Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
GASTROENTERITIS And FOOD POISINING Meral SÖNMEZOĞLU, MD
Yeditepe University Hospital Associate Professor Department of Infectious Diseases and Microbiology

2
Learning Objectives Describe and classify of gastroenteritis and food poisoning Explain the epidemiology of gastroenteritis and possible etiologic agents in various clinical settings Know the pathophysiology of gastroenteritis Develop an information on diagnosis and management plan for gastroenteritis

3
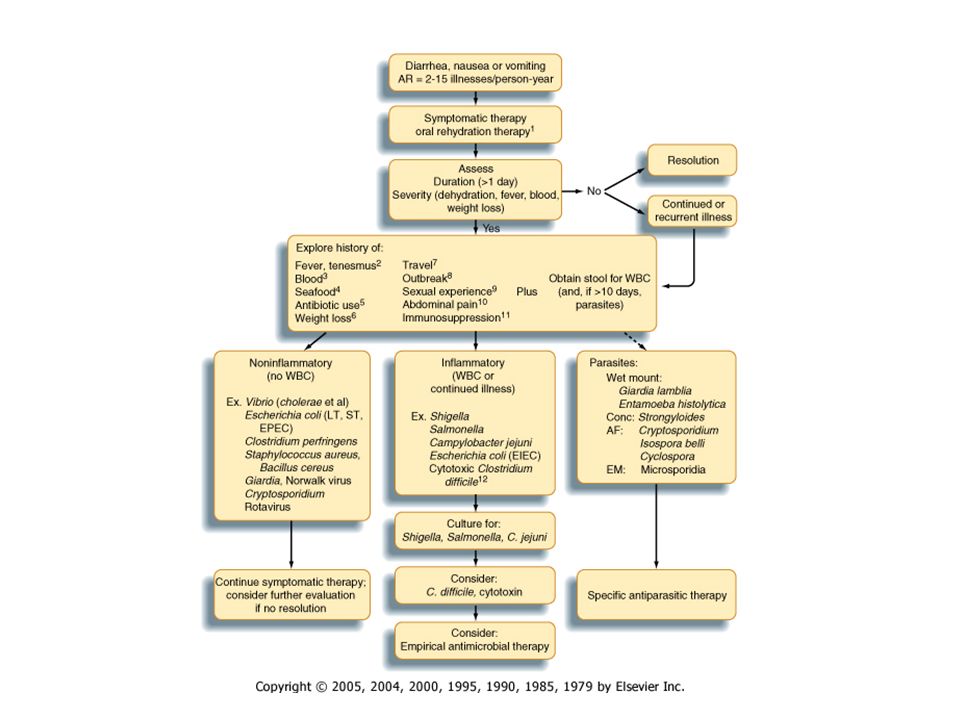
With the exception of Helicobacter pylori gastritis, the term gastroenteritis is applied to syndromes of diarrhea or vomiting that tend to involve noninflammatory infection in the upper small bowel or inflammatory infection in the colon

4
Risk of acquiring a gastrointestinal infection varies greatly with age, living conditions, personal and cultural habits, and group exposures The second epidemiologic determinant of risk for enteric infection is where you are The third determinant of risk is when you are there. The majority of enteric illnesses in temperate climates occur during winter months. The opposite is true in tropical countries, where distinct summer peaks of illnesses are common. The role of rainfall is uncertain, and some adjacent areas with similar monsoon climates have opposite seasons of major diarrheal illnesses, as illustrated by the peak seasons for cholera

5
Host defense factors Gastric acidity Intestinal motility
Intestinal microflora Mucus Systemic and local immune mechanisms Others (e.g. breast feeding)
")
6
Bacterial virulence factors
Adherence Enterotoxin production Cytotoxin production Mucosal invasion

7
Mechanisms of infection
Ingestion of preformed toxin (food poisoning) Fecal-oral contamination Food, flies, fingers, feces, and fomites Contaminated food Animal reservoir Fecal-oral contamination of food Infectious dose varies (~100 to 109)
 Fecal-oral contamination. Food, flies, fingers, feces, and fomites. Contaminated food. Animal reservoir. Fecal-oral contamination of food. Infectious dose varies (~100 to 109)")
8
Infectious Doses of Enteric Pathogens
Shigella 10 to 102 Campylobacter jejuni 102 to 106 Salmonella 105 Escherichia coli 108 Vibrio cholerae Giardia lamblia 10 to 102 cysts Entamoeba histolytica Cryptosporidium parvum 1 to 103 oocysts

9
DIARRHEA Alteration in a normal bowel movement
Characterized by an increased in the water content, volume, or frequency of stools >3 or more stools and at least 200 gr Decrease in consistency (soft or liquid) and an increase in frequency of bowel movement to >3 stools per day
 and an increase in frequency of bowel movement to >3 stools per day.")
10
INFECTIOUS DIARRHEA 3-5 billion episodes yearly
Major cause of worldwide morbidity and mortality 5 million deaths yearly, 80% < 1 year of age Major cause of work/school absenteeism Major economic burden, especially in developing countries

11
INFECTIOUS DIARRHEA Due to an infectious etiology
Accompanied by symptoms of nausea, vomiting, or abdominal cramps. Acute diarrhea is an episode of diarrhea of <14 days in duration Persistent diarrhea is of >14 days in duration Chronic diarrhea lasts >30 days

12
INFECTIOUS DIARRHEA Second leading cause of morbidity and mortality worldwide More than 2 million deaths annually Some causes of infectious diarrhea result in serious long term sequelae (HUS-STEC,G-B Campylobacter)
")
13
Inappropriate feeding Food intolerance Climate
Etiology of Diarrhea Infective Non infective Allergic Symptomatic Inappropriate feeding Food intolerance Climate Viruses Bacteria Parasites Fungi

14
Major Pathogens Bacterial infection Campylobacter, Shigella, and Salmonella Protozoal infection Cryptosporidium species, Giardia lamblia, Isospora belli, Entamoeba histolitica, Microsporidium species Toxin induced E. coli and Clostridium difficile Mycobacterial infection M. tuberculosis, M. Avium complex Helminthic infection Strongyloides stercoralis Fungal infection Candida species (seldom a cause of diarrhea)
")
15
Etiology of Infectious Diarrhea
(in (((8developed countries) • 70-80% is viral • 10-20% is bacterial – Bacterial are responsible for most severe cases • < 10% is parasitic
 • 70-80% is viral. • 10-20% is bacterial. – Bacterial are responsible for most severe cases. • < 10% is parasitic.")
16
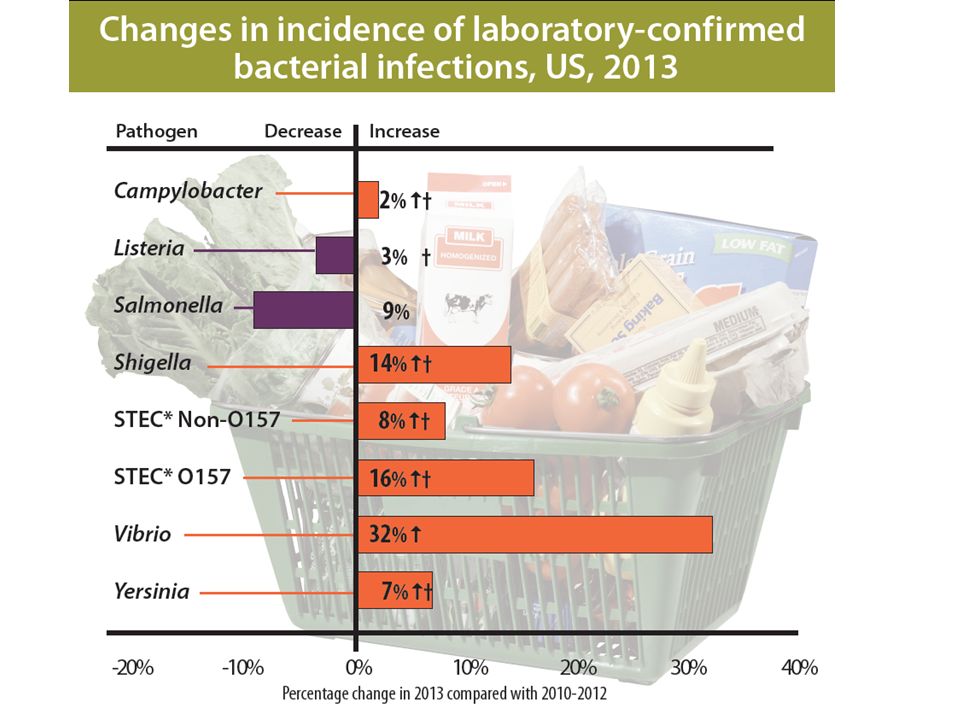
Infectious Causes – Foodnet 2005
Microorganism # Incidence (per 100,000) Salmonella 6,471 14.55 Campylobacter 5,655 12.72 Shigella 2,078 4.67 Cryptosporidium 1,313 2.95 STEC 0157 473 1.06 Yersinia 159 0.36 STEC non-0157 146 0.33 Listeria 135 0.3 Vibrio 119 0.27 Cyclospora 65 0.15 44.5 million persons (15% of the US pop.) Laboratory confirmed infections – 16,614 Salmonella Subtypes Typhimurium 19% Enteritidis 18% Newport 10% Heidelberg 6% Javiana 5%
 Salmonella. 6, Campylobacter. 5, Shigella. 2, Cryptosporidium. 1, STEC Yersinia STEC non Listeria Vibrio Cyclospora million persons (15% of the US pop.) Laboratory confirmed infections – 16,614. Salmonella Subtypes. Typhimurium. 19% Enteritidis. 18% Newport. 10% Heidelberg. 6% Javiana. 5%")
19
Mechanisms of infection
Ingestion of preformed toxin (food poisoning) Fecal-oral contamination Food, flies, fingers, feces, and fomites Contaminated food Animal reservoir Fecal-oral contamination of food Infectious dose varies (~100 to 109)
 Fecal-oral contamination. Food, flies, fingers, feces, and fomites. Contaminated food. Animal reservoir. Fecal-oral contamination of food. Infectious dose varies (~100 to 109)")
21
Host defense factors Gastric acidity Intestinal motility
Intestinal microflora Mucus Systemic and local immune mechanisms Others (e.g. breast feeding)
")
22
Defense Barriers of the Enterocytes
3 1 2 Physical barrier: mucus 2. Bacteriological (flora) 3. Immunological: Secretory IgA
 3. Immunological: Secretory IgA.")
23
Morphology of Intestinal Mucosa
Villi covered mainly (90%) by tall columnar absorptive cells (Enterocytes) having a micrevillar brush border Crypts of lieberkuhn Covered mainly by short columnar secretory cells Goblet cells without brush border
 by tall columnar absorptive cells (Enterocytes) having a micrevillar brush border. Crypts of lieberkuhn. Covered mainly by short columnar secretory cells. Goblet cells. without brush border.")
24
Bacterial virulence factors
Adherence Enterotoxin production Cytotoxin production Mucosal invasion

25
Diarrhea Non-inflammatory Inflammatory
Watery diarrhea, no blood or mucus or pus in stool, no fever or systemic signs Secretory or osmotic mechanism Dehydration may occur Generally self-limited and more benign Therapy generally supportive Inflammatory Frequent lower volume stool, mucoid, bloody, or purulent. Often with fever or systemic signs, tenesmus, urgency Exudative mechanism Dehydration rare Less benign

26
Osmotic Diarrhea Interferes with absorption of water
Definition: Increased amounts of poorly absorbed, osmotically active solutes in gut lumen Interferes with absorption of water Solutes are ingested Magnesium sulfate or citrate or magnesium containing antacids Sorbitol Malabsorption of food Lactase deficiency Celiac sprue Variety of infectious organisms (particularly viruses)
")
27
Secretory Diarrhea Excess secretion of electrolytes and water across mucosal surface Usually coupled with inhibition of absorption Clinical features stools very watery stool volume large fasting does not stop diarrhea

28
Secretory Diarrhea Bacterial or viral enterotoxins
Cholera, enterotoxigenic E. coli, B. cereus, S. aureus, Rotavirus, Norwalk virus Hormonal secretagogues Certain laxatives (castor oil, senna)
")
29
Exudative Diarrhea Intestinal or colonic mucosa inflamed and ulcerated
Leakage of fluid, blood, pus Impairment of absorption Increased secretion (prostaglandins) The extent of bowel involved determines Severity of diarrhea Systemic signs and symptoms (abdominal pain, fever, etc)
 The extent of bowel involved determines. Severity of diarrhea. Systemic signs and symptoms (abdominal pain, fever, etc)")
30
Exudative Diarrhea Infectious, invasive organisms
Shigella, Campylobacter, Yersinia, E. histolytica, EHEC, C diff Idiopathic inflammatory bowel disease Crohns disease Ulcerative Colitis Ischemia

31
Associated Signs & Symptoms
• Systemic illness/fever – invasive pathogen involvement • Vomiting as predominant symptom – likely viral organism or food poisoning • Abdominal pain – inflammatory process (Shigella, Campylobacter, EHEC) • Persistent abdominal pain and fever: Yersinia
 • Persistent abdominal pain and fever: Yersinia.")
32
Antibiotic therapy may be considered however, in the following
When to Consider ABX Most cases of diarrhea resolve spontaneously and do not require treatment with antibiotics. Antibiotic therapy may be considered however, in the following circumstances: – When signs and symptoms include: • Fever • Bloody stools • Presence of fecal leukocytes or occult blood; – To reduce fecal excretion and environmental contamination by a highly infectious agent like Shigella; – For persistent or life-threatening diarrheal infections such as cholera; – For immunocompromised patients.

33
Antibiotics – Shigella, ETEC, ameobiasis, Giardia, cholera, S. typhi
• Most helpful for: – Shigella, ETEC, ameobiasis, Giardia, cholera, S. typhi •May help for: – non-typhi Salmonella & Camplyobacter • Can prolong fecal shedding, use only if severe case • Not useful for viral, EIEC • Can be harmful in EHEC (O157:H7) • Multi-Drug resistance is a rapidly growing problem
 • Multi-Drug resistance is a rapidly growing problem.")
34
Acute infectious diarrhea
Bacterial infection Common nonbacterial infection HKO antigens Common among population – particular day care centers Developing countries – serious health effects, fatal In the U.S., 1/3 due to contaminated food

35
HKO antigens H = flagellar antigen K= capsular antigen
O= cell wall antigen Ex. E. coli O157:H7

36
Bacterial Salmonella Shigella Shiga-toxin producing Escherichia coli
Non-shiga-toxin E. coli Campylobacter Yersinia Clostridium difficile Vibrio cholerae

37
Acute Diarrhea in Children
The most important infective causes of acute diarrhea in developing countries in children are: Rotavirus Enterotoxigenic escherichia coli Shigella Campylobacter jejuni Salmonella typhimurium

38
Salmonella Contaminated animal products Salmonellosis - mild
Typhoid fever – severe Normal flora in animals

39
Cases of typhoid fever and salmonelloses.
Fig Data on the prevalence of typhoid fever and other salmonelloses

40
Nontyphoidal Salmonella
Salmonella typhimurium and enteritidis Clinical syndromes Gastroenteritis and colitis Bacteremia and endocarditis Enteric fever (typhi and paratyphi) Localized tissue infection Carrier state (> 1 year) Food-borne illness (poultry, meat, eggs)
 Localized tissue infection. Carrier state (> 1 year) Food-borne illness (poultry, meat, eggs)")
41
Bacterial infection: Salmonella
Presenting Signs and Symptoms Clinical Symptoms may evolve Fever; general malaise Sometimes no GI symptoms If there are GI symptoms, will see: Bloody diarrhea Abdominal pain Weight loss

42
Salmonellosis Fever, cramping, abdominal pain, and diarrhea within 8-48 hours after ingestion of infective dose (contaminated poultry, shell eggs, dairy products, beef, exotic pets such as reptiles) Inflammatory (neutrophilic) enteritis most typically involving the small bowel mucosa, occasional cause of colitis with crypt abscesses and erosive ulceration of colonic mucosa (Salmonella serotype Typhimurium) Moderate number of fecal neutrophils, usually fewer than in shigellosis except colitis with blood and pus in stool
 Inflammatory (neutrophilic) enteritis most typically involving the small bowel mucosa, occasional cause of colitis with crypt abscesses and erosive ulceration of colonic mucosa (Salmonella serotype Typhimurium) Moderate number of fecal neutrophils, usually fewer than in shigellosis except colitis with blood and pus in stool.")
43
Complications of Salmonellosis
Diarrhea usually self-limited (3-7 days), if persists >10 days another microbial etiology likely Occasional dehydration requiring hospitalization Bacteremia (1-4% immunocompetent cases) (persistent bacteremia suggests endovascular infection site such as atherosclerotic plaques and aneurysms) After resolution of diarrhea mean duration of carriage in stool is 4-5 weeks
, if persists >10 days another microbial etiology likely. Occasional dehydration requiring hospitalization. Bacteremia (1-4% immunocompetent cases) (persistent bacteremia suggests endovascular infection site such as atherosclerotic plaques and aneurysms) After resolution of diarrhea mean duration of carriage in stool is 4-5 weeks.")
44
Bacterial infection: Salmonella Diagnostics
Stool culture Salmonella bacilli may be found in stool/blood cultures Serology: positive Widal test with increased titers

45
Management and Treatment
TMP/SMX 960 mg bid or Chloramphenicol 250 mg qid for 3 weeks In case of sepsis, IV therapy is necessary Shorter regimens are: ciprofloxacin 500 mg bid or ofloxacin 400 mg bid or ceftriaxone 2 g IV for 7-10 days Many patients often relapse after treatment and chronic maintenance therapy (TMP/SMX 1 DD daily) is sometimes necessary.
 is sometimes necessary.")
46
Shigella Primarily a human parasite Infects the large intestine
No perforation of intestine Dysentery Exotoxin (shiga-toxin) Enterotoxin
 Enterotoxin.")
47
Presenting Signs and Symptoms
Shigella Presenting Signs and Symptoms Clinical Symptoms may evolve High fever Abdominal pain Bloody diarrhea

48
Shigella dysenteriae, flexneri, boydii, sonnei
Watery or bloody diarrhea May be complicated by reactive arthritis and rarely HUS Very infectious ( ~100 organisms cause disease)
")
49
Shigella- Diagnostics
Stool microscopy— fresh examination and after concentration Multiple stool samples may be necessary Shigella bacillus found in stool

50
Shigella Management and Treatment
TMP/SMX 960 mg bid x 5 days or amoxicillin 500 mg tid x 5 days If resistant to the above, give norfloxacin 400 mg bid x 5 days nalidixic acid 1 g qid x 10 days ciprofloxacin 500 mg bid

51
Infection of the large intestine by Shigella dysenteriae.
Fig The appearance of the large intestional mucosa In Shigella dysentery.

52
Shigella colitis (Campylobacter or
Salmonella would look much the same.) © University of Alabama at Birmingham, Dept. of Path.
 © University of Alabama at Birmingham, Dept. of Path.")
53
Diarrhea of Shigella – WBCs & RBCs
CDC Diarrhea of Shigella – WBCs & RBCs

54
E. coli Type Clinical Features Complications ETEC (Enterotoxigenic)
Watery diarrhea, travelers diarrhea rare EHEC (Enterohemorrhagic ) Bloody diarrhea Hemolytic uremic syndrome, TTP (mostly 0157:H7) EIEC (Enteroinvasive) watery diarrhea or bloody diarrhea EAEC (Enteroaggregative) EPEC (Enteropathogenic) Watery diarrhea or bloody diarrhea, mainly in children May be protracted
 Bloody diarrhea. Hemolytic uremic syndrome, TTP (mostly 0157:H7) EIEC (Enteroinvasive) watery diarrhea or bloody diarrhea. EAEC (Enteroaggregative) EPEC (Enteropathogenic) Watery diarrhea or bloody diarrhea, mainly in children. May be protracted.")
55
Enterohemorrhagic Escherichia coli
Non-sorbitol fermenting Escherichia coli (Escherichia coli 94% + for sorbitol fermentation) Majority of enterohemorrhagic strains positive for somatic O157 and flagellar H7 antigens (O104 and O111 strains have caused outbreaks in the US) Bacteriophage-mediated production of Shiga-like toxin (Stx1 or Stx2) which are cytotoxic (verotoxin) Accounts for 15% to 36% of cases of bloody diarrhea
 Majority of enterohemorrhagic strains positive for somatic O157 and flagellar H7 antigens (O104 and O111 strains have caused outbreaks in the US) Bacteriophage-mediated production of Shiga-like toxin (Stx1 or Stx2) which are cytotoxic (verotoxin) Accounts for 15% to 36% of cases of bloody diarrhea.")
56
Enterohemorrhagic Escherichia coli
Abdominal cramps and watery diarrhea 3 to 8 days following ingestion of contaminated food (undercooked beef, raw milk, fresh produce) or water Shiga toxin absorbed from intestine and damages vascular endothelial cells (intestinal mucosa and kidney) Watery diarrhea followed by grossly bloody diarrhea Uncomplicated illness lasts 1 to 12 days Use of antibiotics contraindicated (phage-mediated production of Shiga toxin enhanced by ampicillin, norfloxacin, and other antibiotics)
 or water. Shiga toxin absorbed from intestine and damages vascular endothelial cells (intestinal mucosa and kidney) Watery diarrhea followed by grossly bloody diarrhea. Uncomplicated illness lasts 1 to 12 days. Use of antibiotics contraindicated (phage-mediated production of Shiga toxin enhanced by ampicillin, norfloxacin, and other antibiotics)")
57
Complications of Hemorrhagic Escherichia coli Colitis
Fever and neutrophilic leukocytosis herald hemolytic uremic syndrome (HUS) (thrombocytopenia, oliguria, hematuria, microangiopathic hemolytic anemia) HUS in 8% of infections in children with a 3% to 5% mortality
 (thrombocytopenia, oliguria, hematuria, microangiopathic hemolytic anemia) HUS in 8% of infections in children with a 3% to 5% mortality.")
58
Shiga-toxin (E. coli) O157:H7 Enterohemorrhagic E. coli (EHEC)
Serious manifestations – hemolytic uremic syndrome, neurologic symptoms Shiga-toxin gene present on bacteriophage genome Type III secretion system

59
The Type III secretion is a complex bridge formed by the bacteria, enabling binding to the host cell, thereby allowing the bacteria to insert its products in the host cell. Fig Type III secretion system.

60
Non-shiga-toxin (E. coli)
Enterotoxigenic – traveler’s diarrhea Enteroinvasive – no exotoxin Enteropathogenic – similar to EHEC Enteroaggregative – chronic diarrhea

61
Campylobacter Most common bacterial cause of diarrhea
Related to Guillain-Barre syndrome (GBS) – paralysis
 – paralysis.")
62
Campylobacter Mainly C. jejuni
Transmission from infected animals or food products, fresh or salt water Watery diarrhea or dysentery May be complicated by Guillain-Barré and IPSID (Immunoproliferative small intestinal disease)
")
63
Bacterial infection: Campylobacter
Presenting Signs and Symptoms Clinical Symptoms may evolve Fever and general malaise, sometimes without GI symptoms When present, GI symptoms include bloody diarrhea, abdominal pain and weight loss.

64
Campylobacter jejuni…
Spirilla morphology Gram Negative Stain Motile Role as an Enteric Pathogen © 2007 Aichi Prefectural Institute of Health

65
Campylobacter jejuni Relatively fragile Microaerophilic organism.
Seems to be well adapted to birds

66
Campylobacteriosis Known as campylobacter enteritis or gastroenteritis. Infection causes watery or sticky diarrhea, which contain blood and fecal leukocytes. Other symptoms include: fever, abdominal pain, nausea, headache and muscle pain.

67
Management and Treatment
Campylobacter Management and Treatment Erythromycin 500 mg bid x 5 days (1st choice) Fluoroquinolones are also effective, but resistance rates of 30-50% have been reported in some developing countries
 Fluoroquinolones are also effective, but resistance rates of 30-50% have been reported in some developing countries.")
68
Complications of Campylobacteriosis
Enteritis usually self-limiting (1 day to 1 week or longer) Guillain-Barré syndrome (structural homology of LPS O-antigen with human nerve gangliosides) Post-infectious reactive arthritis (associated with HLA-B27) Bacteremia (rate of 1.5/1,000 intestinal infections)
 Guillain-Barré syndrome (structural homology of LPS O-antigen with human nerve gangliosides) Post-infectious reactive arthritis (associated with HLA-B27) Bacteremia (rate of 1.5/1,000 intestinal infections)")
69
Campylobacter jejuni has a unique S-shaped and spiral morphology, and is closely related to H. pylori. Fig Scanning micrograph of Campylobacter jejuni, Showing comma, S, and spiral forms.

70
Yersinia High degree of abdominal pain Mistaken for appendicitis
Infects the small intestine Some can affect the lymphatic system (intracellular)
")
71
Yersinia enterocolitica
Fermentative, rod-shaped or coccoid gram-negative bacteria, non-motile and metabolically inactive at 37oC but motile and metabolically active at 22-30oC Enteropathogenic strains cytotoxic by penetratating human epithelial cells Infection results in inflammatory ileitis (generally) and colitis (occasionally involving ascending colon) with mixed neutrophilic and mononuclear cell response Necrosis of Peyer’s patches, mesenteric lymph node enlargement, and in severe cases thrombosis of mesenteric blood vessels with intestinal necrosis and hemorrhage
 and colitis (occasionally involving ascending colon) with mixed neutrophilic and mononuclear cell response. Necrosis of Peyer’s patches, mesenteric lymph node enlargement, and in severe cases thrombosis of mesenteric blood vessels with intestinal necrosis and hemorrhage.")
72
Yersinosis Febrile diarrhea with abdominal pain 16 to 48 hours following ingestion of an infectious inoculum Duration of illness ranges from 1 day to a prolonged diarrhea of 4 weeks

73
Complications of Yersinosis
Can simulate acute appendicitis (mesenteric lymphadenitis) Bacteremic dissemination with hepatic and splenic abscess formation Reactive arthritis associated with HLA-B27 histocompatibility antigen (10-30%) Exudative pharyngitis (8% of infections accompanied by fever but no diarrhea)
 Bacteremic dissemination with hepatic and splenic abscess formation. Reactive arthritis associated with HLA-B27 histocompatibility antigen (10-30%) Exudative pharyngitis (8% of infections accompanied by fever but no diarrhea)")
74
Treatment Safe food handling
Y. enterocolitica is suscestible to amg,chloram, tetra, TMP/SMZ,pip, cipro, ß lactamase, resis to pen, ampi, 1. gen. ceph. Patients with septicemia should receive antb. Y. pseudotuberculosis usually not require antb, but with septicemia ampi or tetra

75
Clostridium difficile
Pseudomembranous colitis or antibiotic associated colitis Capable of superinfecting the large intestine due to drug treatments Enterotoxins

77
A mild and more severe case of antibiotic-associated colitis.
Fig Antibiotic-associated colitis.

78
Pseudomembranes: Irregular yellow plaques of necrotic debris (black arrow) with intervening edematous bowel mucosa (white arrow) in an 87-year-old woman. These findings are consistent with pseudomembranes caused by Clostridium difficile infection. Schroeder, 2005
 with intervening edematous bowel mucosa (white arrow) in an 87-year-old woman. These findings are consistent with pseudomembranes caused by Clostridium difficile infection. Schroeder,")
79
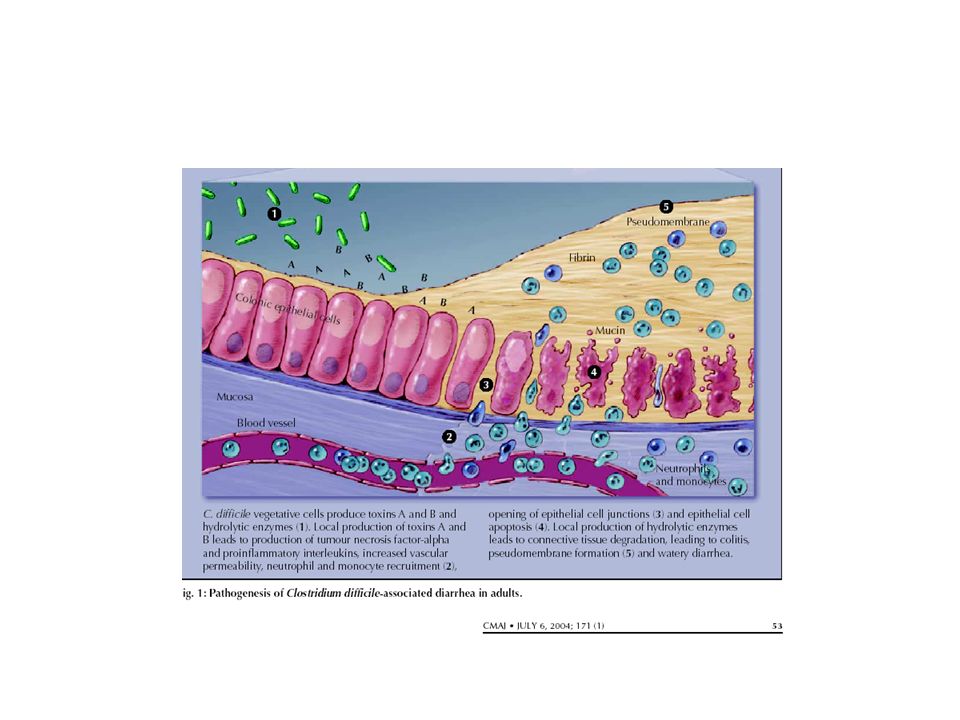
♦ Pathogenesis Accountable for 15-25% of antibiotic-associated diarrhea. Fecal-oral route transmission. Three steps to C. Difficile diarrhea: Alteration of the normal fecal flora ↓ Colonic colonization of C. difficile Growth and production of its toxins LaMont, 2006 Poutanen & Simor, 2004

80
Pathogenesis of C. difficile infection
Uncolonized patient ↓ Antibiotic exposure Disruption of colinic microflora C. Difficile ingestion & colonization ↓ ↓ Good IgG Poor IgG Asymptomatic carrier Production of toxins Colonic mucosal damage Clinical Disease Schroeder, 2005

81
♦ Risk Factors Antibiotics – fluoroquinolones, cephalosporins, clindamycins, penicillins Medications: Proton pump inhibitor Histamine-2 receptor blockers Non-steroidal anti-inflammatories (except aspirin) Laxatives Narcotics Antiperistaltic drugs Advanced age ( ≥ 65yrs.) Chemotherapy
 Laxatives. Narcotics. Antiperistaltic drugs. Advanced age ( ≥ 65yrs.) Chemotherapy.")
82
Medical/Surgical procedures
Gastrointestinal surgery Enemas Enteral tube feedings Endoscopy Underlying illness and its severity Inflammatory bowel disease Diabetes mellitus/Hyperthyroidism Leukemia/Lymphoma Liver/Renal failure History of C. difficile associated diarrhea Prolonged hospital stay/Nursing home resident Louie & Meddings, 2004 McDonald, Owings, & Jernigan, 2006 Melillo, 1998 Poutanon & Simor, 2004

83
Toxic Megacolon LaMont, 2006

84
♦♦ Diagnostic Testing LaMont, 2006

85
♦ Treatment Discontinue the offending agent If unable:
Choose an antibiotic less frequently associated with antibiotic-associated diarrhea (aminoglycosides, sulfonamides, macrolides, vancomycin, tetracyclines) Prescribe Metronidazole 500mg PO TID throughout the needed course of antibiotic therapy and for 7 days after. LaMont, 2006 Schroeder, 2005
 Prescribe Metronidazole 500mg PO TID throughout the needed course of antibiotic therapy and for 7 days after. LaMont, Schroeder,")
86
Vibrio cholerae Cholera Unique O and H antigens
Cholera toxin (CT) – A-B toxin Bacteria never enter host cells Heavy lost of fluid “rice-water stool” Untreated cases can be fatal
 – A-B toxin. Bacteria never enter host cells. Heavy lost of fluid rice-water stool Untreated cases can be fatal.")
87
Vibrio cholerae has a unique curved shaped and single polar flagellum.
Fig Vibrio cholerae

89
Common nonbacterial Cryptosporidium Rotavirus

90
Cryptosporidium Protozoan infection Zoonotic Oocysts Intracellular
AIDS patients are at risk Associated with fresh water outbreaks

91
A SEM of Cryptosporidium shows attachment to the intestinal epithelium, prior to intracellular invasion. Fig Scanning electron micrograph of Cryptosporidium

92
Acid-fast staining enables oocysts to be identified, as they stain red or purple.
Fig Acid-fast stain in Cryptosporidium

93
Rotavirus Responsible for most morbidity and mortality from diarrhea
Babies lacking maternal antibodies are at risk Unique morphological appearance

94
A feces sample containing Rotavirus, which has a unique “spoked-wheel” appearance.
Fig Rotavirus visible in a sample of feces from A child with gastroenteritis.

95
Acute diarrhea is an episode of diarrhea of <14 days in duration
Persistent diarrhea is of >14 days in duration Chronic diarrhea lasts >30 days

96
Features of acute diarrhea.
Checkpoint 22.5 Acute diarrhea

97
Acute diarrhea with vomiting
Food poisoning - toxin Staphylococcus aureus Bacillus cereus Clostridium perfringens

98
Classic Syndromes: Acute food poisoning
Similar illness in 2 or more persons Epidemiologic evidence of common food source Onset of symptoms typically within 6 hours of ingestion Nausea and vomiting prominent Preformed toxin of S. aureus or B. cereus Longer incubation periods for C. perfringens

99
Features of acute diarrhea with vomiting.
Checkpoint 22.6 Acute diarrhea with vomiting

100
Chronic diarrhea Enteroaggregative (EAEC) E. coli
Cyclospora cayetanensis Giardia lamblia Entamoeba histolytica

101
EAEC E. coli can be identified by its ability to adhere to human cells in aggregates.
Fig Enteroaggregative E. coli adhering to epithelial cells.

102
The protozoan Cyclospora can be identified by the acid-fast stain, in which large cysts stain pink to red and have a wrinkled outer wall. Fig An acid-fast stain of Cyclospora in a human Fecal sample.

103
The protozoan Giardia is typically transmitted by its cysts, which eventually germinates into the trophozoite and damages the jejunum. Fig The “face” of a Giardia lamblia trophozoite.

104
Entamoeba histolytica have different cellular forms, which includes a trophozoite that contains a karyosome and hosts cells (rbc) and bacteria, and a mature cyst which undergoes excystment. Fig Cellular forms of Entamoeba hystolytic

105
Features of chronic diarrhea.
Checkpoint 22.7 Chronic diarrhea.

107
History Onset and duration of diarrhea
Timing of exposure to potential pathogens Travel, ingestion history, environment, recent medications, age Character of stool Volume, presence of blood, mucus, or pus Associated symptoms and signs Abdominal pain, fever, vomiting, dehydration

108
Physical examination Vital signs: Fever, tachycardia
Abdominal tenderness or pain Signs of dehydration Blood in stool

109
Evaluation of Infectious Diarrhea
Stool studies fecal leukocytes and RBC/blood Bacterial culture Include C. difficle toxin assay May need to request EHEC screen Endoscopic evaluation may be useful in some especially for bloody diarrhea or chronic diarrhea

110
Laboratory investigations
Stool WBC may be ABSENT PRESENT VARIABLE V. cholerae Enterotoxigenic E. coli Virus E. Histolytica Food poisoning Shigella Campylobacter Invasive E. coli Salmonella Non-cholera vibrio Yersinia C. difficile

111
Laboratory investigation
Not routinely indicated Low yield % Not useful in initial management More sensitive and specific in stool with WBC

112
Fecal PMNs Common in Shigella, Campylobacter, EHEC, EIEC, C. diff
Rare in Salmonella, Yersinia, ETEC, EAEC

113
MANAGING INFECTIOUS DIARRHEA
Initial rehidration Perform thorough clinical and epidemiological evaluation Perform selective fecal studies Institute selective therapy for Traveler’s diarrhea Shigellosis Campylobacter infection Avoid administering antimotilty agents Selectively administer available vaccines

114
Oral rehydration solutions

115
Treatment of Diarrhea Treatment of specific etiology
Non-specific treatment hydration Absorptions (Kaopectate®) Bismuth Antiperistaltics/opiate derivatives Fiber supplementation
 Bismuth. Antiperistaltics/opiate derivatives. Fiber supplementation.")
116
TUS 2010 Kırk iki yaşında erkek hasta akut karın bulguları ile acil servise başvuruyor. Hastanın sağ alt karın bölgesinde belirgin olmak üzere tüm karın bölgelerinde hassasiyet ve defans saptanıyor. Ayakta karın grafisinde serbest hava bulunan hastanın öyküsünden 3 hafta önce yaptığı bir seyahat sonrası ishal başladığı öğreniliyor. Bu hasta için en olası tanı aşağıdakilerden hangisidir? A) Akut apandisit perforasyonu B) Meckel divertiküliti perforasyonu C) Tifo enterit perforasyonu D) Tüberküloz enterit perforasyonu E) Campylobacter enfeksiyonu perforasyonu
 Akut apandisit perforasyonu. B) Meckel divertiküliti perforasyonu. C) Tifo enterit perforasyonu. D) Tüberküloz enterit perforasyonu. E) Campylobacter enfeksiyonu perforasyonu.")
117
TUS 2010 Kırk iki yaşında erkek hasta akut karın bulguları ile acil servise başvuruyor. Hastanın sağ alt karın bölgesinde belirgin olmak üzere tüm karın bölgelerinde hassasiyet ve defans saptanıyor. Ayakta karın grafisinde serbest hava bulunan hastanın öyküsünden 3 hafta önce yaptığı bir seyahat sonrası ishal başladığı öğreniliyor. Bu hasta için en olası tanı aşağıdakilerden hangisidir? A) Akut apandisit perforasyonu B) Meckel divertiküliti perforasyonu C) Tifo enterit perforasyonu D) Tüberküloz enterit perforasyonu E) Campylobacter enfeksiyonu perforasyonu
 Akut apandisit perforasyonu. B) Meckel divertiküliti perforasyonu. C) Tifo enterit perforasyonu. D) Tüberküloz enterit perforasyonu. E) Campylobacter enfeksiyonu perforasyonu.")
118
TUS 2012 Rotavirus enfeksiyonlarının en sık görüldüğü yaş grubu aşağıdakilerden hangisidir? A) 4 aydan küçük olanlar B) 4 ay ile 2 yaş arasında olanlar C) 2 yaş ile 4 yaş arasında olanlar D) 5 yaş ile 7 yaş arasında olanlar E) 8 yaşından büyük olanlar
 4 ay ile 2 yaş arasında olanlar. C) 2 yaş ile 4 yaş arasında olanlar. D) 5 yaş ile 7 yaş arasında olanlar. E) 8 yaşından büyük olanlar.")
119
TUS 2012 Rotavirus enfeksiyonlarının en sık görüldüğü yaş grubu aşağıdakilerden hangisidir? A) 4 aydan küçük olanlar B) 4 ay ile 2 yaş arasında olanlar C) 2 yaş ile 4 yaş arasında olanlar D) 5 yaş ile 7 yaş arasında olanlar E) 8 yaşından büyük olanlar
 4 ay ile 2 yaş arasında olanlar. C) 2 yaş ile 4 yaş arasında olanlar. D) 5 yaş ile 7 yaş arasında olanlar. E) 8 yaşından büyük olanlar.")
120
TUS 2013 45 yaşında erkek hasta akşam yemekle beraber alkol aldıktan 1 saat sonra ani başlayan karın krampları, baş dönmesi, bulantı, yüzde kızarma ve sıcak basması şikayetleriyle acil servise başvurdu. Öyküsünden 4 gündür diş enf nedeniyle adını hatılamadığı bir antibiyotik aldığını söyledi. Fizik muayenesinde kan basıncı 80/40 mmHg nabzı 140/dk. Aşağıdaki ilaçlardan hangisinin buna yol açması en olasıdır? a) Tetrasiklin b) Klaritromisin c) Klindamisin d) Amoksisilin e) Metronidazol
 Tetrasiklin b) Klaritromisin c) Klindamisin d) Amoksisilin e) Metronidazol.")
121
TUS 2013 45 yaşında erkek hasta akşam yemekle beraber alkol aldıktan 1 saat sonra ani başlayan karın krampları, baş dönmesi, bulantı, yüzde kızarma ve sıcak basması şikayetleriyle acil servise başvurdu. Öyküsünden 4 gündür diş enf nedeniyle adını hatılamadığı bir antibiyotik aldığını söyledi. Fizik muayenesinde kan basıncı 80/40 mmHg nabzı 140/dk. Aşağıdaki ilaçlardan hangisinin buna yol açması en olasıdır? a) Tetrasiklin b) Klaritromisin c) Klindamisin d) Amoksisilin e) Metronidazol
 Tetrasiklin b) Klaritromisin c) Klindamisin d) Amoksisilin e) Metronidazol.")
122
TUS 2013 45 yaşında erkek hasta akşam yemekle beraber alkol aldıktan 1 saat sonra ani başlayan karın krampları, baş dönmesi, bulantı, yüzde kızarma ve sıcak basması şikayetleriyle acil servise başvurdu. Öyküsünden 4 gündür diş enf nedeniyle adını hatılamadığı bir antibiyotik aldığını söyledi. Fizik muayenesinde kan basıncı 80/40 mmHg nabzı 140/dk. Aşağıdaki ilaçlardan hangisinin buna yol açması en olasıdır? a) Tetrasiklin b) Klaritromisin c) Klindamisin d) Amoksisilin e) Metronidazol
 Tetrasiklin b) Klaritromisin c) Klindamisin d) Amoksisilin e) Metronidazol.")
123
One of the most common alcohol-antibiotic interactions is with the antimicrobial agent metronidazole (Flagyl). Metronidazole is used for a variety of infections, including gastrointestinal, skin, joint and respiratory tract infections. Taking metronidazole with alcohol may result in a reaction called a “disulfiram-like reaction”. A “disulfiram-like reaction” may include nausea, flushing of the skin, stomach cramps, vomiting, headaches, rapid heart rate, and difficulty breathing. A similar reaction may occur with other antibiotics.

124
TUS 2013 Gastroenterit kliniği olan bir hastanın dışkısından clostridum dif. toksin a/b izole edilmiş. EN OLASI neden nedir? a) antibiyotik kullanımı b) besin zehirlenmesi c) rotavirüs enteriti d) Stafilokok zehirlenmesi
 antibiyotik kullanımı. b) besin zehirlenmesi. c) rotavirüs enteriti. d) Stafilokok zehirlenmesi.")
125
TUS 2013 Gastroenterit kliniği olan bir hastanın dışkısından clostridum dif. toksin a/b izole edilmiş. EN OLASI neden nedir? a) antibiyotik kullanımı b) besin zehirlenmesi c) rotavirüs enteriti d) Stafilokok zehirlenmesi
 antibiyotik kullanımı. b) besin zehirlenmesi. c) rotavirüs enteriti. d) Stafilokok zehirlenmesi.")
126
TUS 2013 Pirinç suyu ishali olan hastada yapılan dışkı yaymasında sinek uçuşması görüntü var? a) Rotavirüs b) Salmonella c) Campylobacter d) Vibrio
 Rotavirüs b) Salmonella c) Campylobacter d) Vibrio .")
127
TUS 2013 Pirinç suyu ishali olan hastada yapılan dışkı yaymasında sinek uçuşması görüntü var? a) Rotavirüs b) Salmonella c) Campylobacter d) Vibrio
 Rotavirüs b) Salmonella c) Campylobacter d) Vibrio .")
128
TUS 2013 8 haftadır günde 6-7 kez süren ishal yakınması. tenezm hissi var. geceleri ishalden dolayı uyuyamıyor. Gaita mikroskopisinde lökosit eritrosit gözlendi . tanı? a- kolon tipi- enflamatuar b- kolon tipi nonenflamayuar c-i barsak tipi enflamatuar d- i. barsak tipi non inflamayuar

129
TUS 2013 8 haftadır günde 6-7 kez süren ishal yakınması. tenezm hissi var. geceleri ishalden dolayı uyuyamıyor. Gaita mikroskopisinde lökosit eritrosit gözlendi . tanı? a- kolon tipi- enflamatuar b- kolon tipi nonenflamayuar c-i barsak tipi enflamatuar d- i. barsak tipi non inflamayuar

130
TUS 2013 Aşağıdaki bakterilerden hangisinin insanda oluşturduğu hastalıkların patogenezinde, bakteri tarafından üretilen ekzotoksin rol oynamaz? A) Vibrio cholerae B) Corynebacterium diphtheriae C) Haemophilus influenzae D) Staphylococcus aureus E) Shigella dysenteriae
 Vibrio cholerae B) Corynebacterium diphtheriae C) Haemophilus influenzae D) Staphylococcus aureus E) Shigella dysenteriae.")
131
TUS 2013 Aşağıdaki bakterilerden hangisinin insanda oluşturduğu hastalıkların patogenezinde, bakteri tarafından üretilen ekzotoksin rol oynamaz? A) Vibrio cholerae B) Corynebacterium diphtheriae C) Haemophilus influenzae D) Staphylococcus aureus E) Shigella dysenteriae
 Vibrio cholerae B) Corynebacterium diphtheriae C) Haemophilus influenzae D) Staphylococcus aureus E) Shigella dysenteriae.")
132
TUS 2013 Aşağıdaki gastroenterit etkenlerinden hangisinin tek doğal kaynağı insandır? A) Campylobacter jejuni B) Escherichia coli O157:H7 C) Salmonella Typhimurium D) Vibrio parahaemolyticus E) Shigella dysenteriae
 Campylobacter jejuni B) Escherichia coli O157:H7 C) Salmonella Typhimurium D) Vibrio parahaemolyticus E) Shigella dysenteriae.")
133
TUS 2013 Aşağıdaki gastroenterit etkenlerinden hangisinin tek doğal kaynağı insandır? A) Campylobacter jejuni B) Escherichia coli O157:H7 C) Salmonella Typhimurium D) Vibrio parahaemolyticus E) Shigella dysenteriae
 Campylobacter jejuni B) Escherichia coli O157:H7 C) Salmonella Typhimurium D) Vibrio parahaemolyticus E) Shigella dysenteriae.")
134
TUS 2013 Otuz altı yaşındaki erkek hasta, dışarıda yemek yedikten 24 saat sonra ani kusma, ishal ve baş ağrısı ile acil servise başvuruyor. Daha sonra aynı şikâyetlerle 6 hastanın daha acil servise başvurduğu öğreniliyor. Bu hastada gastroenterite neden olan virus büyük olasılıkla aşağıdakilerden hangisidir? A) Coronavirus B) Hepatit A virusu C) Norovirus D) Adenovirus E) Echovirus
 Coronavirus B) Hepatit A virusu C) Norovirus D) Adenovirus E) Echovirus.")
135
TUS 2013 Otuz altı yaşındaki erkek hasta, dışarıda yemek yedikten 24 saat sonra ani kusma, ishal ve baş ağrısı ile acil servise başvuruyor. Daha sonra aynı şikâyetlerle 6 hastanın daha acil servise başvurduğu öğreniliyor. Bu hastada gastroenterite neden olan virus büyük olasılıkla aşağıdakilerden hangisidir? A) Coronavirus B) Hepatit A virusu C) Norovirus D) Adenovirus E) Echovirus
 Coronavirus B) Hepatit A virusu C) Norovirus D) Adenovirus E) Echovirus.")
136
TUS 2014

137
STEC’in ürettiği Shigalike toksinleri ilk olarak Vero hücre kültüründe gözlenmiş olduğundan verotoksin olarak da adlandırılmaktadır. Shigalike toksini Vero hücrelerine toksik etki gösteren, protein sentezini inhibe eden ve lizojen bir bakteriyofaj tarafından kodlanan sitotoksinlerdir. Bunlar; Shigella dysenteriae tip 1’in oluşturduğu toksin ile aynı olan shigalike toksin1 (stx 1; verotoksin 1) ve daha az benzeyen shigalike toksin 2’dir (stx 2; verotoksin 2).
 ve daha az benzeyen shigalike toksin 2’dir (stx 2; verotoksin 2).")
138
TUS 2014

139
TUS 2014

140
TUS 2015

141
TUS 2015

142
TUS 2015

143
TUS 2015

Benzer bir sunumlar




 2 friends... you'll have 3 years of good luck!!!>")








 (Yrd. Doç. Dr. Deniz Dal)>")


>")



