Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Kan transfüzyonları ve HIV Bulaş – Güncel tedavi
Prof. Dr. Volkan Korten Marmara Üniversitesi Tıp Fakültesi İnfeksiyon Hast. ve Klin. Mikrobiyoloji AD

2
HIV/AIDS VAKALARI (1 Ekim 1985-30 Haziran 2007) 2073 HIV, 638 AIDS vakası, Toplam 2711
Altan P, 2007

3
MUHTEMEL GEÇiŞ YOLUNA GÖRE HIV/AIDS VAKALARI
(1 Ekim Haziran n:2404) n:5, n:10 hemofili Altan P, 2007
 n:5, n:10 hemofili. Altan P,")
4
Uygun viral antikor ve antijen (P24) taramasına rağmen
Kan, donörden infeksiyonun çok erken dönemlerinde “seronegatif pencere periyodu” toplanırsa HIV bulaşı mümkün Bu nedenle bazı ülkelerde havuzlanmış kanlara “nükleik asid amplifikasyon testleri” uygulanıyor. NAT ile pencere 16 g → 10 g NAT sonrası bulaş: HIV (1:1.4 milyon) HCV 1.2 m, HBV 150 bin TRENDS in Molecular Medicine 2002;8:355-8
 HCV 1.2 m, HBV 150 bin. TRENDS in Molecular Medicine 2002;8:")
5
Avrupa Birliği - ABD Sadece serolojik testlerle bulaş
1:1.3 milyon, NAT ile 1: 2-4 milyon NAT’ın maliyet-yarar oranı çok düşük Yanlış kan transfüzyonları ve immunolojik yan etkileri önlemek çok daha önemli Transfusion Clinique et Biologique 2003;10:1–5.

7
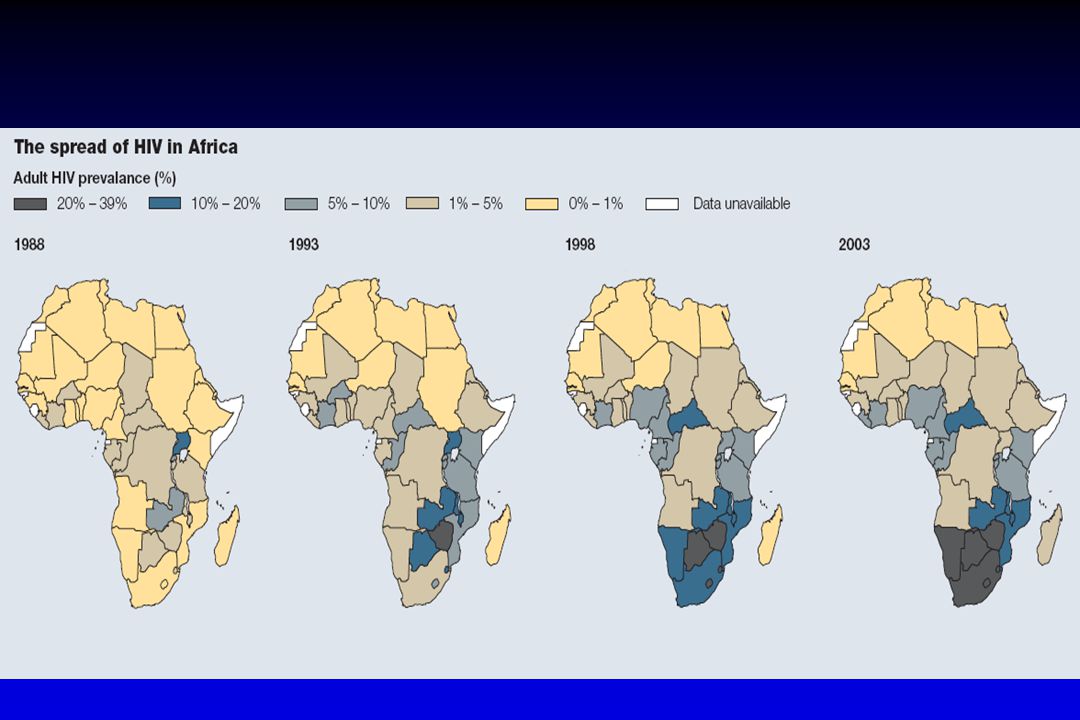
HIV’in yoğun görüldüğü ülkeler
Nijerya (erişkin ~ % 5) Kan bankalarından rastgele serolojik taramada negatif çıkmış 500 kan Antijen (+): 6 (%1.2) = WB: 4 şüpheli, PCR (+): 3 Epideminin yoğun görüldüğü Afrika ülkelerinde transfüzyonla bulaş önemli bir sorun Transactions of the Royal Society of Tropical Medicine and Hygiene (2008) 102, 284—287
 Kan bankalarından rastgele serolojik taramada negatif çıkmış 500 kan. Antijen (+): 6 (%1.2) = WB: 4 şüpheli, PCR (+): 3. Epideminin yoğun görüldüğü Afrika ülkelerinde transfüzyonla bulaş önemli bir sorun. Transactions of the Royal Society of Tropical Medicine and Hygiene (2008) 102, 284—287.")
8
Antiretroviral ilaçlar etki mekanizması
MS18 Antiretroviral ilaçlar etki mekanizması Slide 1.2 PI buraya etkili Protease NNRTI Buraya etkili Viral assembly Translation Protein cleavage RNA and reverse transcription Transcription Injection of capsid contents The combination of STOCRIN™ and indinavir (IDV) provides effective therapy because the combination takes advantage of the different modes of action of these drugs. Together, these agents attack HIV at two critical points in the viral replication cycle.1 STOCRIN acts early in virion assembly. By binding directly to reverse transcriptase and thus blocking the conversion of viral RNA into DNA, STOCRIN prevents the virus from using the host cell’s mechanisms to create another generation of viral particles.1,2 IDV, on the other hand, acts at the final stages of virion assembly. A competitive inhibitor of HIV protease, IDV blocks the cleavage of viral particles into functional enzymes and proteins. Viral proteins formed in the presence of IDV are defective and noninfectious, incapable of establishing new cycles of infection.1 Integrase RNA DNA Provirus (circular structure) Maturation Integration of Provirus DNA into Host DNA HIV particle Binding Completed HIV particle Adapted from HIV/AIDS Handbook. 4th ed. Boston: Total Learning Concepts, 1999; Ritchie DJ. In: Powderly WG, ed. Manual of HIV Therapeutics. Philadelphia: Lippincott-Raven, 1997:33-41.
 provides effective therapy because the combination takes advantage of the different modes of action of these drugs. Together, these agents attack HIV at two critical points in the viral replication cycle.1. STOCRIN acts early in virion assembly. By binding directly to reverse transcriptase and thus blocking the conversion of viral RNA into DNA, STOCRIN prevents the virus from using the host cell’s mechanisms to create another generation of viral particles.1,2. IDV, on the other hand, acts at the final stages of virion assembly. A competitive inhibitor of HIV protease, IDV blocks the cleavage of viral particles into functional enzymes and proteins. Viral proteins formed in the presence of IDV are defective and noninfectious, incapable of establishing new cycles of infection.1. Integrase. RNA. DNA. Provirus (circular structure) Maturation. Integration of Provirus DNA into Host DNA. HIV particle. Binding. Completed HIV particle. Adapted from HIV/AIDS Handbook. 4th ed. Boston: Total Learning Concepts, 1999; Ritchie DJ. In: Powderly WG, ed. Manual of HIV Therapeutics. Philadelphia: Lippincott-Raven, 1997:")
9
Antiretroviral ilaçlar - 2007
NRTI Abacavir ABC Didanosine DDI Emtricitabine FTC Lamivudine 3TC Stavudine D4T Tenofovir TDF Zidovudine ZDV NNRTI Delavirdine DLV Efavirenz EFV Nevirapine NVP Fusion Inhibitor Enfuvirtide T-20 PI Amprenavir APV Atazanavir ATV Darunavir DRV Fosamprenavir FPV Indinavir IDV Lopinavir LPV Nelfinavir NFV Ritonavir RTV Saquinavir SQV hard gel HGC tablet INV Tipranavir TPV CCR5 Coreceptor Antagonist Maraviroc MVC Integrase Inhibitor Raltegravir RAL 22 molekül

10
Geliştirilmekte olan yeni antiretroviraller: Varolan ilaç sınıfları
TNX-355 CCR5 inhibitors CXCR4 inhibitors Maturatio PA-457 MK-0518 GS-9137 Entry inhibitors Reverse transcriptase inhibitors Mature virus Protease inhibitors Integrase inhibitors

11
Yeni antiretrovirallerin piyasaya verilme tahminleri
CXCR4 inhibitors Entry inhibitors (anti-gp120, CCR5) GS-9137 Maturation inhibitors Vicriviroc Integrase inhibitors Maraviroc TNX-355 MK-0518 Bevirimat (PA-457) 2006 2007 2008 2009 2010 Etravirine (TMC125) TMC278 PIs Brecanavir NNRTI Apricitabine NRTI
 GS Maturation inhibitors. Vicriviroc. Integrase inhibitors. Maraviroc. TNX-355. MK Bevirimat (PA-457) Etravirine (TMC125) TMC278. PIs. Brecanavir. NNRTI. Apricitabine. NRTI.")
12
TEDAVİ HEDEFLERİ Etkinlik
Maksimal ve uzun süreli viral yük baskılanması Tedaviye uyum çok önemli Tolerabilite Günlük aktivitelere olan etkiyi minimale indirmek Tedaviye uyumu, böylece etkinliği etkileyebilir Emniyet Zarar verme: emin bir tedavi rejimi sağla Kurtarma rejimine olanak sağla İlerideki tedavi seçeneklerine olanak sağla

13
Başlangıç tedavisi: NNRTI’ler
Avantajlar PI-temelli rejimlere göre daha az yağ dağılımı ve dislipidemi problemi Gelecekte PI seçeneği korunur Dezavantajlar Tek mutasyonla - direnç NNRTI’ler arası çapraz direnç Raş; hepatotoksisite Potansiyel ilaç etkileşimleri (CYP450)
")
14
Başlangıç tedavisi: PI’leri
Avantajlar En uzun prospektif bilgi Gelecekte NNRTI seçeneği korunur Dezavantajlar Metabolik komplikasyonlar (yağ dağılımı, dislipidemi, insulin rezistansı) Daha fazla potansiyel ilaç etkileşimleri (CYP450), özellikle ritonavir ile
 Daha fazla potansiyel ilaç etkileşimleri (CYP450), özellikle ritonavir ile.")
15
NRTI’ler: advers etkiler
Tüm NRTI’ler: Laktik asidoz ve KC yağlanması (stavudine ile daha yüksek) Lipodistrofi (stavudine ile daha yüksek) The combined use of didanosine and stavudine as a 2-NRTI backbone can result in a high incidence of toxicities, particularly peripheral neuropathy, pancreatitis, and lactic acidosis [50, 87, 99].This combination has been implicated in several deaths in HIV-1 infected pregnant women secondary to severe lactic acidosis with or without hepatic steatosis and pancreatitis [100]. In general, a combination containing didanosine and stavudine should be avoided unless other 2-NRTI combinations have failed or have caused unacceptable toxicities, and where potential benefits outweigh the risks of toxicities (DIII).
 Lipodistrofi (stavudine ile daha yüksek) The combined use of didanosine and stavudine as a 2-NRTI backbone can result in a high incidence of toxicities, particularly peripheral neuropathy, pancreatitis, and lactic acidosis [50, 87, 99].This combination has been implicated in several deaths in HIV-1 infected pregnant women secondary to severe lactic acidosis with or without hepatic steatosis and pancreatitis [100]. In general, a combination containing didanosine and stavudine should be avoided unless other 2-NRTI combinations have failed or have caused unacceptable toxicities, and where potential benefits outweigh the risks of toxicities (DIII).")
16
Antiretroviral ilaçların gelişim çizelgesi
Combivir 00 Truvada 08 94 99 DLV 02 ? 98 97 NVP ddC 95 ABC TDF 97 ZDV ddI d4T EFV 06-07 FTC 3TC ’87 ’88 ’89 ’90 ’91 ’92 ’93 ’94 ’95 ’96 ’97 ’98 ’99 ’00 ’01 ’02 ’03 ’04 ’05 ’06 ’07 Speaking Notes: Once again you see all the ARVs currently approved for use in the US market, this time mapped by their year of release. Note that from 1987 to 1995, the first 5 ARV drugs developed were all nucleoside analogues. Thus, when the idea of combining drugs together arose, the first combinations utilized drugs that were then available, i.e., a pair of nucleosides: either zidovudine (Retrovir) and zalcitabine (Hivid), didanosine (Videx), or lamivudine (Epivir), or the combination of lamivudine (Epivir) and stavudine (Zerit). NRTI SQR NFV LPV/r ATV 01 NNRTI FPV DRV PI 97 APV RTV TPV Entry inhibitor T-20 MVC 98 IDV
 and zalcitabine (Hivid), didanosine (Videx), or lamivudine (Epivir), or the combination of lamivudine (Epivir) and stavudine (Zerit). NRTI. SQR. NFV. LPV/r. ATV. 01. NNRTI. FPV. DRV. PI. 97. APV. RTV. TPV. Entry inhibitor. T-20. MVC. 98. IDV.")
17
Daha önce tedavi almamış hastalarda başlangıç tedavisi: Rejimi seçmek
Göz önüne alınması gereken faktörler: Ko-morbidite (KC, psikiyatrik, kardiyovasküler hastalık, tüberküloz, gebelik) Uyum potansiyeli Doz uygunluğu (hap sayısı, doz aralığı) Potansiyel yan etkiler Potansiyel ilaç etkileşimleri Gebe kalma riski Direnç testi sonuçları Cins ve CD4 sayısı, eğer nevirapine düşünülüyorsa
 Uyum potansiyeli. Doz uygunluğu (hap sayısı, doz aralığı) Potansiyel yan etkiler. Potansiyel ilaç etkileşimleri. Gebe kalma riski. Direnç testi sonuçları. Cins ve CD4 sayısı, eğer nevirapine düşünülüyorsa.")
18
Kronik infeksiyonda tedavi başlama endikasyonları
Klinik kategori CD4+ T hücre sayısı Plasma HIV RNA Öneriler Semptomatik (AIDS, şiddetli semptomlar), gebeler, HIVAN, HepB ko-inf. Herhangi bir değer Tedavi et Asemptomatik, AIDS <200 hücre /µL Asemptomatik >200 hücre/µL, fakat <350 hücre/µL The decision to begin therapy for the asymptomatic patient is complex and must be made in the setting of careful patient counseling and education. Considerations of initiating antiretroviral therapy should be primarily based on the prognosis of diseasefree survival as determined by baseline CD4+ T cell count [60-62] (Figure A and Tables 4a, 4b). Also important are baseline viral load [60-62], readiness of the patient to begin therapy; and assessment of potential benefits and risks of initiating therapy for asymptomatic persons, including short-and long-term adverse drug effects; the likelihood, after counseling and education, of adherence to the prescribed treatment regimen. Recommendations vary according to the CD4 count and viral load of the patient, as follows. <200 CD4+ T cell count, with AIDS-defining illness, or symptomatic. Randomized clinical trials provide strong evidence of improved survival and reduced disease progression by treating symptomatic patients and patients with <200 CD4+ T cells/mm3 [63-66]. Observational cohorts indicate a strong relationship between lower CD4+ T cell counts and higher plasma HIV RNA levels in terms of risk for progression to AIDS for untreated persons and antiretroviral-naïve patients beginning treatment. These data provide strong support for the conclusion that therapy should be initiated in patients with CD4+ T cell count <200 cells/mm3 (Figure A and Table 4a) (AI) [60, 61]. CD4+ T cell count, patient asymptomatic. The optimal time to initiate antiretroviral therapy among asymptomatic patients with CD4+ T cell counts >200 cells/mm3 is unknown. For these patients, the strength of the recommendation for therapy must balance other considerations, such as patient readiness for treatment and potential drug toxicities. After considering available data in terms of the relative risk for progression to AIDS at certain CD4+ T cell counts and viral loads, and the potential risks and benefits associated with initiating therapy, most specialists in this area believe that the evidence supports initiating therapy in asymptomatic HIV-infected persons with a CD4+ T cell count of cells/mm3 (BII). There is a paucity of data from randomized, controlled trials concerning clinical endpoints (e.g., the development of AIDS-defining illnesses or death) for asymptomatic persons with >200 CD4+ T cells/mm3 to guide decisions on when to initiate therapy. Observational data from cohorts of HIV-infected persons provide some guidance to assist in risk assessment for disease progression. One source of observational data comes from cohorts of untreated individuals with regular measurements of CD4+ T cell counts and HIV RNA levels. Table 4b is taken from a report by the CASCADE Collaboration, composed of 20 cohorts in Europe and Australia [62]. The information in this table provides an estimate of the short-term (6-month) risk of AIDS progression according to CD4+ T cell count, HIV RNA level, and age. These estimates can be considered in making the decision about whether to start antiretroviral therapy before the next clinic visit. Another source of observational data is from cohorts that follow patients after the initiation of antiretroviral treatment. A pooled analysis of 13 cohorts from Europe and North America provide the most precise information on prognosis following the initiation of treatment [61]. These data indicate that CD4+ T cell count is a much more important prognostic indicator than viral load for those initiating therapy. In this study, risk of progression was also greater for those with a viral load >100,000, older patients, those infected through injecting drug use, and those with a previous diagnosis of AIDS. The following chart shows the risk of progression to AIDS or death after 3 years, according to CD4+ T cell count and HIV RNA level at the time antiretroviral therapy was initiated. These data are from a large subset of patients less than 50 years old and without a history of an AIDSdefining illness or injection drug use: CD4+ T cell count 3 yr-probability VL <105 VL >105 cells/mm3 16 % 20% cells/mm3 12 % 16% cells/mm3 9.3 % 12% cells/mm3 4.7 % 6.1% >350 cells/mm3 3.4 % 4.4% These data provide strong support for the recommendation, based on observational cohort , that therapy should be initiated before the CD4+ T cell count declines to <200 cells/mm3. However, differences in risk for those with CD4+ T cell counts between 200–350 and >350 cells/mm3 are based on too few events, and too short a follow-up period, to make reliable statements about when treatment should be started. Athough there are clear strengths to these observational data, there are also important limitations. Uncontrolled confounding factors could impact estimates in both studies. Furthermore, neither study provides direct evidence on the optimum CD4+ T cell count to begin therapy. Such data will have to come from studies that follow patients who start therapy at different CD4+ T cell counts greater than 200 cells/mm3 and compare them with a similar group of patients (e.g., with similar CD4+ T cell count and HIV RNA level) who defer treatment. To completely balance the benefits and risks of therapy, follow-up will have to examine progression to AIDS, major toxicities, and death. >350 CD4+ T cell count, patient asymptomatic. There is little evidence on the benefit of initiating therapy in asymptomatic patients with CD4+ T cell count > 350 cells/mm3. Most clinicians would defer therapy. • The deferred treatment approach is based on the recognition that robust immune reconstitution still occurs in the majority of patients who initiate treatment while CD4+ T cell counts are in the 200– 350 cells/mm3range. Also, toxicity risks and adherence challenges generally outweigh the benefits of initiating therapy at CD4+ T cell counts >350 cells/mm3. In the deferred treatment approach, increased levels of plasma HIV RNA (i.e., >100,000 copies/mL) are an indication for monitoring of CD4+ T cell counts and plasma HIV RNA levels at least every three months, but not necessarily for initiation of therapy. For patients with HIV RNA <100,000 copies/mL, therapy should be deferred (DII). • In the early treatment approach, asymptomatic patients with CD4+ T cell counts >350 cells/mm3 and levels of plasma HIV RNA >100,000 copies/mL would be treated because of the risk for immunologic deterioration and disease progression (CII). An estimate of the short term risk of AIDS progression may be useful in guiding clinicians and patients as they weigh the risks and benefits of initiating versus deferring therapy in this CD4 cell range. As cited above, Table 4b provides an analysis of data from the CASCADE Collaboration, demonstrating the risk of AIDS progression within 6 months for different strata of CD4+ T cell count, viral load, and age. As seen in Table 4b, a 55 year old with a CD4+ T cell count of 350 and a HIV viral load of 300,000 copies/mL has a 5% chance of progression to an AIDS-defining diagnosis in 6 months, compared with a 1.2% chance for a similar patient with a viral load of 3,000 copies/mL. 1/08
, gebeler, HIVAN, HepB ko-inf. Herhangi bir değer. Tedavi et. Asemptomatik, AIDS. <200 hücre /µL. Asemptomatik. >200 hücre/µL, fakat <350 hücre/µL. The decision to begin therapy for the asymptomatic. patient is complex and must be made in the setting of. careful patient counseling and education. Considerations of initiating antiretroviral therapy. should be primarily based on the prognosis of diseasefree. survival as determined by baseline CD4+ T cell. count [60-62] (Figure A and Tables 4a, 4b). Also. important are baseline viral load [60-62], readiness of. the patient to begin therapy; and assessment of. potential benefits and risks of initiating therapy for. asymptomatic persons, including short-and long-term. adverse drug effects; the likelihood, after counseling. and education, of adherence to the prescribed treatment. regimen. Recommendations vary according to the CD4 count. and viral load of the patient, as follows. <200 CD4+ T cell count, with AIDS-defining illness, or symptomatic. Randomized clinical trials provide. strong evidence of improved survival and reduced. disease progression by treating symptomatic patients. and patients with <200 CD4+ T cells/mm3 [63-66]. Observational cohorts indicate a strong relationship. between lower CD4+ T cell counts and higher plasma. HIV RNA levels in terms of risk for progression to. AIDS for untreated persons and antiretroviral-naïve. patients beginning treatment. These data provide strong. support for the conclusion that therapy should be. initiated in patients with CD4+ T cell count <200. cells/mm3 (Figure A and Table 4a) (AI) [60, 61] CD4+ T cell count, patient. asymptomatic. The optimal time to initiate. antiretroviral therapy among asymptomatic patients. with CD4+ T cell counts >200 cells/mm3 is unknown. For these patients, the strength of the recommendation. for therapy must balance other considerations, such as. patient readiness for treatment and potential drug. toxicities. After considering available data in terms of the relative. risk for progression to AIDS at certain CD4+ T cell. counts and viral loads, and the potential risks and. benefits associated with initiating therapy, most. specialists in this area believe that the evidence supports. initiating therapy in asymptomatic HIV-infected persons. with a CD4+ T cell count of cells/mm3 (BII). There is a paucity of data from randomized, controlled. trials concerning clinical endpoints (e.g., the. development of AIDS-defining illnesses or death) for. asymptomatic persons with >200 CD4+ T cells/mm3 to. guide decisions on when to initiate therapy. Observational data from cohorts of HIV-infected. persons provide some guidance to assist in risk. assessment for disease progression. One source of observational data comes from cohorts. of untreated individuals with regular measurements of. CD4+ T cell counts and HIV RNA levels. Table 4b is. taken from a report by the CASCADE Collaboration, composed of 20 cohorts in Europe and Australia [62]. The information in this table provides an estimate of. the short-term (6-month) risk of AIDS progression. according to CD4+ T cell count, HIV RNA level, and. age. These estimates can be considered in making the. decision about whether to start antiretroviral therapy. before the next clinic visit. Another source of observational data is from cohorts. that follow patients after the initiation of antiretroviral. treatment. A pooled analysis of 13 cohorts from. Europe and North America provide the most precise. information on prognosis following the initiation of. treatment [61]. These data indicate that CD4+ T cell. count is a much more important prognostic indicator. than viral load for those initiating therapy. In this. study, risk of progression was also greater for those. with a viral load >100,000, older patients, those. infected through injecting drug use, and those with a. previous diagnosis of AIDS. The following chart. shows the risk of progression to AIDS or death after 3. years, according to CD4+ T cell count and HIV RNA. level at the time antiretroviral therapy was initiated. These data are from a large subset of patients less than. 50 years old and without a history of an AIDSdefining. illness or injection drug use: CD4+ T cell count 3 yr-probability. VL <105 VL > cells/mm3 16 % 20% cells/mm3 12 % 16% cells/mm3 9.3 % 12% cells/mm3 4.7 % 6.1% >350 cells/mm3 3.4 % 4.4% These data provide strong support for the. recommendation, based on observational cohort , that. therapy should be initiated before the CD4+ T cell. count declines to <200 cells/mm3. However, differences in risk for those with CD4+ T cell counts. between 200–350 and >350 cells/mm3 are based on too. few events, and too short a follow-up period, to make. reliable statements about when treatment should be. started. Athough there are clear strengths to these. observational data, there are also important. limitations. Uncontrolled confounding factors could. impact estimates in both studies. Furthermore, neither. study provides direct evidence on the optimum CD4+ T cell count to begin therapy. Such data will have to. come from studies that follow patients who start. therapy at different CD4+ T cell counts greater than. 200 cells/mm3 and compare them with a similar group. of patients (e.g., with similar CD4+ T cell count and. HIV RNA level) who defer treatment. To completely. balance the benefits and risks of therapy, follow-up. will have to examine progression to AIDS, major. toxicities, and death. >350 CD4+ T cell count, patient asymptomatic. There is little evidence on the benefit of initiating. therapy in asymptomatic patients with CD4+ T cell. count > 350 cells/mm3. Most clinicians would defer. therapy. • The deferred treatment approach is based on the. recognition that robust immune reconstitution still. occurs in the majority of patients who initiate. treatment while CD4+ T cell counts are in the 200– 350 cells/mm3range. Also, toxicity risks and. adherence challenges generally outweigh the. benefits of initiating therapy at CD4+ T cell counts. >350 cells/mm3. In the deferred treatment approach, increased levels of plasma HIV RNA (i.e., >100,000. copies/mL) are an indication for monitoring of. CD4+ T cell counts and plasma HIV RNA levels at. least every three months, but not necessarily for. initiation of therapy. For patients with HIV RNA. <100,000 copies/mL, therapy should be deferred. (DII). • In the early treatment approach, asymptomatic. patients with CD4+ T cell counts >350 cells/mm3. and levels of plasma HIV RNA >100,000. copies/mL would be treated because of the risk for. immunologic deterioration and disease progression. (CII). An estimate of the short term risk of AIDS progression. may be useful in guiding clinicians and patients as they. weigh the risks and benefits of initiating versus. deferring therapy in this CD4 cell range. As cited above, Table 4b provides an analysis of data from the. CASCADE Collaboration, demonstrating the risk of. AIDS progression within 6 months for different strata of. CD4+ T cell count, viral load, and age. As seen in Table. 4b, a 55 year old with a CD4+ T cell count of 350 and a. HIV viral load of 300,000 copies/mL has a 5% chance. of progression to an AIDS-defining diagnosis in 6. months, compared with a 1.2% chance for a similar. patient with a viral load of 3,000 copies/mL. 1/08.")
19
Kronik infeksiyonda tedavi başlama endikasyonları
Klinik kategori CD4+ T hücre sayısı Öneriler Asemptomatik >350 hücre/µL Optimal başlama zamanı belli değil. Hasta senaryoları ve komorbiditeler göz önüne alınmalı ≥100,000 kopye/mL Yılda > 120 hücre CD4 düşüşü Efektif tedavisi olmayan durumlar (demans, PMLE, cryptosporidiosis vs) 1/08
 1/08.")
20
CD4+ hücre sayısına göre HAART başlangıcında kümülatif AIDS/ölüm olasılığı : ART Cohort Collaboration. Sterne J, CROI 2006; Abstract 525.

21
Yıllar içinde CD4 artışı – Johns Hopkins HIV Clinical Cohort
Moore RD, CID 2007; 44:441–6

22
Non-AIDS–Related Death
CASCADE: En düşük düzeydeki CD4+ hücre sayısı - AIDS ve AIDS-dışı olayları belirler CASCADE Collaboration cohort: N = 9858 En son ve en düşük CD4+ hücre sayısı < 350 hücre/mm3 altında geçirilen zaman AIDS-Related Death Non-AIDS–Related Death Nadir CD4+ cell count vs ≥ 350 vs ≥ 350 vs ≥ 350 vs ≥ 350 < 50 vs ≥ 350 < 50 vs ≥ 350 0.01 1.00 100.00 0.01 1.00 100.00 Liver Disease Death Non-AIDS Cancer Death vs ≥ 350 vs ≥ 350 vs ≥ 350 vs ≥ 350 < 50 vs ≥ 350 < 50 vs ≥ 350 0.01 1.00 100.00 0.01 1.00 100.00 Marin B, et al. IAS Abstract WEPEB019.

23
Percentage With HIV-1 RNA < 50 copies/mL at Week 48
HAART etkinliği: > 65% cevap alınan çalışmalar (VL < haftada) COMBINE (NVP + ZDV/3TC) 2NN (NVP BID + d4T + 3TC) ZODIAC (EFV + ABC QD + 3TC) M (LPV/RTV + d4T + 3TC) ZODIAC (EFV + ABC + 3TC) CNA30024 (EFV + ZDV + 3TC) 2NN (NVP QD + d4T + 3TC) 2NN (EFV + d4T + 3TC) CNA30024 (EFV + ABC + 3TC) M (LPV/RTV + FTC + TDF QD) FTC301 (EFV + FTC + ddI QD) DMP (EFV + D4T + 3TC) CLASS (EFV + ABC + 3TC) ANRS (EFV + ddI + 3TC) M (LPV/RTV + d4T + 3TC) Dart 1 (EFV + ddI EC + 3TC) GS903 (EFV + d4T + 3TC) GS903 (EFV + TDF + 3TC) ANRS 091 (EFV + ddI + FTC) NNRTI Boosted PI Efficacy is a primary factor in choosing between NNRTI-based and PI-based regimens. To investigate this issue, Bartlett and colleagues performed a systematic overview of clinical trials that evaluated 3-drug antiretroviral therapy in treatment-naive HIV-infected adults. They included 49 clinical trials involving more than 13,147 patients. The primary endpoint of the analysis was virologic responses, defined as the proportion of patients with HIV RNA < 50 copies/mL at Week 48, based on an intent-to-treat analysis. They also evaluated immunologic responses, defined as mean increases in CD4+ cell count at Week 48, using an on-treatment analysis. Among those regimens with > 65% efficacy, 2 agents stand out: efavirenz and lopinavir/ritonavir. 30 40 50 60 70 80 90 100 Percentage With HIV-1 RNA < 50 copies/mL at Week 48 Bartlett JA, et al. AIDS. 2006;20:
 COMBINE (NVP + ZDV/3TC) 2NN (NVP BID + d4T + 3TC) ZODIAC (EFV + ABC QD + 3TC) M (LPV/RTV + d4T + 3TC) ZODIAC (EFV + ABC + 3TC) CNA30024 (EFV + ZDV + 3TC) 2NN (NVP QD + d4T + 3TC) 2NN (EFV + d4T + 3TC) CNA30024 (EFV + ABC + 3TC) M (LPV/RTV + FTC + TDF QD) FTC301 (EFV + FTC + ddI QD) DMP (EFV + D4T + 3TC) CLASS (EFV + ABC + 3TC) ANRS (EFV + ddI + 3TC) M (LPV/RTV + d4T + 3TC) Dart 1 (EFV + ddI EC + 3TC) GS903 (EFV + d4T + 3TC) GS903 (EFV + TDF + 3TC) ANRS 091 (EFV + ddI + FTC) NNRTI. Boosted PI. Efficacy is a primary factor in choosing between NNRTI-based and PI-based regimens. To investigate this issue, Bartlett and colleagues performed a systematic overview of clinical trials that evaluated 3-drug antiretroviral therapy in treatment-naive HIV-infected adults. They included 49 clinical trials involving more than 13,147 patients. The primary endpoint of the analysis was virologic responses, defined as the proportion of patients with HIV RNA < 50 copies/mL at Week 48, based on an intent-to-treat analysis. They also evaluated immunologic responses, defined as mean increases in CD4+ cell count at Week 48, using an on-treatment analysis. Among those regimens with > 65% efficacy, 2 agents stand out: efavirenz and lopinavir/ritonavir Percentage With HIV-1 RNA < 50 copies/mL at Week 48. Bartlett JA, et al. AIDS. 2006;20:")
24
ARV-ilaç almamış hastalarda önerilen başlangıç rejimleri – 2008 DHHS, 2007 EACS

25
Akut veya yakın (< 6 ay) HIV infeksiyonunun tedavisi
Tedavi opsiyonel (uzun süreli virolojik, immunolojik ve klinik fayda bilinmiyor) Teorik olarak akut hastalığın şiddetini azaltır, tam tahrip olmadan immun sistemi korur, viral mutasyonu azaltır, başlangıç viral platoyu değiştirir, GI lenfoid doku kaybını önler, bulaş riskini azaltır. Başlangıç direnç testi yapılmalı, yapılamıyor veya gecikecekse PI-temelli rejim
 Teorik olarak. akut hastalığın şiddetini azaltır, tam tahrip olmadan immun sistemi korur, viral mutasyonu azaltır, başlangıç viral platoyu değiştirir, GI lenfoid doku kaybını önler, bulaş riskini azaltır. Başlangıç direnç testi yapılmalı, yapılamıyor veya gecikecekse PI-temelli rejim.")
26
EACS – temas sonrası profilaksi
TDF/FTC (Truvada) (alternatif: ZDV/3TC - Combivir) + LPV/r günde 2 kez 4 hf
 (alternatif: ZDV/3TC - Combivir) + LPV/r günde 2 kez. 4 hf.")
Benzer bir sunumlar