Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
DÜNYADA VE TÜRKİYEDE TÜTÜN KULLANIMI VE KONTROLÜ
Prof.Dr.Zeki KILIÇASLAN

2
İKİ SALGIN SARS TÜTÜN SALGINI Ani öldürücü- Korkutucu.
Hızlı global cevap. Binlerce olgu- Yüzlerce ölüm. Temas ve seyahat ile yayılma. TÜTÜN SALGINI Yavaş öldürücü-kabul edilebilir. Geç global cevap. Milyarlarca olgu-Milyonlarca ölüm. Çok Uluslu Şirketler Tarafından yayılır.

3
Dünyada 1.1 milyar, Türkiye’de 17 milyon sigara içici

4
4.9 Milyon 2000 yılında sigaraya bağlanan ölüm:
The World Health Report 2002

5
10 milyonu bulacaktır. Dünya’ da her yıl 5 milyon insan
sigara nedeniyle yaşamını yitirmektedir. Önlem alınmazsa bu sayı önümüzdeki yirmi yılda 10 milyonu bulacaktır.

7
Politik ilgisizlik- (kazanç alanı) Önlemek ve bırakmak zor.
BU SALGIN NASIL OLUŞTU ? Nikotin ve Toksinler. Geç etki. Endüstri desteği. Politik ilgisizlik- (kazanç alanı) Önlemek ve bırakmak zor. Ph.Morris BAT JTI Chine National Tob.
 Önlemek ve bırakmak zor. Ph.Morris. BAT. JTI. Chine National Tob.")
8
Tütün endüstrisinin 2002-2004 yılı karları:
Kazanç (milyon $) Son 3 yılda büyüme British American Tobacco (BAT) 2095 %28.16 Japan Tobacco International (JTI) 710 %24.96 Altria (Philip Morris) 11 102 %13.72 Imperial Tobacco Group 424 %13.15 ALTADIS 541 %426.34 Source: Financial reports from the companies’ web pages. * Final results for 2002 for BAT, Altria and Imperial Tobacco Group.Final results for 2003 for JTI and Altadis. WHO exchange rates as of February 2004.
 Son 3 yılda büyüme. British American Tobacco (BAT) % Japan Tobacco International (JTI) 710. % Altria (Philip Morris) % Imperial Tobacco Group % ALTADIS % Source: Financial reports from the companies’ web pages. * Final results for 2002 for BAT, Altria and Imperial Tobacco Group.Final results for 2003 for JTI and Altadis. WHO exchange rates as of February")
9
Bazı Ülkelerde Sigara İçme Sıklığı (yetişkinler)
Erkek (%) Kadın (%) Çin (1984) 61 7 Japonya (1994) 59 (1966; 84) 15 (1966; 15) Kanada (1994) 29 (1966; 50) 31 (1966; 50) ABD (1993) 28 (1970; 44) 23 (1970; 32) Rusya Fed. (1993) 67 (1985; 53) 30 (1985; 10) Singapore (1995) 32 (1970; 42) 3 (1970; 5) Yunanistan (1994) 46 (1987; 61) 28 (1987; 25) İngiltere (1994) 28 (1980; 42) 26 (1980; 37) Türkiye (1993) 58 (1988; 62) 13 (1988; 24) DÜNYA 47 12
 Kadın (%) Çin (1984) Japonya (1994) 59 (1966; 84) 15 (1966; 15) Kanada (1994) 29 (1966; 50) 31 (1966; 50) ABD (1993) 28 (1970; 44) 23 (1970; 32) Rusya Fed. (1993) 67 (1985; 53) 30 (1985; 10) Singapore (1995) 32 (1970; 42) 3 (1970; 5) Yunanistan (1994) 46 (1987; 61) 28 (1987; 25) İngiltere (1994) 28 (1980; 42) 26 (1980; 37) Türkiye (1993) 58 (1988; 62) 13 (1988; 24) DÜNYA")
10
Bölge Tüketim Dünyada sigara içim oranları Kuzey Amerika % 4.7
Kuzey Amerika % 4.7 Latin Amerika % 8.9 Batı Avrupa % 9.3 Orta ve Doğu Avrupa % 10.8 Afrika ve Orta Doğu % 11.8 Asya % 54.5

12
Sigara ihracata hızla artırılmalıdır çünkü
Amerikan halkı giderek daha az sigara içmekte. Vice President- Dan Qauyle , 1990

14
Kovboy Çin Seddin de ??

20
Gelişmekte olan Ülkeler
Dünya tütün tüketiminde payı % 71 % 61 % 41 1976 1984 2000

21
Pazarlar arası artış Global artış ( %) Asya’da - 33%
 Asya’da - 33%")
22
3 1990 2025 10 Gelişmekte olan ülkeler Global Yıllık Mortalite
7 milyon 7 milyon 3 Gelişmekte olan ülkeler 3 milyon

23
Sigara alışkanlığı eğitim düzeyi düşük kişilerde daha yaygındır (Hindistan 1997)
")
26
Bazı Ülkelerde Sigara İçme Sıklığı (yetişkinler)
Erkek (%) Kadın (%) Çin (1984) 61 7 Japonya (1994) 59 (1966; 84) 15 (1966; 15) Kanada (1994) 29 (1966; 50) 31 (1966; 50) ABD (1993) 28 (1970; 44) 23 (1970; 32) Rusya Fed. (1993) 67 (1985; 53) 30 (1985; 10) Singapore (1995) 32 (1970; 42) 3 (1970; 5) Yunanistan (1994) 46 (1987; 61) 28 (1987; 25) İngiltere (1994) 28 (1980; 42) 26 (1980; 37) Türkiye (1993) 58 (1988; 62) 13 (1988; 24) DÜNYA 47 12
 Kadın (%) Çin (1984) Japonya (1994) 59 (1966; 84) 15 (1966; 15) Kanada (1994) 29 (1966; 50) 31 (1966; 50) ABD (1993) 28 (1970; 44) 23 (1970; 32) Rusya Fed. (1993) 67 (1985; 53) 30 (1985; 10) Singapore (1995) 32 (1970; 42) 3 (1970; 5) Yunanistan (1994) 46 (1987; 61) 28 (1987; 25) İngiltere (1994) 28 (1980; 42) 26 (1980; 37) Türkiye (1993) 58 (1988; 62) 13 (1988; 24) DÜNYA")
30
Kaynak: Önder (2002).
.")
31
Tütün Kontrol Programlarının Amacı
‘‘Tütün ürünlerinin kullanımına bağlı hastalık ve ölümleri azaltmak’’ The long-term mission of global tobacco control is to reduce smoking prevalence, tobacco consumption and the burden of tobacco-induced diseases in all countries and among all groups. Tobacco control can be accomplished through a combination of: helping those who do not use tobacco to stay tobacco-free promoting cessation of tobacco use among smokers protecting the health and rights of non-smokers, by preventing involuntary exposure to environmental tobacco smoke.

32
Neden Tütün Kontrolü Sigara Dünya da on erişkinden birini öldürmektedir. Bu rakam da altı erişkinden birine yükselecektir. Uzun süreli sigara içicilerin yarısı sigaradan ölür. Bunların yarısı ömürlerinden yıl kaybederler. Sigara kullanımı global olarak yılda net 200 milyar dolar kayba neden olur. Smoking is responsible for the death of one in ten adults worldwide (about 4 million deaths per year) and, if current smoking patterns continue, by 2030 the proportion will be one in six (about 10 million deaths per year).1 This means that about 500 million people alive today will eventually be killed by tobacco.2 Since the 1950s, more than 70,000 scientific articles have left no doubt that smoking is an extraordinarily important cause of premature mortality and disability around the world. In populations where cigarette smoking has been common for several decades, about 90% of cases of lung cancer, 15–20% of cases of other cancers, 75% of cases of chronic bronchitis and emphysema and 25% of deaths from cardiovascular diseases in those 35–69 years of age are attributable to tobacco. Studies have shown that half of all long-term smokers will die of a tobacco-related disease and, of these, half will die before the age of 65.1 In 1994, the World Bank estimated that the use of tobacco results in a global net loss of US$200 billion per year, half of this loss being in developing countries. Costs were calculated to include direct medical care for tobacco-related diseases, fire losses, absenteeism from work, reduced productivity and lost income due to early mortality.3 References: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, 1999. 2. Peto R, et al. Mortality from smoking in developing countries 1950– New York, Oxford University Press. 3. World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: World Health Organization; 1998.
 and, if current smoking patterns continue, by 2030 the proportion will be one in six (about 10 million deaths per year).1 This means that about 500 million people alive today will eventually be killed by tobacco.2. Since the 1950s, more than 70,000 scientific articles have left no doubt that smoking is an extraordinarily important cause of premature mortality and disability around the world. In populations where cigarette smoking has been common for several decades, about 90% of cases of lung cancer, 15–20% of cases of other cancers, 75% of cases of chronic bronchitis and emphysema and 25% of deaths from cardiovascular diseases in those 35–69 years of age are attributable to tobacco. Studies have shown that half of all long-term smokers will die of a tobacco-related disease and, of these, half will die before the age of In 1994, the World Bank estimated that the use of tobacco results in a global net loss of US$200 billion per year, half of this loss being in developing countries. Costs were calculated to include direct medical care for tobacco-related diseases, fire losses, absenteeism from work, reduced productivity and lost income due to early mortality.3. References: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, Peto R, et al. Mortality from smoking in developing countries 1950– New York, Oxford University Press. 3. World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: World Health Organization;")
33
Tütün Kontrolünde Engeller
Tütün bağımlılık yapıcı madde olan nikotin içerir. Sigara şirketleri ekonomik ve politik güçlerini tütün kontrolüne karşı kullanırlar. Sigara satışları hükümetlerin gelirlerine katkı yapar. Bazı kişiler sigaraya bağlı hastalıklar konusunda bilgi sahibi değildir. In countries around the world, tobacco use is one of the greatest threats to public health. While some countries have made progress in reducing tobacco use, worldwide consumption of manufactured cigarettes more than doubled between 1967 and Per capita consumption increased by 25% during the same period.1 There are a number of important obstacles to tobacco control around the world. These include: the addictive properties of nicotine that make quitting difficult the tobacco industry’s use of its political and economic power to maintain its markets and oppose tobacco control efforts (e.g. the 1996 annual revenue for Philip Morris, the world’s largest transnational tobacco corporation was US$ 55 billion)2 Government concerns that tobacco control policies may have harmful economic consequences lack of thorough information on the health risks of tobacco use. References: 1. World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: World Health Organization; 1998. 2. Philip Morris Annual Report, 1996.
2. Government concerns that tobacco control policies may have harmful economic consequences. lack of thorough information on the health risks of tobacco use. References: 1. World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: World Health Organization; Philip Morris Annual Report,")
34
Nikotin Bağımlılık Modeli
Etken Vektör Host Incidental Host Sigara Şirketleri Sigara içici Tütün ürünleri İstemsiz sigara içici Çevre Kültür,politika ekonomi, tarih NİKOTİN BAĞIMLILIĞI This figure applies the classic epidemiologic concepts of agent, host, and environment to the problem of cigarette smoking. In this model, the agent is tobacco use (cigarette smoking), with its unique characteristic of nicotine addiction. The vector is the tobacco industry operating in an environment shaped by cultural, political and economic factors, with the overlay of advertising and other promotion. ‘Incidental hosts’ are the non-smokers who are involuntarily exposed to tobacco smoke. Reference: 1. Orleans CT. Nicotine delivery devices. In Nicotine Addiction: Principles and Management, Edited by J Slade. Oxford University Press.
, with its unique characteristic of nicotine addiction. The vector is the tobacco industry operating in an environment shaped by cultural, political and economic factors, with the overlay of advertising and other promotion. ‘Incidental hosts’ are the non-smokers who are involuntarily exposed to tobacco smoke. Reference: 1. Orleans CT. Nicotine delivery devices. In Nicotine Addiction: Principles and Management, Edited by J Slade. Oxford University Press.")
35
Tütün kontrolü konusunda politikacıların endişeleri
İş kaybı. Gelirlerde düşüş. Kaçakçılık artışı. Fiyat artışlarının düşük gelirli sigara içiciler üzerine kötü etkileri. Policy makers often raise highly specific concerns with regards to taking action (especially raising the price of tobacco) to control tobacco use. Some of these concerns include: tobacco control will cause permanent job losses higher taxes will reduce government revenues higher taxes will lead to huge increases in smuggling increases in taxes will have a disproportionate impact on poor consumers. These points have been examined and thoroughly addressed by the World Bank in its 1999 report: ‘Curbing the epidemic: governments and the economics of tobacco control.’1 The 1999 report suggests that most countries will see no long-term job losses if tobacco consumption falls. In addition, since addicted smokers respond slowly to price increases, cigarette tax increases of 10% worldwide are predicted to increase tobacco tax revenues by about 7%. In order for tax increases to be effective, the World Bank recommends that smuggling should be addressed with strict measures. These should include prominent tax stamps and strong enforcement of penalties against smugglers. Finally, earmarking a portion of the revenue generated by tobacco tax increases can help to support low-income tobacco users in their attempts to quit and generally provide resources for tobacco control activity that may serve to diminish the proportionally greater burden that a tax increase can represent for these smokers. Reference: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, 1999. World Bank, 1999
 to control tobacco use. Some of these concerns include: tobacco control will cause permanent job losses. higher taxes will reduce government revenues. higher taxes will lead to huge increases in smuggling. increases in taxes will have a disproportionate impact on poor consumers. These points have been examined and thoroughly addressed by the World Bank in its 1999 report: ‘Curbing the epidemic: governments and the economics of tobacco control.’1 The 1999 report suggests that most countries will see no long-term job losses if tobacco consumption falls. In addition, since addicted smokers respond slowly to price increases, cigarette tax increases of 10% worldwide are predicted to increase tobacco tax revenues by about 7%. In order for tax increases to be effective, the World Bank recommends that smuggling should be addressed with strict measures. These should include prominent tax stamps and strong enforcement of penalties against smugglers. Finally, earmarking a portion of the revenue generated by tobacco tax increases can help to support low-income tobacco users in their attempts to quit and generally provide resources for tobacco control activity that may serve to diminish the proportionally greater burden that a tax increase can represent for these smokers. Reference: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, World Bank,")
36
Sigara endüstrisinin stratejileri
Halkla ilişkiler. Para -politik güç. Tütün çiftçileri gibi kesimleri kendi amaçları doğrultusunda yönlendirmek. Çeşitli yollarla tütün kontrolü ile uğraşan sağlıkçılar, politikacılar , avukatlar ve gazetecileri “korkutmak”. Tobacco use has long been recognized as a source of disease. However, tobacco companies have managed to escape regulations and continue to produce large profits. This is usually done by influencing decision makers, including legislators, and using an array of strategies. The tobacco industry has repeatedly dismissed the health concerns raised by the scientific community, questioned the results of studies showing the effects on health of tobacco, and focused on people’s ‘rights’ and ‘choices’.1 The Advocacy Institute, a non profit-making organization dedicated to building the capacity of social advocates to change public policy, published a book entitled ‘Smoke and Mirrors, how the tobacco industry buys and lies its way to power and profit’. According to the Advocacy Institute, the strategies used by the industry to oppose tobacco control efforts can be divided into ten major categories: public relations, advertising and promotion, philanthropy, funding science, front groups, intimidation, political funding, creating alliances, lobbying, and legislation and public policy. Often the industry operates behind the scenes to influence public opinion on issues that may impact their profits (e.g. by paying for submission of newspaper editorials or for ‘grassroots activity’ on their behalf).2 References: 1. Sweda Jr. EL, Daynard RA. Tobacco industry tactics. British Medical Bulletin 1996; 52:183–92. 2. Advocacy Institute. Smoke and Mirrors, how the tobacco industry buys and lies its way to power and profit. Washington, DC: Advocacy Institute, August 1998. The Advocacy Institute, 1998
.2. References: 1. Sweda Jr. EL, Daynard RA. Tobacco industry tactics. British Medical Bulletin 1996; 52:183– Advocacy Institute. Smoke and Mirrors, how the tobacco industry buys and lies its way to power and profit. Washington, DC: Advocacy Institute, August The Advocacy Institute,")
37
Tütün kontrolünde talebi azaltıcı temel önlemler.
Fiyatları yükseltmek. Reklam ve promosyonu yasaklamak. Dumansız iç ortamların oluşturulması. Kitle iletişim kampanyaları. Tütün ürünü paketleri üzerine uyarıcı yazılar. Sigara bırakma tedavisine ulaşmayı kolaylaştırma. Gençlik temelli programların uygulanması. Okul programları Medya Gençlik etkinlikleri Tobacco control efforts can be classified in various ways. The World Bank classifies interventions as those aimed at decreasing demand for tobacco and those aimed at decreasing supply of tobacco.1 Measures to reduce demand include interventions to decrease affordability (such as raising the price of tobacco products) and acceptability (such as mass media campaigns, bans on advertising, and creating smoke-free environments). Increasing real price by raising tobacco taxes has been shown to be the single most effective measure to decrease demand, especially among young people.1 Reference: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, 1999.
 and acceptability (such as mass media campaigns, bans on advertising, and creating smoke-free environments). Increasing real price by raising tobacco taxes has been shown to be the single most effective measure to decrease demand, especially among young people.1. Reference: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC,")
38
Tütün fiyatlarının yükseltilmesi
Fiyatlar kısa sürede tütün tüketimini azaltan muhtemel en etkili tek yöntemdir. Fiyatlar gençlerin sigaraya başlama oranları üzerine çok önemli oranda etki yapar. Vergi satış fiyatlarının 2/3’ ünü oluşturmalıdır. In spite of the addictive nature of smoking, demand for cigarettes is highly affected by price. The extent to which smokers can afford to purchase cigarettes (affordability) has a major influence on consumption. However, the demand is inelastic. It is not one to one, as a 10% increase in tobacco prices has been shown to reduce consumption in the short-term by 3 to 5% in high income, developed countries and by 8% in low- and -middle income countries. Increasing prices through taxation is considered to be the most effective single tool to control tobacco use. Reductions are greatest in children and in lower-income groups.1 Tax increases in California: an example2 A number of econometric analyses reviewed the impact of an increased tobacco tax on tobacco consumption in California. These studies showed a significant reduction in per capita cigarette consumption, directly associated with the implementation of a tobacco tax increase (instituted under California Proposition 99). From January 1989 through December 1992, the tobacco tax increase was estimated to reduce cigarette consumption by 1.3 billion packs of cigarettes.3 Although there was a significant reduction in cigarette sales due to the tax increase, California’s revenues also increased dramatically since the percentage increase in tax, reflected by the increase in retail price, was higher than the percentage decrease in demand (sales). A 10% increase in price reduced the demand by 4%. References: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, 1999. 2. Hu T, Xu X, Keeler T. Earmarked tobacco taxes: lessons learned. In The Economics of Tobacco Control. Towards an Optimal Policy Mix, 1st edn 1998; Edited by I Abedian, R van der Merwe, N Wilkins & P Jha. Applied Fiscal Research Center, University of Cape Town. 3. Hu T, Sung H, Keeler T. Tobacco taxes and the anti-smoking media campaign: the California experience. American Journal of Public Health Cited in Hu T, Xu X, Keeler T. Earmarked tobacco taxes: lessons learned. In The Economics of Tobacco Control. Towards an Optimal Policy Mix, 1st edn 1998; Edited by I Abedian, R van der Merwe, N Wilkins, P Jha. Applied Fiscal Research Center, University of Cape Town.
 has a major influence on consumption. However, the demand is inelastic. It is not one to one, as a 10% increase in tobacco prices has been shown to reduce consumption in the short-term by 3 to 5% in high income, developed countries and by 8% in low- and -middle income countries. Increasing prices through taxation is considered to be the most effective single tool to control tobacco use. Reductions are greatest in children and in lower-income groups.1. Tax increases in California: an example2. A number of econometric analyses reviewed the impact of an increased tobacco tax on tobacco consumption in California. These studies showed a significant reduction in per capita cigarette consumption, directly associated with the implementation of a tobacco tax increase (instituted under California Proposition 99). From January 1989 through December 1992, the tobacco tax increase was estimated to reduce cigarette consumption by 1.3 billion packs of cigarettes.3 Although there was a significant reduction in cigarette sales due to the tax increase, California’s revenues also increased dramatically since the percentage increase in tax, reflected by the increase in retail price, was higher than the percentage decrease in demand (sales). A 10% increase in price reduced the demand by 4%. References: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, Hu T, Xu X, Keeler T. Earmarked tobacco taxes: lessons learned. In The Economics of Tobacco Control. Towards an Optimal Policy Mix, 1st edn 1998; Edited by I Abedian, R van der Merwe, N Wilkins & P Jha. Applied Fiscal Research Center, University of Cape Town. 3. Hu T, Sung H, Keeler T. Tobacco taxes and the anti-smoking media campaign: the California experience. American Journal of Public Health Cited in Hu T, Xu X, Keeler T. Earmarked tobacco taxes: lessons learned. In The Economics of Tobacco Control. Towards an Optimal Policy Mix, 1st edn 1998; Edited by I Abedian, R van der Merwe, N Wilkins, P Jha. Applied Fiscal Research Center, University of Cape Town.")
40
Philip Morris Tekel Sigaraları
arasındaki fiyat farkını % 30 oranında tutmak için plan yapar.

43
Reklam ve promosyonların yasaklanması
Reklam, promosyon ve sponsorluklar satışları artırmak için yapılır. Sponsorluk firmalar tarafından reklam yasaklarının aşmanın yolu olarak kullanılır. Avrupa’da reklam yasaklarını aşmak için en çok kullanılan yöntem sigara dışı ürünlerde logoların kullanılmasıdır. Reklam, sponsorluk ve promosyonların bütünüyle yasaklanması çok etkilidir. Tobacco companies use a broad range of advertising, sponsorship and promotional activities to boost tobacco sales. Advertising media include point-of-sale, television, magazines, journals and billboards, among others. Sponsorship of events and organizations allows the industry to place their brand logos on race cars, in stadiums and on athletes’ uniforms, which often gets further television coverage (often in spite of television advertising bans). Promotion is a broad category that encompasses the use of coupons redeemable for tobacco products, giveaways, ‘sale’ of non-tobacco products such as baseball caps, bags and tee-shirts emblazoned with brand logos (these can often be purchased with empty cigarette packs), and placement of tobacco products in films and videos. The tobacco industry often fiercely contests policies to restrict or ban tobacco advertising, and finds creative ways to get around bans to keep their brand names and images in front of the public. Although the industry maintains that advertising is targeted at getting current smokers to switch to their brand, their own internal documents show that they clearly rely on advertisements, especially the kind that can affect young people, to attract new customers. According to a 1995 R.J. Reynolds memo: “ the successfully tested ‘Meet the Turk ad campaign and new Marlboro-type blend is another step to meet our marketing objective: to increase our young adult franchise. To ensure increase and longer-term growth for Camel Filter, the brand must increase its share of penetration among the 14–24 age group which have a new set of more liberal values and which represents tomorrow’s cigarette business.”1 A longitudinal study conducted in California showed that between 1993 and 1996, 34% of all experimentation could be attributed to tobacco promotional activities.2 Tobacco advertising is still prevalent in many countries. Billboards are often considered to be among the more egregious of the advertising media. A survey conducted in the UK reported that almost 40% of 8–13 years old said they most often saw cigarettes advertised on billboards.3 When billboard advertising was successfully banned by Baltimore City, Maryland (US), ‘rolling billboards’ (a truck pulling a large billboard on a trailer) were seen cruising the streets of the city. Studies have shown that adolescents smoke the most heavily advertised brands and that their brand choice is influenced by advertising and promotion. The most effective strategy, therefore, is a comprehensive ban on all forms of tobacco advertising, sponsorship and promotion. References: 1. R.J. Reynolds Tobacco Co. Official J W Hind, R.J. Reynolds Tobacco Co. internal memorandum, January 23, 1975. 2. Pierce JP, Choi WS, Gilpin EA, et al. Tobacco industry promotion of cigarettes and adolescent smoking. JAMA. 1998; 279:511–515. 3. Levin G. Poll shows Camel ads are effective with kids; preteens best recognize brand. Advertising Age. 4/7/92.
. Promotion is a broad category that encompasses the use of coupons redeemable for tobacco products, giveaways, ‘sale’ of non-tobacco products such as baseball caps, bags and tee-shirts emblazoned with brand logos (these can often be purchased with empty cigarette packs), and placement of tobacco products in films and videos. The tobacco industry often fiercely contests policies to restrict or ban tobacco advertising, and finds creative ways to get around bans to keep their brand names and images in front of the public. Although the industry maintains that advertising is targeted at getting current smokers to switch to their brand, their own internal documents show that they clearly rely on advertisements, especially the kind that can affect young people, to attract new customers. According to a 1995 R.J. Reynolds memo: the successfully tested ‘Meet the Turk ad campaign and new Marlboro-type blend is another step to meet our marketing objective: to increase our young adult franchise. To ensure increase and longer-term growth for Camel Filter, the brand must increase its share of penetration among the 14–24 age group which have a new set of more liberal values and which represents tomorrow’s cigarette business. 1. A longitudinal study conducted in California showed that between 1993 and 1996, 34% of all experimentation could be attributed to tobacco promotional activities.2. Tobacco advertising is still prevalent in many countries. Billboards are often considered to be among the more egregious of the advertising media. A survey conducted in the UK reported that almost 40% of 8–13 years old said they most often saw cigarettes advertised on billboards.3 When billboard advertising was successfully banned by Baltimore City, Maryland (US), ‘rolling billboards’ (a truck pulling a large billboard on a trailer) were seen cruising the streets of the city. Studies have shown that adolescents smoke the most heavily advertised brands and that their brand choice is influenced by advertising and promotion. The most effective strategy, therefore, is a comprehensive ban on all forms of tobacco advertising, sponsorship and promotion. References: 1. R.J. Reynolds Tobacco Co. Official J W Hind, R.J. Reynolds Tobacco Co. internal memorandum, January 23, Pierce JP, Choi WS, Gilpin EA, et al. Tobacco industry promotion of cigarettes and adolescent smoking. JAMA. 1998; 279:511– Levin G. Poll shows Camel ads are effective with kids; preteens best recognize brand. Advertising Age. 4/7/92.")
45
Döküman No:

47
Formula-1 Marlboro için bulunmaz bir pazarlama aracıdır
Reklam yasağı olan pazarlar için hayati önem taşır

48
Dumansız iç ortamların oluşturulması
Uçaklar İşyerleri Okullar Kamu alanları Lokantalar Reproduced with permission from the National Institute of Respiratory Diseases of Mexico (INER). The primary objective of clean indoor air regulations in schools, workplaces and public places is to protect non-smokers from involuntary exposure to tobacco smoke. Clean indoor air policies have been shown to be highly effective in decreasing involuntary exposures, but have also been shown to decrease both consumption and smoking prevalence. Picture source: Lo Mono del Fumador, Instituto Nacional de Enfermedades Respiratorias, México, D.F., Reproduced with permission from the National Institute of Respiratory Diseases of Mexico (INER).
. The primary objective of clean indoor air regulations in schools, workplaces and public places is to protect non-smokers from involuntary exposure to tobacco smoke. Clean indoor air policies have been shown to be highly effective in decreasing involuntary exposures, but have also been shown to decrease both consumption and smoking prevalence. Picture source: Lo Mono del Fumador, Instituto Nacional de Enfermedades Respiratorias, México, D.F., Reproduced with permission from the National Institute of Respiratory Diseases of Mexico (INER).")
50
Sigarasız işyeri uygulamalarının sigara kullanımına etkileri
Çalışam tipi Sigara/gün Sigara prevelansı Study type No Studies Δ in cigarettes/day* Δ in prevalence* Community – 36% - 7–50% Worksite, retrospective – 40% - 4–16% Worksite, cross-sectional - 7– 20% - 3–5% Worksite, cohort – 53% - 0–23% This table is adapted from a publication by Chapman et al, in which 19 studies of the impact of smoke-free workplaces on cigarette consumption and prevalence were reviewed. Of the 19 studies reviewed, 18 reported reductions in daily smoking rates and 17 reported reductions in smoking prevalence, although the authors noted that outside the healthcare setting, the impact on prevalence was not as clear. Excluding the potential impact on prevalence, and focusing only on consumption, the authors concluded that ‘if workplaces were universally smoke-free, the number of cigarettes foregone annually would increase to 1.14 billion (3.4%) in Australia and 20.9 billion (4.1%) in the US.’1 Reference: 1. Chapman S, Borland R, Scollo M, et al. The impact of smoke-free workplaces on declining cigarette consumption in Australia and the United States. American Journal of Public Health 1999; 89:1018–1023. No – number of; Δ – changes * range of reduction across studies Adapted from Chapman et al, 1999
 in Australia and 20.9 billion (4.1%) in the US.’1. Reference: 1. Chapman S, Borland R, Scollo M, et al. The impact of smoke-free workplaces on declining cigarette consumption in Australia and the United States. American Journal of Public Health 1999; 89:1018–1023. No – number of; Δ – changes. * range of reduction across studies. Adapted from Chapman et al,")
51
Philip Morris’ e göre sigarasız işyeri uygulamalarının etkisi.
İşyerlerinde tam yasaklama endüstriyi çok etkiler. Kısıtlamalar tüketimi % azaltır.Ortalama bırakma oranını % 84 artırır. Hafif kısıtlamalar hem tüketime hem de bırakma eğilimine çok az etki yapar. Reproduced with permission from the National Institute of Respiratory Diseases of Mexico (INER). Philip Morris has conducted its own studies of the impact of smoke-free workplaces on tobacco consumption. In this document, the tobacco company concludes that totally smoke-free workplaces would strongly affect tobacco industry volume. Their assessment is that consumption drops by 11–15% and cessation is increased by 84% among smokers in totally smoke-free workplaces. The document also suggests that the creation of designated smoking areas has limited impact on consumption and prevalence. This is the strategy the industry often promotes as an alternative to smoke-free workplaces/public places. Reference: Philip Morris Inter-Office Correspondence. Philip Morris, USA, Philip Morris Documents. Document ID #: /8283. Available at: http// (accessed July 2000). Source of picture: Lo Mono del Fumador, Instituto Nacional de Enfermedades Respiratorias, México, D.F., Reproduced with permission from the National Institute of Respiratory Diseases of Mexico (INER). Philip Morris Inter-Office Correspondence. Philip Morris, US, 1992 Philip Morris Inter-Office Correspondence. Philip Morris, US, 1992
. Philip Morris has conducted its own studies of the impact of smoke-free workplaces on tobacco consumption. In this document, the tobacco company concludes that totally smoke-free workplaces would strongly affect tobacco industry volume. Their assessment is that consumption drops by 11–15% and cessation is increased by 84% among smokers in totally smoke-free workplaces. The document also suggests that the creation of designated smoking areas has limited impact on consumption and prevalence. This is the strategy the industry often promotes as an alternative to smoke-free workplaces/public places. Reference: Philip Morris Inter-Office Correspondence. Philip Morris, USA, Philip Morris Documents. Document ID #: /8283. Available at: http// (accessed July 2000). Source of picture: Lo Mono del Fumador, Instituto Nacional de Enfermedades Respiratorias, México, D.F., Reproduced with permission from the National Institute of Respiratory Diseases of Mexico (INER). Philip Morris Inter-Office Correspondence. Philip Morris, US, Philip Morris Inter-Office Correspondence. Philip Morris, US,")
52
Arzı azaltıcı tütün kontrol önlemleri.
Tütünün yasaklanması. Gençlerin erişmesinin kısıtlanması. Tütün tarımı yerine başka ürünlerin ikamesi. Uluslar arası ticaretin kısıtlanması. Kaçakçılığa karşı önlemler. As outlined by the World Bank report, theoretical supply-side interventions to control tobacco use include prohibition of tobacco, restricting tobacco sales to youth, crop substitution and diversification, restrictions on international trade and action against smuggling. In general, the report concludes that there is little promise in most supply-side interventions. They are characterized as either politically or economically unfeasible, or unlikely to be effective, or both. The report, however, does make an exception for action to reduce smuggling, noting that this should be a key element in comprehensive tobacco control programs since smuggling can reduce price which is a critical determinant of consumption.1 Reference: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, 1999.

53
20 sene önce Larinks CA nedeniyle opere edilmiş (Total ). Öksürük şikayeti nedeniyle akciğer grafisi çekilmiş. Z.Y .63 yaşında erkek hasta. Rize doğumlu. .

54
90 paket/yıl Sigara içmiş olan hasta halen 1.5-2 paket/gün sigara içmekte Hastanın bir sene önceki grafisi

55
Önemli bir sorun olduğunu sezmişti...
Hastaya akciğerlerinde ciddi bir problem olabileceğini , bazı tetkiklerin yapılması gerektiğini söyledim. Önemli bir sorun olduğunu sezmişti... Dedi ki;

56
“Allahın benden başka guli yok mi ?
Hep dertleri baa verii.”

57
DERTSİZ VE SİGARASIZ Günler Dilerim.

59
CEVAP 2: Dünya Bankası Önerilerilerine Göre Yapılması Gerekenler Sigaranın zararlı etkilerine karşı önlemler alınmalı Reklam yasağı, gençlerin korunması, fiyat politikaları

60
Smoking Issues Status Book, 1997
Countries with Partial or Total Tobacco Advertising and Promotion Bans – 1997 Country TV Radio Press Cinema Sponsorship Point of Sale Sampling Australia X X X X Restrictions Restrictions Restrictions Canada X X Restrictions X Restrictions X X France X X X X X Restrictions X Malaysia X X X X Restrictions X X Singapore X X X X Restrictions X X Thailand X X X X X X X ‘Over 100 countries have bans on tobacco television advertisements, approximately 90 have bans on radio ads, 66 have banned advertising in cinema, 45 prohibit tobacco advertisements in the press, 34 have banned product sampling, 21 do not permit point-of-sale advertisement, and 13 have banned tobacco industry sponsorship’.1 This table shows a few examples of countries with partial or total tobacco advertising and promotion bans during 1997. Reference: 1. Smoking Issues Status Book: Global Overview, International Documentation Center, June 1997; p. 3. Cited in: INFACT. Global aggression: The case for world standards and bold US action challenging Philip Morris and RJR Nabisco. INFACT’s 1998 People’s Annual Report. New York: The Apex Press. Table Source: Smoking Issues Status Book: Global Overview June 1997, International Tobacco Documentation Center. Smoking Issues Status Book, 1997

66
TÜRKİYE SİGARA TÜKETİMİ MİLYAR ADET
CEVAP:4 TÜRKİYE SİGARA TÜKETİMİ MİLYAR ADET 78.938

67
Türk sigaralarında kullanılan tütün miktarı ve tipi 1987 1996 2000
Rapor tahmin edilen (1000 ton) Amerikan tütünü Türk tütünü
 Amerikan tütünü Türk tütünü")
68
Türkiye’ye sigara ithalatı 1984-1991
(1000 ton)
")
69
Türkiye’de Sigara İçme Sıklığı (yetişkinler) (Bilir, N. , Güçiz, B
Türkiye’de Sigara İçme Sıklığı (yetişkinler) (Bilir, N., Güçiz, B., Yıldız, N.) Grup Sayı Yıl Sıklık (%) Doktor 1128 1999 43.1 Öğretmen 1044 48.6 Gazeteci 109 1996 63.9 Şöför 338 74.3 Polis 718 64.7 İmam-müezzin 279 25.1 Artist 130 46.2 Sporcu 149 34.9
 (Bilir, N., Güçiz, B., Yıldız, N.) Grup. Sayı. Yıl. Sıklık (%) Doktor Öğretmen Gazeteci Şöför Polis İmam-müezzin Artist Sporcu")
71
Tütün Kontrolü Uluslararası Çerçeve Anlaşması
21 Mayıs 2003 56. Dünya Sağlık Asamblesi 192 Ülke Dünyanın İlk Halk sağlığı Anlaşmasını İmzaladılar. Türkiye 28 Nisan 2004’de imzaladı.

72
Reklam, promosyoni, sponsorluk yasakları
Sigara paketlerinin yüzünün en az % 30 kaplayacak uyarıcı yazılar Kamusal kapalı alanlarda, taşıma araçlarında sigara yasakları Tütün ürünlerinin üretim ve ticaretinde kaçakcılığın önlenmesi

74
Tablo 2 - Dünya Bankasý Sýnýflamasýna Göre Ülkelerdeki OrtalamaSigara Fiyatlarý ve Vergiler

75
Türkiye’de Sigara Fiyatlarý ve Tüketim İliºkisi Zeynep Önder
Şekil 2b – Türkiye’de Reel Sigara Fiyatlarý ve Vergiler, Türkiye’de Sigara Fiyatlarý ve Tüketim İliºkisi Zeynep Önder

76
2a – Türkiye’de Nominal ve Reel Sigara Fiyatlarý, 1994-2000.
Türkiye’de Sigara Fiyatlarý ve Tüketim İliºkisi Zeynep Önder

77
Dünya sigaralarının % 10-35’I
kaçakçılıkla satılır.

78
Sigaraya Bağlı Ölümler
Dünyada 1.1 milyar sigara içen 4.5 milyon ölüm / yıl milyon (2025) (günde 12 bin ölüm) Türkiye’de 17 milyon sigara içen bin ölüm / yıl (günde ölüm)
 (günde 12 bin ölüm) Türkiye’de. 17 milyon sigara içen bin ölüm / yıl. (günde ölüm)")
79
Sigara İçiminin Yaş ve Cins Dağılımı, Dünya, 1995
Yaş grupları Erkek (%) Kadın (%) 15 – 19 33 5 20 – 29 42 12 30 – 39 57 15 40 – 49 58 50 – 59 51 60 + 40 1 Bütün yaşlar 47
 Kadın (%) 15 – – – – – Bütün yaşlar. 47.")
80
Industry Opposition to Clean Indoor Air: Creating Scientific Controversy
Philip Morris presented… their global strategy on ETS. In every major international area…they are proposing, in key countries, to set up a team of scientists organized by one national coordinating scientist and American lawyers, to review the scientific literature or carry out work on ETS to keep the controversy alive. PM then expect the group of scientists to operate within the confines of decisions taken by PM scientists to determine the general direction of research, which apparently would then be ‘filtered’ by lawyers to eliminate areas of sensitivity…the scientists should be able to produce research or stimulate controversy in a way that public affairs people in their countries would be able to make use of… . Note on a Special Meeting of the UK Industry on Environmental Tobacco Smoke. London, February 17, 1988 In many countries, public opinion has increasingly moved towards strong support for smoke-free indoor air. In the face of this increasing public pressure and increasing local regulations, the industry has worked hard to promote voluntary measures (often designated smoking areas). This document shows how at the time when significant scientific research was emerging, indicating that exposure to environmental tobacco smoke posed a health risk for non-smokers, Philip Morris was planning a worldwide strategy to create controversy around the science. While publicly arguing that their goal was objective scientific consideration of the issue, this note clearly indicates that they were funding science that would be ‘filtered’ by lawyers and would be aimed at “stimulating controversy in a way that public affairs people in their countries would be able to make use of…” Reference: 1. Note on a Special Meeting of the UK Industry on Environmental Tobacco Smoke. London, 17 February, Philip Morris Documents Website: Document ID: /1198.
. This document shows how at the time when significant scientific research was emerging, indicating that exposure to environmental tobacco smoke posed a health risk for non-smokers, Philip Morris was planning a worldwide strategy to create controversy around the science. While publicly arguing that their goal was objective scientific consideration of the issue, this note clearly indicates that they were funding science that would be ‘filtered’ by lawyers and would be aimed at stimulating controversy in a way that public affairs people in their countries would be able to make use of… Reference: 1. Note on a Special Meeting of the UK Industry on Environmental Tobacco Smoke. London, 17 February, Philip Morris Documents Website: Document ID: /1198.")
81
Prevalence of smoking (percentages of current smokers)
95% confidence interval Prevalence of smoking (percentages of current smokers) Year * Mass media led campaigns begin 25 30 35 40 45 50 Prevalence of cigarette smoking in adults aged 16 or over in Australia 1974–1989 Mass Media Campaigns In the US alone the major tobacco companies spend US$5.6 billion each year to advertise their products. Tobacco industry documents have shown that the industry targets young people as a source of new customers, and research has shown that these investments in advertising and promotion are effective. In fact, 86% of young people in the US that smoke prefer Marlboro, Camel and Newport, the most heavily advertised brands.1 A survey released in April 2000, by the Campaign for Tobacco Free Kids showed that more than 70% of 12–17 year olds, and only a third of adults, recalled seeing tobacco advertising in the past two weeks.2 Counter-marketing campaigns are an important and effective component of comprehensive tobacco control programs. These campaigns often utilize television, radio, and billboard advertisements, as well as media advocacy techniques like holding local events to generate news coverage. Their overall goal is to reduce tobacco use, but campaigns use different strategies to achieve this goal. These strategies can include: providing information on the health risks of tobacco use, changing social norms around tobacco use, and encouraging quit attempts, among others. There is currently debate in the literature on the best messages and message types to use in counter-advertising campaigns. For example, in a US based review conducted by Goldman and Glantz, five message types were considered and research (primarily focus group research) on their relative effectiveness was reviewed. The study concluded that the most effective message types for denormalizing tobacco use are those that use the themes of tobacco industry manipulation and second hand smoke, and that ‘aggressive’ strategies are more effective at reducing tobacco use.3 Since the effectiveness of a given message is likely to vary across countries and across populations, however, pre-testing of campaign messages is critical. As seen in the slide, the implementation of a large scale paid media campaign in Australia was associated with reduction in prevalence in both males and females.4 References: 1. Centers for Disease Control and Prevention. Changes in the cigarette brand preference of adolescent smokers, US, 1989–1993. MMWR 1994; 43:577–581. 2. Campaign for Tobacco Free Kids. Available at: (accessed April ). 3. Goldman LK, Glantz SA. Evaluation of antismoking advertising campaigns. JAMA 1998; 279:772–777. 4. Reid DJ, Killoran AJ, McNeill AD, et al. Choosing the most effective health promotion options for reducing a nation’s smoking prevalence. Tobacco Control 1992; 1:185–197. Cited in Reid D. Tobacco control overview. British Medical Bulletin 1996; 52:108–120. Source of graph: Reid DJ, Killoran AJ, McNeill AD, et al. Choosing the most effective health promotion options for reducing a nation’s smoking prevalence. Tobacco Control 1992; 1:185–197. Cited in Reid D. Tobacco control overview. British Medical Bulletin 1996; 52:108–120. British Medical Bulletin, 1996
 Year. * Mass media led campaigns begin Prevalence of cigarette smoking in adults aged 16 or over in Australia 1974–1989. Mass Media Campaigns. In the US alone the major tobacco companies spend US$5.6 billion each year to advertise their products. Tobacco industry documents have shown that the industry targets young people as a source of new customers, and research has shown that these investments in advertising and promotion are effective. In fact, 86% of young people in the US that smoke prefer Marlboro, Camel and Newport, the most heavily advertised brands.1 A survey released in April 2000, by the Campaign for Tobacco Free Kids showed that more than 70% of 12–17 year olds, and only a third of adults, recalled seeing tobacco advertising in the past two weeks.2. Counter-marketing campaigns are an important and effective component of comprehensive tobacco control programs. These campaigns often utilize television, radio, and billboard advertisements, as well as media advocacy techniques like holding local events to generate news coverage. Their overall goal is to reduce tobacco use, but campaigns use different strategies to achieve this goal. These strategies can include: providing information on the health risks of tobacco use, changing social norms around tobacco use, and encouraging quit attempts, among others. There is currently debate in the literature on the best messages and message types to use in counter-advertising campaigns. For example, in a US based review conducted by Goldman and Glantz, five message types were considered and research (primarily focus group research) on their relative effectiveness was reviewed. The study concluded that the most effective message types for denormalizing tobacco use are those that use the themes of tobacco industry manipulation and second hand smoke, and that ‘aggressive’ strategies are more effective at reducing tobacco use.3 Since the effectiveness of a given message is likely to vary across countries and across populations, however, pre-testing of campaign messages is critical. As seen in the slide, the implementation of a large scale paid media campaign in Australia was associated with reduction in prevalence in both males and females.4. References: 1. Centers for Disease Control and Prevention. Changes in the cigarette brand preference of adolescent smokers, US, 1989–1993. MMWR 1994; 43:577– Campaign for Tobacco Free Kids. Available at: (accessed April ). 3. Goldman LK, Glantz SA. Evaluation of antismoking advertising campaigns. JAMA 1998; 279:772– Reid DJ, Killoran AJ, McNeill AD, et al. Choosing the most effective health promotion options for reducing a nation’s smoking prevalence. Tobacco Control 1992; 1:185–197. Cited in Reid D. Tobacco control overview. British Medical Bulletin 1996; 52:108–120. Source of graph: Reid DJ, Killoran AJ, McNeill AD, et al. Choosing the most effective health promotion options for reducing a nation’s smoking prevalence. Tobacco Control 1992; 1:185–197. Cited in Reid D. Tobacco control overview. British Medical Bulletin 1996; 52:108–120. British Medical Bulletin,")
82
Health Warning Labels To be effective warnings should:
contain clear unambiguous messages warn about risk and also about relative size of the risk include graphics or symbols for those who cannot read apply to all tobacco products be prominent at the top of the package covering a minimum 25% of space disclose all harmful constituents and additives exclude misleading names such as ‘light’ or ‘ultra-light’ require manufacturers to rotate a series of warnings Since the 1960s, many governments have required cigarette manufacturers to print health warnings on packages. Studies conducted in Australia, Canada and Poland suggest that health warning labels, when prominent and containing specific information, can be effective. A study conducted in Australia showed that the implementation of stronger warning labels resulted in a 27% increase in the percentage of people noticing the labels, and a 7% increase in people forgoing smoking due to the labels.1 According to Health Canada, in order to be effective, information required on labels should be, “noticeable (stand out and be large enough to read), believable (relevant and factual), and recallable (location and color should influence the ability to remember)”.2 The Canadian government recently implemented new packaging regulations that will start appearing in January 2001 and are considered to be the strongest in the world. They require graphic health warnings and will cover the top half of the front and back of tobacco product packages. Requiring manufacturers to place longer health messages inside the packet is another innovative health promotion opportunity targeted directly at tobacco users that offers a cost-effective health education program. While warning labels can be effective and convey significant health information to consumers, the tobacco industry has historically used the warnings to shelter themselves from legal liability. They have argued that the warnings are proof that smokers know of the health hazards of smoking. These arguments do not consider, however, the critical element of addiction, which is a central impediment to a smoker’s ability to quit in response to information on the hazards of smoking. References: 1. Borland R. Tobacco health warnings and smoking-related cognition and behaviors. Addiction 1997; 92:1427–1435. 2.Health Canada. Proposed new labelling requirements for tobacco products. Available at: (accessed July 2000). Source of picture: Health Canada, Available at releases/2000_07ephotos.htm (accessed June, 2000). Health Canada, 2000
, believable (relevant and factual), and recallable (location and color should influence the ability to remember) .2. The Canadian government recently implemented new packaging regulations that will start appearing in January 2001 and are considered to be the strongest in the world. They require graphic health warnings and will cover the top half of the front and back of tobacco product packages. Requiring manufacturers to place longer health messages inside the packet is another innovative health promotion opportunity targeted directly at tobacco users that offers a cost-effective health education program. While warning labels can be effective and convey significant health information to consumers, the tobacco industry has historically used the warnings to shelter themselves from legal liability. They have argued that the warnings are proof that smokers know of the health hazards of smoking. These arguments do not consider, however, the critical element of addiction, which is a central impediment to a smoker’s ability to quit in response to information on the hazards of smoking. References: 1. Borland R. Tobacco health warnings and smoking-related cognition and behaviors. Addiction 1997; 92:1427– Health Canada. Proposed new labelling requirements for tobacco products. Available at: (accessed July 2000). Source of picture: Health Canada, Available at releases/2000_07ephotos.htm (accessed June, 2000). Health Canada,")
83
Labeling Requirements in Selected Countries
The amount of space occupied by warning messages on tobacco packages in selected countries around the world Country Warning size (% of package) Argentina Australia 20.7 Canada 25.0 Denmark Finland France New Zealand 10.7 Norway Singapore 14.3 South Africa 12.5 South Korea 14.4 Thailand 17.9 US This table shows the results of an international cigarette labeling study published by the US organization, Public Citizen, in While Canada has since increased the percentage of their warnings to cover 50% of the front and back of the packaging, it is clear that most countries are missing an important opportunity by using only a small percentage of the packaging space to send messages about the dangers of tobacco use. Reference: 1. Aftab M, Kolben D, Lurie P et al. Double standards of US tobacco companies in international cigarette labeling, smokescreen. Public Citizen’s Health Research Group, 1998, Washington, DC. Aftab et al, 1998
 Argentina 3.0. Australia Canada Denmark 6.8. Finland 8.3. France 4.8. New Zealand Norway 2.9. Singapore South Africa South Korea Thailand US 5.4. This table shows the results of an international cigarette labeling study published by the US organization, Public Citizen, in While Canada has since increased the percentage of their warnings to cover 50% of the front and back of the packaging, it is clear that most countries are missing an important opportunity by using only a small percentage of the packaging space to send messages about the dangers of tobacco use. Reference: 1. Aftab M, Kolben D, Lurie P et al. Double standards of US tobacco companies in international cigarette labeling, smokescreen. Public Citizen’s Health Research Group, 1998, Washington, DC. Aftab et al,")
84
Promote Cessation: Stages of Change in Smoking Cessation
Studies performed in the US show that, although most smokers (about 70%) want to stop smoking at some time, only a minority (about 15%) are ready to stop smoking at any given time. Prochaska and DiClemente developed a model of the structure of people’s efforts to change their own addictive behavior.1 The basic constructs of their ‘stages of change’ theory are: 1. Pre-contemplation stage: not seriously thinking of a change in smoking behavior within the next 6 months and a tendency to avoid information designed to help bring about change. 2. Contemplation stage: seriously thinking about changing behavior, and expect to do so within the next 6 months but not immediately. Very ambivalent and can become stuck in ‘chronic contemplation’. 3. Preparation stage: planning to stop smoking within the next 30 days and have made previous attempt for at least 24 hours in the last 12 months. Taking significant steps towards quitting. 4. Action stage: have quit smoking and are at great risk of relapse. 5. Maintenance stage: have not smoked for more than 6 months. Most people change through a cyclical process, with relapse being a normal part of the process. Tobacco control policies and interventions can more effectively influence people not to smoke, by segmenting the public according to stages in the tobacco control addiction cycle. Tobacco companies know this, and base their marketing decisions in a given market on the prevalence of consumers at the different stages in that market. Reference: 1. Prochaska JO, DiClemente CC and Norcross JC. In search of how people change: applications to addictive behaviors. American Psychologist 1992; 47:1102–1114. Prochaska et al, 1992
 want to stop smoking at some time, only a minority (about 15%) are ready to stop smoking at any given time. Prochaska and DiClemente developed a model of the structure of people’s efforts to change their own addictive behavior.1 The basic constructs of their ‘stages of change’ theory are: 1. Pre-contemplation stage: not seriously thinking of a change in smoking behavior within the next 6 months and a tendency to avoid information designed to help bring about change. 2. Contemplation stage: seriously thinking about changing behavior, and expect to do so within the next 6 months but not immediately. Very ambivalent and can become stuck in ‘chronic contemplation’. 3. Preparation stage: planning to stop smoking within the next 30 days and have made previous attempt for at least 24 hours in the last 12 months. Taking significant steps towards quitting. 4. Action stage: have quit smoking and are at great risk of relapse. 5. Maintenance stage: have not smoked for more than 6 months. Most people change through a cyclical process, with relapse being a normal part of the process. Tobacco control policies and interventions can more effectively influence people not to smoke, by segmenting the public according to stages in the tobacco control addiction cycle. Tobacco companies know this, and base their marketing decisions in a given market on the prevalence of consumers at the different stages in that market. Reference: 1. Prochaska JO, DiClemente CC and Norcross JC. In search of how people change: applications to addictive behaviors. American Psychologist 1992; 47:1102–1114. Prochaska et al,")
85
The Health Professional’s Role in Promoting Smoking Cessation
Healthcare professionals should: ask every patient at every visit if he or she smokes write a patient’s smoking status on the medical chart under vital signs ask patients about their desire to quit, reinforcing their intentions to quit motivate patients who are reluctant to quit help motivate smokers to set a quit date prescribe nicotine replacement treatment when appropriate help patients resolve problems that result from quitting encourage relapsed smokers to try again Despite the tragic health consequences of smoking, health care professionals often fail to assess and treat tobacco use consistently and effectively. This failure to assess and intervene exists even when there is substantial evidence that even brief smoking cessation treatments can be effective. Brief advice to smokers given by a family doctor during a routine consultation can result in up to 5% of smokers quitting. Smoking cessation interventions, if delivered in a timely and effective manner, greatly reduce the smoker’s risk of suffering from a smoking-related disease. The guideline “Treating tobacco use and dependence” was sponsored by a consortium of seven US Federal Government and non profit-making organizations. The guidelines were published in June 2000 and a summary is available on the World Wide Web.1 The guideline provides information on assessing tobacco use, brief clinical interventions easily delivered in the clinical setting, intensive clinical interventions and also system interventions relevant to healthcare administrators and insurers. The guidelines provide evidence-based strategies and evaluate tobacco interventions for special populations. Its major findings can be summarized as follows: 1. Tobacco dependence is a chronic condition that often requires repeated intervention. 2. Since effective smoking cessation treatments are available, every patient who smokes should be offered at least one of these treatments. 3. It is essential that clinicians and healthcare delivery systems (including administrators, insurers, and purchasers) institutionalize the consistent identification, documentation, and treatment of every tobacco user seen in a healthcare setting. 4. Brief tobacco dependence treatment is effective, and every patient who uses tobacco should be offered at least brief treatment. 5. There is a strong dose-response relationship between the intensity of tobacco dependence counseling and its effectiveness. 6. Three types of counseling and behavioral therapies were especially effective and should be used with all patients attempting tobacco cessation (problem solving/skill training, intra-treatment social support, and extra-treatment social support). 7. Numerous effective pharmacotherapies for smoking cessation now exist. Except in the presence of contraindications, these should be used with all the patients attempting to quit smoking. First-line therapy includes: bupropion SR, nicotine replacement gum, nicotine inhalators, nicotine nasal spray and nicotine patch; second-line therapy includes: clonidine and nortriptyline). 8. Tobacco dependence treatments are both clinically effective and cost-effective relative to other medical and disease prevention interventions.1 Reference: 1. U.S. Public Health Service. Treating tobacco use and dependence Available at (accessed July 2000).
 institutionalize the consistent identification, documentation, and treatment of every tobacco user seen in a healthcare setting. 4. Brief tobacco dependence treatment is effective, and every patient who uses tobacco should be offered at least brief treatment. 5. There is a strong dose-response relationship between the intensity of tobacco dependence counseling and its effectiveness. 6. Three types of counseling and behavioral therapies were especially effective and should be used with all patients attempting tobacco cessation (problem solving/skill training, intra-treatment social support, and extra-treatment social support). 7. Numerous effective pharmacotherapies for smoking cessation now exist. Except in the presence of contraindications, these should be used with all the patients attempting to quit smoking. First-line therapy includes: bupropion SR, nicotine replacement gum, nicotine inhalators, nicotine nasal spray and nicotine patch; second-line therapy includes: clonidine and nortriptyline). 8. Tobacco dependence treatments are both clinically effective and cost-effective relative to other medical and disease prevention interventions.1. Reference: 1. U.S. Public Health Service. Treating tobacco use and dependence Available at (accessed July 2000).")
86
Cessation Medications to Treat Tobacco Dependence
Four types: nicotine receptor agonists nicotine receptor blockers non-nicotine receptor agents combination medications The Public Health Service Guideline published in 2000, entitled ‘Treating tobacco use and dependence’, concluded that the following elements are effective in patients attempting tobacco cessation: intra-treatment and extra-treatment social support, skill training/problem solving and pharmacotherapy including first-line medications (bupropion SR and nicotine replacement therapy) and second-line medications (clonidine and nortriptiline).1 This slide reviews the four types of medications to treat tobacco dependence. All FDA-approved medications for treating tobacco dependence increase immediate, end-of-treatment and long-term smoking cessation rates by 2- to 3- fold. Nicotine receptor agonists – to date, the only nicotine receptor agonist medication available is nicotine itself. It is available in five very different delivery formulations. These include, patch, polacrilex gum, inhaler, nasal spray and lozenge.2 They all reach the central nervous system via the systemic capillary bed, not the pulmonary capillary bed as with cigarettes. Nicotine patch literature consistently shows that short-term treatment (6–12 weeks), doubles end-of- treatment smoking cessation rates. Nicotine nasal spray may be preferentially beneficial for high-nicotine-dependency smokers. It delivers nicotine to the brain faster than any of the nicotine medications, making it useful in ‘crisis’ situations. Nicotine polacrilex gum requires careful use because if it is chewed like regular gum; it has no therapeutic effect. The nicotine inhaler is easy to use and absorption occurs from the oral mucosa. It is the only medication that provides ‘respiratory tract sensory stimulation,’ which is an independent reinforcer for cigarette smoking. Nicotine receptor blockers – the only nicotine receptor blocker is mecamylamine. This has many side effects and is not widely used. Non-nicotine receptor agents – there are many subclasses in this group, including selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants, anxiolytics, and dopaminergic/noradrenergic reuptake inhibitors. Bupropion is a noradrenergic reuptake inhibitor. This is the only subclass that has shown consistent therapeutic effects that also help to relieve the nicotine withdrawal symptoms, including weight gain. The optimal duration for treatment is unknown. Combination medications – only a few of the possible combinations have undergone extensive clinical trials. Only the combination of nicotine patch with bupropion is FDA approved. However, several combinations like nicotine patch plus nicotine spray, or nicotine patch plus nicotine gum, have been effective in smaller trials. Two nicotine medications can be safely combined to increase the treatment result. References: 1. US Public Health Service. Treating tobacco use and dependence Available at (accessed July 2000). 2. Sachs DPL. Tobacco dependence: pathophysiology and treatment. In Pulmonary Rehabilitation: Guidelines for Success. 4th edn Edited by JE Hodgkin, GL Connors, & BR Celli (in Press).
 and second-line medications (clonidine and nortriptiline).1. This slide reviews the four types of medications to treat tobacco dependence. All FDA-approved medications for treating tobacco dependence increase immediate, end-of-treatment and long-term smoking cessation rates by 2- to 3- fold. Nicotine receptor agonists – to date, the only nicotine receptor agonist medication available is nicotine itself. It is available in five very different delivery formulations. These include, patch, polacrilex gum, inhaler, nasal spray and lozenge.2 They all reach the central nervous system via the systemic capillary bed, not the pulmonary capillary bed as with cigarettes. Nicotine patch literature consistently shows that short-term treatment (6–12 weeks), doubles end-of- treatment smoking cessation rates. Nicotine nasal spray may be preferentially beneficial for high-nicotine-dependency smokers. It delivers nicotine to the brain faster than any of the nicotine medications, making it useful in ‘crisis’ situations. Nicotine polacrilex gum requires careful use because if it is chewed like regular gum; it has no therapeutic effect. The nicotine inhaler is easy to use and absorption occurs from the oral mucosa. It is the only medication that provides ‘respiratory tract sensory stimulation,’ which is an independent reinforcer for cigarette smoking. Nicotine receptor blockers – the only nicotine receptor blocker is mecamylamine. This has many side effects and is not widely used. Non-nicotine receptor agents – there are many subclasses in this group, including selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants, anxiolytics, and dopaminergic/noradrenergic reuptake inhibitors. Bupropion is a noradrenergic reuptake inhibitor. This is the only subclass that has shown consistent therapeutic effects that also help to relieve the nicotine withdrawal symptoms, including weight gain. The optimal duration for treatment is unknown. Combination medications – only a few of the possible combinations have undergone extensive clinical trials. Only the combination of nicotine patch with bupropion is FDA approved. However, several combinations like nicotine patch plus nicotine spray, or nicotine patch plus nicotine gum, have been effective in smaller trials. Two nicotine medications can be safely combined to increase the treatment result. References: 1. US Public Health Service. Treating tobacco use and dependence Available at (accessed July 2000). 2. Sachs DPL. Tobacco dependence: pathophysiology and treatment. In Pulmonary Rehabilitation: Guidelines for Success. 4th edn Edited by JE Hodgkin, GL Connors, & BR Celli (in Press).")
87
School-Based Prevention Programs
Can reach a large number of young people although those probably at most risk are not in school Are fairly inexpensive Can delay smoking initiation Most are currently based in the teaching of general life-skills According to the WHO, since 80% of young people in developing countries are enrolled in schools, and 60% complete at least four years of education, school is a place of special importance for the implementation of prevention campaigns.1 Research performed in the US has shown that merely informing teenagers about the health effects of smoking has no effect on their smoking prevalence. However, programs that include the ‘life skills’ approach to substance-use prevention have been shown to reduce smoking initiation between 25% and 87% at 1–6 year follow-up.2 Life skills include: assertiveness, critical thinking, decision making, and problem solving abilities. These skills boost protective factors in students, such as self-confidence, self-esteem, autonomy, and self-control. The Centers for Disease Control (CDC) developed ‘Guidelines for School Programs to Prevent Tobacco Use and Addiction’ based on an extensive review of research and practice. These guidelines suggest that school programs to prevent tobacco use and addiction are most effective if they: “prohibit tobacco use at all school facilities and events, encourage and help students and staff to quit using tobacco, provide developmentally appropriate instruction in grades K-12, address the social and psychological causes of tobacco use, are part of a co-ordinated school health program through which teachers, students, families, administrators, and community leaders deliver consistent messages about tobacco use, and are reinforced by community-wide efforts”.3 References: 1. World Health Organization. Tobacco use prevention: An important entry point for the development of health-promoting schools, WHO Information Series on School Health Document Five. Geneva: WHO / UNESCO / Education International, 1998 (Brussels, Belgium). 2. Botvin GJ, Baker E, Dusenbury L, et al. Long term follow up results of a randomized drug abuse prevention trial in a white middle-class population. JAMA 1995; 273:1106–1112. 3. CDC's Guidelines for School and Community Health Programs. Preventing Tobacco Use and Addiction. Available at: (accessed June 2000).
 developed ‘Guidelines for School Programs to Prevent Tobacco Use and Addiction’ based on an extensive review of research and practice. These guidelines suggest that school programs to prevent tobacco use and addiction are most effective if they: prohibit tobacco use at all school facilities and events, encourage and help students and staff to quit using tobacco, provide developmentally appropriate instruction in grades K-12, address the social and psychological causes of tobacco use, are part of a co-ordinated school health program through which teachers, students, families, administrators, and community leaders deliver consistent messages about tobacco use, and are reinforced by community-wide efforts .3. References: 1. World Health Organization. Tobacco use prevention: An important entry point for the development of health-promoting schools, WHO Information Series on School Health Document Five. Geneva: WHO / UNESCO / Education International, 1998 (Brussels, Belgium). 2. Botvin GJ, Baker E, Dusenbury L, et al. Long term follow up results of a randomized drug abuse prevention trial in a white middle-class population. JAMA 1995; 273:1106– CDC s Guidelines for School and Community Health Programs. Preventing Tobacco Use and Addiction. Available at: (accessed June 2000).")
88
Media Literacy To help young people critically assess how media normalize, glamorize, and create role models for unhealthy lifestyles and behavior Normalization of tobacco use is portraying the use of tobacco as a routine, natural part of everyday life Glamorization associates tobacco use with desirable qualities, such as popularity, success, attractiveness, independence, maturity, fun, celebration and an escape from reality Media literacy programs encourage students to critically analyse the techniques used by the mass media. They “aim to increase students' understanding and enjoyment of how the media work, how they produce meaning, how they are organized, and how they construct reality”.1 Media literacy has been incorporated into school-based tobacco control programs to critically assess the normalization and glamorization of tobacco use through advertising. Analysis through ‘deconstructions’ of tobacco and other types of advertising encourages students to become more critically aware of underlying messages and the techniques used to convey these messages. A good example of media literacy tools are those developed by the Centers for Disease Control and Prevention2 and the New Mexico Media Literacy Project.3 References: 1. Ministry of Education, Ontario, Canada. Resource Guide: Media Literacy, pp. 6–7. Cited at: Media Literacy Online Project. Available at (accessed July 2000). 2. Media Sharp: analyzing tobacco and alcohol messages. A publication by: the Academy of Pediatrics, the Centers for Disease Control and Prevention, SAMHSA, the National Education Association Health Information Network and the Department of Health and Human Services. 3. New Mexico Media Literacy Project. Available at (accessed July 2000).
. 2. Media Sharp: analyzing tobacco and alcohol messages. A publication by: the Academy of Pediatrics, the Centers for Disease Control and Prevention, SAMHSA, the National Education Association Health Information Network and the Department of Health and Human Services. 3. New Mexico Media Literacy Project. Available at (accessed July 2000).")
89
Youth Advocacy and Action
Youth action can include: developing overall program strategies serving as peer leaders advocating for tobacco control policies checking compliance with youth access laws Examples of youth-driven programs include: the ‘Truth Campaign’ in Florida (US) developed for and by teenagers the Massachusetts Tobacco Control Program’s youth tobacco use prevention program Youth participation in tobacco control programs takes many forms. Students can be the best spokespersons for policy change, especially in areas that directly affect them. In a number of programs, young people have become actively involved in advocating for changes in the law (e.g. to eliminate vending machines or to keep advertising from targeting children). In other programs, young people have monitored merchant compliance with laws against selling tobacco to minors, or served as peer leaders in educating their classmates and friends. Active participation in the development of program materials targeted to youths can be critical to their effectiveness. The state of Florida was the first to incorporate television advertisements designed by teenagers into their tobacco prevention strategies. Over the last two years, television advertisements designed and approved by Florida teenagers have been aired as part of an aggressive anti-tobacco campaign. A recent state survey showed that, within the past two years, smoking declined by 54% among middle school students and 24% among high school students.1 This experience has been incorporated by the American Legacy Foundation into their current program to develop a national advertising campaign using funds from the the Master Settlement Agreement (MSA). The MSA was the settlement of lawsuits brought by the State Attorneys General in the US against the tobacco industry to reimburse state expenses for caring for sick smokers. The American Legacy Foundation has created a website to solicit ideas on the campaign from teenagers.2 References: 1. The Christian Science Monitor. Florida ads persuade teens not to smoke. March Available at: (accessed July 2000). 2. The American Legacy Foundation. Promoting Tobacco Free Generations Available at: www. americanlegacy.org/grants.html (accessed July 2000).
 developed for and by teenagers. the Massachusetts Tobacco Control Program’s youth tobacco use prevention program. Youth participation in tobacco control programs takes many forms. Students can be the best spokespersons for policy change, especially in areas that directly affect them. In a number of programs, young people have become actively involved in advocating for changes in the law (e.g. to eliminate vending machines or to keep advertising from targeting children). In other programs, young people have monitored merchant compliance with laws against selling tobacco to minors, or served as peer leaders in educating their classmates and friends. Active participation in the development of program materials targeted to youths can be critical to their effectiveness. The state of Florida was the first to incorporate television advertisements designed by teenagers into their tobacco prevention strategies. Over the last two years, television advertisements designed and approved by Florida teenagers have been aired as part of an aggressive anti-tobacco campaign. A recent state survey showed that, within the past two years, smoking declined by 54% among middle school students and 24% among high school students.1 This experience has been incorporated by the American Legacy Foundation into their current program to develop a national advertising campaign using funds from the the Master Settlement Agreement (MSA). The MSA was the settlement of lawsuits brought by the State Attorneys General in the US against the tobacco industry to reimburse state expenses for caring for sick smokers. The American Legacy Foundation has created a website to solicit ideas on the campaign from teenagers.2. References: 1. The Christian Science Monitor. Florida ads persuade teens not to smoke. March Available at: (accessed July 2000). 2. The American Legacy Foundation. Promoting Tobacco Free Generations Available at: www. americanlegacy.org/grants.html (accessed July 2000).")
90
Efforts to Develop a ‘Safer’ Cigarette
Patent claim and compound Publication year range Reduce tar to 1998 Remove/reduce carbon monoxide (CO) to 1997 Remove/reduce polycyclic aromatic hydrocarbons i.e. benzo[a]pyrene to 1988 Remove/reduce hydrogen cyanide (HCN) to 1988 Remove/reduce nitrosamines to 1998 Remove/reduce nitrogen dioxide/nitrate/nitrite/nitric oxide to 1998 Remove potassium nitrate and 1986 Remove radioactive compounds i.e. polonium and 1980 Remove metal carbonyls 1972 Reduce aldehyde Remove/reduce other miscellaneous compounds to 1998 The focus of much of tobacco control activity has been strategies that are aimed at making people less likely to buy and consume cigarettes. The idea of changing the cigarette itself, however, to make it either ‘less harmful’ or ‘less addicting’, is not new. This list of patents filed by tobacco companies was compiled in a report by ASH (Action on Smoking and Health) in the UK and the Imperial Cancer Research Fund entitled: ‘The safer cigarette: what the tobacco industry could do….and why it hasn’t done it.’1 The report demonstrates that tobacco companies conducted extensive research and filed for patents for technology that would have removed some of the harmful components of tobacco smoke, but never made these ‘safer’ cigarettes available to the public. The problem, according to the report is that in order to successfully market these changed cigarettes as ‘safer’, the industry would have had to admit that all their other products were dangerous. The suggestion that developing a ‘safer’ cigarette might be part of an overall tobacco control strategy is approached by public health practitioners with great caution.2,3 The failure of low-tar cigarettes to produce a public health benefit, and their probable role in postponing or preventing quitting among some smokers have made many wary of a harm reduction approach. References: 1. Action on Smoking and Health. The safer cigarette: what the tobacco industry could do….and why it hasn’t done it. Available at: (accessed June 2000). 2. Kessler DA, Witt AM, Barnett PS, et al. The Food and Drug Administration’s approval of tobacco products. New England Journal of Medicine 1996; 335:988–994. 3. Channel Reduced-smoke cigarette tested. Available at (accessed July 2000). ASH, 1999
 1972 to Remove/reduce polycyclic aromatic hydrocarbons. i.e. benzo[a]pyrene 1971 to Remove/reduce hydrogen cyanide (HCN) 1971 to Remove/reduce nitrosamines 1979 to Remove/reduce nitrogen dioxide/nitrate/nitrite/nitric oxide 1980 to Remove potassium nitrate 1978 and Remove radioactive compounds i.e. polonium 1971 and Remove metal carbonyls Reduce aldehyde Remove/reduce other miscellaneous compounds 1976 to The focus of much of tobacco control activity has been strategies that are aimed at making people less likely to buy and consume cigarettes. The idea of changing the cigarette itself, however, to make it either ‘less harmful’ or ‘less addicting’, is not new. This list of patents filed by tobacco companies was compiled in a report by ASH (Action on Smoking and Health) in the UK and the Imperial Cancer Research Fund entitled: ‘The safer cigarette: what the tobacco industry could do….and why it hasn’t done it.’1 The report demonstrates that tobacco companies conducted extensive research and filed for patents for technology that would have removed some of the harmful components of tobacco smoke, but never made these ‘safer’ cigarettes available to the public. The problem, according to the report is that in order to successfully market these changed cigarettes as ‘safer’, the industry would have had to admit that all their other products were dangerous. The suggestion that developing a ‘safer’ cigarette might be part of an overall tobacco control strategy is approached by public health practitioners with great caution.2,3 The failure of low-tar cigarettes to produce a public health benefit, and their probable role in postponing or preventing quitting among some smokers have made many wary of a harm reduction approach. References: 1. Action on Smoking and Health. The safer cigarette: what the tobacco industry could do….and why it hasn’t done it. Available at: (accessed June 2000). 2. Kessler DA, Witt AM, Barnett PS, et al. The Food and Drug Administration’s approval of tobacco products. New England Journal of Medicine 1996; 335:988– Channel Reduced-smoke cigarette tested. Available at (accessed July 2000). ASH,")
91
Regulation of Tobacco Products
Nicotine is currently most widely available in its deadliest form Move to develop innovative regulatory approaches Suggestions for change include: establishing a single regulatory framework for all nicotine delivery products prohibiting the use of misleading terms such as ‘light’ requirement that manufacturers disclose constituents and their effects seeking genuine harm reduction strategies studying reduction over time of nicotine and other potentially addictive constituents as harm reduction strategy increasing access to effective treatment The irrationality of national policies that make nicotine available with limited regulation in its deadliest form (cigarettes), while strictly regulating it in its safest form (medications to treat nicotine dependence) has been widely commented on Many argue that tobacco should be treated like other consumer products and should no longer enjoy exemptions from safety standards.2 A need to update the testing protocols for tar and nicotine yields has also been noted, since current standards do not provide consumers with accurate information on exposure. At a recent consensus conference on regulating tobacco products, the following suggestions were made regarding new thinking on the development of more rational regulatory approaches: “Evaluate and implement the most effective ways to achieve a unified regulatory framework for nicotine delivery products, including tobacco products, products for treating tobacco dependence and novel nicotine delivery devices… Ban the use of misleading terms such as ‘light’, ‘mild’, and other words or imagery (including certain brand names) which have the aim or effect of implying reduced health risk… Require tobacco manufacturers to disclose the contents, purpose and effects of constituents in all their products at regular intervals. Discontinue harm reduction strategies based on simplistic interpretation of tar and nicotine yield measurements. This means abandoning the strategy of seeking lower nominal tar yields, and, instead, finding approaches that genuinely reduce harm… Give urgent priority to studying the implications of harm reduction, reducing levels of nicotine and other possible addictive constituents in tobacco products over time. Give greater attention to increasing public access to the range of effective methods of treating tobacco dependence….”4 References: 1. Warner KE, Peck CC, Woosley RL, et al. Treatment of tobacco dependence: innovative regulatory approaches to reduce death and disease: Food and Drug Law Journal 1998; 53 (Supplement 1–9):Preface. 2. Action on Smoking and Health. The safer cigarette: what the tobacco industry could do….and why it hasn’t done it. Available at: (accessed June 2000). 3. Sweanor DT. Regulation of tobacco and nicotine: the creation, and potential for resolution, of a public health disaster. In Drugs: Education, Prevention and Policy 1998; 5:135–140. 4. Special Communication. Advancing knowledge on regulating tobacco products, Oslo, Norway. Tobacco Control 2000; 9:224–227.
, while strictly regulating it in its safest form (medications to treat nicotine dependence) has been widely commented on.1-3 Many argue that tobacco should be treated like other consumer products and should no longer enjoy exemptions from safety standards.2 A need to update the testing protocols for tar and nicotine yields has also been noted, since current standards do not provide consumers with accurate information on exposure. At a recent consensus conference on regulating tobacco products, the following suggestions were made regarding new thinking on the development of more rational regulatory approaches: Evaluate and implement the most effective ways to achieve a unified regulatory framework for nicotine delivery products, including tobacco products, products for treating tobacco dependence and novel nicotine delivery devices… Ban the use of misleading terms such as ‘light’, ‘mild’, and other words or imagery (including certain brand names) which have the aim or effect of implying reduced health risk… Require tobacco manufacturers to disclose the contents, purpose and effects of constituents in all their products at regular intervals. Discontinue harm reduction strategies based on simplistic interpretation of tar and nicotine yield measurements. This means abandoning the strategy of seeking lower nominal tar yields, and, instead, finding approaches that genuinely reduce harm… Give urgent priority to studying the implications of harm reduction, reducing levels of nicotine and other possible addictive constituents in tobacco products over time. Give greater attention to increasing public access to the range of effective methods of treating tobacco dependence…. 4. References: 1. Warner KE, Peck CC, Woosley RL, et al. Treatment of tobacco dependence: innovative regulatory approaches to reduce death and disease: Food and Drug Law Journal 1998; 53 (Supplement 1–9):Preface. 2. Action on Smoking and Health. The safer cigarette: what the tobacco industry could do….and why it hasn’t done it. Available at: (accessed June 2000). 3. Sweanor DT. Regulation of tobacco and nicotine: the creation, and potential for resolution, of a public health disaster. In Drugs: Education, Prevention and Policy 1998; 5:135– Special Communication. Advancing knowledge on regulating tobacco products, Oslo, Norway. Tobacco Control 2000; 9:224–227.")
92
Restrict Minors’ Access
Increase age for legal purchase of cigarettes and increase compliance by vendors Restrict vending machine use Prohibit sales of single cigarettes Policies to restrict access to tobacco for minors can include: the elimination of self-service displays (forcing a face-to-face transaction), mail-order sales, and vending machines; enforcing a minimum package size of 20 and prohibiting the distribution of free samples.1 Many countries have attempted to impose restrictions on the sale of cigarettes to minors using these strategies. However, most have not been shown to be successful. Youth restrictions are difficult to enforce because retailers often take advantage of sales to minors. Studies performed in the US, where legislation exists that prohibits tobacco sales to minors, have shown that most teenagers have no difficulty in obtaining cigarettes and buy them in small stores, gas stations and vending machines.2-4 Self-service displays give minors easy access to tobacco products. A study by the Institute of Medicine found that more than 40% of grade-school students who smoked daily had, at some stage, shoplifted cigarettes from self-service displays.5 In general, as the cost of cigarettes increases, young people become less likely to purchase cigarettes. However, when cigarettes are taken out of the pack and sold singly and inexpensively (relative to the price of a pack), young people are more able and thus more likely to buy. A study published in 1994 shows that single cigarettes were sold in almost 50% of the 206 surveyed retail outlets located in the middle-class and lower-class metropolitan areas of San Bernardino and Riverside counties in California. Single cigarettes were more likely to be sold to minors, who paid more for them than adults.4 References: 1. Anderson P & Hughes J. Policy interventions to reduce harm from smoking. Addiction 2000; 95 (Supplement 1): S9–S11. 2. Foster JL, Hourigan M & Mc Govern P. Availability of cigarettes to underage youth in three communities. Preventive Medicine 1992; 21:320–328. 2. Kim TF. Laws ban minors’ tobacco purchases but enforcement is another issue. JAMA 1987; 257:3323–3324. 3. Barovich M, Sussman S, Dent CW, et al. Availability of tobacco products at stores located near public schools. International Journal of Addiction 1991; 26:837–850. 4. Klonoff EA, Fritz JM, Landrine H, et al. The problem and sociocultural context of single-cigarette sales. JAMA 1994; 271:618–620. 5. Institute of Medicine. Growing up tobacco-free – preventing nicotine addiction in children and youth Washington DC. National Academy Press.
, mail-order sales, and vending machines; enforcing a minimum package size of 20 and prohibiting the distribution of free samples.1 Many countries have attempted to impose restrictions on the sale of cigarettes to minors using these strategies. However, most have not been shown to be successful. Youth restrictions are difficult to enforce because retailers often take advantage of sales to minors. Studies performed in the US, where legislation exists that prohibits tobacco sales to minors, have shown that most teenagers have no difficulty in obtaining cigarettes and buy them in small stores, gas stations and vending machines.2-4. Self-service displays give minors easy access to tobacco products. A study by the Institute of Medicine found that more than 40% of grade-school students who smoked daily had, at some stage, shoplifted cigarettes from self-service displays.5. In general, as the cost of cigarettes increases, young people become less likely to purchase cigarettes. However, when cigarettes are taken out of the pack and sold singly and inexpensively (relative to the price of a pack), young people are more able and thus more likely to buy. A study published in 1994 shows that single cigarettes were sold in almost 50% of the 206 surveyed retail outlets located in the middle-class and lower-class metropolitan areas of San Bernardino and Riverside counties in California. Single cigarettes were more likely to be sold to minors, who paid more for them than adults.4. References: 1. Anderson P & Hughes J. Policy interventions to reduce harm from smoking. Addiction 2000; 95 (Supplement 1): S9–S Foster JL, Hourigan M & Mc Govern P. Availability of cigarettes to underage youth in three communities. Preventive Medicine 1992; 21:320– Kim TF. Laws ban minors’ tobacco purchases but enforcement is another issue. JAMA 1987; 257:3323– Barovich M, Sussman S, Dent CW, et al. Availability of tobacco products at stores located near public schools. International Journal of Addiction 1991; 26:837– Klonoff EA, Fritz JM, Landrine H, et al. The problem and sociocultural context of single-cigarette sales. JAMA 1994; 271:618– Institute of Medicine. Growing up tobacco-free – preventing nicotine addiction in children and youth Washington DC. National Academy Press.")
93
Crop Substitution Economies of some developing countries’ depend on tobacco production Tobacco provides high net income per hectare Tobacco industry provides incentives to farmers Arguments for substitution have been made based on deforestation There is little evidence on whether crop substitution is effective at reducing tobacco consumption. In a few countries, such as Zimbabwe and Malawi, economic dependence on tobacco exports is very high (23 and 61% of export earnings, respectively).1 Tobacco provides a higher net income yield per unit of land than most food crops; which makes it a very attractive crop to farmers. Also, unlike other crops, the global price of tobacco is relatively stable, and the tobacco industry may provide farmers with strong in-kind support and loans. However, some have made the case for increasing crop substitution, based on the fact that tobacco farming contributes to tropical deforestation. In 1993, 62% of world tobacco was artificially cured. Flue-cured tobacco accounts for 99% of all artificially cured tobacco. Of land planted with flue-cured tobacco, 74% is located in low-income countries where there are few alternatives to wood as a source of energy or construction material.2 References: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, 1999. 2. Geist H. How tobacco farming contributes to tropical deforestation. In The Economics of Tobacco Control. Towards an Optimal Policy Mix. 1st edn Edited by I Abedian, R van der Merwe, N Wilkins & P Jha. Applied Fiscal Research Center, University of Cape Town.
.1. Tobacco provides a higher net income yield per unit of land than most food crops; which makes it a very attractive crop to farmers. Also, unlike other crops, the global price of tobacco is relatively stable, and the tobacco industry may provide farmers with strong in-kind support and loans. However, some have made the case for increasing crop substitution, based on the fact that tobacco farming contributes to tropical deforestation. In 1993, 62% of world tobacco was artificially cured. Flue-cured tobacco accounts for 99% of all artificially cured tobacco. Of land planted with flue-cured tobacco, 74% is located in low-income countries where there are few alternatives to wood as a source of energy or construction material.2. References: 1. The World Bank. Curbing the Epidemic: Governments and the Economics of Tobacco Control. Washington, DC, Geist H. How tobacco farming contributes to tropical deforestation. In The Economics of Tobacco Control. Towards an Optimal Policy Mix. 1st edn Edited by I Abedian, R van der Merwe, N Wilkins & P Jha. Applied Fiscal Research Center, University of Cape Town.")
94
Smuggling Drives down prices and makes sought-after international brands more affordable 30% of internationally exported cigarettes lost to smuggling Industry involvement Anti-smuggling measures: increased penalties prominent tax stamps special packaging The main problem related to smuggled cigarettes is that they are sold at below market price and therefore are available cheaply. This helps increase consumption and undermines the efforts of governments to deter smoking. Also, smuggling makes top brands available at affordable prices to low-income consumers, and to young people in developing countries where Western products are often status symbols. Contraband cigarettes also evade legal restrictions and health regulations, such as bans on sales to minors, labeling requirements and regulations on additives. The World Bank report estimates that approximately 30% of internationally exported cigarettes (355 billion) are lost to smuggling.1 Factors that are considered to contribute to smuggling, include price differences between countries in addition to non-price factors, such as the degree of corruption and tolerance of contraband in a country. The tobacco industry often uses the smuggling issue as a reason to oppose tax increases, arguing that tax increases will not decrease tobacco use but only serve to increase smuggling. In fact, there is good evidence that a number of tobacco companies have themselves been involved in promoting smuggling. One example is the case of British American Tobacco (BAT). A report released in January 2000 by the International Consortium of Investigative Journalists shows that employees of BAT “controlled the volumes, brands, marketing campaigns, timing and price levels throughout the smuggling distribution networks they exploited”.2 Actions have also been taken in the US against the tobacco industry for involvement in Canadian smuggling. While there is a need for more research on effective strategies to reduce or prevent smuggling, a number of actions are currently being proposed, including: Increased penalties ’Tax-paid’ stamps on tobacco products Special packaging and product markings to indicate duty-exempt status Requirement that manufacturers, exporters, importers, wholesalers, transporters, warehouses and retailers have tobacco-specific licenses. Requirement that every tobacco product manufacturer prints a unique serial number on all tobacco packaging Requirement that every tobacco manufacturer keep records, indicate on the label of exported cigarettes the country of final destination, indicate appropriate and country-specific health warnings Requirement that exporters post bonds on cigarette shipments that can only be released after the cigarettes have reached their final destination.3 These issues will be addressed in the Framework Convention for Tobacco Control. Continued overpage.
 are lost to smuggling.1 Factors that are considered to contribute to smuggling, include price differences between countries in addition to non-price factors, such as the degree of corruption and tolerance of contraband in a country. The tobacco industry often uses the smuggling issue as a reason to oppose tax increases, arguing that tax increases will not decrease tobacco use but only serve to increase smuggling. In fact, there is good evidence that a number of tobacco companies have themselves been involved in promoting smuggling. One example is the case of British American Tobacco (BAT). A report released in January 2000 by the International Consortium of Investigative Journalists shows that employees of BAT controlled the volumes, brands, marketing campaigns, timing and price levels throughout the smuggling distribution networks they exploited .2 Actions have also been taken in the US against the tobacco industry for involvement in Canadian smuggling. While there is a need for more research on effective strategies to reduce or prevent smuggling, a number of actions are currently being proposed, including: Increased penalties. ’Tax-paid’ stamps on tobacco products. Special packaging and product markings to indicate duty-exempt status. Requirement that manufacturers, exporters, importers, wholesalers, transporters, warehouses and retailers have tobacco-specific licenses. Requirement that every tobacco product manufacturer prints a unique serial number on all tobacco packaging. Requirement that every tobacco manufacturer keep records, indicate on the label of exported cigarettes the country of final destination, indicate appropriate and country-specific health warnings. Requirement that exporters post bonds on cigarette shipments that can only be released after the cigarettes have reached their final destination.3. These issues will be addressed in the Framework Convention for Tobacco Control. Continued overpage.")
95
Summary: WHO Recommendations for Comprehensive Tobacco Control
Comprehensive national programs should employ multiple strategies, including fiscal policy, information policy, establishment of smoke-free public places and provision of treatment Adequate support is critical and should include support for capacity building, applied research, surveillance and evaluation Public/media debate on tobacco control-related issues should be encouraged In their report: ‘Guidelines for controlling and monitoring the tobacco epidemic’1 the World Health Organization issued a series of recommendations derived from World Health Assembly resolutions on components of national tobacco control programs. The WHO recommends multi-pronged comprehensive national strategies. Ensuring adequate support for capacity building, applied research, evaluation and surveillance is emphasized, and also the need to encourage media debate on the importance of tobacco control, the fact that effective interventions exist, and the role of the industry in opposing tobacco control actions. Reference: 1. World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: World Health Organization; 1998.

96
WHO Tobacco Free Initiative
WHO Cabinet project established in 1998 by the Director General, Dr Gro Harlem Brundtland, to coordinate an improved global strategic response to tobacco as an important public health issue TFI works to build strong internal and external partnerships to achieve better tobacco control The deadly impact that tobacco poses for global health now and in the future was the primary reason for WHO’s strong explicit support for tobacco control on a worldwide basis. WHO established the Tobacco Free Initiative in July 1998 to co-ordinate a global strategic response. The goals of the Tobacco Free Initiative are to: ‘Galvanize global support for evidence-based tobacco control policies and actions’ ‘Build new and strengthen existing partnerships for action’ ‘Heighten awareness of the need to address tobacco at all levels of society’ ‘Accelerate national, regional and global strategy implementation’ ‘Commission policy research to support rapid, sustained and innovative actions’ ‘Mobilize resources to support required actions’ ‘Integrate tobacco into the broader agenda of health and development’ ‘Facilitate the development of an effective Framework Convention for Tobacco Control and related protocols’.1 Reference: 1. WHO. Tobacco Free Initiative Available at: (accessed June 2000).
.")
97
Framework Convention International legal instrument
Being negotiated by 191 WHO Member States World Health Assembly has called for adoption, no later than May 2003 Aim is to improve transnational tobacco control and cooperation The spectacular rise and spread of tobacco consumption around the world has been seen by the WHO as a challenge and an opportunity for action. A challenge to seek a global solution for a problem that is undermining the world’s health and economy; and an opportunity to propose to the world a first comprehensive response to deal with the burden of tobacco use. On 24 May 1999, the 191 members of the World Health Assembly (WHA) adopted a resolution calling for work to begin on the WHO Framework Convention on Tobacco Control (FCTC) –a new legal instrument that, depending upon political will, will potentially address issues as diverse as tobacco advertising and promotion, agricultural diversification, smuggling, taxes and subsidies. A record 50 nations pledged financial and political support for the Convention.1 The general objectives of the Framework Convention for Tobacco Control (FCTC) can be found on the WHO website. The protocols could include specific obligations to address, amongst other things: prices, smuggling, tax-free tobacco products, advertising/sponsorship, internet advertising/trade, testing methods, package design/labeling, information sharing, and agricultural diversification. The FCTC’s benefits to countries are many. The most significant benefit is that with the convention as a pathfinder and co-ordination vehicle, national public health policies, tailored around national needs, can be advanced without the risk of being undone by transnational phenomena. While the framework convention obligates States to co-operate in key areas, the process also serves to forge important links between countries and other potential partners. Countries can participate in the central framework while still deferring a decision on whether to participate in protocols. Reference: 1. The Framework Convention on Tobacco Control, a primer Available at: (accessed at June 2000).
 adopted a resolution calling for work to begin on the WHO Framework Convention on Tobacco Control (FCTC) –a new legal instrument that, depending upon political will, will potentially address issues as diverse as tobacco advertising and promotion, agricultural diversification, smuggling, taxes and subsidies. A record 50 nations pledged financial and political support for the Convention.1. The general objectives of the Framework Convention for Tobacco Control (FCTC) can be found on the WHO website. The protocols could include specific obligations to address, amongst other things: prices, smuggling, tax-free tobacco products, advertising/sponsorship, internet advertising/trade, testing methods, package design/labeling, information sharing, and agricultural diversification. The FCTC’s benefits to countries are many. The most significant benefit is that with the convention as a pathfinder and co-ordination vehicle, national public health policies, tailored around national needs, can be advanced without the risk of being undone by transnational phenomena. While the framework convention obligates States to co-operate in key areas, the process also serves to forge important links between countries and other potential partners. Countries can participate in the central framework while still deferring a decision on whether to participate in protocols. Reference: 1. The Framework Convention on Tobacco Control, a primer Available at: (accessed at June 2000).")
99
Early Efforts to Control Tobacco Use
King James I of England on active smoking: ‘’Smoking is a custom loathsome to the eye, hateful to the nose, harmful to the brain, dangerous to the lungs, and in the black, stinking fume thereof nearest resembling the horrible Stygian smoke of the pit that is bottomless’’ King James I of England on passive smoking: ‘’The wife must either take up smoking or resolve to live in a perpetual stinking torment’’ Researchers have documented efforts to control tobacco use as early as 1604 when King James I of England published ‘A Counterblaste To Tobacco.’1 Reference: 1. A Counterblaste to Tobacco. Available at: (accessed June 2000).
.")
100
Early Efforts to Control Tobacco Use
1620: Tobacco use is prohibited in Japan 1638: Use or distribution of tobacco is made a crime punishable by decapitation in China 1729: Bhutan, in first documented legislation, bans tobacco use in all religious places 1868: UK Parliament passes the railway bill, which mandates smoke-free cars to prevent injury to non-smokers 1890: 26 US states outlaw sale to minors Around the world during the 17th century, efforts were made to control tobacco use. Early regulations were established, though most did not last long. In 1624, Pope Urban VIII, threatened to excommunicate snuff users. In 1633, Sultan Murad IV (Turkey), ordered that tobacco users were to be executed as infidels, but the ban was lifted in In 1634, Czar Alexis (Russia) created a penalty for smokers. For the first offence, it was whipping, a slit in the nose and transportation to Siberia. For the second offence it was execution, but again, the ban was lifted in Tobacco use was prohibited in Switzerland in 1657. In 1729 in Bhutan, the first documented legislation that prohibited tobacco use in all religious places was passed. This law is still observed in Bhutan.1 Reference: 1. Borio G. Tobacco Timeline Available at: (accessed June 2000). Borio G. Tobacco Timeline, 1998
, ordered that tobacco users were to be executed as infidels, but the ban was lifted in In 1634, Czar Alexis (Russia) created a penalty for smokers. For the first offence, it was whipping, a slit in the nose and transportation to Siberia. For the second offence it was execution, but again, the ban was lifted in Tobacco use was prohibited in Switzerland in In 1729 in Bhutan, the first documented legislation that prohibited tobacco use in all religious places was passed. This law is still observed in Bhutan.1. Reference: 1. Borio G. Tobacco Timeline Available at: (accessed June 2000). Borio G. Tobacco Timeline,")
101
Modern Efforts to Control Tobacco Use
1970: US ban on TV and radio advertisement also ends free counter advertisement 1970: Singapore bans smoking in buses, cinemas, theatres and specified buildings 1971: Singapore bans tobacco advertising 1975: Norway bans tobacco advertising 1987: Hong Kong bans smokeless tobacco 1987: US Congress bans smoking on domestic flights of less than two hours 1998: California is the first state in the US to ban smoking in bars Increased efforts to control tobacco use appeared soon after the publication of scientific data that associated tobacco with specific diseases in the mid-1960s. Currently, over 90 countries have some sort of tobacco control policies. Finland, Iceland, Norway, Portugal and Singapore have comprehensive control measures that have been gradually developed since the 1970s.1 Reference: 1. World Health Organization. Tobacco or Health: A global status report. Geneva: World Health Organization, 1997. Slide Source: Borio G. Tobacco Timeline Available at: (accessed June 2000). Borio G. Tobacco Timeline, 1998
. Borio G. Tobacco Timeline,")
102
Early Indications of Tobacco-related Disease
1600s China: philosopher Fang Yizhi points out “long years of smoking scorches one’s lung” 1701: N. A Boiseregard warns that young people taking too much tobacco have trembling, unsteady hands, staggering feet and suffer a withering of “their noble parts” 1761: John Hill warns of cancer of the nose for snuff users 1795: Sammuel Thomas von Soemmering reports cancers of the lip in pipe smokers Tobacco was first used to treat various diseases. In 1571 Monardes, a doctor in Seville, listed 36 maladies cured by tobacco.1 In 1577, John Frampton translated Monardes into English and published it under the title ‘Joyfull Newes our of the Newe Founde Worlde’.2 Tobacco is recommended for headaches, colds, toothaches, healing wounds, worms, and halitosis among others, ‘this Herb Tobacco has particular virtue to heal griefs of the head, and in especially coming of cold causes, and so it cures the headache when it comes of a cold humor, or of a windy cause, the leaves must be put hot to it upon the grief, and multiplying them the time that is needful, until the grief be taken away’.2 However, as early as 1600, people began associating tobacco use with disease. The relationship between smoking and lung disease was first pointed out in China.1 Before smoking became popular, smokeless tobacco was already related to disease. In 1761, Dr. Hill performed the first clinical study of tobacco effects. He wrote a paper entitled ‘Caution Against the Immoderate Use of Snuff’ in which he described six cases of nasal ulcers/polypusses related to the excessive use of snuff. “It is evident therefore that no man should venture Snuff, who is not sure that he is not so far liable to a cancer: and no man can be sure of that.”3 References: 1. Borio G. Tobacco Timeline Available at: (accessed June 2000). 2. Of the tobacco and of His great vertues. Available at: (accessed June 2000). 3. Whelan E. A Smoking Gun: How The Tobacco Industry Gets Away With Murder, 1994; pp. 35. Philadelphia: Stickley Co. Cited in Hirschfelder AB. Encyclopedia of Smoking and Tobacco, Phoenix, Arizona; The Oryx Press. p.158. Borio G. Tobacco Timeline, 1998
. 2. Of the tobacco and of His great vertues. Available at: (accessed June 2000). 3. Whelan E. A Smoking Gun: How The Tobacco Industry Gets Away With Murder, 1994; pp. 35. Philadelphia: Stickley Co. Cited in Hirschfelder AB. Encyclopedia of Smoking and Tobacco, Phoenix, Arizona; The Oryx Press. p.158. Borio G. Tobacco Timeline,")
103
The Nazis and Tobacco Control
1920s: Nazi medical elite was very supportive of tobacco hazards 1930s–1940s: Researchers in Nazi Germany first showed an association between lung cancer and tobacco Although many believe that studies done in the US and the UK were the first to prove the link between lung cancer and tobacco, researchers in Nazi Germany showed this association in the 1930s and 1940s. The Nazi medical elite was very supportive of tobacco hazards research in the 1920s. Tobacco during the Nazi period was seen as a genetic poison, a cause of infertility, cancer and heart attacks. Back in 1921, JF Lehmann’s antisemitic ‘Munchener Medizinische Wochenscrift’ asked all ‘German doctors’ to combat smoking because of its harm to the body as well as its economic consequences on a country already impoverished by the war.1 Tobacco use was opposed by many: racial hygienists feared the corruption of the German germ plasm, industrial hygienists feared the reduction of the worker’s capacity, and nurses and midwifes feared harms to the ‘maternal organism.’1 “So many excellent men have been lost to tobacco poisoning” Adolf Hitler, 1942. Robert N.Proctor’s book,’The Nazi War on Cancer’ chronicles the story of the Nazi’s research and anti-tobacco campaign. Reference: 1. Proctor R. The campaign against tobacco. In The Nazi War on Cancer, Princeton NJ: Princeton University Press. Proctor, 1999

104
Early Indications that Tobacco Causes Disease: German Research
1929: Fritz Lickint publishes statistical evidence linking lung cancer and cigarettes 1939: Lickint publishes ‘Tabak und Organismus’ a 1,100 page volume, “the most comprehensive scholarly indictment of tobacco ever published” 1939: Muller presents the world’s first controlled epidemiological study of the tobacco–lung cancer relationship Fritz Lickint became Germany’s biggest promoter of the anti-smoking message, cautioning that tobacco had surpassed alcohol as a public health menace. To write his ‘Tabak und Organismus’, he surveyed eight thousand publications worldwide and blamed tobacco for cancers all along the ‘rauchstrasse’ (smoke alley) – lips, tongue, lining of the mouth, jaw, esophagus, windpipe, and lungs. He associated tobacco with arteriosclerosis, infant mortality, ulcers, halitosis, and dozens of other maladies. He characterized tobacco addiction (Tabakismus) and the people afflicted as Tabakisten. He also compared tobacco addicts to morphine addicts and made a convincing argument that ‘passive smoking’ posed a serious threat to non-smokers.1 Franz Muller’s most important contribution was his statistical investigation, prompted by his observation that the lung cancer patients in his care were often heavy smokers and that men were far more likely than women to contract the disease. He compared through questionnaires and medical histories the smoking behavior of lung cancer patients with that of a healthy ‘control group’. He concluded that ‘the extraordinary rise in tobacco use’ was the single most important cause of the rising incidence of lung cancer.1 Reference: 1. Proctor R. The campaign against tobacco. In The Nazi War on Cancer, Princeton NJ: Princeton University Press. Slide Source: Borio G. Tobacco Timeline Available at: (accessed June 2000). Borio G. Tobacco Timeline, 1998
 – lips, tongue, lining of the mouth, jaw, esophagus, windpipe, and lungs. He associated tobacco with arteriosclerosis, infant mortality, ulcers, halitosis, and dozens of other maladies. He characterized tobacco addiction (Tabakismus) and the people afflicted as Tabakisten. He also compared tobacco addicts to morphine addicts and made a convincing argument that ‘passive smoking’ posed a serious threat to non-smokers.1. Franz Muller’s most important contribution was his statistical investigation, prompted by his observation that the lung cancer patients in his care were often heavy smokers and that men were far more likely than women to contract the disease. He compared through questionnaires and medical histories the smoking behavior of lung cancer patients with that of a healthy ‘control group’. He concluded that ‘the extraordinary rise in tobacco use’ was the single most important cause of the rising incidence of lung cancer.1. Reference: 1. Proctor R. The campaign against tobacco. In The Nazi War on Cancer, Princeton NJ: Princeton University Press. Slide Source: Borio G. Tobacco Timeline Available at: (accessed June 2000). Borio G. Tobacco Timeline,")
105
Age-adjusted Prevalence of Smoking Among Men and Women in Europe
% current smokers In this study of smoking prevalence among young Europeans, over 16,400 students aged 18–30 years were surveyed in 21 European countries.1 The overall age-adjusted prevalence of smoking was 33% for men and 29% for women. This table shows that smoking prevalence in Europe ranges from as low as 10% in Finnish women to as high as 47% in Austrian men. In most European countries, smoking by male students was the same, or higher, than smoking by female students. Reference: 1. Steptoe A, Wardle J, Smith H, et al. Tobacco smoking in young adults from 21 European countries: association with attitudes and risk awareness. Addiction 1995; 90:571–582. Steptoe, Wardle and Smith, 1995

106
Leading Causes of Death Worldwide in 1990 and Estimated in 2020
The World Health Organization has estimated that, by 2020, tobacco use will account for 12% of all deaths worldwide (8.4 million).1 Reference: 1. World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: World Health Organization; 1998. Graph Source: World Health Organization. The tobacco epidemic: a global public health emergency. Tobacco Alert. Geneva: World Health Organization; 1996. 1990 2020 Number of deaths (millions) WHO, 1996
.1. Reference: 1. World Health Organization. Guidelines for controlling and monitoring the tobacco epidemic. Geneva: World Health Organization; Graph Source: World Health Organization. The tobacco epidemic: a global public health emergency. Tobacco Alert. Geneva: World Health Organization; Number of deaths (millions) WHO,")
108
Comparative Causes of Annual Deaths in the US
Smoking is the single most important preventable cause of death in the US, and in many other developed countries. Without effective interventions, it is predicted that the developing world will follow a similar pattern. Data for constructing this table came from the Centers for Disease Control (CDC). Using a specially developed software package (SAMMEC II software), CDC estimated that in the US in 1990, deaths were caused by tobacco. This included 30% of all cancer deaths and 21% of cardiovascular disease deaths.1 Reference: 1. Schultz JM, Novotny TE & Rice DP. Quantifying the disease impact of cigarette smoking with SAMMEC II software. Public Health Report 1991; 106:326–333. Graph Source: McGinnis JM & Foege WH. Actual causes of death in the United States. JAMA 1993; 270:2207–2212. McGinnis and Foege, 1993
. Using a specially developed software package (SAMMEC II software), CDC estimated that in the US in 1990, deaths were caused by tobacco. This included 30% of all cancer deaths and 21% of cardiovascular disease deaths.1. Reference: 1. Schultz JM, Novotny TE & Rice DP. Quantifying the disease impact of cigarette smoking with SAMMEC II software. Public Health Report 1991; 106:326–333. Graph Source: McGinnis JM & Foege WH. Actual causes of death in the United States. JAMA 1993; 270:2207–2212. McGinnis and Foege,")
109
Seçilmiş risk faktörlerine bağlı küresel ölüm ve sakatlanma, 1990 (x1000)
5,625 2,634 0.3 0.6

110
Gelenekler,din,yoksulluk halkın sigaraya
Gelişmekte olan ülkeler Sigara içme oranı Erkek % 50-70 Kadın % 2- 10 Gelenekler,din,yoksulluk halkın sigaraya başlamasını engellemiştir.

118
Sigaraya bağlı sakatlı -yıl, “DALYs ”
(disability-adjusted life-years)
")
119
Sigaraya bağlı ; sakatlı -yıl

123
DİKKAT: KANSER İMPOTANS YAPAR
DİKKAT: KANSER İMPOTANS YAPAR

124
Türkiye’deki ihracat firmaları
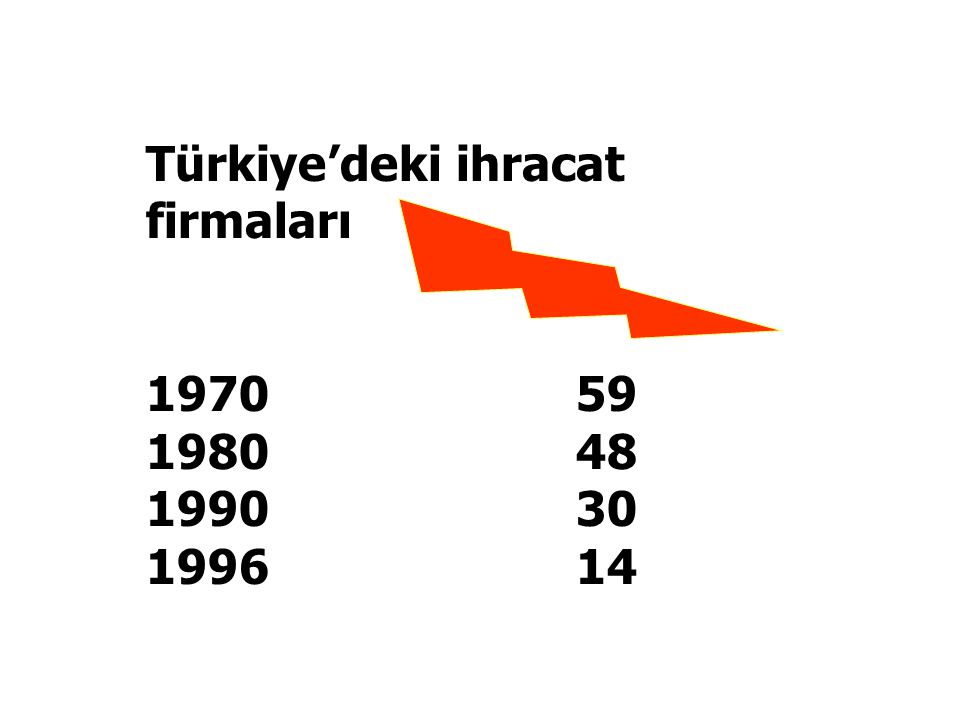
125
Tütün Üreticisi Ülkeler
Üretim (1000 ton) Toplamın yüzdesi Çin 3390 42.1 ABD 746 9.3 Hindistan 624 7.8 Brezilya 577 7.2 Türkiye 296 3.7 Zimbabwe 192 2.4 Endonezya 184 2.3 Diğerleri 2039 27.3 Dünya toplamı 8048 100.0
 Toplamın yüzdesi. Çin ABD Hindistan Brezilya Türkiye Zimbabwe Endonezya Diğerleri Dünya toplamı")
126
SİGARA & YAŞAM Sigara günümüzde tüm dünya da her 10 erişkinden
birinin ölüm nedenidir. 2030 yılında 10 milyon ölüme ve her altı ölümden birisinin nedeni olacak. Şu anda yaşayan insan sigaraya bağlı olarak ölecek. Uzun süredir sigara içenlerin yarısı sagaraya bağlı ölür. Beklenenden 2025 yıl daha az yaşarlar.

127
TÜTÜN KONTROLÜNDE ESASLAR
Bilimsel bilginin artırılması Halk Sağlığı Eğitimleri Kamuya açık alanlarda sınırlama ve yasaklar Tütün Kullanımı ve ticaretini kabul edilir olmaktan çıkarka Tütün ticareti ve kula

128
SİGARAYA BAĞLI ÖLÜMLER

Benzer bir sunumlar
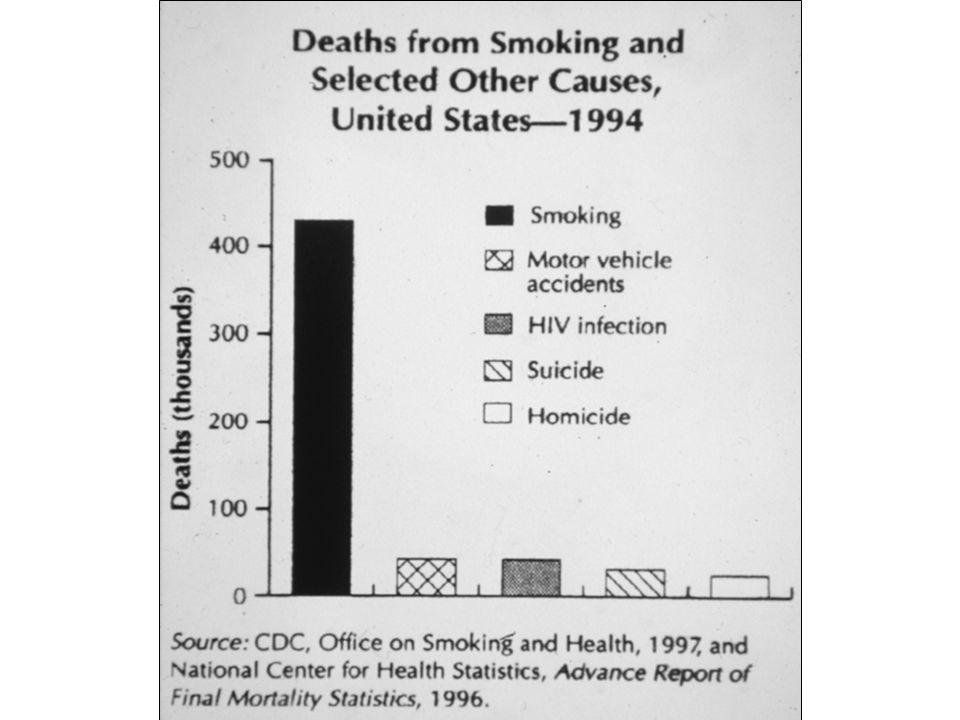






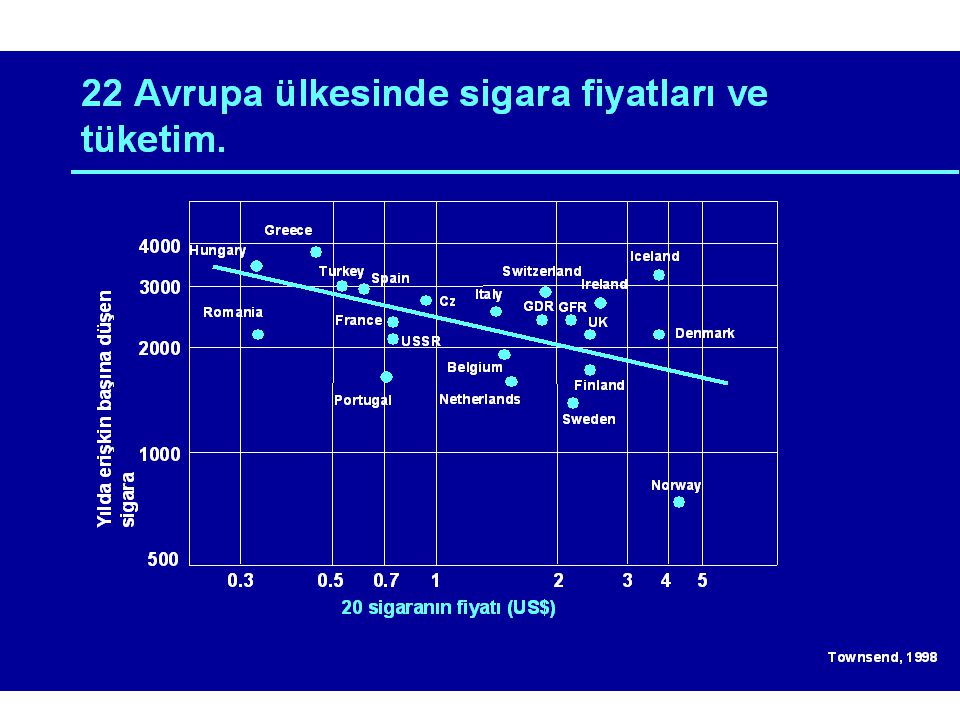
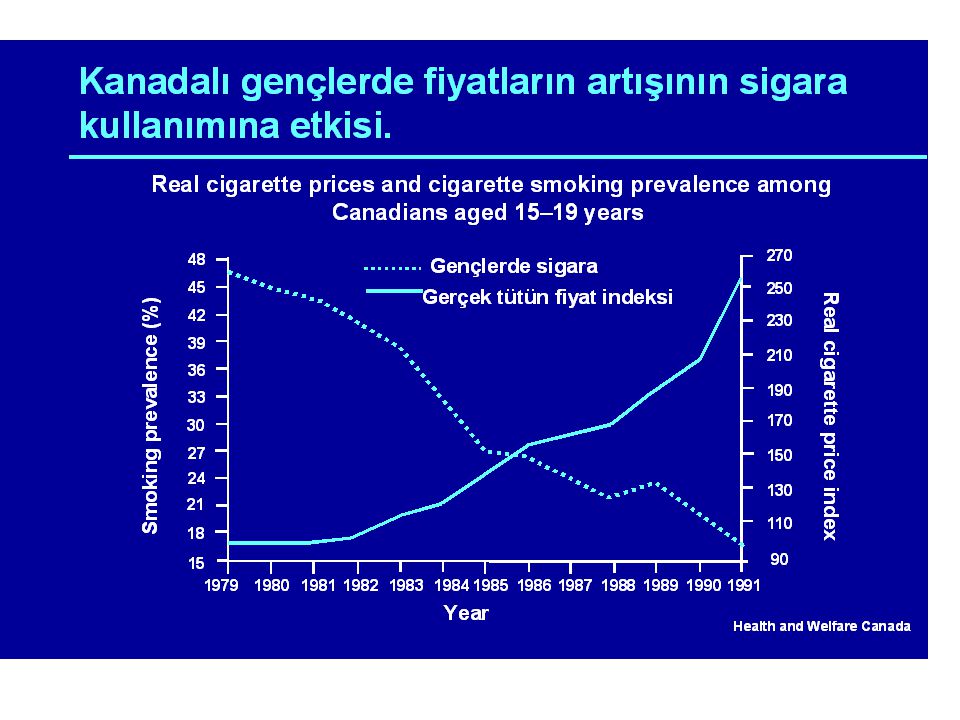
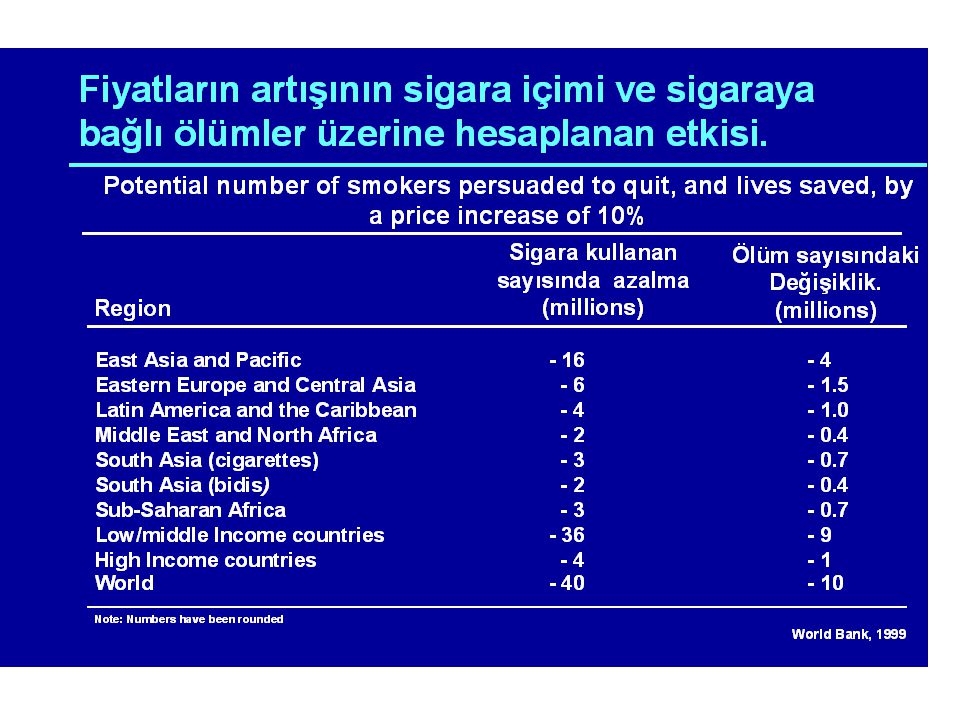
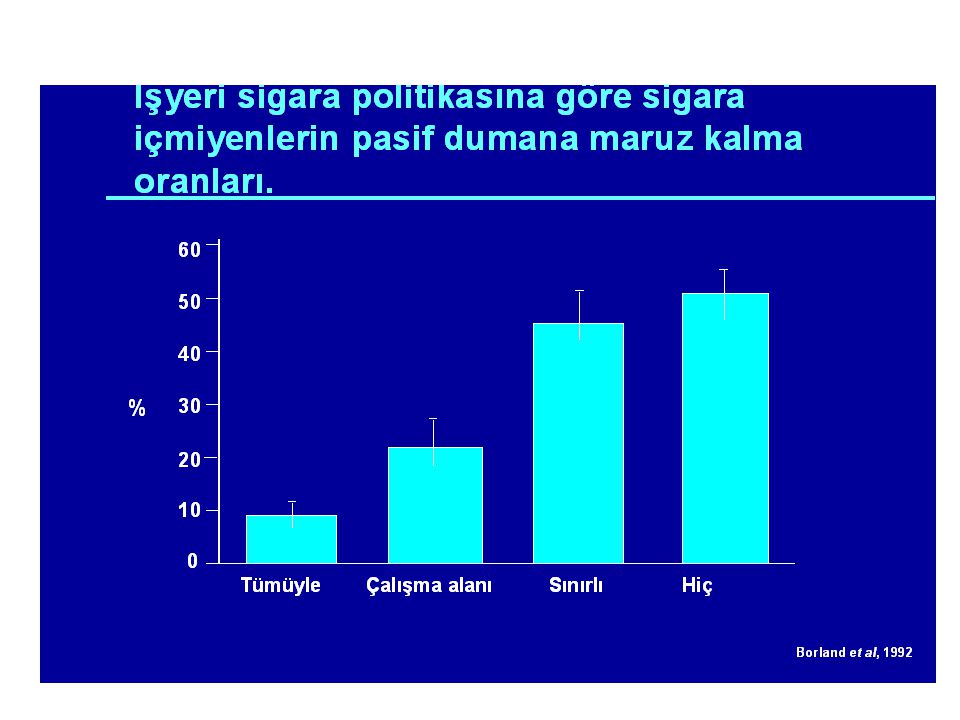


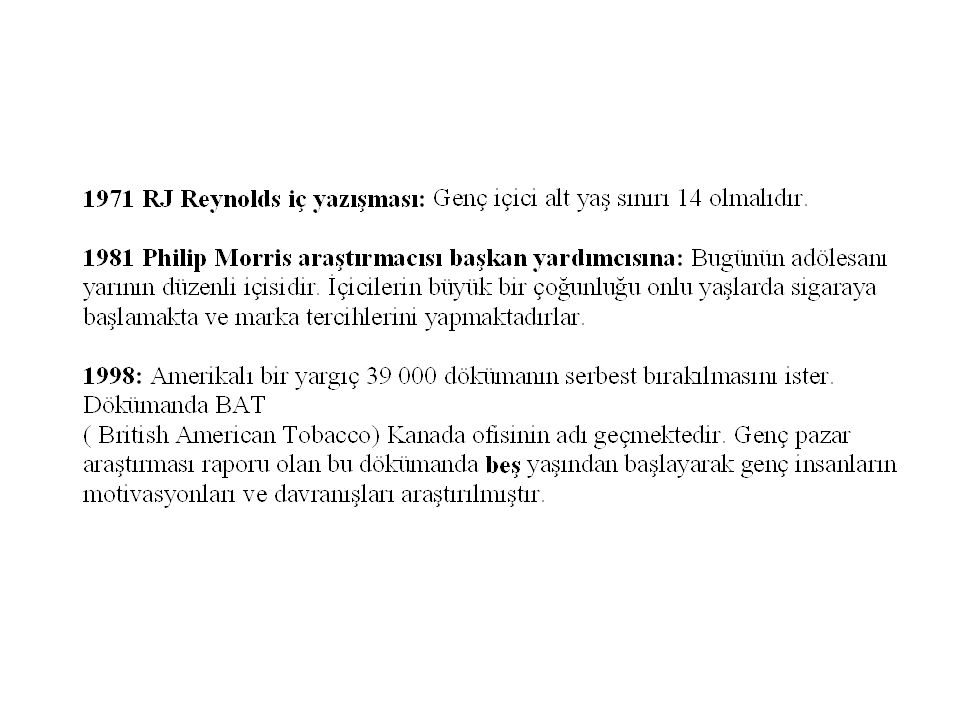

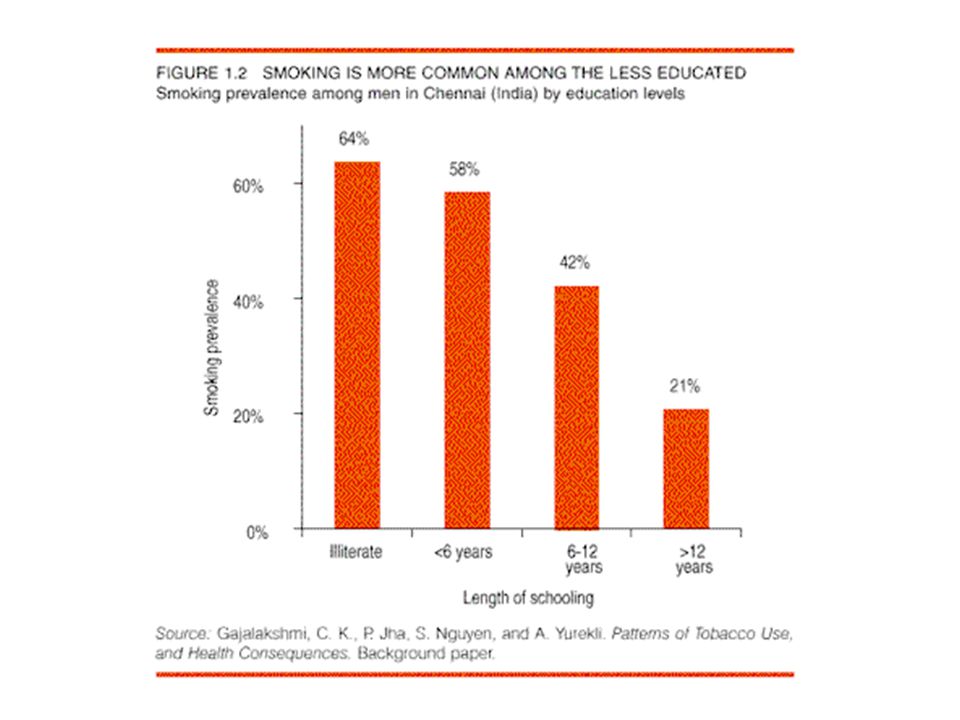
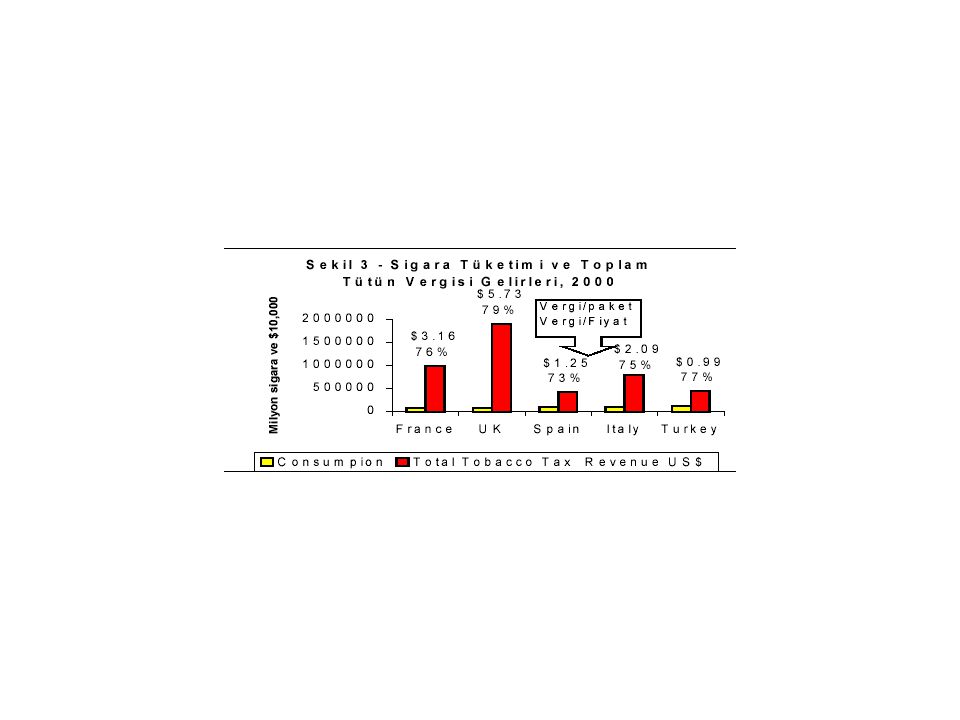
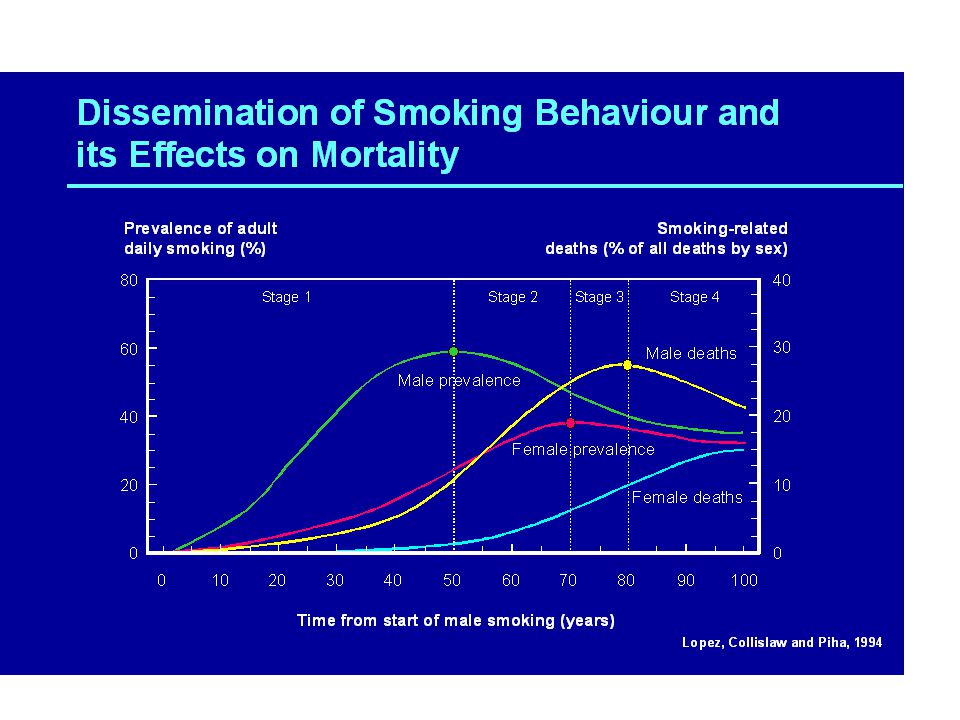
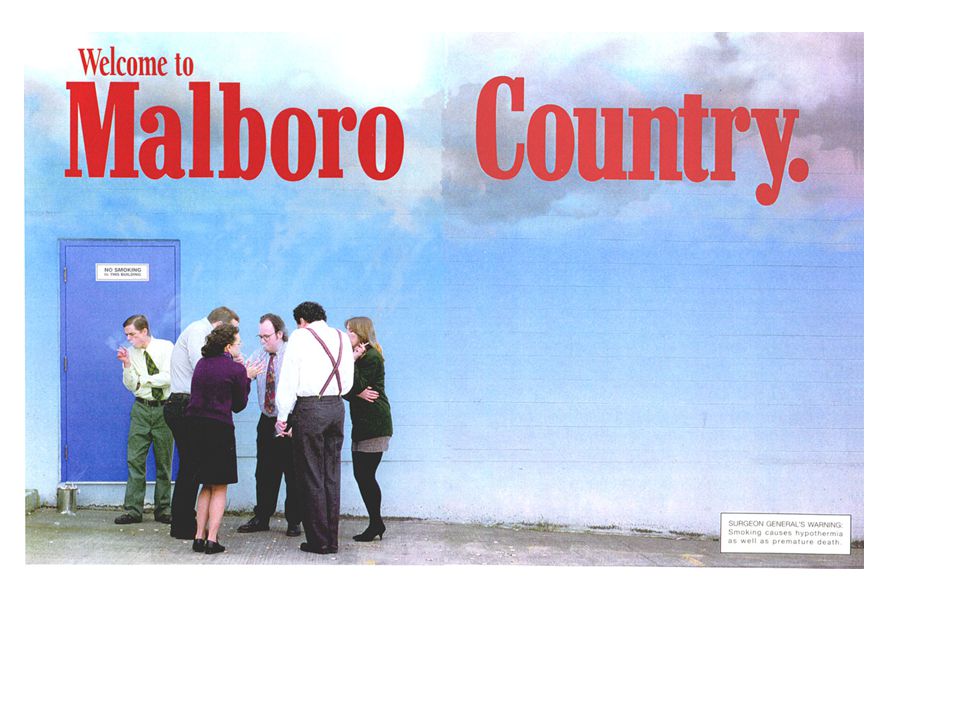




>")














 TURKISH COMMERCIAL.>")
