Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Yrd.Doç.Dr.Olcay ÖZVEREN Yeditepe Üniversite Hastanesi Kardiyoloji ABD 2014-2015 Congestive Heart Failure

4
Notes to heart physiology Notes to heart physiology Essential functions of the heart to cover metabolic needs of body tissue (oxygen, substrates) by adequate blood supply to receive all blood comming back from the tissue to the heart Essential conditions for fulfilling these functions Essential conditions for fulfilling these functions normal structure and functions of the heart adequate filling of the heart by blood
 by adequate blood supply to receive all blood comming back from the tissue to the heart Essential conditions for fulfilling these functions Essential conditions for fulfilling these functions normal structure and functions of the heart adequate filling of the heart by blood")
6
Essential functions of the heart are secured Essential functions of the heart are secured by integration of electrical and mechanical by integration of electrical and mechanical functions of the heart functions of the heart Cardiac output (CO) = heart rate (HR) x stroke vol.(SV) - changes of the heart rate - changes of stroke volume Control of HR: Control of HR: - autonomic nervous system - hormonal(humoral) control Control of SV: Control of SV: - preload - contractility - afterload
 = heart rate (HR) x stroke vol.(SV) - changes of the heart rate - changes of stroke volume Control of HR: Control of HR: - autonomic nervous system - hormonal(humoral) control Control of SV: Control of SV: - preload - contractility - afterload")
11
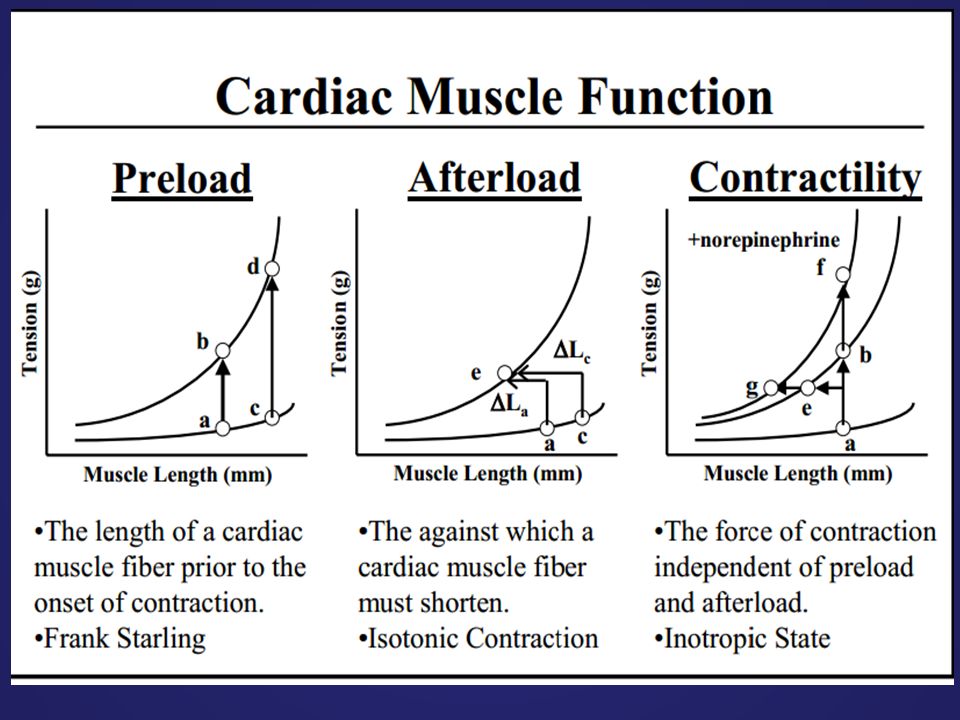
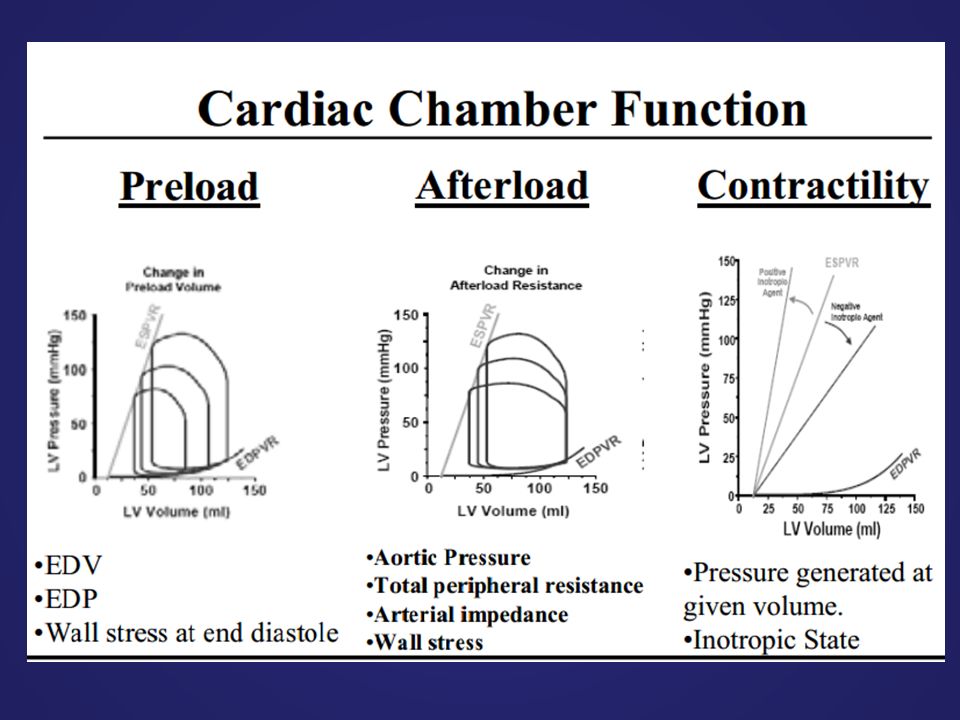
Preload Stretching the myocardial fibers during diastole by increasing end- diastolic volume force of contraction during systole = Starling´s law preload = diastolic muscle sarcomere length leading to increased tension in muscle before its contraction tension in muscle before its contraction - venous return to the heart is important end-diastolic volume is influenced - stretching of the sarcomere maximises the number of actin-myosin bridges responsible for development of force of actin-myosin bridges responsible for development of force - optimal sarcomere length 2.2 m

12
FRANK-STARLING’S LAW

13
Myocardial contractility Contractility of myocardium Changes in ability of myocardium to develop the force Changes in ability of myocardium to develop the force by contraction that occur independently on the by contraction that occur independently on the changes in myocardial fibre length changes in myocardial fibre length Mechanisms involved in changes of contractility Mechanisms involved in changes of contractility amount of created cross-bridges in the sarcomere amount of created cross-bridges in the sarcomere by of Ca ++ i concentration - catecholamines Ca ++ i contractility - catecholamines Ca ++ i contractility - inotropic drugs Ca ++ i contractility contractility shifting the entire ventricular function curve upward and to the left curve upward and to the left contractility shiffting the entire ventricular function curve (hypoxia, acidosis) downward and to the right curve (hypoxia, acidosis) downward and to the right
 downward and to the right curve (hypoxia, acidosis) downward and to the right")
14
The pressure – volume loop It is the relation between ventricular volume and pressure This loop provides a convenient framework for understanding the response of individual left ventricular contractions to alterations in preload, afterload, and contractility It is composed of 4 phases: - filling of the ventricle - isovolumic contraction of ventricle - isotonic contraction of ventricle(ejection of blood) - isovolumic relaxation of ventricle
 - isovolumic relaxation of ventricle")
15
Pressure – volume loops recorded under different conditions

16
It is expressed as tension which must be developed in the wall of ventricles during systole to open the semilunar valves and eject blood to aorta/pulmunary artery Clinically, it is the pressure the heart must pump against to eject blood Laplace law: intraventricular pressure x radius of ventricle wall tension = -------------------------------------------------------- 2 x ventricular wall thickness 2 x ventricular wall thickness afterload: due to of arterial resistance - ventricular size - ventricular size - myocardial hypotrophy - myocardial hypotrophy afterload: due to - arterial resistance - myocardial hypertrophy - myocardial hypertrophy - ventricular size - ventricular size Afterload

23
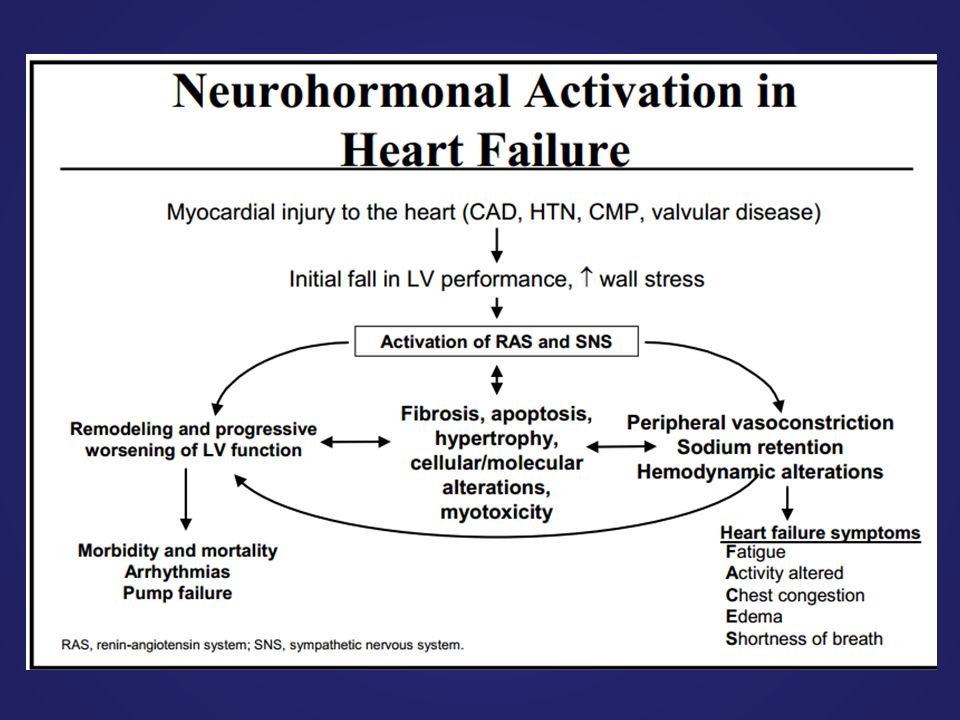
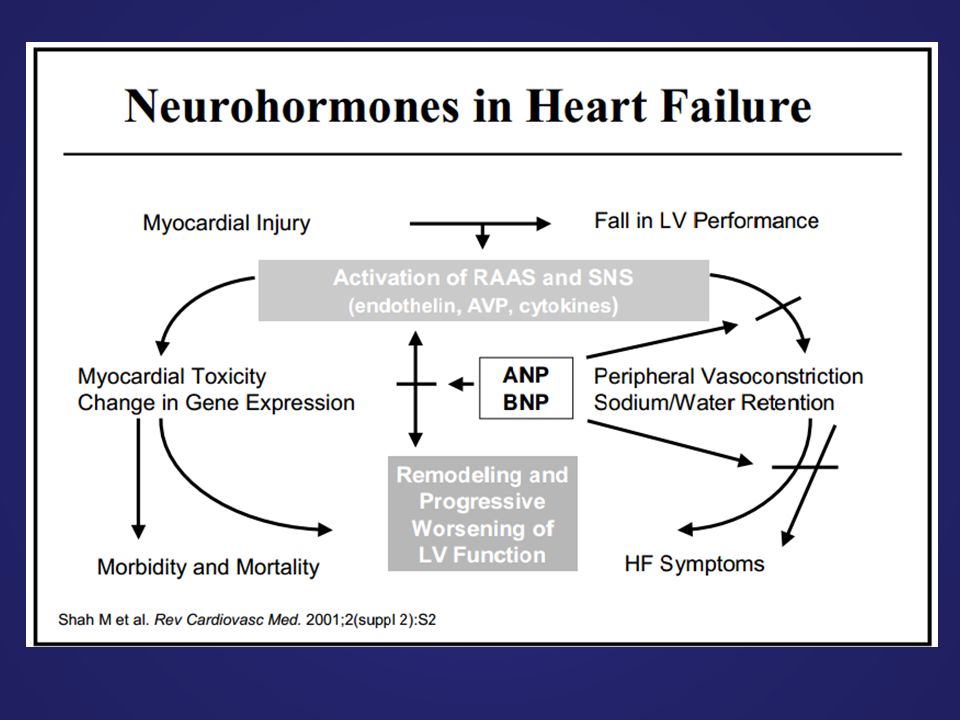
RAAS ACTIVITION

26
Characteristic features of systolic dysfunction (systolic failure) ventricular dilatation reducing ventricular contractility (either generalized or localized) diminished ejection fraction (i.e., that fraction of end-diastolic blood volume ejected from the ventricle during each systolic contraction – les then 45%) in failing hearts, the LV end-diastolic volume (or pressure) may increse as the stroke volume (or CO) decreases
 ventricular dilatation reducing ventricular contractility (either generalized or localized) diminished ejection fraction (i.e., that fraction of end-diastolic blood volume ejected from the ventricle during each systolic contraction – les then 45%) in failing hearts, the LV end-diastolic volume (or pressure) may increse as the stroke volume (or CO) decreases")
27
Characteristic features of diastolic dysfunctions (preserved EF) ventricular cavity size is normal or small myocardial contractility is normal or hyperdynamic ejection fraction is normal (>50%) or supranormal ventricle is usually hypertrophied ventricle is filling slowly in early diastole (during the period of passive filling) end-diastolic ventricular pressure is increased
 ventricular cavity size is normal or small myocardial contractility is normal or hyperdynamic ejection fraction is normal (>50%) or supranormal ventricle is usually hypertrophied ventricle is filling slowly in early diastole (during the period of passive filling) end-diastolic ventricular pressure is increased")
28
DEFINITION

29
CLASSIFICATION of HF Acute/Chronic HF Left/right sided HF High/low output HF

30
ETIOLOGY of HF

31
–Afterload : arteriel hypertension, aortic stenosis –Preload: Volume overload, AR, MR –Pump failure: CAD, cardiomyopathies, arrhythmia, increased workload (infection, high- output states)
")
33
DEFINITIONS in HF A patient who has never exhibited the typical signs or symptoms of HF is described as having asymptomatic LV systolic dysfunction Patients who have had HF for some time are often said to have ‘chronic HF’. A treated patient with symptoms and signs, which have remained generally unchanged for at least a month, is said to be ‘stable’. If chronic stable HF deteriorates, the patient may be described as ‘decompensated’ and this may happen suddenly, i.e. ‘acutely’, usually leading to hospital admission New (‘de novo’) HF may present acutely, for example as a consequence of acute myocardial infarction
 HF may present acutely, for example as a consequence of acute myocardial infarction.")
34
DEFINITIONS of FUNCTIONAL CLASSIFICATION

35
DIAGNOSIS of HEART FAILURE

37
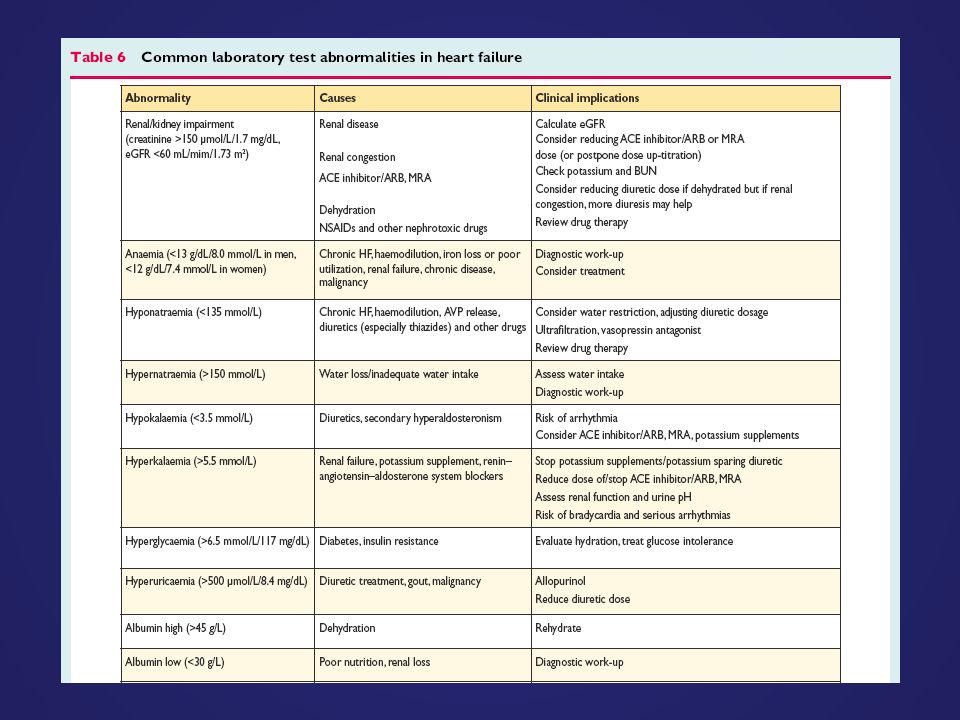
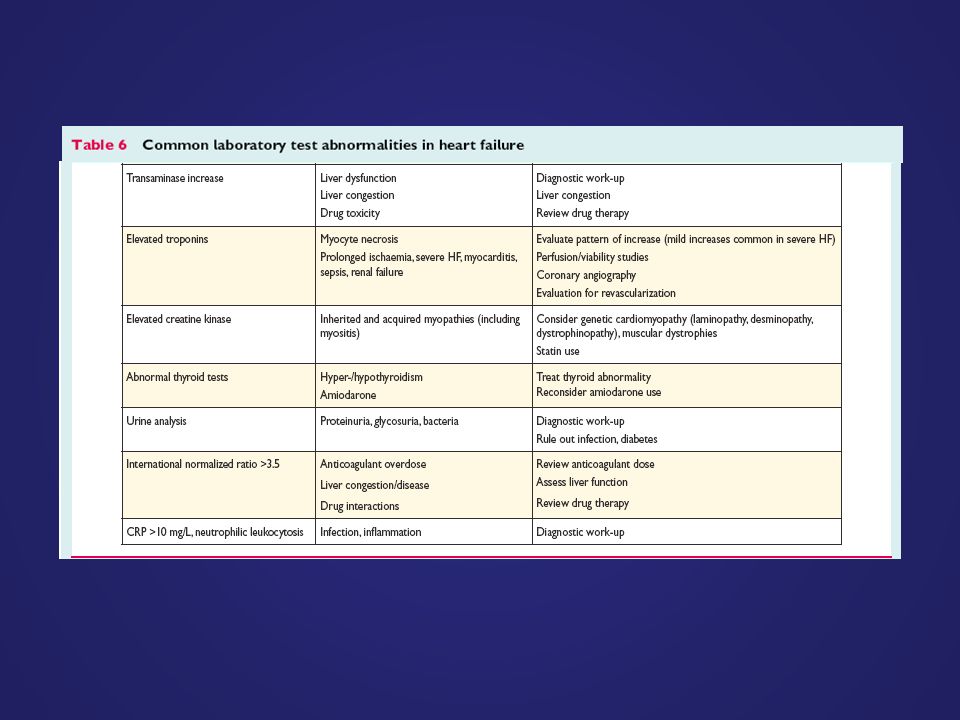
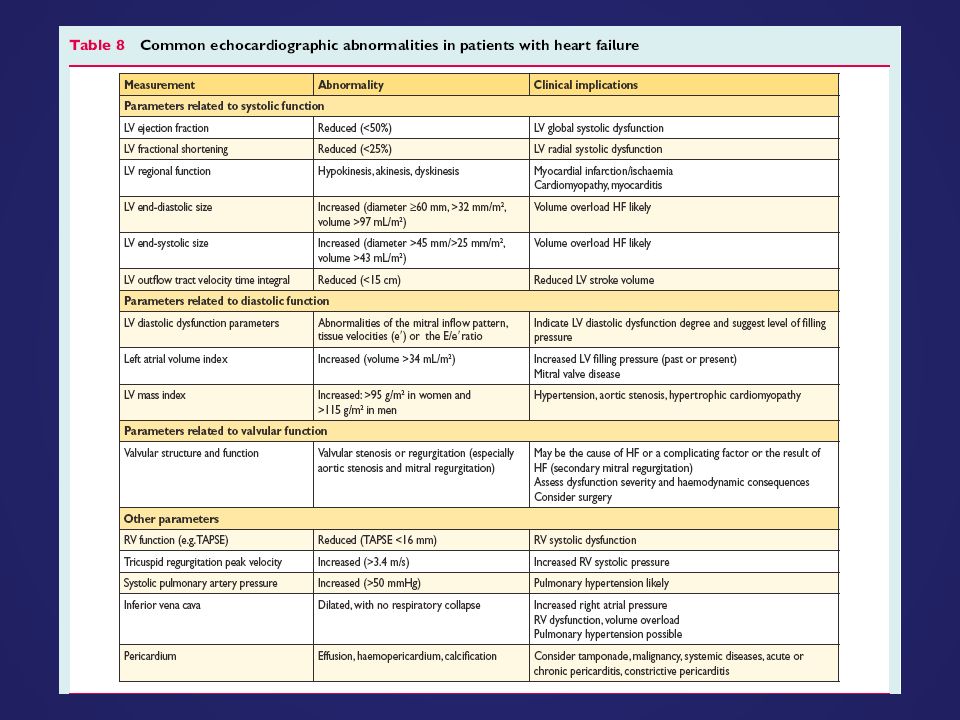
Transthoracic echocardiography is recommended to evaluate cardiac structure and function, including diastolic function and to measure LVEF to make the diagnosis of HF, assist in planning and monitoring of treatment, and to obtain prognostic information. A 12-lead ECG is recommended to determine heart rhythm, heart rate, QRS morphology, and QRS duration, and to detect other relevant abnormalities. This information also assists in planning treatment and is of prognostic importance. A completely normal ECG makes systolic HF unlikely (but still possible!) Measurement of blood chemistry (including sodium, potassium, calcium, urea/blood urea nitrogen, creatinine/estimated glomerular filtration rate, liver enzymes and bilirubin, ferritin/TIBC) and thyroid function is recommended to: (i)Evaluate patient suitability for diuretic, renin–angiotensin–aldosterone antagonist, and anticoagulant therapy (and monitor treatment) (ii) Detect reversible/treatable causes of HF (e.g. hypocalcaemia, thyroid dysfunction) and co-morbidities (e.g. iron deficiency) (iii) Obtain prognostic information. DIAGNOSTİC TESTS in HF
 Measurement of blood chemistry (including sodium, potassium, calcium, urea/blood urea nitrogen, creatinine/estimated glomerular filtration rate, liver enzymes and bilirubin, ferritin/TIBC) and thyroid function is recommended to: (i)Evaluate patient suitability for diuretic, renin–angiotensin–aldosterone antagonist, and anticoagulant therapy (and monitor treatment) (ii) Detect reversible/treatable causes of HF (e.g. hypocalcaemia, thyroid dysfunction) and co-morbidities (e.g. iron deficiency) (iii) Obtain prognostic information. DIAGNOSTİC TESTS in HF.")
38
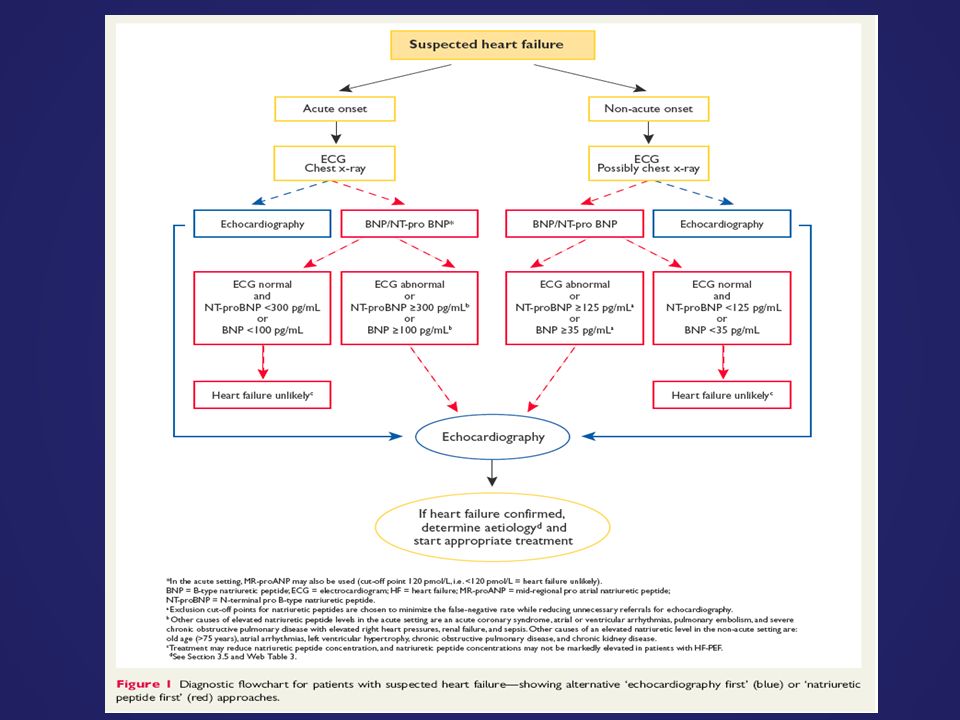
A complete blood count is recommended to: (i)Detect anaemia, which may be an alternative cause of the patient’s symptoms and signs and may cause worsening of HF (ii) Obtain prognostic information. Measurement of natriuretic peptide (BNP, NT-proBNP, or MR-proANP) should be considered to: (i)Exclude alternative causes of dyspnoea (if the level is below the exclusion cut-point HF is very unlikely) (ii) Obtain prognostic information. A chest radiograph (X-ray) should be considered to detect/exclude certain types of lung disease, e.g. cancer (does not exclude asthma/ COPD). It may also identify pulmonary congestion/oedema and is more useful in patients with suspected HF in the acute setting. DIAGNOSTİC TESTS in HF
 should be considered to: (i)Exclude alternative causes of dyspnoea (if the level is below the exclusion cut-point HF is very unlikely) (ii) Obtain prognostic information. A chest radiograph (X-ray) should be considered to detect/exclude certain types of lung disease, e.g. cancer (does not exclude asthma/ COPD). It may also identify pulmonary congestion/oedema and is more useful in patients with suspected HF in the acute setting. DIAGNOSTİC TESTS in HF.")
39
CMR imaging is recommended to evaluate cardiac structure and function, to measure LVEF, and to characterize cardiac tissue, especially in subjects with inadequate echocardiographic images or where the echocardiographic findings are inconclusive or incomplete (but taking account of cautions/contraindications to CMR). Coronary angiography is recommended in patients with angina pectoris, who are considered suitable for coronary revascularization, to evaluate the coronary anatomy. Myocardial perfusion/ischaemia imaging (echocardiography, CMR, SPECT, or PET) should be considered in patients thought to have CAD, and who are considered suitable for coronary revascularization, to determine whether there is reversible myocardial ischaemia and viable myocardium. Left and right heart catheterization is recommended in patients being evaluated for heart transplantation or mechanical circulatory support, to evaluate right and left heart function and pulmonary arterial resistance. Exercise testing should be considered: (i) To detect reversible myocardial ischaemia (ii) As part of the evaluation of patients for heart transplantation and mechanical circulatory support (iii) To aid in the prescription of exercise training (iv) To obtain prognostic information.
 should be considered in patients thought to have CAD, and who are considered suitable for coronary revascularization, to determine whether there is reversible myocardial ischaemia and viable myocardium. Left and right heart catheterization is recommended in patients being evaluated for heart transplantation or mechanical circulatory support, to evaluate right and left heart function and pulmonary arterial resistance. Exercise testing should be considered: (i) To detect reversible myocardial ischaemia (ii) As part of the evaluation of patients for heart transplantation and mechanical circulatory support (iii) To aid in the prescription of exercise training (iv) To obtain prognostic information..")
45
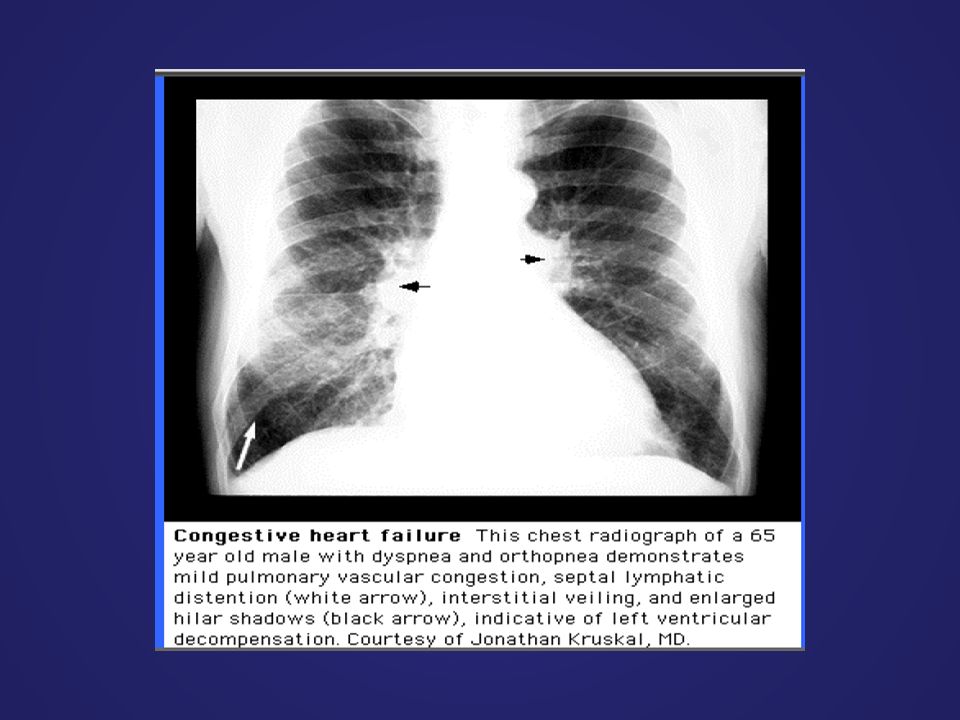
Chest X-ray in Heart Failure Cardiomegaly Cephalization of the pulmonary vessels Kerley B-lines Pleural effusions

46
Cardiomegaly

47
Pulmonary vessel congestion

48
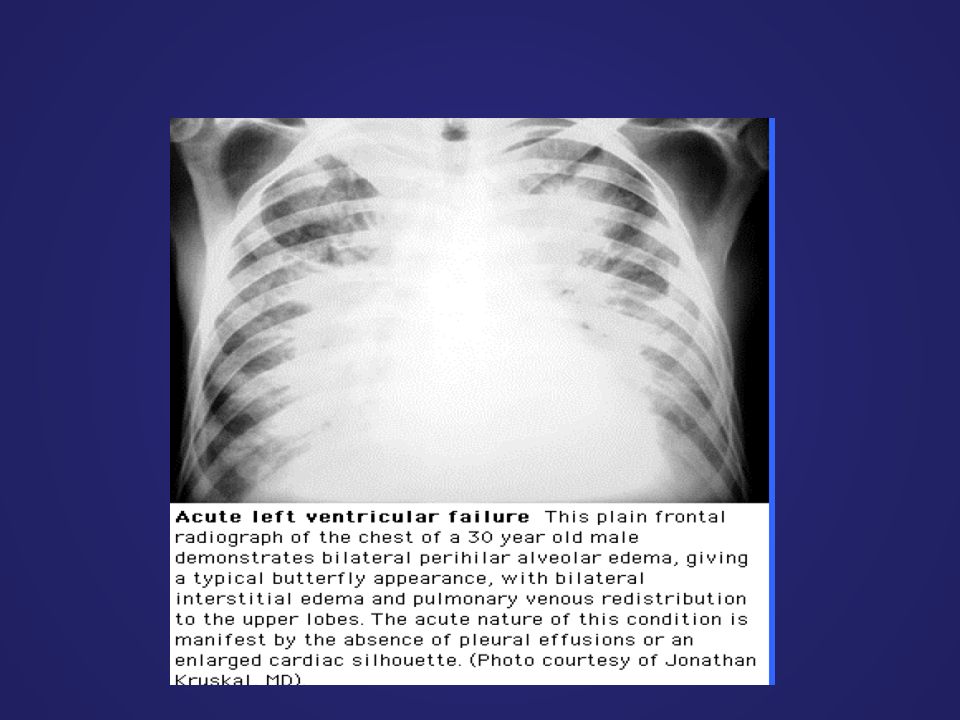
Pulmonary Edema due to Heart Failure

49
Kerley B lines

52
Classification of HF

53
Symptoms and signs of heart failure 1.forward failure: symptoms result from inability of the heart to pump enough symptoms result from inability of the heart to pump enough blood to the periphery (from left heart), or to the lungs (from blood to the periphery (from left heart), or to the lungs (from the right heart) the right heart) a) forward failure of left heart:-muscle weakness, fatigue, a) forward failure of left heart:- muscle weakness, fatigue, dyspepsia, oliguria.... dyspepsia, oliguria.... general mechanism: tissue hypoperfusion b) forward failure of right heart:- hypoperfusion of the b) forward failure of right heart: - hypoperfusion of the lungs disorders of gas lungs disorders of gas exchange exchange - decreased blood supply to the left heart to the left heart
 forward failure of right heart:- hypoperfusion of the b) forward failure of right heart: - hypoperfusion of the lungs disorders of gas lungs disorders of gas exchange exchange - decreased blood supply to the left heart to the left heart.")
54
2. backward failure: symptoms result from inability of the heart to accept – symptoms result from inability of the heart to accept the blood comming from periphery and from lungs the blood comming from periphery and from lungs a.backward failure of left heart: – increased pulmonary capillary pressure dyspnoea – increased pulmonary capillary pressure dyspnoea and tachypnoea, pulmonary edema (cardiac asthma) and tachypnoea, pulmonary edema (cardiac asthma) arterial hypoxemia and hypercapnia.... arterial hypoxemia and hypercapnia.... b. backward failure of right heart: increased pressure in systemic venous system – increased pressure in systemic venous system peripheral edemas, hepatomegaly, ascites nocturnal diuresis.... peripheral edemas, hepatomegaly, ascites nocturnal diuresis....
 and tachypnoea, pulmonary edema (cardiac asthma) arterial hypoxemia and hypercapnia.... arterial hypoxemia and hypercapnia.... b. backward failure of right heart: increased pressure in systemic venous system – increased pressure in systemic venous system peripheral edemas, hepatomegaly, ascites nocturnal diuresis.... peripheral edemas, hepatomegaly, ascites nocturnal diuresis.....")
55
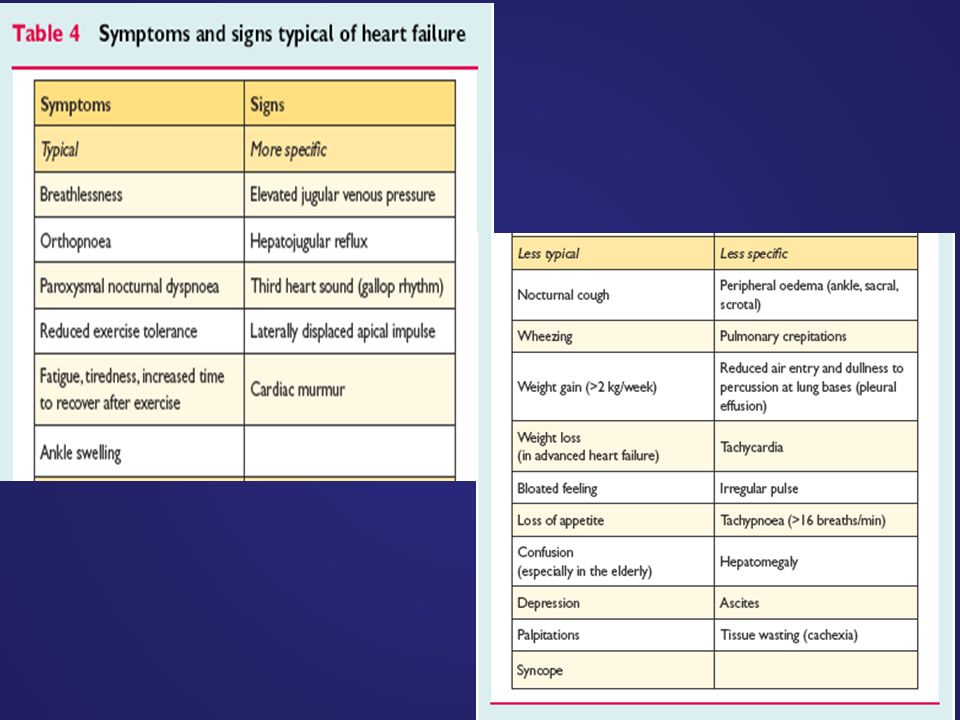
Symptoms

56
Functional and metabolic alterations in HF low CO → poor perfusion of organs (forward failure) blood damming in the vein → pulmonary or systemic edema (backward failure)
 blood damming in the vein → pulmonary or systemic edema (backward failure)")
57
Congestion of pulmonary circulation In LHF, the left ventricular pressure ↑ →left atrium pressure ↑ →pulmonary veins, capillaries →pulmonary congestion and pulmonary edema

58
left heart failure (increased LVEDP) increased pulmonary venous pressure ↓ pulmonary congestion and pulmonary edema ↓↓ increased airway resistance reduced compliance of lung ↓ ↓ decreased O2 inhalation more work of breathing to distend the stiff lungs ↓ increased O2 consumption hypoxemia+ metabolic acidosis dyspnea ↓ ↓
 increased pulmonary venous pressure ↓ pulmonary congestion and pulmonary edema ↓↓ increased airway resistance reduced compliance of lung ↓ ↓ decreased O2 inhalation more work of breathing to distend the stiff lungs ↓ increased O2 consumption hypoxemia+ metabolic acidosis dyspnea ↓ ↓")
59
Exertional dyspnea The patient with exertional dyspnea has no dyspnea at rest, but will feel breathless if he had a exercise. Mechanism: the need for oxygen in exercise↑ HR↑ , diastolic phase ↓ blood back to heart ↑, pulmonary congestion↑, Pulmonary compliance↓

60
Orthopnea Orthopnea indicates the situation that the dyspnea will be relieved by sitting or standing, and will aggravate in the recumbent position..

61
mechanism: In the position of sitting, more blood stay in lower extremities. In the position of sitting, the volume of the thoracic cavity ↑ In the recumbent position, more fluid will be absorbed into the blood and will aggravate the pulmonary congestion.

62
Paroxysmal nocturnal dyspnea The patients awakens suddenly with a feeling of extreme dyspnea, and sits upright, gasps for a while. Then he feels better and sleep again at night. Mechanism: (a)When the patient lies down at night, more blood move back to heart. The volume load is increased. (b) The respiratory center is depressed at night. It is not sensitive to the stimulation of hypoxia, so the attack occurs suddenly. (c) During sleeping, the sympathetic activity is reduced, the caliber of airway reduce, the airway resistance increase.
When the patient lies down at night, more blood move back to heart. The volume load is increased. (b) The respiratory center is depressed at night. It is not sensitive to the stimulation of hypoxia, so the attack occurs suddenly. (c) During sleeping, the sympathetic activity is reduced, the caliber of airway reduce, the airway resistance increase..")
63
Pulmonary edema In LHF, CO↓, left atrial and left ventricular end-diastolic pressure↑, the pulmonary capillary filtration pressure ↑ Permiability of the capillary ↑

64
Right Heart Failure Signs and Symptoms –fatigue, weakness, lethargy –wt. gain, inc. abd. girth, anorexia, RUQ pain –elevated neck veins –Hepatomegaly +HJR –may not see signs of LVF

65
Measuring Jugular Venous Pressure

66
What does this show?

67
What is present in this extremity, common to right sided HF?

68
Decreased cardiac output (CO) Manifestation: –Pale or cyanosis –Fatigue and limb weakness –mental confusion and disturbed behavior (impairment of memory, anxiety, restlessness and insomnia) –Oliguria –Cardiac shock
 Manifestation: –Pale or cyanosis –Fatigue and limb weakness –mental confusion and disturbed behavior (impairment of memory, anxiety, restlessness and insomnia) –Oliguria –Cardiac shock")
69
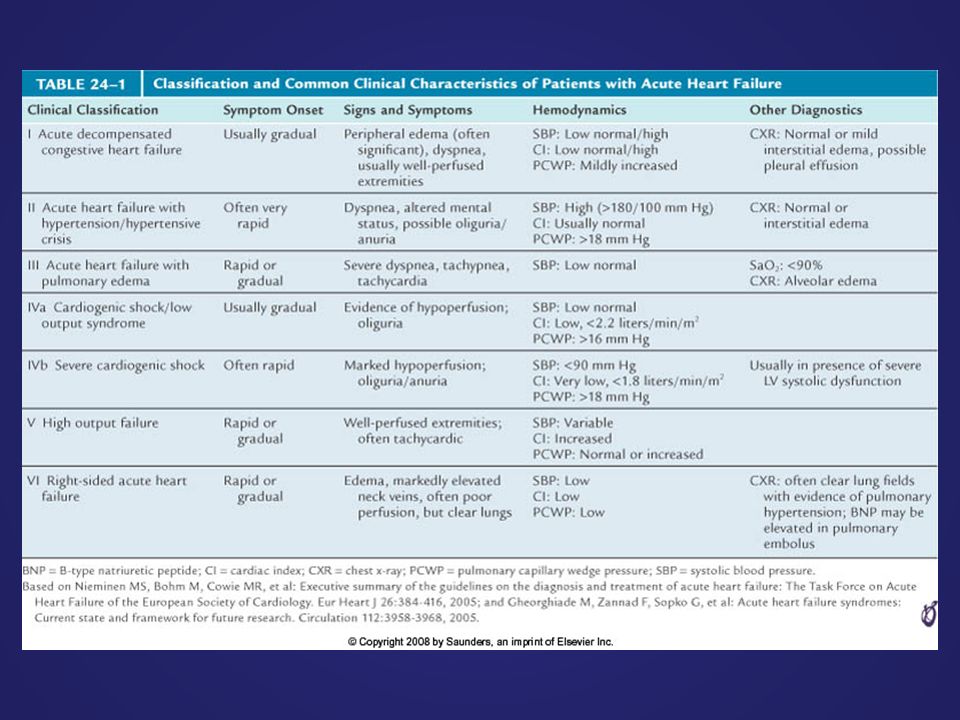
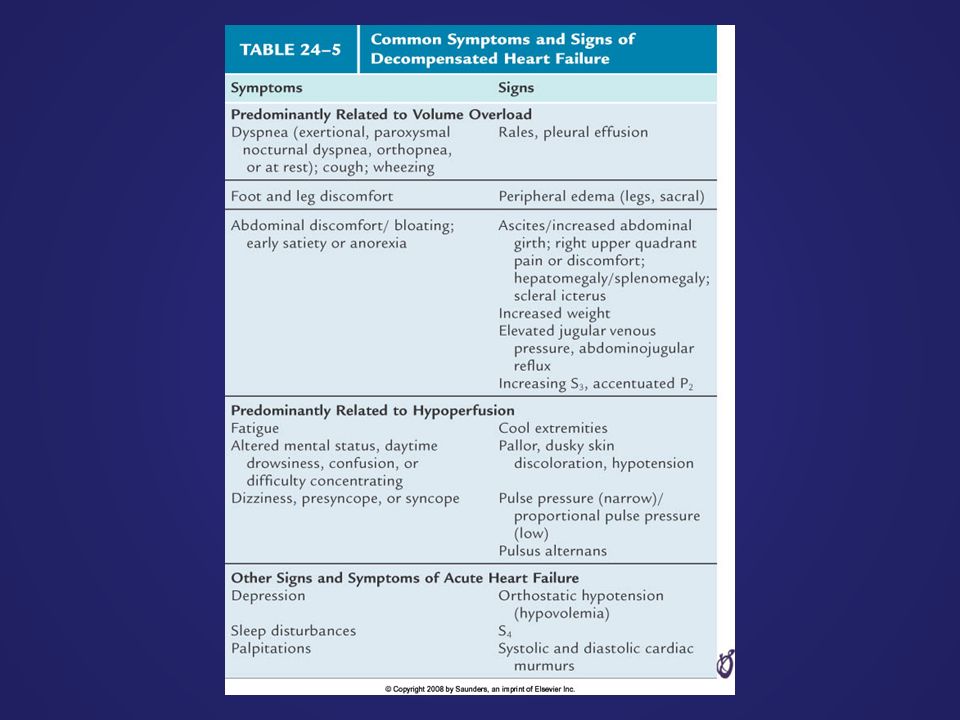
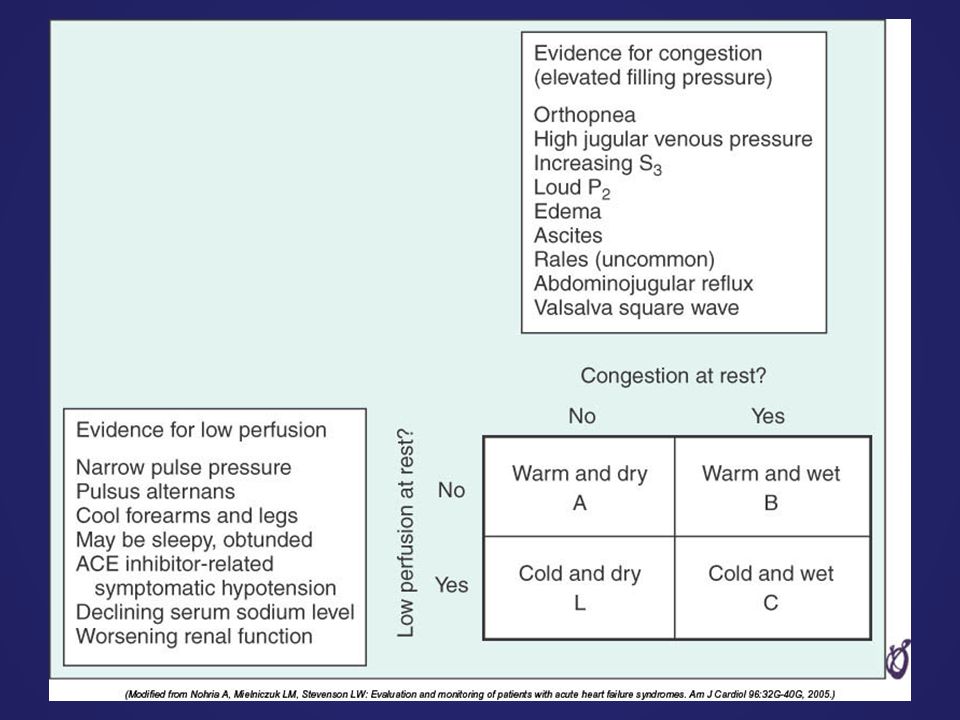
ACUTE HEART FAILURE

70
Concep tu al ill us tr at io n de pi ct in g co n ge sti ve he ar t fa il ur e. Pulmo n ar y ed e m a be gi ns wi th a n in cr ea se d fil tr at io n th ro u g h th e lo os e ju nc ti o ns of th e p ul m o n ar y ca pi ll ar ie s. Cop yrig ht © 1998, Lyn ne Lars on All righ ts rese rved. As the in tr ac a pi ll ar y pr es su re in cr ea se s, n or m al ly i m pe r m ea bl e (ti g ht ) ju nc ti o ns be t w ee n th e al ve ol ar ce lls o pe n, pe r m itt in g al ve ol ar fl oo di n g to oc cu r. | Services | Profile | Clients | Image Gallery | ServicesProfileClientsImage Gallery | Contact Information | Home | Contact InformationHome Concep tu al ill us tr at io n de pi ct in g co n ge sti ve he ar t fa il ur e. Pulmo n ar y ed e m a be gi ns wi th a n in cr ea se d fil tr at io n th ro u g h th e lo os e ju nc ti o ns of th e p ul m o n ar y ca pi ll ar ie s. Cop yrig ht © 1998, Lyn ne Lars on All righ ts rese rved. As the in tr ac a pi ll ar y pr es su re in cr ea se s, n or m al ly i m pe r m ea bl e (ti g ht ) ju nc ti o ns be t w ee n th e al ve ol ar ce lls o pe n, pe r m itt in g al ve ol ar fl oo di n g to oc cu r. | Services | Profile | Clients | Image Gallery | ServicesProfileClientsImage Gallery | Contact Information | Home | Contact InformationHome Pulmonary edema begins with an increased filtration through the loose junctions of the pulmonary capillaries. As the intracapillary pressure increases, normally impermeable (tight) junctions between the alveolar cells open, permitting alveolar flooding to occur. Acute Decompensated Heart Failure (ADHF) Pulmonary Edema
 ju nc ti o ns be t w ee n th e al ve ol ar ce lls o pe n, pe r m itt in g al ve ol ar fl oo di n g to oc cu r. | Services | Profile | Clients | Image Gallery | ServicesProfileClientsImage Gallery | Contact Information | Home | Contact InformationHome Concep tu al ill us tr at io n de pi ct in g co n ge sti ve he ar t fa il ur e. Pulmo n ar y ed e m a be gi ns wi th a n in cr ea se d fil tr at io n th ro u g h th e lo os e ju nc ti o ns of th e p ul m o n ar y ca pi ll ar ie s. Cop yrig ht © 1998, Lyn ne Lars on All righ ts rese rved. As the in tr ac a pi ll ar y pr es su re in cr ea se s, n or m al ly i m pe r m ea bl e (ti g ht ) ju nc ti o ns be t w ee n th e al ve ol ar ce lls o pe n, pe r m itt in g al ve ol ar fl oo di n g to oc cu r. | Services | Profile | Clients | Image Gallery | ServicesProfileClientsImage Gallery | Contact Information | Home | Contact InformationHome Pulmonary edema begins with an increased filtration through the loose junctions of the pulmonary capillaries. As the intracapillary pressure increases, normally impermeable (tight) junctions between the alveolar cells open, permitting alveolar flooding to occur. Acute Decompensated Heart Failure (ADHF) Pulmonary Edema.")
75
Normal sistolik fonksiyonlu KY/HFnlEF More common in obese and women Chronic renal failure, AF, HT is more often + EF≥ %40-50 Symptoms of HF BNP high CAD +/- Often no cardiomegaly, LVH Diastolic disfunction +++

76
Genel görünüm –Hafif KY durumunda kısa süre dinlenme ile çabuk rahatlar ve orta derecede aktivite ile belirgin yakınmaları olur –Ciddi yetmezliği olan olgularda ise sırt üstü yatınca yakınmaları olur (ortopneik) –Son aşamada oturur iken de sıkıntılı ve hava açlığı içinde –Yeni başlangıçlı beslenmesi iyi, kronik olgularda malnutrisyon kaşeksi –Kronik sistemik venöz basınç yükselmesi sonucu exoftalmus –Ciddi triküspit yetmezliği gözde ve boyun venlerinde pulsasyona neden olur –Santral siyanoz, ikter, malar rash ciddi olgularda Fizik muayene
 –Son aşamada oturur iken de sıkıntılı ve hava açlığı içinde –Yeni başlangıçlı beslenmesi iyi, kronik olgularda malnutrisyon kaşeksi –Kronik sistemik venöz basınç yükselmesi sonucu exoftalmus –Ciddi triküspit yetmezliği gözde ve boyun venlerinde pulsasyona neden olur –Santral siyanoz, ikter, malar rash ciddi olgularda Fizik muayene")
77
–Çok ileri olgularda özellikle KO akut olarak düşünce sistolik kan basıncı düşer ve nabız zayıf hızlı alınır, NB/SKB oranı düşer Artmış adrenerjik aktivite –Taşikardi, terleme, solukluk ve sogukluk, periferik siyanoz, periferik venlerde belirgin genişleme Solunum sistemi –Dispneik görünüm –Takipne –Krepitan raller (Akciğer bazalinden başlar) –Akciğer ödeminde ise wheezing öksürük, kanlı ve köpüklü balgam olabilir
 –Akciğer ödeminde ise wheezing öksürük, kanlı ve köpüklü balgam olabilir")
78
Fizik muayene Sistemik venöz hipertansiyon –Jugular ven distansiyonu –Normalde JVD solunumla azalır iken KY de solunumla artar (kussmal belirtisi) Hepatojugular reflü –Sağ taraflı KY olgularında Ödem (pretibial, sacral) –KY kardinal bulgularından –Sistemik venöz basınç ile doğru orantılı değildir –Sağ ve sol KY bulgularının bulunmadığı ND bulunmadığı durumlarda gözlemlenebilir KY özgün değildir. Kronik venöz yetm, Nefrotik send, hipoproteinemi

79
Fizik muayene Hepatomegali –Kronik sağ taraflı KY bulgusudur akut kalp yet. Bulunabilir –Hızlı hassas ağrılı –Ciddi TY olgularında Pulsatil hepatomegali (sağ atr “V” dalgası) –Presistolik pulsasyon (“a” dalgası) tirküspit darlığı, konstriktif perikardit, restriktif KMP ve pulmoner HT Hidrotoraks –Sistemik ve pulmoner hipertansiyon –Genellikle bilateral –Tek taraflı olursa sıklıkla sağ tutulur, dispne ciddiyeti artar.
 –Presistolik pulsasyon ( a dalgası) tirküspit darlığı, konstriktif perikardit, restriktif KMP ve pulmoner HT Hidrotoraks –Sistemik ve pulmoner hipertansiyon –Genellikle bilateral –Tek taraflı olursa sıklıkla sağ tutulur, dispne ciddiyeti artar..")
80
Fizik muayene Asit –Hepatik ven basınç artışı sonucu, uzun süreli venöz hipertansiyon + Pulsus alternans –KY de SV çıkışına resistans olduğu durumlarda HT, AD, koroner atheroskleroz

81
Fizik muayene Kardiyomegali –Nonspesifik bir bulgu Protodiyastolik gallop (s3) –Başka nedenler olmaksızın KKY de dekompanse hastada duyulan en erken fizik muayene bulgusudur. 2.kalp sesi şiddetlenir,sistolik üfürüm –P2 artması pulmoner sistolik hipertansiyon, tedavi sonrası azalır yada kaybolabilir –Dekompanse KY olgularında Mitral ve trikuspit kaçak (ventriküler dilatasyon) Kardiyak kaşeksi –Uzun süreli KY olgularında özellikle sağ ventrikül Yetm. Hepatik ve intestinal kongesyon ve bazen digital intoksikasyonu. –Yağ emilim problemi ve protein kaybettirici enteropati –Miyokard oksijen tüketim artışına sekonder metabolizma artışı, solunum işlevi artar
 Kardiyak kaşeksi –Uzun süreli KY olgularında özellikle sağ ventrikül Yetm. Hepatik ve intestinal kongesyon ve bazen digital intoksikasyonu. –Yağ emilim problemi ve protein kaybettirici enteropati –Miyokard oksijen tüketim artışına sekonder metabolizma artışı, solunum işlevi artar.")
82
Tanısal çalışmalar Kalp kateterizasyonu –KKY etyolojisini belirlemek –KAH varlığının ve yaygınlığının değerlendirilmesi kalp kateterizasyonu ve koroner anjiyografi—özellikler girişimsel müdahaleler düşünülüyorsa

83
Karaciğer fonk testleri –Konjesyon ve kardiyak siroz hepatik fonksiyonların bozulmasına neden olur AST, ALT, LDH ve diğer enzimler yükselir –Hiperbilirubinemi (direkt ve indirekt) Sarılık –Akut hepatik konjesyon belirgin sarılık bil:15-20 mg/dl AST 10 kat yükselir, serum ALK-P yükselir, protrombin zamanı uzar----tablo viral hepatite benzer. TÜMÜ tedavi ile DUZELIR. uzun süreli olgularda albumin sentezi bozulur ve hipoalbuminemi görülür ödem artar. K vit bağımlı koagulasyon faktör yapımı bozulur, PTZ uzar

84
Semptom ve bulgular Nefes darlığı –Dispne yada nefes nefese kalma hali (hava açlığı hissetme) –KKY nin en erken bulgusudur. –Başlangıçta egzersiz ile, hastalığın ilerlediği durumlarda daha az hareket ile ortaya çıkar –Bu aşamadan sonra Paroksismal nakturnal dipne ortopne istirahate ND –Sol kalp Yetm. sağ kalp Yetm. Nefes darlığı yakınması azalır –Sağ kalp yetmezliğinde ND yakınması nadirdir çünkü pulmoner konjesyon yoktur fakat sağ kalp yetm. KO, solunum kası hipoperfüzyonu ve hipoksi nedeni ile gelişen asidoz ND yapabilir.

85
Semptom ve bulgular Paroksismal nokturnal dispne –Bir süre sırt üstü yatıp uyuduktan sonra hasta aniden boğucu karakterde ND ile uyanır oturur yada pencere açarak yada dışarı çıkarak hava açlığını gidermeye çalışır –Ortopneden önce karşılaşılır –Bronkospazm yada wheezing duyulabilir (astım krizi ile karışır) –Yaklaşık 30 dk sürer –Nedeni infratorasik intertisyel sıvının dolaşıma katılması sırt üstü yatmakla pulmoner venöz basınç artışı (özellikle sol ventrikül diyastolik disfonksiyonunda)
 –Yaklaşık 30 dk sürer –Nedeni infratorasik intertisyel sıvının dolaşıma katılması sırt üstü yatmakla pulmoner venöz basınç artışı (özellikle sol ventrikül diyastolik disfonksiyonunda)")
86
Semptom ve bulgular Ortopne –Sırtüstü yatınca oluşan oturunca geçen ND –Ortopneik hasta ancak oturarak uyuyabilir yada yastık sayısını arttırırlar –PND ile benzer mekanizmaya sahiptir fakat daha ileri bir klinik durumu gösterir Halsizlik yorgunluk –Özellikle ektremitelerde –Düşük kardiyak output, düşük kas perfüzyonu, egzersiz intoleransı –Yemeklerden sonra daha fazla (kan akımı mide bağırsak sistemine yönlenir) –Pulmoner konjesyon olmaksızın görülebilir. –Hiponatremiye bağlı görülebilir

87
Semptom ve bulgular Nocturi/oliguri –Sık ve KKY nin erken bulgularından –Su ve tuz filtrasyonu ayaktaki hastada azalır –Sırtüstü yatınca venöz dönüş artar ve gün içindeki kazanılmış tuz ve su atılımı böbrek kan akımının artması ile artar idrar oluşumu artar –Oliguri ciddi KKY bulgusudur son aşama klinik tabloda gözlemlenir

88
Semptom ve bulgular –Serebral semptomlar Yaşlı hastalarda konfüzyon, hafıza sorunları, anksiyete uykusuzluk,dezorientasyon, delirium, halusinasyonlar Neden ?? Serebral perfuzyon azalması

89
Semptom ve bulgular Abdominal semptomlar –Hepatik konjesyon ve karın ön duvarı ve intraabdominal organların ödemi –Asit, abdominal dolgunluk, gerginlik, erken doyma, iştahsızlık gaz, kusma. –Kıyafetlerin dar gelip gelmemesi bedende değişim sorgulanmalı –İntestinal konjesyon –Yağ absorbsiyon bozukluğu –Protein kaybettirici enteropati

Benzer bir sunumlar




















 = Boy (cm)-100 (Erkek) İdeal ağırlık (kg) = Boy (cm)-105 (Kadın) Obezite İdeal ağırlıktan % 20 ↑ Türkiye Toplam nüfusun %>")


 Doç. Dr. Kazım.>")

