Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
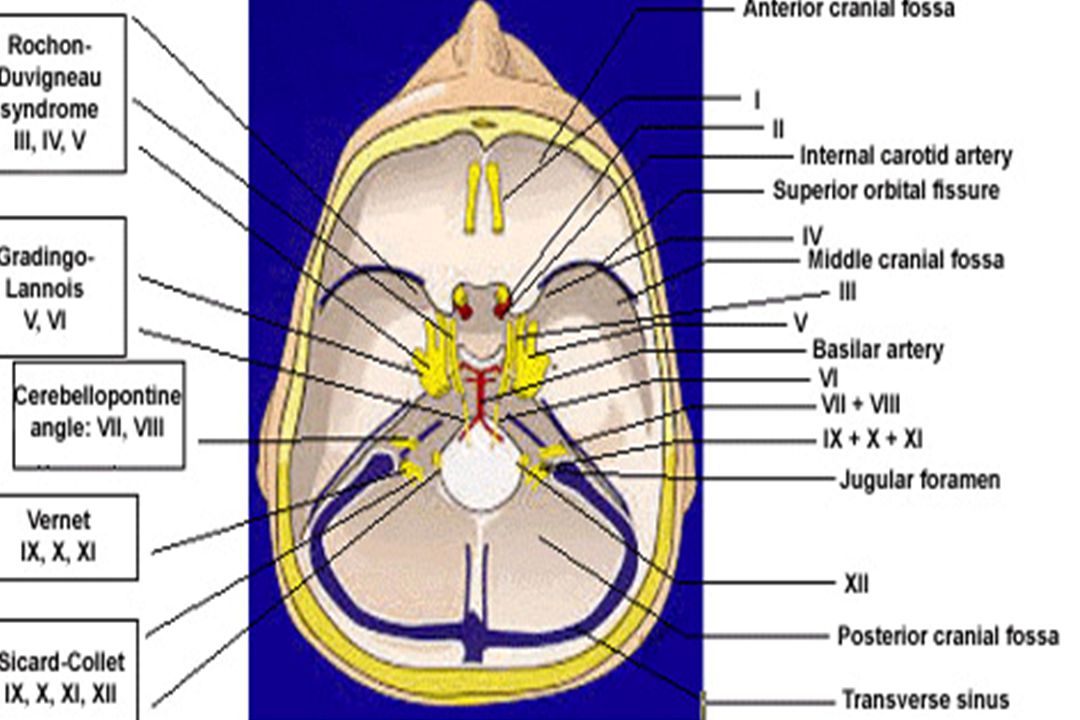
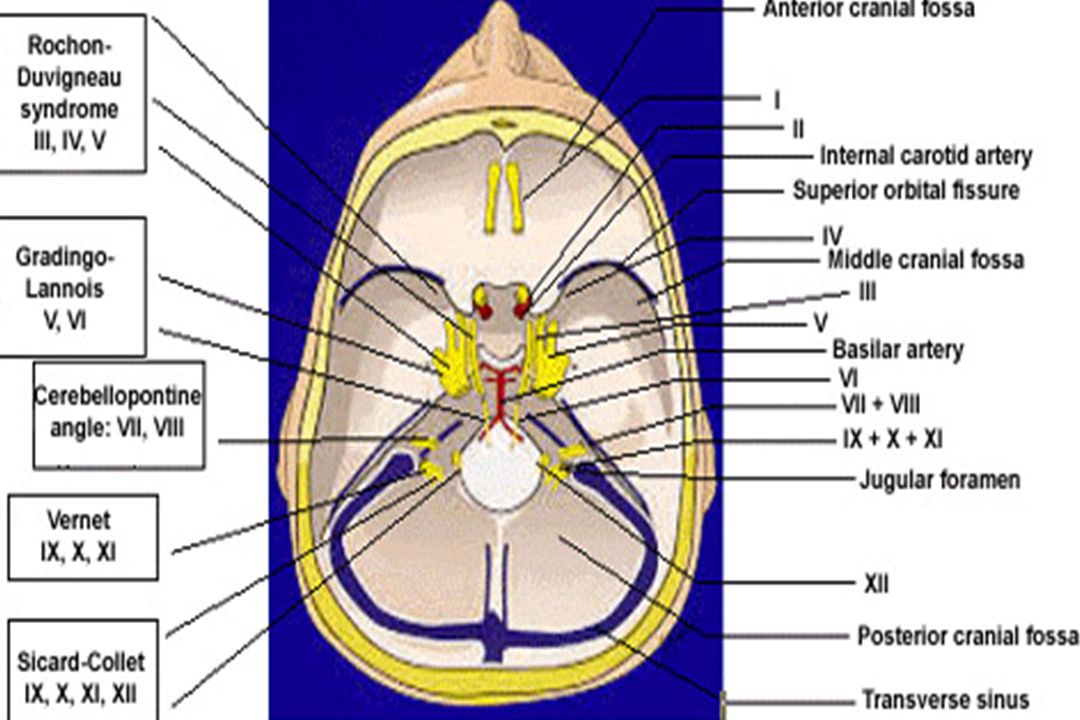
I II III V VI VII&VIII IX &X XII XI

3
Cranial Nerve I: Olfactory
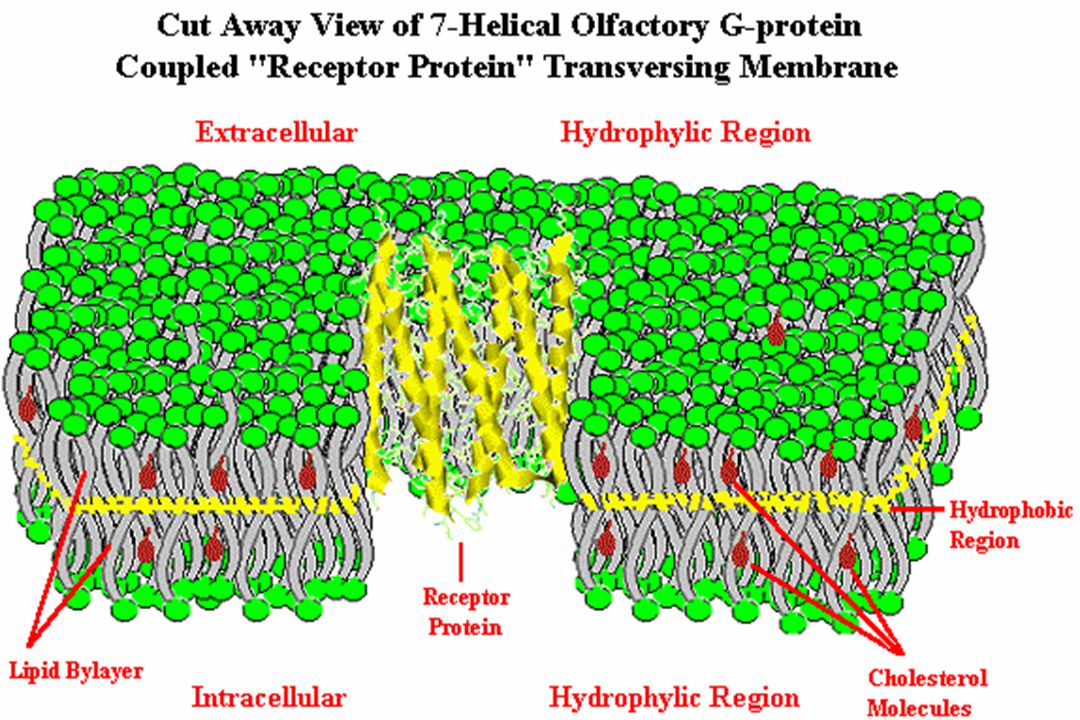
Bulbus olfactorius Cranial Nerve I: Olfactory Bipolar cells Foramen: cribiform plate of ethmoid Region Entered: nasal cavity Components: special sensory Target: olfactory epithelium Function: smell 50 million primary sensory receptor cells in 2.5 cm2

4
Second neurons: First neurons: Unmyelinated
Each olfactory receptor neuron cilia projects down out of the olfactory epithelium into the mucous. 8-20 cilia of in length 60 thick layer of mucous (lipid- rich secretion that bathes the surface of the receptors at the epithelium surface) The mucous lipids assist in transporting the odorant molecules as only volatile materials soluble in the mucous, can interact with the olfactory receptors & produce the signals that our brain interprets as odor
 The mucous lipids assist in transporting the odorant molecules as only volatile materials soluble in the mucous, can interact with the olfactory receptors & produce the signals that our brain interprets as odor.")
6
Lateral stria Medial stria anterior olfactory nucleus pyriform cortex
Summary of main projection pathways in the olfactory system. AON, anterior olfactory nucleus; PC, pyriform cortex; OT, olfactory tubercle; AMYG, amygdala; TEC, transitional entorhinal cortex; NHLDB, nucleus of horizontal limb of diagonal band; MD, mediodorsal. pyriform cortex nucleus of horizontal limb of diagonal band olfactory tubercle Medial stria transitional entorhinal cortex

7
Olfactory Tract Connections& Lesion
Lateral stria primary olfactory cortex (periamygdaloid & prepiriform areas) secondary olfactory cortex (entorhinal area (area 28)) Medial stria cross the anterior commisure to join contralateral olfactory bulb Unilateral anosmia : Compression due to abcess, glioma, meningioma of frontal lob or hypothalamus which may result in ipsilateral optic atropy & contralateral papilledema Foster-Kennedy syndrome
 secondary olfactory cortex (entorhinal area (area 28)) Medial stria cross the anterior commisure to join contralateral olfactory bulb. Unilateral anosmia : Compression due to abcess, glioma, meningioma of frontal lob or hypothalamus which may result in ipsilateral optic atropy & contralateral papilledema Foster-Kennedy syndrome.")
8
Cranial Nerve II: Opticus
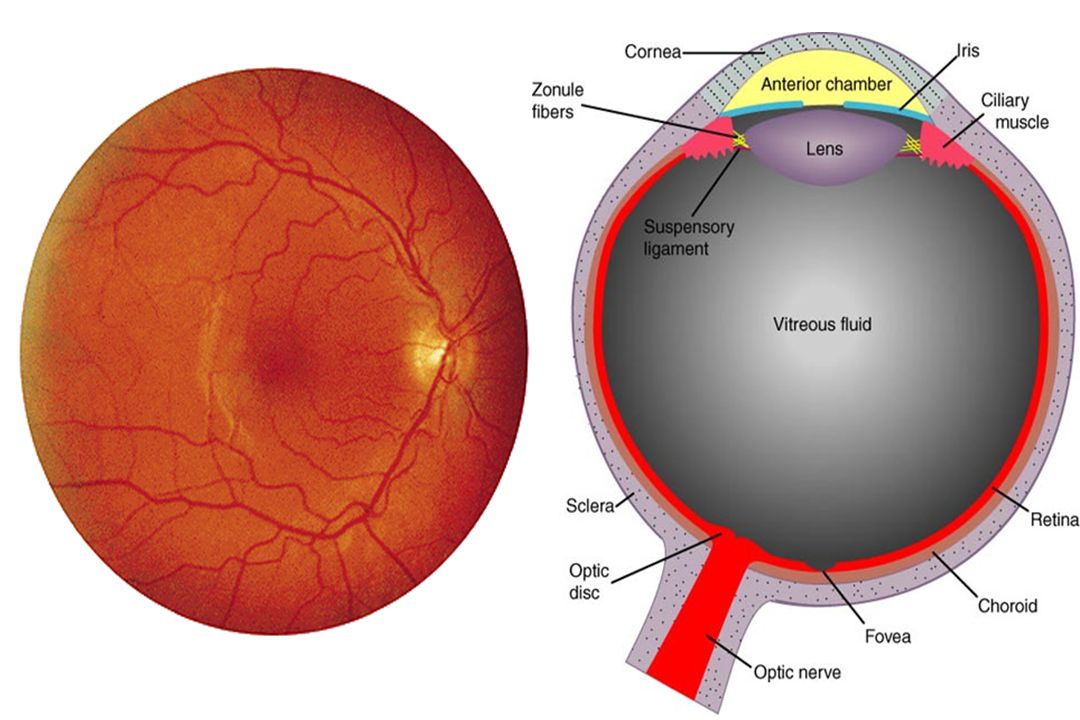
Foramen: optic canal of sphenoid Region Entered: orbit Components: special sensory Target, Function: retina-vision

10
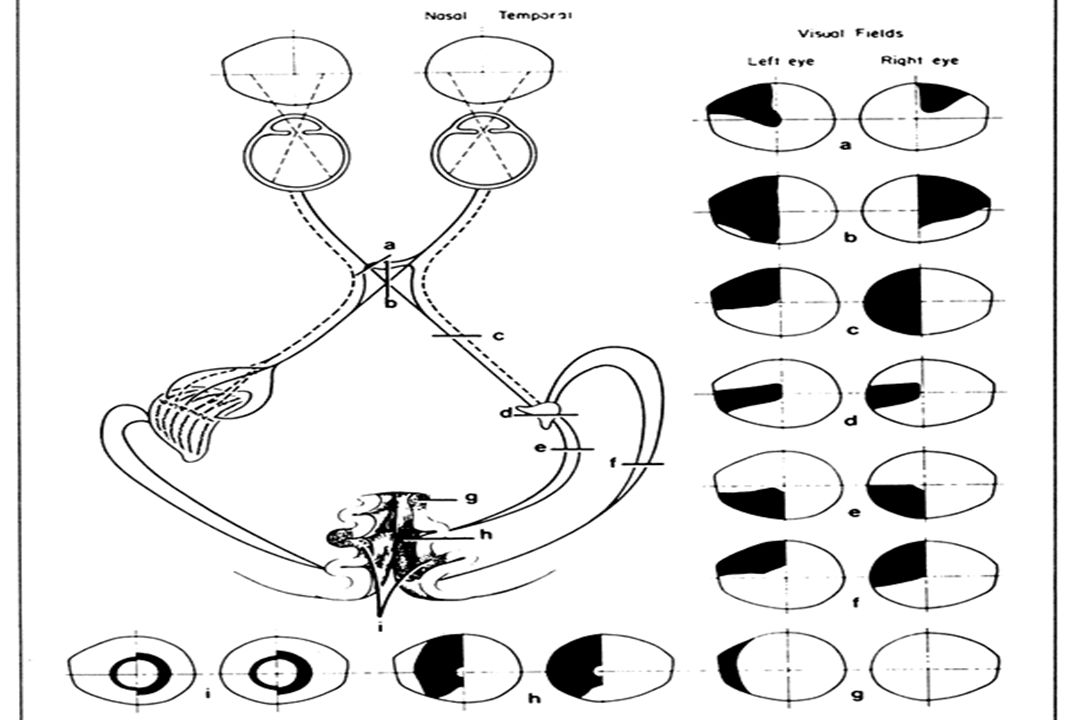
Visual Path 1st neurone: rod & cone cells of the retina
2nd neurone: bipolar neurones of the retina 3rd neurone: multipolar neurones of the retina Axons of the ganglion opticum run via the N. opticus to the chiasma

11
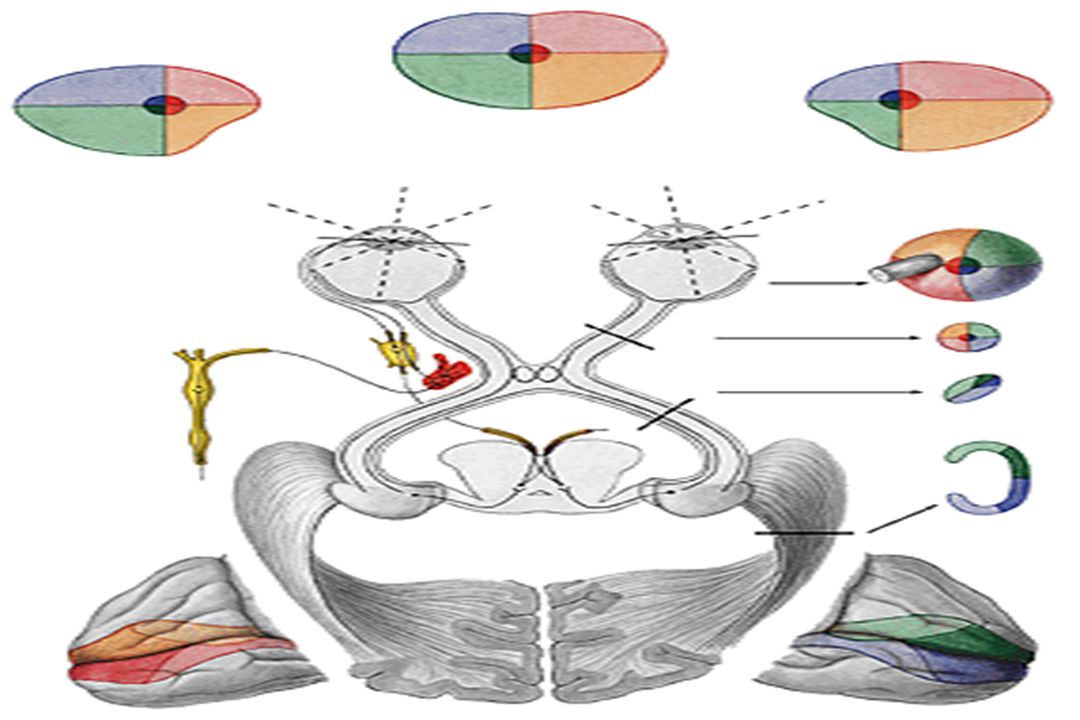
Visual Path In the chiasma opticum, fibres of the nasal part of the retina cross to the contralateral side, and those of the temporal part continue ipsilaterally Each tractus opticus consists of fibres transporting the information from the contralateral halves of the visual field corpus geniculatum laterale&mediale (some fibres), hypothalamus go directly to the cortex of the brain 4th neurone: corpus geniculatum laterale areas 17&18 around the sulcus calcarinus (area striata)
, hypothalamus go directly to the cortex of the brain. 4th neurone: corpus geniculatum laterale areas 17&18 around the sulcus calcarinus (area striata)")
14
Acute right homonymous hemianopsia in a 59-year-old man due to embolus in the left PCA. (A) MRI (TR/TE 2000/80) shows infarction in the medial left occipital lobe (arrow). (B) Occlusion of the left PCA at its origin (arrow) by an embolus (DSA, left vertebral artery, AP view). (C) The capillary phase (arrow) is absent in the left occipital lobe due to the proximal embolus. Acute right homonymous hemianopsia in a 59-year-old man due to embolus in the left PCA. (A) MRI shows infarction in the medial left occipital lobe (arrow). (B) Occlusion of the left PCA at its origin (arrow) by an embolus (DSA, left vertebral artery, AP view). (C) The capillary phase (arrow) is absent in the left occipital lobe due to the proximal embolus.
 MRI shows infarction in the medial left occipital lobe (arrow). (B) Occlusion of the left PCA at its origin (arrow) by an embolus (DSA, left vertebral artery, AP view). (C) The capillary phase (arrow) is absent in the left occipital lobe due to the proximal embolus.")
15
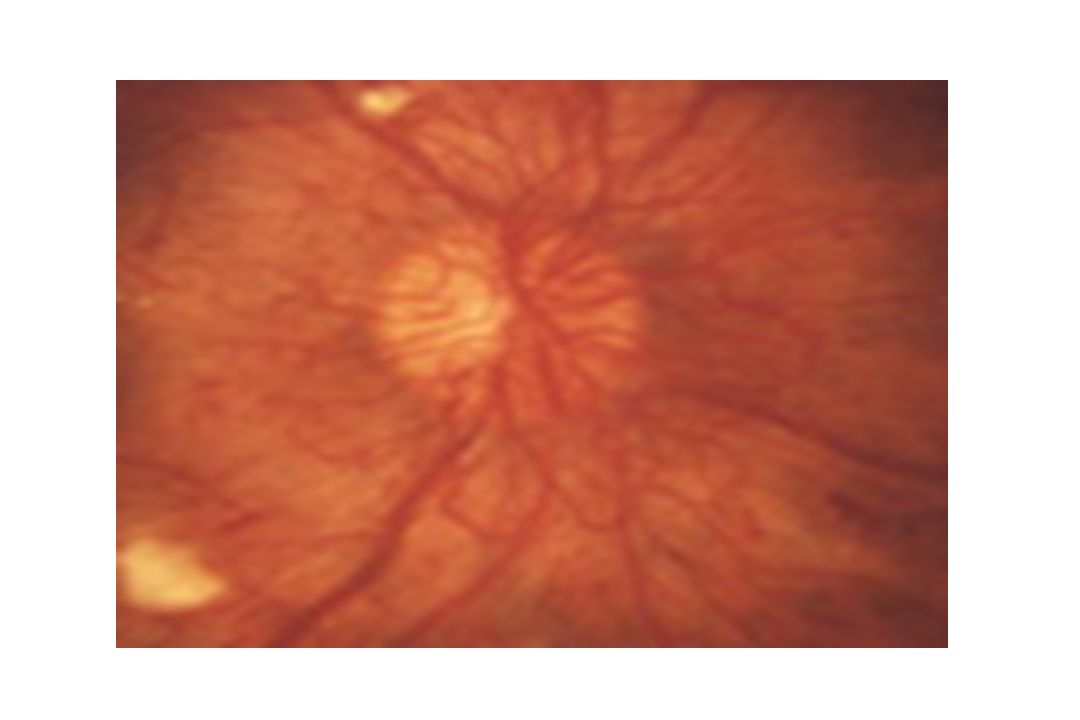
Causes of Papillitis&Retrobulbar Neuritis
Multiple sclerosis Viral illness; Syphilis Temporal arteritis & other kinds of inflammation of the arteries (vasculitis) Poisoning by chemicals: lead, methanol... Tumors that have spread to the optic n. Allergic reactions to beestings Meningitis Uveitis Arteriosclerosis
 Poisoning by chemicals: lead, methanol... Tumors that have spread to the optic n. Allergic reactions to beestings. Meningitis. Uveitis. Arteriosclerosis.")
17
preganglionic parasympathetic
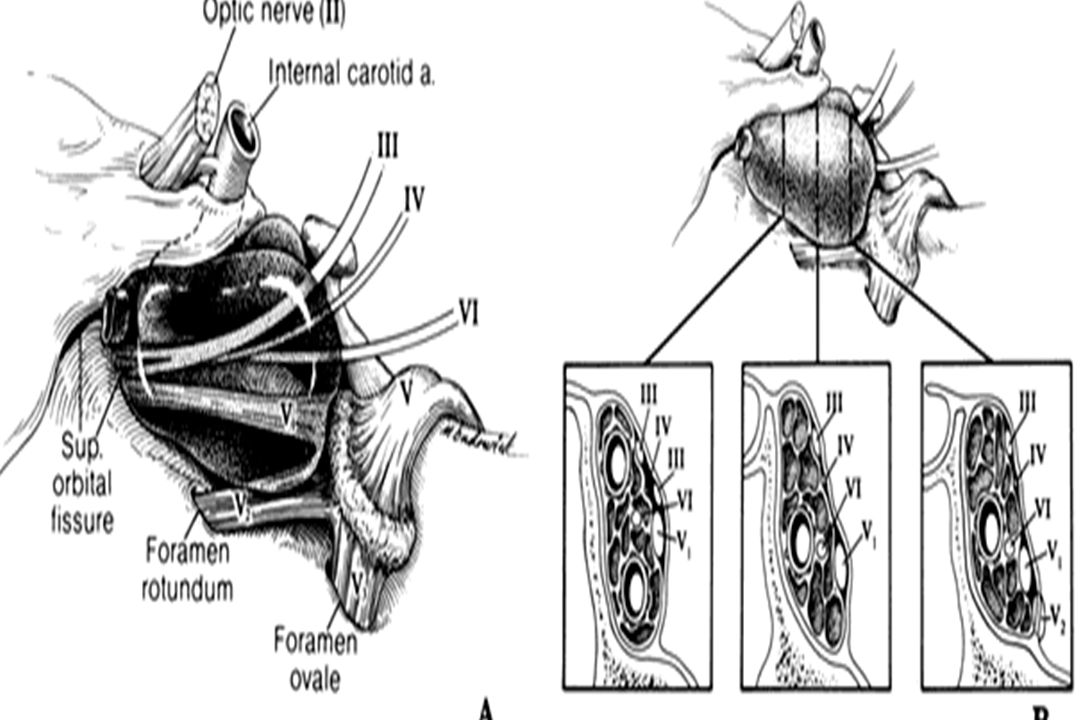
Superior Orbital Fissure Syndrome IV VI III preganglionic parasympathetic to: ciliary ganglion (innervation of sphincter pupillae and ciliary muscle)
")
18
Cranial Nerve III: Oculomotor Foramen: Superior orbital fissure
Region Entered: Orbit Somatomotor Comp.: Target, Function: levator palpebrae sup. superior rectus medial rectus inferior rectus inferior oblique Visceromotor Comp.: preganglionic parasympathetic to: ciliary ganglion Cranial Nerve III: Oculomotor R eye

21
THIRD CRANIAL NERVE PALSIES
During primary gaze, weakness of the muscles innervated by, result in: Ptosis of the lid Mydriasis Outwardly turned eye Pupil is completely spared: Myopathy but all other muscles innervated by the 3rd nerve are affected: diabetic 3rd nerve paresis (ischemic process)
")
23
Neurologic examination with CT or MRI
Fixed dilated pupils: 3rd nerve compression - Aneurysm of the post. communicating art - Trauma - Intracranial mass lesion - Increasingly unresponsive patient with 3rd n. palsy: transtentorial herniation Neurologic examination with CT or MRI When CT does not show blood: Lumbar puncture (suspected SAH) Cerebral angiography: if aneurysm is suspected
 Cerebral angiography: if aneurysm is suspected.")
24
+ Nuc. Ruber infarction in midbrain
Benedict syndrome: contralat. tremor + İpsilat. 3rd n. palsy & fixed pupilla Pupillary Reflex: Afferent: NII Edinger-Westpal nuc. Efferent: NIII parasympath. Argyll Robertson pupil Accomodation Retained Light reflex absent

25
Benedict syndrome:

26
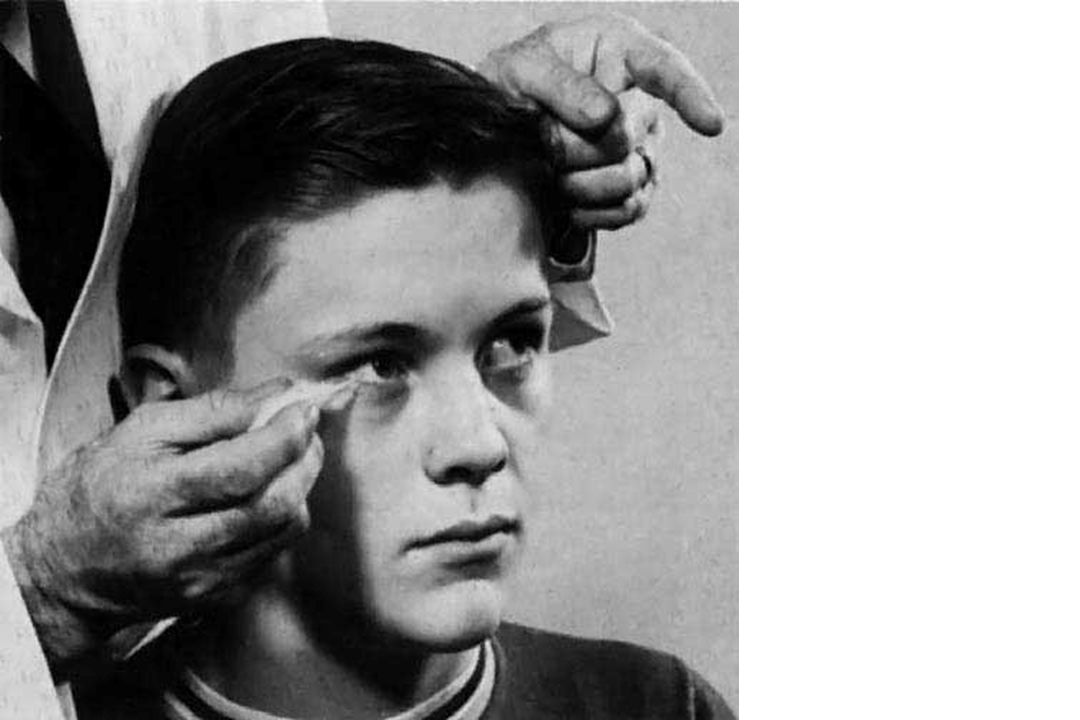
Horner Syndrome Ptosis Myosis Enophthalmus Loss of sweating on the affected side of the face From hypothalamus, sympathetic nn. descend ipsilat. through the brainstem & cervical cord & riches the sympathetic chain via the motor root of T1. From there, fibers pass along the outer sheath of the internal carotid artery&its opht.branch &to the pupilla. Fibers to the face travel with the ext. carotid artery Pancoast tm, mass compress. cervical symp. chain

27
Cranial Nerve IV: Trochlear
Superior Orbital Fissure Syndrome IV VI III Cranial Nerve IV: Trochlear Foramen: Superior orbital fissure Region Entered: Orbit Components: somatomotor Target, Function: Superior oblique muscle

28
Cranial Nerve IV: Trochlear
Superior oblique muscle palsies Affect vertical eye position when the eye is turned inward The patient sees double images: one above & slightly to the side of the other By tilting the head to the side opposite the palsied m., the pt may achieve full ocular motility without double vision Causes: idiopathic, closed head trauma, aneurysms, tm, MS

29
Cranial Nerve VI: Abducens
Foramen: Superior orbital fissure Region Entered: Orbit Components: Somatomotor Target, Function: to lateral rectus (best abductor!)
")
30
6th Nerve Palsy Idiopathic: improvement within 2 mo Elderly or diabetic pts: small vessel disease Compression in cavernous sinus: severe headache & anesthesia in the area of n.V1 Increased intracranial pressure: shift in the brain stretch the 6th n. Trauma (basilar skull fracture) Infections & tumors affecting the meninges Aneurysm, MS Wernicke's encephalopathy
 Infections & tumors affecting the meninges. Aneurysm, MS. Wernicke s encephalopathy.")
32
Saccadic Eye Movements
Retina Optik nerve Corpus geniculatum lat. Area 17. & FEF Mesencephalon Pons (VI. contral. III. & n. nuclei) ıv ııı P R F Lat. rectus Medial rectus VIIIN Pons Mesensephalon MLF vı Nuc. Abducens Frontal eye field (FEF & SEF) VI
 ıv. ııı. P. R. F. Lat. rectus. Medial rectus. VIIIN. Pons. Mesensephalon. MLF. vı. Nuc. Abducens. Frontal eye field. (FEF & SEF) VI.")
33
Saccadic Eye Movements
Frontal eye field (FEF & SEF) Medial rektus Lateral rektus MLF Mesencephalon VI ııı ıv P R F Nuc.VI Pons vı VIII MLF MLF
 Medial rektus. Lateral rektus. MLF. Mesencephalon. VI. ııı. ıv. P. R. F. Nuc.VI. Pons. vı. VIII. MLF. MLF.")
34
Saccadic Eye Movements
Frontal eye field (FEF & SEF) Medial rektus Lateral rektus MLF Mesencephalon VI ııı ıv Nuc. Abducens Pons P R F vı VIII MLF MLF
 Medial rektus. Lateral rektus. MLF. Mesencephalon. VI. ııı. ıv. Nuc. Abducens. Pons. P. R. F. vı. VIII. MLF. MLF.")
37
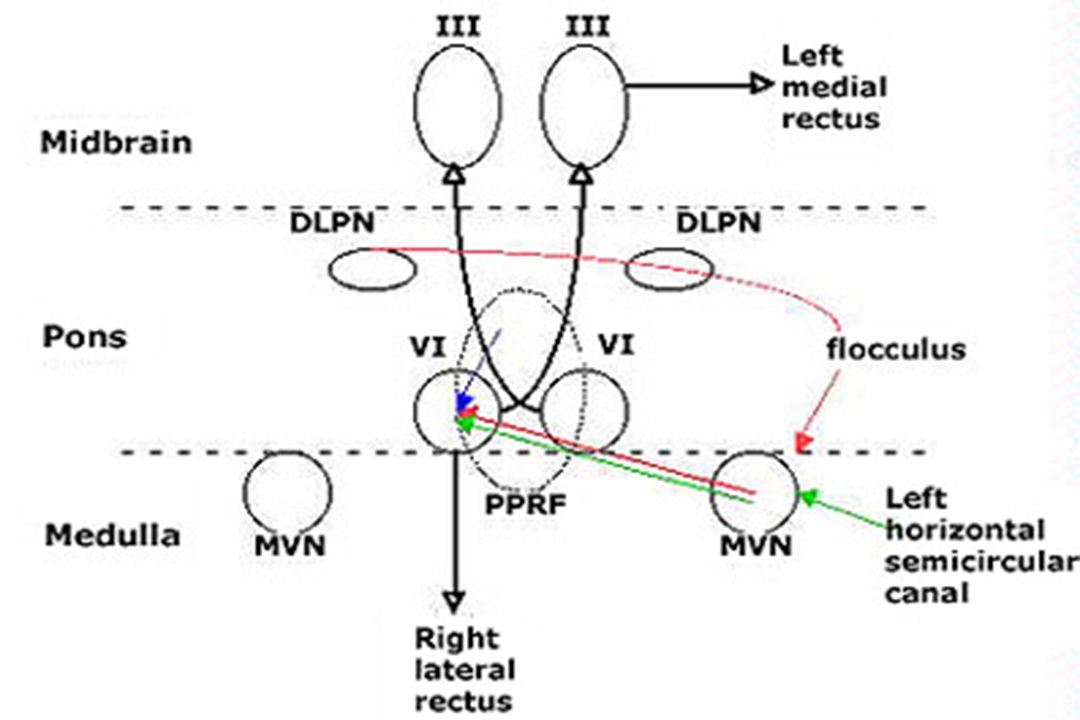
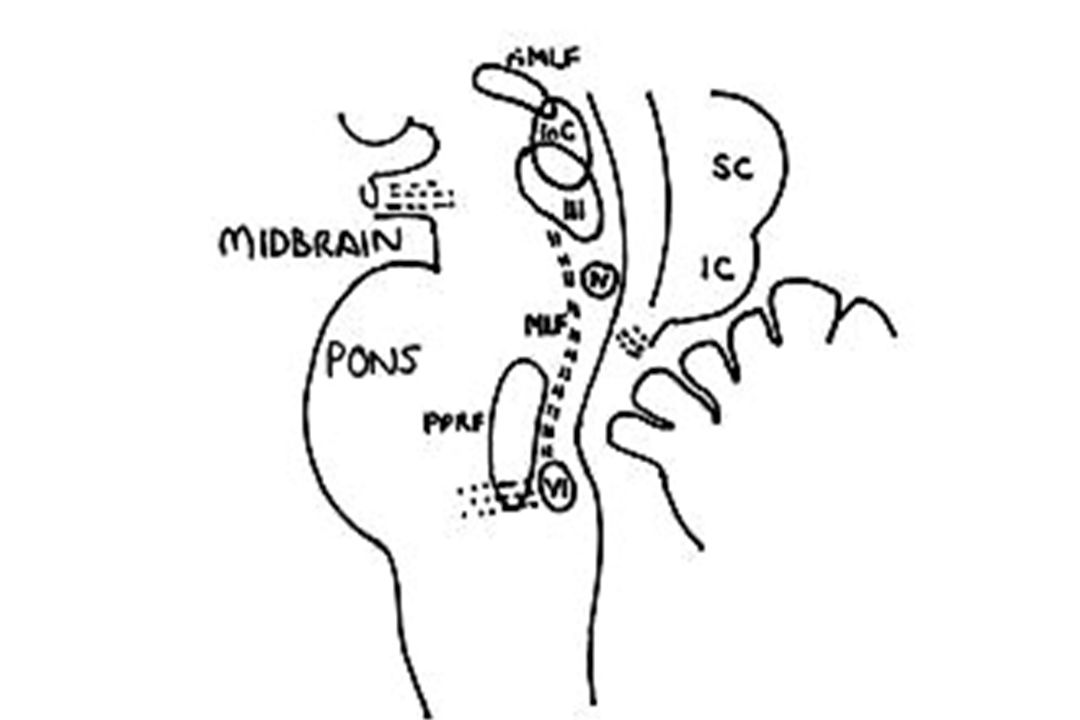
Vertical Gaze Vestibulo-ocular Reflexe paths
Rapid turn of the head to the left Bilateral control Center: Dorsal rostral mesencephalon 3 integral structures: - riMLF - Cajal’s interstitial nuc. - Posterior commisure Inputs from PPRF & vestibular nuclei Each riMLF projects ipsilaterally to III & IV n. nuclei Ant. motion of the fluid in the labyrinth Cupula is stimulated Ipsilat. IIIrd & contralat. VIth nerves are stimulated Eyes turn right in order to sustain forward gaze

38
Cranial Nerve V: Trigeminal V1-Trigeminal ophthalmic Major branches: Lacrimal, Frontal, Nasociliary & Meningeal Foramen: superior orbital fissure Region Entered: orbit Components: general sensory Target, Function: general sensation from skin and mucosa in region at & above orbit

39
Dilin 2/3 ön kısmı: Ağrı-ısı-dokunma Meninksler: Ağrı Motor
V. NERVUS TRİGEMİNUS Duysal Yüz Oral-nazal kavite Dilin 2/3 ön kısmı: Ağrı-ısı-dokunma Meninksler: Ağrı Motor Çiğneme kasları, tensor veli palatini Refleks Kornea-Göz kırpma, çene SUPRANÜKLEER LEZYONLAR: Vasküler, demiyelinizan, tümör Bilateral-yaygın premotor nöron lezyonları Çiğneme kasları paralizisi Çene refleksi Bilateral premotor nöron bulguları Affekt kontrol bozukluğu, demans Talamik lezyonlar Karşı yüz yarımında his kusuru Parietal lezyonlar Karşı taraf kornea refleksi kaybı hemifasiyal his kusuru

40
Cornea Reflex Afferent: N V1 Efferent: N VII (blink) Ciliary ganglion
 Ciliary ganglion")
44
V2-Trigeminal maxillary Infraorbital, Zygomatic,Nasopalatine, Palatine
Foramen:rotundum Region Entered: pterygopalatine fossa Components: general sensory Target, Function: gen.sensation from skin & mucosa in region from orbit to mouth

45
V3-Trigeminal mandibular Buccal, Auriculotemporal, Lingual, Inf
V3-Trigeminal mandibular Buccal, Auriculotemporal, Lingual, Inf. alveolar & Meningeal Foramen: ovale with lesser petrosal from CN9 Region Entered: infratemporal fossa Components: brachiomotor Target, Function: muscles of masticat. tensor tympani & veli palatini, mylohyoid ant. belly digastric

46
Lesion of spinal tract V
IPSILATERAL deficits in pain & temperature from the face etc. (the pain information never gets to the caudal spinal nucleus) Interruption of the trigeminothalamic tract deficits in pain & temperature on the contralateral side of the face (comprised of axons that have crossed the midline)
 Interruption of the trigeminothalamic tract. deficits in pain & temperature on the. contralateral side of the face. (comprised of axons that have crossed. the midline)")
47
Causes of Sensory Trigeminal Neuropathy
Idiopathic Systemic inflammatory disease Sjögren's syndrome Progressive systemic sclerosis (scleroderma) Mixed connective tissue disease Systemic lupus erythematosus Dermatomyositis Rheumatoid arthritis Sarcoidosis Wegener's granulomatosis Undifferentiated connective tissue disease Giant cell arteritis Idiopathic hypertrophic cranial pachymeningitis Multiple sclerosis Tumor Intracranial or extracranial Metastatic Primary: Meningioma, Schwannoma, Epidermoid, Chordoma Trauma Aneurysm Dural external carotid artery cavernous sinus fistula Sickle ceil disease Diabetes mellitus Syringobulbia Infections Sinusitis Herpes simplex Herpes zoster Hepatitis A infection Nonspecific viral infection Tuberculosis Whipple's disease Leprosy Arachnoiditis Tricloroethylene Hydroxystilbamidine Amyloidosis Spinal epidural anesthesia
 Mixed connective tissue disease. Systemic lupus erythematosus. Dermatomyositis. Rheumatoid arthritis. Sarcoidosis. Wegener s granulomatosis. Undifferentiated connective tissue disease. Giant cell arteritis. Idiopathic hypertrophic cranial pachymeningitis. Multiple sclerosis. Tumor. Intracranial or extracranial. Metastatic. Primary: Meningioma, Schwannoma, Epidermoid, Chordoma. Trauma. Aneurysm. Dural external carotid artery cavernous sinus fistula. Sickle ceil disease. Diabetes mellitus. Syringobulbia. Infections. Sinusitis. Herpes simplex. Herpes zoster. Hepatitis A infection. Nonspecific viral infection. Tuberculosis. Whipple s disease. Leprosy. Arachnoiditis. Tricloroethylene. Hydroxystilbamidine. Amyloidosis. Spinal epidural anesthesia.")
48
Piramidal yol İnen sempatik lifler Kontralateral hemiparezi
Spinotalamik demet Kontralateral gövde ve ekstremitelerde his kusuru Orta serebellar pedünkül İpsilateral tremor Medial Longitudinal fasikül İnternükleer oftalmopleji İnen sempatik lifler İpsilateral Horner sendromu

49
Preganglionik sinir kökleri: Subaraknoid alan
TRİGEMİNAL NEVRALJİ ? GASSER GANGLİONUNDA YERLEŞİK LEZYONLAR Vasküler Anevrizma, kollagen doku hastalıkları Tümör İnfeksiyon H. Zoster, abse, petrozitis + Sempatik pleksus Okülosempatik paralizi + IV - VI Diplopi + VIII İşitme kaybı

50
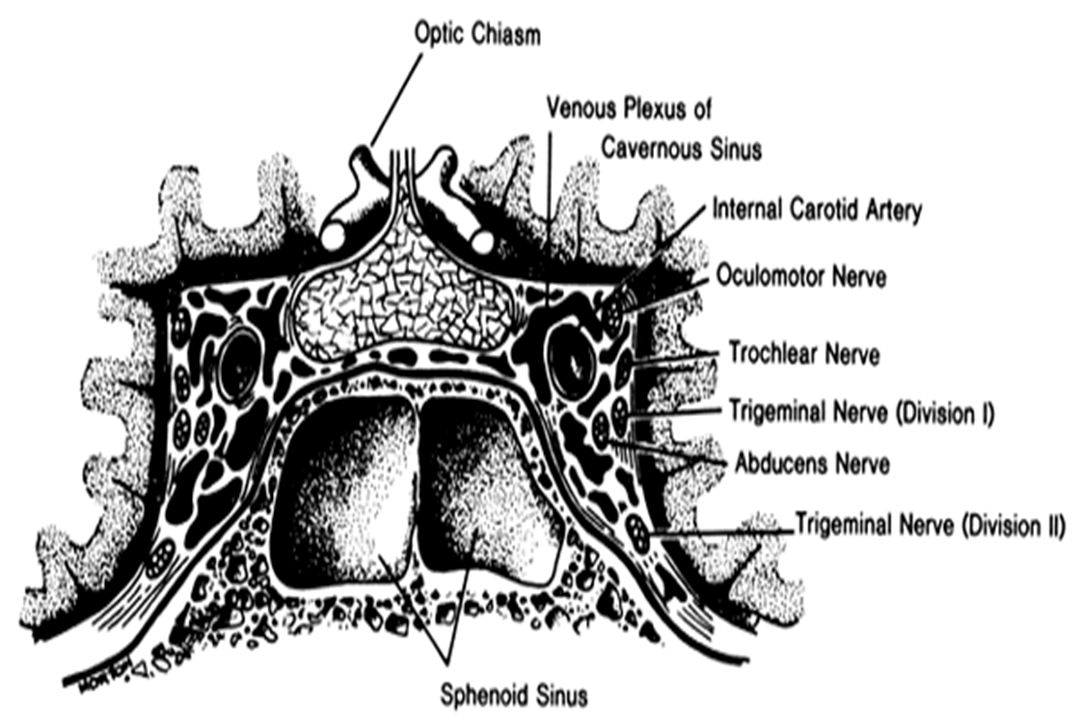
KAVERNÖZ SİNÜSTE YERLEŞİK LEZYONLAR SUPERİOR ORBİTAL FİSSÜRDE YERLEŞİK
PERİFERİK DALLARI ETKİLEYEN LEZYONLAR İnfeksiyon İnflamasyon; Bakteriyel-tbc-karsinomatöz-granülomatöz menenjit Travma Kafa kaidesi fraktürü Tümör Paget hastalığı Vasküler Anevrizma, infarkt (DM) Guillain-Barre sendromu
 Guillain-Barre sendromu.")
51
V. NERVUS FACİALİS Motor Mimik kaslarının innervasyonu Parasempatik
Gözyaşı, Nazal-palatal mukoza ve Tükrük glandlarının innervasyonu Refleks Göz kırpma-kornea, stapedius refleksleri Duysal Farinks (+IX) Burun ve damak mukozası (+V) Dışkulak yolu (+IX), Kulak ve mastoid üzeri derinin Dilin 2/3 ön kısmı: Tad duyusu SUPRANÜKLEER LEZYONLAR: Vasküler, demiyelinizan, tümör Karşı-alt yüz yarımında belirli felç + Emosyonel tepkiler sonucu oluşanlar ile istemli mimik hareketlerin kontrolü korunmuş olabilir + Parasempatik-tad duyusu-refleks işlevler korunmuş
 Burun ve damak mukozası (+V) Dışkulak yolu (+IX), Kulak ve mastoid üzeri derinin. Dilin 2/3 ön kısmı: Tad duyusu. SUPRANÜKLEER LEZYONLAR: Vasküler, demiyelinizan, tümör. Karşı-alt yüz yarımında belirli felç + Emosyonel tepkiler sonucu oluşanlar ile istemli mimik hareketlerin kontrolü. korunmuş olabilir + Parasempatik-tad duyusu-refleks işlevler korunmuş.")
52
ÇEKİRDEK VE ÇEKİRDEK SONRASI LEZYONLAR
Fasiyal paralizi + Stapedius refl. kaybı + Gözyaşı sekr. kaybı + Tad duyusu kaybı (-) Gözyaşı sekr. kaybı (-) Stapedius refl. kaybı (-) Tad duyusu (-) Tükrük sekresyonu kaybı
 Gözyaşı sekr. kaybı. (-) Stapedius refl. kaybı. (-) Tad duyusu. (-) Tükrük sekresyonu. kaybı.")
53
-Çekirdek ve lif demeti;
+ VI PPRF kortikospinal tr V spinal çekirdek Spinotalamik tr. -Posterior fossa; + VIII + V + VI + PONS + Serebellar pedünkül ve hemisfer -Temporal-Petroz kemik içindeki segmentler; Travma, tümör +VIII -Stilomastoid foramenin distali; Lenfadenopati, parotis tm veya inflamasyonu, Sarkoidoz, İnfeksiyöz mononükleoz, Travma

54
BELL PARALİZİSİ; Viral-Herpes simplex (?), Kulak-kulak ardında ağrı 2-3 gün içinde yerleşen yüz felci Tad duyusu bozl Hiperakuzi % olguda 3 ay içinde spontan iyileşme (ancak DM, AHT ile olasılık , Tedavi; Korneanın korunması, ilk hafta içinde başlanan PREDNİZOLON 60 mg/gün: 5 gün, sonra 10 mg/ gün eksiltme, ASİKLOVİR 5 X 800 mg/gün (10 gün).
.")
55
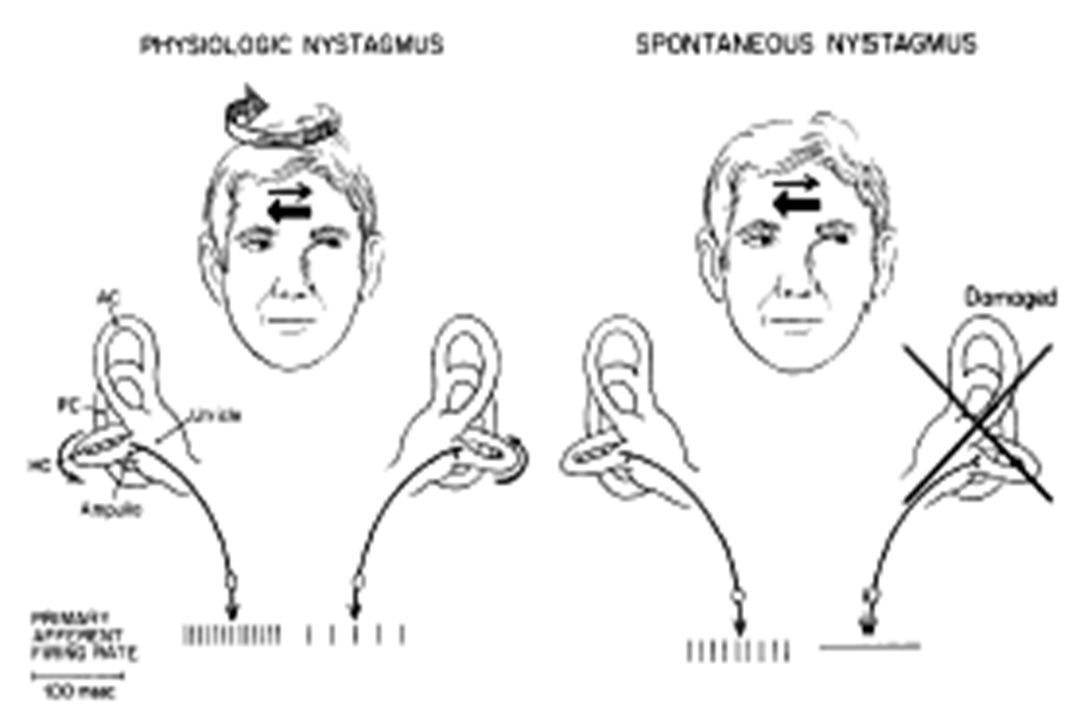
VIII. N. STATOAKUSTİKUS Motor Dengenin sağlanması Duysal İşitme
Refleks Stapedius refleksi İşlev bozukluğu halinde; (-) Ataksi, Hipo/anakuzi (+) Vertigo, Nistagmus, Bulantı-kusma-terleme, Tinnitus, İşitme kaybı çeşitleri; İletim Nörosensoriyel Merkezi İşitme Muayenesi; Fısıltı veya hışırtı algılanması Weber testi Rinne testi Schwabach testi
 Ataksi, Hipo/anakuzi. (+) Vertigo, Nistagmus, Bulantı-kusma-terleme, Tinnitus, İşitme kaybı çeşitleri; İletim. Nörosensoriyel. Merkezi. İşitme Muayenesi; Fısıltı veya hışırtı algılanması. Weber testi. Rinne testi. Schwabach testi.")
56
Saf ton odiometrisi Retrokoklear işitme kaybı örneği
Koklea lezyonları: Düşük frekanslarda kayıp VIII. sinir lezyonu: Kayıp; Hz Ön planda konuşmanın algılanması Saf ton odiometrisi Retrokoklear işitme kaybı örneği Koklea lezyonu: Meniere hastalığı Retrokoklear lezyonlar: Beyinsapı-İnternal akustik kanal girişi arasındaki subaraknoid mesafede yerleşik yapısal lezyonlar Travma: Kafa kaidesi fraktürü Toksin ve ilaçlar: Aminoglikozidler vs.

57
SUPRANÜKLEER LEZYONLAR:
IX. N. GLOSSOFARİNGEUS Motor Stilofaringeus kası ile yutma sırasında larinksin yukarı hareketi, farinksin elevasyonu ve genişlemesi Duysal Dilin 1/3 arka kısmının tad ve somatik duyusu Farinks, tonsiller, larinks Dışkulak yolu, timpan membranın iç yüzeyi Otonom Karotid cisim ve sinüsteki kemo- ve baro reseptörler ile PO2 ve AKB kontrolü, parotis bezesinin innervasyonu Refleks Yumuşak damak, farinks, solunum ve AKB regülasyonu ile ilgili refleksler İŞLEV BOZUKLUĞU HALİNDE Disfaji (+X) Glossofaringeal nevralji AKB refleks kontrolünde bozulma Solunum ritmi ve derinliğinin refleks kontrolünde bozulma Yumuşak damak ve farinks refleksi kaybı SUPRANÜKLEER LEZYONLAR: Bilateral-yaygın premotor nöron lezyonları Retiküler formasyon N. ambiguus (IX, X, XI) Psödobulber paralizi!
 Glossofaringeal nevralji. AKB refleks kontrolünde bozulma. Solunum ritmi ve derinliğinin refleks kontrolünde bozulma. Yumuşak damak ve farinks refleksi kaybı. SUPRANÜKLEER LEZYONLAR: Bilateral-yaygın premotor nöron lezyonları Retiküler formasyon N. ambiguus (IX, X, XI) Psödobulber paralizi!")
58
Wallenberg sendromu + X (ses boğukluğu ve disfaji)
+ VIII (bulantı, kusma, vertigo) V (IL yüz yarımında ağrı, ısı-ağrı duyusu ) spinotalamik yol (KL gövde ve ekstremitelerde ısı-ağrı ) serebellar lifler (ataksi) inen sempatik yol (Horner sendromu)
 V (IL yüz yarımında ağrı, ısı-ağrı duyusu ) spinotalamik yol (KL gövde ve ekstremitelerde ısı-ağrı ) serebellar lifler (ataksi) inen sempatik yol (Horner sendromu)")
59
Serebellopontin köşe Juguler foramen, retrofaringeal alan Travma (kaide kırığı), Tümör (primer, metastatik), Vasküler (AVM), İnfeksiyon Glossofaringeal nevralji +X + XI + XII Orofaringeal bölge, boyun Karsinom, Guillain-Barre send.
, İnfeksiyon. Glossofaringeal nevralji. +X. + XI. + XII. Orofaringeal bölge, boyun. Karsinom, Guillain-Barre send.")
60
SUPRANÜKLEER LEZYONLAR
X. N. VAGUS Motor Palatoglossus kası, Stilofaringeus ve tensor veli palatini dışındaki farinks ve palatal kaslar, larinks kasları, Duysal Arka kafa çukurunun durası Kulak ardı, dışkulak yolu, timpan membranın dış yüzeyi Farinks ve larinksin somatik duyusu Gastrointestinal ve solunum sistemleri Otonom Farinks, larinks, ösefagus-kolon, solunum yolları, kalp, pankreas, karaciğer Refleks Yumuşak damak, farinks, öksürme, kalbin otonom kontrolü İŞLEV BOZUKLUĞU HALİNDE Disfaji Ses kısılması-boğukluğu Kalp ritmi ve AKB kontrol bozukluğu Vazovagal senkop, Barsak hareketlerinin kontrol bozukluğu Yumuşak damak ve farinks refleksi kaybı ASPİRASYON SUPRANÜKLEER LEZYONLAR BEYİNSAPI SEREBELLOPONTİN KÖŞE-SUBARAKNOİD MESAFE JUGULER FORAMEN, RETROFARİNGEAL ALAN OROFARİNGEAL BÖLGE, BOYUN

61
PERİFERİK DALLARI FARİNGEAL SUPERİOR LARİNGEAL REKÜRRAN LARİNGEAL LEZYON SPEKTRUMU Aort anevrizması Mediyastende LAP Akciğer tm Boyun cerrahisi DM Sifiliz Nöritis SEMPTOM Ses kısıklığı Disfaji Akut ise solunum yolu obs.

62
XI. N. ACCESSORIUS Motor Sternokleidomastoid ve trapezius kasları BEYİNSAPI: + Poliyomiyelit + Motor Nöron Hastalığı SEREBELLOPONTİN KÖŞE-SUBARAKNOİD MESAFE JUGULER FORAMEN RETROFARİNGEAL BÖLGE BOYUN Cerrahi Yerel infeksiyonlar Radyoterapi + XII

63
XII. N. HYPOGLOSSUS Motor İntrensek dil kasları Duysal Dilin proprioseptif duyusu BEYİNSAPI JUGULER FORAMEN HİPOGLOSSAL KANAL: Tümör: - Glomus jugulare - Meningiom - Kordoma - Kolesteatoma İnflamasyon Kafa travması İnternal karotid arter Disseksiyonu Motor Nöron Lezyonu - Dilin lezyon tarafına deviasyonu - Atrofi Fasikülasyon RETROFARİNGEAL BÖLGE BOYUN Cerrahi Yerel infeksiyonlar Radyoterapi Tm [primer, metastatik (bronş, lenfoma, lösemi)] + XI
] + XI.")
64
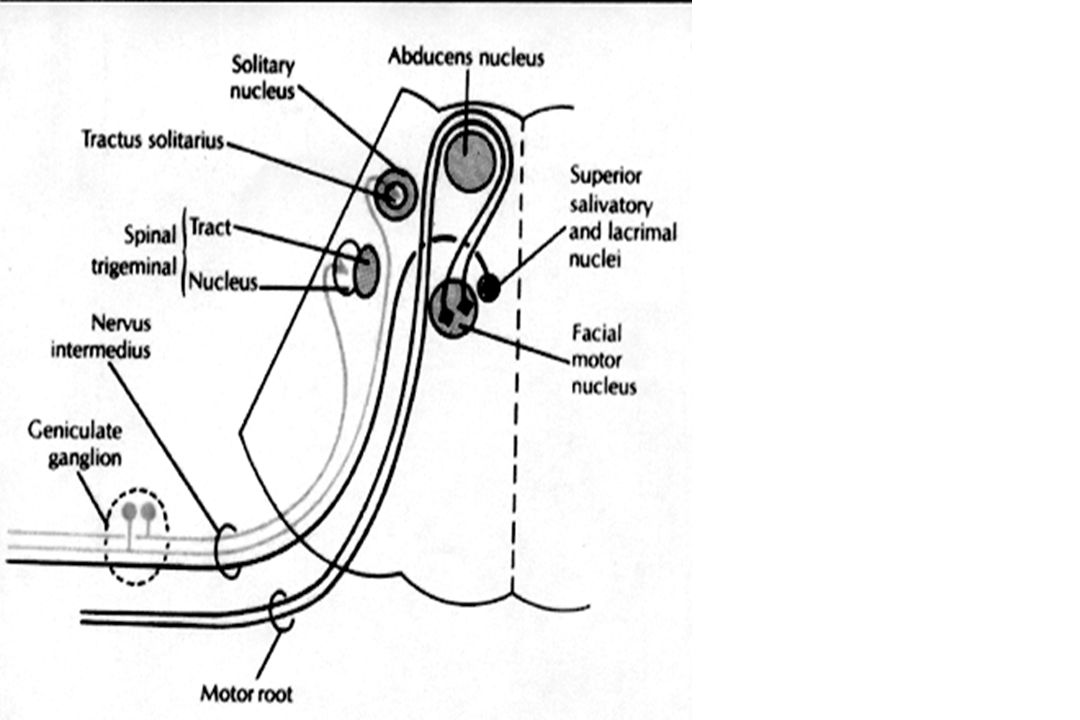
facial canal middle ear chorda tympani petrotympanic fissure
Facial Nerve Temporal, Zygomatic, Buccal, Mandibular, Cervical&Post. Auricular Brachiomotor: m. of facial expr.: stapedius,stylohyoid, mylohyoid, post.belly digastric facial canal middle ear chorda tympani petrotympanic fissure Special sensory: taste, ant. 2/3 tongue: facial canal middle ear chorda tympani petrotympanic fissure Visceromotor: preganglionic parasympathetic to submand. ganglia (innervates submand. &sublingual glands) greater superficial petrosal pterygoid canal pterygopalatine ganglia to lacrimal, nasal & palatine gl. internal acoustic meatus facial canal stylomastoid foramen
 greater superficial petrosal pterygoid canal. pterygopalatine ganglia to lacrimal, nasal & palatine gl. internal acoustic meatus facial canal stylomastoid foramen.")
65
C B A Lesion at A: Ipsilateral paralysis of all facial movements
corneal reflex is lost sensory area to ear is lost Lesion at B: A(+) impaired sublingual, submandi- bular glands’ secretions& taste over ant. 2/3 of the tongue hyperacusis Lesion at C: A&B(+) im- paired ipsilat.lacrimation C B A
 impaired. sublingual, submandi- bular glands’ secretions& taste over ant. 2/3 of the tongue. hyperacusis. Lesion at C: A&B(+) im- paired ipsilat.lacrimation. C. B. A.")
68
Causes of Peripheral Facial Nerve Palsy
Idiopathic (Bell's palsy) Infectious: Herpes simplex Herpes zoster Otitis media Borrelia burgdorferi Human immunodeficiency virus Syphilis Infectious mononucleosis Mastoiditis Poliomyelitis Meningitis Malaria Leprosy Rubella Mumps Osteomyelitis Cat scratch disease Inflammatory Guillain-Barré syndrome Sarcoidosis Multiple sclerosis Arteritis Melkersson-Rosenthal syndrome Behçet syndrome Wegener's granulomatosis Lymphomatoid granulomatosis Kawasaki disease Angioedema Pseudotumor (Tolosa-Hunt syndrome) Amyloidosis Idiopathic hypertrophic cranial pachymeningitis Neoplastic Schwannoma Neurofibroma Meningioma Cholesteatoma Parotid gland tumor Metastasis Carcinomatous meningitis Leukemia Metabolic Diabetes mellitus Hypothyroidism Uremia Porphyria Trauma: Surgical trauma to nerve Congenital, Familial Miscellaneous Pregnancy Paget's disease Osteopetrosis Hypertension Diphtheria-pertussis-tetanus vaccination Pontine infarction Myasthenia gravis Traumatic external carotid artery aneurysm Lumbar extradural blood patch Vascular malformation Pseudotumor cerebri Ethylene glycol poisoning
 Infectious: Herpes simplex. Herpes zoster. Otitis media. Borrelia burgdorferi. Human immunodeficiency virus. Syphilis. Infectious mononucleosis. Mastoiditis. Poliomyelitis. Meningitis. Malaria. Leprosy. Rubella. Mumps. Osteomyelitis. Cat scratch disease. Inflammatory. Guillain-Barré syndrome. Sarcoidosis. Multiple sclerosis. Arteritis. Melkersson-Rosenthal syndrome. Behçet syndrome. Wegener s granulomatosis. Lymphomatoid granulomatosis. Kawasaki disease. Angioedema. Pseudotumor (Tolosa-Hunt syndrome) Amyloidosis. Idiopathic hypertrophic cranial pachymeningitis. Neoplastic. Schwannoma. Neurofibroma. Meningioma. Cholesteatoma. Parotid gland tumor. Metastasis. Carcinomatous meningitis. Leukemia. Metabolic. Diabetes mellitus. Hypothyroidism. Uremia. Porphyria. Trauma: Surgical trauma to nerve. Congenital, Familial. Miscellaneous. Pregnancy. Paget s disease. Osteopetrosis. Hypertension. Diphtheria-pertussis-tetanus vaccination. Pontine infarction. Myasthenia gravis. Traumatic external carotid artery aneurysm. Lumbar extradural blood patch. Vascular malformation. Pseudotumor cerebri. Ethylene glycol poisoning.")
72
Cranial Nerve VIII: Vestibulocochlear

73
1st neurone: bipolar cells of the gang
1st neurone: bipolar cells of the gang. cochleare 2nd neurone: multipolar neurones of nuclei cochleares

74
Auditory path. 2nd neurones corpus trapezoideum opposite side form lemniscus lat. colliculus inferior 3rd or 4th neurone colliculus superior cerebellum & corpus geniculatum mediale 4th or 5th neurone: Heschl's transverse gyrus & Wernicke's centre of the temporal lobe

75
Vestibular path 1st neurone: bipolar cells of the ganglion vestibulare form the N. vestibularis on the floor of the internal acoustic meatus FLM 2nd & following neurones: from nuc.vestibularis lat. (Deiter's) to: formatio reticularis - motor nuclei of nerves III, IV & VI - nuc. ruber & as the tr. vestibulosp. into the ant. column of the sp. cord nuc. ruber nuc. vestibularis sup. (Bechterew's) supplies some fibres to cerebellum
 to: - formatio reticularis - motor nuclei of nerves III, IV & VI - nuc. ruber & as the tr. vestibulosp. into the ant. column of the sp. cord. nuc. ruber. nuc. vestibularis sup. (Bechterew s) supplies some fibres to cerebellum.")
76
Cranial Nerve VIII: Vestibulocochlear
Disease affecting hearing Acoustic neuroma (8th n) Presbyacusis (cochlea) Trauma “ Wax (ext.&middle ear) Otitis media “ Otosclerosis “ Disease affecting balance Vascular diseases(b.stem) Demyelination “ Drugs (DPH, streptomycin) Viral, benign conditions Disease affecting hearing & balance (cochlea&labyrinth) Meniere internal auditory meatus
 Presbyacusis (cochlea) Trauma Wax (ext.&middle ear) Otitis media Otosclerosis Disease affecting balance. Vascular diseases(b.stem) Demyelination Drugs (DPH, streptomycin) Viral, benign conditions. Disease affecting hearing & balance (cochlea&labyrinth) Meniere. internal auditory meatus.")
77
Cochleo-vestibular Disease Main Symptoms Main Signs
Deafness Nystagmus Ataxia Positional nystagmus Deafness Tinnitus Vertigo Loss of balance

79
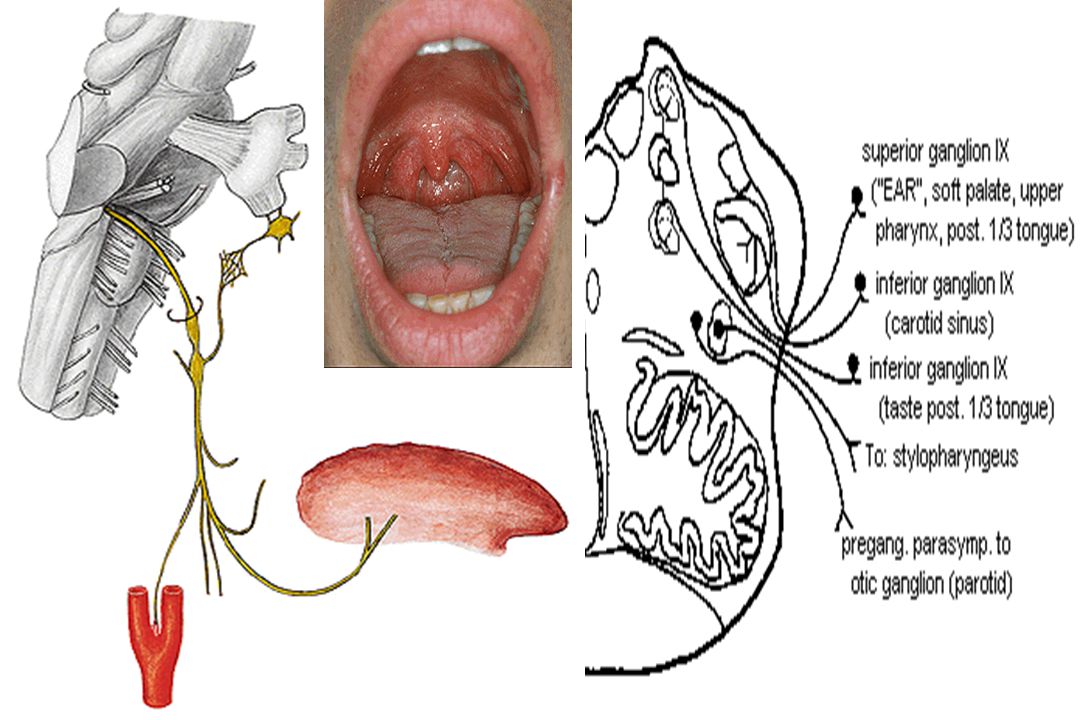
Cranial Nerve IX: Foramen: jugular
Special visceromotor: Function: elevates pharynx nucleus ambiguus stylopharyngeus Gen. Sensory Components Function: general sensation of external, middle ear & auditory tube geniculate ganglion spinal trigeminal nucleus Special Viscerosensory Component: Function: taste, posterior 1/3 tongue=> inferior petrosal ganglion rostral tractus solitarius Region Entered: infratemporal fossa Gen. Viscerosensory: Sensory receptors of ant. surface epiglottis, root of tongue, border of soft palate, uvula, tonsil, pharynx, eustachian tube, carotid sinus & body caudal tractus solitarius Gen.Visceromotor comp.: İnf.salivary nuc.tympani n. lesser petrosal notic ganglionauriculotemporal n. Function: parotid gland secretion

80
Microvilli of the taste receptor cells project into an opening in the epithelium, the taste pore, where they make contact with gustatory stimuli. Cell types in mammalian taste buds. (A) The taste bud is a barrel-shaped structure containing different cell types, including basal cells, dark cells, and light cells. These epithelial receptor cells make synaptic contact with distal processes of cranial nerves VII, IX, or X, whose cell bodies lie within the cranial nerve ganglia. Microvilli of the taste receptor cells project into an opening in the epithelium, the taste pore, where they make contact with gustatory stimuli. (B) The characteristic spindle shape of taste receptor cells is revealed when a subset of light cells is immunoreacted to an antibody against α–gustducin, a gustatory G protein. (C) When sectioned transversely, light cells appear round in cross section, as shown by α–gustducin immunoreactivity (red), whereas the characteristic shape of dark cells produced by their thin cytoplasmic projections enveloping neighboring light cells is revealed with an antibody against the H blood group antigen (green). These epithelial receptor cells make synaptic contact with distal processes of cranial nerves VII, IX, or X
 The taste bud is a barrel-shaped structure containing different cell types, including basal cells, dark cells, and light cells. These epithelial receptor cells make synaptic contact with distal processes of cranial nerves VII, IX, or X, whose cell bodies lie within the cranial nerve ganglia. Microvilli of the taste receptor cells project into an opening in the epithelium, the taste pore, where they make contact with gustatory stimuli. (B) The characteristic spindle shape of taste receptor cells is revealed when a subset of light cells is immunoreacted to an antibody against α–gustducin, a gustatory G protein. (C) When sectioned transversely, light cells appear round in cross section, as shown by α–gustducin immunoreactivity (red), whereas the characteristic shape of dark cells produced by their thin cytoplasmic projections enveloping neighboring light cells is revealed with an antibody against the H blood group antigen (green). These epithelial receptor cells make synaptic contact with distal processes of cranial nerves VII, IX, or X.")
82
Nervus Vagus Special Viscerosensory: taste in epiglottisinf. Gang.rostral tr. solitarius Special visceromotor: (deglutition phonation) n. Ambiguuspalatal, pharynx & larynx muscles General viscerosensory: post.epiglottis,larynx, trachea, bronchi, esopagus, stomach, s. İntestine, colon inf. ganglioncaudal tr. solitarius General somatosensory: : auricle, ext. auditory meatussup. ganglionspinal trigeminal nuc General Visceromotor: dorsal motor nucleus preganglionic parasympathetic to abdomen & thorax cardiac depression, visc. mov., secretion

83
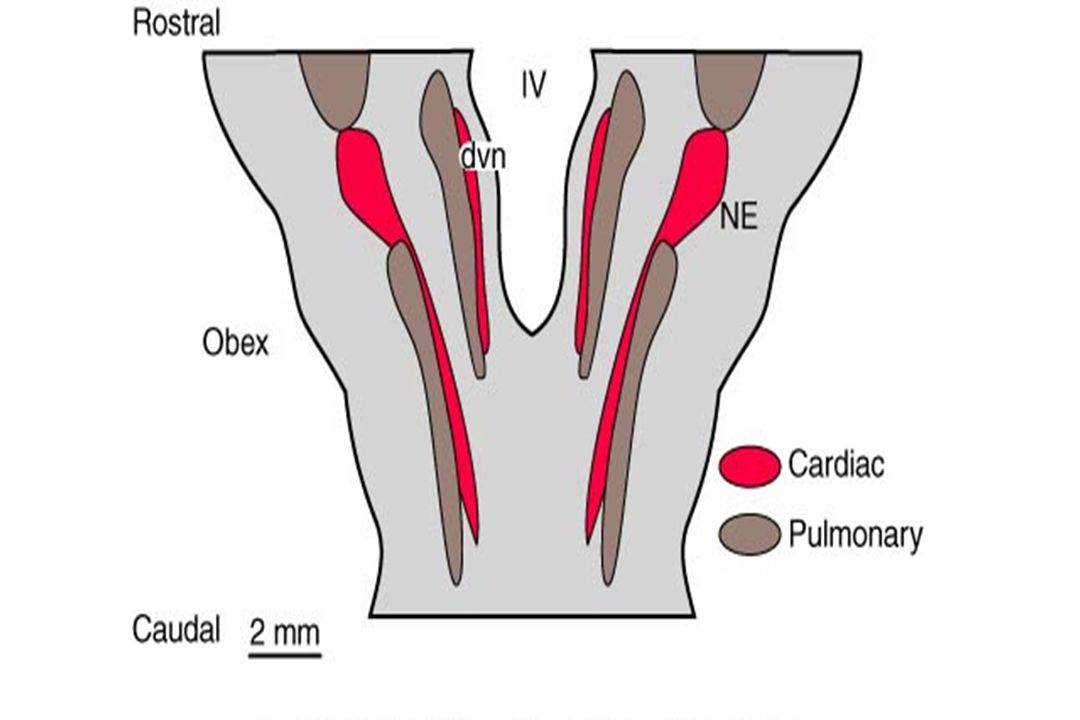
Primary afferents in the IX and X cranial nerves project to the NTS
Neural pathways for the arterial baroreflex. Primary afferents in the IX and X cranial nerves project to the nucleus tractus solitarii (NTS). As shown on the right, interneurons forming sympathetic pathways project from the NTS to the caudal ventrolateral medulla, which in turn project to the rostral ventral lateral medulla, the source of reticulospinal projections to the intermediolateral columns in the spinal cord. Pathways from the NTS to the nucleus ambiguus form the major parasympathetic arm of the reflex, GABA, γ-aminobutyric; L-glu, L-glutamate; ACH, acetylcholine; NA, norepinephrine. (Guyenet, 1990).
. As shown on the right, interneurons forming sympathetic pathways project from the NTS to the caudal ventrolateral medulla, which in turn project to the rostral ventral lateral medulla, the source of reticulospinal projections to the intermediolateral columns in the spinal cord. Pathways from the NTS to the nucleus ambiguus form the major parasympathetic arm of the reflex, GABA, γ-aminobutyric; L-glu, L-glutamate; ACH, acetylcholine; NA, norepinephrine. (Guyenet, 1990).")
84
Vagal visceral afferent projections
Vagal visceral afferent projections. The nodose ganglion contains the somata of vagal afferents. The axons enter the solitary tract and terminate in the nucleus of the solitary tract, the area postrema, the nucleus cuneatus, and the dorsal motor nucleus of the vagus. The nucleus of the solitary tract has a wide projection, either directly or through the parabrachial nucleus. The lines represent most ascending pathways. Some descending pathways also are present, but they are not illustrated (e.g., insular cortex projections to the nucleus of the solitary tract). (DMN, dorsal motor nucleus of the vagus) (Rutechi P: Anatomical, physiological, and theoretical basis for the antiepileptic effect of vagus nerve stimulation. Epilepsia 31 (Suppl 2):52, 1990.) vagal afferents
. (DMN, dorsal motor nucleus of the vagus) (Rutechi P: Anatomical, physiological, and theoretical basis for the antiepileptic effect of vagus nerve stimulation. Epilepsia 31 (Suppl 2):52, 1990.) vagal afferents.")
86
Right & Left recurrent laryngeal nerves
forming the esophageal plexus. (RVN, right vagus nerve; RRLN, right recurrent laryngeal nerve; LVN, left vagus nerve; LRLN, left recurrent laryngeal nerve; Tr, trachea; Es, esophagus; Ao, aorta.) (Lee KS, Im G, Kim IY et al: Tumors involving the intrathoracic vagus and phrenic nerves demonstrated by computed tomography: Anatomical features. Clin Radiol 44:302, 1991.)
 (Lee KS, Im G, Kim IY et al: Tumors involving the intrathoracic vagus and phrenic nerves demonstrated by computed tomography: Anatomical features. Clin Radiol 44:302, 1991.)")
87
Selected Causes of Vagus Nerve Dysfunction
Lateral medullary syndrome Hyperextension injury of upper cervical spine Chronic lead poisoning Radiation therapy to head and neck Glomus vagale tumor Neuroma Schwannoma presenting as cerebellopontine angle mass Nasopharyngeal diphtheria Viral or postviral mononeuritis Herpes simplex Cytomegalovirus Herpes zoster Multiple system atrophy Superior laryngeal neuralgia

88
Cranial Nerve XI: Spinal Accessory
Brachiomotor Comp: Foramen: exits by jugular; enters by foramen magnum ant. horn cells C1-C5 Target: trapezius, sternokleidomastoid Function: head & shoulder movement Spc.Visceromotor Comp.: Caudal nuc. ambiguus vagus muscles of larynx Function: phonation

89
Symptoms of the 11th n. involvement
Torticollis (dystonia) Asymmetric shoulders Impaired arm elevation
 Asymmetric shoulders. Impaired arm elevation.")
91
Cranial Nerve XII: Hypoglossal
Foramen: hypoglossal canal Region Entered: neck Components: somatomotor Target, Function: all tongue muscles, except palatoglossus

92
Infranuclear paralysis of the right trigeminal, facial, and hypoglossal nerves, showing deviation of the mandible and tongue to the right

93
12th n. palsy: Asymmetry Deviation Atrophy Fasciculations 10th nerve

94
Common Condition Affecting 9th, 10th & 12th Nerve Function
Bulbar palsy Dysartria Dysphagia Dysphonia Aspiration Motor neuron disease Cerebrovascular disease Syringobulbia Erosive tm of the skull base Guillain-Barré syndrome Recurrent laryngeal nerve palsy Myastenia gravis

96
Representative levels of the brain stem on which major structures are outlined. The four intrinsic arterial zones are repeated as serial homologies at each of the succeeding levels depicted on the right side of each one. Vertical lines indicate the median zone, horizontal lines the paramedian zone. The lateral zone is stippled, and cross-hatching indicates the dorsal zone. (Lat, lateral) (Gillilau LA: Anatomy and embryology of the arterial system of the brain stem and cerebellum. In Vinken PJ, Bruyn GN (eds): Handbook of Neurology, Vol 11, p 29. New York, Elsevier, 1972.)
 (Gillilau LA: Anatomy and embryology of the arterial system of the brain stem and cerebellum. In Vinken PJ, Bruyn GN (eds): Handbook of Neurology, Vol 11, p 29. New York, Elsevier, 1972.).")
Benzer bir sunumlar