Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
D Vitamininin Kemik Dışı Etkileri
Prof. Dr. Hülya Taşkapan İnönü Üniversitesi Tıp Fakültesi Nefroloji Bilim Dalı

2
Vitamin D Deri + UV ışını Endokrin Vitamin D Karaciğer Vitamin D3
25(OH)D3 1,25(OH)2D3- Endokrin Parakrin 1 hidroksilaz Besinler Vitamin D Vitamin D, biyolojik olarak inaktif. 125(OH)2D3 ün öncüsü Vitamin D nin nutrisyonel durumunun göstergesi 25(OH)D düzeyi 125(OH)2D3 bir çok dokuda bulunan VDR bağlanarak etkisini gösteriyor.
D3. 1,25(OH)2D3- Endokrin. Parakrin. 1 hidroksilaz. Besinler. Vitamin D. Vitamin D, biyolojik olarak inaktif. 125(OH)2D3 ün öncüsü. Vitamin D nin nutrisyonel durumunun göstergesi 25(OH)D düzeyi. 125(OH)2D3 bir çok dokuda bulunan VDR bağlanarak etkisini gösteriyor.")
3
1 hidroksilaz pozitif ve negatif doku
A, normal böbrek korteksi pozitif boyanma (kahverengi) proksimal tübül ve distal tübülde (büyütme 3250). B, Negatif kontrol böbrek korteksi (büyütme 3200). Zehnder et al. The Journal of Clinical Endocrinology & Metabolism
 proksimal tübül ve distal tübülde (büyütme 3250). B, Negatif kontrol böbrek korteksi (büyütme 3200). Zehnder et al. The Journal of Clinical Endocrinology & Metabolism.")
4
Normal ve patolojik dokularda 1 hidroksilaz Ekspresyonu
A. Normal insan dersinin immunohistokimyasal analizinde 1a- hydroxylase proteinin epidermisin stratum bazalisinde güçlü ekspresyonu (büyütme 3150) B. psöriyatik deride epidermisin düzensiz stratum spinosum kısmından ekspresyonu (3100; B). C. deride negatif kontrol D saç follikülünden 1a-hydroxylase protein ekspresyonu (3250 B). E–H, insan lenf nodunda (3100; E); normal tonsil, ( 3200; F); lenf nod granuloma (;3100; G), ve sarkoidozda deriden expesyon (3150; H). Zehnder et al. The Journal of Clinical Endocrinology & Metabolism
 B. psöriyatik deride epidermisin düzensiz stratum spinosum kısmından ekspresyonu (3100; B). C. deride negatif kontrol. D saç follikülünden 1a-hydroxylase protein ekspresyonu (3250 B). E–H, insan lenf nodunda (3100; E); normal tonsil, ( 3200; F); lenf nod granuloma (;3100; G), ve sarkoidozda deriden expesyon (3150; H). Zehnder et al. The Journal of Clinical Endocrinology & Metabolism.")
5
Böbrek dışındaki dokularda 1 Hidroksilaz enzimi
mRNA Protein Enzimatik aktivite Kaynak Kolon Bises ve ark. Dendritik hücreler - Adorini ve ark. Endotel hücreleri Zehnder ve ark. İnsan beyni Eyles ve ark. Meme Segersten ve ark. Pankreas Townsend ve ark. Parathormon Evans ve ark. Plasenta Prostat Ma ve ark. Deri, keratinositler Bikle ve ark.

6
Vitamin D Receptör (VDR)
Doku dağılımı Immun sistem T-hücreleri Makrofajlar B-Hücreleri Nötrofiller Kas-kemik Osteoblastlar Osteositler Kondrositler Çizgili kas hücreleri. Kardiyovasküler Endotel Düz kas Kalp kas hücreleri Endokrin Paratiroid Pankreas -hücreleri Tiroid C- hücreleri Böbrekler Podositler Mezanjial hücreler juxtaglomerular tubuli Bağ dokusu Fibroblastlar Stroma Diğer sistemler Beyin Prostat Meme Karaciğer Epidermis Gastroentestinal Akciğerler Vitamin D-deficiency or insufficiency is associated with renal and cardiovascular disease. A rapidly growing body of evidence has suggested a role of vitamin D in renal and cardiovascular protection. • Vitamin D-deficiency is partly caused by dysregulation of vitamin D metabolism in kidney disease. • Reno-protective actions of vitamin D have been demonstrated in a variety of experimental models of kidney disease. The anti-proteinuric activity of vitamin D and vitamin D analogs is confirmed by randomized clinical trials. • The cardiovascular protective effect of vitamin D is supported by strong epidemiological data. Anti-hypertrophic and anti-atherosclerotic activities of vitamin D and vitamin D analogs have been reported in a number of animal models. • The renal and cardiovascular protective mechanism of vitamin D is multifactorial and involves multiple regulatory pathways

7
Dolaşımdaki ana vitamin D formu
25(OH)Vit D • 1,25(OH)2 Vit D Fizyolojik olarak etkin form 1,25(OH)2 Vitamin D 25 (OH) Vit D’nin yarı ömrü 2-4 hafta 1,25 (OH)2 Vit D’nin yarı ömrü 8 saat Endocrine Reviews 29: 726–776, 2008
Vit D • 1,25(OH)2 Vit D. Fizyolojik olarak etkin form 1,25(OH)2 Vitamin D. 25 (OH) Vit D’nin yarı ömrü 2-4 hafta. 1,25 (OH)2 Vit D’nin yarı ömrü 8 saat. Endocrine Reviews 29: 726–776,")
8
Ana kaynak güneş ışığı Tüm vücudun yazın gün ortası dakika güneş ışığı ile minimal eritem dozu oluşturacak şekilde karşılaşması (~1 MED) Ξ IU (375 g) oral Ellerin, yüzün ve kolların maruz kalması (~%15 vücut yüzeyi) ~1/3 MED : ~1000 IU Kış mevsimi, koyu cilt, güneş koruyucu kremler ve yaşlılık daha az Vit D sentezine neden olur. 1/3 MED üretebilmek için güneş ışığına maruz kalmanın miktarı enleme, mevsime, günün saati, deri tipine göre değişmektedir. UV kısa süreli karşılaşma uzun süreli yüksek doz UV ile karşılaşmaktan daha iyi. Yüksek doz UV previtamin D nin yıkılmasına neden olmaktadır.
 Ξ IU (375 g) oral. Ellerin, yüzün ve kolların maruz kalması (~%15 vücut yüzeyi) ~1/3 MED : ~1000 IU. Kış mevsimi, koyu cilt, güneş koruyucu kremler ve yaşlılık daha az Vit D sentezine neden olur. 1/3 MED üretebilmek için güneş ışığına maruz kalmanın miktarı enleme, mevsime, günün saati, deri tipine göre değişmektedir. UV kısa süreli karşılaşma uzun süreli yüksek doz UV ile karşılaşmaktan daha iyi. Yüksek doz UV previtamin D nin yıkılmasına neden olmaktadır.")
9
Güneş ışığı- UV nm Zenith açısı sabah erken ve akşam saatlerinde D vitamini sentezi efektif olmaz Ülkemizde vitamin D sentezi Nisan-Kasım ayları arasında

11
Diyette vitamin D kaynakları
Pişmiş dana karaciğeri 15IU /100g Vitamin D eklenmiş margarin 400IU/100g Yumurta beyazı 20IU/100g Konserve uskumru balığı 300IU/100g Taze Salmon balığı Taze ringa balığı 1400IU/100g Salamura ringa balığı 600IU/100g Güneşlenme (10 dakika kol ve bacaklar, 0.5 Minimal Eritem Dozu) 3000IU
 3000IU.")
12
Ne kadar vitamin D gereksinim var?
Doğum – 50 yaş 200 IU/gün Gebelik & Laktasyon 51 – 70 yaş 400 IU/gün 70 yaş 600 IU/gün National Institutes of Health Office of Dietary Supplements

13
Vitamin D nasıl ölçülür?
Serum 25(OH)D düzeyi Yetersizliği: < 20 ng/mL (50 nmol/L) Eksikliği: ng/mL (50-80 nmol/L) Yeterli: >= 32 ng/mL (80 nmol/L) “Normal”: ng/mL
D düzeyi. Yetersizliği: < 20 ng/mL (50 nmol/L) Eksikliği: ng/mL (50-80 nmol/L) Yeterli: >= 32 ng/mL (80 nmol/L) Normal : ng/mL.")
14
Optimal D Vitamini Düzeyi
D vitamini eksikliği <20 ng/mL D vitamini yetersizliği <30 ng/mL PTH supresyonu >30-40 ng/mL Kırık riskinde azalma >30-40 ng/mL Düşmede azalma >30 ng/mL İskelet dışı etkiler Bilinmiyor (>30 ng/mL)
")
15
Ref 1, p 4, C2, Table 1, Row 3 + calc, ¶1, L7-13
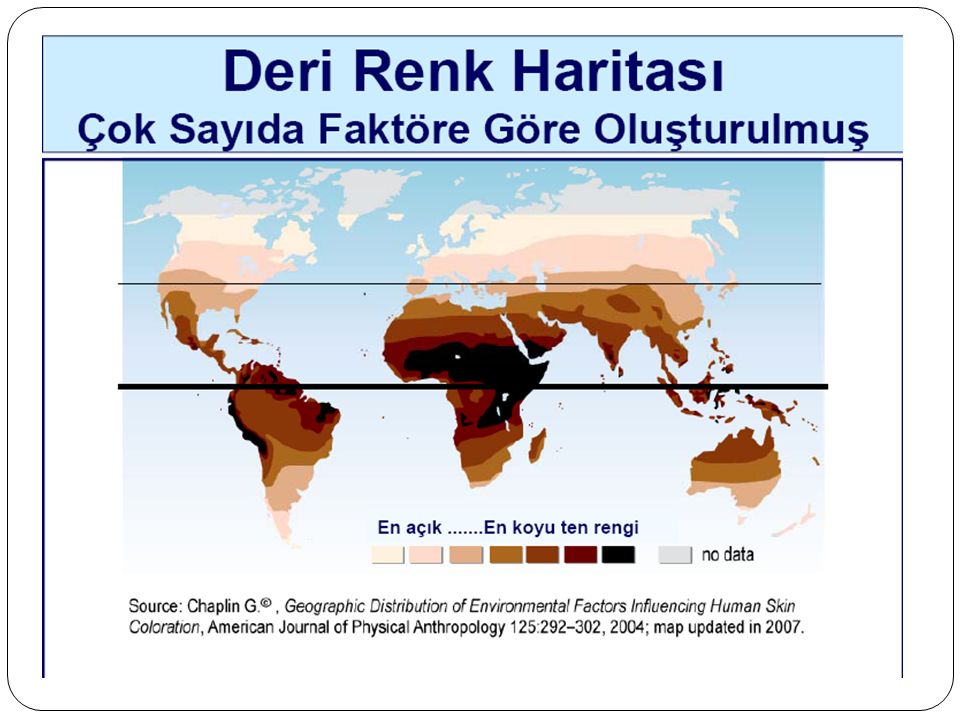
Yüksek D Vitamini Yetersizliği* Prevalansı Tüm Coğrafi Bölgelerde Gözlendi Ref 1, p 2, C2, L2-6, ¶1, L1-3; p 3, C2, ¶3, L1-4 Ref 1, p 3, C2, ¶3, L1-4; p 6, Table 3, Rows 1,10,13,18, 22,23 Ref 1, p 8, C1, ¶1, L20-23 Ref 1, p 2, C2, L2-6, ¶1, L1-3; p 3, C1, ¶2, L1,2, C2, ¶3, L1-4 Osteoporozlu postmenopozal kadınlarda yapılan kesitsel, uluslararası çalışmada 90 N=2589 % 81.8 80 % 71.4 % 63.9 70 % 60.3 % 57.7 60 % 53.4 50 Prevalans (%) Ref 1, p 2, C2, ¶1, L1-3; p 8, C2, ¶3, L1-5 Ref 1, p 2, C2, L2-6, ¶1, L1-3,5-11, ¶2, L9-11; p 3, C1, ¶1, L1,2, C2, ¶3, L1-4; p 8, C1, ¶1, L20-23 Ref 1, p 5, Table 2 (title), Row 23; p 6 Table 3, Rows 1,10, 13,18,22,23 Ref 2, p 1018, Table 3, Rows 10,13, 22,23,27,46 Ref 1, p 4, C2, Table 1, Row 3 + calc, ¶1, L7-13 Calc: 100–45.8=54.2% Uluslararası epidemiyoloji çalışmasının bulguları D vitamini yetersizliğinin tüm dünyada, hatta güneş ışınlarının bol olduğu bölgelerde bile osteoporozlu postmenopozal kadınlarda son derece yaygın olduğunu göstermektedir.1 Bu kesitsel, tek vizitli çalışma Mayıs 2004 ile Mart 2005 tarihleri arasında Avrupa, Latin Amerika, Orta Doğu, Asya ve Avustralya’daki 18 ülkedeki 2589 postmenopozal osteoporozlu kadını içerdi. D vitamini yetersizliği serum 25(OH)D düzeyi <30 ng/ml olarak tanımlandı. 1 Çalışma popülasyonunda ortalama 25(OH)D konsantrasyonu genel olarak 26.8 ng/ml’ydi. Çalışma popülasyonunun yaklaşık %64’ünde serum 25(OH)D konsantrasyonu <30 ng/ml bulundu ve yaklaşık %31’inde konsantrasyon <20 ng/ml’ydi. D vitamini yetersizliği (<30 ng/ml) prevalansı çalışmaya katılan beş bölgenin tümünde en az %53’dü ve Orta Doğu (%81.8) ve Asya’da (%71.4) en yüksekti. 1 Çalışma popülasyonunda D vitamini yetersizliği için risk faktörleri vücut kütle indeksi >30 kg/m2 (olasılık oranı, 2.4 [%95 güven aralığı: 1.83, 3.14]), ekvator bölgesi dışındaki iklimlerde yaşamak (1.91 [1.58, 2.32]), genel sağlığın orta ile kötü arasında olması (1.86 [1.49, 2.33]), güneşli bölgelere yakın tarihte seyahat etmemiş olmak (1.86 [1.54, 2.25]), günde <400 IU D vitamini desteği (1.78 [1.41, 2.24]) ve hiç D vitamini desteği alınmamasını içerdi (2.36 [1.97, 2.82]).2 Çalışma katılımcılarının yaklaşık %59.8’i osteoporoz tedavisi için onaylanmış bir ilaç kullandı (bifosfonatlar, selektif östrojen reseptör modülatörleri, kalsitonin veya paratiroid hormon gibi) ve yaklaşık %54.2’si D vitamini katkıları kullandı. 1 40 30 20 10 Tümü Latin Amerikaa Avrupa Orta Doğu Asya Avustralya Bölgeler * D vitamini yetersizliği serum 25(OH)D <30 ng/ml olarak tanımlandı. Çalışma Tasarımı: 18 ülkedeki osteoporozlu 2589 ambulatuvar kadında serum 25(OH)D dağılımını incelemek amacıyla yapılan kesitsel, uluslararası çalışma, Lips P et al. J Intern Med. Referanslar: Lips P, Hosking D, Lippuner K, et al. The prevalence of vitamin D inadequacy amongst women with osteoporosis: an international epidemiological investigation. J Intern Med. In press. Rizzoli R, Eisman JA, Norquist J, et al. Risk factors for vitamin D inadequacy among women with osteoporosis: an international epidemiological study. Int J Clin Pract. 2006;60:1013–1019.
 Ref 1, p 2, C2, ¶1, L1-3; p 8, C2, ¶3, L1-5. Ref 1, p 2, C2, L2-6, ¶1, L1-3,5-11, ¶2, L9-11; p 3, C1, ¶1, L1,2, C2, ¶3, L1-4; p 8, C1, ¶1, L Ref 1, p 5, Table 2 (title), Row 23; p 6 Table 3, Rows 1,10, 13,18,22,23. Ref 2, p 1018, Table 3, Rows 10,13, 22,23,27,46. Ref 1, p 4, C2, Table 1, Row 3 + calc, ¶1, L7-13. Calc: 100–45.8=54.2% Uluslararası epidemiyoloji çalışmasının bulguları D vitamini yetersizliğinin tüm dünyada, hatta güneş ışınlarının bol olduğu bölgelerde bile osteoporozlu postmenopozal kadınlarda son derece yaygın olduğunu göstermektedir.1 Bu kesitsel, tek vizitli çalışma Mayıs 2004 ile Mart 2005 tarihleri arasında Avrupa, Latin Amerika, Orta Doğu, Asya ve Avustralya’daki 18 ülkedeki 2589 postmenopozal osteoporozlu kadını içerdi. D vitamini yetersizliği serum 25(OH)D düzeyi <30 ng/ml olarak tanımlandı. 1. Çalışma popülasyonunda ortalama 25(OH)D konsantrasyonu genel olarak 26.8 ng/ml’ydi. Çalışma popülasyonunun yaklaşık %64’ünde serum 25(OH)D konsantrasyonu <30 ng/ml bulundu ve yaklaşık %31’inde konsantrasyon <20 ng/ml’ydi. D vitamini yetersizliği (<30 ng/ml) prevalansı çalışmaya katılan beş bölgenin tümünde en az %53’dü ve Orta Doğu (%81.8) ve Asya’da (%71.4) en yüksekti. 1. Çalışma popülasyonunda D vitamini yetersizliği için risk faktörleri vücut kütle indeksi >30 kg/m2 (olasılık oranı, 2.4 [%95 güven aralığı: 1.83, 3.14]), ekvator bölgesi dışındaki iklimlerde yaşamak (1.91 [1.58, 2.32]), genel sağlığın orta ile kötü arasında olması (1.86 [1.49, 2.33]), güneşli bölgelere yakın tarihte seyahat etmemiş olmak (1.86 [1.54, 2.25]), günde <400 IU D vitamini desteği (1.78 [1.41, 2.24]) ve hiç D vitamini desteği alınmamasını içerdi (2.36 [1.97, 2.82]).2. Çalışma katılımcılarının yaklaşık %59.8’i osteoporoz tedavisi için onaylanmış bir ilaç kullandı (bifosfonatlar, selektif östrojen reseptör modülatörleri, kalsitonin veya paratiroid hormon gibi) ve yaklaşık %54.2’si D vitamini katkıları kullandı Tümü. Latin Amerikaa. Avrupa. Orta. Doğu. Asya. Avustralya. Bölgeler. * D vitamini yetersizliği serum 25(OH)D <30 ng/ml olarak tanımlandı. Çalışma Tasarımı: 18 ülkedeki osteoporozlu 2589 ambulatuvar kadında serum 25(OH)D dağılımını incelemek amacıyla yapılan kesitsel, uluslararası çalışma, Lips P et al. J Intern Med. Referanslar: Lips P, Hosking D, Lippuner K, et al. The prevalence of vitamin D inadequacy amongst women with osteoporosis: an international epidemiological investigation. J Intern Med. In press. Rizzoli R, Eisman JA, Norquist J, et al. Risk factors for vitamin D inadequacy among women with osteoporosis: an international epidemiological study. Int J Clin Pract. 2006;60:1013–1019.")
16
Türkiye’de vitamin D eksikliği
Adolesan (Kış-Yaz) %59 - %25 Postmenapozal kadınlarda % 50-75 Acta Paediatr. 2006;95:1266-9 Arch Gerontol Geriatr. 2005;40:53-60 Qual Life Res Nov;16(9):1491-9
 %59 - %25. Postmenapozal kadınlarda % Acta Paediatr. 2006;95: Arch Gerontol Geriatr. 2005;40: Qual Life Res Nov;16(9):")
17
Diyaliz hastalarında vitamin D eksikliği
Türkiye ve Yunanistan dan 273 PD hastası ( kuzey enlemleri) Vit D yetmezliği %92 K/DOQ1 guidelines, Vitamin D yetmezliği 25(OH)D3< = 15 ng/ml Ciddi yet.:<5 ng/ml). Vit D eksikliği : mg/ml Normal: 25(OH)D3 30 ng/ml. Abstract: The aim of this study was to evaluate the prevalence of vitamin D deficiency in chronic renal failure (CRF) patients on peritoneal dialysis (PD) and to correlate findings with various demographic and renal osteodystrophy markers. Method: This cross-sectional, multi-center study was carried among 273 PD patients with a mean age of 61.7±10.9 years and mean duration of PD 3.3±2.2 years. 123 female and 150 male patients from 20 centers in Greece and Turkey, countries which are on the same latitude ( north latitudes), were included in the study. 25(OH)D3 and 1,25(OH)2D3 levels and some other clinical and laboratory indices of bone mineral metabolism were assessed. Results: The prevalence of vitamin D deficiency [i.e serum 25(OH)D3 levels, less than 15 ng/ml] in the 273 patients was 92 % (251 patients): 119 (43.7 %) had severe vitamin D deficiency [i.e serum 25(OH)D3 levels, less than 5 ng/ml], 132 (48.4 %) moderate vitamin D deficiency [i.e serum 25(OH)D3 levels, 5-15ng/ml], 12 (4.4%) vitamin D insufficiency [i.e serum 25(OH)D3 levels 15-30ng/ml] and only 10 (3.6%) had adequate vitamin D stores. There was no correlation between 25(OH)D3 levels and PTH, serum albumin, bone alkaline phosphatase, P, and CaxP. In multiple regresion analyses the independent predictors of 25(OH)D3 were age, presence of diabetes (DM-CRF), serum calcium, and serum 1,25(OH)D3 levels . Taskapan ve ark.Turkish Multicenter Peritoneal Dialysis Study Group (TULIP), Compare-PD Study Group, GRECE Compare-PD Study Group Canada, CANADA Clinical Nephrology 2006
 Vit D yetmezliği %92. K/DOQ1 guidelines, Vitamin D yetmezliği 25(OH)D3< = 15 ng/ml. Ciddi yet.:<5 ng/ml). Vit D eksikliği : mg/ml. Normal: 25(OH)D3 30 ng/ml. Abstract: The aim of this study was to evaluate the prevalence of vitamin D deficiency in chronic renal failure (CRF) patients on peritoneal dialysis (PD) and to correlate findings with various demographic and renal osteodystrophy markers. Method: This cross-sectional, multi-center study was carried among 273 PD patients with a mean age of 61.7±10.9 years and mean duration of PD 3.3±2.2 years. 123 female and 150 male patients from 20 centers in Greece and Turkey, countries which are on the same latitude ( north latitudes), were included in the study. 25(OH)D3 and 1,25(OH)2D3 levels and some other clinical and laboratory indices of bone mineral metabolism were assessed. Results: The prevalence of vitamin D deficiency [i.e serum 25(OH)D3 levels, less than 15 ng/ml] in the 273 patients was 92 % (251 patients): 119 (43.7 %) had severe vitamin D deficiency [i.e serum 25(OH)D3 levels, less than 5 ng/ml], 132 (48.4 %) moderate vitamin D deficiency [i.e serum 25(OH)D3 levels, 5-15ng/ml], 12 (4.4%) vitamin D insufficiency [i.e serum 25(OH)D3 levels 15-30ng/ml] and only 10 (3.6%) had adequate vitamin D stores. There was no correlation between 25(OH)D3 levels and PTH, serum albumin, bone alkaline phosphatase, P, and CaxP. In multiple regresion analyses the independent predictors of 25(OH)D3 were age, presence of diabetes (DM-CRF), serum calcium, and serum 1,25(OH)D3 levels . Taskapan ve ark.Turkish Multicenter Peritoneal Dialysis Study Group (TULIP), Compare-PD Study Group, GRECE Compare-PD Study Group Canada, CANADA Clinical Nephrology")
18
Melamed ARCH INTERN MED 2008
25 (OH) D ve Tüm Sebeplere Bağlı Mortalite birey - the Third National Health and Nutrition Examination Survey Background In patients undergoing dialysis, therapy with calcitriol or paricalcitol or other vitamin D agents is associated with reduced mortality. Observational data suggests that low 25-hydroxyvitamin D levels (25[OH]D) are associated with diabetes mellitus, hypertension, and cancers. However, whether low serum 25(OH)D levels are associated with mortality in the general population is unknown. Methods We tested the association of low 25(OH)D levels with all-cause, cancer, and cardiovascular disease (CVD) mortality in 13 331 nationally representative adults 20 years or older from the Third National Health and Nutrition Examination Survey (NHANES III) linked mortality files. Participant vitamin D levels were collected from 1988 through 1994, and individuals were passively followed for mortality through 2000. Results In cross-sectional multivariate analyses, increasing age, female sex, nonwhite race/ethnicity, diabetes, current smoking, and higher body mass index were all independently associated with higher odds of 25(OH)D deficiency (lowest quartile of 25(OH)D level, <17.8 ng/mL [to convert to nanomoles per liter, multiply by 2.496]), while greater physical activity, vitamin D supplementation, and nonwinter season were inversely associated. During a median 8.7 years of follow-up, there were 1806 deaths, including 777 from CVD. In multivariate models (adjusted for baseline demographics, season, and traditional and novel CVD risk factors), compared with the highest quartile, being in the lowest quartile (25[OH]D levels <17.8 ng/mL) was associated with a 26% increased rate of all-cause mortality (mortality rate ratio, 1.26; 95% CI, ) and a population attributable risk of 3.1%. The adjusted models of CVD and cancer mortality revealed a higher risk, which was not statistically significant. Conclusion The lowest quartile of 25(OH)D level (<17.8 ng/mL) is independently associated with all-cause mortality in the general population. Melamed ARCH INTERN MED 2008
 D ve Tüm Sebeplere Bağlı Mortalite birey - the Third National Health and Nutrition Examination Survey. Background In patients undergoing dialysis, therapy with calcitriol or paricalcitol or other vitamin D agents is associated with reduced mortality. Observational data suggests that low 25-hydroxyvitamin D levels (25[OH]D) are associated with diabetes mellitus, hypertension, and cancers. However, whether low serum 25(OH)D levels are associated with mortality in the general population is unknown. Methods We tested the association of low 25(OH)D levels with all-cause, cancer, and cardiovascular disease (CVD) mortality in nationally representative adults 20 years or older from the Third National Health and Nutrition Examination Survey (NHANES III) linked mortality files. Participant vitamin D levels were collected from 1988 through 1994, and individuals were passively followed for mortality through Results In cross-sectional multivariate analyses, increasing age, female sex, nonwhite race/ethnicity, diabetes, current smoking, and higher body mass index were all independently associated with higher odds of 25(OH)D deficiency (lowest quartile of 25(OH)D level, <17.8 ng/mL [to convert to nanomoles per liter, multiply by 2.496]), while greater physical activity, vitamin D supplementation, and nonwinter season were inversely associated. During a median 8.7 years of follow-up, there were 1806 deaths, including 777 from CVD. In multivariate models (adjusted for baseline demographics, season, and traditional and novel CVD risk factors), compared with the highest quartile, being in the lowest quartile (25[OH]D levels <17.8 ng/mL) was associated with a 26% increased rate of all-cause mortality (mortality rate ratio, 1.26; 95% CI, ) and a population attributable risk of 3.1%. The adjusted models of CVD and cancer mortality revealed a higher risk, which was not statistically significant. Conclusion The lowest quartile of 25(OH)D level (<17.8 ng/mL) is independently associated with all-cause mortality in the general population. Melamed ARCH INTERN MED")
19
Vitamin D ve Kardiyovasküler olaylar
Wang, T. J. et al. Circulation 2008;117: Copyright ©2008 American Heart Association

20
Düşük serum 25 OH-D3 düzeyleri sağlıklı kişilerde myokard enfarktüsü riski
Health Professional’s study. Erkek Yaş yıl. Giovannucci et al.Arch Int Med (2008)
")
21
Kardiyovasküler sistemde VDR
Kardiyomiyosit Endotel hücreleri Vasküler düz kas hücreleri Endotel disfonksiyonu, Vasküler kompliyans, İnflamasyon, Hücre proliferasyonu ve diferansiasyon, PTH ile ilişkili Renin-angiotensin sistem. Several mechanisms have been proposed in the model of vitamin D’s protective effects on the cardiovascular system, including its influence on inflammation, endothelial dysfunction, vascular compliance, inflammation, cell proliferation, and differentiation, as well as its effects relating to parathyroid hormone (PTH) and the renin-angiotensin system. These latter two processes are involved in the initiation and development of endothelial damage and atherosclerosis.10,11 There is clear evidence of VDR agonism’s impact on the inhibition of cytokines involved in calcification and atheroma formation,12,13 on the inhibition of proteins implicated in arterial calcification,14 and on preventing thrombosis.15
 and the renin-angiotensin system. These latter two processes are involved in the initiation and development of endothelial damage and atherosclerosis.10,11 There is clear evidence of VDR agonism’s impact on the inhibition of cytokines involved in calcification and atheroma formation,12,13 on the inhibition of proteins implicated in arterial calcification,14 and on preventing thrombosis.15.")
22
Vitamin D eksikliği ve Kardiyovasküler Risk Mekanizmaları
Mechanisms by which vitamin D deficiency may confer cardiovascular risk. Potential effects of vitamin D metabolism on the cardiovascular system are divergent, but share common initial steps of nuclear and plasma membrane VDR activation. VDR, vitamin D receptor; 1, 25-OH D2, 1, 25-dihydroxyvitamin D; RXR, retinoid-X receptor; Ca+, calcium cation; ANP, atrial natriuretic peptide; MMP, matrix metalloproteinases; VDRE, vitamin D response elements (promoter region of target genes); RAS, renin–angiotensin system; VEGF, vascular endothelial growth factor; VSMC, vascular smooth muscle cells. Al Mheid I et al. Eur Heart J 2013
; RAS, renin–angiotensin system; VEGF, vascular endothelial growth factor; VSMC, vascular smooth muscle cells. Al Mheid I et al. Eur Heart J")
23
Azalan VDR Aktivasyonu Artan Miyokardiyal Hipertrofiye Neden Olur35
Hem sistemik hem de kardiyak RAS aktivasyonu, VDR eksikliği bulunan farelerde kardiyak hipertrofi gelişiminde önemli bir rol oynar VDR eksikliği bulunan farelerin kalp-vücut ağırlığı oranı WT (wild type = doğal tip) farelerdekine göre anlamlı ölçüde yüksektir (%20 ile), bu da mutant farelerde kardiyak hipertrofi bulunduğunu gösterir. VDR aktivasyonu azaldıkça, miyokardiyal hipertrofi artmaktadır. Hem sistemik hem de kardiyak RAS aktivasyonu, VDR eksikliği bulunan farelerde kardiyak hipertrofi gelişiminde önemli bir rol oynar.35 VDR eksikliği bulunan farelerin kalp ağırlığı-vücut ağırlığı oranı normal deneklerdekine göre anlamlı ölçüde yüksektir (%20). 35. Xiang W, et al. Am J Physiol. 2005;288:e125-e132
 farelerdekine göre anlamlı ölçüde yüksektir (%20 ile), bu da mutant farelerde kardiyak hipertrofi bulunduğunu gösterir. VDR aktivasyonu azaldıkça, miyokardiyal hipertrofi artmaktadır. Hem sistemik hem de kardiyak RAS aktivasyonu, VDR eksikliği bulunan farelerde kardiyak hipertrofi gelişiminde önemli bir rol oynar.35. VDR eksikliği bulunan farelerin kalp ağırlığı-vücut ağırlığı oranı normal deneklerdekine göre anlamlı ölçüde yüksektir (%20). 35. Xiang W, et al. Am J Physiol. 2005;288:e125-e132.")
24
VDR reseptörleri tahrip edilmiş -/- farelerde sol ventrikül hipertrofisi gelişir
1 [Xiang2005, E127Figure 1a] 1 [Xiang2005, E127Figure 1c] Miyosit çapı (bağıl birim) Kalp (mg)/vücut (g) It has been shown that VDR-deficient [VDR(/)] mice develop high blood pressure accompanied by an increase in heart-weight-to-body-weight ratio. This reflects, at least in part, effects from activation of the systemic RAAS. The goal was to determine whether the cardiac hypertrophy in VDR(/) mice is associated with activation of the systemic and cardiac RAAS, and whether inhibition of RAAS activation can reverse the hypertrophic process. 1[Xiang2005, E125c] As expected, the heart-weight-to-body-weight ratio of VDR(/) mice was significantly higher (by 20%) than that of WT mice, indicating the presence of cardiac hypertrophy in the mutant mice. Histological analyses confirmed that the size of left ventricular myocytes was markedly increased (by 22% in diameter) in VDR(/) mice compared with WT mice. 1[Xiang2005, E126g] Our results suggest that activation of both systemic and cardiac RAS plays an important role in the development of cardiac hypertrophy in VDR(/) mice. 1[Xiang2005, E126g] Reference: Xiang W, Kong J, Chen S, et al. Cardiac hypertrophy in vitamin D receptor knockout mice: role of the systemic and cardiac renin-angiotensin systems. Am J Physiol Endocrinol Metab. 2005;288(1):E125-E132. Am J Physiol Endocrinol Metab. 2005 Jan;288(1):E Epub 2004 Sep 14. Cardiac hypertrophy in vitamin D receptor knockout mice: role of the systemic and cardiac renin-angiotensin systems. Xiang W1, Kong J, Chen S, Cao LP, Qiao G, Zheng W, Liu W, Li X, Gardner DG, Li YC. Author information Abstract Our recent studies suggest that 1,25-dihydroxyvitamin D3 functions as an endocrine suppressor of renin biosynthesis. Genetic disruption of the vitamin D receptor (VDR) results in overstimulation of the renin-angiotensin system (RAS), leading to high blood pressure and cardiac hypertrophy. Consistent with the higher heart-to-body weight ratio, the size of left ventricular cardiomyocytes in VDR knockout (KO) mice was markedly increased compared with wild-type (WT) mice. As expected, levels of atrial natriuretic peptide (ANP) mRNA and circulating ANP were also increased in VDRKO mice. Treatment of VDRKO mice with captopril reduced cardiac hypertrophy and normalized ANP expression. To investigate the role of the cardiac RAS in the development of cardiac hypertrophy, the expression of renin, angiotensinogen, and AT-1a receptor in the heart was examined by real-time RT-PCR and immunostaining. In VDRKO mice, the cardiac renin mRNA level was significantly increased, and this increase was further amplified by captopril treatment. Consistently, intense immunostaining was detected in the left ventricle of captopril-treated WT and VDRKO mice by use of an anti-renin antibody. Levels of cardiac angiotensinogen and AT-1a receptor mRNAs were unchanged in the mutant mice. These data suggest that the cardiac hypertrophy seen in VDRKO mice is a consequence of activation of both the systemic and cardiac RAS and support the notion that 1,25-dihydroxyvitamin D(3) regulates cardiac functions, at least in part, through the RAS. *p <0,001 *p <0,01 Kalp-Vücut Oranı Miyosit Çapı Xiang W, et al. Am J Physiol. 2005;288:e125-e132 24
 Kalp (mg)/vücut (g) It has been shown that VDR-deficient [VDR(/)] mice develop high blood pressure accompanied by an increase in heart-weight-to-body-weight ratio. This reflects, at least in part, effects from activation of the systemic RAAS. The goal was to determine whether the cardiac hypertrophy in VDR(/) mice is associated with activation of the systemic and cardiac RAAS, and whether inhibition of RAAS activation can reverse the hypertrophic process. 1[Xiang2005, E125c] As expected, the heart-weight-to-body-weight ratio of VDR(/) mice was significantly higher (by 20%) than that of WT mice, indicating the presence of cardiac hypertrophy in the mutant mice. Histological analyses confirmed that the size of left ventricular myocytes was markedly increased (by 22% in diameter) in VDR(/) mice compared with WT mice. 1[Xiang2005, E126g] Our results suggest that activation of both systemic and cardiac RAS plays an important role in the development of cardiac hypertrophy in VDR(/) mice. 1[Xiang2005, E126g] Reference: Xiang W, Kong J, Chen S, et al. Cardiac hypertrophy in vitamin D receptor knockout mice: role of the systemic and cardiac renin-angiotensin systems. Am J Physiol Endocrinol Metab. 2005;288(1):E125-E132. Am J Physiol Endocrinol Metab Jan;288(1):E Epub 2004 Sep 14. Cardiac hypertrophy in vitamin D receptor knockout mice: role of the systemic and cardiac renin-angiotensin systems. Xiang W1, Kong J, Chen S, Cao LP, Qiao G, Zheng W, Liu W, Li X, Gardner DG, Li YC. Author information. Abstract. Our recent studies suggest that 1,25-dihydroxyvitamin D3 functions as an endocrine suppressor of renin biosynthesis. Genetic disruption of the vitamin D receptor (VDR) results in overstimulation of the renin-angiotensin system (RAS), leading to high blood pressure and cardiac hypertrophy. Consistent with the higher heart-to-body weight ratio, the size of left ventricular cardiomyocytes in VDR knockout (KO) mice was markedly increased compared with wild-type (WT) mice. As expected, levels of atrial natriuretic peptide (ANP) mRNA and circulating ANP were also increased in VDRKO mice. Treatment of VDRKO mice with captopril reduced cardiac hypertrophy and normalized ANP expression. To investigate the role of the cardiac RAS in the development of cardiac hypertrophy, the expression of renin, angiotensinogen, and AT-1a receptor in the heart was examined by real-time RT-PCR and immunostaining. In VDRKO mice, the cardiac renin mRNA level was significantly increased, and this increase was further amplified by captopril treatment. Consistently, intense immunostaining was detected in the left ventricle of captopril-treated WT and VDRKO mice by use of an anti-renin antibody. Levels of cardiac angiotensinogen and AT-1a receptor mRNAs were unchanged in the mutant mice. These data suggest that the cardiac hypertrophy seen in VDRKO mice is a consequence of activation of both the systemic and cardiac RAS and support the notion that 1,25-dihydroxyvitamin D(3) regulates cardiac functions, at least in part, through the RAS. *p <0,001. *p <0,01. Kalp-Vücut Oranı. Miyosit Çapı. Xiang W, et al. Am J Physiol. 2005;288:e125-e")
25
Zhou C, Lu F, Cao K, et al. Kidney Int. 2008;74(2):170-179.
Farelerde 1 α(OH)ase +/+ geninin yok edilmesi : Artan Miyokardiyal Hipertrofi ND C 1 α(OH)ase -/- 1 α(OH)ase +/+ VDR aktivasyonu eksikliği : Sol Ventrikül Hipertrofisi Hipertansiyon Serum renin düzeylerinde artış Sol ventrikül hipertrofisi VDR aktivasyonu sağlanırsa: Kan basıncı normalleşir Serum renin düzeyi normalleşir Sol Ventrikül Hipertrofisi önlenir. 1 [Zhou, 172Figure 1] To determine whether the cardiovascular effect of 1,25(OH)2D is dependent on calcium and/or phosphorus, mice with targeted deletion of the 25(OH)D 1-hydroxylase and their wild-type littermates were fed a normal diet or a diet to rescue the ambient serum calcium and phosphorus levels. Mice on the normal diet were treated daily with vehicle or 1,25(OH)2D3 while mice on the rescue diet received vehicle, captopril or losartan. After four weeks the vehicle-treated knockout mice developed hypertension, cardiac hypertrophy and impaired cardiac function along with an up-regulation of the renin-angiotensin system in both renal and cardiac tissues. Although the serum calcium and phosphorus levels were normalized in knockout mice on the rescue diet, abnormalities in blood pressure, cardiac structure-function and the renin-angiotensin system remained. In contrast, 1,25(OH)2D3 not only normalized serum calcium and phosphorus levels but also normalized blood pressure, cardiac structure-function and the renin-angiotensin system. Treatment of the knockout mice with either captopril or losartan normalized blood pressure and cardiac structure and function although renin expression remained elevated. This study shows that 1,25(OH)2D plays a protective role in the cardiovascular system by repressing the renin-angiotensin system independent of extracellular calcium or phosphorus.KO mice develop: 1[Zhou2008, 171cd, 175d Hypertension Increase of serum renin levels Left ventricular hypertrophy 1,25 (OH2)D3: 1[Zhou2008, 171f, 175d-176a] Normalizes BP Normalizes serum renin Prevents LVH References: 1. Zhou C, Lu F, Cao K, et al. Calcium-independent and 1,25(OH)2D3- dependent regulation of the renin-angiotensin system in 1alpha-hydroxylase knockout mice. Kidney Int. 2008;74(2): Zhou C, Lu F, Cao K, et al. Kidney Int. 2008;74(2): 25
ase +/+ geninin yok edilmesi : Artan Miyokardiyal Hipertrofi. ND. C. 1 α(OH)ase -/- 1 α(OH)ase +/+ VDR aktivasyonu eksikliği : Sol Ventrikül Hipertrofisi. Hipertansiyon. Serum renin düzeylerinde artış. Sol ventrikül hipertrofisi. VDR aktivasyonu sağlanırsa: Kan basıncı normalleşir. Serum renin düzeyi normalleşir. Sol Ventrikül Hipertrofisi önlenir. 1 [Zhou, 172Figure 1] To determine whether the cardiovascular effect of 1,25(OH)2D is dependent on calcium and/or phosphorus, mice with targeted deletion of the 25(OH)D 1-hydroxylase and their wild-type littermates were fed a normal diet or a diet to rescue the ambient serum calcium and phosphorus levels. Mice on the normal diet were treated daily with vehicle or 1,25(OH)2D3 while mice on the rescue diet received vehicle, captopril or losartan. After four weeks the vehicle-treated knockout mice developed hypertension, cardiac hypertrophy and impaired cardiac function along with an up-regulation of the renin-angiotensin system in both renal and cardiac tissues. Although the serum calcium and phosphorus levels were normalized in knockout mice on the rescue diet, abnormalities in blood pressure, cardiac structure-function and the renin-angiotensin system remained. In contrast, 1,25(OH)2D3 not only normalized serum calcium and phosphorus levels but also normalized blood pressure, cardiac structure-function and the renin-angiotensin system. Treatment of the knockout mice with either captopril or losartan normalized blood pressure and cardiac structure and function although renin expression remained elevated. This study shows that 1,25(OH)2D plays a protective role in the cardiovascular system by repressing the renin-angiotensin system independent of extracellular calcium or phosphorus.KO mice develop: 1[Zhou2008, 171cd, 175d. Hypertension. Increase of serum renin levels. Left ventricular hypertrophy. 1,25 (OH2)D3: 1[Zhou2008, 171f, 175d-176a] Normalizes BP. Normalizes serum renin. Prevents LVH. References: 1. Zhou C, Lu F, Cao K, et al. Calcium-independent and 1,25(OH)2D3- dependent regulation of the renin-angiotensin system in 1alpha-hydroxylase knockout mice. Kidney Int. 2008;74(2): Zhou C, Lu F, Cao K, et al. Kidney Int. 2008;74(2):")
26
Vitamin D ve Kan Basıncı 1,25(OH)2D3 ve Plasma Renin Arasındaki İlişki
Resnick et al, Ann Intern Med, 1986

27
HT olanlarda (A) ve olmayanlarda B kardiyovasküler olay geçirme olasılığı ve Vitamin D yetersizliği
1739 Framingham Offspring Study katılımcısı (ortalama yaş 59 yıl; %55kadın; beyaz, daha önceden bilinen KVH yok). ortalama 25-OH D düzeyi ng/mL. %28 kişide 25-OH D <15 %9 da having 25-OH D <10 ng/mL. Ortalama izlem süresi 5.4 yıl Vit. D eksikliği olanlar:---- Background— Vitamin D receptors have a broad tissue distribution that includes vascular smooth muscle, endothelium, and cardiomyocytes. A growing body of evidence suggests that vitamin D deficiency may adversely affect the cardiovascular system, but data from longitudinal studies are lacking. Methods and Results— We studied 1739 Framingham Offspring Study participants (mean age 59 years; 55% women; all white) without prior cardiovascular disease. Vitamin D status was assessed by measuring 25-dihydroxyvitamin D (25-OH D) levels. Prespecified thresholds were used to characterize varying degrees of 25-OH D deficiency (<15 ng/mL, <10 ng/mL). Multivariable Cox regression models were adjusted for conventional risk factors. Overall, 28% of individuals had levels <15 ng/mL, and 9% had levels <10 ng/mL. During a mean follow-up of 5.4 years, 120 individuals developed a first cardiovascular event. Individuals with 25-OH D <15 ng/mL had a multivariable-adjusted hazard ratio of 1.62 (95% confidence interval 1.11 to 2.36, P=0.01) for incident cardiovascular events compared with those with 25-OH D 15 ng/mL. This effect was evident in participants with hypertension (hazard ratio 2.13, 95% confidence interval 1.30 to 3.48) but not in those without hypertension (hazard ratio 1.04, 95% confidence interval 0.55 to 1.96). There was a graded increase in cardiovascular risk across categories of 25-OH D, with multivariable-adjusted hazard ratios of 1.53 (95% confidence interval 1.00 to 2.36) for levels 10 to <15 ng/mL and 1.80 (95% confidence interval 1.05 to 3.08) for levels <10 ng/mL (P for linear trend=0.01). Further adjustment for C-reactive protein, physical activity, or vitamin use did not affect the findings. Conclusions— Vitamin D deficiency is associated with incident cardiovascular disease. Further clinical and experimental studies may be warranted to determine whether correction of vitamin D deficiency could contribute to the prevention of cardiovascular disease. Wang, T. J. et al. Circulation 2008;117:
. ortalama 25-OH D düzeyi 19.7 ng/mL. %28 kişide 25-OH D <15. %9 da having 25-OH D <10 ng/mL. Ortalama izlem süresi 5.4 yıl. Vit. D eksikliği olanlar:---- Background— Vitamin D receptors have a broad tissue distribution that includes vascular smooth muscle, endothelium, and cardiomyocytes. A growing body of evidence suggests that vitamin D deficiency may adversely affect the cardiovascular system, but data from longitudinal studies are lacking. Methods and Results— We studied 1739 Framingham Offspring Study participants (mean age 59 years; 55% women; all white) without prior cardiovascular disease. Vitamin D status was assessed by measuring 25-dihydroxyvitamin D (25-OH D) levels. Prespecified thresholds were used to characterize varying degrees of 25-OH D deficiency (<15 ng/mL, <10 ng/mL). Multivariable Cox regression models were adjusted for conventional risk factors. Overall, 28% of individuals had levels <15 ng/mL, and 9% had levels <10 ng/mL. During a mean follow-up of 5.4 years, 120 individuals developed a first cardiovascular event. Individuals with 25-OH D <15 ng/mL had a multivariable-adjusted hazard ratio of 1.62 (95% confidence interval 1.11 to 2.36, P=0.01) for incident cardiovascular events compared with those with 25-OH D 15 ng/mL. This effect was evident in participants with hypertension (hazard ratio 2.13, 95% confidence interval 1.30 to 3.48) but not in those without hypertension (hazard ratio 1.04, 95% confidence interval 0.55 to 1.96). There was a graded increase in cardiovascular risk across categories of 25-OH D, with multivariable-adjusted hazard ratios of 1.53 (95% confidence interval 1.00 to 2.36) for levels 10 to <15 ng/mL and 1.80 (95% confidence interval 1.05 to 3.08) for levels <10 ng/mL (P for linear trend=0.01). Further adjustment for C-reactive protein, physical activity, or vitamin use did not affect the findings. Conclusions— Vitamin D deficiency is associated with incident cardiovascular disease. Further clinical and experimental studies may be warranted to determine whether correction of vitamin D deficiency could contribute to the prevention of cardiovascular disease. Wang, T. J. et al. Circulation 2008;117:")
28
Aloi et al Epidel Infect 2007
Vitamin D ve influenza We conducted a 3-year randomized controlled trial to test the hypothesis that vitamin D3 supplementation would prevent bone loss in calcium-replete, African-American post-menopausal women. A total of 208 women were randomized to receive vitamin D3 (n=104) or placebo (n=104). After 2 years, the vitamin D3 dose was increased to 50 mg/d (2000 IU) in the active group. None of the patients had a history of chronic obstructive pulmonary disease, congestive heart failure, or myocardial infarction. Few patients had a history of asthma and seasonal allergies with no significant difference After 3 years, a total of 34 patients reported cold and influenza symptoms, eight in the vitamin D3 group vs. 26 in the placebo group (P<0.002). When we examined the seasonality of the symptoms, we found that the placebo group had cold/influenza symptoms mostly in the winter. The vitamin D group had symptoms throughout the year while on 20 mg/d, whereas only one subject had a cold/influenza while on 50 mg/d (Fig.). None of the 34 patients with reported cold and influenza symptoms had significant comorbidities. Aloi et al Epidel Infect 2007 28
 or placebo (n=104). After. 2 years, the vitamin D3 dose was increased to 50 mg/d. (2000 IU) in the active group. None of the patients. had a history of chronic obstructive pulmonary. disease, congestive heart failure, or myocardial. infarction. Few patients had a history of asthma. and seasonal allergies with no significant difference. After 3 years, a total of 34 patients reported cold. and influenza symptoms, eight in the vitamin D3. group vs. 26 in the placebo group (P<0.002). When. we examined the seasonality of the symptoms, we. found that the placebo group had cold/influenza. symptoms mostly in the winter. The vitamin D group. had symptoms throughout the year while on 20 mg/d, whereas only one subject had a cold/influenza while. on 50 mg/d (Fig.). None of the 34 patients with. reported cold and influenza symptoms had significant. comorbidities. Aloi et al Epidel Infect")
29
Enfeksiyon ve immünite
49nolu Robert Bals et al. Infect. Immun. 1999;67:

30
Human cathelicidin antimicrobial protein (hCAP18) düzeyleri ve hemodiyaliz hastaları
51 nolu Percentage of individuals in each tertile of human cathelicidin antimicrobial protein (hCAP18) levels who survived for at least 1 year while undergoing hemodialysis (control patients). The remaining subjects died because of infection within 1 year after initiation of hemodialysis (case patients). Individuals within the lowest tertile of hCAP18 levels had a lower chance of survival than did subjects in tertiles 2 or 3 (P=.007). There was no significant difference in mortality between tertiles 2 and 3 (P=.74). Tertiles are based on the distribution of hCAP18 levels among control patients. Tertile 1 hCAP18 levels, 129–487 ng/mL (n=110 ); tertile 2 hCAP18 levels, 488–729 ng/mL ( n=87 ); tertile 3 hCAP18 levels, 732–2856 ng/mL (n= 82 ). Background. Human cathelicidin antimicrobial protein (hCAP18) is an antimicrobial and immunomodulatory peptide that has pleiotropic effects and is transcriptionally regulated by vitamin D. Because the administration of vitamin D analogues has been linked to decreased mortality among patients with end-stage renal disease, we hypothesized that low hCAP18 levels would identify those who are at increased risk of death attributable to infection while undergoing hemodialysis. Methods. We performed a case-control study nested in a prospective cohort of patients ( n=10,044 ) initiating incident hemodialysis. Case patients ( n=81 ) were those who died of an infectious disease within 1 year; control patients ( n=198 ) were those who survived at least 1 year while undergoing dialysis. Results. Mean (±SD) baseline levels of hCAP18 in case patients and control patients were 539±278 ng/mL and 650±343 ng/mL, respectively ( P=.006 ). hCAP18 levels had a modest correlation with 1,25-dihydroxyvitamin D levels ( r=0.23 ; P=.053 ) but not with 25-hydroxyvitamin D levels ( r=-0.06 ; P=.44 ). Patients with hCAP18 levels in the lowest tertile had a 2-fold increased risk (odds ratio, 2.1; 95% confidence interval, 1.2–3.5) of death attributable to infection; after multivariable adjustment, this relationship remained statistically significant (odds ratio, 3.7; 95% confidence interval, 1.2–11.2). Conclusions. In individuals initiating chronic hemodialysis, low baseline levels of hCAP18, a vitamin D–regulated antimicrobial protein, are independently associated with an increased risk of death attributable to infection. Adrian F. Gombart et al. Clin Infect Dis. 2009;48: © 2009 by the Infectious Diseases Society of America
 levels who survived for at least 1 year while undergoing hemodialysis (control patients). The remaining subjects died because of infection within 1 year after initiation of hemodialysis (case patients). Individuals within the lowest tertile of hCAP18 levels had a lower chance of survival than did subjects in tertiles 2 or 3 (P=.007). There was no significant difference in mortality between tertiles 2 and 3 (P=.74). Tertiles are based on the distribution of hCAP18 levels among control patients. Tertile 1 hCAP18 levels, 129–487 ng/mL (n=110 ); tertile 2 hCAP18 levels, 488–729 ng/mL ( n=87 ); tertile 3 hCAP18 levels, 732–2856 ng/mL (n= 82 ). Background. Human cathelicidin antimicrobial protein (hCAP18) is an antimicrobial and immunomodulatory peptide that has pleiotropic effects and is transcriptionally regulated by vitamin D. Because the administration of vitamin D analogues has been linked to decreased mortality among patients with end-stage renal disease, we hypothesized that low hCAP18 levels would identify those who are at increased risk of death attributable to infection while undergoing hemodialysis. Methods. We performed a case-control study nested in a prospective cohort of patients ( n=10,044 ) initiating incident hemodialysis. Case patients ( n=81 ) were those who died of an infectious disease within 1 year; control patients ( n=198 ) were those who survived at least 1 year while undergoing dialysis. Results. Mean (±SD) baseline levels of hCAP18 in case patients and control patients were 539±278 ng/mL and 650±343 ng/mL, respectively ( P=.006 ). hCAP18 levels had a modest correlation with 1,25-dihydroxyvitamin D levels ( r=0.23 ; P=.053 ) but not with 25-hydroxyvitamin D levels ( r=-0.06 ; P=.44 ). Patients with hCAP18 levels in the lowest tertile had a 2-fold increased risk (odds ratio, 2.1; 95% confidence interval, 1.2–3.5) of death attributable to infection; after multivariable adjustment, this relationship remained statistically significant (odds ratio, 3.7; 95% confidence interval, 1.2–11.2). Conclusions. In individuals initiating chronic hemodialysis, low baseline levels of hCAP18, a vitamin D–regulated antimicrobial protein, are independently associated with an increased risk of death attributable to infection. Adrian F. Gombart et al. Clin Infect Dis. 2009;48: © 2009 by the Infectious Diseases Society of America.")
31
Vitamin D Anti-mikrobiyal Aktivite Endojen Anti-mikrobiyal Peptidler
Kathelisidin Gen Aktivasyonu MAKROFAJ 25(OH)D 1,25-(OH)2D 1-hidroksilaz + N Mikrop 31
D. 1,25-(OH)2D. 1-hidroksilaz. + N. Mikrop. 31.")
32
Vitamin D ve enfeksiyonlar
Vitamin D anti-mikrobiyal aktivite Ana aktivasyon defensin geni aktivasyonu KatheliSidin, LL-37, bir antimikrobiyal peptit (AMP) potent antiendotoksin aktivitesi LL-37 bakteriyel enfeksiyonlar ile savaşta yer aldığı ile ilgili güçlü deliller, viral enfeksiyonlar ile savaşta artan deliller mevcut Vitamin D, the TH2 immun yanıtta ve maktofaj ve monosit üretimini artırmakta Mookherjee N, et al. Expert Opin Ther Targets 2007 32
 potent antiendotoksin aktivitesi. LL-37 bakteriyel enfeksiyonlar ile savaşta yer aldığı ile ilgili güçlü deliller, viral enfeksiyonlar ile savaşta artan deliller mevcut. Vitamin D, the TH2 immun yanıtta ve maktofaj ve monosit üretimini artırmakta. Mookherjee N, et al. Expert Opin Ther Targets")
33
Vitamin D ve immun sistem
Bakteriyel defans mekanizmasında artma Otoimmün fenomene tolerejenik profilde artma Dendritik hücreler ve diğer antijen sunan hücrelerin matürasyon, diferansiyon ve fonksiyonlarının düzenlenmesi T lenfositlerden sitokin salınımının baskılanması

34
Vitamin D düzeyleri ve KBH Böbrek ve yaşam survi
168 KBH (evre2-5) Ortalama izlem süresi 48 ay 48 hasta diyalize başladı 78 hasta öldü. Plazma 25(OH)D KBH progresyonu ve ölümün negatif bağımsız göstergesi [25(OH)D düzeyleri 1,25(OH)2 D den daha iyi bir gösterge] Vitamin D deficiency has been linked to cardiovascular disease and early mortality in patients on hemodialysis; however, it is not known if the same association exists at earlier stages of chronic kidney disease. To determine this we enrolled 168 consecutive new referrals to a chronic kidney disease clinic over a 2 year period and followed them for up to 6 years. All patients were clinically stable and had an estimated glomerular filtration rate (eGFR) at stage 2 or less and were without an imminent need for dialysis. Baseline 25- hydroxyvitamin D levels directly and significantly correlated with eGFR. After an average follow-up of 48 months, 48 patients started dialysis and 78 had died. In crude analyses, 25-hydroxyvitamin D predicted both time to death and endstage renal disease. A dual-event Cox’s model confirmed 25-hydroxyvitamin D as an independent predictor of study outcomes when adjusted for age, heart failure, smoking, C-reactive protein, albumin, phosphate, use of converting enzyme inhibitors or angiotensin receptor blockers, and eGFR. Our study shows that plasma 25-hydroxyvitamin D is an independent inverse predictor of disease progression and death in patients with stage 2–5 chronic kidney disease. Ravani ve ark. Kidney International 2009
 Ortalama izlem süresi 48 ay. 48 hasta diyalize başladı. 78 hasta öldü. Plazma 25(OH)D KBH progresyonu ve ölümün negatif bağımsız göstergesi. [25(OH)D düzeyleri 1,25(OH)2 D den daha iyi bir gösterge] Vitamin D deficiency has been linked to cardiovascular. disease and early mortality in patients on hemodialysis; however, it is not known if the same association exists at. earlier stages of chronic kidney disease. To determine this we. enrolled 168 consecutive new referrals to a chronic kidney. disease clinic over a 2 year period and followed them for up. to 6 years. All patients were clinically stable and had an. estimated glomerular filtration rate (eGFR) at stage 2 or less. and were without an imminent need for dialysis. Baseline 25- hydroxyvitamin D levels directly and significantly correlated. with eGFR. After an average follow-up of 48 months, 48. patients started dialysis and 78 had died. In crude analyses, 25-hydroxyvitamin D predicted both time to death and endstage. renal disease. A dual-event Cox’s model confirmed. 25-hydroxyvitamin D as an independent predictor of study. outcomes when adjusted for age, heart failure, smoking, C-reactive protein, albumin, phosphate, use of converting. enzyme inhibitors or angiotensin receptor blockers, and. eGFR. Our study shows that plasma 25-hydroxyvitamin D is. an independent inverse predictor of disease progression and. death in patients with stage 2–5 chronic kidney disease. Ravani ve ark. Kidney International")
35
Kolon kanseri mortalite oranları (solar radyasyon cal/cm2)
")
36
Vitamin D görevleri ve eksikliği
Fizyolojik sistem Biyolojik yanıt Vitamin D eksikliği ve Hastalıklar Bütün hücreler Hücre siklusun düzenlenmesi Hücre proliferasyonun önlenmesi Kanser, Prostat, meme, kolon, lösemi ve diğerleri Kalsiyum dengesi Bağırsaktan Ca emilimi, Kemik remodeling Rikets, osteomalasi,osteoporoz İmmun sistem Makrofaj fonksiyonlarının uyarılması,Dendritik vr T hücre fonk. Enfeksiyonlarda artma, tbc, Otoimmün hast.,Tip 1 DM, MS, psöriasis Pankreas ß hüc. İnsulin salınımı Bozulmuş glikoz intoleransı, DM Kalp-kardiyovasküler Renin anjiotensin düzenlenmesi, koagülasyon, fibrinoliz,Kalp kas fonk. Yüksek reninli HT, artmış trombogenezis Kas Kas iskelet sisteminin gelişimi Kas gücünün artırılması Miyopati, artmış düşme Beyin (Henüz araştırma aşamasında) Sıçanlarda davranış değ.
 Sıçanlarda davranış değ.")
37
Taskapan Int Urol Nephrol 2012
Studies Patients and aims Methods Results Conclusion Steenvoorde et al in 1985 (31) 10 children on HD The effect of 24,25(OH)2D combined with dihydrotachysterol on clinical, radiological, biochemical and bone histological parameters administration of 25 micrograms 25 mcg 24,25(OH)2D combined with dihydrotachysterol for 6 months A decrease in serum Ca levels and significant reduction of the surface percentage of bone trabecula covered with osteoclasts. An increase in bone mineralization was shown by X-rays and measured by dual photonabsorptiometry. Administered 24,25(OH)D interferes with dihydrotachysterol metabolism and increases dihydrotachysterol tolerance. Praino et al in 1986 (32) 10 hypercalcemic dialysis pts and 30 normocalcemic dialysis pts Hypercalcemic pts treated with with 24,25(OH)2D 10-40mcg daily Osteomalacia was more severe and bone aluminum staining was stronger in the hypercalcemic patients than in the control patients. 24,25(OH)D was effective in lowering the serum Ca level. Ben-Ezer et al (33) in 1991 20 CAPD pts Effect of pharmacological doses of 24,25(OH)D on PTH without causing hypercalcemia which 1,25(OH)2D causes 24,25(OH)D was given in addition to existing treatment with 1 alpha-(OH)D3 and calcium carbonate. A significant decrease in intact PTH levels with 24,25(OH)D addition Oral administration of 24,25(OH)D combined with 1 alpha-OH-D3 is safe and capable of suppressing the raised serum PTH levels of ESRD pts without significant hypercalcemia Kazama et al in 1996 (35) Uremic rats the effect of 24,25(OH)D on uremic bone disease The rats were randomly on 0.5 μg/kg BW 24,25(OH)D or on 5 μg/kg BW 24,25(OH)D or0.01 μg/kg BW 1,25(OH)2D or 0.01 μg/kg BW 1,25(OH)2D and 5 μg/kg BW 24,25(OH) 2D or nothing Treatment with 24,25(OH)D (5 Fg/kg BW) not only ameliorated high-turnover bone disease as with 1,25D, but also prevented the reduction of trabecular bone volume without any changes of serum PTH levels 24,25(OH)D prevented the high-turnover bone disease accompanied by bone volume reduction in model rats of mild renal failure. Taskapan Int Urol Nephrol 2012
 10 children on HD. The effect of 24,25(OH)2D combined with dihydrotachysterol on clinical, radiological, biochemical and bone histological parameters. administration of 25 micrograms 25 mcg 24,25(OH)2D combined with dihydrotachysterol for 6 months. A decrease in serum Ca levels and significant reduction of the surface percentage of bone trabecula covered with osteoclasts. An increase in bone mineralization was shown by X-rays and measured by dual photonabsorptiometry. Administered 24,25(OH)D interferes with dihydrotachysterol metabolism and increases dihydrotachysterol tolerance. Praino et al in 1986 (32) 10 hypercalcemic dialysis pts and 30 normocalcemic dialysis pts. Hypercalcemic pts treated with with 24,25(OH)2D 10-40mcg daily. Osteomalacia was more severe and bone aluminum staining was stronger in the hypercalcemic patients than in the control patients. 24,25(OH)D was effective in lowering the serum Ca level. Ben-Ezer et al (33) in CAPD pts. Effect of pharmacological doses of 24,25(OH)D on PTH without causing hypercalcemia which 1,25(OH)2D causes. 24,25(OH)D was given in addition to existing treatment with 1 alpha-(OH)D3 and calcium carbonate. A significant decrease in intact PTH levels with 24,25(OH)D addition. Oral administration of 24,25(OH)D combined with 1 alpha-OH-D3 is safe and capable of suppressing the raised serum PTH levels of ESRD pts without significant hypercalcemia. Kazama et al in 1996 (35) Uremic rats the effect of 24,25(OH)D on uremic bone disease. The rats were randomly on 0.5 μg/kg BW 24,25(OH)D. or on 5 μg/kg BW 24,25(OH)D. or0.01 μg/kg BW 1,25(OH)2D or μg/kg BW 1,25(OH)2D and 5 μg/kg BW 24,25(OH) 2D or nothing. Treatment with 24,25(OH)D (5 Fg/kg BW) not only ameliorated high-turnover. bone disease as with 1,25D, but also prevented the reduction of trabecular bone volume without any changes. of serum PTH levels. 24,25(OH)D prevented the high-turnover bone disease accompanied by bone volume reduction in model rats of mild renal failure. Taskapan Int Urol Nephrol")
38
Taskapan Int Urol Nephrol 2012

39
Ulutas, Taskapan ve ark Int Urol Nephrol 2012
Vitamin D replasmanı öncesi Mean±Std. Deviation Vitamin D replasmanı sonrası P value 25OHD3 (µg/l) 10±4,7 82,9±56,5 0,000 HOMA-IR 4,3±3,2 2,7±1,9 0,010 Ins (µiu/ml) 17,6±11,2 11,9±7,8 0,018 Leptin (ng/ml) 12,9±17, 6 18,1±19,5 0,001 Adip (µg/ml) 14,9±12,0 16,1±11,5 0,251 Glu (mg/dl) 95,4±11,2 93,1±12,2 0,670 BUN (mg/dl) 54, 2±16,3 52,8±15,9 0,569 Cr (mg/dl) 9,4±3,1 9,4±2,9 0,925 Alb (g/dl) 3,1±0,5 3,0±0,4 0,269 Ca (mg/dl) 9,4±0,9 9,2±0,6 0,097 P (mg/dl) 4,7±0,9 4,9±1,4 0,776 PTH (pg/ml) 551,9±276,6 434,0±273,4 0,029 Ulutas, Taskapan ve ark Int Urol Nephrol 2012
 10±4,7. 82,9±56,5. 0,000. HOMA-IR. 4,3±3,2. 2,7±1,9. 0,010. Ins (µiu/ml) 17,6±11,2. 11,9±7,8. 0,018. Leptin (ng/ml) 12,9±17, 6. 18,1±19,5. 0,001. Adip (µg/ml) 14,9±12,0. 16,1±11,5. 0,251. Glu (mg/dl) 95,4±11,2. 93,1±12,2. 0,670. BUN (mg/dl) 54, 2±16,3. 52,8±15,9. 0,569. Cr (mg/dl) 9,4±3,1. 9,4±2,9. 0,925. Alb (g/dl) 3,1±0,5. 3,0±0,4. 0,269. Ca (mg/dl) 9,4±0,9. 9,2±0,6. 0,097. P (mg/dl) 4,7±0,9. 4,9±1,4. 0,776. PTH (pg/ml) 551,9±276,6. 434,0±273,4. 0,029. Ulutas, Taskapan ve ark Int Urol Nephrol")
40
Vitamin D replasmanı ve Metaanaliz çalışması
Objective To evaluate the breadth, validity, and presence of biases of the associations of vitamin D with diverse outcomes. Design Umbrella review of the evidence across systematic reviews and meta-analyses of observational studies of plasma 25-hydroxyvitamin D or 1,25-dihydroxyvitamin D concentrations and randomised controlled trials of vitamin D supplementation. Data sources Medline, Embase, and screening of citations and references. Eligibility criteria Three types of studies were eligible for the umbrella review: systematic reviews and meta-analyses that examined observational associations between circulating vitamin D concentrations and any clinical outcome; and meta-analyses of randomised controlled trials assessing supplementation with vitamin D or active compounds (both established and newer compounds of vitamin D). Results 107 systematic literature reviews and 74 meta-analyses of observational studies of plasma vitamin D concentrations and 87 meta-analyses of randomised controlled trials of vitamin D supplementation were identified. The relation between vitamin D and 137 outcomes has been explored, covering a wide range of skeletal, malignant, cardiovascular, autoimmune, infectious, metabolic, and other diseases. Ten outcomes were examined by both meta-analyses of observational studies and meta-analyses of randomised controlled trials, but the direction of the effect and level of statistical significance was concordant only for birth weight (maternal vitamin D status or supplementation). On the basis of the available evidence, an association between vitamin D concentrations and birth weight, dental caries in children, maternal vitamin D concentrations at term, and parathyroid hormone concentrations in patients with chronic kidney disease requiring dialysis is probable, but further studies and better designed trials are needed to draw firmer conclusions. In contrast to previous reports, evidence does not support the argument that vitamin D only supplementation increases bone mineral density or reduces the risk of fractures or falls in older people. Conclusions Despite a few hundred systematic reviews and meta-analyses, highly convincing evidence of a clear role of vitamin D does not exist for any outcome, but associations with a selection of outcomes are probable. Fig 4 Forest plot of all meta-analyses of randomised controlled trials with relative risk as type of metric by compound administered. CKD=chronic kidney disease patients; NRD=not requiring dialysis; RD=requiring dialysis; UV=ultraviolet Evropi Theodoratou et al. BMJ 2014;348:bmj.g2035
. Results 107 systematic literature reviews and 74 meta-analyses of observational studies of plasma vitamin D concentrations and 87 meta-analyses of randomised controlled trials of vitamin D supplementation were identified. The relation between vitamin D and 137 outcomes has been explored, covering a wide range of skeletal, malignant, cardiovascular, autoimmune, infectious, metabolic, and other diseases. Ten outcomes were examined by both meta-analyses of observational studies and meta-analyses of randomised controlled trials, but the direction of the effect and level of statistical significance was concordant only for birth weight (maternal vitamin D status or supplementation). On the basis of the available evidence, an association between vitamin D concentrations and birth weight, dental caries in children, maternal vitamin D concentrations at term, and parathyroid hormone concentrations in patients with chronic kidney disease requiring dialysis is probable, but further studies and better designed trials are needed to draw firmer conclusions. In contrast to previous reports, evidence does not support the argument that vitamin D only supplementation increases bone mineral density or reduces the risk of fractures or falls in older people. Conclusions Despite a few hundred systematic reviews and meta-analyses, highly convincing evidence of a clear role of vitamin D does not exist for any outcome, but associations with a selection of outcomes are probable. Fig 4 Forest plot of all meta-analyses of randomised controlled trials with relative risk as type of metric by compound administered. CKD=chronic kidney disease patients; NRD=not requiring dialysis; RD=requiring dialysis; UV=ultraviolet. Evropi Theodoratou et al. BMJ 2014;348:bmj.g2035.")
41
25 OH D ve mortalite: metaanaliz çalışması
Conclusions Evidence from observational studies indicates inverse associations of circulating 25-hydroxyvitamin D with risks of death due to cardiovascular disease, cancer, and other causes. Supplementation with vitamin D3 significantly reduces overall mortality among older adults; however, before any widespread supplementation, further investigations will be required to establish the optimal dose and duration and whether vitamin D3 and D2 have different effects on mortality risk. Fig 1 Association of circulating 25-hydroxyvitamin D concentrations with cause specific mortality in observational cohort studies. *Pooled estimates are based on random effects meta-analysis. Using fixed effects models, for primary prevention cohorts, secondary prevention cohorts, and all cohorts, the estimates were 1.40 (1.32 to 1.47), 1.50 (1.35 to 1.66), and 1.42 (1.35 to 1.49) for cardiovascular deaths; 1.10 (1.02 to 1.17), 1.45 (1.28 to 1.65), and 1.16 (1.10 to 1.24) for cancer deaths; 1.28 (1.12 to 1.47), 1.38 (1.09 to 1.75), and 1.30 (1.16 to 1.47) for non-vascular, non-cancer deaths; and 1.45 (1.41 to 1.49), 1.49 (1.42 to 1.56), and 1.44 (1.40 to 1.47) for all cause deaths. Size of data marker is proportional to inverse of variance of relative risk; horizontal line represents 95% CI. Corresponding forest plots and I2 (95% CI) estimates are provided in supplementary material Rajiv Chowdhury et al. BMJ 2014
, 1.50 (1.35 to 1.66), and 1.42 (1.35 to 1.49) for cardiovascular deaths; 1.10 (1.02 to 1.17), 1.45 (1.28 to 1.65), and 1.16 (1.10 to 1.24) for cancer deaths; 1.28 (1.12 to 1.47), 1.38 (1.09 to 1.75), and 1.30 (1.16 to 1.47) for non-vascular, non-cancer deaths; and 1.45 (1.41 to 1.49), 1.49 (1.42 to 1.56), and 1.44 (1.40 to 1.47) for all cause deaths. Size of data marker is proportional to inverse of variance of relative risk; horizontal line represents 95% CI. Corresponding forest plots and I2 (95% CI) estimates are provided in supplementary material. Rajiv Chowdhury et al. BMJ")
42
Çalışma Ülke Grup Doz Amaç Bitiş yılı DIVINE ABD 120 HD hastası (vitamin D <32 ng/ml) IU D2 haftalık veya IU D2 aylık veya plasebo Vitamin D2 >32 ng/ml, cathelicidin ve sitokinler 2013 VITAL yetişkin (erkek >50 ve kadın>55 yaş 2000 IU D2 veya plasebo Kardiovascular hastalık ve kanser 2016 DOHealth 8 Avrupa ülkesi 2150 yetişkin (>70 yaş) Kemik krığı, enfeksiyon, kan basıncı, alt ekstremite fonksiyonu, bilinç 2017 VIDA Yeni Zellenda yetişkin (>50 yaş) D3 bir kez(ve her haziran) ve D3 aylık veya plasebo Kardiovascküler hastalık KOAH da respiratuar hastalık, kemik kırığı FIND Finlandiya yetişkin (erkek >60 ve kadın >65 yaş) 3200 D3 günlük, 1600 D3 günlük veya plasebo Kardiovasküler hastalık, kanser ve DM 2019 VIDAL İngiltere yetişkin (65–85 yaş) IU D3 aylık, veya plasebo Mortalite, morbidite ve vitamin D düzeyleri 2020
 Kemik krığı, enfeksiyon, kan basıncı, alt ekstremite fonksiyonu, bilinç VIDA. Yeni Zellenda yetişkin (>50 yaş) D3 bir kez(ve her haziran) ve D3 aylık veya plasebo. Kardiovascküler hastalık KOAH da respiratuar hastalık, kemik kırığı. FIND. Finlandiya yetişkin (erkek >60 ve kadın >65 yaş) 3200 D3 günlük, 1600 D3 günlük veya plasebo. Kardiovasküler hastalık, kanser ve DM VIDAL. İngiltere yetişkin (65–85 yaş) IU D3 aylık, veya plasebo. Mortalite, morbidite ve vitamin D düzeyleri")
43
Replasman ile Beklenen Sonuç
Proliferasyonunda, Kalsifikasyonda, Arteriyel kalınlaşma Arteriyel sertlikte azalma Gen ve protein ekspresyonunda değişme Glomerüler hücre büyümesi, diferansiasyon, Fibrozis, Proteinüride azalma Antiinflamasyon Antiaterojenik antitrombozis Sol ventrikül hipertrofisinde gerileme RAS baskılanması Klasik olmayan VDRA etkisi Kardiyovasküler mortalitede azalma Veriler henüz yeterli değil

44
Vitamin D ve U –Shape etki
Literature data suggest that a biphasic dose-response curve exists between vitamin D and vascular calcification, with adverse effects associated with very high and very low vitamin D levels. Negative effects associated with vitamin D excess include hyperphosphataemia, hypercalcaemia, increased matrix metalloproteinase (MMP) levels, medial calcification, arterial stiffness and left ventricular hypertrophy. Increased levels of proinflammatory cytokines, increased MMP levels and a decrease in factors protective of endothelial cells are all associated with vitamin D deficiency. Reproduced with permission from Zittermann et al. [26], with slight modifications. Drüeke T B , Massy Z A Nephrol. Dial. Transplant.
 levels, medial calcification, arterial stiffness and left ventricular hypertrophy. Increased levels of proinflammatory cytokines, increased MMP levels and a decrease in factors protective of endothelial cells are all associated with vitamin D deficiency. Reproduced with permission from Zittermann et al. [26], with slight modifications. Drüeke T B , Massy Z A Nephrol. Dial. Transplant.")
45
Vitamin D ve J curve mortalite ilişkisi
This 2012 study analyzed blood serum from 247,574 Danish subjects and found a reverse J-curve for mortality. Durup D, Jørgensen HL, Christensen J, Schwarz P, Heegaard AM, Lind B A RJ Clin Endocrinol Metab. 2012;97: Context: Optimal levels of vitamin D have been a topic of heavy debate, and the correlation between 25-hydroxyvitamin D [25(OH)D] levels and mortality still remains to be established. Objective: The aim of the study was to determine the association between all-cause mortality and serum levels of 25(OH)D, calcium, and PTH. Design and Setting: We conducted a retrospective, observational cohort study, the CopD Study, in a single laboratory center in Copenhagen, Denmark. Participants: Serum 25(OH)D was analyzed from 247,574 subjects from the Copenhagen general practice sector. In addition, serum levels of calcium, albumin-adjusted calcium, PTH, and creatinine were measured in 111,536; 20,512; 34,996; and 189,496 of the subjects, respectively. Main Outcome Measures: Multivariate Cox regression analysis was used to compute hazard ratios for all-cause mortality. Results: During follow-up (median, 3.07 yr), 15,198 (6.1%) subjects died. A reverse J-shaped association between serum level of 25(OH)D and mortality was observed. A serum 25(OH)D level of 50–60 nmol/liter was associated with the lowest mortality risk. Compared to 50 nmol/liter, the hazard ratios (95% confidence intervals) of all-cause mortality everse J-Shaped Association of All-Cause Mortality with Serum 25-Hydroxyvitamin D in General Practice: The CopD Study. at very low (10 nmol/liter) and high (140 nmol/liter) serum levels of 25(OH)D were 2.13 (2.02–2.24) and 1.42 (1.31–1.53), respectively. Similarly, both high and low levels of albumin-adjusted serum calcium and serum PTH were associated with an increased mortality, and secondary hyperparathyroidism was associated with higher mortality (P ). Conclusion: In this study from the general practice sector, a reverse J-shaped relation between the serum level of 25(OH)D and all-cause mortality was observed, indicating not only a lower limit but also an upper limit. The lowest mortality risk was at 50–60 nmol/liter. The study did not allow inference of causality, and further studies are needed to elucidate a possible causal relationship between 25(OH)D leve Durup ve ark. J Clin Endocrinol Metab. 2012
D] levels and mortality still remains to be established. Objective: The aim of the study was to determine the association between all-cause mortality and. serum levels of 25(OH)D, calcium, and PTH. Design and Setting: We conducted a retrospective, observational cohort study, the CopD Study, in. a single laboratory center in Copenhagen, Denmark. Participants: Serum 25(OH)D was analyzed from 247,574 subjects from the Copenhagen general. practice sector. In addition, serum levels of calcium, albumin-adjusted calcium, PTH, and creatinine. were measured in 111,536; 20,512; 34,996; and 189,496 of the subjects, respectively. Main Outcome Measures: Multivariate Cox regression analysis was used to compute hazard ratios. for all-cause mortality. Results: During follow-up (median, 3.07 yr), 15,198 (6.1%) subjects died. A reverse J-shaped association. between serum level of 25(OH)D and mortality was observed. A serum 25(OH)D level of. 50–60 nmol/liter was associated with the lowest mortality risk. Compared to 50 nmol/liter, the. hazard ratios (95% confidence intervals) of all-cause mortality everse J-Shaped Association of All-Cause Mortality with Serum 25-Hydroxyvitamin D in General Practice: The CopD Study. at very low (10 nmol/liter) and high. (140 nmol/liter) serum levels of 25(OH)D were 2.13 (2.02–2.24) and 1.42 (1.31–1.53), respectively. Similarly, both high and low levels of albumin-adjusted serum calcium and serum PTH were associated. with an increased mortality, and secondary hyperparathyroidism was associated with higher. mortality (P ). Conclusion: In this study from the general practice sector, a reverse J-shaped relation between the. serum level of 25(OH)D and all-cause mortality was observed, indicating not only a lower limit but. also an upper limit. The lowest mortality risk was at 50–60 nmol/liter. The study did not allow. inference of causality, and further studies are needed to elucidate a possible causal relationship. between 25(OH)D leve. Durup ve ark. J Clin Endocrinol Metab")
46
D Vitamini Preparatları
Oral damla 15 ml = IU 10 damla = 1000 IU Bir kutu fiyatı = 4.53 TL D Vitamini kapsülü 1000, 1200, 2000 4000 IU Ülkemizde 1000 IU fiyatları = TL Kalsitriol 0.25 ve 0.5 mcg 0.25 mcg 30 kapsül = TL 100 kapsül =70.97 TL 0.5 mcg 30 kapsül = Tl 100 kapsül = TL Ampul 1 ml = IU Bir kutu fiyatı = 1.93 TL Eksiklik tedavisinde önerilmez

Benzer bir sunumlar