Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
RAHİM İÇİ ARAÇ UYGUNLUK KRİTERLERİ
KENAN ERTOPÇU

2
BAKIR İÇEREN RAHİM İÇİ ARAÇLAR
ÜLKEMİZDE YOK ÜLKEMİZDE ARTIK YOK

3
Copper containing, framed intra-uterine devices for contraception Regina Kulier1, Paul O'Brien2, Frans M Helmerhorst3, Margaret Usher-Patel4, Catherine d'Arcangues5 KANITA DAYALI TIP CuT 380A ve 380S diğer bakırlı RİA’lara göre daha etkin gözükmektedirler. Kanama ve ağrı nedeniyle çıkarılmada RİA’lar arası belirgin fark gözlenmemiştir. Doğum yapmamış kadında herhangi bir RİA’nın diğerine üstünlüğü görülmemiştir.

4
HORMON İÇEREN RAHİM İÇİ SİSTEMLER
Progestasert Nova-T LNG (Mirena) FibroPlant LNG ÜLKEMİZDE YOK ÜLKEMİZDE YOK
 FibroPlant LNG. ÜLKEMİZDE YOK. ÜLKEMİZDE YOK.")
5
Kontraseptif Uygunluk Kriterleri
Kontraseptif yöntemlerin kimlere uygun olup olmadığı ile ilgili bilgiler, farklı yayınlarda farklı başlıklar altında veriliyor. "Endikasyonlar", "kimler kullanabilir"; "kontrendikasyonlar", "kimler kullanamaz", "kullanım için uyarılar" ve "rölatif kontrendikasyonlar", "önlem gerektiren durumlar"

6
Aile planlaması programlarını desteklemek ve nitelikli hizmetleri güçlendirmek üzere kontraseptif kullanımı ile ilgili uygunluk kriterlerinin gözden geçirildiği uluslararası çalışmalar DSÖ tarafından 1994 yılında başlatılmıştır.

7
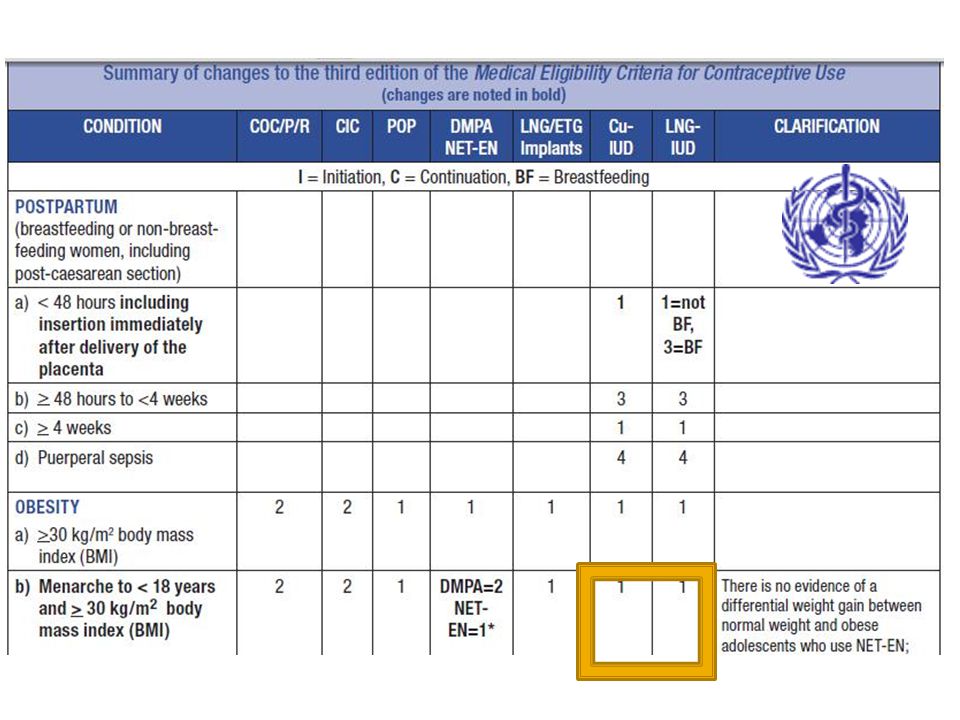
DSÖ Kontraseptif Uygunluk Kriterlerinin Gelişme Kronolojisi
1994 İki ayrı bilimsel grupta yürütülen toplam 21 ülke adına katılan uzmanların katılımı ile çalışmaların başlaması 1996 İlk çalışmaların dökümantasyonlarının yayınlanması 2000 Seçilmiş durumlarda kontraseptif kullanımının ağırlıklı olduğu çalışmaların derlenmesiyle 1996 yayınının güncellenmesi Ekim 2003 İsviçre’de DSÖ merkezinde 35’ten fazla uzmanın kontraseptif uygunluk kriterleri rehberini geliştirmesi 1-4 Nisan İsviçre 23 Ülke 43 Uzman en son revizyon 2010 da CDC nin WHO kriterlerini ABD için uyarlaması

8
Uzman çalışma grubunun kontraseptif uygunluk kriterlerini geliştirirken göz önünde bulundurduğu kaynaklar 1. Medline, Premedline, Popline ve /veya benzeri bibliyografik databaseler 'dan 2008'e kadar yayınlanmış ve tekrar değerlendirilmiş yayınlar 3. Raporlanmış verilerin sistematik olarak tekrar değerlendirilmiş çalışmaları veya metaanalizleri (spesifik sağlık durumunda olan kadınların kontraseptif yöntem kullanımı ile ilgili sağlık durumundaki değişmeleri gösteren çalışmaların metaanalizi)
")
9
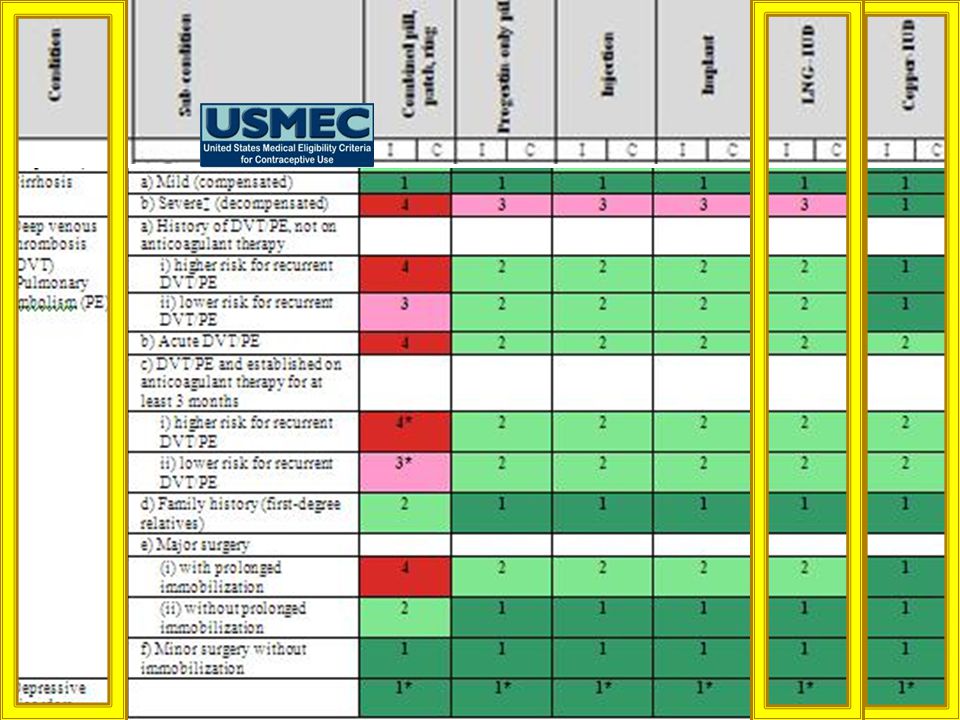
DSÖ KATEGORİLERİ 1.Kategori: Güvenle kullanılabilir-yöntem kullanımı
için hiçbir sınırlama yok 2.Kategori:Kullanılabilir- yöntem kullanımının olumlu yönleri, genel olarak teorik ve kanıtlanmış risklerden fazla (kararda diğer yöntem seçeneklerinin varlığı ya da izlem sıklığına dikkat edilmeli) 3.Kategori:İlk seçenek değil -teorik ve kanıtlanmış riskler genel olarak olumlu yönlerinden fazla (karar diğer seçeneklerin varlığı/ulaşılabilirliği, yakın izleme olanakları ve durumun şiddeti değerlendirilerek verilmeli) 4.Kategori:Kullanılmamalı- kabul edilemez sağlık riski
 3.Kategori:İlk seçenek değil -teorik ve kanıtlanmış riskler genel olarak olumlu yönlerinden fazla (karar diğer seçeneklerin varlığı/ulaşılabilirliği, yakın izleme olanakları. ve durumun şiddeti değerlendirilerek verilmeli) 4.Kategori:Kullanılmamalı- kabul edilemez sağlık riski.")
11
KİMLER BAKIRLI RAHİM İÇİ ARAÇ KULLANABİLİR
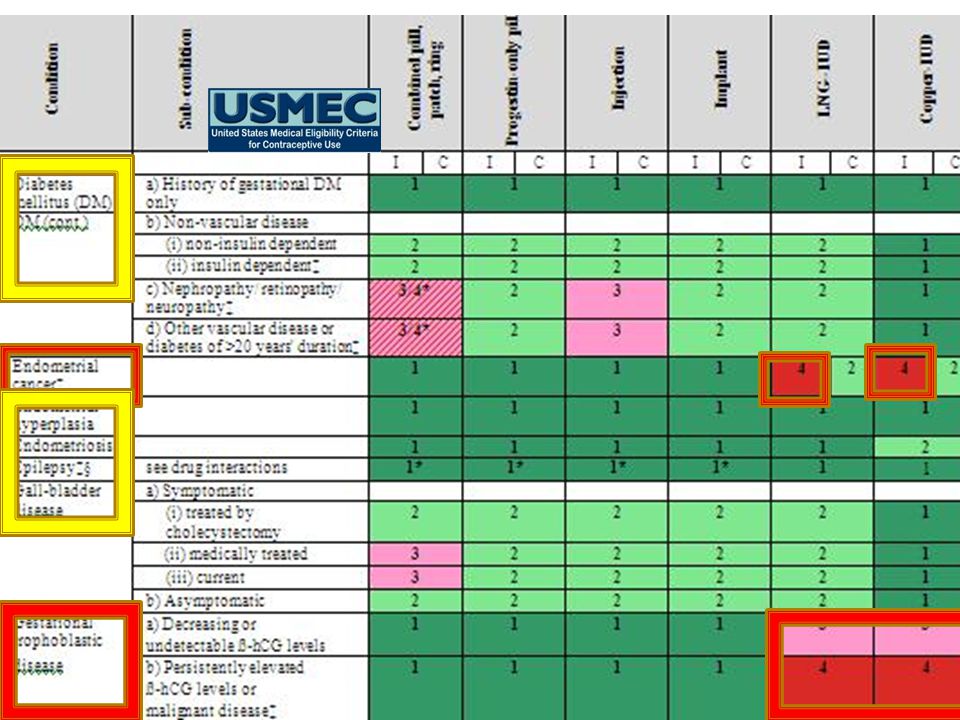
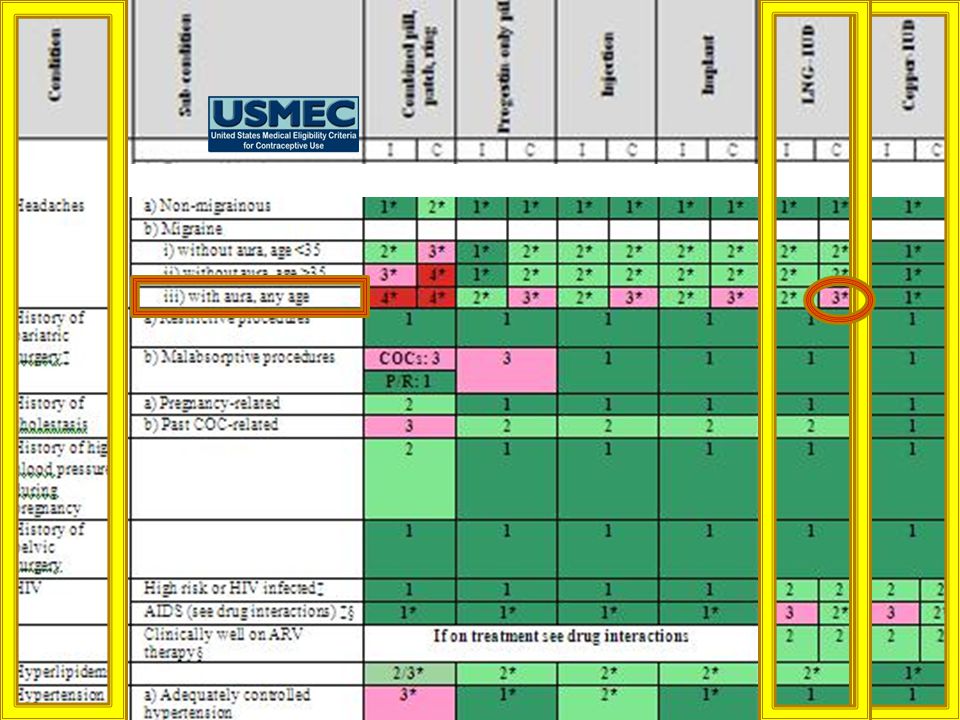
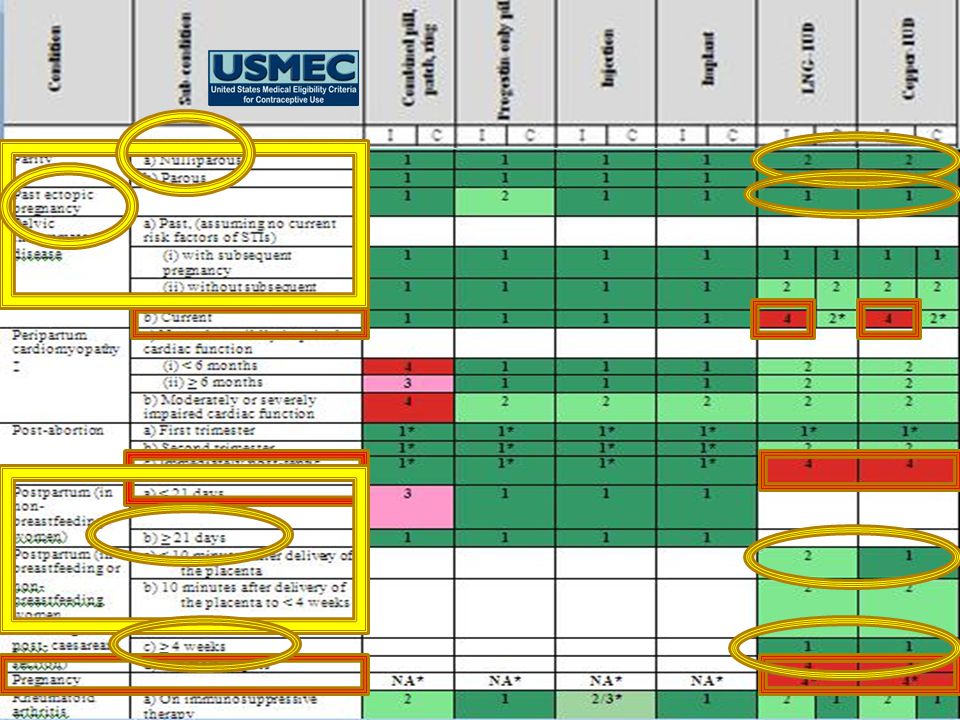
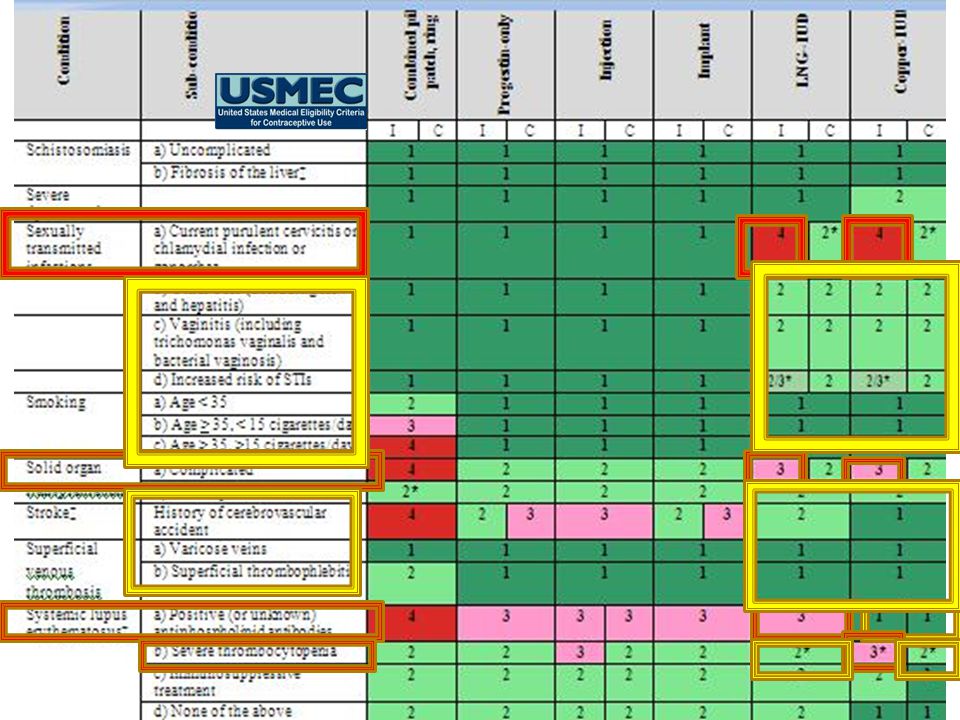
WHO Category Conditions Category 1 ≥20 yaş , hipertansiyon, derin ven trombozu, iskemik kalp hastalığı, migren,meme hastalıkları(meme kanseri dahil) EKTOPİK GEBELİK GEÇİREN , SERVİKAL EKTOPİ MENARŞ <20 YAŞ, NULLİPAR, POSTPARTUM <48 SAATTEN ÖNCE, UZAMIŞ VE ŞİDDETLİ KANAMA, ŞİDDETLİ DİSMENORE,KAVİTEYİ DİSTORSİYONA UĞRATMAYAN MYOMLAR, ENDOMETRİOZİS, ANEMİ, ESKİ PID,YÜKSEK HIV RİSKİ Category 2 The IUD is safe for the overwhelming majority of women. The MEC identifies a number of medical conditions that do not prohibit IUD use. █ According to the MEC, the IUD can be used without any restrictions by women with category 1 conditions. For example, the IUD can be used freely by women who are older than 20 years, have hypertension, deep venous thrombosis, current or history of ischemic heart disease, migraine headaches, cervical ectopy, or breast disease, including breast cancer. █ For women with category 2 conditions, the advantages of using the method outweigh the theoretical or proven risks. Thus, the IUD can generally be used by women with category 2 conditions, but careful follow-up may be required in some cases. Examples of such conditions include being younger than 20 years, never giving birth or nulliparous, being within 48 hours postpartum, heavy or prolonged bleeding patterns, severe dysmenorrhea, endometriosis, iron deficiency and sickle cell anemia, and at high risk of becoming HIV-infected. In settings where clinical judgment is limited, category 2 conditions are treated in the same manner as category 1 conditions, meaning that women with either category 1 or 2 conditions should be able to obtain and use an IUD without restrictions.22 █ Discussion questions: Use the MEC quick reference chart (included with the course materials) to find: Other Category 1 conditions that are not included in this slide (e.g., smoking, non-migrainous headaches, superficial thrombophelitis, diabetes, malaria, non-pelvic tuberculosis (TB), thyroid disease, known hyperlipidemias, uterine fibroids without cavity distortion, irregular bleeding patterns without heavy bleeding, cirrhosis, gall bladder disease, cholestasis, hepatitis, liver tumors, and use of antibiotics) Other Category 2 conditions that are not included in this slide (e.g., complicated valvular heart disease; continued use with cervical, endometrial, or ovarian cancer; continued use with unexplained vaginal bleeding; initiate use with increased risk and some STIs; continued use with all STIs/PID, HIV-infected; and continued use with AIDS or on ARV therapy). Remind participants that the quick reference chart is not a comprehensive listing of all the conditions that WHO has categorized. Participants can review the WHO guidelines for a comprehensive list and explanations. Reference: 22. World Health Organization (WHO). Medical Eligibility Criteria for Contraceptive Use. Third Edition. Geneva: WHO, 2004. Source: WHO, 2004. February Adapted from Contraception for Clients with HIV
 EKTOPİK GEBELİK GEÇİREN , SERVİKAL EKTOPİ. MENARŞ <20 YAŞ, NULLİPAR, POSTPARTUM <48 SAATTEN ÖNCE, UZAMIŞ VE ŞİDDETLİ KANAMA, ŞİDDETLİ DİSMENORE,KAVİTEYİ DİSTORSİYONA UĞRATMAYAN MYOMLAR, ENDOMETRİOZİS, ANEMİ, ESKİ PID,YÜKSEK HIV RİSKİ. Category 2. The IUD is safe for the overwhelming majority of women. The MEC identifies a number of medical conditions that do not prohibit IUD use. █ According to the MEC, the IUD can be used without any restrictions by women with category 1 conditions. For example, the IUD can be used freely by women who are older than 20 years, have hypertension, deep venous thrombosis, current or history of ischemic heart disease, migraine headaches, cervical ectopy, or breast disease, including breast cancer. █ For women with category 2 conditions, the advantages of using the method outweigh the theoretical or proven risks. Thus, the IUD can generally be used by women with category 2 conditions, but careful follow-up may be required in some cases. Examples of such conditions include being younger than 20 years, never giving birth or nulliparous, being within 48 hours postpartum, heavy or prolonged bleeding patterns, severe dysmenorrhea, endometriosis, iron deficiency and sickle cell anemia, and at high risk of becoming HIV-infected. In settings where clinical judgment is limited, category 2 conditions are treated in the same manner as category 1 conditions, meaning that women with either category 1 or 2 conditions should be able to obtain and use an IUD without restrictions.22 █ Discussion questions: Use the MEC quick reference chart (included with the course materials) to find: Other Category 1 conditions that are not included in this slide (e.g., smoking, non-migrainous headaches, superficial thrombophelitis, diabetes, malaria, non-pelvic tuberculosis (TB), thyroid disease, known hyperlipidemias, uterine fibroids without cavity distortion, irregular bleeding patterns without heavy bleeding, cirrhosis, gall bladder disease, cholestasis, hepatitis, liver tumors, and use of antibiotics) Other Category 2 conditions that are not included in this slide (e.g., complicated valvular heart disease; continued use with cervical, endometrial, or ovarian cancer; continued use with unexplained vaginal bleeding; initiate use with increased risk and some STIs; continued use with all STIs/PID, HIV-infected; and continued use with AIDS or on ARV therapy). Remind participants that the quick reference chart is not a comprehensive listing of all the conditions that WHO has categorized. Participants can review the WHO guidelines for a comprehensive list and explanations. Reference: 22. World Health Organization (WHO). Medical Eligibility Criteria for Contraceptive Use. Third Edition. Geneva: WHO, Source: WHO, February 2008 Adapted from Contraception for Clients with HIV.")
12
KİMLER RAHİM İÇİ ARAÇ KULLANAMAZ
WHO Category Conditions Category 3 postpartum 48 saat <4 hafta, ovarian kanser/yeni RİA uygulanacak, benign trofoblastik hastalık, yüksek gonore ,klamidya riski,HIV ARV ye yanıtsızsa Category 4 gebelik; postpartum/postabortif sepsis; uygulama öncesi açıklanmayan vaginal kanama ; kaviteyi distorsiyona uğratan myomlar; uygulama zamanı PID; purulan servisit; endometriyal veya servikal kanser veya uygulama öncesi pelvik tuberkuloz While the IUD is safe for the majority of women, a small number of women with certain characteristics or certain medical conditions are not considered good candidates for IUD use. █ According to the MEC, the IUD is not generally recommended for women with category 3 conditions, when theoretical or proven risks usually outweigh the advantages of using the method. Some examples of these conditions include: being between 48 hours and 4 weeks postpartum; ovarian cancer for initiation only – women who develop ovarian cancer while using the IUD can continue using it while awaiting treatment; benign gestational trophoblast disease, high individual risk of STIs; and AIDS in cases where ARV therapy is not available or the woman is not clinically well while on ARVs. Women with these conditions should not use the IUD unless other more appropriate methods are not available or acceptable. Careful follow-up will be required. █ Women with category 4 conditions should not initiate IUD use because of unacceptable health risk. Examples of such conditions include: pregnancy; postpartum or postabortion sepsis; unexplained vaginal bleeding, prior to evaluation; uterine fibroids with cavity distortion; current PID; purulent cervicitis; endometrial or cervical cancer or pelvic tuberculosis for initiation only – women who develop endometrial or cervical cancer or pelvic tuberculosis while using the IUD can continue using it while awaiting treatment. In settings where clinical judgment is limited, category 3 conditions are treated in the same manner as category 4 conditions, meaning that women with either category 3 or 4 conditions should not initiate and use the IUD.23 █ Discussion questions: Use the MEC quick reference chart (included with the course materials) to find: Other Category 3 conditions that are not included in this slide (e.g., pelvic tuberculosis if the woman develops the condition while using the IUD) Other Category 4 conditions that are not included in this slide (e.g., malignant gestational trophoblast disease) Remind participants that the quick reference chart is also not a comprehensive listing of all the conditions that WHO has categorized. Participants can review the WHO guidelines for a comprehensive list and explanations. Reference: 23. World Health Organization (WHO). Medical Eligibility Criteria for Contraceptive Use. Third Edition. Geneva: WHO, 2004. Source: WHO, 2004. . World Health Organization (WHO). Medical Eligibility Criteria for Contraceptive Use. Third Edition. Geneva: WHO, 2004. February Adapted from Contraception for Clients with HIV
 to find: Other Category 3 conditions that are not included in this slide (e.g., pelvic tuberculosis if the woman develops the condition while using the IUD) Other Category 4 conditions that are not included in this slide (e.g., malignant gestational trophoblast disease) Remind participants that the quick reference chart is also not a comprehensive listing of all the conditions that WHO has categorized. Participants can review the WHO guidelines for a comprehensive list and explanations. Reference: 23. World Health Organization (WHO). Medical Eligibility Criteria for Contraceptive Use. Third Edition. Geneva: WHO, Source: WHO, World Health Organization (WHO). Medical Eligibility Criteria for Contraceptive Use. Third Edition. Geneva: WHO, February 2008 Adapted from Contraception for Clients with HIV.")
13
Nullipar Kadınlarda RİA Kullanımı
Tubal infertilitede artma yok PID’de artma yok Gebelik oranları aynı %1 in altında Atılma oranları yakındır %2-3 Kanama ve ağrı nedeniyle çıkarılma oranları yakındır. DOĞUM YAPMAMIŞ KADINLAR GÜVENLE KÜLLANABİLİR (DSÖ KATEGORİ 2) Adv Contraception 1991, J Clin Epidemiology 1991,Contraception 1996
 Adv Contraception 1991, J Clin Epidemiology 1991,Contraception")
15
RİA uygulama zamanı INTERVAL UYGULAMA
Gebelik kuşkusu dışında siklusun herhangi bir günü uygulanabilir. Uygulamanın 5 gün öncesine kadar gebelikten koruyacaktır. An interval insertion can be performed anytime during the menstrual cycle, as long as the woman is not pregnant. Some providers recommend the IUD be inserted during the last few days of menstruation when the cervical opening is a little larger than usual and it is certain the woman is not pregnant. However, it is easier to examine for signs of reproductive tract infections when a women is not menstruating. Therefore, IUDs can be inserted at the client’s convenience if the provider can be reasonably sure she is not pregnant. █ An IUD can be inserted postpartum. This assumes the provider has received adequate training in the procedure, the woman has been counseled appropriately prior to delivery, and there is no infection or bleeding. The IUD can be placed manually in the uterus immediately after a cesarean section delivery or a vaginal delivery. An IUD insertion following a vaginal delivery can be done during the first 10 minutes after delivery of the placenta. Early postpartum insertions within the first 48 hours are also considered safe. Otherwise, it is best to wait until the woman is four to six weeks postpartum, when the uterus returns to its normal size. █ An IUD can be inserted immediately after a first-trimester abortion if there is no infection. However, if the pregnancy was 16 weeks or more, IUD insertion should be performed by a specially trained provider or be delayed for six weeks.24 █ Reference: 24. World Health Organization (WHO). Selected practice recommendations for contraceptive use. Second Edition. Geneva: WHO, 2004. Source: WHO, 2004 February Adapted from Contraception for Clients with HIV
. Selected practice recommendations for contraceptive use. Second Edition. Geneva: WHO, Source: WHO, February 2008 Adapted from Contraception for Clients with HIV.")
18
RİA Kullanım Kriterleriyle İlgili Diğer Durumlar
Uterin kaviteyi distorsiyona uğratmayan myomlar RİA kullanımına engel değildir. BU KRİTERLER HORMON İÇEREN RİA’LAR İÇİN DE GEÇERLİDİR.

24
Postpartum RİA Uygulaması
[Insert Lecture Name Here] Postpartum RİA Uygulaması KANITA DAYALI TIP Postpasental 10 dakika içinde tercih edilir Postpartum 48 saat içinde uygulanabilir 48 saat-4 hafta içinde uygulanmaz. 4 hafta sonra mens. olmadan da güvenle uygulanır 47. EROGLU, K., AKKUZU, G., VURAL, G., DILBAZ, B., AKIN, A.,TASKIN, L., and HABERAL, A. Comparison of effi cacy and complications of IUD insertion in immediate postplacental/ early postpartum period with interval period: 1 year followup. Contraception 74(5): Nov 59. GRIMES, D., SCHULZ, K., VAN VLIET, H., and STANWOOD, N. Immediate post-partum insertion of intrauterine devices. Cochrane Database of Systematic Reviews (2): CD 2001. Talking Points: Many clinicians postpone insertion of intrauterine contraception until 12 weeks postpartum because of concerns that earlier insertion may lead to higher rates of expulsion and more complications. However, copper T IUDs may be inserted safely as early as 4 weeks postpartum. Some suggest that the IUD may be safely inserted immediately after delivery of the placenta. Immediate postpartum insertion provides an opportunity for women to secure effective contraception at a convenient time. Early postpartum insertion—between 48 hours and 4 weeks postpartum—is associated with a higher rate of expulsion and perforation and is not generally recommended. Package labeling recommends that IUDs should not be inserted until involution of the uterus is complete. References: Treiman K, Liskin L, Kols A, Rinehart W. IUDs—an update. Population Reports, Series B, no. 6. Baltimore, MD: Population Information Program, Johns Hopkins University; 1995. Mishell DR Jr, Roy S. Am J Obstet Gynecol. 1982;143:29. [TITLE NEEDED] Morrison C, Waszak C, Katz K, et al. Clinical outcomes of two early postpartum IUD insertion programs in Africa. Contraception. 1996;53(1):17-21. Darney PD. In: Intrauterine Contraception in the US: A Current Perspective. Conference Proceedings. 1996;37. Manufacturer’s prescribing information. Kennedy KI, Trussell J. Postpartum contraception and lactation. In: Hatcher RA, Trussell J, Stewart F, et al., eds. Contraceptive Technology. 18th revised ed. New York: Ardent Media; 2004. Treiman K, et al. Population Reports. 1995; Mishell DR, et al. Am J Obstet Gynecol. 1982; Kennedy KI, et al. In Hatcher RA, et al. Contraceptive Technology. 18th revised ed
: Nov GRIMES, D., SCHULZ, K., VAN VLIET, H., and STANWOOD, N. Immediate post-partum insertion of intrauterine devices. Cochrane Database of Systematic Reviews (2): CD Talking Points: Many clinicians postpone insertion of intrauterine contraception until 12 weeks postpartum because of concerns that earlier insertion may lead to higher rates of expulsion and more complications. However, copper T IUDs may be inserted safely as early as 4 weeks postpartum. Some suggest that the IUD may be safely inserted immediately after delivery of the placenta. Immediate postpartum insertion provides an opportunity for women to secure effective contraception at a convenient time. Early postpartum insertion—between 48 hours and 4 weeks postpartum—is associated with a higher rate of expulsion and perforation and is not generally recommended. Package labeling recommends that IUDs should not be inserted until involution of the uterus is complete. References: Treiman K, Liskin L, Kols A, Rinehart W. IUDs—an update. Population Reports, Series B, no. 6. Baltimore, MD: Population Information Program, Johns Hopkins University; Mishell DR Jr, Roy S. Am J Obstet Gynecol. 1982;143:29. [TITLE NEEDED] Morrison C, Waszak C, Katz K, et al. Clinical outcomes of two early postpartum IUD insertion programs in Africa. Contraception. 1996;53(1): Darney PD. In: Intrauterine Contraception in the US: A Current Perspective. Conference Proceedings. 1996;37. Manufacturer’s prescribing information. Kennedy KI, Trussell J. Postpartum contraception and lactation. In: Hatcher RA, Trussell J, Stewart F, et al., eds. Contraceptive Technology. 18th revised ed. New York: Ardent Media; Treiman K, et al. Population Reports. 1995; Mishell DR, et al. Am J Obstet Gynecol. 1982; Kennedy KI, et al. In Hatcher RA, et al. Contraceptive Technology. 18th revised ed")
25
Postabortif RİA uygulaması
[Insert Lecture Name Here] Postabortif RİA uygulaması KANITA DAYALI TIP Spontan düşük veya rahim tahliye sonrası RİA uygulanması güvenlidir RİA uygulaması septik abortus sonrası önerilmez Talking Points: Intrauterine contraception may be safely inserted immediately after spontaneous or induced abortions of a routine nature. Event rates following first-trimester terminationexpulsion, pregnancy, and removals for medical reasonsare comparable to those found in studies in which the device was inserted during or immediately after menses. The shorter the period of gestation at the time of spontaneous or induced abortion, the lower the event rates after IUD insertion. Insertion of a copper T IUD is contraindicated after septic abortion. Package labeling for ParaGard recommends that insertion of a copper T IUD be delayed until involution of the uterus is complete. References: Grimes D, et al. Cochrane Library. 2000;4:2. [FIRST 3 AUTHORS AND TITLE NEEDED] World Health Organization Task Force on Intrauterine Devices for Fertility Regulation, Special Programme of Research, Development and Research Training in Human Reproduction. Stud Fam Plann. 1983;14:99. Manufacturers’ prescribing information. Grimes D, et al. Cochrane Library

27
Rahim İçi Araçlar CYBH veya PID Tedavisi Süresince Çıkartılmayabilir
Tedavi başarı ile sonuçlandığı sürece RİA’nın çıkarılması veya yerinde kalması süreci etkilememektedir. Ayrıca sifiliz ve herpes gibi ülseratif hastalıklar da dahil CYBH’larda RİA kullanımına başlanabilir. Sadece klamidya ve gonore veya pürülan servisitte RİA kullanımına başlanamaz. CYBH:Cinsel Yolla Bulaşan Hastalıklar

29
TEŞEKKÜR EDERİM

Benzer bir sunumlar