Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
DEMİR EKSİKLİĞİ ANEMİSİ

2
İnsidans Demir yeryüzünde en sık bulunan 2.element
Dünyada > 3.5 milyar kişi (2/3) DE Okul öncesi çocukların %40 (%5-75) WHO Gelişmiş ülkelerde 1-2 yaşda %20-30 DE,%4-12 DEA
 DE. Okul öncesi çocukların %40 (%5-75) WHO. Gelişmiş ülkelerde 1-2 yaşda %20-30 DE,%4-12 DEA.")
3
Demirin önemi O2 taşır ve depolar(Hb,mb)
Bir çok redoks enzimde (sitokromlar) İki stabil oksidasyon durumunda olması (Fe +2 ve Fe +3) nedeniyle katalitik rol Çeşitli metabolik ara ürün yapımı Konak savunması(NHDPH oksidaz)
 İki stabil oksidasyon durumunda olması (Fe +2 ve Fe +3) nedeniyle katalitik rol. Çeşitli metabolik ara ürün yapımı. Konak savunması(NHDPH oksidaz)")
4
Demir Metabolizması Demir 2+ (ferröz) veya 3+ (ferrik) durumdadır
Çok az serbest demir vardır Proteinlere ve diğer moleküllere bağlıdır Solubul olmasını sağlar Oxygen Redox reaksiyonlarına katılımını sınırlar Mikrobların kullanımını sınırlar

5
Demir toksititesi O2- + Fe3+ O2 + Fe2+ Fe2+ + H2O2 Fe3+ + OH- + HO
O2 - + H2O2 O2 + OH- + HO Proteinler, lipidler , DNA oksidasyonu

6
Demir dağılımı Hb: %65 RES : ferritin , hemosiderin %20-30
Kas :-myoglobin%10 Plazma :Transferrin bağlı %0.1 Hücresel enzimler :sitokromlar , katalaz

7
Distribution of Iron in Adults
Figure 1. Distribution of Iron in Adults. In the balanced state, 1 to 2 mg of iron enters and leaves the body each day. Dietary iron is absorbed by duodenal enterocytes. It circulates in plasma bound to transferrin. Most of the iron in the body is incorporated into hemoglobin in erythroid precursors and mature red cells. Approximately 10 to 15 percent is present in muscle fibers (in myoglobin) and other tissues (in enzymes and cytochromes). Iron is stored in parenchymal cells of the liver and reticuloendothelial macrophages. These macrophages provide most of the usable iron by degrading hemoglobin in senescent erythrocytes and reloading ferric iron onto transferrin for delivery to cells. Andrews N. N Engl J Med 1999;341:
 and other tissues (in enzymes and cytochromes). Iron is stored in parenchymal cells of the liver and reticuloendothelial macrophages. These macrophages provide most of the usable iron by degrading hemoglobin in senescent erythrocytes and reloading ferric iron onto transferrin for delivery to cells. Andrews N. N Engl J Med 1999;341:")
8
Demir metabolizması eritrositler Diyet makrofajlar Absorbsiyon
hücresel demir hemoztazı O O transferrin Transferrin reseptor Kİ

9
DEMİR ABSORBSİYONU Diyet yaklaşık 10-15mg/gün demir içerir.
3mg Fe mukozal hücrelerce alınır 1mg Fe portal kan akımına geçer Esas duedenum, az jejunum Diyet Absorbsiyon

10
DEMİR ABSORBSİYONUNU ETKİLEYEN FAKTÖRLER
Fiziksel durum: Hem >Fe 2+ >Fe 3+ İnhibitörler:Fitatlar,tannin, demir yüklenmesi Yarışmaya girenler:Kurşun, stronsiyum Arttıranlar:Askorbat,aa,DE, eritropoezin artması, hipoksi, asit ortam Diyet Absorbsiyon

11
Regulation of the Absorption of Intestinal Iron
Figure 4. Regulation of the Absorption of Intestinal Iron. The iron-absorbing cells of the duodenal epithelium originate in the intestinal crypts and migrate toward the tip of the villus as they differentiate (maturation axis). Absorption of intestinal iron is regulated by at least three independent mechanisms. First, iron absorption is influenced by recent dietary iron intake (dietary regulator). After a large dietary bolus, absorptive cells are resistant to iron uptake for several days. Second, iron absorption can be modulated considerably in response to body iron stores (stores regulator). Third, an unidentified signal communicates the state of bone marrow erythropoiesis to the intestine (erythroid regulator). When red-cell production in the bone marrow is accelerated because of ineffective erythropoiesis, absorption of intestinal iron is increased. This process occurs even when there is systemic iron overload. Andrews N. N Engl J Med 1999;341:
. Absorption of intestinal iron is regulated by at least three independent mechanisms. First, iron absorption is influenced by recent dietary iron intake (dietary regulator). After a large dietary bolus, absorptive cells are resistant to iron uptake for several days. Second, iron absorption can be modulated considerably in response to body iron stores (stores regulator). Third, an unidentified signal communicates the state of bone marrow erythropoiesis to the intestine (erythroid regulator). When red-cell production in the bone marrow is accelerated because of ineffective erythropoiesis, absorption of intestinal iron is increased. This process occurs even when there is systemic iron overload. Andrews N. N Engl J Med 1999;341:")
12
Iron Transport across the Intestinal Epithelium
Figure 3. Iron Transport across the Intestinal Epithelium. Iron must cross two membranes to be transferred across the absorptive epithelium. Each transmembrane transporter is coupled to an enzyme that changes the oxidation state of iron. The apical transporter has been identified as DMT1. It acts in concert with a type of ferrireductase activity that has not yet been cloned. The basolateral transporter has not yet been identified. This transporter requires hephaestin, a ceruloplasmin-like molecule, for the transfer of iron to the plasma. On the basis of its structure, hephaestin is presumed to be a form of ferroxidase. In this diagram, hephaestin is depicted at the basolateral surface of the cell, although it has not yet been established that it functions in that location. Iron within enterocytes is stored as ferritin. Andrews N. N Engl J Med 1999;341:

13
Understanding Heme Transport - N
Understanding Heme Transport - N.C Andrews - New England Journal of Medicine:353;

14
HÜCRELERE DEMİR TAŞINMASI
Transferrin:2Fe 3+ taşır, KC’de yapılır, plazma yarı ömrü 8-10 gün,normalde 1/3’ü demir ile bağlıdır Transferrin reseptör:En fazla Kİ,KC ve plesentada bulunur Bir Tf molekülü 100 veya daha fazla kez Fe transport siklusuna katılır Demir regülatuar protein (IRP1 & IRP2) tarafından düzenlenir O O Transferrin Y reseptör Kİ
 tarafından düzenlenir. O O. Transferrin. Y. reseptör. Kİ.")
15
DEMİRİN HÜCRE İÇİNE TRANSPORTU
Fe 2+Tf ,KK’daki TfR1’e bağlanır. Fe 2+Tf/TfR1 clathrin-kaplı çukurlarda bulunur, endosomu oluşturur. Proton pompa pH , demir salınımı. DMT1 sitoplazmaya taşır. Apo-Tf& TfRl hücre yüzeyine geri döner.KK’da demir hem oluşturmak için protoporfirine bağlanır (mitokondri).
.")
16
DEMİR METABOLİZMASI Kİ 300 mg Fe bulunur erythropoez & depolanım. Kİ
Her gün Hb sentezi için 20 mg Fe gerekir. 450 ml tam kanda 200 mg demir vardır Kİ eritrositler

17
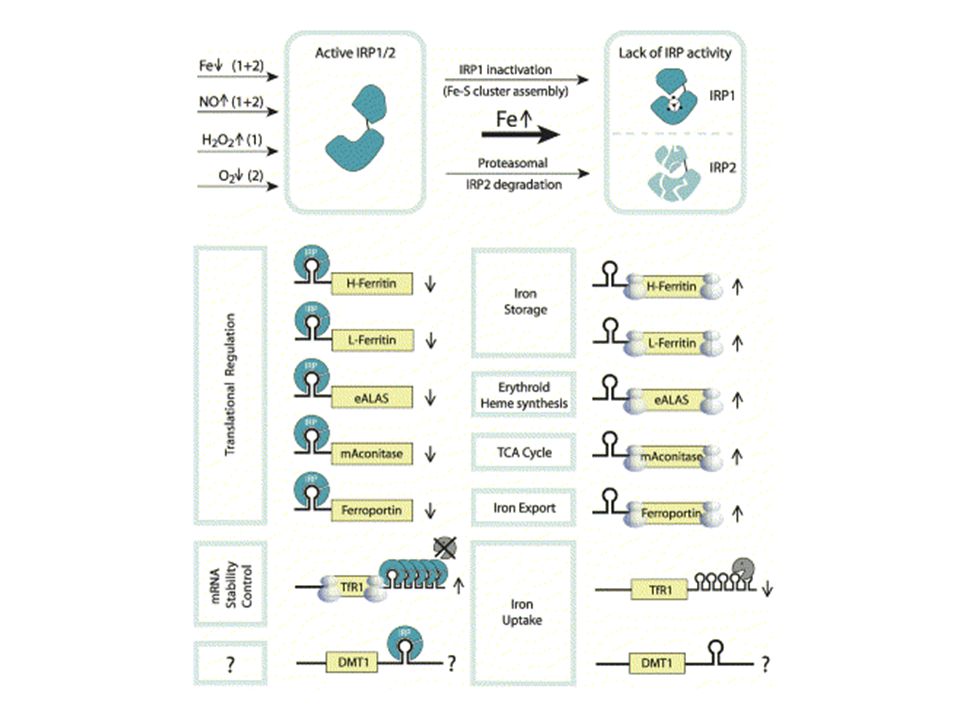
IRP-1 ile Ferritin ve Transferrin Reseptör mRNA’nın etkileşimi
Int J Biochem & Cell Biol 31: , 1999

18
Int J Biochem Cell Biol 33:940-59, 2000

20
Protein Fonksiyon Ekspresyon
Ft (H and L subunit) ( IREs 5’UTR ) Demir depolanımı Çoğu hücrede TfR1 ( IREs 3’UTR ) Demir alımı Eritroid h, epitel h (intestinal kript hücreleri),makrofajlar ve diğer h TfR2 Hepatosit, dolaşan monositler DMT1 (Nramp2/DCT1) Demir alımı; endosomdan stoplazmaya demir salınımı intestinal villusların fırçamsı kenarlarındaki apikal yüzeyler.Endosomal vesiküllerde FP1/IR1/MTP1 Demir atılımı intestinal villusların bazolateral kısımlarında; plasenta; diğer hücre tipleri Proteins, carriers & « regulators » in iron metabolism.
 ( IREs 5’UTR ) Demir depolanımı. Çoğu hücrede. TfR1. ( IREs 3’UTR ) Demir alımı. Eritroid h, epitel h (intestinal kript hücreleri),makrofajlar ve diğer h. TfR2. Hepatosit, dolaşan monositler. DMT1 (Nramp2/DCT1) Demir alımı; endosomdan stoplazmaya demir salınımı. intestinal villusların fırçamsı kenarlarındaki apikal yüzeyler.Endosomal vesiküllerde. FP1/IR1/MTP1. Demir atılımı. intestinal villusların bazolateral kısımlarında; plasenta; diğer hücre tipleri. Proteins, carriers & « regulators » in iron metabolism.")
21
DMT1,NRAMP2,DCT1 (MAJOR APİKAL FERRÖZ TAŞIYICI)
Fe 2+ ,Mn 2+ ,Cu 2+ ,Zn 2+ ,Co 2+ . Ca 2+:DMT1(G185R) mutasyonu sonucu DMT1 kalsiyum iyon kanalına metal taşır Homozigot mutasyonu farede mikrositik anemi (mk)
 mutasyonu sonucu DMT1 kalsiyum iyon kanalına metal taşır. Homozigot mutasyonu farede mikrositik anemi (mk)")
22
HEPHAESTIN Ferroxidaz aktivite Demiri okside eder
Mutasyonu farede hemizigot veya homozigot X-linked anemi(sla) ve demir eksikliği
 ve demir eksikliği.")
23
TFR2 KC ve periferal mononukleer hücrelerde
Transferrin’eTFR1’den daha az afinite TFR1’in %60 homoloğu Mutasyonları hemokromatosise neden olur

24
HEPCİDİN 25 aa peptid. 2000yılında tanımlandı
Antimikrobiyal aktivite. Hepatic bacteriocidal protein Demiri düzenleyen hormon İntestinal Fe absorbsiyonunu düzenleyen faktörler aynı zamanda hepcidin ekspresyonunu da düzenler Demir depolarının artması Eritropoetik aktivitenin artması Hepcidin exp Hipoksi İnflamasyon Hepcidin eksikliği:herediter hemokromatosis fazlalığı:kronik hastalık anemisi

25
HEPCİDİN Interplay of Key Proteins in Iron Homeostasis. In the duodenal enterocyte, dietary iron is reduced to the ferrous state by duodenal ferric reductase (Dcytb), transported into the cell by divalent metal transporter 1 (DMT1), and released by way of ferroportin into the circulation. Hephaestin facilitates enterocyte iron release. Hepatocytes take up iron from the circulation either as free iron or transferrin-bound iron (through transferrin receptor 1 and transferrin receptor 2). Transferrin receptor 2 may serve as a sensor of circulating transferrin-bound iron, thereby influencing expression of the iron regulatory hormone hepcidin. The hepcidin response is also modulated by HFE and hemojuvelin. Hepcidin is secreted into the circulation, where it down-regulates the ferroportin-mediated release of iron from enterocytes, macrophages, and hepatocytes (dashed red lines).
, transported into the cell by divalent metal transporter 1 (DMT1), and released by way of ferroportin into the circulation. Hephaestin facilitates enterocyte iron release. Hepatocytes take up iron from the circulation either as free iron or transferrin-bound iron (through transferrin receptor 1 and transferrin receptor 2). Transferrin receptor 2 may serve as a sensor of circulating transferrin-bound iron, thereby influencing expression of the iron regulatory hormone hepcidin. The hepcidin response is also modulated by HFE and hemojuvelin. Hepcidin is secreted into the circulation, where it down-regulates the ferroportin-mediated release of iron from enterocytes, macrophages, and hepatocytes (dashed red lines).")
27
HEMOJUVELİN Hepatositlerde yüksek oranda eksprese edilir
Demir rezervleri için duyarlı olduğu ve HAMP (Hepcidin)’i regüle ettiği düşünülür
’i regüle ettiği düşünülür.")
28
Interplay of Key Proteins in Iron Homeostasis
Interplay of Key Proteins in Iron Homeostasis. In the duodenal enterocyte, dietary iron is reduced to the ferrous state by duodenal ferric reductase (Dcytb), transported into the cell by divalent metal transporter 1 (DMT1), and released by way of ferroportin into the circulation. Hephaestin facilitates enterocyte iron release. Hepatocytes take up iron from the circulation either as free iron or transferrin-bound iron (through transferrin receptor 1 and transferrin receptor 2). Transferrin receptor 2 may serve as a sensor of circulating transferrin-bound iron, thereby influencing expression of the iron regulatory hormone hepcidin. The hepcidin response is also modulated by HFE and hemojuvelin. Hepcidin is secreted into the circulation, where it down-regulates the ferroportin-mediated release of iron from enterocytes, macrophages, and hepatocytes (dashed red lines). Fleming, R. E. et al. N Engl J Med 2005;352:
, transported into the cell by divalent metal transporter 1 (DMT1), and released by way of ferroportin into the circulation. Hephaestin facilitates enterocyte iron release. Hepatocytes take up iron from the circulation either as free iron or transferrin-bound iron (through transferrin receptor 1 and transferrin receptor 2). Transferrin receptor 2 may serve as a sensor of circulating transferrin-bound iron, thereby influencing expression of the iron regulatory hormone hepcidin. The hepcidin response is also modulated by HFE and hemojuvelin. Hepcidin is secreted into the circulation, where it down-regulates the ferroportin-mediated release of iron from enterocytes, macrophages, and hepatocytes (dashed red lines). Fleming, R. E. et al. N Engl J Med 2005;352:")
29
Herediter Hemokromatosis (HH)
Tip (1): Klasik herediter HH HFE gen mutasyonları. Tip (2): Juvenile-başlangıçlı HH Tip 2A: hemojuvelin HJV mutasyonu Tip 2B: hepcidini kodlayan HAMP geninde mutasyon Tip (3): TfR2-ilişkili HH TfR2 gen mutasyonları Tip (4): Ferroportin-ilişkili demir yüklenmesi Ferroportin-1 gen mutasyonu.
: Klasik herediter HH. HFE gen mutasyonları. Tip (2): Juvenile-başlangıçlı HH. Tip 2A: hemojuvelin HJV mutasyonu. Tip 2B: hepcidini kodlayan HAMP geninde mutasyon. Tip (3): TfR2-ilişkili HH. TfR2 gen mutasyonları. Tip (4): Ferroportin-ilişkili demir yüklenmesi. Ferroportin-1 gen mutasyonu.")
30
DEMİR EKSİKLİĞİ İÇİN RİSKLİ İNFANTLAR
Demir gereksiniminin artması Düşük doğum ağırlığı Yüksek büyüme hızı Kronik hipoksi:siyanotik kalp hastalığı Kan kaybı Perinatal kanama Diyetsel faktörler Erken inek sütü veya solid gıda alımı Düşük et veya C vit alımı Demir desteği yapılmaksızın 6 aydan fazla emzirme Düşük sosyoekonomik durum

31
DEMİR EKSİKLİĞİ İÇİN RİSK FAKTÖRLERİ
Büyüme hızının artması Prematürite, bebeklik, adelosan Yetersiz demir alımı Demir desteği olmayan mamalarla beslenme, 1 yaşından önce inek sütü, 6 aydan sonra demir desteği olmaksızın sadece anne sütü, katı vejeteryan diyet Kan kayıpları Menoraji, GİS’den kan kaybı, Meckel divertikülü, reflüye bağlı özefajit, peptik ülser, inflamatuar barsak hastalığı, parazitler, hemosidenüri, pulmoner hemosiderosis

32
DEMİR EKSİKLİĞİNDE KLİNİK
DE’nin erken dönemlerinde klinik bulgu (-) DE sonucu 1)Hematolojik bulgular:anizositoz, mikrositoz,anemi 2)Sistemik bulgular : davranışsal (yorgunluk,irritabilite, baş ağrısı,uyku bozuklukları),epitelyal(anguler stomatit, glossit, kaşık tırnak,disfaji), algılama
 DE sonucu. 1)Hematolojik bulgular:anizositoz, mikrositoz,anemi. 2)Sistemik bulgular : davranışsal (yorgunluk,irritabilite, baş ağrısı,uyku bozuklukları),epitelyal(anguler stomatit, glossit, kaşık tırnak,disfaji), algılama.")
33
TANISAL TESTLER Periferik yayma
hipokromik mikrositik eritrositler(MCV , MCH<27p, MCHC<%30), RDW>17 Serum demir düzeyi TDBK Demir saturasyonu (<%16): ekonomik,kolay,diürnal değişim, hastalıklardan etkilenim Serum ferritin düzeyi Kİ incelemesi ZPP/hem:kolay,Pb intoksikasyonunda yüksek,bil yüksekliğide ve hemodiyaliz hastalarında hatalı yüksek
, RDW>17. Serum demir düzeyi. TDBK. Demir saturasyonu (<%16): ekonomik,kolay,diürnal değişim, hastalıklardan etkilenim. Serum ferritin düzeyi. Kİ incelemesi. ZPP/hem:kolay,Pb intoksikasyonunda yüksek,bil yüksekliğide ve hemodiyaliz hastalarında hatalı yüksek.")
34
TANISAL TESTLER ZPP/hem:kolay,Pb intoksikasyonunda yüksek,bil yüksekliğide ve hemodiyaliz hastalarında hatalı yüksek Serum transferrin reseptör düzeyi Retikülosit Hb içeriği(CHr) Hipokromik eritrosit yüzdesi Demir tedavisine yanıt
 Hipokromik eritrosit yüzdesi. Demir tedavisine yanıt.")
35
Serum demiri Hemoliz Bilirubin>40 mg Lipidemi
Antikoagülan varlığı:ETDA

36
TOTAL DEMİR BAĞLAMA KAPASİTESİ
DE’de artmıştır(artmış hepatik sentez) Transferrinin bağlıyabileceği max demir konsantrasyonunun ölçümüdür Serm demiri(sature) ve sature olmayan demir bağlama kapasitesi TDBK’ni gösterir
 Transferrinin bağlıyabileceği max demir konsantrasyonunun ölçümüdür. Serm demiri(sature) ve sature olmayan demir bağlama kapasitesi TDBK’ni gösterir.")
37
PERİFERİK YAYMA

38
ORAL DEMİR PREPARATLARI
Ferroglisin sülfat: ferro sanol Damla :1 damla=1 mg Draje :40 mg Duodenal kapsül:100 mg ferro sanol B Şurup: 5ml 20mg demir Vitamin B1, B2, B6 Ferröz sulfat: Tardyferon depo draje: 80mg

39
ORAL DEMİR PREPARATLARI
Ferröz fumarat Vi-fer cap: 175 mg Fe Vitamin B 12, Folik asit, Vitamin C,Tiamin, riboflavin,Nikotinamid, Pridoksin, Ca-pantothenate içerir. Ferröz glukonat Lösferron forte efervesan tablet:695 mg Fe

40
ORAL DEMİR PREPARATLARI
Demir protein süksinilat: Ferplex oral solusyon:Fe III 40mg Ferro III hidroksi polimaltoz: Ferrum hausmann : Damla:50mg/ml Forte tablet :100 mg Şurup:50 mg/5ml

41
DEMİR EKSİKLİĞİ ANEMİSİ (TEDAVİ2)
Demir Tedavisine Yanıt Geçen Süre Yanıt 12-24 saat İntraselüler enzimlerin yerine konması, irritabilitenin azalması, iştah artışı 36-48 saat Kemik iliği yanıtının başlaması, eritroid hiperplazi 48-72 saat Retikülositoz (5-7. günde en yüksek) 4-30 gün Hemoglobin düzeyinde artma 1-3 ay Depoların dolması
 4-30 gün. Hemoglobin düzeyinde artma. 1-3 ay. Depoların dolması.")
42
ORAL DEMİR TEDAVİSİNE CEVAPSIZLIK
Tedaviye uyumsuzluk Devam eden kan kayıpları Yetersiz tedavi süresi Yüksek gastrik Ph antiasit, H2 blokör,gastrik asit pompa inhibitörleri kullanımı Demir absorbsiyon/ütilizasyon inhibitörleri Kurşun Al intoksikasyonu(hemodiyaliz hastaları) Kr inflamasyon Kanser Yanlış tanı Talasemi Sideroblastik anemi
 Kr inflamasyon. Kanser. Yanlış tanı. Talasemi. Sideroblastik anemi.")
43
DEMİR EKSİKLİĞİ ANEMİSİ (PROFİLAKSİ)
Term >6 ay mg/kg/gün Preterm >2 ay mg/kg/gün

44
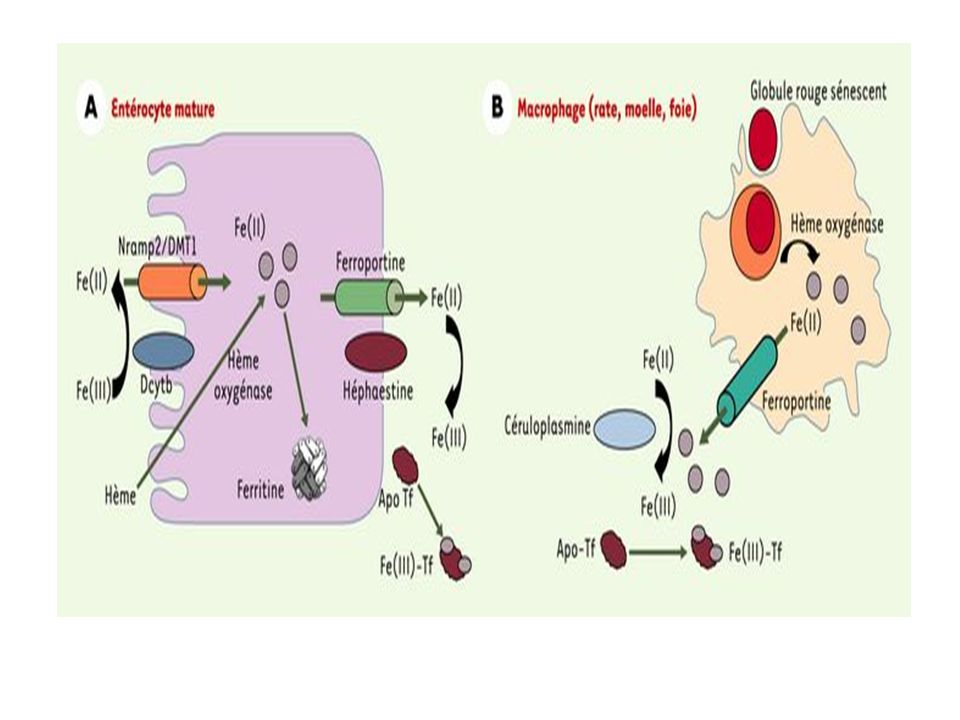
GENERİC CELLULAR IRON UPTAKE

Benzer bir sunumlar