Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
YBÜ’DE SEPSİS DIŞI AKI NEDENLERİ
Doç Dr Serhan Tuğlular Marmara Üniversitesi Tıp Fakültesi Nefroloji BD

2
ABY- TANI ALGORİTMASI Prerenal Fonksiyonel ABY Intrensek renal
Hipotansiyon, ESV İlaçlar, İdrar göstergeleri Intrensek renal Organik ABY Klinik özellikler, US Normal, İdrar göstergeleri Causes of acute renal failure can be broadly divided into three categories (figure 1). In the prerenal form there is a reversible increase in serum creatinine and blood urea concentrations; it results from decreased renal perfusion, which leads to a reduction in glomerular filtration rate (GFR). Postrenal acute renal failure is due to obstruction of the urinary collection system by either intrinsic or extrinsic masses. The remaining patients have the renal form, in which structures of the nephron, such as the glomeruli, tubules, vessels, or interstitium, are affected. Postrenal Obstrüktif ABY Ağrı, Hematüri, Anüri İdrar yolu dilatasyonu
. In the prerenal form there is a reversible increase in serum creatinine and blood urea. concentrations; it results from decreased renal perfusion, which leads to a reduction in glomerular filtration rate (GFR). Postrenal acute renal failure is due to obstruction of the urinary collection system by either intrinsic or extrinsic masses. The remaining patients have the renal form, in which structures of the nephron, such as the glomeruli, tubules, vessels, or interstitium, are affected. Postrenal. Obstrüktif ABY. Ağrı, Hematüri, Anüri. İdrar yolu dilatasyonu.")
3
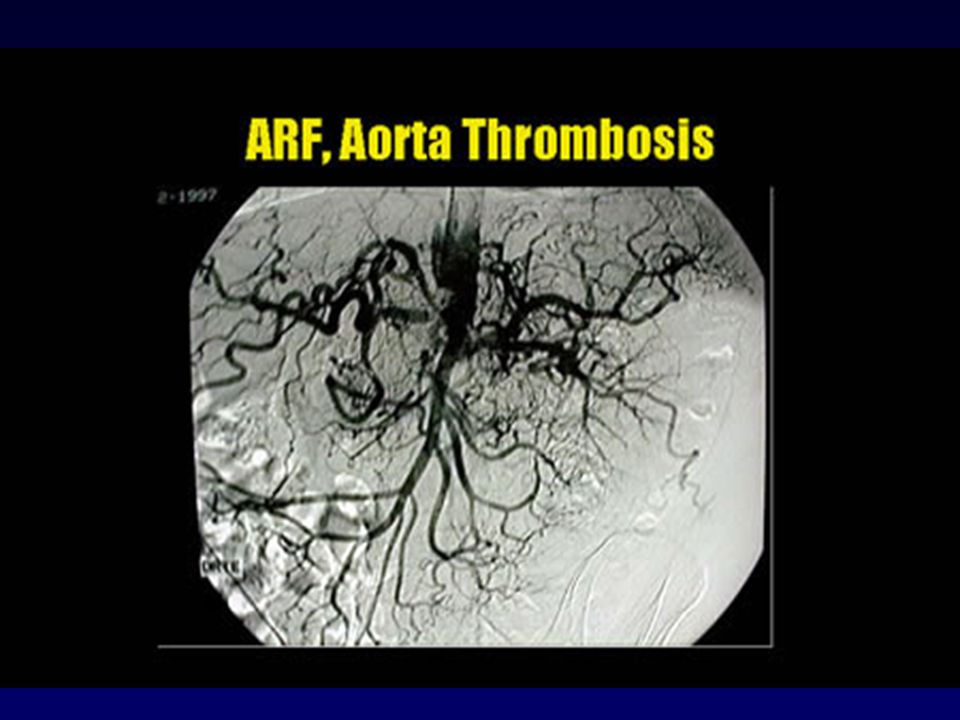
Eff Dolaşım hacminde mutlak azalma Renal arter Trombozu ya da stenozu
Prerenal ABY Eff Dolaşım hacminde mutlak azalma Kanama Volüm Eksikliği Kan Hacminde görece ↓ KKY Dekompanse KC Sirozu Renal arter Trombozu ya da stenozu Hemodinamik Tip NSAID ACEI/ARB: RAS ya da KKY’de

5
Eff Dolaşım hacminde mutlak azalma Renal arter Trombozu ya da stenozu
Prerenal ABY Eff Dolaşım hacminde mutlak azalma Kanama Volüm Eksikliği Kan Hacminde görece ↓ KKY Dekompanse KC Sirozu Renal arter Trombozu ya da stenozu Hemodinamik Tip NSAID ACEI/ARB: RAS ya da KKY’de

6
Intrensek Renal ABY Vasküler Akut tubuler nekroz
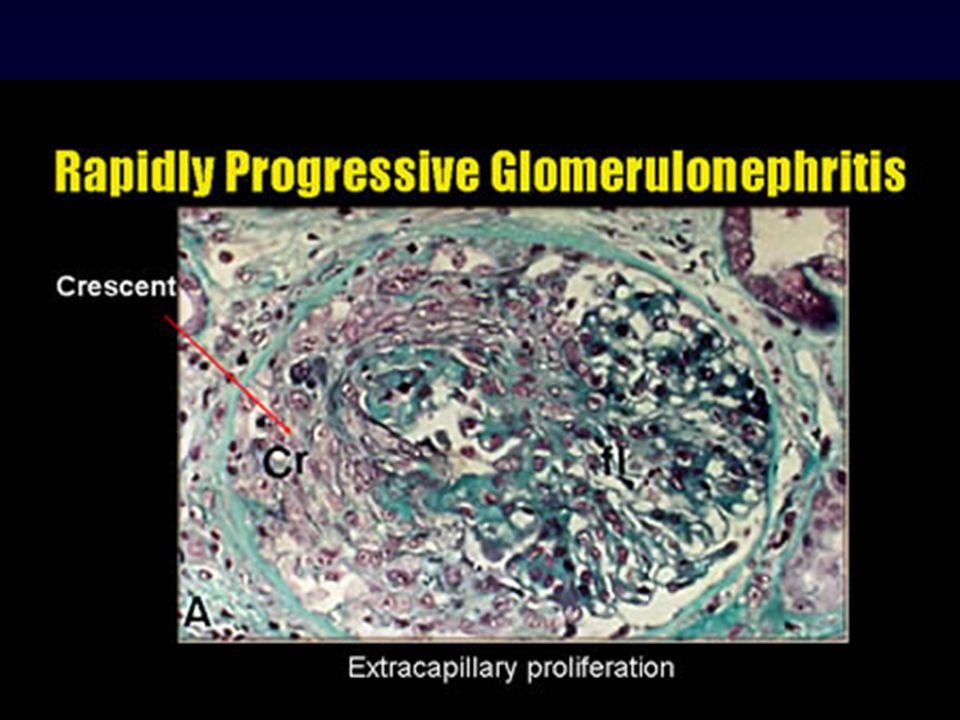
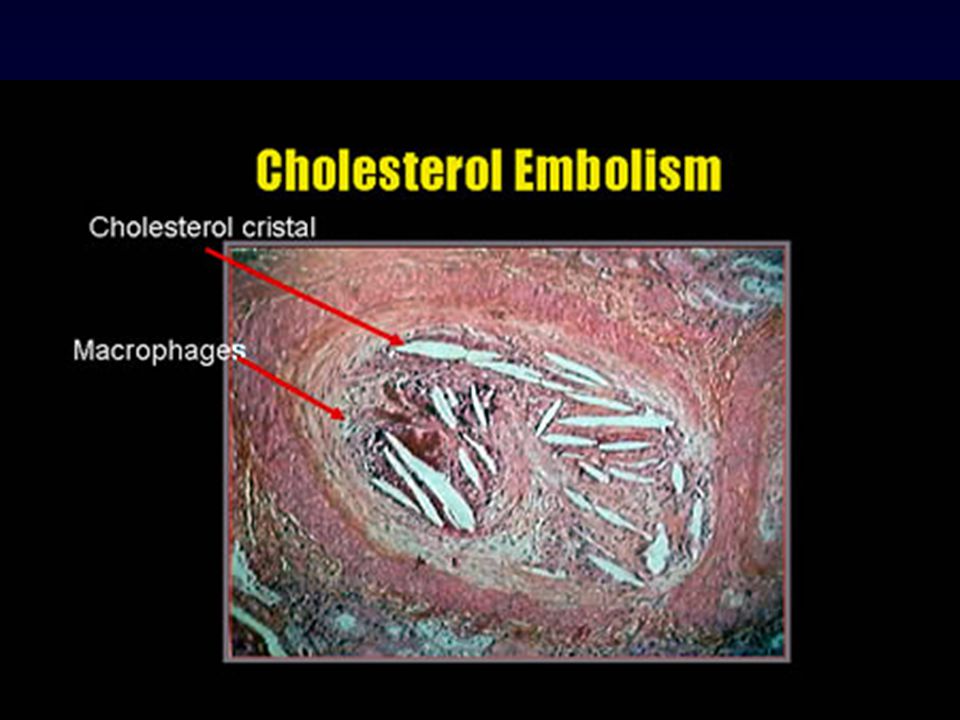
Vaskülit Malign HT Akut GN Postinfeksiyöz GN Anti GBM GN Akut Interstisyel nefrit Akut tubuler nekroz İskemik Nefrotoksik Endojen İntratubuler Pigmentler Proteinler Kristaller Ekzojen Antibiyotikler Radyokontrast Cis-platin

9
Intrensek Renal ABY Vasküler Akut tubuler nekroz
Vaskülit Malign HT Akut GN Postinfeksiyöz GN Anti GBM GN Akut Interstisyel nefrit Akut tubuler nekroz İskemik/Hemodinamik Nefrotoksik Hipoperfüzyon Hepatorenal S İntrabd. Komprt.S Endojen İntratubuler Pigmentler Proteinler Kristaller Ekzojen Antibiyotikler Radyokontrast Cis-platin

10
(%17) (%72) N=253 Kidney Int 1998;53: S16-S24
 (%72) N=253 Kidney Int 1998;53: S16-S24")
11
GFR Düşmeden BUN ve Kreatinin Yükselme Nedenleri
Üre sentezinde GİS kanama Kortikosteroidler Tetrasiklin Protein alımında artış Amino asit uygulanması Katabolizmada artış ve ateşli hastalık Kreatinin yapımında Rabdomiyoliz Tubuler Kr sekresyonunda Cimetidine Trimethoprim

12
RADYOKONTRAST NEFROPATİSİ (1)
Kontrasttan saat sonra Kr ↑ Kr günde zirve yapar 7-10. günde bazale geri döner Çoğunlukla nonoligurik İdrar analizi: granüler silendirler, tubuler epitel hücreleri, minimal proteinüri FE Na ↓ Patients with CN typically present with an acute rise in serum creatinine anywhere from 24 to 48 h after the contrast study. Serum creatinine generally peaks at 3 to 5 d and returns to baseline value by 7 to 10 d (2– 4). The acute renal failure is nonoliguric in most cases (5,6). Urinalysis often reveals granular casts, tubular epithelial cells, and minimal proteinuria, but in many cases may be entirely bland. Most, but not all, patients exhibit low fractional excretion of sodium (5,7). The diagnosis of CN is frequently obvious if the typical course of events follows the administration of contrast.
. The acute renal failure is nonoliguric in most cases (5,6). Urinalysis often reveals granular casts, tubular epithelial cells, and minimal proteinuria, but in many cases may be entirely bland. Most, but not all, patients exhibit low fractional excretion of sodium (5,7). The diagnosis of CN is frequently obvious if the typical course of events follows the administration of contrast.")
13
Doğrudan hücresel toksisite
RKN: PATOGENEZ Doğrudan hücresel toksisite Renal Medüller iskemi CN appears to be the result of a synergistic combination of direct renal tubular epithelial cell toxicity and renal medullary ischemia (8). Direct cytotoxicity in CN is suggested by histologic changes of cell injury and enzymuria after contrast administration (9). The nature of the contrast, associated ions, concentration, and concomitant hypoxia are all important to the degree of cellular damage, while the osmolality of the solution seems to be of secondary importance (8). The injection of contrast induces a biphasic hemodynamic change in the kidney, with an initial, transient increase and then a more prolonged decrease in renal blood flow (2). The mediators of these changes are still unknown. Alterations in the metabolism of prostaglandin, nitric oxide, endothelin, or adenosine may play a role. Kontrastın tipi Eşlik eden hipoksi Risk faktörleri
. Direct cytotoxicity in CN is suggested by histologic changes of cell injury and enzymuria after contrast administration (9). The nature of the contrast, associated ions, concentration, and concomitant hypoxia are all important to the degree of cellular damage, while the osmolality of the solution seems to be of secondary importance (8). The injection of contrast induces a biphasic hemodynamic change in the kidney, with an initial, transient increase and then a more prolonged decrease in renal blood flow (2). The mediators of these changes are still unknown. Alterations in the metabolism of prostaglandin, nitric oxide, endothelin, or adenosine may play a role. Kontrastın tipi. Eşlik eden hipoksi. Risk faktörleri.")
14
RKN: RİSK FAKTÖRLERİ Önceden varolan BY >2ml/kg kontrast dozu
Diyabetes Mellitus Effektif arteriyel volümde↓ KKY Dehidratasyon Nefrotik sendrom Siroz >2ml/kg kontrast dozu Yaş>60 Eş zamanlı nefrotoksik ilaç: NSAID ACEI/ARB Preexisting renal impairment Diabetes mellitus Decrease in effective arterial volume congestive heart failure dehydration nephrosis cirrhosis High doses of contrast Concurrent use of nephrotoxic drugs nonsteroidal anti-inflammatory drugs angiotensin-converting enzyme inhibitors

15
ALINMASI GEREKLİ ÖNLEMLER
RKN ALINMASI GEREKLİ ÖNLEMLER Gerekliliğinin sorgulanması Öncesinde Kr. Kontolü Non-Nefrotoksik ajan tercihi Kontrast dozu YETERLİ HİDRASYON : %0.45 SF → 1ml/kg/saat 1-2 saat öncesinden 24 saat sonrasına kadar A reasonable starting protocol might use intravenous 0.45% saline at a rate of 1 ml/kg per h, beginning 1 to2 h before contrast and continuing for up to 24 h, depending on the duration of the attendant diuresis. The protocol should be flexible to allow an increase in rate if a negative fluid balance seems to be developing.

16
ALINABİLECEK ÖNLEMLER
RKN: ALINABİLECEK ÖNLEMLER Oral theophylline (5mg/kg) 1 saat öncesinden-48 saat > N-acetylcystein (600mg; 2x1) 1 gün öncesinden-48 saat > Ca Kanal blokerleri İdrarın alkalinizasyonu These studies suggest that theophylline prevents some of the contrast-associated changes in renal function, but a benefit over saline hydration alone has not been convincingly demonstrated. This is particularly true with respect to patients with preexisting renal impairment. Nevertheless, there may be some value to the use of theophylline for reduction of CN in those at risk. Although the dose, duration, and route of administration of theophylline differed in each study, it seems likely that a dose of ,5 mg/kg for less than 2 d, starting before contrast, would suffice. The Renal Insufficiency Following Contrast Media Administration Trial (REMEDIAL) was a randomized trial comparing 3 strategies for the prevention of contrast-induced AKI in patients with CKD (as defined by a serum creatinine 2.0 mg/dL [177 mol/L] or eGFR 40 mL/min/1.73 m2 [0.67 mL/s/1.73 m2]) undergoing coronary or peripheral angiography and/or angioplasty.6 Patient were randomly assigned to prophylactic administration of either (1) intravenous 0.9% normal saline (1
 1 saat öncesinden-48 saat > N-acetylcystein (600mg; 2x1) 1 gün öncesinden-48 saat > Ca Kanal blokerleri. İdrarın alkalinizasyonu. These studies suggest that theophylline prevents some of the contrast-associated changes in renal function, but a benefit over saline hydration alone has not been convincingly demonstrated. This is particularly true with respect to patients with preexisting renal impairment. Nevertheless, there may be some. value to the use of theophylline for reduction of CN in those at risk. Although the dose, duration, and route of administration of theophylline differed in each study, it seems likely that a dose of ,5 mg/kg for less than 2 d, starting before contrast, would suffice. The Renal Insufficiency Following Contrast. Media Administration Trial (REMEDIAL) was a randomized trial comparing 3 strategies for the prevention of contrast-induced AKI in patients with CKD (as defined by a serum creatinine 2.0 mg/dL [177 mol/L] or eGFR 40 mL/min/1.73 m2 [0.67 mL/s/1.73 m2]) undergoing coronary or peripheral angiography and/or angioplasty.6 Patient were randomly assigned to prophylactic administration of either (1) intravenous 0.9% normal saline (1.")
17
iv NaH2CO3+%5 Dx 3mL/kg/saat
RKN- REMEDİAL (Renal Insufficiency Following Contrast Media Administration Trial) AKI iv SF 1mL/kg/saat <12 saat> NAC 1200mg 2x1 %9.9 iv NaH2CO3+%5 Dx 3mL/kg/saat <1 saat 1mL/kg/saat 6 saat NAC 1200mg 2x1 %1.9 The Renal Insufficiency Following Contrast Media Administration Trial (REMEDIAL) was a randomized trial comparing 3 strategies for the prevention of contrast-induced AKI in patients with CKD (as defined by a serum creatinine 2.0 mg/dL [177 mol/L] or eGFR 40 mL/min/1.73 m2 [0.67 mL/s/1.73 m2]) undergoing coronary or peripheral angiography and/or angioplasty.6 Patient were randomly assigned to prophylactic administration of either (1) intravenous 0.9% normal saline (1mL/kg/h for 12 hours before and 12 hours after the procedure) plus NAC (1,200 mg orally twice daily before and after) (n 111); (2) intravenous sodium bicarbonate (154 mEq/L [154 mmol/L] in dextrose and H2O, 3 mL/kg bolus for 1 hour before and 1 mL/kg/h for 6 hours after the procedure) plus NAC (as above) (n 108); or (3) normal saline (as above) plus ascorbic acid (3 g intravenously before and 2 g intravenously for 2 doses afterwards) plus NAC (as above) (n 107). Based on this definition, AKI developed in 11 of 111 patients (9.9%) in the saline plus NAC group, in 2 of 108 (1.9%) in the bicarbonate plus NAC group (P v saline plus NAC), and in 11 of 107 (10.3%) in the saline plus ascorbic acid plus NAC group (P v saline plus NAC group). Ascorbic asit 3giv –önce 2giv-sonra x2 iv SF 1mL/kg/saat <12 saat> %10.3
 AKI. iv SF 1mL/kg/saat. <12 saat> NAC 1200mg 2x1. %9.9. iv NaH2CO3+%5 Dx 3mL/kg/saat. <1 saat. 1mL/kg/saat. 6 saat. NAC 1200mg 2x1. %1.9. The Renal Insufficiency Following Contrast Media Administration Trial (REMEDIAL) was a randomized trial comparing 3 strategies for. the prevention of contrast-induced AKI in patients with CKD (as defined by a serum creatinine 2.0 mg/dL [177 mol/L] or eGFR 40 mL/min/1.73 m2 [0.67 mL/s/1.73 m2]) undergoing coronary or peripheral angiography and/or angioplasty.6 Patient were randomly assigned to prophylactic administration of either (1) intravenous 0.9% normal saline (1mL/kg/h for 12 hours before and 12 hours after the procedure) plus NAC (1,200 mg orally twice daily before and after) (n 111); (2) intravenous sodium bicarbonate (154 mEq/L [154 mmol/L] in dextrose and H2O, 3 mL/kg bolus for 1 hour before and 1 mL/kg/h for 6 hours after the procedure) plus NAC (as above) (n 108); or (3) normal saline (as above) plus ascorbic acid (3 g intravenously before and 2 g intravenously for 2 doses afterwards) plus NAC (as above) (n 107). Based on this. definition, AKI developed in 11 of 111 patients (9.9%) in the saline plus NAC group, in 2 of 108 (1.9%) in the bicarbonate plus NAC group. (P 0.02 v saline plus NAC), and in 11 of 107 (10.3%) in the saline plus ascorbic acid plus. NAC group (P 1.00 v saline plus NAC group). Ascorbic asit. 3giv –önce. 2giv-sonra x2. iv SF 1mL/kg/saat. <12 saat> %10.3.")
18
RKN: EPİDEMİYOLOJİK BİLGİLER
Hastanede yatan hastalarda 3.sık ABY nedeni Olguların %7’si geçici diyaliz ya da SDBY Hastanede yatış süresini ve maliyeti ↑ Ölüm riskini ↑ Acute radiocontrast nephropathy is the third most common cause of acute renal failure in patients admitted to a hospital (1). Up to 7% of patients with this condition need temporary dialysis or progress to end-stage renal disease (2). Radiocontrast nephropathy does not only cause extended hospitalization and increased cost (3), but is also associated with an increased risk of death
. Up to 7% of patients with this. condition need temporary dialysis or progress to end-stage renal disease (2). Radiocontrast nephropathy does not only cause extended hospitalization and increased cost (3), but is also associated with an increased risk of death.")
19
Contrast- Induced Nephropathy (CIN) ConsensusWorking Panel: Executive Summary.
Rev Cardiovasc Med 7: , 2006 Consensus Statement 1 Patients and clinicians should be aware that contrast-induced AKI is a common and potentially serious complication following the administration of contrast media in patients at risk for AKI. Consensus Statement 2 The risk of contrast-induced AKI is elevated and of clinical importance in patients with CKD (particularly when diabetes is also present), recognized by an eGFR of less than 60 mL/min/1.73 m2. Consensus Statement 3 When serum creatinine or estimated glomerular filtration rate is unavailable, then a medical history (inquiring about risk factors for CKD) may be used to identify patients at higher risk for contrast-induced AKI than the general population. Consensus Statement 4 In the setting of emergency procedures, where the benefit of very early imaging outweighs the risk of waiting, the procedure can be performed without knowledge of serum creatinine or eGFR. Consensus Statement 5 Clinicians should recognize the presence of multiple contrast-induced AKI risk factors in the same patient or high-risk clinical scenarios can create a very high risk (approximately 50%) for contrast-induced AKI and (approximately 15%) for need for dialysis after contrast exposure. Consensus Statement 6 In patients at increased risk for contrast-induced AKI undergoing intra-arterial administration of contrast, nonionic, isoosmolar contrast (iodixanol) is associated with the lowest risk of contrast-induced AKI. Consensus Statement 7 Iodinated contrast volumes should be minimized. Higher contrast volumes (100 mL) are associated with higher rates of contrast-induced AKI in patients at risk. However, even small (approximately 30 mL) volumes of iodinated contrast in very high-risk patients can cause contrast-induced AKI and need for dialysis, suggesting the absence of a threshold effect. Consensus Statement 8 Intra-arterial administration of iodinated contrast appears to pose a greater risk of contrast-induced AKI above that with intravenous administration, thus when possible, intravenous studies are preferred. Consensus Statement 9 Adequate intravenous volume expansion with isotonic crystalloid ( mL/kg/h) for 3 to 12 hours before the procedure and continued for 6 to 24 hours afterwards can lessen the probability of contrast-induced AKI in patients at risk. Consensus Statement 10 No adjunctive medical or mechanical treatment has been proven to be effective in reducing the risk of AKI after exposure to iodinated contrast. Hence use of a prophylactic agent is at the discretion of the treating physician. Prophylactic hemodialysis or hemofiltration has not been validated as an effective strategy.
, recognized by an eGFR of less than 60 mL/min/1.73 m2. Consensus Statement 3. When serum creatinine or estimated glomerular filtration rate is unavailable, then a medical history (inquiring about risk. factors for CKD) may be used to identify patients at higher risk for contrast-induced AKI than the general population. Consensus Statement 4. In the setting of emergency procedures, where the benefit of very early imaging outweighs the risk of waiting, the. procedure can be performed without knowledge of serum creatinine or eGFR. Consensus Statement 5. Clinicians should recognize the presence of multiple contrast-induced AKI risk factors in the same patient or high-risk. clinical scenarios can create a very high risk (approximately 50%) for contrast-induced AKI and (approximately 15%) for. need for dialysis after contrast exposure. Consensus Statement 6. In patients at increased risk for contrast-induced AKI undergoing intra-arterial administration of contrast, nonionic, isoosmolar. contrast (iodixanol) is associated with the lowest risk of contrast-induced AKI. Consensus Statement 7. Iodinated contrast volumes should be minimized. Higher contrast volumes (100 mL) are associated with higher rates of. contrast-induced AKI in patients at risk. However, even small (approximately 30 mL) volumes of iodinated contrast in. very high-risk patients can cause contrast-induced AKI and need for dialysis, suggesting the absence of a threshold. effect. Consensus Statement 8. Intra-arterial administration of iodinated contrast appears to pose a greater risk of contrast-induced AKI above that with. intravenous administration, thus when possible, intravenous studies are preferred. Consensus Statement 9. Adequate intravenous volume expansion with isotonic crystalloid ( mL/kg/h) for 3 to 12 hours before the procedure. and continued for 6 to 24 hours afterwards can lessen the probability of contrast-induced AKI in patients at risk. Consensus Statement 10. No adjunctive medical or mechanical treatment has been proven to be effective in reducing the risk of AKI after exposure. to iodinated contrast. Hence use of a prophylactic agent is at the discretion of the treating physician. Prophylactic. hemodialysis or hemofiltration has not been validated as an effective strategy.")
20
İLACA İKİNCİL ABY Akut Tubuler Hasar Otoregülasyon bozukluğu
Aminoglikozidler Bazı sefalosporinler Amfoterisin B Otoregülasyon bozukluğu ACE inhibitörleri AII reseptör blokerleri NSAID Radyokontrast ajanlar Akut Interstisyel nefrit Tüm ilaçlar

21
İlaç Dozunun Ayarlanması
İdrar çıkışı <400ml/gün ise, serum kreatinin değeri ne olursa olsun, klirens <10ml/dk >60 yaşta klirens 10-50ml/dk OLARAK KABUL EDİLMELİDİR YÜKLEME DOZU DEĞİŞMEZ İDAME DOZU: DOZ AZALTILABİLİR DOZ ARASI UZATILABİLİR

22
HEPATORENAL SENDROM

23
HEPATORENAL SENDROM TANI KRİTERLERİ
MAJÖR KRİTERLER 1-Scr >1.5 mg/dl ve/veya GFR <40 ml/dk 2-Şok, Bakteriyel infeksiyon, sıvı kaybı ve nefrotoksik ilaç kullanımı olmaması 3-1,5 L sıvı verilmesine / diüretiklerin Kesilmesine rağmen Scr’nin düşmemesi EK KRİTERLER İdrar volümü <500ml/gün İdrar Na <10 mEq/L İdrar osm>plasma osm Hematüri <50/HPF Serum Na <130mEq/L

24
HRS’A YAKLAŞIM Oluşumunu tetikleyen faktörlerden kaçınmak /varsa tedavisi Renal doz dopamin Terlipressin + albumin Ornipressin + albumin TIPS Tx planlanıyorsa DESTEK

25
INTRA-ABDOMİNAL HYPERTENSION & COMPARTMENT SYNDROME
IAHT: Batın içi basınçta artış ACS: IAHT’a ikincil organ disfonksiyonu “Intra-abdominal hypertension”, the presence of elevated intra-abdominal pressure, and “abdominal compartment syndrome”, the development of pressure-induced organ-dysfunction and failure, have been increasingly recognized over the past decade as causes of significant morbidity and mortality among critically ill surgical and medical patients. Although initially recognized over 150 years ago, the pathophysiologic implications of elevated intraabdominal pressure (IAP) have essentially been rediscovered only within the past two decades [1-3]. An explosion of scientific investigation and accumulation of clinical experience has confirmed the significant detrimental impact of both “intra-abdominal hypertension” (IAH) (see figure 1), the presence of elevated intra-abdominal pressure, and “abdominal compartment syndrome” (ACS), the development of IAH-induced organ-dysfunction and failure, among the critically ill [4,5]. Mortalite ↑ Morbiditeyi ↑
 have essentially been rediscovered only within the past two decades [1-3]. An explosion of scientific investigation and accumulation of clinical experience has confirmed the. significant detrimental impact of both intra-abdominal hypertension (IAH) (see figure 1), the. presence of elevated intra-abdominal pressure, and abdominal compartment syndrome (ACS), the. development of IAH-induced organ-dysfunction and failure, among the critically ill [4,5]. Mortalite ↑ Morbiditeyi ↑")
26
IAH ve ACS ve BÖBREK Renal kan akımı ve fonksiyon↓
IAP >15 mmHg Oliguri IAP > 30 mmHg Anuri Renal arteryel kan akımı ↓ Renal ven basıncı ve RVR↑ Renal Kortexte kan akımı↓ Glomeruler ve tubuler fonksiyon ↓ IAH-induced reductions in renal blood flow and function have been demonstrated in both animal and human models [33,35,42,51,77]. These changes occur in direct response to increasing IAP with oliguria developing at an IAP of 15 mmHg and anuria at 30 mmHg [32,33,42]. Renal artery blood flow has been demonstrated to be preferentially diminished in comparison to both celiac and superior mesenteric artery blood flow [68]. Renal vein pressure and renal vascular resistance are both significantly elevated [35,42,48]. All of these changes shunt blood away from the renal cortex and functioning glomeruli leading to impaired glomerular and tubular function and significant reductions in urinary output. IAH decreases glomerular filtration rate causing a rise in both blood urea nitrogen and serum creatinine and a reduction in creatinine clearance [33,35,42,48,51,79]. Osmolar clearance is similarly decreased and fractional excretion of sodium increased [79]. Urinary sodium and chloride concentrations decrease and urinary potassium concentrations increase [33]. Plasma renin activity and aldosterone levels increase significantly [33,48]. Antidiuretic hormone levels have been demonstrated to increase to more than twice basal levels [82]. All of these pathophysiologic changes appear to be potentially reversible if the patient’s IAH is recognized and treated appropriately before significant organ dysfunction has developed [32,48]. BUN ve Kreatinin ↑ Ozmoler klirens ↓ Fe Na ↑ İdrarda Na ve Cl ↓; K ↑ PRA ve aldosterone ↑ ADH↑

27
APB: Abdominal perfüzyon basıncı
World Society of the Abdominal Compartment Syndrome 2004 Consensus Conference (WSACS) ( IAP: Batın içi basınç APB: Abdominal perfüzyon basıncı APB= MAP - IAP Viseral perfüzyon Resusitason hedefi defined as MAP minus IAP, has been demonstrated to be an accurate predictor of visceral perfusion and an endpoint for resuscitation APP is also superior to other common resuscitation endpoints such as arterial pH, base deficit, arterial lactate, and hourly urinary output. Failure to maintain an APP of at least 60 mmHg by day 3 of critical illness has been demonstrated to predict survival from IAH and ACS [64,105,106]. APP thus figures prominently in the resuscitation strategy recommended by the WSACS. Filtration Gradient Arteryel pH Baz defisiti Arteryel laktat Saatlik idrar çıkışı APB Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2009
 ( IAP: Batın içi basınç. APB: Abdominal perfüzyon basıncı. APB= MAP - IAP. Viseral perfüzyon. Resusitason hedefi. defined as MAP minus IAP, has been demonstrated to be an accurate predictor of visceral. perfusion and an endpoint for resuscitation APP is also superior to other common. resuscitation endpoints such as arterial pH, base deficit, arterial lactate, and hourly urinary output. Failure to maintain an APP of at least 60 mmHg by day 3 of critical illness has been demonstrated to. predict survival from IAH and ACS [64,105,106]. APP thus figures prominently in the resuscitation. strategy recommended by the WSACS. Filtration Gradient. Arteryel pH. Baz defisiti. Arteryel laktat. Saatlik idrar çıkışı. APB. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine")
28
IAP için Normal ve Patolojik Değerler
Normal IAP :Sub-atmosferik- 0 mmHg Tipik YBÜ hastası : 5-7 mmHg Yeni Batın cerrahisi geçirmiş Sepsis Organ yetmezliği Dehidratasyon >25 mmhg – mortalite ↑ IAHT: >12mmHg (persistan) ACS: > 20 mmHg 10-20 mmhg Normal IAP ranges from sub-atmospheric to zero mmHg [109,113,116]. In the typical intensive care unit patient, however, IAP is commonly elevated to a range of 5-7 mmHg while patients with recent abdominal surgery, sepsis, organ failure, or need for volume resuscitation may demonstrate IAPs of mmHg [11,15]. Prolonged elevation in IAP to such levels can result in organ dysfunction and failure while pressures above 25 mmHg are associated with significant potential mortality Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2009
 ACS: > 20 mmHg mmhg. Normal IAP ranges from sub-atmospheric to zero mmHg [109,113,116]. In the typical intensive care. unit patient, however, IAP is commonly elevated to a range of 5-7 mmHg while patients with recent. abdominal surgery, sepsis, organ failure, or need for volume resuscitation may demonstrate IAPs of mmHg [11,15]. Prolonged elevation in IAP to such levels can result in organ dysfunction and. failure while pressures above 25 mmHg are associated with significant potential mortality. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine")
29
ACS Belirti ve Bulguları
Abdominal distention Elevated IAP Oliguria refractory to volume administration Refractory metabolic acidosis Elevated PIP Hypercarbia Hypoxemia refractory to increasing FiO2 and PEEP Elevated ICP Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2009

30
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2009

31
IAB ÖLÇÜM YÖNTEMİ Current Opinion in Critical Care 2005, 11:156—171

32
Current Opinion in Critical Care 2005, 11:156—171

33
Current Opinion in Critical Care 2005, 11:156—171

34
‘Kronik’ zeminde ‘Akut’ Olgusu
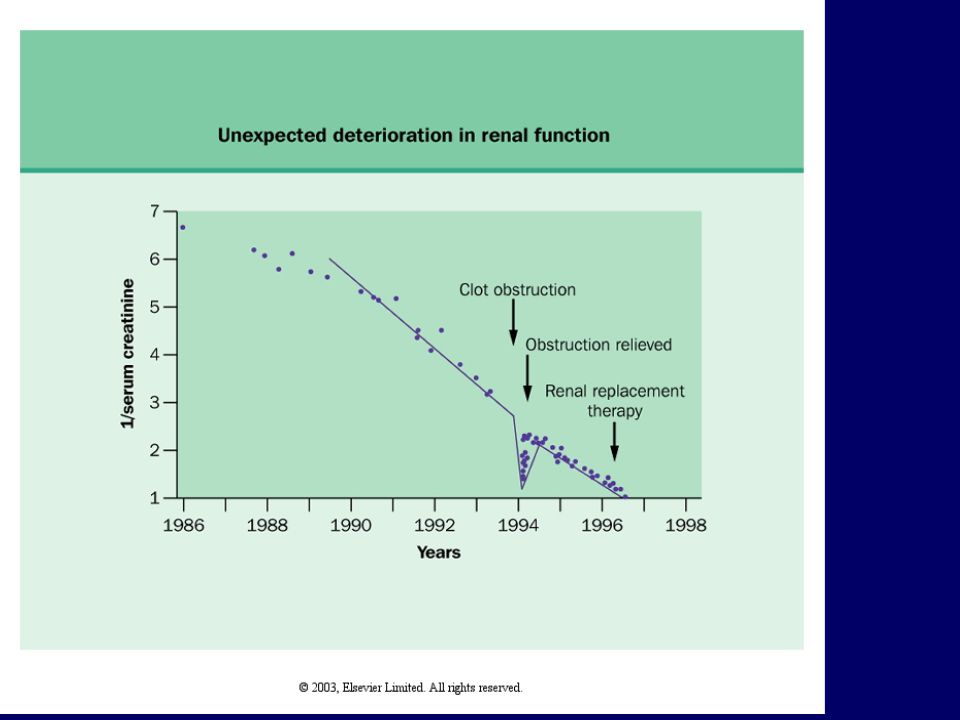
KBY zemininde araya giren ek bir sorun nedeniyle renal işlevde Akut kötüleşme Hipovolemi Nefrotoksik ilaç kullanımı Infeksiyon Obstrüksiyon Kalp yetersizliği Akselere hipertansiyon

36
SONUÇ ABY gelişmemesi için önlemlerin alınması önemli
Özellikle riskli hasta gruplarının belirlenmesi önemli IAHT ve ACS AKI gelişmesinin belirteçleri arasında giderek önem kazanıyor

37
Teşekkürler…

38
Böbrek yetersizliğinin İlaç kullanımına etkisi
Oral alımda biyoyararlanım düşer i.v. yol tercih edilmeli Proteine bağlanma oranı azalır İlaç toksisite riski artar Dağılım hacmi etkilenir Metabolizması etkilenir Atılımı etkilenir Böbrek yetersizliğinde ilaç kullanım rehberlerinden yararlanılmalıdır

Benzer bir sunumlar