Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
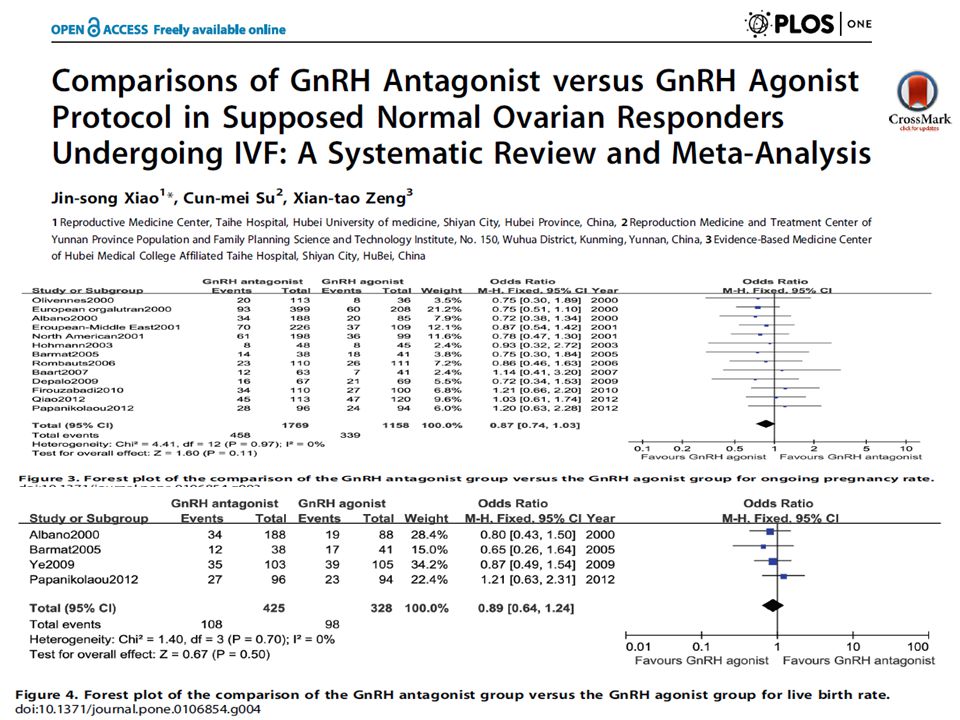
GnRH Antagonist ve İmplantasyon
Prof. Dr. Cem S. Atabekoğlu Ankara Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum AD.

2
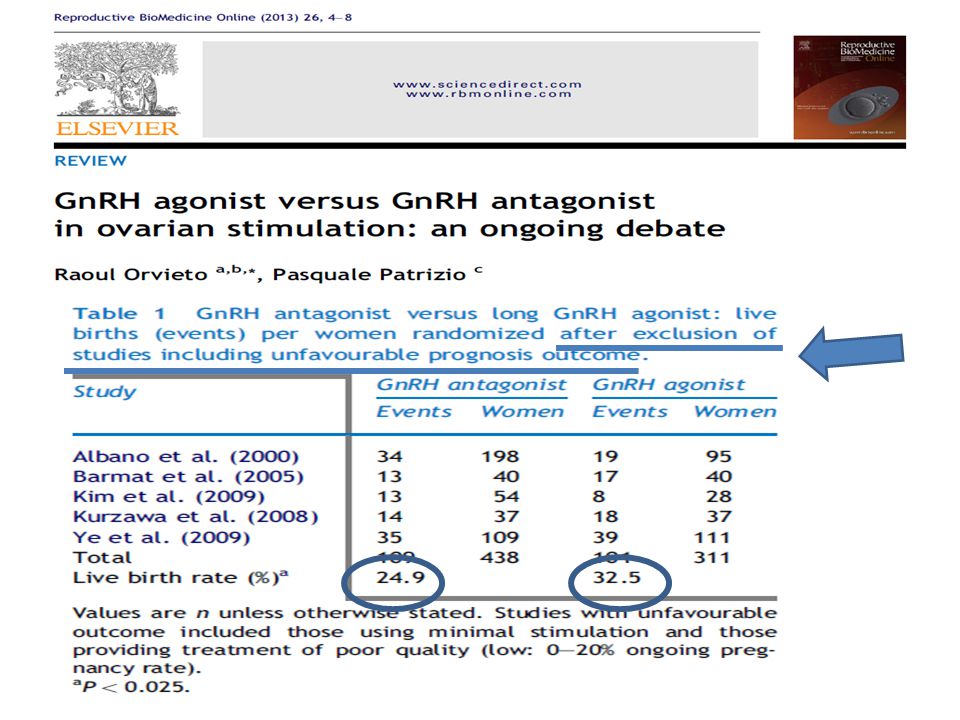
GnRHa vs. GnRH ant (45 RCT) Live birth
Al Inany, Cochrane Database Syst Rev,2011

4
Trend GnRH Antagonist Kısa tedavi süresi Daha az gonadotropin
Daha az ciddi OHSS Benzer canlı doğum oranları

6
GnRH-a vs. GnRH-ant Bals-Pratsch, Reproduktionsmed Endokrinol 2010
Alman IVF Arşiv Data GnRHa / GnRHant Bals-Pratsch, Reproduktionsmed Endokrinol 2010

7
GnRH-a vs. GnRH-ant Patrizio, RMB Online, 2013

10
2006-2010 AÜTF data Genel Agonist Antagonist TOS 13.8 11 MII OOSİT
12.3 9.9 Gn SÜRE E MAX 3796 2559 TES 2.96 2.69 DOZ 2760 3000 GEBELİK (HCG) %49 %42 KL.GEBELİK %38 İMPLANTASYON %22.4 %19.1
 %49. %42. KL.GEBELİK. %38. İMPLANTASYON. %22.4. %19.1.")
11
2006-2010 AÜTF data NORMO Agonist Antagonist TOS 10.9 9.8 MII OOSİT
9.7 9 Gn SÜRE 9.9 TES 2.8 2.7 E MAX 2512 2248 GEBELİK (HCG) %50.5 KL.GEBELİK %43.5 %45.3 İMPLANTASYON %24.6 %20.6
 %50.5. KL.GEBELİK. %43.5. %45.3. İMPLANTASYON. %24.6. %20.6.")
12
2006-2010 AÜTF data HİPER Agonist Antagonist TOS 19.2 17.8 MII OOSİT
17.3 TES 3.1 E MAX 5472 4349 GEBELİK (HCG) %51 %35 KL.GEBELİK %42 %30.2 İMPLANTASYON %21.9 %15.3
 %51. %35. KL.GEBELİK. %42. %30.2. İMPLANTASYON. %21.9. %15.3.")
13
2006-2010 AÜTF data POOR Agonist Antagonist TOS 4.5 MII OOSİT 4.2 3.9
TES 2.1 E MAX 861 907 GEBELİK (HCG) %30.7 %33.3 KL.GEBELİK %27 %26 İMPLANTASYON %20 %15.8
 %30.7. %33.3. KL.GEBELİK. %27. %26. İMPLANTASYON. %20. %15.8.")
14
GnRH-a for Pituitary Control
Genç normogonadotropik kadınlarda analog sikluslar da ovaryan stimülasyon için altın standart long GnRH-a protocoldür. Şeçim yapılmamış KOS siklus çalışmalarında GnRH-antagonist protokolün, agonist protokole üstün olduğunu gösteren kanıt yoktur.

15
Long agonist Antagonist

17
Antagonist = Agonist Oosit kalitesi Fertilizasyon oranı
Embriyo kalitesi

18
NEDEN? OOSİT KALİTESİ, EMBRİYO KALİTESİ, FERTİLİZASYON ORANLAR ARASINDA FARK YOK FROZEN SİKLUSLARDA İMPLANTASYON VE GEBELİK ORANLARINDA FARK YOK!!!! İMPLANTASYON ???????

20
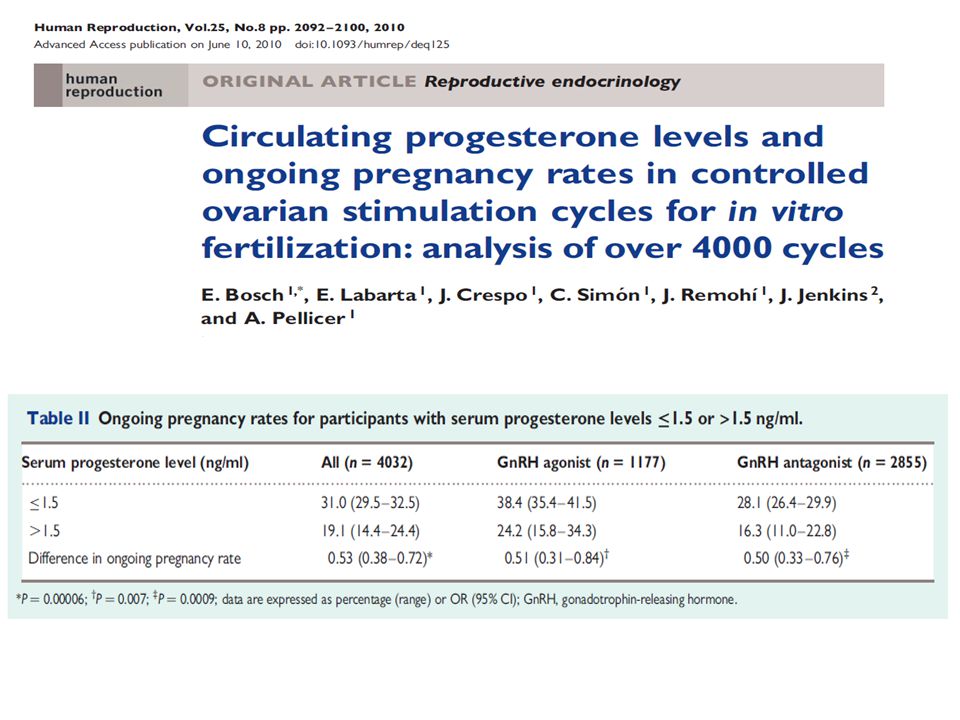
GnRH agonist n-=1117 GnRH antagonist n= 2865 P>1.5 ng/ml
rFSH n= 138 % 8.7 +LH n=979 % 8.1 P>1.5 ng/ml rFSH n= 261 % 11.5 +LH n=2594 % 5.2 Nevertheless it is interesting to note that of 1117 IVF/ICSI cycles with a GnRH agonist long protocol the progesterone level on the day of hCG administration was above 1.5 ng/ml in 8.7% of 138 treatment cycles using rFSH alone compared with 8.1% of 979 treatment cycles using a stimulation protocol with LH activity. Of even more interest in 2855 patients undergoing IVF/ICSI with a GnRH antagonist daily protocol the progesterone level on the day of hCG administration was above 1.5 ng/ml in 11.5% of 261 cycles using rFSH alone compared with 5.2% of 2594 cycles using a stimulation protocol with LH activity.

25
Patients and methods: We reviewed the files of all consecutive patients undergoing COH with
either GnRH-agonist or antagonist in our IVF unit during a 10-year period and who had their peak serum progesterone levels determined on the day of human chorionic gonadotropin (hCG) administration. Results: Of the 2244 IVF cycles evaluated, 2103 had peak progesterone level of 51.5 ng/mL (normal-P group) and 141 of41.5 ng/mL (high-P group) (6.28% of all the study population). Clinical pregnancy rate was significantly higher in the normal-P group (25.4% versus 16.6%; p50.006). Moreover, among the high-P group patients, the use of the long GnRH-agonist suppressive protocol (GnRH-ag) was more prevalent in patients who conceived as compared to those who did not (60.9% versus 39%, respectively; p50.05), with a tendency toward an increase pregnancy rate in those using GnRH-ag compared with GnRH-antagonist protocol (GnRH-antag; p50.059) COH protocols.
 administration. Results: Of the 2244 IVF cycles evaluated, 2103 had peak progesterone level of 51.5 ng/mL. (normal-P group) and 141 of41.5 ng/mL (high-P group) (6.28% of all the study population). Clinical pregnancy rate was significantly higher in the normal-P group (25.4% versus 16.6%; p50.006). Moreover, among the high-P group patients, the use of the long GnRH-agonist. suppressive protocol (GnRH-ag) was more prevalent in patients who conceived as compared to. those who did not (60.9% versus 39%, respectively; p50.05), with a tendency toward an. increase pregnancy rate in those using GnRH-ag compared with GnRH-antagonist protocol. (GnRH-antag; p50.059) COH protocols.")
26
Conclusion: While subtle progesterone elevation in patients undergoing COH using GnRH-antag
COH protocols, should dictate embryo cryopreservation and cancelation of the fresh transfer, in those undergoing the GnRH-ag COH protocol, a fresh embryo transfer should be recommended. As expected [1,3], the high-P group had higher estradiol levels on the day of hCG administration and achieved a significantly higher oocytes yield. Moreover, patients in the high-P group who conceived, also had higher oocyte yields, used more frequently the GnRH-ag rather than the GnRH-antag protocols. These aforementioned observations were also observed by Venetis et al. [1] in the group of patients undergoing the GnRH-ag COH protocol and were attributed to an excess number of follicles, each one producing a normal, for the late follicular phase, amount of progesterone. As a result, the excess granulosa cells proliferating leads to an increased progesterone production, independently of LH exposure [1,4].

27
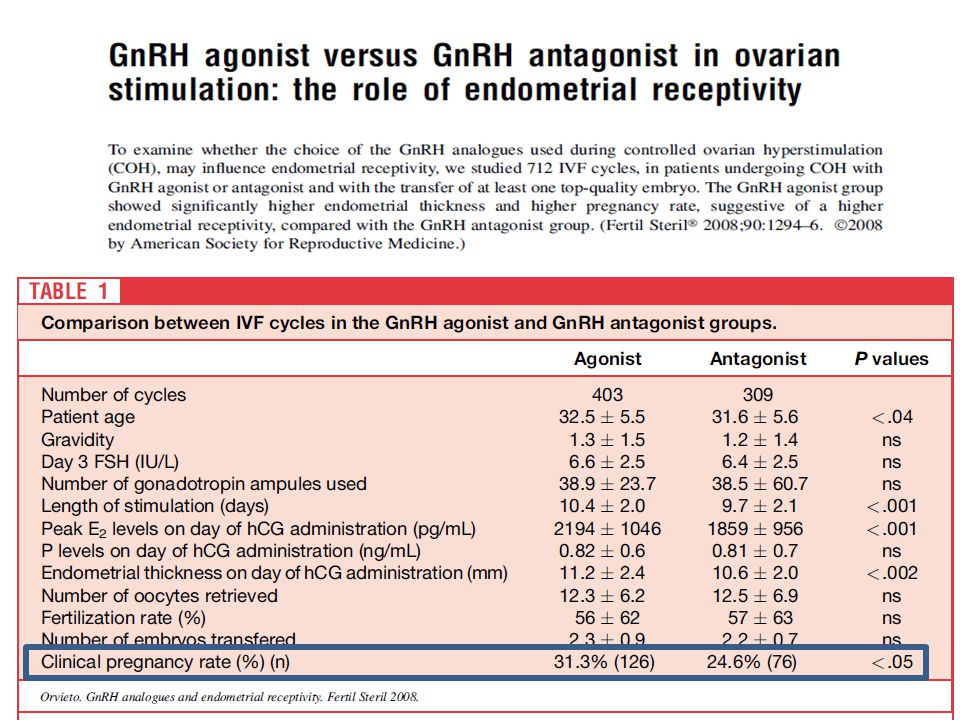
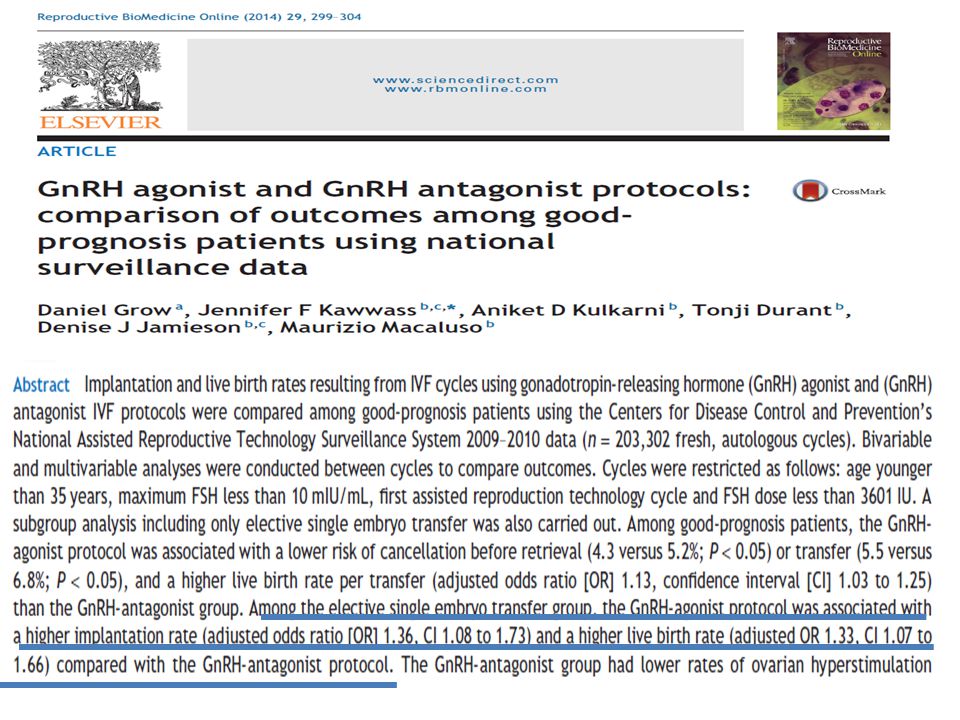
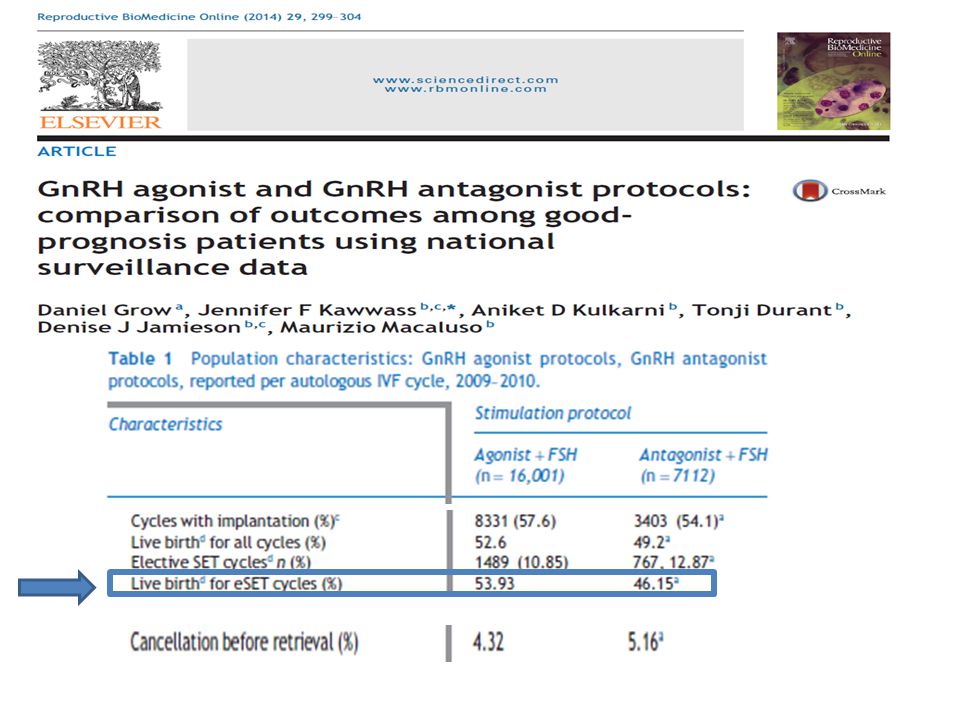
GnRH Antagonist ve İmplantasyon
FSH ve GnRH Reseptörleri endometriumda gösterilmiştir. Gonadotropinlerin ve GnRH analoglarının endometrium üzerine direkt ya da indirekt etkisi olabilir. Yüksek serum E2 düzeyleri yada diğer hormonal değişiklikler endometriyumu olumsuz etkileyebilir.

29
GnRH-a vs. GnRH-ant

31
GnRH-a vs. GnRH-ant

32
GnRH-a vs. GnRH-ant

34
GnRH Antagonist ve İmplantasyon
GnRH antagonistin endometrial GnRH reseptorlerine bağlanmasının implantasyon aşamasında rol alan post reseptör olaylar üzerinde olumsuz etkisi olabilir. Preovulatuar GnRH agonist verilmesi endometrial reseptörlerde GnRH antagonist ile yer değiştirip implantasyon için uygun postreseptör değişikliklerin oluşmasını sağlayabilirmi ??????

36
GnRH Antagonist ve İmplantasyon
Luteal fazda tek doz GnRH-agonist kullanımı implantasyon oranını hem GnRH-agonist hem de GnRH-antagonist protokollerde arttırır, Anlamlı klinik gebelik oran artışı sadece GnRH antagonist protokol ile tedavi edilen grupta izlenmiştir. Oliveira JB, Administration of single-dose GnRH agonist in the luteal phase in ICSI cycles: a meta-analysis. Reprod Biol Endocrinol 2010;8:107.

37
GnRH Antagonist ve İmplantasyon
GnRH antagonistlerinin implantasyona etkisi doz bağımlıdır. Ganirelix (0.5, 1, and 2 mg) dozları düşük implantasyon oranları göstermiştir. 0.25-mg (21.9%) 2-mg (1.5%), Doz artıkça abortus oranı artar In contrast, when embryos were cryopreserved after an ovulation stimulation cycle in which high-dose GnRH antagonists were used and later thawed and transfered, the implantation and pregnancy rates were unaffected by the use of GnRH antagonist during the initial stimulation cycle (20, 25). These data suggest an effect of GnRH antagonists on the endometrium and therefore an effect on endometrial receptivity. Ganirelix Dose-Finding Study Group. Hum Reprod 1998;13:3023–31.
 dozları düşük implantasyon oranları göstermiştir mg (21.9%) 2-mg (1.5%), Doz artıkça abortus oranı artar. In. contrast, when embryos were cryopreserved after an ovulation. stimulation cycle in which high-dose GnRH antagonists. were used and later thawed and transfered, the implantation. and pregnancy rates were unaffected by the use of GnRH antagonist. during the initial stimulation cycle (20, 25). These. data suggest an effect of GnRH antagonists on the endometrium. and therefore an effect on endometrial receptivity. Ganirelix Dose-Finding Study Group. Hum Reprod 1998;13:3023–31.")
38
GnRH Antagonist ve İmplantasyon
Endometrial gelişim histolojik olarak GnRH antagonist kullanılan sikluslarda, GnRH agonist sikluslara göre natürel sikluslara daha benzerdir. Simon C. Hum Reprod 2005;20: 3318–27.

39
PINOPODE Y. Meng et al.Proteomics 2014, 14, 2350–2359
In our biopsies, we found developing, fully developed, and regressing pinopodes in each group which is the ultrastructural markers of the implantation window [25, 26] (Fig. 1). In GnRH antagonists group (represented by “S”), the apical surfaces of cells were similar to agonists group (defined as “D”) and a little different from nonstimulated ones. It seemed that there weremore fully developed pinopodes in natural cycle group (defined as “N”) and more regressing pinopodes in GnRH analogs treatment group. These results cannot suggest a different pattern of endometrial development in GnRH analogs treatment group because of the limited sample size in our study. But it confirmed that the endometrial dating was corresponding to the putative window of implantation. Y. Meng et al.Proteomics 2014, 14, 2350–2359
. In GnRH antagonists group (represented by S ), the apical. surfaces of cells were similar to agonists group (defined as. D ) and a little different from nonstimulated ones. It seemed. that there weremore fully developed pinopodes in natural cycle. group (defined as N ) and more regressing pinopodes. in GnRH analogs treatment group. These results cannot suggest. a different pattern of endometrial development in GnRH. analogs treatment group because of the limited sample size. in our study. But it confirmed that the endometrial dating. was corresponding to the putative window of implantation. Y. Meng et al.Proteomics 2014, 14, 2350–2359.")
41
METHODS: Mid-luteal phase endometrial biopsies
were obtained from oocyte donors undergoing ovarian stimulation and from control women with regular periods. Immunohistochemistry and real-time quantitative–polymerase chain reaction (QRT–PCR) were used to compare protein and mRNA expression of progesterone receptor (PR), estrogen receptor a (ERa), estrogen receptor b (ERb), androgen receptor (AR), 3bHSD1, 3bHSD2, 17bHSD2 and 17bHSD5. RESULTS: Cetrorelix–rFSH treatment caused a mid-luteal suppression of PR protein expression in the endometrial stroma, surface epithelium and glands, although expression in the glands of control samples was variable. In contrast, the treatment caused an increase in PR staining in perivascular cells. No other significant differences in protein expression were observed between the two groups. mRNA levels of AR, ERa, 3bHSD1 and 17bHSD2 were significantly reduced in the treatment group. PR mRNA levels were also reduced by GnRH antagonist–rFSH treatment, but the difference was not significant. CONCLUSIONS: Changes in the expression of sex-steroid receptors and metabolizing enzymes may lead to alterations in the activity and intracellular availability of estrogens, progestogens and androgens in endometrium of women treated with Cetrorelix and rFSH. Their impact on embryo implantation merits further evaluation.
 were used to compare. protein and mRNA expression of progesterone receptor (PR), estrogen receptor a (ERa), estrogen receptor b. (ERb), androgen receptor (AR), 3bHSD1, 3bHSD2, 17bHSD2 and 17bHSD5. RESULTS: Cetrorelix–rFSH treatment. caused a mid-luteal suppression of PR protein expression in the endometrial stroma, surface epithelium and. glands, although expression in the glands of control samples was variable. In contrast, the treatment caused an. increase in PR staining in perivascular cells. No other significant differences in protein expression were observed. between the two groups. mRNA levels of AR, ERa, 3bHSD1 and 17bHSD2 were significantly reduced in the treatment. group. PR mRNA levels were also reduced by GnRH antagonist–rFSH treatment, but the difference was not significant. CONCLUSIONS: Changes in the expression of sex-steroid receptors and metabolizing enzymes may lead to. alterations in the activity and intracellular availability of estrogens, progestogens and androgens in endometrium. of women treated with Cetrorelix and rFSH. Their impact on embryo implantation merits further evaluation.")
42
GnRH Antagonist /Adezyon molekülleri
Muc-1 antiadheziv özellik gösteren bir moleküldür. Farelerde embriyonun tutunmasından önce endometrium epitelinde down-regüle olduğu gösterilmiştir. Buna karşılık insanda reseptif dönemde ekspresyonda artış olmaktadır. Ancak dikkatle incelendiğinde embriyonun bulunmasının Muc-1 yapımını epitelyumda yakınlaşma safhasında arttırdığı, ancak adezyon safhasında embriyonun bulunmasının implantasyon sahasındaki Muc-1 konsantrasyonunu azalmasını indüklediği gösterilmiştir

43
GnRH antagonist /Adezyon molekülleri
integrin β3 leukaemia-inhibitory factor (LIF) Compared with the PMSG alone protocol, OS with GnRH agonist co-treatment showed elevated expression levels of endometrial integrin β3 subunit and LIF and a higher embryonic implantation rate, suggesting that OS with GnRH agonist co-treatment, but not with GnRH antagonist co-treatment, may potentially improve uterine receptivity, and this improvement of uterine receptivity in mice might be partially through the restoration of physiologically endometrial secretion changed in the OS cycle
 Compared. with the PMSG alone protocol, OS with GnRH agonist. co-treatment showed elevated expression levels of endometrial. integrin β3 subunit and LIF and a higher embryonic implantation. rate, suggesting that OS with GnRH agonist co-treatment, but not with GnRH antagonist co-treatment, may potentially. improve uterine receptivity, and this improvement of uterine. receptivity in mice might be partially through the restoration of. physiologically endometrial secretion changed in the OS cycle.")
44
GnRH Antagonist /Adezyon molekülleri

45
GnRH Antagonist ve İmplantasyon
Gonadotropin-releasing hormon plasental trofoblastlarda matrix metalloproteinaz (MMPs) modüle eder. Ekstraselüler matriks degredasyonu ve trofoblast hücre invazyonunda önemlidir. Liu J, Reprod Biol Endocrinol 2010;8:5. Sasaki K, Curr Opin Endocrinol Diabetes Obes 2011;18:401–8.
 modüle eder. Ekstraselüler matriks degredasyonu ve trofoblast hücre invazyonunda önemlidir. Liu J, Reprod Biol Endocrinol 2010;8:5. Sasaki K, Curr Opin Endocrinol Diabetes Obes 2011;18:401–8.")
46
Patient(s): Nineteen subjects were included: 12 subjects underwent controlled ovarian hyperstimulation with recombinant FSH and used either a GnRH antagonist or a GnRH agonist; seven control subjects underwent natural cycles. Intervention(s): Pipelle endometrial biopsies were obtained 11 days after hCG administration or spontaneous LH surge in untreated cycles, respectively. Immunohistochemistry was used to assess HOXA10 protein expression in endometrial glands and stroma. Main Outcome Measure(s): Endometrial HOXA10 protein expression. Result(s): HOXA10 expression was significantly decreased in endometrial stromal cells in GnRH antagonist– treated cycles compared with GnRH agonist–treated cycles or natural cycle control subjects. There was no significant difference in glandular cell HOXA10 expression among the three groups. Conclusion(s): Use of GnRH antagonists may be associated with impaired HOXA10 expression in endometrial stromal cells and thus may affect endometrial receptivity.
: Pipelle endometrial biopsies were obtained 11 days after hCG administration or spontaneous LH. surge in untreated cycles, respectively. Immunohistochemistry was used to assess HOXA10 protein expression in. endometrial glands and stroma. Main Outcome Measure(s): Endometrial HOXA10 protein expression. Result(s): HOXA10 expression was significantly decreased in endometrial stromal cells in GnRH antagonist– treated cycles compared with GnRH agonist–treated cycles or natural cycle control subjects. There was no significant. difference in glandular cell HOXA10 expression among the three groups. Conclusion(s): Use of GnRH antagonists may be associated with impaired HOXA10 expression in endometrial. stromal cells and thus may affect endometrial receptivity.")
47
Study design: This study was conducted at the Department of Obstetrics and Gynecology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand. Thirty-five volunteers were recruited into this prospective, self-controlled study, which was divided into two cycles, the first a natural control cycle and the second a GnRH antagonist-treated cycle. The two cycles were separated by one resting cycle. In the GnRH antagonist-treated cycle, when the leading follicle was 15 mm, ganirelix (Orgalutran1) 0.25 mg was administered daily. In both cycles, ovulation was induced when the largest follicle reached 18 mm in diameter. Finally, endometrial biopsy was performed on day 6 after documented ovulation, which corresponds to the window of implantation. Endometrial HOXA10 protein expression, a marker of endometrial receptivity, was analyzed by immunohistochemistry. The protein expression was compared between the two cycles regarding their percentage of immunostained cells and IHC-scores (percentage of stained cells intensity of nuclear staining).
 0.25 mg was administered daily. In both cycles, ovulation was induced when the largest follicle reached 18 mm in diameter. Finally, endometrial biopsy was performed on day 6 after documented ovulation, which corresponds to the window of implantation. Endometrial HOXA10 protein expression, a marker of endometrial receptivity, was analyzed by immunohistochemistry. The protein expression was compared between the two cycles regarding their percentage of immunostained cells and IHC-scores (percentage of stained cells intensity of nuclear staining)..")
49
NATUREL SİKLUS / AGONİST SİKLUS 24 PROTEİN FARKLI EKSPRESE OLUYOR
NATUREL SİKLUS/ ANTAGONİST 39 PROTEİN FARKLI EKSPRESE OLUYOR ANTAGONİST SİKLUSLARDA 7 PROTEİN FARKLI OLARAK EKSPRESE OLUR

50
Sonuç Eldeki verilere göre implantasyon açısından GnRH agonistleri daha iyi gözükmektedir. İndirekt etkiler olabileceği gibi, endometriumda bulunan GnRH reseptörleri burada direkt etken olabilir. Yüksek progesteron seviyelerinde embriyo freezing önerilmelidir. Dual trigger ve freeze all stratejisi ile bu olumsuzluk giderilebilir.

51
Teşekkürler

Benzer bir sunumlar