Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
TÜBERKÜLOZ ELİMİNASYON
Prof.Dr.Zeki KILIÇASLAN İ.Ü.İstanbul Tıpa Fakültesi.

2
that should take us towards the achievable goal of TB elimination.
No one ever said this would be an easy fight. However, with the Global Plan to Stop TB 2011–2015 the direction is set with renewed intensity in care and control efforts, and new approaches and tools finally becoming available. We are now at the start of a road that should take us towards the achievable goal of TB elimination. Mario Raviglione Director, WHO Stop TB Department

3
DSÖ’nün önerdiği TB kontrol stratejisi - DOTS
Politik ve finans konusunda kararlılık. Balgam mikroskopik muayenesi ve TB şüphelilerde kültür. Doğrudan gözetimli ve standart kısa süreli anti-TB ilaç rejimleri. Bütün esas anti-TB ilaçların düzenli ve kesintisiz olarak sağlanması. Standardize kayıt ve raporlama sistemi. Bugünkü modern TB Kontrol stratejisi 1990’lar da başladı.. TB Register World Health Organization Regional Office for Europe 2. World Health Organization. Forty-fourth World Health Assembly. Geneva:World Health Organization, 1991.

4
DOTS DOTS stratejisinin 184 ülkede uygulanması ile
132 milyon hastaya tedavi verildi ve bunların 125 milyonu kür edildi. 4. World Health Organization. Global Tuberculosis Control. Geneva: World Health Organization, 2008.

5
Full implementation of Global Plan: 2015 MDG
target reached but TB not eliminated by 2050 1 10 100 1000 10000 2000 2010 2020 2030 2040 2050 Year Incidence/million/yr Elimination 16%/yr Global Plan 6%/yr Current trajectory 1%/yr Elimination target: 1 / million / year by 2050 TB incidence 10x lower than today, but >100x higher than elimination target in 2050 Current rate of decline

6
Stop TB Partnership. The Global Plan to Stop TB 2006–2015
Stop TB Partnership. The Global Plan to Stop TB 2006–2015. Geneva: World Health Organization, 2006.

8
DOTS STOP TB STRATEJİ:

9
Stop TB Stratejisinin hedefleri ;
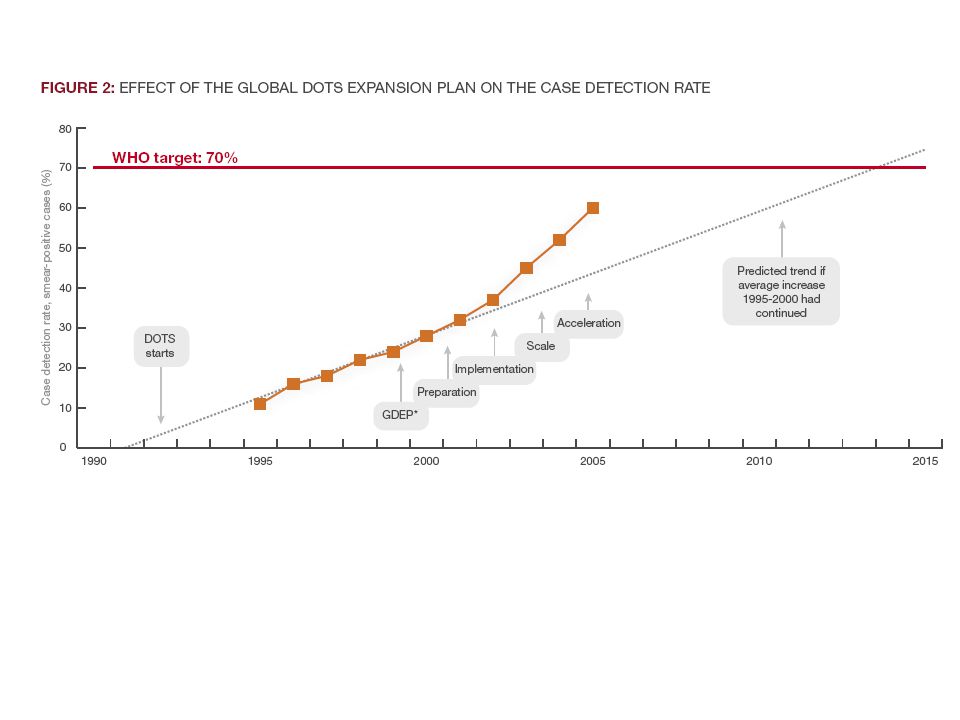
yılında beklenen olguların en az % 70’ini bulmak ve bunların en az % 85’ ini kür etmek (% 84 ile kür hedefine ulaşılmasına rağmen beklenen oluların dünya ölçüsünde ancak % 60’ı yakalanabilmiştir (1) yılında 1990 yılına göre TB prevelansını ve TB’a bağlı ölümleri % 50 azaltmak, Prevelansı de 155’e ölümü de 14’ e indirmek. yılında Dünyada TB eliminasyonunu sağlamak (< 1/ )
 yılında 1990 yılına göre TB prevelansını ve TB’a bağlı ölümleri % 50 azaltmak, Prevelansı de 155’e ölümü de 14’ e indirmek yılında Dünyada TB eliminasyonunu sağlamak (< 1/ )")
10
Stop TB Stratejisinin Temel Uygulamaları:
Yüksek kalitede DOTS uygulamalarının yaygınlaştırılması. HIV/TB, ÇİD-TB ve diğer sorunlara yönelmek. Genel sağlık sistemlerinin güçlendirilmense katkı yapmak. Kamu ve özel tüm hizmet sunucular ile işbirliği sağlanması. TB hastalarının ve toplumun TB kontrol programlarına aktif katılımının desteklenmesi. Yeni tanı araçları, ilaç ve aşı geliştirilmesi için araştırmalar yapılması.

11
Global TB Eliminasyonunu Zorlaştıran Faktörler
TB bulaşmasını/ hastalığını önleme TB Yönetim Sistemi Gerekli Fonların Elde Edilmesi. Epidemiology and Challenges to the Elimination of Global Tuberculosis Mandeep S. Jassal1 and William R. Bishai2.Clinical Infectious Diseases 2010; 50(S3):S156–S164
:S156–S164.")
12
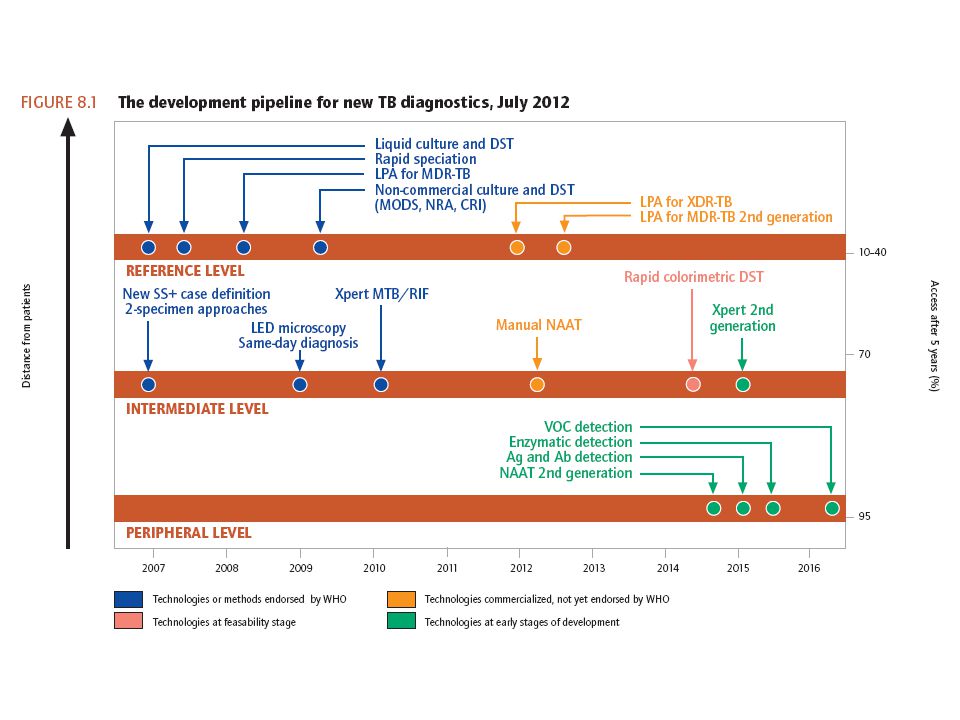
a) Daha iyi tanı araçları
TB hastalığını önleme a) Daha iyi tanı araçları Olgu bulama hızında hedefe varılamadı. HIV Pozitifler Akciğer Dışı TB
 Daha iyi tanı araçları. Olgu bulama hızında hedefe varılamadı. HIV Pozitifler. Akciğer Dışı TB.")
13
ÇİD-TB için Line Probe Assays.
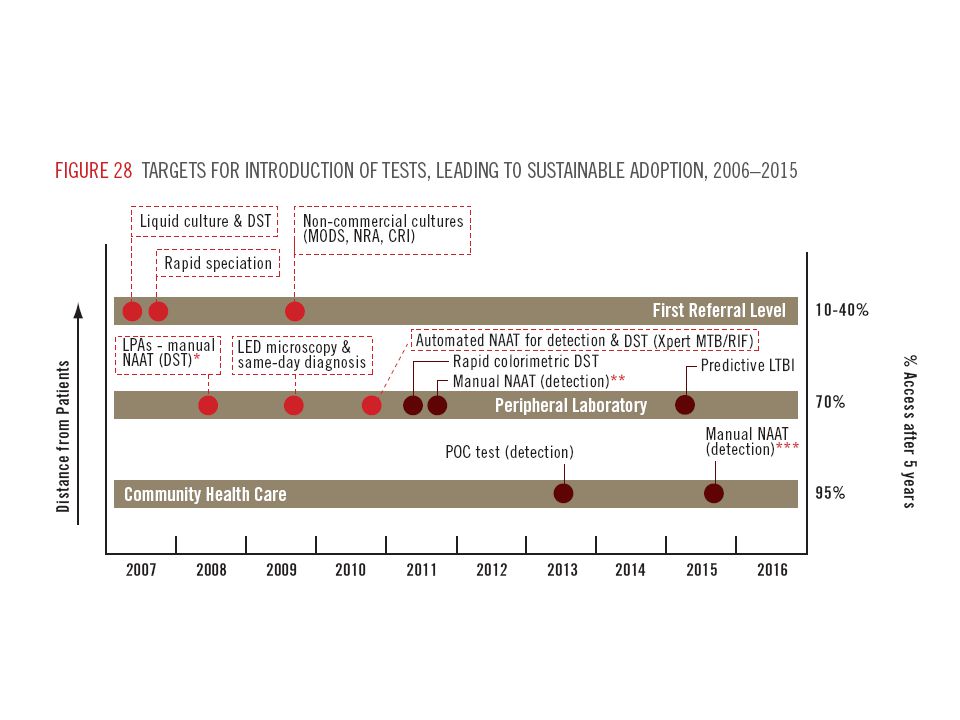
Son yıllarda DSÖ’ nün Tanı için yeni yaklaşım ve test yeni yaklaşım önerileri. Sıvı besiyerleri ÇİD-TB için Line Probe Assays. LED mikroskopi. Xpet MTB/RIF Hızlı tanı ve RİF-direnç yöntemi

18
Population Attributable Fraction
TB hastalığını önleme b) Genel sağlık sorunları ve sosyal riskler için; Etkin ulusal sağlık stratejileri TB Risk faktörleri TB Rölatif risk Prevelans (22 HBCs) Population Attributable Fraction HIV Infection 8.3 1.1% 7% Malnutrition 4.0 17.2% 34% Diabetes 3.0 3.4% 6% Alcohol Use (>40g / d) 2.9 7.9% 13% Active Smoking 2.6 18.2% 23% Indoor Air Pollution 1.5 71.1% 26%
 Genel sağlık sorunları ve sosyal riskler için; Etkin ulusal sağlık stratejileri. TB Risk faktörleri. TB Rölatif risk. Prevelans. (22 HBCs) Population Attributable Fraction. HIV Infection % 7% Malnutrition % 34% Diabetes % 6% Alcohol Use (>40g / d) % 13% Active Smoking % 23% Indoor Air Pollution % 26%")
19
TB hastalığını önleme enfeksiyonun bulaşmasını
c) Toplumda sağlık kurumlarında enfeksiyonun bulaşmasını önlemek için gerekli politikalar Etkili vantilasyon ve maske kullanımı ile sağlık kurumlarında bulaşma çok ileri derecede azaltılabilir !
 Toplumda sağlık kurumlarında. enfeksiyonun bulaşmasını. önlemek için gerekli politikalar. Etkili vantilasyon ve maske. kullanımı ile sağlık kurumlarında. bulaşma çok ileri derecede. azaltılabilir !")
20
2. TB Yönetim Konuları a)DOTS stratejisine özel ve sivil toplum organizasyonlarının katılımı b) İlaç direnci gelişimini engelleyecek güçlü TB programı Fon gereksinimi-Çin/Hindistan c)TB hastaları içinde HIV enfeksiyonun erken tanınması Trimethoprim-sulfamethoxazole. d) HIV hastaları içinde erken TB tanısı
 İlaç direnci gelişimini engelleyecek güçlü TB programı. Fon gereksinimi-Çin/Hindistan. c)TB hastaları içinde HIV enfeksiyonun erken tanınması. Trimethoprim-sulfamethoxazole. d) HIV hastaları içinde erken TB tanısı.")
22
2. TB Yönetim Konuları HIV infekte kişilerin sadece % 1’ de INH profilaksisi alıyor ! Düşük ve orta gelirli ülkelerde temaslı taraması ve risklilerde koruyucu tedavi etkili olarak kullanılmalıdır (*) *Morrison J, Pai M, Hopewell. Tuberculosis and latent tuberculosis infection in close contacts of people with pulmonary tuberculosis in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis 2008; 8:359–368.
 *Morrison J, Pai M, Hopewell. Tuberculosis and latent tuberculosis infection in close contacts of people with pulmonary tuberculosis in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis 2008; 8:359–368.")
26
3. TB Kontrolü Bütçe Sorunu

28
2011-2015 Gereken her yıl 8 Milyar $ Bulunan her yıl 4.8 Milyar$
2015’ e kadar her yıl 2-3 Milyar $ gerekli

29
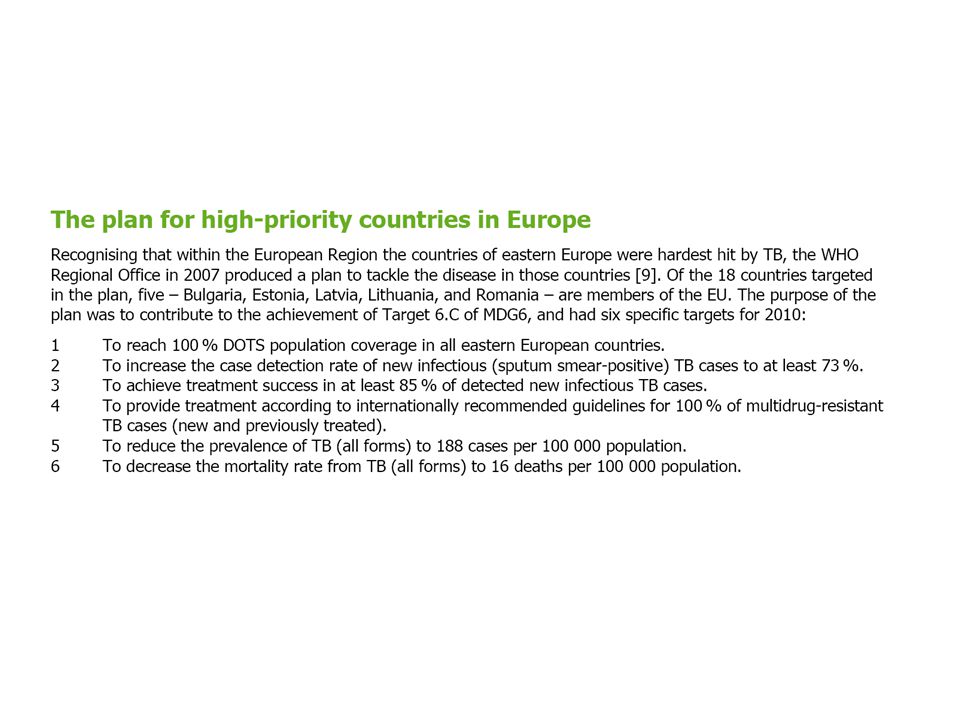
Avrupa’ da TB Eliminasyonu
1980’ ler de Avrupa’ da bazı ülkelerin yıllarında eliminasyona Ulaşacağına inanıyorlardı. 1989, Styblo bunun düşük insidanslı ülkelerde bile 35-50 yıl alacağını hesapladı. Styblo K. Rev Infect Dis Mar-Apr;11 Suppl 2:S339-

31
TB Eliminasyon fazında ülke;
Bir çok Avrupa ülkesinde TB insidansı < 20/ Bu ülkeler gayretlerini Tüberkülozu elimine etme amacı doğrultusunda yoğunlaştırmalıdırlar. TB Eliminasyon fazında ülke; TB olgu bildirim hızı < 20/ ve TB olgu hızlarında son 5 yıldır kesintisiz azalma olan ülkeler

32
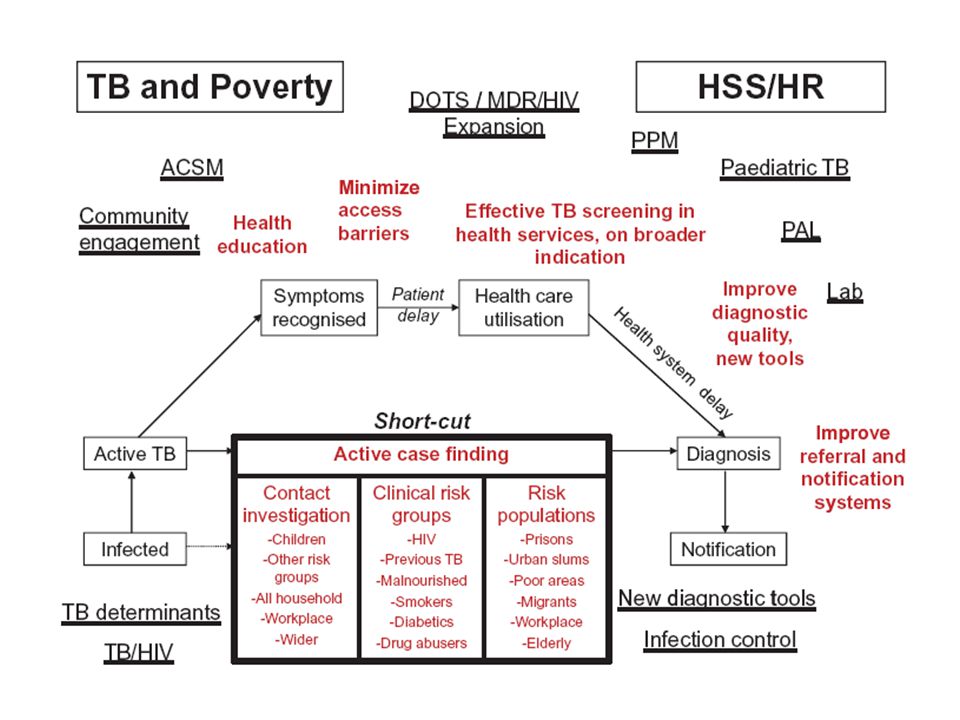
TB Bulaşma hızını ölçmek
Bir toplumda olgu hızı azaldıkça ülkede hastalığın bulaşma düzeyini ortaya koymakta daha önemli hale gelir. Bulaşma hızını doğrudan ölçmek için geçerli test yok. Bulaşma hızını dolaylı ölçmekte kullanılan dört parametre. TB Hasta bildirim hızının eğilimi ÇİD-TB bildirim hızı eğilimi Bildirilen Çocuk TB/Erişkin TB oranının eğilimi TB olgularının ortalama yaş eğilimi. Sürveyans sistemi olguların % 100 ‘nü kapsıyor mu ? Sürveyans sisteminin olguları kapsama gücünde değişim oluyor mu?

33
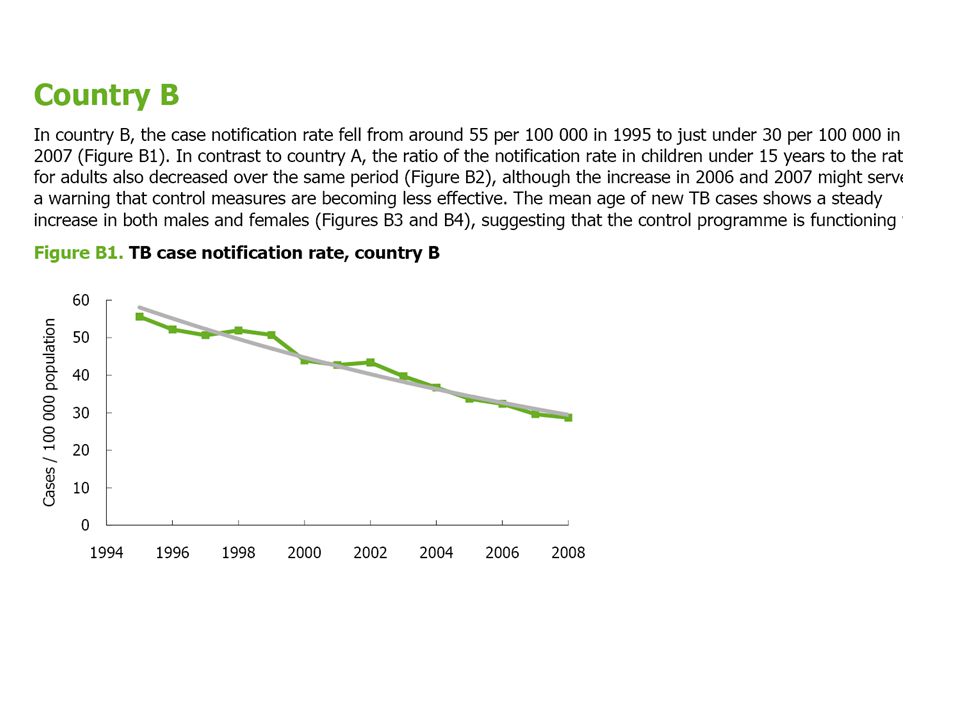
İndikatör 1. TB Hasta bildirim hızının eğilimi
Bir yılda bildirilen TB sayısı x Ülkenin toplam nüfusu Hedef: TB olgu bildirim hızındaki 5 yıllık ortalama azalış trendi önceki 5 yılın üzerinde Olgu saptama hızının yüksek olduğu toplumlarda hastalığın gidişi üzerine anlamlı bilgi sağlar.

34
İndikatör 2. ÇİD-TB bildirim hızı eğilimi
Bir yılda bildirilen ÇİD-TB sayısı x Ülkenin toplam nüfusu Hedef: ÇİD-TB olgu bildirim hızındaki 5 yıllık ortalama azalış trendi önceki 5 yılın üzerinde Koşul: Olguların % 50 den fazlası kültür pozitif ve bunların % 80 den fazlasında RIF ve INH direnci bakılmışsa

35
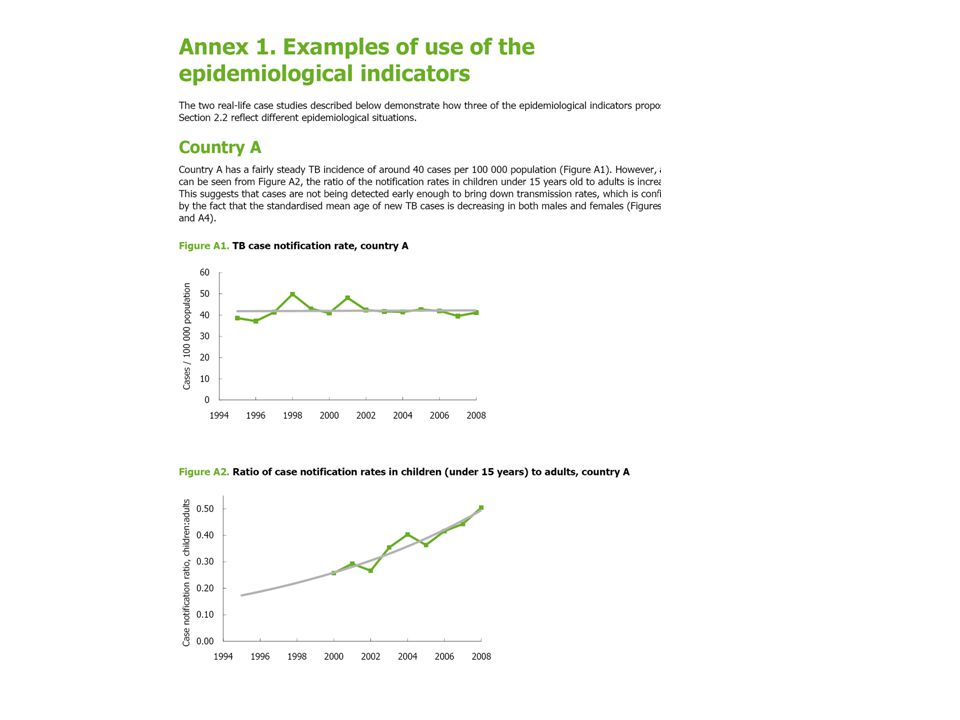
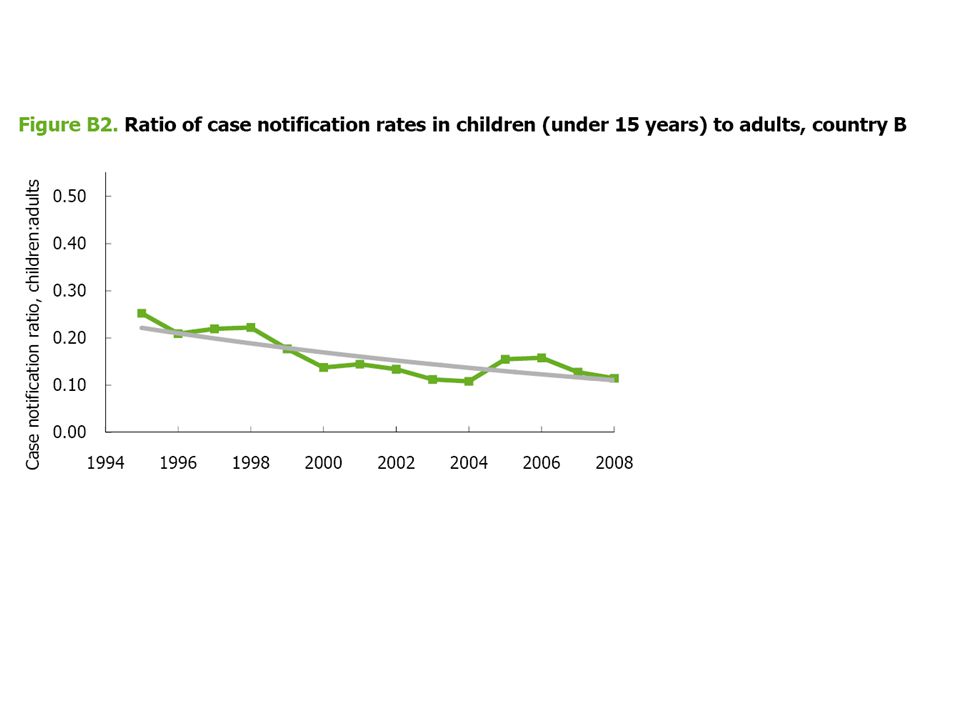
İndikatör 3. Bildirilen Çocuk TB/Erişkin TB oranının eğilimi
Çocuklarda olgu bildirim hızı(<15 yaş) Erişkinlerde olgu bildirim hızı (> 15 ) Hedef: Çocuk/erişkin TB oranındaki azalış azalış trendi önceki son 10 yıllın üzerinde olmalı. Çocuklarda TB sıklığı özellikle yeni doğanlarda, bulaşmanın çok önemli indirekt göstergesidir
 Erişkinlerde olgu bildirim hızı (> 15 ) Hedef: Çocuk/erişkin TB oranındaki azalış azalış trendi önceki. son 10 yıllın üzerinde olmalı. Çocuklarda TB sıklığı özellikle yeni doğanlarda, bulaşmanın çok önemli indirekt göstergesidir.")
36
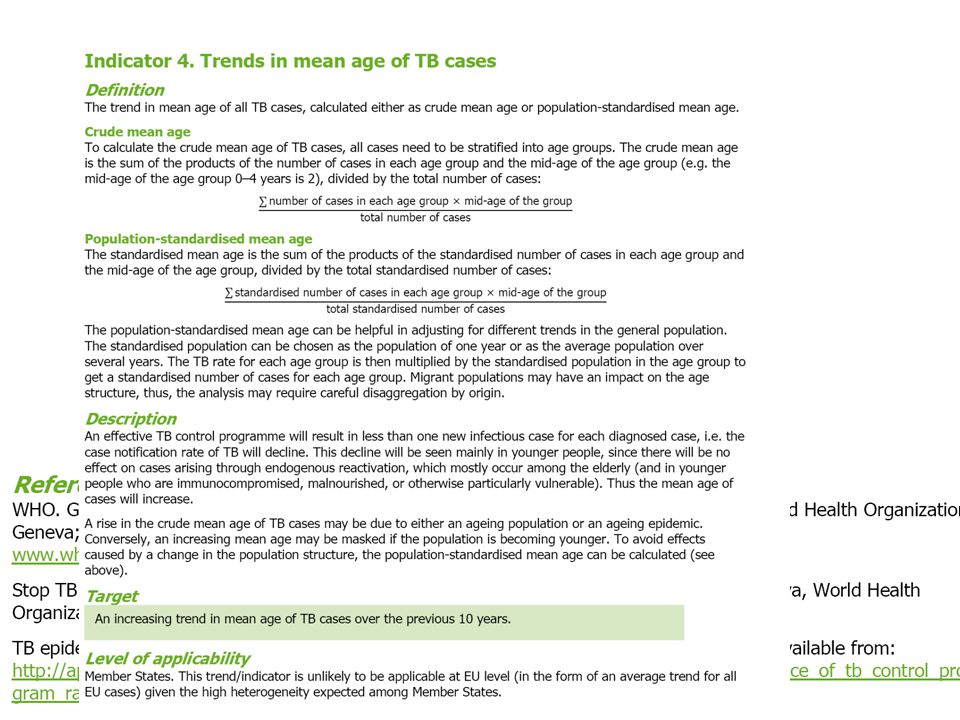
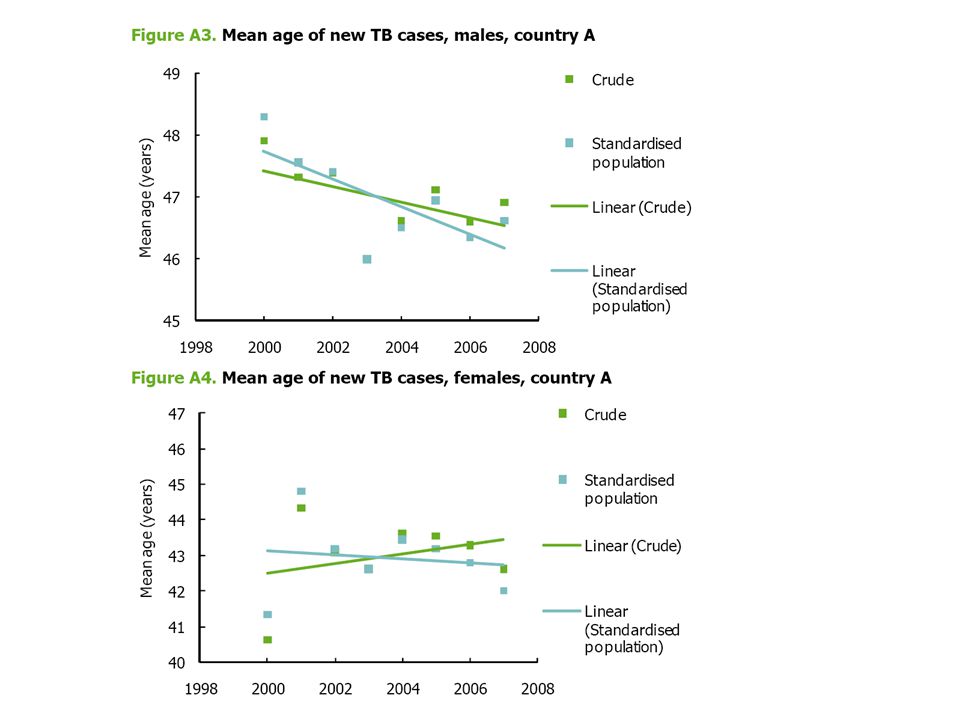
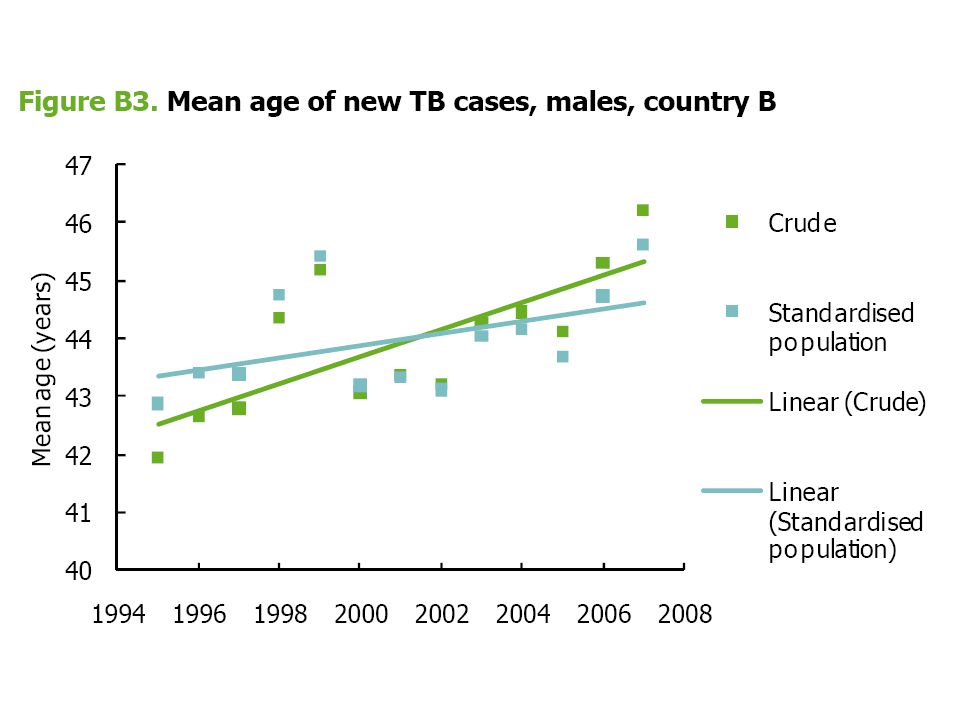
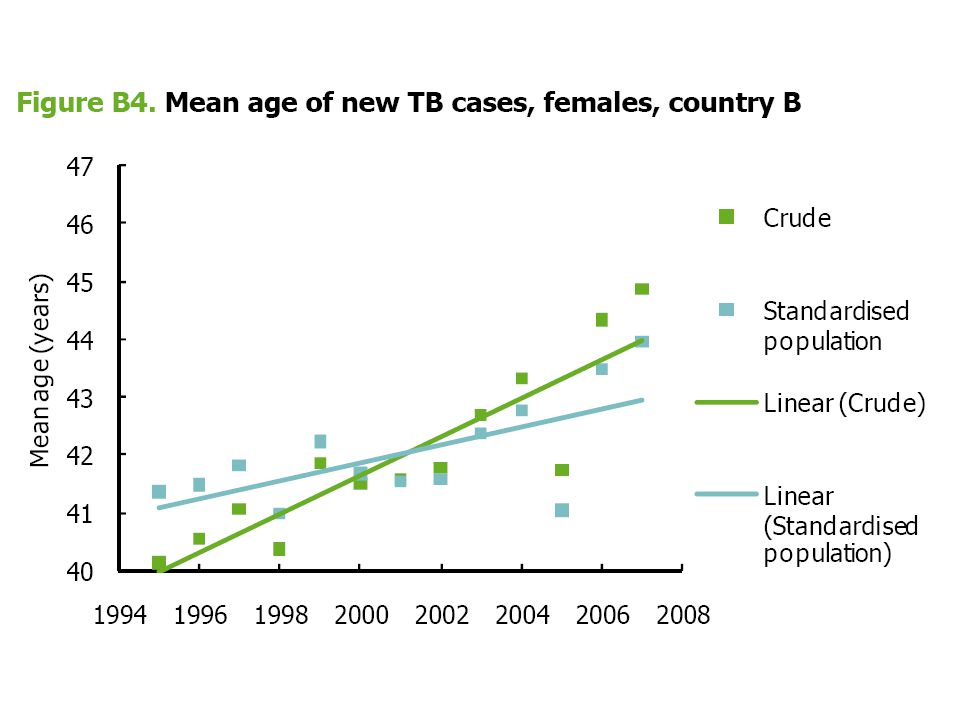
İndikatör 4. TB olgularının ortalama yaş eğilimi.
Her bir yaş grubundaki olguların sayısı x grubun ortanca yaşı Toplam olgu sayısı Hedef: TB hastalarının ortalama yaşındaki artış eğilimi önceki 10 yılın üzerinde Etkili TB kontrolü ile yeni enfeksiyon azalır. Hastalık sayısı özellikle gençlerde düşer. Hastalık yaşlılar ve TB hastalanma riski yüksek olan gençlerde görülür. Hastaların ortalama yaşı artar.

37
TB Eliminasyonu-ABD IOM 2000 yılı raporunda
2035 yılında eliminasyon öngördü. 2009 değerlendirmesi: Bu hızla giderse ( Yılda % 3.5 insidans Azalması) 97 yıl daha gerekli !!
 97 yıl daha gerekli !!")
42
Aktif TB olgularının tedavisi, 2050 de insidansı 1/1 000000’e
Tek strateji olarak Aktif TB olgularının tedavisi, 2050 de insidansı 1/ ’e İndireme hedefine ulaşamaz. Christopher Dye* and Brian G. William.Eliminating human tuberculosis in the twenty-first century. J. R. Soc. Interface (2008) 5, 653–662
 5, 653–662.")
43
TB Eliminasyonu- Yeni Gereksinimler
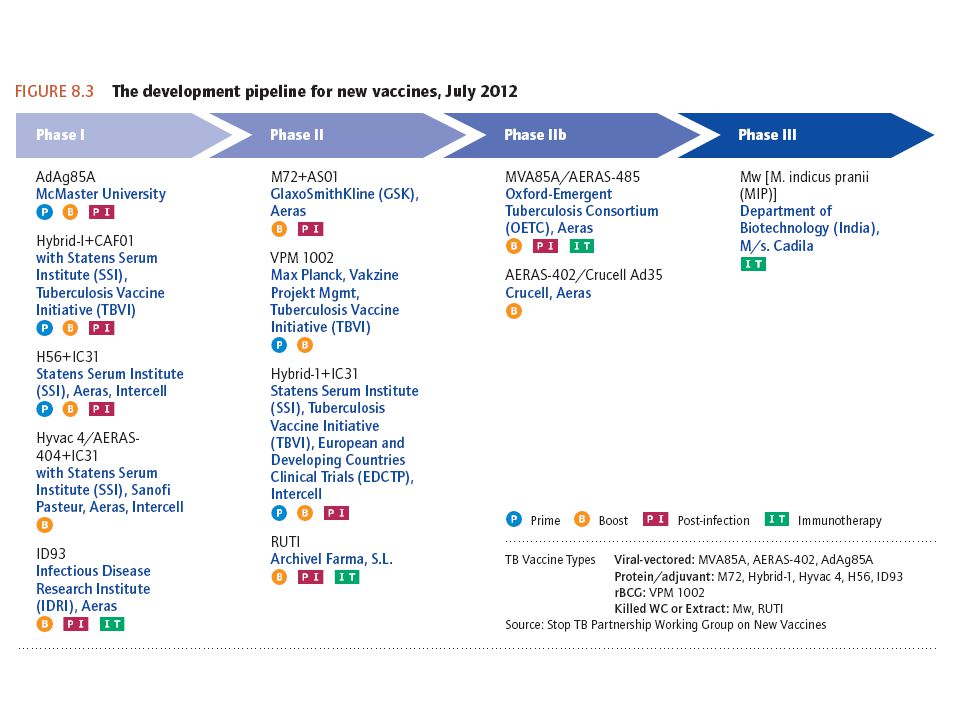
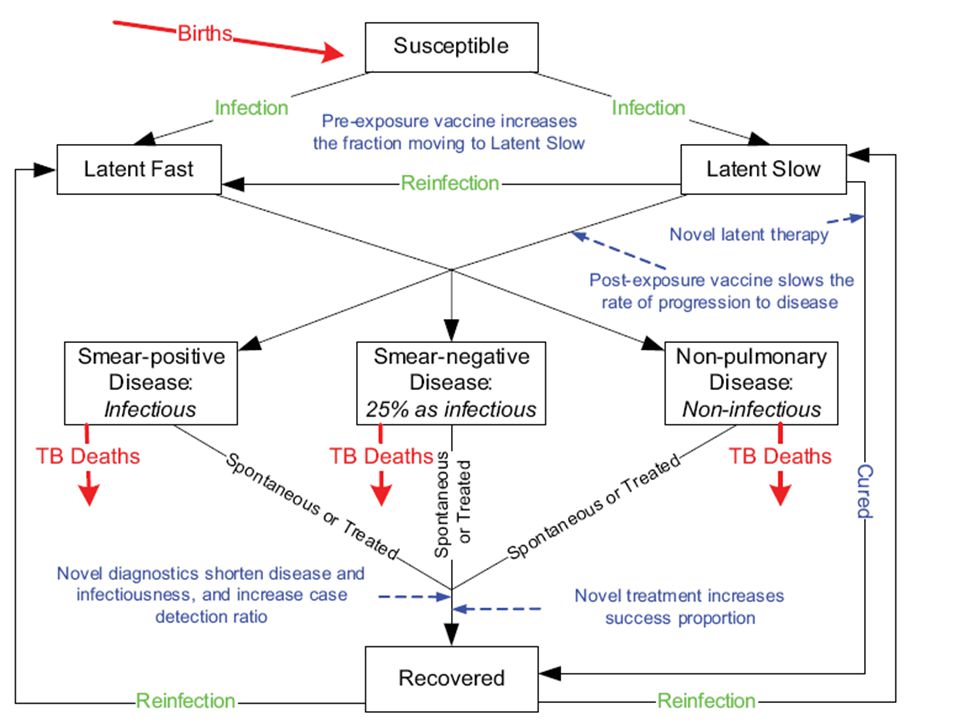
Hedefle ulaşsak ve insidans yılda % 10 azalmaya devam etse bile TB insidansı 2050 yılında 1/ hedefinin 20 katında kalacaktır. Kaliteli olgu bulma ve tedavi programı ile yeni infeksiyonları önlesek bile eski enfeksiyon havuzundan hasta çıkmaya devam eder. Latent enfeksiyonun basit araçlarla tanısını koymak ve etkili yöntemle müdahale edilerek hastalanmayı önleme esastır. Yeni etkili aşı !

47
Yeni aşıların muhtemel etkisi
TB İnsidansı Yeni aşıların muhtemel etkisi TB Mortalite

48
Yeni TB tanı araçlarının Muhtemel etkisi
TB İnsidansı Yeni TB tanı araçlarının Muhtemel etkisi TB Mortalite

49
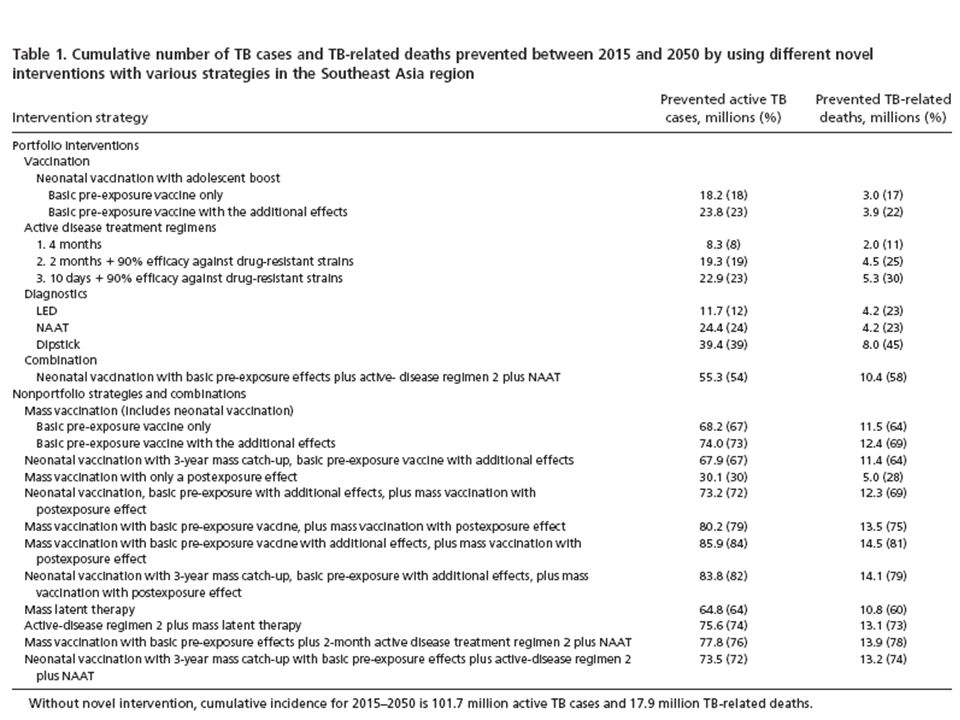
Aktif hastalarda yeni tedavi Rejimleri (1,2,3) , Kitlesel
TB İnsidansı Aktif hastalarda yeni tedavi Rejimleri (1,2,3) , Kitlesel Koruyucu tedavi ve Rejim 2+Koruyucu tedavi TB Mortalite 1.Rejim: 4 aylık tedavi 2.rejim : 2 aylık tedavi 3.Rejim: 10 günlük tedavi
 , Kitlesel. Koruyucu tedavi ve. Rejim 2+Koruyucu tedavi. TB Mortalite. 1.Rejim: 4 aylık tedavi. 2.rejim : 2 aylık tedavi. 3.Rejim: 10 günlük tedavi.")
50
TB İnsidansı Yeni doğan aşısı, Tedavi rejimi 2 Ve NAAT tanı testi kombinasyonu TBmortalitesi

51
25 March 2013 | Cape Town | "TB elimination can only be possible with intensified research and development particularly for new vaccines,” said Dr. Mario Raviglione, the Director of the WHO’s Stop TB Department.

52
Eliminasyon gerçekten hedefleniyorsa. Sorunlar çok.!
Para garanti değil. Beklenen olguların sadece % 63’ i bildiriliyor. Afrika’ da TB/HIV major etkiye sahip. MDR-TB yükü eski Sovyet ülkelerinde , Çin’de Hindistan ‘da ciddi. Sağlık sistem, hizmet ve politikaları yetersiz. Devlet dışı kuruluşlar yeterli işbirliği içinde değil. Toplumlar bilgisiz, katılımsız,hareketsiz durumda. 8. Yeni tanı, tedavi araçları için araştırmalar daha yeni başladı. However, Even at maximum DOTS coverage, case detection seems to remain below the 70% target level in most settings (Dye et al 2002) So we need innovative approaches to case detection. The DEWG is a mechanism to do whatever it needs to be done We need to ensure we make good use of it. The 2nd ad hoc Committee produced some recommendations for action, the DEWG is a tool to facilitate/implement some of them.
 So we need innovative approaches to case detection. The DEWG is a mechanism to do whatever it needs to be done. We need to ensure we make good use of it. The 2nd ad hoc Committee produced some recommendations for action, the DEWG is a tool to facilitate/implement some of them.")
53
Teşekkürler

54
Action Plans to Accelerate Tuberculosis Elimination among US-born Populations
Community-Based Tuberculosis Activities 2. Awareness of Tuberculosis among Healthcare and Service Pro 3. Advocacy and Mobilization

55
Interconnected Health Problems and Social Conditions
2. Strategies for Identifying and Treating Latent Tuberculosis Infection among Foreign-born Residents 3. Enhanced Tuberculosis Control Tools for Working with Foreign-born Populations 4. Programmatic Strategies for Ensuring Continuity of Care 5. Investment in Global Tuberculosis Control and Elimination

56
VI. Tuberculosis in Low-incidence Areas
Stopping the Loss of Infrastructure and Capacity Regional Collaboration among State Tuberculosis Control Programs Collaboration among Disease Programs Education and Training to Build Public Awareness and Provider Expertise 5. Interstate Collaboration for Access to Special Facilities 6. Enhancing Laboratory Capacity and Access to Services 7. Public and Community Health Teams

57
Evidence of these gaps is that the global rate of decrease
CONCLUSIONS Evidence of these gaps is that the global rate of decrease in the number of TB cases is less than what would be required to achieve the Millennium Development goal of TB elimination by Moreover, these gaps have led to the increase in the number of drug-resistant cases most prominently in population- dense countries, such as China and India. The deadly duo of TB and HIV coinfection is fueling the TB epidemic in many countries. Strategies that should be considered include policies that enhance DOTS by improving diagnostics to increase case detection, including using private practitioners and closing the funding gap in DOTS-based programs. Risk factors for continued TB transmission could be addressed by reducing socioeconomic health disparities and improving financial support to national TB-control programs. Better management of HIV and TB coinfection may occur by enhancing diagnostic applications of both disease processes and using isoniazid prophylactic therapy. These strategies could serve as part of the foundation to address the emergence of drug-resistant TB and, ultimately, the elimination of the disease. Underlying any effort in TB elimination, however, will be increased funding and political will from both the international community and national health sectors.

58
TB Kontrolü ile ilgili Global amaç ve hedefler:
MDG 6: HIV/AIDS, Malarya ve diğer hastalıklar. Hedef 6. Indikatör TB insidans, prevelans ve ölüm hızları İndikatör DOTS programı altında saptanan ve kür edilen TB olguları 2015 yılına kadar 1990 yılına göre prevelans ve ölüm hızlarını % 50 azaltmak 2050 yılına kadar TB’ u bir halk sağlığı sorunu olarak elimine etmek ( İnsidans < 1/ )
")
60
Rapid communications Epidemiology of tuberculosis in the EU/EEA in 2010 – monitoring the progress towards tuberculosis elimination A Sandgren V Hollo1, E Huitric1, C Ködmön1 1. European Centre for Disease Prevention and Control (ECDC), Stockholm, Sweden Citation style for this article: Sandgren A, Hollo V, Huitric E, Ködmön C. Epidemiology of tuberculosis in the EU/EEA in 2010 – monitoring the progress towards tuberculosis elimination. Euro Surveill. 2012;17(12):pii= Available online: Article published on 22 March 2012
, Stockholm, Sweden. Citation style for this article: Sandgren A, Hollo V, Huitric E, Ködmön C. Epidemiology of tuberculosis in the EU/EEA in 2010 – monitoring the progress towards tuberculosis elimination. Euro Surveill. 2012;17(12):pii= Available online: ArticleId= Article published on 22 March")
61
Indicator Target EU/EEA Number of Member Statesreaching the targetStates reporting
status Epidemiological indicators Trend in TB case notification rate Mean five-year decline %a Trend in MDR-TB case notification rate Mean five-year decline -3.4%a Trend in ratio of notification rate in children versus adults Mean 10-year decline %a 25 Trend in mean age of TB casesb Increasing trend over 10 years %a

64
96 Horne NW. Eradication of tuberculosis in Europe—so near and
yet so far. Eur. J. Respir. Dis. 1983; 126: 169–73. 97 Styblo K. Overview and epidemiological assessment of the current global tuberculosis situation with an emphasis and control in developing countries. Rev. Infect.Dis. 1989; 11: S339– 46. 98 Sutherland I, Springett VH, Nunn AJ. Changes in tuberculosis notification rates in ethnic groups in England between 1971 and 1978/79. Tubercle 1984; 65: 83–91. 99 Roche PW, Krause V, Konstantinos A et al. Tuberculosis notifications in Australia, Commun. Dis. Intell. 2008; 32: 1–11

66
Beyond the current efforts to prevent, detect and cure
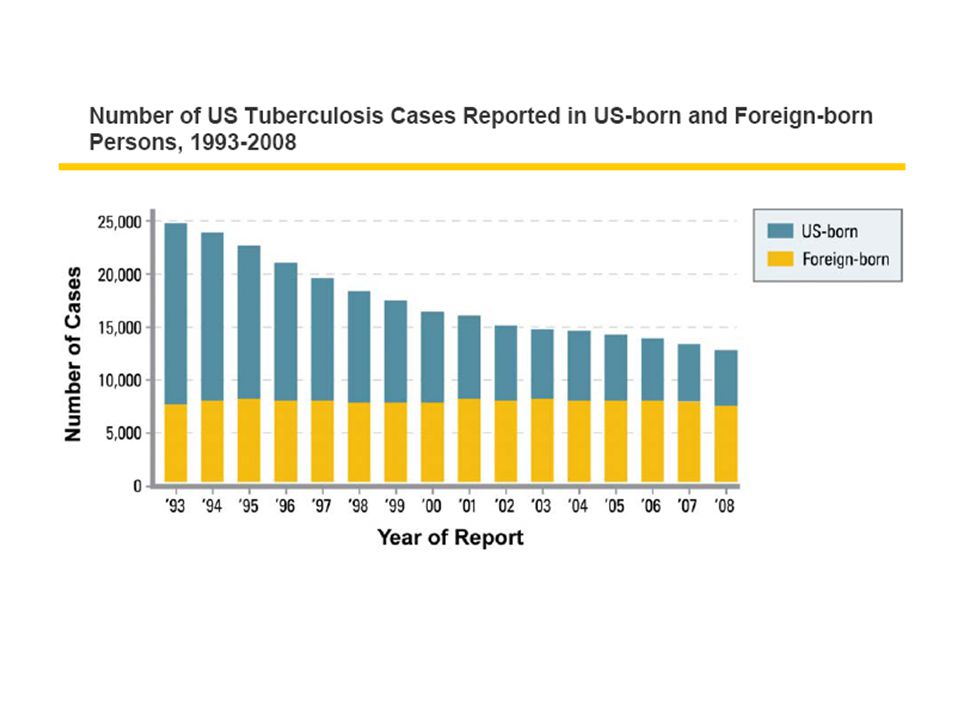
TB, new tools are needed to radically transform the fight against TB and seriously target elimination by 2050. In the 1980s, it was estimated that some countries in Europe would reach the elimination target around 2025– In 1989, Styblo estimated that it would take at least 35–40 years to eliminate TB in countries where the prevalence was low.97 However, it was already recognized that continued immigration from high-TB-incidence areas had a substantial effect on slowing the downward trend of national TB notification rates at that time.98 While the TB notification rate in non-Indigenous Australian-born population was 0.9/ in 2006, those in people born overseas and Indigenous Australians were 20.7 and 6.6, respectively. As a result, the crude notification rate in Australia was 5.8 in 2006 up from5.3 in Between 1996 and 2005, the State of Connecticut, USA, experienced 53.6% decline of TB notifications among USA-born persons. However, that in foreign-born persons was only 8.7%. The median annual notification rates were 1.5 and 19.7, respectively.100 Progress towards TB elimination even in a limited geographical area will rely not only on maintenance of high standard of TB care and control practices, but also on regional and global TB control efforts due to the unlikely capacity to stop an air-born disease such as TB from rapidly spreading across borders.

67
Eliminating Tuberculosis One Neighborhood at a Time
J. Peter Cegielski, MD, Objectives. We evaluated a strategy for preventing tuberculosis (TB) in communities most affected by it. Methods. In 1996, we mapped reported TB cases (1985–1995) and positive tuberculin skin test (TST) reactors (1993–1995) in Smith County, Texas. We delineated the 2 largest, densest clusters, identifying 2 highest-incidence neighborhoods (180 square blocks, 3153 residents). After extensive community preparation, trained health care workers went door-to-door offering TST to all residents unless contraindicated. TST-positive individuals were escorted to a mobile clinic for radiography, clinical evaluation, and isoniazid preventive treatment (IPT) as indicated. To assess long-term impact, we mapped all TB cases in Smith County during the equivalent time period after the project. Results. Of 2258 eligible individuals, 1291 (57.1%) were tested, 229 (17.7%) were TST positive, and 147 were treated. From 1996 to 2006, there were no TB cases in either project neighborhood, in contrast with the preintervention decade and the continued occurrence of TB in the rest of Smith County. Conclusions. Targeting high-incidence neighborhoods for active, community-based screening and IPT may hasten TB elimination in the United States. (Am J Public Health. Published online ahead of print October 18, 2012: e1-e9. doi: /AJPH )
 in communities most affected by it. Methods. In 1996, we mapped reported TB cases (1985–1995) and positive tuberculin skin test (TST) reactors (1993–1995) in Smith County, Texas. We delineated the 2 largest, densest clusters, identifying 2 highest-incidence neighborhoods (180 square blocks, 3153 residents). After extensive community preparation, trained health care workers went door-to-door offering TST to all residents unless contraindicated. TST-positive individuals were escorted to a mobile clinic for radiography, clinical evaluation, and isoniazid preventive treatment (IPT) as indicated. To assess long-term impact, we mapped all TB cases in Smith County during the equivalent time period after the project. Results. Of 2258 eligible individuals, 1291 (57.1%) were tested, 229 (17.7%) were TST positive, and 147 were treated. From 1996 to 2006, there were no TB cases in either project neighborhood, in contrast with the preintervention decade and the continued occurrence of TB in the rest of Smith County. Conclusions. Targeting high-incidence neighborhoods for active, community-based screening and IPT may hasten TB elimination in the United States. (Am J Public Health. Published online ahead of print October 18, 2012: e1-e9. doi: /AJPH )")
70
Globally, this implementation gap has been closing as
a result of reliance on the evidence-based strategy for TB control, originally known as Directly Observed Treatment Short-course (DOTS Furthermore, TB control has been demonstrated to be among the most cost effective of health interventions (13). Implementation Gap In his 1963 lecture Even when all countries of the world have adopted policies consistent with the DOTS strategy, a sizable proportion of estimated cases (≈37%) are undetected, and those infected are likely not receiving optimal treatment regimens Emerging Infectious Diseases • • Vol. 17, No. 3, March 2011
. Implementation Gap. In his 1963 lecture. Even. when all countries of the world have adopted policies. consistent with the DOTS strategy, a sizable proportion of. estimated cases (≈37%) are undetected, and those infected. are likely not receiving optimal treatment regimens. Emerging Infectious Diseases • • Vol. 17, No. 3, March")
71
An analysis from India has reported that 72% of
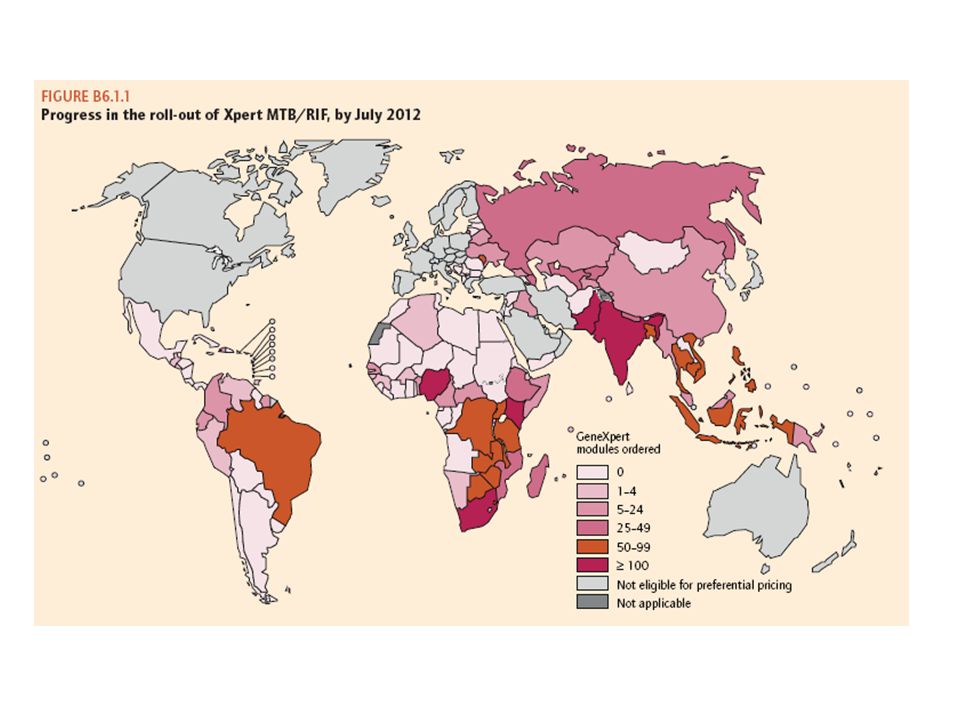
TB patients who had a low standard of living (e.g., earning US $1–$2/d) fi rst saw private providers and spent, on average, $145 before starting treatment with the Revised National TB Program, thus documenting the devastating economic toll incurred by poor persons with TB Efforts must now focus on tackling social determinants of illness associated with TB by expanding and facilitating access to impoverished persons in densely populated urban areas and remote villages. Most recently, technologic advances have demonstrated the ability to rely on detection of bacterial DNA by PCR. The WHO policy recommendation to rely on Xpert MTB/RIF (Cepheid, Sunnyvale, CA, USA) for same-day diagnosis accentuates and magnifi es this implementation gap (18) A growing concern has to do with the gap in successfully addressing concurrent conditions associated with TB, such as HIV, diabetes, smoking, indoor air pollution, alcoholism, and malnutrition (16).
 fi rst saw private providers and spent, on. average, $145 before starting treatment with the Revised. National TB Program, thus documenting the devastating. economic toll incurred by poor persons with TB. Efforts. must now focus on tackling social determinants of illness. associated with TB by expanding and facilitating access to. impoverished persons in densely populated urban areas and. remote villages. Most recently, technologic advances have demonstrated the ability to rely. on detection of bacterial DNA by PCR. The WHO policy. recommendation to rely on Xpert MTB/RIF (Cepheid, Sunnyvale, CA, USA) for same-day diagnosis accentuates. and magnifi es this implementation gap (18) A growing concern has to do with the gap in. successfully addressing concurrent conditions associated. with TB, such as HIV, diabetes, smoking, indoor air. pollution, alcoholism, and malnutrition (16).")
72
Knowledge Gap There remain critical areas of collective ignorance with regard to M. tuberculosis. These include knowledge of rapid, simple, and inexpensive methods of detection; molecular mechanisms of resistance to chemotherapy; virulence; host defense correlates of susceptibility to and protection against the organism; and optimal targets for development of new antimicrobial drugs. Until the past 2 decades, defi nitive detection of M. tuberculosis relied exclusively on culture, which takes weeks because of the requisite generation time of 18–24 hours, giving rise to the apt descriptor of M. tuberculosis as “slow growing” bacteria. In low resource settings, even culture may not be available and diagnosis must be based on smear microscopy, which fails to detect nearly half of patients with TB (14). Only relatively recently has a promising new molecular diagnostic test become available, the Xpert TB/ RIF, that is both simple and accurate (21). However, even with concessionary pricing for low-income countries, cost still remains an issue.
. Only relatively recently has a promising new. molecular diagnostic test become available, the Xpert TB/ RIF, that is both simple and accurate (21). However, even. with concessionary pricing for low-income countries, cost. still remains an issue.")
73
Similarly, detection of drug resistance almost solely
relies on phenotypic culture-based methods. Here, also, advances in molecular biology are moving the fi eld forward, but the situation is more complex than for detection of the organism. Fortunately, for the most important anti- TB drug, rifampin, >95% of resistance can be attributed to mutations in 1 gene, which has greatly simplifi ed the development of molecular tests to detect rifampin resistance (22). Commercial assays that use line-probe and molecular beacon technologies have been produced that are rapid and accurate (22,23). However, for other fi rst-line drugs (such as isoniazid and ethambutol) and second-line drugs, the molecular mechanisms
. Commercial assays that use line-probe and. molecular beacon technologies have been produced that. are rapid and accurate (22,23). However, for other fi rst-line. drugs (such as isoniazid and ethambutol) and second-line. drugs, the molecular mechanisms.")
74
Virulence of M. tuberculosis, especially variation
among strains, is also poorly understood. There is evidence suggesting some strains may result in higher rates of disease progression, treatment failure, and relapse (25). Identifying genetic markers of M. tuberculosis virulence would enable additional attention to be focused on patients infected with strains manifesting such markers and who are therefore at the greatest risk for poor outcomes.
. Identifying. genetic markers of M. tuberculosis virulence would enable. additional attention to be focused on patients infected with. strains manifesting such markers and who are therefore at. the greatest risk for poor outcomes.")
75
ceptibility to and protection against M. tuberculosis has
stymied progress in 2 key areas: vaccine development and prevention through treatment of latent TB. A vaccine that uses an attenuated strain of M. bovis (M. bovis BCG) has been available for nearly a century and is one of the most widely used vaccines in the world. Although the vaccine does offer substantial protection against dissemination of M. tuberculosis infection in children, it only provides modest and highly variable protection against TB in general (26,27). Clearly, more effi cacious and safe vaccines are needed; these are only likely to be produced through a better understanding of immunologic mechanisms and correlates of protection. A related knowledge gap is the lack of understanding of why only a small fraction (≈5%–10%) of persons infected with M. tuberculosis later exhibit disease (28).
 has. been available for nearly a century and is one of the most. widely used vaccines in the world. Although the vaccine. does offer substantial protection against dissemination. of M. tuberculosis infection in children, it only provides. modest and highly variable protection against TB in general. (26,27). Clearly, more effi cacious and safe vaccines are. needed; these are only likely to be produced through a. better understanding of immunologic mechanisms and. correlates of protection. A related knowledge gap is. the lack of understanding of why only a small fraction. (≈5%–10%) of persons infected with M. tuberculosis later. exhibit disease (28).")
76
Ambition Gap The report from the 1959 Arden House Conference on TB made a daring statement, possibly well ahead of its time, indicating that TB control “has progressed to the point where virtual elimination of the disease as a public health problem appears to be within reach” (31). However, it was not until 3 decades later that the Centers for Disease Control published a formal consensus plan for the elimination of TB in the United States (32). This plan was ambitious, yet initially naive about the full extent of the effects on TB incidence due to HIV infection; multidrug resistance; institutional transmission of M. tuberculosis; and the time lag for the development of new technologies for more effective prevention, prompt diagnosis and detection of drug resistance, and superior treatment of TB. These various factors converged to produce the unprecedented resurgence of TB experienced in the United States during 1985–1992 (33). The rapid dissemination of multidrug-resistant TB among HIV-infected persons and their caregivers was accompanied by unacceptably high mortality rates and served as a clarion call to elicit concerted efforts and mobilize new resources to implement the 1992 National Action Plan to Combat Multidrug Resistant TB (34). The US Federal TB task force coordinated interagency work and successfully worked with health department-based TB programs across the nation to reverse this trend over ensuing years. In 2000, the Institute of Medicine reaffi rmed the goal of TB elimination and recommended additional steps required for accelerated progress, including the need to commit to elimination as a national goal and to monitor progress (35). In recent years
. However, it was. not until 3 decades later that the Centers for Disease Control. published a formal consensus plan for the elimination of. TB in the United States (32). This plan was ambitious, yet initially naive about the full extent of the effects on. TB incidence due to HIV infection; multidrug resistance; institutional transmission of M. tuberculosis; and the time. lag for the development of new technologies for more. effective prevention, prompt diagnosis and detection of. drug resistance, and superior treatment of TB. These various. factors converged to produce the unprecedented resurgence. of TB experienced in the United States during 1985–1992. (33). The rapid dissemination of multidrug-resistant TB. among HIV-infected persons and their caregivers was. accompanied by unacceptably high mortality rates and. served as a clarion call to elicit concerted efforts and. mobilize new resources to implement the 1992 National. Action Plan to Combat Multidrug Resistant TB (34). The. US Federal TB task force coordinated interagency work. and successfully worked with health department-based. TB programs across the nation to reverse this trend over. ensuing years. In 2000, the Institute of Medicine reaffi rmed. the goal of TB elimination and recommended additional. steps required for accelerated progress, including the need. to commit to elimination as a national goal and to monitor. progress (35). In recent years.")
77
In recent years, the risk of renewed complacency,
resource limitations experienced by local health departments, and the direct effects of global TB on US disease rates (nearly 60% of incident TB cases reported in the United States in 2009 occurred in foreign-born persons) challenges advances to TB elimination in the near future. Bold ambition and expectations with sustained actions are a requisite to successfully eliminating TB in the United States and globally. The report of the 1997 Dahlem Workshop on the Eradication of Infectious Diseases recognizes that “[t]he success of any disease eradication initiative depends strongly on the level of societal and political commitment… Elimination and eradication are the ultimate goals of public health, evolving naturally from disease control. The basic question is whether these goals are to be achieved in the present or some future generation” (36).
 challenges advances to TB elimination in the near future. Bold ambition and expectations with sustained actions are a. requisite to successfully eliminating TB in the United States. and globally. The report of the 1997 Dahlem Workshop. on the Eradication of Infectious Diseases recognizes that. [t]he success of any disease eradication initiative depends. strongly on the level of societal and political commitment… Elimination and eradication are the ultimate goals of public. health, evolving naturally from disease control. The basic. question is whether these goals are to be achieved in the. present or some future generation (36).")
78
This frame of mind was aptly
recognized in 1963 by William Brown, who advocated for syphilis eradication during the 1960s. He argued that diseases targeted for eradication (or elimination) should attain a “status of intolerability” by both health authorities and the public, such that any occurrence of the disease, “no matter how small,” gives cause for immediate action (37). Public clamor would help ensure sustained political commitment and ongoing work. With relatively World Health Organization. The global plan to stop TB 2011–2015: transforming the fi ght towards the elimination of tuberculosis [cited 2011 Jan 3]. TB_GlobalPlanToStopTB pdf
 should attain a status of intolerability by both health. authorities and the public, such that any occurrence of the. disease, no matter how small, gives cause for immediate. action (37). Public clamor would help ensure sustained. political commitment and ongoing work. With relatively. World Health Organization. The global plan to stop TB 2011–2015: transforming the fi ght towards the elimination of tuberculosis [cited Jan 3]. TB_GlobalPlanToStopTB pdf.")
79
Christopher Dye and Brian G. Williams
Slow Elimination of Multidrug-Resistant Tuberculosis Sci Transl Med 1, 3ra8 (2009); where there may be regions in which drug-resistant strains are self-sustaining. Thus, present efforts at eradication, that the R for each of the drug-resistant strains tested in each country is less than 1, with the exception of Russia resistant to rifampicin, isoniazid, or both drugs. When analyzed with a model of disease spreading, the data indicate Kingdom, and others), Russia, Hong Kong, and the United States to estimate the values of R for bacterial strains (though the years differ among countries) from European countries (Estonia, Germany, Latvia, Lithuania, United track for disease elimination. Dye and Williams used data reported to the World Health Organization from M. tuberculosis. With this information, ongoing eradication efforts can be adjusted to keep R at less than 1 and on
; where there may be regions in which drug-resistant strains are self-sustaining. Thus, present efforts at eradication, that the R for each of the drug-resistant strains tested in each country is less than 1, with the exception of Russia. resistant to rifampicin, isoniazid, or both drugs. When analyzed with a model of disease spreading, the data indicate. Kingdom, and others), Russia, Hong Kong, and the United States to estimate the values of R for bacterial strains. (though the years differ among countries) from European countries (Estonia, Germany, Latvia, Lithuania, United. track for disease elimination. Dye and Williams used data reported to the World Health Organization from M. tuberculosis. With this information, ongoing eradication efforts can be adjusted to keep R at less than 1 and on.")
88
The total cost of the Global Plan was $56 billion, of
which $47 billion was slated for implementation of currently available interventions and $9 billion for research and development [9, 12]. However, even when launched in 2006 (a time when the global economy was relatively strong), the overall estimated funding gap for the Global Plan was 1$30 billion [13]. In past recessions, several countries had reduced spending on overseas developmental programs [14–16]. 14. International Monetary Fund. The implications of the global financial crisis for developing countries. Washington, DC: IMF, 2009. 15. Calı` M, Massa I, te Velde DW. The global financial crisis: financial flows to developing countries set to fall by one quarter. ODI background paper. London, Overseas Development Institute, 2009 9. Raviglione MC. The new Stop TB Strategy and the Global Plan to Stop TB, 2006–2015. Bull World Health Organ 2007; 85:327. 10. Stop TB Partnership. The Global Plan to Stop TB 2006–2015. Geneva: World Health Organization, 2006. 11. Komatsu R, Low-Beer D, Schwartla¨nder B. Global Fund-supported programmes contribution to international targets and the Millenium Development Goals: an initial analysis. Bull World Health Organ 2007; 85:805–811. 12. Young DB, Perkins MD, Duncan K, Barry CE. Confronting the scientific obstacles to global control of tuberculosis. J Clin Invest 2008; 118:1255–1265.
, the overall estimated funding gap for. the Global Plan was 1$30 billion [13]. In past recessions, several countries had reduced spending on overseas. developmental programs [14–16]. 14. International Monetary Fund. The implications of the global financial. crisis for developing countries. Washington, DC: IMF, Calı` M, Massa I, te Velde DW. The global financial crisis: financial. flows to developing countries set to fall by one quarter. ODI background. paper. London, Overseas Development Institute, Raviglione MC. The new Stop TB Strategy and the Global Plan to Stop. TB, 2006–2015. Bull World Health Organ 2007; 85: Stop TB Partnership. The Global Plan to Stop TB 2006–2015. Geneva: World Health Organization, Komatsu R, Low-Beer D, Schwartla¨nder B. Global Fund-supported. programmes contribution to international targets and the Millenium. Development Goals: an initial analysis. Bull World Health Organ. 2007; 85:805– Young DB, Perkins MD, Duncan K, Barry CE. Confronting the scientific. obstacles to global control of tuberculosis. J Clin Invest 2008; 118:1255–1265.")
89
Son Rapor MDR Dağılım IV Diğerler

91
TB FUNDING ISSUES Close the funding gap for DOTS. The existing funding gap among the 94 countries with 93% of global cases in 2009 is $1.6 billion [26]. if DOTS was sustained at 2005 coverage levels in key countries with a high burden of TB, there would be an estimated economic gain of ∼$1.6 trillion (during 2006– 2015), ranging from $0.74 billion (95% CI, $0.64–$0.84) in Zimbabwe to $748 billion (95% CI, $638–$857) in China
, ranging from $0.74 billion (95% CI, $0.64–$0.84) in. Zimbabwe to $748 billion (95% CI, $638–$857) in China.")
92
Fully fund TB-control programs
Among the 94 countries that reported 93% of TB cases, a total of $4.2 billion is required for full implementation of country plans in Eighty-seven percent of funding derives from national governments (including loans), 9% from the Global Plan, and 4% from donors other than the Global Plan.
, 9% from the Global Plan, and 4% from donors. other than the Global Plan.")
93
Greater funding to integrate TB and HIV services.
Of the total of $2.9 billion required for full implementation of the country plans in the 22 countries with the highest burden of TB in 2009, only 3% is dedicated to joint TB and HIV–related activities [26]. Cost-effective strategies may be immediately implemented using currently available technologies in resource-limited settings

Benzer bir sunumlar
























 TURKISH COMMERCIAL.>")

