Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Doç.Dr.Jale Çoban Clinical Enzymology AMAÇ:
Hangi doku hasarında hangi doku enzimlerinin hangi şartlara bağlı olarak kana diffüze oldukları ve kandaki düzeylerinin hangi anlama geldiğini kavramaktır. Fizyolojik şartlar ve hastalık durumunun iyi ayırt edilmesi ve kanda düzeyi değişen enzim veya enzimlerin değişme nedenlerini yorumlayabilmektir. Doç.Dr.Jale Çoban

2
GENERAL PROPERTIES OF ENZYMES
Enzyme Specificity Enzyme Concentration and Activity Molecular Basis for Enzyme Catalysis Nomenclature of Enzymes Isozymes Enzyme Cofactors Factors Affecting Plasma Enzyme Activities Factors Affecting the Lifetime of Enzymes in Blood

3
All enzymes are proteins and function as catalysts (accelerate the rates of chemical reactions in the body but do not become chemically altered themselves in these reactions). Enzymes lower the activation energies of the chemical reactions that they catalyze, so as to cause greatly enhanced rates of reaction. every reaction that occurs in the body, both intracellularly and extracellularly, is catalyzed by an enzyme.

4
Enzymes interact very specifically with their substrates (do not interact with any molecules other than their substrates). The lock and key model of substrate binding to the ezyme active site.

5
Nomenclature of Enzymes
Each enzyme has two names: a practical or trivial name, and a systematic name. The latter consists of a unique numeric code designation and the nature of the catalytic reaction, as follows: Enzymes are named by citing the name of the substrate molecule and by following that with the suffix, -ase; sometimes the name also includes a designation of the type of reaction catalyzed. Katalizlenen reaksiyonun doğasına göre ve özel sayısal kod . Enzimin etki ettiği substratın veya etki ettiği grup ismine ek bir –az

6
Canlıdaki hemen hemen tüm kimyasal reaksiyonlar özgün enzimler ile katalizlenmektedir. Bundan dolayı, yaşamın kendisi, birleşmiş enzimatik reaksiyonlar serisi; The concentrations and/or activities of different enzymes in blood give vital information about the functioning of specific tissues (enzymes can serve as biomarkers for diseases in specific tissues).
.")
7
Isozymes Many enzymes have isozymes- polypeptide chains that differ in sequence but have similar enzymatic activity. Different isoenzymes are found in specific organs or tissues; determination of the type of isoenzyme present can then be of use in identifying the damaged tissue and releasing the enzyme. Isoenzymes are those that are composed of varying combinations of subunits. Common examples are creatine kinase (CK), a dimer of muscle (M) and brain (B) subunits, and lactate dehydrogenase (LDH), a tetramer of heart (H) and (M) subunits. Isoenzymes may have the same protein component but may differ based on modifications made by the cell of origin. Bir enzimin çoklu formlarıdır. Aynı reaksiyonu katalizler, ancak farklı yapısal genlerden kodlandıklarından yapıları birbirinden farklıdır.
, a dimer of muscle (M) and brain (B) subunits, and lactate dehydrogenase (LDH), a tetramer of heart (H) and (M) subunits. Isoenzymes may have the same protein component but may differ based on modifications made by the cell of origin. Bir enzimin çoklu formlarıdır. Aynı reaksiyonu katalizler, ancak farklı yapısal genlerden kodlandıklarından yapıları birbirinden farklıdır.")
8
Enzyme Cofactors Two thirds of all enzymes contain cofactors.
They are low molecular weight organic molecules and inorganic ions. The combination of cofactor plus the protein portion (apoenzyme), forms the complete catalytic entity and is known as the holoenzyme. Organic cofactors are bound covalently or noncovalently to the apoenzyme. Covalently bound cofactors are sometimes referred to as prosthetic groups. Cofactors are observed in oxidation–reduction, group transfer. Inorganic Cofactors for Enzymes bazı enzimlerin aktiviteleri için organik veya inorganik ek kimyasal bileşenlere gerekvardır olan ve kofaktör diye adlandırılan.
, forms the complete catalytic entity and is known as the holoenzyme. Organic cofactors are bound covalently or noncovalently to the apoenzyme. Covalently bound cofactors are sometimes referred to as prosthetic groups. Cofactors are observed in oxidation–reduction, group transfer. Inorganic Cofactors for Enzymes. bazı enzimlerin aktiviteleri için organik veya inorganik ek kimyasal bileşenlere gerekvardır olan ve kofaktör diye adlandırılan.")
9
Relative Amounts of Enzymes in Various Organs
(Relative to Serum) Tissue localization Sceletal muscle serum Red cells liver heart kidney AST x x x x x 5000 ALT x x x x x 300 LDH x x x x x 700 Transaminazlar (AST, ALT), laktat dehidrojenaz (LD) ve alkalen fosfataz (ALP), kanda bulunan önemli hücre içi enzimlerdir. bir enzimin herhangi bir hastalığın tanı veya ayırıcı tanısındaki yararı, dağılım gösterdiği organ ve doku sayısıyla ters orantılıdır.Bir sellüler enzimin dağılım gösterdiği organ ve doku sayısı fazla ise bu enzim nonspesifik bir enzimdir, tanı veya ayırıcı tanıdaki yararı azdır. Dağılım gösterdiği organ ve doku sayısı az olan sellüler enzim spesifik bir enzimdir, tanı veya ayırıcı tanıdaki yararı fazladır. Örneğin prostatik asit fosfataz, amilaz ve lipaz, spesifik enzimlerdir. CPK x x x
 Tissue localization. Sceletal muscle. serum. Red cells. liver. heart. kidney. AST 1 x 15 x 7000 x 8000 x4500 x ALT 1 x 7 x 3000 x 400 x1200 x 300. LDH 1 x 500 x 7000 x 600 x500 x 700. Transaminazlar (AST, ALT), laktat dehidrojenaz (LD) ve alkalen fosfataz (ALP), kanda bulunan önemli hücre içi enzimlerdir. bir enzimin herhangi bir hastalığın tanı veya ayırıcı tanısındaki yararı, dağılım gösterdiği organ ve doku sayısıyla ters orantılıdır.Bir sellüler enzimin dağılım gösterdiği organ ve doku sayısı fazla ise bu enzim nonspesifik bir enzimdir, tanı veya ayırıcı tanıdaki yararı azdır. Dağılım gösterdiği organ ve doku sayısı az olan sellüler enzim spesifik bir enzimdir, tanı veya ayırıcı tanıdaki yararı fazladır. Örneğin prostatik asit fosfataz, amilaz ve lipaz, spesifik enzimlerdir. CPK x x10 x")
10
Molecular localization
1.membraner - ALP, GGT, 5’NU 2.Sitoplazmik - AST, ALT, LDH, CK 3.Mitokondriyal - AST, CK 4.lizozomal - ACP 5.Nükleer- Polimerazlar 6.mikrozomal - GGT

11
Hücre membranı, enzimlerin hücre dışına çıkmasını engelleyerek sellüler enzimlerin normalde hücre içinde kalmasını sağlar, sellüler enzimlerin ancak çok az bir kısmı hücre dışına çıkar ve dolayısıyla serumda bulunabilir.

12
Hücre membranının bütünlüğü, hücrenin enerji üretimine bağımlıdır
Hücre membranının bütünlüğü, hücrenin enerji üretimine bağımlıdır. Enerji üretimi için gerekli oksijen girişinin kısıtlanması gibi enerji üretimini bozan her türlü etken, hücre membranının bozulmasını artırır. Bu gibi durumlarda, membran hücresel bileşenlerini sızdırır ve eğer hücresel hasar dönüşümsüz hale gelirse hücre ölür.

13
Enzimlerin hücrelerden serbest kalma hızının arttığı iki temel durum:
hücre harabiyeti (nekroz) ve enflamasyondur.
 ve. enflamasyondur.")
14
NEKROZ Nekroz, hücre membranı ve organel membranlarının bütünlüğünün bozulmasıyla hücre içeriğinin hücre dışına boşalmasıdır. Bu durumda hem sitozolik hem mitokondriyal enzimler hücre dışına çıkar ve dolayısıyla serumda hem sitozolik hem mitokondriyal enzimlerin aktivitelerinin arttığı saptanır. Serum enzim düzeyi artışının saptanması suretiyle hücre harabiyetinin derecesi ve yaygınlığı hakkında bilgi edinilebilir. Hücre harabiyeti ve ölümüne neden olan faktörler şunlardır: Hipoksi, kimyasal ajanlar ve ilaçlar, fiziksel ajanlar, genetik bozukluklar, beslenme bozuklukları, enfeksiyöz ajanlar, immün bozukluklar.

15
Anemi ve kardiyorespiratuvar yetmezlik hallerinde hipoksi gelişebilir.

16
Kurşun, cıva, alkol, tütün gibi kimyasal ajanlar ve antiepileptikler gibi ilaçlar, hücre harabiyeti veya hücre ölümüne sonuçta da serumda hem sitozolik hem mitokondriyal enzimlerin aktivitelerinin artışına neden olabilir.

17
Travmalar, aşırı sıcak veya soğuk, radyasyon, hücre harabiyeti veya hücre ölümüne sonuçta da serumda hem sitozolik hem mitokondriyal enzimlerin aktivitelerinin artışına neden olan önemli fiziksel ajanlardır.

18
Vitamin ve mineral eksiklikleri ile sonuçlanan beslenme bozuklukları, serumda hem sitozolik hem mitokondriyal enzimlerin aktivitelerinin artışına neden olabilir.

19
Enflamasyon, kan damarları duvarı ve çevre dokularda hücre membranı geçirgenliğinin artışı ile ilgili reversibl bir olaydır, kimyasal veya biyolojik bir uyarı sonucu gelişir. Enflamasyonda organel membranları etkilenmediğinden serumda sadece sitozolik enzimlerin aktivitesi artar, mitokondriyal enzimlerin aktivitesinde önemli artış olmaz.

20
Factors Affecting Plasma Enzyme Activities

21
Factors Affecting Plasma Enzyme Activities
The most common cause for increased plasma enzymes is death of enzyme-containing cells. Direct damage to the cell membrane by viruses or by chemical substances Hypoxia, anoxia and ischemia of the tissues Plasma levels of enzymes may be increased by several mechanisms. SERUM ENZİM DÜZEYİNİ ETKİLEYEN FAKTÖRLER: Herhangi bir enzimin kandaki düzeyi, kaynaklandığı hücreden dolaşıma katılım hızı ve uzaklaştırıldığı hız arasındaki dengenin bir sonucudur. Causes of pathological enzyme release. Hipoksi, hücrede enerji üretiminin bozulduğu önemli bir klinik durumdur. Anemi ve kardiyorespiratuvar yetmezlik hallerinde hipoksi gelişebilir. Normalde hücre membranının bütünlüğü, enerji ile sağlanır ve korunur. Hücrede okside olabilecek substratların azalması veya doku oksijenasyonunun yetersizliği nedeniyle enerji üretiminde bozulma, hücre membranının bütünlüğünün bozulmasına ve sonuçta hücre harabiyetine veya hücre ölümüne neden olabilir, hücre içinden ekstrasellüler ortama artan miktarlarda enzim sızıntısı olur.

22
Factors Affecting Plasma Enzyme Activities
Enzymes are also released in the process of normal cell turnover. Increased synthesis of enzymes by cells also leads to increased plasma enzyme levels. İncreased activity of osteoblasts, plasma levels of the bone isoenzyme of ALP increase. İncrease in muscle-related enzymes seen with increased exercise. Many drugs that stimulate microsomal enzymes, including ethanol and antiepileptic agents, lead to increased plasma γ- glutamyl transferase (GGT). hücre yapım-yıkım döngüsünde hızlanma Enzim üretiminin artması (sentezin artması veya enzimin sentezlendiği hücrelerin proliferasyonu), Enzim üretiminin azalması, enzimlerin dolaşımdan uzaklaştırılma veya inaktive edilme hızını artıran nonspesifik nedenlerin varlığı hallerinde serum enzim düzeyi azalır. Enzim üretiminde artma, sık görülür. Uyarıya bağlı olarak enzim aktivitesi artışına enzim indüksiyonu denir. Osteoblastik aktivite artışında serum alkalen fosfataz (ALP) aktivitesi artar. İlaçların etkisiyle indüksiyona bağlı olarak bazı enzimlerin serumdaki aktivitesi artar. Örneğin alkol, barbitürat veya fenitonin gibi ilaçların kullanılması, mikrozomal enzim indüksiyonu sonucu GGT’yi artırır.
. hücre yapım-yıkım döngüsünde hızlanma. Enzim üretiminin artması (sentezin artması veya enzimin sentezlendiği hücrelerin proliferasyonu), Enzim üretiminin azalması, enzimlerin dolaşımdan uzaklaştırılma veya inaktive edilme hızını artıran nonspesifik nedenlerin varlığı hallerinde serum enzim düzeyi azalır. Enzim üretiminde artma, sık görülür. Uyarıya bağlı olarak enzim aktivitesi artışına enzim indüksiyonu denir. Osteoblastik aktivite artışında serum alkalen fosfataz (ALP) aktivitesi artar. İlaçların etkisiyle indüksiyona bağlı olarak bazı enzimlerin serumdaki aktivitesi artar. Örneğin alkol, barbitürat veya fenitonin gibi ilaçların kullanılması, mikrozomal enzim indüksiyonu sonucu GGT’yi artırır.")
23
Factors Affecting Plasma Enzyme Activities
Release of enzyme from cells occurs without cell death or increased synthesis. Ethanol causes expression of the mitochondrial isoenzyme of AST(mAST) on the surface of hepatocytes and increased plasma levels. Ischemia of myocardial cells leads to loss of glycogen phosphorylase BB isoenzyme and the MB isozyme of CK into plasma. Ingestion of food leads to release of intestinal ALP into plasma. A number of liver enzymes (ALP, GGT, leucine aminopeptidase, 5′- nucleotidase are bound to the canalicular surface of the hepatocyte. Increased concentrations of bile salts with canalicular obstruction may release fragments of membrane with enzyme attached into the circulation. Biliyer tıkanmada karaciğerde enzim sentezi uyarılır ve serum alkalen fosfataz (ALP), gama glutamat transpeptidaz (GGT, γ-GT) aktivitesi artar. γ-GT artışı daha fazladır.
 on the surface of hepatocytes and increased plasma levels. Ischemia of myocardial cells leads to loss of glycogen phosphorylase BB isoenzyme and the MB isozyme of CK into plasma. Ingestion of food leads to release of intestinal ALP into plasma. A number of liver enzymes (ALP, GGT, leucine aminopeptidase, 5′- nucleotidase are bound to the canalicular surface of the hepatocyte. Increased concentrations of bile salts with canalicular obstruction may release fragments of membrane with enzyme attached into the circulation. Biliyer tıkanmada karaciğerde enzim sentezi uyarılır ve serum alkalen fosfataz (ALP), gama glutamat transpeptidaz (GGT, γ-GT) aktivitesi artar. γ-GT artışı daha fazladır.")
24
Factors Affecting Plasma Enzyme Activities
İncreased plasma enzyme levels may be due to decreased clearance of enzymes from the circulation. Some smaller enzymes, such as amylase and lipase, are partially cleared by glomerular filtration; renal failure increases their plasma levels. For many enzymes, autoantibodies against one or more isoenzymes may cause the development of enzyme– antibody complexes (often termed macroenzymes), which result in enzyme half-lives similar to the 3-week half-life of immunoglobulin G. for example: against the intestinal isoenzyme of ALP in persons with bacterial infection
, which result in enzyme half-lives similar to the 3-week half-life of immunoglobulin G. for example: against the intestinal isoenzyme of ALP in persons with bacterial infection")
25
Information available from enzyme measurements
Magnitude of damage (i.e. how many cells damaged?) Severity of damage (i.e. how badly is each cell damaged?) Stage of illness and prognosis Which tissue is damaged hücre harabiyetinin derecesi ve yaygınlığı hakkında bilgi edinilebilir.
 Severity of damage (i.e. how badly is each cell damaged ) Stage of illness and prognosis. Which tissue is damaged. hücre harabiyetinin derecesi ve yaygınlığı hakkında bilgi edinilebilir.")
26
Factors Affecting the Lifetime of Enzymes in Blood
With cell death, defects in cellular membranes enlarge gradually over time; thus, smaller cytoplasmic enzymes will leak from damaged cells sooner than larger ones. For example: with myocardial injury, CK and AST are smaller than LDH and appear in plasma sooner. Some enzymes are not cytoplasmic, but may be within mitochondria (isoenzymes of CK and AST) or bound to plasma membranes (such as ALP and GGT); cell death typically does not lead to release of such enzymes. The time course of appearance and disappearance of enzymes with cell injury is dependent on a number of factors.
 or bound to plasma membranes (such as ALP and GGT); cell death typically does not lead to release of such enzymes. The time course of appearance and disappearance of enzymes with cell injury is dependent on a number of factors.")
27
DETERMİNATİON OF TOTAL ENZYME CONCENTRATİONS İN SERUM AND OTHER BODY FLUİDS

28
Determination of enzyme activity
(IU)
")
29
In principle, in the measurement of enzyme activity, either the rate of disappearance of substrate or the rate of appearance of product can be measured. In general, it is easier to measure small increases in product than to measure small decreases in a relatively high concentration of substrate often needed to achieve saturation.

30
KLİNİK ENZİMOLOJİDE ENZİM ÖLÇÜMLERİ
1) Reaksiyon hızlarının ölçülmesi 2) Enzim kütlesinin ölçümü 3) İzoenzimlerin ve izoformların ölçümü
 Reaksiyon hızlarının ölçülmesi. 2) Enzim kütlesinin ölçümü. 3) İzoenzimlerin ve izoformların ölçümü.")
31
Measure enzyme activity in a sample, it is most common to use substrates at saturating concentrations where zero-order kinetics with respect to [S] occur. Under these conditions, the reaction rate is directly proportional to the total amount of enzyme present.
![Measure enzyme activity in a sample, it is most common to use substrates at saturating concentrations where zero-order kinetics with respect to [S] occur.](http://slideplayer.biz.tr/slide/4105716/12/images/31/Measure+enzyme+activity+in+a+sample%2C+it+is+most+common+to+use+substrates+at+saturating+concentrations+where+zero-order+kinetics+with+respect+to+%5BS%5D+occur..jpg "Under these conditions, the reaction rate is directly proportional to the total amount of enzyme present.")
32
Reaksiyon hızlarının ölçülmesi
Enzim katalizli reaksiyonların hızı, sistemde mevcut olan aktif enzimin miktarı ile doğru orantılıdır. Reaksiyon hızının belirlenmesi, tanımlanmış bir zaman aralığında ortaya çıkan miktar değişiminin kinetik ölçümü suretiyle olur. Reaksiyon hızının ölçülmesinde sabit zaman ve sürekli izleme yöntemleri kullanılır. Sabit zamanlı reaksiyonda, enzim tarafından dönüştürülen ürün miktarı, sabit zaman aralığının sonunda reaksiyon durdurularak ölçülür. Sürekli izleme yönteminde, reaksiyonun ilerleyişi sürekli olarak izlenir. Reaksiyon hızının ölçümü, aktivite birimi ile ifade edilir. Klinik enzimolojide enzim aktivitesi genelde belli bir hacimde (100 mL’deki, L serumda, 1 mL eritrositteki gibi) verilir. Reaksiyon hızı pH, çözelti tipi, sıcaklık, substratın doğası, iyonik güç, aktivatör konsantrasyonu ve diğer değişkenler gibi deneysel parametrelere dayandığından, bu gibi parametreler birimin tanımlanmasında belirtilmelidir.
 verilir. Reaksiyon hızı pH, çözelti tipi, sıcaklık, substratın doğası, iyonik güç, aktivatör konsantrasyonu ve diğer değişkenler gibi deneysel parametrelere dayandığından, bu gibi parametreler birimin tanımlanmasında belirtilmelidir.")
33
Sabit zamanlı reaksiyonda, enzim tarafından dönüştürülen ürün miktarı, sabit zaman aralığının sonunda reaksiyon durdurularak ölçülür. Sürekli izleme yönteminde, reaksiyonun ilerleyişi sürekli olarak izlenir.

34
Reaksiyon hızının ölçümü, aktivite birimi ile ifade edilir.
Klinik enzimolojide enzim aktivitesi genelde belli bir hacimde (100 mL’deki, L serumda, 1 mL eritrositteki gibi) verilir. Reaksiyon hızı pH, çözelti tipi, sıcaklık, substratın doğası, iyonik güç, aktivatör konsantrasyonu ve diğer değişkenler gibi deneysel parametrelere dayandığından, bu gibi parametreler birimin tanımlanmasında belirtilmelidir.
 verilir. Reaksiyon hızı pH, çözelti tipi, sıcaklık, substratın doğası, iyonik güç, aktivatör konsantrasyonu ve diğer değişkenler gibi deneysel parametrelere dayandığından, bu gibi parametreler birimin tanımlanmasında belirtilmelidir.")
35
Enzim aktivitesinin tanımlanmasını standardize etmek için IUB Enzim Komitesi, enzim aktivite biriminin dakikada 1 mikromolar substratı ürüne dönüştüren enzim miktarı olarak tanımlanmasını ve bu birimin uluslararası ünite (IU, U) olmasını önermiştir. Katalitik konsantrasyon, sayısal olarak daha uygun bir değer olduğu için, U/L veya mU/L birimleriyle ifade edilir.

36
Eğer bir enzim reaksiyonu ölçüm sistemindeki bazı bileşenlerin görünen veya ultraviyole spektrumda absorbans özelliklerinde değişiklikler ile beraber gerçekleşiyorsa bu durum spektrofotometrik olarak saptanır.

37
Spectrophotometric Assays

38
Determination of enzyme activity
Photometrically measured change in the absorbance of an indicator per unit of time is used as a measure of the rate of reaction. This is proportional to the enzyme activity, provided that the enzyme is working at maximum rate (with sufficient substrate and coenzyme)
")
39
Determination of enzyme activity
The coenzymes NAD and NADH are often used as indicators (optical test), less often the absorbance of the substrate or the reaction product (colorimetrik test). The activity is expressed in kinetic unit: International unit (IU) is the quantity of enzyme which catalyzes one micromole (mol) of substrate per minute. (Enzyme activity is expressed in IU/L, or in mU/L Lactate LDH Pyruvate NAD NADH
, less often the absorbance of the substrate or the reaction product (colorimetrik test). The activity is expressed in kinetic unit: International unit (IU) is the quantity of enzyme which catalyzes one micromole (mol) of substrate per minute. (Enzyme activity is expressed in IU/L, or in mU/L. Lactate LDH Pyruvate. NAD+ NADH.")
40
For example, the NADH/NAD+ molecule is often used in enzymatic oxidation/reduction reactions. During these reactions NADH is often oxidized to NAD+, or NAD+ is reduced to NADH. NADH absorbs light at 340 nm, however NAD+ does not hold that property. A spectrophotometer can be used to measure the change in absorbance of 340 nm light, thus indicating a change in amount of NADH.

41
Lactate LDH Pyruvate NAD NADH Bu reaksiyonlara önemli örnekler, yükseltgenme ve indirgenmelerde NADH ve NADPH koenzimlerinin 339 (340) nm’deki absorbans değişimleri izlenerek dehidrogenaz aktivitesinin belirlenmesi
 nm’deki absorbans değişimleri izlenerek dehidrogenaz aktivitesinin belirlenmesi.")
42
1 enzim ünitesi, optimal şartlarda (optimal ısı ve optimal pH) 1 mikromol substratı 1 dakikada ürüne dönüştüren enzim aktivitesidir; buna internasyonal ünite adı verilir. Günümüzde enzim ölçüm birimi olarak genelde bu ünite kullanılır; IU veya kısaca U şeklinde kısaltılır. 1 saniyede 1 mol substratı ürüne dönüştüren enzim aktivitesine 1 katal veya 1 SI ünitesi denir

43
KAN ENZİMLERİNİN AKTİVİTE TAYİNLERİNDE DİKKAT EDİLECEKLER

44
Kan enzim aktiviteleri tayini için ideal örnek serumdur, plazmadaki antikoagulanlar enzimatik aktiviteyi düşürürler. Enzim aktivitesi tayini yapılacak kan, antikoagulansız tüpe (düz tüp) alınmalıdır.
 alınmalıdır..")
45
Kan alırken hemolizden kaçınmalıdır.
Çünkü eritrositler, enzim bakımından çok zengindirler, hemoliz sonucunda eritrositlerdeki enzimler seruma geçerler ve sonuçta enzim aktivitesinde yanlış olarak yüksek değerler bulunur. Ayrıca seruma geçen hemoglobinin kırmızı rengi de interferans etkisiyle ölçüm hatalarına neden olur.

46
Serum için alınan kan, pıhtılaşmasından hemen sonra santrifüj edilerek serum ayrılmalıdır. Serumun hemen ayrılmaması halinde hücresel elemanlardaki enzimler seruma sızabilir ve enzim aktivitesinde yanlış olarak yüksek değerler bulunur.

47
Enzim tayinlerinde günlük taze kan kullanılması en iyisidir.
Çünkü enzimlerin aktiviteleri zamanla azalır. Bazı enzimlerin aktivitelerinde +4oC de 1-2 gün büyük bir kayıp olmadığı halde bazı enzimler oda sıcaklığında birkaç saat içinde inaktive olurlar.

48
Specific Enzymes

49
Diagnostic enzymes Alanine aminotransferase (ALT)
Aspartate aminotransferase (AST) Alkaline phosphatase (ALP) Gamma glutamyl transferase (GGT) Lactate dehydrogenase (LDH) α-Amilase Lipase Creatine kinase (CPK), Creatine kinase MB (CK-MB) Acid phosphatase 5′-Nucleotidase Leucine aminopeptidase Aldolase G-6-PD ChE
 Alkaline phosphatase (ALP) Gamma glutamyl transferase (GGT) Lactate dehydrogenase (LDH) α-Amilase. Lipase. Creatine kinase (CPK), Creatine kinase MB (CK-MB) Acid phosphatase. 5′-Nucleotidase. Leucine aminopeptidase. Aldolase. G-6-PD. ChE.")
50
Malignant diseases enzymes
Liver enzymes ALT AST LDH GGT ALP 5’nükleotidaz Pancreatic enzymes Alfa-amilaz Lipaz Bone enzymes ALP Muscle enzymes CK, CK-MB LDH Aldolaz AST Malignant diseases enzymes ACP ALP GGT LDH Karaciğer hastalıklarının tanısında yararlı enzimler Kas hastalıklarının tanısında yararlı enzimler Kemik hastalıklarının tanısında yararlı enzimler Pankreas hastalıklarının tanısında yararlı enzimler Malignitelerin tanısında yararlı enzimler Genetik hastalıkların tanısında yararlı enzimler Hematolojik hastalıkların tanısında yararlı enzimler Haematologyc enzymes G-6-PDH Piruvat kinase

51
Liver enzymes

52
hepatocellular enzymes
As metabolically complex cells, hepatocytes contain high levels of a number of enzymes. With liver injury, these enzymes may leak into plasma and can be useful for diagnosis and monitoring of liver injury. Within the hepatocyte, the commonly measured enzymes are found in specific locations; the type of liver injury will determine the pattern of enzyme change.

53
Location of hepatocellular enzymes
ALT and the cytoplasmic isoenzyme of aspartate aminotransferase (ASTc) are found primarily in the cytosol. With membrane injury as in viral or chemically induced hepatitis, raising plasma AST and ALT activities. Mitochondrial aspartate aminotransferase (ASTm) is released primarily with mitochondrial injury, as caused by ethanol as in alcoholic hepatitis.
 are found primarily in the cytosol. With membrane injury as in viral or chemically induced hepatitis, raising plasma AST and ALT activities. Mitochondrial aspartate aminotransferase (ASTm) is released primarily with mitochondrial injury, as caused by ethanol as in alcoholic hepatitis.")
54
Location of hepatocellular enzymes
ALP and GGT are found primarily on the canalicular surface of the hepatocyte. Bile acids accumulate in cholestasis and dissolve membrane fragments, releasing bound enzymes into plasma. are increased by obstructive processes. GGT is also found in the microsomes, microsomal enzyme-inducing drugs, such as etanol and phenobarbital, can also increase GGT synthesis and raise plasma GGT activity.

55
Aminotransferases (Transaminases)
aspartate aminotransferase (AST) and alanine aminotransferase (ALT) Two diagnostically very useful enzymes in this category are AST (SGOT), also known as serum glutamate oxaloacetate transaminase, and ALT,(SGPT) formerly called serum glutamate pyruvate transaminase
 and. alanine aminotransferase (ALT) Two diagnostically very useful enzymes in this category are AST (SGOT), also known as serum glutamate oxaloacetate transaminase, and ALT,(SGPT) formerly called serum glutamate pyruvate transaminase.")
56
Both enzymes require pyridoxal phosphate (vitamin B6) as a cofactor.
These enzymes catalyze reversibly the transfer of an amino group of AST or ALT to α-ketoglutarate to yield glutamate plus the corresponding ketoacid of the starting amino acid (i.e., oxaloacetate or pyruvate, respectively). Both enzymes require pyridoxal phosphate (vitamin B6) as a cofactor. Transaminazlar (aminotransferazlar), bir amino grubunun bir -amino asitten bir -keto aside aktarılmasını katalizleyen, böylece amino asitler ile -keto asidlerin birbirine çevrilmesini gerçekleştiren enzimlerdir.
. Both enzymes require pyridoxal phosphate (vitamin B6) as a cofactor. Transaminazlar (aminotransferazlar), bir amino grubunun bir -amino asitten bir -keto aside aktarılmasını katalizleyen, böylece amino asitler ile -keto asidlerin birbirine çevrilmesini gerçekleştiren enzimlerdir.")
57
AST and ALT have respective blood half-lives of 17 and 47 hours, respectively, and have upper reference range limits of around 35 IU/L. AST is both intramitochondrial and extramitochondrial, but ALT is completely extramitochondrial. Mitochondrial AST isoenzyme has a half-life of 87 hours. AST is ubiquitously distributed in the body tissues, including the heart and muscle, whereas ALT is found primarily in the liver, although significant amounts are also present in the kidney.

58
Relative Amounts of Enzymes in Various Organs
(Relative to Serum) Tissue localization Sceletal muscle erythocytes liver heart kidney AST x x x x x 5000 AST, vücutta çok geniş ölçüde dağılmıştır. Kalp, karaciğer, iskelet kasları, böbrek ve eritrositlerde çok yüksek konsantrasyonlarda bulunur. En yüksek konsantrasyonda kalpte bulunur. Karaciğerde mitokondriyal bir yerleşim gösterirken diğer dokularda sitozolik yerleşim gösterir. ALT, karaciğer kalp, iskelet kası ve böbrekte yüksek konsantrasyonlarda bulunur. En yüksek konsantrasyonda karaciğerde bulunur; sitozolik bir enzimdir. ALT x x x x x 300
 Tissue localization. Sceletal muscle. erythocytes. liver. heart. kidney. AST x 15 x 7000 x 8000 x4500 x AST, vücutta çok geniş ölçüde dağılmıştır. Kalp, karaciğer, iskelet kasları, böbrek ve eritrositlerde çok yüksek konsantrasyonlarda bulunur. En yüksek konsantrasyonda kalpte bulunur. Karaciğerde mitokondriyal bir yerleşim gösterirken diğer dokularda sitozolik yerleşim gösterir. ALT, karaciğer kalp, iskelet kası ve böbrekte yüksek konsantrasyonlarda bulunur. En yüksek konsantrasyonda karaciğerde bulunur; sitozolik bir enzimdir. ALT x 7 x 3000 x 400 x 1200 x 300.")
59
Mechanisms of Enzyme Release from hepatocytes
Enzymes are released from hepatocytes as a result of injury to the cell membrane that directly causes extrusion of the cytosolic contents. Agents like ethanol cause release of mAST from hepatocytes and its expression on cell surfaces. Accumulation of bile salts with canalicular obstruction causes release of membrane fragments with attached canalicular enzymes. Increased synthesis of GGT, and to a lesser extent alkaline phosphatase, can occur with medications that induce microsomal enzyme synthesis, notably ethanol, phenytoin, and carbamazepine.

60
Assays for AST and ALT In this reaction, nicotinamide adenine dinucleotide (NADH) is converted to NAD that is measured by a decrease in absorbance at 340 nm. As noted earlier, it is vital that pyridoxal phosphate be present in sufficient quantity to allow these reactions to proceed. TRIS ,L-Alanin ,LDH (mikrobiyal),Piridoksal fosfat L,NADH,2-Oksoglutarat pH (37 °C) NADH yükseltgenmesinin hızı katalitik ALT aktivitesiyle doğru orantılıdır. Absorbanstaki azalma 340 nm’de ölçülerek tayin edilir. L-Alanin + 2-oksoglutarat ALT piruvat + L-glutamat Piruvat + NADH + H LDH L-laktat + NAD+
 is converted to NAD that is measured by a decrease in absorbance at 340 nm. As noted earlier, it is vital that pyridoxal phosphate be present in sufficient quantity to allow these reactions to proceed. TRIS ,L-Alanin ,LDH (mikrobiyal),Piridoksal fosfat L,NADH,2-Oksoglutarat. pH (37 °C) NADH yükseltgenmesinin hızı katalitik ALT aktivitesiyle doğru orantılıdır. Absorbanstaki azalma 340 nm’de ölçülerek tayin edilir. L-Alanin + 2-oksoglutarat ALT piruvat + L-glutamat. Piruvat + NADH + H+ LDH L-laktat + NAD+")
61
AST AST L-Aspartat + 2-oksoglutarat oksaloasetat + L-glutamat MDH Oksaloasetat + NADH + H+ L-malat + NAD+ Numune içindeki AST oksaloasetat ve L-glutamatın oluşması için L-aspartat ile 2-oksoglutarat arasında bir amino grubunun transferini katalize eder. Oksaloasetat daha sonra NAD+’nın oluşması için malat dehidrojenaz (MDH) varlığında NADH ile reaksiyona girer. Piridoksal fosfat, amino transfer reaksiyonunda bir koenzim olarak görev yapar. Enzim aktivasyonunun tam olmasını sağlar. NADH yükseltgenmesinin hızı katalitik AST aktivitesiyle doğru
 varlığında NADH ile reaksiyona girer. Piridoksal fosfat, amino transfer. reaksiyonunda bir koenzim olarak görev yapar. Enzim aktivasyonunun tam olmasını sağlar. NADH yükseltgenmesinin hızı katalitik AST aktivitesiyle doğru.")
62
AST ALT Stabilite: 15-25 °C’de 3 gün 2-8 °C’de 7 gün
Sitrat ve florür enzim aktivitesini inhibe eder. AST 15-25 °C’de 7 gün

63
Enflamasyon durumlarında da serum ALT (SGPT) düzeyi artar.
Clinical Causes of Increased or Decreased Serum AST and ALT Activity Normally not affected 2-5 x normal Acute Pancreatitis Up to 3 x normal Pulmonary emboli Normal to slightly increase Skeletal muscle injury Variable increases, up to 2 x normal Cirrhosis Up to 5 x normal Obstructive jaundice, cholangitis Up to 20 x normal Toxic Hepatitis x normal Viral Hepatitis 5-10 x normal >10 x normal Heart failure with liver congestion 4-5 x normal Myocarditis Pericarditis Congestive Heart Failure Normal to slightly increase in uncomplicated infarcts 4-5 x normal; >10-15 x normal ~ fatal infarcts Myocardial Infarction Increased Activity Low normal to below normal; corrected by some methods Vitamin B6 deficiency Not applicable Suppression of activity Uremia Decreased Activity ALT AST Condition enzimin yüksek konsantrasyonda bulunduğu dokulardan herhangi birinin harabiyeti hallerinde saptanır. AST - MI’de, viral hepatitte, toksik karaciğer nekrozunda, şok ve hipoksi ile birlikte olan dolaşım yetersizliğinde, serum AST düzeyinde normalin misli artış saptanabilir. Kronik hepatit ve sirozda, kolestatik sarılıkta, karaciğerin malign infiltrasyonunda, iskelet kası hastalıklarında, travma ve cerrahi girişimlerden sonra, şiddetli hemolitik anemilerde, enfeksiyöz mononükleozda, perikardit ve miyokardit durumlarında, taşikardi durumlarında, akciğer embolisinde, akut batın hastalıklarında, mide ve duodenum ülserlerinde serum AST düzeyinde orta derecede artış saptanabilir. Enflamasyon durumlarında da serum ALT (SGPT) düzeyi artar.
 düzeyi artar.")
64
Aspartate Aminotransferase (AST)
Interfering factors: Increased with exercise, antihypertensive drugs, cholinergic agents, coumadin, digitalis. erythromycin, oral contraceptives, opiates, salicylates. False decrease in uremia, severe long-standing liver disease, diabetic ketoacidosis

65
Alanine Aminotransferase (ALT)
Interfering factors: Increased large number of IM injections Acetaminophen, ampicillin, codeine, nafcillin, oral contraceptives, salicylates, tetracycline, other drugs

66
Enzymes Primarily Reflecting Canalicular Injury
These enzymes are located predominantly on the canalicular membrane of the hepatocyte. alkaline phosphatase (ALP) γ-glutamyl transferase (GGT) and 5′-nucleotidase. In contrast to cytoplasmic enzyme activities, canalicular enzyme activities within hepatocytes are typically quite low; focal hepatocyte injury seldom causes significant increases in canalicular enzyme levels.
 γ-glutamyl transferase (GGT) and 5′-nucleotidase. In contrast to cytoplasmic enzyme activities, canalicular enzyme activities within hepatocytes are typically quite low; focal hepatocyte injury seldom causes significant increases in canalicular enzyme levels.")
67
Alkaline Phosphatase (ALP)
")
68
Alkaline phosphatases represent a family of enzymes coded for by different genes.
ALP is present in a number of tissues, including liver, bone, kidney, intestine, and placenta, each of which contains distinct isozymes that can be separated from one another by electrophoresis. Hepatocytes produce ALP in the liver, where it is found attached to the canalicular surface of the cells . Osteoblasts produce bone ALP, which appears to be involved in cleavage of pyrophosphate, an inhibitor of bone mineralization. Intestinal epithelial cells produce intestinal ALP, which is released into the intestine following ingestion of fatty foods. Plasental ALP ALP, karaciğer, kemik, plasenta, bağırsak, dalak ve böbrekte bulunur. ALP’ın idandifiye edilmiş dört izoenzimi ve idandifiye edilmemiş izoenzimleri vardır.

69
mechanisms for release of ALP from cells
With liver injury, ALP synthesis increases, but bile acids dissolve fragments of canalicular cell membranes with attached enzymes (including ALP, GGT, leucine aminopeptidase, and 5′-NT. In normal serum, a single form (of liver or bone origin) of ALP is typically seen The intestinal isoenzyme of ALP is released in large amounts into duodenal fluid, and large amounts enter lymphatic fluid, draining the intestinal tract following a meal
 of ALP is typically seen. The intestinal isoenzyme of ALP is released in large amounts into duodenal fluid, and large amounts enter lymphatic fluid, draining the intestinal tract following a meal")
70
Reference ranges for ALP are highly dependent on age and gender
The higher values in children are due to the bone isoenzyme. Pregnancy causes a two- to threefold increase in ALP, mainly due to the placental isoenzyme, but also because of an increase in bone isoenzyme. Normalde serumda çocuklarda kemik izoenzimi çok, yetişkinlerde ise karaciğer izoenzimi çoktur. ALP, osteoblastik hücrelerde kemik oluşumu sırasında sentezlenir. Serum ALP düzeyi, osteoblastik aktivitenin arttığı çocuklukta 16 yaşlarına kadar yüksektir.

71
Preanalytic Variation
High body mass index is associated with a 10% average increase in ALP. Oral contraceptives decrease ALP by an average of 20%. Fibric acid derivatives decrease total ALP by 25% and the liver isoenzyme by 40%. Antiepileptic agents commonly cause increased total ALP ( mainly because of increases in the liver isoenzyme). Smoking causes an average 10% increase in total ALP as the result of pulmonary production of placental-like ALP .
. Smoking causes an average 10% increase in total ALP as the result of pulmonary production of placental-like ALP .")
72
Measurement ALP activity is usually measured using p-nitrophenyl phosphate as the substrate at alkaline pH. Hydrolysis of this phosphate ester yields inorganic phosphate plus the highly colored and easily measured para-nitrophenoxide anion. ALP p-nitrofenil fosfat + H2O fosfat + p-nitrofenol Zn is a component of the enzyme, and Mg and other cations activate the enzyme. Chelators present in collection tubes (such as EDTA, citrate, and oxalate) falsely lower ALP activity; in the case of EDTA, activity is often too low to measure. p-nitrofenil fosfat, ortamda magnezyum ve çinko iyonları bulunduğunda, fosfataz aracılığıyla fosfat ve p-nitrofenole ayrılır. Açığa çıkan p-nitrofenol katalitik ALP aktivesi ile doğrudan orantılıdır. Absorbanstaki artış ölçülerek tayin edilir.
 falsely lower ALP activity; in the case of EDTA, activity is often too low to measure. p-nitrofenil fosfat, ortamda magnezyum ve çinko iyonları bulunduğunda, fosfataz aracılığıyla fosfat ve p-nitrofenole ayrılır. Açığa çıkan p-nitrofenol katalitik ALP aktivesi ile doğrudan orantılıdır. Absorbanstaki artış ölçülerek tayin edilir.")
73
ALP The activity of the enzyme increases slowly on storage because of loss of inhibitors, but specimens are relatively stable at : 15-25 °C - 7 d 2-8 °C - 7 d (-15)-(-25) °C - 2 m
-(-25) °C - 2 m.")
74
Causes of Abnormal Results
The most common causes of increased ALP are liver and bone disease. Disorders causing cholestasis more frequently cause elevation of ALP than do hepatocellular disorders. In obstructive cholestasis, ALP most commonly rises to twice the upper limit of normal or greater, roughly paralleling the rate of rise in serum bilirubin. If obstruction is partial, ALP usually increases as much as with complete obstruction, often out of proportion to the increase in conjugated bilirubin. Serum ALP düzeyinde patolojik artış, hemen hemen daima kolestatik karakterli bir karaciğer hastalığı veya osteoblastik aktivitede artışla birlikte olan bir kemik hastalığı ile ilgilidir. Karaciğer hastalığında ALP artışının nedeni, safra kanaliküllerini örten hücrelerin enzim üretiminde artıştır.

75
Passive congestion of the liver can occasionally result in moderate ALP elevations, more so than abnormal bilirubin levels. ALP is also moderately elevated in most instances of jaundice resulting from hepatic injury. When the resulting cholestasis is relieved, serum ALP levels fall to normal more slowly than bilirubin.

76
Causes of Abnormal Results
Increased osteoblastic activity in Paget's disease, osteosarcoma, tumor metastatic to bone, and metabolic bone disease are the most common causes of elevated bone isoenzyme. Patients will have elevations of both bone and liver isoenzymes, especially in metastatic carcinoma. Increases in intestinal ALP may occur in patients with intestinal infarction, inflammation, and ulceration.

77
Causes of Abnormal Results
Increases in placenta-like isoenzymes, such as Regan and Nagao, are commonly found in patients with malignancies (ovary, cervix, lung, breast, colon, pancreas) and are due to ectopic production by the neoplasm. Decreased ALP can also occur in zinc deficiency because zinc is a necessary cofactor for ALP activity, as well as other conditions. Placental alkaline phosphatase (PLAP) is a useful tumor marker in serum and cerebrospinal fluid (CSF) for most germ cell tumors. İdandifiye edilmemiş izoenzimlerden REGAN izoenzimi, malign dokudan (akciğer kanseri, over kanseri ve meme kanseri) ektopik olarak üretilir, kardiyoplasental izoenzim diye de bilinir. Nagaro izoenzimi, özellikle pankreas ve plavra kavitesini tutan karsinomalarda artar.
 and are due to ectopic production by the neoplasm. Decreased ALP can also occur in zinc deficiency because zinc is a necessary cofactor for ALP activity, as well as other conditions. Placental alkaline phosphatase (PLAP) is a useful tumor marker in serum and cerebrospinal fluid (CSF) for most germ cell tumors. İdandifiye edilmemiş izoenzimlerden REGAN izoenzimi, malign dokudan (akciğer kanseri, over kanseri ve meme kanseri) ektopik olarak üretilir, kardiyoplasental izoenzim diye de bilinir. Nagaro izoenzimi, özellikle pankreas ve plavra kavitesini tutan karsinomalarda artar.")
78
GAMMA-Glutamyl Transferase
(GGT)
")
79
This enzyme regulates the transport of amino acids across cell membranes by catalyzing the transfer of a glutamyl group from glutathione to a free amino acid. GGT, hücre membranında amino asit ve peptitlerin -glutamil peptitleri şeklinde hücre içine alınmasında görev yapar. glutatyon sentezinde görev alır, protein biyosentezinde görev alır.

80
GGT, mikrozomal bir enzimdir.
Fenobarbital, antidepresanlar, antikonvülzanlar, kontraseptifler gibi bazı ilaçlar tarafından sentezi indüklenir. GGT, kas dışında serum ve diğer tüm hücrelerde bulunur; hepatobiliyer sistem, böbrekler, pankreas ve bağırsaklarda bulunur.

81
Not elevated with pregnancy, bone disease, childhood or adolescence.
Normal GGT + Elevated ALP is suggestive of bone disease. Elevated GGT + Elevated ALP is suggestive of liver or bile-duct disease.

82
Its major use is to discriminate the source of elevated ALP (i. e
Its major use is to discriminate the source of elevated ALP (i.e., if ALP is elevated and GGT is correspondingly elevated, then the source of the elevated ALP is most likely the biliary tract). The highest values, often greater than 10 times the upper limit of normal, may be found in chronic cholestasis due to primary biliary cirrhosis or sclerosing cholangitis. Serum GGT düzeyinde patolojik artış, hepatobiliyer hastalıkların tanısında ve ayırıcı tanısında önem taşır. Kolestaz, alkolik karaciğer, sekonder karaciğer tümörleri, viral hepatit gibi durumlarda serum GGT düzeyi artar. Yüksek serum GGT düzeyi, kolestazı %93 oranında doğrular. Kemik ve plasentada bulunmadığından, kolestazın tanısı için ALP’dan daha spesifiktir. Özellikle hamilelerde ve bebeklerde hepatobiliyer hastalıkların tanısı için önemlidir. Serumdaki GGT’nin büyük çoğunluğunu karaciğer karşılar. GGT aktivitesi tüm karaciğer hastalıklarında artar. İntrahepatik ve posthepatik safra kanalı tıkanmalarında en fazla artış gösteren enzim, normal değerin 5-30 katına kadar yükselir.
. The highest values, often greater than 10 times the upper limit of normal, may be found in chronic cholestasis due to primary biliary cirrhosis or sclerosing cholangitis. Serum GGT düzeyinde patolojik artış, hepatobiliyer hastalıkların tanısında ve ayırıcı tanısında önem taşır. Kolestaz, alkolik karaciğer, sekonder karaciğer tümörleri, viral hepatit gibi durumlarda serum GGT düzeyi artar. Yüksek serum GGT düzeyi, kolestazı %93 oranında doğrular. Kemik ve plasentada bulunmadığından, kolestazın tanısı için ALP’dan daha spesifiktir. Özellikle hamilelerde ve bebeklerde hepatobiliyer hastalıkların tanısı için önemlidir. Serumdaki GGT’nin büyük çoğunluğunu karaciğer karşılar. GGT aktivitesi tüm karaciğer hastalıklarında artar. İntrahepatik ve posthepatik safra kanalı tıkanmalarında en fazla artış gösteren enzim, normal değerin 5-30 katına kadar yükselir.")
83
This enzyme is also elevated in about 60%–70% of those who chronically abuse alcohol, with a rough correlation between amount of alcohol intake and GGT activity. Levels often decline slowly with abstention from alcohol and remain elevated for at least 1 month after abstinence begins. GGT has a half-life of 10 days, but, in recovery from alcohol abuse, the half-life may be as long as 28 days. It tends to be higher in obstructive disorders and with space-occupying lesions in the liver than with hepatocyte injury. Kronik alkolizimde, alkolün mikrozomal enzim indüksiyonu yapmasından dolayı serum GGT düzeyi yükselir.

84
Serum levels of GGT differ from those of ALP during pregnancy, in which GGT remains normal even during cholestasis in pregnancy. GGT is often increased in alcoholics even without liver disease; in some obese people; and in the presence of high concentrations of therapeutic drugs, such as acetaminophen and phenytoin and carbamazepine (increased up to five times the reference limits)
")
85
Measurement GGT L-γ-glutamil-3-karboksi-4-nitroanilit + glisilglisin
Most assays for GGT utilize the substrate γ-glutamyl–p- nitroanilide. In the reaction catalyzed by GGT, p-nitroaniline is liberated and is chromogenic, enabling this colored product to be measured spectrophotometrically. GGT L-γ-glutamil-3-karboksi-4-nitroanilit + glisilglisin L-γ-glutamil-glisilglisin + 5-amino-2-nitrobenzoat γ-glutamiltransferaz, L-γ-glutamil-3-karboksi-4-nitroanilidin γ-glutamil grubunu glisilglisine transfer eder. Serbest kalan 5-amino-2-nitrobenzoat miktarı numune içindeki GGT aktivitesi ile orantılıdır. Absorbanstaki artış fotometrik olarak ölçülerek tayin edilir.

86
Other Enzymes 5′-Nucleotidase activity is increased in cholestatic disorders with virtually no increase in activity in patients with bone disease. Measurement of 5′-nucleotidase can corroborate the elevation of ALP from a hepatic source. Leucine aminopeptidase (LAP), can be used for the same purpose but virtually never are. Isocitrate dehydrogenase activity is elevated in hepatocellular injury and parallel ALT and AST.. Again, as with LAP, they are virtually never used in routine laboratory assays
, can be used for the same purpose but virtually never are. Isocitrate dehydrogenase activity is elevated in hepatocellular injury and parallel ALT and AST.. Again, as with LAP, they are virtually never used in routine laboratory assays.")
87
Lactate Dehydrogenase

88
This cytosolic glycolytic enzyme catalyzes the reversible oxidation of lactate to pyruvate. LDH Lactate Pyruvate NAD NADH Laktat dehidrojenaz L-laktatın piruvata dönüşümünü katalize eder; işlem sırasında NAD+ NADH’ye indirgenir. NADH oluşumunun başlangıç hızı katalitik LDH aktivitesiyle doğru orantılıdır. Absorbanstaki artış 340 nm’de ölçülerek tayin edilir.

89
Tissue localization Sceletal muscle erythocytes liver heart kidney
LDH is present in varying amounts in the e cytoplasm of all cell in the body.Elevations of total LDH activity are therefore found in many pathological conditions. Tissue localization Sceletal muscle erythocytes liver heart kidney LDH x x x x x 700 LD, organizmada geniş bir dağılım gösterir. Sitozolik bir enzimdir. Kalp, iskelet kası, eritrositler, lenfositler, karaciğer, dalak, pankreas, böbrek ve akciğerlerde yüksek konsantrasyonlarda bulunur. LD aktivitesinin ölçümü için serum tercih edilir. Plazma örnekleri kullanılması önerilmez; çünkü trombositler yüksek konsantrasyonda LD aktivitesi içerdiği için kontamine olabilir. Örnek alındıktan sonra en kısa sürede serum ayrılmalıdır. Eritrositlerde seruma göre 500 kat daha fazla LD aktivitesi bulunduğu için hemolizli serum kullanılmamalıdır.

90
LDH 1 ; HHHH; H4 Heart, erythrocytes,kidney LDH 2 ; HHHM; H3M
Each LDH molecule consists of 4 subunits: Heart (H) and Muscle (M) type. İn the tissues the H and M type are combined into five izoenzymes. The H type predominates in tissues with high O2 consumption, the M type in tissues with high glycolytic activity. LDH 1 ; HHHH; H Heart, erythrocytes,kidney LDH 2 ; HHHM; H3M LDH 3 ; HHMM; H2M Spleen, lung, lymph nodes,platelets LDH 4 ; HMMM; H3M Liver, skeletal muscle LDH 5 ; MMMM; M4 LD, dört polipeptit zincirden oluşmuş bir tetramer yapısındadır. Yapıları farklı beş izoenzimi (LD1, LD2, LD3, LD4, LD5) tanımlanmıştır. Elektroforezde en hızlı göçen LD1 izoenzimidir, plazmada en yüksek konsantrasyonda bulunan LD2 izoenzimidir. Kalp kası, eritrositler ve renal kortekste LD1 ve LD2 izoenzimleri yüksek konsantrasyondadır. Akciğerler, lenfositler, dalak ve pankreasta LD3 izoenzimi hakimdir. İskelet kası ve karaciğerde LD4 ve LD5 izoenzimleri yüksek konsantrasyondadır
 and Muscle (M) type. İn the tissues the H and M type are combined into five izoenzymes. The H type predominates in tissues with high O2 consumption, the M type in tissues with high glycolytic activity. LDH 1 ; HHHH; H4 Heart, erythrocytes,kidney. LDH 2 ; HHHM; H3M. LDH 3 ; HHMM; H2M2 Spleen, lung, lymph nodes,platelets. LDH 4 ; HMMM; H3M. Liver, skeletal muscle. LDH 5 ; MMMM; M4. LD, dört polipeptit zincirden oluşmuş bir tetramer yapısındadır. Yapıları farklı beş izoenzimi (LD1, LD2, LD3, LD4, LD5) tanımlanmıştır. Elektroforezde en hızlı göçen LD1 izoenzimidir, plazmada en yüksek konsantrasyonda bulunan LD2 izoenzimidir. Kalp kası, eritrositler ve renal kortekste LD1 ve LD2 izoenzimleri yüksek konsantrasyondadır. Akciğerler, lenfositler, dalak ve pankreasta LD3 izoenzimi hakimdir. İskelet kası ve karaciğerde LD4 ve LD5 izoenzimleri yüksek konsantrasyondadır.")
91
The total LDH measurable in serum consists of the activities of the five isoenzymes LDH1 to LDH 5.
However, if the total LDH is elevated, quantitative differention of the isoenzymes can provide diagnostically useful organ-related information.

92
The upper reference range limit for total LDH activity in serum is around 150 IU/L.
LDH values are highest in newborns and infants; values do not change with age in adults, and there is no gender difference. Serum LDH levels become elevated in hepatitis; often, these increases are transient and return to normal by the time of clinical presentation because LDH isozymes originating in liver (LD4 and LD5) have relatively low activity in hepatocytes relative to plasma (about 500 times) and a half-life of approximately 4–6 hours.
 have relatively low activity in hepatocytes relative to plasma (about 500 times) and a half-life of approximately 4–6 hours.")
93
Preanalytic Variation
Even trace to slight hemolysis invalidates LD and LD isoenzyme analyses. Contact with the clot increases LD, and physical agitation of specimens, as occurs in most pneumatic tube systems, tends to cause some hemolysis and increased LD. Exercise has little effect on LD or its isoenzymes. Extreme exercise can cause LD1 to become greater than LD2. Total LDH increases transiently after blood transfusion but returns to baseline within 24 hours. Delayed separation of red cells from serum does not affect LD values for 1 to 2 days. Few drugs directly affect LDH activity, but granulocyte- macrophage colony-stimulating factor appears to increase LDH in parallel to the increase in white blood cell. (WBC) count .
 count .")
94
Measurement LD activity can be measured using either the forward (lactate-to-pyruvate) or the reverse (pyruvate-to-lactate) direction of the reaction. A vast majority of laboratories use the forward reaction. The reverse (pyruvate-to-lactate) reaction is used in a few laboratories currently because of faster reaction kinetics, the less costly cofactor (NADH) needed, and the smaller specimen volume requirement. Disadvantages of the pyruvate-to-lactate reaction include early loss of linearity of reaction kinetics, the effect of potent LD inhibitors in some NADH preparations, and use of suboptimal concentrations of pyruvate because of substrate inhibition. Also, lactate is a more specific substrate for this enzyme; pyruvate is less specific and serves as a substrate for such enzymes as pyruvate dehydrogenase. Electrophoretic separation of LD isoenzymes is typically used when quantitation of different isoenzymes is required; agarose gel is most commonly used. Quantitation usually uses the forward reaction, allowing detection of fluorescent NADH or a reduced formazan dye in a colorimetric development step.
 or the reverse (pyruvate-to-lactate) direction of the reaction. A vast majority of laboratories use the forward reaction. The reverse (pyruvate-to-lactate) reaction is used in a few laboratories currently because of faster reaction kinetics, the less costly cofactor (NADH) needed, and the smaller specimen volume requirement. Disadvantages of the pyruvate-to-lactate reaction include early loss of linearity of reaction kinetics, the effect of potent LD inhibitors in some NADH preparations, and use of suboptimal concentrations of pyruvate because of substrate inhibition. Also, lactate is a more specific substrate for this enzyme; pyruvate is less specific and serves as a substrate for such enzymes as pyruvate dehydrogenase. Electrophoretic separation of LD isoenzymes is typically used when quantitation of different isoenzymes is required; agarose gel is most commonly used. Quantitation usually uses the forward reaction, allowing detection of fluorescent NADH or a reduced formazan dye in a colorimetric development step.")
95
Serum LD is, on average, 30 IU/L higher than plasma LD, owing to release of LD from platelets.
LD is not stable on storage at 4° C because of cold lability of LD5. Specimens can be stored for up to 24 hours at room temperature with little change. Three days of storage at room temperature decreases total LD by about 20%. If specimens are frozen, LD5 decreases significantly and the isoenzyme pattern shifts with an artifactual increase in LD1 and decrease in LD5. Serum should not be frozen for assay of LD or for its isoenzymes.

96
Causes of Abnormal Results
LD is a highly nonspecific test; an abnormal value is not specific for damage to any particular organ. Relative amounts of LD, AST, and ALT (along with CK) may provide clues to the source of LD elevation. If LD is markedly elevated, but AST, ALT, and CK are normal or minimally increased, this suggests damage to cells such as red or white blood cells, kidney, lung, lymph nodes, or tumors. Increases in both CK and LD, with greater increases in AST than ALT, occur with cardiac or skeletal muscle injury. Increases in LD occur in liver disease, and LD can be elevated in hepatitis, although these increases by themselves are not specific to liver injury. In fulminant hepatic failure, the serum levels of ALT and LD both increase such that LD increases more rapidly initially. An ALT-LD index has been computed in these patients and was found to be a reliable predictor of survival in patients with this condition. Serum LD düzeyinde patolojik artışlar, enzimin yüksek konsantrasyonda bulunduğu dokulardan herhangi birinin enflamasyonu veya harabiyeti hallerinde saptanır. Serum LD düzeyi, miyokard enfarktüsü, kan hastalıkları, çeşitli karaciğer hastalıklarının tanısında ve hastalığın seyrini kontrolde değerlidir. Miyokard enfarktüsü, pernisiyöz anemi gibi kan hastalıkları, şok ve hipoksi ile beraber olan dolaşım yetmezliği durumlarında serum LD düzeyinde belirgin artış görülür.
 may provide clues to the source of LD elevation. If LD is markedly elevated, but AST, ALT, and CK are normal or minimally increased, this suggests damage to cells such as red or white blood cells, kidney, lung, lymph nodes, or tumors. Increases in both CK and LD, with greater increases in AST than ALT, occur with cardiac or skeletal muscle injury. Increases in LD occur in liver disease, and LD can be elevated in hepatitis, although these increases by themselves are not specific to liver injury. In fulminant hepatic failure, the serum levels of ALT and LD both increase such that LD increases more rapidly initially. An ALT-LD index has been computed in these patients and was found to be a reliable predictor of survival in patients with this condition. Serum LD düzeyinde patolojik artışlar, enzimin yüksek konsantrasyonda bulunduğu dokulardan herhangi birinin enflamasyonu veya harabiyeti hallerinde saptanır. Serum LD düzeyi, miyokard enfarktüsü, kan hastalıkları, çeşitli karaciğer hastalıklarının tanısında ve hastalığın seyrini kontrolde değerlidir. Miyokard enfarktüsü, pernisiyöz anemi gibi kan hastalıkları, şok ve hipoksi ile beraber olan dolaşım yetmezliği durumlarında serum LD düzeyinde belirgin artış görülür.")
97
Causes of Abnormal Results
Serum elevations of LD and ALP frequently occur in space-occupying lesions of the liver; most cases are identified as metastatic carcinoma or primary hepatocellular carcinoma. In many conditions, such as shock and metastatic carcinoma, LD is increased because of damage to multiple organs, so that mixed patterns can be seen.

98
Causes of Abnormal Results
Marked elevations of LD (>5 to 10 times normal) are seen in megaloblastic anemia, hemolytic anemias, malignancies (particularly lymphoma and leukemia), sepsis or other causes of shock, and cardiopulmonary arrest. In cases where the cause of elevated LD cannot be determined by other means, LD isoenzymes may be useful in determining the source of injury. In normal serum, the LD isoenzymes, in decreasing order of activity, are 2 > 1 > 3 > 4 > 5. In germ cell tumors (particularly seminoma and dysgerminoma), LD1 is increased and can serve as a tumor marker.
 are seen in megaloblastic anemia, hemolytic anemias, malignancies (particularly lymphoma and leukemia), sepsis or other causes of shock, and cardiopulmonary arrest. In cases where the cause of elevated LD cannot be determined by other means, LD isoenzymes may be useful in determining the source of injury. In normal serum, the LD isoenzymes, in decreasing order of activity, are 2 > 1 > 3 > 4 > 5. In germ cell tumors (particularly seminoma and dysgerminoma), LD1 is increased and can serve as a tumor marker.")
99
Changes in Serum LDH and LDH Isoenzymes in MI
Myocardial Infarction (MI) Up to 10 x normal A rise in LDH occurs 8-12 hours after the onset of pain. Peak activity occurs between hours. Activity returns to normal by the 5th-6th day but may remain elevated up to 10 days. The LDH-1 isoenzyme is increased: LDH-1>LDH-2 pattern increases the specificity of the test. Miyokard enfarktüsünde serum LD düzeyi,8-12 saat sonra yükselir, saatte pik değerine erişir, 5-10 günde normale döner. CPK (CK) artışıyla birlikte olan LD1 / LD2 oranı artışı, akut miyokard enfarktüsünde (AMI) tanı koydurucudur.
 Up to 10 x normal. A rise in LDH occurs 8-12 hours after the onset of pain. Peak activity occurs between hours. Activity returns to normal by the 5th-6th day but may remain elevated up to 10 days. The LDH-1 isoenzyme is increased: LDH-1>LDH-2 pattern increases the specificity of the test. Miyokard enfarktüsünde serum LD düzeyi,8-12 saat sonra yükselir, saatte pik değerine erişir, 5-10 günde normale döner. CPK (CK) artışıyla birlikte olan LD1 / LD2 oranı artışı, akut miyokard enfarktüsünde (AMI) tanı koydurucudur.")
100
Acute MI markers

101
Relative or Absolute Change
Changes in Serum LDH and LDH Isoenzymes in Certain Disease States. Variable increases, especially LDH-5, depending on the amount of trauma. Muscular trauma due to physical exercise or crush injuries >10 x normal. Cancer, Metastasis 2 x normal. LDH-5 predominates. Cirrhosis and Obstructive Jaundice Up to 5 x normal. LDH-5 predominates Viral Hepatitis and Infectious Mononucleosis Increases in total LDH >5 x normal. Rises in the LDH-1 and LDH-2 isoenzymes. Megaloblastic Anemia Up to 10 x normal A rise in LDH occurs 8-12 hours after the onset of pain. Peak activity occurs between hours. Activity returns to normal by the 5th-6th day but may remain elevated up to 10 days. The LDH-1 isoenzyme is increased: a LDH-1>LDH-2 pattern increases the specificity of the test. Myocardial Infarction (MI) Relative or Absolute Change Condition Megaloblastik anemide de LD1 / LD2 oranı artar. Akut viral hepatit, siroz, toksik karaciğer nekrozu, özellikle karaciğere metastaz yapmış karsinom, iskelet kası hastalıkları, akciğer embolisi, pnömoni, lenfositoz, akut pankreatit, tıkanma sarılığı gibi durumlarda serum LD düzeyinde orta derecede artış saptanır. Pulmoner emboli, pnömoni, lenfositoz, akut pankreatit ve karsinomada LD3 artışı ön plandadır. Kanser, metastaz ve müsküler distrofide LD4 ve LD5 artar. Viral hepatit, siroz ve tıkanma sarılığında LD5 artar.
 Relative or Absolute Change. Condition. Megaloblastik anemide de LD1 / LD2 oranı artar. Akut viral hepatit, siroz, toksik karaciğer nekrozu, özellikle karaciğere metastaz yapmış karsinom, iskelet kası hastalıkları, akciğer embolisi, pnömoni, lenfositoz, akut pankreatit, tıkanma sarılığı gibi durumlarda serum LD düzeyinde orta derecede artış saptanır. Pulmoner emboli, pnömoni, lenfositoz, akut pankreatit ve karsinomada LD3 artışı ön plandadır. Kanser, metastaz ve müsküler distrofide LD4 ve LD5 artar. Viral hepatit, siroz ve tıkanma sarılığında LD5 artar.")
102
Creatine Phosphokinase
CK

103
CK requires metalloactivators, especially Mg++
Creatine Kinase (CK) is a cytoplasmic and mitochondrial enzyme that catalyzes both the formation of ATP and reversible phosphorylation of creatine with ATP as a donor phosphate group. CK requires metalloactivators, especially Mg++ CK activity is especially important in muscle tissue, where it catalyzes the synthesis of Creatine Phosphate, a high energy storage molecule. Upon muscle contraction, the phosphate group is used to form ATP to provide immediate energy for the muscles. CK (CPK), kas kasılması sırasında kreatin fosfattan ATP oluşumunu sağlayarak kas kasılma-gevşemesi için gerekli olan ATP’nin hızla eksilmesini önleyen enzimdir.
 is a cytoplasmic and mitochondrial enzyme that catalyzes both the formation of ATP and reversible phosphorylation of creatine with ATP as a donor phosphate group. CK requires metalloactivators, especially Mg++ CK activity is especially important in muscle tissue, where it catalyzes the synthesis of Creatine Phosphate, a high energy storage molecule. Upon muscle contraction, the phosphate group is used to form ATP to provide immediate energy for the muscles. CK (CPK), kas kasılması sırasında kreatin fosfattan ATP oluşumunu sağlayarak kas kasılma-gevşemesi için gerekli olan ATP’nin hızla eksilmesini önleyen enzimdir.")
104
Tissue sources The largest distribution of CK is found in skeletal muscle. Other tissue sources : brain, rectum, stomach, bladder, colon, uterus, prostate, small intestine and kidney. Negligible in the liver, placenta and thyroid tissue.

105
CK is composed of three types of dimers:
This enzyme has two major isoenzymes, M and B, each of which has the same activity. CK is composed of three types of dimers: CK- MM (mainly in skeletal muscle), CK- MB (found mainly in cardiac tissue), and CK- BB (found predominantly in brain and intestine). CK, iki subüniteden oluşan dimer yapıdadır. CK-1 (CK-BB), CK-2 (CK-MB) ve CK-3 (CK-MM) diye adlandırılan üç izoenzimi tanımlanmıştır. Hücrede bu izoenzimlerin her üçü sitozolde veya miyofibriler yapılara bağlı olarak bulunur.
, CK- MB (found mainly in cardiac tissue), and. CK- BB (found predominantly in brain and intestine). CK, iki subüniteden oluşan dimer yapıdadır. CK-1 (CK-BB), CK-2 (CK-MB) ve CK-3 (CK-MM) diye adlandırılan üç izoenzimi tanımlanmıştır. Hücrede bu izoenzimlerin her üçü sitozolde veya miyofibriler yapılara bağlı olarak bulunur.")
106
The major CK isoenzyme in the serum of healthy subjects is CK-MM, where it represents % of total CK activity. CK-MB is found in concentrations of less than %6 normally, whereas CK-BB is rarely detected.

107
Skeletal muscle injury can occur from a variety of sources.
Direct trauma, as occurs with physical injury (including contact sports), surgery, strenuous exercise, and intramuscular injection, are common causes of mild elevations of CK (up to about five to six times reference limits). In these situations, CK typically increases rapidly and then falls quickly, returning to baseline with a half-life of approximately 24 hours. Serum CK düzeyinde fizyolojik artışlar olabilir. Yeni doğanda hafifçe yüksektir. Erkeklerde kas kitlesi fazlalığı nedeniyle yüksektir. Doğum yapanda da birkaç gün yüksek bulunur. İskelet kasını, kalbi, merkezi sinir sistemini ve tiroidi etkileyen birçok hastalıkta CK aktivitesi artar. Kas yaralanmalarında, cerrahi girişimlerden sonra, yoğun fizik egzersizden sonra, hipotiroidizmde, alkolizmde, akut psikotik nöbetlerde, bazı kafa travması olgularında serum CK düzeyinde orta derecede artış saptanır. Orta derecede egzersiz ve kas içi enjeksiyonlar da serum CK düzeyinde artışlara neden olur.
, surgery, strenuous exercise, and intramuscular injection, are common causes of mild elevations of CK (up to about five to six times reference limits). In these situations, CK typically increases rapidly and then falls quickly, returning to baseline with a half-life of approximately 24 hours. Serum CK düzeyinde fizyolojik artışlar olabilir. Yeni doğanda hafifçe yüksektir. Erkeklerde kas kitlesi fazlalığı nedeniyle yüksektir. Doğum yapanda da birkaç gün yüksek bulunur. İskelet kasını, kalbi, merkezi sinir sistemini ve tiroidi etkileyen birçok hastalıkta CK aktivitesi artar. Kas yaralanmalarında, cerrahi girişimlerden sonra, yoğun fizik egzersizden sonra, hipotiroidizmde, alkolizmde, akut psikotik nöbetlerde, bazı kafa travması olgularında serum CK düzeyinde orta derecede artış saptanır. Orta derecede egzersiz ve kas içi enjeksiyonlar da serum CK düzeyinde artışlara neden olur.")
108
An important clinical disorder associated with acute muscle injury is neuroleptic malignant syndrome, a rare complication of treatment with phenothiazines or other psychotropic agents. Typically, affected individuals present with muscle rigidity, fever, and elevated WBC counts; CK is considered a diagnostic test for this disorder. Prompt recognition and treatment are necessary to prevent death from this syndrome; discontinuation of medications and use of the muscle-stabilizing agent dantrolene are the cornerstones of treatment. Erken teşhis ve tedavi bu sendromda ölümden korumak için gereklidir. Tedavinin temel taşlarından

109
Chronic damage to muscle causes more persistent elevation of CK.
Common causes of chronic muscle injury include medications (particularly 3-hydroxy-3-methylglutaryl- coenzyme A reductase inhibitors and glucocorticoids), congenital myopathies (such as Duchenne's muscular dystrophy), inflammatory disorders (such as polymyositis and dermatomyositis), hypothyroidism, and alcohol abuse. In chronic myopathies, CK-MB is often increased, reflecting its production by regenerating muscle. Kas yaralanmalarında, cerrahi girişimlerden sonra, yoğun fizik egzersizden sonra, hipotiroidizmde, alkolizmde, akut psikotik nöbetlerde, bazı kafa travması olgularında serum CK düzeyinde orta derecede artış saptanır. Orta derecede egzersiz ve kas içi enjeksiyonlar da serum CK düzeyinde artışlara neden olur.
, congenital myopathies (such as Duchenne s muscular dystrophy), inflammatory disorders (such as polymyositis and dermatomyositis), hypothyroidism, and alcohol abuse. In chronic myopathies, CK-MB is often increased, reflecting its production by regenerating muscle. Kas yaralanmalarında, cerrahi girişimlerden sonra, yoğun fizik egzersizden sonra, hipotiroidizmde, alkolizmde, akut psikotik nöbetlerde, bazı kafa travması olgularında serum CK düzeyinde orta derecede artış saptanır. Orta derecede egzersiz ve kas içi enjeksiyonlar da serum CK düzeyinde artışlara neden olur.")
110
With severe acute damage to muscle, a clinical picture termed rhabdomyolysis may develop.
In such situations, CK-MB/total CK may be elevated above normal, in the absence of myocardial infarction (cardiac troponin levels are normal); this is commonly seen in patients with inflammatory muscle disease. In addition to normal cardiac troponin levels with elevated CK levels, two distinct isoforms (representing fast or slow skeletal fiber types) of serum skeletal troponin I may be identified.
; this is commonly seen in patients with inflammatory muscle disease. In addition to normal cardiac troponin levels with elevated CK levels, two distinct isoforms (representing fast or slow skeletal fiber types) of serum skeletal troponin I may be identified.")
111
Acetylcholinesterase

112
AChE and PChE are two different enzymes produced by different tissues that are able to cleave acetylcholine, one of the body's major neurotransmitters. PChE is important in the cleavage of acetylcholine antagonists such as succinylcholine and mivacurium, muscle relaxants used during surgery.

113
Pancreatic Enzymes Amylase and Lipase

114
Amylase

115
Two isoenzymes for 1. Salivary 2. Pancreatic
In normal conditions, about 60% of circulating amylase is salivary and 40% pancreatic.

116
Plasma specimens that have been anticoagulated with citrate or oxalate should be avoided for amylase determination because amylase is a calcium-containing enzyme. Heparinized plasma specimens do not interfere with the amylase assay. Diagnosis is confirmed by detection of elevated serum amylase threefold above normal. It peaks in 20–30 hours, often at 10–20 times the upper reference limit . Amylase returns to normal in 48–72 hours.

117
Elevated values persisting longer than this suggest continuing necrosis or possible pseudocyst formation. Serum amylase sensitivity is 72%, and specificity is 99%. Serum amylase has poor sensitivity for pancreatitis; it is not increased in about 20% of patients with pancreatitis.

118
Serum amylase increases nonspecifically in many acute abdominal conditions.
In hyperlipidemic patients with pancreatitis, normal serum and urine amylase levels are frequently encountered. The spuriously normal levels are believed to be the result of suppression of amylase activity by triglyceride or by a circulating inhibitor in serum. Serum amylase levels do not correlate with cause or severity of pancreatitis. Amylase is also produced by the salivary glands.

119
The urine amylase activity rises promptly, often within several hours of the rise in serum activity, and may remain elevated after the serum level has returned to the normal range. Values greater than 1000 Somogyi units/hour are seen almost exclusively in patients with acute pancreatitis. In a majority of patients with acute pancreatitis, serum amylase activity is elevated, and a concomitant increase in urine amylase activity occurs.

120
Lower than normal serum amylase activity may be found in patients with chronic pancreatitis and has been seen in such diverse conditions as congestive heart failure, pregnancy (during the second and third trimesters), gastrointestinal (GI) cancer, bone fracture, and pleurisy.
, gastrointestinal (GI) cancer, bone fracture, and pleurisy.")
121
Serum amylase may be elevated in patients with pancreatic carcinoma, but often too late to be diagnostically useful. Serum amylase activity may also be elevated in patients with cholecystitis, peptic ulcer, renal transplant, viral hepatitis, or ruptured ectopic pregnancy, or post gastrectomy.

122
Lipase

123
The pancreas is the major and primary source of serum lipase.
Lipase is not present in the salivary glands Serum lipase is more specific for the diagnosis of acute pancreatitis. Serum lipase increases in 4–8 hours and remains elevated for 8– 14 days. Increased lipase activity rarely lasts longer than 14 days; prolonged increases suggest a poor prognosis or the presence of a pancreatic cyst. Calcium is necessary for maximal lipase activity, but at higher concentrations it has an inhibitory effect. Similar to serum albumin, bile salts prevent the denaturation of lipase at the interface. Heavy metals and quinine inhibit lipase activity.

124
Lipase is filtered by the glomeruli owing to its low molecular weight; it is normally completely reabsorbed by the proximal tubules and is absent from normal urine. In patients with failure of renal tubular reabsorption caused by renal disorders, lipase is found in the urine. Urine lipase activity in the absence of pancreatic disease is inversely related to creatinine clearance. Kreatinin klerensi ile ters ilişkili.

125
Serum lipase is stable up to 1 week at room temperature and may be kept stable longer if it is refrigerated or frozen. The optimal reaction temperature is about 40° C. The optimal pH is 8.8. Serum is the specimen of choice for blood lipase assays. Icterus, lipemia, and hemolysis do not interfere with turbidimetric lipase assays.

126
Both serum lipase and amylase are useful in ruling out acute pancreatitis.
Although determination of serum lipase has diagnostic advantages over serum amylase for acute pancreatitis, this value is not specific for acute pancreatitis. Serum lipase may also be elevated in patients with chronic pancreatitis, obstruction of the pancreatic duct, and nonpancreatic conditions, including renal disease, acute cholecystitis, intestinal obstruction or infarction, duodenal ulcer, and liver disease, as well as alcoholism and diabetic ketoacidosis, and in patients who have undergone ERCP. Patients with trauma to the abdomen have increases in both serum amylase and lipase. Elevation of serum lipase activity in patients with mumps strongly suggests significant pancreatic involvement by the disease. Mumps – kabakulak pankreatik tutulumu

127
Acid Phosphatase

128
Acid Phosphatase Greatest concentrations occur in prostate, liver, spleen, and bone Lysosomal, prostatic, erythrocyte, macrophage, and osteoclastic ACP are five important types found in humans. Normally, concentrations in serum are low The activity of erythrocyte ACP can be distinguished from that of the other ACP isoenzymes in that it is inhibited by 2% formaldehyde solution and 1 mM cupric sulfate solution. This is in contrast to the other isoenzymes, which are not inhibited by these agents. In addition, erythrocyte ACP is not inhibited by 20 mM tartrate solution, which does inhibit the other isoenzymes. Tartrate-resistant acid phosphatase (TRAP) is present in certain chronic leukemias and some lymphomas Bakır sülfat
 is present in certain chronic leukemias and some lymphomas. Bakır sülfat.")
129
Acid Phosphatase Usually the test is utilized for the measurement of prostatic serum ACP in the diagnosis or monitoring of prostatic adenocarcinoma.

132
Alkalen Fosfataz Referans aralıkları

139
Metastatik mide Ca

148
AKUT PANKREATİT

153
Metastatik mide Ca

157
Metastatik meme Ca

159
Metastatik prostat Ca

160
KOLESİSTİT

162
Metastatik Akciğer Ca

163
SAFRA KESESİ TAŞI

165
Parotitis?

166
Hepatit

167
Which disease?

168
Liver disease Hepatocellular damage best assessed by ALT or AST.
Biliary damage best assessed by ALP or GGT. Pattern of enzyme changes will often show which is predominant.

169
Cardiac damage Total CK and more especially CK-MB isoenzyme most useful markers of cardiac damage. CK-MB is the most specific marker of myocardial infarct, positive in greater than 98% of patients. Other useful enzymes are AST and LDH (especially LD1 and LD2 isoenzymes) though these may be raised in liver diseases also.
 though these may be raised in liver diseases also.")
170
Pancreas disease Acute pancreatitis usually shows an elevation of amylase, which is small enough to pass through the glomerulus and appear in the urine.

171
Bone disease Alkaline phosphatase is raised in bone diseases that have a rise in osteoblastic activity, e.g. Pagets disease, rickets, etc. There is a bone isoenzyme which may be differentiated from the other isoenzymes.

172
Skeletal muscle disease
Total CK, and more especially CK-MM isoenzyme, most sensitive marker of skeletal muscle damage, e.g. muscular dystrophies, polymyositis, etc. AST and LDH may also be raised.

173
Prostate disease Acid phosphatase (ACP) is generally raised if prostate carcinoma has spread outside the capsule. Useful enzyme to monitor effect of therapy. Nowadays replaced by prostate specific antigen (PSA).
.")
174
Which Enzyme?

175
AST - Useful in liver disease, cardiac damage, skeletal muscle disease; may be raised with haemolysis. ALT - Useful in liver disease, especially hepatocellular, more specific than AST, but longer half life. ALP - Useful in liver disease, especially biliary disease and cholestasis; bone disease with osteoblastic involvement and carcinoma with osteoblastic metastases. GGT - Raised in virtually all liver diseases. Very sensitive (almost too much so), inducible enzyme, i.e. raised by certain drugs and alcohol. Associated with biliary system and may be used to differentiate between liver and bone ALP.
, inducible enzyme, i.e. raised by certain drugs and alcohol. Associated with biliary system and may be used to differentiate between liver and bone ALP.")
176
CK - has three isoenzyme forms:
CK-MM found in high concentration in skeletal muscle CK-MB accounts for up to 20% of cardiac CK activity CK-BB found in neurological tissue Total CK is raised after MI or any myocardial damage (e.g. pacemaker insertion, cardiac surgery etc.) and skeletal muscle damage. CK-MB will differentiate between cardiac and skeletal muscle damage.
 and skeletal muscle damage. CK-MB will differentiate between cardiac and skeletal muscle damage.")
177
L-Alanin + 2-oksoglutarat piruvat + L-glutamat LDH
ALT L-alanin ile 2-oksoglutarat arasındaki reaksiyonu katalize eder. Oluşan piruvat L-laktat ve NAD+’nın oluştuğu laktat dehidrojenazın (LDH) katalize ettiği bir reaksiyonda NADH tarafından indirgenir. Piridoksal fosfat, amino transfer reaksiyonunda bir koenzim olarak görev yapar. Enzim aktivasyonunun tam olmasını sağlar. ALT L-Alanin + 2-oksoglutarat piruvat + L-glutamat LDH Piruvat + NADH + H L-laktat + NAD+ NADH yükseltgenmesinin hızı katalitik ALT aktivitesiyle doğru orantılıdır. Absorbanstaki azalma 340 nm’de ölçülerek tayin edilir. Test prensibi
 katalize ettiği bir reaksiyonda NADH. tarafından indirgenir. Piridoksal fosfat, amino transfer reaksiyonunda bir koenzim olarak görev yapar. Enzim aktivasyonunun tam olmasını sağlar. ALT. L-Alanin + 2-oksoglutarat piruvat + L-glutamat. LDH. Piruvat + NADH + H+ L-laktat + NAD+ NADH yükseltgenmesinin hızı katalitik ALT aktivitesiyle doğru orantılıdır. Absorbanstaki azalma 340 nm’de ölçülerek tayin edilir. Test prensibi.")
178
Serum (hemolizsiz). Plazma (hemolizsiz): Li-heparin veya EDTA plazma. Diğer antikoagülanları kullanmayın. Tercih edilen örnek hemolize olmayan serumdur. Stabilite: °C’de 3 gün 2-8 °C’de 7 gün -70 °C’de > 7 gün

179
Numune içindeki AST oksaloasetat ve L-glutamatın oluşması için L- aspartat ile 2-oksoglutarat arasında bir amino grubunun transferini katalize eder. Oksaloasetat daha sonra NAD+’nın oluşması için malat dehidrojenaz (MDH) varlığında NADH ile reaksiyona girer. Piridoksal fosfat, amino transfer reaksiyonunda bir koenzim olarak görev yapar. Enzim aktivasyonunun tam olmasını sağlar. AST L-Aspartat + 2-oksoglutarat oksaloasetat + L-glutamat MDH Oksaloasetat + NADH + H L-malat + NAD+ NADH yükseltgenmesinin hızı katalitik AST aktivitesiyle doğru orantılıdır. Absorbanstaki azalma 340 nm’de ölçülerek tayin edilir.

180
Serum (hemolizsiz). Standart numune alma tüplerini kullanarak serum alın.
Plazma (hemolizsiz): Li-heparin veya EDTA plazma. Diğer antikoagülanları kullanmayın. Tercih edilen örnek hemolize olmayan serumdur. Stabilite: °C’de 7 gün 2-8 °C’de 7 gün
: Li-heparin veya EDTA plazma. Diğer antikoagülanları kullanmayın. Tercih edilen örnek hemolize olmayan serumdur. Stabilite: °C’de 7 gün. 2-8 °C’de 7 gün.")
181
ALP Standardize edilmiş bir yönteme göre kolorimetrik test p-nitrofenil fosfat, ortamda magnezyum ve çinko iyonları bulunduğunda, fosfataz aracılığıyla fosfat ve p-nitrofenole bölünür. ALP p-nitrofenil fosfat + H2O fosfat + p-nitrofenol Açığa çıkan p-nitrofenol katalitik ALP aktivesi ile doğrudan orantılıdır. Absorbanstaki artış 409 nm’de ölçülerek tayin edilir.

182
Serum Plazma: Heparin (Li-, Na-, NH4 +-) plazma. Stabilite: 15-25°C’de 7 gün 2-8°C’de 7 gün -20°C’de 2 ay

183
Sınırlamalar - etkileşim
Kriter: Başlangıç değerinin ±%10’u içerisinde telafi edilir. Serum, plazma İkter Belirgin etkileşim yok. Hemoliz H indeksi 250 olana kadar belirgin etkileşim yok (yaklaşık hemoglobin konsantrasyonu: 155 μmol/L veya 250 mg/dL). Lipemi Belirgin etkileşim yok. Diğer Çok nadir durumlarda, gammopati, özellikle tip IgM (Waldenström makroglobulinemi) güvenilmez sonuçlara neden olabilir.
. Lipemi Belirgin etkileşim yok. Diğer Çok nadir durumlarda, gammopati, özellikle tip IgM (Waldenström makroglobulinemi) güvenilmez sonuçlara neden olabilir.")
Benzer bir sunumlar
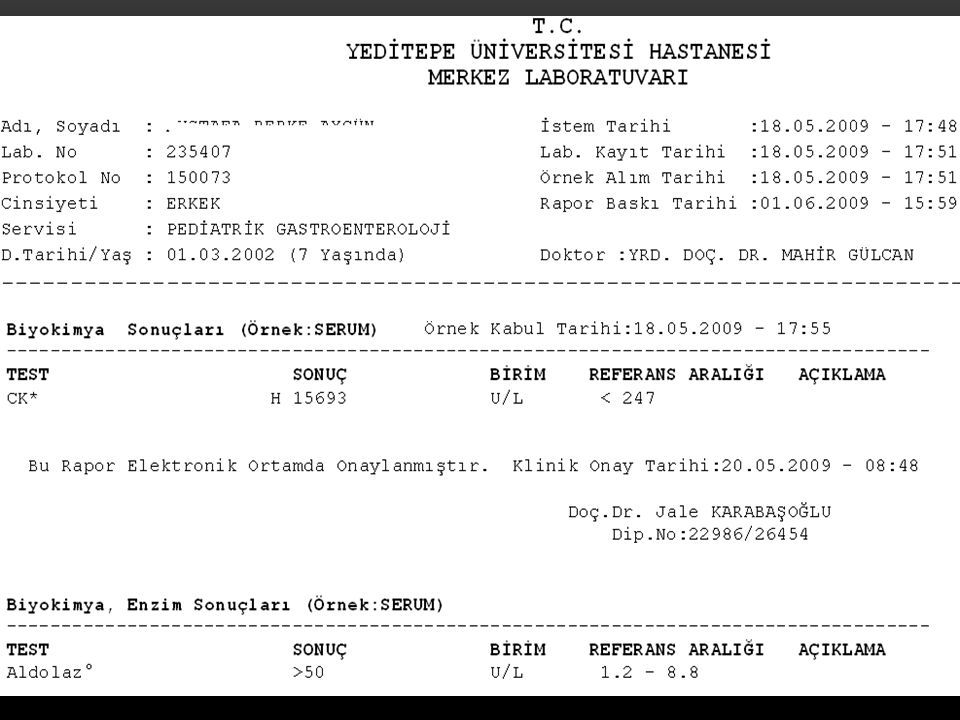
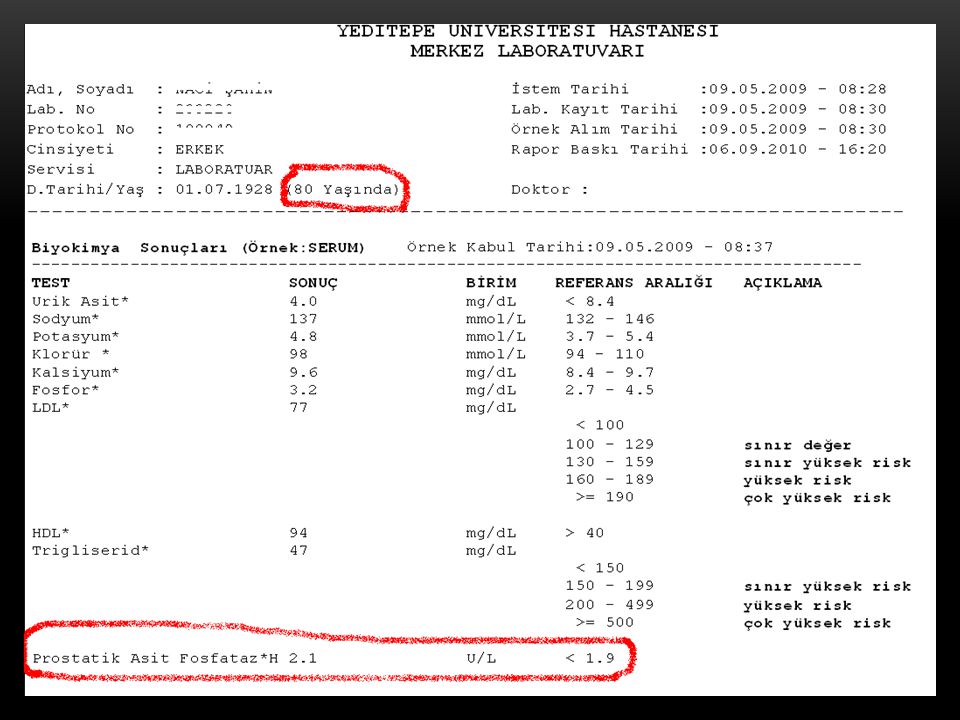
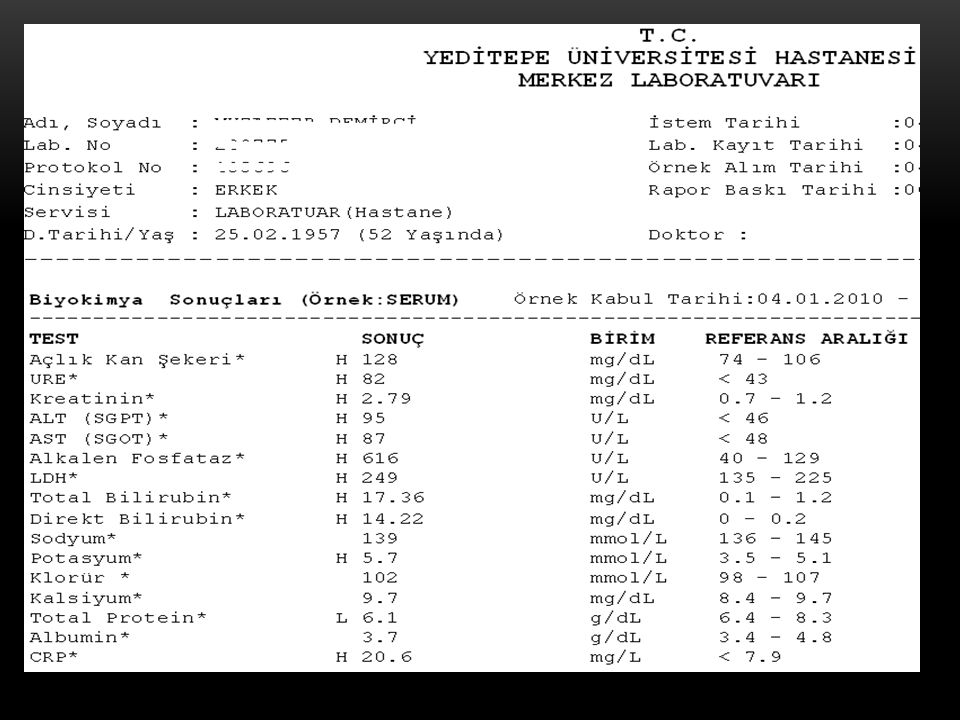
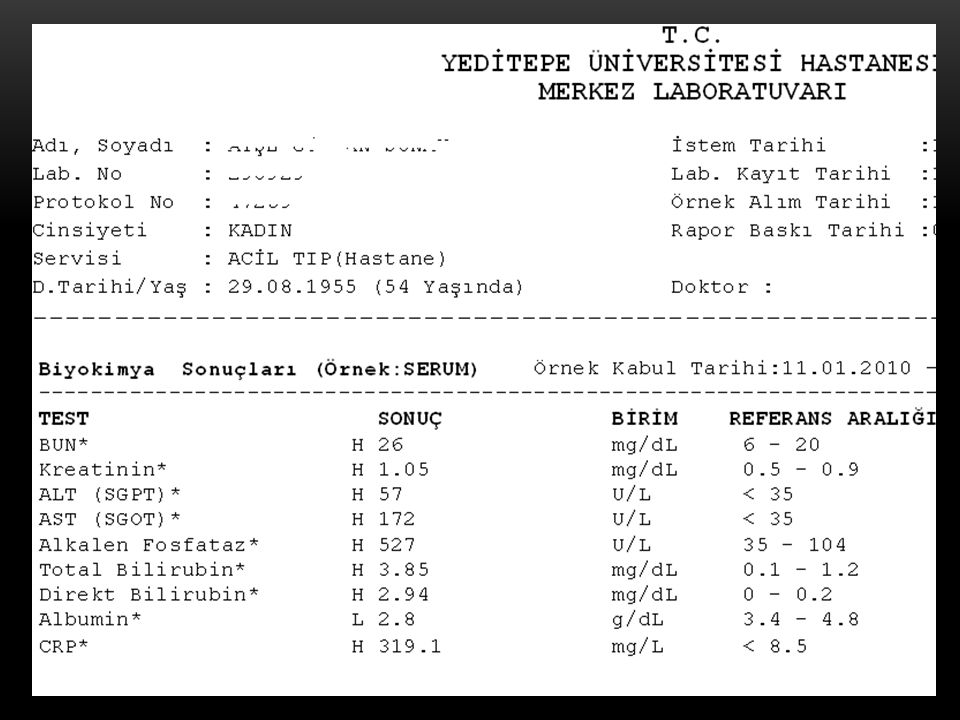

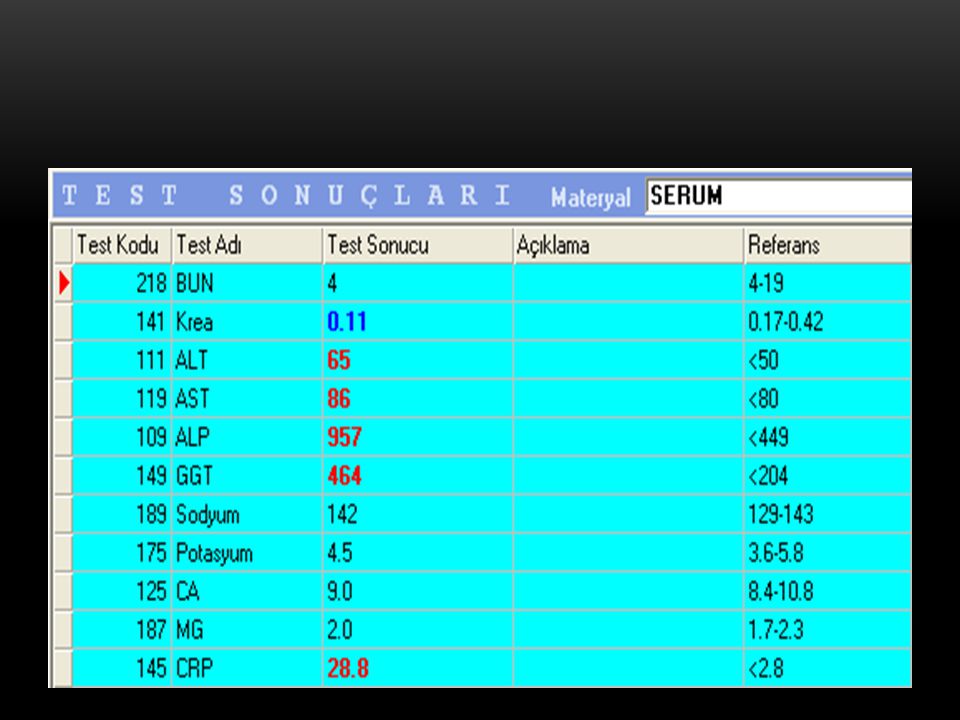
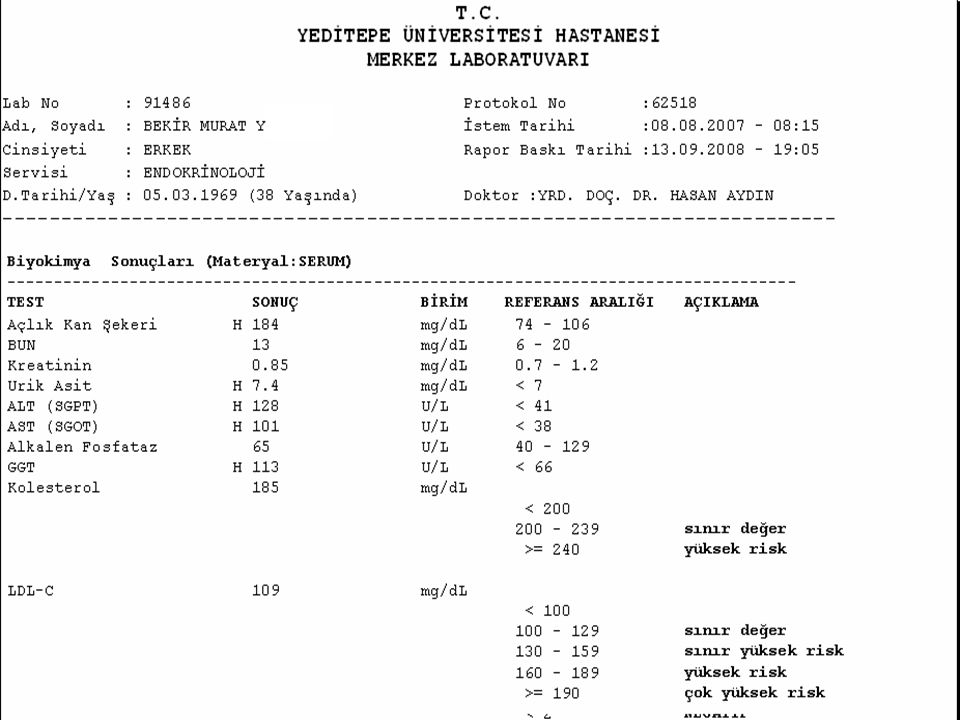
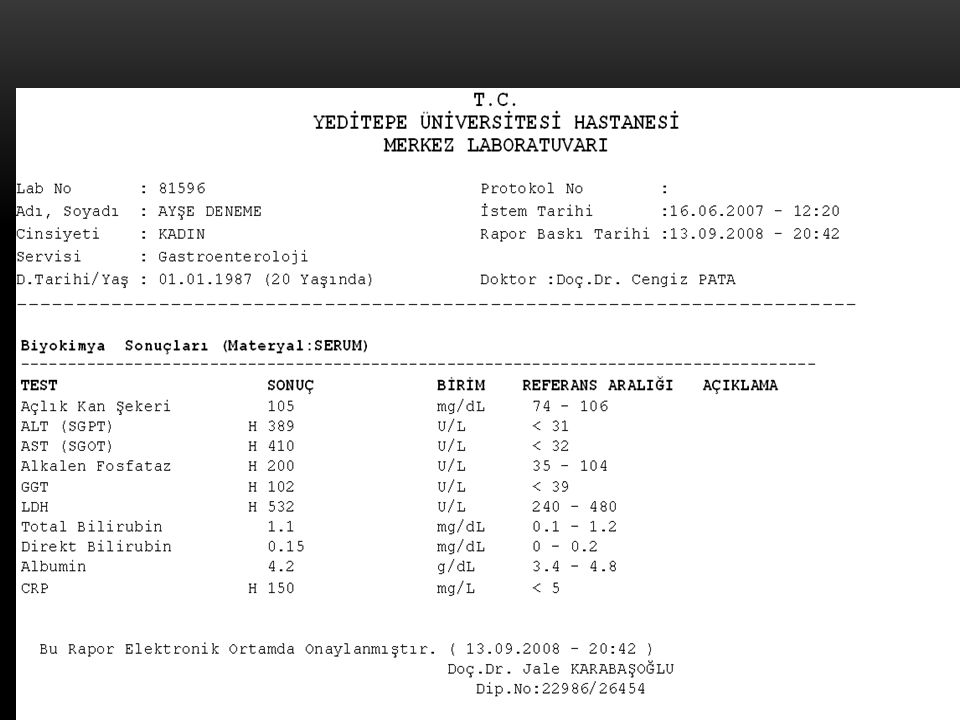
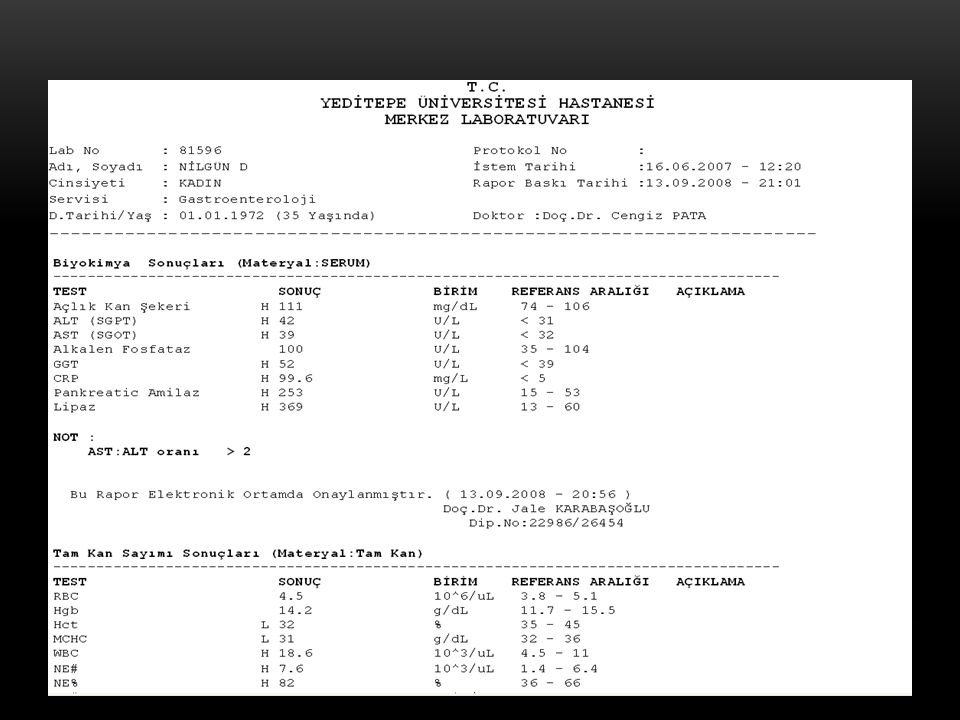

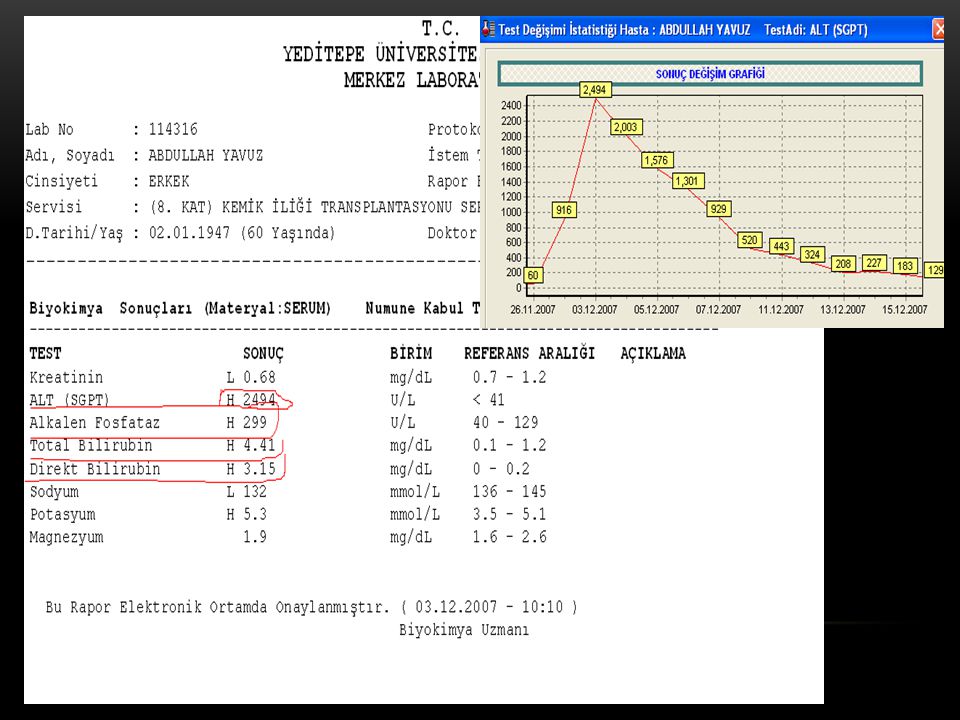
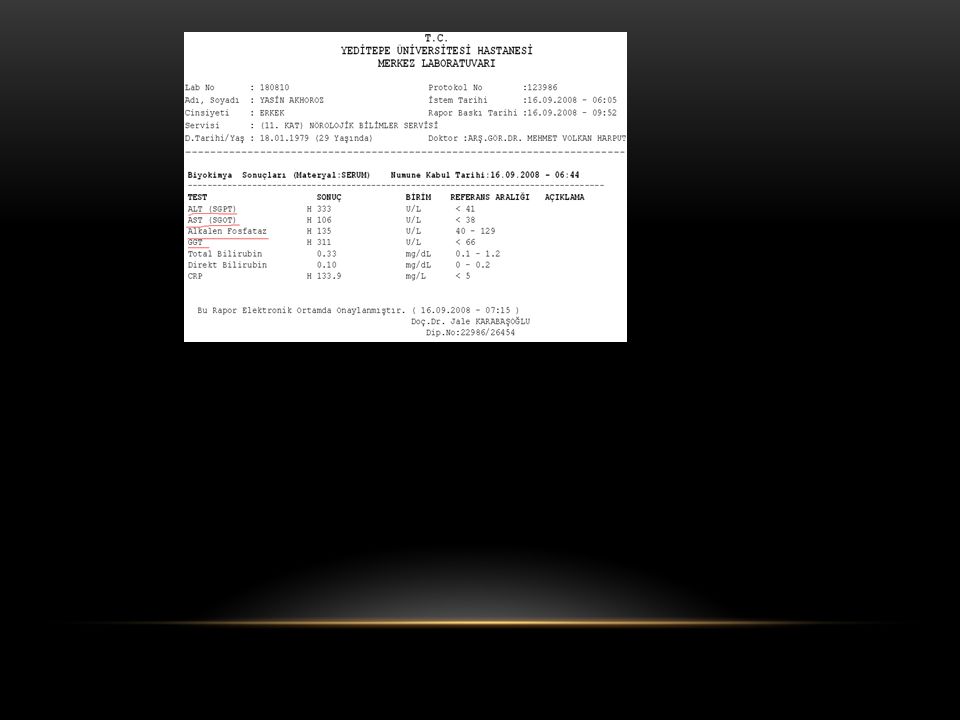
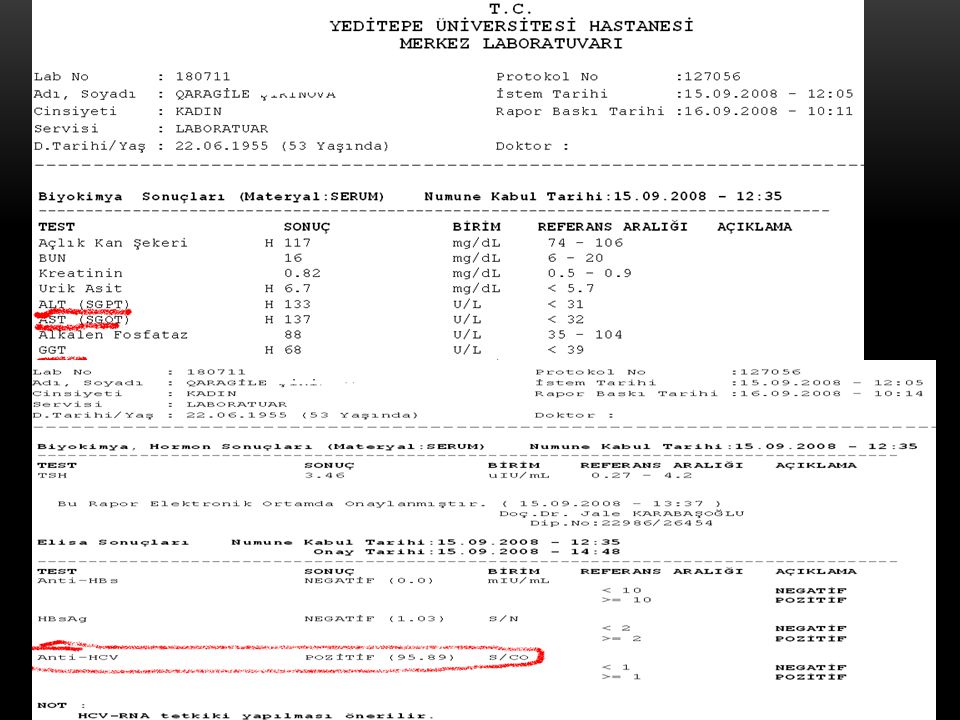
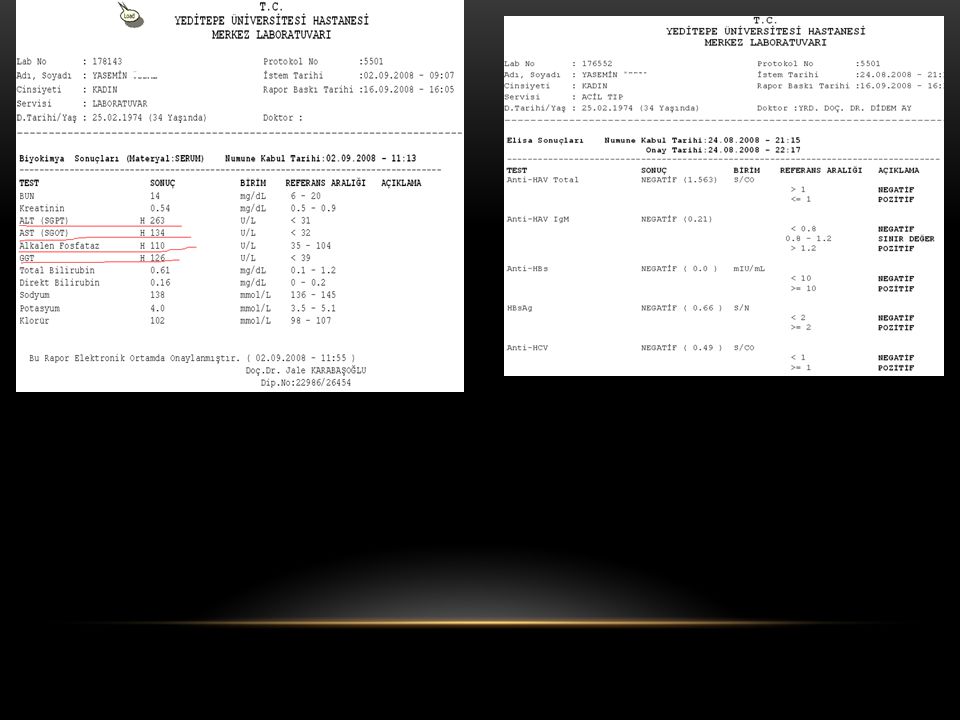
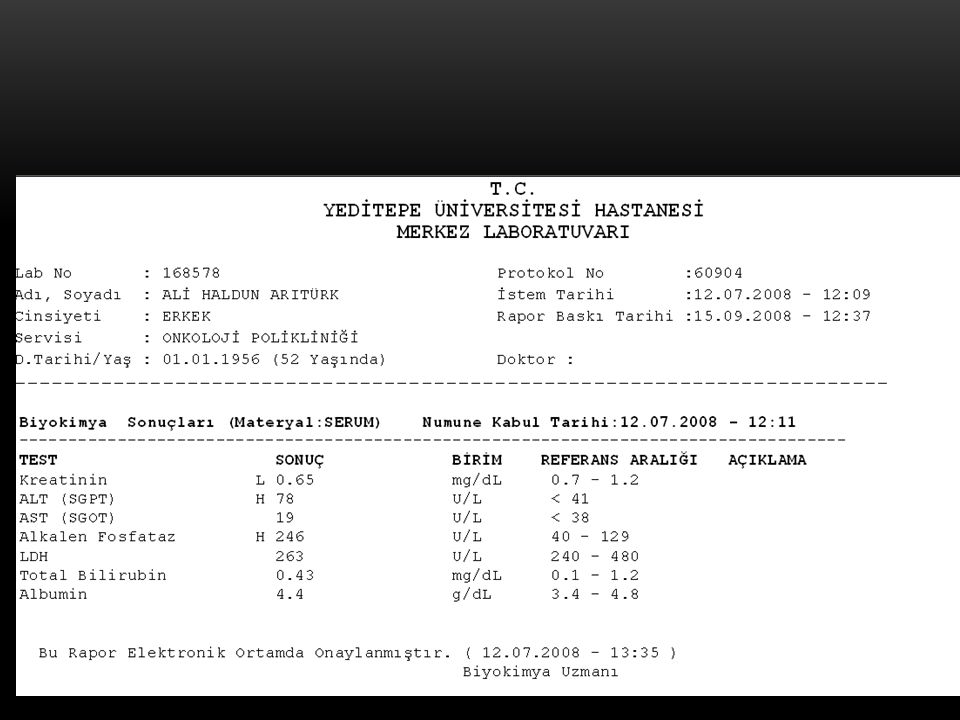
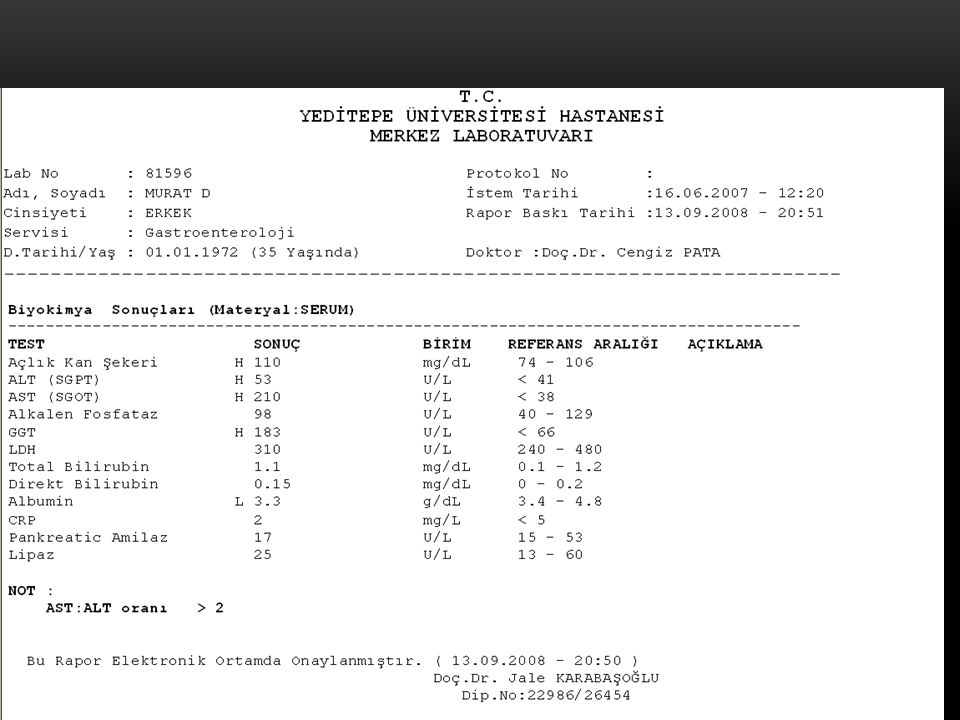
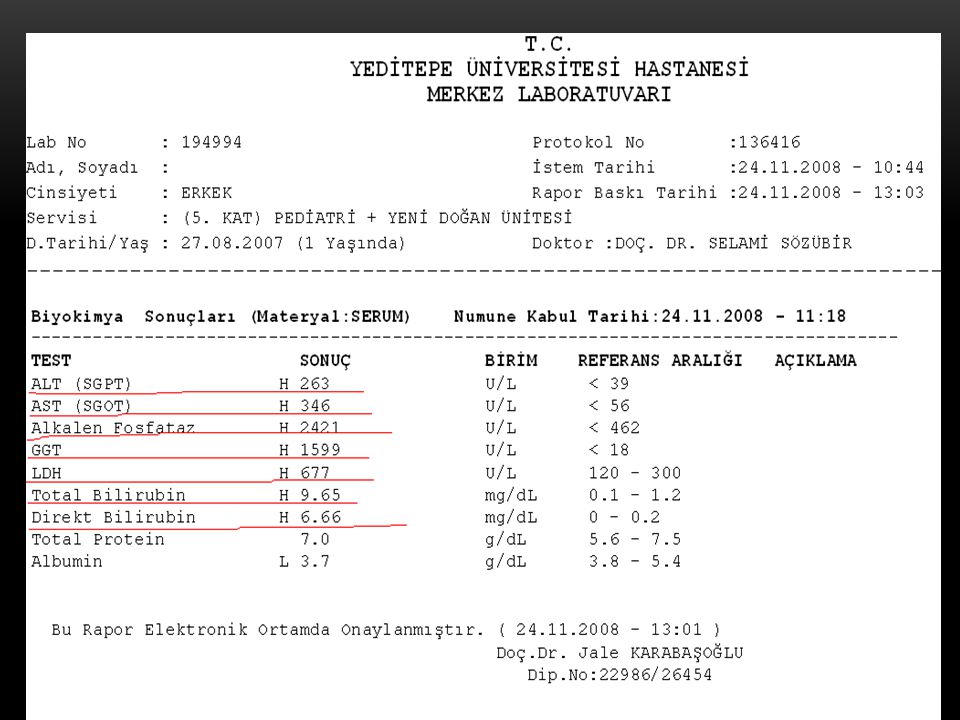
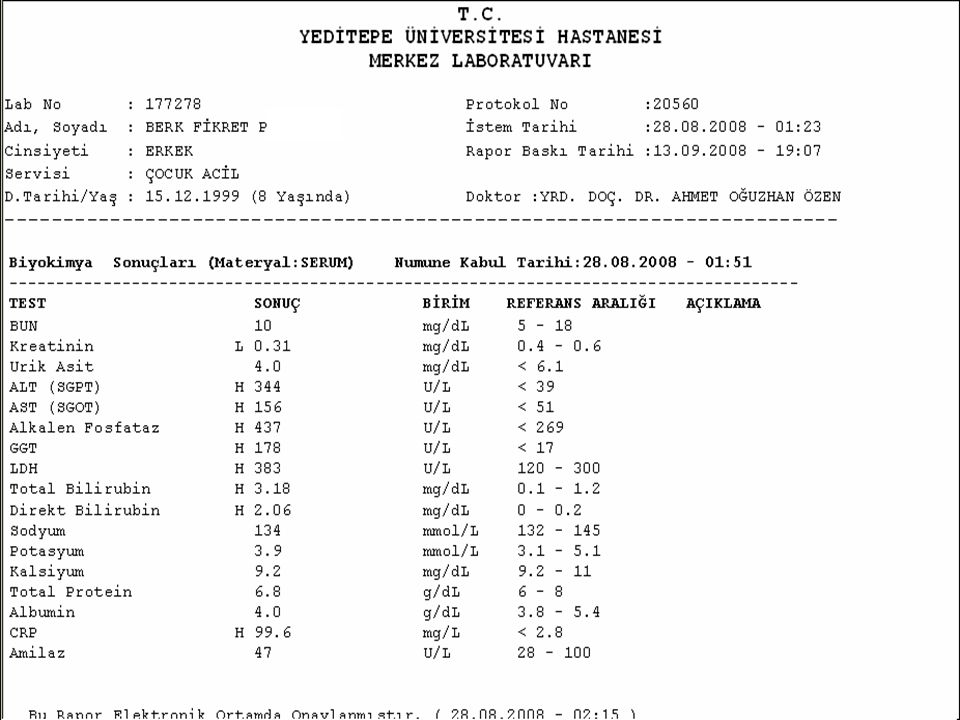
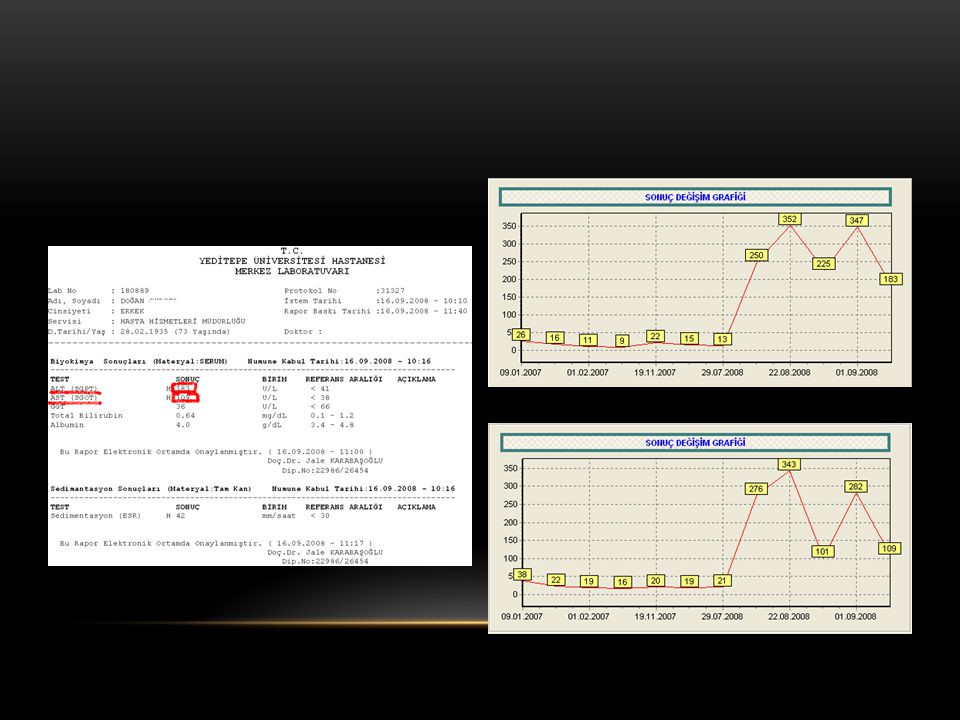

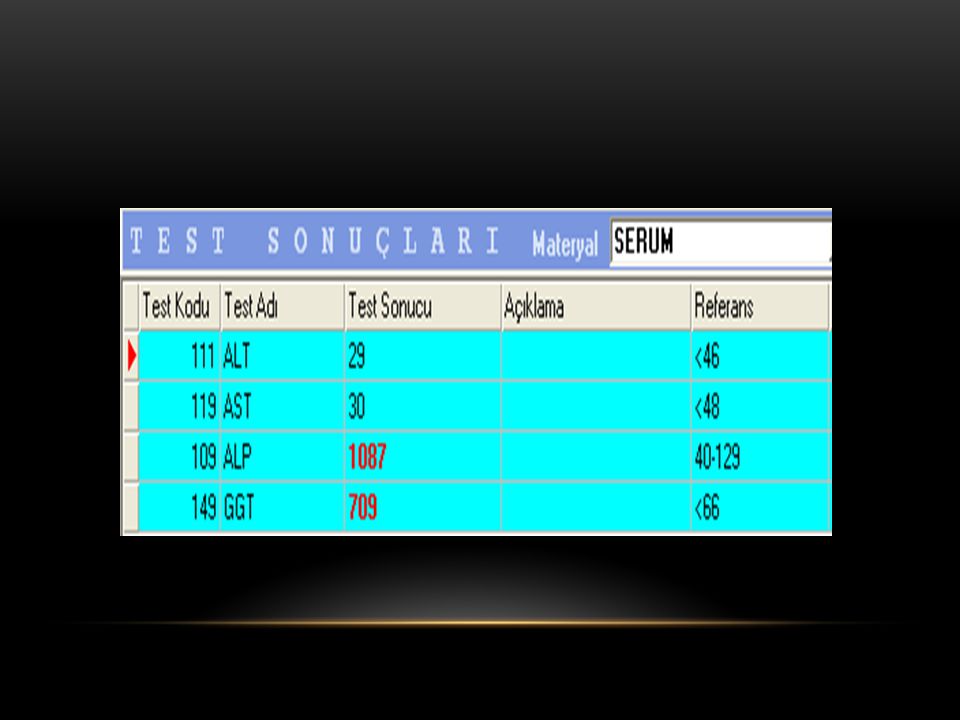
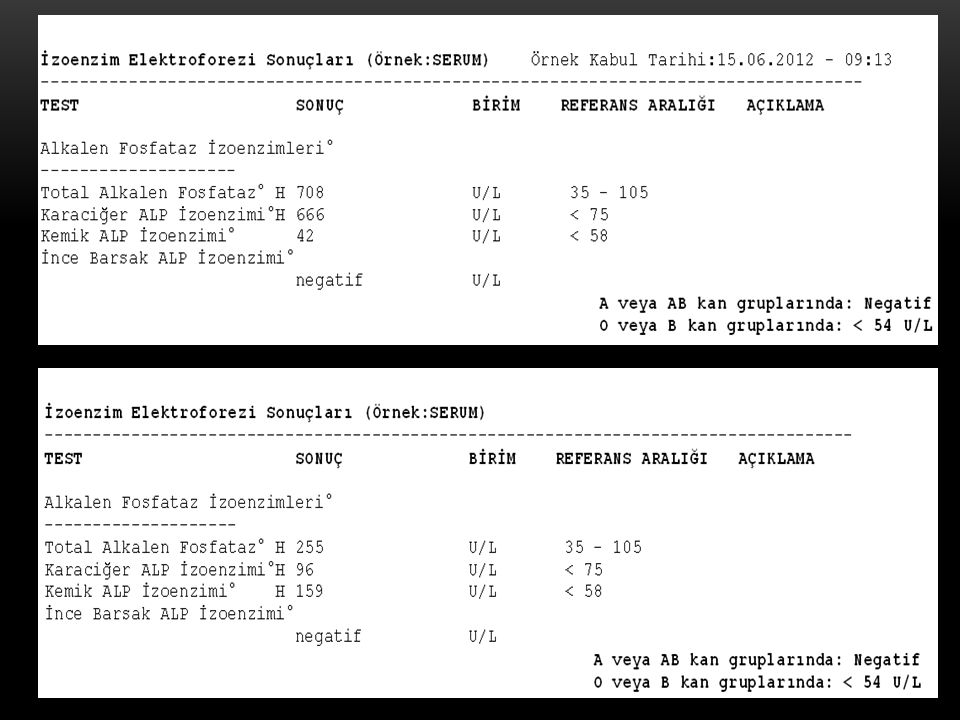
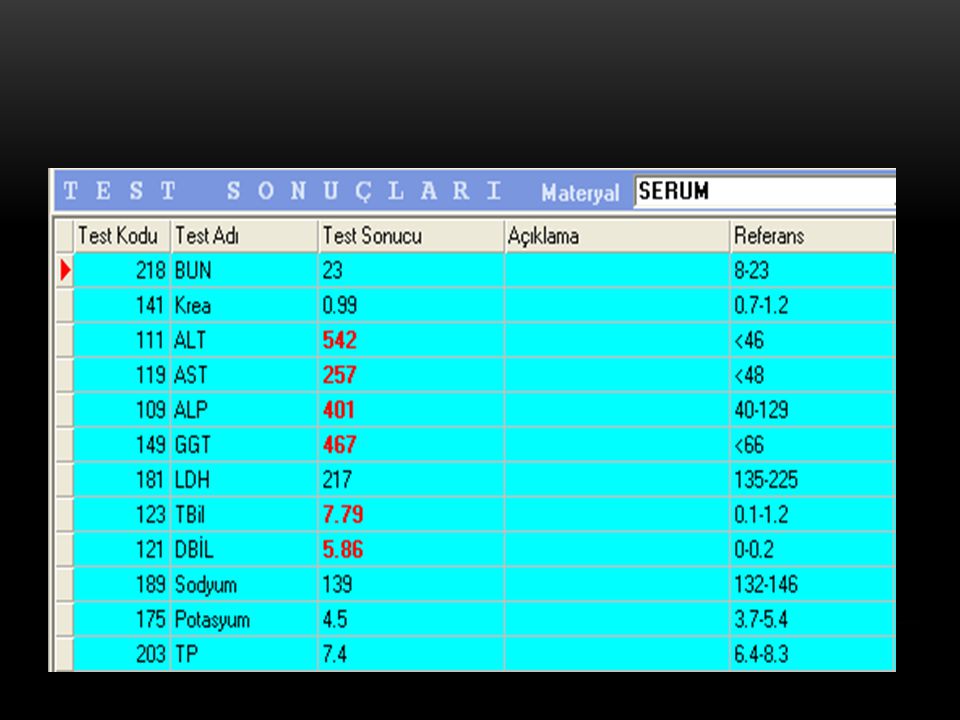






 problemleri (Matching and Assignment problems)>")


 Kristalize olanlar (Hb C)>")










 (Yrd. Doç. Dr. Deniz Dal)>")
