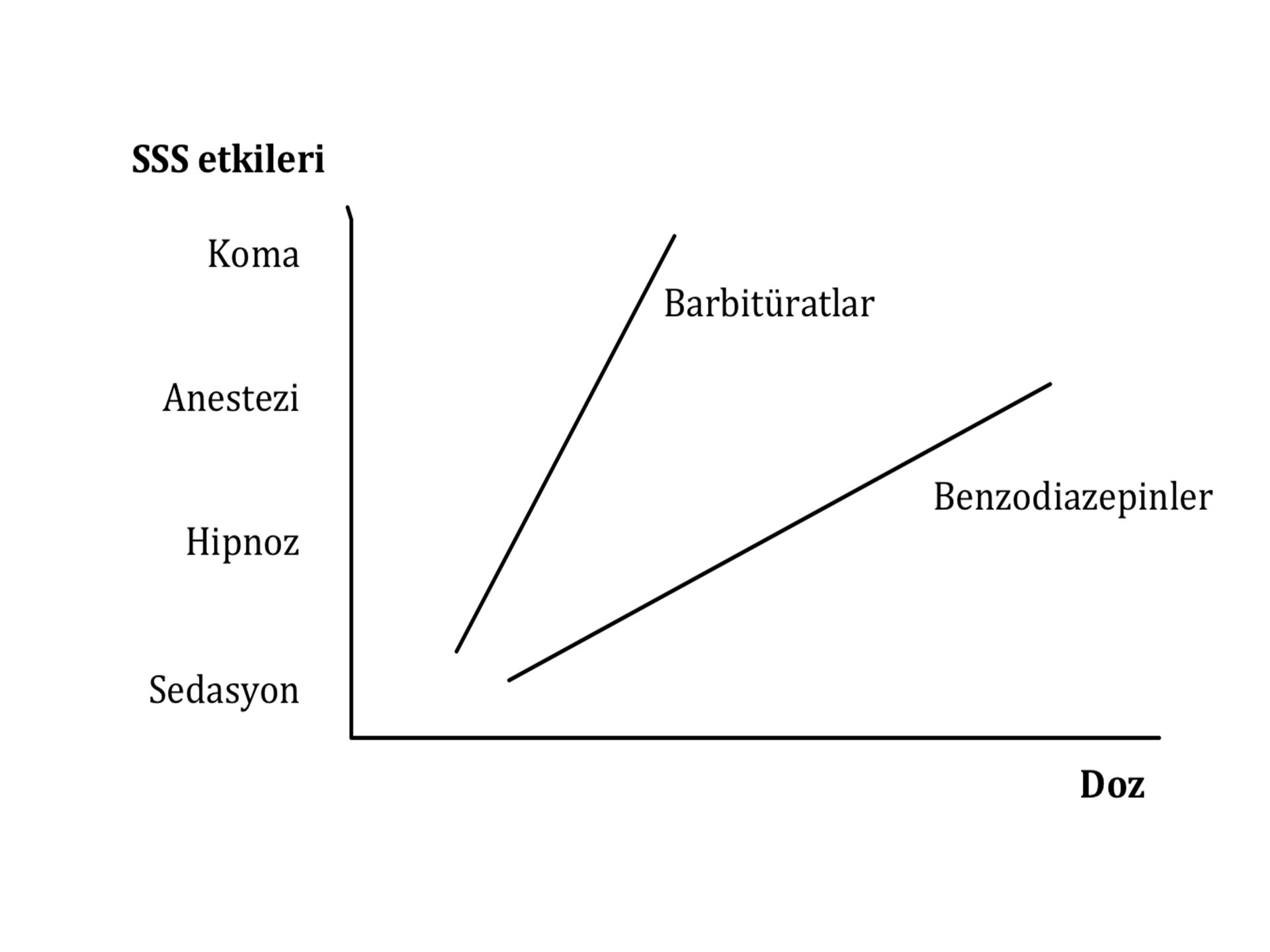
Sedatif-Hipnotik İlaçlar
Benzodiazepinler Buspiron Zopiklon Zolpidem Barbitüratlar Diğer Hipnotikler

3
GABAA Reseptör Kompleksi
GABA bağlanma yeri (+) Agonist: GABA, musimol Antagonist: bikukulin Barbitürat bağlanma yeri (+) Agonist: barbitüratlar Benzodiazepin bağlanma yeri (+) Agonist: benzodiazepinler Ters agonist: β-CCE, β-CCM Antagonist: flumazenil Benzodiazepin bağlanma yerinin en az 2 alt tipi olduğu saptanmıştır: BZ1 (ω1) ve BZ2 (ω2) γ-Aminobutyric acid (GABA) is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor- Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. For this reason it is referred to as a GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. You should refer to pages 220 to 226 of the text for a discussion of the GABAergic synapse as the primary site of action of benzodiazepines and also refer to pages 194 to 197 for a brief discussion of how some anticonvulsants work via activation of GABAergic receptors. Objectives A student should be able to: 1. Reproduce the biosynthetic and metabolic pathways of GABA. 2. Identify the step at which sodium valproate exerts its anticonvulsant response in the above pathways. 3. Reproduce the model of the GABAA Receptor-Benzodiazepine Receptor-Chloride Channel Complex and explain the effect on the receptor and the biological response of each type of drug or endog enous compound, which interacts with the receptor complex. 4. Explain the location and function of GABA’s presynaptic receptor. 5. Account for the mechanism of action of baclofen and its structural relationship to GABA and its structural differences from the more classical muscle relaxants. 6. Account for the mechanism of action of irreversible GABA transaminase (GABA-T) inhibitors. 7. Identify the receptor bound conformation of GABA. 8. Explain why GABA must be present in order for barbiturates or benzodiazepines to exert their pharmacological activity.
 Agonist: GABA, musimol. Antagonist: bikukulin. Barbitürat bağlanma yeri (+) Agonist: barbitüratlar. Benzodiazepin bağlanma yeri (+) Agonist: benzodiazepinler. Ters agonist: β-CCE, β-CCM. Antagonist: flumazenil. Benzodiazepin bağlanma yerinin en az 2 alt tipi olduğu saptanmıştır: BZ1 (ω1) ve BZ2 (ω2) γ-Aminobutyric acid (GABA) is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor- Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. For this reason it is referred to as a GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. You should refer to pages 220 to 226 of the text for a discussion of the GABAergic synapse as the primary site of action of benzodiazepines and also refer to pages 194 to 197 for a brief discussion of how some anticonvulsants work via activation of GABAergic receptors. Objectives. A student should be able to: 1. Reproduce the biosynthetic and metabolic pathways of GABA. 2. Identify the step at which sodium valproate exerts its anticonvulsant response in the above pathways. 3. Reproduce the model of the GABAA Receptor-Benzodiazepine Receptor-Chloride Channel Complex and explain the effect on the receptor and the biological response of each type of drug or endog enous compound, which interacts with the receptor complex. 4. Explain the location and function of GABA’s presynaptic receptor. 5. Account for the mechanism of action of baclofen and its structural relationship to GABA and its structural differences from the more classical muscle relaxants. 6. Account for the mechanism of action of irreversible GABA transaminase (GABA-T) inhibitors. 7. Identify the receptor bound conformation of GABA. 8. Explain why GABA must be present in order for barbiturates or benzodiazepines to exert their pharmacological activity.")
5
Uzun etki süreli Diazepam Ank., Ak. Prototip BZ'dir, en hızlı absorbe edilen BDZ Klordiazepoksid Ank. Prazepam Halazepam Klorazepat Ank. Hpn. Ön ilaçtır, nordazepam'a dönüşür. Anksiyeteli uykusuzlukta yararlı Klonazepam Ak. Antikonvülsan olarak kullanılır Flurazepam Hpn. Kronik kullanımda aktif metabolileri birikir Kuvazepam Orta etki süreli Lorazepam Amnezi yapıcı etkisi diğerlerinden daha fazladır, antipanik etkilidir Oksazepam Alprazolam Ank., Ad Antidepresan etkili BZ, antipanik etkilidir Flunitrazepam Hpn., Ans. Türkiye'deki suistimalinin fazlalığı nedeniyle diğer BDZ'ler gibi yeşil reçeteye değil, kırmızı reçeteye yazılması gerekir. Bir reçetede en fazla toplam 20 mg'lık dozda yazılır (ampul şekli için en fazla 10 mg toplam doz). Belirgin amnezi yapar. Nitrazepam Temazepam Estazolam Kısa etki süreli Midazolam Hpn., Ans Triazolam Hpn Belirgin amnezi yapar. Fiziksel bağımlılık yapma eğilimi yüksektir.
. Belirgin amnezi yapar. Nitrazepam. Temazepam. Estazolam. Kısa etki süreli. Midazolam. Hpn., Ans. Triazolam. Hpn. Belirgin amnezi yapar. Fiziksel bağımlılık yapma eğilimi yüksektir.")
6
Benzodiazepinlerin Etkileri
Normal dozlarda Anksiyolitik etki Sedatif etki Hipnotik etki Antikonvülsan etki Çizgili kas tonusu ↓ (rijidite varsa özellikle) Yüksek dozlarda Motor koordinasyonu bozarlar Anterograd belleği bozarlar Psikomotor reaksiyon hızını ↓
 Yüksek dozlarda. Motor koordinasyonu bozarlar. Anterograd belleği bozarlar. Psikomotor reaksiyon hızını ↓")
7
Benzodiazepin Preparatları
Diazepam DİAZEM 2 mg, 5 mg ve 10 mg, 25 kapsül 10 mg, 10 ampul DİAPAM 10 mg/2ml, 10 ve 100 ampul LİZAN 2 mg ve 5 mg, 25 kapsül NERVİUM 5 mg, 50 tablet Klorazepat ANKSEN 5 mg ve 10 mg, 30 kapsül TRANXİLENE Klordiazepoksit LİBKOL 5 mg, 50 kapsül LİBRAX 5 mg, 40 ve 100 draje KLİPAKS Alprazolam XANAX 0,5 ve 1 mg, 30 tablet Lorazepam ATİVAN EXPİDET 1 ve 2.5 mg, 20 tablet

8
Benzodiazepinlerin Yan Etkileri
SSS depresyonu Anterograd amnezi Artık etki Rebound uykusuzluk Bağımlılık

9
Flumazenil Benzodiazepin antagonistidir.
Hem benzodiazepinleri hem de ters agonistleri antagonize eder. Benzodiazepin aşırı dozajına bağlı belirtilerin giderilmesinde kullanılır. Benzodiazepin bağımlılarına verildiğinde yoksunluk sendromuna neden olur. ANEXATE 0,5 mg/5 ml, 5x5 ml ampul 1 mg/10 ml, 5x10 ml ampul

10
Sedatif-Hipnotik İlaçlar
Benzodiazepinler Buspiron Zopiklon Zolpidem Barbitüratlar Diğer Hipnotikler

11
Atipik Benzodiazepin Reseptör Agonistleri
Zopiklon Zolpidem Zaleplon

12
Barbitüratlar Barbitürik asit türevidirler. Bağımlılık yaparlar.
Yeşil reçeteye yazılırlar. Karaciğer mikrozomal enzimlerini indüklerler.

13
Barbitüratların Etki Süreleri ve Dozları
Doz (mg) Sedatif* Hipnotik Uzun etki süreli (> 6 saat) Fenobarbital 15-30 Barbital 65-130 Orta etki süreli (3 - 6 saat) Pentobarbital 15-40 60-125 Allobarbital 32-64 Amobarbital 20-60 Butalbital Siklobarbital 50-100 Butabarbital 10-60 Kısa etki süreli (< 3 saat) Sekobarbital - Heksobarbital Tetrabarbital Çok kısa etki süreli (birkaç dakika) Tiopental Tiamilal Metoheksital Barbitüratların Etki Süreleri ve Dozları * Bir kezlik dozu gösterir. Bu doz günde 3-4 kez verilir.
 Sedatif* Hipnotik. Uzun etki süreli (> 6 saat) Fenobarbital Barbital Orta etki süreli (3 - 6 saat) Pentobarbital Allobarbital Amobarbital Butalbital Siklobarbital Butabarbital Kısa etki süreli (< 3 saat) Sekobarbital. - Heksobarbital Tetrabarbital. Çok kısa etki süreli (birkaç dakika) Tiopental. Tiamilal. Metoheksital. Barbitüratların Etki Süreleri ve Dozları. * Bir kezlik dozu gösterir. Bu doz günde 3-4 kez verilir.")
14
Sedatif-Hipnotik İlaçlar
Benzodiazepinler Buspiron Zopiklon Zolpidem Barbitüratlar Diğer Hipnotikler

15
Buspiron 5-HT1A reseptörlerinin parsiyel agonistidir. GABA ve BZ reseptörlerini etkilemez. Anksiyolitik etkisi 1-3 haftalık bir uygulamadan sonra (latent dönem) ortaya çıkar. Antidepresan etkinlik de gösterir. Avantajları Anksiyolitik etkisine daha az psikomotor bozukluk eşlik eder. Sedasyon ve amnezi oluşturmaz veya çok hafif oluşturur. Tolerans ve bağımlılık gelişmez; kesilme sendromu oluşturmaz. Yeşil reçeteye yazılması gerekmez. Alkol ve diğer sedatif ilaçlarla birlikte alındığında onların depresif etkilerini artırmaz. Kısmen karaciğerde metabolize edilir; kısmen de değişmeden böbreklerden atılır. İleri derecede karaciğer veya böbrek yetmezliği olanlarda kontrendikedir. Doz: 5 mg x 3 kez/gün ile başlanır. Günlük doz 2-3 günde bir yeterli bir cevap alınana kadar 5 mg artırılır. Optimal günlük doz mg'dır. Diğer türevler: ipsapiron, gepiron BUSPON 5 mg, 50 kapsül
 ortaya çıkar. Antidepresan etkinlik de gösterir. Avantajları. Anksiyolitik etkisine daha az psikomotor bozukluk eşlik eder. Sedasyon ve amnezi oluşturmaz veya çok hafif oluşturur. Tolerans ve bağımlılık gelişmez; kesilme sendromu oluşturmaz. Yeşil reçeteye yazılması gerekmez. Alkol ve diğer sedatif ilaçlarla birlikte alındığında onların depresif etkilerini artırmaz. Kısmen karaciğerde metabolize edilir; kısmen de değişmeden böbreklerden atılır. İleri derecede karaciğer veya böbrek yetmezliği olanlarda kontrendikedir. Doz: 5 mg x 3 kez/gün ile başlanır. Günlük doz 2-3 günde bir yeterli bir cevap alınana kadar 5 mg artırılır. Optimal günlük doz mg dır. Diğer türevler: ipsapiron, gepiron. BUSPON. 5 mg, 50 kapsül.")
16
Antipsikotikler (Nöroleptikler)
A characteristic feature of schizophrenia is a defect in 'selective attention'. Whereas a normal individual quickly accommodates to stimuli of a familiar or inconsequential nature, and responds only to stimuli that are unexpected or significant, the ability of schizophrenic patients to discriminate between significant and insignificant stimuli seems to be impaired. Thus, the ticking of a clock may command as much attention as the words of a companion; a chance thought, which a normal person would dismiss as inconsequential, may become an irresistible imperative. 'Latent inhibition' is a form of behavioural testing in animals, which can be used as a model for this type of sensory habituation. If a rat is exposed to a 'conditioned' stimulus (such as a bell), followed by an 'unconditioned' stimulus (e.g. a foot shock) that it can avoid (e.g. by pressing a bar), it will quickly learn to press the bar as soon as it hears the bell-the conditioned response. But if it has previously heard the bell several times without any ensuing foot shock, it will learn the conditioned response less quickly, having learned to disregard the bell. Latent inhibition is a measure of the inhibitory effect of pre-exposure to the conditioned stimulus on acquisition of the conditioned response. It is often impaired in schizophrenic subjects and in animals treated with amphetamine or psychotomimetic drugs such as lysergic acid diethylamide (LSD), and is restored by many antipsychotic drugs.
, followed by an unconditioned stimulus (e.g. a foot shock) that it can avoid (e.g. by pressing a bar), it will quickly learn to press the bar as soon as it hears the bell-the conditioned response. But if it has previously heard the bell several times without any ensuing foot shock, it will learn the conditioned response less quickly, having learned to disregard the bell. Latent inhibition is a measure of the inhibitory effect of pre-exposure to the conditioned stimulus on acquisition of the conditioned response. It is often impaired in schizophrenic subjects and in animals treated with amphetamine or psychotomimetic drugs such as lysergic acid diethylamide (LSD), and is restored by many antipsychotic drugs.")
17
Nöroleptiklerin Etkilerinde Reseptörlerin Rolü
Antipsikotik etki D2 ve D4 5-HT2 Ekstrapiramidal yan etkiler D2 Endokrin yan etkiler Rang & Dale 6th Ed Dopamine theory None The dopamine theory was proposed by Carlson-awarded a Nobel Prize in 2000-on the basis of indirect pharmacological evidence in humans and experimental animals. Amphetamine releases dopamine in the brain and can produce in humans a behavioural syndrome indistinguishable from an acute schizophrenic episode-very familiar to doctors who treat drug users. In animals, dopamine release causes a specific pattern of stereotyped behaviour that resembles the repetitive behaviours sometimes seen in schizophrenic patients. Potent D2-receptor agonists (e.g. apomorphine and bromocriptine; Ch. 34) produce similar effects in animals, and these drugs, like amphetamine, exacerbate the symptoms of schizophrenic patients. Furthermore, dopamine antagonists and drugs that block neuronal dopamine storage (e.g. reserpine) are effective in controlling the positive symptoms of schizophrenia, and in preventing amphetamine-induced behavioural changes. There is a strong correlation between clinical antipsychotic potency and activity in blocking D2-receptors (fig. 38.1), and receptor-imaging studies have shown that clinical efficacy of antipsychotic drugs is consistently achieved when D2-receptor occupancy reaches about 80%.3 There is no consistent biochemical evidence for excessive dopamine synthesis or release in schizophrenia. Furthermore, the production of prolactin, which might be expected to be abnormally low if dopaminergic transmission was facilitated, is normal in schizophrenic patients. One difficulty in interpreting such studies is that nearly all schizophrenic patients are treated with drugs that are known to affect dopamine metabolism, whereas the non-schizophrenic control group are not. Even where it has been possible to allow for this factor, however, most findings have proved negative. The best evidence for increased dopamine release in schizophrenic patients comes from imaging studies (Laruelle et al., 1999). A radioligand imaging technique was used to measure binding of a specific antagonist (raclopride) to D2-receptors in the striatum. Injection of amphetamine caused dopamine release and thus displacement of raclopride, measured as a reduction of the signal intensity. This reduction was greater by a factor of 2 or more in schizophrenic subjects compared with in control subjects, implying a greater amphetamine-induced release of dopamine. The effect was greatest in schizophrenic individuals during acute attacks, and absent during spontaneous remissions-clear evidence linking dopamine release to the symptomatology. An increase in dopamine receptor density in schizophrenia has been reported in some studies, but not consistently, and the interpretation is complicated by the fact that antipsychotic drug treatment is known to increase dopamine receptor expression. The D4-receptor has also attracted attention on account of the high degree of genetic polymorphism that it shows in human subjects, and because some of the newer antipsychotic drugs (e.g. clozapine; see below) turn out to have a high affinity for this receptor subtype. Genetic studies have, however, failed to show any relationship between schizophrenia and D4-receptor polymorphism. Moreover, a specific D4-receptor antagonist proved ineffective in clinical trials. Another variant of the dopamine hypothesis (see Abi-Dargham & Laruelle, 2005) suggests that schizophrenia reflects an imbalance between excessive activation of D2-receptors in subcortical regions (causing positive symptoms) and deficient activation of cortical D1-receptors (causing negative symptoms). It is fair to say that, although dopamine is undoubtedly involved, the details remain far from clear. Glutamate theory Another transmitter implicated in the pathophysiology of schizophrenia is-you will not be surprised to learn-glutamate (see Goff & Coyle, 2001; Moghaddam, 2003). NMDA receptor antagonists such as phencyclidine, ketamine and dizocilpine (Ch. 33) produce psychotic symptoms (e.g. hallucinations, thought disorder) in humans, and reduced glutamate concentrations and glutamate receptor densities have been reported in post-mortem schizophrenic brains-one of the few fairly consistent findings. Although schizophrenia is difficult to diagnose in a mouse, transgenic mice in which NMDA receptor expression is reduced (not abolished, because this is fatal) show stereotypic behaviours and reduced social interaction that are suggestive of schizophrenia and that respond to antipsychotic drugs-evidence that supports the glutamate hypothesis. According to this view, glutamate and dopamine exert excitatory and inhibitory effects, respectively, on GABAergic striatal neurons, which project to the thalamus and constitute a sensory 'gate' (see below). Too little glutamate, or too much dopamine, disables the gate, allowing uninhibited sensory input to reach the cortex. It is also suggested that abnormal glutamate function-specifically reduced NMDA-receptor activation-could account for the cognitive deficit that is increasingly recognised as a central feature of schizophrenia, responsible in part for the negative symptoms of the disorder. One possibility is therefore that excess dopamine receptor activation is mainly responsible for positive symptoms, deficient NMDA-receptor activation for the negative symptoms. Although undoubtedly too simple, this idea is driving current efforts to develop novel antipsychotic drugs that increase NMDA-receptor activation. Other theories Other transmitters that may be important include 5-HT and noradrenaline (norepinephrine). The idea that 5-HT dysfunction could be involved in schizophrenia was based on the fact that LSD (see Ch. 42) produces schizophrenia-like symptoms, and has drifted in and out of favour many times (see Busatto & Kerwin, 1997). Many effective antipsychotic drugs, in addition to blocking dopamine receptors (see below), also act as 5-HT-receptor antagonists. 5-HT modulates dopamine pathways, so the two theories are not incompatible. Many 'atypical' antipsychotic drugs (see below) produce fewer extrapyramidal side effects than dopamine-selective compounds, and combine with 5-HT2A-receptors. Whether 5-HT2A-receptor blockade accounts directly for their antipsychotic effects, or merely reduces undesirable side effects associated with D2-receptor antagonists, remains controversial. In conclusion, the dopamine hyperactivity theory of schizophrenia remains attractive. It is undoubtedly an oversimplification, and relates only to the positive symptoms, but it provides the best framework for understanding the action of antipsychotic drugs, although effects on 5-HT and other receptors may contribute significantly to the clinical profile of some of the newer drugs. The glutamate hypothesis is, however, gaining ground, and there are reasonable hopes that it will lead to the next generation of antipsychotic drugs (see Javitt, 2004).
 produce similar effects in animals, and these drugs, like amphetamine, exacerbate the symptoms of schizophrenic patients. Furthermore, dopamine antagonists and drugs that block neuronal dopamine storage (e.g. reserpine) are effective in controlling the positive symptoms of schizophrenia, and in preventing amphetamine-induced behavioural changes. There is a strong correlation between clinical antipsychotic potency and activity in blocking D2-receptors (fig. 38.1), and receptor-imaging studies have shown that clinical efficacy of antipsychotic drugs is consistently achieved when D2-receptor occupancy reaches about 80%.3. There is no consistent biochemical evidence for excessive dopamine synthesis or release in schizophrenia. Furthermore, the production of prolactin, which might be expected to be abnormally low if dopaminergic transmission was facilitated, is normal in schizophrenic patients. One difficulty in interpreting such studies is that nearly all schizophrenic patients are treated with drugs that are known to affect dopamine metabolism, whereas the non-schizophrenic control group are not. Even where it has been possible to allow for this factor, however, most findings have proved negative. The best evidence for increased dopamine release in schizophrenic patients comes from imaging studies (Laruelle et al., 1999). A radioligand imaging technique was used to measure binding of a specific antagonist (raclopride) to D2-receptors in the striatum. Injection of amphetamine caused dopamine release and thus displacement of raclopride, measured as a reduction of the signal intensity. This reduction was greater by a factor of 2 or more in schizophrenic subjects compared with in control subjects, implying a greater amphetamine-induced release of dopamine. The effect was greatest in schizophrenic individuals during acute attacks, and absent during spontaneous remissions-clear evidence linking dopamine release to the symptomatology. An increase in dopamine receptor density in schizophrenia has been reported in some studies, but not consistently, and the interpretation is complicated by the fact that antipsychotic drug treatment is known to increase dopamine receptor expression. The D4-receptor has also attracted attention on account of the high degree of genetic polymorphism that it shows in human subjects, and because some of the newer antipsychotic drugs (e.g. clozapine; see below) turn out to have a high affinity for this receptor subtype. Genetic studies have, however, failed to show any relationship between schizophrenia and D4-receptor polymorphism. Moreover, a specific D4-receptor antagonist proved ineffective in clinical trials. Another variant of the dopamine hypothesis (see Abi-Dargham & Laruelle, 2005) suggests that schizophrenia reflects an imbalance between excessive activation of D2-receptors in subcortical regions (causing positive symptoms) and deficient activation of cortical D1-receptors (causing negative symptoms). It is fair to say that, although dopamine is undoubtedly involved, the details remain far from clear. Glutamate theory. Another transmitter implicated in the pathophysiology of schizophrenia is-you will not be surprised to learn-glutamate (see Goff & Coyle, 2001; Moghaddam, 2003). NMDA receptor antagonists such as phencyclidine, ketamine and dizocilpine (Ch. 33) produce psychotic symptoms (e.g. hallucinations, thought disorder) in humans, and reduced glutamate concentrations and glutamate receptor densities have been reported in post-mortem schizophrenic brains-one of the few fairly consistent findings. Although schizophrenia is difficult to diagnose in a mouse, transgenic mice in which NMDA receptor expression is reduced (not abolished, because this is fatal) show stereotypic behaviours and reduced social interaction that are suggestive of schizophrenia and that respond to antipsychotic drugs-evidence that supports the glutamate hypothesis. According to this view, glutamate and dopamine exert excitatory and inhibitory effects, respectively, on GABAergic striatal neurons, which project to the thalamus and constitute a sensory gate (see below). Too little glutamate, or too much dopamine, disables the gate, allowing uninhibited sensory input to reach the cortex. It is also suggested that abnormal glutamate function-specifically reduced NMDA-receptor activation-could account for the cognitive deficit that is increasingly recognised as a central feature of schizophrenia, responsible in part for the negative symptoms of the disorder. One possibility is therefore that excess dopamine receptor activation is mainly responsible for positive symptoms, deficient NMDA-receptor activation for the negative symptoms. Although undoubtedly too simple, this idea is driving current efforts to develop novel antipsychotic drugs that increase NMDA-receptor activation. Other theories. Other transmitters that may be important include 5-HT and noradrenaline (norepinephrine). The idea that 5-HT dysfunction could be involved in schizophrenia was based on the fact that LSD (see Ch. 42) produces schizophrenia-like symptoms, and has drifted in and out of favour many times (see Busatto & Kerwin, 1997). Many effective antipsychotic drugs, in addition to blocking dopamine receptors (see below), also act as 5-HT-receptor antagonists. 5-HT modulates dopamine pathways, so the two theories are not incompatible. Many atypical antipsychotic drugs (see below) produce fewer extrapyramidal side effects than dopamine-selective compounds, and combine with 5-HT2A-receptors. Whether 5-HT2A-receptor blockade accounts directly for their antipsychotic effects, or merely reduces undesirable side effects associated with D2-receptor antagonists, remains controversial. In conclusion, the dopamine hyperactivity theory of schizophrenia remains attractive. It is undoubtedly an oversimplification, and relates only to the positive symptoms, but it provides the best framework for understanding the action of antipsychotic drugs, although effects on 5-HT and other receptors may contribute significantly to the clinical profile of some of the newer drugs. The glutamate hypothesis is, however, gaining ground, and there are reasonable hopes that it will lead to the next generation of antipsychotic drugs (see Javitt, 2004).")
18
Nöroleptikler D. Diğer Nöroleptikler A. Fenotiazinler
1. Tipik nöroleptikler Pimozid Penfluridol Molindon Oksipertin 2. Atipik nöroleptikler Klozapin D2 etkinliği Olanzapin azaltılmış, Risperidon 5-HT2 etkinliği Sertindol artırılmış Amisülprid olanlar Aripiprazol (ketiapin, seroquel, zotepin) 3. Arada kalan nöroleptikler Sülpirid D2 reseptörlere Remoksiprid ileri derecede Rakloprid selektif olanlar A. Fenotiazinler 1. Alifatik fenotiazinler Klorpromazin (asepromazin, levopromazin, promazin, metotrimeprazin trifluopromazin) 2. Piperidinli fenotiazinler Tioridazin (mezoridazin, perisiyazin, pipotiyazin) 3. Piperazinli fenotiazinler Flufenazin (trifluoperazin, perfenazin, proklorperazin, asetofenazin, karfenazin) B. Yapıca Fenotiazinlere Benzeyenler Klorprotiksen, Tiotiksen Zuklopentiksol, Flupentiksol Loksapin C. Butirofenonlar Haloperidol (melperon, droperidol, benperidol)
 3. Arada kalan nöroleptikler. Sülpirid D2 reseptörlere. Remoksiprid ileri derecede. Rakloprid selektif olanlar. A. Fenotiazinler. 1. Alifatik fenotiazinler. Klorpromazin. (asepromazin, levopromazin, promazin, metotrimeprazin trifluopromazin) 2. Piperidinli fenotiazinler. Tioridazin. (mezoridazin, perisiyazin, pipotiyazin) 3. Piperazinli fenotiazinler. Flufenazin. (trifluoperazin, perfenazin, proklorperazin, asetofenazin, karfenazin) B. Yapıca Fenotiazinlere Benzeyenler. Klorprotiksen, Tiotiksen. Zuklopentiksol, Flupentiksol. Loksapin. C. Butirofenonlar. Haloperidol. (melperon, droperidol, benperidol)")
19
Klorpromazin NÖROLEPTİK SENDROM (25-50 mg, p.o. veya i.m.)
Hipnoz veya aşırı bir sedasyon hali oluşturmaksızın Spontan hareketlerde yavaşlama Çevreye karşı ilgisizlik Çevreden gelen uyarılara yanıt vermeye isteksizlik Yavaşlama, heyecansızlık İnisiyatif ve merakta azalma Motor fonksiyonlar normal Kognitif yetenekler normal (zihinden hesap yapma, çağrışım vb)
")
20
Klorpromazin Sedatif Etki Katalepsi (Katatoni) (yüksek dozda)
Prokonvülsan Etki CTZ İnhibisyonu Hipotermi Endokrin Etkiler prolaktin salgısında artış FSH ve LH salgısında inhibisyon Ekstrapiramidal Etkiler Otonom ve Diğer Etkiler a1-blokaj antikolinerjik etki lokal anestezik etki antihistaminik etki 5-HT2 blokajı Vazomotor ve Solunum Merkezi Üzerine Depresan (Zayıf) Etki
 Etki.")
21
Nöroleptiklerin Yan Etkileri
Doz (mg/gün) Sed. Etki EP Etki Hipo TA Diğer Alifatik fenotiyazinler Klorpromazin +++ ++ Fotosensitizasyon (en fazla) Asepromazin 6-9 Çocuklardaki bulantı-kusma ve ajitasyonda kullanılır Promazin Piperidinli fenotiyazinler Tioridazin + Kardiyotoksisite (en fazla), pigmenter retinopati Mezoridazin 75-300 Kardiyotoksisite Piperazinli fenotiyazinler Flufenazin 2-20 ++++ Perfenazin 8-32 Proklorperazin 75-100 Trifluoperazin 5-20
 Sed. Etki. EP Etki. Hipo TA. Diğer. Alifatik fenotiyazinler. Klorpromazin Fotosensitizasyon (en fazla) Asepromazin Çocuklardaki bulantı-kusma ve ajitasyonda kullanılır. Promazin Piperidinli fenotiyazinler. Tioridazin Kardiyotoksisite (en fazla), pigmenter retinopati. Mezoridazin Kardiyotoksisite. Piperazinli fenotiyazinler. Flufenazin Perfenazin Proklorperazin Trifluoperazin")
22
Nöroleptiklerin Yan Etkileri (devam)
Doz (mg/gün) Sed. Etki EP Etki Hipo TA Diğer Yapıca fenotiyazinlere benzeyenler Klorprotiksen 50-400 +++ ++ Tiotiksen 5-30 +/++ Flupentiksol 6-18 Zuklopentiksol 20-30 Loksapin 60-100 + Butirofenonlar Haloperidol 2-20 ++++ Melperon Droperidol Benperidol Diğer Nöroleptikler (TİPİK) Pimozid 2-6 Hepatit yapabilir Molindon 50-225 Oksipertin 80-120 Fotosensitizasyon
 Sed. Etki. EP Etki. Hipo TA. Diğer. Yapıca fenotiyazinlere benzeyenler. Klorprotiksen Tiotiksen /++ Flupentiksol Zuklopentiksol Loksapin Butirofenonlar. Haloperidol Melperon Droperidol. Benperidol. Diğer Nöroleptikler (TİPİK) Pimozid Hepatit yapabilir. Molindon Oksipertin Fotosensitizasyon.")
23
Nöroleptiklerin Yan Etkileri (devam)
Doz (mg/gün) Sed. Etki EP Etki Hipo TA Diğer Diğer Nöroleptikler (ATİPİK) Klozapin ++ +++ Agranülositoz Plazma prolaktin düzeyinde belirgin artma yapmaz Olanzapin 5-20 + Risperidon 2-8 Sertindol 12-20 QT uzaması, ventriküler aritmi Ketiapin Amisulprid Aripiprazol 15-30 - Ziprasidon Paliperidon There has been a proliferation of atypical antipsychotic drugs since the introduction of clozapine in the late 1980s. The defining characteristic of atypical antipsychotic medications is their low risk of EPS and the related reduced risk of tardive dyskinesia. Although the risk for EPS and tardive dyskinesia appears to be absent only with clozapine, the other atypical drugs present a favorable EPS profile and a 0.5 to 1 percent per year cumulative occurrence of tardive dyskinesia, a marked improvement over conventional agents [7,8] . With the exception of clozapine, there is limited evidence of superior efficacy for any one of these drugs. Many head-to-head comparison trials have been sponsored by pharmaceutical companies; one study found that 90.9 percent of published pharmaceutical-sponsored studies reported results favorable for the sponsor's drug, with contradictory results from different studies comparing the same drugs [9] . There is anecdotal evidence, however, of a differential response for individual patients to particular drugs. The only basis for prediction of patient response is prior response to the same agent. Factors including diagnosis, symptom profile, or specific genetic markers have not proven useful in drug selection. These agents have comparable overall tolerability, but specific side effects seen with each of the drugs differ significantly. In Phase 1 of the CATIE study, a large (n = 1493), randomized, double-blind comparison of antipsychotics for maintenance treatment of schizophrenia, patients were significantly less likely to discontinue treatment with olanzapine than with perphenazine, quetiapine, risperidone, or ziprasidone, but other measures of efficacy and severity of side effects were comparable among them [10] . Treatment choice, therefore, may reasonably be based on individual patient response, side effect profile, and cost.
 Sed. Etki. EP Etki. Hipo TA. Diğer. Diğer Nöroleptikler (ATİPİK) Klozapin Agranülositoz. Plazma prolaktin düzeyinde belirgin artma yapmaz. Olanzapin Risperidon Sertindol QT uzaması, ventriküler aritmi. Ketiapin Amisulprid Aripiprazol Ziprasidon. Paliperidon. There has been a proliferation of atypical antipsychotic drugs since the introduction of clozapine in the late 1980s. The defining characteristic of atypical antipsychotic medications is their low risk of EPS and the related reduced risk of tardive dyskinesia. Although the risk for EPS and tardive dyskinesia appears to be absent only with clozapine, the other atypical drugs present a favorable EPS profile and a 0.5 to 1 percent per year cumulative occurrence of tardive dyskinesia, a marked improvement over conventional agents [7,8] . With the exception of clozapine, there is limited evidence of superior efficacy for any one of these drugs. Many head-to-head comparison trials have been sponsored by pharmaceutical companies; one study found that 90.9 percent of published pharmaceutical-sponsored studies reported results favorable for the sponsor s drug, with contradictory results from different studies comparing the same drugs [9] . There is anecdotal evidence, however, of a differential response for individual patients to particular drugs. The only basis for prediction of patient response is prior response to the same agent. Factors including diagnosis, symptom profile, or specific genetic markers have not proven useful in drug selection. These agents have comparable overall tolerability, but specific side effects seen with each of the drugs differ significantly. In Phase 1 of the CATIE study, a large (n = 1493), randomized, double-blind comparison of antipsychotics for maintenance treatment of schizophrenia, patients were significantly less likely to discontinue treatment with olanzapine than with perphenazine, quetiapine, risperidone, or ziprasidone, but other measures of efficacy and severity of side effects were comparable among them [10] . Treatment choice, therefore, may reasonably be based on individual patient response, side effect profile, and cost.")
24
Nöroleptiklerin Yan Etkileri (devam)
Doz (mg/gün) Sed. Etki EP Etki Hipo TA Diğer Diğer Nöroleptikler (ARADA KALANLAR) Sülpirid + - Antiotistik ve antidepresan. Belirgin antiemetik ve antivertigo etki. Kan basıncını yükseltir. Gebelerde ve böbrek yetmezliğinde kontrendikedir. Remoksiprid ? Aplastik anemi yapar. Tedavinin ilk 6 ayında haftada bir, daha sonra ayda bir kan sayımı yapılmalıdır.
 Sed. Etki. EP Etki. Hipo TA. Diğer. Diğer Nöroleptikler (ARADA KALANLAR) Sülpirid Antiotistik ve antidepresan. Belirgin antiemetik ve antivertigo etki. Kan basıncını yükseltir. Gebelerde ve böbrek yetmezliğinde kontrendikedir. Remoksiprid Aplastik anemi yapar. Tedavinin ilk 6 ayında haftada bir, daha sonra ayda bir kan sayımı yapılmalıdır.")
25
Yan Etkiler Ekstrapiramidal Yan Etkiler Sedasyon Otonomik Yan Etkiler
Akut distonik reaksiyonlar Akatisia Parkinsonizm Tardif diskinezi Sedasyon Otonomik Yan Etkiler Ortostatik hipotansiyon (-blokaj) Atropin benzeri etkiler: Ağız-boğaz kuruluğu, midriyazis, bulanık görme, konstipasyon, ileus, taşikardi, idrar retansiyonu (anti muskarinik etkili olanlar) Yan Etkiler
 Atropin benzeri etkiler: Ağız-boğaz kuruluğu, midriyazis, bulanık görme, konstipasyon, ileus, taşikardi, idrar retansiyonu (anti muskarinik etkili olanlar) Yan Etkiler.")
26
Dil, yüz, boyun ve sırt kaslarında kasılmalar.
Reaksiyon Özellikleri Riskin Maksimum Olduğu Dönem Öne Sürülen Mek. Tedavi ve Önlemler Akut distonik reaksiyonlar Dil, yüz, boyun ve sırt kaslarında kasılmalar. Konvülsiyonu taklit edebilir, histeri değildir. 1. 5. gün Çocuklarda ve 25 yaş gençlerde daha sıktır ? Antiparkinson ilaçlar1 Reversibldir, nöroleptik dozu azaltılınca belirtiler hafifler, kesilince ortadan kalkar Akatisia Aşırı hareketlilik, yerinde duramama 5. 60. gün Doz azaltılmalı veya başka ilaca geçilmeli Antiparkinson ilaçlar, benzodiazepinler veya propranolol2 kullanılabilir. Parkinsonizm Bradikinezi, rijidite, tremor, maske yüz 5. 30. gün DAerjik ant. Antiparkinson ilaçlar Tardif diskinezi Oral-fasiyal diskinezi; yaygın koreoatetoz veya distoni Tedavinin başlangıcından aylar veya yıllar sonra Aşırı DAerjik etkinlik İlaç dozunun azaltılması belirtileri şiddetlendirir. Başarılı bir tedavi yöntemi henüz yoktur; bu nedenle profilaksisi önemlidir. Malign nöroleptik sendrom Kaslarda rijidite ve akinezi, bilinç bulanıklığı, ateş, kreatin fosfokinaz Öldürücü olabilir Haftalar (Nöroleptik kesildikten sonraki birkaç gün boyunca da risk yüksektir) Nöroleptik kesilir Mekanik soğutma Dantrolen3 veya bromokriptin4 (dopaminerjik agonist olarak) Antiparkinson ilaçların yararı yok 1 difenhidramin HCl 25 veya 50 mg i.m.; benztropin mezilat 1 veya 2 mg i.m. veya yavaş i.v. injeksiyonla başlanır, sürdürme tedavisi aynı ilacın oral formu ile birkaç hafta sürdürülür. 2 propranololün nisbeten düşük dozları (20-80 mg/gün) sıklıkla etkindir. Selektif 1 blokörler daha az etkindir. 3 dantrolene yanıt vermekle birlikte, iskelet kası Ca2+ transport sisteminde bir patoloji söz konmusu değildir. 4 bromokriptin mg/gün
 Nöroleptik kesilir. Mekanik soğutma. Dantrolen3 veya bromokriptin4 (dopaminerjik agonist olarak) Antiparkinson ilaçların yararı yok. 1 difenhidramin HCl 25 veya 50 mg i.m.; benztropin mezilat 1 veya 2 mg i.m. veya yavaş i.v. injeksiyonla başlanır, sürdürme tedavisi aynı ilacın oral formu ile birkaç hafta sürdürülür. 2 propranololün nisbeten düşük dozları (20-80 mg/gün) sıklıkla etkindir. Selektif 1 blokörler daha az etkindir. 3 dantrolene yanıt vermekle birlikte, iskelet kası Ca2+ transport sisteminde bir patoloji söz konmusu değildir. 4 bromokriptin mg/gün.")
27
Yan Etkiler Seksüel Disfonksiyon Nöroendokrin Yan Etkiler
Ejakulasyonun inhibisyonu ( blokaj) Bu etki tioridazinde en belirgindir. İmpotens. Ejakulasyonun inhibisyonuna ve hormonal bozukluklara bağlı olarak Nöroendokrin Yan Etkiler FSH, LH ; Prolaktin Kadınlar: Amenore, galaktore Erkekler: Jinekomasti, ödem, kilo , libidoda Yan Etkiler
 Bu etki tioridazinde en belirgindir. İmpotens. Ejakulasyonun inhibisyonuna ve hormonal bozukluklara bağlı olarak. Nöroendokrin Yan Etkiler. FSH, LH ; Prolaktin Kadınlar: Amenore, galaktore. Erkekler: Jinekomasti, ödem, kilo , libidoda Yan Etkiler.")
28
Yan Etkiler Hepatotoksisite Hematolojik Yan Etkiler
Kolestatik sarılık. (Klorpromazin ve diğer alifatik nöroleptikler tarafından oluşturulur. Muhtemelen alerjiktir.) Genellikle ilk 4 hafta içinde ortaya çıkar. Hematolojik Yan Etkiler Lökopeni Nadiren agranülositoz ve aplastik anemi Klozapin nisbeten sık olarak agranülositoz yapar. Alerjik Reaksiyonlar Ürtiker Makülopapüler ve peteşiyal döküntüler Nadiren Stevens-Johnson sendromu Klorpromazin ve diğer alifatik yapılı fenotiazinler dozda fotosensitizasyonciltte koyu pigmentasyon Yan Etkiler
 Genellikle ilk 4 hafta içinde ortaya çıkar. Hematolojik Yan Etkiler. Lökopeni. Nadiren agranülositoz ve aplastik anemi. Klozapin nisbeten sık olarak agranülositoz yapar. Alerjik Reaksiyonlar. Ürtiker. Makülopapüler ve peteşiyal döküntüler. Nadiren Stevens-Johnson sendromu. Klorpromazin ve diğer alifatik yapılı fenotiazinler dozda fotosensitizasyonciltte koyu pigmentasyon. Yan Etkiler.")
29
Yan Etkiler Göz Toksik Psikoz Konvülsiyona Eğilim Kardiyotoksisite
Nadiren kornea ve lens opasiteleri, konjontival melanozis Tioridazin - pigmenter retinopati Toksik Psikoz Nöroleptik tedavisi sırasında nadiren oluşabilir. Muhtemelen ilacın antikolinerjik etkisine bağlıdır. Belirtileri atropin zehirlenme belirtilerine benzer. Hastalığın nüksettiği izlenimini verebilir. Konvülsiyona Eğilim Yeni atipik nöroleptiklerden risperidon ve remoksipridin konvülsan etkinliği yoktur veya çok azdır. Kardiyotoksisite Tioridazin aritmi Malign Nöroleptik Sendrom Yan Etkiler

30
Spesiyaliteler Haloperidol NORODOL 2 mg /ml, 20 ml damla
5 mg, 50 tablet 10 mg, 30 tablet 20 mg, 20 tablet 5 mg/ml, 5 ampul 10 mg/ml, 5 ampul Pimozid NÖROFREN 2 mg, 30 tablet Klorpromazin LARGACTİL 100 mg, 30 tablet 25 mg/5 ml, 10 ampul Flupentiksol FLUANXOL 3 mg, 50 tablet 20 mg/ml, 1 depo ampul Asepromazin PLEGİCİL 1 mg/10 damla, 30 ml Melperon BURONON 25 mg, 50 draje 100 mg, 30 draje 50 mg, 5 ampul Trifluoperazin STİLİZAN 1 mg/ml, 5 ampul 1 mg, 2 mg ve 5 mg 30 draje Tioridazin MELLERETTES 10 mg, 30 draje 30 mg/ml, 30 ml damla MELLERİL 25 mg ve 100 mg, 30 draje Mezoridazin LİDANİL 5 mg, 20 draje

31
Spesiyaliteler Sülpirid DOGMATİL 200 mg, 24 tablet SÜLPİR
50 mg, 30 kapsül ZEPRİD 200 mg, 24 ve 48 tablet 25 mg/5 ml, 200 ml oral solüsyon Zuklopentiksol CLOPİXOL 20 mg/ml, 20 ml damla 2 mg, 10 ve 25 mg, 50 tablet 50 mg/ml, 1 ACUPHASE ampul İM 200 mg/ml, 1 DEPO ampul İM Risperidon RİSPERDAL 1 mg, 2 mg, 3 mg ve 4 mg, 20 tablet Klozapin CLONEX 25 mg ve 100 mg, 50 tablet LEPONEX Amisülprid SOLİAN 200 mg ve 400 mg 60 ve 90 tablet Apipiprazol ABİLİFY 10, 15 ve 30 mg 28 tablet Olanzapin REXAOİN 5 mg ve 10 mg, 28 tablet ZYPREXA 2,5; 5; 7,5 mg ve 10 mg, 28 tablet Ketiapin SEROQUEL 25 mg ve 100 mg, 30 tablet 200 mg, 30 ve 60 tablet

32
Antidepresanlar Trisiklik antidepresanlar
Non-trisiklik antidepresanlar MAO inhibitörleri Lityum karbonat

33
Antidepresanların Etki Mekanizması
Noradrenalin ve/veya serotonin geri alımını (re-uptake) inhibe ederler. Antidepresif etki en az 15 gün devamlı kullanıldıktan sonra ortaya çıkmaktadır.
 inhibe ederler. Antidepresif etki en az 15 gün devamlı kullanıldıktan sonra ortaya çıkmaktadır.")
34
Schematic diagram showing some of the potential sites of action of antidepressant drugs. The primary neuron is shown as releasing a transmitter amine (NT). A modulating neuron may release a second transmitter (NTx), regulating the activity of the primary neuron. The most consistent observed effect of the antidepressants (other than MAO inhibitors) is inhibition of the reuptake transporters (T) for norepinephrine or serotonin. The MAO inhibitors increase the vesicular stores of both NE and 5-HT. Other direct or indirect effects include initial increase in activation of pre- and postsynaptic receptors and subsequent desensitization or down-regulation of transmitter synthesis from an amino acid (AA), receptor numbers, or postreceptor mechanisms. Desensitization resulting from antidepressant use has been reported for a2, b, and 5-HT1A systems (color). VAT denotes a vesicle-associated transporter.
. A modulating neuron may release a second transmitter (NTx), regulating the activity of the primary neuron. The most consistent observed effect of the antidepressants (other than MAO inhibitors) is inhibition of the reuptake transporters (T) for norepinephrine or serotonin. The MAO inhibitors increase the vesicular stores of both NE and 5-HT. Other direct or indirect effects include initial increase in activation of pre- and postsynaptic receptors and subsequent desensitization or down-regulation of transmitter synthesis from an amino acid (AA), receptor numbers, or postreceptor mechanisms. Desensitization resulting from antidepressant use has been reported for a2, b, and 5-HT1A systems (color). VAT denotes a vesicle-associated transporter..")
35
Trisiklik Antidepresanlar
İlaç Doz (mg/gün) Etki Sed. etki Antikol. Hipo TA Kard. YE Konv. nöbet Kilo alma Amitriptilin NA, S +++ ++ Klomipramin S, NA + Doksepin İmipramin Trimipramin Opipramol Farmakolojik etki profili bakımından amitriptiline benzer. Sedatif etkisi belirgindir
 Etki. Sed. etki. Antikol. Hipo. TA. Kard. YE. Konv. nöbet. Kilo. alma. Amitriptilin NA, S Klomipramin. S, NA. + Doksepin. İmipramin. Trimipramin. Opipramol Farmakolojik etki profili bakımından amitriptiline benzer. Sedatif etkisi belirgindir.")
36
Trisiklik Antidepresanlar (devam)
İlaç Doz (mg/gün) Etki Sed. etki Antikol. Hipo TA Kard. YE Konv. nöbet Kilo alma Amoksapin NA, D + ++ Desipramin NA 0/+ Maprotilin +++ Nortriptilin 75-150 Protriptilin 15-40
 Etki. Sed. etki. Antikol. Hipo. TA. Kard. YE. Konv. nöbet. Kilo. alma. Amoksapin NA, D Desipramin NA. 0/+ Maprotilin Nortriptilin Protriptilin")
37
Non-Trisiklik Antidepresanlar
İlaç Doz (mg/gün) Etki Sed. etki Antikol. Hipo TA Kard. YE Konv. nöbet Kilo alma Mirtazapin 15-45 α2 ant. (ayrıca güçlü 5-HT2, 5-HT3 ant.) ++ + Plazma kolesterol ve trigliserid düzeyinde artma. Lökopeni ve agranülositoz. Miyalji. Trazodon1 S (ayrıca 5-HT1, 5-HT2, α2 ant.) +++ 0/+ Bupropion DA ++++ Venlafaksin 75-225 S, NA ? Nefazodon2 (ayrıca 5-HT2 ant.) Reboksetin2 8 NA (Sel.NA RI) Taşikardi, vertigo, parestezi Diğer yan etki 1 priapism (+); 2 impotens (+)
 Etki. Sed. etki. Antikol. Hipo. TA. Kard. YE. Konv. nöbet. Kilo. alma. Mirtazapin α2 ant. (ayrıca güçlü 5-HT2, 5-HT3 ant.) ++ + Plazma kolesterol ve trigliserid düzeyinde artma. Lökopeni ve agranülositoz. Miyalji. Trazodon S. (ayrıca 5-HT1, 5-HT2, α2 ant.) +++ 0/+ Bupropion DA Venlafaksin S, NA. Nefazodon (ayrıca 5-HT2 ant.) Reboksetin2. 8. NA. (Sel.NA RI) Taşikardi, vertigo, parestezi. Diğer yan etki 1 priapism (+); 2 impotens (+)")
38
Non-Trisiklik Antidepresanlar (devam)
İlaç Doz (mg/gün) Etki Mek. Yan etki Mianserin 30-90 ? (Hafif NA reuptake inh.) (5-HT2, H ve 2 ant.) Tetrasiklik bir bileşiktir. Sedatif ve prokonvülsif etkileri vardır. Kardiyotoksik değildir. Aplastik anemi ve agranülositoz gibi ciddi hematolojik bozukluklara yol açması nedeniyle güvenilirliği düşüktür. Amineptin DA Yapıca TAD'lere benzer; ancak, etki kalıbı benzemez. NA ve S sistemlerini etkilemez. Amfetamin benzeri psikostimülan etkilidir. İmmunoalerjik nitelikte hepatik bozukluk, artralji ve ateş yapabilir. Kardiyotoksik değildir. Antikolinerjik etkinliği zayıftır. Tianeptin 37,5 S Reuptake aktivatörü Bulantı, kusma, anksiyete, irritabilite, sedasyon. Antikolinerjik ve kardiyotoksik etkisi diğer ilaçlara göre düşüktür. Viloksazin ? Amfetamin benzeri psikostimülan etkisi vardır. Antikolinerjik, kardiyotoksik ve prokonvülsif etkinliği zayıftır.
 Etki. Mek. Yan etki. Mianserin (Hafif NA reuptake inh.) (5-HT2, H ve 2 ant.) Tetrasiklik bir bileşiktir. Sedatif ve prokonvülsif etkileri vardır. Kardiyotoksik değildir. Aplastik anemi ve agranülositoz gibi ciddi hematolojik bozukluklara yol açması nedeniyle güvenilirliği düşüktür. Amineptin DA. Yapıca TAD lere benzer; ancak, etki kalıbı benzemez. NA ve S sistemlerini etkilemez. Amfetamin benzeri psikostimülan etkilidir. İmmunoalerjik nitelikte hepatik bozukluk, artralji ve ateş yapabilir. Kardiyotoksik değildir. Antikolinerjik etkinliği zayıftır. Tianeptin. 37,5. S Reuptake aktivatörü. Bulantı, kusma, anksiyete, irritabilite, sedasyon. Antikolinerjik ve kardiyotoksik etkisi diğer ilaçlara göre düşüktür. Viloksazin Amfetamin benzeri psikostimülan etkisi vardır. Antikolinerjik, kardiyotoksik ve prokonvülsif etkinliği zayıftır.")
39
Non-Trisiklik Antidepresanlar Selektif Serotonin Reuptake İnhibitörleri (SSRI)
İlaç Doz (mg/gün) Etki Sed. etki Antikol. Hipo TA Kard. YE Konv. nöbet Kilo alma Fluoksetin 20-40 S 0/+ Fluvoksamin Paroksetin Sertralin Sitalopram 20 Uyuşukluk, uykusuzluk, bulantı, kusma, ağız kuruluğu, anksiyete, libidoda azalma, diyare, tremor, artralji Esitalopram 10 Sitalopramın izomeridir. Yan etkileri ona benzer. There is concern that selective serotonin reuptake inhibitors (SSRIs) and other antidepressants may increase the risk of suicidal ideation and behavior in children, adolescents, and adults younger than 25 years [1-3] . In early 2004, the United States Food and Drug Administration (FDA) asked manufacturers of a number of antidepressants to make labeling changes to include a warning about a possible increased risk of suicidal ideation or behavior, particularly at the initiation of therapy or at the time of dose changes [4] . After further analysis, in October 2004, the FDA directed manufacturers of all antidepressants (including tricyclic antidepressants [TCAs] and monoamine oxidase inhibitors) to include a warning stating that antidepressants may increase the risk of suicidal ideation and behavior in children and adolescents.
 Etki. Sed. etki. Antikol. Hipo. TA. Kard. YE. Konv. nöbet. Kilo. alma. Fluoksetin S. 0/+ Fluvoksamin Paroksetin. Sertralin Sitalopram. 20. Uyuşukluk, uykusuzluk, bulantı, kusma, ağız kuruluğu, anksiyete, libidoda azalma, diyare, tremor, artralji. Esitalopram. 10. Sitalopramın izomeridir. Yan etkileri ona benzer. There is concern that selective serotonin reuptake inhibitors (SSRIs) and other antidepressants may increase the risk of suicidal ideation and behavior in children, adolescents, and adults younger than 25 years [1-3] . In early 2004, the United States Food and Drug Administration (FDA) asked manufacturers of a number of antidepressants to make labeling changes to include a warning about a possible increased risk of suicidal ideation or behavior, particularly at the initiation of therapy or at the time of dose changes [4] . After further analysis, in October 2004, the FDA directed manufacturers of all antidepressants (including tricyclic antidepressants [TCAs] and monoamine oxidase inhibitors) to include a warning stating that antidepressants may increase the risk of suicidal ideation and behavior in children and adolescents.")
40
Spesiyaliteler Mianserin TOLVON 10 mg, 30 tablet 30 mg, 14 tablet
Opipramol DEPRENİL 50 mg, 30 tablet İNSİDON 50 mg, 30 draje İNSOMİN İNZETON OPRİDON Amitriptilin LAROXYL 10 mg, 30 draje 25 mg, 40 draje TRİPTİLİN 10 mg, 30 tablet 25 mg, 40 tablet İmipramin TOFRANİL 10 mg ve 25 mg, 50 draje Trazodon DESYREL 50 mg ve 100 mg, 30 tablet Maprotilin LUDİOMİL 25 mg, 30 tablet 75 mg, 14 tablet 25 mg, 10 ampul MAPROTİL Klomipramin ANAFRANİL 10 mg ve 25 mg, 30 draje 75 mg, 20 SR divitab 25 mg/ml, 2 ml’lik 10 ampul

41
Spesiyaliteler Fluoksetin DEPREKS 20 mg, 16 kapsül 20 mg, 24 kapsül
DEPSET FLORAC FULSAC PROZAC 20 mg/5 ml, 70 ml likid SERONİL ZEDPREX Spesiyaliteler Sitalopram CİPRAM 20 mg, 28 tablet CİTARA 40 mg, 28 tablet CİTOLAP 20 mg, 30 tablet CİTOL 20 mg, 28 ve 56 tablet ESTALOPRAM RELAXOL Paroksetin SEROXAT 20 mg, 14 tablet Esitalopram CİPRALEX 10 mg, 28 tablet 20 mg, 28 tablet ESTOLEX 10 mg, 28 tablet

42
Spesiyaliteler SERTRALİN LUSTRAL Paroksetin 50 mg, 14 kapsül PAXİL
SELECTRA 100 mg, 14 kapsül 25 mg, 28 kapsül SERALİN SERDEP Paroksetin PAXİL 20 mg, 28 tablet SEROXAT 20 mg, 14 tablet XETANOR 20 mg, 30 tablet Reboksetin EDRONAX 4 mg, 60 tablet Tianeptin STABLON 12,5 mg, 30 tablet Mirtazapin REMERON 30 mg, 14 tablet 30 mg, 28 tablet MİRTARON Fluvoksamin FAVERİN 50 mg, 30 tablet 100 mg, 30 tablet Venlafaksin EFEXOR 37,5 mg, 28 tablet 75 mg ve 150 mg, 14 XR kapsül

43
MAO İnhibitörleri İlaç Spesiyalite Günlük Doz (mg) MAO A Selektif
Moklobemid AURORIX Selektif olmayanlar Nialamid 75-300 İsokarboksazid 30-50 Fenelzin 30-45 Tranilsipromin 30-60 MAO B Selektif Selejilin DEPRENIL Antidepresif etkinliği vardır, Parkison hst. tedavisinde kullanılır. Selegiline — Selegiline is a selective MAOb inhibitor at low doses and a non-selective MAO inhibitor at higher doses. Selegiline primarily increases dopaminergic neurotransmission at lower doses, and increases serotonergic, noradrenergic, and dopaminergic neurotransmission at higher doses. Low dose selegiline does not appear to have antidepressant properties and is primarily used in treatment of Parkinson disease; it does not require dietary restrictions because of its lack of inhibition of MAOa. Selegiline functions as a traditional MAOI at higher dose. It inhibits both MAOa and MAOb, has antidepressant properties, and, when taken orally, requires dietary restrictions to prevent hypertensive reactions. A transdermal patch form of selegiline (EMSAM) was approved by the FDA in 2006 for use in the treatment of depression [4] . Daily transdermal administration of selegiline allows for dosing that is high enough to produce antidepressant effects (by inhibiting MAOa and MAOb), but bypasses the gut. Direct inhibition of MAOa in the GI tract is avoided when transdermal selegiline is used at a dose of 6 mg/24 hours. There are no dietary restrictions when transdermal selegiline is used at the recommended starting and target dose, 6 mg/24 hours. MAOI dietary restrictions are required if the 9 mg/24 hours or 12 mg/24 hours patch is used, because of limited clinical and experimental experience with higher doses. While it is not known if doses higher than 6 mg/24 hours are clinically more effective, clinicians may prescribe higher doses based on clinical judgment. Dose increases should occur in increments of 3 mg/24 hours (up to a maximum dose of 12 mg/24 hours) at intervals of no less than two weeks. Care must be taken in starting and stopping selegiline, to avoid precipitating a hypertensive reaction of serotonin syndrome (see "Initiating or discontinuing MAO inhibitors" below). The selegiline patch is the first transdermal antidepressant and is of particular benefit to patients who cannot take oral medications. Patients who respond to the 6 mg/24 hour dose may avoid dietary restrictions. Limited data are available to determine which patients are likely to respond at this dose, and whether higher doses, necessitating MAOI dietary restrictions, are indicated for patients who do not respond. Two randomized studies, both using the 6 mg/24 hour patch, found that short term selegiline (six and eight weeks), compared to placebo, improved depression scores and, in patients with less severe depression, increased remission rates [5,6] .
 was approved by the FDA in 2006 for use in the treatment of depression [4] . Daily transdermal administration of selegiline allows for dosing that is high enough to produce antidepressant effects (by inhibiting MAOa and MAOb), but bypasses the gut. Direct inhibition of MAOa in the GI tract is avoided when transdermal selegiline is used at a dose of 6 mg/24 hours. There are no dietary restrictions when transdermal selegiline is used at the recommended starting and target dose, 6 mg/24 hours. MAOI dietary restrictions are required if the 9 mg/24 hours or 12 mg/24 hours patch is used, because of limited clinical and experimental experience with higher doses. While it is not known if doses higher than 6 mg/24 hours are clinically more effective, clinicians may prescribe higher doses based on clinical judgment. Dose increases should occur in increments of 3 mg/24 hours (up to a maximum dose of 12 mg/24 hours) at intervals of no less than two weeks. Care must be taken in starting and stopping selegiline, to avoid precipitating a hypertensive reaction of serotonin syndrome (see Initiating or discontinuing MAO inhibitors below). The selegiline patch is the first transdermal antidepressant and is of particular benefit to patients who cannot take oral medications. Patients who respond to the 6 mg/24 hour dose may avoid dietary restrictions. Limited data are available to determine which patients are likely to respond at this dose, and whether higher doses, necessitating MAOI dietary restrictions, are indicated for patients who do not respond. Two randomized studies, both using the 6 mg/24 hour patch, found that short term selegiline (six and eight weeks), compared to placebo, improved depression scores and, in patients with less severe depression, increased remission rates [5,6] .")
44
Parkinson Hastalığı Tedavisinde Kullanılan İlaçlar

46
Santral etkili antikolinerjik ilaçlar Biperiden Bornaprin HCl
Triheksifenidil Benztropin mezilat Orfenadrin Prosiklidin Dopaminerjik etkinliği artıran ilaçlar Dopamin prekürsörü Levodopa Dopaminerjik agonistler Bromokriptin Lisurid Pergolid Ropinirol Pramipeksol MAO-B inhibitörü Selegilin Rasagilin KOMT inhibitörü Tolkapon Entakapon Amantadin

Benzer bir sunumlar










 Kullanım özellikleri:>")










