Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
PCOS Non-IVF'te Gonadotropin Tedavisinde Kritik Noktalar
Dr Batuhan Özmen Ankara Üniversitesi KHD AD USAUM, Üreme Sağlığı Merkezi

2
PCOS: OI Amaç: Anovulatuar PCOS hastalarında fertilitenin sağlanması ve tek canlı doğuma ulaşılması,

3
İnsidans %6-7 Female İnfertilite: %40 sebep anovulasyon Anovulatuar infertilite: %75-80 sebep PCOS PCOS’a sekonder anovulatuar infertilitede ilk-basamak tedavi halen CC

4
PCOS:OI Klomifen Sitrat
Homburg R, Hum Reprod, 2005

5
PCOS:OI Klomifen Sitrat
Imani et al Fertil Steril 2002

6
CRA ? Birçok merkez 150-mg CC’ye rağmen ovulasyon yoksa CCR
The Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group Hum Reprod 2008

7
CC / Ovulasyon Oranları
50 mg %46 100mg %21 150mg %8 %75 %25 olguda CRA Anovulation is estimated to cause 40% of female infertility, and many cases are due to the polycystic ovary syndrome (PCOS). In these cases of euestrogenic anovulation, clomiphene citrate (CC) remains the primary therapy to induce ovulation; 75% of patients ovulate in response to CC treatment (1). Approximately 70% of patients who respond do so at a dose of 50 or 100 mg of CC (2); the maximum dose is usually 250 mg. However, we and many other infertility specialists consider patients who do not ovulate while receiving the 150-mg dose of CC to be resistant to the drug. Homburg R, Hum Reprod, 2005 7
. In. these cases of euestrogenic anovulation, clomiphene. citrate (CC) remains the primary therapy. to induce ovulation; 75% of patients ovulate in. response to CC treatment (1). Approximately. 70% of patients who respond do so at a dose of. 50 or 100 mg of CC (2); the maximum dose is. usually 250 mg. However, we and many other. infertility specialists consider patients who do. not ovulate while receiving the 150-mg dose of. CC to be resistant to the drug. Homburg R, Hum Reprod,")
8
CC rezistan olguda kabul edilmiş standart bir yaklaşım yok …
PCOS / ESHRE – ASRM Tanı: Rotterdam kriterleri, 2003 Tedavi: Selanik, 2007 First-line tedavi CC Second-line tedavi LOS Gn CC rezistan olguda kabul edilmiş standart bir yaklaşım yok … The Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group Hum Reprod 2008

9
SOGC Clinical Practice Guideline 2010
Gonadotropin Oİ 2nd-line tedavi olarak anovülatuar PCOS hastalarında önerilmektedir. Tedavi ultrason ve laboratuar olarak takip gerektirir. Yüksek maliyet ve çoğul gebelik ile OHSS en önemli risklerdir. (II-2A) J Obstet Gynaecol Can 2010
 J Obstet Gynaecol Can")
10
%71 Kümülatif Gebelik CC takiben Gnd OI Eijkemans et al Hum Reprod 2003

11
GONADOTROPİN Ovulatuar siklus % 70-98 Kümülatif gebelik oranı % 35-70
van Santbrinket al., 1995 White et al., 1996 Mulders et al., 2003 DEZAVANTAJ Çoğul gebelik >%10-30 OHSS %1-10 Siklus iptali %3-10 Fauser and Van Heusden, 1997.

13
PCOS OI: Gonadotropin Kritik Noktalar
Hasta seçimi Protokol tipi Gonadotropin tipi GnRH Ant ? Adjuvant Ajanlar İptal kriterleri Sonuçlar Coğul Gebelik OHSS Siklus başarısı

14
Ovulasyon İndüksiyon Protokolleri
Standart doz step-up Düşük doz protokoller Kronik düşük doz step-up Düşük doz step-down Ardışık düşük doz step-up/ step-down Kronik ultra düşük doz step up

15
Klasik (Konvansiyonel) Protokol
18 mm hCG IU 16 mm 14 mm E 2 12 mm 10 mm 300 ıu 225 IU 150 IU 1 2 7 14 21 28 35 Başlangıç dozu 150 IU, 2-4. günü USG sonucuna göre doz artışı 75 IU Doz artışı her 5-7 günde

16
Klasik (Konvansiyonel) Protokol
Ovulasyon %62-98 Konsepsiyon (siklus başına) %10-20 Çoğul gebelik %15-36 Abortus %24-42 OHSS %1.1-14
 % Çoğul gebelik % Abortus % OHSS %")
17
Düşük Doz Step-down Protokolü
150 IU FSH 5 gün süre ile, follikül > 10 mm olana kadar 3 gün aralıklarla 37.5 IU doz artımı, daha sonra hCG kriterleri sağlanana kadar 3 günde bir 37.5 doz azaltımı

18
van Santbrink,European Journal of Endocrinology (2002)
")
19
Klasik ve Düşük Doz Klasik Protokol Düşük Doz Protokol 94 %16 %27 %6.3
Siklus Gebelik Çoğul gebelik OHSS Homburg, 95 48 6 2 5 59 10 Hedon, 98 46 9 1 42 14 Total 94 %16 %27 %6.3 101 %24 %8 %0.9

20
Düşük doz Step-down OHSS↑ Stimülasyon süresi ↓
Kötü cevaplı hastalarda uygun yöntem olabilir. These regimens have proved to be successful in reducing the risk of ovarian hyperstimulation while maintaining a satisfactory pregnancy rate (7, 10). However, these protocols were imprecise, as it was necessary for the patient to self-administer half or two-thirds of a 75-IU ampoule of urinary gonadotropins. With the availability of recombinant FSH (rFSH) preparations in vials containing 50 IU (follitropin beta) or 37.5 IU (follitropin alfa), it was easier for patients to use smaller doses. The hCG was withheld if there was an insufficient ovarian response after 35 days of treatment or in the case of ovarian hyperresponse (3 follicles of 15 mm). In the latter instance, conversion to IVF-ET was allowed. Stimulation is cancelled when multifollicular growth is apparent and more than three folliclesO12 mmin diameter are present. 20
. However, these. protocols were imprecise, as it was necessary for the patient to. self-administer half or two-thirds of a 75-IU ampoule of urinary. gonadotropins. With the availability of recombinant FSH (rFSH) preparations. in vials containing 50 IU (follitropin beta) or 37.5 IU. (follitropin alfa), it was easier for patients to use smaller. doses. The hCG was withheld. if there was an insufficient ovarian response after 35. days of treatment or in the case of ovarian hyperresponse. (3 follicles of 15 mm). In the latter instance, conversion. to IVF-ET was allowed. Stimulation. is cancelled when multifollicular growth is apparent and. more than three folliclesO12 mmin diameter are present. 20.")
21
Kronik Düşük Doz Step-up Protokolü
hCG gününe kadar follikül > 10 mm sağlayan dozda devam

22
Düşük Doz Step-up Protokolü
Ovulasyon (monofoliküler) %70-92 Konsepsiyon (siklus başına) %20 Çoğul gebelik %5.7 Abortus %11-28 OHSS %0.14
 % Konsepsiyon (siklus başına) %20. Çoğul gebelik %5.7. Abortus % OHSS %0.14.")
23
Step-up versus step down protocols in PCOS (Messinis,2005)
")
24
Christin-Maitre S, Hum Reprod 2003

25
CRA olgularda Gnd CC dirençli hastalarda düşük doz step-up protokolü daha güvenilirdir Takip eden sikluslarda step-up protokollere başlangıç dozu, cevap alınan dozun 25 veya 37.5 IU altı olmalıdır Düşük doz step-down protokol dirençli hastalar için uygun yaklaşım olabilir İptal kriterlerini belirlemek gerekli

26
Düşük Doz Step-up: Kritik Noktalar
Başlangıç Dozu (37.5, 50, 75) Doz artım süresi (7 vs 14, 3 vs 7) Doz artım düzeyi (25, 37.5, 50) Doz düşüş gerekli mi İptal kriterleri
 Doz artım süresi (7 vs 14, 3 vs 7) Doz artım düzeyi (25, 37.5, 50) Doz düşüş gerekli mi. İptal kriterleri.")
27
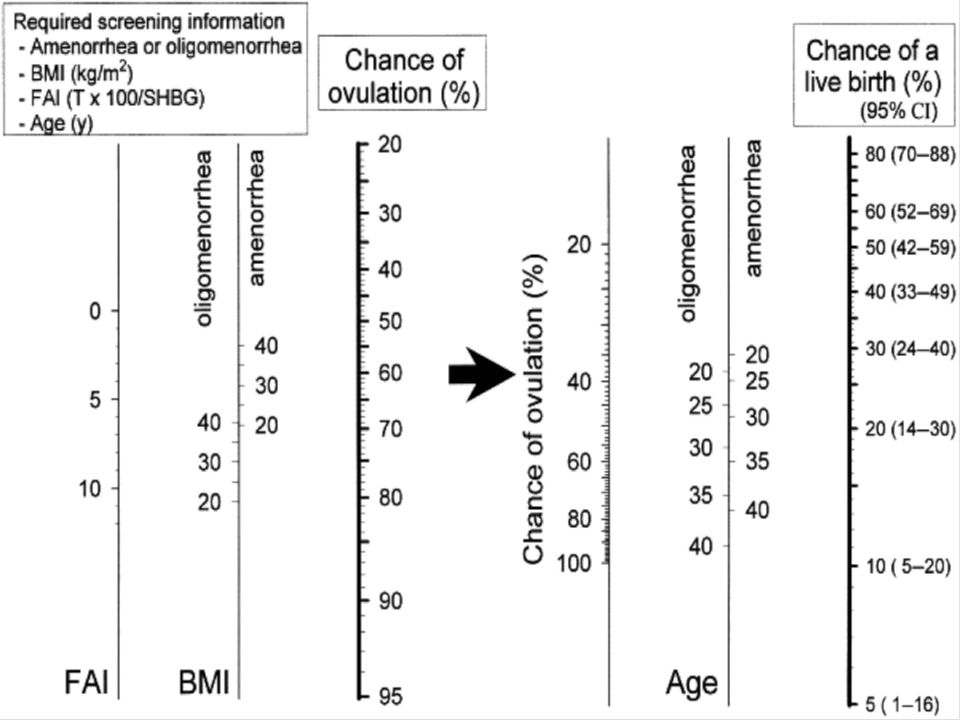
FSH Eşik Yaş BMI, Önceki CC siklus cevabı, IGF-1 düzeyi
Bazal FSH konsantrasyonu Imani B,Fertil Steril 2002

29
Probability Increased İnfertilty duration < 2 years FAI < 9
Cumulative ongoing pregnancy rate over time expressed per cycle in 85 women with clomiphene citrate-resistant PCOS. Presented at each treatment cycle is the number of pregnancies attained at that treatment cycle per number of women still under treatment. Probability Increased İnfertilty duration < 2 years FAI < 9 Oligomenorrhea Cumulative ongoing pregnancy rate over time expressed per cycle in 85 women with clomiphene citrate-resistant PCOS. Presented at each treatment cycle is the number of pregnancies attained at that treatment cycle per number of women still under treatment. van Wely M et al. Hum. Reprod. 2005;20: © The Author Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please

30
Düşük doz step-up Folikül çapı < 10 mm Folikül çapı > 18 mm hCG
These regimens have proved to be successful in reducing the risk of ovarian hyperstimulation while maintaining a satisfactory pregnancy rate (7, 10). However, these protocols were imprecise, as it was necessary for the patient to self-administer half or two-thirds of a 75-IU ampoule of urinary gonadotropins. With the availability of recombinant FSH (rFSH) preparations in vials containing 50 IU (follitropin beta) or 37.5 IU (follitropin alfa), it was easier for patients to use smaller doses. The hCG was withheld if there was an insufficient ovarian response after 35 days of treatment or in the case of ovarian hyperresponse (3 follicles of 15 mm). In the latter instance, conversion to IVF-ET was allowed. 52.5 IU 75 IU 112.5 IU 150 IU 187.5 IU 225 IU WHITE ET AL JCE 30
. However, these protocols were imprecise, as it was necessary for the patient to self-administer half or two-thirds of a 75-IU ampoule of urinary gonadotropins. With the availability of recombinant FSH (rFSH) preparations in vials containing 50 IU (follitropin beta) or 37.5 IU (follitropin alfa), it was easier for patients to use smaller doses. The hCG was withheld. if there was an insufficient ovarian response after 35. days of treatment or in the case of ovarian hyperresponse. (3 follicles of 15 mm). In the latter instance, conversion. to IVF-ET was allowed IU. 75 IU IU. 150 IU IU. 225 IU. WHITE ET AL JCE. 30.")
31
Düşük doz step-up Ovulasyon başarısızlığı < %5 hasta
Ciddi OHSS (-) ,İkiz gebelik %6 75 IU başlangıç dozunda %20 siklus iptali 52.5 başlangıç dozuna Ovulatuar siklus %72 Ovulatuar siklus %71 % 50 (37-79) monofoliküler %84 monofoliküler Gebelik %45 Gebelik %57 Düşük %35 Düşük %20 WHITE ET AL JCE Balash et al 2001 Hum Reprod
 ,İkiz gebelik %6. 75 IU başlangıç dozunda %20 siklus iptali başlangıç dozuna. Ovulatuar siklus %72. Ovulatuar siklus %71. % 50 (37-79) monofoliküler. %84 monofoliküler. Gebelik %45. Gebelik %57. Düşük %35. Düşük %20. WHITE ET AL JCE. Balash et al 2001 Hum Reprod.")
32
Low dose step up 37.5 vs 50 FSH Başlangıç dozu 37.5 IU n=12
Gün 13.5 ± 0.9 12.47 ± 0.72 NS IU 522.5 ± 45.9 623.3 ± 35.8 <0.05 EŞİK IU 40.0 ± 2.5 50 ± 0 <0.005 hCG günündeki Fol 10-13mm 0.33 ±0.16 0.2 ±0.14 Fol 13-17mm 0.27 ±0.12 0.53±0.17 Fol >17mm 1.7 ±0.24 1.7 ±0.24 E2 286 ± 22.7 296 ± 24.7 Unifoliküler % 67 % 60 Bifoliküler % 33 % 40 Prospective, randomized, crossover study including 15 women with clomiphene citrate-resistant chronic anovulatory infertility. Patients were treated with subcutaneous recombinant FSH at starting doses of 37.5 IU and 50 IU, respectively, according to a low-dose step-up protocol. Each woman received both treatments, in a randomized order, with an interval of 1 month between treatments. Balasch Journal of Assisted Reproduction and Genetics, 32

33
Düşük doz step-up önceki siklus ovulasyon(+) gebelik (-)
Folikül çapı < 10 mm Folikül çapı > 10 mm Folikül çapı > 18 mm hCG 52.5 IU 75 IU 112.5 IU Folikül çapı > 10 mm In women who developed multiple follicles, the treatment protocol was amended so that either a smaller starting dose was used (some patients will respond to 37.5 IU) or the increment in dose was less than usual (i.e. 25 Folikül çapı > 18 mm Folikül çapı < 10 mm hCG 75 IU 112.5 IU 33
 or the increment in dose was less than usual (i.e. 25. Folikül çapı > 18 mm. Folikül çapı < 10 mm. hCG. 75 IU IU. 33.")
34
%36 siklus iptal oranı Folikül çapı > 18 mm Folikül çapı < 10 mm
hCG 50 IU 100 IU 150 IU 200IU All the patients exhibited a follicular response: 6 (54%) of 11 ovulated, of whom 2 conceived. Four had their cycles cancelled because of overstimulation. Three of these had an explosive response, and 1 underwent diffuse ovarian enlargement and was discontinued from treatment because of a failure of unifollicular domination and a high risk of hyperstimulation. One patient did not ovulate despite the development of a follicle. One had an ovulatory cycle with the initial dose of 50 IU without any increase. %36 siklus iptal oranı Hayden Fertil Steril 34
 of 11 ovulated, of whom 2 conceived. Four had their cycles cancelled because of overstimulation. Three of these had an explosive response, and 1 underwent diffuse ovarian. enlargement and was discontinued from treatment because of a failure of unifollicular domination and a high risk of hyperstimulation. One patient did not ovulate despite the development of a follicle. One had an ovulatory cycle with the initial dose of 50 IU without any increase. %36 siklus iptal oranı. Hayden Fertil Steril. 34.")
35
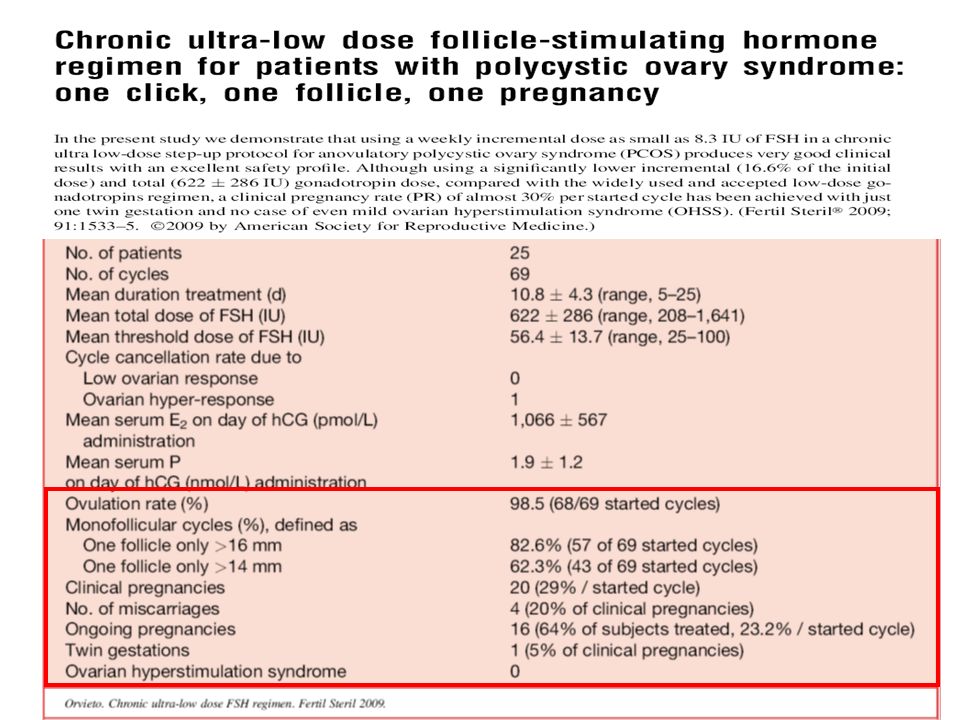
%13 siklus iptali % 84 ovülasyon % 6.8 OHSS (minimal-mild)
% 14 gebelik /siklus % 36.5 gebelik /hasta % 5.8 çoğul gebelik (ikiz) % 1.5 ektopik gebelik Alsina 2003, BJOG
 % 1.5 ektopik gebelik. Alsina 2003, BJOG.")
36
Düşük doz step-up Folikül çapı < 12 mm Folikül çapı > 18 mm hCG
These regimens have proved to be successful in reducing the risk of ovarian hyperstimulation while maintaining a satisfactory pregnancy rate (7, 10). However, these protocols were imprecise, as it was necessary for the patient to self-administer half or two-thirds of a 75-IU ampoule of urinary gonadotropins. With the availability of recombinant FSH (rFSH) preparations in vials containing 50 IU (follitropin beta) or 37.5 IU (follitropin alfa), it was easier for patients to use smaller doses. The hCG was withheld if there was an insufficient ovarian response after 35 days of treatment or in the case of ovarian hyperresponse (3 follicles of 15 mm). In the latter instance, conversion to IVF-ET was allowed. 50 IU 75 IU 100 IU 125 IU 150IU 175 IU Leader et al. Fertil Steril 2006 36
. However, these. protocols were imprecise, as it was necessary for the patient to. self-administer half or two-thirds of a 75-IU ampoule of urinary. gonadotropins. With the availability of recombinant FSH (rFSH) preparations. in vials containing 50 IU (follitropin beta) or 37.5 IU. (follitropin alfa), it was easier for patients to use smaller. doses. The hCG was withheld. if there was an insufficient ovarian response after 35. days of treatment or in the case of ovarian hyperresponse. (3 follicles of 15 mm). In the latter instance, conversion. to IVF-ET was allowed. 50 IU. 75 IU. 100 IU. 125 IU. 150IU. 175 IU. Leader et al. Fertil Steril")
37
(Fertil Steril 2006; In total, 118 women completed the trial (68 in the 25-IU dose increment group and 50 in the 50-IU dose increment group). The mean (SD) total dose of follitropin beta administered was lower in the 25-IU group than in the 50-IU group ( IU vs IU). The estimated treatment difference (adjusted for center) was also statistically significant (160.7 IU; P .013; 95% CI of difference, 287.2 to 34.3). 37
 total dose of follitropin beta administered. was lower in the 25-IU group than in the 50-IU group. ( IU vs IU). The estimated. treatment difference (adjusted for center) was also statistically. significant (160.7 IU; P .013; 95% CI of difference, to 34.3). 37.")
38
Leader et al. Fertil Steril 2006
No statistically significant differences were found for the cancellation rate due to low response, the total number of treatment days, and the mean serum FSH level. Nor was the difference in ongoing pregnancy rate (20.0% in the 25-IU group vs. 12.8% in the 50-IU group) statistically significant. Leader et al. Fertil Steril 2006 38
 statistically significant. Leader et al. Fertil Steril")
39
%20.5 %5.0 Leader et al. Fertil Steril 2006
Figure 3 shows the cancellation rate due to ovarian hyperresponse by treatment period. A considerably higher number of women in the 50-IU group developed an ovarian hyperresponse: 20.5 % versus 5.0% in the 25-IU group (P .004). In the present study, one woman (1.3%) in each group was hospitalized because of OHSS. This indicates that both dose regimens are adequate to minimize the risk of OHSS in a group of patients particularly sensitive to it. The low occurrence of multiple gestations (only two cases) supports the importance of careful monitoring of follicle development during ovarian stimulation in PCOS patients. A surprising finding was the relatively low incidence of miscarriage (11.1% of pregnancies) in our 25-IU group. Most large series of pregnant patients with PCOS report an early miscarriage rate of 20%–30% (7). However, a similarly low miscarriage rate (15%) was also observed in a small study of the sequential step-up and step-down regimen (20). Leader et al. Fertil Steril 2006 39
. In the present study, one woman (1.3%) in each group was. hospitalized because of OHSS. This indicates that both dose. regimens are adequate to minimize the risk of OHSS in a group. of patients particularly sensitive to it. The low occurrence of. multiple gestations (only two cases) supports the importance of. careful monitoring of follicle development during ovarian stimulation. in PCOS patients. A surprising finding was the relatively. low incidence of miscarriage (11.1% of pregnancies) in. our 25-IU group. Most large series of pregnant patients with. PCOS report an early miscarriage rate of 20%–30% (7). However, a similarly low miscarriage rate (15%) was also observed. in a small study of the sequential step-up and step-down. regimen (20). Leader et al. Fertil Steril")
41
Step-up sonrası Step-down protokol
İlk siklus step-up protokol ile FSH eşik değeri belirlenir Takip eden siklusta eşik değerin 37.5 IU fazlası ile step down siklusu başlanır. kümülatif gebelik oranı % 82 devam eden gebelik oranı %58 Tekil canlı doğum %43 Çoğul canlı doğum % 5 Mulders, et al Reprod. Biomed Online 41

42
Step-Up / Down Protokolü
Sequential Protocol 10 mm hCG IU 18 mm 14 mm 16 mm 12 mm E 2 150 IU 112.5 IU 112.5 IU 75 IU 75 IU 35 1 2 6 12 step-up 14 mm foll. sonra step-down

43
Doz Düşürülmesi Hugues, et al. Hum Reprod 2006

44
GnRH Ant: OI, PCOS

45
Metformin + FSH vs FSH: OI POS CLD step-up
Moll E et al. Hum. Reprod. Update 2007;13: Yarali et al., 2002; Tasdemir et al., 2004; Palomba et al., 2005; van Santbrink et al., 2005

46
Metformin + FSH vs FSH: OI POS CLD step-up
Figure 3 Results of FSH ovulation induction using a low-dose step-up protocol in 17 normogonadotropic insulin-resistant anovulatory subfertile patients after randomization and co-treatment with metformin or placebo (n = 7). Results of FSH ovulation induction using a low-dose step-up protocol in 17 normogonadotropic insulin-resistant anovulatory subfertile patients after randomization and co-treatment with metformin or placebo (n = 7). van Santbrink E J P et al. Eur J Endocrinol 2005;152:
. Results of FSH ovulation induction using a low-dose step-up protocol in 17 normogonadotropic insulin-resistant anovulatory subfertile patients after randomization and co-treatment with metformin or placebo (n = 7). van Santbrink E J P et al. Eur J Endocrinol 2005;152:")
47
5. Recombinant FSH versus urinary Gonadotrophins ( van Wely et al

48
rFSH vs uFSH: PCOS OI Outcome or subgroup title Statistical method
Studies Participant Statistical method Effect size 1 Ovulation rate (per cycle) 2 457 Peto Odds Ratio (Peto, Fixed, 95% CI) 1.19 [0.78, 1.80] 2 Pregnancy rate (per patient) 3 445 0.95 [0.64, 1.41] 3 Miscarriage rate (per pregnancy) 172 1.26 [0.59, 2.70] 4 OHSS rate (per patient) 1.55 [0.50, 4.84] 5 Multiple pregnancy rate (per pregnancy) 0.44 [0.16, 1.21] 6 Mean duration of stimulation (days) 1 96 Mean Difference (IV, Fixed, 95% CI) -0.32 [-2.95, 2.31] Bayram et al Cochrane Review
 Peto Odds Ratio (Peto, Fixed, 95% CI) 1.19 [0.78, 1.80] 2 Pregnancy rate (per patient) [0.64, 1.41] 3 Miscarriage rate (per pregnancy) [0.59, 2.70] 4 OHSS rate (per patient) 1.55 [0.50, 4.84] 5 Multiple pregnancy rate (per pregnancy) 0.44 [0.16, 1.21] 6 Mean duration of stimulation (days) Mean Difference (IV, Fixed, 95% CI) [-2.95, 2.31] Bayram et al Cochrane Review.")
49
Siklus İptal Endikasyonları
> 2 follikül >16 mm >1 folliküle >16 mm + 2 follikül >14 mm, >Serum E pg/mL

50
Sonuç-I CC dirençli hastalarda düşük doz step-up protokolü daha güvenilirdir. PCOS’ lu hastalarda FSH eşik değerini belirlemek için gonadotropin uygulamalarında düşük doz step-up protokolü ilk seçenek olmalıdır. Başlangıç Gonadotropin dozu hastanın prediktif özelliklerine göre ayarlanmalıdır. Düşük doz step-up protokolünün en önemli dezavantajı uzamış tedavi süresidir 50

51
Sonuç-II Takip eden sikluslarda step-up protokollere başlangıç dozu, cevap alınan dozun 25 veya 37.5 IU altı olmalıdır. Düşük doz step-down protokol dirençli hastalar için uygun yaklaşım olabilir ve cevap alınan dozun IU üstü doz ile başlanır. 51

52
TEŞEKKÜRLER

Benzer bir sunumlar



>")








>")







