Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Endometriosis Update (Infertility)
Dr.Engin Oral Cerrahpaşa Medical Faculty Department of Obstet & Gynecology Div of Reproductive Endocrinology

4
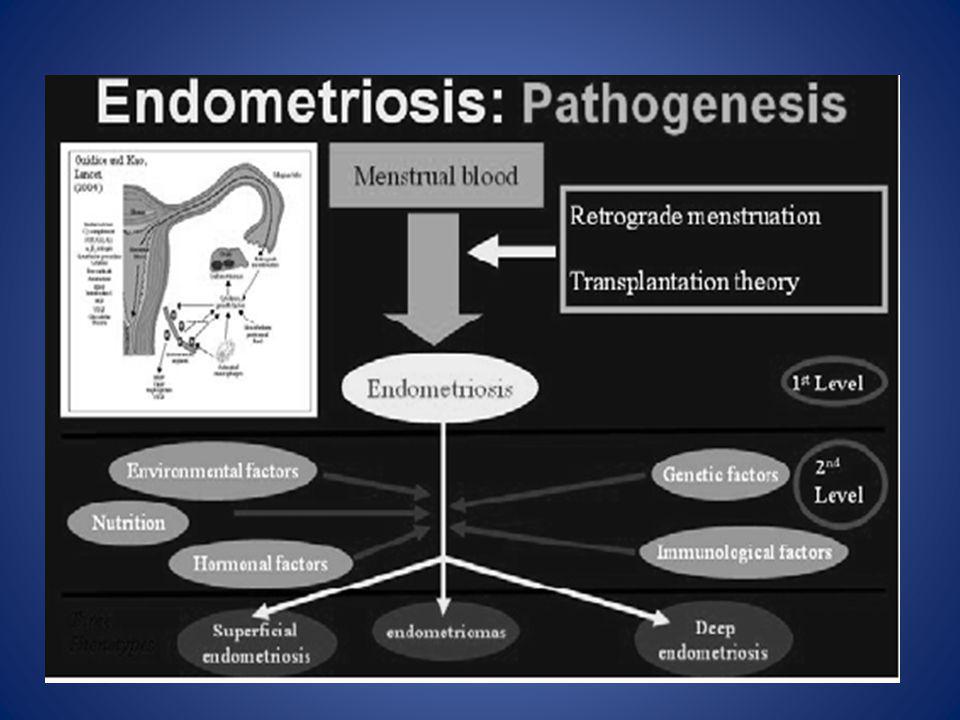
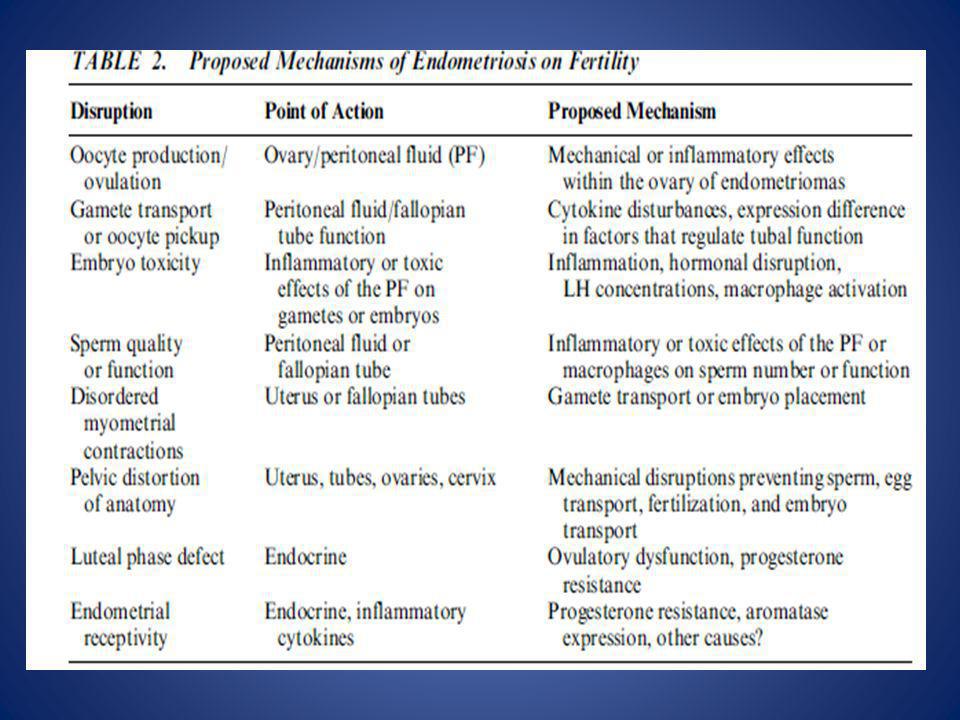
Pathophysiology of Pain and Infertility Associated with Endometriosis.
Retrograde transplanted endometrial tissue and cells attach to peritoneal surfaces, establish a blood supply, and invade nearby structures. They are infiltrated by sensory, sympathetic, and parasympathetic nerves and elicit an inflammatory response. Endometriotic implants secrete estradiol (E2) as well as prostaglandin E2 (PGE2), agents that attract macrophages (monocyte chemotactic protein 1 [MCP-1]), neurotrophic peptides (nerve growth factor [NGF]), enzymes for tissue remodeling (matrix metalloproteinases [MMPs]) and tissue inhibitors of MMPs (TIMPs), and proangiogenic substances such as vascular endothelial growth factor (VEGF) and interleukin-8. Lesions secrete haptoglobin, which decreases macrophage adhesion and phagocytic function. Lesions and activated macrophages, which are abundant in the peritoneal fluid in women with endometriosis, also secrete proinflammatory cytokines (interleukin-1β, interleukin-8, interleukin-6, and tumor necrosis factor α [TNF-α]). Local (and systemic) estradiol can stimulate lesion production of PGE2, which can activate pain fibers, enhance neuronal invasion of lesions by stimulating production of NGF and other neurotrophins, and promote sprouting of nociceptors that contribute to persistent inflammatory pain and inhibit neuronal apoptosis. Endometrial bleeding factor (EBAF) is misexpressed and may contribute to uterine bleeding. Infertility results from the toxic effects of the inflammatory process on gametes and embryos, compromised fimbrial function, and eutopic endometrium that is resistant to the action of progesterone and is inhospitable to embryonic implantation. HoxA10 and HoxA11 genes and αVβ3 integrin are not up-regulated by progesterone, and thus the endometrium is inhospitable to an implanting embryo. Endocrine-disrupting chemicals can contribute to progesterone resistance and perhaps immune dysfunction.1,4 ERFFI1 (ErbB receptor feedback inhibitor 1) is constitutively expressed and there is excess mitogenic signaling. Linda C. Giudice, 2010
 as well as prostaglandin E2 (PGE2), agents that attract macrophages (monocyte chemotactic protein 1 [MCP-1]), neurotrophic. peptides (nerve growth factor [NGF]), enzymes for tissue remodeling (matrix metalloproteinases [MMPs]) and tissue inhibitors of. MMPs (TIMPs), and proangiogenic substances such as vascular endothelial growth factor (VEGF) and interleukin-8. Lesions secrete haptoglobin, which decreases macrophage adhesion and phagocytic function. Lesions and activated macrophages, which are abundant in the. peritoneal fluid in women with endometriosis, also secrete proinflammatory cytokines (interleukin-1β, interleukin-8, interleukin-6, and tumor. necrosis factor α [TNF-α]). Local (and systemic) estradiol can stimulate lesion production of PGE2, which can activate pain fibers, enhance. neuronal invasion of lesions by stimulating production of NGF and other neurotrophins, and promote sprouting of nociceptors that. contribute to persistent inflammatory pain and inhibit neuronal apoptosis. Endometrial bleeding factor (EBAF) is misexpressed and may. contribute to uterine bleeding. Infertility results from the toxic effects of the inflammatory process on gametes and embryos, compromised. fimbrial function, and eutopic endometrium that is resistant to the action of progesterone and is inhospitable to embryonic implantation. HoxA10 and HoxA11 genes and αVβ3 integrin are not up-regulated by progesterone, and thus the endometrium is inhospitable to an implanting. embryo. Endocrine-disrupting chemicals can contribute to progesterone resistance and perhaps immune dysfunction.1,4 ERFFI1. (ErbB receptor feedback inhibitor 1) is constitutively expressed and there is excess mitogenic signaling. Linda C. Giudice,")
5
Effects of endometriosis on human reproduction
Inflamasyona bağlı olarak anormal insitu E2 yapımı ve progesteronun etkilerine lokal rezistans olur Dominique de Ziegler,, 2010

7
Soru Hangisi endometriozis sıklığını azaltır Müller anomalisi Eksersiz
Kızıl saç Alkol/kafein Düşük doğum ağırlığı Cevap B

8
BRANDI S. MCLEOD, and MATTHEW G. RETZLOFF, 2010

9
% 22 CTF n:891

11
2009

12
Endometriosis-associated infertility: a decade’s trend study of women from the Estrie Region of Quebec, Canada N: 6845 Annual variation of the number of newly diagnosed ENDO, EAI and INF cases between 1997 and Using simple linear regression analysis, there was a significative increase of ENDO (r2¼0.717, p¼0.001) and EAI (r2¼0.601, p¼0.003), while there was no increase of INF over years (r2¼2813 e7005, p¼0.987). Endometriosis (ENDO) has been believed to increase during the last years, but recent data supporting this trend are lacking. The aim of this study was to verify whether the incidence of ENDO, infertility (INF) and the both increased during the last 10 years among women living in the Estrie region of Quebec. This retrospective cross-sectional study was realised using data from the CIRESS (Centre Informatise´ de Recherche E´ valuative en Services et Soins de Sante´) system, the database of the CHUS (Centre Hospitalier Universitaire de Sherbrooke), Sherbrooke, Canada. Among the 6845 studied patients, 2564 had ENDO, 4537 were infertile and 256 suffered from both. According to the last 10 years, a significant increase in the number of cases with ENDO (r2¼0.717, p¼0.001) and endometriosis-associated infertility (r2¼0.601, p¼0.003) was noted, while INF remained stable (r2¼2813 e7005, p¼0.987). We showed a prevalence of ENDO of 10.91%. Women with ENDO were at increased risk for being infertile (OR¼2.30; 95% CI¼2.014–2.626, p ). An increase of ENDO in women 18–24 years of age has been shown (r2¼0.418, p¼0.023), suggesting an earlier onset of the disease. KRYSTEL PARIS & AZIZ ARIS, 2010
 and EAI (r2¼0.601, p¼0.003), while there was no increase of INF over years (r2¼2813 e7005, p¼0.987). Endometriosis (ENDO) has been believed to increase during the last years, but recent data supporting this trend are lacking. The aim of this study was to verify whether the incidence of ENDO, infertility (INF) and the both increased during the last. 10 years among women living in the Estrie region of Quebec. This retrospective cross-sectional study was realised using data. from the CIRESS (Centre Informatise´ de Recherche E´ valuative en Services et Soins de Sante´) system, the database of the. CHUS (Centre Hospitalier Universitaire de Sherbrooke), Sherbrooke, Canada. Among the 6845 studied patients, 2564 had. ENDO, 4537 were infertile and 256 suffered from both. According to the last 10 years, a significant increase in the number of. cases with ENDO (r2¼0.717, p¼0.001) and endometriosis-associated infertility (r2¼0.601, p¼0.003) was noted, while. INF remained stable (r2¼2813 e7005, p¼0.987). We showed a prevalence of ENDO of 10.91%. Women with ENDO. were at increased risk for being infertile (OR¼2.30; 95% CI¼2.014–2.626, p ). An increase of ENDO in women. 18–24 years of age has been shown (r2¼0.418, p¼0.023), suggesting an earlier onset of the disease. KRYSTEL PARIS & AZIZ ARIS,")
15
Eijkemans et al., 2008

16
14. Collins JA, Burrows EA, Wilan AR. The prognosis for live birth
among untreated infertile couples. Fertil Steril. 1995;64(1):22–8. Collins JA , 1995
:22–8. Collins JA ,")
17
Cumulative conception rates with untreated endometriosis related to disease grading, compared with normal conception rate N Minor Cumulative conception rates with untreated endometriosis related to disease grading, compared with normal conception rate. Disease grading: n, normal; l, minor (Portuondo et al., 1983; Hull et al., 1987; Badawy et al., 1988; Hull, 1990); s, moderate ovarian (Hull, 1990); t, severe (Garcia and David, 1977; Olive et al., 1985). Redrawn from Hull (1992) with permission from Oxford University Press/Human Reproduction. Moderate Severe Kevin D. Jones, 2002
; s, moderate ovarian. (Hull, 1990); t, severe (Garcia and David, 1977; Olive et al., 1985). Redrawn from Hull (1992) with permission from Oxford University. Press/Human Reproduction. Moderate Severe. Kevin D. Jones,")
18
Fertility in women with minimal endometriosis compared with normal women was assessed by means of a donor insemination program in unstimulated cycles N: 51 N: 24 OBJECTIVE: The purpose of this study was to compare the pregnancy rate in an artificial insemination donor program in women with minimal endometriosis and in women without endometriosis. STUDY DESIGN: A prospective double-blinded study was conducted in women with azoospermic partners. RESULTS: The per-cycle pregnancy rate was 8.6% (9/104 women) in the minimal endometriosis group vs 13.3% (26/196 women) in the control group. The per-woman pregnancy rate was 37.5% (9/24 women) in the minimal endometriosis group and 51.0% (26/51 women) in the control group. CONCLUSION: Pregnancy rates were statistically similar in normal women and in women with minimal endometriosis. Roberto Matorras 2010
 in. the minimal endometriosis group vs 13.3% (26/196 women) in the control. group. The per-woman pregnancy rate was 37.5% (9/24 women) in. the minimal endometriosis group and 51.0% (26/51 women) in the. control group. CONCLUSION: Pregnancy rates were statistically similar in normal. women and in women with minimal endometriosis. Roberto Matorras")
20
Success in intrauterine insemination: the role of etiology
A total of 1,171 cycles among 532 infertile couples were retrospectively studied and the impact of different prognostic factors on pregnancy rate in five different etiology subgroups was analyzed. Results. The pregnancy rate/cycle was highest (19.2%) among women with anovulatory infertility and lowest (11.9%) in endometriosis based infertility. Background. We aimed to identify the prognostic factors for the highest pregnancy rate and lowest multiple pregnancy rate in different infertility etiology groups among women undergoing insemination treatment. Methods. A total of 1,171 cycles among 532 infertile couples were retrospectively studied and the impact of different prognostic factors on pregnancy rate in five different etiology subgroups was analyzed. Results. The pregnancy rate/cycle was highest (19.2%) among women with anovulatory infertility and lowest (11.9%) in endometriosis based infertility. Multiple pregnancy rate varied between 3.6% (male infertility) and 13.2% (anovulatory infertility). In unexplained infertility ovarian stimulation resulting in three follicles (pregnancy rate 24.2%) and inseminated motile sperm count30106 (pregnancy rate 19.8%) were significant prognostic factors. In anovulatory infertility stimulation with sequential clomiphene citrate and human menopausal gonadotrophin was a positive predictive factor, with a pregnancy rate of 36%. In male infertility stimulation with sequential clomiphene citrate/ human menopausal gonadotrophin resulted in the best pregnancy rate (25.0%). In endometriosis-based infertility the pregnancy rate was best with clomiphene citrate stimulation (21.1%) and inseminated motile sperm count30106 (24.3%). In combined infertility the highest pregnancy rate was with sequential clomiphene citrate/human menopausal gonadotrophin stimulation and with three follicles (30%), and even 18.2% with inseminated motile sperm countB5.0 106. Conclusions. The etiology of the infertility is important when optimal insemination treatment is planned. The impact of the woman’s age, sperm count, stimulation protocol, and the follicle number on the pregnancy rate and multiple pregnancy rate is associated with the etiology of the infertility. Katja Ahinko-Hakamaa 2007
 among women with anovulatory infertility and lowest (11.9%) in endometriosis based infertility. Background. We aimed to identify the prognostic factors for the highest pregnancy rate and lowest multiple pregnancy rate in. different infertility etiology groups among women undergoing insemination treatment. Methods. A total of 1,171 cycles. among 532 infertile couples were retrospectively studied and the impact of different prognostic factors on pregnancy rate in. five different etiology subgroups was analyzed. Results. The pregnancy rate/cycle was highest (19.2%) among women with. anovulatory infertility and lowest (11.9%) in endometriosis based infertility. Multiple pregnancy rate varied between 3.6% (male infertility) and 13.2% (anovulatory infertility). In unexplained infertility ovarian stimulation resulting in three follicles. (pregnancy rate 24.2%) and inseminated motile sperm count30106 (pregnancy rate 19.8%) were significant prognostic. factors. In anovulatory infertility stimulation with sequential clomiphene citrate and human menopausal gonadotrophin was. a positive predictive factor, with a pregnancy rate of 36%. In male infertility stimulation with sequential clomiphene citrate/ human menopausal gonadotrophin resulted in the best pregnancy rate (25.0%). In endometriosis-based infertility. the pregnancy rate was best with clomiphene citrate stimulation (21.1%) and inseminated motile sperm count (24.3%). In combined infertility the highest pregnancy rate was with sequential clomiphene citrate/human menopausal. gonadotrophin stimulation and with three follicles (30%), and even 18.2% with inseminated motile sperm countB Conclusions. The etiology of the infertility is important when optimal insemination treatment is planned. The impact of. the woman’s age, sperm count, stimulation protocol, and the follicle number on the pregnancy rate and multiple pregnancy. rate is associated with the etiology of the infertility. Katja Ahinko-Hakamaa")
21
KOH + IUI İleri evre endometrioziste KOH+IUI ‘ın etkinliğini gösteren RCT mevcut değil KOH+IUI maksimum 3-4 siklusla sınırlanmalı (ESHRE Guidelines, Recommedation grade A ,evidence level 1b)
")
22
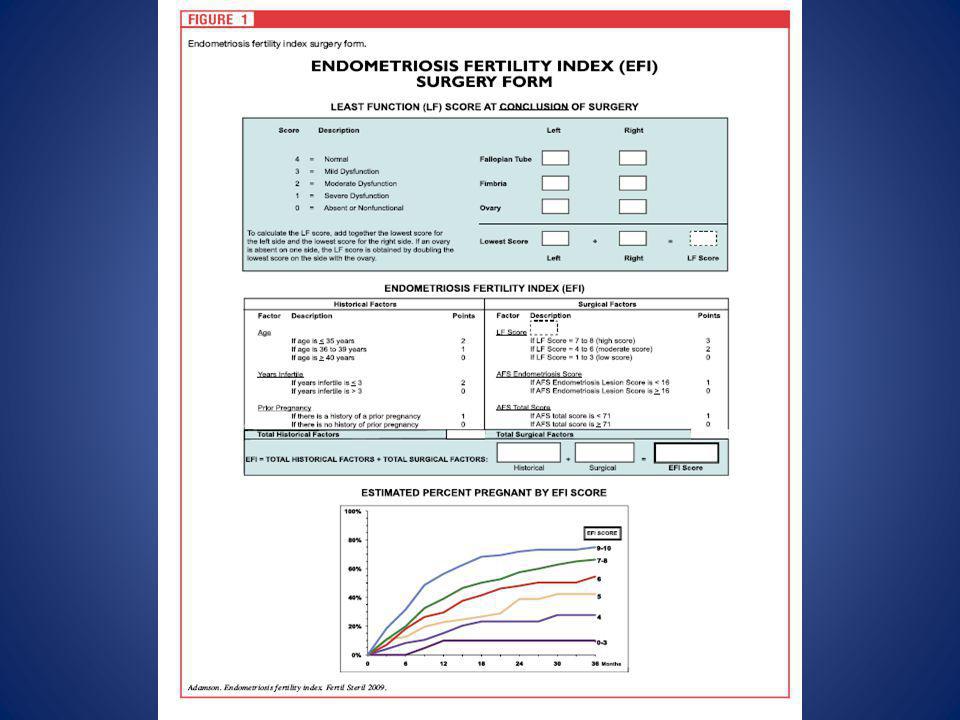
2009 OBJECTIVE: To develop a clinical tool that predicts pregnancy rates (PRs) in patients with surgically documented endometriosis who attempt non-IVF conception. DESIGN: Prospective data collection on 579 patients and comprehensive statistical analysis to derive a new staging system-the endometriosis fertility index (EFI)-from data rather than a priori assumptions, followed by testing the EFI prospectively on 222 additional patients for correlation of predicted and actual outcomes. SETTING: Private reproductive endocrinology practice. PATIENT(S): A total of 801 consecutively diagnosed and treated infertile patients with endometriosis. INTERVENTION(S): Surgical diagnosis and treatment followed by non-IVF fertility management. MAIN OUTCOME MEASURE(S): The EFI and life table PRs. RESULT(S): A statistically significant variable used to create the EFI was the least function score (i.e., the sum of those scores determined intraoperatively after surgical intervention that describe the function of the tube, fimbria, and ovary on both sides). Sensitivity analysis showed that the EFI varies little, even with variation in the assignment of functional scores, and predicted PRs. CONCLUSION(S): The EFI is a simple, robust, and validated clinical tool that predicts PRs after endometriosis surgical staging. Its use provides reassurance to those patients with good prognoses and avoids wasted time and treatment for those with poor prognoses To develop a clinical tool that predicts pregnancy rates (PRs) in patients with surgically documented endometriosis who attempt non-IVF conception.
 in patients with surgically documented endometriosis who attempt non-IVF conception. DESIGN: Prospective data collection on 579 patients and comprehensive statistical analysis to derive a new staging system-the endometriosis fertility index (EFI)-from data rather than a priori assumptions, followed by testing the EFI prospectively on 222 additional patients for correlation of predicted and actual outcomes. SETTING: Private reproductive endocrinology practice. PATIENT(S): A total of 801 consecutively diagnosed and treated infertile patients with endometriosis. INTERVENTION(S): Surgical diagnosis and treatment followed by non-IVF fertility management. MAIN OUTCOME MEASURE(S): The EFI and life table PRs. RESULT(S): A statistically significant variable used to create the EFI was the least function score (i.e., the sum of those scores determined intraoperatively after surgical intervention that describe the function of the tube, fimbria, and ovary on both sides). Sensitivity analysis showed that the EFI varies little, even with variation in the assignment of functional scores, and predicted PRs. CONCLUSION(S): The EFI is a simple, robust, and validated clinical tool that predicts PRs after endometriosis surgical staging. Its use provides reassurance to those patients with good prognoses and avoids wasted time and treatment for those with poor prognoses. To develop a clinical tool that predicts pregnancy rates (PRs) in patients with surgically documented endometriosis who attempt non-IVF conception.")
25
Decreased anti-Mullerian hormone and altered ovarian follicular cohort in infertile patients with mild/minimal endometriosis p:0.004 N:17 N:17 EE CC Objective: To evaluate the ovarian reserve and follicular cohort of infertile patients with minimal/mild endometriosis. Design: Prospective study. Setting: University hospital. Patient(s): Patients were divided into two groups: group I, minimal/mild endometriosis and group II, tubal obstruction. The following exclusion criteria were established: [1] patients with previous endocrine disorders; and [2] cases in which the cause for infertility was other than endometriosis (except for patients with tubal obstruction, in the control group). Intervention(s): Serum FSH and anti-M€ullerian hormone were measured on day 3. On the same day all patients were submitted to transvaginal ultrasound to evaluate the antral follicular count and the ovarian follicular cohort. Main Outcome Measure(s): Serum FSH, anti-M€ullerian hormone, and the follicular cohort with the respective antral follicular count. Result(s): Serum FSH were not different between the groups. However, infertile patients with endometriosis have a decreased serum anti-Mullerian hormone ( ng/mL) compared to the control group ( ng/mL). The analysis of follicular cohort showed that the number of selectable follicles were similar, but the follicular diameter was different. Conclusion(s): Minimal/mild endometriosis is associated with a decrease in the follicular ovarian reserve. In addition, the follicular cohort of these patients is more heterogeneous in comparison to the control group. Nadiane Albuquerque Lemos, 2009
: Patients were divided into two groups: group I, minimal/mild endometriosis and group II, tubal obstruction. The following exclusion criteria were established: [1] patients with previous endocrine disorders; and. [2] cases in which the cause for infertility was other than endometriosis (except for patients with tubal obstruction, in the control group). Intervention(s): Serum FSH and anti-M€ullerian hormone were measured on day 3. On the same day all patients. were submitted to transvaginal ultrasound to evaluate the antral follicular count and the ovarian follicular cohort. Main Outcome Measure(s): Serum FSH, anti-M€ullerian hormone, and the follicular cohort with the respective. antral follicular count. Result(s): Serum FSH were not different between the groups. However, infertile patients with endometriosis have. a decreased serum anti-Mullerian hormone ( ng/mL) compared to the control group ( ng/mL). The analysis of follicular cohort showed that the number of selectable follicles were similar, but the follicular. diameter was different. Conclusion(s): Minimal/mild endometriosis is associated with a decrease in the follicular ovarian reserve. In addition, the follicular cohort of these patients is more heterogeneous in comparison to the control group. Nadiane Albuquerque Lemos,")
26
Anti mullerian hormone serum levels in women with endometriosis: A case–control study
909 patients undergoing in vitro fertilisation/intracytoplasmic sperm injection (IVF/ICSI) treatment or consulting our specific endometriosis unit. Mean AMH serum level was significantly lower in the study than in the control group ( ng/ml vs ng/ml, p 0.001). In women with mild endometriosis (rAFS I-II), the mean AMH level was almost equal to the control group ( ng/ml vs ng/ml; p 0.61). A significant difference in mean AMH serum level was found between women with severe endometriosis (rAFS III-IV) and the control group ( ng/ml vs ng/ml; p ). Objective. To compare the anti muellerian hormone (AMH) serum levels in women with and without endometriosis. Design. A case–control study Setting. Women’s General Hospital, Linz, Austria. Patient(s). Our study included a total of 909 patients undergoing in vitro fertilisation/intracytoplasmic sperm injection (IVF/ICSI) treatment or consulting our specific endometriosis unit. After proofing the exclusion criteria, 153 of these patients with endometriosis (study group) were matched with 306 patients undergoing IVF/ICSI treatment because of a male factor (control group). Interventions. None. Main outcome measures. AMH serum level. Results. Mean AMH serum level was significantly lower in the study than in the control group ( ng/ml vs. ng/ml, p50.001). In women with mild endometriosis (rAFS I-II), the mean AMH level was almost equal to the control group ( ng/ml vs ng/ml; p¼0.61). A significant difference in mean AMH serum level was found between women with severe endometriosis (rAFS III-IV) and the control group ( ng/ml vs. ng/ml; p ). Conclusion. Lower AMH serum levels and an association with the severity were found in women with endometriosis. Physicians have to be aware of this fact. Because of the expected lower response on a controlled ovarian hyperstimulation (COH), AMH serum level should be measured to optimise the dose of gonadotropin treatment previous to a COH, especially in women with severe endometriosis. OMAR SHEBL, 2009
 treatment or consulting our specific endometriosis unit. Mean AMH serum level was significantly lower in the study than in the control group ( ng/ml vs ng/ml, p 0.001). In women with mild endometriosis (rAFS I-II), the mean AMH level was almost equal to the control group ( ng/ml vs ng/ml; p 0.61). A significant difference in mean AMH serum level was found between women with severe endometriosis (rAFS III-IV) and the control group ( ng/ml vs ng/ml; p ). Objective. To compare the anti muellerian hormone (AMH) serum levels in women with and without endometriosis. Design. A case–control study. Setting. Women’s General Hospital, Linz, Austria. Patient(s). Our study included a total of 909 patients undergoing in vitro fertilisation/intracytoplasmic sperm injection. (IVF/ICSI) treatment or consulting our specific endometriosis unit. After proofing the exclusion criteria, 153 of these. patients with endometriosis (study group) were matched with 306 patients undergoing IVF/ICSI treatment because of a male. factor (control group). Interventions. None. Main outcome measures. AMH serum level. Results. Mean AMH serum level was significantly lower in the study than in the control group ( ng/ml vs ng/ml, p50.001). In women with mild endometriosis (rAFS I-II), the mean AMH level was almost equal to the. control group ( ng/ml vs ng/ml; p¼0.61). A significant difference in mean AMH serum level was. found between women with severe endometriosis (rAFS III-IV) and the control group ( ng/ml vs ng/ml; p ). Conclusion. Lower AMH serum levels and an association with the severity were found in women with endometriosis. Physicians have to be aware of this fact. Because of the expected lower response on a controlled ovarian hyperstimulation. (COH), AMH serum level should be measured to optimise the dose of gonadotropin treatment previous to a COH, especially in women with severe endometriosis. OMAR SHEBL,")
27
Effects of ovarian endometrioma on the number of oocytes retrieved for in vitro fertilization
Objective: To evaluate the effects of ovarian endometrioma on the number of oocytes retrieved for IVF. Setting: University-based tertiary medical center. Patient(s): We studied 81 women with unilateral endometrioma who underwent their first IVF cycle. Intervention(s): Oocyte collection. Main Outcome Measure(s): The numbers of antral follicles and the retrieved oocytes in the ovary that contained endometrioma were compared with those from the contralateral ovary. Antral follicle count and the total number of oocytes retrieved from these women then were compared with those in 162 age-matched women with no endometrioma or endometriosis, who also underwent the first IVF treatment cycle. Result(s): There was no significant difference in the number of antral follicles and oocytes retrieved in the endometrioma-containing ovary ( and , respectively) and in the opposite ovary ( and 8.50.9, respectively). There was no correlation between the size and the number of endometriomas with the number of retrieved oocytes. Antral follicle count and the number of retrieved oocytes in these women ( and ) were similar to those in women with no endometrioma ( and , respectively). Conclusion(s): The presence of ovarian endometrioma in a controlled ovarian hyperstimulation cycle for IVF treatment is not associated with a reduced number of oocytes retrieved from the affected ovary Benny Almog, 2010
: We studied 81 women with unilateral endometrioma who underwent their first IVF cycle. Intervention(s): Oocyte collection. Main Outcome Measure(s): The numbers of antral follicles and the retrieved oocytes in the ovary that contained. endometrioma were compared with those from the contralateral ovary. Antral follicle count and the total number of. oocytes retrieved from these women then were compared with those in 162 age-matched women with no endometrioma. or endometriosis, who also underwent the first IVF treatment cycle. Result(s): There was no significant difference in the number of antral follicles and oocytes retrieved in the. endometrioma-containing ovary ( and , respectively) and in the opposite ovary ( and , respectively). There was no correlation between the size and the number of endometriomas with the number. of retrieved oocytes. Antral follicle count and the number of retrieved oocytes in these women ( and ) were similar to those in women with no endometrioma ( and , respectively). Conclusion(s): The presence of ovarian endometrioma in a controlled ovarian hyperstimulation cycle for IVF. treatment is not associated with a reduced number of oocytes retrieved from the affected ovary. Benny Almog,")
28
Soru Endometriozise bağlı infertilitede cerrahi tedavi sonrası spontan gebelik şansı ne kadardır? (tüm evrelerde ve ilk 1 yıl içinde) 10 25 50 70 90 Cevap C

34
A comparison of histopathologic findings of ovarian tissue inadvertently excised with endometrioma and other kinds of benign ovarian cyst in patients undergoing laparoscopy versus laparotomy Objective: To evaluate ovarian tissue inadvertently excised with benign cysts during laparotomy or laparoscopy. Design: Prospective study. Setting: Private and university hospitals. Patient(s): 260 women, 20 to 35 years old, with unilateral benign ovarian cysts. Intervention(s): One hundred fifty women operated by laparoscopic cystectomy stripping technique, and 110 women operated by laparotomy with the same technique. Main Outcome Measure(s): Histopathologic findings of ovarian tissue inadvertently excised in endometrioma compared with other kinds of benign cysts in laparoscopy versus laparotomy. Result(s): In the laparoscopy group, ovarian tissue was present in 65% of endometrioma and in 32% of nonendometriotic cysts. In the laparotomy group, ovarian tissue was seen in 80% of endometrioma and 41% of nonendometriotic cysts. Conclusion(s): The surgical approach had no statistically significant impact on conservation of ovarian reserves. The nature of the ovarian cyst played a greater role in the quality and quantity of the excised ovarian tissue Saeed Alborzi, 2009
: 260 women, 20 to 35 years old, with unilateral benign ovarian cysts. Intervention(s): One hundred fifty women operated by laparoscopic cystectomy stripping technique, and 110. women operated by laparotomy with the same technique. Main Outcome Measure(s): Histopathologic findings of ovarian tissue inadvertently excised in endometrioma. compared with other kinds of benign cysts in laparoscopy versus laparotomy. Result(s): In the laparoscopy group, ovarian tissue was present in 65% of endometrioma and in 32% of nonendometriotic. cysts. In the laparotomy group, ovarian tissue was seen in 80% of endometrioma and 41% of nonendometriotic. cysts. Conclusion(s): The surgical approach had no statistically significant impact on conservation of ovarian reserves. The nature of the ovarian cyst played a greater role in the quality and quantity of the excised ovarian tissue. Saeed Alborzi,")
35
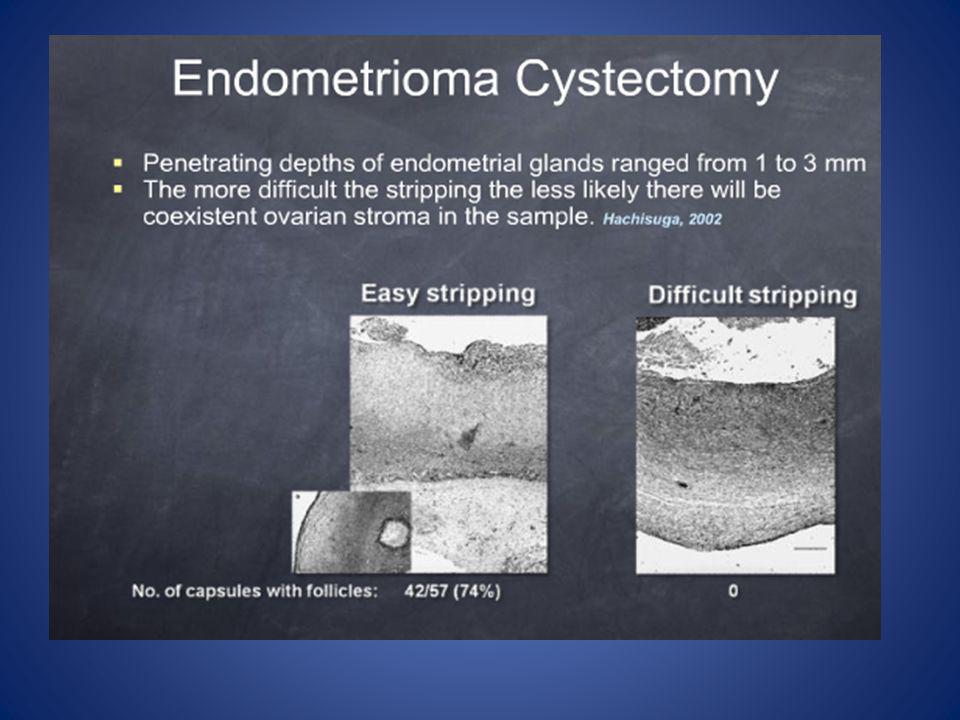
Excision of endometriotic cyst wall may cause loss of functional ovarian tissue
patient, evaluated five different full-thickness sections including blinded to the clinical and surgical history of the After excising the cyst wall completely, the same pathologist, evaluated for the presence or absence of ovarian tissue cyst and one section from the central portion. Cyst wall was four different sections from the periphery of the the cyst wall according to morphologic characteristics semiquantitave scale of 0 to 4 (7). The pathologist evaluated adjacent to the excised cyst wall and graded according to presence of only primordial follicles was grade 1, presence of regard, complete absence of follicles was described as grade 0, of the excised ovarian tissue within the cyst wall. In this Endometriotic cysts and infertility is a well known association. of secondary follicles was grade 3 and grade 4. primordial and primary follicles were grade 2, and detection fertilization rates (1). In addition, repeated ovarian surgeries ovarian stimulation, oocyte recovery, and implantation and Ovarian endometriomas could affect the response to Pathogenesis of ovarian endometriomas is still controversial. the loss of ovarian reserve. for recurrent endometriomas might be associated with cortex is a well known hypothesis (2). However, metaplasia ovarian endometriotic implants into the ovarian Inversion and progressive invagination of the superficial mechanism in the genesis of ovarian endometriomas (1). of invaginated coelomic epithelium is another proposed procedures for the treatment of endometriotic cysts laser or electrocoagulation are commonly performed surgical Cyst aspiration, fenestration, and ablation of cyst wall by low recurrence rates (3, 4). The excision of the cyst wall is surgical treatment of ovarian endometriotic cysts owing to (1). Excision of the cyst wall is accepted technique for able to save the normal ovarian tissue by using stripping tissue (5). However, Muzii et al. (6) reported that they were disputable because it may result in loss of normal ovarian laparoscopy is a tissue sparing technique. aimed to determine whether the stripping of cyst wall by technique at laparoscopic cyst removal. In this study, we dysmenorrhea, and persistent ovarian cystic mass. cyst excision because of chronic pelvic pain, infertility, Between 2002 and 2004, 46 patients underwent laparoscopic 6.5-MHz transvaginal probe. Serum CA-125 levels were 500 Pro (Milwaukee, WI) and 3.5-MHz convex probe and Ultrasonographic examination was performed by GE Logiq of earlier ovarian surgery, especially due to ovarian endometriomas, Women with body mass greater than 30 kg/m2, history determined from all subjects preoperatively. use, bilateral ovarian cysts, and multiple ovarian cysts that history of GnRH analogs and oral contraceptive team performed laparoscopic cystectomy in the dorsal cases underwent laparoscopic cyst removal. The same surgical were occupying the same ovary were excluded. Selected the cyst was not punctured and every effort was made to In case of ultrasonographic diagnosis of dermoid cyst, lithotomy position in all subjects. aspirated. Following the puncture, the surgeon found the Other cysts including endometriomas were punctured and excise the entire cyst without spilling its sebaceous content. ovarian tissue by traction and countertraction. cleavage plane and stripped cyst wall from the normal To compare continuous variables, Student t test was statistically significant. We did not request institutional of categorical variables. P.05 was considered used. Chi-squared or Fisher exact test was used for comparison as usually followed at our center. In addition, cystectomy change our management of the patients with ovarian cysts review board approval for the study, because it did not of malignancy. at our center for ovarian cysts except under suspicion by route of laparoscopy or laparotomy is standard procedure the 46 patients, and no intraoperative or postoperative Laparoscopic cystectomy was completed successfully in mass. Infertility in 7 patients (15.2%), chronic pelvic pain, laparoscopy because of persistence of ovarian cystic complications were seen. Thirteen patients (28.2%) underwent (84.7%). We preferred bipolar electrocautery to achieve step, the surgeon aspirated cyst content in 39 cases and cyclic dysmenorrhea in 26 patients (56.52%) wereother indications for laparoscopic intervention. As a first Histopathologic diagnosis of the surgical specimens and suture was required in only 2 cases (4.34%). hemostasis in 40 cases (87%), and reconstruction by laparoscopic There is no statistical difference between the endometriotic Two endometriotic cyst walls were histopathologic grade 4. grading of residual ovarian tissue are shown in Table 1. However, there is a statistically significant difference between ovarian tissue adjacent to removed cyst wall (P.414). cysts and nonendometriotic cysts for presence of normal removed cyst wall (P.02), although this correlation was cyst and presence of normal ovarian tissue adjacent to the preoperative ultrasonographic diameter of ovarian weak (Pearson correlation coefficient 0.377). Umut Dilek, 2006
. The pathologist evaluated. adjacent to the excised cyst wall and graded according to. presence of only primordial follicles was grade 1, presence of. regard, complete absence of follicles was described as grade 0, of the excised ovarian tissue within the cyst wall. In this. Endometriotic cysts and infertility is a well known association. of secondary follicles was grade 3 and grade 4. primordial and primary follicles were grade 2, and detection. fertilization rates (1). In addition, repeated ovarian surgeries. ovarian stimulation, oocyte recovery, and implantation and. Ovarian endometriomas could affect the response to. Pathogenesis of ovarian endometriomas is still controversial. the loss of ovarian reserve. for recurrent endometriomas might be associated with. cortex is a well known hypothesis (2). However, metaplasia. ovarian endometriotic implants into the ovarian. Inversion and progressive invagination of the superficial. mechanism in the genesis of ovarian endometriomas (1). of invaginated coelomic epithelium is another proposed. procedures for the treatment of endometriotic cysts. laser or electrocoagulation are commonly performed surgical. Cyst aspiration, fenestration, and ablation of cyst wall by. low recurrence rates (3, 4). The excision of the cyst wall is. surgical treatment of ovarian endometriotic cysts owing to. (1). Excision of the cyst wall is accepted technique for. able to save the normal ovarian tissue by using stripping. tissue (5). However, Muzii et al. (6) reported that they were. disputable because it may result in loss of normal ovarian. laparoscopy is a tissue sparing technique. aimed to determine whether the stripping of cyst wall by. technique at laparoscopic cyst removal. In this study, we. dysmenorrhea, and persistent ovarian cystic mass. cyst excision because of chronic pelvic pain, infertility, Between 2002 and 2004, 46 patients underwent laparoscopic. 6.5-MHz transvaginal probe. Serum CA-125 levels were. 500 Pro (Milwaukee, WI) and 3.5-MHz convex probe and. Ultrasonographic examination was performed by GE Logiq. of earlier ovarian surgery, especially due to ovarian endometriomas, Women with body mass greater than 30 kg/m2, history. determined from all subjects preoperatively. use, bilateral ovarian cysts, and multiple ovarian cysts that. history of GnRH analogs and oral contraceptive. team performed laparoscopic cystectomy in the dorsal. cases underwent laparoscopic cyst removal. The same surgical. were occupying the same ovary were excluded. Selected. the cyst was not punctured and every effort was made to. In case of ultrasonographic diagnosis of dermoid cyst, lithotomy position in all subjects. aspirated. Following the puncture, the surgeon found the. Other cysts including endometriomas were punctured and. excise the entire cyst without spilling its sebaceous content. ovarian tissue by traction and countertraction. cleavage plane and stripped cyst wall from the normal. To compare continuous variables, Student t test was. statistically significant. We did not request institutional. of categorical variables. P.05 was considered. used. Chi-squared or Fisher exact test was used for comparison. as usually followed at our center. In addition, cystectomy. change our management of the patients with ovarian cysts. review board approval for the study, because it did not. of malignancy. at our center for ovarian cysts except under suspicion. by route of laparoscopy or laparotomy is standard procedure. the 46 patients, and no intraoperative or postoperative. Laparoscopic cystectomy was completed successfully in. mass. Infertility in 7 patients (15.2%), chronic pelvic pain, laparoscopy because of persistence of ovarian cystic. complications were seen. Thirteen patients (28.2%) underwent. (84.7%). We preferred bipolar electrocautery to achieve. step, the surgeon aspirated cyst content in 39 cases. and cyclic dysmenorrhea in 26 patients (56.52%) wereother indications for laparoscopic intervention. As a first. Histopathologic diagnosis of the surgical specimens and. suture was required in only 2 cases (4.34%). hemostasis in 40 cases (87%), and reconstruction by laparoscopic. There is no statistical difference between the endometriotic. Two endometriotic cyst walls were histopathologic grade 4. grading of residual ovarian tissue are shown in Table 1. However, there is a statistically significant difference between. ovarian tissue adjacent to removed cyst wall (P.414). cysts and nonendometriotic cysts for presence of normal. removed cyst wall (P.02), although this correlation was. cyst and presence of normal ovarian tissue adjacent to. the preoperative ultrasonographic diameter of ovarian. weak (Pearson correlation coefficient 0.377). Umut Dilek,")
36
The impact of electrocoagulation on ovarian reserve after laparoscopic excision of ovarian cysts: a prospective clinical study of 191 patients 191 patients with benign ovarian cysts undergoing ovarian cystectomy. When comparing the bipolar group and ultrasonic scalpel group with the suture group, a statistically significant increase of the mean FSH value was found in bilateral-cyst patients at 1-, 3-, 6-, and 12-month follow-up evaluations and in unilateral-cyst patients at the 1-month follow-up evaluation. Statistically significant decreases of basal antral follicle number and mean ovarian diameter were found during the 3-, 6-, 12-month follow-up evaluations as well as statistically significant decreases of peak systolic velocity at all of the follow-up evaluations. Conclusion(s): Electrocoagulation after laparoscopic excision of ovarian cysts is associated with a statistically significant reduction in ovarian reserve, which is partly a consequence of the damage to the ovarian vascular system. Objective: To investigate the impact of electrocoagulation on ovarian reserve after laparoscopic excision of ovarian cysts and the possible mechanisms. Design: A prospective study. Setting: Obstetrics and Gynecology Department of a university hospital. Patient(s): 191 patients with benign ovarian cysts undergoing ovarian cystectomy. Intervention(s): Laparoscopic ovarian cystectomy using bipolar or ultrasonic scalpel electrocoagulation and laparotomic ovarian cystectomy using sutures after the excision of ovarian cysts. Main Outcome Measure(s): Follicle-stimulating hormone (FSH) assay and transvaginal ultrasound evaluating basal antral follicle number, mean ovarian diameter, and ovarian stromal blood flow velocity at day 3 of menstrual cycles 1, 3, 6, and 12 after surgery. Result(s): When comparing the bipolar group and ultrasonic scalpel group with the suture group, a statistically significant increase of the mean FSH value was found in bilateral-cyst patients at 1-, 3-, 6-, and 12-month follow- up evaluations and in unilateral-cyst patients at the 1-month follow-up evaluation. Statistically significant decreases of basal antral follicle number and mean ovarian diameter were found during the 3-, 6-, 12-month follow-up evaluations as well as statistically significant decreases of peak systolic velocity at all of the follow-up evaluations. Conclusion(s): Electrocoagulation after laparoscopic excision of ovarian cysts is associated with a statistically significant reduction in ovarian reserve, which is partly a consequence of the damage to the ovarian vascular system Chang-Zhong Li, 2009
: Electrocoagulation after laparoscopic excision of ovarian cysts is associated with a statistically significant reduction in ovarian reserve, which is partly a consequence of the damage to the ovarian vascular system. Objective: To investigate the impact of electrocoagulation on ovarian reserve after laparoscopic excision of ovarian. cysts and the possible mechanisms. Design: A prospective study. Setting: Obstetrics and Gynecology Department of a university hospital. Patient(s): 191 patients with benign ovarian cysts undergoing ovarian cystectomy. Intervention(s): Laparoscopic ovarian cystectomy using bipolar or ultrasonic scalpel electrocoagulation and laparotomic. ovarian cystectomy using sutures after the excision of ovarian cysts. Main Outcome Measure(s): Follicle-stimulating hormone (FSH) assay and transvaginal ultrasound evaluating. basal antral follicle number, mean ovarian diameter, and ovarian stromal blood flow velocity at day 3 of menstrual. cycles 1, 3, 6, and 12 after surgery. Result(s): When comparing the bipolar group and ultrasonic scalpel group with the suture group, a statistically. significant increase of the mean FSH value was found in bilateral-cyst patients at 1-, 3-, 6-, and 12-month follow- up evaluations and in unilateral-cyst patients at the 1-month follow-up evaluation. Statistically significant decreases. of basal antral follicle number and mean ovarian diameter were found during the 3-, 6-, 12-month follow-up. evaluations as well as statistically significant decreases of peak systolic velocity at all of the follow-up evaluations. Conclusion(s): Electrocoagulation after laparoscopic excision of ovarian cysts is associated with a statistically significant. reduction in ovarian reserve, which is partly a consequence of the damage to the ovarian vascular system. Chang-Zhong Li,")
37
Analysis of risk factors for the removal of normal ovarian tissue during laparoscopic cystectomy for ovarian endometriosis A total of 121 patients who had histologically confirmed ovarian endometriosis and 56 control patients who had other histologically confirmed benign cysts were included Normal ovarian tissue adjacent to the cyst wall was detected in 71 patients (58.7%) with endometriosis, whereas normal ovarian tissue was removed from only three patients (5.4%) with other benign cysts. A significant factor that was independently associated with the removal of normal ovarian tissue with ovarian endometriosis was pre-operative medical treatment background: The aim of this study was to identify risk factors for the removal of normal ovarian tissue during laparoscopic cystectomy for endometriosis. methods: A total of 121 patients who had histologically confirmed ovarian endometriosis and 56 control patients who had other histologically confirmed benign cysts were included for the present analysis. The blocks of removed tissue were sectioned at 120 mm intervals and a total of five sections were analyzed for each ovarian cyst. Eight variables (age, pre-operative medical treatment, previous surgery for ovarian endometriosis, single or multiple cysts, size of the largest cyst, side of cyst, co-existence of deep endometriosis, revised American Society for Reproductive Medicine classification) were evaluated using a generalized linear modeling analysis to identify major factors associated with the removal of normal ovarian tissue. results: Normal ovarian tissue adjacent to the cyst wall was detected in 71 patients (58.7%) with endometriosis, whereas normal ovarian tissue was removed from only three patients (5.4%) with other benign cysts. A significant factor that was independently associated with the removal of normal ovarian tissue with ovarian endometriosis was pre-operative medical treatment. conclusions: The present retrospective, controlled study suggests that pre-operative medical treatment might be a risk factor for the removal of normal ovarian tissue during laparoscopic cystectomy for ovarian endometriosis. Sachiko Matsuzaki1,2009
 with endometriosis, whereas normal ovarian tissue was removed from only three patients (5.4%) with other benign cysts. A significant factor that was independently associated with the removal of normal ovarian tissue with ovarian endometriosis was pre-operative medical treatment. background: The aim of this study was to identify risk factors for the removal of normal ovarian tissue during laparoscopic cystectomy. for endometriosis. methods: A total of 121 patients who had histologically confirmed ovarian endometriosis and 56 control patients who had other histologically. confirmed benign cysts were included for the present analysis. The blocks of removed tissue were sectioned at 120 mm intervals. and a total of five sections were analyzed for each ovarian cyst. Eight variables (age, pre-operative medical treatment, previous surgery for. ovarian endometriosis, single or multiple cysts, size of the largest cyst, side of cyst, co-existence of deep endometriosis, revised American. Society for Reproductive Medicine classification) were evaluated using a generalized linear modeling analysis to identify major factors associated. with the removal of normal ovarian tissue. results: Normal ovarian tissue adjacent to the cyst wall was detected in 71 patients (58.7%) with endometriosis, whereas normal. ovarian tissue was removed from only three patients (5.4%) with other benign cysts. A significant factor that was independently associated. with the removal of normal ovarian tissue with ovarian endometriosis was pre-operative medical treatment. conclusions: The present retrospective, controlled study suggests that pre-operative medical treatment might be a risk factor for the. removal of normal ovarian tissue during laparoscopic cystectomy for ovarian endometriosis. Sachiko Matsuzaki1,2009.")
38
IVF-ICSI outcome in women operated on for bilateral endometriomas.
68 cases (bilat. cystectomy)- 136 controls the number of follicles (P = 0.006), oocytes retrieved (P = 0.024) and embryos obtained (P = 0.024) were significantly lower. The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P = 0.037) CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas. BACKGROUND: The influence of previous conservative surgery for endometriomas on IVF–ICSI outcome is debated. Conflicting information emerging from the literature may be consequent to the fact that endometriomas are mostly monolateral. The contralateral intact ovary may adequately supply for the reduced function of the affected one. To clarify this point, we assess IVF–ICSI outcome in women operated on for bilateral endometriomas. METHODS: Women selected for IVF–ICSI cycles who previously underwent bilateral endometriomas cystectomy were matched (1:2) for age and study period with patients who did not undergo prior ovarian surgery. RESULTS: Sixty-eight cases and 136 controls were recruited. Women operated on for bilateral endometriotic ovarian cysts had a higher withdrawal rate for poor response (P < 0.001). In these patients, despite the use of higher doses of gonadotrophins, the number of follicles (P ), oocytes retrieved (P ) and embryos obtained (P ) were significantly lower. The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P ) and the delivery rate per started cycle was 4% and 17%, respectively (P ). CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas. Edgardo Somigliana1, 2008
- 136 controls. the number of follicles (P = 0.006), oocytes retrieved. (P = 0.024) and embryos obtained (P = 0.024) were significantly lower. The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P = 0.037) CONCLUSIONS: IVF outcome is significantly impaired in women operated on for bilateral ovarian endometriomas. BACKGROUND: The influence of previous conservative surgery for endometriomas on IVF–ICSI outcome is. debated. Conflicting information emerging from the literature may be consequent to the fact that endometriomas. are mostly monolateral. The contralateral intact ovary may adequately supply for the reduced function of the affected. one. To clarify this point, we assess IVF–ICSI outcome in women operated on for bilateral endometriomas. METHODS: Women selected for IVF–ICSI cycles who previously underwent bilateral endometriomas cystectomy. were matched (1:2) for age and study period with patients who did not undergo prior ovarian surgery. RESULTS: Sixty-eight cases and 136 controls were recruited. Women operated on for bilateral endometriotic ovarian cysts. had a higher withdrawal rate for poor response (P < 0.001). In these patients, despite the use of higher doses of gonadotrophins, the number of follicles (P ), oocytes retrieved (P ) and embryos obtained (P ) were. significantly lower. The clinical pregnancy rate per started cycle in cases and controls was 7% and 19% (P ) and the delivery rate per started cycle was 4% and 17%, respectively (P ). CONCLUSIONS: IVF outcome is. significantly impaired in women operated on for bilateral ovarian endometriomas. Edgardo Somigliana1,")
40
P¨ aivi H¨arkki, 2010

43
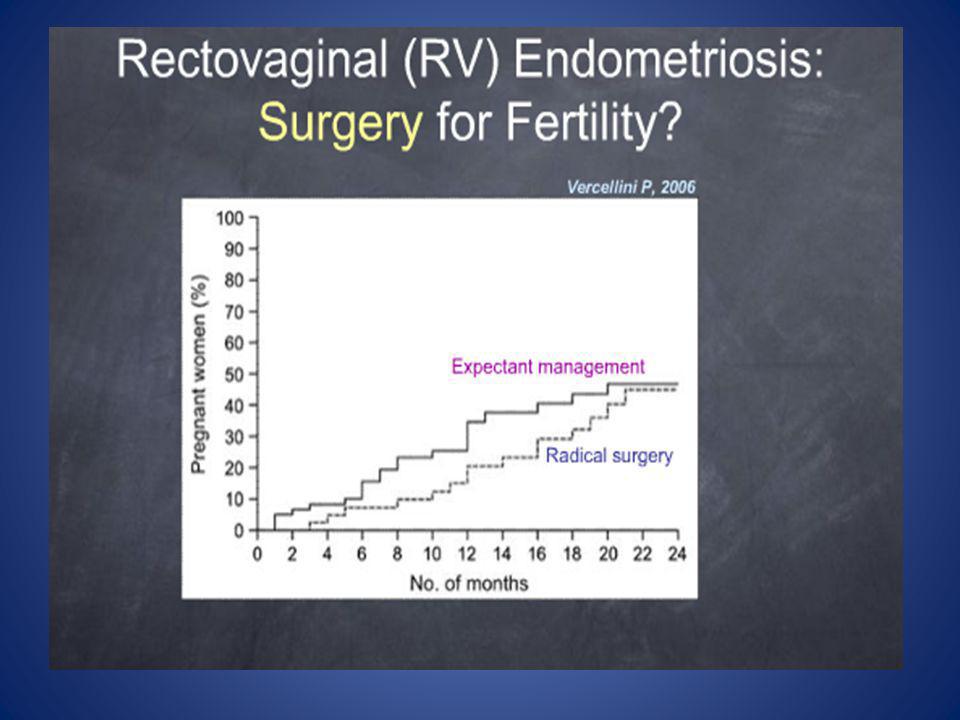
Results of studies comparing IVF-ET with second-line surgery in infertile women with recurrent moderate to severe endometriosis P. Vercellini , 2009

44
Tekrarlayan Endometriozis ve İnfertilite; Cerrahi
Primer cerrahi sonrası spontan gebelik /577 (% 41) Sekonder cerrahi sonrası spontan gebelik /124 (% 23)
 Sekonder cerrahi sonrası spontan gebelik 28/124 (% 23)")
45
Tekrarlayan Endometriozis ve İnfertilite; Cerrahi
Laparotomi ile yapılan cerrahi sonrası spontan gebelik % 12 – 47 (%27) Laparoskopi ile yapılan cerrahi sonrası spontan gebelik % (%25)
 Laparoskopi ile yapılan cerrahi sonrası spontan gebelik % (%25)")
47
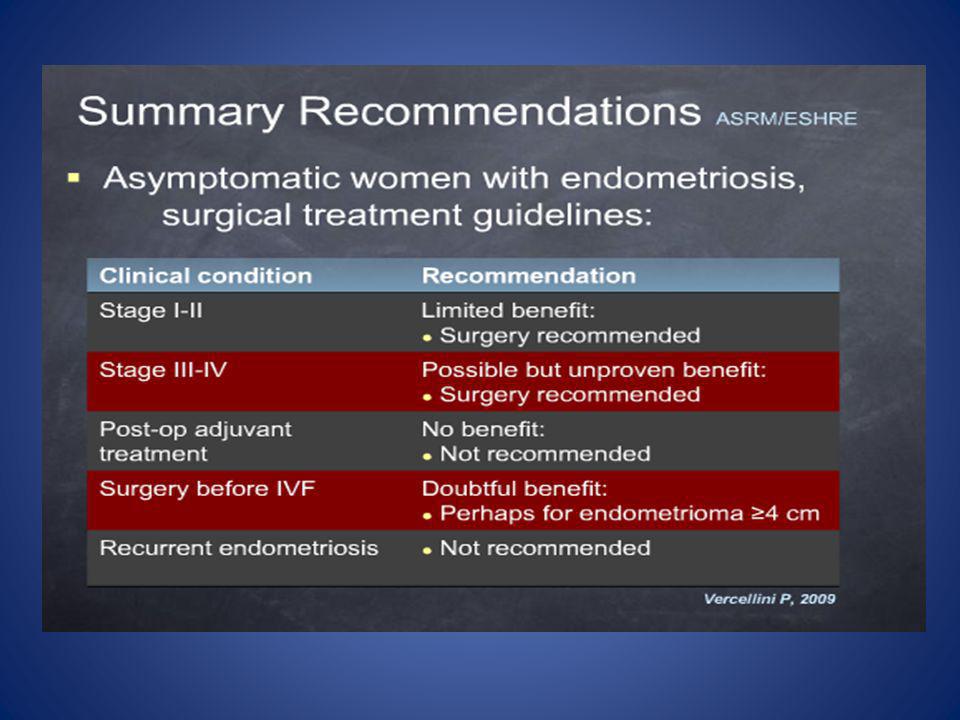
Endometrioma and IVF GPP Laparoscopic ovarian cystectomy is recommended if an ovarian endometrioma ≥4 cm in diameter is present to confirm the diagnosis histologically; reduce the risk of infection; improve access to follicles and possibly improve ovarian response. The woman should be counselled regarding the risks of reduced ovarian function after surgery and the loss of the ovary. The decision should be reconsidered if she has had previous ovarian surgery. 30 June 2007

48
Endometriosis-associated infertility: surgery and IVF, a comprehensive therapeutic approach
825 patients Infertility is a common problem presented by patients with endometriosis. At present, whichever treatment is chosen, half of patients with advanced stages of the disease will remain infertile afterwards. This observational study looked at the reproductive outcome achieved after treating a group of 825 patients aged between 20 and 40 years with endometriosis-associated infertility during the period 2001–2008. Of the 483 patients who had surgery as the primary option, 262 became pregnant (54.2%). Among the patients who did not become pregnant, 144 underwent 184 IVF cycles and 56 additional pregnancies were obtained (30.4% clinical pregnancy rate per retrieval). It is notable that, before any treatment, patients with endometriosis had a poorer ovarian reserve than the control group. The combined strategy of endoscopic surgery and subsequent IVF led to a total of 318 pregnancies, which represents a combined clinical pregnancy rate of 65.8%. This percentage is significantly higher than that obtained with surgery alone (P < ), with 173 patients who were not operated on and who went to IVF as the primary option (P < ) and with 169 patients who had no treatment and achieved 20 spontaneous pregnancies (P < ). Pedro N Barri, 2010
. Among. the patients who did not become pregnant, 144 underwent 184 IVF cycles and 56 additional pregnancies were obtained (30.4% clinical. pregnancy rate per retrieval). It is notable that, before any treatment, patients with endometriosis had a poorer ovarian reserve. than the control group. The combined strategy of endoscopic surgery and subsequent IVF led to a total of 318 pregnancies, which. represents a combined clinical pregnancy rate of 65.8%. This percentage is significantly higher than that obtained with surgery alone. (P < ), with 173 patients who were not operated on and who went to IVF as the primary option (P < ) and with 169. patients who had no treatment and achieved 20 spontaneous pregnancies (P < ). Pedro N Barri,")
49
Does Controlled Ovarian Hyperstimulation in Women with a History of Endometriosis Influence Recurrence Rate? retrospective cohort study of 592 patients submitted to laparoscopy for endometriosis, 177 with infertility-related endometriosis who underwent a periodic ultrasound follow-up after laparoscopy were selected. Women who started ART after laparoscopy (n90) were compared with the control group, who did not undergo ART (n87). Recurrence of endometriosis was defined as the presence of endometriotic lesions observed through TV-US. During a long-term TV-US follow-up (1–15 years), 40 (22.6%) recurrences were observed. Patients submitted to ART showed a cumulative recurrence rate similar to that of the control group (28.6% and 37.9% respectively, p0.471). Background: Endometriosis is a common estrogen-dependent disease. The aim of this study was to assess whether controlled ovarian hyperstimulation (COH) for assisted reproductive technology (ART) was associated with an increased incidence in endometriosis recurrence as documented by transvaginal ultrasound (TV-US). Methods: In a retrospective cohort study of 592 patients submitted to laparoscopy for endometriosis, 177 with infertility-related endometriosis who underwent a periodic ultrasound follow-up after laparoscopy were selected. Women who started ART after laparoscopy (n¼90) were compared with the control group, who did not undergo ART (n¼87). Recurrence of endometriosis was defined as the presence of endometriotic lesions observed through TV-US. Results: During a long-term TV-US follow-up (1–15 years), 40 (22.6%) recurrences were observed. Patients submitted to ART showed a cumulative recurrence rate similar to that of the control group (28.6% and 37.9% respectively, p¼0.471). Recurrent lesions were ovarian cysts (47.5%), ovarian nodules (37.5%), and rectovaginal disease (15%). The stratified analysis based on stages of endometriosis and pelvic pain did not show differences. Conclusions: Gonadotropin treatments do not seem to affect the natural history of endometriotic lesions. The most important prognostic factors in recurrent disease observed by TV-US seem to be the stage of endometriosis and the presence of pelvic pain at the time of the first laparoscopic treatment. Maria Elisabetta Coccia, 2010
 were compared with the control group, who did not undergo ART (n87). Recurrence of endometriosis was defined as the presence of endometriotic lesions observed through TV-US. During a long-term TV-US follow-up (1–15 years), 40 (22.6%) recurrences were observed. Patients submitted to ART showed a cumulative recurrence rate similar to that of the control group (28.6% and 37.9% respectively, p0.471). Background: Endometriosis is a common estrogen-dependent disease. The aim of this study was to assess. whether controlled ovarian hyperstimulation (COH) for assisted reproductive technology (ART) was associated. with an increased incidence in endometriosis recurrence as documented by transvaginal ultrasound (TV-US). Methods: In a retrospective cohort study of 592 patients submitted to laparoscopy for endometriosis, 177 with. infertility-related endometriosis who underwent a periodic ultrasound follow-up after laparoscopy were selected. Women who started ART after laparoscopy (n¼90) were compared with the control group, who did not. undergo ART (n¼87). Recurrence of endometriosis was defined as the presence of endometriotic lesions observed. through TV-US. Results: During a long-term TV-US follow-up (1–15 years), 40 (22.6%) recurrences were observed. Patients. submitted to ART showed a cumulative recurrence rate similar to that of the control group (28.6% and 37.9% respectively, p¼0.471). Recurrent lesions were ovarian cysts (47.5%), ovarian nodules (37.5%), and rectovaginal. disease (15%). The stratified analysis based on stages of endometriosis and pelvic pain did not show differences. Conclusions: Gonadotropin treatments do not seem to affect the natural history of endometriotic lesions. The. most important prognostic factors in recurrent disease observed by TV-US seem to be the stage of endometriosis. and the presence of pelvic pain at the time of the first laparoscopic treatment. Maria Elisabetta Coccia,")
50
Soru SART sonuclarına göre endometriozisli olgularda canlı doğum oranları nedir ? ( ) 18-22 25-28 32-34 38-41 45-47 Cevap C

51
SART-2005

52
SART-2006

53
SART-2007

54
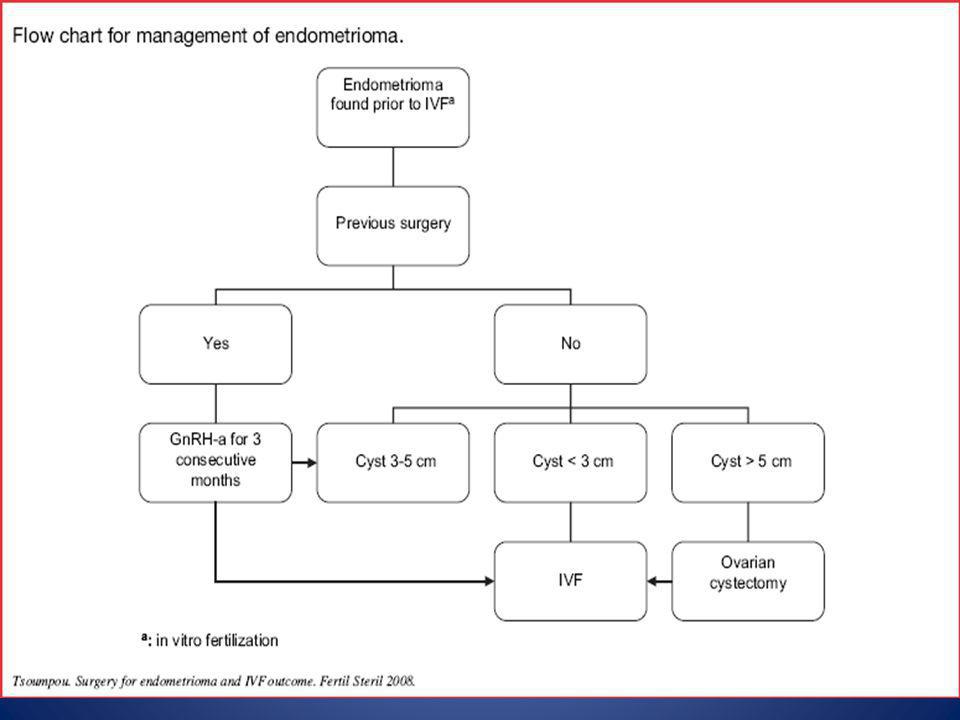
Algorithm for management of infertility associated with endometriosis
Dominique de Ziegler,, 2010

55
ŞG 37 y, 3yıldır pr infertilite
Sol overde 6 cm end’oma+ male faktör(3mil/ml+%10+%37) FSH:10 Op vs ART anlatıldı. Hasta önce ART’yi tercih etti. Nisan’08 Hybrid px; 300IU FSH+ 2 amp HMG step down, 11 gün stimülasyon, 7 oosit 5 MII 5x 2pn, 2. gün 5 ET ( grade 1) Sonuç(+) tekil gebelik, 38 GH SCA, 2850 gr, E
 FSH:10. Op vs ART anlatıldı. Hasta önce ART’yi tercih etti. Nisan’08 Hybrid px; 300IU FSH+ 2 amp HMG step down, 11 gün stimülasyon, 7 oosit 5 MII 5x 2pn, 2. gün 5 ET ( grade 1) Sonuç(+) tekil gebelik, 38 GH SCA, 2850 gr, E.")
57
EÇ 29y, 5 yıldır pr infertilite
Dismenore+, dyspareni+, kr pelvik ağrı+ Kasım’05de L/S, Evre IV end’zis; Adezyolizis ve sağ overden5 cm end’oma ekstirpasyonu. Şubat’06 Antg px 3 MII 3x2pn, 2. gün 3 ET sonuç(-) Mayıs’06 Antg px 5 MII, 2. gün 2 ET Sonuç(-) Temmuz’06 da her iki overde loküller halinde 3-4 cm boyutunda multipl end’oma odakları izleniyor. Geri kalan over rezervi grade 2
 Mayıs’06 Antg px 5 MII, 2. gün 2 ET Sonuç(-) Temmuz’06 da her iki overde loküller halinde 3-4 cm boyutunda multipl end’oma odakları izleniyor. Geri kalan over rezervi grade 2.")
59
2 ay depo GnRH analog tx - Eylül’06 da mikrodoz px, 15 oosit, 15 MII,7x 2pn 3.gün 4 ET sonuç negatif -Ocak ‘07 de Antg px ( 2 ay GnRH analog tx yi takiben) 12 oosit, 12 MII 9x2pn 3. Gün 4ET sonuç(+) 33. Haftada dikor-diamn ikiz gebelik , Pl.previa , 2095gr kız/ 1885 gr kız bebek SCA ile doğurdu.
 12 oosit, 12 MII 9x2pn 3. Gün 4ET sonuç(+) 33. Haftada dikor-diamn ikiz gebelik , Pl.previa , 2095gr kız/ 1885 gr kız bebek SCA ile doğurdu.")
60
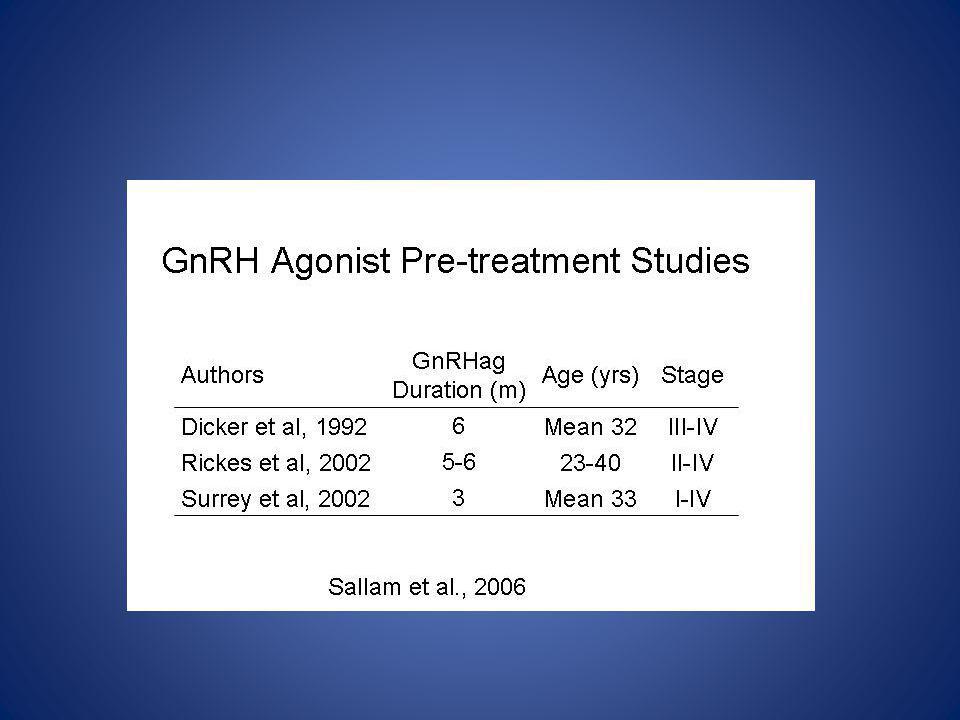
Endometriosis-GnRHa Before IVF Pain After operation for the prevention
Empirical

64
Sallam et al, Cochrane Database Syst Rev 25;(1):CD004635, 2006
GnRH agonist v/s no agonist before IVF (Clinical pregnancy rate per woman) Sallam et al, Cochrane Database Syst Rev 25;(1):CD004635, 2006
 Sallam et al, Cochrane Database Syst Rev 25;(1):CD004635,")
66
Use of oral contraceptives in women with endometriosis before assisted reproduction treatment improves outcomes In women with endometriosis, including those with endometriomas, 6 to 8 weeks of continuous use of oral contraception (OC) before assisted reproduction treatment (ART) maintains ART outcomes comparable with the outcomes of age-matched controls without endometriosis. In contrast, ART outcomes are markedly compromised in endometriosis patients who are not pretreated with OC. Ovarian responsiveness to stimulation was not altered by 6 to 8 weeks’ use of pre-ART OC, including in poor responders with endometriomas Dominique de Ziegler, 2010
 before assisted reproduction treatment (ART) maintains ART outcomes comparable with the outcomes of age-matched controls without endometriosis. In contrast, ART outcomes are markedly compromised in endometriosis patients who are not pretreated with OC. Ovarian responsiveness to stimulation was not altered by 6 to 8 weeks’ use of pre-ART OC, including in poor responders with endometriomas. Dominique de Ziegler,")
67
Cryopreservation of oocytes in a young woman with severe and symptomatic endometriosis: a new indication for fertility preservation. 2009 25 y, symptomatic endometriosis, one ovary, low AFC, 3 Cycles, 21 Oocytes OBJECTIVE: To report a new indication for fertility preservation. DESIGN: Case report. SETTING: Academic teaching hospital. PATIENT(S): A 25-year-old nulliparous woman with severe and symptomatic endometriosis and low antral follicular count. INTERVENTION(S): Oocyte cryopreservation. MAIN OUTCOME MEASURE(S): Number of cryopreserved oocytes. RESULT(S): After three cycles of ovarian stimulation, we cryopreserved 21 oocytes. CONCLUSION(S): We recommend fertility preservation as part of preoperative counseling in young women with severe endometriosis.
: A 25-year-old nulliparous woman with severe and symptomatic endometriosis and low antral follicular count. INTERVENTION(S): Oocyte cryopreservation. MAIN OUTCOME MEASURE(S): Number of cryopreserved oocytes. RESULT(S): After three cycles of ovarian stimulation, we cryopreserved 21 oocytes. CONCLUSION(S): We recommend fertility preservation as part of preoperative counseling in young women with severe endometriosis.")
68
Soru Derin endometriozisli olgularda infertilite oranı ne kadardır ? (%) 2 10 25 40 60 Cevap B
 Cevap B")
69
Deep Endometriosis: Symptoms
OBJECTIVE: To examine the short-term surgical outcomes in women undergoing fertility-sparing laparoscopic excision of deeply infiltrating pelvic endometriosis. DESIGN: Retrospective cohort study. SETTING: Tertiary referral center for treatment of endometriosis, a university teaching hospital, London, United Kingdom. PATIENT(S): A total of 177 women who underwent fertility-sparing laparoscopic excision of deeply infiltrating endometriosis between January 1, 2006, and December 31, INTERVENTION(S): Eligible women were identified from the surgeons' database, and their medical notes were reviewed. Data from preoperative assessment, surgery, and postoperative outcomes were analyzed. MAIN OUTCOME MEASURE(S): Complication rate. RESULT(S): One hundred seventy-seven women underwent fertility-sparing laparoscopic excision of deeply infiltrating endometriosis including excision of uterosacral ligaments (43, 24.3%), excision of rectovaginal septum (56, 31.6%), rectal shave (56, 31.6%), disk excision (7, 4%) or bowel resection (15, 8.5%). The median operative time was 95 minutes with a range of 30 to 270 minutes (interquartile range minutes). Overall, complications developed in 18 women (10.2%). In 12 (6.8%) of these only uncomplicated pyrexia developed whereas significant intraoperative and/or postoperative complications developed in the remaining 6 (3.4%). Women spent a median of 2 days recovering in hospital (range 1-7, interquartile range 2-3 days). CONCLUSION(S): Fertility-sparing laparoscopic excision of deeply infiltrating endometriosis appears to be safe with a low short-term complication rate. Pandis GK, 2010
: A total of 177 women who underwent fertility-sparing laparoscopic excision of deeply infiltrating endometriosis between January 1, 2006, and December 31, INTERVENTION(S): Eligible women were identified from the surgeons database, and their medical notes were reviewed. Data from preoperative assessment, surgery, and postoperative outcomes were analyzed. MAIN OUTCOME MEASURE(S): Complication rate. RESULT(S): One hundred seventy-seven women underwent fertility-sparing laparoscopic excision of deeply infiltrating endometriosis including excision of uterosacral ligaments (43, 24.3%), excision of rectovaginal septum (56, 31.6%), rectal shave (56, 31.6%), disk excision (7, 4%) or bowel resection (15, 8.5%). The median operative time was 95 minutes with a range of 30 to 270 minutes (interquartile range minutes). Overall, complications developed in 18 women (10.2%). In 12 (6.8%) of these only uncomplicated pyrexia developed whereas significant intraoperative and/or postoperative complications developed in the remaining 6 (3.4%). Women spent a median of 2 days recovering in hospital (range 1-7, interquartile range 2-3 days). CONCLUSION(S): Fertility-sparing laparoscopic excision of deeply infiltrating endometriosis appears to be safe with a low short-term complication rate. Pandis GK,")
70
Deep endometriosis: Excisional surgery Pregnancy rates
Vercellini et al., Hum Reprod (2009)
")
72
Fertility and clinical outcome after bowel resection in infertile women with endometriosis
62 infertile women who underwent laparoscopic excision of endometriosis with segmental bowel resection performed for severe intestinal symptoms. Among women younger than 30 years trying to conceive spontaneously, the cumulative pregnancy rate was 58% and the cumulative pregnancy rate was 45% in those aged 30–34 years. Bowel resection for endometriosis improves pain symptoms and quality of life in symptomatic women. However, little is known about fertility after surgery, particularly after such treatment in women suffering from infertility. The aim of the present study was to evaluate post-operative fertility and long-term clinical outcome after laparoscopic colorectal resection for endometriosis in infertile women. This study reports clinical outcomes in 62 infertile women who underwent laparoscopic excision of endometriosis with segmental bowel resection performed for severe intestinal symptoms. Among women younger than 30 years trying to conceive spontaneously, the cumulative pregnancy rate was 58% and the cumulative pregnancy rate was 45% in those aged 30–34 years. The total pain recurrence was 9.7% (six cases) and endometriosis recurrence was diagnosed by ultrasound in 14.5% (nine cases) during the follow-up period. Four of these patients needed further surgery because of severe symptoms. The surgical treatment of bowel endometriosis seems to improve pain symptoms and patients’ satisfaction rates, and it could also be indicated in infertile women. Anna Stepniewska, 2010
 and endometriosis recurrence was diagnosed by ultrasound in 14.5% (nine. cases) during the follow-up period. Four of these patients needed further surgery because of severe symptoms. The surgical treatment. of bowel endometriosis seems to improve pain symptoms and patients’ satisfaction rates, and it could also be indicated in. infertile women. Anna Stepniewska,")
73
Results of first in vitro fertilization cycle in women with colorectal endometriosis compared with those with tubal or male factor infertility This retrospective study of women undergoing IVF (29 with colorectal endometriosis, 157 with tubal factor infertility, and 340 with male factor infertility) found similar fertility outcomes between the groups In conclusion, our results indicate that fertility outcomes after one cycle of IVF in women with colorectal endometriosis are similar to those of patients with tubal or male factor infertility. Hence, women with colorectal endometriosis and a desire to become pregnant should be encouraged to consider IVF before undergoing colorectal resection Emmanuelle Mathieu d’Argent, 2010
 found similar fertility outcomes between the groups. In conclusion, our results indicate that fertility outcomes after. one cycle of IVF in women with colorectal endometriosis are similar. to those of patients with tubal or male factor infertility. Hence, women with colorectal endometriosis and a desire to become pregnant. should be encouraged to consider IVF before undergoing. colorectal resection. Emmanuelle Mathieu d’Argent,")
74
Deep endometrisois: Complications
Vercellini et al., Hum Reprod (2009)
")
75
Endometrioma ve oosit toplanması
Hacim artması Enfeksiyon, abse Akut abdomen Toksik etki Malignite

76
Endometrioma and oocyte retrieval–induced pelvic abscess: a clinical concern or an exceptional complication The authors evaluated the risk of developing a pelvic abscess in a series of 214 in vitro fertilization cycles that were performed in women with endometriomas. This complication was never recorded, indicating that its risk is very low (0.0; 95% confidence interval, 0.0–1.7%). Literature nine cases were described. Prophylactic antibiotics have been administered in at least eight cases. The endometrioma was punctured at the time of oocyte retrieval in at least six cases. The authors evaluated the risk of developing a pelvic abscess in a series of 214 in vitro fertilization cycles that were performed in women with endometriomas. This complication was never recorded, indicating that its risk is very low (0.0; 95% confidence interval, 0.0–1.7%). Laura Benaglia, 2008
. Literature. nine cases were described. Prophylactic antibiotics have been administered in at least eight cases. The endometrioma was punctured at the time of oocyte retrieval in at least six cases. The authors evaluated the risk of developing a pelvic abscess in a series of 214 in vitro fertilization cycles that. were performed in women with endometriomas. This complication was never recorded, indicating that its risk. is very low (0.0; 95% confidence interval, 0.0–1.7%). Laura Benaglia,")
77
Shavi Fernando, 2009 Preterm birth, ovarian endometriomata, and assisted reproduction technologies Objective: To report preterm birth and small for gestational age (SGA) rates from assisted reproduction technologies (ART) patients with ovarian endometriomata compared with control groups. Design: Retrospective cohort study. Setting: Tertiary university affiliated ART center and Perinatal Data Collection Unit (PDCU). Patient(s): Every woman who had an ART singleton baby born between 1991 and 2004 had her database record assessed (N ¼4382). Control groups included 1201 singleton babies from ART patients without endometriosis and 2400 randomly selected women from the PDCU database of 850,000 births. Intervention(s): There were 95 singleton ART babies from patients with ovarian endometriomata and 535 ART singleton babies from patients who had endometriosis but no ovarian endometriomata. Main Outcome Measure(s): Preterm birth rates and SGA birth rates. Result(s): Preterm birth rate increased only in the ovarian endometriomata group when compared with community birth records (n ¼ 850,000). Furthermore, ART patients with ovarian endometriomata had a statistically significantly increased likelihood of having a SGA baby when compared with other forms of endometriosis. Conclusion(s): Rates of preterm birth and SGA babies doubled in infertility patients with ovarian endometriomata who required ART. In a nationwide Swedish study including 1,442,675 singleton births, the association between adverse pregnancy outcome, ART, and previous diagnosis of endometriosis was assessed.49 In this study, 11.9% of patients with endometriosis had conceived after ART. The risk of preterm birth in women with endometriosis was elevated (adjusted OR 1.33; 95% CI 1.23–1.44). In patients with endometriosis, the risk of pretermbirth was 1.24 (95% CI 0.99–1.57) if pregnancy was induced with ART, and 1.37 (95% CI 1.25–1.50) if pregnancy started spontaneously; thus, ART was not associated with an elevated risk forpretermbirthinpatientswith endometriosis. Womenwith endometriosiswere more often subject to antepartal bleeding/placental complications, preeclampsia, and Caesarean section. There was no association between endometriosis and risk of small-for-gestational-age (SGA) birth or stillbirth. The authors concluded that endometriosis appears to be a risk factor for preterm birth, irrespective of the use of ART.49. Stephansson, O., H. Kieler, F. Granath, et al Endometriosis, assisted reproduction technology, and risk of adverse pregnancy outcome. Hum. Reprod. 24: 2341– 2347. 50. Fernando, S., S. Breheny, A.M. Jacques, et al Preterm birth, ovarian endometriomata, and assisted reproduction technologies. Fertil. Steril. 91: 325–330.
 rates from assisted reproduction technologies. (ART) patients with ovarian endometriomata compared with control groups. Design: Retrospective cohort study. Setting: Tertiary university affiliated ART center and Perinatal Data Collection Unit (PDCU). Patient(s): Every woman who had an ART singleton baby born between 1991 and 2004 had her database record. assessed (N ¼4382). Control groups included 1201 singleton babies from ART patients without endometriosis and randomly selected women from the PDCU database of 850,000 births. Intervention(s): There were 95 singleton ART babies from patients with ovarian endometriomata and 535 ART. singleton babies from patients who had endometriosis but no ovarian endometriomata. Main Outcome Measure(s): Preterm birth rates and SGA birth rates. Result(s): Preterm birth rate increased only in the ovarian endometriomata group when compared with community. birth records (n ¼ 850,000). Furthermore, ART patients with ovarian endometriomata had a statistically significantly. increased likelihood of having a SGA baby when compared with other forms of endometriosis. Conclusion(s): Rates of preterm birth and SGA babies doubled in infertility patients with ovarian endometriomata. who required ART. In a nationwide Swedish study including. 1,442,675 singleton births, the association between. adverse pregnancy outcome, ART, and previous diagnosis. of endometriosis was assessed.49 In this. study, 11.9% of patients with endometriosis had. conceived after ART. The risk of preterm birth in. women with endometriosis was elevated (adjusted. OR 1.33; 95% CI 1.23–1.44). In patients with endometriosis, the risk of pretermbirth was 1.24 (95% CI 0.99–1.57) if pregnancy was induced with ART, and 1.37 (95% CI 1.25–1.50) if pregnancy started. spontaneously; thus, ART was not associated with. an elevated risk forpretermbirthinpatientswith endometriosis. Womenwith endometriosiswere more. often subject to antepartal bleeding/placental complications, preeclampsia, and Caesarean section. There was no association between endometriosis. and risk of small-for-gestational-age (SGA) birth or. stillbirth. The authors concluded that endometriosis. appears to be a risk factor for preterm birth, irrespective of the use of ART.49. Stephansson, O., H. Kieler, F. Granath, et al Endometriosis, assisted reproduction technology, and risk. of adverse pregnancy outcome. Hum. Reprod. 24: 2341– Fernando, S., S. Breheny, A.M. Jacques, et al Preterm. birth, ovarian endometriomata, and assisted reproduction. technologies. Fertil. Steril. 91: 325–330.")
78
Sorular ve cevaplar Evre I-II Endometriozis infertilite nedeni mi
Evet Endometrioziste KOH+IUI etkin mi I-II de etkin III-IV de yeri yok Endometriozis over rezervini azaltıyor mu Derin endometriozis infertilite nedeni mi Endometriozis düşük riskini arttırıyor mu Hayır

79
Sorular ve cevaplar Endometriozis IVF sonuclarina etkili mi
Etkili değil (ileri evre ?) Endometrioma varlığı fertiliteyi etkiliyor mu değiştirmiyor Ivf oncesi endometrioma cerrahisi ivf sonuçları etkiliyor mu Değiştirmiyor (azalmış over rezervi ) IVF endometriozis rekürrensini arttırıyor mu Hayır Başarısız IVF sonrası cerrahi faydalı mı Hayır (Bazı olgularda)
 Endometrioma varlığı fertiliteyi etkiliyor mu. değiştirmiyor. Ivf oncesi endometrioma cerrahisi ivf sonuçları etkiliyor mu. Değiştirmiyor (azalmış over rezervi ) IVF endometriozis rekürrensini arttırıyor mu. Hayır. Başarısız IVF sonrası cerrahi faydalı mı. Hayır (Bazı olgularda)")
80
Sorular ve cevaplar IVF oncesi depo GnRHa faydalı mı
Etkili gibi ama daha çok çalışmaya gerek var Endometrioma varlığında ovum toplanmasında risk var mı yok Tekrarlayan endometriomanın yönetim (Cerrahi vs. ivf) İvf Hangi protokol Fark yok Ne zaman IVF Olguya göre değişir
 İvf. Hangi protokol. Fark yok. Ne zaman IVF. Olguya göre değişir.")
Benzer bir sunumlar