Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
HİPOVOLEMİK HASTAYA YAKLAŞIM VE SIVI TEDAVİSİ
Dr.Enver İNCE ANKARA UMKE

2
ÖĞRENİM HEDEFLERİ ŞOKU TANIMLAYABİLMEK ŞOK ÇEŞİTLERİNİ BİLMEK
FİZYOPATOLOJİSİNİ BİLMEK TEDAVİSİNİNDE UYGULANACAK İLAÇ VE SIVILARI BİLMEK ANJİOKETLERİ TANIMAK

3
Şok HÜCRE ÖLÜMÜ Yetersiz Doku Perfüzyonu
Hücrelerin Metabolik Gereksinimi Karşılanamaz Hücre Membran İşlevleri Bozulur HÜCRE ÖLÜMÜ

4
Şok Tipleri Hipovolemik Şok Kardiyojenik Şok Distrübitif Şok

5
Doku Perfüzyonunun Belirleyicileri
Kan hacmi Kalp dolma basıncı (Preload) Miyokard kontraktilitesi Afterload Kalp atım hacmi Kalp atım hızı Kalp debisi Periferik vasküler direnç Sistemik arteriyal kan basıncı Doku vasküler direnci Doku kapiller yatağının durumu DOKU PERFÜZYONU
 Miyokard kontraktilitesi. Afterload. Kalp atım hacmi. Kalp atım hızı. Kalp debisi. Periferik vasküler direnç. Sistemik arteriyal kan basıncı. Doku vasküler direnci. Doku kapiller yatağının durumu. DOKU PERFÜZYONU.")
6
Hipovolemik Şok Nedenler Ani ve Aşırı Kanama Aşırı Sıvı Kayıpları
Ağır GİS Kanamaları Travmatik Dış Kanamalar Aort Anevrizması Yırtılması Retroperitoneal Kanamalar … Geniş Yanıklar Aşırı Kusma ve İshal (Peritonit, Pankreatit, İntestinal Obstrüksiyon)
")
7
Periferik Vasküler Direnç
Hipovolemik Şok Efektif Kan Hacmi Periferik Vasküler Direnç Beyin Kalp Deri Splanknik Böbrek Kan Akımı Kan Akımı

8
Hipovolemik Şok İntravasküler Hacim Sempatik Hiperaktivite
PVR Miyokard Kontraktilitesi Venöz Dönüş Atım Hacmi Kalp Debisi Kan Basıncı Kontrol Altına Alınır Miyokardın O2 Tüketimi Artar

9
Hipovolemik Şok Dolaşan Kan Hacmi Kapiller Hidrostatik P
İnterstisyel Sıvı Kapiller Alana Geçer Kan Vizkozitesi Kan Hacmi

10
Protein Katabolizması
Hipovolemik Şok Kan Hacmi Katekolaminler Vazokonstrüksiyon Taşikardi Kalp Debisi Kan Basıncı Glukojenoliz Lipoliz Kan Yıkımı İnsülin Glukoz Mobilizasyonu Protein Katabolizması (-) Nitrojen Dengesi
 Nitrojen Dengesi.")
11
Hipovolemik Şok Hücrede Anabolik Metabolizma Laktik Asit (Asidoz)
Hemoglobin O2 Affinitesi Hipoksi Hiperventilasyon (Resp. Asidoz) Eritrositte 2,3 DPG Sentezi Hemoglobin O2 Affinitesi O2 Dokuya Bırakılır
 Eritrositte 2,3 DPG Sentezi Hemoglobin O2 Affinitesi O2 Dokuya Bırakılır.")
12
Arteriyal Vazokonstrüksiyon
Hipovolemik Şok Arteriyal Vazokonstrüksiyon Dolaşan Kan Hacmi Renal Kan Akımı İdrar Miktarı Na, H2O Tutulumu

13
Sıvı Tedavisi Hangi Hastaya ? Nerede ? Hangi Yolla ? Hangi Sıvıları ?
Ne Zamana Kadar ? Gelecek ?

14
Hangi Hastaya ? “ Aksi İspatlanmadıkça Hipotansiyonu Olan Bir Travma Hastasında Hemoraji Olduğu Düşünülmelidir.”

19
Hangi Hastaya ? Yaralanmanın Tipi KÜNT PENETRAN
İnternal veya Kontrol Edilemeyen Bir Kanama Varsa Hasta Hızla Değerlendirmeli ve Kesin Cerrahi İçin Sevk Edilmelidir.

20
Hangi Hastaya ? Kontrol Altına Alınabilecek Kanamalarda
(İzole Ekstremite Yaralanmaları) Dolaşım Bozukluğu Gösteren Yaralanmalarda KÜNT YA DA PENETRAN TRAVMA OLDUĞUNA BAKILMAKSIZIN HIZLA SIVI İNFÜZYONUNA BAŞLANMALIDIR
 Dolaşım Bozukluğu Gösteren Yaralanmalarda. KÜNT YA DA PENETRAN TRAVMA OLDUĞUNA BAKILMAKSIZIN HIZLA SIVI İNFÜZYONUNA BAŞLANMALIDIR.")
21
Hangi Hastaya ? Penetran Travmalarda;
Nabız Alınamıyor, Bilinç Kaybı gibi terminal dönem bulguları var ise hızlı sıvı infüzyonuna başlanmalıdır. Aksi takdirde, özellikle penetran gövde yaralanmalarında sıvı kısıtlamasına gidilmelidir

22
Hangi Hastaya ? Künt travmalı hastalarda tabloya özellikle şiddetli kafa travması eşlik ediyorsa klinik bulgulara göre perfüzyon devamlılığını sağlayacak kadar sıvı infüzyonu yapılmalıdır. (serebral-pulmoner ödem ve sekonder hemoraji riski)
")
23
“Kontrollü hipotansiyon”
Cerrahi olarak kanamanın kesin kontrolü sağlanana kadar penetran gövde yaralanmalarında faydalı olabilir

24
Nerede ?

25
Nerede ? Alanda.. Ambulansta.. Acil Serviste.. Ameliyathanede..

26
Hangi Yolla ?

27
Kateter Çapı Değişik ülkelerde üretilen kateterler için değişik numaralandırma sistemleri geliştirilmiştir. Çap büyüdükçe dakikada verilebilecek sıvı miktarı artar

28
Intravenöz Kateter Yerleştirme Endikasyonları
Her hangi bir anstabil veya potansiyel olarak anstabil olan bir hastaya Hızla tıbbi tedavi uygulayabilmek, İntravasküler Volümü Sağlayabilmek, Kan Transfüzyonu uygulayabilmek.

29
Hangi Sıvıları ?

30
Ortalama Kan Hacmi Erişkin Tüm Vücut Ağırlığının % 7 70cc/kg
( 70kg x 70cc/kg = 4900cc) Çocuk cc/kg Yenidoğan cc/kg If your going to resuscitate someone for hemorrhagic it’s go to be able to estimate their normal blood volume.
 Çocuk 80 cc/kg. Yenidoğan 90 cc/kg. If your going to resuscitate someone for hemorrhagic it’s go to be able to estimate their normal blood volume.")
31
Seçenekler (I) Kristaloidler 0.9 % SF (150 mmol/l NaCL) 5 % Dekstroz
0.18 % SF % Dekstroz Diğer Therapeutic fluids that we prescribe for intravenous administration, can be divided into 2 basic types. Crystalloids are simple solutions of small solutes, whilst colloids are suspensions of macromolecules, or in the case of blood, cells. The most commonly used crystalloids are saline and dextrose, where the dissolved solutes are sodium-chloride and glucose respectively. The standard saline solution is 0.9% saline, often referred to as " normal saline ", which contains 150 mmol/l of NaCl, and is therefore not normal, being slightly hypertonic, and hypernatraemic. Dextrose is usually given as 5% dextrose, which means that it contains 5 grams of glucose per 100 ml of water. This solution is roughly isotonic to serum, but the glucose is rapidly utilised, leaving behind pure water. A host of other crystalloids exist and are beyond the scope of these notes. Multiple colloid preparations are available, but the essential ones are either natural, such as blood, human albumin or plasma, or synthetic, where the macromolecule is manufactured. Common synthetic colloids are " haemaccel "and " gelofusine ", in which hydrolysed gelatin is suspended in saline.

32
Seçenekler (II) Kolloidler Haemaccel Gelofusine Kan Plazma / Albumin
Sentetik Ürünler Haemaccel Gelofusine Therapeutic fluids that we prescribe for intravenous administration, can be divided into 2 basic types. Crystalloids are simple solutions of small solutes, whilst colloids are suspensions of macromolecules, or in the case of blood, cells. The most commonly used crystalloids are saline and dextrose, where the dissolved solutes are sodium-chloride and glucose respectively. The standard saline solution is 0.9% saline, often referred to as " normal saline ", which contains 150 mmol/l of NaCl, and is therefore not normal, being slightly hypertonic, and hypernatraemic. Dextrose is usually given as 5% dextrose, which means that it contains 5 grams of glucose per 100 ml of water. This solution is roughly isotonic to serum, but the glucose is rapidly utilised, leaving behind pure water. A host of other crystalloids exist and are beyond the scope of these notes. Multiple colloid preparations are available, but the essential ones are either natural, such as blood, human albumin or plasma, or synthetic, where the macromolecule is manufactured. Common synthetic colloids are " haemaccel "and " gelofusine ", in which hydrolysed gelatin is suspended in saline.

33
SERUM GLİKOZE % 5 5 % Glukoz (Su İçinde) 50 Gram / litre
200 Kalori / litre pH 4.5 252 mOsm / litre

34
hypernatremic & hyperchloremic
NORMAL SALİN, % 0.9 SALİN - NS 154 meq / litre Na 154 meq / litre Cl 308 mOsm / litre pH 4 – 5 Serbest Su Desteği Yok hypernatremic & hyperchloremic

35
RİNGER LAKTAT - LR 130 meq / litre Na 28 meq / litre laktat
109 meq / litre Cl 4.0 meq / litre K 3.0 meq / litre Ca 28 meq / litre laktat 273 mOsm / litre pH Ek Olarak 100 cc su / litre

36
Şok Resüsitasyonu Kristaloidler Kolloidler Hipertonik Salin Kan
Kan Ürünleri Most of this talk will be about resuscitation, and I'll also talk about the resuscitation fluid that we have in the field which the Air Force is currently carrying with the mobile field surgical team, and I'll also talk briefly about some of the new blood substitutes that we're looking at. One is in a clinical trial here. There are a couple out there -- one has already been taken off the market for an increased mortality in some patients -- and so we'll talk a little bit about those and where we're going with those, and some of these things that you don't use in your daily setting and we don't use here (hypertonic saline), but they're perfectly safe. It's a smaller volume to carry into the forward environment, and they can be used and have been used in shock before.
, but they re perfectly safe. It s a smaller volume to carry into the forward environment, and they can be used and have been used in shock before.")
37
Hangi Sıvıları ? EVRE I Tedavi Kristaloid (3:1) IV
Kan Kaybı < 750 cc % TKV Kaybı SSS Semptomları Hafif Anksiyöz Sistolik KB Normal Diastolik KB Normal Solunum Sayısı Nabız İdrar Çıkışı (ml/saat) 30 EVRE I Tedavi Kristaloid (3:1) IV
 30. EVRE I. Tedavi Kristaloid (3:1) IV.")
38
Hangi Sıvıları ? EVRE II Kan Kaybı 750-1500 cc % TKV Kaybı 15 -30
SSS Semptomları Ilımlı Anksiyöz Sistolik KB Normal Diastolik KB Solunum Sayısı Nabız > 100 İdrar Çıkışı (ml/saat) cc/saat EVRE II Tedavi Kristaloid (3:1) IV / Kan ?
 cc/saat. EVRE II. Tedavi Kristaloid (3:1) IV / Kan")
39
Hangi Sıvıları ? EVRE III Kan Kaybı TKV Kaybı % 30 - 40
SSS Semptomları Konfüze, Anksiyete Sistolik KB Diastolik KB Solunum Sayısı Nabız > 120 İdrar Çıkışı (ml/saat) Tedavi Kristaloid (3:1) IV ve Kan
 Tedavi Kristaloid (3:1) IV ve Kan.")
40
Hangi Sıvıları ? EVRE IV Kan Kaybı > 2000 cc % TKV Kaybı > 40
SSS Semptomları Letharjik / Bilinçsiz Sistolik KB Diastolik KB Solunum Sayısı > 40 Nabız > 140 İdrar Çıkışı Çok Az Tedavi Hızlı Kristaloid (3:1) IV / Kan / Cerrahi
 IV / Kan / Cerrahi.")
41
Şok Resüsitasyonu Kristaloidler - İzotonik ESF’a hızlı geçer Ucuzdur
Hazır Bekletilir 3:1 Replasman Oranı Bolus - Erişkin 2 litre Çocuk 20cc/kg Gerekirse Tekrarlanabilir Crystalloids are kind of gold standard in a big hospital. They're isotonic, and they rapidly equilibrate with your extra-cellular fluid volume. How rapid? Well, after an hour, only about a third of that LR is still in the vascular space, and so the reason you're not catching up is, you're not giving it fast enough, and enough, with these patients who are in class III shock. When they are in shock, the rate of the equilibration is even faster because of a lot of capillary leaks in a bunch of organ systems, and so it's a good fluid, it's inexpensive, it's readily available, and that's why we have this three-to-one replacement ratio that the anesthesiologists came up with, for the most part, is that for every blood loss amount of a liter you should expect at least 3 liters of saline or LR to be required, but you'll find that it's probably even higher than that in a trauma setting. This is a general elective case where it tends to work out with the blood loss. Again, for adults we still bolus 2 liters if they're hypotensive here. I would be happy to talk at the end more about this. I always get questions about the limited resuscitation that Dr. Maddox has shown in his particular setting, and that may be very worthwhile, but in reality most of us do not have the same kind of EMS system that he has where the patient is deposited in the ER pretty quickly, and that will not be our situation in the field either. It may take them an hour or two to get to you, and not giving them any fluid may not be the best plan in that particular situation, but clearly, on new horizons we are learning that probably the aggressive fluid resuscitation we've done in the past may be a little bit overboard.

42
Hipertonik Salin 7.5 % ve 12 % NaCl
Hiperosmotiktir. İnterstisiyel alandan ve hücrelerden sıvıların intravasküler alana geçişini sağlar. Myokardiyal Kontraktiliteyi ve Katekölamin Seviyesini Artırır. Periferik Vazodilatasyon Yapar, Vagal Refleks ile Venokonstrüksiyonu artırır. İntrakraniyal Basıncı azaltır Hypertonic saline and shock -- I'll spend a little more time on this particular fluid. We actually carry it in the MFST. It comes at 7.5% or 12%, and actually 3% is what you see most of the time in your regular hospitals and what a lot of people are comfortable giving to the head injured patient who gets profound hyponatremia, but it does come in these higher concentrations and has been used in these higher concentrations specifically for trauma patients. It is very hyperosmotic and pulls fluid into the vascular space from cells in the interstitial space, so again, it's like the colloid. It's cheating the interstitial space, where you really may not have that much reserve, the difference is, this fluid tends to increase myocardial contractility and catecholamine levels, and the mechanism behind this is not completely obvious. It also results in some peripheral vasodilatation and some venoconstriction, and tends to decrease intracranial pressure. There is also a decreased priming of neutrophils in that selectin expression, going back to the whole neutrophil response to shock and how those intracellular adhesion molecules may set off cell death with shock, and there is a lot of work that's been looking at all of the different colloids and crystalloids, and which ones really prime our own inflammatory response, because we know our inflammatory response is doing some good for us, but it is actually doing a lot of harm as well. One of this fluid's most interesting characteristics is that it tends to decrease the priming of those cells and may increase survival long-term; again, no one's proven that, but that's kind of the theory, and especially as we're finding out that these things are more important in the whole pathophysiology of shock, it may be pretty interesting. It has been looked at in a very good fashion, a prospective randomized blinded trial in 200 trauma patients where their initial fluid again was this 7.5% or 12% hypertonic saline 250 cc, versus standard LR resuscitation for these patients.

43
Hipertonik Salin (HTS)
Prospektif ve Randomize , Çift Kör Çalışmada 200 Travma Hastası 250cc 7.5% or 12% hipertonik salin Sonuçlar Tüm Sağ Kalım LR 49% HTS 60% (NS) Kafa Travması Sağ Kalım LR 12% HTS 26% You can see that overall survival was a little improved with hypertonic saline, but that was not significant, but in head injured patients the survival was statistically significant, and again, this was a subset they took out at the end of the study, so there are always criticisms of that. However, clearly it was not harmful and these patients did quite well, and this again was used as their initial fluid on arrival, and then they proceeded with a standard resuscitation, but it has clearly been used before. It's safe; none of these patients had bad outcomes because of saline. In fact there were more survivors in all groups; it just didn't come out to statistical significance. So you'll have that, and we'll tell you exactly what the MFST has available in the field; you should feel comfortable giving it. What we carry is 3%, so it's going to be even less hypertonic than these, but clearly patients can tolerate hypertonic saline. The hypertonic saline was used as the initial resuscitation fluid in the field, the paramedics had both and they did not know which one was being given. When the patient arrived in the ED they were continued with a normal crystalloid resuscitation. While overall survival was not statistically significant the head injury survival was. I asked that the first time I revised this talk when I got here, and it really became, again, the comfort issue; no surgeons had ever really used that. There is a web site -- you know, you can always find everything on the web now You can go read all about all of the research that has been in Galveston and every study that has ever been done; there are approximately 12 of them out there, and none of them showed bad effects in the patients, but again it's a comfort issue and people want to give what they're used to giving at home. Question: Is it used here in the medical center? Dr. Mueller: No, we don't use it here in the medical center at all, even for head-injured patients. It's kind of interesting. It's out there, and it's probably a good thing, but again, people stick to the old tried and true, and especially with some of the literature on decreased resuscitation in the initial period. Hypertonic saline is going to increase your intravascular space significantly more than LR or saline, so it may depend on the particular injury, and if they have a complex of injuries, it may be worse Dr. Mueller: The remainder of that study was, they were in the hospital and got LR and normal saline. They were just trying to use their initial bolus as that and see what happened. Question: Would you bolus the same as you would, with 2 liters? Dr. Mueller: No, just the 250-cc aliquot, and wait for response. We'll talk about it when we talk about what the MFST has.
 Kafa Travması Sağ Kalım LR 12% HTS 26% You can see that overall survival was a little improved with hypertonic saline, but that was not significant, but in head injured patients the survival was statistically significant, and again, this was a subset they took out at the end of the study, so there are always criticisms of that. However, clearly it was not harmful and these patients did quite well, and this again was used as their initial fluid on arrival, and then they proceeded with a standard resuscitation, but it has clearly been used before. It s safe; none of these patients had bad outcomes because of saline. In fact there were more survivors in all groups; it just didn t come out to statistical significance. So you ll have that, and we ll tell you exactly what the MFST has available in the field; you should feel comfortable giving it. What we carry is 3%, so it s going to be even less hypertonic than these, but clearly patients can tolerate hypertonic saline. The hypertonic saline was used as the initial resuscitation fluid in the field, the paramedics had both and they did not know which one was being given. When the patient arrived in the ED they were continued with a normal crystalloid resuscitation. While overall survival was not statistically significant the head injury survival was. I asked that the first time I revised this talk when I got here, and it really became, again, the comfort issue; no surgeons had ever really used that. There is a web site -- you know, you can always find everything on the web now -- You can go read all about all of the research that has been in Galveston and every study that has ever been done; there are approximately 12 of them out there, and none of them showed bad effects in the patients, but again it s a comfort issue and people want to give what they re used to giving at home. Question: Is it used here in the medical center Dr. Mueller: No, we don t use it here in the medical center at all, even for head-injured patients. It s kind of interesting. It s out there, and it s probably a good thing, but again, people stick to the old tried and true, and especially with some of the literature on decreased resuscitation in the initial period. Hypertonic saline is going to increase your intravascular space significantly more than LR or saline, so it may depend on the particular injury, and if they have a complex of injuries, it may be worse. Dr. Mueller: The remainder of that study was, they were in the hospital and got LR and normal saline. They were just trying to use their initial bolus as that and see what happened. Question: Would you bolus the same as you would, with 2 liters Dr. Mueller: No, just the 250-cc aliquot, and wait for response. We ll talk about it when we talk about what the MFST has.")
44
Kan Transfüzyonu Ototransfüzyon O Negatif Kan Tipe Spesifik
Tipine Uygun ve Crossmatch yapılmış Göz Önüne Alınmalıdır : 2,3-DPG , Trombositopeni, Koagülasyon Defektleri, Potasyum Anormallikleri, Sitrat Toksisitesi, Hipokalsemi, Hipotermi, Enfeksiyon Riskleri Blood transfusions -- Well, obviously if you can autotransfuse blood, if you have that capability, you should do it. No more than 3 liters of that autotransfused blood should ever be given, because it can lead to significant coagulopathy. O-negative blood, again universal blood type, type specific is ten minutes to get here, type and cross match about an hour to an hour and a half on a bad day around here, which is almost every day. These things obviously are not going to really be available in the field, especially in the forward sites -- very limited blood capability. Things to remember about blood transfusions are the thrombocytopenia from massive transfusions and coagulation defects that exist, the hyperkalemia you can get into with multiple transfusions, hypocalcemia, hypothermia, and all of the infectious risks of blood products. Again, if a patient needs blood and if a patient is in class III shock defined by hypotension, they should get blood. They've lost 30-40% of their blood volume; you're just wasting time and possibly potentiating class IV shock before you treat then effectively, and so that's who gets emergency release blood from most of us downstairs, is obvious hypotension, because we already know where they are. Question: You said not to autotransfuse more than 3 units? Dr. Mueller: Three liters -- either from your chest tube evacuation or Cell Saver's. It is not recommended you ever give back more than 3 liters of that autotransfusable blood.

45
Ne Zamana Kadar ?

46
Monitorizasyon Mental durum ve konuşma Nabız, kan basıncı (Wo)
İdrar çıkışı Kapiller geri dolum / deri perfüzyonu CVP Laktat Seviyesi (Abramson)
")
47
İlk sıvı tedavisine yanıt
Hızlı yanıt Geçici yanıt Yanıt yok Vital bulgular Normale döner Geçici düzelme; tekrar KB düşer, nabız artar Anormal kalır Tahmin edilen kan kaybı Minimal (%10 - %20) Orta derece ve artan (%20 - %40) Ciddi (>%40) Daha fazla kristaloid ihtiyacı Düşük Yüksek Kan ihtiyacı Orta - yüksek Hemen Kan hazırlığı Gruba özgü ve kroslanmış Gruba özgü Acil kan verilmesi (0 Rh -) Cerrahi girişim ihtiyacı Belki Olasılıkla Büyük olasılıkla Cerrahi konsültasyon Evet
 Orta derece ve artan. (%20 - %40) Ciddi. (>%40) Daha fazla kristaloid ihtiyacı. Düşük. Yüksek. Kan ihtiyacı. Orta - yüksek. Hemen. Kan hazırlığı. Gruba özgü ve kroslanmış. Gruba özgü. Acil kan verilmesi. (0 Rh -) Cerrahi girişim ihtiyacı. Belki. Olasılıkla. Büyük olasılıkla. Cerrahi konsültasyon. Evet.")
48
Çocuklar İçin 24 Saatte Verilebilecek sıvı Miktarı(idame)
10 Kg Çocuk 100 cc / Kg 10 – 20 Kg Çocuk cc + 50 cc / Kg 20 – 30 Kg çocuk 1500 cc + 20 cc / Kg Erişkinler İçin 24 Saatte Verilebilecek sıvı Miktarı(idame) En Az 2 litre / 24 saat (1000 cc idrar cc insensible kayıp) Artmış İnsensible kayıp : 500 cc / 24 saat /Her derece F ateş ( cc / Santigrad Derece) 500 cc / 24 saat / Taşipne Diğer Sıvı Kayıpları da hesaplanıp eklenmelidir. (NG, drenler, diare, etc.)
 En Az 2 litre / 24 saat (1000 cc idrar cc insensible kayıp) Artmış İnsensible kayıp : 500 cc / 24 saat /Her derece F ateş ( cc / Santigrad Derece) 500 cc / 24 saat / Taşipne. Diğer Sıvı Kayıpları da hesaplanıp eklenmelidir. (NG, drenler, diare, etc.)")
51
Olarak Kanamayı Durdurmak
Şok’un Resüsitasyonu Cerrahi Olarak Kanamayı Durdurmak The most important thing in treating shock is to stop the bleeding.

52
Şok Resüsitasyonunu Sonlandırma Parametreleri
Kalp Hızı, Kan Basıncı,İdrar Çıkışı ve Bilinç Düzeyi Baz Defisiti Laktat Düzeyi Oksijen Akımı ve Tüketimi Gastrik Tonometri I'll talk very briefly about the endpoints of resuscitation and the differences. Clearly, here we have everything we could possibly imagine to figure out whether the patient is resuscitated or not, and we used a big reliance on laboratory values that you may or may not have in the field. Clearly, base deficit and the severity of your base deficit on arrival in a trauma center correlates with your likelihood of survival. Less than 5 means highly survivable usually. You get over 10, and most of those patients aren't going to make it out of here. So it kind of gives you a guide, tells you how far in shock. Many times the patient will look good, and we get the blood gas back and realize something's going on here, we just haven't figured it out yet. It's a very good guide to the lack of resuscitation that has happened or the severity of shock. We can use lactate; lactate takes a little bit longer to get back, may be inaccurate in some people with liver failure, but again a very good guide, and it has been shown that if you can improve your lactate and make it normal in 48 hours, most of those patients are going to survive. If it takes you longer than 72 hours to correct someone's lactate level after hemorrhagic shock, over 75% of those patients go on to die. So again, it's a guide to use for resuscitation that we can use here. Dr. Mueller: In the field, what are you going to have? You're going to have normal vital signs at the most, and one of the biggest ones will be responsiveness of the patient. In a setting where you're limited by fluids, you may elect not to give someone fluid initially, because you're just limited in what you have, but probably using mental status and whether they're responsive may be the best guide you have to whether you're keeping them at least resuscitated enough to make it through your little scenario. Again, here a Wilford Hall we have the ability to use oxygen delivery and consumption, and I think when Dave was here as a resident, we were doing all of this supernormalization of oxygen delivery and put Swans in everybody, making their hemoglobin 10, trying to get better oxygen delivery to the cells, and that was the big hot thing in trauma care and care for other patients. In reality, it has not been shown to increase survival in many populations, and actually in some of the elderly, has led to an increased myocardial infarction rate when dobutamine was added to increase their cardiac output, and so we still don't know the answer to this, and making people's oxygen delivery supernormal doesn't seem to make them survive a whole lot more, and so that's kind of fallen out of favor, but when many of you were residents, it may have been in. That's the only reason I touch on it here.

53
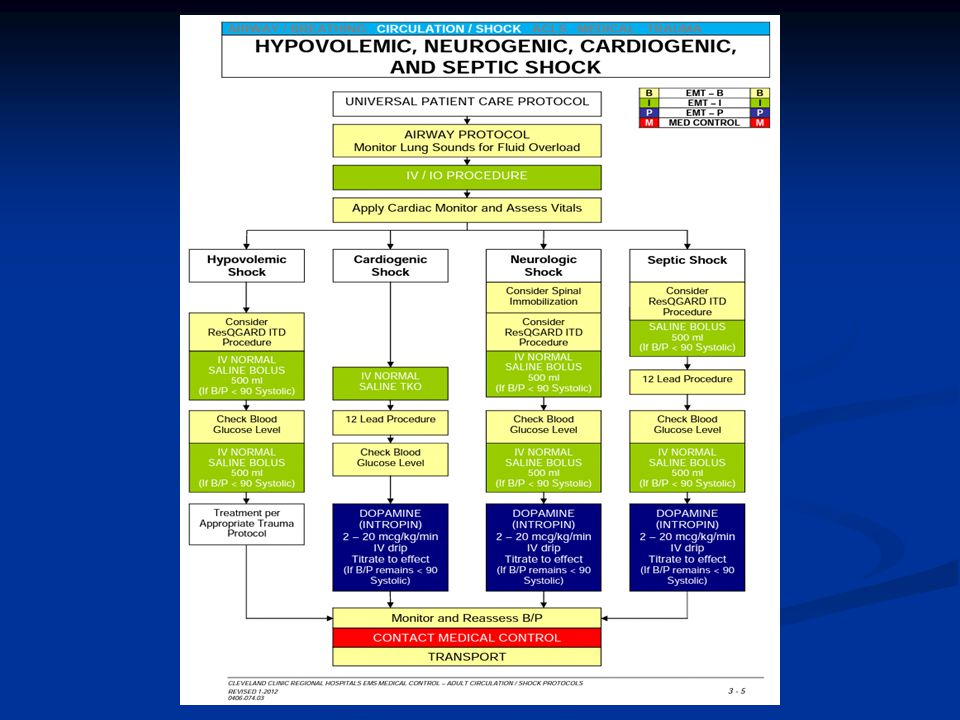
CLEVELAND EMS PROTOCOLS

Benzer bir sunumlar