Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Congestive Heart Failure
Yrd.Doç.Dr.Olcay ÖZVEREN Yeditepe Üniversite Hastanesi Kardiyoloji ABD

2
DEFINITION of HF Heart Failure is the clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood, or the ability to do this by increasing the end-diastolic pressure to pathologic levels Kalp yetmezliği kardiyak fonksiyonlardaki bozulma nedeni ile vücudun metabolik ihtiyacı olan kanı pompalayamaması ya da bu ihtiyacı, ventrikülün diyastol sonu basıncını normalin üstünde arttırarak yerine getirebilmesi durumudur.

3
FIGURE 21–18 The mechanical events in the cardiac cycle, first assembled by Lewis in 1920 but conceived earlier by Wiggers, in Note that mitral valve closure occurs after the crossover point of atrial and ventricular pressures at the start of systole. For explanation of phases a to g, see Table ECG = electrocardiogram; JVP = jugular venous pressure; M1 = mitral component of first sound at time of mitral valve closure; T1 = tricuspid valve closure, second component of first heart sound; AO = aortic valve opening, normally inaudible; A2 = aortic valve closure, aortic component of second sound; P2 = pulmonary component of second sound, pulmonary valve closure; MO = mitral valve opening, may be audible in mitral stenosis as the opening snap; S3 = third heart sound; S4 = fourth heart sound; a = wave produced by right atrial contraction; c = carotid wave artifact during rapid LV ejection phase; v = venous return wave, which causes pressure to rise while tricuspid valve is closed. Cycle length of 800 milliseconds for 75 beats/min. (Top panel from Opie LH: Heart Physiology: From Cell to Circulation. Lippincott Williams & Wilkins, Philadelphia, © LH Opie, 2004; bottom panel modified from Shepherd JT, Vanhoutte PM: The Human Cardiovascular System. New York, Raven Press, 1979, p 68.)
.")
5
PRELOAD/ÖNYÜK Amount of force stretching the myofibrile before contraction Maximizing preload results in Maximized stroke volume Maximized contractility FRANK-STARLING’S LAW!!!

6
FRANK-STARLING’S LAW

7
AFTERLOAD/ARTYÜK Tension on heart wall during contraction
Clinically, it is the pressure the heart must pump against to eject blood Afterload reduction reduces cardiac work Determined by peripheral vascular resistance and the cardiac chamber size

8
FIGURE 21–21 Wall stress increases as the afterload increases
FIGURE 21–21 Wall stress increases as the afterload increases. The formula shown is derived from the Laplace law. The increased left ventricular (LV) pressure in aortic stenosis is compensated for by LV wall hypertrophy, which decreases the denominator on the right side of the equation. R = radius. (From Opie LH: Heart Physiology: From Cell to Circulation. Philadelphia, Lippincott Williams & Wilkins, © LH Opie, 2004.)
 pressure in aortic stenosis is compensated for by LV wall hypertrophy, which decreases the denominator on the right side of the equation. R = radius. (From Opie LH: Heart Physiology: From Cell to Circulation. Philadelphia, Lippincott Williams & Wilkins, © LH Opie, 2004.)")
9
FIGURE 22–10 The pattern of cardiac remodeling that occurs in response to hemodynamic overloading depends on the nature of the inciting stimulus. When the overload is predominantly due to an increase in pressure (e.g., with systemic hypertension or aortic stenosis), the increase in systolic wall stress leads to the parallel addition of sarcomeres and widening of the cardiac myocytes, resulting in concentric cardiac hypertrophy. When the overload is predominantly due to an increase in ventricular volume, the increase in diastolic wall stress leads to the series addition of sarcomeres, lengthening of cardiac myocytes, and LV dilation, which is referred to as eccentric chamber hypertrophy. (From Colucci WS [ed]: Heart Failure: Cardiac Function and Dysfunction. 2nd ed. Philadelphia, Current Medicine, 1999, p 4.2.)
, the increase in systolic wall stress leads to the parallel addition of sarcomeres and widening of the cardiac myocytes, resulting in concentric cardiac hypertrophy. When the overload is predominantly due to an increase in ventricular volume, the increase in diastolic wall stress leads to the series addition of sarcomeres, lengthening of cardiac myocytes, and LV dilation, which is referred to as eccentric chamber hypertrophy. (From Colucci WS [ed]: Heart Failure: Cardiac Function and Dysfunction. 2nd ed. Philadelphia, Current Medicine, 1999, p 4.2.).")
10
FIGURE 21–23 Major determinants of the oxygen (O2) demand of the normal heart—heart rate, wall stress, and contractile function. For use of pressure-volume area as index of oxygen uptake, see Figure (Modified from Opie LH: Heart Physiology: From Cell to Circulation. Philadelphia, Lippincott Williams & Wilkins, © LH Opie, 2004.)
.")
12
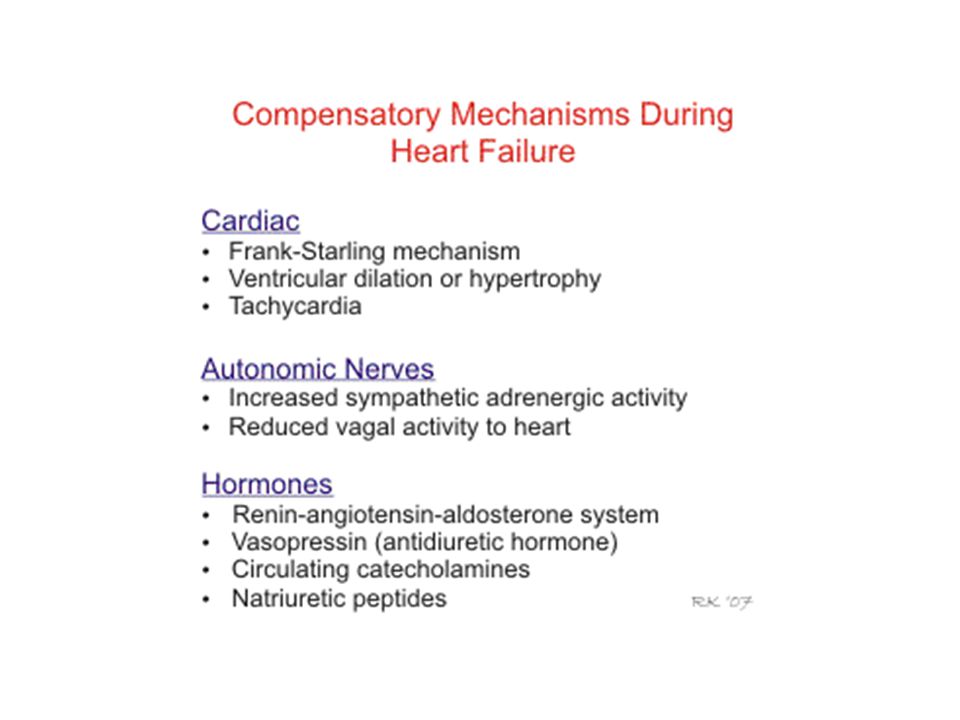
Neurohumoral responses
Neurohumoral responses include activation of sympathetic nerves and the renin-angiotensin system, and increased release of antidiuretic hormone (vasopressin) and natriuretic peptides. The net effect of these neurohumoral responses is to produce arterial vasoconstriction (to help maintain arterial pressure), venous constriction (to increase venous pressure), and increased blood volume. In general, these neurohumoral responses can be viewed as compensatory mechanisms, but they can also aggravate heart failure by increasing ventricular afterload (depresses stroke volume) and increasing preload to the point where pulmonary or systemic congestion and edema occur.
 and natriuretic peptides. The net effect of these neurohumoral responses is to produce arterial vasoconstriction (to help maintain arterial pressure), venous constriction (to increase venous pressure), and increased blood volume. In general, these neurohumoral responses can be viewed as compensatory mechanisms, but they can also aggravate heart failure by increasing ventricular afterload (depresses stroke volume) and increasing preload to the point where pulmonary or systemic congestion and edema occur.")
13
FIGURE 22–2A Mechanisms for generalized sympathetic activation and parasympathetic withdrawal in HF. A, Under normal conditions, inhibitory (−) inputs from arterial and cardiopulmonary baroreceptor afferent nerves are the principal influence on sympathetic outflow. Parasympathetic control of heart rate is also under potent arterial baroreflex control. Efferent sympathetic traffic and arterial catecholamines are low, and heart rate variability is high. B, As HF progresses, inhibitory input from arterial and cardiopulmonary receptors decreases and excitatory (+) input increases. The net response to this altered balance includes a generalized increase in sympathetic nerve traffic, blunted parasympathetic and sympathetic control of heart rate, and impairment of the reflex sympathetic regulation of vascular resistance. Anterior wall ischemia has additional excitatory effects on efferent sympathetic nerve traffic. See text for details. Ach = acetylcholine; CNS = central nervous system; E = epinephrine; Na+ = sodium; NE = norepinephrine. (From Floras JS: Alterations in the sympathetic and parasympathetic nervous system in HF. In Mann DL [ed]: Heart Failure: A Companion to Braunwald’s Heart Disease. Philadelphia, Elsevier, 2004, pp )
 inputs from arterial and cardiopulmonary baroreceptor afferent nerves are the principal influence on sympathetic outflow. Parasympathetic control of heart rate is also under potent arterial baroreflex control. Efferent sympathetic traffic and arterial catecholamines are low, and heart rate variability is high. B, As HF progresses, inhibitory input from arterial and cardiopulmonary receptors decreases and excitatory (+) input increases. The net response to this altered balance includes a generalized increase in sympathetic nerve traffic, blunted parasympathetic and sympathetic control of heart rate, and impairment of the reflex sympathetic regulation of vascular resistance. Anterior wall ischemia has additional excitatory effects on efferent sympathetic nerve traffic. See text for details. Ach = acetylcholine; CNS = central nervous system; E = epinephrine; Na+ = sodium; NE = norepinephrine. (From Floras JS: Alterations in the sympathetic and parasympathetic nervous system in HF. In Mann DL [ed]: Heart Failure: A Companion to Braunwald’s Heart Disease. Philadelphia, Elsevier, 2004, pp ).")
14
FIGURE 22–2B Mechanisms for generalized sympathetic activation and parasympathetic withdrawal in HF. A, Under normal conditions, inhibitory (−) inputs from arterial and cardiopulmonary baroreceptor afferent nerves are the principal influence on sympathetic outflow. Parasympathetic control of heart rate is also under potent arterial baroreflex control. Efferent sympathetic traffic and arterial catecholamines are low, and heart rate variability is high. B, As HF progresses, inhibitory input from arterial and cardiopulmonary receptors decreases and excitatory (+) input increases. The net response to this altered balance includes a generalized increase in sympathetic nerve traffic, blunted parasympathetic and sympathetic control of heart rate, and impairment of the reflex sympathetic regulation of vascular resistance. Anterior wall ischemia has additional excitatory effects on efferent sympathetic nerve traffic. See text for details. Ach = acetylcholine; CNS = central nervous system; E = epinephrine; Na+ = sodium; NE = norepinephrine. (From Floras JS: Alterations in the sympathetic and parasympathetic nervous system in HF. In Mann DL [ed]: Heart Failure: A Companion to Braunwald’s Heart Disease. Philadelphia, Elsevier, 2004, pp )
 inputs from arterial and cardiopulmonary baroreceptor afferent nerves are the principal influence on sympathetic outflow. Parasympathetic control of heart rate is also under potent arterial baroreflex control. Efferent sympathetic traffic and arterial catecholamines are low, and heart rate variability is high. B, As HF progresses, inhibitory input from arterial and cardiopulmonary receptors decreases and excitatory (+) input increases. The net response to this altered balance includes a generalized increase in sympathetic nerve traffic, blunted parasympathetic and sympathetic control of heart rate, and impairment of the reflex sympathetic regulation of vascular resistance. Anterior wall ischemia has additional excitatory effects on efferent sympathetic nerve traffic. See text for details. Ach = acetylcholine; CNS = central nervous system; E = epinephrine; Na+ = sodium; NE = norepinephrine. (From Floras JS: Alterations in the sympathetic and parasympathetic nervous system in HF. In Mann DL [ed]: Heart Failure: A Companion to Braunwald’s Heart Disease. Philadelphia, Elsevier, 2004, pp ).")
15
FIGURE 22–6 Unloading of high-pressure baroceptors (circles) in the left ventricle, carotid sinus, and aortic arch generates afferent signals that stimulate cardioregulatory centers in the brain, resulting in the activation of efferent pathways in the sympathetic nervous system. The sympathetic nervous system appears to be the primary integrator of the neurohumoral vasoconstrictor response to arterial underfilling. Activation of renal sympathetic nerves stimulates the release of arginine vasopressin (AVP). Sympathetic activation also causes peripheral and renal vasoconstriction, as does angiotensin II. Angiotensin II constricts blood vessels and stimulates the release of aldosterone from the adrenal gland, and it also increases tubular sodium reabsorption and causes remodeling of cardiac myocytes. Aldosterone may also have direct cardiac effects, in addition to increasing the reabsorption of sodium and the secretion of potassium and hydrogen ions in the collecting duct. The lines designate circulating hormones. (See also Chaps. 40 and 88). (Modified from Schrier RW, Abraham WT: Hormones and hemodynamics in heart failure. N Engl J Med 341:577, 1999.)
. Sympathetic activation also causes peripheral and renal vasoconstriction, as does angiotensin II. Angiotensin II constricts blood vessels and stimulates the release of aldosterone from the adrenal gland, and it also increases tubular sodium reabsorption and causes remodeling of cardiac myocytes. Aldosterone may also have direct cardiac effects, in addition to increasing the reabsorption of sodium and the secretion of potassium and hydrogen ions in the collecting duct. The lines designate circulating hormones. (See also Chaps. 40 and 88). (Modified from Schrier RW, Abraham WT: Hormones and hemodynamics in heart failure. N Engl J Med 341:577, 1999.).")
16
RAAS ACTIVITION

17
Başlangıç Adaptif Mekanizmalar ve Sonuçları
Cevap Kısa dönem etkiler Uzun dönem etkiler Su ve tuz tutulumu Preload artışı Pulmoner kongesyon,extremite ödemi, anasarca Vasokonstriksiyon KB yeterliliği sağlanır ve vital organ perfüzyonu idame edilir Afterload artışı nedeni ile kliniği kötüleştirir ve miyokard enerji ihtiyacını arttırır Sempatik sistem uyarılması KH artışı Enerji tüketimini arttırır

18
DEFINITION

19
CLASSIFICATION of HF Acute/Chronic HF Left/right sided HF
High/low output HF

20
ETIOLOGY of HF

21
Afterload : arteriel hypertension, aortic stenosis
Preload: Volume overload, AR, MR Pump failure: CAD, cardiomyopathies, arrhythmia, increased workload (infection, high-output states) FIGURE 21–23 Major determinants of the oxygen (O2) demand of the normal heart—heart rate, wall stress, and contractile function. For use of pressure-volume area as index of oxygen uptake, see Figure (Modified from Opie LH: Heart Physiology: From Cell to Circulation. Philadelphia, Lippincott Williams & Wilkins, © LH Opie, 2004.)
 FIGURE 21–23 Major determinants of the oxygen (O2) demand of the normal heart—heart rate, wall stress, and contractile function. For use of pressure-volume area as index of oxygen uptake, see Figure (Modified from Opie LH: Heart Physiology: From Cell to Circulation. Philadelphia, Lippincott Williams & Wilkins, © LH Opie, 2004.)")
22
DEFINITIONS in HF A patient who has never exhibited the typical signs or symptoms of HF is described as having asymptomatic LV systolic dysfunction Patients who have had HF for some time are often said to have ‘chronic HF’. A treated patient with symptoms and signs, which have remained generally unchanged for at least a month, is said to be ‘stable’. If chronic stable HF deteriorates, the patient may be described as ‘decompensated’ and this may happen suddenly, i.e. ‘acutely’, usually leading to hospital admission New (‘de novo’) HF may present acutely, for example as a consequence of acute myocardial infarction
 HF may present acutely, for example as a consequence of acute myocardial infarction.")
23
DEFINITIONS of FUNCTIONAL CLASSIFICATION

24
DIAGNOSIS of HEART FAILURE

26
DIAGNOSTİC TESTS in HF Transthoracic echocardiography is recommended to evaluate cardiac structure and function, including diastolic function and to measure LVEF to make the diagnosis of HF, assist in planning and monitoring of treatment, and to obtain prognostic information. A 12-lead ECG is recommended to determine heart rhythm, heart rate, QRS morphology, and QRS duration, and to detect other relevant abnormalities. This information also assists in planning treatment and is of prognostic importance. A completely normal ECG makes systolic HF unlikely (but still possible!) Measurement of blood chemistry (including sodium, potassium, calcium, urea/blood urea nitrogen, creatinine/estimated glomerular filtration rate, liver enzymes and bilirubin, ferritin/TIBC) and thyroid function is recommended to: Evaluate patient suitability for diuretic, renin–angiotensin–aldosterone antagonist, and anticoagulant therapy (and monitor treatment) (ii) Detect reversible/treatable causes of HF (e.g. hypocalcaemia, thyroid dysfunction) and co-morbidities (e.g. iron deficiency) (iii) Obtain prognostic information.
 Measurement of blood chemistry (including sodium, potassium, calcium, urea/blood urea nitrogen, creatinine/estimated glomerular filtration rate, liver enzymes and bilirubin, ferritin/TIBC) and thyroid function is recommended to: Evaluate patient suitability for diuretic, renin–angiotensin–aldosterone antagonist, and anticoagulant therapy (and monitor treatment) (ii) Detect reversible/treatable causes of HF (e.g. hypocalcaemia, thyroid dysfunction) and co-morbidities (e.g. iron deficiency) (iii) Obtain prognostic information.")
27
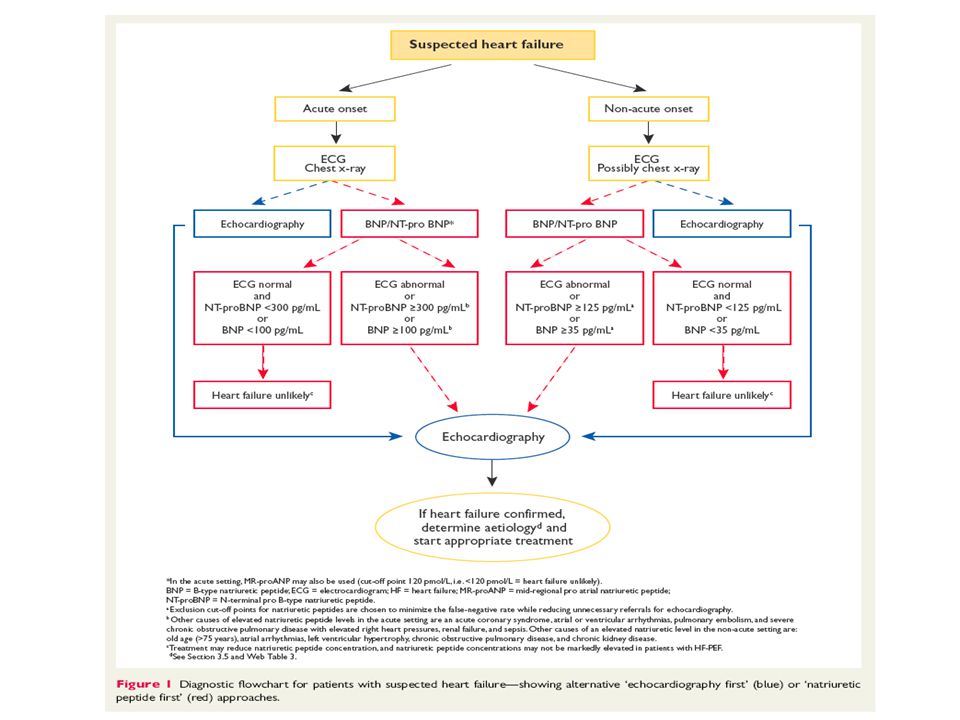
DIAGNOSTİC TESTS in HF A complete blood count is recommended to:
Detect anaemia, which may be an alternative cause of the patient’s symptoms and signs and may cause worsening of HF (ii) Obtain prognostic information. Measurement of natriuretic peptide (BNP, NT-proBNP, or MR-proANP) should be considered to: Exclude alternative causes of dyspnoea (if the level is below the exclusion cut-point HF is very unlikely) A chest radiograph (X-ray) should be considered to detect/exclude certain types of lung disease, e.g. cancer (does not exclude asthma/ COPD). It may also identify pulmonary congestion/oedema and is more useful in patients with suspected HF in the acute setting.
 Obtain prognostic information. Measurement of natriuretic peptide (BNP, NT-proBNP, or MR-proANP) should be considered to: Exclude alternative causes of dyspnoea (if the level is below the exclusion cut-point HF is very unlikely) A chest radiograph (X-ray) should be considered to detect/exclude certain types of lung disease, e.g. cancer (does not exclude asthma/ COPD). It may also identify pulmonary congestion/oedema and is more useful in patients with suspected HF in the acute setting.")
28
CMR imaging is recommended to evaluate cardiac structure and function, to measure LVEF, and to characterize cardiac tissue, especially in subjects with inadequate echocardiographic images or where the echocardiographic findings are inconclusive or incomplete (but taking account of cautions/contraindications to CMR). Coronary angiography is recommended in patients with angina pectoris, who are considered suitable for coronary revascularization, to evaluate the coronary anatomy. Myocardial perfusion/ischaemia imaging (echocardiography, CMR, SPECT, or PET) should be considered in patients thought to have CAD, and who are considered suitable for coronary revascularization, to determine whether there is reversible myocardial ischaemia and viable myocardium. Left and right heart catheterization is recommended in patients being evaluated for heart transplantation or mechanical circulatory support, to evaluate right and left heart function and pulmonary arterial resistance. Exercise testing should be considered: (i) To detect reversible myocardial ischaemia (ii) As part of the evaluation of patients for heart transplantation and mechanical circulatory support (iii) To aid in the prescription of exercise training (iv) To obtain prognostic information.
 should be considered in patients thought to have CAD, and who are considered suitable for coronary revascularization, to determine whether there is reversible myocardial ischaemia and viable myocardium. Left and right heart catheterization is recommended in patients being evaluated for heart transplantation or mechanical circulatory support, to evaluate right and left heart function and pulmonary arterial resistance. Exercise testing should be considered: (i) To detect reversible myocardial ischaemia. (ii) As part of the evaluation of patients for heart transplantation and mechanical circulatory support. (iii) To aid in the prescription of exercise training. (iv) To obtain prognostic information.")
29
AV ¼ atrioventricular; CMR ¼ cardiac magnetic resonance; CRT-P ¼ cardiac resynchronization therapy pacemaker; CRT-D ¼ cardiac resynchronization therapy defibrillator; ECG ¼ electrocardiogram; HF ¼ heart failure; ICD ¼ implantable cardioverter-defibrillator; LBBB ¼ left bundle branch block; LV ¼ left ventricular. 99mTc-DPD ¼ technetium-99m 3,3-diphosphono-1,2-propanodicarboxylic acid.

30
ACE ¼ angiotensin-converting enzyme; ARB ¼ angiotensin receptor blocker; AVP ¼ arginine vasopressin; BNP ¼ B-type natriuretic peptide; BUN ¼ blood urea nitrogen; CRP ¼ C-reactive protein; eGFR ¼ estimated glomerular filtration rate; HF ¼ heart failure; MRA ¼ mineralocorticoid receptor antagonist; NSAID ¼ non-steroidal anti-inflammatory drug.

31
ACE ¼ angiotensin-converting enzyme; ARB ¼ angiotensin receptor blocker; AVP ¼ arginine vasopressin; BNP ¼ B-type natriuretic peptide; BUN ¼ blood urea nitrogen; CRP ¼ C-reactive protein; eGFR ¼ estimated glomerular filtration rate; HF ¼ heart failure; MRA ¼ mineralocorticoid receptor antagonist; NSAID ¼ non-steroidal anti-inflammatory drug.

33
E/e’ ¼ ratio of the mitral inflow E wave to the tissue Doppler e’ wave; HF¼ heart failure; LV ¼ left ventricular; RV ¼ right ventricular; TAPSE ¼ tricuspid annular plane systolic excursion.

34
Common chest X-ray abnormalities in HF

38
KY EVRELEMESİ (yapısal)
Stage A KY için yüksek risk/Yapısal kalp hastalığı yok/KY semptomu yok Stage B Yapısal Kalp hastalığı + Kalp yetmezliği bulgusu yok Stage C Semptomatik KY Stage D Yoğun tedavi gerektiren refrakter KY

39
Classification of HF by structural abnormality,or by symptoms relating to functional Capacity (NYHA)
")
40
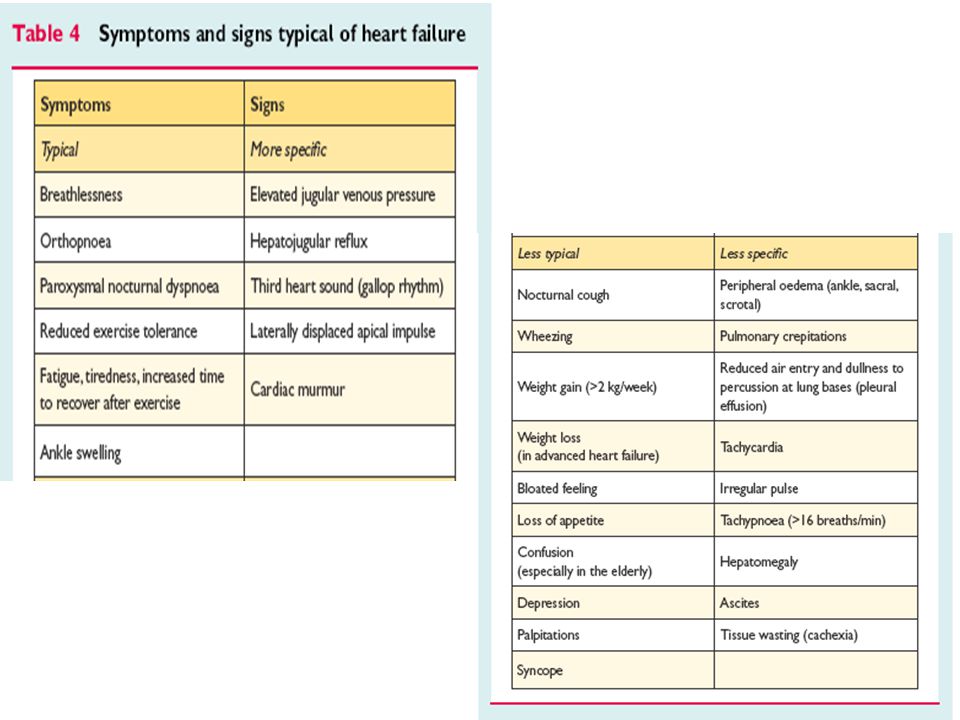
Semptom ve bulgular Nefes darlığı
Dispne yada nefes nefese kalma hali (hava açlığı hissetme) KKY nin en erken bulgusudur. Başlangıçta egzersiz ile, hastalığın ilerlediği durumlarda daha az hareket ile ortaya çıkar Bu aşamadan sonra Paroksismal nakturnal dipne ortopneistirahate ND Sol kalp Yetm.sağ kalp Yetm. Nefes darlığı yakınması azalır Sağ kalp yetmezliğinde ND yakınması nadirdir çünkü pulmoner konjesyon yoktur fakat sağ kalp yetm. KO, solunum kası hipoperfüzyonu ve hipoksi nedeni ile gelişen asidoz ND yapabilir.
 KKY nin en erken bulgusudur. Başlangıçta egzersiz ile, hastalığın ilerlediği durumlarda daha az hareket ile ortaya çıkar. Bu aşamadan sonra Paroksismal nakturnal dipne ortopneistirahate ND. Sol kalp Yetm.sağ kalp Yetm. Nefes darlığı yakınması azalır. Sağ kalp yetmezliğinde ND yakınması nadirdir çünkü pulmoner konjesyon yoktur fakat sağ kalp yetm. KO, solunum kası hipoperfüzyonu ve hipoksi nedeni ile gelişen asidoz ND yapabilir.")
41
Semptom ve bulgular Paroksismal nokturnal dispne
Bir süre sırt üstü yatıp uyuduktan sonra hasta aniden boğucu karakterde ND ile uyanır oturur yada pencere açarak yada dışarı çıkarak hava açlığını gidermeye çalışır Ortopneden önce karşılaşılır Bronkospazm yada wheezing duyulabilir (astım krizi ile karışır) Yaklaşık 30 dk sürer Nedeni infratorasik intertisyel sıvının dolaşıma katılması sırt üstü yatmakla pulmoner venöz basınç artışı (özellikle sol ventrikül diyastolik disfonksiyonunda)
 Yaklaşık 30 dk sürer. Nedeni infratorasik intertisyel sıvının dolaşıma katılması sırt üstü yatmakla pulmoner venöz basınç artışı (özellikle sol ventrikül diyastolik disfonksiyonunda)")
42
Semptom ve bulgular Ortopne Halsizlik yorgunluk
Sırtüstü yatınca oluşan oturunca geçen ND Ortopneik hasta ancak oturarak uyuyabilir yada yastık sayısını arttırırlar PND ile benzer mekanizmaya sahiptir fakat daha ileri bir klinik durumu gösterir Halsizlik yorgunluk Özellikle ektremitelerde Düşük kardiyak output, düşük kas perfüzyonu, egzersiz intoleransı Yemeklerden sonra daha fazla (kan akımı mide bağırsak sistemine yönlenir) Pulmoner konjesyon olmaksızın görülebilir. Hiponatremiye bağlı görülebilir
 Pulmoner konjesyon olmaksızın görülebilir. Hiponatremiye bağlı görülebilir.")
43
Semptom ve bulgular Nocturi/oliguri Sık ve KKY nin erken bulgularından
Su ve tuz filtrasyonu ayaktaki hastada azalır Sırtüstü yatınca venöz dönüş artar ve gün içindeki kazanılmış tuz ve su atılımı böbrek kan akımının artması ile artar idrar oluşumu artar Oliguri ciddi KKY bulgusudur son aşama klinik tabloda gözlemlenir

44
Semptom ve bulgular Serebral semptomlar
Yaşlı hastalarda konfüzyon, hafıza sorunları, anksiyete uykusuzluk,dezorientasyon, delirium, halusinasyonlar Neden ?? Serebral perfuzyon azalması

45
Semptom ve bulgular Abdominal semptomlar
Hepatik konjesyon ve karın ön duvarı ve intraabdominal organların ödemi Asit, abdominal dolgunluk, gerginlik, erken doyma, iştahsızlık gaz, kusma. Kıyafetlerin dar gelip gelmemesi bedende değişim sorgulanmalı İntestinal konjesyon Yağ absorbsiyon bozukluğu Protein kaybettirici enteropati

46
Fizik muayene Genel görünüm
Hafif KY durumunda kısa süre dinlenme ile çabuk rahatlar ve orta derecede aktivite ile belirgin yakınmaları olur Ciddi yetmezliği olan olgularda ise sırt üstü yatınca yakınmaları olur (ortopneik) Son aşamadaoturur iken de sıkıntılı ve hava açlığı içinde Yeni başlangıçlı beslenmesi iyi, kronik olgularda malnutrisyon kaşeksi Kronik sistemik venöz basınç yükselmesi sonucu exoftalmus Ciddi triküspit yetmezliği gözde ve boyun venlerinde pulsasyona neden olur Santral siyanoz, ikter, malar rash ciddi olgularda
 Son aşamadaoturur iken de sıkıntılı ve hava açlığı içinde. Yeni başlangıçlı beslenmesi iyi, kronik olgularda malnutrisyon kaşeksi. Kronik sistemik venöz basınç yükselmesi sonucu exoftalmus. Ciddi triküspit yetmezliği gözde ve boyun venlerinde pulsasyona neden olur. Santral siyanoz, ikter, malar rash ciddi olgularda.")
47
Fizik muayene Solunum sistemi Artmış adrenerjik aktivite
Çok ileri olgularda özellikle KO akut olarak düşünce sistolik kan basıncı düşer ve nabız zayıf hızlı alınır, NB/SKB oranı düşer Artmış adrenerjik aktivite Taşikardi, terleme, solukluk ve sogukluk, periferik siyanoz, periferik venlerde belirgin genişleme Solunum sistemi Dispneik görünüm Takipne Krepitan raller (Akciğer bazalinden başlar) Akciğer ödeminde ise wheezing öksürük, kanlı ve köpüklü balgam olabilir
 Akciğer ödeminde ise wheezing öksürük, kanlı ve köpüklü balgam olabilir.")
48
Fizik muayene Sistemik venöz hipertansiyon Hepatojugular reflü
Jugular ven distansiyonu Normalde JVD solunumla azalır iken KY de solunumla artar (kussmal belirtisi) Hepatojugular reflü Sağ taraflı KY olgularında Ödem (pretibial, sacral) KY kardinal bulgularından Sistemik venöz basınç ile doğru orantılı değildir Sağ ve sol KY bulgularının bulunmadığı ND bulunmadığı durumlarda gözlemlenebilir KY özgün değildir. Kronik venöz yetm, Nefrotik send, hipoproteinemi
 Hepatojugular reflü. Sağ taraflı KY olgularında. Ödem (pretibial, sacral) KY kardinal bulgularından. Sistemik venöz basınç ile doğru orantılı değildir. Sağ ve sol KY bulgularının bulunmadığı ND bulunmadığı durumlarda gözlemlenebilir KY özgün değildir. Kronik venöz yetm, Nefrotik send, hipoproteinemi.")
49
Fizik muayene Hepatomegali Hidrotoraks
Kronik sağ taraflı KY bulgusudur akut kalp yet. Bulunabilir Hızlıhassas ağrılı Ciddi TY olgularında Pulsatil hepatomegali (sağ atr “V” dalgası) Presistolik pulsasyon (“a” dalgası) tirküspit darlığı, konstriktif perikardit, restriktif KMP ve pulmoner HT Hidrotoraks Sistemik ve pulmoner hipertansiyon Genellikle bilateral Tek taraflı olursa sıklıkla sağ tutulur, dispne ciddiyeti artar.
 Presistolik pulsasyon ( a dalgası) tirküspit darlığı, konstriktif perikardit, restriktif KMP ve pulmoner HT. Hidrotoraks. Sistemik ve pulmoner hipertansiyon. Genellikle bilateral. Tek taraflı olursa sıklıkla sağ tutulur, dispne ciddiyeti artar.")
50
Fizik muayene Asit Pulsus alternans
Hepatik ven basınç artışı sonucu, uzun süreli venöz hipertansiyon + Pulsus alternans KY de SV çıkışına resistans olduğu durumlarda HT, AD, koroner atheroskleroz

51
Fizik muayene Kardiyomegali Protodiyastolik gallop (s3)
Nonspesifik bir bulgu Protodiyastolik gallop (s3) Başka nedenler olmaksızın KKY de dekompanse hastada duyulan en erken fizik muayene bulgusudur. 2.kalp sesi şiddetlenir,sistolik üfürüm P2 artması pulmoner sistolik hipertansiyon, tedavi sonrası azalır yada kaybolabilir Dekompanse KY olgularında Mitral ve trikuspit kaçak (ventriküler dilatasyon) Kardiyak kaşeksi Uzun süreli KY olgularında özellikle sağ ventrikül Yetm. Hepatik ve intestinal kongesyon ve bazen digital intoksikasyonu. Yağ emilim problemi ve protein kaybettirici enteropati Miyokard oksijen tüketim artışına sekonder metabolizma artışı, solunum işlevi artar
 Başka nedenler olmaksızın KKY de dekompanse hastada duyulan en erken fizik muayene bulgusudur. 2.kalp sesi şiddetlenir,sistolik üfürüm. P2 artması pulmoner sistolik hipertansiyon, tedavi sonrası azalır yada kaybolabilir. Dekompanse KY olgularında Mitral ve trikuspit kaçak (ventriküler dilatasyon) Kardiyak kaşeksi. Uzun süreli KY olgularında özellikle sağ ventrikül Yetm. Hepatik ve intestinal kongesyon ve bazen digital intoksikasyonu. Yağ emilim problemi ve protein kaybettirici enteropati. Miyokard oksijen tüketim artışına sekonder metabolizma artışı, solunum işlevi artar.")
52
Tanısal çalışmalar Kalp kateterizasyonu KKY etyolojisini belirlemek
KAH varlığının ve yaygınlığının değerlendirilmesi kalp kateterizasyonu ve koroner anjiyografi—özellikler girişimsel müdahaleler düşünülüyorsa

53
Karaciğer fonk testleri
Konjesyon ve kardiyak siroz hepatik fonksiyonların bozulmasına neden olur AST, ALT, LDH ve diğer enzimler yükselir Hiperbilirubinemi (direkt ve indirekt) Sarılık Akut hepatik konjesyon belirgin sarılık bil:15-20 mg/dl AST 10 kat yükselir, serum ALK-P yükselir, protrombin zamanı uzar----tablo viral hepatite benzer. TÜMÜ tedavi ile DUZELIR. uzun süreli olgularda albumin sentezi bozulur ve hipoalbuminemi görülürödem artar. K vit bağımlı koagulasyon faktör yapımı bozulur, PTZ uzar
 Sarılık. Akut hepatik konjesyon. belirgin sarılık bil:15-20 mg/dl AST 10 kat yükselir, serum ALK-P yükselir, protrombin zamanı uzar----tablo viral hepatite benzer. TÜMÜ tedavi ile DUZELIR. uzun süreli olgularda albumin sentezi bozulur ve hipoalbuminemi görülürödem artar. K vit bağımlı koagulasyon faktör yapımı bozulur, PTZ uzar.")
54
ACUTE HEART FAILURE

55
TABLE 24–1 Classification and Common Clinical Characteristics of Patients with Acute Heart Failure.

56
TABLE 24–4 Common Precipitants of Acute Heart Failure.

57
TABLE 24–5 Common Symptoms and Signs of Decompensated Heart Failure.

58
FIGURE 24–7 Hemodynamic profiles of patients presenting with advanced heart failure as described by a 2 × 2 table. Assessment of clinical symptoms and signs allows for classification of patient into a hemodynamic profile and may assist in selecting initial therapy and providing prognostic information. Although this classification scheme was developed for patients with predominantly systolic dysfunction and advanced heart failure, it provides a useful construct for the evaluation of patients with AHF as well. (Modified from Nohria A, Mielniczuk LM, Stevenson LW: Evaluation and monitoring of patients with acute heart failure syndromes. Am J Cardiol 96:32G-40G, 2005.)
.")
59
Normal sistolik fonksiyonlu KY/HFnlEF
More common in obese and women Chronic renal failure, AF, HT is more often + EF≥ %40-50 Symptoms of HF BNP high CAD +/- Often no cardiomegaly, LVH Diastolic disfunction +++

Benzer bir sunumlar