Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
ARTERİOSKLEROZ VE İLİŞKİLİ NÖROLOJİK PROBLEMLERE GENEL YAKLAŞIM
Oturum Başkanı ve Konuşmacı: Konuşmacı: Prof. Dr. Abdülkadir KOÇER Prof. Dr. Talip ASIL

2
Beyin Damar Hastalıklarına Yaklaşım
Prof Dr Talip Asil Bezmialem Vakıf Üniversitesi Tıp Fakültesi Nöroloji Anabilim Dalı

3
Alt Başlıklar Tanımlar ve istatistikler İnme geçiren hastaya yaklaşım
İnmeden korunma

4
İnme Dünya Sağlık Örgütü tanımlamasına göre İnme, vasküler nedenler dışında görünür bir neden olmaksızın, fokal serebral fonksiyon kaybına ait belirti ve bulguların hızla yerleşmesi ile karakterize klinik bir sendromdur. Semptomlar tanım gereği 24 saatten uzun sürer veya ölümle sonlanabilir

5
İnme Gelişmiş ülkelerde kalp hastalıkları ve kanserlerden sonra üçüncü, dünya genelinde ikinci ölüm nedenidir. Erişkin çağda en önemli uzun dönem özürlülük kaynağıdır. Alzheimer hastalığından sonra ikinci sırada demansa yol açar Hastaneye yatışa neden olan en sık nörolojik hastalıktır

6
İstatistikler Amerika’da
Tahmini 3 milyon inme geçirmiş hasta yaşamaktadır. Her yıl 500 bin kişi ilk kez veya tekrarlayıcı inme geçirmektedir İnme geçiren hastaların yaklaşık %20’si uzun dönem özel bakıma gereksinim göstermektedir Her yıl yaklaşık 150 bin ölüme neden olmaktadır.

7
Yıllık İnme İnsidansı 55- 64 yaşında 1.3- 3.6/ 1000,
75 yaş üzerinde / 1000 Tüm inmelerin ancak % 3- 5’ i ise 44 yaşından önce görülmektedir. Kadınlarda yaşları arasında inme insidansı erkeklerden 2- 3 kat daha azdır. Bu fark 85 yaşına doğru azalmaktadır

8
İnme Alt Grupları Tıkayıcı İnme %80 İntraserebral Kanama%15
Subaraknoid Kanama %5

11
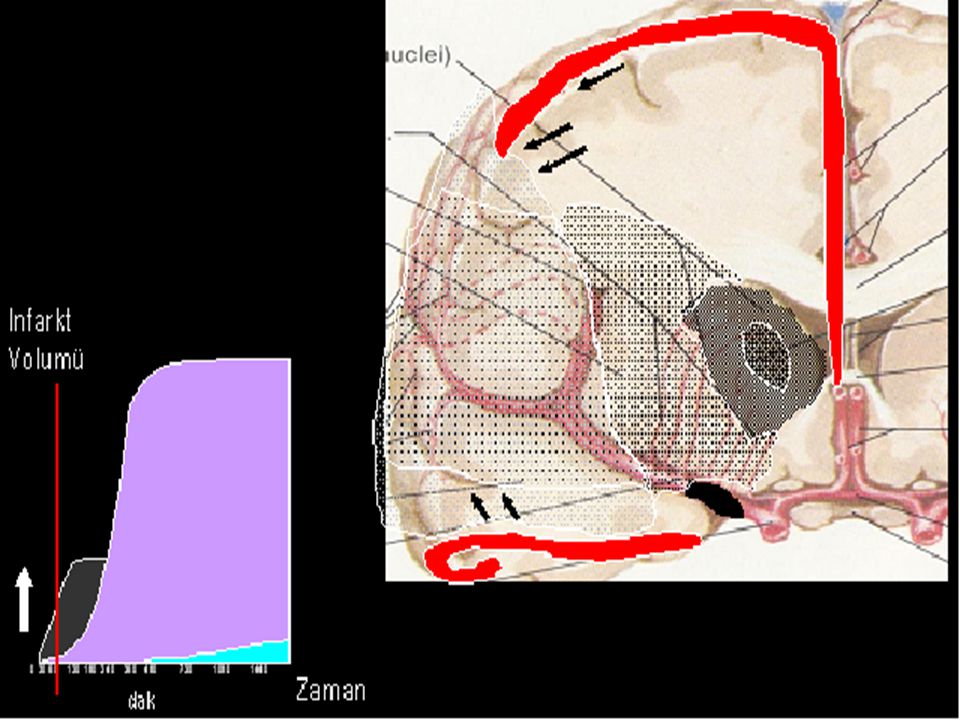
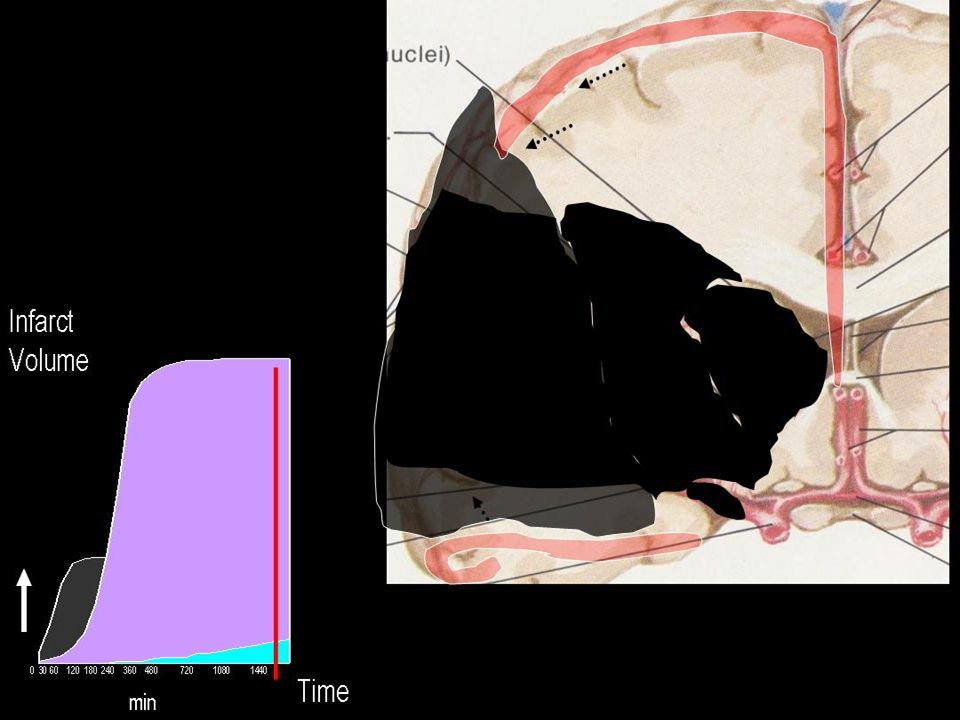
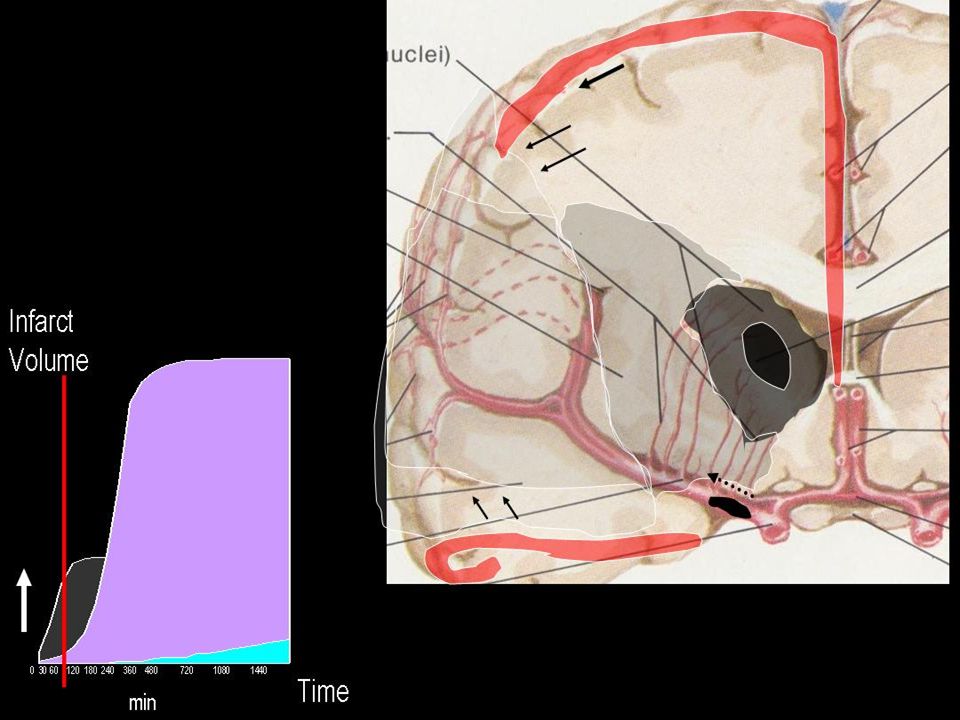
Kritik Serebral Kan Akımı

12
Etyoloji Küçük Damar Hastalığı Geniş Damar Hastalığı 25% 25%
Stroke 2001;32:2735 Neurology 1994;44:626 Geniş Damar Hastalığı Küçük Damar Hastalığı 25% 25% Kardiyoembolik Diğer etyolojiler ve sebebi bulunamayanlar 25% 25%

13
İntraserebral Kanama

14
Vaka 70 Y Erkek Yakınma görmede bulanıklaşma (tek göz emin değil)
Bulguları birkaç dakika içinde düzelmiş Risk faktör HT Muayene Normal

15
Vaka 42 Yaş bayan 14 kez sol vücut yarısında 2-20 dakika süren uyuşma
Risk faktörü yok Muayene normal

16
Vaka 52 yaş erkek 3 hafta önce sağ tarafta güçsüzlük ve konuşma bozukluğu (afazi) Risk faktorleri : sigara ve obez MUAYENE : normal (sadece sol karotiste üfürüm)
")
17
Vaka 75 y erkek Sağ tarafta güçsüzlük 4 gün önce olmuş 2 saatte düzelmiş Risk faktor HT Muayene normal

18
ABCD2 Skorlaması Yaş >60 1 A (age) Kan basıncı > 140/90 mmHg
B (Blood Pressure) Klinik Özellikler Tek taraflı güçsüzlük Konuşma bozukluğu 2 C (Clinical Features) Semptomların süresi >60 dakika 10-59 dakika < 10 dakika D (Duration) Diabetes Mellitus D (Diabetes)
 Klinik Özellikler. Tek taraflı güçsüzlük. Konuşma bozukluğu. 2. C (Clinical Features) Semptomların süresi. >60 dakika dakika. < 10 dakika. D (Duration) Diabetes Mellitus. D (Diabetes)")
19
ABCD2 Skorlaması 0-3 risk düşük 4-5 orta derecede risk
>5 yüksek derecede risk

20
Minör inme veya Geçici İskemik Ataklı hastalarda zamanlama

21
77 yaşında erkek hasta DM, HT, Hiperlipidemi öyküsü var 40 yıl 1 paket/gün sigara öyküsü var 1 yıl önce sağ hemiparezi geçirmiş damar tıkanıklığı olduğu söylenmiş Aspirin 300 mg, ACE inhibitörü ve insülin kullanıyor

22
Risk Faktörleri Değiştirilemeyen Risk Faktörleri Yaş Cinsiyet Etnisite
Genetik Faktörler Modifiye Edilebilir Risk Faktörleri HT AF ve diğer kardiyak nedenler DM Hiperlipidemi Sigara Fiziksel Aktivite Karotis Darlığı ve TIA Potansiyel Risk Faktörleri Alkol Hiperhomosisteinemi Migren Oral Kontraseptifler İnfeksiyonlar……

23
İnme Semptomları Hemiparezi/ monoparezi Konuşma Bozukluğu
Görme Problemleri Başağrısı Dengesizlik EMS Response: Stroke Symptoms Stroke should be suspected by the emergency medical services in any patient with sudden onset of focal neurological signs such as hemiparesis, aphasia or hemianopia, or altered consciousness.1 Symptoms can develop in isolation but usually appear in combination;1 they may include any of those listed on the slide. In stroke, the early course of events may be characterised by gradually worsening deterioration, by the sudden appearance of severe deficits or by fluctuations in symptom severity.2–6 When a patient is comatose and there is no-one able to provide a history, it is important to consider other causes of loss of consciousness, including hypoglycaemia, drug overdose, seizures or craniocerebral trauma.1 References 1. Adams HP, Brott TG, Crowell RM et al. Guidelines for the management of patients with acute ischemic stroke: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1995; 25: 1901–14. 2. Mohr J, Caplan LR, Melski JW et al. The Harvard Cooperative Stroke Registry. A prospective registry. Neurology 1978; 28: 754–62. 3. Caplan LR, Hier DB, D’Cruz I. Cerebral embolism in the Michael Reese Stroke Registry. Stroke 1983; 14: 530–6. 4. Bougousslavsky J, Van Melle G, Regli F. The Lausanne Stroke Registry. Analysis of 1000 consecutive patients with first stroke. Stroke 1988; 19: 1083–92. 5. Foulkes MA, Wolf PA, Price TR et al. The Stroke Data Bank. Design, methods and baseline characteristics. Stroke 1988; 19: 547–554. 6. Goldstein M, Barnett HJM, Orgogozo JM et al. Report of the WHO Task Force on stroke and other cerebrovascular disorders. Stroke 1989; 20: 1407–31. 16

24
Fasiyal Paralizi ANORMAL NORMAL EMS Response: Face Value
This slide shows the facial expression of a stroke victim, emphasising facial droop in particular. It is illuminating to compare the plight of the stroke victim with that of a patient with myocardial infarction. The face of a heart attack patient is likely to show that he is in pain, making the urgency of his need clearly evident. In contrast, as we see in this slide, the appearance of the stroke victim does not suggest pain and symptoms such as hemiparesis or aphasia make it unlikely that he will be clamouring for attention. Yet both these patients deserve equally high priority – for the stroke victim, time is brain. ANORMAL NORMAL 17

25
İNME ÜNİTESİ ORGANİZASYONU
PRiMER KORUMA İKİNCİL KORUMA PRIMARY PREVENTION SECONDARY PREVENTION İNME ÜNİTESİ ORGANİZASYONU ACİL MÜDAHELELER REHABİLİTASYON Treatment Puzzle A comprehensive approach to the management of stroke requires the consideration of all major aspects: not only the acute care and rehabilitation of stroke victims, but also primary prevention to reduce overall risk of stroke in the population as a whole, as well as secondary prevention to reduce the risk of second or subsequent strokes in stroke survivors. Given these multiple considerations, and the difficulties inherent in intermeshing them successfully, the organisation of services becomes the central link in the treatment puzzle. It is increasingly established that optimising pathways improves care. Streamlining the process of management provision has been shown to reduce mortality and may improve functional outcome, even without changes in acute medical therapy. In a meta-analysis of 10 randomised trials, mortality during the first 4 months was 28% lower in the stroke unit than it was in the general ward.1 This mortality benefit was shown to persist throughout the first year after stroke.1 Moreover, the reduction in mortality does not result from salvage of patients who survive with increased disability: 9 of the 10 studies analysed also reported gains in a variety of functional measures.1 Improving the organisation of stroke care may also provide important economic benefits. The specification of a critical care path for stroke has been shown to reduce the overall length of the patient’s hospital stay, as well as the cost per patient.2 There is also evidence that the introduction of such measures may be able to reduce the incidence of complications.3 References 1. Langhorne P, Williams BO, Gilchrist W, Howie K. Do stroke units save lives? Lancet 1993; 342: 395–8. 2. Bowen J, Yaste C. Effect of a stroke protocol on hospital costs of stroke patients. Neurology 1994; 44: 1961–4. 3. Odderson IR, McKenna BS. A model for management of patients with stroke during the acute phase. Outcome and economic implications. Stroke 1993; 24: 1823–7. 7

26
Beyin Krizi Akut İnme: Beyin Krizi Her Dakika önemlidir Zaman beyindir
Terapötik çaresizlikle mücadele

27
İnmeli hastalar için görüntülemede teknolojik yenililikler
tPA CT ASA İnme Ünitesi TCD DWI- MRI PWI-MRI 4th gen CT Power Mmode TCD 4 - slice CTA CTP 64 slice-CTA Toshiba Aquilion 320

28
İnme Tedavisinde Gelişmeler (Level A Kanıtlar)
tPA CT ASA hemikranyektomi İnme Ünitesi

29
Akut İnmeli Hastaya Yaklaşım

30
İnmeli Hastada Acil Yaklaşım Hedefleri
Progresyonu engellemek Rekürrensi engellemek Komplikasyonları engellemek Hayatı tehdit eden durumlarla mücadele etmek Nöroprotektif tedaviler Tedavi edici yaklaşımlar

31
Vital Fonksiyonlar Airway - entübasyon koma
hipoventilation aspirasyon riski Breathing - pulse oxymetry - normoventilasyon Circulation - i.v. yol, No Dekstroz - EKG - Kan Basıncı Kontrol et Kan Şekeri (hypoglisemi) tansiyon, hipotansiyonu düzelt Hidrasyon sağla Ateş yüksekliğine izin verme EMS Response: Vital Functions In about half of all patients who are thought to have stroke at the time the ambulance is dispatched, this diagnosis will be found to be incorrect once the patient arrives in hospital.1 Yet many of these people will have other diagnoses that remain serious and may be equally life-threatening. In view of this, it is vital that emergency medical personnel attend first to the ABCs of general medical resuscitation– i.e. Airway, Breathing and Circulation.2 In early ischaemic stroke, the airway is usually stable, except in cases with brainstem infarction or repetitive seizures. Airway problems are more likely in haemorrhagic stroke or large hemispheric infarction, especially if there is alteration of consciousness. In these cases, airway resistance can be decreased with the jaw-thrust manoeuvre and, if necessary, ventilation can be assisted temporarily using a bag-valve-mask device, or with a nasopharyngeal airway. If there is evidence of inadequate ventilation, or if the gag reflex is absent, intubation is needed. Assisted ventilation should be continued until the patient can receive further treatment at the hospital.3 Circulatory collapse is unusual in isolated stroke, except in cases of impending brain herniation. In patients who are found unconscious or in a state of collapse, other causes such as myocardial infarction should always be considered first. However, it should be remembered that patients with stroke frequently have concomitant problems that may predispose to circulatory collapse – heart disease, for example.3 In view of this, the close monitoring of heart rhythm by ECG is another essential step. Blood pressure needs close monitoring although, in stroke patients, hypotension is uncommon in the prehospital setting.3 Reactive hypertension is quite commonly present, but does not usually require treatment while the patient is en route to hospital.3 Indeed, the general rule should be that hypertension is not treated at all in the acute phase4 – this aspect is discussed more fully in Section 3 (Emergency Room Procedure). If there is hypotension, the usual cause is volume depletion. Correction of hypovolaemia and the restoration of cardiac output is an important part of care during the first few hours after stroke.5 Intravenous access should be established in all patients, with normal saline or lactated Ringer’s solution administered at a keep-open rate.2 However, in the absence of volume depletion, the administration of large volumes of fluid should be avoided, as there is a definite risk of cardiac failure – and some risk of cerebral oedema – in these (elderly) patients. Monitoring and maintaining blood oxygenation is very important, especially in patients with impaired consciousness. Hypoxia promotes anaerobic metabolism and depletes energy stores in the injured brain, thereby causing extension of the lesion.6 For monitoring purposes, continuous recording of arterial blood gases provides the ideal in information terms, but fingertip pulse oxymetry offers greater practical utility as it is easier to set up and patients find the procedure less distressing. Blood glucose should be measured, since hypoglycaemia can sometimes mimic stroke and hyperglycaemia can worsen the situation. The close monitoring of body temperature is also important,4 as rising body temperature is a valuable indicator of possible infection, and there is also evidence that raised body temperature is associated with a worse outcome. 7–9 Raised body temperature should be reduced with antipyretics, despite the fact that the evidence for benefit from this measure remains equivocal. References 1. Kothari R, Barsan W, Brott T et al. Frequency and accuracy of prehospital diagnosis of acute stroke. Stroke 1995; 26: 937–41. 2. Kerber RE, Ornato JP, Brown DD et al. Guidelines for cardiopulmonary resuscitation and emergency cardiac care. III. Adult advanced cardiac life support. JAMA 1992; 268: 2199–41. 3. Brott T, Kothari R. Prehospital management of stroke patients. Cerebrovasc Dis 1997; 7 (suppl 3): 2–4. 4. European Ad Hoc Consensus Group. European strategies for early intervention in stroke: a report of an Ad Hoc Consensus Group meeting. Cerebrovasc Dis 1996; 6: 315–24. 5. Grotta JC, Pettigrew LE, Allen S et al. Baseline hemodynamic state and response to hemodilution in patients with acute cerebral ischemia. Stroke 1985; 16: 790–5. 6. Yamaguchi T, Minematsu K, Hasegawa Y. General care in acute stroke. Cerebrovasc Dis 1997; 7 (suppl 3): 12–7. 7. Azzimondi G, Bassein L, Nonino F et al. Fever in acute stroke worsens prognosis. Stroke 1996; 26: 2040–43. 8. Reith J, Jorgensen HO, Pedersen PM et al. Body temperature in acute stroke: relation to stroke severity, infarct size, mortality and outcome. Lancet 1996; 347: 422–5. 9. Davalos A, Castillos J, Pumar JM, Noya M. Body temperature and fibrinogen are related to early neurological deterioration in acute ischemic stroke. Cerebrovasc Dis 1997; 7: 64–9. 18
 tansiyon, hipotansiyonu düzelt. Hidrasyon sağla. Ateş yüksekliğine izin verme. EMS Response: Vital Functions. In about half of all patients who are thought to have stroke at the time the ambulance is dispatched, this diagnosis will be found to be incorrect once the patient arrives in hospital.1 Yet many of these people will have other diagnoses that remain serious and may be equally life-threatening. In view of this, it is vital that emergency medical personnel attend first to the ABCs of general medical resuscitation– i.e. Airway, Breathing and Circulation.2. In early ischaemic stroke, the airway is usually stable, except in cases with brainstem infarction or repetitive seizures. Airway problems are more likely in haemorrhagic stroke or large hemispheric infarction, especially if there is alteration of consciousness. In these cases, airway resistance can be decreased with the jaw-thrust manoeuvre and, if necessary, ventilation can be assisted temporarily using a bag-valve-mask device, or with a nasopharyngeal airway. If there is evidence of inadequate ventilation, or if the gag reflex is absent, intubation is needed. Assisted ventilation should be continued until the patient can receive further treatment at the hospital.3. Circulatory collapse is unusual in isolated stroke, except in cases of impending brain herniation. In patients who are found unconscious or in a state of collapse, other causes such as myocardial infarction should always be considered first. However, it should be remembered that patients with stroke frequently have concomitant problems that may predispose to circulatory collapse – heart disease, for example.3 In view of this, the close monitoring of heart rhythm by ECG is another essential step. Blood pressure needs close monitoring although, in stroke patients, hypotension is uncommon in the prehospital setting.3. Reactive hypertension is quite commonly present, but does not usually require treatment while the patient is en route to hospital.3 Indeed, the general rule should be that hypertension is not treated at all in the acute phase4 – this aspect is discussed more fully in Section 3 (Emergency Room Procedure). If there is hypotension, the usual cause is volume depletion. Correction of hypovolaemia and the restoration of cardiac output is an important part of care during the first few hours after stroke.5 Intravenous access should be established in all patients, with normal saline or lactated Ringer’s solution administered at a keep-open rate.2 However, in the absence of volume depletion, the administration of large volumes of fluid should be avoided, as there is a definite risk of cardiac failure – and some risk of cerebral oedema – in these (elderly) patients. Monitoring and maintaining blood oxygenation is very important, especially in patients with impaired consciousness. Hypoxia promotes anaerobic metabolism and depletes energy stores in the injured brain, thereby causing extension of the lesion.6 For monitoring purposes, continuous recording of arterial blood gases provides the ideal in information terms, but fingertip pulse oxymetry offers greater practical utility as it is easier to set up and patients find the procedure less distressing. Blood glucose should be measured, since hypoglycaemia can sometimes mimic stroke and hyperglycaemia can worsen the situation. The close monitoring of body temperature is also important,4 as rising body temperature is a valuable indicator of possible infection, and there is also evidence that raised body temperature is associated with a worse outcome. 7–9 Raised body temperature should be reduced with antipyretics, despite the fact that the evidence for benefit from this measure remains equivocal. References. 1. Kothari R, Barsan W, Brott T et al. Frequency and accuracy of prehospital diagnosis of acute stroke. Stroke 1995; 26: 937– Kerber RE, Ornato JP, Brown DD et al. Guidelines for cardiopulmonary resuscitation and emergency cardiac care. III. Adult advanced cardiac life support. JAMA 1992; 268: 2199– Brott T, Kothari R. Prehospital management of stroke patients. Cerebrovasc Dis 1997; 7 (suppl 3): 2–4. 4. European Ad Hoc Consensus Group. European strategies for early intervention in stroke: a report of an Ad Hoc Consensus Group meeting. Cerebrovasc Dis 1996; 6: 315– Grotta JC, Pettigrew LE, Allen S et al. Baseline hemodynamic state and response to hemodilution in patients with acute cerebral ischemia. Stroke 1985; 16: 790–5. 6. Yamaguchi T, Minematsu K, Hasegawa Y. General care in acute stroke. Cerebrovasc Dis 1997; 7 (suppl 3): 12–7. 7. Azzimondi G, Bassein L, Nonino F et al. Fever in acute stroke worsens prognosis. Stroke 1996; 26: 2040– Reith J, Jorgensen HO, Pedersen PM et al. Body temperature in acute stroke: relation to stroke severity, infarct size, mortality and outcome. Lancet 1996; 347: 422–5. 9. Davalos A, Castillos J, Pumar JM, Noya M. Body temperature and fibrinogen are related to early neurological deterioration in acute ischemic stroke. Cerebrovasc Dis 1997; 7: 64–")
32
Nörostatus Glasgow koma skoru (Koma)
Kas güçsüzlüğü, unilateral/bilateral Fasial parezi veya göz deviasyonu Konuşma (Afazi dizartri) Hemianopi veya major duysal defisit Semptomlarda düzelme veya kötüleşme? Nöbet, travma, ense sertliği? * 2 dakika maximum EMS Response: Neurostatus It is important that the attending EMS team makes a neurological examination prior to transportation, because the evolving pattern of neurological abnormalities may provide help in localising the site of the stroke lesion and in assessing the severity of the problem. However, given the time pressure of the situation, this examination need not be completely exhaustive. It is very important to look for evidence of head or neck injury, cardiac murmur, arterial bruit or absent cranial artery pulses.1 Assessment of the degree of passive flexion in neck should be made, provided there is no suggestion of neck injury.1 Features such as aphasia, memory disturbance, visual field defects, and hemianopia are important localising signs, while the pattern of motor and sensory deficits may also provide clues to stroke subtype. 1,2 References 1. Adams HP, Brott TG, Crowell RM et al. Guidelines for the management of patients with acute ischemic stroke: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1995; 25: 1901–14. 2. Goldstein M, Barnett HJM, Orgogozo JM et al. Report of the WHO Task Force on stroke and other cerebrovascular disorders. Stroke 1989; 20: 1407–31. 19
 Hemianopi veya major duysal defisit. Semptomlarda düzelme veya kötüleşme Nöbet, travma, ense sertliği * 2 dakika maximum. EMS Response: Neurostatus. It is important that the attending EMS team makes a neurological examination prior to transportation, because the evolving pattern of neurological abnormalities may provide help in localising the site of the stroke lesion and in assessing the severity of the problem. However, given the time pressure of the situation, this examination need not be completely exhaustive. It is very important to look for evidence of head or neck injury, cardiac murmur, arterial bruit or absent cranial artery pulses.1 Assessment of the degree of passive flexion in neck should be made, provided there is no suggestion of neck injury.1 Features such as aphasia, memory disturbance, visual field defects, and hemianopia are important localising signs, while the pattern of motor and sensory deficits may also provide clues to stroke subtype. 1,2. References. 1. Adams HP, Brott TG, Crowell RM et al. Guidelines for the management of patients with acute ischemic stroke: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1995; 25: 1901– Goldstein M, Barnett HJM, Orgogozo JM et al. Report of the WHO Task Force on stroke and other cerebrovascular disorders. Stroke 1989; 20: 1407–")
33
Laboratuar incelemeler
Hb, Hcr, thromb, leuc gluc, CRP, SR, CK, CK-MB, creat APTT, TT-SPA/INR Elektrolitler İdrar incelemesi EKG PA Akciğer BT

34
Kritik Fonksiyonlar Kardiyak PA Akc Vücut Isısı Kan Gazları BP EKG
> 37.5°C tedavi et Kan Gazları

35
Acil i.v. Tedaviler Kusma Hyperglisemi:
anti-emetik Hyperglisemi: insulin Çok yüksek BP (sistolik > 220, diastolik > 130 mm Hg): Kaptopril Furosemid Ajitasyon: Kısa süre, sedatifler ER Procedure: Immediate i.v. Therapy When the patient arrives in hospital, it is sometimes necessary to initiate certain intravenous therapies immediately, to stabilise the patient’s symptoms before further investigations. A patient who is vomiting may need an anti-emetic, for example, and treatment with insulin is imperative in cases of hyperglycaemia (although the exact definition of qualifying hyperglycaemia may be subject to revision). As discussed previously, there are rare situations in which treatment with antihypertensives might be considered. A short-acting sedative may be needed if the patient is agitated, particularly if a CT scan is proposed. Sedation should not be used routinely in acute stroke patients. 30
: Kaptopril Furosemid. Ajitasyon: Kısa süre, sedatifler. ER Procedure: Immediate i.v. Therapy. When the patient arrives in hospital, it is sometimes necessary to initiate certain intravenous therapies immediately, to stabilise the patient’s symptoms before further investigations. A patient who is vomiting may need an anti-emetic, for example, and treatment with insulin is imperative in cases of hyperglycaemia (although the exact definition of qualifying hyperglycaemia may be subject to revision). As discussed previously, there are rare situations in which treatment with antihypertensives might be considered. A short-acting sedative may be needed if the patient is agitated, particularly if a CT scan is proposed. Sedation should not be used routinely in acute stroke patients. 30.")
37
İnmeden korunma

38
Birincil Korunma İnme için yüksek riskli hastaları belirlemek ve inmeden korunma stratejileri oluşturmak -Aile öyküsü, özgeçmiş bilgileri ve risk faktörlerinin belirlenmesi -Yaşam tarzı değişiklikleri -Kan Basıncı ayarlaması -Kan Şekeri düzenlemeleri -Kan Kolesterol düzeyi takibi ve tedavisi -Sigara ve alkol

39
Damarsal Yaşlanma

40
Risk Faktörleri İnme ilişkisi
Wolf PA, Stroke 1991

41
Kan Basıncı İnme İlişkisi

42
Hipertansiyon Tedavisi ve İnme Riski

43
İnmeli hastalar için kan basıncı ile ilgili öneriler
İlk inmeden korunmak için Sistolik KB <140 mmHg (Kanıt düzeyi C) Diastolik KB<90 (Kanıt Düzeyi A) İnme veya TİA geçiren hastalarda tekrarı önlemek için KB <140/90 (Kanıt Düzeyi C) diabetik hastalarda <130/80 (Kanıt Düzeyi B) İnmeli hastalarda antihipertansif ACE inhibitörü veya diüretik (Kanıt Düzeyi B) İnmeli hastada antihipertansif tedavi başlama zamanı ile ilgili net veri yok
 Diastolik KB<90 (Kanıt Düzeyi A) İnme veya TİA geçiren hastalarda tekrarı önlemek için KB <140/90 (Kanıt Düzeyi C) diabetik hastalarda <130/80 (Kanıt Düzeyi B) İnmeli hastalarda antihipertansif ACE inhibitörü veya diüretik (Kanıt Düzeyi B) İnmeli hastada antihipertansif tedavi başlama zamanı ile ilgili net veri yok.")
44
Diabet İnme İlişkisi Abbott RD.JAMA 1987

45
Diabet-İnme Mortalitesi İlişkisi
Stamler J Diabetes Care 1993

46
İnmeli hastalar için kan şekeri ile ilgili öneriler
40 yaş üstü tüm bireylerde her 3 yılda bir açlık kan şekeri bakılması (Kanıt Düzeyi C) Diabet için ilave risk faktörü varsa test daha sık tekrar edilmeli ve/veya yükleme testi yapılmalı (Kanıt düzeyi C) İnmeli hastalarda kan şekeri ayarlaması bireysel olmalı ancak HbA1c düzeyi<7 olmalı (Kanıt Düzeyi A) Tüm erişkin diabetik hastalarda kontrendikasyon yoksa düşük doz ASA (Kanıt Düzeyi A)
 Diabet için ilave risk faktörü varsa test daha sık tekrar edilmeli ve/veya yükleme testi yapılmalı (Kanıt düzeyi C) İnmeli hastalarda kan şekeri ayarlaması bireysel olmalı ancak HbA1c düzeyi<7 olmalı (Kanıt Düzeyi A) Tüm erişkin diabetik hastalarda kontrendikasyon yoksa düşük doz ASA (Kanıt Düzeyi A)")
47
İnmeli hastalar için kan lipitleri ile ilgili öneriler
40 yaş üstü erkeklerde ve postmenapozal kadınlarda açlık kan lipit düzeyleri (HDL, LDL, total kolesterol ve total trigliserit) her 1-3 yılda bir ölçülmeli (Kanıt Düzeyi C) Herhangi bir yaşta ilave vasküler risk faktörü olan her hastada kan lipitleri ölçülmeli (Kanıt Düzeyi C) İskemik inmeli hastalarda LDL 100 mg/dl’nin altında tutulmalı (Kanıt Düzeyi A) İskemik inmeli hastalarda kan lipit düzeyinden bağımsız olarak statin başlanmalı (Kanıt Düzeyi A)
 her 1-3 yılda bir ölçülmeli (Kanıt Düzeyi C) Herhangi bir yaşta ilave vasküler risk faktörü olan her hastada kan lipitleri ölçülmeli (Kanıt Düzeyi C) İskemik inmeli hastalarda LDL 100 mg/dl’nin altında tutulmalı (Kanıt Düzeyi A) İskemik inmeli hastalarda kan lipit düzeyinden bağımsız olarak statin başlanmalı (Kanıt Düzeyi A)")
48
Sigara ve İnme Günde 20 veya fazla sigara içenlerde inme riski 2-4 kat daha fazla Aktif sigara içenlerde inme veya TİA geçirme oranı %18 Sigara inme ilişkisi günlük sigara sayısı ile doğru orantılı Günlük 20 den az sigara içenlerde inme riski 1.56 kat 20 den fazla sigara içenlerde 2.25 kat artmaktadır Aktif sigara içenlerde ölümcül inme oranı1.60 kat artar

49
Yaşam tarzı ile ilgili öneriler
Diyetle günlük Na alımı 9-50 yaş arası 1500 mg, yaş arası 1300mg 70 yaş sonrası 1200 mg olmalı Haftada 4-7 kez dk egzersiz (hızlı yürüyüş, yüzme, bisiklet sürme, jogging vs) Vücut kitle indeksi <25 göbek çevresi kadınlarda <88cm erkeklerde <102cm olmalı Alkol kullanımı <günlük 2 kadeh erkeklerde haftalık <14 kadeh kadınlarda <9 kadeh olmalı
 Vücut kitle indeksi <25 göbek çevresi kadınlarda <88cm erkeklerde <102cm olmalı. Alkol kullanımı <günlük 2 kadeh erkeklerde haftalık <14 kadeh kadınlarda <9 kadeh olmalı.")
Benzer bir sunumlar