Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Laparoskopik Ovarian Drilling
Prof.Dr. Cem Atabekoğlu Ankara Üniversitesi Tıp Fakültesi

2
PCOS /Cerrahi Tedavi PCOS ta ilk cerrahi tedavi 1935 yılında Stein ve Leventhal tarafından tanımlanmıştır. arasında tek tedavi seçeneği İlk sonuçlar umut verici olsa da Adezyon Doku kaybı Medikal tedavinin çok olumlu sonuçlar vermesi nedenleri ile terk edilmiştir. Stein,6 in his initial study of a group of women with amenorrhea, noted that they had bilateral polycystic ovaries at the time of laparotomy. He originally performed ovarian wedge biopsies in the hope of discovering the cause of their amenorrhea. The surgery failed to determine the cause of the amenorrhea but produced the unexpected results of regular menses and pregnancies. This finding lead to his study of the wedge resection as a fertility procedure.7

3
Cerrahi Tedavide Güncel Yaklaşım
Laparoskopik Overyan Diatermi (LOD) 1984 Gjönnaess ilk olarak tanımlamıştır. Ovulasyon oranı %90 Gebelik oranı %58 Saleh and Khalil [7] reviewed 18 articles related to this topic and stated that there was no statistically significant difference in the ovulation rates between LOD electrocoagulation and laser. They found significantly higher cumulative pregnancy rates, however, in women treated with electrocoagulation after a 1-year period [65% compared with 54.5%; odds ratio (OR) = 1.5; 95% confidence interval (CI) 1.1–2.1].
 1984 Gjönnaess ilk olarak tanımlamıştır. Ovulasyon oranı %90. Gebelik oranı %58. Saleh. and Khalil [7] reviewed 18 articles related to this topic. and stated that there was no statistically significant. difference in the ovulation rates between LOD electrocoagulation. and laser. They found significantly higher. cumulative pregnancy rates, however, in women treated. with electrocoagulation after a 1-year period [65% compared. with 54.5%; odds ratio (OR) = 1.5; 95% confidence. interval (CI) 1.1–2.1].")
4
PCOS infertilite tedavisi
CC ilk seçenektir. Ucuz, Güvenilir, Kolay uygulanır %60-85 ovulasyon, %30-40 gebelik Kousta E, Hum Reprod Update 1997; 3:359 %15-40 hasta CC karşı dirençlidir. Hughes E, Cochrane Database Syst Rev 2000 Pritts EA. Obstet Gynecol Surv 2002;

5
CC dirençli hastada yaklaşım
Metformin Gonadotropinler Cerrahi tedavi Gonadotropin treatment requires a high degree of skill, and extensive hormone and ultrasound monitoring in PCOS, because follicular response tends to be slow initially, but explosive at later stages of stimulation. Surgical treatment of infertile women with PCOS has reemerged as an alternative to gonadotropins in women who are clomiphene citrate-resistant as a result of major advances in laparoscopic surgery.

6
Laparoskopik Overyan Diatermi (LOD) Reprodüktif Ronuçlar
Unlu & Atabekoglu. Curr Opin Obstet Gynecol 2006

7
The Cochrane Library 2012, Issue 6

8
LOD İnfertilite Tedavisi Mekanizma
Androjenlerin Kritik Rolü

9
Serbest E2↑ Testosteron↑ Östron↑ SHBG↓ Serbest T↑
Yüksek Östrojenik Ortam Serbest T↑ Östron↑ Periferik aromatizasyon GnRh’a Hipofizer sensivite artışı (Reseptör artışı) (- ) feedback NEJM 352;12:24 ,2005
 (- ) feedback. NEJM 352;12:24 ,2005.")
10
Azalmış opioid inhibisyonu
Anovulasyon Düşük Progesteron Düzeyi

11
LOD İnfertilite Tedavisi Mekanizma
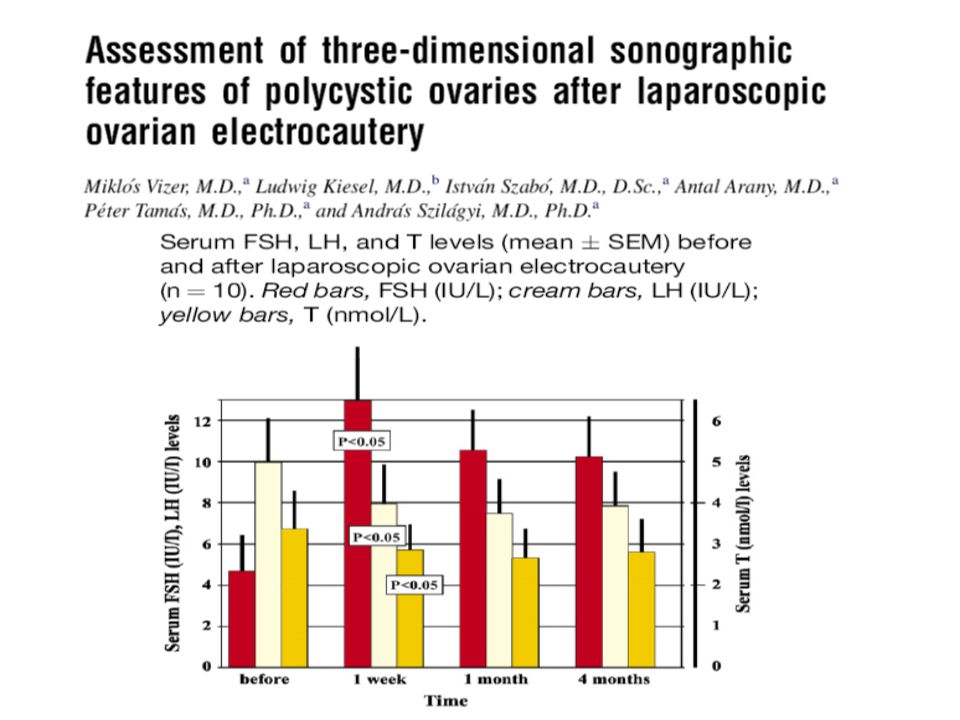
Androjenik mikro çevrenin foliküler gelişim üzerine olumsuz etkisi düzeltilir Estrojenik ortam folikülün gelişimine olanak sağlar Androjenik substrartın azalması periferal aromatizasyon ile östrojen oluşumunu azaltır Bu hormonal değişiklik hipotalamo-hipofiz-over aksının yeniden düzenlenmesine yol açar Operasyon sonrası azalan inhibin seviyesi FSH düzeyindeki artıma yardımcıdır.

13
Vizer et al.

14
İnsülinin Hücre İçindeki Etkisi
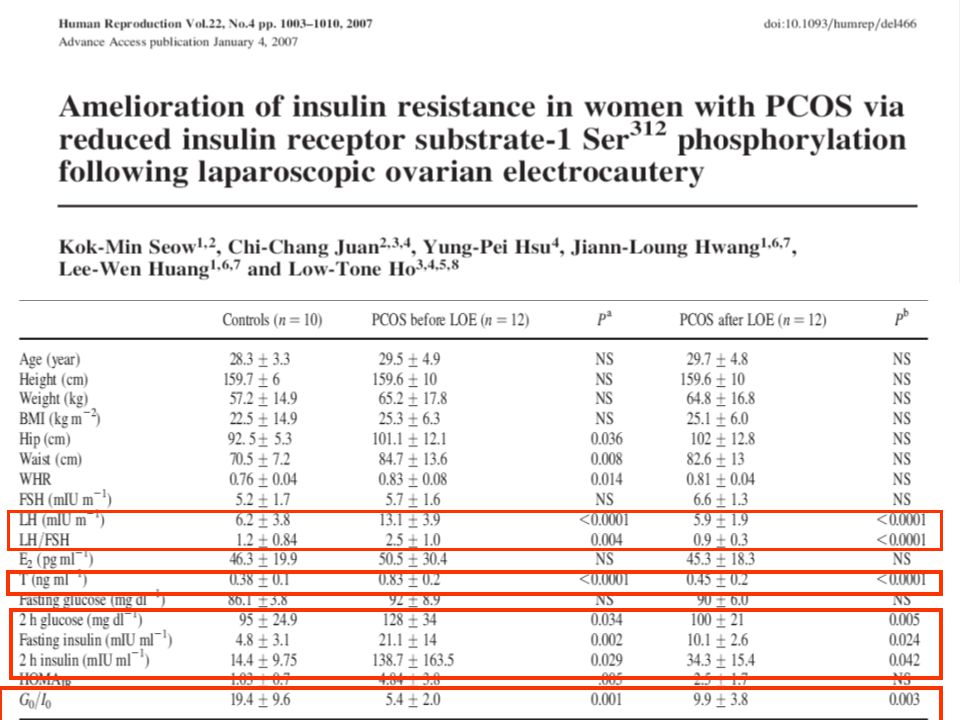
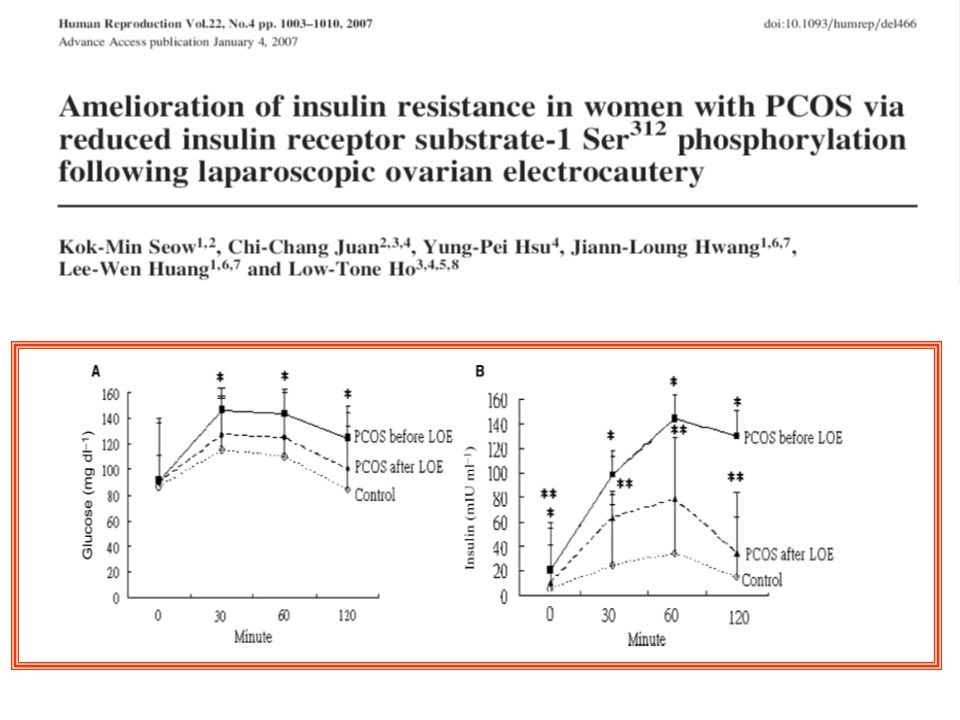
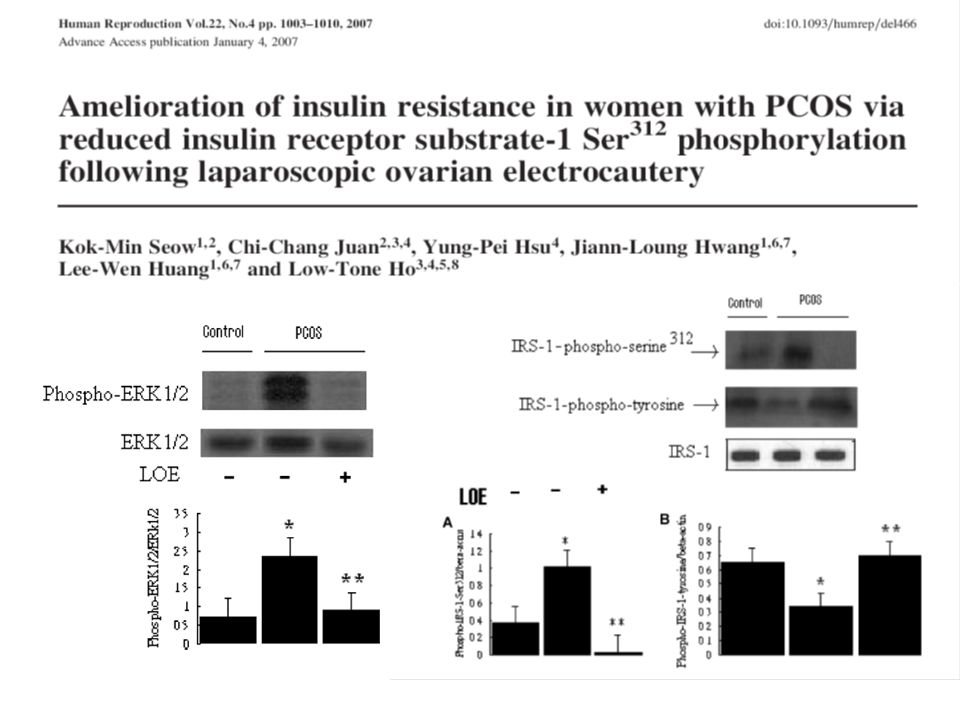
subünitler subünitler -P P- ATP IRS Tyr ADP İnsülin molekülü İnsülin bağlanma bölgesi P Hücre dışı Hücre içi Membran MAP kinaz yolu Fosfotidilinositol-3 kinaz yolu + Tirozin kinaz İnsülin etkisi PCOS manifests a post-binding defect in insulin signaling in adipocyte and decreased activity of PI3-kinase in muscle biopsies during euglycemic hyperinsulinaemic clamps. Dunaif et al. (1995) reported that the impaired action of insulin on glycogen synthesis in cultured skin fibroblasts from POCS women is associated with constitutively increased insulin receptor (IR)b-subunit serine phosphorylation and decreased insulin receptor tyrosine kinase activity. In addition, Corbould et al. (2005) showed that in cultured skeletal muscle cells from PCOS women Ser312 phosphorylation of IRS-1 is constitutively increased. Furthermore, MAPK activity that is constitutively increased in the skeletal muscle of women with PCOS (Corbould et al., 2006) suggests that ERK1/2 or ERK-regulated kinases are responsible for the increased Ser312 phosphorylation of IRS-1. These observations provide strong support for the hypothesis that increased Ser312 phosphorylation is an important mechanism for insulin resistance in PCOS. Glukoz transport proteini (GLUT-4)
 reported that the impaired action of insulin on glycogen synthesis in cultured skin fibroblasts from POCS women is associated with constitutively increased insulin receptor (IR)b-subunit serine phosphorylation and decreased insulin receptor tyrosine kinase activity. In addition, Corbould et al. (2005) showed that in cultured skeletal muscle cells from PCOS women Ser312 phosphorylation of IRS-1 is constitutively increased. Furthermore, MAPK activity that is constitutively increased in the skeletal muscle of women with PCOS (Corbould et al., 2006) suggests that ERK1/2 or ERK-regulated kinases are responsible for the increased Ser312 phosphorylation of IRS-1. These observations provide strong support for the hypothesis that increased Ser312 phosphorylation is an important mechanism for insulin resistance in PCOS. Glukoz transport proteini (GLUT-4)")
15
İnsülinin Hücre İçindeki Etkisi
There is experimental evidence to indicate that in women with polycystic ovaries, the peripheral insulin resistance is due to a defect beyond activation of the receptor kinase, specifically leading to reduced tyrosine autophosphorylation of the insulin receptor. The phosphorylation of serine and threonine residues on the insulin receptor reduces signal transmission, and excessive serine phosphorylation (by a mechanism extrinsic to the insulin receptor) has been demonstrated as a possible postreceptor defect in these patients, changing signal transduction. It has been suggested that serine phosphorylation of the beta chain of the insulin receptor and at the same time of the adrenal and ovarian P450c17 enzyme (the origin or cause of serine phosphorylation is uncertain, but presumably it would have a genetic basis) would explain both the hyperinsulinemia and hyperandrogenism (serine phosphorylation increases 17,20-lyase activity and androgen production). Stated simply, serine instead of tyrosine phosphorylation is an “off” mechanism for glucose transport but an “on” mechanism for P450c17 enzyme activity. This change in phosphorylation would be consistent with no abnormality in the number of receptors or in receptor function; the impaired insulin signal for glucose transport would be due to a postreceptor problem.
 has been demonstrated as a possible postreceptor defect in these patients, changing signal transduction. It has been suggested that serine phosphorylation of the beta chain of the insulin receptor and at the same time of the adrenal and ovarian P450c17 enzyme (the origin or cause of serine phosphorylation is uncertain, but presumably it would have a genetic basis) would explain both the hyperinsulinemia and hyperandrogenism (serine phosphorylation increases 17,20-lyase activity and androgen production). Stated simply, serine instead of tyrosine phosphorylation is an off mechanism for glucose transport but an on mechanism for P450c17 enzyme activity. This change in phosphorylation would be consistent with no abnormality in the number of receptors or in receptor function; the impaired insulin signal for glucose transport would be due to a postreceptor problem.")
16
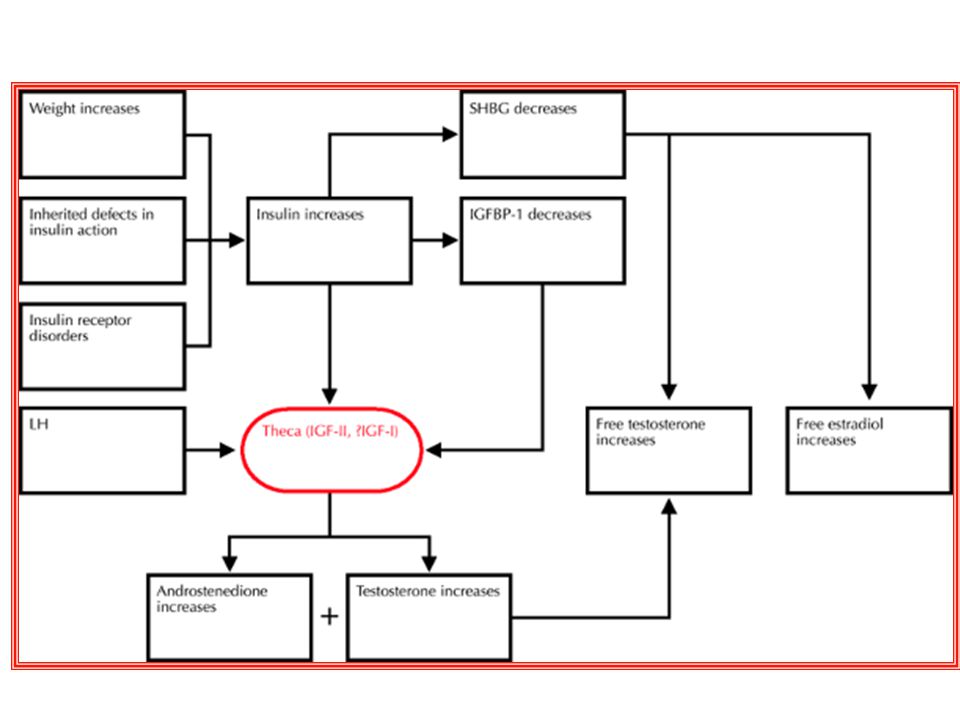
İnsülin İnsulin LH ile sinerjik etki gösterir ve teka hücrelerinde androjen sentezini arttırır.(hem kendi hem de IGF-1 reseptörü aracılığı ile) P450c17 sisteminde hiper aktivasyona yol açar İnsulin hepatik SHBG sentezini inhibe eder free testosteron artar IGFBP-1 in hepatik üretimini azaltır. Serin fosforilasyonu ile 17alfa hidroksilaz ve 17,20 liyaz aktivite artışı androjen artışına katkıda bulunur. Insulin plays both direct and indirect roles in the pathogenesis of hyperandrogenemia in the polycystic ovary syndrome (Fig. 2). Insulin acts synergistically with luteinizing hormone to enhance the androgen production of theca cells. Insulin also inhibits hepatic synthesis of sex hormone–binding globulin, the key circulating protein that binds to testosterone, and thus increases the proportion of testosterone that circulates in the unbound, biologically available, or free, state. Because women with the polycystic ovary syndrome typically have hyperinsulinemia, the concentration of free testosterone is often elevated when the total testosterone concentration is at the upper range of normal or only modestly elevated.
. Insulin acts synergistically. with luteinizing hormone to enhance the. androgen production of theca cells. Insulin also inhibits. hepatic synthesis of sex hormone–binding. globulin, the key circulating protein that binds to. testosterone, and thus increases the proportion of. testosterone that circulates in the unbound, biologically. available, or free, state. Because women with. the polycystic ovary syndrome typically have hyperinsulinemia, the concentration of free testosterone. is often elevated when the total testosterone concentration. is at the upper range of normal or only. modestly elevated.")
21
LOD Ne Kadar Girişim ve Termal Enerji Gereklidir?
Kişiselleştirilmelidir Mümkün olan en az uygulama yapılmalıdır. 4 girişim 5 sn 30 W optimal Amer SA, Hum Reprod 2003; 18:1693–1698. Fazla sayıda girişim ve enerji overyan rezervin kaybına yol açabilir. 8 girişim 400 W Dabirashrafi H. Fertil Steril 1989; 52:878–879. Yüksek miktarda girişim ve enerji peri-overyan adezyonlara yol açabilir!!!

22
Cauterization of ovaries was performed as recommended
by Gjoannaess2 by using a unipolar current (300 W to 400 W, 5 to 6 seconds at each point). Tabrizi NM,JSLS 2005
. Tabrizi NM,JSLS")
23
30 W – 5 Sn 150 J/puncture. Amer SA, Hum Reprod 2003

24
in these women, improving their clinical and reproductive outcome.
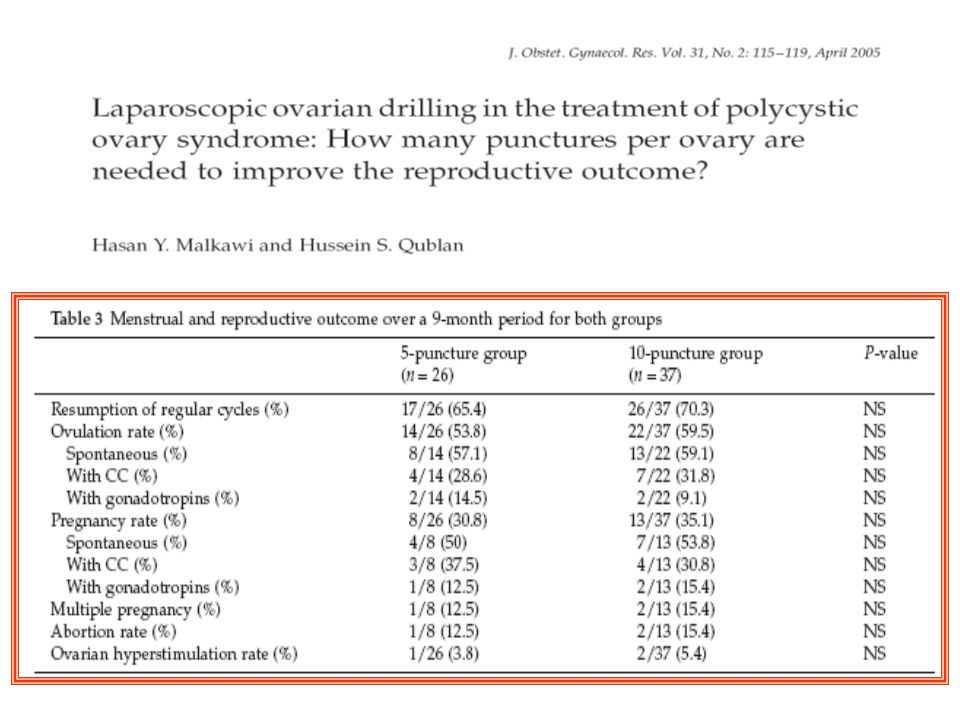
Conclusion: Laparoscopic ovarian drilling is an effective treatment in clomiphene-citrate-resistant women with PCOS. Five, instead of ≥10, punctures per ovary are sufficient to ameliorate the hyperandrogenic status in these women, improving their clinical and reproductive outcome. 40 W-2-3 sn

26
In conclusion, LOD using a thermal dose of 60 J/cm3 has a better
reproductive outcome compared with fixed thermal dosage of 600 J per ovary in treatment of patients with PCOS with CC resistance. Large powered studies are needed to demonstrate the effect of this dosage on potential risks of adnexal adhesions and ovarian failure.

27
LAZER / ELEKTROKOTER Elektrokoter sonuçları lazere üstündür!!!
Elektrokoter Lazer OR Kümülatif Gebelik oranı % % (CI ) Saleh AM. Acta Obstet Gynecol Scand 2004
 Saleh AM. Acta Obstet Gynecol Scand")
28
Lazerin dezavantajları
Sadece 2-4 mm termal penetrasyon yapar. Over yüzeyinde daha fazla hasar ve adezyon oluşumuna yol açar Sekond look sonuçları adezyon oluşumu Lazer %41.5 Elektrokoter %31 Felemban A, Tulandi T.. Infertil Reprod Med Clin North Am 2000; 11:49–60. CO2 lazer Nd:YAG lazere göre daha fazla adezyon oluşturur

29
Ünilateral / Bilateral
The Cochrane Library 2012, Issue 6

32
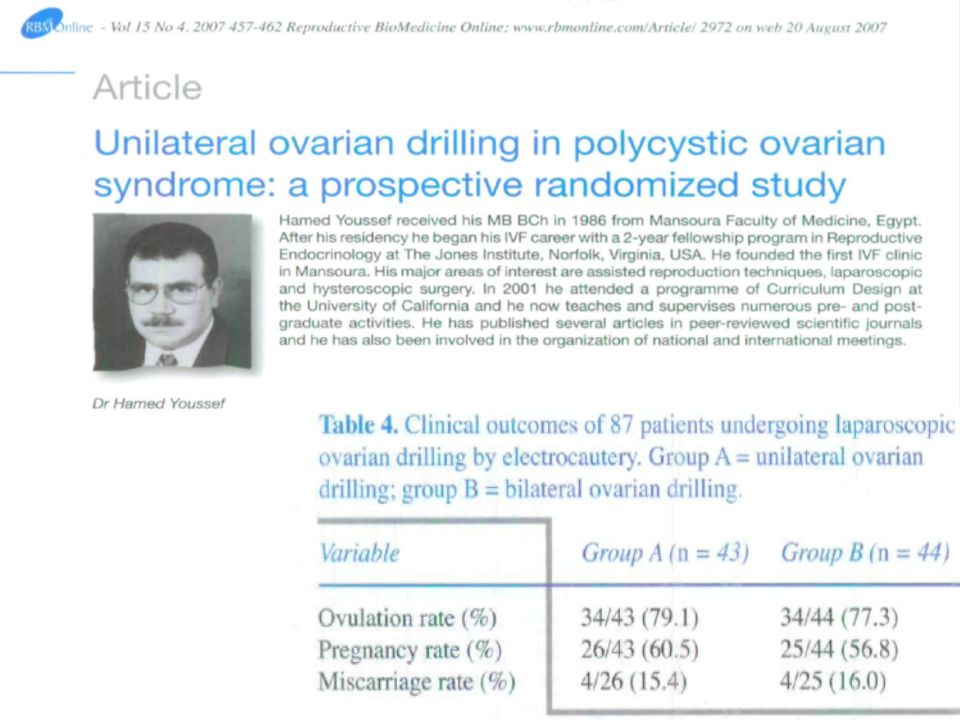
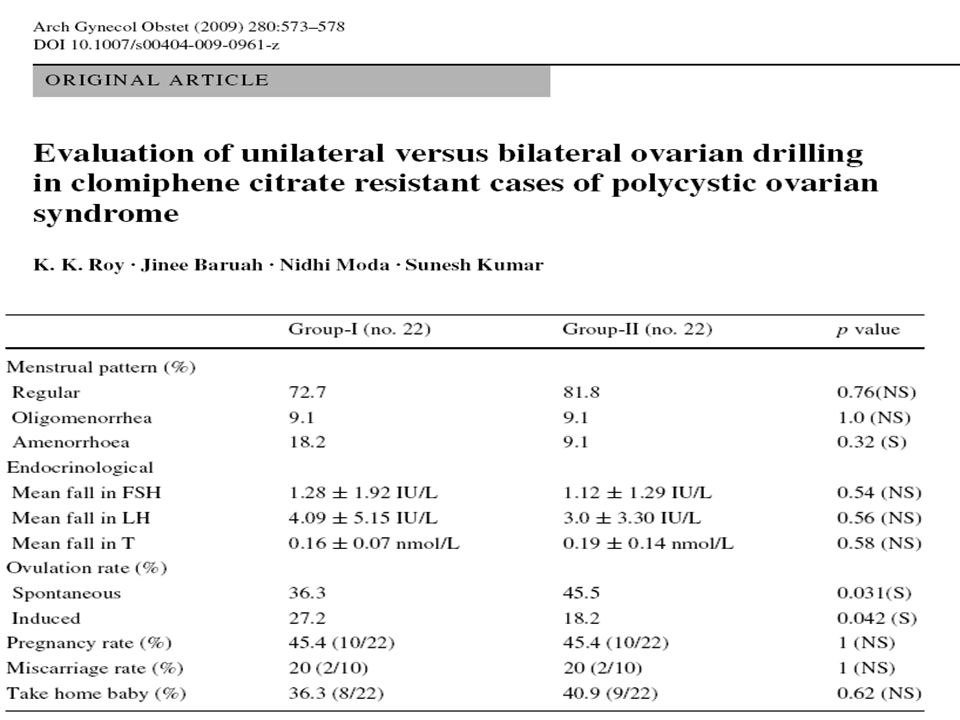
participants/materials, setting, methods: Patients were assigned to two groups; one group underwent laparoscopic ovarian drilling of the right ovary alone, while both ovaries were treated in the second group. The ULOD group (n ¼ 49) received thermal doses adjusted to the volume of the right ovary (60 J/cm3). The BLOD group (n ¼ 47) received fixed doses of 600 J per ovary, regardless of its volume. The two treatment groups were matched by the number of participants, age and baseline parameters. main results and the role of chance: The ovulation rate during the first menstrual cycle after LOD was significantly higher in the ULODgroup than in the BLODgroup [73 versus 49%; absolute risk reduction (ARR), 20.25; 95% confidence interval (CI), to 20.03; P ¼ 0.014]. Treatment withULODon the right ovary significantly increased the chances of ovulation in patients with a larger right ovary compared with those who had a smaller right ovary (100 versus 36%; ARR, 20.64; 95% CI, to 20.37; P ¼ 0.004). Interestingly, the chances of ovulationwere also significantly higher in patients in the BLODgroup who had a larger right ovary compared with those who had a smaller right ovary (88 versus 33%; ARR, 20.55; 95% CI, to 20.28; P ¼ 0.002). The pregnancy rate was also significantly higher in patients with a larger right ovary compared with those with a smaller right ovary, regardless of the treatment group. Unilateral treatment induces activity in both ovaries (Balen and Jacobs, 1994) and minimizes procedure time as well as the risk of post-operative adhesions and ovarian tissue damage.
 received thermal. doses adjusted to the volume of the right ovary (60 J/cm3). The BLOD group (n ¼ 47) received fixed doses of 600 J per ovary, regardless of. its volume. The two treatment groups were matched by the number of participants, age and baseline parameters. main results and the role of chance: The ovulation rate during the first menstrual cycle after LOD was significantly higher in. the ULODgroup than in the BLODgroup [73 versus 49%; absolute risk reduction (ARR), 20.25; 95% confidence interval (CI), to 20.03; P ¼ 0.014]. Treatment withULODon the right ovary significantly increased the chances of ovulation in patients with a larger right ovary compared. with those who had a smaller right ovary (100 versus 36%; ARR, 20.64; 95% CI, to 20.37; P ¼ 0.004). Interestingly, the chances of ovulationwere. also significantly higher in patients in the BLODgroup who had a larger right ovary compared with those who had a smaller right ovary. (88 versus 33%; ARR, 20.55; 95% CI, to 20.28; P ¼ 0.002). The pregnancy rate was also significantly higher in patients with a larger right. ovary compared with those with a smaller right ovary, regardless of the treatment group. Unilateral treatment induces activity in both ovaries (Balen and Jacobs, 1994) and minimizes procedure time as well as the risk of post-operative. adhesions and ovarian tissue damage.")
33
LOD de başarısızlık %20-30 anovulasyon devam eder.
Obezite (BMI) >35 kg/m2 Belirgin hiperandrojenizm free androgen index ≥15 Testosteron >4.5 nmol/l. İnfertilite süresinin >3 yıl olması Amer SA,Hum Reprod 2004; 19:1719 Düşük LH/FSF oranı (<2) Operasyon öncesi düşük glukoz seviyesi Erken menarş persistan anovulasyonu olasılığı artar ancak hiçbir tedavi başarısızlığını predikte etmez van Wely M, Hum Reprod 2005;20:900 The authors reported that the presence or absence of acne, the menstrual pattern, luteinizing hormone/FSH ratio and ovarian volume did not influence the outcome of LOD. PCOS. They did not find any correlation between either the androgen levels or the BMI with ovarian response following laparoscopic electrocautery. According to the authors, women who had early menarche, low luteinizing hormone/FSH ratios and low glucose levels before the operation were more likely to have persistent anovulation. Luteinizing hormone/FSH level was found to be the strongest predictor of ovarian response after electrocautery. It was shown that women with a luteinizing hormone/FSH ratio below 2 were more likely to be anovulatory after operation. Women with a higher luteinizing hormone/ FSH ratio were more likely to ovulate and would be more relevant for clinical practice. Although van Wely et al. [17••]
 >35 kg/m2. Belirgin hiperandrojenizm. free androgen index ≥15. Testosteron >4.5 nmol/l. İnfertilite süresinin >3 yıl olması. Amer SA,Hum Reprod 2004; 19:1719. Düşük LH/FSF oranı (<2) Operasyon öncesi düşük glukoz seviyesi. Erken menarş. persistan anovulasyonu olasılığı artar ancak hiçbir tedavi başarısızlığını predikte etmez. van Wely M, Hum Reprod 2005;20:900. The authors reported that the presence. or absence of acne, the menstrual pattern, luteinizing hormone/FSH ratio and ovarian volume did. not influence the outcome of LOD. PCOS. They did not find. any correlation between either the androgen levels or. the BMI with ovarian response following laparoscopic. electrocautery. According to the authors, women who. had early menarche, low luteinizing hormone/FSH. ratios and low glucose levels before the operation were. more likely to have persistent anovulation. Luteinizing. hormone/FSH level was found to be the strongest predictor. of ovarian response after electrocautery. It was. shown that women with a luteinizing hormone/FSH. ratio below 2 were more likely to be anovulatory after. operation. Women with a higher luteinizing hormone/ FSH ratio were more likely to ovulate and would be. more relevant for clinical practice. Although van Wely. et al. [17••]")
34
LOD de başarısızlık YAŞ <25 25-29 30-35 >35 Ovulasyon Gebelik
23/34 %67.6 77/111 %69.4 36/52 %69.2 9/57 %15.8* Gebelik 6/34 (%17.6) 18/111 (%16.2) 8/52 (%15.4) 1/57 %1.8* Kümülatif gebelik 6/9 %66.7 18/28 %64.3 8/13 %61.5 1/10 %10.0* Abortus 1/6 %16.7 3/18 1/8 %12.5 1/1 %100.0* Specifically, female age is the better predictor of oocyte quality, whereas basal FSH level is the better predictor of oocyte quantity Palomba et al. Gynecological Endocrinology, 2006; 22(6): 329–335
 18/111. (%16.2) 8/52. (%15.4) 1/57. %1.8* Kümülatif gebelik. 6/9. % /28. % /13. % /10. %10.0* Abortus. 1/6. % /18. 1/8. % /1. %100.0* Specifically, female. age is the better predictor of oocyte quality, whereas. basal FSH level is the better predictor of oocyte. quantity. Palomba et al. Gynecological Endocrinology, 2006; 22(6): 329–335.")
35
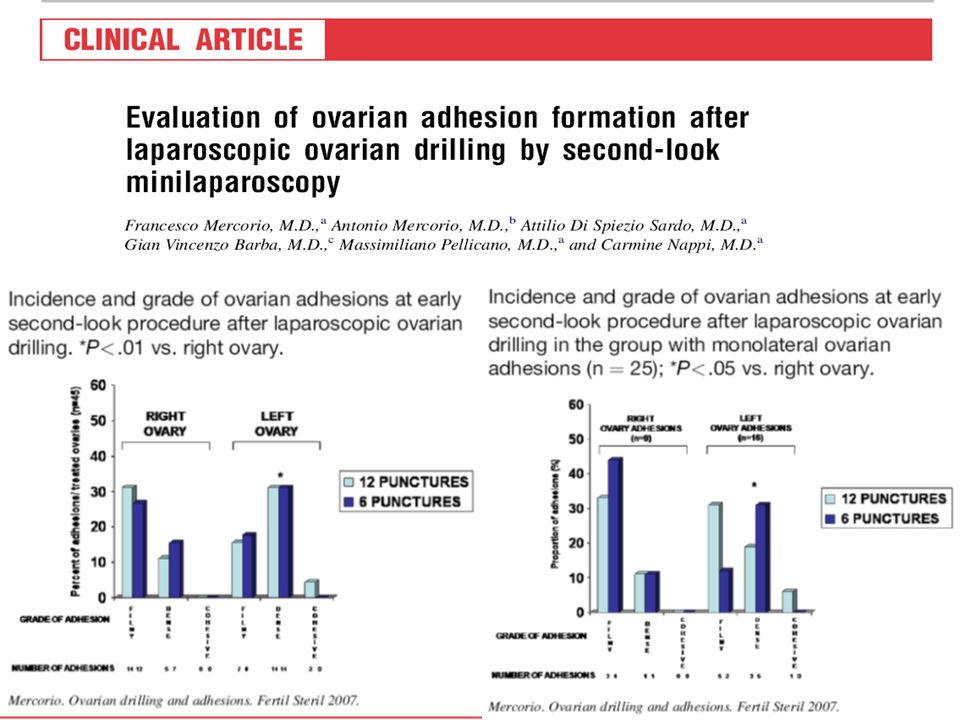
LOD Postoperatif Adezyon
%18-%82 C/S , İnfertilite Genellikle hafif reprodüktif potansiyeli etkilemiyecek derecede Peritoneal lavaj adezyon formasyonunu azaltıyor Sol overde daha fazla

37
GONADOTROPİN Ovulatuar siklus % 70 Kümülatif gebelik oranı % 55
van Santbrinket al., 1995 White et al., 1996 Mulders et al., 2003 DEZAVANTAJ Çoğul gebelik >%10 OHSS Siklus iptali

38
CC dirençli hastalarda tedavide Gonadotropin/LOD
3-6 siklus FSH kullanımlarında 6. aya kadar gebelik oranları gonadotropin kullanımı lehine (OR = 0.48, 95% CI 0.28–0.81). 12 aylık sonuçlar benzer (OR = 1.27,95% CI 0.77–2.09) Farquhar CM. Best Pract Res Clin Obstet Gynaecol 2004
. 12 aylık sonuçlar benzer (OR = 1.27,95% CI 0.77–2.09) Farquhar CM. Best Pract Res Clin Obstet Gynaecol")
39
CC dirençli hastalarda tedavide Gonadotropin/LOD
Çoğul gebelik Farquhar CM. Best Pract Res Clin Obstet Gynaecol 2004

40
OHSS!!!!! CC dirençli hastalarda tedavide Gonadotropin/LOD
Very recently, in a randomized controlled clinical trial, Bayram et al. [20] compared the effectiveness of an electrocautery strategy with ovulation induction using recombinant follicle-stimulating hormone (rFSH) in patients with clomiphene citrateresistant PCOS. If anovulation persisted 8 weeks after the operation, clomiphene citrate was used at first for six cycles. If the patient remained anovulatory, rFSH treatment was started. The cumulative rate of ongoing pregnancy was found to be 67% at 12 months in both groups. Nevertheless, the ongoing pregnancy rate after 6 months was lower with electrocautery than with rFSH, and approximately more than half the patients had to receive clomiphene citrate and rFSH. Since all multiple- pregnancies were found in patients who received rFSH, the authors proposed that multiple pregnancies could largely be avoided by electrocautery and clomiphene citrate before this treatment. OHSS!!!!! Bayram N , BMJ 2004
 in patients with clomiphene citrateresistant. PCOS. If anovulation persisted 8 weeks after. the operation, clomiphene citrate was used at first for. six cycles. If the patient remained anovulatory, rFSH. treatment was started. The cumulative rate of ongoing. pregnancy was found to be 67% at 12 months in both. groups. Nevertheless, the ongoing pregnancy rate after. 6 months was lower with electrocautery than with rFSH, and approximately more than half the patients had to. receive clomiphene citrate and rFSH. Since all multiple- pregnancies were found in patients who received. rFSH, the authors proposed that multiple pregnancies. could largely be avoided by electrocautery and clomiphene. citrate before this treatment. OHSS!!!!! Bayram N , BMJ")
41
CC dirençli hastalarda tedavide Gonadotropin/LOD
LOD maliyet etkin M.van Wely Human Reproduction 2004

42
CC dirençli hastalarda tedavide Gonadotropin/LOD
LOD maliyet/etkin Reprodüktif performans ve hormonal etki ve menstrual regülarite LOD de yıllar boyu sürmekte yıl Gjonnaess H. Fertil Steril 1998; 69:697–701. LOD uygulana hastalarda takip eden Oİ daha kolay LOD geçiren hastalarda Gonadotropinler kullanıldığında süre, total doz azalırken gebelik oranları yükseliyor Pirwany I, Fertil Steril 2003; 80:241–251. IVF hastalarında LOD geçiren grupta ciddi OHSS oranı ve bu nedenle siklus iptal oranı az bulunmuş Rimington Hum Reprod 1997; 12:1443–1447.

43
CC Dirençli Hastalarda Tedavide Metformin/LOD
PCOS’lu hastaların %50-80’inde insülin rezistansı var. Teka hücrelerinde insülin ve LH androjen üretiminde sinerjik etkili. Metformin insan teka hücrelerinde androjen üretimini direkt olarak inhibe ediyor. CC-rezistan hastalarda CC kombine edildiğinde LOD benzer şekilde %80 ovulasyon bildirilmiştir. Malkawi HY, J Obstet Gynaecol 2003

44
CC dirençli hastalarda tedavide Metformin/LOD

45
CC dirençli hastalarda tedavide Metformin/LOD

46
CC Dirençli Hastalarda Tedavide Metformin/LOD RCT
LOD+plasebo Metformin +Diag L/S Ovulasyon %54.8 % 53.3 Gebelik /siklus % 13.4 % 21.8 Gebelik kümülatif %56.4 % 72.2 Abortus % 29.0 %9.3 Canlı doğum(gebelik başına) %64.5 %82.1 Palomba et al. [33••] compared the effectiveness of LOD with metformin administration for the treatment of clomiphene citrate-resistant women with PCOS in a RCT. The first group underwent only diagnostic laparoscopy and were treated for 6 months with metformin (850 mg twice daily) after the operation. The second group underwent LOD and received placebo for 6 months. After 6 months of metformin or placebo treatment in women who did not achieve ovulation, clomiphene citrate was administered by the authors at doses of 150 mg daily five times from day 3 to day 7 of cycles. At the end of the study, although there were no statistically significant differences between the groups according to the total ovulation rate (54.8% compared with 53.2%, respectively), the pregnancy rate per cycle was found to be significantly higher in the first group (21.8% compared with 13.4%). The abortion rate was also found to be lower in the metformin group than the LOD group (9.3% compared with 29.0%, respectively). After six cycles of treatment, the cumulative pregnancy rate was found to be 72.2% (39 of 54) in the metformin group, whereas it was 56.4% (31 of 55) in the LOD group. Besides these reproductive outcomes, the authors also compared the cost–benefit between the Palomba S, J Clin Endocrinol Metab 2004; 89:4801
 %64.5. %82.1. Palomba et al. [33••] compared the effectiveness. of LOD with metformin administration for the. treatment of clomiphene citrate-resistant women with. PCOS in a RCT. The first group underwent only diagnostic. laparoscopy and were treated for 6 months with. metformin (850 mg twice daily) after the operation. The second group underwent LOD and received placebo. for 6 months. After 6 months of metformin or. placebo treatment in women who did not achieve ovulation, clomiphene citrate was administered by the authors. at doses of 150 mg daily five times from day 3 to day 7 of. cycles. At the end of the study, although there were no. statistically significant differences between the groups. according to the total ovulation rate (54.8% compared. with 53.2%, respectively), the pregnancy rate per cycle. was found to be significantly higher in the first group. (21.8% compared with 13.4%). The abortion rate was. also found to be lower in the metformin group than. the LOD group (9.3% compared with 29.0%, respectively). After six cycles of treatment, the cumulative. pregnancy rate was found to be 72.2% (39 of 54) in the. metformin group, whereas it was 56.4% (31 of 55) in the. LOD group. Besides these reproductive outcomes, the. authors also compared the cost–benefit between the. Palomba S, J Clin Endocrinol Metab 2004; 89:4801.")
47
CC Dirençli Hastalarda Tedavide Metformin/LOD RCT
Metformin 20 kat maliyet/etkin ilave olarak metformin genel anestezi ve L/S riskleri taşımıyor. CC rezistan hastalarda ilk seçenek olmalı Palomba S, J Clin Endocrinol Metab 2004; 89:4801

48
LOD sonrası Anovulatuar hastalarda tekrar CC tedavisi ile
%31.1 Ovulasyon (23/74 siklus) %16.2 gebelik
 %16.2 gebelik.")
51
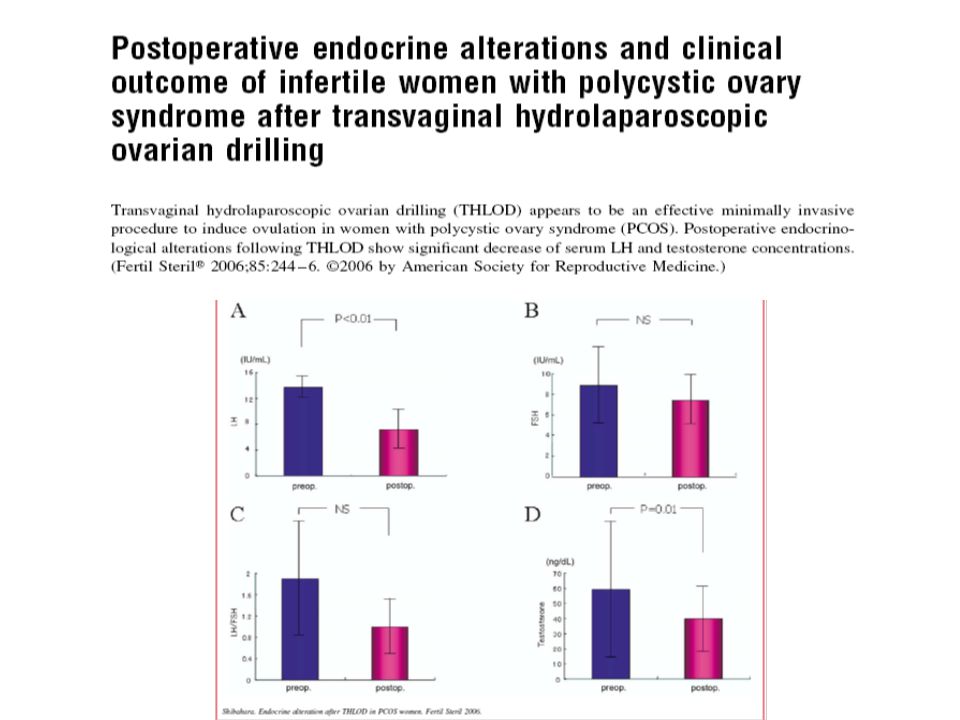
%86 regüler mens %36 6-aylık kümülaif gebelik BJOG 2006
Compared with transvaginal, ultrasound-guided follicular aspiration,13,14 this new procedure causes thermal effects not only on the intraovarian subcapsular follicles but also on intraovarian stromal tissue. Therefore, a reduced serum testosterone level follows the surgery, which further leads to a reduction of LH levels and LH/FSH ratios.

54
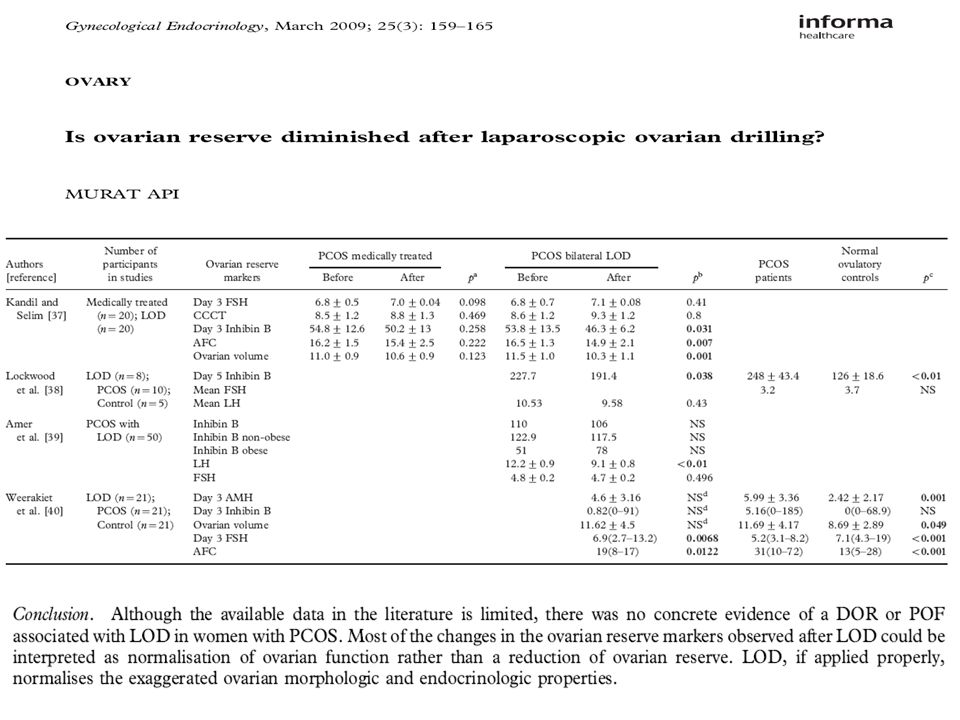
LOD ve Overyan rezerv

55
LOD ve Overyan rezerv

57
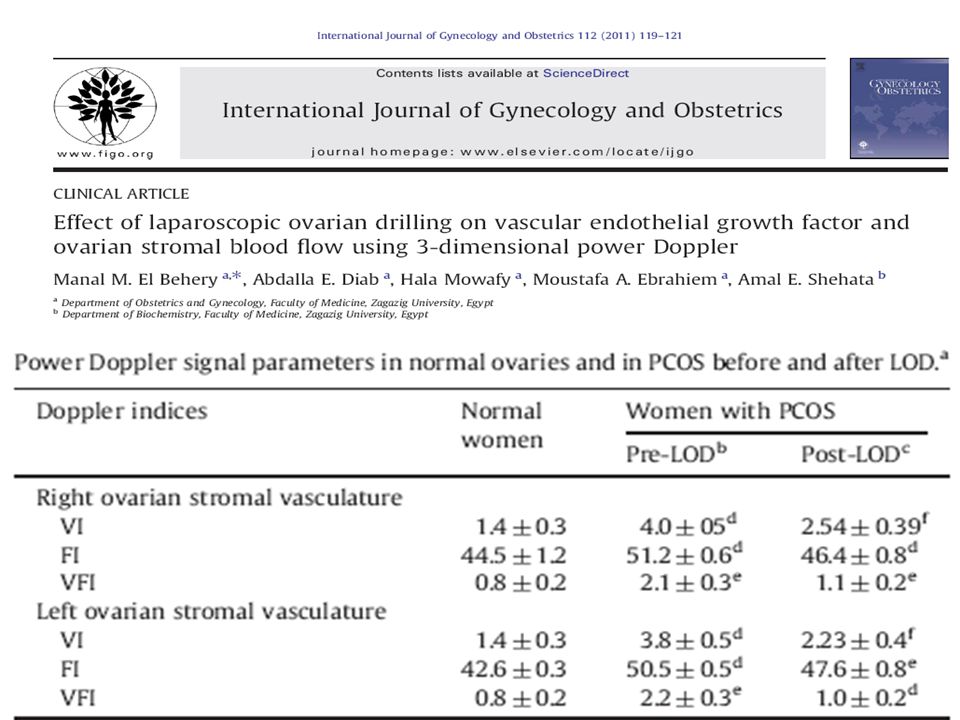
Fertil Steril 2011;95:2342–6.

59
IVF öncesi LOD LOD sonrası serumda VEGF ve IGF-1 seviyeleri azalmakta, over stroması kan akımı artmaktadır. Bu nedenle özellikle daha önce OHSS gelişmiş hastaların IVF tedavisinde bu işlem önerilmektedir

62
PCOS İnfertilite Tedavisi
Zayıflama ve Egzersiz Klomifen Sitrat Metformin + Klomifen Sitrat Gonodatropin LOD IVF

63
Androjenik Semptomları Düzeltilmesinde LOD Yeri
Konsensus yok Uzun süreli etkinlik avantajıdır. Daha fazla puncture veya overyan wedge rezeksiyon veya unilateral ooferektomi gerekli Diğer nedenle yapılmış operasyonlarda hirsutizmi olan vakalarda uygulanabilir. Premature overyan yetmezlik !!!

64
Sonuçlar I PCOS lu hastalarda infertilite tedavisinden CC ilk secenektir. CC dirençli hastalarda ilk seçenek olarak metformin tedavisi düşünülmelidir. Anovulasyonu devam eden hastalarda gonodatropin ve LOD seçenekleri tartışılmalıdır. LOD intraoveryan androjenik mikro çevreyi düzelterek hipatolamo-hipofiz-over aksını düzelterek etki gösterir. LOD insülin rezistansınada etkili olduğu gösterilmiştir.

65
Sonuçlar II LOD de tedavi kişiselleştirilmelidir ve mümkün olan en az uygulama yapılmalıdır. Obez, hiperandrojenizmi olan, 3 yıldan fazla infertilitesi olan, FSH >10 ve yaş >35 olan hastalarda başarı şansı azalmaktadır. Androjenik semptomların giderilmesinde konsensus yoktur. Başka endikasyon nedeni ile L/S yapılan hastalarda bu endikasyon için önerilebilir.

66
TEŞEKKÜRLER

Benzer bir sunumlar















>")






