Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
TROMBOFİLİ ve ÜYT Prof.Dr. Mehmet Zeki TANER
Gazi Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum Anabilim Dalı Yüksek Riskli Gebelikler-Prenatal Tanı ve Tedavi Ünitesi

2
Trombofili Tanımı : Tromboza Eğilim
1-Tromboz oluşumunu kolaylaştıran 2-Kalıtsal ve-veya edinsel nedenlerin meydana getirdiği 3-Klinik tablo(lar)
")
3
Trombofilinin Klinik Bulguları
Venöz tromboembolizm (DVT±PE) Yüzeyel ven trombozu Alışılmadık bölgelerde tromboz Purpura Fulminans (erişkin-neonatal-çocuk) Varfarine bağlı deri nekrozu Arteryel tromboz (olası?) (AMİ, İskemik inme) İmplantasyon ( IVF) başarısızlığı ? Tekrarlayan gebelik kayıpları Olası gebelik komplikasyonları (prematüre , ölü doğum, fötal gelişme geriliği, preeklampsi, plesenta dekolmanı)
 Yüzeyel ven trombozu. Alışılmadık bölgelerde tromboz. Purpura Fulminans (erişkin-neonatal-çocuk) Varfarine bağlı deri nekrozu. Arteryel tromboz (olası ) (AMİ, İskemik inme) İmplantasyon ( IVF) başarısızlığı Tekrarlayan gebelik kayıpları. Olası gebelik komplikasyonları (prematüre , ölü doğum, fötal gelişme geriliği, preeklampsi, plesenta dekolmanı)")
4
TROMBOFİLİLER Kalıtsal Faktor V Leiden (FVL) mutasyonu
Protrombin gen mutasyonu (G20210A), Protein C eksikliği Protein Seksikliği Antitrombin III (ATIII) eksikliği Methylenetetrahidrofolat reduktaz mutasyonu (MTHFR) (C677T), Edinsel Antifosfolipd sendromu Primer Sekonder have been recently implicated in early pregnancy loss and IVF implantation failure, by impairing the initial vascularization process occurring at implantation, which is necessary for a successful pregnancy (Geva et al., 1995; Grandone et al., 2001; Azem et al., 2004; Kujovich, 2004). Antiphospholipid antibodies and reproduction.William H. Kutteh. Journal of Reproductive Immunology 1997 (35) :
, Protein C eksikliği. Protein Seksikliği. Antitrombin III (ATIII) eksikliği. Methylenetetrahidrofolat reduktaz mutasyonu (MTHFR) (C677T), Edinsel. Antifosfolipd sendromu. Primer. Sekonder. have been recently implicated in early pregnancy loss and IVF. implantation failure, by impairing the initial vascularization. process occurring at implantation, which is necessary for a successful pregnancy (Geva et al., 1995; Grandone et al., 2001; Azem et al., 2004; Kujovich, 2004). Antiphospholipid antibodies and reproduction.William H. Kutteh. Journal of Reproductive Immunology 1997 (35) :")
5
Antifosfolipid Sendromu Sınıflaması
I. Primer APS II. Sekonder APS A. Otoimmun hastalıklar (1) Connective tissue disease Sistemik lupus eritematozus ‘Lupus-benzeri’ hastalık (‘muhtemel ’ SLE) Diskoid lupus Romatoid artritis Mikst Konnektif Doku Hastalığı Sjiigren‘s sendromu Sistemik skleroz Ankilozan spondilitis Vaskulitis Poliarteritis nodoza Dev hücreli arteritis/poliartraljia romatika Behcet’s hastalığı Undiferansiye konnektif doku hastalığı (2) Diğer Diabetes mellitus Crohn‘s hastalığı Otoimmun troid hastalığı B. Maligniteler 1) (Solid tumörler Timoma Akciğer, böbrek, over, serviks, prostat karsinomu 2) Hematolojik Lenfoma Lösemi Waldenstrom’s makroglobinemi Myeloproliferatif hastalıklar C.İlaçların Oluşturduğu durumlar Fenotiazinler Prokainamid Klorotiazid Etosuksimid Oral kontraseptifler Alfa-interferon Fenitoin Quinine, quinidine Hidralazin D. Enfeksiyon Hastalıkları Sifiliz HIV enfeksiyonu Malaria E. Diğer Son safha böbrek yetmezliği Komplike kronik graft-konakçı hastalığı Antiphospholipid antibodies and reproduction.William H. Kutteh. Journal of Reproductive Immunology 1997 (35) :
 Connective tissue disease. Sistemik lupus eritematozus. ‘Lupus-benzeri’ hastalık (‘muhtemel ’ SLE) Diskoid lupus. Romatoid artritis. Mikst Konnektif Doku Hastalığı. Sjiigren‘s sendromu. Sistemik skleroz. Ankilozan spondilitis. Vaskulitis. Poliarteritis nodoza. Dev hücreli arteritis/poliartraljia romatika. Behcet’s hastalığı. Undiferansiye konnektif doku hastalığı. (2) Diğer. Diabetes mellitus. Crohn‘s hastalığı. Otoimmun troid hastalığı. B. Maligniteler. 1) (Solid tumörler. Timoma. Akciğer, böbrek, over, serviks, prostat karsinomu. 2) Hematolojik. Lenfoma. Lösemi. Waldenstrom’s makroglobinemi. Myeloproliferatif hastalıklar. C.İlaçların Oluşturduğu durumlar. Fenotiazinler. Prokainamid. Klorotiazid. Etosuksimid. Oral kontraseptifler. Alfa-interferon. Fenitoin. Quinine, quinidine. Hidralazin. D. Enfeksiyon Hastalıkları. Sifiliz. HIV enfeksiyonu. Malaria. E. Diğer. Son safha böbrek yetmezliği. Komplike kronik graft-konakçı hastalığı. Antiphospholipid antibodies and reproduction.William H. Kutteh. Journal of Reproductive Immunology 1997 (35) :")
6
Edinsel Trombofili Nedenleri
Kanıtı Güçlü Olan Nedenler Kanıtı Zayıf Olan Nedenler Aktif Kanser Kemoterapi, AFLA Send., Miyeloproliferatif Hastalıklar HİT, Nefrotik Sendrom YDP, TTP, Orak Hücreli anemi OKS, Östrojen tedavisi, Hamilelik-Lohusalık Vaskülitler İnflamatuvar bağırsak Hast. Tromboenjitis obliterans Behçet sendromu, SLE Variköz venler, Dehidratasyon Venöz damar anomalileri Progesteron tedavisi İnfertilite tedavisi Hiperhomosisteinemi HIV İnfeksiyonu

7
Kalıtsal Trombofililer-Sıklık
Tipi Sağlıklı Popülasyon (%) Trombozlu Olgular (%) Aktive Protein C- FV Leiden 3-7 20-40 Hiperhomosisteinemi 5-10 10-25 Protrombin Gen Mutasyonu 1-3 6 Protein C eksikliği 3 Protein S eksikliği 1-2 Antitrombin eksikliği 1
 Trombozlu. Olgular (%) Aktive Protein C- FV Leiden Hiperhomosisteinemi Protrombin Gen Mutasyonu Protein C eksikliği Protein S eksikliği Antitrombin eksikliği")
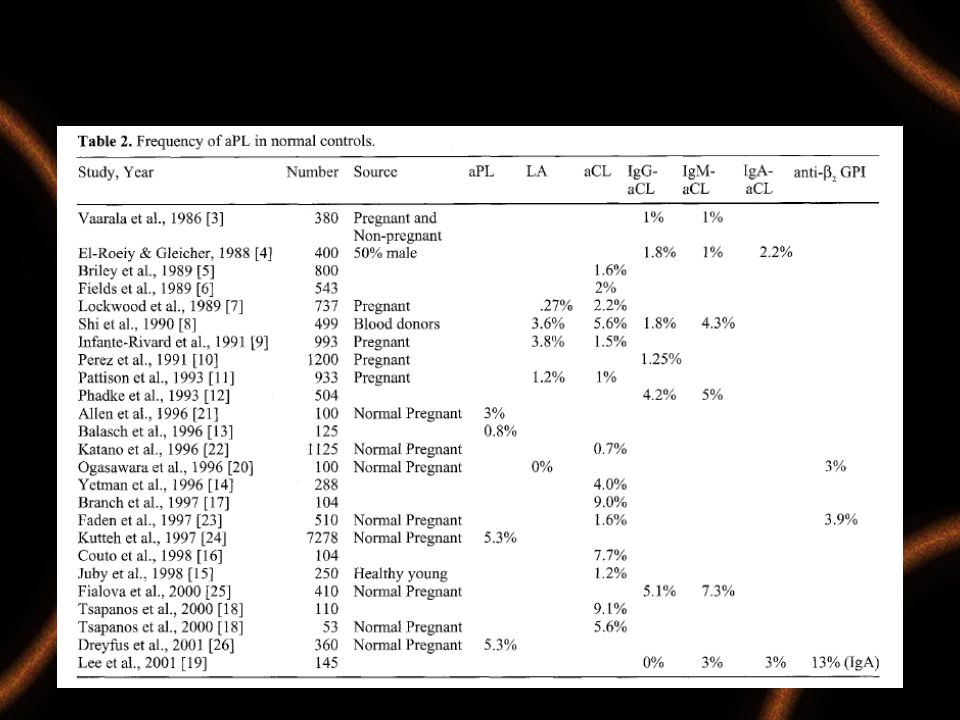
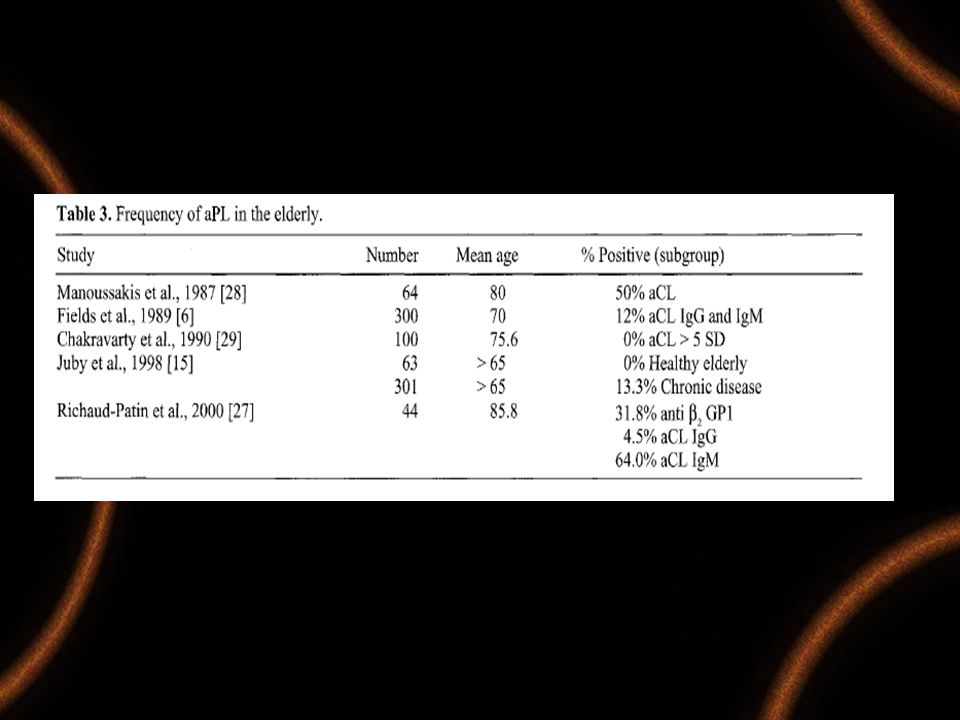
8
AP Sıklığı Normal Gebelerde %2-5 Sistemik Lupus ta %50

11
Laboratory thrombophilias and venous thromboembolism Hylton V Joffe and Samuel Z Goldhaber Vascular Medicine 2002; 7: 93–102

12
Thromboz Risk Faktörleri
Herediter Trombofili Edinsel Trombofili Ateroskleroz Thrombosis Cerrahi travma Hareketsizlik Estrogenler Enflamasyon Malignite

13
Maternal Fetal Tıp ve Perinatoloji Derneği 2008-M.Demir
NORMAL BİREYLER Pıhtılaşma sistemi Normal kan akımı Doğal antikoagülanlar Sağlam endotel Fibrinoliz ŞEMATİZE ETMEK GEREKİRSE, NORMAL ŞARTLAR ALTINDA HEMOSTATİK DENGE BURADA İZLENDİĞİ GİBİDİR. DIŞ GÖRÜNÜŞÜMÜZÜN FARKLILIĞINA BENZER ŞEKİLDE PIHTILAŞMA SİSTEMİMİZ ile PIHTIYI ENGELLEYİCİ SİSTEMLERİMİZ ARASINDAKİ DENGENİN ŞEKLİ DE FARKLIDIR: Maternal Fetal Tıp ve Perinatoloji Derneği 2008-M.Demir 13

14
Maternal Fetal Tıp ve Perinatoloji Derneği 2008-M.Demir
Sağlam endotel Normal kan akımı Pıhtılaşma sistemi Doğal antikoagülanlar Fibrinoliz GENETİK YATKINLIĞI OLANLAR BAZILARIMIZDA DENGE BURADA İZLENDİĞİ ŞEKİLDE KURULMUŞTUR. İŞTE, BU KİŞİLERİN TROMBOZ GEÇİRME EŞİKLERİ DÜŞÜKTÜR. HEMOSTATİK DENGELERİ BURADAKİ GİBİ HASSAS BİR ŞEKİLDE KURULMUŞ OLAN KİŞİLERE BİR ÖRNEK VERMEK İSTİYORUM: NORMAL FAKTÖR V 506. AMİNOASİT KONUMUNDA ARGİNİN BULUNDURUR. ANCAK, ÜLKEMİZDE HER 100 KİŞİNİN 8 KADARINDA BU KONUMDA ARGİNİN DEĞİL, GLUTAMİN BULUNUR. BU POLİMORFİZME FAKTÖR V LEIDEN ADI VERİLMEKTEDİR. FAKTÖR V LEIDEN TAŞIYAN KİŞİLERİN KANLARI DOĞAL ANTİKOAGÜLAN SİSTEMİN İŞLEYİŞİNDEKİ BİR BOZUKLUK NEDENİYLE DAHA KOLAY PIHTILAŞIR. FAKTÖR V LEIDENin SEBEP OLDUĞU BU BOZUK PIHTILAŞMA FENOTİPİNE AKTİVE PROTEİN C REZİSTANSI DENİLİR. AKTİVE PROTEİN C REZİSTANSI OLAN BİR KİŞİNİN HEMOSTATİK DENGESİ BURADA İZLENDİĞİ GİBİDİR. BU KİŞİLER TROMBOZ İÇİN EK BİR RİSK FAKTÖRÜNE MARUZ KALDIKLARINDA –MESELA ...- Maternal Fetal Tıp ve Perinatoloji Derneği 2008-M.Demir 14

15
Maternal Fetal Tıp ve Perinatoloji Derneği 2008-M.Demir
Doğal antikoagülanlar GEBELİKTE Normal kan akımı Sağlam endotel Fibrinoliz Pıhtılaşma sistemi Tetikleyici Faktör GEBE KALDIKLARINDA DENGE TERSİNE DÖNÜP .... VEN PIHTISI OLUŞABİLMEKTEDİR. Maternal Fetal Tıp ve Perinatoloji Derneği 2008-M.Demir 15

16
Edinsel ve Kalıtsal Etmenlerin Birlikteliği
Bauer KA, Hematology 2002 16

17
Traditional model (individual factors; left) and new model (threshold level; right) for evaluation of causes of recurrent pregnancy loss.
 and new model (threshold level; right) for evaluation of causes of recurrent pregnancy loss.")
18
BARDAĞI TAŞIRAN SON DAMLA

19
Antifosfolipid Sendromu Tanı Kriterleri
Klinik Kriterler 1)Arteryel/venoz tromboz Thrombocytopenia CNS syndromes—stroke, chorea Cardiac valve disease Livedo Reticularis 2)Gebelik Morbiditesi RPL, IUGR, Preeklampsi, P.Dekolmanı Laboratuvar Kriterleri -IgG/IgM anticardiolipin antikor -orta/yüksek titrede - Lupus Antikoagulan 6 hafta ara ile Wilson A, Gharavi AE, Koike T, et al International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome: report of an international workshop. Arthritis Rheum 1999; 42:1309–11.
Arteryel/venoz tromboz. Thrombocytopenia. CNS syndromes—stroke, chorea. Cardiac valve disease. Livedo Reticularis. 2)Gebelik Morbiditesi. RPL, IUGR, Preeklampsi, P.Dekolmanı. Laboratuvar Kriterleri. -IgG/IgM anticardiolipin antikor -orta/yüksek titrede. - Lupus Antikoagulan. 6 hafta ara ile. Wilson A, Gharavi AE, Koike T, et al International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome: report of an international workshop. Arthritis Rheum 1999; 42:1309–11.")
20
Antifosfolipid Sendrom SYDNEY SAPPORO KRİTERLERİ REVİZYONU (2006)
")
21
Selected Data From a Systematic Review of Thrombophilia and Pregnancy Outcomes, Meta-analysis Robertson L, Wu O, Langhorne P, et al. Thrombophilia in pregnancy: a systematic review. Br J Haematol. 2006;132: 171–196. IUFD indicates intrauterine fetal death; IUGR, intrauterine growth restriction; MTHFR, methylenetetrahydrofolate reductase; PT, prothrombin; SAB, spontaneous abortion.

22
% Obstetric manifestations 9 Pre-eclampsia/eclampsia 3 Toxemia 0.6
OBSTETRICAL AND FETAL MANIFESTATIONS IN THE COHORT OF 1,000 APS PATIENTS ENROLLED BY THE EUROPEAN APL FORUM % Obstetric manifestations 9 Pre-eclampsia/eclampsia 3 Toxemia 0.6 Abruptio placentae 0.3 Post-partum cardio-pulmonary syndrome Fetal manifestations 36 Early fetal losses 17 Late fetal losses

23
PCO TROMBOFİLİ

24
Plazminojen aktivator sistem:
The plasminogen activator system in women with polycystic ovary syndrome William U. Atiomo,.,*SusieA. Bates, John E. Condon, Steve Shaw, Jonathan I-/. West, Archibald G. Prentice, Fertil Steril 1998;69: 7 PCOS 12 kontrol olgusu Plazminojen aktivator sistem: Euglobulin clot lysis times, plasminogen activator inhibitor 1 (PAI-1) activity, fibrinogen, plasminogen, lpha-2 antiplasmin concentrations Sonuç: PCOS’lu olgularda proteolitik enzim üretiminde azalma eğilimi saptandı.
 activity, fibrinogen, plasminogen, lpha-2 antiplasmin concentrations. Sonuç: PCOS’lu olgularda proteolitik enzim üretiminde azalma eğilimi saptandı.")
25
OHSS TROMBOFİLİ

26
11/41 kontrol grubunda %26.8 trombofili markırları (+) bulundu.
Increased prevalence of thrombophilia among women with severe ovarian hyperstimulation syndrome Mordechai Dulitzky, M.D.,a Shlomo B. Cohen, M.D.,a Aida Inbal, M.D.,b Daniel S. Seidman, M.D.,a Daniel Soriano, M.D.,a Arieh Lidor, M.D.,a Shlomo Mashiach, M.D.,a and Jaron Rabinovici. Fertil Steril 2002;77:463–7 OI yapılan 20 OHSS gelişen 41 OHSS gelişmeyen Luteal fazda serum alındı: Antithrombin, protein S, protein C, antiphospholipid Ab., faktör V Leiden mutasyonu ve MTHFR 677T polimorfizm. 17/20 OHSS’li hastada %85 11/41 kontrol grubunda %26.8 trombofili markırları (+) bulundu. Çalışma grubunda 1 den fazla kontrol grubunda sadece 1 tane
 bulundu. Çalışma grubunda 1 den fazla kontrol grubunda sadece 1 tane.")
27
Sonuç: OHSS’li olgularda trombofili prevalasnı yüksek olduğundan tarama ve heparin proflaksisi düşünülmelidir. Dulitzky. Severe OHSS and thrombophilia. Fertil Steril 2002;77:463–7 Vaka sayısı az, ve sadece anrikor pozitifliği vardır klinik tanı kriteri tromboz v.s yoktru.

28
Grup III:100 sağlıklı kontrol
Prevalence of thrombophilia in women with severe ovarian hyperstimulation syndrome and cost-effectiveness of screening Francisco Fa´ bregues, Dolors Ta` ssies, Juan C. Reverter, Francisco Carmona, Antonio Ordinas, and Juan Balasch, Fertil Steril 2004;81:989 –95. COH uygulanan Grup I : OHSS (-) Grup II: 40 OHSS (+) Grup III:100 sağlıklı kontrol Bakılan parametreler : APC-R, Protein C, Protein S, Faktör V Leiden mut., AT eksikliği, PM G20210A , LPa, ACL SONUÇ: OHSS ve kontrol grubuplarında antitrombin, protein C, Protein S aPL (-) idi Grup I de : faktör v Leiden ve PM yoktu. PM G20210A Grup II de 1 olguda ( 52.5) Kontrol Grup III’te 2 (%2) The estimated cost of preventing one thrombotic event arising as a consequence of screening for factor V Leiden and prothrombin G20210A mutation is a minimum of $418,970 and $2,430,000, respectively. Trombofili OHSS’li olgularda artmaz, FVL ve PM G20210A bakılması maliyetine değer bulunmadı.
 Grup II: 40 OHSS (+) Grup III:100 sağlıklı kontrol. Bakılan parametreler : APC-R, Protein C, Protein S, Faktör V Leiden mut., AT eksikliği, PM G20210A , LPa, ACL. SONUÇ: OHSS ve kontrol grubuplarında antitrombin, protein C, Protein S aPL (-) idi. Grup I de : faktör v Leiden ve PM yoktu. PM G20210A Grup II de 1 olguda ( 52.5) Kontrol Grup III’te 2 (%2) The estimated cost of preventing one thrombotic event arising as a. consequence of screening for factor V Leiden and prothrombin G20210A mutation is a minimum of $418,970. and $2,430,000, respectively. Trombofili OHSS’li olgularda artmaz, FVL ve PM G20210A bakılması. maliyetine değer bulunmadı.")
29
IVF-ET Başarısızlığı

30
Aetiological factors in implantation failure duringin-vitro fertilization Bolarinde Ola and Tin-Chiu Li. Implantation failure following in-vitro fertilization Curr Opin Obstet Gynecol, 2006; 18:440–445. Maternal age, oocyte and embryo quality Poor ovarian reserve age related chromosomal aneuploidies Parental balanced translocation Polycystic ovary syndrome Immunological factors Antiphospholipid antibodies Autoimmune diseases Abnormal expression of endometrial cytokines and natural killer cells Shared parental human leukocyte antigens Endometrial receptivity Abnormal expression of endometrial oestrogen and progesterone receptors Abnormal expression of endometrial integrins and pinopods Luteal phase defects Uterine, tubal and peritoneal factors Endometrial polyps and submucous fibroids Intramural fibroids Hydrosalpinges Endometriosis Infection Stimulation protocols and culture media

31
IVF-ET Başarısızlığında Trombofili
2001 de Grandone Grup a (n:18): En az 3 IVF-ET başarısız (10) veya fetal kayıp (n. 8) Grup b ( n:24) : IVF başarılı Grup c( n: 224) ;Spontan gebelik Faktör V Leiden ve Fatör IIA Grup a’da 5/18 ( %27) Grup b’ de 0/24 Grup c de 13/224 (%6) (GRANDONE, E., D. COLAIZZO, A. LO BUE et al Inherited thrombophilia andimplantation failure. Fertil. Steril. 77: 201–202) Azem ve arkadaşları, En az bir trombotik faktör pozitifliğini 45 IVF-ET başarısız olguda %44, Spontan gebelikte %18 başarılı IVF grubunda % 20 buldular. (AZEM, F., A. MANY, I. YOVEL et al Increased rates of thrombophilia in woman with repeated IVF failures. Hum. Reprod. 19: 368–370 )
: En az 3 IVF-ET başarısız (10) veya fetal kayıp (n. 8) Grup b ( n:24) : IVF başarılı. Grup c( n: 224) ;Spontan gebelik. Faktör V Leiden ve Fatör IIA. Grup a’da 5/18 ( %27) Grup b’ de 0/24. Grup c de 13/224 (%6) (GRANDONE, E., D. COLAIZZO, A. LO BUE et al Inherited thrombophilia andimplantation failure. Fertil. Steril. 77: 201–202) Azem ve arkadaşları, En az bir trombotik faktör pozitifliğini 45 IVF-ET başarısız olguda %44, Spontan gebelikte %18. başarılı IVF grubunda % 20 buldular. (AZEM, F., A. MANY, I. YOVEL et al Increased rates of thrombophilia in woman with repeated IVF failures. Hum. Reprod. 19: 368–370 )")
32
Multiple thrombophilic gene mutations are risk factors for implantation failure Coulam CB, Jeyendran RS, Fishel LA, Roussev R. Reprod Biomed Online Mar;12(3):322-7 10 adet trombotik Gen mutasyonu 42 IVF-ET başarısızlığı olan 20 fertil kontrol hasta IVF-ET başarısızlığı olan grupta PAI-1 4G/5G mutasyonu daha sık bulundu( P:0.007) Sporadik gen mutasyonları bakımından gruplar arası fark yoktu. Total gen mutasyonları IVF-ET başarısız grupta daha sık bulundu. 3 genden fazla mutasyon IVF-ET başarısız grupta %74 kontrol grubunda %20 bulundu( P:0.0004) . SONUÇ: Kalıtsal trombofililer IVF-ET başarısızlığına eşlik ederler.
 Sporadik gen mutasyonları bakımından gruplar arası fark yoktu. Total gen mutasyonları IVF-ET başarısız grupta daha sık bulundu. 3 genden fazla mutasyon IVF-ET başarısız grupta %74 kontrol grubunda %20 bulundu( P:0.0004) . SONUÇ: Kalıtsal trombofililer IVF-ET başarısızlığına eşlik ederler.")
33
MTHFR C677T polimorfizmi çalışma grubunda yüksek bulundu.
Thrombophilic gene polymorphisms are risk factors for unexplained infertility Carolyn B. Coulam, R. S. Jeyendran Fertil Steril 2008 ( baskıda ) 9 gen polimorfizmi 92 açıklanamayan infertilite 60 fertil ile karşılaştırıldı. MTHFR C677T polimorfizmi çalışma grubunda yüksek bulundu. Bu fark implantasyon başarısızlığını açıklayabilir mi?
 9 gen polimorfizmi. 92 açıklanamayan infertilite. 60 fertil ile karşılaştırıldı. MTHFR C677T polimorfizmi çalışma grubunda yüksek bulundu. Bu fark implantasyon başarısızlığını açıklayabilir mi")
34
Grup A ( Çalışma n:90) 23-44 yaş(31)en az 3 başarısız IVF
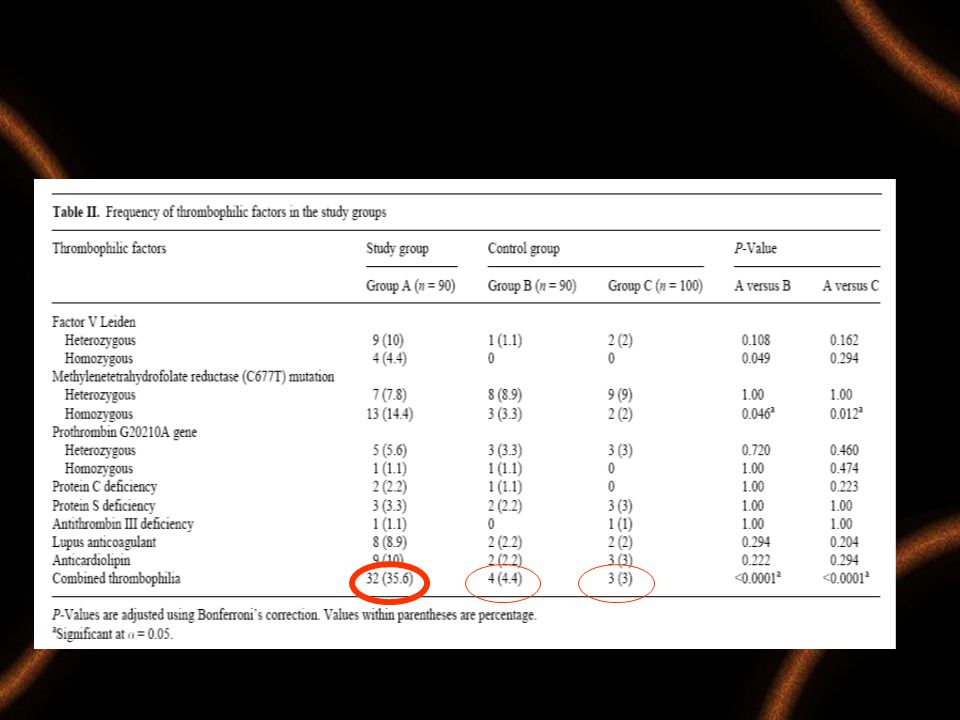
Acquired and inherited thrombophilia: implication in recurrent IVF and embryo transfer failure Hussein S.Qublan, Suhair S.Eid, Hani A.Ababneh, Zouhair O.Amarin, Aiman Z.Smadi,Farakaid F.Al-Khafaji5 and Yousef S.Khader. Human Reproduction 2006( 21) 10: 2694–2698 Grup A ( Çalışma n:90) yaş(31)en az 3 başarısız IVF Grup B(n:90 ) (30) İlk IVF başarılı Grup C (n:100) (30) Spontan gebelik Her üç grupta:FVL, PM, MTHFR, Protein S, C, ATIII eksikliği ve edinsel LA and ACL bakıldı. En az bir herediter veya edinsel trombolik faktör Grup A ‘da %68.9 (62/90) Grup B’de %25.6 ( 23/90) Grup C‘ de %25 ( 25/100) Fark istatsitiksel anlamlı bulundu. (P < 0.01). study (group A). Women’s age ranged from 23 to 44 years (mean ± SD, 31 ± 4.2). Two control groups were enrolled: group B (n = 90) included women who have had successful pregnancy after their first IVF–embryo transfer cycle. Their ages ranged from 22 to 40 years (mean ± SD, 30 ± 3.1). The second group (group C) consisted of 100 women who had conceived spontaneously with at least one uneventful pregnancy and no previous history of miscarriages. Women’s age in this group ranged from 17 to 41 years (mean ± SD, 30 ± 2.8). Women with endometriosis, hydrosalpinx, abnormal uterine cavity on the hysterosalpingogram and history of thromboembolic disease and those who were receiving hormonal treatment were not included in the study group. All women were investigated for the presence of inherited (FVL mutation, prothrombin mutation, MTHFR mutation and deficiencies in proteins S and C and ATIII) or acquired (LA and ACL) thrombophilic factors. In the IVF–embryo transfer cycles, only cycles in which grade 1 and 2 embryos were transferred were included in the study group. Indications for IVF treatment included anovulation, unexplained infertility and male and tubal factor Sonuç, trombofilinin IVF-ET başarısızlığında rolü vardır. Bu olgularda trombofili taraması yapılmalıdır.
 10: 2694–2698. Grup A ( Çalışma n:90) yaş(31)en az 3 başarısız IVF. Grup B(n:90 ) (30) İlk IVF başarılı. Grup C (n:100) (30) Spontan gebelik. Her üç grupta:FVL, PM, MTHFR, Protein S, C, ATIII eksikliği ve edinsel LA and ACL bakıldı. En az bir herediter veya edinsel trombolik faktör. Grup A ‘da %68.9 (62/90) Grup B’de %25.6 ( 23/90) Grup C‘ de %25 ( 25/100) Fark istatsitiksel anlamlı bulundu. (P < 0.01). study (group A). Women’s age ranged from 23 to 44 years (mean ± SD, 31 ± 4.2). Two control groups were enrolled: group B (n = 90) included women who have had successful pregnancy after their first. IVF–embryo transfer cycle. Their ages ranged from 22 to 40 years. (mean ± SD, 30 ± 3.1). The second group (group C) consisted of 100. women who had conceived spontaneously with at least one uneventful. pregnancy and no previous history of miscarriages. Women’s age in. this group ranged from 17 to 41 years (mean ± SD, 30 ± 2.8). Women. with endometriosis, hydrosalpinx, abnormal uterine cavity on the hysterosalpingogram. and history of thromboembolic disease and those. who were receiving hormonal treatment were not included in the. study group. All women were investigated for the presence of inherited. (FVL mutation, prothrombin mutation, MTHFR mutation and. deficiencies in proteins S and C and ATIII) or acquired (LA and ACL) thrombophilic factors. In the IVF–embryo transfer cycles, only cycles. in which grade 1 and 2 embryos were transferred were included in the. study group. Indications for IVF treatment included anovulation, unexplained infertility and male and tubal factor. Sonuç, trombofilinin IVF-ET başarısızlığında rolü vardır. Bu olgularda trombofili taraması yapılmalıdır.")
36
Grup I: 51 ≥ 3 başarısız IVF-ET denemesi
Repeated in vitro Fertilization Failure and Its Relation with Thrombophilia Aynur Simur, Suna Özdemir, Hasan Acar, M. Cengiz Çolakoğlu, Hüseyin Görkemli, Osman Balcı, Süleyman Nergis Gynecol Obstet Invest 2009;67:109–112 Grup I: 51 ≥ 3 başarısız IVF-ET denemesi Kontrol grubu: 50 Spontan başarılı gebelik Tüm olgularda; FVL, PM (G20210A) ve MTHFR(C677T)mutasyonu bakıldı. Sonuçlar: Her iki grupta trombofili faktörleri pozitifliği yanı sıklıkta bulundu. En az bir trombofilik faktör çalışma grubunda %62.7 kontrol grubunda %53.9 (+) bulundu. Aradaki fark istatiski anlamlı bulunmadı. Bu çalışmaya göre FVL, PM (G20210A) ve MTHFR(C677T)mutasyonunun IVF-ET başarısızlığına etkisi yoktur.
 ve MTHFR(C677T)mutasyonu bakıldı. Sonuçlar: Her iki grupta trombofili faktörleri pozitifliği yanı sıklıkta bulundu. En az bir trombofilik faktör çalışma grubunda %62.7 kontrol grubunda %53.9 (+) bulundu. Aradaki fark istatiski anlamlı bulunmadı. Bu çalışmaya göre FVL, PM (G20210A) ve MTHFR(C677T)mutasyonunun. IVF-ET başarısızlığına etkisi yoktur.")
37
Summary of the prevalence of inherited thrombophiliain the groups
Simur et al. Gynecol Obstet Invest 2009;67:109–112

38
GOPEL, W. , M. LUDWIG, A. K. JUNGE et al
GOPEL, W., M. LUDWIG, A.K. JUNGE et al. . Selection pressure for the Factor-VLeiden mutation and embryo implantation. Lancet 2001(358): 1238–1239.
: 1238–1239.")
39
Homstein MD, Davis OK, Massey JB, et al Antiphospholipid antibodies and in vitro fertilization success: a metaanalysis. Fertil Steril 2000; 73:330–3 7 çalışmada, en az 1 anormal aPL testi olan 703/2000 kadında IVF başarısızlığı ve aPL antikorları arasında ilişki saptanmamıştır.

40
Haematologica 2003;88:

41
Screening of thrombophilia in women with failure of embryo implantation: far from being recommended I. Martinelli, T. Battaglioli, P.M. Mannucci A. Bianchi Bonomi Hemophilia and Thrombosis Center, IRCCS Maggiore Hospital, University of Milan, Italy Haematologica 2007; 88:(12)e172 Faktör V Leiden mutasyonu ve Protrombin gen ( G20210A9) embryo implantasyonuna etkisi tartışmalıdır. Bu konuda az sayıda çalışma vardır . Bir yanda FV Leiden mutasyonunda ilk ET de implantasyon şansını arttırdığı iddia edilirken On one hand, it has been suggested that carriers of factor V Leiden have a selective advantage in embryo implantation, occurring more frequently at the first attempt than in non-carriers.1 On the other hand, these data were not confirmed by others 2 and Grandone and colleagues found not only the lack of such a selective advantage, but a possible association between thrombophilia and failure of 3 or more attempts of embryo transfer.3 In our study,4 when women were stratified according to the number of embryo transfers attempted, we found a similar frequency of thrombophilia markers in any group. Given the paucity of data and the uncertainties on the relationship between embryo implantation after assisted reproductive procedures and thrombophilia, we believe that suggesting a routine screening for thrombophilia in infertile women is at present unjustified, even in women with 3 or more implantation failures. More studies of adequate sample size are needed to elucidate the causes of failure of embryo implantation and the role of thrombophilia References 1. Gopel W, Ludwig M, Junge AK, Kohlmann T, Diedrich K, Moller J. Selection pressure for the factor V Leiden mutation and embryo implantation. Lancet 2001;358:1238-9 2. Juul K, Tybjaerg-Hansen A. Factor V Leiden: relation to fertility? Lancet 2001;359:894 3. Grandone E, Colaizzo D, Lo Bue A, Checola MG, Cittadini E, Margaglione M. Inherited thrombophilia and in vitro fertilization implantation failure. Fertil Steril 2001:76:201-2 4. Martinelli I, Taioli E, Ragni G, Levi-Setti P, Passamonti SM, Battaglioli T, Lodigiani C, Mannucci PM. Embryo implantation after assisted reproductive procedures and maternal thrombophilia. Haematologica 2003;88:789-93 The association was statistically significant for Factor V Leiden, prothrombin mutation, and activated protein C resistance. Methylenetetrahydrofolate mutation and protein C and antithrombin deficiencies were not significantly associated with fetal loss.59 59. REY, E., S.R. KAHN et al Thrombophilic disorders and fetal loss: a meta-analysis. Lancet 361: 901–908
 embryo implantasyonuna etkisi tartışmalıdır. Bu konuda az sayıda çalışma vardır . Bir yanda FV Leiden mutasyonunda ilk ET de implantasyon şansını arttırdığı iddia edilirken. On one hand, it has been suggested that carriers of factor V Leiden have a selective advantage in embryo implantation, occurring more frequently at the first attempt than in non-carriers.1. On the other hand, these data were not confirmed by others 2 and Grandone and colleagues found not only the lack of such a selective advantage, but a possible association between thrombophilia and failure of 3 or more attempts of embryo transfer.3. In our study,4 when women were stratified according to the number of embryo transfers attempted, we found a similar frequency of thrombophilia markers in any group. Given the paucity of data and the uncertainties on the relationship between. embryo implantation after assisted reproductive procedures and thrombophilia, we believe that suggesting a routine screening for thrombophilia in infertile women is at present unjustified, even in women with 3 or more implantation failures. More studies of adequate sample size are needed to elucidate the causes of failure of. embryo implantation and the role of thrombophilia. References. 1. Gopel W, Ludwig M, Junge AK, Kohlmann T, Diedrich K, Moller J. Selection pressure for the factor V Leiden mutation. and embryo implantation. Lancet 2001;358: Juul K, Tybjaerg-Hansen A. Factor V Leiden: relation to fertility Lancet 2001;359: Grandone E, Colaizzo D, Lo Bue A, Checola MG, Cittadini E, Margaglione M. Inherited thrombophilia and in vitro fertilization. implantation failure. Fertil Steril 2001:76: Martinelli I, Taioli E, Ragni G, Levi-Setti P, Passamonti SM, Battaglioli T, Lodigiani C, Mannucci PM. Embryo implantation. after assisted reproductive procedures and maternal. thrombophilia. Haematologica 2003;88: The association was statistically significant. for Factor V Leiden, prothrombin mutation, and activated protein C resistance. Methylenetetrahydrofolate mutation and protein C and antithrombin deficiencies. were not significantly associated with fetal loss REY, E., S.R. KAHN et al Thrombophilic disorders and fetal loss: a meta-analysis. Lancet 361: 901–908.")
42
Tedavi/Proflaksi Çalışmaları

43
Prednisolone plus low-dose aspirin improves the implantation rate in women with autoimmune conditions who are undergoing in vitro fertilization Isao Hasegawa, Yasuaki Yamanoto, Mina Suzuki, Haruo Murakawa, Takumi Kurabayashi, Koichi Takakuwa,and Kenichi Tanaka, Fertil Steril 1998;70:1044–8 Objective: To evaluate the effect of prednisolone plus low-dose aspirin (PSL/LDA) in women with autoimmune conditions who were enrolled in an IVF-ET program. Design: A retrospective clinical study. Setting: In vitro fertilization unit, Niigata University Hospital, Niigata, Japan. Patient(s): 307 women who underwent IVF-ET between Jan and Dec Intervention(s): Prednisolone (10 mg/d) and aspirin (81 mg/d) were administered to the women with autoantibodies who chose to participate. Main Outcome Measure(s): Pregnancy and implantation rates with IVF-ET. Result(s): Women undergoing IVF who had positive ANA, with or without aPL, had significantly lower pregnancy and implantation rates than did women without autoantibodies (14.8% versus 21.7% and 6.8% versus 10.4%, respectively). The administration of PSL/LDA to women with antinuclear antibodies significantly improved the outcome of IVF-ET (40.6% pregnancy rate and 20.3% implantation rate). Conclusion(s): A high proportion of women who are undergoing IVF-ET have autoantibodies, which areassociated with poor IVF outcomes. The administration of PSL/LDA to these women may improve their implantation rate.
 in women with autoimmune conditions who were enrolled in an IVF-ET program. Design: A retrospective clinical study. Setting: In vitro fertilization unit, Niigata University Hospital, Niigata, Japan. Patient(s): 307 women who underwent IVF-ET between Jan and Dec Intervention(s): Prednisolone (10 mg/d) and aspirin (81 mg/d) were administered to the women with autoantibodies who chose to participate. Main Outcome Measure(s): Pregnancy and implantation rates with IVF-ET. Result(s): Women undergoing IVF who had positive ANA, with or without aPL, had significantly lower pregnancy and implantation rates than did women without autoantibodies (14.8% versus 21.7% and 6.8% versus 10.4%, respectively). The administration of PSL/LDA to women with. antinuclear antibodies significantly improved the outcome of IVF-ET (40.6% pregnancy rate and 20.3% implantation rate). Conclusion(s): A high proportion of women who are undergoing IVF-ET have autoantibodies, which areassociated with poor IVF outcomes. The administration of PSL/LDA to these women may improve their implantation rate.")
44
Recurrent Pregnancy Loss With Antiphospholipid Antibody: A Systematic Review of Therapeutic Trials Marianne Empson, MBChB, M Marissa Lassere, Jonathan C. Craig, MBChB, James R. ScottObstet Gynecol 2002;99:135– 44 Kaynak: Cochrane Controlled Trials Register, Cochrane Collaboration Pregnancy and Childbirth Group’s Specialized Register of Controlled Trials, EMBASE, and MEDLINE were searched in December ( ) Quantitative analysis of summary data was performed using the fixed- and randomeffects models with heterogeneity assessments. Pregnancy loss and adverse neonatal outcomes were the main outcome measures. Ten trials (n 627) fulfilled the inclusion criteria (of which four lacked adequate allocation concealment). Three trials of aspirin alone showed no significant reduction in pregnancy loss (relative risk [RR] 1.05, 95% confidence interval [CI] 0.66, 1.68). Heparin combined with aspirin (two trials, 140 patients) significantly reduced pregnancy loss compared with aspirin alone (RR 0.46, 95% CI 0.29, 0.71). Prednisone and aspirin resulted in a significant increase in prematurity (RR 4.83, 95% CI 2.85, 8.21) but no significant reduction in pregnancy loss (RR 0.85, 95% CI 0.53, 1.36).
 Quantitative analysis of summary data was performed using the fixed- and randomeffects models with heterogeneity assessments. Pregnancy loss and adverse neonatal outcomes were the main outcome measures. Ten trials (n 627) fulfilled the inclusion criteria (of which four lacked adequate allocation concealment). Three trials of aspirin alone showed no significant reduction in pregnancy loss (relative risk [RR] 1.05, 95% confidence interval [CI] 0.66, 1.68). Heparin combined with aspirin (two trials, 140 patients) significantly reduced pregnancy loss compared with aspirin alone (RR 0.46, 95% CI 0.29, 0.71). Prednisone and aspirin resulted in a significant increase in prematurity (RR 4.83, 95% CI 2.85, 8.21) but no significant reduction in pregnancy loss (RR 0.85, 95% CI 0.53, 1.36).")
45
SİSTEMATİK DEĞERLENDİRMEYE UYGUN ÇALIŞMALAR
SİSTEMATİK DEĞERLENDİRMEYE UYGUN ÇALIŞMALAR ??? Schema of literature search results. Empson. Antiphospholipid Antibodies. Obstet Gynecol 2002

46
Aspirin or anticoagulants for the treatment of recurrent miscarriage in women without antiphospholipid syndrome (Review) Di Nisio M, Peters LW, Middeldorp S The Cochrane Library 2008;4: 1-15 Two studies (242 participants) were included in the review and for both of them data were extracted for the subgroups of women fulfilling the inclusion criteria of the review. In one study, 54 pregnant women with recurrent spontaneous abortion without detectable anticardiolipin antibodies were randomised to low-dose aspirin or placebo. Similar live-birth rates were observed with aspirin and placebo (relative risk (RR) 1.00, 95% confidence interval (CI) 0.78 to 1.29). In another study, a subgroup of 20 women who had had a previous fetal loss after the 20th week and had a thrombophilic defect were randomised to enoxaparin or aspirin. Enoxaparin treatment resulted in an increased live-birth rate, as compared to low-dose aspirin, RR 10.00, 95% CI 1.56 to 64.20). Authors’ conclusions: The evidence on the efficacy and safety of thromboprophylaxis with aspirin and heparin in women with a history of at least two spontaneous miscarriages or one later intrauterine fetal death without apparent causes other than inherited thrombophilias is too limited to recommend the use of anticoagulants in this setting. Large, randomised, placebo-controlled trials are urgently needed. The effect of anticoagulant treatment on the live-birth rate in women with a history of at least two spontaneous miscarriages or one later intrauterine fetal death without apparent causes other than inherited thrombophilias were eligible. Interventions included aspirin, unfractionated heparin, and low molecular weight heparin for the prevention of birth loss. One treatment could be compared with another or with placebo.
 were included in the review and for both of them data were extracted for the subgroups of women fulfilling the inclusion criteria of the review. In one study, 54 pregnant women with recurrent spontaneous abortion without detectable anticardiolipin antibodies were randomised to low-dose aspirin or placebo. Similar live-birth rates were observed with aspirin and placebo (relative risk (RR) 1.00, 95% confidence interval (CI) 0.78 to 1.29). In another study, a subgroup of 20 women who had had a previous fetal loss after the 20th week and had a thrombophilic defect were randomised to enoxaparin or aspirin. Enoxaparin treatment resulted in an increased live-birth rate, as compared to low-dose aspirin, RR 10.00, 95% CI 1.56 to 64.20). Authors’ conclusions: The evidence on the efficacy and safety of thromboprophylaxis with aspirin and heparin in women with a history of at least two spontaneous miscarriages or one later intrauterine fetal death without apparent causes other than inherited thrombophilias is too limited to recommend the use of anticoagulants in this setting. Large, randomised, placebo-controlled trials are urgently needed. The effect of anticoagulant treatment on the live-birth rate in women with a history of at least two spontaneous miscarriages or one later intrauterine fetal death without apparent causes other than inherited thrombophilias were eligible. Interventions included aspirin, unfractionated heparin, and low molecular weight heparin for. the prevention of birth loss. One treatment could be compared with another or with placebo.")
47
A randomized, double-blind, placebo controlledtrial of heparin and aspirin for women with in vitro fertilization implantation failure and antiphospholipid or antinuclear antibodies Catharyn Stern, Lawrence Chamley, Helen Norris, Lyndon Hale and Gordon Baker Fertil Steril 2003(80):376–83 Design: A double-blind, randomized, transfer-by-transfer of fresh or cryopreserved embryos, crossover trial. Patient(s): Women seropositive for at least one antiphospholipid (APA), antinuclear (ANA), or 2 glycoprotein I autoantibody and 10 embryos transferred without achieving pregnancy (n 143). Intervention(s): Subcutaneous unfractionated heparin (5,000 IU b.i.d.) and aspirin (100 mg daily) (158 transfers of 296 embryos) or placebo (142 transfers of 259 embryos) from the day of embryo transfer. Main Outcome Measure(s): Fetal heart per embryo transferred (implantation rate).
: Women seropositive for at least one antiphospholipid (APA), antinuclear (ANA), or 2 glycoprotein I autoantibody and 10 embryos transferred without achieving pregnancy (n 143). Intervention(s): Subcutaneous unfractionated heparin (5,000 IU b.i.d.) and aspirin (100 mg daily) (158 transfers of 296 embryos) or placebo (142 transfers of 259 embryos) from the day of embryo transfer. Main Outcome Measure(s): Fetal heart per embryo transferred (implantation rate).")
48
Result(s): There was no significant difference in pregnancy rates or implantation
rates between treated and placebo cycles; for example, fetal hearts per embryo transferred implantation rates were 6.8% (20/296) and 8.5% (22/259), respectively. The implantation rate for seropositive trial participants (42/555, 7.6%) compared favorably with that for IVF implantation-failure patients continuing treatment outside the trial (147/3237, 4.5%). Conclusion(s): Heparin and aspirin did not improve pregnancy or implantation rates for APA-positive or ANA-positive patients with IVF implantation failure.
 and 8.5% (22/259), respectively. The implantation rate for seropositive trial participants (42/555, 7.6%) compared. favorably with that for IVF implantation-failure patients continuing treatment outside the trial (147/3237, 4.5%). Conclusion(s): Heparin and aspirin did not improve pregnancy or implantation rates for APA-positive or ANA-positive patients with IVF implantation failure.")
49
TARAMA

50
Screening for thrombophiliain high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study O Wu, L Robertson, S Twaddle, GDO Lowe, P Clark, M Greaves, ID Walker, P Langhorne, I Brenkel, L Regan, IA Greer. Health Technology Assessment 2006; Vol. 10: No. 11 201 oral estrogen ile, 234 gebelik, 49 ortopedik cerrahi Bunlardan 81‘i değerlendirmeye alındı ( 9’u OKS, 72 Gebelik ve Ortopedik cerrahi) Universal thrombophilia screening in women prior to prescribing oral oestrogen preparations, in women during pregnancy and in patients undergoing major orthopaedic surgery is not supported by the evidence. The findings from this study show that selective screening based on prior VTE history is more cost-effective than universal screening. Gebelik komplikasyonları ile ilişkisi kesin olmasına rağmen rutin tarama önerilmiyor bu nedenle başarısız YÜT’de tarama ??
 Universal thrombophilia screening in women prior to prescribing oral oestrogen preparations, in women during pregnancy and in patients undergoing major orthopaedic surgery is not supported by the evidence. The findings from this study show that selective screening based on prior VTE history is more cost-effective than universal screening. Gebelik komplikasyonları ile ilişkisi kesin olmasına rağmen rutin tarama önerilmiyor bu nedenle başarısız YÜT’de tarama")
51
Ne Zaman Tarama I Koagülasyon faktörleri ve antikoagulan seviyeleri VTE ve gebelikte değişir Biyokimyasal değerlendirme tedavi sonuna kadar beklemeli PCR(Factor V-Factor II) her zaman yapılabilir LA ve ACA VTE’de değişmez 12 hf. Sonra tekrarlanmalı VTE sırasında antitrombin seviyelerine bakılabilir Pıhtılaşma testleri(Protein S ve Faktor VIII) VTE, gebelik,OAK sırasında yapılmaz Gebelikten 3 ay, OAK’dan 1 ay sonra
 her zaman yapılabilir. LA ve ACA VTE’de değişmez 12 hf. Sonra tekrarlanmalı. VTE sırasında antitrombin seviyelerine bakılabilir. Pıhtılaşma testleri(Protein S ve Faktor VIII) VTE, gebelik,OAK sırasında yapılmaz. Gebelikten 3 ay, OAK’dan 1 ay sonra.")
52
ACOG I Tekrarlayan gebelik kaybı, erken-ağır preeklampsia, ağır açıklanamayan IUGG AFS taranmalı Profilaktik antikoagülan tedavi gebelik sonuçlarını iyileştirir

53
ACOG II Protein C,S, AT III, FVL, PT ve MTHFR mutasyonları ağır-erken preeklampsi, açıklanamayan fetal kayıp, ölü doğum, dekolmanla ilgili Antikoagülan tedavinin gebelik sonuçlarını iyileştirdiği yönünde randomize kontrollü çalışma yok Tarama?

54
Hangi Testler Öncelikli tetsler Lupus antikoagülanı
Factor V leiden Factor II Homosistein artışı Factor VIII artışı Lupus antikoagülanı Orta Öncelikli Testler Protein C aktivitesi Protein S Azalmış antitrombin aktivitesi ACA Diğer Testler Disfibrinojenemi Artmış fibrinojen Factor IX ve XI artışı MTHFR

55
Baha M. Sibai Hypertension 2005;46;1252-1253
Thrombophilia and Severe Preeclampsia Time to Screen and Treat in Future Pregnancies? Baha M. Sibai Hypertension 2005;46;

56
Practical management considerations after repeated in-vitro fertilization failures Bolarinde Ola and Tin-Chiu Li. Implantation failure following in-vitro fertilization Curr Opin Obstet Gynecol, 2006; 18:440–445. Interventions of proven benefits Unilateral or bilateral salpingectomies for ultrasound detectable hydrosalpinx or hydrosalpinges Metformin treatment in patients with PCOSEgg or embryo donation in older women Interventions with possible benefits Preimplantation aneuploidy screening and blastocyst transfer for women below the age of 41 years Blastocyst culture without preimplantation aneuploidy screening Intramural myomectomy (even if fibroid is less than 5cm in average diameter) Surgical treatment of minimal/mild endometriosis, Routine diagnostic hysteroscopy after repeated IVF failure Hysteroscopic polypectomy- Hysteroscopic submucous myomectomy - Hysteroscopic adhesiolysis of uterine synechiae Interventions that are yet unproven Heparin and/or aspirin therapy, Steroid therapy, Intravenous immunotherapy Assisted hatching
 Surgical treatment of minimal/mild endometriosis, Routine diagnostic hysteroscopy after repeated IVF failure. Hysteroscopic polypectomy- Hysteroscopic submucous myomectomy - Hysteroscopic adhesiolysis of. uterine synechiae. Interventions that are. yet unproven. Heparin and/or aspirin therapy, Steroid therapy, Intravenous immunotherapy. Assisted hatching.")
57
APA Patofizyolojisi

58
APA Patofizyolojisi Damar tıkanıklığı Plasental infarkt
Endotelial hücre anormallikleri Platelet etkilenimi Antiplatelet aktivite Monositler aracılığı ile pro-koagulan aktivitenin uyarılması Protein C Aktivasyonunun inhibisyonu Plasental fonksiyonun değişmesi Plasental Perfüzyonun Bozulması Antiphospholipid antibodies and reproduction.William H. Kutteh. Journal of Reproductive Immunology 1997 (35) :
 :")
59
2. Reduction of antiphospholipid antibodies binding
Heparin treatment in pregnancy loss:Potential therapeutic benefits beyond anticoagulation Guillermina Girardi Journal of Reproductive Immunology 2005(66):45–51 1. Anticoagulation 2. Reduction of antiphospholipid antibodies binding 3. Antiinflammatory effects 4. Heparin facilitates implantation 5. Heparin as a complement inhibitor 2. Reduction of antiphospholipid antibodies binding: Wagenknecht and McIntyre (1992) suggested there is a direct binding of heparin to antiphospholipid antibodies, and using an ELISA, showed a decrease in antiphospholipid antibody activity with increasing doses of heparin, though the doses used in these studies are several times higher than the therapeutic doses used in women 3. Antiinflammatory effects: Deciduas from women with both APS and antiphospholipid-like syndromes showed more necrosis, acute and chronic inflammation, and vascular thrombosis compared to those of women with normal pregnancies (Van Horn et al., 2004). Heparin preparations affect inflammatory cell behavior and have promising therapeutic, anti-inflammatory properties by preventing leukocyte adhesion/influx and tissue damage in kidney (Rops et al., 2004). Heparin also has effects on the attachment of leukocytes to activated endothelium, as well as the adhesion reaction of tumors during malignancy. These actions may be due to blockade of interactions with adhesion molecules such as selectins (Borsig, 2004). Wagenknecht, D.R., McIntyre, J.A., Interaction of heparin with B2-glycoprotein I and antiphospholipid antibodies in vitro. Thromb. Res. 68, 495–500. Van Horn, J.T., Craven, C., Ward, K., Branch, D.W., Silver, R.M., Histologic features of placentas and abortion specimens from women with antiphospholipid and antiphospholipid-like syndromes. Placenta 25, 642–648. Rops, A.L., van der Vlag, J., Lensen, J.F., Wijnhoven, T.J., van den Heuvel, L.P., van Kuppevelt, T.H., Berden, J.H., Heparan sulfate proteoglycans in glomerular inflammation. Kidney Int. 65, 768–785 Borsig, L., Selectins facilitate carcinoma metastasis and heparin can prevent them. News Physiol. Sci. 19, 16–21. 4. Heparin facilitates implantation: Di Simone et al. (1999) suggested that IgG from women with APS cause pregnancy loss by binding to phospholipids expressed on the invading trophoblast, thereby inhibiting placental development and, as a consequence, embryonic implantation in early pregnancy. In this study, heparin caused a significant increase in in vitro trophoblast invasiveness and differentiation. Similarly, LMWH restored in vitro placental invasiveness and differentiation in trophoblasts incubated with antiphospholipid antibodies in a dose-dependent fashion (Di Simone et al., 1997). Heparin also has been shown to increase cellular motility in a first trimester extravillous trophoblast cell line (Lash et al., 2003). Others suggest that heparin is directly or indirectly, e.g. via heparan sulfate proteoglycans or heparin-binding EGF involved in the adhesion of the blastocyst to the endometrial epithelium and the subsequent invasion (Fiedler andWurfel, 2004). A heparin-binding epidermal growth factor-like (HB-EGF) is a critical signaling molecule in blastocyst-uterine crosstalk in implantation (Hamatani et al., 2004), and developing extravillous trophoblasts accumulate HB-EGF. HB-EGF is downregulated in placentae of women with preeclampsia, a disorder associated with deficient trophoblast invasion, raising important questions about its physiological impact on cytotrophoblasts. Addition of HB-EGF during explants culture of first-trimester chorionic villi enhances extravillous trophoblast differentiation and invasive activity (Leach et al., 2004) Di Simone, N., Ferrazzani, S., Castellani, R., De Carolis, S., Mancuso, S., Caruso, A., Heparin and low-dose aspirin restore placental human chorionic gonadatrophin secretion abolished by antiphospholipid antibodycontaining sera. Hum. Reprod. 12, 2061–2065. Di Simone, N., Caliandro, D., Castellani, R., Ferrazzani, S., De Carolis, S., Caruso, A., Low-molecular weight heparin restores in-vitro trophoblast invasiveness and differentiation in presence of immunoglobulin G fractions obtained from patients with antiphospholipid syndrome. Hum. Reprod. 14, 489–495. Lash, G.E.,Warren, A.Y., Underwood, S., Baker, P.N., 2003.Vascular endothelial growth factor is a chemoattractant for trophoblast cells. Placenta 24, 549–556. Fiedler, K., Wurfel, W., Effectivity of heparin in assisted reproduction. Eur. J. Med. Res. 9, 207–214. Hamatani, T., Daikoku, T., Wang, H., Matsumoto, H., Carter, M.G., Ko, M.S., Dey, S.K., Global gene expression analysis identifies molecular pathways distinguishing blastocyst dormancy and activation. Proc. Natl. Acad. Sci. USA 101, 10326–10331. Leach, R.E., Kilburn, B., Wang, J., Liu, Z., Romero, R., Armant, D.R., Heparin-binding EGF-like growth factor regulates human extravillous cytotrophoblast development during conversion to the invasive phenotype. Dev. Biol. 266, 223–237. 5. Heparin as a complement inhibitor: The complement system consists of more than 30 proteins in plasma and on cell surfaces that protect the host against invading organisms, initiates inflammation and tissue injury (reviewed in Walport, 2001) There are three pathways of complement activation: the classical, mannose-binding lectin and alternative pathways. Studies performed over a decade ago found evidence of complement activation in pregnant patients with SLE (Lockshin et al., 1986), and certain patterns of complement activation are associated with either a flare of disease or preeclampsia (Buyon et al., 1992). Elevated levels of complement activation fragments have been detected in patients with other manifestations of antiphospholipid antibodies-associated disease such as stroke and TIA (Davis and Brey, 1992). Walport, M.J., Complement. First of two parts. N. Engl. J. Med. 344, 1058–1066 Lockshin, M.D., Qamar, T., Redecha, P., Harpel, P.C., Hypocomplementemia with low C1s–C1r inhibitor complex in systemic lupus erythematosus. Arthritis Rheum. 29, 1467–1472. Buyon, J.P., Tamerius, J., Ordorica, S., Young, B., Abramson, S.B., Activation of the alternative complement pathway accompanies disease flares in systemic lupus erythematosus during pregnancy. Arthritis Rheum. 35, 55–61 Davis, W.D., Brey, R.L., Antiphospholipid antibodies and complement activation in patients with cerebral ischemia. Clin. Exp. Immunol. 10, 455–460. The complement system consists of more than 30 proteins in plasma and on cell surfaces that protect the host against invading organisms, initiates inflammation and tissue injury (reviewed in Walport, 2001) There are three pathways of complement activation: the classical, mannose-binding lectin We now know G. Girardi / Journal of Reproductive Immunology 66 (2005) 45–51 49 from our experiments performed in a mouse model of APS that activation of the complement cascade is absolutely required to induce pregnancy loss and thrombosis (Girardi et al., 2004, 2003). We demonstrated that complement activation is a central mechanism of antiphospholipid antibody-induced pregnancy loss in a mouse model, in which pregnant mice receive human IgG containing antiphospholipid antibodies or monoclonal antiphospholipid antibodies. Using different approaches to block complement activation (mice lacking complement components or their receptors, complement inhibitors, etc.) we were able to protect the mice from antiphospholipid antibody-induced pregnancy loss. Complement component C5 and particularly its cleavage product C5a, and neutrophils are key mediators of fetal injury and show that treatments with antibodies or peptides that block C5a–C5a receptor interactions prevent pregnancy complications in our mouse model. Interestingly, heparin, the standard anticoagulant treatment used to prevent obstetric complications in patients with APS (Derksen et al., 2004) was shown to have “anti-complementary effects” as early as 1929 (Ecker and Gross, 1929). Subsequent studies identified several possible mechanisms by which heparin can inhibit complement activation at various points in the classical, alternative and terminal pathways (Loos et al., 1976; Rent et al., 1976;Weiler et al., 1978; Kazatchkine et al., 1981; Edens et al., 1994; Ninomiya et al., 2000 Girardi, G., Berman, J., Redecha, P., Spruce, L., Thurman, J.M., Kraus, D., Hollmann, T.J., Casali, P., Caroll, M.C., Wetsel, R.A., Lambris, J.D., Holers, V.M., Salmon, J.E., Complement C5a receptors and neutrophils mediate fetal injury in the antiphospholipid syndrome. J. Clin. Invest. 112, 1644–1654. Derksen, R.H., Khamashta, M.A., Branch, D.W., Management of the obstetric antiphospholipid syndrome. Arthritis Rheum. 50, 1028–1039 Ecker, E., Gross, P., Anticomplementary power of heparin. J. Infect. Dis. 44, 250–257. Loos, M., Volanakis, J.E., Stroud, R.M., Mode of interaction of different polyanions with the first (C1, C1), the second (C2) and the fourth (C4) component of complement–III. Inhibition of C4 and C2 binding site(s) on C1s by polyanions. Immunochemistry 13, 789–791. Rent, R., Myhrman, R., Fiedel, B.A., Gewurz, H., Potentiation of C1-esterase inhibitor activity by heparin. Clin. Exp. Immunol. 23, 264–271. Weiler, J.M., Yurt, R.W., Fearon, D.T., Austen, K.F., Modulation of the formation of the amplification convertase of complement, C3b, Bb, by native and commercial heparin. J. Exp. Med. 147, 409–421. Kazatchkine, M.D., Fearon, D.T., Metcalfe, D.D., Rosenberg, R.D., Austen, K.F., Structural determinants of the capacity of heparin to inhibit the formation of the human amplification C3 convertase. J. Clin. Invest. 67, 223–228 Edens, R.E., Linhardt, R.J., Bell, C.S., Weiler, J.M., Heparin and derivatized heparin inhibit zymosan and cobra venom factor activation of complement in serum. Immunopharmacology 27, 145–153. Ninomiya, H., Kawashima, Y., Nagasawa, T., Inhibition of complement-mediated haemolysis in paroxysmal nocturnal haemoglobinuria by heparin or low-molecular weight heparin. Br. J. Haematol. 109, 875–881.
:45– Anticoagulation. 2. Reduction of antiphospholipid antibodies binding. 3. Antiinflammatory effects. 4. Heparin facilitates implantation. 5. Heparin as a complement inhibitor. 2. Reduction of antiphospholipid antibodies binding: Wagenknecht and McIntyre (1992) suggested there is a direct binding of heparin to antiphospholipid. antibodies, and using an ELISA, showed a decrease in antiphospholipid antibody activity. with increasing doses of heparin, though the doses used in these studies are several times. higher than the therapeutic doses used in women. 3. Antiinflammatory effects: Deciduas from women with both APS and antiphospholipid-like syndromes showed. more necrosis, acute and chronic inflammation, and vascular thrombosis compared to those. of women with normal pregnancies (Van Horn et al., 2004). Heparin preparations affect inflammatory. cell behavior and have promising therapeutic, anti-inflammatory properties by preventing. leukocyte adhesion/influx and tissue damage in kidney (Rops et al., 2004). Heparin also has. effects on the attachment of leukocytes to activated endothelium, as well as the adhesion. reaction of tumors during malignancy. These actions may be due to blockade of interactions. with adhesion molecules such as selectins (Borsig, 2004). Wagenknecht, D.R., McIntyre, J.A., Interaction of heparin with B2-glycoprotein I and antiphospholipid antibodies in vitro. Thromb. Res. 68, 495–500. Van Horn, J.T., Craven, C., Ward, K., Branch, D.W., Silver, R.M., Histologic features of placentas and. abortion specimens from women with antiphospholipid and antiphospholipid-like syndromes. Placenta 25, 642–648. Rops, A.L., van der Vlag, J., Lensen, J.F., Wijnhoven, T.J., van den Heuvel, L.P., van Kuppevelt, T.H., Berden, J.H., Heparan sulfate proteoglycans in glomerular inflammation. Kidney Int. 65, 768–785. Borsig, L., Selectins facilitate carcinoma metastasis and heparin can prevent them. News Physiol. Sci. 19, 16– Heparin facilitates implantation: Di Simone et al. (1999) suggested that IgG from women with APS cause pregnancy loss by binding to phospholipids expressed on. the invading trophoblast, thereby inhibiting placental development and, as a consequence, embryonic implantation in early pregnancy. In this study, heparin caused a significant increase. in in vitro trophoblast invasiveness and differentiation. Similarly, LMWH restored. in vitro placental invasiveness and differentiation in trophoblasts incubated with antiphospholipid. antibodies in a dose-dependent fashion (Di Simone et al., 1997). Heparin also has. been shown to increase cellular motility in a first trimester extravillous trophoblast cell line. (Lash et al., 2003). Others suggest that heparin is directly or indirectly, e.g. via heparan sulfate proteoglycans. or heparin-binding EGF involved in the adhesion of the blastocyst to the endometrial. epithelium and the subsequent invasion (Fiedler andWurfel, 2004). A heparin-binding epidermal. growth factor-like (HB-EGF) is a critical signaling molecule in blastocyst-uterine. crosstalk in implantation (Hamatani et al., 2004), and developing extravillous trophoblasts. accumulate HB-EGF. HB-EGF is downregulated in placentae of women with preeclampsia, a disorder associated with deficient trophoblast invasion, raising important questions. about its physiological impact on cytotrophoblasts. Addition of HB-EGF during explants. culture of first-trimester chorionic villi enhances extravillous trophoblast differentiation and. invasive activity (Leach et al., 2004) Di Simone, N., Ferrazzani, S., Castellani, R., De Carolis, S., Mancuso, S., Caruso, A., Heparin and low-dose. aspirin restore placental human chorionic gonadatrophin secretion abolished by antiphospholipid antibodycontaining. sera. Hum. Reprod. 12, 2061–2065. Di Simone, N., Caliandro, D., Castellani, R., Ferrazzani, S., De Carolis, S., Caruso, A., Low-molecular. weight heparin restores in-vitro trophoblast invasiveness and differentiation in presence of immunoglobulin G. fractions obtained from patients with antiphospholipid syndrome. Hum. Reprod. 14, 489–495. Lash, G.E.,Warren, A.Y., Underwood, S., Baker, P.N., 2003.Vascular endothelial growth factor is a chemoattractant. for trophoblast cells. Placenta 24, 549–556. Fiedler, K., Wurfel, W., Effectivity of heparin in assisted reproduction. Eur. J. Med. Res. 9, 207–214. Hamatani, T., Daikoku, T., Wang, H., Matsumoto, H., Carter, M.G., Ko, M.S., Dey, S.K., Global gene. expression analysis identifies molecular pathways distinguishing blastocyst dormancy and activation. Proc. Natl. Acad. Sci. USA 101, 10326– Leach, R.E., Kilburn, B., Wang, J., Liu, Z., Romero, R., Armant, D.R., Heparin-binding EGF-like growth. factor regulates human extravillous cytotrophoblast development during conversion to the invasive phenotype. Dev. Biol. 266, 223– Heparin as a complement inhibitor: The complement system consists of more than 30 proteins in plasma and on cell surfaces that protect the host against invading organisms, initiates inflammation and tissue injury (reviewed in Walport, 2001) There are three pathways of complement activation: the classical, mannose-binding lectin. and alternative pathways. Studies performed over a decade ago found evidence of complement activation in pregnant patients with SLE (Lockshin et al., 1986), and certain patterns of complement activation are associated with either a flare of disease or preeclampsia (Buyon et al., 1992). Elevated levels of complement activation fragments have been detected in patients with. other manifestations of antiphospholipid antibodies-associated disease such as stroke and TIA (Davis and Brey, 1992). Walport, M.J., Complement. First of two parts. N. Engl. J. Med. 344, 1058–1066. Lockshin, M.D., Qamar, T., Redecha, P., Harpel, P.C., Hypocomplementemia with low C1s–C1r inhibitor. complex in systemic lupus erythematosus. Arthritis Rheum. 29, 1467–1472. Buyon, J.P., Tamerius, J., Ordorica, S., Young, B., Abramson, S.B., Activation of the alternative complement. pathway accompanies disease flares in systemic lupus erythematosus during pregnancy. Arthritis Rheum. 35, 55–61. Davis, W.D., Brey, R.L., Antiphospholipid antibodies and complement activation in patients with cerebral. ischemia. Clin. Exp. Immunol. 10, 455–460. The complement system consists of more than 30 proteins in plasma and on cell surfaces that protect the host against invading organisms, initiates inflammation and tissue injury (reviewed in Walport, 2001) There are three pathways of complement activation: the classical, mannose-binding lectin. We now know. G. Girardi / Journal of Reproductive Immunology 66 (2005) 45– from our experiments performed in a mouse model of APS that activation of the complement. cascade is absolutely required to induce pregnancy loss and thrombosis (Girardi. et al., 2004, 2003). We demonstrated that complement activation is a central mechanism. of antiphospholipid antibody-induced pregnancy loss in a mouse model, in which. pregnant mice receive human IgG containing antiphospholipid antibodies or monoclonal. antiphospholipid antibodies. Using different approaches to block complement activation. (mice lacking complement components or their receptors, complement inhibitors, etc.) we were able to protect the mice from antiphospholipid antibody-induced pregnancy loss. Complement component C5 and particularly its cleavage product C5a, and neutrophils. are key mediators of fetal injury and show that treatments with antibodies or peptides. that block C5a–C5a receptor interactions prevent pregnancy complications in our mouse. model. Interestingly, heparin, the standard anticoagulant treatment used to prevent obstetric complications. in patients with APS (Derksen et al., 2004) was shown to have anti-complementary. effects as early as 1929 (Ecker and Gross, 1929). Subsequent studies identified several possible. mechanisms by which heparin can inhibit complement activation at various points in. the classical, alternative and terminal pathways (Loos et al., 1976; Rent et al., 1976;Weiler. et al., 1978; Kazatchkine et al., 1981; Edens et al., 1994; Ninomiya et al., Girardi, G., Berman, J., Redecha, P., Spruce, L., Thurman, J.M., Kraus, D., Hollmann, T.J., Casali, P., Caroll, M.C., Wetsel, R.A., Lambris, J.D., Holers, V.M., Salmon, J.E., Complement C5a receptors and neutrophils. mediate fetal injury in the antiphospholipid syndrome. J. Clin. Invest. 112, 1644–1654. Derksen, R.H., Khamashta, M.A., Branch, D.W., Management of the obstetric antiphospholipid syndrome. Arthritis Rheum. 50, 1028–1039. Ecker, E., Gross, P., Anticomplementary power of heparin. J. Infect. Dis. 44, 250–257. Loos, M., Volanakis, J.E., Stroud, R.M., Mode of interaction of different polyanions with the first (C1, C1), the second (C2) and the fourth (C4) component of complement–III. Inhibition of C4 and C2 binding site(s) on C1s by polyanions. Immunochemistry 13, 789–791. Rent, R., Myhrman, R., Fiedel, B.A., Gewurz, H., Potentiation of C1-esterase inhibitor activity by heparin. Clin. Exp. Immunol. 23, 264–271. Weiler, J.M., Yurt, R.W., Fearon, D.T., Austen, K.F., Modulation of the formation of the amplification. convertase of complement, C3b, Bb, by native and commercial heparin. J. Exp. Med. 147, 409–421. Kazatchkine, M.D., Fearon, D.T., Metcalfe, D.D., Rosenberg, R.D., Austen, K.F., Structural determinants. of the capacity of heparin to inhibit the formation of the human amplification C3 convertase. J. Clin. Invest. 67, 223–228. Edens, R.E., Linhardt, R.J., Bell, C.S., Weiler, J.M., Heparin and derivatized heparin inhibit zymosan and. cobra venom factor activation of complement in serum. Immunopharmacology 27, 145–153. Ninomiya, H., Kawashima, Y., Nagasawa, T., Inhibition of complement-mediated haemolysis in paroxysmal. nocturnal haemoglobinuria by heparin or low-molecular weight heparin. Br. J. Haematol. 109, 875–881.")
61
SONUÇ

62
SİSTEMATİK DEĞERLENDİRMEYE UYGUN ÇALIŞMALAR
SİSTEMATİK DEĞERLENDİRMEYE UYGUN ÇALIŞMALAR ??? Schema of literature search results. Empson. Antiphospholipid Antibodies. Obstet Gynecol 2002

63
Son Mesajlar Trombofilinin kalıtsal ve-veya edinsel nedene bağlı protrombotik tabloları tanımladığı, Edinsel nedenlerin daha sık raslandığı ve daha güçlü faktörler olduğu, Kalıtsal nedenler arasında güçlü risk faktörlerin daha seyrek olarak ortaya çıktığı, Kalıtsal nedenler için her olgunun taranmaması gerektiği, Kalıtsal nedenlerin bilinmesinin gerek genetik danışmanlık ve gerekse korunma-tedavi açısından gerekli olduğu,

64
Son Mesajlar YUT başarısızlığı ve trombofili arasında İlişki vardır ancak net değil Genel olarak çalışma sayısı ve olgu sayısı az. Randomize kontrollü geniş olgu sayılı çalışmalara ihtiyaç vardır Anemnezde TE olması testlerden daha anlamlıdır. Testleri (+) çıkanlar gebelik boyu sonrası ve yaşamın ileri döenmlerinde riskler açısından bilgilendirilmeli, yönlendirilmeli ve izlenmelidir. Proflaktik heparin ve asp ?? Kullanılacaksa heparin OPU dan saat önce kesilmeli ve 6-12 saat sonra başlanmalıdır. Doğumdan sonra da 6 hafta devam edimelidir. 41. Udoff LC, Branch DW. Management of patients with antiphospholipid antibodies undergoing in vitro fertilization. J Autoimmun 2000; 15:209–11.
 çıkanlar gebelik boyu sonrası ve yaşamın ileri döenmlerinde riskler açısından bilgilendirilmeli, yönlendirilmeli ve izlenmelidir. Proflaktik heparin ve asp Kullanılacaksa heparin OPU dan saat önce kesilmeli ve 6-12 saat sonra başlanmalıdır. Doğumdan sonra da 6 hafta devam edimelidir. 41. Udoff LC, Branch DW. Management of patients with antiphospholipid antibodies undergoing in vitro fertilization. J Autoimmun 2000; 15:209–11.")
66
TROMBOFİLİ ve ÜYT Prof.Dr. Mehmet Zeki TANER
Gazi Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum Anabilim Dalı Yüksek Riskli Gebelikler-Prenatal Tanı ve Tedavi Ünitesi

Benzer bir sunumlar