Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Congestive Heart Failure/Treatment
Yeditepe Üniversite Hastanesi Kardiyoloji ABD

2
TREATMENT STRATEGY*

3
Treatment Objectives*
Survival Morbidity Exercise capacity Quality of life Neurohormonal changes Progression of CHF Symptoms Treatment of Heart Failure. Objectives The objectives of treatment of the patient with heart failure are many, but they may be summarized in two principles: decrease symptoms and prolong life. In daily practice, the first priority is symptom control and the best plan is to adjust to the individual patient’s particular circumstances over the course of therapy. Nevertheless, the rest of the listed objectives should not be forgotten, as medical therapy now has the potential for decreasing morbidity (hospital admissions, embolism, etc.), increasing exercise capacity (all of the usually prescribed drugs), improve the quality of life, control neurohormonal changes (ACE-I, beta blockers), retard progression (ACEI) and prolong life.
, increasing exercise capacity (all of the usually prescribed drugs), improve the quality of life, control neurohormonal changes (ACE-I, beta blockers), retard progression (ACEI) and prolong life.")
4
Treatment All Prevention. Control of risk factors Life style
Treat etiologic cause / aggravating factors Drug therapy Personal care. Team work Revascularization if ischemia causes HF ICD (Implantable Cardiac Defibrillator) Ventricular resyncronization Ventricular assist devices Heart transplant Artificial heart Neoangiogenesis, Gene therapy All Selected patients
 Ventricular resyncronization. Ventricular assist devices. Heart transplant. Artificial heart. Neoangiogenesis, Gene therapy. All. Selected patients.")
5
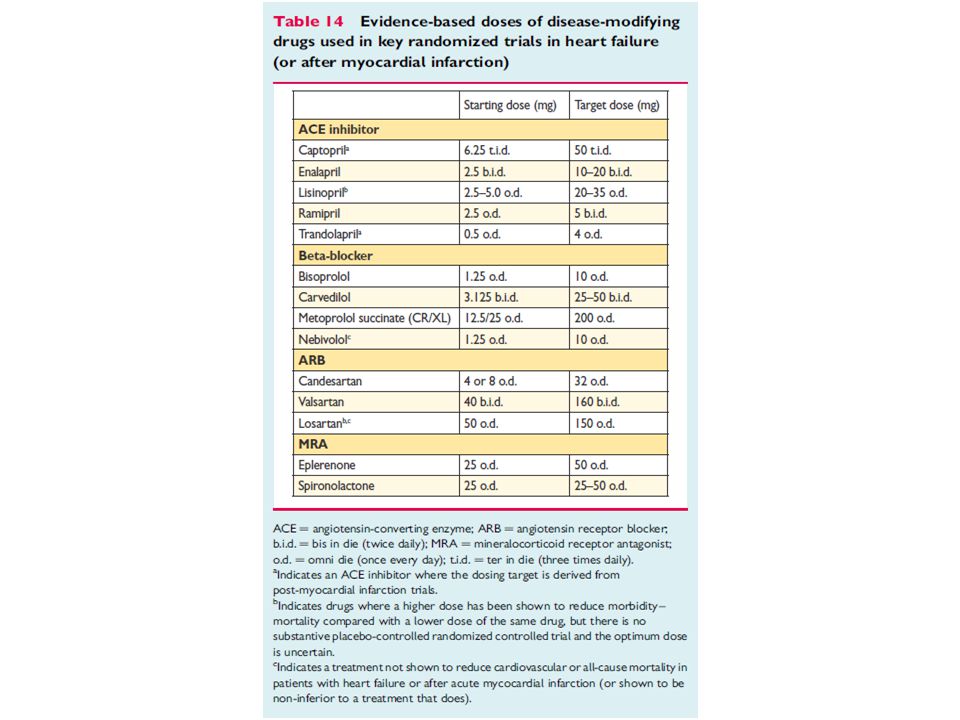
* ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; CRT-D = cardiac resynchronization therapy defibrillator; CRT-P = cardiac resynchronization therapy pacemaker; H-ISDN = hydralazine and isosorbide dinitrate; HR = heart rate; ICD = implantable cardioverter-defibrillator; LBBB = left bundle branch block; LVAD = left ventricular assist device; LVEF = left ventricular ejection fraction; MR antagonist = mineralocorticoid receptor antagonist; NYHA = New York Heart Association. a Diuretics may be used as needed to relieve the signs and symptoms of congestion (see Section 7.5) but they have not been shown to reduce hospitalization or death. b Should be titrated to evidence-based dose or maximum tolerated dose below the evidence-based dose. c Asymptomatic patients with an LVEF ≤35% and a history of myocardial infarction should be considered for an ICD. d If mineralocorticoid receptor antagonist not tolerated, an ARB may be added to an ACE inhibitor as an alternative. e European Medicines Agency has approved ivabradine for use in patients with a heart rate ≥75 b.p.m. May also be considered in patients with a contraindication to a beta-blocker or beta-blocker intolerance. f See Section 9.2 for details—indication differs according to heart rhythm, NYHA class, QRS duration, QRS morphology and LVEF. g Not indicated in NYHA class IV. h Digoxin may be used earlier to control the ventricular rate in patients with atrial fibrillation—usually in conjunction with a beta-blocker. i The combination of hydralazine and isosorbide dinitrate may also be considered earlier in patients unable to tolerate an ACE inhibitor or an ARB.
 but they have not been shown to reduce hospitalization or death. b Should be titrated to evidence-based dose or maximum tolerated dose below the evidence-based dose. c Asymptomatic patients with an LVEF ≤35% and a history of myocardial infarction should be considered for an ICD. d If mineralocorticoid receptor antagonist not tolerated, an ARB may be added to an ACE inhibitor as an alternative. e European Medicines Agency has approved ivabradine for use in patients with a heart rate ≥75 b.p.m. May also be considered in patients with a contraindication to a beta-blocker. or beta-blocker intolerance. f See Section 9.2 for details—indication differs according to heart rhythm, NYHA class, QRS duration, QRS morphology and LVEF. g Not indicated in NYHA class IV. h Digoxin may be used earlier to control the ventricular rate in patients with atrial fibrillation—usually in conjunction with a beta-blocker. i The combination of hydralazine and isosorbide dinitrate may also be considered earlier in patients unable to tolerate an ACE inhibitor or an ARB.")
6
*

7
*

8
ESSENTIALS of HF TREATMENT
* An ACE inhibitor is recommended, in addition to a beta-blocker, for all patients with an EF ≤40% to reduce the risk of HF hospitalization and the risk of premature death. A beta-blocker is recommended, in addition to an ACE inhibitor (or ARB if ACE inhibitor not tolerated), for all patients with an EF ≤40% to reduce the risk of HF hospitalization and the risk of premature death. An MRA is recommended for all patients with persisting symptoms (NYHA class II–IV) and an EF ≤35%, despite treatment with an ACE inhibitor (or an ARB if an ACE inhibitor is not tolerated) and a beta-blocker, to reduce the risk of HF hospitalization and the risk of premature death.
, for all patients with an EF ≤40% to reduce the risk of HF. hospitalization and the risk of premature death. An MRA is recommended for all patients with persisting symptoms (NYHA class II–IV) and an EF ≤35%, despite treatment with an ACE inhibitor (or an ARB if an ACE inhibitor is not tolerated) and a beta-blocker, to reduce the risk of HF hospitalization and the risk of premature death.")
10
Essential to control symptoms secondary to fluid retention
Diuretics* Essential to control symptoms secondary to fluid retention The effects of diuretics on mortality and morbidity have not been studied in patients with HF, unlike ACE inhibitors, betablockers, and MRAs (and other treatments). However, diuretics relieve dyspnoea and oedema and are recommended for this reason in patients with signs and symptoms of congestion, irrespective of EF. Loop diuretics produce a more intense and shorter diuresis than thiazides, which cause a more gentle and prolonged diuresis. Thiazides may be less effective in patients with reduced kidney function. Loop diuretics are usually preferred to thiazides in HF-REF although they act synergistically and the combination may be used (usually on a temporary basis) to treat resistant oedema. The aim of using diuretics is to achieve and maintain euvolaemia (the patient’s ‘dry weight’) with the lowest achievable dose. This means that the dose must be adjusted, particularly after restoration of dry body weight, to avoid the risk of dehydration leading to hypotension and renal dysfunction.
. However, diuretics relieve dyspnoea and oedema and are recommended for this reason in patients with signs and symptoms of congestion, irrespective of EF. Loop diuretics produce a more intense and shorter diuresis than thiazides, which cause a more gentle and prolonged diuresis. Thiazides may be less effective in patients with reduced kidney function. Loop diuretics are usually preferred to thiazides in HF-REF although they act synergistically and the combination may be used (usually on a temporary basis) to treat resistant oedema. The aim of using diuretics is to achieve and maintain euvolaemia (the patient’s ‘dry weight’) with the lowest achievable dose. This means that the dose must be adjusted, particularly after restoration of dry body weight, to avoid the risk of dehydration leading to hypotension and renal dysfunction.")
11
Diuretics Thiazides Cortex K-sparing Loop diuretics Medulla
Inhibit active exchange of Cl-Na in the cortical diluting segment of the ascending loop of Henle Cortex K-sparing Inhibit reabsorption of Na in the distal convoluted and collecting tubule Loop diuretics Treatment of heart failure. Diuretics: Classification and mechanisms of action Diuretics are drugs which eliminate Na and water by acting directly on the kidney. This category does not include other drugs with principle actions different from the diuretics, but which increase diuresis by improving heart failure or by mechanisms on the kidney which are incompletely understood. The diuretics are the primary line of therapy for the majority of patients with heart failure and pulmonary congestion. Diuretics (loop, thiazides and potassium-sparing) produce a net loss of Na and water acting directly on the kidney, decrease acute symptoms which result from fluid retention (dyspnea, edema). Diuretic drugs are classically divided into three groups: 1) thiazides, 2) loop diuretics and 3) potassium-sparing. Thiazide diuretics inhibit the active transport of Cl-Na in the cortical diluting segment of the ascending limb of the Loop of Henle. Loop diuretics inhibit the transport of Cl-Na-K in the thick portion of the ascending limb of the Loop of Henle. Potassium-sparing diuretics inhibit the reabsorption of Na in the distal convoluted and collecting tubules. Inhibit exchange of Cl-Na-K in the thick segment of the ascending loop of Henle Medulla Loop of Henle Collecting tubule
 produce a net loss of Na and water acting directly on the kidney, decrease acute symptoms which result from fluid retention (dyspnea, edema). Diuretic drugs are classically divided into three groups: 1) thiazides, 2) loop diuretics and 3) potassium-sparing. Thiazide diuretics inhibit the active transport of Cl-Na in the cortical diluting segment of the ascending limb of the Loop of Henle. Loop diuretics inhibit the transport of Cl-Na-K in the thick portion of the ascending limb of the Loop of Henle. Potassium-sparing diuretics inhibit the reabsorption of Na in the distal convoluted and collecting tubules. Inhibit exchange of Cl-Na-K in. the thick segment of the ascending. loop of Henle. Medulla. Loop of Henle. Collecting tubule.")
12
Diuretics. Indications
1. Symptomatic HF, with fluid retention Edema Dyspnea Lung Rales Jugular distension Hepatomegaly Pulmonary edema (Xray) 11
 11.")
13
Loop Diuretics / Thiazides. Practical Use
Start with variable dose. Titrate to achieve dry weight Monitor serum K+ at “frequent intervals” Reduce dose when fluid retention is controlled Teach the patient when, how to change dose Combine to overcome “resistance” Do not use alone

14
Loop diuretics. Dose (mg)
Initial Maximum Bumetanide 0.5 to 1.0mg/12-24h 10mg /day Furosemide 20 to 40mg/12-24h 400mg /day Torsemide 10 to 20mg/12-24h 200mg /day

15
Thiazides, Loop Diuretics. Adverse Effects
• K+, Mg+ ( %) (sudden death ???) • Na+ • Stimulation of neurohormonal activity • Hyperuricemia ( %) • Hypotension. Ototoxicity. Gastrointestinal. Alkalosis. Metabolic
 (sudden death ) • Na+ • Stimulation of neurohormonal activity. • Hyperuricemia ( %) • Hypotension. Ototoxicity. Gastrointestinal. Alkalosis. Metabolic.")
16
ACE-i. Mechanism of Action
VASOCONSTRICTION VASODILATATION ALDOSTERONE PROSTAGLANDINS VASOPRESSIN Kininogen tPA SYMPATHETIC Kallikrein Angiotensinogen RENIN BRADYKININ Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibitors (ACEI) :Mechanisms of action ACE-inhibitors competitively block the converting enzyme that transforms angiotensin I into angiotensin II. The reduction in angiotensin II levels explains its arteriovenous vasodilatory actions, as angiotensin II is a potent vasoconstrictor that augments sympathetic tone in the arteriovenous system. Additionally, angiotensin causes vasopressin release and produces sodium and water retention, both through a direct renal effect and through the liberation of aldosterone. Since converting enzyme has a similar structure to kinase II that degrades bradykinin, ACE-inhibitors increase kinin levels that are potent vasodilators (E2 and F2) and increase release of fibrinolytic substances such as tPA. Angiotensin I A.C.E. Inhibitor Kininase II ANGIOTENSIN II Inactive Fragments
 :Mechanisms of action. ACE-inhibitors competitively block the converting enzyme that transforms angiotensin I into angiotensin II. The reduction in angiotensin II levels explains its arteriovenous vasodilatory actions, as angiotensin II is a potent vasoconstrictor that augments sympathetic tone in the arteriovenous system. Additionally, angiotensin causes vasopressin release and produces sodium and water retention, both through a direct renal effect and through the liberation of aldosterone. Since converting enzyme has a similar structure to kinase II that degrades bradykinin, ACE-inhibitors increase kinin levels that are potent vasodilators (E2 and F2) and increase release of fibrinolytic substances such as tPA. Angiotensin I. A.C.E. Inhibitor. Kininase II. ANGIOTENSIN II. Inactive Fragments.")
17
ACE-I. Clinical Effects*
Improve symptoms Reduce remodelling / progression Reduce hospitalization Improve survival Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI): Mechanisms of action ACE-inhibitors cause arteriovenous vasodilatation. Venodilation is accompanied by reduction in PAD, PCWP, and LVEDP. Arterial vasodilatation decreases SVR and MAP and increases cardiac output, ejection fraction, and exercise tolerance. Heart rate and contractility do not change, and, thus, double product and myocardial oxygen demand are decreased. These effects are more noticeable in patients with low sodium levels, in whom there is an increased plasma renin activity. Vasodilatation is seen in various vascular territories: renal, coronary, cerebral, and musculoskeletal (increasing exercise capacity). Additionally, ACE-inhibitors cause diuretic and natriuretic effects that are a consequence of the inhibition of angiotensin II and aldosterone synthesis, as well as the increase in cardiac output and renal perfusion. It is now known that the magnitude and duration of blood pressure reduction correlates better with the activity of ACE in certain tissues (heart, vessels, kidney, adrenal, etc.) than with its plasma levels, which indicates that ACE-inhibitors act by inhibiting local tissue production of angiotensin II. Plasma levels of ACE are not good predictors of the magnitude of hemodynamic effects of ACE-inhibition.
: Mechanisms of action. ACE-inhibitors cause arteriovenous vasodilatation. Venodilation is accompanied by reduction in PAD, PCWP, and LVEDP. Arterial vasodilatation decreases SVR and MAP and increases cardiac output, ejection fraction, and exercise tolerance. Heart rate and contractility do not change, and, thus, double product and myocardial oxygen demand are decreased. These effects are more noticeable in patients with low sodium levels, in whom there is an increased plasma renin activity. Vasodilatation is seen in various vascular territories: renal, coronary, cerebral, and musculoskeletal (increasing exercise capacity). Additionally, ACE-inhibitors cause diuretic and natriuretic effects that are a consequence of the inhibition of angiotensin II and aldosterone synthesis, as well as the increase in cardiac output and renal perfusion. It is now known that the magnitude and duration of blood pressure reduction correlates better with the activity of ACE in certain tissues (heart, vessels, kidney, adrenal, etc.) than with its plasma levels, which indicates that ACE-inhibitors act by inhibiting local tissue production of angiotensin II. Plasma levels of ACE are not good predictors of the magnitude of hemodynamic effects of ACE-inhibition.")
18
Mortality Reduction with ACE-i
Study ACE-i Clinical Seting CONSENSUS Enalapril CHF SOLVD treatment Enalapril CHF AIRE Ramipril CHF Vheft-II Enalapril CHF TRACE Trandolapril CHF / LVD SAVE Captopril LVD SMILE Zofenopril High risk HOPE Ramipril High risk

19
ACE-i. Indications Symptomatic heart failure
Asymptomatic ventricular dysfunction - LVEF < % Selected high risk subgroups (CAD+HT, DM+HT with LVH) Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibits (ACEI) Indications. ACE-inhibitors probably constitute the cornerstone of drug therapy for heart failure, in that administration over time leads to amelioration of symptoms, beneficial hemodynamic changes, increased functional capacity, regression of structural changes, and, unequivocally, prolongation of survival. Thus, ACE-inhibitors are first-line therapy, not only in symptomatic heart failure patients, but also in patients with asymptomatic left ventricular dysfunction. The exact degree of ventricular dysfunction below which it is advisable to begin therapy with an ACE-inhibitor has not been defined; however, in general terms they can be helpful in patients with ejection fractions less than 35%.
 Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibits (ACEI) Indications. ACE-inhibitors probably constitute the cornerstone of drug therapy for heart failure, in that administration over time leads to amelioration of symptoms, beneficial hemodynamic changes, increased functional capacity, regression of structural changes, and, unequivocally, prolongation of survival. Thus, ACE-inhibitors are first-line therapy, not only in symptomatic heart failure patients, but also in patients with asymptomatic left ventricular dysfunction. The exact degree of ventricular dysfunction below which it is advisable to begin therapy with an ACE-inhibitor has not been defined; however, in general terms they can be helpful in patients with ejection fractions less than 35%.")
20
ACE-i Practical Use* Start with very low dose
Increase dose if well tolerated Renal function & serum K+ after 1-2 w Avoid fluid retention / hypovolemia (diuretic use) Dose NOT determined by symptoms Combine to overcome “resistance” Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI): Mechanisms of action ACE-inhibitors cause arteriovenous vasodilatation. Venodilation is accompanied by reduction in PAD, PCWP, and LVEDP. Arterial vasodilatation decreases SVR and MAP and increases cardiac output, ejection fraction, and exercise tolerance. Heart rate and contractility do not change, and, thus, double product and myocardial oxygen demand are decreased. These effects are more noticeable in patients with low sodium levels, in whom there is an increased plasma renin activity. Vasodilatation is seen in various vascular territories: renal, coronary, cerebral, and musculoskeletal (increasing exercise capacity). Additionally, ACE-inhibitors cause diuretic and natriuretic effects that are a consequence of the inhibition of angiotensin II and aldosterone synthesis, as well as the increase in cardiac output and renal perfusion. It is now known that the magnitude and duration of blood pressure reduction correlates better with the activity of ACE in certain tissues (heart, vessels, kidney, adrenal, etc.) than with its plasma levels, which indicates that ACE-inhibitors act by inhibiting local tissue production of angiotensin II. Plasma levels of ACE are not good predictors of the magnitude of hemodynamic effects of ACE-inhibition.
 Dose NOT determined by symptoms. Combine to overcome resistance Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI): Mechanisms of action. ACE-inhibitors cause arteriovenous vasodilatation. Venodilation is accompanied by reduction in PAD, PCWP, and LVEDP. Arterial vasodilatation decreases SVR and MAP and increases cardiac output, ejection fraction, and exercise tolerance. Heart rate and contractility do not change, and, thus, double product and myocardial oxygen demand are decreased. These effects are more noticeable in patients with low sodium levels, in whom there is an increased plasma renin activity. Vasodilatation is seen in various vascular territories: renal, coronary, cerebral, and musculoskeletal (increasing exercise capacity). Additionally, ACE-inhibitors cause diuretic and natriuretic effects that are a consequence of the inhibition of angiotensin II and aldosterone synthesis, as well as the increase in cardiac output and renal perfusion. It is now known that the magnitude and duration of blood pressure reduction correlates better with the activity of ACE in certain tissues (heart, vessels, kidney, adrenal, etc.) than with its plasma levels, which indicates that ACE-inhibitors act by inhibiting local tissue production of angiotensin II. Plasma levels of ACE are not good predictors of the magnitude of hemodynamic effects of ACE-inhibition.")
21
ACE-i Dose (mg) Initial Maximum Captopril 6.25 / 8h 50 / 8h
Enalapril 2.5 / 12 h 10 to 20 / 12h Fosinopril 5 to 10 / day 40 / day Lisinopril 2.5 to 5.0 / day 20 to 40 / day Quinapril 10 / 12 h 40 / 12 h Ramipril to 2.5 / day 10 / day

22
ACE-I. Adverse Effects*
Hypotension (1st dose effect) Worsening renal function Hyperkalemia Cough Angioedema Rash, ageusia, neutropenia, … Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI) : Undesirable Effects These can be classified into two groups. One group includes those effects that are inherent to its mechanism of action, and therefore are common to all ACE-inhibitors. The other includes those effects that are related to the specific chemical structure of the drug. In this case, substitution of one ACE-inhibitor for another could possibly reduce the intensity of the adverse reaction (e.g. choosing an ACE-inhibitor without a sulfhydryl moiety).
 Worsening renal function. Hyperkalemia. Cough. Angioedema. Rash, ageusia, neutropenia, … Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI) : Undesirable Effects. These can be classified into two groups. One group includes those effects that are inherent to its mechanism of action, and therefore are common to all ACE-inhibitors. The other includes those effects that are related to the specific chemical structure of the drug. In this case, substitution of one ACE-inhibitor for another could possibly reduce the intensity of the adverse reaction (e.g. choosing an ACE-inhibitor without a sulfhydryl moiety).")
23
ACE-I. Contraindications*
Intolerance (angioedema, anuric renal fail.) Bilateral renal artery stenosis Pregnancy Renal insufficiency (creatinine > 3 mg/dl) Hyperkalemia (> 5,5 mmol/l) Severe hypotension Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibitors (ACEI) Contraindications. There are few absolute contraindications for the use of ACE-inhibitors. The most important one is the presence of renal artery stenosis. The most frequent contraindication is intolerance of the drug. Hypotension, the presence of renal insufficiency, or hyperkalemia limits their use, or the ability to administer adequate doses, in up to 20% of patients.
 Bilateral renal artery stenosis. Pregnancy. Renal insufficiency (creatinine > 3 mg/dl) Hyperkalemia (> 5,5 mmol/l) Severe hypotension. Treatment of Heart Failure. Angiotensin Converting-Enzyme Inhibitors (ACEI) Contraindications. There are few absolute contraindications for the use of ACE-inhibitors. The most important one is the presence of renal artery stenosis. The most frequent contraindication is intolerance of the drug. Hypotension, the presence of renal insufficiency, or hyperkalemia limits their use, or the ability to administer adequate doses, in up to 20% of patients.")
24
ß-Adrenergic Blockers Mechanism of action*
Density of ß1 receptors Inhibit cardiotoxicity of catecholamines Neurohormonal activation HR Antiischemic Antihypertensive Antiarrhythmic Antioxidant, Antiproliferative Treatment of congestive heart failure. Possible benefits of beta adrenergic blockers The use of ß-blockers in patients with heart failure is controversial. Nevertheless, this slide lists some of the potentially beneficial effects of these drugs for patients in heart failure.

25
ß-Adrenergic Blockers Clinical Effects*
Improve symptoms (only long term) Reduce remodelling / progression Reduce hospitalization Reduce sudden death Improve survival
 Reduce remodelling / progression. Reduce hospitalization. Reduce sudden death. Improve survival.")
26
ß-Adrenergic Blockers Indications*
Symptomatic heart failure Asymptomatic ventricular dysfunction LVEF < % After AMI Treatment of Heart Failure Angiotensin Converting-Enzyme Inhibits (ACEI) Indications. ACE-inhibitors probably constitute the cornerstone of drug therapy for heart failure, in that administration over time leads to amelioration of symptoms, beneficial hemodynamic changes, increased functional capacity, regression of structural changes, and, unequivocally, prolongation of survival. Thus, ACE-inhibitors are first-line therapy, not only in symptomatic heart failure patients, but also in patients with asymptomatic left ventricular dysfunction. The exact degree of ventricular dysfunction below which it is advisable to begin therapy with an ACE-inhibitor has not been defined; however, in general terms they can be helpful in patients with ejection fractions less than 35%.
 Indications. ACE-inhibitors probably constitute the cornerstone of drug therapy for heart failure, in that administration over time leads to amelioration of symptoms, beneficial hemodynamic changes, increased functional capacity, regression of structural changes, and, unequivocally, prolongation of survival. Thus, ACE-inhibitors are first-line therapy, not only in symptomatic heart failure patients, but also in patients with asymptomatic left ventricular dysfunction. The exact degree of ventricular dysfunction below which it is advisable to begin therapy with an ACE-inhibitor has not been defined; however, in general terms they can be helpful in patients with ejection fractions less than 35%.")
27
ß-Adrenergic Blockers When to start*
Patient stable No physical evidence of fluid retention No need for i.v. inotropic drugs Start ACE-I / diuretic first No contraindications In hospital or not

28
ß-Adrenergic Blockers Dose (mg)
Initial Target Bisoprolol / 24h 10 / 24h Carvedilol / 12h 25 / 12h Metoprolol tartrate 6.25 / 12h 75 / 12h Metoprolol succinnate 12,5-25 / 24h 200 / 24h Nebivolol Start Low, Increase Slowly Increase the dose every weeks 25

29
ß-Adrenergic Blockers Adverse Effects*
Hypotension Fluid retention / worsening heart failure Fatigue Bradycardia / heart block Review treatment (+/-diuretics, other drugs) Reduce dose Consider cardiac pacing Discontinue beta blocker only in severe cases
 Reduce dose. Consider cardiac pacing. Discontinue beta blocker only in severe cases.")
30
ß-Adrenergic Blockers Contraindications*
Asthma (reactive airway disease) AV block (unless pacemaker) Symptomatic hypotension / Bradycardia Diabetes is NOT a contraindication Progressive severe PAD (relative)
 AV block (unless pacemaker) Symptomatic hypotension / Bradycardia. Diabetes is NOT a contraindication. Progressive severe PAD (relative)")
31
- Digitalis Na-K ATPase Na-Ca Exchange Na+ K+ Na+ Ca++ Ca++ K+ Na+
Treatment of heart failure. Digoxin: Mechanism of action Digoxin attaches to specific receptors which form a part of the enzyme, Na+/K+-dependent ATP-ase (sodium pump), inhibiting it. This blockade produces a progressive increase in the intracellular concentration of Na, which in turn activates the exchange of Na+-Ca++ and increases the influx of Ca++ and its intracellular concentration, [Ca++]i. This increase in the [Ca++]i at the level of the contractile proteins explains the resultant increase in cardiac contractility. Myofilaments Ca++ K+ Na+ CONTRACTILITY
, inhibiting it. This blockade produces a progressive increase in the intracellular concentration of Na, which in turn activates the exchange of Na+-Ca++ and increases the influx of Ca++ and its intracellular concentration, [Ca++]i. This increase in the [Ca++]i at the level of the contractile proteins explains the resultant increase in cardiac contractility. Myofilaments. Ca++ K+ Na+ CONTRACTILITY.")
32
Digitalis. Mechanism of Action
Blocks Na+ / K+ ATPase => Ca+ + • Inotropic effect • Natriuresis • Neurohormonal control - Plasma Noradrenaline - Peripheral nervous system activity - RAAS activity - Vagal tone - Normalizes arterial baroreceptors

33
Digitalis Clinical Effects*
Improve symptoms Modest reduction in hospitalization Does not improve survival In patients with symptomatic HF and AF, digoxin may be used to slow a rapid ventricular rate, although other treatments are preferred Digoxin may also be used in patients in sinus rhythm with symptomatic HF and an LVEF ≤40% Digoxin can cause atrial and ventricular arrhythmias, particularly in the context of hypokalaemia, and serial monitoring of serum electrolytes and renal function is mandatory

34
Digitalis. Indications*
When no adequate response to ACE-i + diuretics + beta-blockers, in combination with ACE-i + diuretics if persisting symptoms AF, to slow AV conduction Dose to mg / day

35
Digoxin. Contraindications*
Digoxin toxicity Advanced A-V block without pacemaker Bradycardia or sick sinus without PM PVC’s and VT Marked hypokalemia W-P-W with atrial fibrillation Treatment of heart failure Digoxin: Contraindications The only absolute contraindication for digoxin use is the presence of digoxin toxicity. Relative contraindications include: a) presence of advanced A-V blocks without pacemaker, as incremental blockade of conduction through the A-V node increases the risk of complete A-V block; b) ventricular extrasystoles and tachycardias, as these may be aggravated; nevertheless, digoxin may be given if the patient’s extrasystoles are secondary to heart failure; c) marked bradycardia or sinus node disease without pacemaker; d) marked, uncontrolled hypokalemia, and e) patients with Wolff-Parkinson-White syndrome and atrial fibrillation.
 presence of advanced A-V blocks without pacemaker, as incremental blockade of conduction through the A-V node increases the risk of complete A-V block; b) ventricular extrasystoles and tachycardias, as these may be aggravated; nevertheless, digoxin may be given if the patient’s extrasystoles are secondary to heart failure; c) marked bradycardia or sinus node disease without pacemaker; d) marked, uncontrolled hypokalemia, and e) patients with Wolff-Parkinson-White syndrome and atrial fibrillation.")
36
- Spironolactone Aldosterone Inhibitors ALDOSTERONE Edema Fibrosis
Competitive antagonist of the aldosterone receptor (myocardium, arterial walls, kidney) Retention Na+ Retention H2O Excretion K+ Excretion Mg2+ Collagen deposition Fibrosis - myocardium - vessels Edema Treatment of congestive heart failure. Aldosterone inhibitors: Mechanism of action Aldosterone acts directly on specific receptors. At the renal level it produces retention of sodium and water, resulting in an increase in preload and afterload, edema formation and the appearance of symptoms of pulmonary and systemic venous congestion. In addition, it increases the elimination of potassium and magnesium, creating an electrolyte imbalance which may be responsible in part for cardiac arrhythmias. At the tissue level, aldosterone stimulates the production of collagen, being in large part responsible for the fibrosis that is found in hypertrophied myocardium and in the arterial walls of patients with heart failure. The beneficial effects of spironolactone derive from the direct and competitive blockade of specific aldosterone receptors. Aldosterone inhibitors therefore have three types of effects: - Diuretic effect, which is most noticeable when fluid retention and increased levels of aldosterone are present. - Antiarrhythmic effect, mediated by the correction of hypokalemia and hypomagnesemia. - Antifibrotic effect. This effect, demonstrated in animal models, can contribute to a decrease in the progression of structural changes in patients with heart failure. Arrhythmias
 Retention Na+ Retention H2O. Excretion K+ Excretion Mg2+ Collagen. deposition. Fibrosis. - myocardium. - vessels. Edema. Treatment of congestive heart failure. Aldosterone inhibitors: Mechanism of action. Aldosterone acts directly on specific receptors. At the renal level it produces retention of sodium and water, resulting in an increase in preload and afterload, edema formation and the appearance of symptoms of pulmonary and systemic venous congestion. In addition, it increases the elimination of potassium and magnesium, creating an electrolyte imbalance which may be responsible in part for cardiac arrhythmias. At the tissue level, aldosterone stimulates the production of collagen, being in large part responsible for the fibrosis that is found in hypertrophied myocardium and in the arterial walls of patients with heart failure. The beneficial effects of spironolactone derive from the direct and competitive blockade of specific aldosterone receptors. Aldosterone inhibitors therefore have three types of effects: - Diuretic effect, which is most noticeable when fluid retention and increased levels of aldosterone are present. - Antiarrhythmic effect, mediated by the correction of hypokalemia and hypomagnesemia. - Antifibrotic effect. This effect, demonstrated in animal models, can contribute to a decrease in the progression of structural changes in patients with heart failure. Arrhythmias.")
37
Mineralocorticoid/aldosterone receptor antagonists *
Spironolactone and eplerenone block receptors that bind aldosterone and other corticosteroids, and are best characterized as MRAs.

38
Spironolactone. Practical use *
Do not use if hyperkalemia, renal insuf. Monitor serum K+ at “frequent intervals” Start ACE-i first Start with 25 mg / 24h If K+ >5.5 mmol/L, reduce to 25 mg / 48h If K+ is low or stable consider 50 mg / day New studies in progress

39
Other Drugs. (only in selected patients)*
Inotropics: refractory HF Nitrates: ischemia, angina, pulmonary congestion ARB: Contraindications to ACE-i Antiarrhythmics: (only amiodarone) H risk arrhyth. Anticoagulants: High risk of embolysm Ca channel blockers: (only amlodipine) ischemia 28
 H risk arrhyth. Anticoagulants: High risk of embolysm. Ca channel blockers: (only amlodipine) ischemia. 28.")
40
Angiotensin I ANGIOTENSIN II
Angiotensin II Receptor Blockers (ARB) RENIN Angiotensinogen Angiotensin I ANGIOTENSIN II ACE Other pathways AT1 Receptor Blockers Treatment of congestive heart failure. Angiotensin II inhibitors Angiotensin II has different effects mediated via specific receptors. There are two types of tissue receptors for angiotensin: AT1 and AT2. Stimulation of AT1 receptors has a proliferative and vasoconstrictor effect, while stimulation of AT2 receptors has the opposite effects, that is, vasodilatory and antiproliferative. In the treatment of heart failure, specific blockade of the AT1 receptors is desirable. Drugs which create a selective and competitive block of the AT1 receptors include:losartan, valsartan, irbersartan and candersartan. RECEPTORS AT1 AT2 Vasoconstriction Proliferative Action Vasodilatation Antiproliferative Action
 RENIN. Angiotensinogen. Angiotensin I ANGIOTENSIN II. ACE. Other pathways. AT1. Receptor. Blockers. Treatment of congestive heart failure. Angiotensin II inhibitors. Angiotensin II has different effects mediated via specific receptors. There are two types of tissue receptors for angiotensin: AT1 and AT2. Stimulation of AT1 receptors has a proliferative and vasoconstrictor effect, while stimulation of AT2 receptors has the opposite effects, that is, vasodilatory and antiproliferative. In the treatment of heart failure, specific blockade of the AT1 receptors is desirable. Drugs which create a selective and competitive block of the AT1 receptors include:losartan, valsartan, irbersartan and candersartan. RECEPTORS. AT1. AT2. Vasoconstriction. Proliferative. Action. Vasodilatation. Antiproliferative. Action.")
41
Angiotensin II Receptor Blockers (ARB)
Candesartan, Eprosartan, Irbesartan Losartan, Telmisartan, Valsartan Efficacy not equal / superior to ACE-I Not indicated with beta blockers Indicated in patients intolerant to ACE-I Treatment of congestive heart failure. Angiotensin II inhibitors Drugs which create a selective and competitive block of the AT1 receptors include: losartan, valsartan, irbersartan and candersartan. AHA / ACC HF guidelines 2001 ESC HF guidelines 2001

42
Vasodilators VENOUS MIXED ARTERIAL Venous Vasodilatation Nitrates
Molsidomine MIXED Calcium antagonists a-adrenergic Blockers ACE-I, ARBs K+ channel activators Nitroprusside Arterial Vasodilatation ARTERIAL Minoxidil Hydralazine

43
NITRATES HEMODYNAMIC EFFECTS
1- VENOUS VASODILATATION Preload 2- Coronary vasodilatation Myocardial perfusion 3- Arterial vasodilatation Afterload 4- Others Pulmonary congestion Ventricular size Vent. Wall stress MVO2 Treatment of Heart Failure. Nitrates: Hemodynamic effects At therapeutic doses, nitrates produce venodilatation that reduces systemic and pulmonary venous resistances. As a consequence, right atrial pressure, pulmonary capillary pressure, and LVEDP decrease. The preload reduction improves the signs of pulmonary congestion and decreases myocardial wall tension and ventricular size, which in turn reduce oxygen consumption. With higher doses, nitrates produce arterial vasodilatation that decreases peripheral vascular resistance and mean arterial pressure, leading to a decrease in afterload, and thereby reduce oxygen consumption. This arterial vasodilatation increases cardiac output, counteracting the possible reduction caused by the reduction in preload caused by venodilatation. The overall effect on cardiac output depends on the LVEDP; when LVEDP is high, nitrates increase cardiac output, while when it is normal nitrates can decrease cardiac output. Nitrates can also produce coronary vasodilatation, as much through reducing preload as through a direct effect on the vascular endothelium. This vasodilatation can decrease the mechanical compression of subendocardial vessels and increases blood flow at this level. Additionally, nitrates reduce coronary vascular tone, overcoming vasospasm. • Cardiac output • Blood pressure

44
Nitrates. Clinical Use CHF with myocardial ischemia
Orthopnea and paroxysmal nocturnal dyspnea In acute CHF and pulmonary edema:NTG sl / iv Nitrates + Hydralazine in intolerance to ACE-I (hypotension, renal insufficiency) Treatment of Heart Failure. Nitrates: Use in Heart Failure Through venodilation, nitrates reduce LVEDP, PAD, and PCWP, thereby improving pulmonary congestion and exercise tolerance. The reduction in end-diastolic pressure and volume decrease wall tension and oxygen consumption. Cardiac output and arterial pressure are not significantly changed, although a decrease in the LVEDP of 12 mmHg can decrease cardiac output. Nitrates are particularly useful in patients with signs of pulmonary congestion (PCWP > 18 mm Hg) and normal cardiac outputs, or in patients with orthopnea and PND. Recommended doses are well tolerated and rarely cause reflex tachycardia or hypotension. In patients with acute heart failure accompanied by pulmonary edema nitroglycerine can be given sublingually or i.v. I.V. administration allows for immediate onset of action, and rapid disappearance of effect within minutes of stopping the infusion. Patients receiving I.V. nitroglycerin should be monitored. In patients with low cardiac output, nitrates can be used in conjunction with arterial vasodilators, dopamine, or dobutamine. In the treatment of chronic heart failure preparations with long half-lives are used. Topical nitroglycerine and other nitrates administered qHS are effective in patients with orthopnea and PND.
 Treatment of Heart Failure. Nitrates: Use in Heart Failure. Through venodilation, nitrates reduce LVEDP, PAD, and PCWP, thereby improving pulmonary congestion and exercise tolerance. The reduction in end-diastolic pressure and volume decrease wall tension and oxygen consumption. Cardiac output and arterial pressure are not significantly changed, although a decrease in the LVEDP of 12 mmHg can decrease cardiac output. Nitrates are particularly useful in patients with signs of pulmonary congestion (PCWP > 18 mm Hg) and normal cardiac outputs, or in patients with orthopnea and PND. Recommended doses are well tolerated and rarely cause reflex tachycardia or hypotension. In patients with acute heart failure accompanied by pulmonary edema nitroglycerine can be given sublingually or i.v. I.V. administration allows for immediate onset of action, and rapid disappearance of effect within minutes of stopping the infusion. Patients receiving I.V. nitroglycerin should be monitored. In patients with low cardiac output, nitrates can be used in conjunction with arterial vasodilators, dopamine, or dobutamine. In the treatment of chronic heart failure preparations with long half-lives are used. Topical nitroglycerine and other nitrates administered qHS are effective in patients with orthopnea and PND.")
45
IVABRADIN* Ivabradine is a drug that inhibits the If channel in the sinus node. Its only known pharmacological effect is to slow the heart rate in patients in sinus rhythm (it does not slow the ventricular rate in AF). Should be considered to reduce the risk of HF hospitalization in patients in sinus rhythm with an EF ≤35%, a heart rate remaining ≥70 b.p.m., and persisting symptoms (NYHA class II–IV) despite treatment with an evidence-based dose of beta-blocker (or maximum tolerated dose below that), ACE inhibitor (or ARB), and an MRA (or ARB)
. Should be considered to reduce the risk of HF hospitalization in patients in sinus rhythm with an EF ≤35%, a heart rate remaining ≥70 b.p.m., and persisting symptoms (NYHA class II–IV) despite treatment with an evidence-based dose of beta-blocker (or maximum tolerated dose below that), ACE inhibitor (or ARB), and an MRA (or ARB)")
46
Positive Inotropes Digitalis Sympathomimetics Catecholamines
B-adrenergic agonists Phosphodiesterase inhibitors Amrinone, Milrinone, Enoximone Calcium sensitizers Levosimendan, Pimobendan Treatment of heart failure. Positive inotropic agents The use of inotropic agents in heart failure is intended to increase contractility and cardiac output to meet the metabolic needs of the body. Theoretically, their use should be greatest in heart failure associated with a decrease in systolic function and marked cardiomegaly, depression of ejection fraction and elevated left ventricular filling pressure. In addition to the cardiac glycosides, other positive inotropic agents include: a) the sympathomimetics, represented by the ß1 agonists (which stimulate cardiac contractility) and ß2-adrenergics (vasodilators). Both groups increase the intracellular concentration of cAMP by stimulating the activity of adenylate cyclase which converts ATP to cAMP; b) Phosphodiesterase inhibitors, which inhibit the enzyme that breaks down cAMP, increase cardiac contractility and have arteriovenous vasodilatory effect; c) other ionotropic drugs including glucagon and Na+ channels agonists.
 the sympathomimetics, represented by the ß1 agonists (which stimulate cardiac contractility) and ß2-adrenergics (vasodilators). Both groups increase the intracellular concentration of cAMP by stimulating the activity of adenylate cyclase which converts ATP to cAMP; b) Phosphodiesterase inhibitors, which inhibit the enzyme that breaks down cAMP, increase cardiac contractility and have arteriovenous vasodilatory effect; c) other ionotropic drugs including glucagon and Na+ channels agonists.")
47
Positive Inotropic Therapy*
May increase mortality Exception: Digoxin, Levosimendan Use only in refractory CHF NOT for use as chronic therapy Treatment of heart failure. Inotropes: General problems Positive inotropic drugs which increase cellular levels of cAMP have important proarrhythmic effects and seem to accelerate the progression of heart failure. Their hemodynamic effects decreased with prolonged treatment which suggests that they should not be used for chronic treatment. Safety and efficacy increases when they are used in low doses, with which the increase in contractility is slight. This points out that their beneficial effects probably do not depend on their positive inotropic action. The reduction in neurohumoral activation produced by digoxin and ibopamine, the antiarrhythmic action of Vesnarinone or the vasodilatory effects of dopamine, dobutamine or PDE III inhibitors may be more important than the increase in contractility that until recently was though to be their utility in the treatment of heart failure. With the exception of digoxin, chronic administration of these drugs increases mortality, so their use, in low doses, should be restricted to patients with refractory heart failure, with persistent symptoms despite treatment with combinations of other drugs. As it is precisely the sickest patients who manifest the increase in mortality, treatment with inotropic drugs is not likely to prolong the survival of these patients.

48
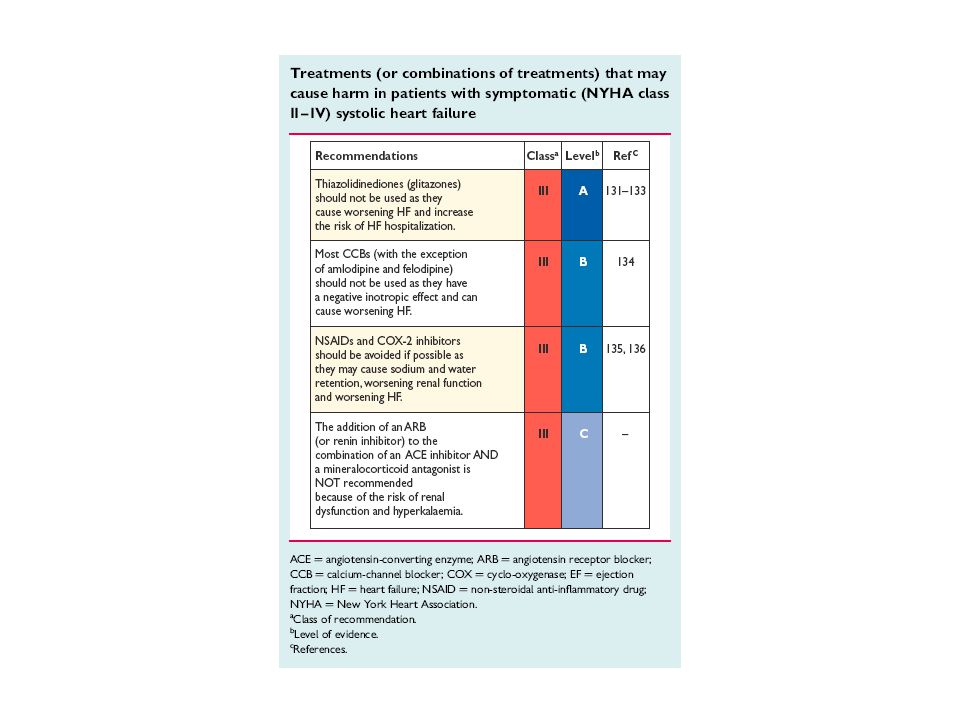
Drugs to Avoid (may increase symptoms, mortality)
Inotropes, long term / intermittent Antiarrhythmics (except amiodarone) Calcium antagonists (except amlodipine) Non-steroidal antiinflammatory drugs (NSAIDS) Tricyclic antidepressants Corticosteroids Lithium ESC HF guidelines 2001
 Calcium antagonists (except amlodipine) Non-steroidal antiinflammatory drugs (NSAIDS) Tricyclic antidepressants. Corticosteroids. Lithium. ESC HF guidelines")
50
NEW DRUGS (ongoing research)
1. New neurohormonal modulators 2. New inotropics 3. Gene therapy 4. Myocyte transplant and mitosis 5. Neoangiogenesis / Growth factors

51
Refractory End-Stage HF
Review etiology, treatment & aggrav. factors Control fluid retention Resistance to diuretics Ultrafiltration ? iv inotropics / vasodilators during decompensation Consider resynchronization Consider mechanical assist devices Consider heart transplantation

52
Heart Transplantation Indications
Refractory cardiogenic shock Documented dependence on IV inotropic support to maintain adequate organ perfusion Peak VO2 < 10 ml / kg / min Severe symptoms of ischemia not amenable to revascularization Recurrent symptomatic ventricular arrhythmias refractory to all therapeutic modalities Contraindications: age, severe comorbidity

53
Heart Failure and Myocardial Ischemia
Coronary HD is the cause of 2/3 of HF Segmental wall motion abnormalities are not specific if ischemia Angina : coronary angio and revascularization Treatment of Heart Failure. Correction of aggravating factors Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation.

54
Supraventricular Arrhythmias
Risk of embolization (AF) Anticoagulation in AF Systolic & diastolic dysfunction Digoxin, beta blockers Amiodarone if b-blocker ineffective/ contraind. Treatment of Heart Failure. Correction of aggravating factors Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation.
 Anticoagulation in AF. Systolic & diastolic dysfunction. Digoxin, beta blockers. Amiodarone if b-blocker ineffective/ contraind. Treatment of Heart Failure. Correction of aggravating factors. Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation.")
55
Ventricular Arrhythmias / Sudden Death
Antiarrhythmics ineffective (may increase mortality) Amiodarone do not improve survival ß-blockers reduce all cause mortality and SD Control ischemia Control electrolyte disturbances ICD (Implantable Cardiac Defibrillator) Treatment of Heart Failure. Correction of aggravating factors Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation.
 Amiodarone do not improve survival. ß-blockers reduce all cause mortality and SD. Control ischemia. Control electrolyte disturbances. ICD (Implantable Cardiac Defibrillator) Treatment of Heart Failure. Correction of aggravating factors. Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation.")
56
Diastolic Heart Failure/HF-PEF
Treat as HF with low LVEF Control: Hypertension Tachycardia Fluid retention Myocardial ischemia Ongoing research

57
HEART FAILURE MODELS* CONGESTIVE - Digoxin, Diurétics
HEMODYNAMIC - Vasodilators NEUROHUMORAL - ACE inhibitors, - Blockers, Spironolactone Despite advances in treatment of systolic heart failure, our pending task is diastolic heart failure that appears isolated in 40% of patients. Symptomatic treatment includes administration of nitrates and adequate doses of diuretics. Studies suggest that beta blockers (BB) and calcium channel blockers (CCB) could be beneficial in some patient subgroups. We don’t know about the effects of ACE inhibitors in these patients, although because of their antihypertensive, antiproliferative and antianginal properties could be expected to have beneficial effects. IMMUNOLOGICAL - Cytokine inhibitors
 and calcium channel blockers (CCB) could be beneficial in some patient subgroups. We don’t know about the effects of ACE inhibitors in these patients, although because of their antihypertensive, antiproliferative and antianginal properties could be expected to have beneficial effects. IMMUNOLOGICAL - Cytokine inhibitors.")
58
Neurohumoral activation
TREATMENT STRATEGIES Vasodilators Inotropics Symptom relief Diuretics Neurohumoral activation ACE-is, -blockers Spironolatone ARBs?, ANP? ET-1? Prevention of disease progression Gene therapy? Anti-remodeling strategies Reversal of HF Mann. Circulation 1999; 100:

59
TEDAVİ Genel yaklaşımlar Engelleyici tedavi
Hipertansiyonu DM ve metabolik abnormaliteleri tespit etmek ve tedavi Miyokard iskemisini uygun bir şekilde tedavi Bozulmuş ventrikül fonksiyonlarını semptomlar gelişmeden düzeltmek Optimal tedavi ile ventrikülü artmış yükten kurtarmak, duvar gerilimini azaltmak, miyokard oksijen ihtiyacını azaltmak, nörohormonal aktiviteyi düzenlemek

60
TEDAVİ Kolaylaştırıcı faktörleri tedavi etmek Aktivite ve diyet
Yaşam tarzı modifikasyonu KY septomlarını ve tedavi ihtiyacını azaltır. Orta ileri KY de geçici fiziksel aktivite kısıtlanması ve yatak istirahati Su ve tuz kısıtlaması (1.5-2 g/gün) Emosyonel stres ve psikolojik destek
 Emosyonel stres ve psikolojik destek.")
61
FARMAKOLOJİK TEDAVİ 3 ana amaç 1—preload azaltımı
Pulmoner kapiller hidrostatik basınç intertisyel mesafe ve alveol içi sıvı transudasyonu azalır 2—afterload azaltımı (sistemik vasküler direnç) KO renal perfuzyon -diurez 3—RAAS ve nörohormonal sistem inhibisyonu VasodilatasyonKO oksijen ihtiyacı İlk 2 amaç semptomatik gerileme sağlar iken RAAS ve nörohormonal vasokonstriktör inhibisyonu mortalite ve morbidite üzerine anlamlı etkileri vardır.
 KO renal perfuzyon -diurez. 3—RAAS ve nörohormonal sistem inhibisyonu. VasodilatasyonKO oksijen ihtiyacı İlk 2 amaç semptomatik gerileme sağlar iken RAAS ve nörohormonal vasokonstriktör inhibisyonu mortalite ve morbidite üzerine anlamlı etkileri vardır.")
62
FARMAKOLOJİK TEDAVİ Preload azaltımı Nitrogliserin Loop diuretikler
NTG en etkin , hızlı preload azaltımı Sublingual NTG 5 dakika içinde preload ve az afterload Topikal NTG SL kadar etkin fakat ciddi KY de cutanöz kan akımı azalmıştır IV NTG titre edilebilir hızlı Loop diuretikler Tedavinin temelini oluştururlar Frosemid en sık kullanılan, bumetanide biyoyararlanın daha yüksek ciddi KY de kullanılabilir Preloadı 2 yolla azaltırlar 1-diurez 2-pulmoner arter vasodilatasyon ve venodilatasyon

63
FARMAKOLOJİK TEDAVİ Potasyum tutucu diuretikler
Bir çok hastada diurez dk gecikebilir Diyastolik KY olgularında sıvı tutulumu daha azdır, klinik tablo düzeldikten sonra diuretikler kliniği kötüleştirebilirlerde. Potasyum tutucu diuretikler Spiranolakton, triamterene,amiloride distal renal tubule etki ederler. Distal Na tutulumu K ve H ion exchange mekanizması ile yürütülür. Hepsi aktif Na tutulumu ve K atılımını engeller—hiperkalemi riski

64
FARMAKOLOJİK TEDAVİ Morfine sulfat Dikkatle kullanılmalıdır
Solunum baskılanması, bulantı kusma Etkinliği anksiyolitik etkisinden kaynaklanmaktadır– katekolamine salınımı azalır ve sistemik resistans azalır. Hipotansif etki

65
FARMAKOLOJİK TEDAVİ ACE inhibitörleri
Afterload azaltımıatım hacmi artar KO Preload Hemodinamisi kötü hastalarda dikkat Remodelling üzerine etkili

66
FARMAKOLOJİK TEDAVİ Ang II reseptör blokerleri Hidralazine
ACE inhibitörlerini tolere edemeyen olgularda Öksürük Daha sık kullanılmakta KKY de ACE ve Ang II bloker kombinasyonu faydası klinik çalışmalarla desteklenmektedir. Hidralazine ACE öncesi en populer pre/afterload azaltıcı ajan Direkt vasodilatör Uzun etkili nitratlara kullanıldığında KKY olgularında Yaşam süresini uzattığı gösterilmiş ACE ye en üstün özelliği gebelerde kullanılabilmesidir, ACE yi tolere edemeyen olgularda kullanılır

67
Beta-blokerler Semptomları azaltır, egzersiz toleransını arttırır, kardiyak hemodinami üzerine olumlu etkileri vardır KKY de mortaliteyi azaltır Uzun dönemde kardiyak fonksiyonlarda düzelme sağlar, miyokard iskemisini azaltır,miyokard oksijen ihtiyacını azaltır Ventriküler aritmilere bağlı ani ölüm sıklığını azaltır Etkilerin görülmeye başlanması için 1-3 aylık süreç yapısal değişimler için ise 1-1,5 yıl süreç gereklidir. Tedaviye başlangıç elektif şartlarda kontraindikasyon olmayan olgularda düşük dozda uygulanır. Dekompanse olgularda klinik düzelme sağlanmadan uygulanmamalı, intoleran olgularda tedavi kesilir

68
FARMAKOLOJİK TEDAVİ İnotropik destek Digoksin
Yıllarca KKY tedaviisinin temellerini oluşturdu Mevcut tek oral inotropik ajandır Na+/K+-ATPase transport pompasını ve Na ,K hücre duvarında transferini engeller buda kalp kasının kasılma hızı ve kısalmasını artttırır (Hem sağlıklı hemde yetmezlikli kalpte, atriyal ve ventriküler kasta) Pozitif inotropik etki sitozoldeki Ca artışı nedeni iledir Sistemik vasküler direnç yada KB değiştirmez Tüm veriler kısa dönemde orta düzeyde etkin inotropik etkinlik sağlar. Tedavide entoksikasyondan kaçınmak gereklidir. Bazı ilaçlar kan seviyesini yükseltir Böbrek yetm doz ayarlaması gerekir Yaşam süresini uzatmazlar fakat hastane kalım süresini kısaltırlar. Yaşam kalitesini arttırırlar Atriyal taşiaritm tedavisinde etkindir
 Pozitif inotropik etki sitozoldeki Ca artışı nedeni iledir. Sistemik vasküler direnç yada KB değiştirmez. Tüm veriler kısa dönemde orta düzeyde etkin inotropik etkinlik sağlar. Tedavide entoksikasyondan kaçınmak gereklidir. Bazı ilaçlar kan seviyesini yükseltir. Böbrek yetm doz ayarlaması gerekir. Yaşam süresini uzatmazlar fakat hastane kalım süresini kısaltırlar. Yaşam kalitesini arttırırlar. Atriyal taşiaritm tedavisinde etkindir.")
69
FARMAKOLOJİK TEDAVİ nitroprusside
Düz kas relaksasyonu ile pre/afterload azaltımı fakat en etkin mekanizma afterload azaltımıdır Potent ve hızlı etkilidir kritik hastalarda kullanılır Afterload azaltımı sonucunda KO artar Ciddi KB düşmelerinden kaçınmak için yakın hemodinamik monitorisayyon yapmak gereklidir Uzun süreli kullanımlarda thiocyanidte toksisitesi Gebelerde fetal thiocyanidte toksisitesi

70
FARMAKOLOJİK TEDAVİ Dobutamine (sempatomimetik)
B1 reseptör agonisti (B2 ve alfa reseptör aktivitesi vardır) IV uygulamada yeterli inotropik etkinlil sağlar ve hafif kronotropik etkiside vardır Hafif periferik vasodilatasyon (afterload azaltımı) Bu etkilerinde ciddi KO artımı aluşur Dekompanse hastalarda IV formu ile IV NTG ideal tedavidir Klinik uygulamada <80 mmHg altındaki hastalarda çok dikkatli kullanılmalıdır.
 IV uygulamada yeterli inotropik etkinlil sağlar ve hafif kronotropik etkiside vardır. Hafif periferik vasodilatasyon (afterload azaltımı) Bu etkilerinde ciddi KO artımı aluşur. Dekompanse hastalarda IV formu ile IV NTG ideal tedavidir. Klinik uygulamada <80 mmHg altındaki hastalarda çok dikkatli kullanılmalıdır.")
71
FARMAKOLOJİK TEDAVİ Dopamine
Vasküler ve miyokardiyal reseptör etkileri doza bağımlıdır Etki dopaminerjik reseptör uyarılması ile gerçekleşir 0.5-3 mcg/kg/dk böbrek kan akımında artma ve diurez etkisi vardır 3-10 mcg/kg/dk miyokardta B reseptorlerini uyarır kontraktilite ve kalp hızı artar Yüksek dozlarda alfa reseptörlerde uyarılırperiferik vasokonstriksiyonkan basıncı yükselir Aritmojeniketkiye sahiptirler Miyokard oksşjen ihtiyacını artttırırlar KY de dobutamin tolere edemeyen olgularda kullanılır (ciddi hipotansiyonu olan olgular)
")
72
Fosfodiesteraz inhibitörleri
Norepinefrin Primer olarak alfa reseptörlerini uyarır Ciddi afterload artışı olur PVR artar ve KO azalır Ciddi hipotansiyonu olan olgularda Kan basıncı düzelen olgularad kesilerek diğer tedavi yöntemlerine geçilir Fosfodiesteraz inhibitörleri Hücre içi cAMP artışına—periferik vaodilatasyon, inotropik etki, pulmoner vasküler direnç azalır adrenereseptör aktiviteye ihtiyaç duymazlar Tolerans gelişmez, taşiaritmiye neden olur Oral ajanların Önemi yok hatta klas IV KKY olgularında mortaliteyi % 53 arttırmıştır Kardiyak aritmi sıklığı artmıştır

73
Diyastolik kalp yetmezliği tedavisi
2 tedavi yaklaşımı 1---diyastolik yetmezliğe neden olan durum tedavisi 2---doluş basıncını ve venöz kongesyonu zaltmak

74
Diyastolik disfonksiyon tedavisi
Perikardiyectomi—konstrktif perikardit Sistolik yüklenmenin giderilmesi ACE ve Ang II reseptörleri miyokard fibrozunu azaltır hatta geriletebilir. Anti iskemik ajanlar B-bloker, Ca kanal blokerleri, NTG Trombolitik tedavi yada primer anjiyoplasty Verapamil ventrikül gevşeme özelliğini arttırır ve hipertrofik kardiyomiyopati ve hipertansif kalp hastalıklarında etkilidir Ventriküler hipertrofinin düzeltilmesi Hipertansiyonun etkin tedavisi Aort kapak darlıklarında kapak cerrahisi

75
FARMAKOLOJİK TEDAVİ Ventrikül doluş basıncının düşürülmesi
Tuz kısıtlanması Diuretikler ve venodilatörler NTG yada uzun etkili nitratlar Normal ritmin ve hızın korunması Diyastolik yetmezliğin öncelikli olduğu olgularda digoksin kullanımının anlamı yoktur. İyi korunmuş ejeksiyon fraksiyonu olan olgularda kliniği kötüleştirebilirler.

76
FARMAKOLOJİK TEDAVİ İntraaortik balon pompası
Perkütan olarak femoral arterden retrograd ilerletilerek aort içine yerleştirilir Aort kapandıktan sonra şişip açılmadan kapanmalıdır Sistolik ve diyastolik KB üzerine etkileri vardır Afterload azaltılır—KO artarVentrıkül stresi azaltılır, Sol Vent. Hacmi küçülür Koroner kan akımı miyokard perfuzyonu artar Doluş basıncını % azaltır KO %20 artar Kesin tedavi uygulanabilinecek olgularda geçiş tedavisi olarak Kardiyojenik şok tablosundaki hastalarda kullanılır Akut kalp yetmezliklerinde hayat kurtarıcıdır

77
FARMAKOLOJİK TEDAVİ Ventriküler asist device Biventriküler Pacemaker
Transplant adayı hastalarda geçiş tedavisi Biventriküler Pacemaker Geniş QRS ve uzun PR mesafesi olan KMP li hastalarda Kardiyomyoplasti Ventrikülektomi Kalp nakli

Benzer bir sunumlar