Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
İnfravezikal obstruksiyon fizyopatolojisi
Cenk Gürbüz İstanbul Göztepe Eğitim ve Araştırma Hastanesi Üroloji Kliniği İnfravezikal obstruksiyon fizyopatolojisi

2
İnfravezikal Obstruksiyon

3
İnfravezikal Obstruksiyon
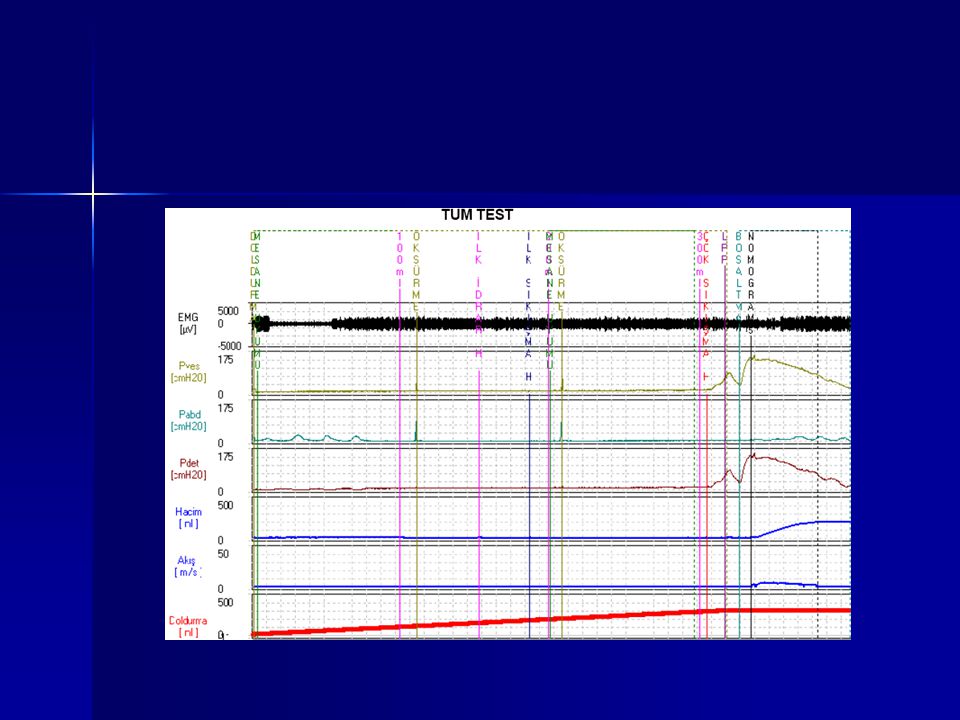
Etyoloji ;Anatomik ve fonksiyonel. Konjenital ( Posterior/anterior üretral valve- üreterosel –üreteral divertikül ve diğerleri) Kazanılmış ( taş- tümör- post operatif oluşan darlık – üretra darlık- benin prostat obstruksiyonu ( BPO)- nörojenik mesane disfonksiyonları ve diğerleri) Tanı ; Basınç Akım Çalışması
 Kazanılmış ( taş- tümör- post operatif oluşan darlık – üretra darlık- benin prostat obstruksiyonu ( BPO)- nörojenik mesane disfonksiyonları ve diğerleri) Tanı ; Basınç Akım Çalışması.")
4
14/198/200

6
Miksiyonda Merkezi Sinir Sistemi Rolü

7
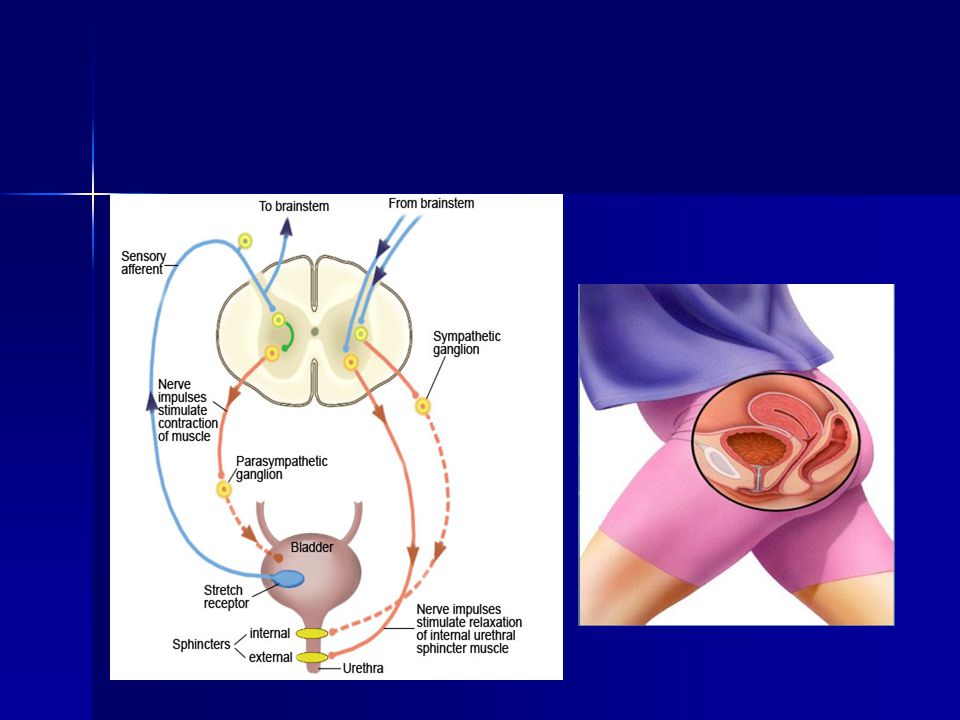
Otonomik ve Somatik Kontrol

8
Mesane ve Mesane boynu resöptör dağılımı

9
Parasempatik Sistem Aktivasyonu
Preganglionik nöronlar sakral intermediate gri maddede bulunur (S2-S4) Parasempatik lifler pelvik sinir içinde rektumun iki yanında pelvik pleksusa katılır Postganglionik nöronlar pelvik pleksus ve detrusor duvarında bulunur
 Parasempatik lifler pelvik sinir içinde. rektumun iki yanında pelvik pleksusa katılır. Postganglionik nöronlar pelvik pleksus ve. detrusor duvarında bulunur.")
10
Sempatik Sistem Aktivasyonu
Preganglionik nöronlar lomber kordda bulunur (T11-L2) Aksonlar önce inferior splenik sinir içinde inferior mezenterik gangliona ulaşır Daha sonra hipogastrik sinir ile pelvik pleksusa ulaşır Parasempatik sinirler ile de sinapslar yaparlar
 Aksonlar önce inferior splenik sinir içinde. inferior mezenterik gangliona ulaşır. Daha sonra hipogastrik sinir ile pelvik. pleksusa ulaşır. Parasempatik sinirler ile de sinapslar. yaparlar.")
11
Somatik Sistem Aktivasyonu
Motor nöronlar Onuf’s nükleusunda bulunur Pudental sinir Eksternal üretral sifinkter Pelvik taban kaslarını uyarır

14
Eski Paradigma Small prostate, thin bladder wall Enlarged prostate,
thick bladder wall Classically, it has been assumed that a small prostate gland is associated with a thin bladder wall and a large prostate gland with a thick bladder wall. In the absence of bladder outlet obstruction by an enlarged prostate gland or other pathologic condition, the wall of the urinary bladder is normally thin. When an enlarging prostate gland impinges upon and narrows the urethra and/or bladder outlet, there is a compensatory hypertrophy of the bladder wall muscle with thickening of the wall. Obstructive symptoms associated with BPH, including reduced urine flow rate and voiding difficulties, are thought to be of a static nature and due almost exclusively to the enlarged prostate gland. Irritative or storage LUTS associated with BPH have been ascribed to bladder dysfunction that is secondary to outflow obstruction. 2.2 14

15
Küçük prostat ve -receptor
Ardından …. Normal prostat Küçük prostat ve -receptor Büyümüş prostat It was subsequently found that obstructive symptoms associated with BPH have not only a static component—the enlarged prostate gland—but also a dynamic component that reflects increased prostatic stromal and urethral smooth muscle tone. Increased tone of this smooth muscle is dependent upon stimulation of a1-adrenoreceptors by noradrenaline released from adrenergic nerves. It has also been found that irritative LUTS may have a neural component. The appreciation that there is no direct correlation between LUTS and the size of the prostate gland or the degree of bladder outlet obstruction was followed by the findings that LUTS may be caused by hypertrophy or denervation of lower urinary tract smooth muscle, defective central processing of afferent information, and defects in efferent neurotransmission, in addition to prostatic enlargement. 2.3 15

16
Brain/ Spinal column/ Prostate
Şimdiki Paradigma Normal Enlarged -receptors Brain/ Spinal column/ Prostate It is currently believed that both obstructive and irritative LUTS associated with BPH involve a1-adrenoreceptors. Much of the current understanding of the mechanisms underlying BPH-related symptoms has come from observations that the administration of a1-adrenoreceptor antagonists improve both irritative LUTS and flow rate in patients with BPH, even in the absence of outflow obstruction. • a1-Adrenoreceptors affecting the lower urinary tract are found in prostatic stroma, bladder detrusor and trigone, urethra, ganglia, and spinal and supraspinal structures. The beneficial effects of a1-adrenoreceptor antagonists on symptoms of BPH may come from action on receptors in any of these areas. Nerves that affect the bladder, prostate, and urethra include the hypogastric (sympathetic) and pudendal (somatic) nerves, which maintain prostatic and urethral tone during bladder filling, and the pelvic nerves (parasympathetic), which induce detrusor contraction and micturition. 2.4 16
 and pudendal (somatic) nerves, which maintain prostatic and urethral tone during bladder filling, and the pelvic nerves (parasympathetic), which induce detrusor contraction and micturition")
17
Schematic diagram of cholinergic nerves and muscarinic receptors in the human prostate. Note that M2 receptors on stromal smooth muscle cells quantitatively play a smaller role than M1 receptors on epithelial cells or a1A-adrenoceptors on smooth muscle cells and that signal transduction and smooth muscle and epithelial cell function presently have been tested in few studies only (see text for details

18
Gecikmiş EUS gevşemesi
The skeletal muscle tone is regulated by a spinal reflex arc (gamma loop), which may be exaggerated with an extrapyramidal neurological lesion.13 Impaired sphincter coordination or poor relaxation of the pelvic floor muscle could be the result of increased excitability of the gamma neurons in Parkinson's disease. It has been presumed that this phenomenon of bradykinesia may be related to the disease severity of parkinsonian patients. We need more data to elucidate the relationship between poor relaxation with urethral sphincter hyperactivity and Parkinson's disease Videourodynamic study of a 67-year-old male patient with Parkinson's disease. Left, increased EMG intensity was noted during the filling phase which did not cease during the voiding phase(arrow). Right, fluoroscopy revealed a narrow membranous urethra (arrow). Qmax = 4 ml/s; Pdet.Qmax = 43 cmH2O. Fig. 2. Videourodynamic study of a 64-year-old male patient with Parkinson's disease. Left, several involuntary detrusor contractions with a guarding reflex of external urethral sphincter were noted during the filling phase. Delayed relaxation of the external sphincter (arrow) was noted during the voiding phase. Right, fluoroscopy revealed a narrow bladder neck and membranous urethra (arrow). Qmax = 11 ml/s; Pdet.Qmax = 62 cmH2O. Pdet.Qmax = 43 cmH2O/ 4 ml/s Psododisinerji Pdet.Qmax= 62 cmH2O./11 Gecikmiş EUS gevşemesi
, which. may be exaggerated with an extrapyramidal neurological. lesion.13 Impaired sphincter coordination or poor relaxation. of the pelvic floor muscle could be the result of. increased excitability of the gamma neurons in. Parkinson s disease. It has been presumed that this phenomenon. of bradykinesia may be related to the disease. severity of parkinsonian patients. We need more data to. elucidate the relationship between poor relaxation with. urethral sphincter hyperactivity and Parkinson s disease. Videourodynamic study of a 67-year-old male patient. with Parkinson s disease. Left, increased EMG. intensity was noted during the filling phase which. did not cease during the voiding phase(arrow). Right, fluoroscopy revealed a narrow membranous urethra. (arrow). Qmax = 4 ml/s; Pdet.Qmax = 43 cmH2O. Fig. 2. Videourodynamic study of a 64-year-old male patient. with Parkinson s disease. Left, several involuntary. detrusor contractions with a guarding reflex of. external urethral sphincter were noted during the filling. phase. Delayed relaxation of the external sphincter. (arrow) was noted during the voiding phase. Right, fluoroscopy revealed a narrow bladder neck and membranous. urethra (arrow). Qmax = 11 ml/s; Pdet.Qmax. = 62 cmH2O. Pdet.Qmax = 43 cmH2O/ 4 ml/s. Psododisinerji. Pdet.Qmax= 62 cmH2O./11. Gecikmiş EUS gevşemesi.")
19
BOO is perceived by the bladder wall as a mechanical
stress, which activates stretch-inducible signals leading to important morphologic and functional modifications in the epithelium, in the SMCs, in the extracellular matrix, and in the neuronal network. Molecular mechanisms supporting this complex process are currently being investigated, and only an incomplete and questionable model can be traced. However, strong evidence is available that both epithelial cells and SMCs are featured with mechanosensitive systems and are able to change gene expression and protein synthesis in response to obstruction, through several transduction signals (Fig. 1). The latter include mainly JNK/AP-1 pathway, PKC, and autocrine angiotensin II stimulation loop. Therefore, although urinary storage-phase symptoms can be more easily and directly linked to bladder detrusor modifications than to prostatic obstruction, in patients with BPH, the BOO is the first initiator of a cascade of events ultimately leading to LUTS, in which the bladder participates essentially as the earliest innocent victim Fig. 1 – Mechanical stretch stress activates bladder wall mechanosensors, which activate intracellular transduction pathways leading to modify gene expression. BOO = bladder outlet obstruction; PDGF-R = platelet-derived growth factor receptor; JNK = c-jun NH2-terminal kinase; AP-1 = transcription factor activator protein-1; AT2 = angiotensin 2; AT1 = angiotensin receptor 1; PKC = protein kinase C; HB-EGF = heparin-binding epidermal growth factor; BMP-2 = bone morphogenetic protein 2; SUPAR = soluble urokinase plasminogen activator receptor; THBD = thrombomodulin; COX- 2 = cyclooxygenase 2; GEM = guanosine triphosphate-binding protein overexpressed in skeletal muscle; LIF = leukemia inhibitory factor; DUSP-1 = dual specificity phosphatase 1; ELL-2 = elongation factor; PAR2 = protease-activated receptor 2; NGF = nerve growth factor.
. The latter include mainly JNK/AP-1 pathway, PKC, and autocrine angiotensin II stimulation loop. Therefore, although urinary storage-phase symptoms. can be more easily and directly linked to. bladder detrusor modifications than to prostatic. obstruction, in patients with BPH, the BOO is the first. initiator of a cascade of events ultimately leading to. LUTS, in which the bladder participates essentially. as the earliest innocent victim. Fig. 1 – Mechanical stretch stress activates bladder wall mechanosensors, which activate intracellular transduction. pathways leading to modify gene expression. BOO = bladder outlet obstruction; PDGF-R = platelet-derived growth factor. receptor; JNK = c-jun NH2-terminal kinase; AP-1 = transcription factor activator protein-1; AT2 = angiotensin 2; AT1 = angiotensin receptor 1; PKC = protein kinase C; HB-EGF = heparin-binding epidermal growth factor; BMP-2 = bone. morphogenetic protein 2; SUPAR = soluble urokinase plasminogen activator receptor; THBD = thrombomodulin; COX- 2 = cyclooxygenase 2; GEM = guanosine triphosphate-binding protein overexpressed in skeletal muscle; LIF = leukemia. inhibitory factor; DUSP-1 = dual specificity phosphatase 1; ELL-2 = elongation factor; PAR2 = protease-activated receptor 2; NGF = nerve growth factor.")
Benzer bir sunumlar










>")










