Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

2
2 Measures listed as Class I recommendations for patients in Stages A and B are also appropriate for patients in Stage C. Diuretics and salt restriction are indicated in patients with current or prior symptoms of HF and reduced LVEF who have evidence of fluid retention. Measuring LVEF

3
3 Angiotensin-converting enzyme (ACE) inhibitors are recommended for all patients with current or prior symptoms of HF and reduced LVEF, unless contraindicated. Use of 1 of the 3 beta blockers proven to reduce mortality (i.e., bisoprolol, carvedilol, and sustained release metoprolol succinate) is recommended for all stable patients with current or prior symptoms of HF and reduced LVEF, unless contraindicated.
 is recommended for all stable patients with current or prior symptoms of HF and reduced LVEF, unless contraindicated..")
4
4 Angiotensin II receptor blockers are recommended in-patient with current or prior symptoms of HF and reduced LVEF who are ACE- inhibitor intolerant (see full text guidelines). Drugs known to adversely affect the clinical status of patients with current or prior symptoms of HF and reduced LVEF should be avoided or withdrawn whenever possible (e.g., nonsteroidal anti-inflammatory drugs, most antiarrhythmic drugs, and most calcium channel blocking drugs). Angiotensin ll Receptor Blockers
. Angiotensin ll Receptor Blockers.")
5
5 A cardioverter-defibrillator (ICD) is recommended as secondary prevention to prolong survival in patients with current or prior symptoms of HF and reduced LVEF who have a history of cardiac arrest, ventricular fibrillation, or hemodynamically destabilizing ventricular tachycardia. Secondary Prevention: Implantable Cardioverter-Defibrillator

6
6 ICD therapy is recommended for primary prevention of sudden cardiac death to reduce total mortality in patients with nonischemic dilated cardiomyopathy or ischemic heart disease at least 40 days post-myocardial infraction, have an LVEF less than or equal to 35%, with NYHA functional class II or III symptoms while receiving chronic optimal medical therapy, and who have reasonable expectation of survival with a good functional status for more than 1 year. Primary Prevention: Implantable Cardioverter-Defibrillator

7
7 Patients with LVEF less than or equal to 35%, sinus rhythm, and NYHA functional class III or ambulatory class IV symptoms despite recommended, optimal medical therapy and who have cardiac dyssynchrony, which is currently defined as a QRS duration greater than or equal to 0.12 seconds, should receive cardiac resynchronization therapy, with or without an ICD, unless contraindicated. Resynchronization Therapy

8
8 Addition of an aldosterone antagonist is recommended in selected patients with moderately severe to severe symptoms of HF and reduced LVEF who can be carefully monitored for preserved renal function and normal potassium concentration. Creatinine 2.5 mg/dL or less in men or 2.0 mg/dL or less in women and potassium should be less than 5.0 mEq/L. Under circumstances where monitoring for hyperkalemia or renal dysfunction is not anticipated to be feasible, the risks may outweigh the benefits of aldosterone antagonists. Aldosterone Antagonists

9
9 The combination of hydralazine and nitrates is recommended to improve outcomes for patients self- described as African-Americans, with moderate- severe symptoms on optimal therapy with ACE inhibitors, beta blockers, and diuretics. Recommendations for Hydralazine and Nitrates The addition of a combination of hydralazine and a nitrate is reasonable for patients with reduced LVEF who are already taking an ACE inhibitor and beta blocker for symptomatic HF and who have persistent symptoms.

10
10 Digitalis can be beneficial in patients with current or prior symptoms of HF and reduced LVEF to decrease hospitalizations for HF. The Benefits of Digitalis

11
11 Hydralazine and Nitrate Combination A combination of hydralazine and a nitrate might be reasonable in patients with current or prior symptoms of HF and reduced LVEF who cannot be given an ACE inhibitor or ARB because of drug intolerance, hypotension, or renal insufficiency.

12
12 The addition of an ARB may be considered in persistently symptomatic patients with reduced LVEF who are already being treated with conventional therapy. Routine combined use of an ACE inhibitor, ARB, and aldosterone antagonist is not recommended for patients with current or prior symptoms of HF and reduced LVEF. ARB and Conventional Therapy Calcium channel blocking drugs are not indicated as routine treatment for HF in patients with current or prior symptoms of HF and reduced LVEF. Calcium Channel Blocking Drugs

13
13 Long-term use of an infusion of a positive inotropic drug may be harmful and is not recommended for patients with current or prior symptoms of HF and reduced LVEF, except as palliation for patients with end-stage disease who cannot be stabilized with standard medical treatment. Infusion of Positive Inotropic Drugs

14
14 Hormonal therapies other than to replete deficiencies are not recommended and may be harmful to patients with current or prior symptoms of HF and reduced LVEF. Hormonal Therapies Nutritional Supplements Use of nutritional supplements as treatment for HF is not indicated in patients with current or prior symptoms of HF and reduced LVEF.

15
15 Titiz tanımlama ve sıvı retansiyonun kontrolu Potansiyel olarak uygun hastalarda kardiyak transplantasyon için sevk. Kalp yetmezliği ile özel olarak ilgilenen bir merkeze veya bir kalp yetmezliği programı olan uzmana sevk Şiddetli Semptomları olan Dirençli Son Dönem KY olan Hastalarda

16
16 ICD’li hastalar için defibrilatörün inaktivasyonu seçeneği hakkında bilgi verilmesi gerekir. End-of-life care seçeneklerinin hasta ve ailesi ile tartışılması gerekir. Şiddetli Semptomları olan Dirençli Son Dönem KY olan Hastalarda Medikal tedavi ile tahmin edilen 1 yıllık mortalite oranı % 50 nin üzerinde olan seçilmiş hastalarda kalıcı tedavi olarak left ventricular assist device” mantıklı bir yaklaşımdır.

17
17 Pulmoner arter kateteri yerleştirilmesi Pulmonar Arter Kateteri Yerleştirilmesi Bu tip hastalarda etkinliği bilinmiyor. Mitral Kapak Tamiri veya Yerleştirilmesi

18
18 Pozitif İnotropik Ajanların Sürekli IV Infuzyonu Semptomların giderilmesi için düşünülebilinir. Pozitif İnotropik Ajanların Sürekli IV Infuzyonu Noniskemik KMP li hastalarda kısmi sol ventriküloktemi tavsiye edilmemektedir. Rutin aralıklı vazoaktif ve pozitif inotropik ajanların verilmesi tavsiye edilmemektedir.

19
19 Ultrafiltrasyon uygulanabilir Ultrafiltrasyon Periton dializi ile ilgili umut verici sonuçlar var

20
20 Hastanın fonksiyonel kapasitesi ve yaşam süresi ile ilgili kendisinin ve yakının eğitimine devam edilmesi Hasta ve yakının end of life care seçenekleri açısından eğitimi Choosing where to die Home care Inpatient care Spirituality at the end of life Saying goodbye Recognizing when death is near Providing comfort Keeping vigil

21
21 Bu hastaların ayaktan ve yatarak tedavi arasındaki tıbbi bakımın devamlılığını sağlamak önemlidir. Hastayı rahatlatmak için opiatlarıda içeren uygun yaşlı bakım yerleri tavsiye edilir ancak bu hastaların medikal tedavi seçeneklerinin önüne geçmemelidir. Kalp yetmezlikli hastalarla çalışan tüm profesyoneller güncel end of life yöntemlerini incelemeleri ve bu yöntemlerin dahada iyileştirilmesi için çalışmaları gerekir

22
22 Yaşamının son günlerinde yapılacak agresif yöntemler uygun değildir. Entübasyon ICD

23
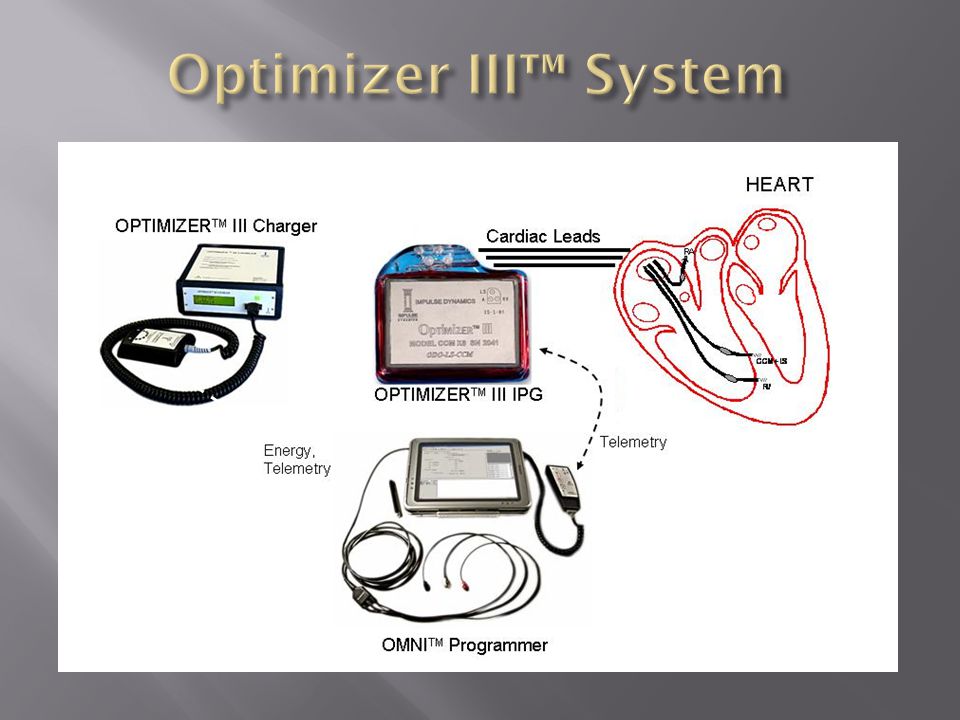
Kalbin kontraktil siklusunun refraktor periyodu boyunca elektrik impulslarının uygulanması Pacemakır sistemi gibi leadler kullanılıyor. Pozitif inotropi sağlıyor. CRT uygulanamıyan hastalarla sınırlı Mortalite üzerinde anlamlı etkisi yok Yaşam kalitesi üzerine olumlu etkisi var European Journal of HF 2011

24
Detect local activation Apply electric signal during absolute refractory period Delay Duration Amplitude

25
Timing and characteristics of CCM signal. Mohri S et al. Am J Physiol Heart Circ Physiol 2002;282:H1642-H1647 ©2002 by American Physiological Society

27
Güvenlik ve tolerabilite çalışması var Bu konuda randomize çalışmalara ihtiyaç olmakla beraber Cihaz güvenilir ve hastalar tarafından tolere edilebilir Yaşam kalitesi üzerine olumlu etkileri var NYHA class da düzelmeler sağladı 6 min WT de yürüme mesafesinde artma LV sistolik volüm ve fonksiyonunda iyileşme

Benzer bir sunumlar












 TURKISH COMMERCIAL.>")







