Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Gebelik ve HPV Gebeliğin etkisi, Gebeliğe etki
Doç. Dr. İzzet ŞAHİN

2
Yanıtlanması gerek sorular
Vertikal geçiş mekanizmaları ve vertikal geçiş hızı? Genital siğil olan kadınlarda yenidoğanda JoRRP riski? Doğum şekli vertikal geçişi ve neonatal enfeksiyonu etkiler mi? Gebelik HPV enfeksiyonunun seyrini ve prevalansını etkiler mi? HPV gebelik sonucunu etkiler mi?

3
Epidemiyoloji Kadınların
%4’ünde kolposkopik (subklinik) değişiklikler %10’unda görünür lezyon olmaksızın DNA (+) biyopsiler %60’ında HPV antikor pozitifliği (HPV-DNA veya klinik lezyon olmaksızın) Kadınların > % 50’de ilk ilişkiden sonraki 4 yıl içinde HPV (+) Doğurganlık çağındaki kadınların %25’inde genital traktusta HPV (+) En yüksek prevalans yaşlarda Klinik HPV enfeksiyonu gebelerin % 1,5 – 5’inde (US) The universality of HPV in the lower genital tract rivals that of any other sexually transmitted disease in humans. It is estimated that at least one million cases of genital papillomas occur per year in the United States. 29 These are most commonly manifested as condylomata acuminata involving the cervix, vulva, or other anogenital sites in women or the penis of male sexual partners of affected women. Colposcopic (subclinical) changes are seen in about 4% of women, whereas DNA positive biopsies without a visible lesion are seen in 10% of women. HPV antibody positivity (without DNA or a clinical lesion) is estimated in 60% of women (81 million). HPV has been estimated to be present in the genital tract of as many as 25% of all women of child-bearing age worldwide. One study reported that the incidence of HPV infections in sexually active young college women is highest, with a cumulative incidence of 43% during a 36-month period. 30 Clinically apparent HPV infection has been noted in 1.5% to 5% of pregnant women in the United States. 31 More than 30% of American women are currently infected with HPV with 7.5 million 14- to 24-year-olds currently infected and one fourth of women younger than 60 years of age infected at any given time. 32 Up to 90% of lesions are undetectable clinically at 2 years. The highest prevalence is in women 20 to 24 years of age. More than 50% of women will initially acquire HPV within 4 years of their first sexual intercourse. As in RRP, HPV 6 and HPV 11 are the most common subtypes identified in cervical condylomata. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby.
 değişiklikler. %10’unda görünür lezyon olmaksızın DNA (+) biyopsiler. %60’ında HPV antikor pozitifliği (HPV-DNA veya klinik lezyon olmaksızın) Kadınların > % 50’de ilk ilişkiden sonraki 4 yıl içinde HPV (+) Doğurganlık çağındaki kadınların %25’inde genital traktusta HPV (+) En yüksek prevalans yaşlarda. Klinik HPV enfeksiyonu gebelerin % 1,5 – 5’inde (US) The universality of HPV in the lower genital tract rivals that of any other sexually transmitted disease in humans. It is estimated that at least one million cases of genital papillomas occur per year in the United States. 29 These are most commonly manifested as condylomata acuminata involving the cervix, vulva, or other anogenital sites in women or the penis of male sexual partners of affected women. Colposcopic (subclinical) changes are seen in about 4% of women, whereas DNA positive biopsies without a visible lesion are seen in 10% of women. HPV antibody positivity (without DNA or a clinical lesion) is estimated in 60% of women (81 million). HPV has been estimated to be present in the genital tract of as many as 25% of all women of child-bearing age worldwide. One study reported that the incidence of HPV infections in sexually active young college women is highest, with a cumulative incidence of 43% during a 36-month period. 30 Clinically apparent HPV infection has been noted in 1.5% to 5% of pregnant women in the United States. 31 More than 30% of American women are currently infected with HPV with 7.5 million 14- to 24-year-olds currently infected and one fourth of women younger than 60 years of age infected at any given time. 32 Up to 90% of lesions are undetectable clinically at 2 years. The highest prevalence is in women 20 to 24 years of age. More than 50% of women will initially acquire HPV within 4 years of their first sexual intercourse. As in RRP, HPV 6 and HPV 11 are the most common subtypes identified in cervical condylomata. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby.")
4
Geçiş Yolları Seksüel temas (erişkin ve çocuklarda primer geçiş şekli)
Penetratif seksüel temas Yakın genital temas Non-seksüel temas (direkt / indirekt) Maternal temas (=vertical transmission) (direkt / indirekt) Human Papillomavirus has been shown to be transmitted in several modes. 1 2 5 6 7 9 12 14 20 21 22 26 The modes of transmission include: sexual contact, non-sexual contact (either directly or indirectly), and maternal contact either directly or indirectly. 1421 26 27 Sexual contact is the primary mode of transmission in both adults and children. 7 14 21 28 Transmission can occur through penetrative sexual contact or intimate genital contact. 4 26 29 Non-sexual acquisition can occur when HPV on skin surfaces or contaminated fomites comes in contact with microscopic injuries in the skin surface. 21 22 This has been demonstrated in school aged children who acquire HPV from the sharing of school supplies. 30 Auto inoculation occurs from the transmission of HPV from one site to another scratching or bathing. 21 22 31 Human Papillomavirus in Infants: Transmission, Prevalence, and Persistence, Delese E. LaCour, and Connie Trimble, J Ped Adolescent Gynecol, 2012; 25 (2); 93-97
 Maternal temas (=vertical transmission) (direkt / indirekt) Human Papillomavirus has been shown to be transmitted in several modes The modes of transmission include: sexual contact, non-sexual contact (either directly or indirectly), and maternal contact either directly or indirectly Sexual contact is the primary mode of transmission in both adults and children Transmission can occur through penetrative sexual contact or intimate genital contact Non-sexual acquisition can occur when HPV on skin surfaces or contaminated fomites comes in contact with microscopic injuries in the skin surface This has been demonstrated in school aged children who acquire HPV from the sharing of school supplies. 30 Auto inoculation occurs from the transmission of HPV from one site to another scratching or bathing Human Papillomavirus in Infants: Transmission, Prevalence, and Persistence, Delese E. LaCour, and Connie Trimble, J Ped Adolescent Gynecol, 2012; 25 (2);")
5
Vertikal Geçiş (Olası Mekanizmalar)
Perikonsepsiyonel geçiş Erkeklerde reprodüktif traktusta, semende ve sperm hücrelerinde; Kadınlarda endometriumda ve overlerde HPV DNA’sı bulunmasına rağmen bu geçiş yolunu teyit edecek yeterli veri yok. JoRRP gelişen çocukların %50’sinde maternal HPV saptanmaması perikonsepsiyonel geçiş ile açıklanabilir POSSIBLE MECHANISMS OF HPV VERTICAL TRANSMISSION Although HPV DNA has been detected in different sites of the male reproductive tract [8–10], sperm cells [4, 11, 12], semen [13, 14], endometrium, and ovaries [15], which suggests that HPV could be transmitted during the fertilization of an oocyte or immediately afterward, the significance of these findings is still unknown. In vitro analyses have indicated the viability of HPV infection in spermatozoids and the transcription of HPV genes in fecund oocytes [8–10, 16–20], and the transcriptional activity of HPV-16 in sperm was confirmed in vivo [21]. However, further investigations are necessary to confirm this route of transmission. For this reason, the discussion about the possible mechanisms of HPV vertical transmission will center on the prenatal and perinatal routes, which are better understood. RENATAL TRANSMISSION The observation of infants showing signs of HPV-induced lesions at birth, such as laryngeal and anogenital lesions, has led to the belief that intrauterine HPV transmission can occur [22, 23]. HPV DNA has been detected in amniotic fluid [3], placenta, and the umbilical cord [7]. Both chorionic and placental tissue can be infected through the hematogenous route and hence, HPV can be spread to amniotic cells that are then ingested by the fetus [2, 3]. Transplacental infection, another possible means of HPV intrauterine transmission, can occur through the ascending route from the maternal genital tract, as it has been shown that the presence of HPV-DNA, both in amniotic fluid [3] and the umbilical cord [2], is correlated with cervical intraepithelial lesions in pregnant women. Once believed to be low, the HPV vertical transmission rate has shown inconsistent results, probably due to the heterogeneous nature of the clinical trials [24]. Despite this, in a systematic quantitative review, Medeiros et al [24] reported a pooled relative risk of mother-to-child HPV transmission (4.8) when the mother is shown to be HPV positive. Additionally, the risk of the newborn having the same HPV type as that found in the maternal genital tract is 4 times greater when the umbilical cord blood is positive for the same HPV [25]. Evidence from the cervical samples indicates that mothers who transmit HPV to their infants have a higher viral load than those who do not [26]. Sarkola et al [25] reported that peripheral blood samples from all mothers who had HPV in the placenta and umbilical cord tested negative for HPV. According to these authors, the detection of viral DNA in their samples appears to be due to a maternal history of productive infection and not the detection of viral genetic material during pregnancy. However, there remains the possibility that HPV infected the placenta during early pregnancy and had already cleared the cervix at the time of delivery [2]. During pregnancy, the uterine canal undergoes anatomic and immunologic changes that may increase the susceptibility of pregnant women to infections [27]. In addition to other human viruses such as HIV, cytomegalovirus, and Epstein-Barr virus, HPV may be able to infect the placenta or cells of fetal origin [28]. The transplacental transmission of HIV and maternal cells, including lymphocytes, is a phenomenon that has already been described and can be stimulated by pathologic conditions [28, 29]. Reports of the presence of HPV in polymorphonuclear cells suggest that the transfer of maternal cells could allow the virus to pass through maternal–fetal barrier. Additionally, as observed for hepatitis B virus and herpesvirus, under certain immunosuppressive conditions, there can be an increase in the passage of lymphocytes carrying latent HPV through the maternal–fetal barrier [28]. HPV trophoblast infection has been described in different studies [25, 30,31]. Furthermore, You et al [32] demonstrated in vitro that trophoblast cells are broadly permissive for HPV and that this virus is able to complete its life cycle in trophoblast cell cultures. PERINATAL TRANSMISSION In this section, perinatal transmission will be considered as the result of the fetus coming into contact with infected cells of the vagina and cervix during birth. Some authors have demonstrated that there is both an increased rate of HPV detection among newborns by vaginal delivery (51.4%), compared to those delivered by cesarean section (27.3%) [33] and an increased incidence of juvenile respiratory papillomatosis after prolonged delivery (>10 hours) [34]. At the same time, Tenti et al [35] observed a low potential for viral transmission to the oropharyngeal mucosa of newborns from mothers without changes iThe view that a cesarean delivery provides protection against the transmission of neonatal herpes in pregnant women with obvious injuries has led to the suggestion that this procedure can be adopted for perinatal pregnant women with genital warts [27]. However, there is no clear consensus about the degree of protection that cesarean delivery can offer against maternal–fetal transmission of HPV [2]. This lack of agreement is based on 3 hypotheses: (1) the risk of disease transmission would be low; (2) a cesarean delivery does not ensure complete protection, because papillomatosis transmission has even been observed in elective cesarean delivery; and (3) the risks resulting from a cesarean section are greater than the potential benefits [5, 34]. In rare circumstances, the cesarean is recommended for women with genital warts that cause obstruction in the birth canal, or in cases where vaginal delivery will result in excessive bleeding due to laceration of the warty lesions [27].n oncotic colpocytology or a history of genital warts.
 when the mother is shown to be HPV positive. Additionally, the risk of the newborn having the same HPV type as that found in the maternal genital tract is 4 times greater when the umbilical cord blood is positive for the same HPV [25]. Evidence from the cervical samples indicates that mothers who transmit HPV to their infants have a higher viral load than those who do not [26]. Sarkola et al [25] reported that peripheral blood samples from all mothers who had HPV in the placenta and umbilical cord tested negative for HPV. According to these authors, the detection of viral DNA in their samples appears to be due to a maternal history of productive infection and not the detection of viral genetic material during pregnancy. However, there remains the possibility that HPV infected the placenta during early pregnancy and had already cleared the cervix at the time of delivery [2]. During pregnancy, the uterine canal undergoes anatomic and immunologic changes that may increase the susceptibility of pregnant women to infections [27]. In addition to other human viruses such as HIV, cytomegalovirus, and Epstein-Barr virus, HPV may be able to infect the placenta or cells of fetal origin [28]. The transplacental transmission of HIV and maternal cells, including lymphocytes, is a phenomenon that has already been described and can be stimulated by pathologic conditions [28, 29]. Reports of the presence of HPV in polymorphonuclear cells suggest that the transfer of maternal cells could allow the virus to pass through maternal–fetal barrier. Additionally, as observed for hepatitis B virus and herpesvirus, under certain immunosuppressive conditions, there can be an increase in the passage of lymphocytes carrying latent HPV through the maternal–fetal barrier [28]. HPV trophoblast infection has been described in different studies [25, 30,31]. Furthermore, You et al [32] demonstrated in vitro that trophoblast cells are broadly permissive for HPV and that this virus is able to complete its life cycle in trophoblast cell cultures. PERINATAL TRANSMISSION. In this section, perinatal transmission will be considered as the result of the fetus coming into contact with infected cells of the vagina and cervix during birth. Some authors have demonstrated that there is both an increased rate of HPV detection among newborns by vaginal delivery (51.4%), compared to those delivered by cesarean section (27.3%) [33] and an increased incidence of juvenile respiratory papillomatosis after prolonged delivery (>10 hours) [34]. At the same time, Tenti et al [35] observed a low potential for viral transmission to the oropharyngeal mucosa of newborns from mothers without changes iThe view that a cesarean delivery provides protection against the transmission of neonatal herpes in pregnant women with obvious injuries has led to the suggestion that this procedure can be adopted for perinatal pregnant women with genital warts [27]. However, there is no clear consensus about the degree of protection that cesarean delivery can offer against maternal–fetal transmission of HPV [2]. This lack of agreement is based on 3 hypotheses: (1) the risk of disease transmission would be low; (2) a cesarean delivery does not ensure complete protection, because papillomatosis transmission has even been observed in elective cesarean delivery; and (3) the risks resulting from a cesarean section are greater than the potential benefits [5, 34]. In rare circumstances, the cesarean is recommended for women with genital warts that cause obstruction in the birth canal, or in cases where vaginal delivery will result in excessive bleeding due to laceration of the warty lesions [27].n oncotic colpocytology or a history of genital warts.")
6
Vertikal Geçiş (Olası Mekanizmalar)
Prenatal geçiş (intrauterin geçiş) Doğumda bebeklerde HPV lezyonlarının bulunması HPV DNA’sının amniyotik sıvı, plasenta ve umbilikal kordda saptanması Koryonik ve plasental doku hematojen yolla enfekte olup amniyona geçebilir ve fetus bunu oral alabilir Asendan olarak transplasental enfeksiyon olabilir POSSIBLE MECHANISMS OF HPV VERTICAL TRANSMISSION Although HPV DNA has been detected in different sites of the male reproductive tract [8–10], sperm cells [4, 11, 12], semen [13, 14], endometrium, and ovaries [15], which suggests that HPV could be transmitted during the fertilization of an oocyte or immediately afterward, the significance of these findings is still unknown. In vitro analyses have indicated the viability of HPV infection in spermatozoids and the transcription of HPV genes in fecund oocytes [8–10, 16–20], and the transcriptional activity of HPV-16 in sperm was confirmed in vivo [21]. However, further investigations are necessary to confirm this route of transmission. For this reason, the discussion about the possible mechanisms of HPV vertical transmission will center on the prenatal and perinatal routes, which are better understood. RENATAL TRANSMISSION The observation of infants showing signs of HPV-induced lesions at birth, such as laryngeal and anogenital lesions, has led to the belief that intrauterine HPV transmission can occur [22, 23]. HPV DNA has been detected in amniotic fluid [3], placenta, and the umbilical cord [7]. Both chorionic and placental tissue can be infected through the hematogenous route and hence, HPV can be spread to amniotic cells that are then ingested by the fetus [2, 3]. Transplacental infection, another possible means of HPV intrauterine transmission, can occur through the ascending route from the maternal genital tract, as it has been shown that the presence of HPV-DNA, both in amniotic fluid [3] and the umbilical cord [2], is correlated with cervical intraepithelial lesions in pregnant women. Once believed to be low, the HPV vertical transmission rate has shown inconsistent results, probably due to the heterogeneous nature of the clinical trials [24]. Despite this, in a systematic quantitative review, Medeiros et al [24] reported a pooled relative risk of mother-to-child HPV transmission (4.8) when the mother is shown to be HPV positive. Additionally, the risk of the newborn having the same HPV type as that found in the maternal genital tract is 4 times greater when the umbilical cord blood is positive for the same HPV [25]. Evidence from the cervical samples indicates that mothers who transmit HPV to their infants have a higher viral load than those who do not [26]. Sarkola et al [25] reported that peripheral blood samples from all mothers who had HPV in the placenta and umbilical cord tested negative for HPV. According to these authors, the detection of viral DNA in their samples appears to be due to a maternal history of productive infection and not the detection of viral genetic material during pregnancy. However, there remains the possibility that HPV infected the placenta during early pregnancy and had already cleared the cervix at the time of delivery [2]. During pregnancy, the uterine canal undergoes anatomic and immunologic changes that may increase the susceptibility of pregnant women to infections [27]. In addition to other human viruses such as HIV, cytomegalovirus, and Epstein-Barr virus, HPV may be able to infect the placenta or cells of fetal origin [28]. The transplacental transmission of HIV and maternal cells, including lymphocytes, is a phenomenon that has already been described and can be stimulated by pathologic conditions [28, 29]. Reports of the presence of HPV in polymorphonuclear cells suggest that the transfer of maternal cells could allow the virus to pass through maternal–fetal barrier. Additionally, as observed for hepatitis B virus and herpesvirus, under certain immunosuppressive conditions, there can be an increase in the passage of lymphocytes carrying latent HPV through the maternal–fetal barrier [28]. HPV trophoblast infection has been described in different studies [25, 30,31]. Furthermore, You et al [32] demonstrated in vitro that trophoblast cells are broadly permissive for HPV and that this virus is able to complete its life cycle in trophoblast cell cultures. PERINATAL TRANSMISSION In this section, perinatal transmission will be considered as the result of the fetus coming into contact with infected cells of the vagina and cervix during birth. Some authors have demonstrated that there is both an increased rate of HPV detection among newborns by vaginal delivery (51.4%), compared to those delivered by cesarean section (27.3%) [33] and an increased incidence of juvenile respiratory papillomatosis after prolonged delivery (>10 hours) [34]. At the same time, Tenti et al [35] observed a low potential for viral transmission to the oropharyngeal mucosa of newborns from mothers without changes iThe view that a cesarean delivery provides protection against the transmission of neonatal herpes in pregnant women with obvious injuries has led to the suggestion that this procedure can be adopted for perinatal pregnant women with genital warts [27]. However, there is no clear consensus about the degree of protection that cesarean delivery can offer against maternal–fetal transmission of HPV [2]. This lack of agreement is based on 3 hypotheses: (1) the risk of disease transmission would be low; (2) a cesarean delivery does not ensure complete protection, because papillomatosis transmission has even been observed in elective cesarean delivery; and (3) the risks resulting from a cesarean section are greater than the potential benefits [5, 34]. In rare circumstances, the cesarean is recommended for women with genital warts that cause obstruction in the birth canal, or in cases where vaginal delivery will result in excessive bleeding due to laceration of the warty lesions [27].n oncotic colpocytology or a history of genital warts.
 Doğumda bebeklerde HPV lezyonlarının bulunması. HPV DNA’sının amniyotik sıvı, plasenta ve umbilikal kordda saptanması. Koryonik ve plasental doku hematojen yolla enfekte olup amniyona geçebilir ve fetus bunu oral alabilir. Asendan olarak transplasental enfeksiyon olabilir. POSSIBLE MECHANISMS OF HPV VERTICAL TRANSMISSION. Although HPV DNA has been detected in different sites of the male reproductive tract [8–10], sperm cells [4, 11, 12], semen [13, 14], endometrium, and ovaries [15], which suggests that HPV could be transmitted during the fertilization of an oocyte or immediately afterward, the significance of these findings is still unknown. In vitro analyses have indicated the viability of HPV infection in spermatozoids and the transcription of HPV genes in fecund oocytes [8–10, 16–20], and the transcriptional activity of HPV-16 in sperm was confirmed in vivo [21]. However, further investigations are necessary to confirm this route of transmission. For this reason, the discussion about the possible mechanisms of HPV vertical transmission will center on the prenatal and perinatal routes, which are better understood. RENATAL TRANSMISSION. The observation of infants showing signs of HPV-induced lesions at birth, such as laryngeal and anogenital lesions, has led to the belief that intrauterine HPV transmission can occur [22, 23]. HPV DNA has been detected in amniotic fluid [3], placenta, and the umbilical cord [7]. Both chorionic and placental tissue can be infected through the hematogenous route and hence, HPV can be spread to amniotic cells that are then ingested by the fetus [2, 3]. Transplacental infection, another possible means of HPV intrauterine transmission, can occur through the ascending route from the maternal genital tract, as it has been shown that the presence of HPV-DNA, both in amniotic fluid [3] and the umbilical cord [2], is correlated with cervical intraepithelial lesions in pregnant women. Once believed to be low, the HPV vertical transmission rate has shown inconsistent results, probably due to the heterogeneous nature of the clinical trials [24]. Despite this, in a systematic quantitative review, Medeiros et al [24] reported a pooled relative risk of mother-to-child HPV transmission (4.8) when the mother is shown to be HPV positive. Additionally, the risk of the newborn having the same HPV type as that found in the maternal genital tract is 4 times greater when the umbilical cord blood is positive for the same HPV [25]. Evidence from the cervical samples indicates that mothers who transmit HPV to their infants have a higher viral load than those who do not [26]. Sarkola et al [25] reported that peripheral blood samples from all mothers who had HPV in the placenta and umbilical cord tested negative for HPV. According to these authors, the detection of viral DNA in their samples appears to be due to a maternal history of productive infection and not the detection of viral genetic material during pregnancy. However, there remains the possibility that HPV infected the placenta during early pregnancy and had already cleared the cervix at the time of delivery [2]. During pregnancy, the uterine canal undergoes anatomic and immunologic changes that may increase the susceptibility of pregnant women to infections [27]. In addition to other human viruses such as HIV, cytomegalovirus, and Epstein-Barr virus, HPV may be able to infect the placenta or cells of fetal origin [28]. The transplacental transmission of HIV and maternal cells, including lymphocytes, is a phenomenon that has already been described and can be stimulated by pathologic conditions [28, 29]. Reports of the presence of HPV in polymorphonuclear cells suggest that the transfer of maternal cells could allow the virus to pass through maternal–fetal barrier. Additionally, as observed for hepatitis B virus and herpesvirus, under certain immunosuppressive conditions, there can be an increase in the passage of lymphocytes carrying latent HPV through the maternal–fetal barrier [28]. HPV trophoblast infection has been described in different studies [25, 30,31]. Furthermore, You et al [32] demonstrated in vitro that trophoblast cells are broadly permissive for HPV and that this virus is able to complete its life cycle in trophoblast cell cultures. PERINATAL TRANSMISSION. In this section, perinatal transmission will be considered as the result of the fetus coming into contact with infected cells of the vagina and cervix during birth. Some authors have demonstrated that there is both an increased rate of HPV detection among newborns by vaginal delivery (51.4%), compared to those delivered by cesarean section (27.3%) [33] and an increased incidence of juvenile respiratory papillomatosis after prolonged delivery (>10 hours) [34]. At the same time, Tenti et al [35] observed a low potential for viral transmission to the oropharyngeal mucosa of newborns from mothers without changes iThe view that a cesarean delivery provides protection against the transmission of neonatal herpes in pregnant women with obvious injuries has led to the suggestion that this procedure can be adopted for perinatal pregnant women with genital warts [27]. However, there is no clear consensus about the degree of protection that cesarean delivery can offer against maternal–fetal transmission of HPV [2]. This lack of agreement is based on 3 hypotheses: (1) the risk of disease transmission would be low; (2) a cesarean delivery does not ensure complete protection, because papillomatosis transmission has even been observed in elective cesarean delivery; and (3) the risks resulting from a cesarean section are greater than the potential benefits [5, 34]. In rare circumstances, the cesarean is recommended for women with genital warts that cause obstruction in the birth canal, or in cases where vaginal delivery will result in excessive bleeding due to laceration of the warty lesions [27].n oncotic colpocytology or a history of genital warts.")
7
Vertikal Geçiş (Olası Mekanizmalar)
Perinatal (doğumda) Fetusun doğum sırasında vajina ve serviksteki enfekte hücrelerle temasıyla geçiş Vajinal doğumda sezaryene göre daha sık Uzamış doğumda (>10 saat) daha sık Sezaryen olan annelerin bebeklerinde de görülebilir POSSIBLE MECHANISMS OF HPV VERTICAL TRANSMISSION Although HPV DNA has been detected in different sites of the male reproductive tract [8–10], sperm cells [4, 11, 12], semen [13, 14], endometrium, and ovaries [15], which suggests that HPV could be transmitted during the fertilization of an oocyte or immediately afterward, the significance of these findings is still unknown. In vitro analyses have indicated the viability of HPV infection in spermatozoids and the transcription of HPV genes in fecund oocytes [8–10, 16–20], and the transcriptional activity of HPV-16 in sperm was confirmed in vivo [21]. However, further investigations are necessary to confirm this route of transmission. For this reason, the discussion about the possible mechanisms of HPV vertical transmission will center on the prenatal and perinatal routes, which are better understood. RENATAL TRANSMISSION The observation of infants showing signs of HPV-induced lesions at birth, such as laryngeal and anogenital lesions, has led to the belief that intrauterine HPV transmission can occur [22, 23]. HPV DNA has been detected in amniotic fluid [3], placenta, and the umbilical cord [7]. Both chorionic and placental tissue can be infected through the hematogenous route and hence, HPV can be spread to amniotic cells that are then ingested by the fetus [2, 3]. Transplacental infection, another possible means of HPV intrauterine transmission, can occur through the ascending route from the maternal genital tract, as it has been shown that the presence of HPV-DNA, both in amniotic fluid [3] and the umbilical cord [2], is correlated with cervical intraepithelial lesions in pregnant women. Once believed to be low, the HPV vertical transmission rate has shown inconsistent results, probably due to the heterogeneous nature of the clinical trials [24]. Despite this, in a systematic quantitative review, Medeiros et al [24] reported a pooled relative risk of mother-to-child HPV transmission (4.8) when the mother is shown to be HPV positive. Additionally, the risk of the newborn having the same HPV type as that found in the maternal genital tract is 4 times greater when the umbilical cord blood is positive for the same HPV [25]. Evidence from the cervical samples indicates that mothers who transmit HPV to their infants have a higher viral load than those who do not [26]. Sarkola et al [25] reported that peripheral blood samples from all mothers who had HPV in the placenta and umbilical cord tested negative for HPV. According to these authors, the detection of viral DNA in their samples appears to be due to a maternal history of productive infection and not the detection of viral genetic material during pregnancy. However, there remains the possibility that HPV infected the placenta during early pregnancy and had already cleared the cervix at the time of delivery [2]. During pregnancy, the uterine canal undergoes anatomic and immunologic changes that may increase the susceptibility of pregnant women to infections [27]. In addition to other human viruses such as HIV, cytomegalovirus, and Epstein-Barr virus, HPV may be able to infect the placenta or cells of fetal origin [28]. The transplacental transmission of HIV and maternal cells, including lymphocytes, is a phenomenon that has already been described and can be stimulated by pathologic conditions [28, 29]. Reports of the presence of HPV in polymorphonuclear cells suggest that the transfer of maternal cells could allow the virus to pass through maternal–fetal barrier. Additionally, as observed for hepatitis B virus and herpesvirus, under certain immunosuppressive conditions, there can be an increase in the passage of lymphocytes carrying latent HPV through the maternal–fetal barrier [28]. HPV trophoblast infection has been described in different studies [25, 30,31]. Furthermore, You et al [32] demonstrated in vitro that trophoblast cells are broadly permissive for HPV and that this virus is able to complete its life cycle in trophoblast cell cultures. PERINATAL TRANSMISSION In this section, perinatal transmission will be considered as the result of the fetus coming into contact with infected cells of the vagina and cervix during birth. Some authors have demonstrated that there is both an increased rate of HPV detection among newborns by vaginal delivery (51.4%), compared to those delivered by cesarean section (27.3%) [33] and an increased incidence of juvenile respiratory papillomatosis after prolonged delivery (>10 hours) [34]. At the same time, Tenti et al [35] observed a low potential for viral transmission to the oropharyngeal mucosa of newborns from mothers without changes I The view that a cesarean delivery provides protection against the transmission of neonatal herpes in pregnant women with obvious injuries has led to the suggestion that this procedure can be adopted for perinatal pregnant women with genital warts [27]. However, there is no clear consensus about the degree of protection that cesarean delivery can offer against maternal–fetal transmission of HPV [2]. This lack of agreement is based on 3 hypotheses: (1) the risk of disease transmission would be low; (2) a cesarean delivery does not ensure complete protection, because papillomatosis transmission has even been observed in elective cesarean delivery; and (3) the risks resulting from a cesarean section are greater than the potential benefits [5, 34]. In rare circumstances, the cesarean is recommended for women with genital warts that cause obstruction in the birth canal, or in cases where vaginal delivery will result in excessive bleeding due to laceration of the warty lesions [27].n oncotic colpocytology or a history of genital warts.
 Fetusun doğum sırasında vajina ve serviksteki enfekte hücrelerle temasıyla geçiş. Vajinal doğumda sezaryene göre daha sık. Uzamış doğumda (>10 saat) daha sık. Sezaryen olan annelerin bebeklerinde de görülebilir. POSSIBLE MECHANISMS OF HPV VERTICAL TRANSMISSION. Although HPV DNA has been detected in different sites of the male reproductive tract [8–10], sperm cells [4, 11, 12], semen [13, 14], endometrium, and ovaries [15], which suggests that HPV could be transmitted during the fertilization of an oocyte or immediately afterward, the significance of these findings is still unknown. In vitro analyses have indicated the viability of HPV infection in spermatozoids and the transcription of HPV genes in fecund oocytes [8–10, 16–20], and the transcriptional activity of HPV-16 in sperm was confirmed in vivo [21]. However, further investigations are necessary to confirm this route of transmission. For this reason, the discussion about the possible mechanisms of HPV vertical transmission will center on the prenatal and perinatal routes, which are better understood. RENATAL TRANSMISSION. The observation of infants showing signs of HPV-induced lesions at birth, such as laryngeal and anogenital lesions, has led to the belief that intrauterine HPV transmission can occur [22, 23]. HPV DNA has been detected in amniotic fluid [3], placenta, and the umbilical cord [7]. Both chorionic and placental tissue can be infected through the hematogenous route and hence, HPV can be spread to amniotic cells that are then ingested by the fetus [2, 3]. Transplacental infection, another possible means of HPV intrauterine transmission, can occur through the ascending route from the maternal genital tract, as it has been shown that the presence of HPV-DNA, both in amniotic fluid [3] and the umbilical cord [2], is correlated with cervical intraepithelial lesions in pregnant women. Once believed to be low, the HPV vertical transmission rate has shown inconsistent results, probably due to the heterogeneous nature of the clinical trials [24]. Despite this, in a systematic quantitative review, Medeiros et al [24] reported a pooled relative risk of mother-to-child HPV transmission (4.8) when the mother is shown to be HPV positive. Additionally, the risk of the newborn having the same HPV type as that found in the maternal genital tract is 4 times greater when the umbilical cord blood is positive for the same HPV [25]. Evidence from the cervical samples indicates that mothers who transmit HPV to their infants have a higher viral load than those who do not [26]. Sarkola et al [25] reported that peripheral blood samples from all mothers who had HPV in the placenta and umbilical cord tested negative for HPV. According to these authors, the detection of viral DNA in their samples appears to be due to a maternal history of productive infection and not the detection of viral genetic material during pregnancy. However, there remains the possibility that HPV infected the placenta during early pregnancy and had already cleared the cervix at the time of delivery [2]. During pregnancy, the uterine canal undergoes anatomic and immunologic changes that may increase the susceptibility of pregnant women to infections [27]. In addition to other human viruses such as HIV, cytomegalovirus, and Epstein-Barr virus, HPV may be able to infect the placenta or cells of fetal origin [28]. The transplacental transmission of HIV and maternal cells, including lymphocytes, is a phenomenon that has already been described and can be stimulated by pathologic conditions [28, 29]. Reports of the presence of HPV in polymorphonuclear cells suggest that the transfer of maternal cells could allow the virus to pass through maternal–fetal barrier. Additionally, as observed for hepatitis B virus and herpesvirus, under certain immunosuppressive conditions, there can be an increase in the passage of lymphocytes carrying latent HPV through the maternal–fetal barrier [28]. HPV trophoblast infection has been described in different studies [25, 30,31]. Furthermore, You et al [32] demonstrated in vitro that trophoblast cells are broadly permissive for HPV and that this virus is able to complete its life cycle in trophoblast cell cultures. PERINATAL TRANSMISSION. In this section, perinatal transmission will be considered as the result of the fetus coming into contact with infected cells of the vagina and cervix during birth. Some authors have demonstrated that there is both an increased rate of HPV detection among newborns by vaginal delivery (51.4%), compared to those delivered by cesarean section (27.3%) [33] and an increased incidence of juvenile respiratory papillomatosis after prolonged delivery (>10 hours) [34]. At the same time, Tenti et al [35] observed a low potential for viral transmission to the oropharyngeal mucosa of newborns from mothers without changes I. The view that a cesarean delivery provides protection against the transmission of neonatal herpes in pregnant women with obvious injuries has led to the suggestion that this procedure can be adopted for perinatal pregnant women with genital warts [27]. However, there is no clear consensus about the degree of protection that cesarean delivery can offer against maternal–fetal transmission of HPV [2]. This lack of agreement is based on 3 hypotheses: (1) the risk of disease transmission would be low; (2) a cesarean delivery does not ensure complete protection, because papillomatosis transmission has even been observed in elective cesarean delivery; and (3) the risks resulting from a cesarean section are greater than the potential benefits [5, 34]. In rare circumstances, the cesarean is recommended for women with genital warts that cause obstruction in the birth canal, or in cases where vaginal delivery will result in excessive bleeding due to laceration of the warty lesions [27].n oncotic colpocytology or a history of genital warts.")
8
Geçiş Hızı Anne ve bebek arasında HPV genotipleri açısından %71 konkordans (Smith, 2010) HPV klinik bulgusu olmayan kadınlarda yenidoğana HPV geçiş hızı %1–18 (Rombaldi, 2009; Watts 1998; Smith, 2004) Gebelikte saptanabilir HPV (HPV klinik bulgusu veya servikal örneklerde HPV DNA pozitifliği) olan kadınlarda geçiş hızı %5-72 (Rombaldi, 2009; Smith 1995; Fredericks 1993) Vertical transmission of HR-HPV has been demonstrated when the maternal HPV type is concordant with the HPV type isolated from the newborn. In a large study, Smith found a 71% concordance rate of HPV genotypes in mother-baby pairs. They also found a high concordance (93%) and a low discordance rate when maternal and neonatal antibodies to HPV virus-like particles were analyzed. 37 Rombaldi and Gajewska estimate that the prevalence of HPV in pregnant women is 25%. 38 39 Several studies have evaluated the rate at which HPV is transmitted from mother to child, but the reported rates of transmission vary. Reported rates of transmission of HPV in women without clinical evidence of HPV to the neonate range from 1–18%. 38 40 41 Watts reported a 1% transmission rate of HPV in infants who were born to women without clinical evidence of HPV or the presence of HPV DNA.40 Smith et al found similar rates of transmission in their study population of 203 infants born from 198 women. Of the 203 infants, two had detectable HPV in oral or genital swabs. 41 42 At the other end of the spectrum, Fredericks detected HPV DNA in 1/19 (a transmission rate of 5%) infants born from 19 women who had HPV negative cervical swabs. 43 Pararkain detected HPV in either buccal or genital swabs in 9% (1/11) of infants born to women without evidence of HPV in cervical swabs using PCR. This number increased to 18% when the infant were examined six weeks later. 44 The rate of transmission was also examined in infants whose mothers had clinically evidence of HPV or cervical samples that were positive for HPV DNA at delivery. In women who had detectable HPV during pregnancy, reported HPV transmission rates range from 5–72%. 38 42 43 Kaye et al studied 15 pregnant women known to be positive for HPV 16, 8 women had infants that had HPV DNA at birth. The eight women had higher viral loads (3.5 to 5 × 10 6 copies per PCR sample) compared with the 7 women who did not (17–195 copies per PCR sample). 46
 Gebelikte saptanabilir HPV (HPV klinik bulgusu veya servikal örneklerde HPV DNA pozitifliği) olan kadınlarda geçiş hızı %5-72 (Rombaldi, 2009; Smith 1995; Fredericks 1993) Vertical transmission of HR-HPV has been demonstrated when the maternal HPV type is concordant with the HPV type isolated from the newborn. In a large study, Smith found a 71% concordance rate of HPV genotypes in mother-baby pairs. They also found a high concordance (93%) and a low discordance rate when maternal and neonatal antibodies to HPV virus-like particles were analyzed. 37. Rombaldi and Gajewska estimate that the prevalence of HPV in pregnant women is 25% Several studies have evaluated the rate at which HPV is transmitted from mother to child, but the reported rates of transmission vary. Reported rates of transmission of HPV in women without clinical evidence of HPV to the neonate range from 1–18% Watts reported a 1% transmission rate of HPV in infants who were born to women without clinical evidence of HPV or the presence of HPV DNA.40 Smith et al found similar rates of transmission in their study population of 203 infants born from 198 women. Of the 203 infants, two had detectable HPV in oral or genital swabs At the other end of the spectrum, Fredericks detected HPV DNA in 1/19 (a transmission rate of 5%) infants born from 19 women who had HPV negative cervical swabs. 43 Pararkain detected HPV in either buccal or genital swabs in 9% (1/11) of infants born to women without evidence of HPV in cervical swabs using PCR. This number increased to 18% when the infant were examined six weeks later. 44. The rate of transmission was also examined in infants whose mothers had clinically evidence of HPV or cervical samples that were positive for HPV DNA at delivery. In women who had detectable HPV during pregnancy, reported HPV transmission rates range from 5–72% Kaye et al studied 15 pregnant women known to be positive for HPV 16, 8 women had infants that had HPV DNA at birth. The eight women had higher viral loads (3.5 to 5 × 10 6 copies per PCR sample) compared with the 7 women who did not (17–195 copies per PCR sample). 46.")
9
Yüksek viral yükte geçiş daha fazla
Geçiş Hızı HPV 16 (+) olduğu bilinen 15 gebe 8 kadının bebeğinde doğumda HPV DNA (+) 8 kadındaki viral yük (her PCR örneğinde 3.5 to 5 × 106 kopya) saptanmayan 7 kadından daha yüksek (17–195 kopya). Kaye et al studied 15 pregnant women known to be positive for HPV 16, 8 women had infants that had HPV DNA at birth. The eight women had higher viral loads (3.5 to 5 × 10 6 copies per PCR sample) compared with the 7 women who did not (17–195 copies per PCR sample). 46 (Kaye, 1994) Yüksek viral yükte geçiş daha fazla
 olduğu bilinen 15 gebe. 8 kadının bebeğinde doğumda HPV DNA (+) 8 kadındaki viral yük (her PCR örneğinde 3.5 to 5 × 106 kopya) saptanmayan 7 kadından daha yüksek (17–195 kopya). Kaye et al studied 15 pregnant women known to be positive for HPV 16, 8 women had infants that had HPV DNA at birth. The eight women had higher viral loads (3.5 to 5 × 10 6 copies per PCR sample) compared with the 7 women who did not (17–195 copies per PCR sample). 46. (Kaye, 1994) Yüksek viral yükte geçiş daha fazla.")
10
Geçiş Hızı Vertical transmission of the human papillomavirus: a systematic quantitative review Medeiros LR, Cad Saude Publica, 2005. In order to clarify the risk of transmission, Medeiros performed a meta-analysis of prospective cohort studies. These studies included pregnant women of all races. 47 Nine studies (conducted from 1994–2004) totaling 2111 women and 2113 offspring were included in the analysis.
 totaling 2111 women and 2113 offspring were included in the analysis.")
11
Anneden bebeğe geçiş riski
Vertical transmission of the human papillomavirus: a systematic quantitative review Medeiros LR, Cad Saude Publica, 2005. In order to clarify the risk of transmission, Medeiros performed a meta-analysis of prospective cohort studies. These studies included pregnant women of all races. 47 Nine studies (conducted from 1994–2004) totaling 2111 women and 2113 offspring were included in the analysis. The estimated prevalence of HPV was 24.3%. The transmission rates in these studies varied from 1.5% to 46.6%. The rate of transmission for the pooled data was 6.5%. The pooled relative risk (RR) was 4.8. Analysis was also conducted on the seven studies that compared vaginal delivery versus cesarean delivery. The RR for HPV transmission was 18% in vaginal delivery compared with 8% in cesarean delivery.
 totaling 2111 women and 2113 offspring were included in the analysis. The estimated prevalence of HPV was 24.3%. The transmission rates in these studies varied from 1.5% to 46.6%. The rate of transmission for the pooled data was 6.5%. The pooled relative risk (RR) was 4.8. Analysis was also conducted on the seven studies that compared vaginal delivery versus cesarean delivery. The RR for HPV transmission was 18% in vaginal delivery compared with 8% in cesarean delivery.")
12
Geçiş Hızı(C/S vs VD) Vajinal vs C/S doğumu karşılaştıran 7 çalışmada
Vertical transmission of the human papillomavirus: a systematic quantitative review Medeiros LR, Cad Saude Publica, 2005. Vajinal vs C/S doğumu karşılaştıran 7 çalışmada HPV geçiş hızı vajinal doğumda %18, sezaryende %8 (RR 1,81)
")
13
Geçiş Hızı (C/S vs VD) HPV DNA-pozitifliği, enfekte maternal hücreler ile kontaminasyonu gösterir enfeksiyonu göstermez (Sadece 1 çalışmada bebekler uzun süre takip edilmiş) Tüm HPV DNA-pozitif annelerde sezaryen doğumu önermek için yeterli kanıt yoktur
 Tüm HPV DNA-pozitif annelerde sezaryen doğumu önermek için yeterli kanıt yoktur.")
14
Jüvenil başlangıçlı Rekürrent Respiratuvar Papillomatosis (JoRRP)
İlk tanımlandıktan (Hayekin 1956) 30 yıl sonra maternal HPV enfeksiyonu bu lezyonlarla ilişkilendirildi HPV-6 & 11’le yenidoğanda oluşur, nadir Obstrüksiyona sekonder respiratuvar distres Tedavi sonrası rekürrens sık. İntrapartum geçiş hızı düşük (enfekte kadınların bebeklerinde RRP 1/1000 olgu) Juvenile onset recurrent laryngeal papillomatosis. First described as a condition in which by Hayekin 1956) Thirty years later, maternal HPV infection was linked to these lesions. 12 22 33 34 Respiratory papillomatosis (laryngeal papilloma) is a rare disease in the neonate that is caused by HPV-6 and HPV-11. Laryngeal papillomas can be particularly troublesome, because they may produce respiratory distress secondary to obstruction and because recurrence after treatment is common. The fact that genital papillomavirus infection is so common and respiratory papillomatosis is rare means that the risk of intrapartum transmission is low, perhaps on the order of 1 case of juvenile respiratory papillomatosis per 1000 children born to infected mothers. Watts and associates 94 reported that, among 151 pregnant women evaluated for HPV by clinical, colposcopic, and PCR tests at less than 20, 34, and 36 weeks of gestation, 112 (74%) had evidence of HPV. HPV was identified in only 3 (4%) of 80 infants born to women with HPV detected at 34 to 36 weeks' gestation, but it also was found in 5 (8%) of 63 infants born to women in whom HPV DNA was not detected. Creasy and Resnik's Maternal-Fetal Medicine: Principles and Practice , Seventh Edition, Robert K. Creasy, Robert Resnik, Jay D. Iams, Charles J. Lockwood, Thomas R. Moore, and Michael F. Greene, 51, e7, Copyright © 2014, 2009, 2004, 1999, 1994, 1989, 1984 by Saunders, an imprint of Elsevier Inc.
 30 yıl sonra maternal HPV enfeksiyonu bu lezyonlarla ilişkilendirildi HPV-6 & 11’le yenidoğanda oluşur, nadir. Obstrüksiyona sekonder respiratuvar distres. Tedavi sonrası rekürrens sık. İntrapartum geçiş hızı düşük. (enfekte kadınların bebeklerinde RRP 1/1000 olgu) Juvenile onset recurrent laryngeal papillomatosis. First described as a condition in which by Hayekin 1956) Thirty years later, maternal HPV infection was linked to these lesions Respiratory papillomatosis (laryngeal papilloma) is a rare disease in the neonate that is caused by HPV-6 and HPV-11. Laryngeal papillomas can be particularly troublesome, because they may produce respiratory distress secondary to obstruction and because recurrence after treatment is common. The fact that genital papillomavirus infection is so common and respiratory papillomatosis is rare means that the risk of intrapartum transmission is low, perhaps on the order of 1 case of juvenile respiratory papillomatosis per 1000 children born to infected mothers. Watts and associates 94 reported that, among 151 pregnant women evaluated for HPV by clinical, colposcopic, and PCR tests at less than 20, 34, and 36 weeks of gestation, 112 (74%) had evidence of HPV. HPV was identified in only 3 (4%) of 80 infants born to women with HPV detected at 34 to 36 weeks gestation, but it also was found in 5 (8%) of 63 infants born to women in whom HPV DNA was not detected. Creasy and Resnik s Maternal-Fetal Medicine: Principles and Practice , Seventh Edition, Robert K. Creasy, Robert Resnik, Jay D. Iams, Charles J. Lockwood, Thomas R. Moore, and Michael F. Greene, 51, e7, Copyright © 2014, 2009, 2004, 1999, 1994, 1989, 1984 by Saunders, an imprint of Elsevier Inc.")
15
Jüvenil başlangıçlı Rekürrent Respiratuvar Papillomatosis (JoRRP)
Cerrahi eksizyon temel tedavi şekli Çoğu etkilenen hastada spontan remisyon. Bazılarında, defalarca cerrahi gereksinimi. Yeni antiviral ilaçlar (e.g., cidofovir) ve önleyici ve terapötik aşılar JoRRP insidansını azaltmada ve hatta virüsün eliminasyonunda umut verici. Genital siğiller çocuklarda olguların %75’inde spontan geriler. Genital HPV infections in pregnant women have long been suspected to cause genital warts or laryngeal papillomatosis in the respective infants. 219 Juvenile laryngeal papillomatosis represents the most common neoplasm of the larynx in infants and young children and usually occurs by age 5. 220 The symptoms range from hoarseness to complete upper airway obstruction. A history of genital warts can be obtained from over 50% of women whose infants subsequently develop laryngeal papillomatosis. 221 However, the absolute risk of laryngeal papillomatosis following exposure to maternal infection is extremely low. Conservative estimates suggest the risk of papillomatosis developing in an offspring of a mother with HPV genital infection is approximately 1 in 400. 220 Surgical excision is the mainstream therapy, and most afflicted patients experience spontaneous remission. However, some endure several hundred surgical procedures. Further development of new antiviral drugs (e.g., cidofovir) and preventive and therapeutic vaccines hold promise for reducing the incidence of recurrent respiratory papillomatosis and, at best, eliminating the virus. 222 , 223 Genital warts in children show spontaneous resolution in up to 75% of cases. In a cohort of 41 children, overall resolution of condylomata was noted in 31 infants (76%), with spontaneous resolution in 22 of 41 (54%); girls were affected three times more often than boys. 224 HPV vaccination should reduce the incidence of vertical HPV transmission. 225 High-Risk Pregnancy , Fourth Edition, David James, Philip J. Steer, Carl P. Weiner, and Bernard Gonik, Chapter 30, e6, Copyright © 2011 by Saunders, an imprint of Elsevier Inc. 219. Sedlaceck TV, Lindheim S, Eder C,et al: Mechanism for human papillomavirus transmission at birth. Am J Obstet Gynecol 1989; 161: 55-59CrossRef 220. Kashima HK, Shah K: Recurrent respiratory papillomatosis: Clinical overview and management principles. Obstet Gynecol Clin North Am 1987; 14: 221. Hallden C, Majmudar B: The relationship between juvenile laryngeal papillomatosis and maternal condylomata acuminata. J Reprod Med 1986; 31: 222. Milczuk HA: Intralesional cidofovir for the treatment of severe juvenile recurrent respiratory papillomatosis: Long-term results in 4 children. Otolaryngol Head Neck Surg 2003; 128: CrossRef 223. Auborn KJ: Therapy for recurrent respiratory papillomatosis. Antivir Ther 2002; 7: 1-9 224. Allen AL, Siegfried EC: The natural history of condylomas in children. J Am Acad Dermatol 1998; 39: CrossRef 225. Markowitz LE, Dunne EF, Saraiya M,et al : Quadrivalent human papillomavirus vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2007; 56: 1-24
 ve önleyici ve terapötik aşılar JoRRP insidansını azaltmada ve hatta virüsün eliminasyonunda umut verici. Genital siğiller çocuklarda olguların %75’inde spontan geriler. Genital HPV infections in pregnant women have long been suspected to cause genital warts or laryngeal papillomatosis in the respective infants. 219 Juvenile laryngeal papillomatosis represents the most common neoplasm of the larynx in infants and young children and usually occurs by age The symptoms range from hoarseness to complete upper airway obstruction. A history of genital warts can be obtained from over 50% of women whose infants subsequently develop laryngeal papillomatosis. 221 However, the absolute risk of laryngeal papillomatosis following exposure to maternal infection is extremely low. Conservative estimates suggest the risk of papillomatosis developing in an offspring of a mother with HPV genital infection is approximately 1 in Surgical excision is the mainstream therapy, and most afflicted patients experience spontaneous remission. However, some endure several hundred surgical procedures. Further development of new antiviral drugs (e.g., cidofovir) and preventive and therapeutic vaccines hold promise for reducing the incidence of recurrent respiratory papillomatosis and, at best, eliminating the virus. 222 , 223 Genital warts in children show spontaneous resolution in up to 75% of cases. In a cohort of 41 children, overall resolution of condylomata was noted in 31 infants (76%), with spontaneous resolution in 22 of 41 (54%); girls were affected three times more often than boys. 224 HPV vaccination should reduce the incidence of vertical HPV transmission High-Risk Pregnancy , Fourth Edition, David James, Philip J. Steer, Carl P. Weiner, and Bernard Gonik, Chapter 30, e6, Copyright © 2011 by Saunders, an imprint of Elsevier Inc Sedlaceck TV, Lindheim S, Eder C,et al: Mechanism for human papillomavirus transmission at birth. Am J Obstet Gynecol 1989; 161: 55-59CrossRef Kashima HK, Shah K: Recurrent respiratory papillomatosis: Clinical overview and management principles. Obstet Gynecol Clin North Am 1987; 14: Hallden C, Majmudar B: The relationship between juvenile laryngeal papillomatosis and maternal condylomata acuminata. J Reprod Med 1986; 31: Milczuk HA: Intralesional cidofovir for the treatment of severe juvenile recurrent respiratory papillomatosis: Long-term results in 4 children. Otolaryngol Head Neck Surg 2003; 128: CrossRef Auborn KJ: Therapy for recurrent respiratory papillomatosis. Antivir Ther 2002; 7: Allen AL, Siegfried EC: The natural history of condylomas in children. J Am Acad Dermatol 1998; 39: CrossRef Markowitz LE, Dunne EF, Saraiya M,et al : Quadrivalent human papillomavirus vaccine: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2007; 56:")
16
Jüvenil başlangıçlı Rekürrent Respiratuvar Papillomatosis (JoRRP)
Risk factors for the development and severity of juvenile-onset recurrent respiratory papillomatosis: a systematic review (Nyibizi et al, 2014, Int J Pediatr Otorhinolaryngol) 2296 JoRRP olgusu (32/116 gözlemsel çalışma) Risk faktörleri çoğunlukla maternal (doğum öyküsü, viral genotip, konak faktörleri) açıdan değerlendirilmiş Gebelikte ve doğumda genital siğil varlığı ile JoRRP arasında kuvvetli ilişki. Etnisiteye de bağlı olarak spesifik HLA class II alelleri ve immun yanıt faktörleri JoRRp varlığı ve şiddeti için önemli determinantlar HPV-11 genotipi ve JoRRP’nin daha erken yaşta başlaması şiddetli hastalığın önemli prediktörleri olarak saptanmış Int J Pediatr Otorhinolaryngol. 2014 Feb;78(2): doi: /j.ijporl Epub 2013 Dec 6. Risk factors for the development and severity of juvenile-onset recurrent respiratory papillomatosis: a systematic review. Niyibizi J1, Rodier C2, Wassef M3, Trottier H4. Author information Abstract OBJECTIVES: Juvenile-onset recurrent respiratory papillomatosis (JoRRP) is a rare yet aggressive disease caused by human papillomavirus (HPV). Although many newborns are likely exposed to HPV, few develop JoRRP and the clinical course of the disease varies from one child to another. This systematic review seeks to provide an up-to-date understanding of the risk factors for acquisition and severity. METHODS: We conducted a comprehensive literature search in EMBASE, MEDLINE and EBMR databases using various combinations of keywords related to JoRRP etiology, risk factors and severity. We also searched Google Scholar and the reference lists of eligible studies. Our search was limited to original studies published in French or English between 1995 and July 2012 and to patients under 20 years of age. RESULT Of 1362 citations, we retrieved 102 articles and found 14 additional studies. We retained 32 studies meeting inclusion criteria. All were observational and together included 2296 JoRRP cases. Risk factors could be classified mainly as maternal and birth history, viral genotype, and host factors. A history of genital warts during pregnancy and delivery was strongly linked to the development of JoRRP. Depending on ethnicity, specific human leukocyte antigen class II alleles and immune response factors were important determinants of JoRRP acquisition and severity. HPV-11 genotype and younger age at onset of JoRRP were important predictors of severity. CONCLUSIONS: Genetic and immunological profiles underlying the acquisition and clinical course are not readily modifiable. Thus, preventing condylomas in women of childbearing age could reduce the burden of this life-threatening disease.
 2296 JoRRP olgusu (32/116 gözlemsel çalışma) Risk faktörleri çoğunlukla maternal (doğum öyküsü, viral genotip, konak faktörleri) açıdan değerlendirilmiş. Gebelikte ve doğumda genital siğil varlığı ile JoRRP arasında kuvvetli ilişki. Etnisiteye de bağlı olarak spesifik HLA class II alelleri ve immun yanıt faktörleri JoRRp varlığı ve şiddeti için önemli determinantlar. HPV-11 genotipi ve JoRRP’nin daha erken yaşta başlaması şiddetli hastalığın önemli prediktörleri olarak saptanmış. Int J Pediatr Otorhinolaryngol Feb;78(2): doi: /j.ijporl Epub 2013 Dec 6. Risk factors for the development and severity of juvenile-onset recurrent respiratory papillomatosis: a systematic review. Niyibizi J1, Rodier C2, Wassef M3, Trottier H4. Author information. Abstract. OBJECTIVES: Juvenile-onset recurrent respiratory papillomatosis (JoRRP) is a rare yet aggressive disease caused by human papillomavirus (HPV). Although many newborns are likely exposed to HPV, few develop JoRRP and the clinical course of the disease varies from one child to another. This systematic review seeks to provide an up-to-date understanding of the risk factors for acquisition and severity. METHODS: We conducted a comprehensive literature search in EMBASE, MEDLINE and EBMR databases using various combinations of keywords related to JoRRP etiology, risk factors and severity. We also searched Google Scholar and the reference lists of eligible studies. Our search was limited to original studies published in French or English between 1995 and July 2012 and to patients under 20 years of age. RESULT. Of 1362 citations, we retrieved 102 articles and found 14 additional studies. We retained 32 studies meeting inclusion criteria. All were observational and together included 2296 JoRRP cases. Risk factors could be classified mainly as maternal and birth history, viral genotype, and host factors. A history of genital warts during pregnancy and delivery was strongly linked to the development of JoRRP. Depending on ethnicity, specific human leukocyte antigen class II alleles and immune response factors were important determinants of JoRRP acquisition and severity. HPV-11 genotype and younger age at onset of JoRRP were important predictors of severity. CONCLUSIONS: Genetic and immunological profiles underlying the acquisition and clinical course are not readily modifiable. Thus, preventing condylomas in women of childbearing age could reduce the burden of this life-threatening disease.")
17
C/S RRP’yi önler mi? Jüvenil başlangıçlı RRP olan olguların çoğu ilk doğum ve vajinal doğmuş bebeklerdir Eylemin 2. evresinin uzun olması ve virüse maruziyet süresinin artması ilk bebekte enfeksiyon riskini artırır (Kashima et al) Düşük sosyokenomik durumlu annelerin bebeklerinde insidans daha fazla HPV vb CTB hastalıklar daha sık ve yeni edinilmiş genital HPV lezyonlarından virüsün yayılması uzun süreli lezyonlara göre daha fazla Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby.
 Düşük sosyokenomik durumlu annelerin bebeklerinde insidans daha fazla. HPV vb CTB hastalıklar daha sık ve yeni edinilmiş genital HPV lezyonlarından virüsün yayılması uzun süreli lezyonlara göre daha fazla. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby.")
18
C/S RRP’yi önler mi? Doğumda genital kondiloma maruz kalan bebeklerin gerçekte çok azında klinik JoRRP gelişir. Doğum kanalında HPV’ye maruz kalan bebeklerin %30’nun nasofaringeal salgılarında HPV saptanmasına karşın çok azında JoRRP gelişir. Diğer faktörler (hasta immunitesi, virüs maruziyetinin zamanlaması, süresi ve miktarı, lokal travma) JoRRP gelişiminde belirleyici rolü olabilir. Despite the close association between maternal condylomata and the development of RRP, only a small portion of children exposed to genital condylomata at birth actually go on to development of clinical RRP. 37 Although HPV could be recovered from the nasopharyngeal secretions of 30% of infants exposed to HPV in the birth canal, the number of infants expected to manifest evidence of RRP is only a small fraction of this population. 37 Clearly, other factors (patient immunity, timing, length and volume of virus exposure, local trauma) must be important determinants in the development of RRP. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby.
 JoRRP gelişiminde belirleyici rolü olabilir. Despite the close association between maternal condylomata and the development of RRP, only a small portion of children exposed to genital condylomata at birth actually go on to development of clinical RRP. 37 Although HPV could be recovered from the nasopharyngeal secretions of 30% of infants exposed to HPV in the birth canal, the number of infants expected to manifest evidence of RRP is only a small fraction of this population. 37 Clearly, other factors (patient immunity, timing, length and volume of virus exposure, local trauma) must be important determinants in the development of RRP. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby.")
19
C/S RRP’yi önler mi? C/S hastalığın geçiş hızını azaltır (daha yüksek maternal morbidite ve mortalite ve daha fazla ekonomik yük) Geçiş in utero olabilir Bebekler C/S’ye rağmen farklı HPV suşları iIe enfekte olabilirler Even though cesarean section delivery would seem to reduce the risk of transmission of the disease, this procedure is associated with a higher morbidity and mortality for the mother and a much higher economic cost than elective vaginal delivery. Furthermore, reports of neonatal papillomatosis suggest that, in at least some cases, transmission may occur in utero. 1 However, with such a high rate of subclinical maternal HPV infection and such a low rate of actual new cases of childhood RRP, elective cesarean delivery as a means of preventing RRP is currently not practical or recommended. 1 The risk of a child contracting the disease from a mother who has an active genital condyloma lesion during vaginal delivery is only approximately 1 in 231 to 400. 22. 34. 36. The characteristics that distinguish this one child from the other 230 to 399 remain elusive. In summary, a better understanding of the risk factors associated with RRP is needed before the efficacy of cesarean delivery or other preventive measures can be fully assessed. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby. Yüksek subklinik maternal HPV enfeksiyonu ve yeni JoRRP oranının gerçekte çok düşük olması nedeniyle RRP’yi önlemek için C/S yapılmasını öngören yeterli veri yoktur ve önerilmez.

20
RRP için risk faktörlerinin tam olarak anlaşılması gerekir
C/S RRP’yi önler mi? Aktif genital kondilomu olan annenin çocuğunda vajinal doğum sırasında RRP gelişme 1 / Bu tek çocuğu diğer çocuktan ayıran özellikler belirsizdir C/S doğumun veya diğer prevantif metodların etkinliğinin belirlenmesi için RRP için risk faktörlerinin tam olarak anlaşılması gerekir Even though cesarean section delivery would seem to reduce the risk of transmission of the disease, this procedure is associated with a higher morbidity and mortality for the mother and a much higher economic cost than elective vaginal delivery. Furthermore, reports of neonatal papillomatosis suggest that, in at least some cases, transmission may occur in utero. 1 However, with such a high rate of subclinical maternal HPV infection and such a low rate of actual new cases of childhood RRP, elective cesarean delivery as a means of preventing RRP is currently not practical or recommended. 1 The risk of a child contracting the disease from a mother who has an active genital condyloma lesion during vaginal delivery is only approximately 1 in 231 to 400. 22. 34. 36. The characteristics that distinguish this one child from the other 230 to 399 remain elusive. In summary, a better understanding of the risk factors associated with RRP is needed before the efficacy of cesarean delivery or other preventive measures can be fully assessed. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby.

21
C/S RRP’yi önler mi? C/S pelvik çıkışı tıkayan genital siğili olan kadınlarda veya vajinal doğum aşırı kanamaya yol açma olasılığı varsa endikedir. Even though cesarean section delivery would seem to reduce the risk of transmission of the disease, this procedure is associated with a higher morbidity and mortality for the mother and a much higher economic cost than elective vaginal delivery. Furthermore, reports of neonatal papillomatosis suggest that, in at least some cases, transmission may occur in utero. 1 However, with such a high rate of subclinical maternal HPV infection and such a low rate of actual new cases of childhood RRP, elective cesarean delivery as a means of preventing RRP is currently not practical or recommended. 1 The risk of a child contracting the disease from a mother who has an active genital condyloma lesion during vaginal delivery is only approximately 1 in 231 to 400. 22. 34. 36. The characteristics that distinguish this one child from the other 230 to 399 remain elusive. In summary, a better understanding of the risk factors associated with RRP is needed before the efficacy of cesarean delivery or other preventive measures can be fully assessed. Cummings Otolaryngology Head & Neck Surgery , Fifth Edition, Paul W. Flint, CHAPTER 204, , 2010, Mosby. Centers for Disease Control and Prevention (CDC). Genital warts. In: Sexually transmitted diseases treatment guidelines, MMWR Recomm Rep 2010 Dec 17;59(RR-12):70-4.
. Genital warts. In: Sexually transmitted diseases treatment guidelines, MMWR Recomm Rep 2010 Dec 17;59(RR-12):70-4.")
22
Gebeliğin HPV enfeksiyonuna etkisi
Endoservikal epitelin eversiyonu → vajina asiditesine maruziyet → artmış skuamöz metaplazi (HPV üremesi ve hücreleri transforme etmesi için artmış selüler akitvite gerekir) Immunosupresif durumlar → HPV viral düzeylerinde artış ve HPV’ye bağlı CIN lezyonlarının daha hızlı progresyonu. Kondilomlar da gebelikte artar. Eversion of the endocervical epithelium results in exposure to the acidity of the vaginal environment, producing a high degree of squamous metaplasia. This metaplasia is important because HPV requires active cellular machinery to reproduce and transform cells. Immunosuppressive states result in increased viral titers of HPV and more rapid progression of HPV disease–associated cervical intraepithelial neoplasia (CIN).
 Immunosupresif durumlar. → HPV viral düzeylerinde artış ve HPV’ye bağlı CIN lezyonlarının daha hızlı progresyonu. Kondilomlar da gebelikte artar. Eversion of the endocervical epithelium results in exposure to the acidity of the vaginal environment, producing a high degree of squamous metaplasia. This metaplasia is important because HPV requires active cellular machinery to reproduce and transform cells. Immunosuppressive states result in increased viral titers of HPV and more rapid progression of HPV disease–associated cervical intraepithelial neoplasia (CIN).")
23
Gebelikte HPV Prevalansı değişir mi?
The prevalence and risk of human papillomavirus infection in pregnant women (Liu et al, 2014, meta-analiz) Kriterlere uygun 28 çalışma, gebe → Gebelerde HPV prevalansı %16,82, yaşa göre eşleştirilmiş gebe olmayan kadınlarda %12,25 → Trimesterlerde prevalans sırasıyla %18,20 - % 14,38 ve %19,32 → HPV 16 en sık görülen tip (prevalans %3,86) HPV prevalansı çalışılan bölgeye, yaşa ve HPV tipine göre farklılık gösteriyor The prevalence and risk of human papillomavirus infection in pregnant women P. LIUa1, L. XUa2, Y. SUNa1 and Z. WANGa1 c1 a1 Department of Epidemiology and Health Statistics, School of Public Health, Shandong University, Shandong, P.R. China a2 Department of Health, Jinan Maternal and Child Care Service Centre, Shandong, P.R. China SUMMARY A series of observational studies were evaluated concerning the risk of human papillomavirus (HPV) infection in pregnancy; however, the results were controversial. We systematically reviewed and collected data on studies regarding HPV prevalence published up to 30 April 2013, in which HPV was detected in pregnant women or both in pregnant and non-pregnant women. In total, 28 eligible studies were included that provided data on HPV infection concerning 13 640 pregnant women. The overall HPV prevalence in pregnant and age-matched non-pregnant women was 16·82% [95% confidence interval (CI) 16·21–17·47] and 12·25% (95% CI 11·50–13·01), respectively. The prevalence in the in three trimesters was 18·20%, 14·38%, and 19·32%, respectively. HPV-16 was the most frequently observed type, with a prevalence of 3·86% (95% CI 3·40–4·32). The overall HPV prevalence varied by study region, age, and HPV type. The meta-analysis showed a significantly increased risk of HPV infection in pregnant women, with a summary odds ratio (OR) of 1·42 (95% CI 1·25–1·61), especially for those aged <25 years (OR 1·79, 95% CI 1·22–2·63). The results suggest that pregnant women, especially those aged <25 years, are more susceptible to HPV infection. Gebede HPV riski anlamlı olarak artar (OR = 1,42) <25 yaş gebelerde risk belirgin artar (OR = 1,79)
 Kriterlere uygun 28 çalışma, gebe. → Gebelerde HPV prevalansı %16,82, yaşa göre eşleştirilmiş gebe olmayan kadınlarda %12,25. → Trimesterlerde prevalans sırasıyla %18,20 - % 14,38 ve %19,32. → HPV 16 en sık görülen tip (prevalans %3,86) HPV prevalansı çalışılan bölgeye, yaşa ve HPV tipine göre farklılık gösteriyor. The prevalence and risk of human papillomavirus infection in pregnant women. P. LIUa1, L. XUa2, Y. SUNa1 and Z. WANGa1 c1. a1 Department of Epidemiology and Health Statistics, School of Public Health, Shandong University, Shandong, P.R. China. a2 Department of Health, Jinan Maternal and Child Care Service Centre, Shandong, P.R. China. SUMMARY. A series of observational studies were evaluated concerning the risk of human papillomavirus (HPV) infection in pregnancy; however, the results were controversial. We systematically reviewed and collected data on studies regarding HPV prevalence published up to 30 April 2013, in which HPV was detected in pregnant women or both in pregnant and non-pregnant women. In total, 28 eligible studies were included that provided data on HPV infection concerning pregnant women. The overall HPV prevalence in pregnant and age-matched non-pregnant women was 16·82% [95% confidence interval (CI) 16·21–17·47] and 12·25% (95% CI 11·50–13·01), respectively. The prevalence in the in three trimesters was 18·20%, 14·38%, and 19·32%, respectively. HPV-16 was the most frequently observed type, with a prevalence of 3·86% (95% CI 3·40–4·32). The overall HPV prevalence varied by study region, age, and HPV type. The meta-analysis showed a significantly increased risk of HPV infection in pregnant women, with a summary odds ratio (OR) of 1·42 (95% CI 1·25–1·61), especially for those aged <25 years (OR 1·79, 95% CI 1·22–2·63). The results suggest that pregnant women, especially those aged <25 years, are more susceptible to HPV infection. Gebede HPV riski anlamlı olarak artar (OR = 1,42) <25 yaş gebelerde risk belirgin artar (OR = 1,79)")
24
HPV’nin Gebeliğe Etkisi
Am J Obstet Gynecol, 2014

26
Am J Reprod Immunol 2014 Am J Reprod Immunol 2014

27
Özet Vertikal geçiş en sık perinatal olmak üzere prenatal ve perikonsepsiyonel olabilir Vajinal doğumda geçiş hızı daha yüksektir. Doğum süresi uzadıkça risk artar. HPV klinik bulgusu olanlarda, viral yük fazla olduğunda, HR-HPV olduğunda geçiş hızı artar. Tüm HPV-DNA + annelerde C/S doğumu önermek için yeterli veri yoktur.

28
Özet JoRRP’yi önlemek için C/S önerilmez (Pelvik çıkışı tıkayan genital siğil varsa veya yaygın kondilomlardan dolayı kanama riski varsa C/S yapılabilir) Gebelikte HPV enfeksiyonunun seyri negatif yönde değişebilir. Gebelikte HPV prevalansı artar, 25 yaş altı gebelerde risk daha fazla. HR-HPV preeklampsi, PROM riski ile ilişkili olabilir.
 Gebelikte HPV enfeksiyonunun seyri negatif yönde değişebilir. Gebelikte HPV prevalansı artar, 25 yaş altı gebelerde risk daha fazla. HR-HPV preeklampsi, PROM riski ile ilişkili olabilir.")
29
Teşekkürler

30
Gebelikte sitolojik ve histolojik anormallikler
HPV Gebelikte sitolojik ve histolojik anormallikler

31
HPV ve ilişkin anormalliklerin tanısı
Sitoloji (Pap smear) Kolposkopi eşliğinde biyopsi HPV DNA (yüksek riskli HPV DNA saptanması) The goal of cytology and colposcopy during pregnancy is to identify invasive cancer that requires treatment before or at the time of delivery. However, unless cancer is identified or suspected, treatment of CIN is contraindicated during pregnancy. 212 HPV isolation in culture is difficult to accomplish. Highly specific and sensitive DNA methods utilizing type-specific HPV gene probes can identify HPV infection in vaginal washings, Pap smears, and amniotic fluid. In situ hybridization technique is useful to demonstrate type-specific HPV infection in tissues and cervical cell scrapings. PCR methods can identify even the lowest levels of HPV infection in blood and other kinds of fluids or in tissue samples. High-Risk Pregnancy , Fourth Edition, David James, Philip J. Steer, Carl P. Weiner, and Bernard Gonik, Chapter 30, e6 Copyright © 2011 by Saunders, an imprint of Elsevier Inc. 95. Workowski KA, Berman SM: Sexually transmitted diseases treatment guidelines, MMWR Recomm Rep 2006; 55: 1-91 212. American College of Obstetricians and Gynecologists : Management of abnormal cervical cytology and histology (ACOG Practice Bulletin No. 99). Obstet Gynecol 2008; 112: CrossRef
 Kolposkopi eşliğinde biyopsi. HPV DNA (yüksek riskli HPV DNA saptanması) The goal of cytology and colposcopy during pregnancy is to identify invasive cancer that requires treatment before or at the time of delivery. However, unless cancer is identified or suspected, treatment of CIN is contraindicated during pregnancy. 212 HPV isolation in culture is difficult to accomplish. Highly specific and sensitive DNA methods utilizing type-specific HPV gene probes can identify HPV infection in vaginal washings, Pap smears, and amniotic fluid. In situ hybridization technique is useful to demonstrate type-specific HPV infection in tissues and cervical cell scrapings. PCR methods can identify even the lowest levels of HPV infection in blood and other kinds of fluids or in tissue samples. High-Risk Pregnancy , Fourth Edition, David James, Philip J. Steer, Carl P. Weiner, and Bernard Gonik, Chapter 30, e6 Copyright © 2011 by Saunders, an imprint of Elsevier Inc. 95. Workowski KA, Berman SM: Sexually transmitted diseases treatment guidelines, MMWR Recomm Rep 2006; 55: American College of Obstetricians and Gynecologists : Management of abnormal cervical cytology and histology (ACOG Practice Bulletin No. 99). Obstet Gynecol 2008; 112: CrossRef.")
32
Sitoloji ve Kolposkopi
Gebelikte sitoloji ve kolposkopinin amacı doğumda veya öncesinde tedavi gerektiren invazif kanseri saptamaktır. Kanser tanısı veya şüphesi olmadıkça gebelikte CIN tedavisi kontrendikedir.. The goal of cytology and colposcopy during pregnancy is to identify invasive cancer that requires treatment before or at the time of delivery. However, unless cancer is identified or suspected, treatment of CIN is contraindicated during pregnancy. 212 HPV isolation in culture is difficult to accomplish. Highly specific and sensitive DNA methods utilizing type-specific HPV gene probes can identify HPV infection in vaginal washings, Pap smears, and amniotic fluid. In situ hybridization technique is useful to demonstrate type-specific HPV infection in tissues and cervical cell scrapings. PCR methods can identify even the lowest levels of HPV infection in blood and other kinds of fluids or in tissue samples. High-Risk Pregnancy , Fourth Edition, David James, Philip J. Steer, Carl P. Weiner, and Bernard Gonik, Chapter 30, e6 Copyright © 2011 by Saunders, an imprint of Elsevier Inc. 95. Workowski KA, Berman SM: Sexually transmitted diseases treatment guidelines, MMWR Recomm Rep 2006; 55: 1-91 212. American College of Obstetricians and Gynecologists : Management of abnormal cervical cytology and histology (ACOG Practice Bulletin No. 99). Obstet Gynecol 2008; 112: CrossRef Gebelikte biyopsi alınması fetal kayıp veya erken riskini artırmaz ancak biopsi alınmadığında invazif kanseri atlama riski olabilir..
. Obstet Gynecol 2008; 112: CrossRef. Gebelikte biyopsi alınması fetal kayıp veya erken riskini artırmaz ancak. biopsi alınmadığında invazif kanseri atlama riski olabilir..")
33
HPV DNA HR-HPV tiplerinin belirlenmesi ASCUS saptanan kadınlarda takip stratejilerinde yararlı olabilir.. Genital siğillerde klinik tanıda HPV DNA bakılması hiçbir veriyle desteklenmemiştir. Subklinik HPV enfeksiyon için DNA taraması sadece 30 yaş ve üstü kadınlarda yapılabilir Identification of high risk HPV types might prove helpful for follow-up strategies of women in whom cervical cytology has demonstrated atypical squamous cells of undetermined significance (ASCUS). 212 The usefulness of DNA technology in the clinical diagnosis of genital warts is not supported by any data. 95 Routine screening for subclinical HPV infection by DNA tests should be reserved for women aged 30 years and older. 95 , 212 High-Risk Pregnancy , Fourth Edition, David James, Philip J. Steer, Carl P. Weiner, and Bernard Gonik, Chapter 30, e6 Copyright © 2011 by Saunders, an imprint of Elsevier Inc. 95. Workowski KA, Berman SM: Sexually transmitted diseases treatment guidelines, MMWR Recomm Rep 2006; 55: 1-91 212. American College of Obstetricians and Gynecologists : Management of abnormal cervical cytology and histology (ACOG Practice Bulletin No. 99). Obstet Gynecol 2008; 112: CrossRef
 The usefulness of DNA technology in the clinical diagnosis of genital warts is not supported by any data. 95 Routine screening for subclinical HPV infection by DNA tests should be reserved for women aged 30 years and older. 95 , 212. High-Risk Pregnancy , Fourth Edition, David James, Philip J. Steer, Carl P. Weiner, and Bernard Gonik, Chapter 30, e6 Copyright © 2011 by Saunders, an imprint of Elsevier Inc. 95. Workowski KA, Berman SM: Sexually transmitted diseases treatment guidelines, MMWR Recomm Rep 2006; 55: American College of Obstetricians and Gynecologists : Management of abnormal cervical cytology and histology (ACOG Practice Bulletin No. 99). Obstet Gynecol 2008; 112: CrossRef.")
34
Gebelikte Kolposkopi Gebelikte kolposkopinin amacı = kanseri ekarte etmek İleri displastik değişiklik için en şüpheli alandan tek bir biyopsi Rastgele veya yönlendirilmemiş biyopsi yapılmamalıdır (yanlış-negatif sonuçlar 8%-40) Artmış vaskülarite nedeniyle aşırı kanama olabilir (Ag- nitrat veya Monsel solüsyon ile kontrol edilebilir) Gebelikte ECC yapılmamalıdır. The aim of colposcopy in pregnancy is to exclude cancer, and only one directed biopsy of the site compatible with the most advanced area of dysplastic change should be performed to establish the histologic level of disease. Because of false-negative results ranging from 8% to 40%, random or nondirected biopsies should be avoided. Great care must be exercised because the increased vascularity may lead to precipitous, heavy bleeding. A Tischler or baby Tischler biopsy forceps should be used, followed by immediate placement of a cotton-tipped applicator above the cervical epithelium. If bleeding occurs, it may be controlled with three silver nitrate sticks or with dehydrated Monsel's solution. An endocervical curettage, however, is best avoided during pregnancy. Clinical Gynecologic Oncology , Eighth Edition, Philip J. Di Saia, and William T. Creasman, Chapter 15, , 2012 (Saunders, Elsevier Inc.)
 Artmış vaskülarite nedeniyle aşırı kanama olabilir (Ag- nitrat veya Monsel solüsyon ile kontrol edilebilir) Gebelikte ECC yapılmamalıdır. The aim of colposcopy in pregnancy is to exclude cancer, and only one directed biopsy of the site compatible with the most advanced area of dysplastic change should be performed to establish the histologic level of disease. Because of false-negative results ranging from 8% to 40%, random or nondirected biopsies should be avoided. Great care must be exercised because the increased vascularity may lead to precipitous, heavy bleeding. A Tischler or baby Tischler biopsy forceps should be used, followed by immediate placement of a cotton-tipped applicator above the cervical epithelium. If bleeding occurs, it may be controlled with three silver nitrate sticks or with dehydrated Monsel s solution. An endocervical curettage, however, is best avoided during pregnancy. Clinical Gynecologic Oncology , Eighth Edition, Philip J. Di Saia, and William T. Creasman, Chapter 15, , 2012 (Saunders, Elsevier Inc.)")
35
Gebelikte Anormal Sitoloji
Postpartum regresyon sıktır CIN 1 %36 regresyon CIN 2, 3 %48-70 regresyon Paraskevaidis E, 2002 Yost NP, 1999

36
tedavi (LEEP, konizasyon) ertelenebilir.
Gebelikte Anormal Sitoloji Temel Kuramlar If SCJ görünüyor ve Atipik glandüler hücreler Sitolojik veya histolojik invazif Ca bulgusu 2 veya daha fazla kadranda kolposkopik CIN III görünümü yoksa; tedavi (LEEP, konizasyon) ertelenebilir.
 ertelenebilir.")
38
Gebede ASCUS’da HSIL riski %2-4
Gebelikte ASCUS Gebede ASCUS olgularında invazif kanser riski relatif olarak düşük (% ) Gebede ASCUS’da HSIL riski %2-4 Bond S, 2009
 Gebede ASCUS’da HSIL riski %2-4. Bond S,")
39
Gebelikte ASCUS Yönetimi
Yönetim opsiyonları (20 yaş üstünde) gebe olmayanla aynı. Tek fark kolposkopiyi postpartum 6. haftaya ertelemek kabul edilebilir [CIII] ECC yapılmamalıdır [EIII] HR-HPV test gereksiz kolposkopileri önleyebilir
 gebe olmayanla aynı. Tek fark kolposkopiyi postpartum 6. haftaya ertelemek kabul edilebilir [CIII] ECC yapılmamalıdır [EIII] HR-HPV test gereksiz kolposkopileri önleyebilir.")
40
Gebelikte ASC-H Yönetimi
CIN 2, 3 olasılığı %20-50 Konservatif yaklaşık kabul edilebilir Kolposkopi yapılmalıdır İnvazif Ca şüphesi yoksa ECC and tedavi doğum sonrasına ertelenebilir

41
Gebelikte ASC-H Yönetimi
Histoloji CIN 2,3 ise kolposkopi her trimesterde tekrarlanabilir (ECC ertelenir) If CIN 2,3 yoksa, kolposkopi + ECC 6. haftada yapılmalıdır
 If CIN 2,3 yoksa, kolposkopi + ECC 6. haftada yapılmalıdır.")
42
Gebelikte LSIL Yönetimi
Kolposkopinin amacı: İnvazif Ca ekarte etmek Daha düşük lezyonlar asla tedavi edilmez Adolesan olmayan gebe kadında kolposkopi tercih edilebilir [BII] Postpartum en az 6 ay sonrasına kolposkopinin ertelenmesi kabul edilebilir [BIII] ECC is kabul edilemez [EIII] Thomas C, Wright Jr,MD et al.: Amer J Obstet Gynecol , 2007. Thomas C, Wright Jr,MD et al.: Amer J Obstet Gynecol , 2007.

43
Gebelikte LSIL Yönetimi
İlk kolposkopide sitolojik, histoloji veya kolposkopik CIN II-III veya Ca şüphesi yoksa, PP takio tavsiye edilir. [BIII] Tekrarlayan kolposkopi veya sitolojik incelemeler kabul edilemez [DIII] CIN 2,3 ASCCP önerilerine göre tedavi edilir HPV testi gereksizdir Thomas C, Wright Jr,MD et al.: Am J Obstet Gynecol , 2007. Thomas C, Wright Jr,MD et al.: Am J Obstet Gynecol , 2007.

44
Adolesan Gebede ASCUS/LSIL Yönetimi
Gebe olmayan adolesanlarla aynı HPV testi önerilmez Kolposkopi önerilmez

45
Adolesan Gebede ASCUS/LSIL Yönetimi
Sitolojik takip (Postpartum 6. hafta veya 1 yıl sonra) @ 1 yıl ASC-US or LSIL (+) 1 yıl sonra sitoloji tekrarı @ 24 ayda ASCUS veya LSIL hala (+) Kolposkopi yapılmalı
 1 yıl sonra sitoloji 24 ayda ASCUS veya LSIL hala (+) Kolposkopi yapılmalı.")
46
Gebelikte HSIL Yönetim
Kolposkopi önerilir [AII] Deneyimli klinisyence yapılmalı CIN II-III veya kanser şüphesi olan lezyonlardan biyopsi tercih edilir [BIII] Diğer lezyonların biyopsisi kabul edilebilir [BIII] ECC gebelikte kabul edilemez [EIII] PP 6. haftada sitoloji / kolposkopi ile yeniden değerlendirme önerilir İnvazif kanser şüphesi olmadıkça tanısal exsizyon kabul edilemez Thomas C, Wright Jr,MD et al.: Amer J Obstet Gynecol , 2007. Thomas C, Wright Jr,MD et al.: Amer J Obstet Gynecol , 2007.

47
Gebelikte HSIL Yönetimi
Kanser HSIL olgularının %2’sinde (gebe veya değil) Kolposkopide CIN 2,3 saptanmadığı sürece tekrar sitoloji veya kolposkopi gereksiz CIN 2,3 saptanırsa, sitoloji ve kolposkopi 12 haftada bir tekrarlanmalı Bond S, 2009
 Kolposkopide CIN 2,3 saptanmadığı sürece tekrar sitoloji veya kolposkopi gereksiz. CIN 2,3 saptanırsa, sitoloji ve kolposkopi 12 haftada bir tekrarlanmalı. Bond S,")
48
Adolesan Gebede HSIL Yönetimi
Kolposkopi yapılmalı ECC kabul edilmez Tanısal eksizyonel biyopsiler (LEEP vb) önerilmez (gebe veya değil) CIN 2, 3 dışı lezyonlar kolposkopi ve sitoloji ile 6 ayda bir takip edilmeli Bond S, 2009
 önerilmez (gebe veya değil) CIN 2, 3 dışı lezyonlar kolposkopi ve sitoloji ile 6 ayda bir takip edilmeli. Bond S,")
49
Gebelikte Glandüler Hücre Anormalliklerinin Yönetimi
Halen belirsiz Kolposkopi eşliğinde biyopsi Yapılmalıdır Malignite (-) Sitoloji & kolposkopi ile takip kabul edilebilir Endoservikal örnekleme kabul edilemez Koni Preterm & EMR riski Kuvvetli Ca şüphesinde kabul edilebilir Postpartum >8 hf nihai değerlendirme Tam KF. Atypical glandular cells in cervical smear during pregnancy and postpartum period. Clin Med Res 2005; 3(1): 1-3.
 Sitoloji & kolposkopi ile takip kabul edilebilir. Endoservikal örnekleme kabul edilemez. Koni. Preterm & EMR riski Kuvvetli Ca şüphesinde kabul edilebilir. Postpartum >8 hf nihai değerlendirme. Tam KF. Atypical glandular cells in cervical smear during pregnancy and postpartum period. Clin Med Res 2005; 3(1): 1-3.")
50
Gebelikte CIN 1 Yönetimi
Gebede CIN 1 histolojik tanısında tedavisiz takip önerilir (BII) Gebelikte CIN 1 tedavisi kabul edilemez (EII)
 Gebelikte CIN 1 tedavisi kabul edilemez (EII)")
51
Biyopsi ile CIN II ve CIN III saptanan olguların postpartum durumu
Yost NP, ve ark., Obstet Gynecol 1999

Benzer bir sunumlar
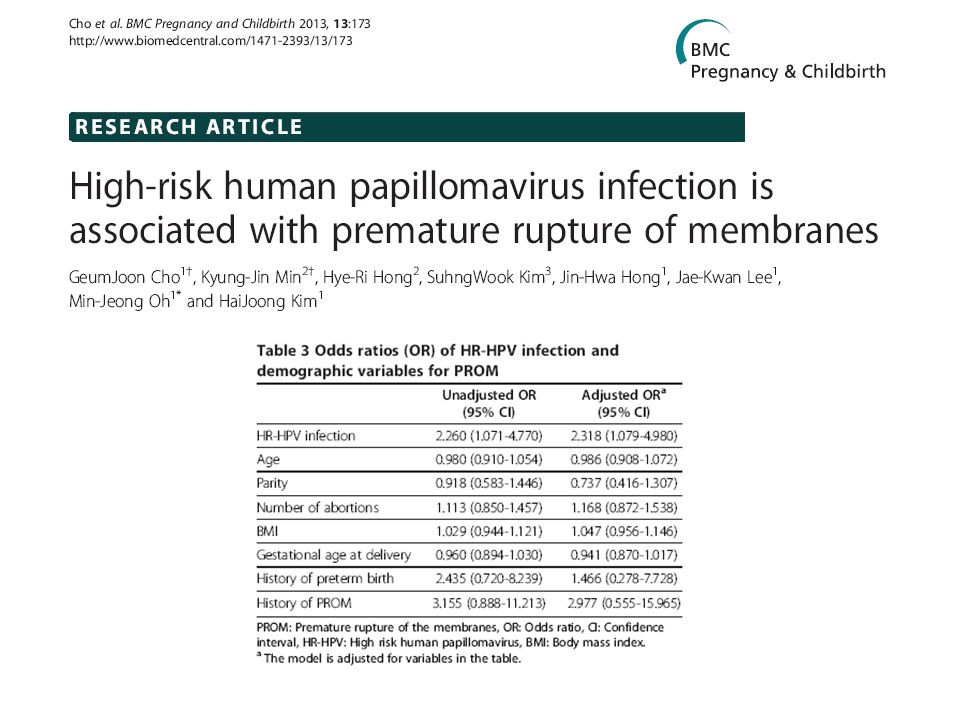

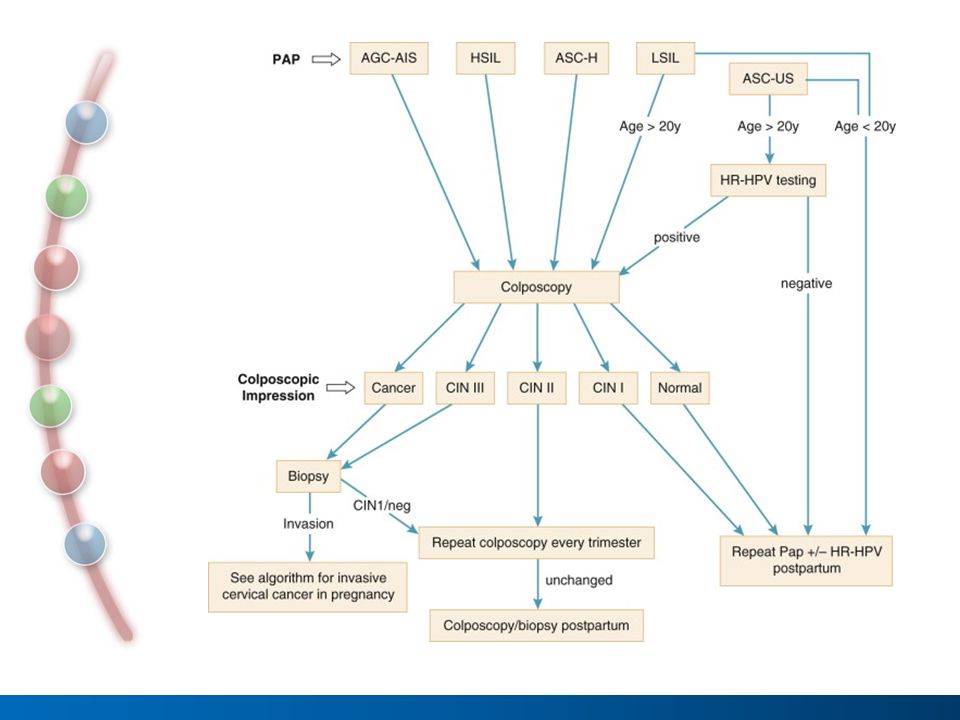


 KANSERİ>")
















