Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Renal Function Tests Doç.Dr.Jale Çoban

2
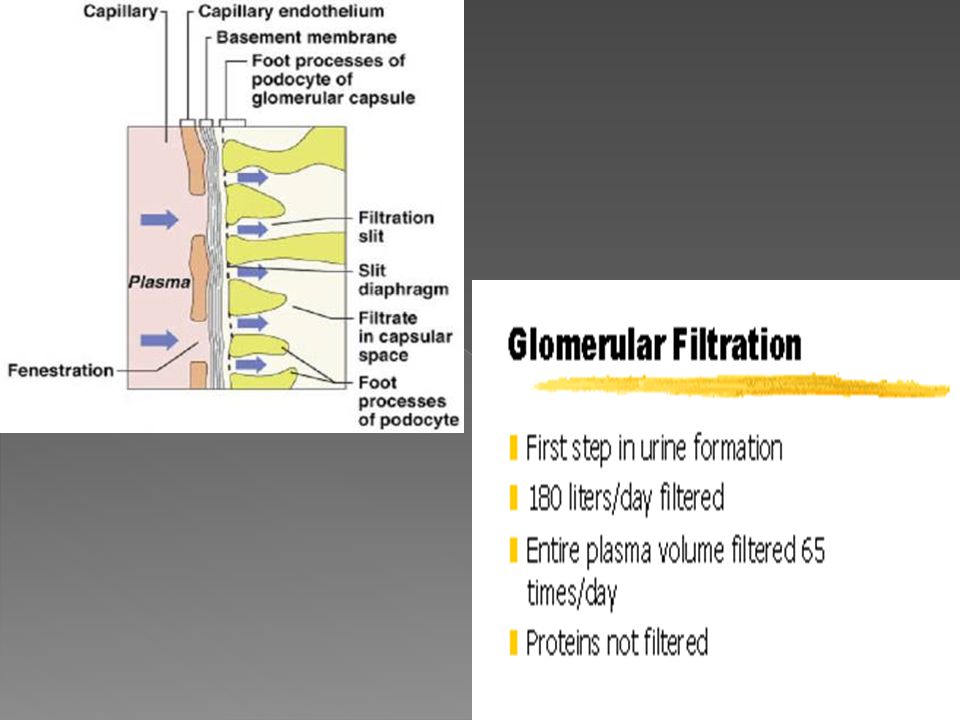
Structural overview Functional overview Clinical features of kidney disease Laboratory investigations

4
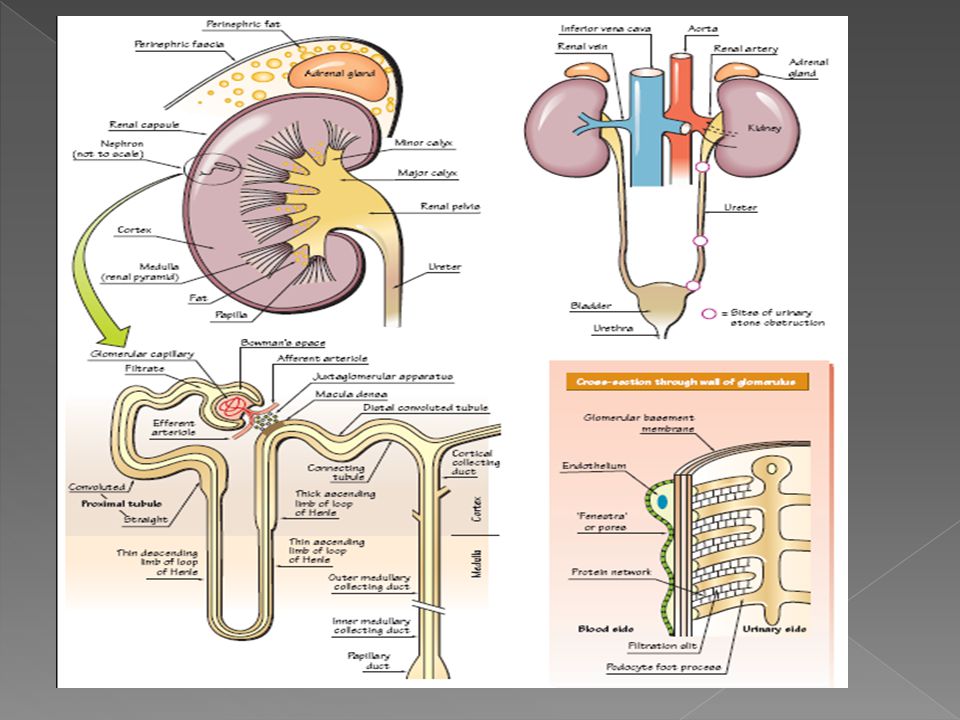
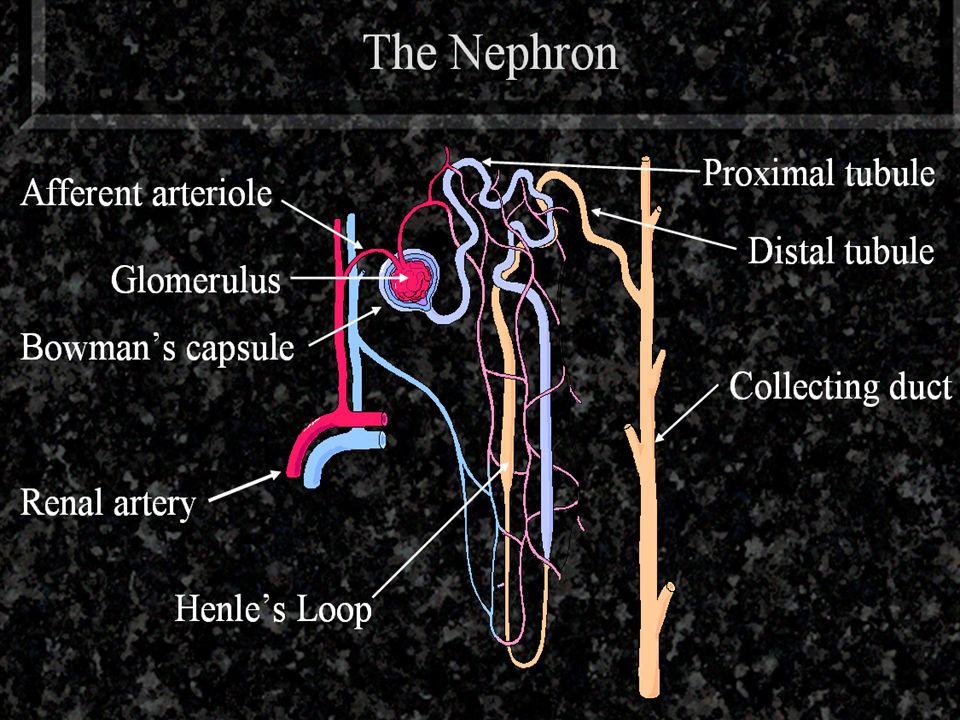
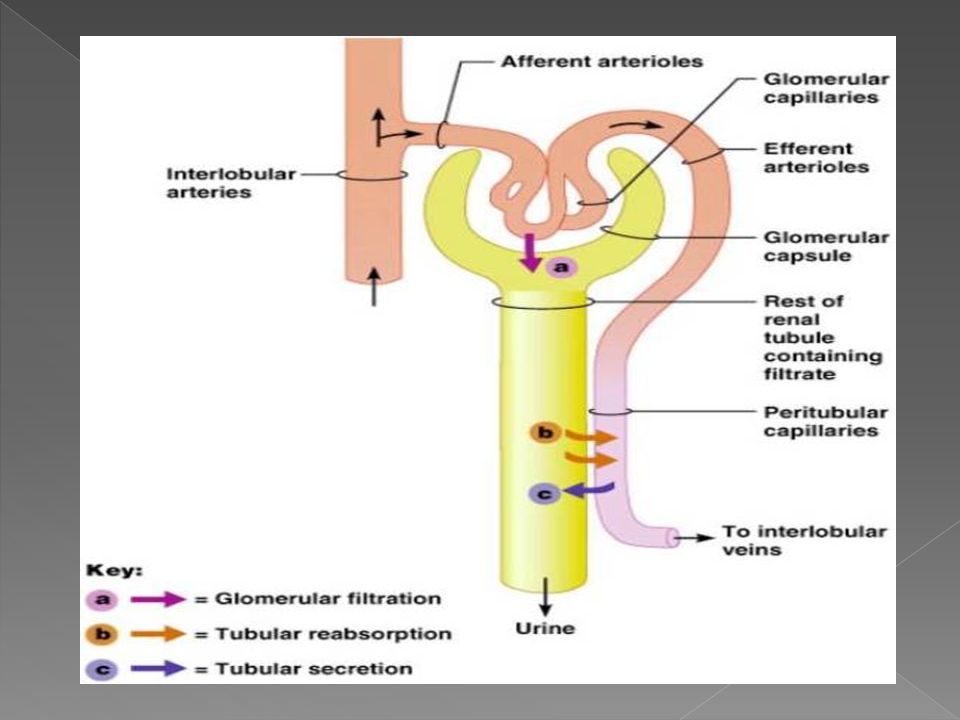
The nephron is the basic unit of the kidney.
Each kidney has – nephrons. A nephron consists of the glomerulus and the associated tubule that leads to the collecting duct. Urine is formed by filtration in the glomerulus; it is then modified in the tubules by the reabsorption and secretion of substances

6
Functions of the kidney

8
Homeostasis acid-base balance,
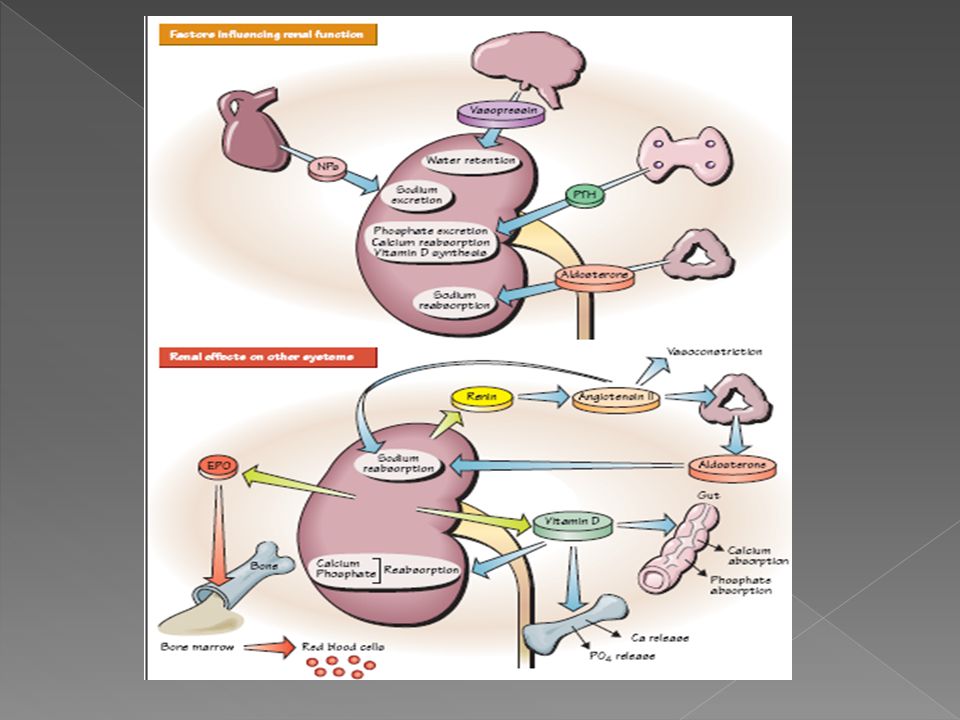
The kidney is one of the major organs involved in whole-body homeostasis. Among its homeostatic functions are acid-base balance, regulation of electrolyte concentrations, control of blood volume, and regulation of blood pressure. The kidneys accomplish these homeostatic functions independently and through coordination with other organs, particularly those of the endocrine system. The kidney communicates with these organs through hormones secreted into the bloodstream.

9
Acid-base balance The kidneys regulate the pH of blood by adjusting H+ ion levels, referred as augmentation of mineral ion concentration, as well as water composition of the blood.

10
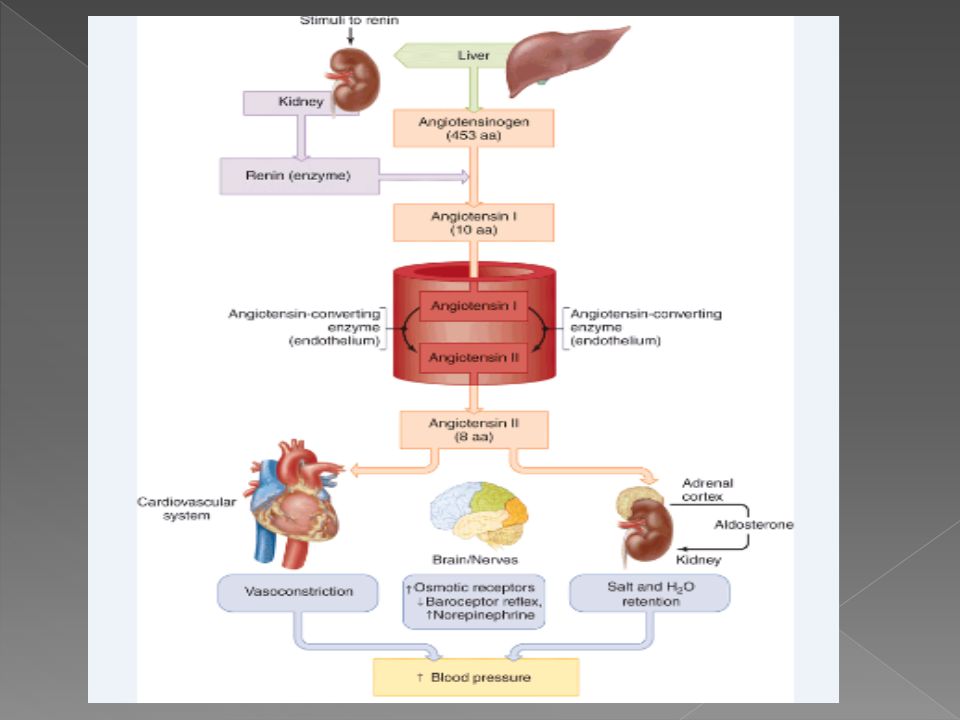
Blood pressure - Renin-angiotensin system
Sodium ions are controlled in a homeostatic process involving aldosterone which increases sodium ion reabsorption in the distal convoluted tubules.

12
Plasma volume Any significant rise or drop in plasma osmolality is detected by the hypothalamus, which communicates directly with the posterior pituitary gland. A rise in osmolality causes the gland to secrete antidiuretic hormone, resulting in water reabsorption by the kidney and an increase in urine concentration. The two factors work together to return the plasma osmolality to its normal levels.

13
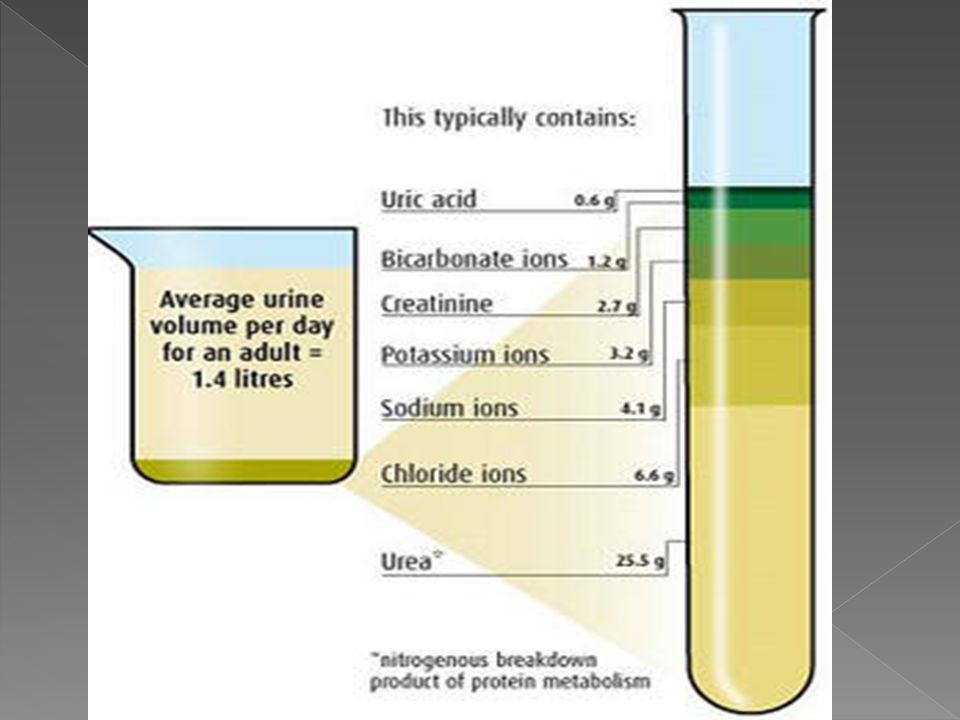
Excretion of waste products
The kidneys excrete a variety of waste products produced by metabolism, including the nitrogenous wastes: urea (from protein catabolism) and uric acid (from nucleic acid metabolism)
 and. uric acid (from nucleic acid metabolism)")
14
erythropoietin, vitamin D. Hormone secretion
The kidneys secrete a variety of hormones, including: renin, erythropoietin, vitamin D.

15
Regulation e.g. homeostasis, water, acid/base
Excretion e.g. urea, creatinine Endocrine e.g. renin, erythropoietin, 1,25 dihydroxycholecalciferol- conversion only in kidney! The kidneys excrete the end products of metabolism, urea from amino acid breakdown, uric acid from purine (nucleic acids) metabolism and creatinine from the catabolism of creatine an amino acid found in muscle. Homeostatic functions include the maintenance of water balance by regulating urine volume, acid base balance by altering hydrogen ion excretion, sodium balance by altering the rate of sodium reabsorption. Endocrine functions include the secretion of renin from the JGA which influences aldosterone. Erythropoietin effects the rate of red cell production and 1,25-dihydroxycholecalciferol is the active form of vitamin D, effecting calcium homeostasis. Patients with chronic renal disease and impaired renal functions will show defects in endocrine and excretory functions before the loss of homeostatic control. When the homeostatic functions cease then the patient is in renal failure and would die if there were no interventions.
 metabolism and creatinine from the catabolism of creatine an amino acid found in muscle. Homeostatic functions include the maintenance of water balance by regulating urine volume, acid base balance by altering hydrogen ion excretion, sodium balance by altering the rate of sodium reabsorption. Endocrine functions include the secretion of renin from the JGA which influences aldosterone. Erythropoietin effects the rate of red cell production and 1,25-dihydroxycholecalciferol is the active form of vitamin D, effecting calcium homeostasis. Patients with chronic renal disease and impaired renal functions will show defects in endocrine and excretory functions before the loss of homeostatic control. When the homeostatic functions cease then the patient is in renal failure and would die if there were no interventions.")
19
RENAL DİSORDERS ACUTE RENAL FAİLURE Prerenal acute renal failure
Intrinsic acute renal failure Postrenal renal failur Chronic renal failure

20
Prerenal acute renal failure
haemorrhage, fluid loss, cardiac failure or hypotension that leads to renal hypoperfusion and a decrease in GFR

21
Intrinsic acute renal failure
Many cases are due to nephrotoxic drugs (aminoglycosides and non-steroidal anti-inflamatory drugs) Renal ischaemia (following severe blood loss or hypotension) leading to acute tubuler necrosis
 Renal ischaemia (following severe blood loss or hypotension) leading to acute tubuler necrosis.")
22
Postrenal renal failure
Obstruction to the flow of urine leads to an increase in hydrostatic pressure, which acts in opposition to glomerular filtration and, if prolonged, leads to secondary renal tubular damage. Causes of obstruction include renal calculi, prostatic enlargement (hypertrophic or neoplastic), other neoplasms of the urinary tract.
, other neoplasms of the urinary tract.")
23
Chronic renal failure Many disease processes (glomerulonephritis, Diabetes mellitus, hypertansion, pyelonephritis and polycystic kidneys) can lead to progressive, irreversible impairment of renal function. Chronic renal failure develops insidiously, often over many years, and is irreversible, leanding eventually to end-stage renal failure. Patients with end-stage renal failure require either long-term renal replacement treatment (i.e., dialysis) or a successful renal transplant in order to survive.
 can lead to progressive, irreversible impairment of renal function. Chronic renal failure develops insidiously, often over many years, and is irreversible, leanding eventually to end-stage renal failure. Patients with end-stage renal failure require either long-term renal replacement treatment (i.e., dialysis) or a successful renal transplant in order to survive.")
24
Renal function tests detect renal damage monitor functional damage
help determine etiology From a clinical perspective it is important to have test which would have these characteristics. No such test exists. An early test to detect renal damage, for instance a simple strip test for haematuria is important in screening for heavy metal poisoning. There is a clinical need to monitor a patient with renal disease and this is achieved by serial plasma measurements. We need to know when to start dialysis in renal failure and laboratory tests assist the clinical decision making. There are about a million nephrons in each kidney and this represents a considerable functional reserve. In renal disease about half the nephrons have to lose their functioning before the abnormality can be detected by conventional laboratory tests.

26
Inorganic constituents

28
Laboratory tests of renal function
Urinalysis by test strips Serum Creatinine or Urea /BUN(blood urea nitrogen) Creatinine clearance Urinary proteins Urinary stones tests
 Creatinine clearance. Urinary proteins. Urinary stones tests.")
29
Diseases affecting the kidneys can selectively damage
glomerular or tubuler function

30
The principal function of the glomeruli is to filter water and low molecular weigh components of the blood and retaining cells and high molecular weigth components

31
Laboratory tests of renal function
Urinalysis by test strips – Tests of glomerular filtration rate Tests of renal tubular function

32
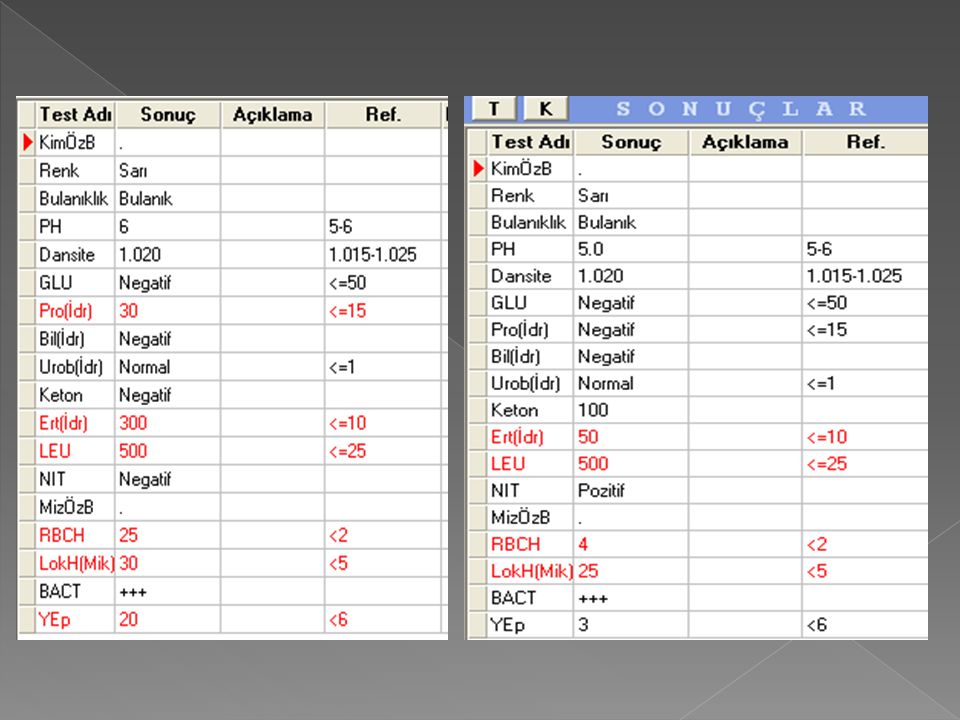
Urinalysis by test strips
Now a really easy, cheap, sensitive, routine way of testing subjects, but not good enough on its own and not quantitative

33
Urinanalysis Oligouria – excrete < 300 ml/day.
Might be “physiological” as in hypotension or hypovolaemia where we compensate, but more often due to renal disease or obstructive nephropathy. Polyuria – persistent, large increase in urine output associated with nocturia. Must distinguish from higher frequency of small volumes of urine. Usually due to hysterical intake of water, increased excretion of solute (e.g. hyperglycaemia/glycosuria), defect in concentrating ability or ADH failure). Osmolality – useful for determining whether ionic imbalances exist in subject. May indicate renal failure (e.g. excess urea) or problems with ADH. Urinary pH – mainly for acidosis/alkalosis determination – important when studying metabolism of various nutrients e.g. glucose during exercise
, defect in concentrating ability or ADH failure). Osmolality – useful for determining whether ionic imbalances exist in subject. May indicate renal failure (e.g. excess urea) or problems with ADH. Urinary pH – mainly for acidosis/alkalosis determination – important when studying metabolism of various nutrients e.g. glucose during exercise.")
34
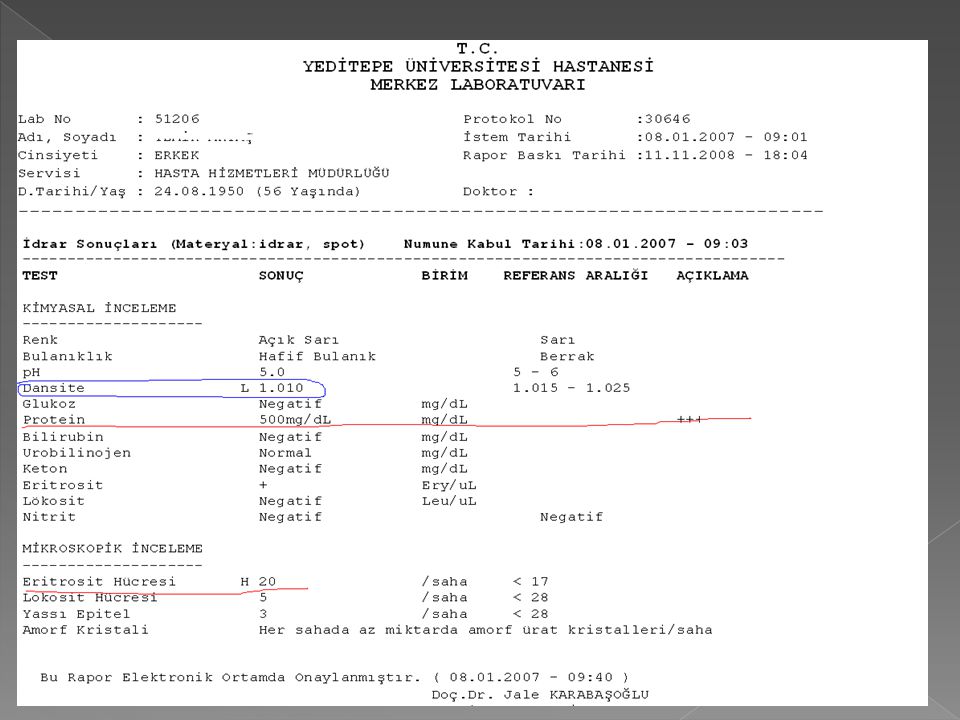
Chemical (Stix) testing
Blood – very sensitive – 2 or more cells can produce result. Sometimes TOO sensitive, giving false positives. Can’t distinguish between blood and free Hb, so usually double-check with microscope. Protein Strips detect 100 mg/l or more in urine – react with albumin. Check throughout 24 hr period Some protein always excreted, but can be falsely increased by exercise, growth, fever etc. Time of day taken – lying down causes protein to settle and it’s not detected in urine. Glucose Positive test can mean diabetes mellitus. Have to exclude ingestion of high sugar diet.

35
Urine Microscopy

37
Urine Microscopy Clean, mid-stream sample needed. White cells
10 or more WBC’s per cm3 indicates inflammation (e.g. urinary tract infection) Red cells – again, subject may be aware of it already via pain. Casts Cylindrical bodies made from precipitated proteins, often seen normally after exercise. Red cell casts (even one) always means disease. Bacteria – allows you to decide which antibiotic is best for subject. Checking for blood/urine not always good for checking for infections, since these subjects can have completely clear urine
 Red cells – again, subject may be aware of it already via pain. Casts. Cylindrical bodies made from precipitated proteins, often seen normally after exercise. Red cell casts (even one) always means disease. Bacteria – allows you to decide which antibiotic is best for subject. Checking for blood/urine not always good for checking for infections, since these subjects can have completely clear urine.")
38
Epitel Hücreleri Squamoz epitelyal hücreler:
Üriner yolun son kısmı olan üretra ve kadında vagina kontaminasyonu kaynaklıdır.İdrarda en yaygın bulunan epitel hücreleridir Çok büyük olup (idrar mikroskopisinde görülen en büyük hücre), küçük (hücreye göre çok küçük) ve tek çekirdekli, iri sitoplazmalı, yassı, düzensiz sınırları bulunan hücrelerdir. Bazılarında çift çekirdek görülebilir İdrarda her sahada 5 adet bulunması normal kabul edilir Vaginal kontaminasyon, idrar örneğinin cilt florası ile muhtemel kontaminasyonu, Üretrovaginal/ üretrovezikal fistül, Üretrit gibi durumları düşündürmelidir
, küçük (hücreye göre çok küçük) ve tek çekirdekli, iri sitoplazmalı, yassı, düzensiz sınırları bulunan hücrelerdir. Bazılarında çift çekirdek görülebilir. İdrarda her sahada 5 adet bulunması normal kabul edilir. Vaginal kontaminasyon, idrar örneğinin cilt florası ile muhtemel kontaminasyonu, Üretrovaginal/ üretrovezikal fistül, Üretrit gibi durumları düşündürmelidir.")
39
Renal Tübüler Epitelyal Hücreler
Böbrek korteks ve medullasındaki tübülleri oluşturan epitelden kaynaklıdır. Küçük, yuvarlak, çok köşeli (poliglonal) dir. Lökositlerden biraz büyük olup, granüler ve yassı epitel hücresine göre büyük bir çekirdeği bulunur. Dansitesi düşük bir idrarda lökositlere çok benzer. Nefrotik sendrom ve akut tübüler hasarda idrardaki sayıları artar. İdrarda normalde bulunmaz. Lökositlerle karışabilir. Ancak Lökositten daha büyüktürler. Yukarıdaki resimde likosit ve tübüler epitel bir arada görülüyor.
 dir. Lökositlerden biraz büyük olup, granüler ve yassı epitel hücresine göre büyük bir çekirdeği bulunur. Dansitesi düşük bir idrarda lökositlere çok benzer. Nefrotik sendrom ve akut tübüler hasarda idrardaki sayıları artar. İdrarda normalde bulunmaz. Lökositlerle karışabilir. Ancak Lökositten daha büyüktürler. Yukarıdaki resimde likosit ve tübüler epitel bir arada görülüyor.")
40
Transizyonel Epitelyal Hücreler:
Böbrek pelvisinden üretra çıkışına kadar üriner sistemin büyük çoğunluğunun iç yüzeyini döşeyen epitelden kaynaklanır. Daha düzenli ve hücre sınırları mevcuttur. Merkezi nükleuslu, füsiform (sferik, poliheral, iğ şeklinde, armudumsu, değişik şekillerde) sitoplazmalı epiteldir. Mesaneden gelenler daha çok köşeli-iri - pul gibidir. İdrarda her sahada 5 adet bulunması normal kabul edilir. İdrarda her sahada 5 den fazla bulunması na değişici epitel (transisyonel epitelüri) atılımı denir. Üriner sistem inflamatuar hastalıklar ,travmaya bağlı (sistoskopi) ve mesane kanserinde artabilir.
 sitoplazmalı epiteldir. Mesaneden gelenler daha çok köşeli-iri - pul gibidir. İdrarda her sahada 5 adet bulunması normal kabul edilir. İdrarda her sahada 5 den fazla bulunması na değişici epitel (transisyonel epitelüri) atılımı denir. Üriner sistem inflamatuar hastalıklar ,travmaya bağlı (sistoskopi) ve mesane kanserinde artabilir.")
41
Hyalen Silendir İdrarda en sık bulunan silendirdir. Saydam, renksizdir. Işık kontrast hale getirilince daha kolay görülür Hyalen silendirlerin klinikte önemleri fazla değildir. Klinik değeri azdır. Her sahada 2 tane bulunması normal kabul edilir.Ancak; genişse böbrek tubulus hastalıklarını gösterir. Ayrıca idrarda devamlı görülmesi organik böbrek has. gösterir. Akut nefritik sendrom, akut glomerulonefrit ve nefrotik sendromda rastlanabilir. Asit idrarda, konsantre idrarda ve diüretik tedavisinde, dehidratasyonda ve normalde görülebilirler.

42
Eritrosit Silendir Hiyalen silendire eritrosit girmesiyle oluşur.
İdrarda normalde bulunmaz. Eritrosit silendir aşikar bir glomerül lezyonunu ve özellikle aktif bir glomerülonefriti gösterir. Akut nefritik sendrom (akut glomerülonefrit ve diğerleri) için tipiktir.
 için tipiktir.")
43
Lökosit Silendir Hiyalen silendire lökosit girmesiyle oluşur. Bazen lökositler; parçalar halinde, kümeler şeklinde, deforme şekilde bulunur. Bol piyüri ile beraber görülürse piyelonefrit veya tübülointerstisyel hastalık için karakteristiktir. Eritrosit silendiri ile beraber görüldüğünde glomerülonefrit düşünülmelidir.

44
Epitel Silendir Hiyalen silendire epitel girmesiyle oluşur. Burada ufak bir hatırlatma yapmakta yarar var: silendirler tübülüslerde oluşur, bu yüzden yapısına sadece renal tübüler epitel girebilir, tübülüslerin altında lokalize olan transisyonel epitel ya da yassı epitel asla sediment yapısına giremez Tubulusları (tubuler epitel hücreleri) etkileyen olaylarda görülür. Viral enf. Akut piyelonefrit ABY-ATN Amiloidoz Ağır metal toksikasyonunda görülür.
 etkileyen olaylarda görülür. Viral enf. Akut piyelonefrit. ABY-ATN. Amiloidoz. Ağır metal toksikasyonunda görülür.")
45
Yağ Silendir Anlamlı proteinürili hastalar arasında epitelyal silendir içindeki hücrelerin Dejenerasyonu karakteristik „maltese cross“ görünümüne ve yağ silendirlerine neden olabilir. Bu damlacıklar kolesterol ve kolesterol esterlerinden oluşur . Nefrotik senromda görülür.

46
Granüler Silendir Homojen, granüler, yoğun, düz, silendirik yapıdadır. Şekli ve büyüklüğü hiyalin silendire benzer ama şeffaf- mat değildir, granüllüdür. Görünümüne göre iki tiptir: İnce granüllü silendirler: Granüller küçük ve düzenlidir. Işığı az kırar.Kaba granüllü silendirler: Granüller büyük ve düzensizdir (irregüler). Işığı çok kırar. Hücresel hasarı göstergesidir Nefrotik, nefritik sendrom ve glomerülonefritlerde görülür. Silendirler daha önce var olan hücre silendirlerinde eritrosit, lökosit veya epitellerin dejenere olup parçalanması sonucunda oluşurlar.
. Işığı çok kırar. Hücresel hasarı göstergesidir. Nefrotik, nefritik sendrom ve glomerülonefritlerde görülür. Silendirler daha önce var olan hücre silendirlerinde eritrosit, lökosit veya epitellerin dejenere olup parçalanması sonucunda oluşurlar.")
48
KALSİYUM OKZALAT KRİSTALİ
En sık görülen kristal oluşumudur. pH=6-7 civarında oluşur. Renksizdir. İki şekli bulunur: Dihidrat şekli: Mektup zarfı şeklindedir.Daha sık rastlanır.Monohidrat şekli: Yuvarlak, halter şeklindedir. Daha nadir rastanır. İdrarda normalde bulunabilir. Klinikle uyumlu görülmesi patolojik sayılabilir. Ispanak- portakal- domates-sarımsak- asparagus- meyan kökü gibi okzalik asit yönünden zengin besinler alındığında görülür. Yüksek doz askorbik asid alımında Taş: Taze idrarda kümeler halinde olup eritrosit ve lökosit ile beraber görülürse önem taşır.DM, karaciğer has, kalp has, akc. has artar

49
TRİPLE FOSFAT (AMONYUM MAGNESYUM FOSFAT) KRİSTALİ
Sarımtrak- renksizdir. Tabut kapağı şeklindedir. X harfi- tavuk tüyüne benzer şekilde de görülebilir. Bakteriyel artışla birliktedir. Üriner stazda (Prostat büyümesi) Kronik enf. (kronik sistitde)
 Kronik enf. (kronik sistitde)")
50
AMORF FOSFAT KRİSTALİ Amorf şekilde görülür. Büyük kümeler haline ince granüller şeklinde görülür. Santrifüj sonrası tüpün dibinde beyaz bir çökelek oluşur Görüldüğü duruml Yüksek ateş Sıvı kaybı

51
KALSİYUM FOSFAT KRİSTALİ
Renksizdir. Geniş- ince- düzensiz- noktalı tabakalar şeklindedir. Geniş plaklar şeklinde de olabilir. Prizmalar birleşerek rozet veya yıldız şeklinde görülebilir (Yıldızı gibi fosfatlar da denir). Görüldüğü durumlar Kronik sistit Prostat hipertrofisinde
. Görüldüğü durumlar. Kronik sistit. Prostat hipertrofisinde.")
52
ÜRİK ASİT KRİSTALİ Sarı- kahverengi renkte veya renksizdir.
Kama, halter, baklava, prizmatik rozetler, kübik, oval, düzensiz- hexagonal tabakalar halinde görülebilir. Santrifüj sonrası tüpün dibinde pembe bir çökelti oluşturur İdrarda normalde bulunabilir. Klinikle uyumlu olarak görülmesi patolojik sayılabilir. Görüldüğü durumlar: - Taş (Taze idrarda bulunması teşhisi açısından önemli olabilir kümeler halide saptanırsa böbrek- mesanede taş göstergesidir) - Gut - Akut ateşli hastalıklar - Kronik nefritik sendrom
 - Gut. - Akut ateşli hastalıklar. - Kronik nefritik sendrom.")
53
SİSTİN KRİSTALİ Renksiz - hexagonaldir (6 köşeli). Refraktildir. Taze idrarda biraraya gelme eğilimdedir. İdrarda normalde bulunabilir. Klinikle uyumlu görülmesi patolojik sayılabilir. Sistinüri denir. Görüldüğü Durumlar: - Konjenital sistinüri (Klinik olarak tek anlamlı kristalüridir) - Wilson hastalığı
 - Wilson hastalığı.")
54
BİLURİBİN KRİSTALİ Sarı- kırmızı- kahverengi renktedir. Baklava, iğne, granüler şekilinde görünür. Biluribin yüksekliği olan durumlarda: Obs. Sarılık, karaciğer kanseri, karaciğer sirozu, tifo, kızıl, fosfor zehirlenmesinde görülür.

55
ÜRAT KRİSTALLERİ Sarı-pembe- turuncu (tuğla rengi) renktedir. İdrarda normalde bulunabilir.Yüksek ateş, sıvı kaybında da olabilir

56
SODYUM ÜRAT KRİSTALİ Sarı-kahverenkli renksizdir.Amorf veya kristal şekilde olabilir.Yelpaze, ince uzun prizmalar şeklindedir. İdrarda normalde bulunabilir. Ateşli hastalıklar durumlarında da görülebili

57
KOLESTEROL KRİSTALİ Renksizdir. Bir- birkaç köşesi kesik veya çentikli, geniş, yassı dikdörtgen tabakalar şeklinde görülür. İdrarda normalde bulunabilir - Dondurulmuş- beklemiş idrarda. - Nefrotik sendrom - Lenfatik obs. - Lipoid nefroz, membranöz glomerülonefrit - Sistit, pyelit gibi hastalıklarda görülür.

58
KALSİYUM SÜLFAT KRİSTALİ
Uzun renksiz iğneler- uzun prizmalar şeklinde görülür. Klinik önemi yoktur

60
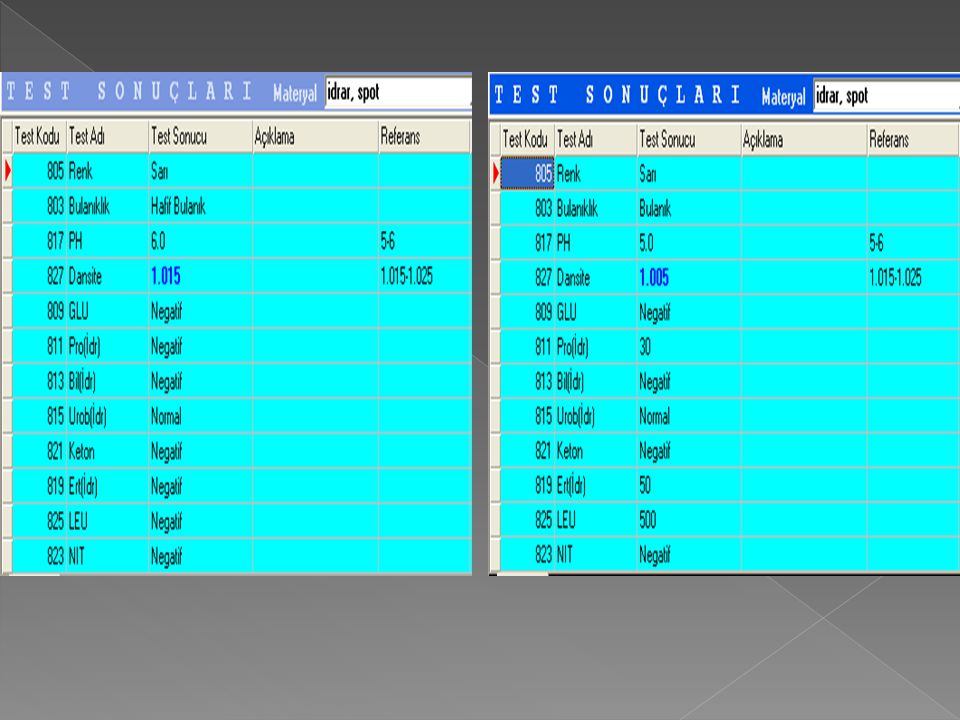
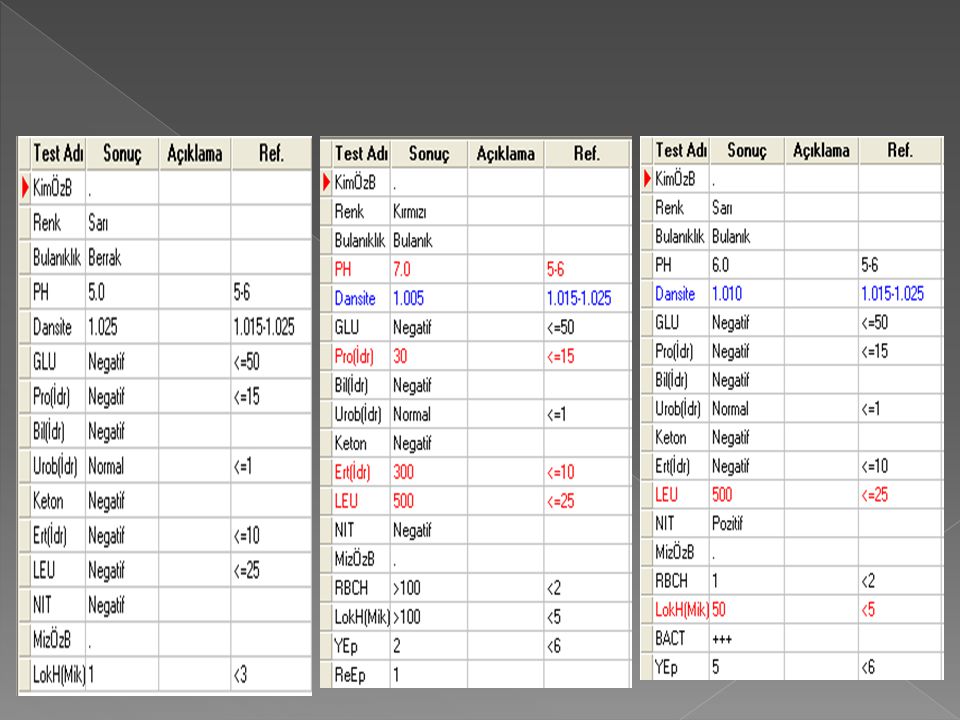
Urinalysis by test strips
Urinalysis can be done macroscopically, biochemically microscopically (urinary sediment) I shall review the tests in the left column today. The measurement of urine protein is important in certain conditions, e.g.diabetes. The detection of substances such as red cells or glucose could be an early indicator of renal damage.
 I shall review the tests in the left column today. The measurement of urine protein is important in certain conditions, e.g.diabetes. The detection of substances such as red cells or glucose could be an early indicator of renal damage.")
61
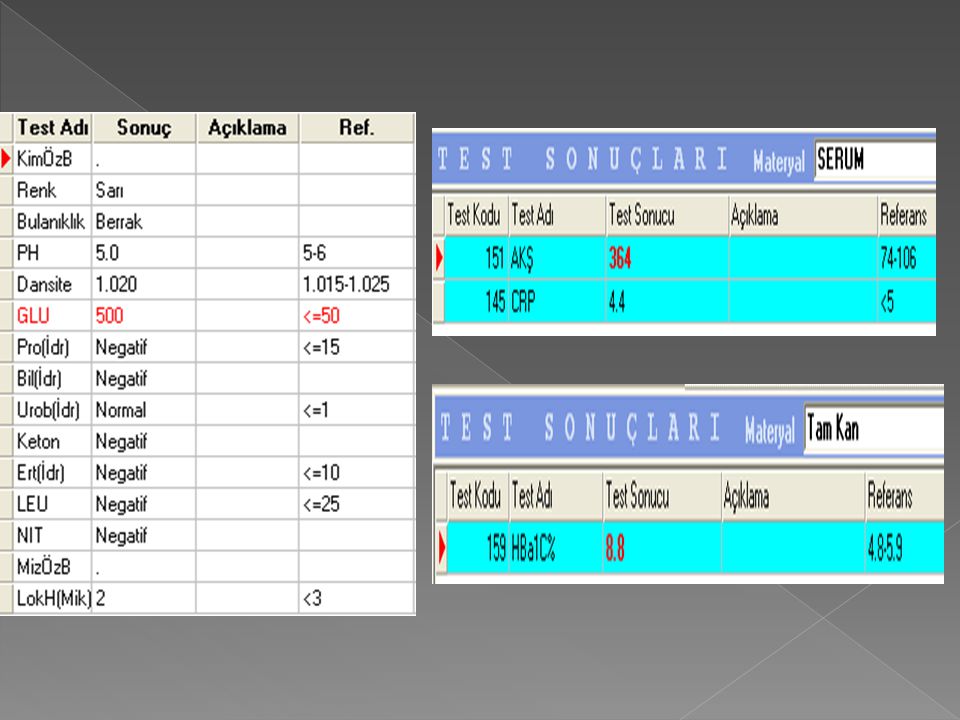
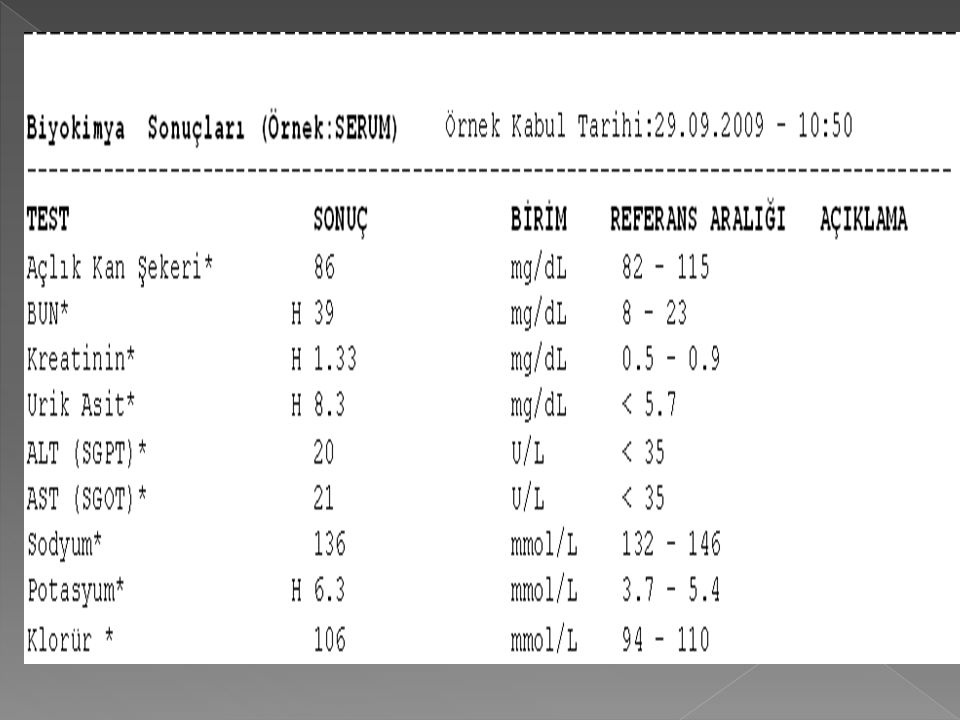
Blood values – indirect indicators of renal function
If there is poor renal function, you might expect any one of: Hyperkalaemia Decreased bicarbonate – poor filtration or acid/base disorders Elevated urea Elevated creatinine Elevated uric acid Hypocalcaemia Hyperphosphataemia pH – acid/base disorders pCO2 away from 40mmHg – acid/base disorders Hypernatraemia These are the most common plasma constituents we would measure if we were analysing renal function in the lab. Cheap, easy, routinely done, and provide a large amount of information quickly.

62
GLOMERULAR FUNCTION TESTS

63
Serum urea /BUN = BUN (blood urea nitrogen)
Urea: product of protein catabolism Synthesized by liver, majority excreted by kidney, partially reabsorbed in tubuli Plasma concentration increases with decreased GFR Urea is easily measured. It has a wide reference range and the value increases after a meal. Its concentration is increased in many different conditions which makes it sensitive to the presence of disease but a non-specific test.

64
Serum UREA/BUN Urea production is rapidly affected by protein intake. It fluctuates more widely than creatinine. When protein catabolism is increased, urea rises rapidly as in haemorrhage in the bowels or body tissues, severe infections, burns, muscle injury, ingestion of steroids and tetracycline Urea level falls with a low protein diet, starvation and liver damage.

65
Plasma urea /BUN BUN (Blood Urea Nitrogen) Urea MA=60g/mol (%28 N)
60/28=2.14 Urea / 2.14 = BUN BUN x 2.14 = Urea Normal range BUN – 8-20 mg/dl Urea – mg/dl Urea is easily measured. It has a wide reference range and the value increases after a meal. Its concentration is increased in many different conditions which makes it sensitive to the presence of disease but a non-specific test.

66
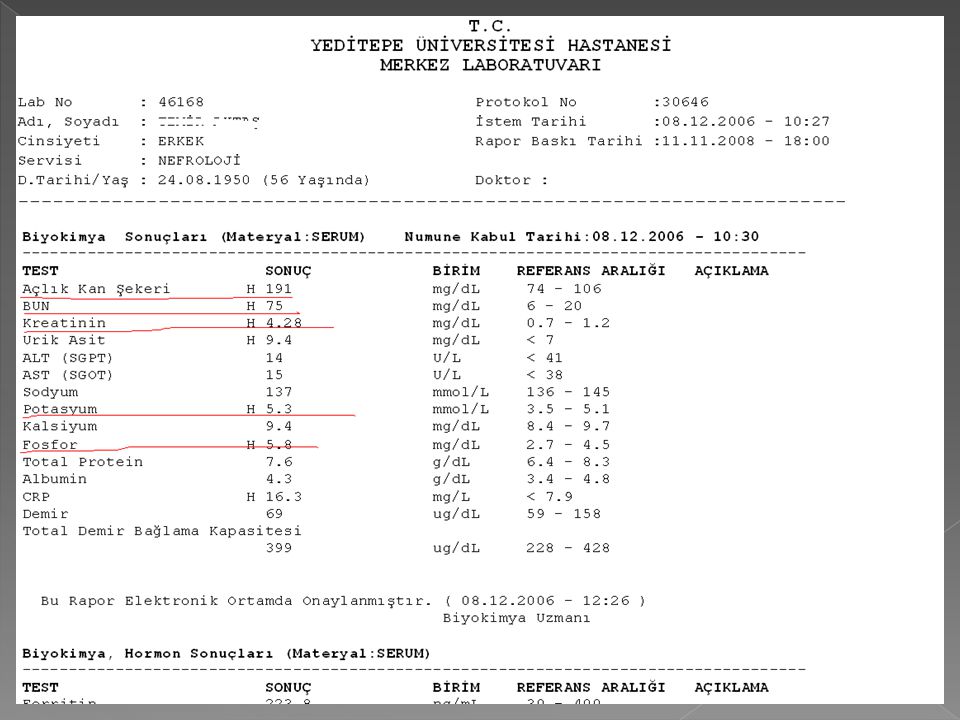
Serum urea (BUN) BUN influenced by diet and hormones, so it is NOT as good an indicator of renal function as serum creatinine levels BUN increased in kidney disease, high protein diet, and after administration of steroids BUN decreased in starvation, pregnancy and in persons on a low protein diet Urea is easily measured. It has a wide reference range and the value increases after a meal. Its concentration is increased in many different conditions which makes it sensitive to the presence of disease but a non-specific test.

67
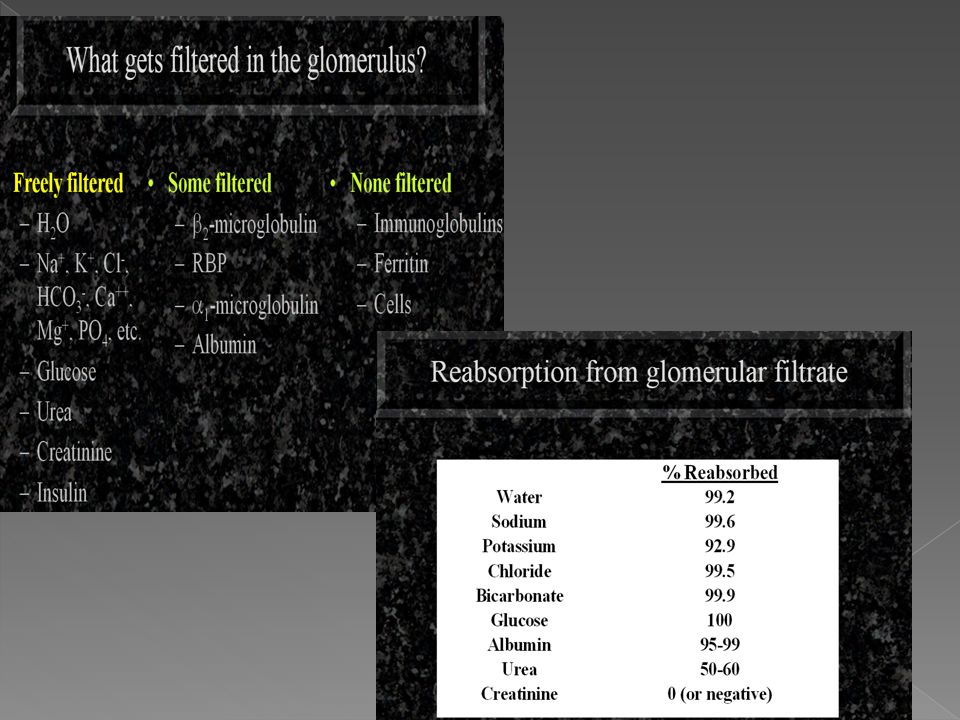
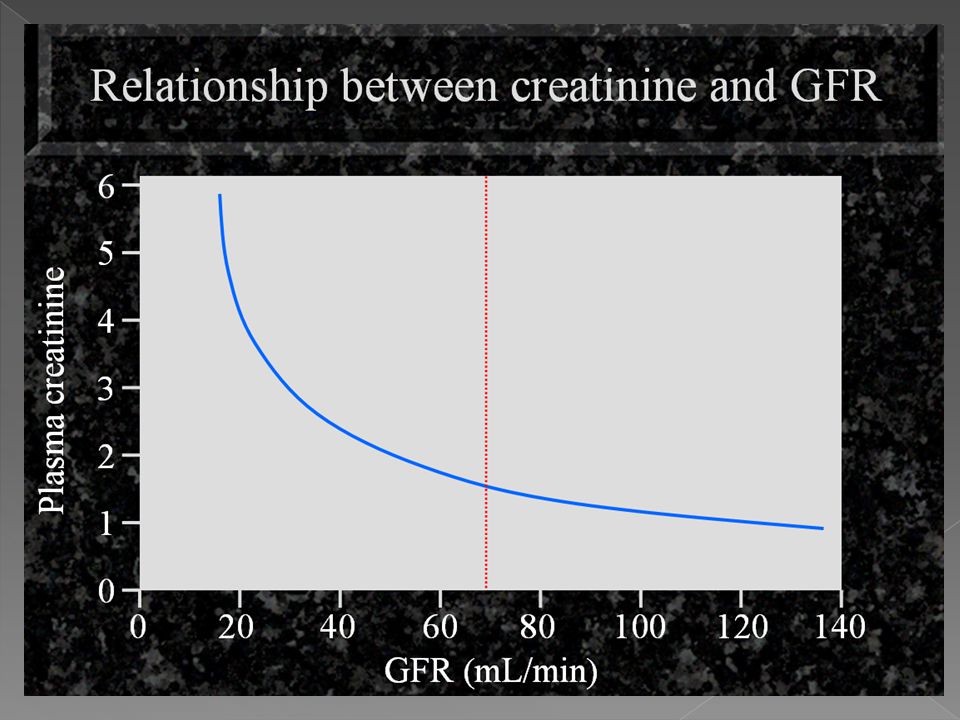
Serum Creatinine Creatine: main storage compound of high energy phosphate needed for muscle metabolism. Creatinine: anhydride of creatine! Creatine Creatinine (Waste product) In most circumstances the measurement of plasma creatinine can provide a specific test of glomerular function. The reference range is wide. A body builder may have a plasma creatinine at the top end and an old lady a value at the low end and this reflects muscle mass. Plasma creatinine should not be measured until 8 hours after a meal as there is some evidence that the concentration increases after meat ingestion. Plasma creatinine concentration increases when GFR falls. The problem is that GFR has to fall quite a bit before plasma creatinine concentration reliably increases. There are some important analytical interferences which you should check with the laboratory. A patient with ketoacidosis, jaundice or infection might have agents in the plasma which could invalidate the measurement of creatinine. Overhead 1 follows H2O
 In most circumstances the measurement of plasma creatinine can provide a specific test of glomerular function. The reference range is wide. A body builder may have a plasma creatinine at the top end and an old lady a value at the low end and this reflects muscle mass. Plasma creatinine should not be measured until 8 hours after a meal as there is some evidence that the concentration increases after meat ingestion. Plasma creatinine concentration increases when GFR falls. The problem is that GFR has to fall quite a bit before plasma creatinine concentration reliably increases. There are some important analytical interferences which you should check with the laboratory. A patient with ketoacidosis, jaundice or infection might have agents in the plasma which could invalidate the measurement of creatinine. Overhead 1 follows. H2O.")
68
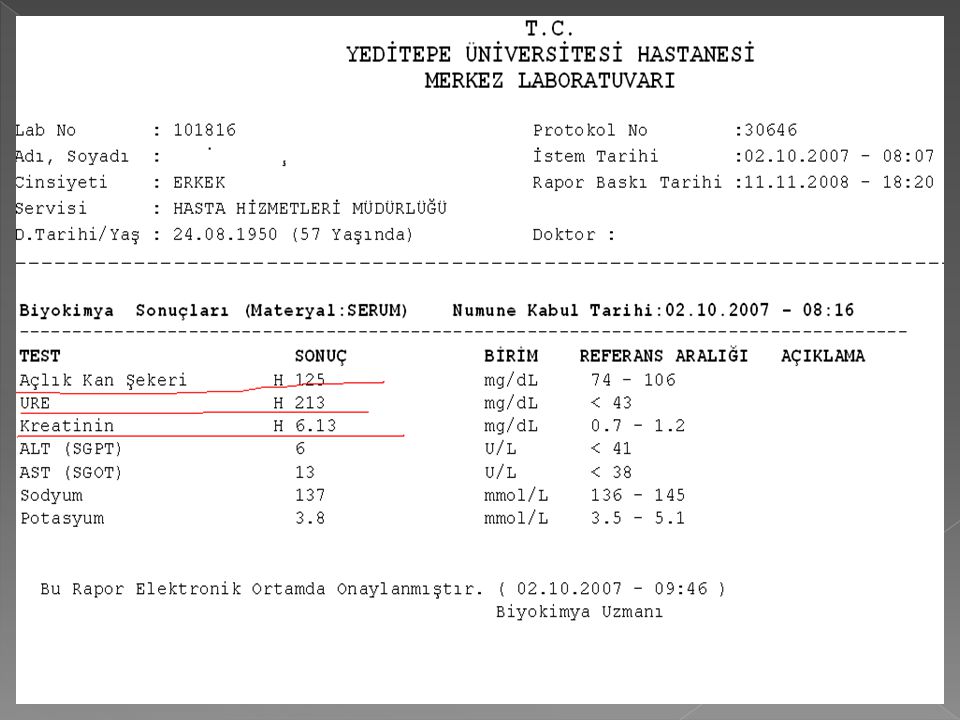
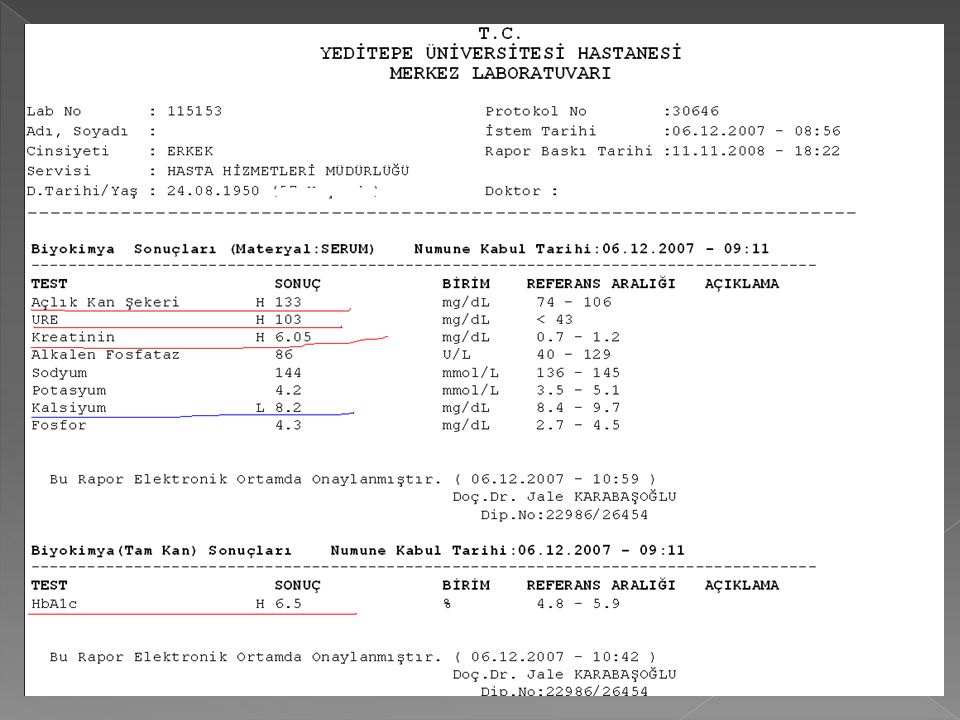
Serum Creatinine Male 0.6-1.2 mg/dL, Female 0.5-1.0 mg/dL
Best test for overall kidney function; not affected by diet or hormone levels Waste product of muscle metabolism Serum creatinine rises when kidney function is impaired

69
Glomerular filtration rate (GFR)
Normal GFR ml/min/1.73 m2 Urea is easily measured. It has a wide reference range and the value increases after a meal. Its concentration is increased in many different conditions which makes it sensitive to the presence of disease but a non-specific test.

71
Clearance test Clearance is theoretical concept and is defind as the volume of plasma from which a measured amound of substance can be completely eliminated (cleared) into the urine per unit of time. This depends on the plasma concetration and excretory rate, wich, in turn, involve the glomerular filtration rate (GFR) and plasma flow.
 into the urine per unit of time. This depends on the plasma concetration and excretory rate, wich, in turn, involve the glomerular filtration rate (GFR) and plasma flow.")
72
Glomerular filtration rate(GFR)
Clearance test GFR is the most widely used test of renal function. Ideally, it is measured using a substance which is: Eliminated only by the kidney Completely filtered from the blood by the glomeruli is not secreted, reabsorbed or metabolized by the renal tubules. Easily and accurately measured

73
INULİN CLEARENCE Its accuracy is therefore a gold standard.
The volume of blood from which inulin is cleared or completely removed in one minute is know as the inulin clearence and is equal to the GFR. GFR as measured by inulin clearance is a research tool. Measurement of İnulin clearence requires the infusion of inulin into the blood and is not suitable for routin clinical use.

74
CREATİNİNE CLEARANCE The most frequently used clearance test is based on the measurement of creatinine. This endogenous substance is derived mainly from the turnover of creatine in muscle and daily production is relatively constant. A small amount of creatinine is derived from meat in the diet. There is a slight amount secreted by the tubules but common methods slightly overestimate plasma concentration. A 24-hour urine collection is necessary. This urine specimen is also useful for quantitation of urinary protein. The GFR varies inversely with the plasma concentration.

75
CREATİNİNE CLEARANCE

76
CREATİNİNE CLEARANCE is calculated according to the clearance formula
1.73 A C (mL/min/1.73m2) = Creatinine(urine) Creatinine(serum) V x x C = clearance in mL per min V = urine quantity per collection time A = body surface area in surface area in sguare meters I shall review the tests in the left column today. The measurement of urine protein is important in certain conditions, e.g.diabetes. The detection of substances such as red cells or glucose could be an early indicator of renal damage. Referans Range = Man 120 mL/min/1.73m2 Women 100 ml/min/1.73 m2
 = Creatinine(urine) Creatinine(serum) V. x. x. C = clearance in mL per min. V = urine quantity per collection time. A = body surface area in surface area in sguare meters. I shall review the tests in the left column today. The measurement of urine protein is important in certain conditions, e.g.diabetes. The detection of substances such as red cells or glucose could be an early indicator of renal damage. Referans Range = Man 120 mL/min/1.73m2. Women 100 ml/min/1.73 m2.")
77
CLEARANCE = U x V S U = concentration of creatinine in urine
I shall review the tests in the left column today. The measurement of urine protein is important in certain conditions, e.g.diabetes. The detection of substances such as red cells or glucose could be an early indicator of renal damage. U = concentration of creatinine in urine S = serum creatinine concentration V = urine quantity per collection time

79
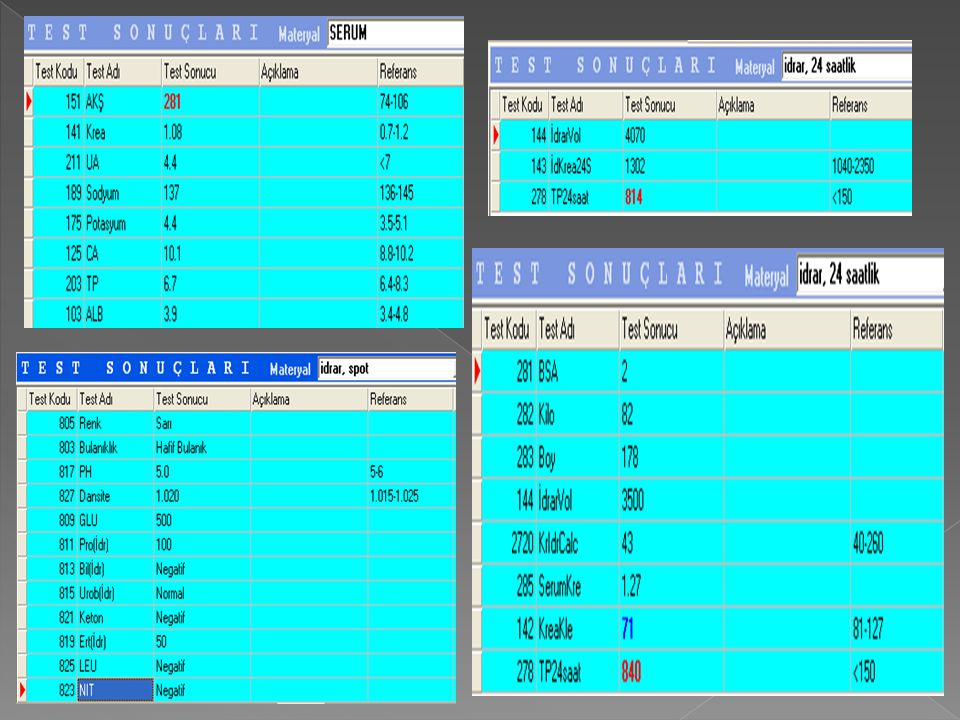
CREATİNİNE CLEARANCE Test protocol
5 ml of blood is collected for the determination of creatinine A 24-hour urine sample is collected. The collection period of the 24-h urine sample includes one daytime period and one nighttime period. The creatinine concentration is determined in the collected urine sample The clearence value is calculated. Besides the volume of urine collection, the height and body weight of the patient need to be known as well. Clearance results are related to 1.73 m2 body surface area of a person weighing 75 kg. The patient’s body surface area is derived from a nomogram, using his height and body weight. I shall review the tests in the left column today. The measurement of urine protein is important in certain conditions, e.g.diabetes. The detection of substances such as red cells or glucose could be an early indicator of renal damage.

80
Renal Function Tests- Urine volumes
Adults: 1.5 L/24 h typical in health, oliguria < 400 mL, anuria < 100 mL, polyuria > 3000 mL Urine volume depends on how much you drink and sweat. In health it is closely matched to water balance by the hormone ADH or vasopressin, AVP. We define abnormally low urine volume as a 24 hour volume less than 400 mL. This is known as oliguria. A patient is considered anuric when there is no or little urine, less than 100 mL/24 h. There is no absolute definition for polyuria as some people can drink an awful lot and match it with a high urine output. If a patient has a urine volume greater than 3 litres per day and is not drinking then this is polyuria.

81
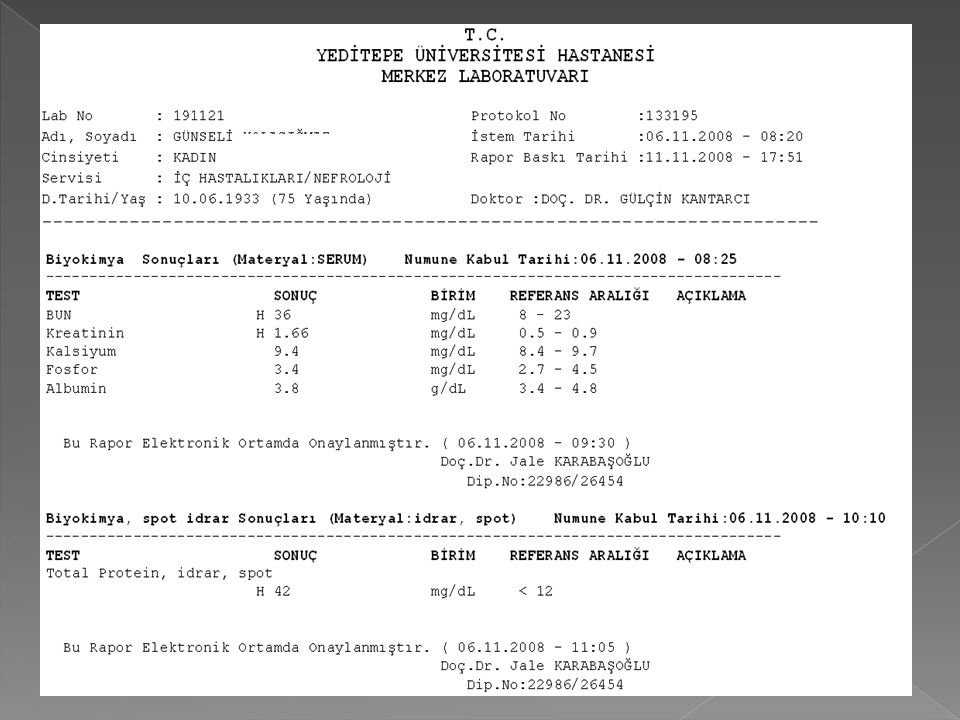
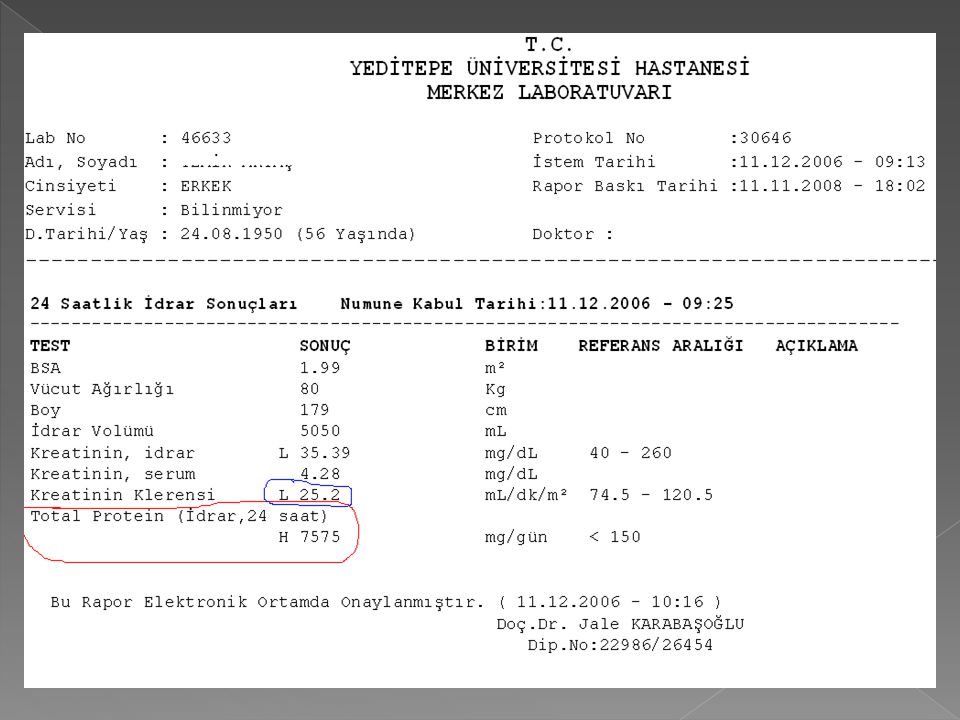
QUANTITATIVE MEASUREMENT OF PROTEINURIA
Absence of significant proteinuria is a sign of renal integrity and its presence indicates renal disease. In normal individuals the 24-hour urinary protein is less than 150 mg per day. Proteinuria could be due to: Increased glomerular filtration because of increased permeability of basement membrane Decreased reabsorption of proteins. Addition of protein to urine (renal tubular cells, lymphatics, genitalia). In Bence Jones proteinuria, there are abnormal light chains which coagulate on heating at a temperature of 45" to 55°C and redissolve on boiling.
. In Bence Jones proteinuria, there are abnormal light chains which coagulate on heating at a temperature of 45 to 55°C and redissolve on boiling.")
82
Jaffe´ reaction for measuring creatinine, simple, but better is enzymatic method
Creatinine + alkaline picrate solution Bright orange/red colored complex absorbs light at 485nm (many interfering substances in blood Can be minimized using rate method) GFR is not often measured in clinical practice. It requires a patient to come to hospital. Currently people who are considering donating a kidney whilst they are alive have their GFR measured. Before administering a drug with potentially toxic effects some patients will require a GFR measurement before the chemotherapy. This enables the oncologist to calculate the exact dose of drug after estimating its elimination rate. GFR used to be measured by calculating the clearance of inulin. Nowadays radioactive substances are used, either technetium labelled diethylenediaminetetra acetic acid DTPA or 51-chromium labelled EDTA ethylenediaminetetra acetic acid.
 GFR is not often measured in clinical practice. It requires a patient to come to hospital. Currently people who are considering donating a kidney whilst they are alive have their GFR measured. Before administering a drug with potentially toxic effects some patients will require a GFR measurement before the chemotherapy. This enables the oncologist to calculate the exact dose of drug after estimating its elimination rate. GFR used to be measured by calculating the clearance of inulin. Nowadays radioactive substances are used, either technetium labelled diethylenediaminetetra acetic acid DTPA or 51-chromium labelled EDTA ethylenediaminetetra acetic acid.")
83
Plasma b2-microglobulin
B2-microglobulin is a small peptid. İt is present on the surface of the most cells and in low concentrations in the plasma. İt is completely filtered by the glomeruli and is reabsorbed and catabolized by proximal tubular cells. Measurement of b2-microglobulin excretion provides a sensitive method of assesing tubular integrity.

84
Cystatin C This low molecular weight peptide is produced by all nucleated cells. İt is cleared from the plasma by glomerular filtration and its plasma concentration reflects the GFR.

96
Nefrotik sendrom

Benzer bir sunumlar




















 (Yrd. Doç. Dr. Deniz Dal)>")
>")
