Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Uterus septum Dr. Engin Oral İ.Ü. Cerrahpaşa Tıp Fakültesi
Kadın Hastalıkları ve Doğum Anabilim Dalı Reprodüktif Endokrinoloji Bilim Dalı

4
Grimbizis GF, 2001

5
Grimbizis GF, 2001

6
İnfertilite-Septum sıklık
Retrospektif 375 primer infertil kadında histeroskopi bulguları % Normal uterin kavite Anormal uterin kavite Subseptat uterus 6.9 İntrauterin Adezyon 3.2 Nawroth F, 2003 STUDY OBJECTIVE: To evaluate the importance of routine minihysteroscopy in the diagnosis of primary infertility. DESIGN: Retrospective study (Canadian Task Force classification II-2). SETTING: Endoscopic center at a university hospital. PATIENTS: Three hundred seventy-nine patients with primary infertility. INTERVENTION: Diagnostic minihysteroscopy without anesthesia or sedation. MEASUREMENTS AND MAIN RESULTS: Hysteroscopy was normal in 337 patients (89.9%). In 38 patients (10.1%) an intrauterine pathology was found: 26 intrauterine adhesions, 12 cases of uterus subseptus. The procedure could not be completed in four women. CONCLUSION: Minihysteroscopy should become a routine diagnostic procedure in women with primary infertility, even those with no suspected intrauterine pathology or other risk factors
. SETTING: Endoscopic center at a university hospital. PATIENTS: Three hundred seventy-nine patients with primary infertility. INTERVENTION: Diagnostic minihysteroscopy without anesthesia or sedation. MEASUREMENTS AND MAIN RESULTS: Hysteroscopy was normal in 337 patients (89.9%). In 38 patients (10.1%) an intrauterine pathology was found: 26 intrauterine adhesions, 12 cases of uterus subseptus. The procedure could not be completed in four women. CONCLUSION: Minihysteroscopy should become a routine diagnostic procedure in women with primary infertility, even those with no suspected intrauterine pathology or other risk factors.")
7
Septum- IVF Feghali J 2003 Hinckley MD 2004 de Silva AC 2005 Doldi N
Retrospektif Prospektif Hasta sayısı 145 1000 574 300 Anormal kavite % 45 36 10.1 40 Mullerian anom. % - 0.8 3 Polip % 10.3 (+myom) 32 2.6 26 Sineşi % 2 1.6 < 5 Endometrit % 17.2 Myom % Diğer % 15.5 1.2 2.8 7 hiperplazi
 Sineşi % < 5. Endometrit % Myom % Diğer % hiperplazi.")
8
Septum-Tekrarlayan implantasyon başarısızlığı
La Sala BG 1998 Oliveira FG 2003 Demirol A 2004 Prospektif Prospektif randomize Hasta sayısı 100 55 421 Anormal kavite % 18 46 26.7 Polip % 2 15.7 İntrauterin adezyon % 6 11 8.5 Myom % 4 - Septum Endometrit 1.2 13* Diğer 1 2.3** *Histolojik olarak kanıtlanmış endometrit **servikal adezyon

10
Grimbizis GF, 2001

11
Troiano RN. Magnetic resonance imaging of mullerian duct
anomalies of the uterus. Top Magn Reson Imaging. 2003;14:269– 279. Troiano RN., 2003

12
Endometriozis Amenore İnfertilite

14
Konjenital uterin anomaliler (Sınıflama)
Sınıf I (Hipoplazi / agenezi) Sınıf II (Unikornu uterus) Sınıf III (Uterus didelfis) Sınıf IV (Bikornu uterus) Sınıf V (Septat uterus) Sınıf VI (Arkuat uterus) Sınıf VII (DES-ile ilgili) The American Fertility Society. Classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49:944–955. ASRM, 1988
 Sınıf II (Unikornu uterus) Sınıf III (Uterus didelfis) Sınıf IV (Bikornu uterus) Sınıf V (Septat uterus) Sınıf VI (Arkuat uterus) Sınıf VII (DES-ile ilgili) The American Fertility Society. Classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal. ligation, tubal pregnancies, mullerian anomalies and intrauterine. adhesions. Fertil Steril. 1988;49:944–955. ASRM,")
15
Tanı HSG USG MRI H/S ve L/S TA, TV, Doppler SİS (Sonohisterografi)
2D-3D MRI H/S ve L/S

16
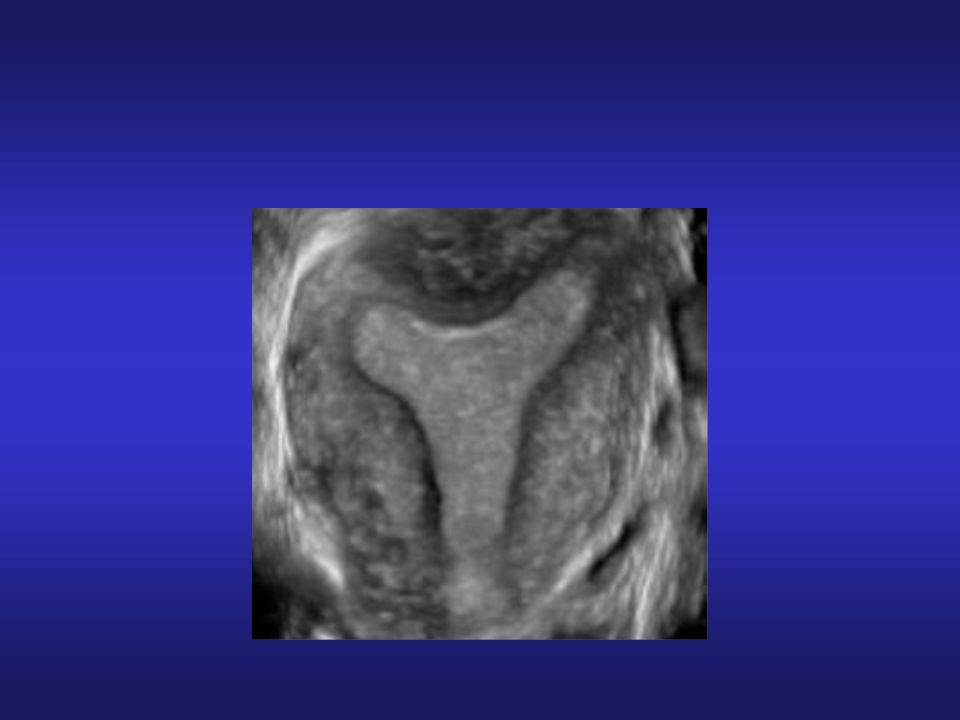
Figure 1 Transvaginal scan with color Doppler facilities demonstrates
a septate uterus. Note the two separate endometrial echoes divided by a thick septum. Figure 2 Septate uterus at sonohysterography. Note the two separate endometrial echoes divided by a thick septum. Figure 11 Three-dimensional scan of a septate uterus characterized by a normal outer uterine contour and thick septum extending into the uterine cavity.

17
Septum-sıklık Fertil ~%1 İnfertil ~%1-3.4 Mükerrer abortus ~%3.3-15.8
Homer et al. Fertil Steril 2000; 73: 1-14

18
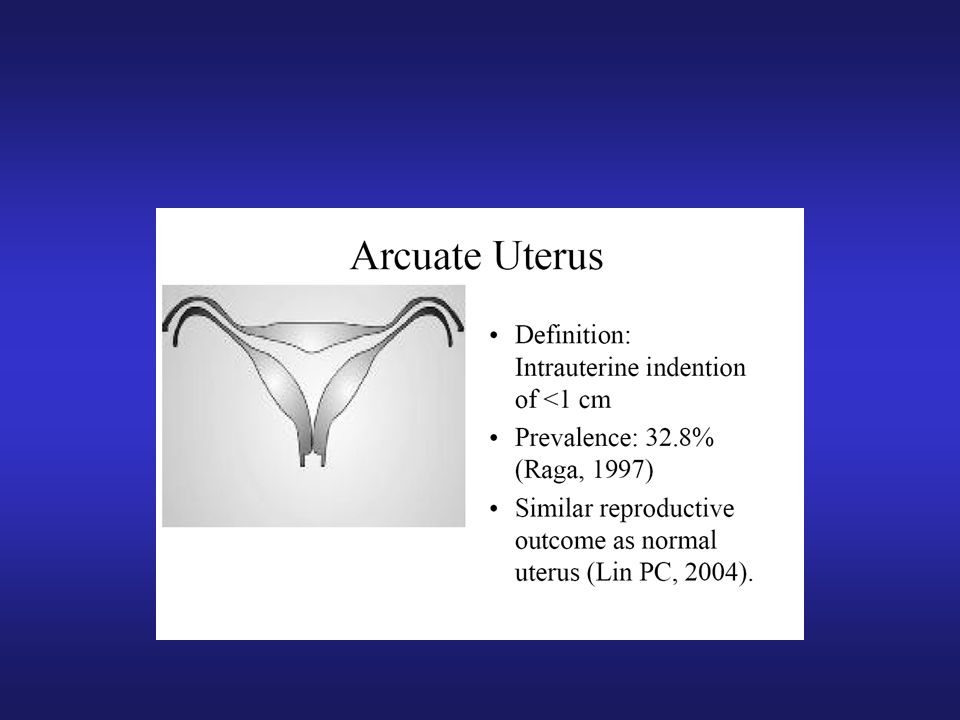
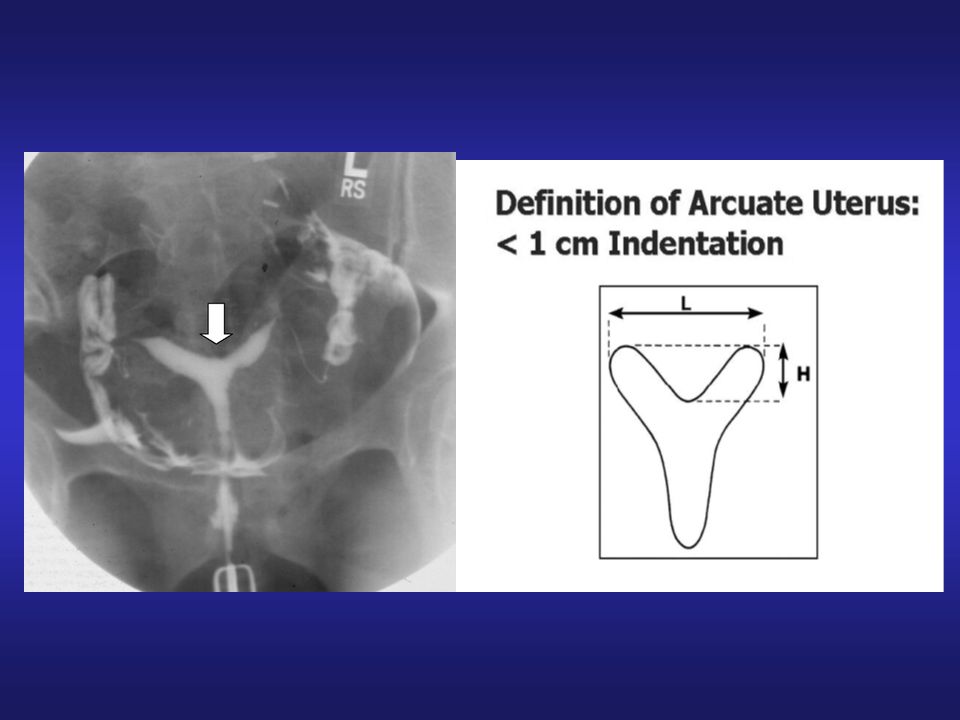
Komplet septum İnkomplet septum Arcuat uterus

19
BİKORNİS - SEPTUM

20
Uterus dış konturu genelde konveks ya da düz
Bazen fundal konkavite (< 1cm) Endometrial ekonun hipoekoik bir alan ile ikiye bölünmesi )fundus İnce, fibroz doku USG’de ekojenik endometral kaviteler fundal kesimde myometriumun ekojenitesi ile ayrılmıştır
 Endometrial ekonun hipoekoik bir alan ile ikiye bölünmesi )fundus. İnce, fibroz doku. USG’de ekojenik endometral kaviteler fundal kesimde myometriumun ekojenitesi ile ayrılmıştır.")
21
Normal Arkuat Subseptus
3D-USG ve SEPTUM Normal Arkuat Subseptus Komplet

22
Komplet Uterin Septum Parsiyal Uterin Septum

23
Müllerian Anomalilerin Tanısında Yöntemlerin Etkinliği
MRI % 100 3D TV-USG % 92 HSG % 20 Braun, 2005

24
Smooth broad fundus of septate uterus viewed through a laparoscope

26
Histeroskopi Deneyim sınıflandırılması
1.seviye Diagnostik histeroskopi Biopsi Polipektomi RİA cıkartılması 2.seviye Pedinküle myom çıkarılması Basit adezyolizis Fallop tübü kanalizasyonu 3.seviye Septum rezeksiyonu Major adezyolizis Transservikal myom rezeksiyonu Endometrial rezeksiyon RCOG

27
Septum surgery-Clinical pearls
timing of surgery use of gonadotropin-releasing hormone (GnRH) agonist or agents such as danazol before surgery scissors, resectoscopic incision, laser metroplasty, and bipolar needle electrodes. Laparoscope Septum removal or incision End point Complet servical septum fluid input and output Intravenous antibiotics balloon catheters or occasionally inert intrauterine devices (IUDs) Estrogen reevaluated with HSG or hysteroscopy Multiple methodologies exist for the actual performance of the surgery, including operative hysteroscopywith scissors, resectoscopic incision, laser metroplasty, and bipolar needle electrodes. Not one of these techniques has been demonstrated to be superior to another. There were early discussions that with the use of electrosurgery or laser, there might be lateral thermal damage, which might decrease healing or increase the likelihood of subsequent adhesion formation. Fortunately, the uterus and the endometrium in particular appear to have a high inherent ability to heal, making these concerns largely unfounded. Advantages of the use of scissors (or laser) include the ability to use isotonic solutions such as normal saline or lactated Ringer’s, which are electrolyte containing, because electrosurgery is not being used. In addition, scissors may often be introduced through a relatively small operative hysteroscope versus the larger caliber of the resectoscope. Alternatively, the 180◦ loop may be used with the resectoscope, and given the larger diameter, it may be easier to have greatermovement of fluidswithin the cavity, thus improving visualization. Once the work-up has been completed and a decision made to proceed with surgery, consideration as to the timing of surgery should occur. Generally, we prefer to perform surgery in the follicular phase as early as possible after the patient has finished menses.At this point, there is minimal endometrial tissue present to obscure visualization during hysteroscopy as well as limited vascularity. An alternative to performance of the surgery during the follicular phase that has been proposed by some is the use of gonadotropin-releasing hormone (GnRH) agonist or agents such as danazol before surgery be superior to another Although data suggest it is possible to perform metroplasty without a laparoscopy in patients in whom the diagnosis of a uterine septum is assured, many surgeons still prefer to have a laparoscope in place to guide the procedure
 agonist or agents such as danazol before surgery. scissors, resectoscopic incision, laser metroplasty, and bipolar needle electrodes. Laparoscope. Septum removal or incision. End point. Complet servical septum. fluid input and output. Intravenous antibiotics. balloon catheters or occasionally inert intrauterine devices (IUDs) Estrogen. reevaluated with HSG or hysteroscopy. Multiple methodologies exist for the actual performance of. the surgery, including operative hysteroscopywith scissors, resectoscopic. incision, laser metroplasty, and bipolar needle electrodes. Not one of these techniques has been demonstrated to. be superior to another. There were early discussions that with the. use of electrosurgery or laser, there might be lateral thermal damage, which might decrease healing or increase the likelihood of. subsequent adhesion formation. Fortunately, the uterus and the. endometrium in particular appear to have a high inherent ability. to heal, making these concerns largely unfounded. Advantages. of the use of scissors (or laser) include the ability to use isotonic. solutions such as normal saline or lactated Ringer’s, which are. electrolyte containing, because electrosurgery is not being used. In addition, scissors may often be introduced through a relatively. small operative hysteroscope versus the larger caliber of the. resectoscope. Alternatively, the 180◦ loop may be used with the. resectoscope, and given the larger diameter, it may be easier to. have greatermovement of fluidswithin the cavity, thus improving. visualization. Once the work-up has been completed and a decision made to. proceed with surgery, consideration as to the timing of surgery. should occur. Generally, we prefer to perform surgery in the follicular. phase as early as possible after the patient has finished. menses.At this point, there is minimal endometrial tissue present. to obscure visualization during hysteroscopy as well as limited. vascularity. An alternative to performance of the surgery during the. follicular phase that has been proposed by some is the use of. gonadotropin-releasing hormone (GnRH) agonist or agents such. as danazol before surgery. be superior to another. Although data suggest it is possible to perform metroplasty. without a laparoscopy in patients in whom the diagnosis of a. uterine septum is assured, many surgeons still prefer to have a. laparoscope in place to guide the procedure.")
28
Preoperative preparation of the endometrium
Progestins Danazol GnRH analogs OC Wide septa Complete septa

29
Teknik Mekanik (makas)
Elektrocerrahi: Resektoskop (Monopolar), Versapoint (bipolar) Fiberoptik laser:Argon-krypton(KTP532), Nd:YAG, Argon Histeroskopik septum rezeksiyonu ilk kez Ed strom tarafından 1974 uygulanmıştır. Various techniques and instruments are used either to incise or remove the septum, including semirigid or rigid scissors (7 French) or unipolar wire loop (8 mm) urologic resectoscope (21 to 26 French sheath); Versapoint® bipolar electrode (1.6 mm; 5 mm sheath); or Potassium-titan-phosphate (KTP/532), neodynamic:yttrium aluminum garnet (Nd:YAG), or argon lasers Hangi Teknik:Makas,Elektocerrahi, Laser? Septum insizyonunda yapılış şeklinden bağımsız iki teknik vardır. : 1. “shortening” teknik (ince septalarda), 2. “thinning” teknik (geniş septalarda), Makas :Teorik olarak yapışıklık az olur. Rezektoskop:İğne,point,loop elektrod kullanılr.İşlemi hızlandırır ,basitleştirir,hemostaz sağlar
, Versapoint (bipolar) Fiberoptik laser:Argon-krypton(KTP532), Nd:YAG, Argon. Histeroskopik septum rezeksiyonu ilk kez Ed. strom tarafından 1974 uygulanmıştır. Various techniques and instruments are used either to incise or remove the septum, including semirigid or rigid scissors (7 French) or unipolar wire loop (8 mm) urologic resectoscope (21 to 26 French sheath); Versapoint® bipolar electrode (1.6 mm; 5 mm sheath); or Potassium-titan-phosphate (KTP/532), neodynamic:yttrium aluminum garnet (Nd:YAG), or argon lasers. Hangi Teknik:Makas,Elektocerrahi, Laser Septum insizyonunda yapılış şeklinden bağımsız iki teknik vardır. : 1. shortening teknik (ince septalarda), 2. thinning teknik (geniş septalarda), Makas :Teorik olarak yapışıklık az olur. Rezektoskop:İğne,point,loop elektrod kullanılr.İşlemi hızlandırır ,basitleştirir,hemostaz sağlar.")
30
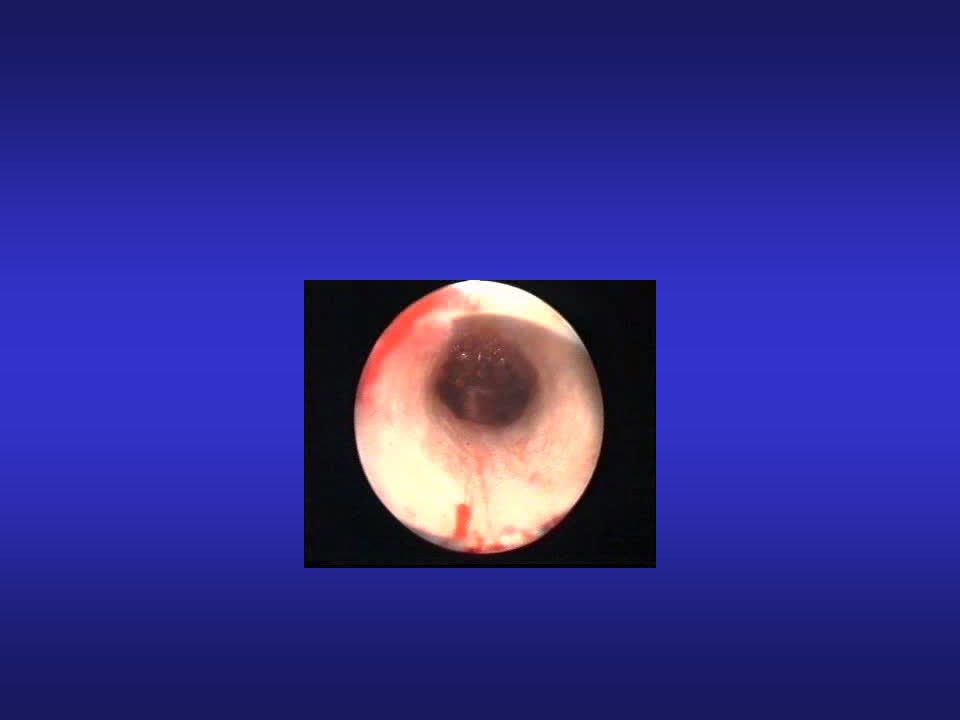
Nerede durmalı ? Histeroskop kavitede serbestçe gezdirilebilince ve her iki tubal ostium aynı anda görünür hale gelince işleme son verilir. Laparoskopi de yapılıyorsa fundusta ışığın görülmesi yeterli rezeksiyonu ifade eder. Myometrium kanamaya başlayınca işleme son verilir. Kalan septum 1 cm den küçükse fertiliteyi etkilemez. Fundusun aşırı inceltilmesi gebelikte rüptür olasılığını arttırır.

31
Teknik: No simultaneous hemostasis. Saline used, rigid, flexible ve semirigid. Semirigid: targetted division of tissue, selectively directed to the arear to be dissected can be retrieved back for a better panaromic view.

34
Septum-Lazer Nd–YAG laser

35
Versapoint (Gynecare-Ethicon)
Teknik: Resectoscope: ufak lezyonlarda bile büyük çaplı bir enstrüman. Bu nedenle CX dilatasyonu gerekiyor. Bunun için genel anestezi. 5 mm sheath, eskiden diagnostik scopelar için olan sheath kadar. Ama bu yeni 5 mm sheathde working channel ve continous flow da var. Diğer avantaj bipolar enerji (unipolar değil) Saline kullanıldığı için hiponatremi, hiponatremik ensefalopati, hiperkapni, geçici kan oxygen desatürasyonu, koagülopati ve postop hiperammonemia deriving from oxidative deamination of the aminoacid glycine gibi komp. Oranı azalıyor, riski ortadan kalkıyor. Bunlar hipotonik solüsyonların indüklediği komplikasyonlar. Laser can be used with saline through 5 Fr op. Port but expensive. Servikal dilatsyona gerek olmadığı için genel anesteziye gerek yok. Pain during H/S occurs with CX os dilatation and uterine cavity distension. Ayrıca yalnızca aktif elektrodla kontakt halindeki doku desike veya vaporize oluyor yani lateral termal yaralanma minimal. Twizzle elektrod can be bent by derece to obtain a kind of hook elektrod. The sensitive innervation in the uterus starts from the myometrium out, while the endometrium and any fibrotic tissue are not sensitive . Paraservikal anestezi with 10 ml of 1% mepivacaine HCl solution injected with a 22 G spinal needle on four sites (3, 5, 7, 9 o clock positions at the junction of the Cx and vagina. Sedasyon: IV 0.5 mg atropine ve 0.25 mg fentanyl followed by an IV slow injection of 2.0 mg of midazolam. Minimal cx dilatation, normal saline distention 5 Fr bipolar elektrod 5 mm sheath – continuos flow ve 5 Fr working channel Saline solüsyonu 2.9 mm scope 50 W cutting mode Lokal anestezi - sedasyon Versapoint (Gynecare-Ethicon)
 Saline kullanıldığı için hiponatremi, hiponatremik ensefalopati, hiperkapni, geçici kan oxygen desatürasyonu, koagülopati ve postop hiperammonemia deriving from oxidative deamination of the aminoacid glycine gibi komp. Oranı azalıyor, riski ortadan kalkıyor. Bunlar hipotonik solüsyonların indüklediği komplikasyonlar. Laser can be used with saline through 5 Fr op. Port but expensive. Servikal dilatsyona gerek olmadığı için genel anesteziye gerek yok. Pain during H/S occurs with CX os dilatation and uterine cavity distension. Ayrıca yalnızca aktif elektrodla kontakt halindeki doku desike veya vaporize oluyor yani lateral termal yaralanma minimal. Twizzle elektrod can be bent by derece to obtain a kind of hook elektrod. The sensitive innervation in the uterus starts from the myometrium out, while the endometrium and any fibrotic tissue are not sensitive . Paraservikal anestezi with 10 ml of 1% mepivacaine HCl solution injected with a 22 G spinal needle on four sites (3, 5, 7, 9 o clock positions at the junction of the Cx and vagina. Sedasyon: IV 0.5 mg atropine ve 0.25 mg fentanyl followed by an IV slow injection of 2.0 mg of midazolam. Minimal cx dilatation, normal saline distention. 5 Fr bipolar elektrod. 5 mm sheath – continuos flow ve 5 Fr working channel. Saline solüsyonu. 2.9 mm scope. 50 W cutting mode. Lokal anestezi - sedasyon. Versapoint (Gynecare-Ethicon)")
36
Resectoscope or Versapoint for hysteroscopic metroplasty
Objective: To assess the feasibility, safety, and reproductive outcome of hysteroscopic metroplasty using the Versapoint device compared with the resectoscope using the Collins loop. Methods: Sixty-three women diagnosed with partial septate uterus were included in the study. Forty-two women underwent hysteroscopic metroplasty using Versapoint and 21 women had the procedure using the resectoscope. Operating time, complications, pregnancy rate, and mode of delivery were recorded. Data were analyzed with the Mann–Whitney test. Results: Operating time was 20.5 min for the resectoscope group and 15.4 min for the Versapoint group (Pb0.05). Pregnancy rate, delivery rate, and spontaneous abortions were similar in both groups. Conclusion: Operative hysteroscopy with Versapoint does not require cervical dilation, thus avoiding cervical incompetence, cervical lacerations, and uterine perforation. The Versapoint technique is a safe and effective alternative to the resectoscope. It could be used predominantly in nulligravida women, especially in those with cervical canal stenosis. It could be used predominantly in nulligravida women, especially in those with cervical canal stenosis Pietro Litta, 2008
. Pregnancy rate, delivery rate, and spontaneous abortions were similar in both groups. Conclusion: Operative hysteroscopy with Versapoint does not require cervical dilation, thus. avoiding cervical incompetence, cervical lacerations, and uterine perforation. The Versapoint. technique is a safe and effective alternative to the resectoscope. It could be used predominantly. in nulligravida women, especially in those with cervical canal stenosis. It could be used predominantly. in nulligravida women, especially in those with cervical canal stenosis. Pietro Litta,")
37
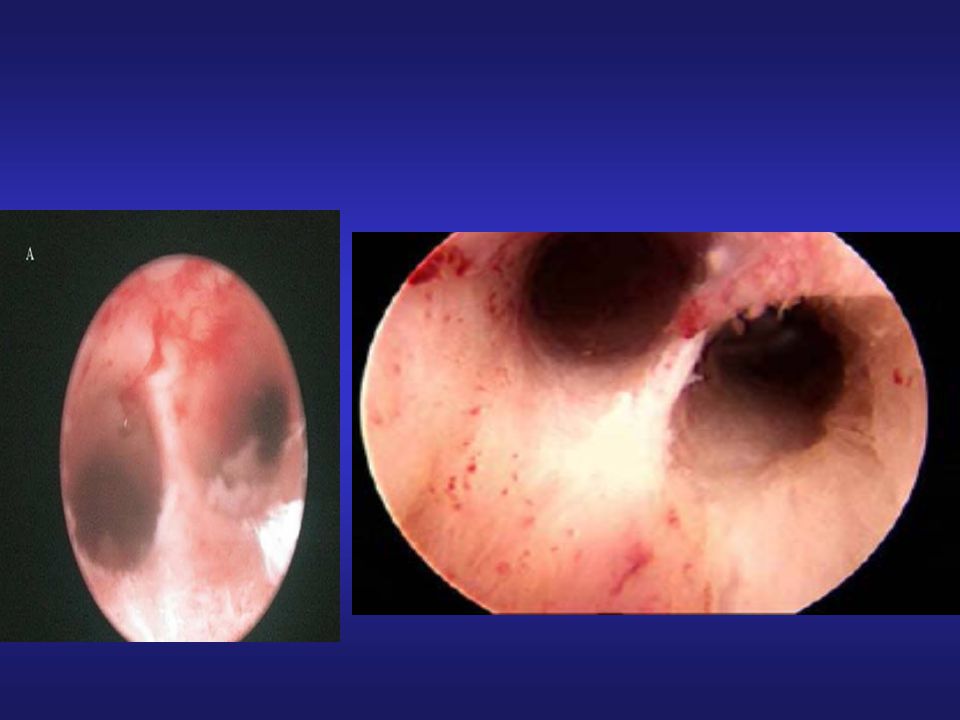
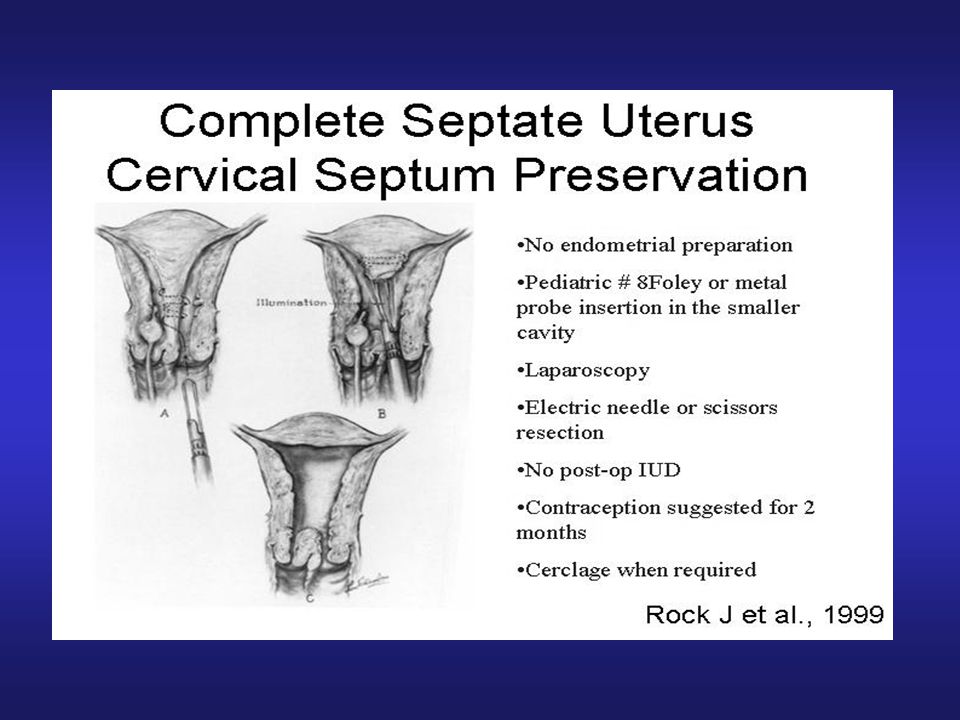
Complete Septate Uterus: Should the Cervical Septum Be Removed?
Among a total of 517 reported cases of septate uterus, 74 (14%) were found to be a complete septate uterus. The incidence of cervical incompetence after removal of the complete septum is rare. Possibly impeding vaginal delivery in a subsequent pregnancy.
 were found to be a complete septate uterus. The incidence of cervical incompetence after removal of the complete septum is rare. Possibly impeding vaginal delivery in a subsequent pregnancy.")
40
Hysteroscopic metroplasty of the complete uterine septum, duplicate cervix, and vaginal septum
Objective: To determine if sectioning of the cervical septum in hysteroscopic metroplasty of the complete uterine septum is associated with intraoperative bleeding, cervical incompetence, and secondary infertility. Design: Multicenter, randomized, controlled clinical trial. Setting: University hospitals. Patient(s): Twenty-eight women with a diagnosis of complete uterine septum who had a history of pregnancy wastage or infertility. They were randomized into two groups: group A underwent metroplasty including section of the cervical septum; group B underwent the same procedure with preservation of the cervical septum. Intervention(s): Hysteroscopic metroplasty was performed for all patients in the two groups. Main Outcome Measure(s): Operating time, distending media deficit, total distending media used, intraoperative bleeding, complications, and reproductive outcome. Result(s): Operating times were minutes and minutes in group A and group B, respectively. Distending media deficit was mL in group A, while in group B it was Two cases of pulmonary edema and three cases of significant bleeding (150 mL) were seen in group B. The cesarean section rate was significantly higher in group B. There were no significant differences in the reproductive outcome in the two groups. Conclusion(s): Resection of the cervical septum during hysteroscopic metroplasty of complete uterine septum makes the procedure safer, easier, and less complicated than the procedure with preservation of the cervical septum. This procedure is recommended for all cases of complete uterine septum Mohammad Ebrahim Parsanezhad, 2006
: Twenty-eight women with a diagnosis of complete uterine septum who had a history of pregnancy. wastage or infertility. They were randomized into two groups: group A underwent metroplasty including section. of the cervical septum; group B underwent the same procedure with preservation of the cervical septum. Intervention(s): Hysteroscopic metroplasty was performed for all patients in the two groups. Main Outcome Measure(s): Operating time, distending media deficit, total distending media used, intraoperative. bleeding, complications, and reproductive outcome. Result(s): Operating times were minutes and minutes in group A and group B, respectively. Distending media deficit was mL in group A, while in group B it was Two cases of pulmonary edema and three cases of significant bleeding (150 mL) were seen in group. B. The cesarean section rate was significantly higher in group B. There were no significant differences in the. reproductive outcome in the two groups. Conclusion(s): Resection of the cervical septum during hysteroscopic metroplasty of complete uterine septum. makes the procedure safer, easier, and less complicated than the procedure with preservation of the cervical. septum. This procedure is recommended for all cases of complete uterine septum. Mohammad Ebrahim Parsanezhad,")
41
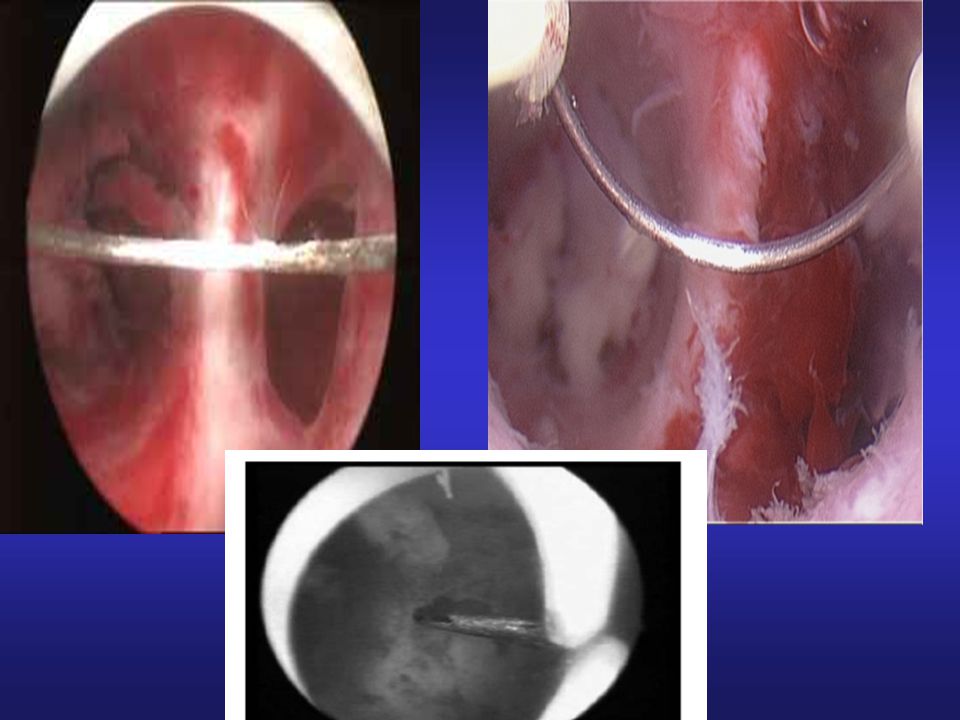
A. )The cervical septum is incised with the scissors
A.)The cervical septum is incised with the scissors. (B) The external cervical os is completely normal. (C) Dilatation of thecervical canal before the uterine septum resection.
The cervical septum is incised with the scissors. (B) The external cervical os is completely normal. (C) Dilatation of thecervical canal before the uterine septum resection.")
42
What is the role of laparoscopy ?
To differentiate accurately between a septate and a bicornuate uterus. To monitor hysteroscopic surgery (Perforation). To complete the diagnostic workup in patients with infertility. To aspirate any distention fluid that has leaked into the abdomen during the hysteroscopic procedure.
. To complete the diagnostic workup in patients with infertility. To aspirate any distention fluid that has leaked into the abdomen during the hysteroscopic procedure.")
43
Postoperative Management
There is no role for the routine postoperative use of an IUD. The beneficial role of routine antibiotic therapy has not been firmly established. The administration of estrogen after hysteroscopic metroplasty probably is unnecessary.

44
Postoperative management
Once the postoperative examination (by HSG, hysteroscopy, or US) reveals normal findings, there is no reason to delay attempts at pregnancy for >2 cycles. Reproductive performance was not adversely affected by a residual septum of up to 1 cm.
 reveals normal findings, there is no reason to delay attempts at pregnancy for >2 cycles. Reproductive performance was not adversely affected by a residual septum of up to 1 cm.")
45
Hayden A. Homer, 2000

47
Hayden A. Homer, 2000

48
Hayden A. Homer, 2000

50
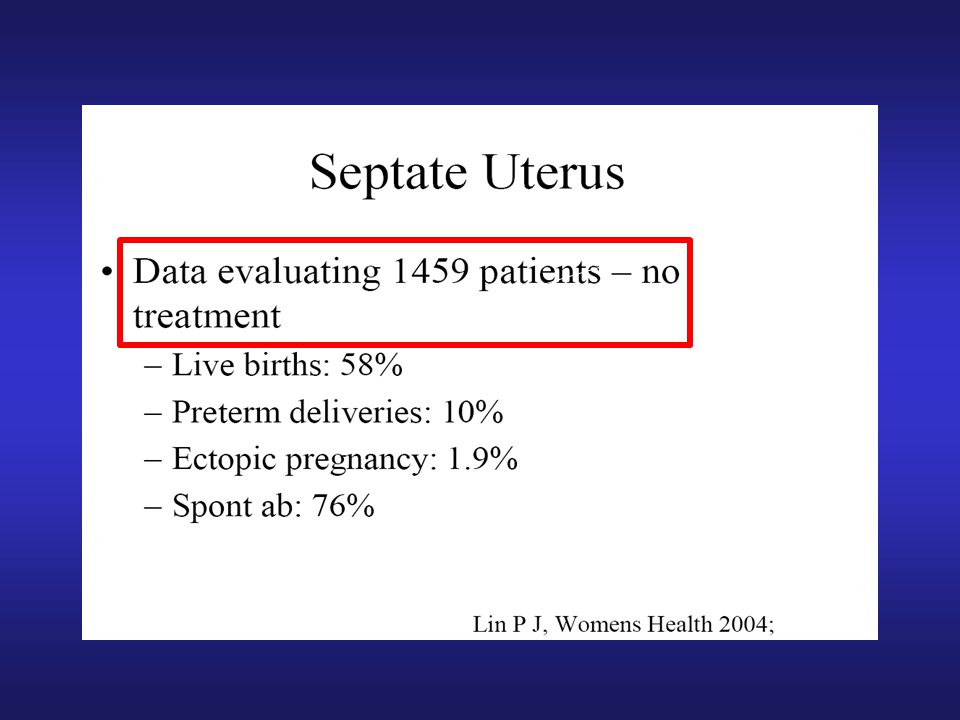
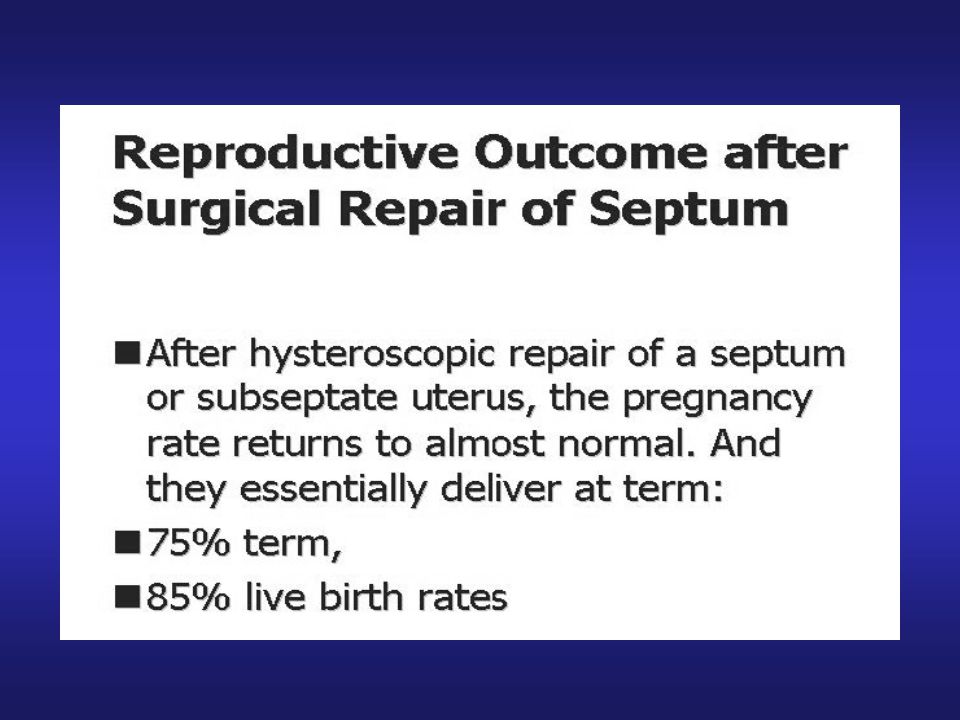
Septum prognoz (bekleme vs. Tedavi)
% Düşük Erken doğum Dış gebelik Term doğum Canlı doğum % Düşük Erken doğum 6.8 Dış gebelik Term doğum Canlı doğum Heinonen 1982, Buttram 1983, Acien 1993, Raga 1997 DeCherney 1986, Fayez 1986, Valla ve Sciarria 1986, March ve Israel 1987, Perino 1987, Daly 1989, Choe ve Baggish 1992, Fedele 1993, Grimbizis 1998

51
Hysteroscopic septum resection in patients with unexplained infertility
Group I consisted of 69 women (mean±SD age 30±4) with unexplained infertility of at least two years duration. Criteria for inclusion were 1. no endocrine disorders with at least six months of regular biphasic basal body temperature records, 2. progesterone levels above 2 ng/ml in the mid-luteal phase, 3. patency of the Fallopian tubes demonstrated by laparoscopy, 4. partners with normal semen analyses. S. Venturoli, 2002
 with unexplained. infertility of at least two years duration. Criteria for inclusion. were. 1. no endocrine disorders with at least six months of regular biphasic. basal body temperature records, 2. progesterone levels above 2 ng/ml in the mid-luteal phase, 3. patency of the Fallopian tubes demonstrated by laparoscopy, 4. partners with normal semen analyses. S. Venturoli,")
52
Reproductive outcome after hysteroscopic metroplasty in
% 11.5 Objective: To evaluate the reproductive outcome of hysteroscopic metroplasty performed in women with septate uterus and otherwise unexplained primary infertility. Design: Prospective, observational study. Setting: Tertiary center for reproductive medicine. Patient(s): Sixty-one patients with uterine septa and otherwise unexplained primary infertility. Intervention(s): Hysteroscopic division of the uterine septum. Main Outcome Measure(s): Reproductive outcome after hysteroscopic metroplasty. Result(s): Of 61 women, 25 (41%) conceived within 8–14 (mean 11.2) months after hysteroscopic metroplasty. Of these, 18 (29.5% of the total group) had live births (13 carried to term and 5 had preterm deliveries), and 7 (11.5% of the total group) had spontaneous abortions. Cervical cerclage was performed in 9 women; only 1 (11.1%) of these patients and 4 (44.4%) of the 9 who did not have a cerclage had preterm deliveries. Twelve of the 18 women (66.6%) who had live births were delivered by cesarean section. Conclusion(s): Women with uterine septum and otherwise unexplained infertility might benefit from hysteroscopic metroplasty. Recai Pabuccu and Victor Gomel, 2004
: Sixty-one patients with uterine septa and otherwise unexplained primary infertility. Intervention(s): Hysteroscopic division of the uterine septum. Main Outcome Measure(s): Reproductive outcome after hysteroscopic metroplasty. Result(s): Of 61 women, 25 (41%) conceived within 8–14 (mean 11.2) months after hysteroscopic metroplasty. Of these, 18 (29.5% of the total group) had live births (13 carried to term and 5 had preterm deliveries), and 7 (11.5% of the total group) had spontaneous abortions. Cervical cerclage was performed in 9 women; only 1 (11.1%) of these patients and 4 (44.4%) of the 9 who did not have a cerclage had preterm deliveries. Twelve of the 18 women (66.6%) who had live births were delivered by cesarean section. Conclusion(s): Women with uterine septum and otherwise unexplained infertility might benefit from hysteroscopic. metroplasty. Recai Pabuccu and Victor Gomel,")
53
RANDOMİZE ÇALIŞMALAR: Septum-İnfertilite (Tedavi vs. Bekleme)
1 2 3 4 5 6

54
Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: a prospective controlled trial Surgery Objective: To assess fecundity of infertile women after surgical correction of uterine septum. Design: Prospective controlled trial. Setting: Three academic infertility clinics. Patient(s): Forty-four women affected by septate uterus and otherwise unexplained infertility represented the study group (group A), and 132 women with unexplained infertility were enrolled as control subjects (group B). Intervention(s): Hysteroscopic metroplasty was performed in group A, and group B was managed expectantly. All women were followed-up for 1 year without any other intervention. Main Outcome Measure(s): Fecundity rate was calculated as the number of pregnancies per 100 person-months Result(s): Pregnancy rate (38.6% vs. 20.4%) and live birth rate (34.1% and 18.9%) were significantly higher in group A than in group B. The survival analysis showed that the probability of a pregnancy in the twelve-months follow up was significantly higher in patients who had undergone metroplasty than in women with unexplained infertility. The corresponding fecundity (10-week pregnancy) rates were 4.27 and 1.92 person-months in women who had undergone metroplasty and in women with unexplained infertility, respectively. Conclusion(s): Hysteroscopic resection of the septum improves fecundity of women with septate uterus and otherwise unexplained infertility. Patients with septate uterus and no other cause of sterility have a significantly higher probability of conceiving after removal of the septum than patients affected by idiopathic sterility Antonio Mollo, 2008
: Forty-four women affected by septate uterus and otherwise unexplained infertility represented the. study group (group A), and 132 women with unexplained infertility were enrolled as control subjects (group B). Intervention(s): Hysteroscopic metroplasty was performed in group A, and group B was managed expectantly. All. women were followed-up for 1 year without any other intervention. Main Outcome Measure(s): Fecundity rate was calculated as the number of pregnancies per 100 person-months. Result(s): Pregnancy rate (38.6% vs. 20.4%) and live birth rate (34.1% and 18.9%) were significantly higher in. group A than in group B. The survival analysis showed that the probability of a pregnancy in the twelve-months. follow up was significantly higher in patients who had undergone metroplasty than in women with unexplained. infertility. The corresponding fecundity (10-week pregnancy) rates were 4.27 and 1.92 person-months in women. who had undergone metroplasty and in women with unexplained infertility, respectively. Conclusion(s): Hysteroscopic resection of the septum improves fecundity of women with septate uterus and otherwise. unexplained infertility. Patients with septate uterus and no other cause of sterility have a significantly higher. probability of conceiving after removal of the septum than patients affected by idiopathic sterility. Antonio Mollo,")
55
26 Residu sonra cerrahi 58 no residu 7 rezidu
BACKGROUND: To learn more about the obstetric outcome after initial septum resection and remnant septum (< or =1 cm) resection. METHODS: In 94 patients with septate uteri who underwent uterine septum resection, the reproductive efficiency was analysed in a prospective observational study. The reproductive outcome was analysed after initial resection and (if required) consecutive procedures. RESULTS: A total of 94 women were enrolled in the study; all had had two or more miscarriages. The septum was completely removed during the first hysteroscopy in 58 (62%) cases. A residual septum was observed in 36 (38%) patients. Subsequent operative hysteroscopy was performed in the cases (29/36; 80.5%) involving repeated miscarriage and unsuccessful conception. The minimum observation time was 24 months. The difference in delivery rate after the first hysteroscopy between those with a normalized uterine cavity (26/58; 44.8%) and those with remnants (7/36; 19.4%) was statistically significant (P < 0.05). In fact, following the normalization of the uterine cavity, 62.1% (18/29) of the patients delivered, as compared with 19.4% of those (7/36) with a residue and Kaplan-Meyer curves revealed a statistically significant difference (P < 0.05). CONCLUSIONS: Women with a remnant uterine septum have an increased chance of successful pregnancy with an improved obstetric outcome after normalization of the uterine cavity. 7 rezidu
 resection. METHODS: In 94 patients with septate uteri who underwent uterine septum resection, the reproductive efficiency was analysed in a prospective observational study. The reproductive outcome was analysed after initial resection and (if required) consecutive procedures. RESULTS: A total of 94 women were enrolled in the study; all had had two or more miscarriages. The septum was completely removed during the first hysteroscopy in 58 (62%) cases. A residual septum was observed in 36 (38%) patients. Subsequent operative hysteroscopy was performed in the cases (29/36; 80.5%) involving repeated miscarriage and unsuccessful conception. The minimum observation time was 24 months. The difference in delivery rate after the first hysteroscopy between those with a normalized uterine cavity (26/58; 44.8%) and those with remnants (7/36; 19.4%) was statistically significant (P < 0.05). In fact, following the normalization of the uterine cavity, 62.1% (18/29) of the patients delivered, as compared with 19.4% of those (7/36) with a residue and Kaplan-Meyer curves revealed a statistically significant difference (P < 0.05). CONCLUSIONS: Women with a remnant uterine septum have an increased chance of successful pregnancy with an improved obstetric outcome after normalization of the uterine cavity. 7 rezidu.")
58
Septum-Tedavi endikasyonları
Tekrarlayan gebelik kayıpları Düşükler 1 Düşük 2 Düşük 3 Düşük Erken doğum İnfertilite Primer Sekonder ART Öncesinde Başarısız denemeler sonrası Asemptomatik/primer dismenora Septumun kesilmesi tekrarlayan gebelik kayıpları, obstetrik komplikasyonlar ve IVF öncesi önerilir. Septumu HSG ile tespit edilen infertilite hastalarında tedavisi tartışmalıdır. İnfertilite 1. unexplained infertilitesi olanlarda yaş 3. Başka nedenle LS veya HS yapılanlarda 4.ART ye gideceklerde yapılmalıdır.

60
Kime septum rezeksiyonu yapalım
Kime septum rezeksiyonu yapalım ? Hysteroscopic removal of the septum may be considered in the following populations: Uzun süre açıklanamayan infertilite 35 yaş üstü Başka nedenlerle L/S ve H/S yapılacaklarda ART düşünülen olgularda Minimal uterine septumlar(1,5 cm’ den küçük) ve arkuat uterusun düzeltilmesi gerekmez. Luca Mencaglia et all.1997,Susa Davie et all 1997 Klinik olarak gerekmedikçe H/S ile uterin anomalileri düzeltmek fertiliteyi düzeltici etkisi olmadığı için önerilmez.(B) Hayden A. Homer, 2000
 ve arkuat uterusun düzeltilmesi gerekmez. Luca Mencaglia et all.1997,Susa Davie et all Klinik olarak gerekmedikçe H/S ile uterin anomalileri düzeltmek fertiliteyi düzeltici etkisi olmadığı için önerilmez.(B) Hayden A. Homer,")
61
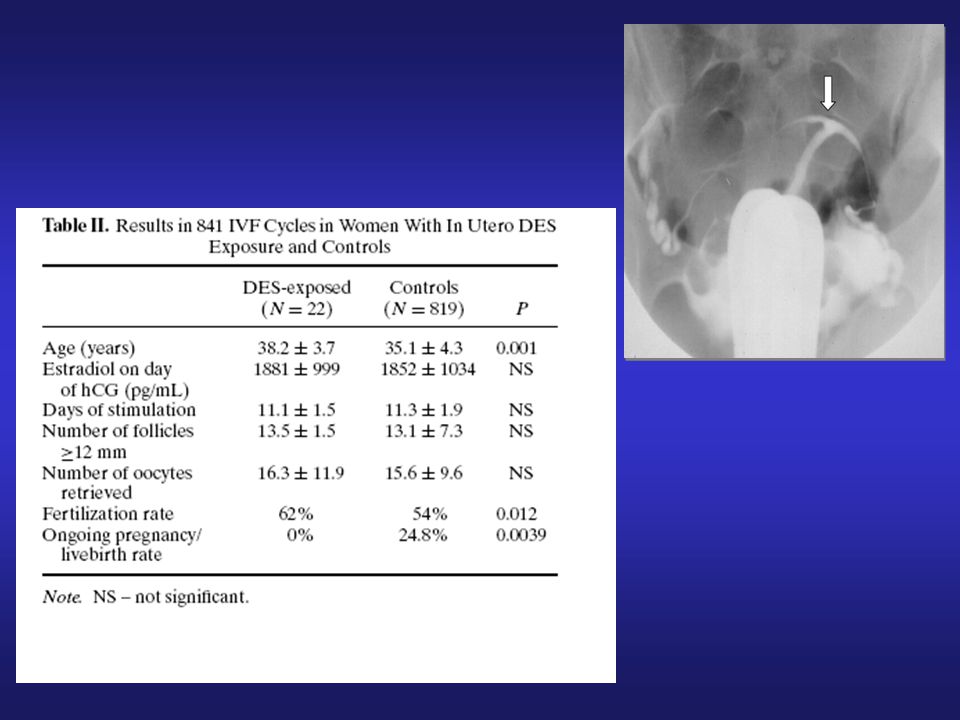
Finally, IVF is less successful in women with a septate uterus compared with women who have undergone metroplasty. For this reason, hysteroscopic metroplasty should be considered in women before undergoing IVF, an emotionally and financially expensive procedure However, women with a septate uterus and otherwise unexplained infertility may benefit from metroplasty, although the improvement in pregnancy rate is relatively modest in comparison with those who experienced recurrent pregnancy loss Elizabeth Taylor and Victor Gomel, 2008

63
Uterine rupture at the 29th week of subsequent pregnancy after hysteroscopic resection of uterine septum Objective: To describe a patient with uterine rupture in the subsequent pregnancy after hysteroscopic resection of a uterine septum. Design: Case report. Setting: University hospital. Patient(s): A 30-year-old nulliparous woman, with a history of a first trimester spontaneous abortion, hysteroscopic uterine septum resection by cutting diathermy using the operating hysteroscope, and a second hysteroscopic procedure for a residual septum, was admitted to our clinic with symptoms of hemodynamic shock at the 29th week of gestation. Intervention(s): Immediate laparotomy was performed. Main Outcome Measure(s): Uterine rupture in the second trimester of the subsequent pregnancy with fetal loss. Result(s): Midfundal complete uterine rupture was observed at the site of the resected uterine septum, accompanied by an extrauterine exanimate fetus. Conclusion(s): Uterine rupture may occur in pregnancies after hysteroscopic resection of the uterine septum. Clinicians who perform this procedure, especially in the cases with repeated procedures using cutting diathermy, must warn and inform their patients about the risks of their later pregnancies Şatıroğlu MH, 2009
: A 30-year-old nulliparous woman, with a history of a first trimester spontaneous abortion, hysteroscopic. uterine septum resection by cutting diathermy using the operating hysteroscope, and a second hysteroscopic. procedure for a residual septum, was admitted to our clinic with symptoms of hemodynamic shock at the 29th week. of gestation. Intervention(s): Immediate laparotomy was performed. Main Outcome Measure(s): Uterine rupture in the second trimester of the subsequent pregnancy with fetal loss. Result(s): Midfundal complete uterine rupture was observed at the site of the resected uterine septum, accompanied. by an extrauterine exanimate fetus. Conclusion(s): Uterine rupture may occur in pregnancies after hysteroscopic resection of the uterine septum. Clinicians who perform this procedure, especially in the cases with repeated procedures using cutting diathermy, must warn and inform their patients about the risks of their later pregnancies. Şatıroğlu MH,")
64
Risk of Uterine Perforation during Hysteroscopic Surgery
Procedure(no) Mean Age(yrs) No. (%) ofPerforations Synechiolysis (199) 35 ± 2.8 15 (7.54) Uterine septa section (90) 33 ± 3.8 1 (1.11) Myoma resection (782) 46.2 ± 4.2 9 (1.15) Polyp resection (422) 48.5 ± 6.2 4 (0.95) Endometrectomy (623) ( 45.3 ± 7.9 5 0.80) Totals (2116) 41.5 ± 6.1 34 (1.61) Aubert Agostini M , 2002)
 Mean Age(yrs) No. (%) ofPerforations. Synechiolysis (199) 35 ± (7.54) Uterine septa section (90) 33 ± (1.11) Myoma resection (782) 46.2 ± (1.15) Polyp resection (422) 48.5 ± (0.95) Endometrectomy (623) ( 45.3 ± ) Totals (2116) 41.5 ± (1.61) Aubert Agostini M , 2002)")
68
Is hysteroscopic correction of an incomplete uterine septum justified prior to IVF?
This retrospective study examined the effect of hysteroscopic correction of an incomplete uterine septum on IVF outcome. Measurement of the Fm (fundal myometrial thickness) and Cm (cornual myometrial thickness) was performed by sonohysterography. Group 1 included patients diagnosed with incomplete septum (n = 119), fulfi lling the two criteria of Fm >11 mm and Fm–Cm >5 mm, who underwent hysteroscopic incision of the incomplete septum. Group 2 consisted of 116 age-matched control patients with a normal uterine cavity who underwent IVF within the same time period. Main outcome measures were clinical pregnancy and spontaneous abortion rates. Patients in group 1 had a history of more spontaneous abortions than patients in group 2 (14.20 versus 6.03%, P = 0.04) as well as higher previous IVF failure (32.7 versus 20.6%, P = 0.04). After surgical correction of the septum in group 1, IVF pregnancy outcome was similar in both groups (clinical pregnancy and pregnancy loss of versus 46.50% and versus 20.3% respectively). A similar pregnancy outcome was found after the incision of the incomplete septum compared with a group with normal uterine cavity. Larger prospective and randomized controlled studies are needed to prove the positive effect of correction of an incomplete uterine septum on IVF outcome. Ozgur K, 2007
 and Cm (cornual myometrial thickness) was performed by. sonohysterography. Group 1 included patients diagnosed with incomplete septum (n = 119), fulfi lling the two criteria of Fm. >11 mm and Fm–Cm >5 mm, who underwent hysteroscopic incision of the incomplete septum. Group 2 consisted of 116. age-matched control patients with a normal uterine cavity who underwent IVF within the same time period. Main outcome. measures were clinical pregnancy and spontaneous abortion rates. Patients in group 1 had a history of more spontaneous. abortions than patients in group 2 (14.20 versus 6.03%, P = 0.04) as well as higher previous IVF failure (32.7 versus 20.6%, P = 0.04). After surgical correction of the septum in group 1, IVF pregnancy outcome was similar in both groups (clinical. pregnancy and pregnancy loss of versus 46.50% and versus 20.3% respectively). A similar pregnancy outcome. was found after the incision of the incomplete septum compared with a group with normal uterine cavity. Larger prospective. and randomized controlled studies are needed to prove the positive effect of correction of an incomplete uterine septum on. IVF outcome. Ozgur K,")
69
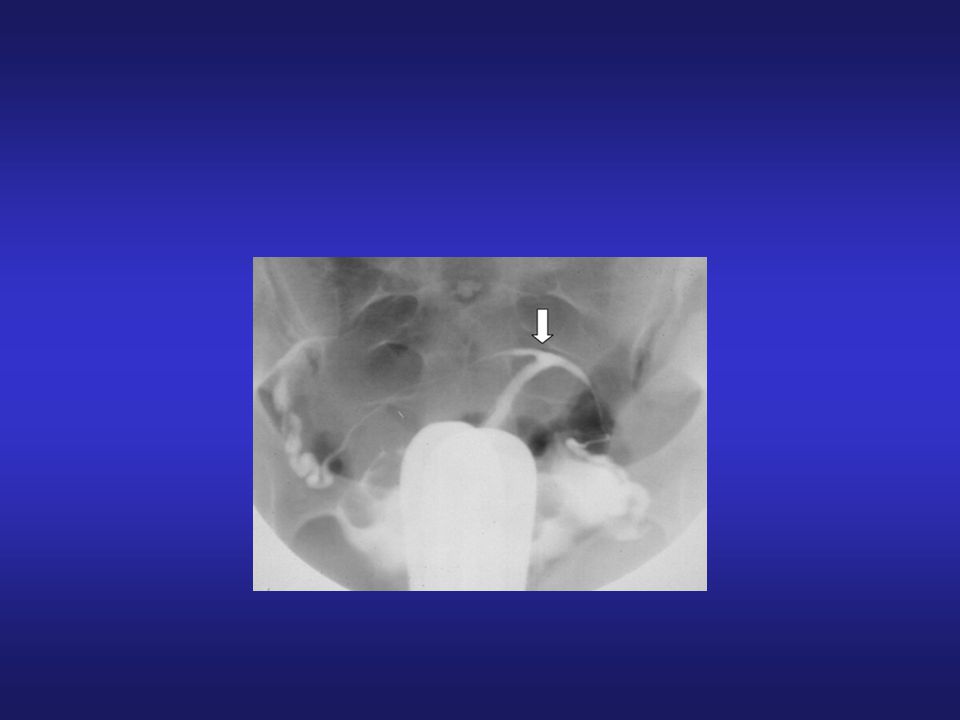
DES HSG: Perfect imaging modality
Hypoplasic uterus, constriction bands T configuration Bulbous lower ut segment

70
ıı USG: Reduction in ut volume Lack of fundal expansion TVS:
Done at secretory phase to maximize subtle cavity considerations

73
Uterin Anomaliler DES Uterus

Benzer bir sunumlar




 A: _____ nerede? B: _____ evde. (…at home) OR: tell the location using.>")

 Test ve Tartışma Varlıklar Bölümler 14 &15.>")















Gelecekte bir eylemi ne kadar zamandır yapıyor olacağımızı ifade eder By next year,>")
