Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Renal Yetmezlik ve Renal Replasman Tedavisi
Prof Dr Serhan Tuğlular Marmara Üniversitesi Tıp Fakültesi Nefroloji BD

2
YBÜ’de Renal Yetmezlik
Akut böbrek Hasarı (AKI) Kronik Böbrek Hastalığı zemininde AKI Kronik Böbrek hastalığı/ yetmezliği
 Kronik Böbrek Hastalığı zemininde AKI. Kronik Böbrek hastalığı/ yetmezliği.")
3
GFR Düşmeden BUN ve Kreatinin Yükselme Nedenleri
Üre sentezinde GİS kanama Kortikosteroidler Tetrasiklin Protein alımında artış Amino asit uygulanması Katabolizmada artış ve ateşli hastalık Kreatinin yapımında Rabdomiyoliz Tubuler Kr sekresyonunda Cimetidine Trimethoprim

4
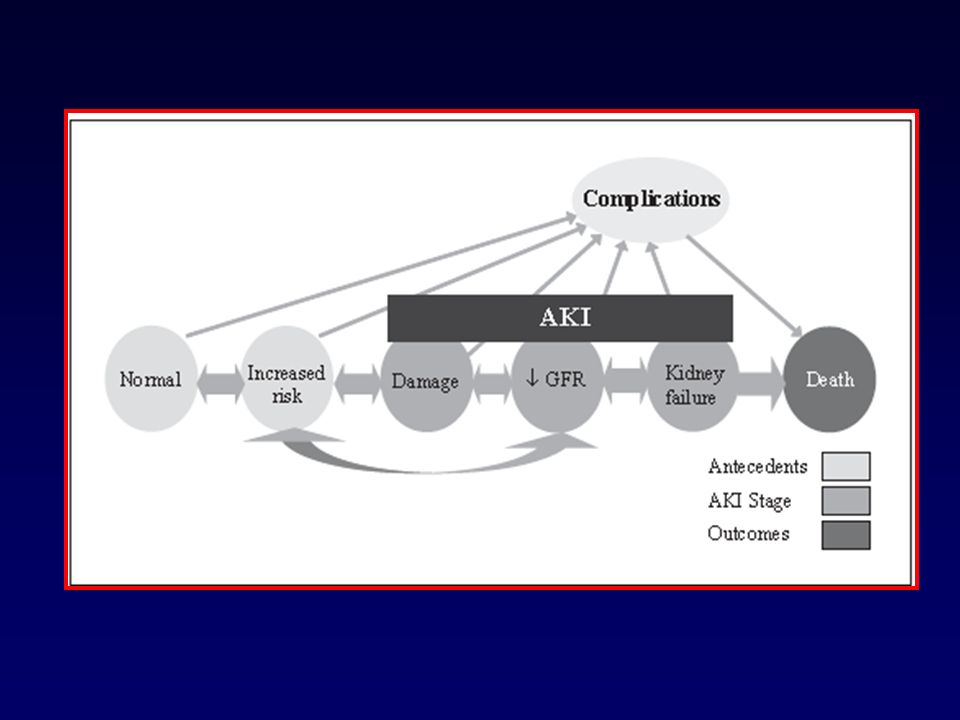
ABY AKI Artan Böbrek Hasarı (Acute Kidney Injury) (Akut Böbrek Hasarı)
It now appears that kidney dysfunction is often under-recognized, although its severity is clearly associated with outcome. AKI is now considered the correct nomenclature for the clinical disorder formerly termed ‘acute renal failure’ (ARF). This new taxonomy underscores the fact that AKI exists along a continuum, recognizing that the greater the severity of injury, the more likely it is that the overall outcome will be unfavourable. AKI is not acute tubular necrosis and it is not ARF. Rather, it includes both as well as other, less severe conditions that are not necessarily ‘structural damage’ but also include ‘dysfunction’ (slight, apparently innocuous increases in serum creatinine; decreases in urine output due to volume depletion, generally defining prerenal ARF, with the implied and flawed meaning of a benign and reversible form of renal dysfunction). Instead of focusing exclusively on patients with severe and established renal failure, those who are receiving dialysis and those who have a specific clinical syndrome, the robust association of all AKI classes with hospital mortality behoves us to raise the profile of this disorder as a matter of urgency [2].
. This new taxonomy underscores the fact that AKI exists along a continuum, recognizing that the greater the severity of injury, the more likely it is that the overall outcome will be unfavourable. AKI is not acute tubular necrosis and it is not ARF. Rather, it includes both as well as other, less severe conditions that are not necessarily ‘structural damage’ but also include ‘dysfunction’ (slight, apparently innocuous increases in serum creatinine; decreases in urine output due to volume depletion, generally defining prerenal ARF, with the implied and flawed meaning of a benign and reversible form of renal dysfunction). Instead of focusing exclusively on patients with severe and established renal failure, those who are receiving dialysis and those who have a specific clinical syndrome, the robust association of all AKI classes with hospital mortality behoves us to raise the profile of this disorder as a matter of urgency [2].")
6
AKI: Tanımı Renal işlevde ani (48 saat içinde) bozulma
AKIN redefined AKI as ‘An abrupt (within 48 hours) reduction in kidney function currently defined as an absolute increase in serum creatinine of more than or equal to 0.3 mg/dl, a percentage increase in serum creatinine of more than or equal to 50% (1.5-fold from baseline), or a reduction in urine output (documented oliguria of less than 0.5 ml/kg per hour for more than six hours).’ Several specifications were provided by the workgroup to this updated definition and were followed by a new staged classification of AKI severity Serum BUN ve Kreatinin > 0.3mg/dl ve/veya %50 (1.5 x Bazal) İdrar çıkışında azalma <0.5ml/kg/saat > 6 saat
 reduction in kidney function currently defined as an. absolute increase in serum creatinine of more than or equal to 0.3 mg/dl, a percentage increase in serum creatinine of more. than or equal to 50% (1.5-fold from baseline), or a reduction in urine output (documented oliguria of less than 0.5 ml/kg. per hour for more than six hours).’ Several specifications were provided by the workgroup to this updated definition and. were followed by a new staged classification of AKI severity. Serum BUN ve Kreatinin > 0.3mg/dl ve/veya %50 (1.5 x Bazal) İdrar çıkışında azalma <0.5ml/kg/saat > 6 saat.")
7
AKI Klasifikasyon/Evreleme sistemi
Sınıf/Evre Kr Kriteri İdrar kriteri RIFLE Risk Injury Failure x 1.5 /GFR↓>%25 x 2 / GFR↓>%50 x 3 / GFR↓>%75; Kr>4mg/dl + en az akut 0.5mg/dl↑ <0.5ml/kg/saat -6saat <0.5ml/kg/saat -12 saat Anuri- 12 saat AKIN Evre 1 Evre 2 Evre 3 >0.3 mg/dl veya Bazal x 1.5-2 Bazal x 2-3 Bazal x > 3 veya Kr>4mg/dl + en az akut 0.5mg/dl↑ RRT gereksinimi <0.3 ml/kg/saat -24 saat veya anuri-12 saat

8
AKI (+) AKI (-) 45.8 %16.4 Mortalite (%) RIFLE Çalışmasının
Meta analizi Kidney Int 2008, 73:- The goal of adopting these sets of explicit diagnostic criteria is to increase clinical awareness and diagnosis of AKI. Both RIFLE and AKIN criteria may cause an increase in false positives, such that some patients regarded as having AKI will not have the condition. Nonetheless, the decision to adopt less inclusive criteria should raise the index of suspicion for AKI, allow its earlier identification during the course of critical illness, and enhance opportunities to prevent or manage kidney damage. Risk for death among patients with AKI. The data were obtained in a recent review of 13 studies that used RIFLE criteria where patient level data on mortality were available for Risk, Injury and Failure patients, as well as those without AKI [3]. The review was conducted to establish a pooled estimate of risk ratio (RR) for mortality for patients of Risk, Injury or Failure classes compared with non-AKI patients. More than 71,000 patients were included in the analysis of published reports. With respect to non-AKI patients, there appeared to be a step-wise increase in RR for death going from Risk class (RR = 2.40) to Injury class (RR = 4.15) and to Failure class (RR = 6.37; P < for all). AKI, acute kidney injury; RIFLE, Risk, Injury, Failure, Loss and Endstage kidney disease. Mortalite (%) AKI (+) AKI (-) 45.8 %16.4 N=120 AKIN Kriterleri Crit Care Med 2008, 36:
 for mortality for patients of Risk, Injury or Failure classes compared with non-AKI patients. More than 71,000 patients were included in the analysis of published reports. With respect to non-AKI patients, there appeared to be a step-wise increase in RR for death going from Risk class (RR = 2.40) to Injury class (RR = 4.15) and to Failure class (RR = 6.37; P < for all). AKI, acute kidney injury; RIFLE, Risk, Injury, Failure, Loss and Endstage kidney disease. Mortalite (%) AKI (+) AKI (-) %16.4. N=120. AKIN. Kriterleri. Crit Care Med 2008, 36:")
9
AKI Bio-belirteçleri var mı?
Sitokinler Platelet aktive edici faktör IL-18 Diğerleri Kidney injury molekül-1 Na/H exchanger isoform-3 Genler Nötrofil gelatinaz associated lipocalin (NGAL) Düşük molekül ağırlıklı proteinler B2-mikroglobulin A1-mikroglobulin Adenozin deaminaz bağlayıcı protein Sistatin-C Renal tubuler epitelyal antijen Enzimler N-asetil-b-glukosaminidaz Alanine aminopeptidaz Alkalen fosfataz Laktat dehidrogenaz g/n glutatyon –S-transferaz G-glutamil transpeptidaz Bazıları ümit vaat ediyor Ancak genel kullanımları için kanıtlar henüz yetersiz (β2-microglobulin, α1-microglobulin, adenosine deaminase binding protein, retinol binding protein, cystatin C and renal tubular epithelial antigen-1), enzymes (N-acetyl-β-glucosaminidase, alanine aminopeptidase, alkaline phosphatase, lactate dehydrogenase, α/π-glutathione-S-transferase, and γ-glutamyl transpeptidase), cytokines (platelet-activating factor and IL-18)and other biomarkers (kidney injury molecule-1 and Na/H exchanger isoform-3). Increased levels of platelet-activating factor, IL-18 and Na/H exchanger isoform-3 were detected early in septic AKI and predicted kidney failure. Several additional biomarkers were evident early in AKI, but their diagnostic value in sepsis remains unknown. In one study, IL-18 excretion was greater in septic than in nonseptic AKI. IL-18 also predicted deterioration in kidney function, with increased values preceding clinically significant kidney failure by 24 to 48 hours. Detection of cystatin C, α1-microglobulin and IL-18 predicted need for renal replacement therapy (RRT). The authors concluded that that selected biomarkers may be promising in early detection of AKI in sepsis and may have value for predicting subsequent deterioration in kidney function. scientific basis for use of urinary biochemistry, indices and microscopy in patients with septic AKI is weak. More research is required to describe the accuracy, pattern and time course of these parameters in patients with septic AKI.
 Düşük molekül ağırlıklı proteinler. B2-mikroglobulin. A1-mikroglobulin. Adenozin deaminaz bağlayıcı protein. Sistatin-C. Renal tubuler epitelyal antijen. Enzimler. N-asetil-b-glukosaminidaz. Alanine aminopeptidaz. Alkalen fosfataz. Laktat dehidrogenaz. g/n glutatyon –S-transferaz. G-glutamil transpeptidaz. Bazıları ümit vaat. ediyor. Ancak genel. kullanımları. için kanıtlar. henüz yetersiz. (β2-microglobulin, α1-microglobulin, adenosine deaminase binding protein, retinol binding protein, cystatin C and renal tubular epithelial antigen-1), enzymes (N-acetyl-β-glucosaminidase, alanine. aminopeptidase, alkaline phosphatase, lactate dehydrogenase, α/π-glutathione-S-transferase, and γ-glutamyl transpeptidase), cytokines (platelet-activating factor and IL-18)and other biomarkers (kidney injury molecule-1 and Na/H exchanger isoform-3). Increased levels of platelet-activating factor, IL-18 and Na/H exchanger isoform-3 were detected early in septic AKI and predicted kidney failure. Several additional biomarkers were evident early in AKI, but their diagnostic value in sepsis remains unknown. In one study, IL-18 excretion was greater in septic than in nonseptic AKI. IL-18 also predicted deterioration in kidney function, with increased values preceding clinically significant kidney failure by 24 to 48 hours. Detection of cystatin C, α1-microglobulin. and IL-18 predicted need for renal replacement therapy (RRT). The authors concluded that that selected biomarkers may be promising in early detection of AKI in sepsis and may have value for predicting subsequent deterioration in kidney function. scientific basis for use of urinary biochemistry, indices and microscopy in patients with septic AKI is weak. More research is required to describe the accuracy, pattern and time course of these parameters in patients with septic AKI.")
10
Pre- renal Intra-renal Post- renal

11
(%17) (%72) N=253 Kidney Int 1998;53: S16-S24
 (%72) N=253 Kidney Int 1998;53: S16-S24")
12
YBÜ’de en sık AKI nedeni : ATN
İSKEMİK ABY ESV kaybı Postoperatif Ağır Kalp Yetersizliği Sepsis Pankreatit Travma Yanıklar NEFROTOKSİSİTE VE İLACA İKİNCİL ABY Myoglobinürik Radyokontrast İlaçlar ATN

13
RADYOKONTRAST NEFROPATİSİ
RİSK FAKTÖRLERİ Önceden varolan BY Diyabetik nefropati >2ml/kg kontrast dozu Volüm eksikliği Yaş>60 Hiperürisemi Karaciğer yetersizliği ÖNLEMLER Öncesinde Kr kontrolü Non-Nefrotoksik ajan tercihi Kontrast dozu Hidrasyon - Altın standart Teofilin Ca-kanal blokerleri Asetilsistein Alkalinizasyon

14
İLACA İKİNCİL ABY Akut Tubuler Hasar Otoregülasyon bozukluğu
Aminoglikozidler Bazı sefalosporinler Amfoterisin B Vancomycin Otoregülasyon bozukluğu ACE inhibitörleri AII reseptör blokerleri NSAID Radyokontrast ajanlar Akut Interstisyel nefrit Tüm ilaçlar

15
‘Kronik’ zeminde ‘Akut’ Olgusu
KBY zemininde araya giren ek bir sorun nedeniyle renal işlevde Akut kötüleşme Hipovolemi Nefrotoksik ilaç kullanımı Infeksiyon Obstrüksiyon Kalp yetersizliği Akselere hipertansiyon

17
Renal İşlev Nasıl Değerlendirilmeli ?
Kreatinin klirensi 24 saatlik idrar toplanarak Cockroft ve Gault formülüne göre: (140-yaş) x Ağırlık 72 X PCr (mg/dl) (Erkek) Kadın: x 0.8
 x Ağırlık. 72 X PCr (mg/dl) (Erkek) Kadın: x 0.8.")
18
İlaç Dozunun Ayarlanması
İdrar çıkışı <400ml/gün ise, serum kreatinin değeri ne olursa olsun, klirens <10ml/dk >60 yaşta klirens 10-50ml/dk OLARAK KABUL EDİLMELİDİR Oral alımda biyoyararlanım düşer i.v. yol tercih edilmeli Proteine bağlanma oranı azalır İlaç toksisite riski artar Dağılım hacmi etkilenir Metabolizması etkilenir Atılımı etkilenir. Böbrek yetersizliğinde ilaç kullanım rehberlerinden yararlanılmalıdır YÜKLEME DOZU DEĞİŞMEZ İDAME DOZU: DOZ AZALTILABİLİR DOZ ARASI UZATILABİLİR

19
YBÜ’DE AKI’YE KONSERVATİF YAKLAŞIM : ÖNLENMESİ
HİPOVOLEMİDEN KAÇINILMASI RADYOKONTRASTTAN KAÇINILMASI VE/VEYA PROFİLAKTİK ÖNLEMLER İLAÇ UYGULAMALARINDA DOZLARA VE NEFROTOKSİK AJANLARA DİKKAT HEMODİNAMİK DESTEK

20
Intensive Care Med 2008

21
YBÜ’DE ABY’NE KONSERVATİF YAKLAŞIM-BESLENME
KALORİ VE BESİN GEREKSİNİMİ DİĞER YBÜ HASTALARINDAN FARKLI DEĞİL 35 KCAL/kg/GÜN g/kg/gün protein G:L=70/30 RRT SIRASINDA EK OLARAK 0.2g/kg/gün PROTEİN ALMALILAR ENTERAL YOL TERCİH EDİLMELİ ESANSİYEL-NONESANSİYEL AA AYRIMI GEREKLİ DEĞİL VOLÜM KISITLAMASI ÖNEMLİ Patients with AKI often have PEW (preexisting and/or hospital acquired), which represents a major negative prognostic factor. Nutritional support is frequently required in the form of parenteral and/or enteral nutrition, even though no formal demonstration exists concerning its positive effect on major outcomes. The primary goals of nutritional support in AKI are basically the same as those suggested for critically ill patients having normal renal function. Patients with AKI on RRT should receive at least 1.5 g/kg per day of proteins, and not more than 30 kcal nonprotein calories or 1.3BEE calculated by the Harris–Benedict equation, with lipid supply representing about 30–35% of energy. To compensate for amino acid losses during RRT, protein supply should be increased by some 0.2 g/kg per day. Even in patients with AKI, the enteral route should represent the preferred route for nutrient delivery; however, parenteral nutrition is often required to fulfill nutritional requirements. A close integration between nutritional support and RRT is needed in AKI, with the aim of carefully tailoring both therapies on patients’ changing needs. RRT BESLENMENİN DAHA SERBEST OLMASINI SAĞLAR
, which represents a major negative prognostic factor. Nutritional support is frequently required in the form of parenteral and/or enteral nutrition, even though no formal demonstration exists concerning its positive effect on major outcomes. The primary goals of nutritional support in AKI are basically. the same as those suggested for critically ill patients having normal renal function. Patients with AKI on RRT should receive at least 1.5 g/kg per day of proteins, and not more than 30 kcal nonprotein calories or 1.3BEE calculated by the Harris–Benedict equation, with lipid supply representing about 30–35% of energy. To compensate for amino acid losses during RRT, protein supply should be increased by some 0.2 g/kg per day. Even in patients with AKI, the enteral route should represent the preferred route for nutrient delivery; however, parenteral nutrition is often required to fulfill nutritional requirements. A close integration between nutritional support and RRT is needed in AKI, with the aim of carefully tailoring both therapies on patients’ changing needs. RRT BESLENMENİN DAHA. SERBEST OLMASINI SAĞLAR.")
22
Düşük Doz Dopamin ve Furosemide: ASILSIZ EFSANE
Crit Care Med 1981; 9: ; Parker ve ark. Crit Care Med 1982;10: Davis ve ark Intensive Care Med 1996;22: ; Lerm T ve ark Anesth Analg 1998; 86: 3-8 ; Lema G ve ark (+) Kidney Int 1996; 50: 4-14; Denton ve ark. N Engl J Med 1996;334: ; Thadhani ve ark Kidney Int 1998; 54: ; Star RA J Am Soc Nephrol 2000; 11:97-104,Lassnigg ve ark. Lancet December 23/30, 2000; 356: ;ANZIC CTG JAMA November 27, 2002; 288: ;Mehta ve ark. JAMA November 27,2002; 288: ;Lameire ve ark.. (-)
 Kidney Int 1996; 50: 4-14; Denton ve ark. N Engl J Med 1996;334: ; Thadhani ve ark. Kidney Int 1998; 54: ; Star RA. J Am Soc Nephrol 2000; 11:97-104,Lassnigg ve ark. Lancet December 23/30, 2000; 356: ;ANZIC CTG. JAMA November 27, 2002; 288: ;Mehta ve ark. JAMA November 27,2002; 288: ;Lameire ve ark.. (-)")
23
Lack of Renoprotective Effects of Dopamine and Furosemide
During Cardiac Surgery Lassnigg ve ark. J Am Soc Nephrol 11:97-104, 2000

24
YBÜ’DE AKI DAHA ÇOK MOYS’NUN PARÇASIDIR
Kidney Int 1998;53: S16-S24

25
Critical Care 2008, 12:R144

26
AKI+OSY SAYISI ARTTIKÇA MORTALİTE DE ARTMAKTADIR
Kidney Int 1998;53: S16-S24

27
N=2619 İspanyol çalışması

28
Ciddi AKI %6.3 %83.7 %47.3 %63.9 Cerrahi nedenli olamayan N=17 326
Sepsis This study pools data from the UK Intensive Care National Audit and Research Center (ICNARC) Case Mix Programme (CMP) to evaluate the case mix, outcome and activity for 17,326 patients with severe acute kidney injury (AKI) occurring during the first 24 hours of admission to intensive care units (ICU). Results Severe AKI occurred in 17,326 out of 276,731 admissions (6.3%). The source of admission was nonsurgical in 83.7%. Sepsis was present in 47.3% and AKI was nonoliguric in 63.9% of cases. Admission to ICU with severe AKI accounted for 9.3% of all ICU bed-days. Oliguric AKI was associated with longer length of stay for survivors and shorter length of stay for nonsurvivors compared with nonoliguric AKI. Oliguric AKI was associated with significantly greater ICU and hospital mortality (55.8% and 77.3%, respectively) compared with nonoliguric AKI (33.4% and 49.3%, respectively). Surgery during the 1week before admission or during the first week in the CMP unit was associated with decreased odds of mortality. UK APACHE II and the Mehta scores under-predicted the number of deaths,whereas SHARF T0 and SHARF II0 over-predicted the number of deaths. %63.9 Non-oligurik YBU Yatak günlerinin %9.3’ü ciddi AKI Critical Care 2008, 12:S2
 Case Mix Programme (CMP) to evaluate the case mix, outcome and. activity for 17,326 patients with severe acute kidney injury (AKI) occurring during the first 24 hours of admission to intensive care units (ICU). Results Severe AKI occurred in 17,326 out of 276,731 admissions (6.3%). The source of admission was nonsurgical in 83.7%. Sepsis was present in 47.3% and AKI was nonoliguric in 63.9% of cases. Admission to ICU with severe AKI accounted for 9.3% of all ICU bed-days. Oliguric AKI was associated with longer length of stay for survivors and shorter length of stay for nonsurvivors compared with nonoliguric AKI. Oliguric AKI was associated with significantly greater ICU and hospital mortality (55.8% and 77.3%, respectively) compared with nonoliguric AKI (33.4% and 49.3%, respectively). Surgery during the 1week before admission or during the first week in the CMP unit. was associated with decreased odds of mortality. UK APACHE II and the Mehta scores under-predicted the number of deaths,whereas SHARF T0 and SHARF II0 over-predicted the number of deaths. %63.9. Non-oligurik. YBU Yatak günlerinin %9.3’ü ciddi AKI. Critical Care 2008, 12:S2.")
29
Skorlama sistemleri mükemmel değil, ölüm öngörüsü ↓ veya ↑ çıkıyor
AKI Oligurik Non-oligurik YBÜ mortalitesi (%) 55.8 33.4 Hastane (%) 77.3 49.3 N=17 326 Oliguric AKI was associated with longer length of stay for survivors and shorter length of stay for nonsurvivors compared with nonoliguric AKI. Oliguric AKI was associated with significantly greater ICU and hospital mortality (55.8% and 77.3%, respectively) compared with nonoliguric AKI (33.4% and 49.3%, respectively). Surgery during the 1week before admission or during the first week in the CMP unit was associated with decreased odds of mortality. UK APACHE II and the Mehta scores under-predicted the number of deaths,whereas SHARF T0 and SHARF II0 over-predicted the number of deaths. Skorlama sistemleri mükemmel değil, ölüm öngörüsü ↓ veya ↑ çıkıyor Critical Care 2008, 12:S2
 Hastane (%) N= Oliguric AKI was associated with longer length of stay for survivors and shorter length of stay for nonsurvivors compared with nonoliguric AKI. Oliguric AKI was associated with significantly greater ICU and hospital mortality (55.8% and 77.3%, respectively) compared with nonoliguric AKI (33.4% and 49.3%, respectively). Surgery during the 1week before admission or during the first week in the CMP unit was associated with decreased odds of mortality. UK APACHE II and the Mehta scores under-predicted the number of deaths,whereas SHARF T0 and SHARF II0 over-predicted the number of deaths. Skorlama sistemleri mükemmel değil, ölüm öngörüsü ↓ veya ↑ çıkıyor. Critical Care 2008, 12:S2.")
30
HATIRLAMAYA DEĞER GERÇEKLER
YBÜ’DE ABY: HATIRLAMAYA DEĞER GERÇEKLER ABY hastalarının başka organ sistemleri de hastadır ABY’de RRT önemli ancak yaşam kurtarma açısından yetersizdir Amacımız, böbrek yetersizliğine bağlı, komplikasyonları, ölümü ve tedaviye bağlı ölümleri önlemektir

31
Ne zaman diyaliz? Oligüri-anüri
Kr progresif yükselme 4-5mg/dl’ye ulaştığında BUN değerleri >100 mg/dl Asidoz Hiperkalemi Hipervolemi

32
YBÜ’DE RENAL REPLASMAN TEDAVİSİ
IHD- Intermittan Hemodiyaliz Günaşırı Hergün CRRT-Sürekli Renal Replasman Tedavisi CVVHDF CVVHF SLED- Sustained Low Efficiency Dialysis These novel techniques of renal substitution therapy have permitted a conceptual shift from renal ‘‘replacement’’ to renal ‘‘support’’ therapies (4), whereby the strategies to treat AKI have become an integral part of overall critically ill patient management, with ‘‘renal’’ and ‘‘nonrenal’’ applications such as sepsis and acute respiratory distress syndrome (ARDS).
, whereby the strategies to treat AKI have. become an integral part of overall critically ill patient. management, with ‘‘renal’’ and ‘‘nonrenal’’ applications. such as sepsis and acute respiratory distress syndrome. (ARDS).")
34
ABY’de RRT Diyalizin zamanlaması ve dozu Diyalizör biyo-uyumluluğu
Diyalizör performansı Diyaliz tipi (CRRT vs IHD vs SLED vs PD)
")
35
Fig. 1. Modalities of continuous renal replacement therapies (CRRT)
Fig. 1. Modalities of continuous renal replacement therapies (CRRT). Techniques available today for renal replacement in the intensive care unit. CAVH, continuous arterio–venous hemofiltration; CHP, continuous hemoperfusion; CPFA, plasmafiltration coupled with adsorption; CPF-PE, continuous plasmafiltration-plasma exchange; CVVH, continuous veno-venous hemofiltration; CVVHD, continuous veno-venous hemodialysis; CVVHDF, continuous veno-venous hemodiafiltration; CVVHDF, continuous high-flux dialysis; D, dialysate;HVVF, high-volume hemofiltration; K, clearance; Pf, plasmafiltrate flow; Qb, blood flow; Qd, dialysate flow; Qf, ultrafiltration rate; R, replacement; SCUF, slow continuous ultrafiltration; SLED, sustained low efficiency daily dialysis; UFC, ultrafiltration control system.
. Techniques available today for renal replacement in the intensive care unit. CAVH, continuous arterio–venous hemofiltration; CHP, continuous hemoperfusion; CPFA, plasmafiltration coupled with adsorption; CPF-PE, continuous plasmafiltration-plasma exchange; CVVH, continuous veno-venous hemofiltration; CVVHD, continuous veno-venous hemodialysis; CVVHDF, continuous veno-venous hemodiafiltration; CVVHDF, continuous high-flux dialysis; D, dialysate;HVVF, high-volume hemofiltration; K, clearance; Pf, plasmafiltrate flow; Qb, blood flow; Qd, dialysate flow; Qf, ultrafiltration rate; R, replacement; SCUF, slow continuous ultrafiltration; SLED, sustained low efficiency daily dialysis; UFC, ultrafiltration control system.")
36
DİYALİZ REÇETELENMESİNİN İNCE AYARI
Vasküler giriş yolu Venöz çift lümenli kateterler Juguler /femoral Membran tipi Geçirgenlik-biyo-uyum Diyalizat elektrolit içeriği Na-K-Ca-HCO3 Diyalizat sıvısının saflığı Diyaliz makinesi monitorizasyonu Antikoagülasyon

37
Since the original formulation of the dose concept for renal replacement therapy more than 30 years ago [1] and the establishment of a link between dose and clinical outcome [2,3], individualized patient dosing based on urea clearance is now routine in end-stage renal disease (ESRD) patients. More recently, similar principles have been applied to critically ill patients with acute kidney injury (AKI) treated both with continuous renal replacement therapy (CRRT) and with intermittent modalities. Using the normalized effluent rate as a dose surrogate in postdilution continuous venovenous hemofiltration, Ronco and colleagues reported higher survival in patients receiving a dose of 35 or 45 ml/hour/kg than in patients receiving a dose of 20 ml/hour/kg [4].
![Since the original formulation of the dose concept for renal replacement therapy more than 30 years ago [1] and the establishment of a link between dose and clinical outcome [2,3], individualized patient dosing based on urea clearance is now routine in end-stage renal disease (ESRD) patients. More recently, similar principles have been applied to critically ill patients with acute kidney injury (AKI) treated both with continuous renal replacement therapy (CRRT) and with intermittent modalities.](http://slideplayer.biz.tr/slide/7855383/24/images/37/Since+the+original+formulation+of+the+dose+concept+for+renal+replacement+therapy+more+than+30+years+ago+%5B1%5D+and+the+establishment+of+a+link+between+dose+and+clinical+outcome+%5B2%2C3%5D%2C+individualized+patient+dosing+based+on+urea+clearance+is+now+routine+in+end-stage+renal+disease+%28ESRD%29+patients.+More+recently%2C+similar+principles+have+been+applied+to+critically+ill+patients+with+acute+kidney+injury+%28AKI%29+treated+both+with+continuous+renal+replacement+therapy+%28CRRT%29+and+with+intermittent+modalities..jpg "Using the normalized effluent rate as a dose surrogate in postdilution continuous venovenous hemofiltration, Ronco and colleagues reported higher survival in patients receiving a dose of 35 or 45 ml/hour/kg than in patients receiving a dose of 20 ml/hour/kg [4].")
38
Çok merkezli, randomize kontrollü
CRRT vs IHD Çok merkezli, randomize kontrollü * * n=166 65.5 59.5 56.6 50.6 47.6 41.5 * p<0.02 Mehta ve ark. Kidney Int 2001;60:

39
IHD CRRT p %Male 68.3 83.3 <0.023 %KC yetersiz. 29.3 42.9 <0.05
Randomize olmasına rağmen hasta dağılımı IHD lehine IHD CRRT p %Male 68.3 83.3 <0.023 %KC yetersiz. 29.3 42.9 <0.05 APACHE III 87.7 96.4 <0.045 Mehta ve ark. Kidney Int 2001;60:

40
AKI (+) YBÜ Hastası – en az 1 böbrek dışı organ tutulumu veya sepsis
Primer sonlanım noktası – 60 günde tüm nedenli ölüm We randomly assigned critically ill patients with acute kidney injury and failure of at least one nonrenal organ or sepsis to receive intensive or less intensive renal-replacement therapy. The primary end point was death from any cause by day 60. In both study groups, hemodynamically stable patients underwent intermittent hemodialysis, and hemodynamically unstable patients underwent continuous venovenous hemodiafiltration or sustained low-efficiency dialysis. Patients receiving the intensive treatment strategy underwent intermittent hemodialysis and sustained low-efficiency dialysis six times per week and continuous venovenous hemodiafiltration at 35 ml per kilogram of body weight per hour; for patients receiving the less-intensive treatment strategy, the corresponding treatments were provided thrice weekly and at 20 ml per kilogram per hour. Results Baseline characteristics of the 1124 patients in the two groups were similar. The rate of death from any cause by day 60 was 53.6% with intensive therapy and 51.5% with less-intensive therapy (odds ratio, 1.09; 95% confidence interval, 0.86 to 1.40; P = 0.47). There was no significant difference between the two groups in the duration of renal replacement therapy or the rate of recovery of kidney function or nonrenal organ failure. Hypotension during intermittent dialysis occurred in more patients randomly assigned to receive intensive therapy, although the frequency of hemodialysis sessions complicated by hypotension was similar in the two groups. Conclusions Intensive renal support in critically ill patients with acute kidney injury did not decrease mortality, improve recovery of kidney function, or reduce the rate of nonrenal organ failure as compared with less-intensive therapy involving a defined dose of intermittent hemodialysis three times per week and continuous renal-replacement therapy at 20 ml per kilogram per hour. (ClinicalTrials.gov number, NCT ) Yoğun RRT Az Yoğun RRT Hemodinamik stabil→ IHD Hemodinamik stabil olmayan → CVVHD/SLED
. There was no significant difference between the two groups in the duration of renal replacement therapy or the rate of recovery of kidney function or nonrenal organ failure. Hypotension during intermittent dialysis occurred in more patients randomly assigned to receive intensive therapy, although the frequency of hemodialysis sessions complicated by hypotension was similar in the two groups. Conclusions Intensive renal support in critically ill patients with acute kidney injury did not decrease. mortality, improve recovery of kidney function, or reduce the rate of nonrenal organ failure as compared with less-intensive therapy involving a defined dose of intermittent hemodialysis three times per week and continuous renal-replacement therapy. at 20 ml per kilogram per hour. (ClinicalTrials.gov number, NCT ) Yoğun RRT. Az Yoğun RRT. Hemodinamik stabil→ IHD. Hemodinamik stabil olmayan → CVVHD/SLED.")
41
NEJM 2008 :359; 7-20

43
Ciddi eleştiriler getiriyor.
Critical Care 2008, 12:308

44
CRRT ‘deki membranlar Yüksek geçirgenlikli Biyouyumlu Su
Küçük ve orta moleküler ağırlıklı solutler Biyouyumlu The main feature of convective treatments is the use of high-flux membranes, characterized by high permeability for water as well as low- and middle-molecular weight solutes (in the range of 1000–12,000Daltons) and high ‘‘biocompatibility.’’ It is a widespread opinion that convective treatments like high-flux hemodialysis, hemodiafiltration, and hemofiltration offer a clinical advantage over standard dialysis when considering physiological outcomes. The crucial point is that up until now, studies have not been able to demonstrate superiority of these techniques on morbidity, mortality, and quality of life (6,13–18).
 and. high ‘‘biocompatibility.’’ It is a widespread opinion that convective treatments like high-flux hemodialysis, hemodiafiltration, and hemofiltration offer a clinical advantage over standard dialysis when considering physiological outcomes. The crucial point is that up until now, studies have not been able to demonstrate superiority of these techniques on morbidity, mortality, and quality of life (6,13–18).")
46
Sitokin Uzaklaştırılması
Sürekli Tedavi ile Sitokin Uzaklaştırılması Cytokine Removal during Continuous Hemofiltration in Septic Patients DE VRIESE*, FRANCIS A. COLARDYN , JAN J. PHILIPPÉ , RAYMOND C. VANHOLDER*, JOHAN H. DE SUTTER and NORBERT H. LAMEIRE* JASN, 10:4; : 1999

47
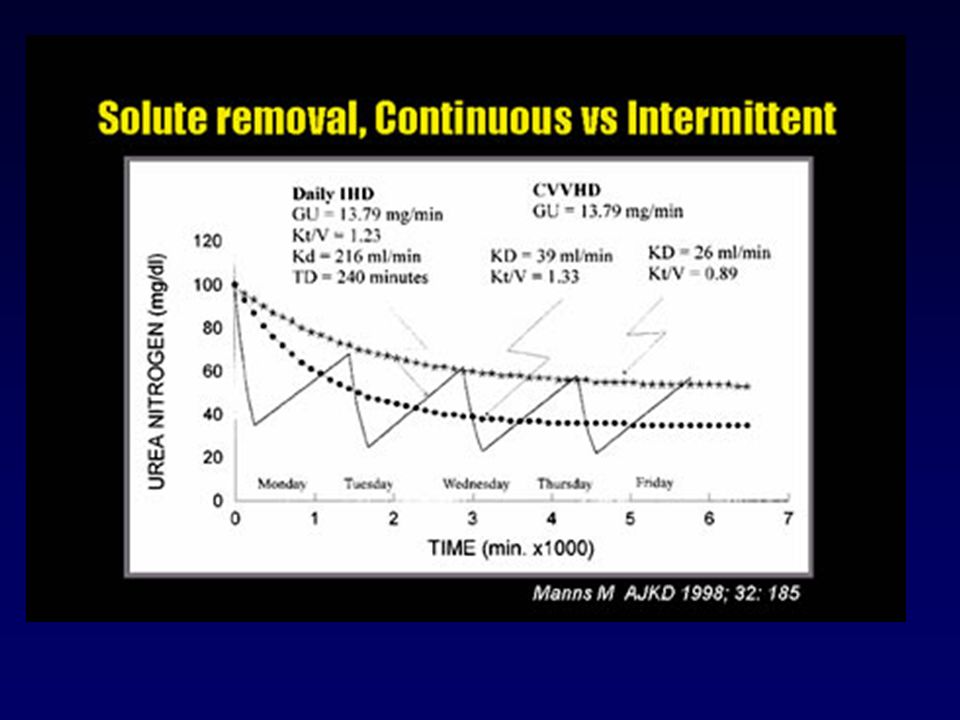
IHD vs CRRT Deneyim çok Modern makinalarla
Kontrollü UF Online- diyalizat Intradiyalitik solüt klirensi Tedavi süresi kısa Hemodinamik instabiliteye yol açabilir Ultrafiltrasyona tolerans daha iyi Sürekli Azotemi kontrolü Pahalı Tedavi süresi devamlı Devamlı antikoagülasyon gerekli

48
SLED CRRT ile aynı tedavi amaçlarına sahip
IHD gibi aralıklı tedavi olanağı sağlıyor Yavaş diyalizle başlanır: Qb=150ml/dk Qd= ml/dk UF hızı= max:350 ml/saat

49
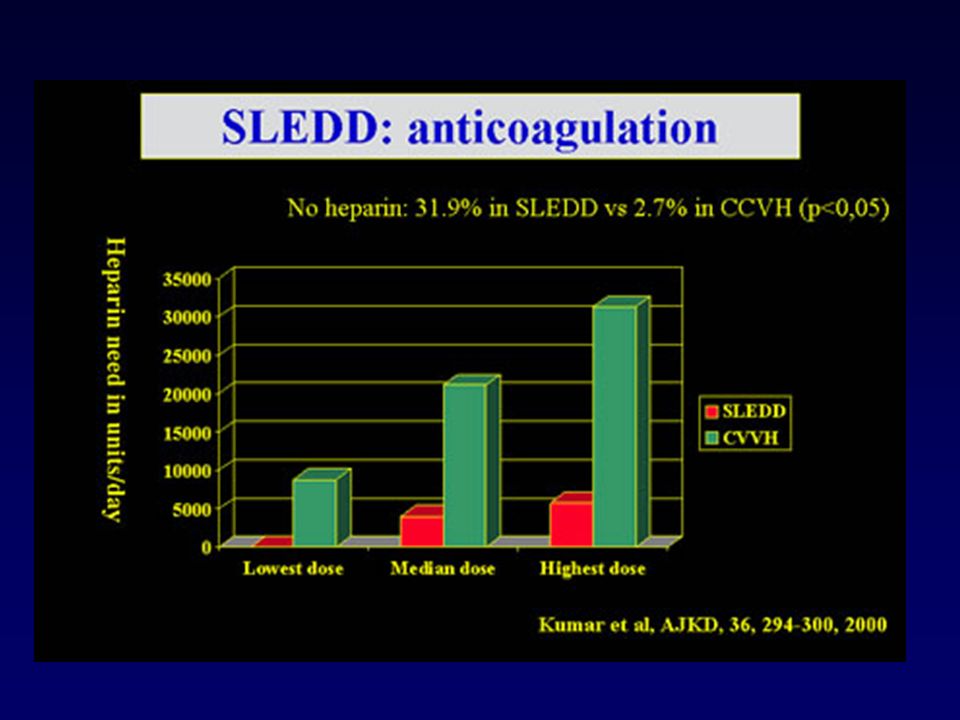
SLEDD:HEMODİNAMİK STABİLİTE
Kumar ve ark. AJKD:2000:36:

51
Intensive Care Med 33:1563–1570, 2007

52
YBÜ’de Ne Tip RRT seçilmeli?
IHD Diürez>500 ml/gün Tek organ yeters. IHD + UF CVVH Oligo-anuria Tek organ yeters. Tek organ yetersizliği UGR CVVH Her gün IHD SLED Diürez>500 ml MOY In practice, hemodynamic stability of the critically ill patient is the main determinant of the choice of dialysis modality (5) (Table 3). In addition to the patient’s hemodynamic stability, the choice between the various RRTs rests on solute clearance goals, volume control, and anticoagulation (Table 4). Volümlü CVVH SLED saat Oligo-anuria MOY KB stabil değil UGR
 (Table 3). In addition to the patient’s hemodynamic stability, the choice between the various RRTs rests on solute clearance goals, volume control, and anticoagulation (Table 4). Volümlü CVVH. SLED saat. Oligo-anuria. MOY. KB stabil değil. UGR ")
53
Ciddi metabolik asidoz
Amaç Hemodinami Tercih edilen RRT Sıvı Çekilmesi Stabil Stabil değil Aralıklı izole UF Yavaş sürekli UF Üre klirensi IHD CRRT Ciddi hiperkalemi Stabil / stabil değil Ciddi metabolik asidoz Ciddi Hiperfosfatemi Stabil/stabil değil

54
AKI-EPİDEMİYOLOJİ Çalışma sırasında AKI insidansı↑ : %2.8/sene
Avustralya’da 20 YBÜ ’e kabul edilen tüm hastalar: 91254 hasta ; 4745 AKI olgusunun analizi : İnsidans %5.2 Çalışma sırasında AKI insidansı↑ : %2.8/sene Hastane mortalitesi AKI (+) %42.7; AKI(-) %13.4 YBÜ’deki AKI hastaları giderek daha Yaşlı Ko-morbid hastalıklı Sepsis insidansı fazla Daha ağır organ yetmezlikli An Australian survey of data of all adult admissions to 20 Australian ICUs for 24 hours or more from 1 January 1996 to 31 December 2005 was conducted to assess trends in incidence and mortality for ICU admissions associated with early AKI [23]. The authors analyzed 91,254 patient admissions, including 4,754 cases of AKI, for an estimated crude cumulative incidence of 5.2%. The incidence of AKI increased during the study period, with an estimated annual increment of 2.8%. The crude hospital mortality was significantly higher in patients with AKI than in those without it (42.7% versus 13.4%). There was also a decrease in AKI crude mortality (annual percentage change: -3.4%), however, which was not observed in patients without AKI. After covariate adjustment, AKI remained associated with a higher mortality (odds ratio = 1.23; P < 0.001), but there was a declining trend in the odds ratio for hospital mortality. Such retrospective studies and many other observational ones suggest that critically ill patients with AKI are increasingly older, have more co-morbid disease, have a higher incidence of sepsis, and have greater severity of illness and organ failure [24]. It is possible, however, that outcomes in patients treated about 10 years ago is not meaningful when compared with prospective data from multinational and multicentre assessment of patients who are all critically ill, treated in an ICU, and typically receiving mechanical ventilation and vasopressor therapy [25]. Despite the much greater severity of illness in patients treated today,the mortality of AKI has not increased and has perhaps slightly decreased, the duration of treatment has clearly decreased in terms of need for dialysis; also, the time spent in the ICU and in hospital, and artificial renal support techniques have also changed markedly (significant findings have been reported for the subgroup of AKI patients who have suffered trauma [23]). It is likely, hence, that the 50% to 60% crude mortality associated with AKI will not change dramatically in the coming years, because as therapeutic (and diagnostic) capabilities improve, the health care system will admit and treat progressively sicker patients with AKI. Comparisons that do not take into account this continuing adjustment and that do not appreciate the continuing change in illness severity will present a misleading picture of achievements associated with improvements in technology and medications. AKI MORTALİTESİNİN ARTTIĞI SÖYLENEMEZ
 %42.7; AKI(-) %13.4. YBÜ’deki AKI hastaları giderek daha. Yaşlı. Ko-morbid hastalıklı. Sepsis insidansı fazla. Daha ağır organ yetmezlikli. An Australian survey of data of all adult admissions to 20 Australian ICUs for 24 hours or more from 1 January 1996 to. 31 December 2005 was conducted to assess trends in incidence and mortality for ICU admissions associated with. early AKI [23]. The authors analyzed 91,254 patient admissions, including 4,754 cases of AKI, for an estimated. crude cumulative incidence of 5.2%. The incidence of AKI increased during the study period, with an estimated annual increment of 2.8%. The crude hospital mortality was significantly higher in patients with AKI than in those without it (42.7% versus 13.4%). There was also a decrease in AKI crude mortality (annual percentage change: -3.4%), however, which was not observed in patients without AKI. After covariate adjustment, AKI remained associated with a higher mortality (odds ratio = 1.23; P < 0.001), but there was a declining trend in the odds ratio for hospital mortality. Such retrospective studies and many other observational. ones suggest that critically ill patients with AKI are increasingly older, have more co-morbid disease, have a. higher incidence of sepsis, and have greater severity of illness and organ failure [24]. It is possible, however, that. outcomes in patients treated about 10 years ago is not meaningful when compared with prospective data from multinational and multicentre assessment of patients who are all critically ill, treated in an ICU, and typically receiving mechanical ventilation and vasopressor therapy [25]. Despite the much greater severity of illness in patients treated today,the mortality of AKI has not increased and has perhaps slightly decreased, the duration of treatment has clearly decreased in terms of need for dialysis; also, the time spent in the ICU and in hospital, and artificial renal support techniques have also changed markedly (significant findings have been. reported for the subgroup of AKI patients who have suffered. trauma [23]). It is likely, hence, that the 50% to 60% crude. mortality associated with AKI will not change dramatically in. the coming years, because as therapeutic (and diagnostic) capabilities improve, the health care system will admit and. treat progressively sicker patients with AKI. Comparisons that. do not take into account this continuing adjustment and that. do not appreciate the continuing change in illness severity. will present a misleading picture of achievements associated. with improvements in technology and medications. AKI MORTALİTESİNİN ARTTIĞI SÖYLENEMEZ.")
55
SONUÇ ABY gelişmemesi için önlemlerin alınması gerekli
Özellikle riskli hasta gruplarının belirlenmesi önemli ABY’de Dopamin ve furosemid kullanımını destekleyen kanıt yok RRT seçimi ünite koşulları ve hasta gereksinimine göre belirlenmeli

56
Teşekkürler…

Benzer bir sunumlar



 yönlendirilmelidir?>")

















