Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Prostaglandin Analogları ve KMÖ
DR.EMİNE KAYA ÖZYURT PROF.DR.HALİL ATEŞ

2
PROSTAGLANDİNLER 1934’de prostat sıvısından izole edilmişler
Gözde 1960’de irisin lipidik ekstraktı “Irin” (PGE ve PGF karışımı) 1970’de Ambache, oküler irritasyonda etkileri olduğunu göstermiştir Vücutta birçok dokuda üretilirler, lokal hormonlardır 20-karbonlu yağ asitlerinden türerler (çoğunlukla araşidonik asitten) “Eikosanoidler” olarak bilinirler Siklopentan halkası içerirler (PGA-F, 9 grup) İnsan gözünde GİB düşürücü etki (1985) (PGF2 trometamin tuzu) Göz PG üretiminin gösterildiği ilk eksternal organdır. Siklopentan halkasının konfigürasyonuna göre çeşitli gruplara ayrılırlar, yan zincirlerdeki çift bağ sayısı alt rakamlarla gösterilir.
 1970’de Ambache, oküler irritasyonda etkileri olduğunu göstermiştir. Vücutta birçok dokuda üretilirler, lokal hormonlardır. 20-karbonlu yağ asitlerinden türerler (çoğunlukla araşidonik asitten) Eikosanoidler olarak bilinirler. Siklopentan halkası içerirler (PGA-F, 9 grup) İnsan gözünde GİB düşürücü etki (1985) (PGF2 trometamin tuzu) Göz PG üretiminin gösterildiği ilk eksternal organdır. Siklopentan halkasının konfigürasyonuna göre çeşitli gruplara ayrılırlar, yan zincirlerdeki çift bağ sayısı alt rakamlarla gösterilir.")
3
PROSTAGLANDİNLERİN ETKİ MEKANİZMALARI
FP reseptörü (yedi transmembranal segmentli G-proteini ile kenetli) GTP bağlayıcı protein Fosfolipaz C aktivasyonu IP3 oluşması İntrasellüler Ca+2 artışı Dokularda mekanik ve kimyasal değişiklik UVEOSKLERAL DIŞA AKIM ARTIŞI
 GTP bağlayıcı protein. Fosfolipaz C aktivasyonu. IP3 oluşması. İntrasellüler Ca+2 artışı. Dokularda mekanik ve kimyasal değişiklik. UVEOSKLERAL DIŞA AKIM ARTIŞI.")
4
Hümör Aköz Yapımı α2-agonistler β1-blokerler Karbonik anhidraz inh. Trabeküler Dışa akım Prostamidler Kolinerjikler Uveoskleral Dışa akım Prostaglandinler α2-agonistler Prostamidler

6
? ? ? KMÖ’de Etyopatogenez Vitreomakuler traksiyon?? PG salınımı??
Vasküler yetersizlik?? İnflamasyon??** *Hipoksi/iskemi mikrodolaşımdaki inflamatuar değişiklikler ? ? ?

7
KMÖ ve Göz İçi İnflamasyon
İnflamasyon PG’ler *Antienflamatuar ilaçlara cevap PG SENTEZİ VE İNHİBİTÖR AJANLAR Membran lipidleri Fosfolipaz A2(kortikosteroidler inhibe eder) Araşidonik asit Siklooksijenaz (aspirin ve indometazin inhibe eder) Endoperoksitler (tromboksan,prostosiklin,prostoglandin) Lökotrienler
 Araşidonik asit. Siklooksijenaz. (aspirin ve indometazin inhibe eder) Endoperoksitler. (tromboksan,prostosiklin,prostoglandin) Lökotrienler.")
8
Araşidonik asit kaskadının tek ürünü PG ler değildir; komplemanlar, platelet-activating faktor(PAF), lizozomal enzimler, sitokinler, nitrik oksit, endotelin. Bu ürünler de inflamasyona karışır. Örneğin aköz humörde IL-6 düzeyinin artması klinik semptomlarla yakından paralellik gösterir. Ayrıca VEGF ve IGF-1 kan-retina bariyerinin bozulmasına neden olarak KMÖ ye neden olabilir.

9
Katarakt ve İOL cerrahisini takiben KMÖ ve PG ler
PG sentezi önceden verilen NSAI ile azaltılabilir -KMÖ gelişimindeki diğer bir faktör de kan-aköz bariyerin ve kan-retina bariyerinin frajilitesidir.(diyabet, hipertansiyon,yaşlanma ve üveit bu yapılarda zayıflama+). Bu hastalarda gelişim olasılığı daha fazla olacağı düşünülmelidir Kan-retina bariyeri veya kan-aköz bariyerinin bozulmasının ardından KMÖ gelişir. Aslında bu ödem makula ile sınırlı kalmaz, diffüz yayılır.
. Bu hastalarda gelişim olasılığı daha fazla olacağı düşünülmelidir. Kan-retina bariyeri veya kan-aköz bariyerinin bozulmasının ardından KMÖ gelişir. Aslında bu ödem makula ile sınırlı kalmaz, diffüz yayılır.")
10
Katarakt ve İOL cerrahisini takiben KMÖ ve PG ler
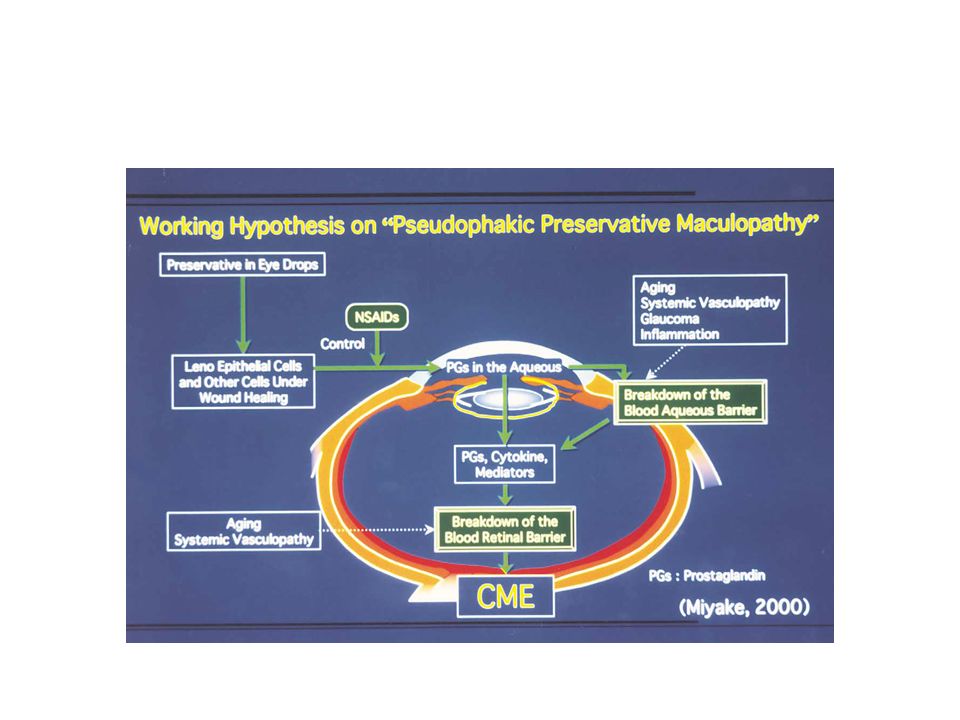
Pg sentezi oküler veya cerrahi travma sonrası irritatif reaksiyona neden olur. Medyatörlerin düzeyi ile inflamatuar semptomların şiddeti paraleldir Afakik ve pseudofakik KMÖ nün gelişimi (1997 den beri kabul edilen hipotez); -iris, silyer body veya lens epitel hücrelerine cerrahi travma hümör aközde PG sentezine neden olmakta -PG ler kan-aköz bariyerini bozar -PG ler ve diğer inflamatuar medyatörler (endotoksin, immun komplekler ve sitokinler) hümör aközde birikir -biriken medyatörler diffüzyonla vitreusa geçerek retinaya ulaşır ve kan-retina bariyerini bozarlar -sonuçta retinal kapillerden ve sinir başından serum sızar ve retinal dokuya yayılır Primer lezyon tarafından kimyasal medyatörlerin serbest kalarak intraoküler sıvılara karışması nedeniyle bu fenomen oluşur
; -iris, silyer body veya lens epitel hücrelerine cerrahi travma hümör aközde PG sentezine neden olmakta. -PG ler kan-aköz bariyerini bozar. -PG ler ve diğer inflamatuar medyatörler (endotoksin, immun komplekler ve sitokinler) hümör aközde birikir. -biriken medyatörler diffüzyonla vitreusa geçerek retinaya ulaşır ve kan-retina bariyerini bozarlar. -sonuçta retinal kapillerden ve sinir başından serum sızar ve retinal dokuya yayılır. Primer lezyon tarafından kimyasal medyatörlerin serbest kalarak intraoküler sıvılara karışması nedeniyle bu fenomen oluşur.")
11
Kmö ve pg analogu antiglokomatöz damlalar
Oküler hipotansif lipidlerle KMÖ arasındaki ilişki hala tartışmalı Komplikasyonsuz fako cerrahisi sonrası klinik olarak anlamlı KMÖ insidansı %3 * P. C. Yeh and S. Ramanathan, “Latanoprost and clinically significant cystoid macular edema after uneventful phacoemulsification with intraocular lens implantation,” Journal of Cataract and Refractive Surgery, vol. 28, no. 10, pp. 1814– 1818, 2002. Perioperatif periyotta kullanımı ile ilgili fikir birliği yoktur Katarakt ve intraoküler lens cerrahisini takiben oluşan KMÖ de PG lerin rolü bir çok çalışmada araştırılmıştır Prosroglandinler katarakt veya intraoküler cerrahi sonrası kmö nün potansiyel nedeni ?

12
Agange N, Mosaed S. “Prostaglandin-Induced CystoidMacular Edema Following Routine Cataract Extraction”. Journal of Ophthalmology Volume 2010, Article ID M. Furuichi, T. Chiba, K. Abe et al., “Cystoid macular edema associated with topical latanoprost in glaucomatous eyes with a normally functioning blood-ocular barrier,” Journal of Glaucoma, vol. 10, no. 3, pp. 233–236, 2001. P. C. Yeh and S. Ramanathan, “Latanoprost and clinically significant cystoid macular edema after uneventful phacoemulsification with intraocular lens implantation,” Journal of Cataract and Refractive Surgery, vol. 28, no. 10, pp. 1814– 1818, 2002. K. Miyake, I. Ota, K. Maekubo, S. Ichihashi, and S. Miyake, “Latanoprost accelerates disruption of the blood-aqueous barrier and the incidence of angiographic cystoid macular edema in early postoperative pseudophakias,” Archives of Ophthalmology, vol. 117, no. 1, pp. 34–40, 1999. D. L. Halpern and L. R. Pasquale, “Cystoidmacular edema in aphakia and pseudophakia after use of prostaglandin analogs,” Seminars in Ophthalmology, vol. 17, no. 3-4, pp. 181–186, 2002.

13
P. C. Yeh and S. Ramanathan, “Latanoprost and clinically significant cystoid macular edema after uneventful phacoemulsification with intraocular lens implantation,” Journal of Cataract and Refractive Surgery, vol. 28, no. 10, pp. 1814–1818, 2002. Ayyala RS, Cruz DA, Margo CE, Harman LE, Pautler SE, Misch DM, et al.”Cystoid macular edema associated with latanoprost in aphakic and pseudophakic eyes”. Am J Ophthalmol 1998, 126:602–604. Callanan D, Fellman RL, Savage JA: Latanoprost-associated cystoid macular edema. Am J Ophthalmol 1998, 126:134–135. Moroi SE, Gottfredsdottir MS, Schteingart MT, Elner SG, Lee CM, Schertzer RM, et al.: Cystoid macular edema associated with latanoprost therapy in a case series of patients with glaucoma and ocular hypertension. Ophthalmology 1999, 106:1024–1029. Arcieri ES, Santan A, Rocha FN, Guapo GL, Costa VP.” Blood-aqueous barrier changes after the use of prostaglandin analogues in patients with pseudophakia and aphakia: a 6-month randomized trial.” Arch Ophthalmol Feb;123(2):
:")
14
Kmö ve pg analogu antiglokomatöz damlalar
PG ler kan-aköz bariyerini etkileyerek erken dönemde KMÖ e nadiren neden olur *Bir çok yayında yüksek riskli gözlerde bile latanoprost ile tedavide çok nadiren kmö izlendiği belirtilmiştir Eşzamanlı NSAİ damlaların kullanımı bu yan etkiyi önler Bazı çalışmalarda da etken maddeden ziyade preservanların bu yan etkiye neden olduğu sonucuna ulaşılmıştır

15
Timolol ve PG analogları ile aynı şekilde dizayn edilen iki farklı çalışmanın sonuçları değerlendirildiğinde Latanoprost, timolol ve preservan maddelerin her biri iyileşme sürecinde intraoküler hücreleri stimüle eder 5. haftada FFA ile KMÖ insidansında gruplar arasında fark saptanmamıştır Kan-aköz bariyerinin bozulması ve KMÖ insidansı eşzamanlı NSAİ ilaç kullanımı ile önlenebilmiştir Bu yan etkilerin başlamasında, asıl etken madde olan latanoprost veya timololden ziyade preservan olarak kullanılan benzalkonium chlorid rol oynar 1-Miyake K, Ota I, Maekubo K, et al: Latanoprost accelerates disruption of the blood–aqueous barrier and the incidence of angiographic cystoid macular edema in early postoperative pseudophakias. Arch Ophthalmol 117:34–40, 1999 2-Miyake K, Ota I, Ibaraki N, et al: Enhanced disruption of the blood–aqueous barrier and the incidence of angiographic cystoid macular edema by topical timolol and its preservative in early postoperative pseudophakia. Arch Ophthalmol 119:387–94, 2001

17
Benzalkonium chloride içeren damlalar katarakt cerrahisi sonrası iyileşme döneminde lens epitel hücreleri veya ön üveal dokuya temas ederse PG gibi kimyasal medyatörlerin sentezi artar Kan-aköz bariyerinin bozulma PG lerin ve diğer sitokinlerin hümör aköz ve vitreusta dağılması Kan-retina bariyerinin bozulması KMÖ insidansında artış

18
Latanoprost and cystoid macular edema: is there a causal relation?
Published reports of the occurrence of cystoid macular edema (CME) in eyes being treated with latanoprost have led to concern regarding a possible causal relation between the two. Review of all published cases (28 eyes in 25 patients), plus another case reported here for the first time, indicates that all eyes had independent risk for development of CME, so that definitive conclusions about a causal relation cannot be established. In addition, controlled clinical trials and experimental studies with latanoprost have given no indication that latanoprost causes clinical CME. Pharmacokinetic considerations indicate that the concentration of latanoprost expected in the posterior segment of the eye is too low to have a pharmacologic effect, and latanoprost is not known to exhibit vasoactive or inflammatory properties. Nevertheless, reports of a possible association between CME and latanoprost use must be given serious consideration, and in eyes that are at risk for CME, an increased level of surveillance for its development is recommended. Curr Opin Ophthalmol 2000, 11:94–100
 in eyes being treated with latanoprost have led to concern regarding a possible causal relation between the two. Review of all published cases (28 eyes in 25 patients), plus another case reported here for the first time, indicates that all eyes had independent risk for development of CME, so that definitive conclusions about a causal relation cannot be established. In addition, controlled clinical trials and experimental studies with latanoprost have given no indication that latanoprost causes clinical CME. Pharmacokinetic considerations indicate that the concentration of latanoprost expected in the posterior segment of the eye is too low to have a pharmacologic effect, and latanoprost is not known to exhibit vasoactive or inflammatory properties. Nevertheless, reports of a possible association between CME and latanoprost use must be given serious consideration, and in eyes that are at risk for CME, an increased level of surveillance for its development is recommended. Curr Opin Ophthalmol 2000, 11:94–100.")
19
Miyake K, Ibaraki N. ”Prostaglandins and Cystoid Macular Edema”
Miyake K, Ibaraki N.”Prostaglandins and Cystoid Macular Edema”. Survey of Ophthalmology, vol 47,sup 1, August 2002. Cochereau I.” Cataract surgery and prostaglandin analogs? Yes, but under certain conditions”. J Fr Ophtalmol Jun;27(6 Pt 2):706-7. Ibaraki N, Goto Y, Kobayashi S, Miyake K: Effects of latanoprost and timolol maleate on the expression of cytokine in human lens epithelial SRA01/04 cells [abstract]. Invest Ophtalmol Vis Sci 42(Suppl):289, 2001
: Ibaraki N, Goto Y, Kobayashi S, Miyake K: Effects of latanoprost and timolol maleate on the expression of cytokine in human lens epithelial SRA01/04 cells [abstract]. Invest Ophtalmol Vis Sci 42(Suppl):289,")
20
Lens epitel hücrelerinde yara yeri iyileşmesi ne kadar sürer?
*2-3 yıl sonra sekonder katarakt daha sık izlenir Cerrahi sonrası uzun bir süre anti-glokomatöz ihtiyacında eşzamanlı olarak NSAİ ajanların da başlanması?

21
Cystoid Macular Edema in a Low-Risk Patient After Switching From Latanoprost to Bimatoprost
PURPOSE: To report a case of angiographically documented cystoid macula edema occurring after switching a pseudophakic patient from latanoprost to bimatoprost. DESIGN: Observational case report. METHODS: A 68-year-old man developed intense conjunctival hyperemia and cystoid macula edema after switching from latanoprost to bimatoprost 9 months after cataract surgery in an eye at low-risk for this cystoid macular edema. RESULTS: Bimatoprost was discontinued and diclofenac initiated. After 2 months, visual acuity and ocular hyperemia returned to baseline levels. Fundus examination revealed resolution of cystoid macula edema. CONCLUSION: It is possible that pseudophakic eyes that develop intense conjunctival hyperemia associated with ocular hypotensive lipids might be at higher risk for developing cystoid macula edema. Am J Ophthalmol 2004;137:966–968 Düşük riskli bir hastada latanoprottan bimatoprosta geçildikten bir hafta sonra ciddi konjonktival hiperemi gelişmiş, bir ay sonra da kmö gelişmiş Bu hasta PAAG nedeniyle latanoprsot kullanıyormuş, komplikasyonsuz fako cerrahisi sonrası 1. ayda gibnın yüksek seyretmesi nedeniyle latanoprost başlanmış, 8 ay sonra gib hedef değerin üzerine çıkınca bimatoprosta geçilmiş. Kmö gelişince bimatoprost kesilerek, diclofenak başlanmış ve 1 ay sonra kmö kalmamış. 2 yıl sonra tekrar gib kontrol edilemeyince latanoprost başlanmış ve kmö izlenmemiş -bu hiperemi durumunun bariyerleri bozarak kmö gelişimi için risk oluşturduğu düşünülmüş

22
Cystoid macular edema associated with latanoprost therapy in a pseudophakic vitrectomized patient after removal of silicone oil endotamponade PURPOSE: To describe the occurrence of cystoid macular edema in a pseudophakic vitrectomized patient following use of latanoprost (0.005%). METHODS: A 58-year-old patient underwent routine cataract surgery with posterior chamber lens implantation complicated by rhegmatogenous retinal detachment three months later. A pars plana vitrectomy was performed with silicone oil endotamponade which was removed six months later. Five months after oil removal, the patient presented with secondary open-angle glaucoma treated with latanoprost 0.005% eye drops once daily. RESULTS: Two weeks after initiation of latanoprost treatment, visual acuity dropped from 0.8 to 0.3 due to cystoid macular edema confirmed by fluorescein angiography. After discontinuing Latanoprost therapy and with topical corticosteroid treatment, cystoid macular edema slowly resolved, and within 6 months, visual acuity improved to 0.8. CONCLUSIONS: Despite its marked ocular hypotensive effect, latanoprost should be carefully used in patients after uncomplicated cataract surgery if the vitreous body was removed by pars Piana vitrectomy. Eur J Ophthalmol Mar;13(2):221-2. Pseudofakik vitrektomize bir hastada silikon alımı sonrası latanoprost tedavisiyle ilgili KMÖ
. METHODS: A 58-year-old patient underwent routine cataract surgery with posterior. chamber lens implantation complicated by rhegmatogenous retinal detachment three. months later. A pars plana vitrectomy was performed with silicone oil endotamponade. which was removed six months later. Five months after oil removal, the patient presented with. secondary open-angle glaucoma treated with latanoprost 0.005% eye drops once daily. RESULTS: Two weeks after initiation of latanoprost treatment, visual acuity dropped from 0.8 to. 0.3 due to cystoid macular edema confirmed by fluorescein angiography. After discontinuing. Latanoprost therapy and with topical corticosteroid treatment, cystoid macular edema slowly. resolved, and within 6 months, visual acuity improved to 0.8. CONCLUSIONS: Despite its marked ocular hypotensive effect, latanoprost should be carefully. used in patients after uncomplicated cataract surgery if the vitreous body was removed by pars. Piana vitrectomy. Eur J Ophthalmol Mar;13(2): Pseudofakik vitrektomize bir hastada silikon alımı sonrası latanoprost tedavisiyle ilgili KMÖ.")
23
Association Between Topical Prostaglandin Analog Use and Development of Choroidal Neovascular Membranes in Patients with Concurrent Glaucoma and Age-Related Macular Degeneration Purpose: Matrix metalloproteinases (MMPs) are a family of enzymes that act to degrade extracellular matrix (ECM) molecules, such as collagen, elastin, and gelatin. The glaucoma medication latanoprost, and possibly other topical prostaglandin analogs, increase uveoscleral outflow and lower intraocular pressure (IOP) in primary open-angle glaucoma (POAG) by activating MMPs 1, 2, 3, and 9 in the ciliary body. It has been reported that latanoprost may also gain access to the posterior segment and induce cystoid macular edema, although the mechanism is unknown. In the choroid, activation of some of the same subtypes of MMPs (particularly subtypes 2 and 9) has been implicated in the formation of choroidal neovascular membranes (CNVMs) in age-related macular degeneration (AMD). This study examined whether topical prostaglandin analog use is associated with a greater risk of CNVM formation in patients diagnosed with both AMD and POAG. Methods: A retrospective record review was performed to identify patients with a concurrent diagnosis of AMD and POAG between 1998 and Four hundred and eighty-four (484) eyes were identified and grouped as wet (n = 65) or dry (n = 419) AMD. Prostaglandin usage was compared between the two groups. Usage of other glaucoma medications was also compared. A minimum of 1 year of topical glaucoma medication was required for inclusion in the study. Exclusion criteria included a history of CNVM prior to starting glaucoma medications and a previous history of glaucoma surgery. Results: Fifty-six percent (56%) of dry AMD and 62% of wet AMD eyes were using a topical prostaglandin (P > 0.10; not significant). Analysis of specific topical prostaglandin analog usage in the wet versus dry AMD groups revealed no statistically significant differences in the percentage of eyes treated with latanoprost (37.7% versus 41.5%), bimatoprost (12.9% versus 10.8%), or travoprost (9.2% versus 5.3%), respectively. No significant differences in the use of other glaucoma medications were observed between the two groups. Conclusions: No association between long-term topical prostaglandin use and CNVM development was found in patients with AMD and POAG. Journal of Ocular Pharmacology and Therapeutics. April 2006, 22(2):
 are a family of enzymes that act to degrade extracellular matrix (ECM) molecules, such as collagen, elastin, and gelatin. The glaucoma medication latanoprost, and possibly other topical prostaglandin analogs, increase uveoscleral outflow and lower intraocular pressure (IOP) in primary open-angle glaucoma (POAG) by activating MMPs 1, 2, 3, and 9 in the ciliary body. It has been reported that latanoprost may also gain access to the posterior segment and induce cystoid macular edema, although the mechanism is unknown. In the choroid, activation of some of the same subtypes of MMPs (particularly subtypes 2 and 9) has been implicated in the formation of choroidal neovascular membranes (CNVMs) in age-related macular degeneration (AMD). This study examined whether topical prostaglandin analog use is associated with a greater risk of CNVM formation in patients diagnosed with both AMD and POAG. Methods: A retrospective record review was performed to identify patients with a concurrent diagnosis of AMD and POAG between 1998 and Four hundred and eighty-four (484) eyes were identified and grouped as wet (n = 65) or dry (n = 419) AMD. Prostaglandin usage was compared between the two groups. Usage of other glaucoma medications was also compared. A minimum of 1 year of topical glaucoma medication was required for inclusion in the study. Exclusion criteria included a history of CNVM prior to starting glaucoma medications and a previous history of glaucoma surgery. Results: Fifty-six percent (56%) of dry AMD and 62% of wet AMD eyes were using a topical prostaglandin (P > 0.10; not significant). Analysis of specific topical prostaglandin analog usage in the wet versus dry AMD groups revealed no statistically significant differences in the percentage of eyes treated with latanoprost (37.7% versus 41.5%), bimatoprost (12.9% versus 10.8%), or travoprost (9.2% versus 5.3%), respectively. No significant differences in the use of other glaucoma medications were observed between the two groups. Conclusions: No association between long-term topical prostaglandin use and CNVM development was found in patients with AMD and POAG. Journal of Ocular Pharmacology and Therapeutics. April 2006, 22(2):")
Benzer bir sunumlar
 problemleri (Matching and Assignment problems)>")






 (Yrd. Doç. Dr. Deniz Dal)>")

>")








 Tanım : Bütün konularda kısa ve öz bilgi içeren bir çalışmadır. Belirli bir konu ile sınırlı yada genel kapsamlı olabilir.>")
