Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Enfeksiyon Hastalıkları ve Klinik Mikrobiyoloji Anabilim Dalı
HIV/AIDS Dr.Hayati Demiraslan Enfeksiyon Hastalıkları ve Klinik Mikrobiyoloji Anabilim Dalı 1

2
SUNUM PLANI Nedir Yapısı Tarihçe Epidemiyoloji Bulaşma yolları Tanı
Korunma

3
HIV enfeksiyonu Human immunodeficiency virus (HIV) tarafından sebep olunan ilerledikçe immün sistemi yıkan bir hastalıktır Akut HIV enfeksiyonu (bir kaç haftada sonlanır) Asemptomatik HIV enfeksiyonu (10 yıl) Erken semptomatik HIV enfeksiyonu AIDS İleri AIDS
 Asemptomatik HIV enfeksiyonu (10 yıl) Erken semptomatik HIV enfeksiyonu. AIDS. İleri AIDS")
4
Retrovirus ailesi İkozahedral yapıda, zarflı, Çift zincirli RNA virüsü
Lentivirus sınıfı Onkovirus Spumavirus HIV-1 HTLV-1 Doğada yaygın HIV-2 HTLV-II patojenite? Simian IDV Felin leukemia virus Bovin leukemia virus Simian virüs HIV1in prokürsörüdür. Retrovirüsler viral RNA’nın reverz transkriptazını kullanarak lineer çift zincirli DNA’ya döner ve konak genomuna integre olur. Pariste bir hastanın LN’da izole edildi. HIV-2 birçok maymun türünü enfekte edebilir. ENV ve GAG genlerine göre A-J’ye kadar 10 farklı türü vardır Retrovirüsler viral RNA’nın reverz transkriptazını kullanarak lineer çift zincirli DNA’ya döner ve konak genomuna integre olur. 4

5
İntegraz ZARF

6
Once HIV comes into contact with a T-cell, it must attach itself to the cell so that it can fuse with the cell and inject its genetic material (a blueprint for making more HIV) into it. Attachment is a specific binding between proteins on the surface of the virus and proteins that serve as receptors on the surface of the T-cell. Normally, these receptors help the cell communicate with other cells. Two receptors in particular, CD4 and a beta-chemokine receptor (either CCR5 or CXCR4), are used by HIV to latch onto the cell. On the surface of the viral envelope, two sets of proteins (also known as antireceptors) called gp120 and gp41 attach to CD4 and CCR5/CXCR4. Drugs called attachment or entry inhibitors are currently being studied in clinical trials. These drugs block the interaction between the cellular receptors and the antireceptor on the virus by binding to or altering the receptor sites. Scientists have found that people who naturally lack these cellular receptors because of a genetic mutation, or those who have them blocked by natural chemokines (chemical messengers), may not get infected as readily with HIV or may progress more slowly to AIDS. Scientists are also examining vaccines that may help the body block these receptors. After attachment is completed, viral penetration occurs. Penetration allows the nucleocapsid -- the genetic core -- of the virus to be injected directly into the cell's cytoplasm. gp120 actually contains three sugar-coated proteins (glycoproteins) and, once gp120 attaches itself to CD4, these three proteins spread apart. This allows the gp41 protein, which is normally hidden by the gp120 proteins, to become exposed and bind to the chemokine receptor. Once this has occurred, the viral envelope and the cell membrane are brought into direct contact and essentially melt into each other. Drugs called fusion inhibitors prevent the binding of gp41 and the chemokine receptor. T-20 (enfuvirtide, Fuzeon), an experimental fusion inhibitor that is nearing FDA approval, binds to a portion of gp41, preventing it from binding to the chemokine receptor. Once HIV has penetrated the cell membrane, it is ready to release its genetic information (RNA) into the cell. The viral RNA is protected in the nucleocapsid. The nucleocapsid needs to be partially dissolved so that the virus's RNA can be converted into DNA, a necessary step if HIV's genetic material is to be incorporated into the T-cell's genetic core. The process by which HIV's RNA is converted to DNA is called reverse transcription. This transcription process happens in almost every human cell, but in the opposite direction -- from DNA to RNA. DNA from the cell nucleus is transcribed into messenger RNA, which then directs the cell's various metabolic functions needed to do its job in the body. HIV uses an enzyme called reverse transcriptase to accomplish this transcription. The single-stranded viral RNA is transcribed into a double strand of DNA, which contains the instructions HIV needs to hijack a T-cell's genetic machinery in order to reproduce itself. Reverse transcriptase uses nucleotides -- building blocks of DNA -- from the cell cytoplasm to make this process possible. Drugs called reverse transcriptase inhibitors block HIV's reverse transcriptase from using these nucleotides. Nucleoside and nucleotide analog reverse transcriptase inhibitors (NRTIs) -- such as Zerit, Epivir, and Viread -- contain faulty imitations of the nucleotides found in a T-cell's cytoplasm. Instead of incorporating a nucleotide into the growing chain of DNA, the imitation building blocks in NRTIs are inserted, which prevents the double strand of DNA from becoming fully formed. Non-nucleoside reverse transcriptase inhibitors (NNRTIs) -- such as Viramune and Sustiva -- block reverse transcription by attaching to the enzyme in a way that prevents it from functioning. 6
, may not get infected as readily with HIV or may progress more slowly to AIDS. Scientists are also examining vaccines that may help the body block these receptors. After attachment is completed, viral penetration occurs. Penetration allows the nucleocapsid -- the genetic core -- of the virus to be injected directly into the cell s cytoplasm. gp120 actually contains three sugar-coated proteins (glycoproteins) and, once gp120 attaches itself to CD4, these three proteins spread apart. This allows the gp41 protein, which is normally hidden by the gp120 proteins, to become exposed and bind to the chemokine receptor. Once this has occurred, the viral envelope and the cell membrane are brought into direct contact and essentially melt into each other. Drugs called fusion inhibitors prevent the binding of gp41 and the chemokine receptor. T-20 (enfuvirtide, Fuzeon), an experimental fusion inhibitor that is nearing FDA approval, binds to a portion of gp41, preventing it from binding to the chemokine receptor. Once HIV has penetrated the cell membrane, it is ready to release its genetic information (RNA) into the cell. The viral RNA is protected in the nucleocapsid. The nucleocapsid needs to be partially dissolved so that the virus s RNA can be converted into DNA, a necessary step if HIV s genetic material is to be incorporated into the T-cell s genetic core. The process by which HIV s RNA is converted to DNA is called reverse transcription. This transcription process happens in almost every human cell, but in the opposite direction -- from DNA to RNA. DNA from the cell nucleus is transcribed into messenger RNA, which then directs the cell s various metabolic functions needed to do its job in the body. HIV uses an enzyme called reverse transcriptase to accomplish this transcription. The single-stranded viral RNA is transcribed into a double strand of DNA, which contains the instructions HIV needs to hijack a T-cell s genetic machinery in order to reproduce itself. Reverse transcriptase uses nucleotides -- building blocks of DNA -- from the cell cytoplasm to make this process possible. Drugs called reverse transcriptase inhibitors block HIV s reverse transcriptase from using these nucleotides. Nucleoside and nucleotide analog reverse transcriptase inhibitors (NRTIs) -- such as Zerit, Epivir, and Viread -- contain faulty imitations of the nucleotides found in a T-cell s cytoplasm. Instead of incorporating a nucleotide into the growing chain of DNA, the imitation building blocks in NRTIs are inserted, which prevents the double strand of DNA from becoming fully formed. Non-nucleoside reverse transcriptase inhibitors (NNRTIs) -- such as Viramune and Sustiva -- block reverse transcription by attaching to the enzyme in a way that prevents it from functioning")
7
“Zinc finger” inh Nukleusa giriş İntegrasyon Montaj ve tomurcuklanma
Nukleus por kompleksi İmportin alfa, beta, Nup62 İntegrasyon Montaj ve tomurcuklanma “Zinc finger” inh If HIV succeeds in translating its instructions from RNA to DNA, HIV must then insert its DNA (also called the preintegration complex) into the cell's DNA. This process is called integration. In most human cells, there is a structure called the cell nucleus, where the cell's DNA is stored. In order for integration to occur, the newly translated DNA must be transported across the nuclear membrane into the nucleus. Although the exact mechanism that HIV uses to transport its genetic cargo into the cell nucleus is still unclear, viral protein R (VPR), which is carried by HIV, may facilitate the movement of the preintegration complex to the nucleus. Once the viral RNA has successfully bridged the nuclear membrane and been escorted to the nucleus, HIV uses an enzyme called integrase to insert HIV's double-stranded DNA into the cell's existing DNA. Drugs that inhibit the HIV preintegration complex from traveling to the nucleus -- integrase inhibitors -- are currently in early clinical trials. After successful integration of the viral DNA, the host cell is now latently infected with HIV. This viral DNA is referred to as provirus. The HIV provirus now awaits activation. When the immune cell becomes activated, this latent provirus awakens and instructs the cellular machinery to produce the necessary components of HIV, like plastic pieces of a model airplane. From the viral DNA, two strands of RNA are constructed and transported out of the nucleus. One strand is translated into subunits of HIV such as protease, reverse transcriptase, integrase, and structural proteins. The other strand becomes the genetic material for the new viruses. Compounds that inhibit or alter viral RNA have been identified as potential antiviral agents. Once the various viral subunits have been produced and processed, they must be separated for the final assembly into new virus. This separation, or cleavage, is accomplished by the viral protease enzyme. Drugs called protease inhibitors -- such as Kaletra, Crixivan, and Viracept -- bind to the protease enzyme and prevent it from separating, or cleaving, the subunits. If cleavage is successfully completed, the HIV subunits combine to make up the content of the new virons. In the next step of the viral life cycle, the structural subunits of HIV mesh with the cell's membrane and begin to deform a section of the membrane. This allows the nucleocapsid to take shape and viral RNA is wound tightly to fit inside the nucleocapsid. Researchers are looking at drugs called zinc finger inhibitors, which interfere with the packaging of the viral RNA into the nucleocapsid. The final step of the viral life cycle is called budding. In this process, the genetic material enclosed in the nucleocapsid merges with the deformed cell membrane to form the new viral envelope. With its genetic material tucked away in its nucleocapsid and a new outer coat made from the host cell's membrane, the newly formed HIV pinches off and enters into circulation, ready to start the whole process again. During HIV's life cycle, the T-cell, known as the host cell, is altered and perhaps damaged, causing the death of the cell. Scientists are not sure exactly how the cell dies but have come up with a number of scenarios. First, after the cell becomes infected with a virus or other pathogen, internal signals may tell it to commit suicide. This is known as apoptosis or programmed cell death -- a self-destruct program intended to kill the cell with the hopes of killing the virus as well. A second possible mechanism for the death of the cell is that, as thousands of HIV particles bud or escape from the cell, they severely damage the cell's membrane, resulting in the loss of the cell. Another possible cause for the cell's death is that other cells of the immune system, known as killer cells, recognize that the cell is infected and inject it with chemicals that destroy it. Montaj Nukleus por kompleksi “Zinc finger” inh İmportin alfa, beta, Nup62 7
 into the cell s DNA. This process is called integration. In most human cells, there is a structure called the cell nucleus, where the cell s DNA is stored. In order for integration to occur, the newly translated DNA must be transported across the nuclear membrane into the nucleus. Although the exact mechanism that HIV uses to transport its genetic cargo into the cell nucleus is still unclear, viral protein R (VPR), which is carried by HIV, may facilitate the movement of the preintegration complex to the nucleus. Once the viral RNA has successfully bridged the nuclear membrane and been escorted to the nucleus, HIV uses an enzyme called integrase to insert HIV s double-stranded DNA into the cell s existing DNA. Drugs that inhibit the HIV preintegration complex from traveling to the nucleus -- integrase inhibitors -- are currently in early clinical trials. After successful integration of the viral DNA, the host cell is now latently infected with HIV. This viral DNA is referred to as provirus. The HIV provirus now awaits activation. When the immune cell becomes activated, this latent provirus awakens and instructs the cellular machinery to produce the necessary components of HIV, like plastic pieces of a model airplane. From the viral DNA, two strands of RNA are constructed and transported out of the nucleus. One strand is translated into subunits of HIV such as protease, reverse transcriptase, integrase, and structural proteins. The other strand becomes the genetic material for the new viruses. Compounds that inhibit or alter viral RNA have been identified as potential antiviral agents. Once the various viral subunits have been produced and processed, they must be separated for the final assembly into new virus. This separation, or cleavage, is accomplished by the viral protease enzyme. Drugs called protease inhibitors -- such as Kaletra, Crixivan, and Viracept -- bind to the protease enzyme and prevent it from separating, or cleaving, the subunits. If cleavage is successfully completed, the HIV subunits combine to make up the content of the new virons. In the next step of the viral life cycle, the structural subunits of HIV mesh with the cell s membrane and begin to deform a section of the membrane. This allows the nucleocapsid to take shape and viral RNA is wound tightly to fit inside the nucleocapsid. Researchers are looking at drugs called zinc finger inhibitors, which interfere with the packaging of the viral RNA into the nucleocapsid. The final step of the viral life cycle is called budding. In this process, the genetic material enclosed in the nucleocapsid merges with the deformed cell membrane to form the new viral envelope. With its genetic material tucked away in its nucleocapsid and a new outer coat made from the host cell s membrane, the newly formed HIV pinches off and enters into circulation, ready to start the whole process again. During HIV s life cycle, the T-cell, known as the host cell, is altered and perhaps damaged, causing the death of the cell. Scientists are not sure exactly how the cell dies but have come up with a number of scenarios. First, after the cell becomes infected with a virus or other pathogen, internal signals may tell it to commit suicide. This is known as apoptosis or programmed cell death -- a self-destruct program intended to kill the cell with the hopes of killing the virus as well. A second possible mechanism for the death of the cell is that, as thousands of HIV particles bud or escape from the cell, they severely damage the cell s membrane, resulting in the loss of the cell. Another possible cause for the cell s death is that other cells of the immune system, known as killer cells, recognize that the cell is infected and inject it with chemicals that destroy it. Montaj. Nukleus por kompleksi. Zinc finger inh. İmportin alfa, beta, Nup")
8
EPİDEMİYOLOJİ İlk kez 1981 yılında ABD de tanımlanmıştır
‘Akkiz immün yetmezlik sendromu’ adı verilmiştir Etken virus 1983 yılında izole edilmiştir Türkiye’de ilk vaka 1985 8

9
bir tür SIVcpz keşfettiler
Şubat 1999’da Alabama’da bir tür SIVcpz keşfettiler Pan troglodytes troglodytes In February 1999 a group of researchers from the University of Alabama2 announced that they had found a type of SIVcpz that was almost identical to HIV-1. This particular strain was identified in a frozen sample taken from a captive member of the sub-group of chimpanzees known as Pan troglodytes troglodytes (P. t. troglodytes), which were once common in west-central Africa.
, which were once common in west-central Africa")
10
Tarihçe HIV, Simian Immunodeficiency virüsün torunudur.
SIV’in bazı türleri HIV-1 ve HIV-2 ile sıkı benzerlikler taşır.

11
HIV enfeksiyonu örnekleri
1959’da Kongo’dan erişkin erkekten alınan serumda elde edildi. 1960’da Kongo’dan erişkin kadının lenf bezinden saptandı. 1969’da St. Louis’de ölen bir Amerikalı delikanlının (teeneger) doku örneğinde 1976’da ölen bir denizcinin doku örneklerinde HIV saptandı Hunter; The most commonly accepted theory is that of the 'hunter'. In this scenario, SIVcpz was transferred to humans as a result of chimps being killed and eaten or their blood getting into cuts or wounds on the hunter. Zhu, T et. al (1998, 5th February) 'An African HIV-1 Sequence from 1959 and Implications for the Origin of the Epidemic' Nature, 391(6667) Worobey, M et. al (2008, 2nd October) 'Direct Evidence of Extensive Diversity of HIV-1 in Kinshasa by 1960' Nature, 455(7213) Kolata, G (1987, 28th October) 'Boy's 1969 death suggests AIDS invaded U.S. several times' New York Times Frøland, SS et. al (1988, 11th June) 'HIV-1 infection in Norwegian family before 1970' The Lancet 331(8598)
 doku örneğinde. 1976’da ölen bir denizcinin doku örneklerinde HIV saptandı. Hunter; The most commonly accepted theory is that of the hunter . In this scenario, SIVcpz was transferred to humans as a result of chimps being killed and eaten or their blood getting into cuts or wounds on the hunter. Zhu, T et. al (1998, 5th February) An African HIV-1 Sequence from 1959 and Implications for the Origin of the Epidemic Nature, 391(6667) Worobey, M et. al (2008, 2nd October) Direct Evidence of Extensive Diversity of HIV-1 in Kinshasa by 1960 Nature, 455(7213) Kolata, G (1987, 28th October) Boy s 1969 death suggests AIDS invaded U.S. several times New York Times. Frøland, SS et. al (1988, 11th June) HIV-1 infection in Norwegian family before 1970 The Lancet 331(8598)")
13
Milyon

14
Türkiye’de HIV * *İlk 6 ay

15
Olası bulaş yolları

17
Kayseri civarında HIV (1996-2009)
55 hasta takip edilmiş ve %78 erkek %71 evli %44 yurtdışında çalışma öyküsü %91 şüpheli heteroseksüel cinsel ilişki Mikrobiyol Bul 2011; 45 (1): 17
:")
18
Patogenez

19
BULAŞ Cinsel yolla bulaş Kan ve diğer dokularla bulaş Perinatal bulaş
Sağlık bakımında HIV bulaşı Bulaşın diğer yolları 19

20
Vücut sıvılarında HIV Vücut sıvılarının 1ml’sinde ortalama HİV partikül sayısı Kan 18,000 Semen 11,000 Vajinal sıvı 7,000 Amniyotik sıvı 4,000 Tükürük 1 20

21
BULAŞ YOLLARI Cinsel yolla bulaş En önemli ve en sık bulaş yoludur
Bulaş için HIV pozitif kişiyle yapılan tek bir cinsel temas yeterlidir Korunmasız cinsel temasta; virusun enfekte erkekten kadına bulaş riski, enfekte kadından erkeğe bulaş riskinden fazladır 21

22
Cinsel yolla bulaş Heteroseksüel Homoseksüel Afrika, Güney Amerika
Karaipler Kuzey Amerika Avrupa

23
Cinsel yolla bulaş riski
Korunmasız %40 bulaş VAJİNAL ORAL 23

24
Cinsel yolla bulaş 1000 koitus başına olgu, UGANDA
24 Wawer, J Infect Dis 2005;191:1403

25
Cinsel yolla bulaş riski
Sünnet (%50-60) Kondom kullanımı Tek eşlilik HIV RNA Genital ülser Kanama Birden çok cinsel eş CYBH (üretrit, gonore)
 Kondom kullanımı. Tek eşlilik. HIV RNA. Genital ülser. Kanama. Birden çok cinsel eş. CYBH (üretrit, gonore)")
26
Kan ve kan ürünleri ile bulaş
HIV yönünden tarama yapılmaya (1985) başlandığından beri bu yolla bulaş azalmıştır Kan ve KÜ transfüzyonu Organ transplantasyonu Kornea ve işlenmiş dokularla Bulaş riski yok Yıl Test Risk 1996 p24 antijeni 1/ / 2002 Nukleik asit testleri (12 gün) 1/ 26
 başlandığından beri bu yolla bulaş azalmıştır. Kan ve KÜ transfüzyonu. Organ transplantasyonu. Kornea ve işlenmiş dokularla. Bulaş riski yok. Yıl. Test. Risk p24 antijeni. 1/ / Nukleik asit testleri (12 gün) 1/")
27
Damar içi madde kullanımı
İlişkili faktörler Enjektör ve diğer aletlerle bulaş Damar içi madde kullananlar İğne paylaşma sıklığı Paylaşılan kişi sayısı Enjeksiyon sayısı Bölgedeki HIV sıklığı Kokain enjeksiyonu daha riskli bulunmuş 27

28
Anneden bebeğe bulaş Preterm doğum Uzamış membran rüptürü (>4 saat)
Perinatal risk %13-40 Gebelik süresince %30-50 doğumda + Doğum sırasında (%40) Postpartum dönemde emzirmekle %14-29 Preterm doğum Uzamış membran rüptürü (>4 saat) Madde kullanımı Antenatal düşük CD4+ sayısı Düşük doğum ağırlığı HIV can be transmitted from mother to infant during pregnancy, childbirth, or breastfeeding. 28
 Postpartum dönemde emzirmekle. % Preterm doğum. Uzamış membran rüptürü (>4 saat) Madde kullanımı. Antenatal düşük CD4+ sayısı. Düşük doğum ağırlığı. HIV can be transmitted from mother to infant during pregnancy, childbirth, or breastfeeding")
29
Viral yük ve bulaş riski
N Engl J Med 1999; 341: pp

30
Sağlık bakımında HIV bulaşı
Sağlık personeline bulaş İğne,enjektör batması ile (risk % ) Kanlı vücut sıvıları ile mukozal temasla (risk <%0.1) Sağlık personelinden hastaya 53 HIV’li çalışanın 2’sinin hastalarında + Hastadan hastaya Malzemelerin tekrar kullanılması İlaçların çoklu kullanımı Dişçi ve ortopedist 30
 Kanlı vücut sıvıları ile mukozal temasla (risk <%0.1) Sağlık personelinden hastaya. 53 HIV’li çalışanın 2’sinin hastalarında + Hastadan hastaya. Malzemelerin tekrar kullanılması. İlaçların çoklu kullanımı. Dişçi ve ortopedist")
31
Bulaşın diğer yolları Tükrükle ve ısırıkla bulaş nadirdir (kan yoksa)
HIV inhibitör etkisi Sivrisinekler?? Dövme, pearcing? 31

32
HCV koenfeksiyonu, agamaglobulinemi Antikor yanıtının
PEP almak, HCV koenfeksiyonu, agamaglobulinemi Antikor yanıtının gecikmesine sebep olabilir

33
HIV-enfekte erişkinlerde CDC sınıflaması CD4 hücre sayısı kategorileri
Klinik Kategori : PGL = persistan generalize lenfadenopati A B* C# Asemptomatik, Akut HIV veya PGL Semptomatik, A veya C dışı AIDS-indikatör durumlar (1) ≥500 /µL (%26) A1 B1 C1 (2) /µL (%15-25) A2 B2 C2 (3) <200 /µL (%14) A3 B3 C3 Recommendations and Reports. MMWR April 11, 2014; Vol. 63: No.3
 ≥500 /µL (%26) A1. B1. C1. (2) /µL (%15-25) A2. B2. C2. (3) <200 /µL (%14) A3. B3. C3. Recommendations and Reports. MMWR April 11, 2014; Vol. 63: No")
34
Kategori B Semptomatik durumlar 1. Bacillary angiomatosis
2. Orofaringeal kandidiyaz (thrush) 3. Vulvovaginal kandidiyaz, persistan veya rezistan 4. Pelvik inflammatuvar hastalık (PID) 5. Servikal displazi (orta, ağır)/servikal karsinoma in situ 6. Oral hairy lökoplaki, 7. Herpes zoster,en az bir dermatomu tutan veya ≥2 epizod 8. Idiopatik trombositopenik purpura 9. Konstitusyonel semptomlar (ateş>38.5ºC) ishal >1 ay 10. Periferik nöropati
 3. Vulvovaginal kandidiyaz, persistan veya rezistan. 4. Pelvik inflammatuvar hastalık (PID) 5. Servikal displazi (orta, ağır)/servikal karsinoma in situ. 6. Oral hairy lökoplaki, 7. Herpes zoster,en az bir dermatomu tutan veya ≥2 epizod. 8. Idiopatik trombositopenik purpura. 9. Konstitusyonel semptomlar (ateş>38.5ºC) ishal >1 ay. 10. Periferik nöropati")
35
# Kategori C AIDS-indikatör durumlar
Rekürren bakteriyel pnömoni (12 ayda ≥2 epizod) Bronş, trakea, akciğer kandidozu Özefageal kandidoz Servikal karsinoma, invaziv, dissemine veya extrapulmoner koksidiyomikoz extrapulmoner kriptokokkoz Kronik intestinal kriptosporidyaz (>1 ay) Cytomegalovirus hastalığı (KC, dalak ve LN dışı) HIV-ensefalopatisi Herpes simplex: kronik ülserler >1 ay, bronşit, pnömoni, özefajit Histoplasmoz, disseminated or extrapulmonary Izosporiyaz, kronick intestinal (>1 ay) Kaposi sarkomu Lenfoma, Burkitt, immunoblastik, primer santral sinir sistemi Mycobacterium avium complex (MAC) veya Mycobacterium kansasii, dissemine veya ekstrapulmoner Mycobacterium tuberculosis, pulmoner veya ekstrapulmoner Mycobacterium, diğer türler, dissemine veya ekstrapulmoner Pneumocystis jiroveci pnömonisi (PCP) Progressif multifokal lökoensefalopati (PML) Salmonella septisemi, rekürren Beyin toxoplasmozu Wasting sendromu (İstemeden kilo kaybı>%10) associated with either chronic diarrhea (hergün≥2 dışkılama ≥1 ay), kroniik yorgunluk, ateş ≥1 ay
 Bronş, trakea, akciğer kandidozu. Özefageal kandidoz. Servikal karsinoma, invaziv, dissemine veya extrapulmoner koksidiyomikoz. extrapulmoner kriptokokkoz. Kronik intestinal kriptosporidyaz (>1 ay) Cytomegalovirus hastalığı (KC, dalak ve LN dışı) HIV-ensefalopatisi. Herpes simplex: kronik ülserler >1 ay, bronşit, pnömoni, özefajit. Histoplasmoz, disseminated or extrapulmonary. Izosporiyaz, kronick intestinal (>1 ay) Kaposi sarkomu. Lenfoma, Burkitt, immunoblastik, primer santral sinir sistemi. Mycobacterium avium complex (MAC) veya Mycobacterium kansasii, dissemine veya ekstrapulmoner. Mycobacterium tuberculosis, pulmoner veya ekstrapulmoner. Mycobacterium, diğer türler, dissemine veya ekstrapulmoner. Pneumocystis jiroveci pnömonisi (PCP) Progressif multifokal lökoensefalopati (PML) Salmonella septisemi, rekürren. Beyin toxoplasmozu. Wasting sendromu (İstemeden kilo kaybı>%10) associated with either chronic diarrhea (hergün≥2 dışkılama ≥1 ay), kroniik yorgunluk, ateş ≥1 ay")
36
Oral kandidiyazis

37
Hairy lökoplaki

38
Kaposi sarkomu

39
Kaposi sarkomu

40
CD4 <50 kandida cilt enfeksiyonu

42
Zona

43
Yaygın konsolidasyon, hipoksi ile başvuran hasta CD4 5 hücre/mm3

44
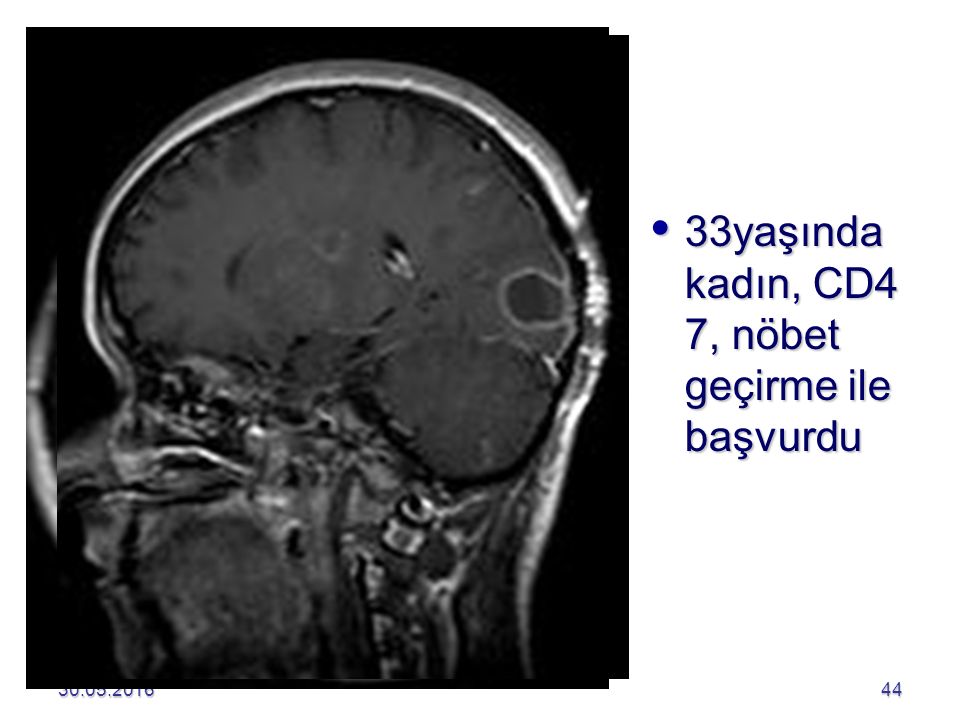
33yaşında kadın, CD4 7, nöbet geçirme ile başvurdu
45
bilateral pulmonary infiltrate (white triangles),
caving formation“ (black arrows) present in the right apical region
 present in the right apical region.")
46
Mediastinal LAP

47
HIV tanımlayıcı maligniteler
Kaposi sarkomu Non-Hodgkin lenfoma Primer santral sinir sistemi lenfoması Primer efüzyon lenfoması (PEL) Plazmablastik lenfoma İnvaziv serviks Ca Anal Ca Hodgkin Lymphoma Multicentric Castleman’s disease Diffüz Büyük B hücreli lenfoma Burkitt lenfoma Bower M et al, British HIV Association guidelines for HIV-associated malignancies 2014, HIV MEDICINE, 15 (Supplement 2) March 2014
 Plazmablastik lenfoma. İnvaziv serviks Ca. Anal Ca. Hodgkin Lymphoma. Multicentric Castleman’s disease. Diffüz Büyük B hücreli lenfoma. Burkitt lenfoma. Bower M et al, British HIV Association guidelines for HIV-associated malignancies 2014, HIV MEDICINE, 15 (Supplement 2) March")
48
DSÖ’nün 2020 hedefleri HIV’lilerin %90’ına tanı konulması
Tanı konulanların %90’ı ARTye ulaşması sağlanacak ART alanların %90’ında viral baskılanma sağlanacak

49
HIV’lilerin ne kadarı ART’ye ulaşıyor?
2014 yılında 14.9 milyon HIV’li antiretroviral alıyor (ART) %40 Güncelleme: Temmuz 2015
 %40. Güncelleme: Temmuz")
50
Kimler tedavi edilmeli?
KLİNİK KATEGORİ CD4 HÜCRE SAYISI DHHS rehberi 2015 EACS 2015/10 BASHH rehberi Semptomatik hasta Herhangi bir değer Önerilir Mutlaka önerilir Asemptomatikhasta <350/mm3 Önerilir (AI) Asemptomatik hasta /mm3 Önerilir (AII) >500/mm3 Önerilir (BIII) - Belli durumlarda öner DHHS: Department of Health and Human Services (U.S) EACS: European AIDS clinical society BASHH: British association for sexual health and HIV
 Asemptomatik hasta /mm3. Önerilir (AII) >500/mm3. Önerilir (BIII) - Belli durumlarda öner. DHHS: Department of Health and Human Services (U.S) EACS: European AIDS clinical society. BASHH: British association for sexual health and HIV")
51
KORUNMA Cinsel yolla bulaşa karşı korunma
Genital ve oral mukoza membranlarının cinsel ilişki sırasında kan,semen,vajinal ve servikal sekresyonlarla temasının azaltılması Kondom kullanımının teşvik edilmesi ve yaygınlaştırılması Cinsel yolla bulaşan diğer hastalıkların tedavisi Güvenli cinsel temasın yaygınlaştırılması (tek eşli cinsel yaşam veya uygun ve güvenli cinsel eş seçimi) 51
")
52
Cinsel yolla bulaşa karşı korunma
Kadın kondomu kullanımı (%11-26 yetersiz) Erkek kondomunun koruyuculuğu %60-96 52
 Erkek kondomunun koruyuculuğu %")
53
Cinsel yolla bulaşa karşı korunma
Spermisit (nonoxinol 9) kullanımı HIV bulaşını artırır Mikrobisit (polinaftalen sülfonat gel (PRO-2000) HIV sıklığını kısmen azalttı 53
 kullanımı HIV bulaşını artırır. Mikrobisit (polinaftalen sülfonat gel (PRO-2000) HIV sıklığını kısmen azalttı")
54
Kan ve kan ürünleriyle bulaşa karşı korunma
Antikor testleri bulunduğundan beri bu yolla bulaş azalmıştır Damar içi madde kullananlarda Bu alışkanlığın önlenmesi ve tedavi edilmesi Ortak enjektör kullanım risklerinin anlatılması Steril enjektör kullanımının sağlanması Eğitim 54

55
Anneden bebeğe geçişe karşı korunma
HIV pozitif kadına doğum kontrol yöntemleri öğretilmelidir Hamile kalan HIV pozitif kadına erken dönemde kürtaj yapılmalıdır Bebeği doğurmakta ısrarlı ise gebeliğin son trimesterinde anneye, doğumdan sonra da bebeğe antiretroviral tedavi başlanmalıdır Elektif sezaryan uygulanırsa bebeğe HIV geçişi 4-5 kat azalır Virüsün anne sütü ile geçişi gösterildiğinden emzirme önerilmez 55

56
PrEp profilaksi Truvada (emtricitabine/tenofovir disoproxil fumarate),
HIV enfeksiyonu riski yüksek ve HIV enfekte eşlerle seksüel aktivitede bulunan HIV (-) kişilerde bulaş riskini azaltır 56
 kişilerde bulaş riskini azaltır")
57
Gelecekte KÜR KÜR

58
Kaynaklar http://www.who.int/hiv/en/
59
TEŞEKKÜRLER SORULAR

Benzer bir sunumlar