Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Erken Artrite Yaklaşım
Dr. Hatice Bodur

2
1987 ARA Kriterleri Sabah tutukluğu
3 veya daha fazla eklem alanında artrit El eklemlerinde artrit Simetrik artrit Romatoid nodüller Romatoid faktör pozitifliği Radyografik değişiklikler RA kronik progresif sinovitle karakterize bir hastalıktır tanımlanan sınıflama kriterleri erken evredeki hastaları tanımak konusunda yetersiz kalmı ve 90’lardan itibaren erken artritleri ayırt etmek için erken artrit klnikleri ve kohortları oluşmaya başalamıştır.Bu durumu iyi ayırdetmek için erken RA gelişecek kişiler için “kriterler” oluşturmak gerekecektir. The currently widely used 1987 RA classification criteria of the ACR were developed using patients with established RA (mean disease duration close to 8 years) and had a sensitivity of 91% and a specificity of 89%. Among the 7 components of these criteria, 1 is a radiologic criterion that is met only rarely in early disease; among patients with very early arthritis (symptom duration 3 months [median 8 weeks]) who all developed RA, erosions were found in only 13% (27), whereas joint erosions are present in 50–70% of RA patients 2 years after onset (28). Another component of the 1987 criteria is serologic in nature, i.e., rheumatoid factor (RF), which also is seen less frequently in early than in established disease (29). Among the 5 clinical components of the criteria set, rheumatoid nodules are very rare in early RA. Thus, only 4 of the 7 components of the ACR criteria set are clinical and joint related and may therefore have a reasonable probability of being fulfilled in early RA. Moreover, 1 of these remaining 4 clinical criteria relates to involvement of at least 3 joint areas whereas RA frequently initially presents as a mono- or oligoarticular disease, further reducing the diagnostic potential of these criteria in early RA. Not surprisingly, therefore, the sensitivity of the ACR classification criteria in early RA ranges from 40 to 60% and the specificity is no better than 80–90%. Taken together, these data indicate that the usefulness of the ACR criteria in early RA is low. 2
 and had a sensitivity of 91% and a specificity of 89%. Among the 7 components of these criteria, 1 is a radiologic criterion that is met only rarely in early disease; among patients with very early arthritis (symptom duration 3 months [median 8 weeks]) who all developed RA, erosions were found in only 13% (27), whereas joint erosions are present in 50–70% of RA patients 2 years after onset (28). Another component of the 1987 criteria is serologic in nature, i.e., rheumatoid factor (RF), which also is seen less frequently in early than in established disease (29). Among the 5 clinical components of the criteria set, rheumatoid nodules are very rare in early RA. Thus, only 4 of the 7 components of the ACR criteria set are clinical and joint related and may therefore have a reasonable probability of being fulfilled in early RA. Moreover, 1 of these remaining 4 clinical criteria relates to involvement of at least 3 joint areas whereas RA frequently initially presents as a mono- or oligoarticular disease, further reducing the diagnostic potential of these criteria in early RA. Not surprisingly, therefore, the sensitivity of the ACR classification criteria in early RA ranges from 40 to 60% and the specificity is no better than 80–90%. Taken together, these data indicate that the usefulness of the ACR criteria in early RA is low. 2.")
3
≥6 = Kesin RA Geçerlilik çalışmalarında iyi tanısal değer taşıdığı görülmüştür.

4
Erken Dönem Kavramı Önceleri hastalık süresi < 5 yıl
1990’larda semptom süresi ay Bugün için bu sürenin haftalar veya aylar ACR/EULAR RA 2010 kriterlerinde, hastalık süresi kestirim değeri 6 haftadır

5
Yeni RA Kriterleri: Niçin ?
Kriterler geliştirildiğinde tedavi seçenekleri kısıtlıydı: Tedavi Piramidi Düşük başla, yavaş git RKÇ ve gözlem çalışmalarının metaanalizleri bize fırsat penceresi denilen bir terapötik kritik dönemin varlığını gösterdi. Bu dönemde tedavi başlamanın hastalığın seyrini değiştirebileceğini gösterdi. Erken agresif tedavinin yararları görüldü Klinik durum, morbidite ve mortalitede azalma RKÇ’lerle gösterildi Birinci basamakta hastanın erken refere edilmesinde kriterlerin yetersiz kaldığı izlendi

6
Radyolojik değişikliklerin başlangıcı
Fırsat Penceresi Kavramı DMARD Başlangıcı Tedavi yok Geç tedavi Erken tedavi Progresyon İlk Vizit İdeal durum RA’nın erken tanınması ve erkenden DMARD’larla tedavi edilmesinin, hastalığın procesini değiştirerek klasik hasar ve özürlülük progresyon yolağını keseceğinin düşünülmesi yeni bir paradigmadır. A meta-analysis [6] found that delaying antirheumatic therapy for 9 months after symptom onset results in significantly worse long-term outcomes. Bu konudaki son kanıtlar, semptomların ortaya çıkmasını takip eden 3 aylık bir dönemde, klinik manifestasyonlar tam olarak oturmadan başlanan DMARD tedavisinin remisyona sokmada ve major radyografik hasarı önlemede oldukça yüksek bir oranda etkin olduğunu göstermektedir. Zira bu dönemde immunolojik sistem bu dönemde müdahalelere ve yeniden programlanmaya açıktır. Bu döneme fırsat penceresi dönemi denir. Halihazırda anti romatizmal tedavi relatif olarak geç başlanmaktadır ki sıklıkla bu süre semptomlar başladıktan sonraki 12 aydan daha fazladır. Bir çok hastada, bir kere RA oturduktan sonra hastalık aktivitesi ve progresyon klinik olarak anlamlı bir seviyeye çekilemez. Yine de anlamlı gelişmeler görülen bir çok hastada, rezidüel aktivite saptanabilir. Günümüzde uzman hekimler hastaları ilk fırsatta görmek isterler, ancak yine de erken RA tanısında sorunlar vardır. Genelde klinik semptomlar ortaya çıkan inflamatuvar poliartritli hastalar ilk 4 hafta içinde hekime başvururlar, fakat RA tanısı ortalama 36 hafta gecikerek konur. Bunda ACR kriterlerin erken RA için bile düşük duyarlılık ve hassasiyete sahip olması önemli etkendir. Bu gecikme bir taraftan da gereklidir. (Neden?) Nevertheless, in many patients, disease activity and progression cannot be reduced to a clinically meaningful extent once RA is established, and in many who experience significant improvement, there is residual activity (22). While remissions are rare in established disease, remission is the ultimate aim of therapeutic intervention. Interference with the disease process may be easier in the very early stages of the disease. here are often profound problems in recognizing early RA. Patients with inflammatory polyarthritis consult a physician on average within 4 weeks of symptom onset, yet the diagnosis of RA is delayed on average by 36 weeks. Zaman İlk Semptomlar Radyolojik değişikliklerin başlangıcı 3 ay……..9 ay……..12 ay 6
 Nevertheless, in many patients, disease activity and progression cannot be reduced to a clinically meaningful extent once RA is established, and in many who experience significant improvement, there is residual activity (22). While remissions are rare in established disease, remission is the ultimate aim of therapeutic intervention. Interference with the disease process may be easier in the very early stages of the disease. here are often profound problems in recognizing early RA. Patients with inflammatory polyarthritis consult a physician on average within 4 weeks of symptom onset, yet the diagnosis of RA is delayed on average by 36 weeks. Zaman. İlk. Semptomlar. Radyolojik değişikliklerin başlangıcı. 3 ay……..9 ay……..12 ay. 6.")
7
Fırsat Penceresi Semptomların ortaya çıkmasını takip eden 3 aylık dönem Klinik tablo tam olarak oturmadan DMARD tedavisi remisyon sağlama ve major radyografik hasarı önlemede oldukça yüksek bir oranda etkindir Bu dönemde immunolojik sistem müdahalelere ve yeniden programlanmaya açıktır 7

8
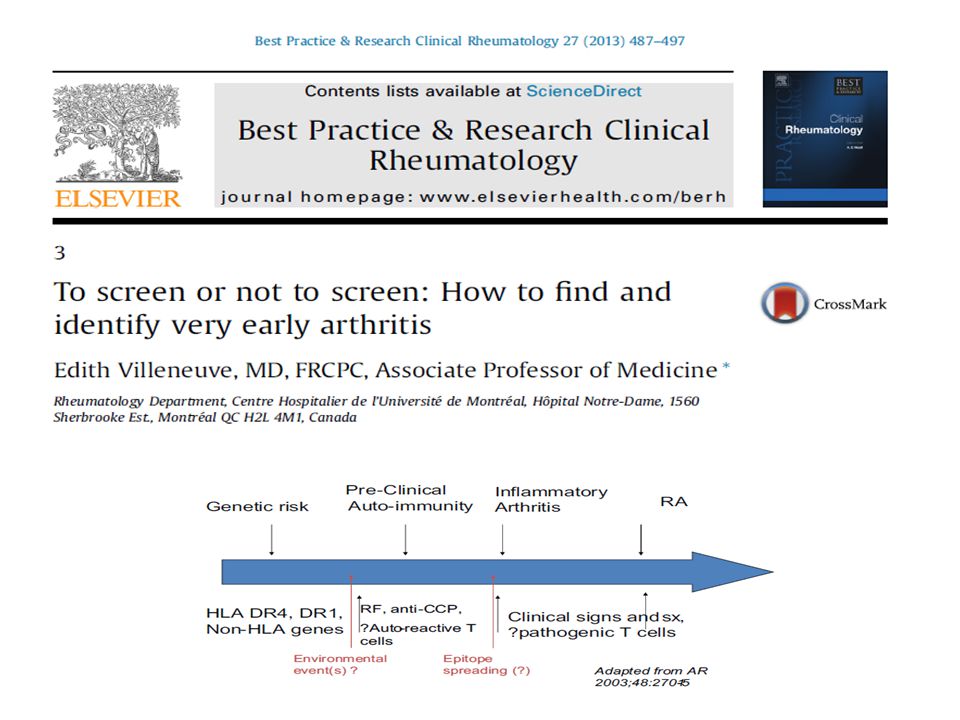
RA Gelişme Fazları FAZ 1 kişisel genetik riskleri temsil eder. Çevresel faktörler faz 2’yi tetikler. Otoantikorlar gelişir,hastalığın klnik semptom ve bulguları yoktur ve preklinik otoimmünite fazıdır. Sonunda bazı hastalar 3.faza geçer ve aşikar inflamtuar artrit tablosu ortaya çıkar.

9
RA Gelişme Fazları Klinik Pre-klinik dönemi Semptom yok
Genetik yatkınlığı olan bireyler gelişme dönemi Otoimmünite Sinovitin ortaya çıktığı dönem Pre-klinik dönemi Semptom yok RF, CCP, Sitokinler, otoreaktif T ve B hücreleri Nielen et al. found rheumatic factor–immunoglobulim M (RF–IgM) and anti-CCP to be positive in, respectively, 28% and 41% of 79 RA patients with preclinical stored serum [15]. RF was positive a median of 2 years prior to RA diagnosis and anti-CCP, 4.5 years. Klinik 9
 and anti-CCP to be positive in, respectively, 28% and 41% of 79 RA patients with preclinical stored serum [15]. RF was positive a median of 2 years prior to RA diagnosis and anti-CCP, 4.5 years. Klinik. 9.")
10
Tanım Erken İnflamatuar Artrit - EİA Erken Andiferansiye Artrit-EAA
Süre, tutulan eklem sayısı, akut faz reaktanları vb faktörlere göre görüş birliği yoktur Erken Artrit kohortlarının ~ %30’u AA (%23-81) Ortalama %30’lar civarında birleşilmiştir.
 Ortalama %30’lar civarında birleşilmiştir.")
11
Erken Andiferansiye Artrit
Kesin bir tanı koyulamayan ve zamanla kronik inflamatuar bir hastalığa dönüşebilecek veya remisyona girecek inflamatuar oligo/poliartrittir Erken sinovitin bir subgrubudur ve SpA, kristal artopati gibi diğer hastalık kriterlerini taşımaz Tanı dışlama ile konulur ve sınıflama kriterleri yoktur

12
Erken Artrit Klinikleri
Avrupa erken artrit kohortlarında % AA’dır Kalan erken sinovitlerde ilk vizitte tanı konulmaktadır AA sıklığı semptom süresi ile ilişkilidir ve süre uzadıkça karakteristik semptomlar ortaya çıkar Leiden erken artrit kliniği verileri %30 remisyon, %30 RA, >%20 AA In contrast, the remission rate in RA is at most 10% to 15%

13
AA Doğal Öyküsü Teşhis değişebilir Andiferansiye artrit dönemi
İnflamatuvar Artritler 1- kendini sınırlayan 2- Kalıcı Erozif Non erozif Kendi kendini sınırlayan hastaların kalıcı inflamatuvar ve erozif artrit riski taşıyanlardan ayrılması, erken dönemde uygun tedaviyi başlatmak için gerekmektedir. Bazıları RA’ya ve bazıları da diğer romatizmal hastalıklara dönüşecekleri görülmüş Bir kısım hastalar da andiferansiye kaldıkları veya remisyona girdikleri gösterilmiştir Andiferansiye artrit dönemi Klinik, laboratuvar ve görüntülemeden yararlanılır 13

14
Erken Dönemde Yaklaşım

15
Erken RA’da gecikmiş tedavinin etkisi. A
Erken RA’da gecikmiş tedavinin etkisi.A. Erken ve gecikmiş tedavinin farkı. B.Etkili DMARD tedavisi plasebo veya daha az etkili rejimle karşılaşılaştırıl mıştır.Daire DMARD başlama zamanını temsil eder.

16
6 yıllık izlem 12 haftalık uzman değerlendirmesi farkını göstermektedir. Radyolojik veriler normal dağılmadığı için median değerler verilmiştir. Sharp/van der Heijde skorlar. Tedavi rejimi 1993–1996, başlangıç analjezikler ve takine HK veya SSZ. if the patient had persistently active disease (delayed treatment) (B); during 1996–1998, prompt treatment with either chloroquine or sulfasalazine (C); and during 1999–2006, prompt treatment with either sulfasalazine or methotrexate (D). Figure 2. Probability of achieving sustained disease-modifying antirheumatic drug (DMARD)–free remission in rheumatoid arthritis (RA) patients according to the different categories of delay in assessment by a rheumatologist. Remission was used as an outcome measure for the amount of total delay. Remission was defined as the persistent absence of synovitis for at least 1 year after the cessation of DMARD therapy and the identification of disease remission by the patient’s rheumatologist (14). Total delay was calculated as the sum of the patient delay (time from symptom onset until being seen by the general practitioner [GP]) and the GP delay (time from assessment by the GP until being seen by the rheumatologist) (see Patients and Methods for details).
 (B); during 1996–1998, prompt treatment with either chloroquine or sulfasalazine. (C); and during 1999–2006, prompt treatment with either sulfasalazine or methotrexate (D). Figure 2. Probability of achieving sustained disease-modifying antirheumatic drug (DMARD)–free remission in rheumatoid arthritis (RA) patients according to the different categories of delay in assessment by a rheumatologist. Remission was used as an outcome measure for the amount of total delay. Remission was defined as the persistent. absence of synovitis for at least 1 year after the cessation of DMARD. therapy and the identification of disease remission by the patient’s rheumatologist (14). Total delay was calculated as the sum of the patient delay (time from symptom onset until being seen by the general practitioner [GP]) and the GP delay (time from assessment by the GP until being seen by the rheumatologist) (see Patients and Methods for. details).")
17
AA’nın Tedavi Yaklaşımı
Tartışmalıdır 1/3 hastada RA gelişir Hangi hastalar kalıcı olacaktır Sağlıklı donörlerde, RA gelişiminden 10 yıl kadar önce anti –CCP (+) olabilir Lehte ve aleyhte görüşler…
 olabilir. Lehte ve aleyhte görüşler…")
19
“Leiden Tahmin Kuralı”
Erken artritte prognozu belirlemede literatürde en çok adı geçen en iyi valide edilmiş sistematik değerlendirmelerden biri “ Leiden (hollanda) tahmin kuralı” dır. Among the 570 patients with recent-onset undifferentiated arthritis, 177 patients developed RA, 150 achieved remission, and 94 developed another rheumatologic disorder after 1 year of follow-up. Using regression analysis, nine independent clinical parameters could be identified that predict the risk of developing RA within 1 year (sex, age, localization of symptoms,morning stiffness, tender joint count, swollen joint count, C-reactive protein level, rheumatoid factor positivity, and anti-CCP status). These were simplified into a 14-point, easy-to-use, weighted score (Table 1). Usage of this instrument should allow improving individualized treatment decisions for patients suffering from early undifferentiated arthritis. A score of 0 represents the lowest risk of developing RA, and a score of 14 represents the highest risk. The positive predicted value for patients with a prediction score of 8 or greater was 97%; the negative predictive value for patients with a score of 6 or lower was 83% and virtually none of the patientswith a score of 3 or less was ultimately diagnosed with RA [28]. On the basis of these findings, for patients with a score of at least 8, DMARD therapy should be considered, whereas for patients with a score of 6 or less, the risk of progression is low and careful clinical supervision might be enough. …………………………………………………………. Depo Despite these caveats, J. M. W. Hazes reported an effort to identify determinants of the disease course in patients with early RA, in which 524 consecutive patients with recent-onset arthritis who were referred to Leiden University Medical Center were investigated. This cohort was followed up for 2 years, predict outcome at 2 years. In this model, 7 variables were found to be optimal for the prediction of persistent or erosive disease. These 7 variables were symptom duration at first visit, morning stiffness 1 hour, arthritis in 3 joints, presence of pain bilaterally on compression of metatarsophalangeal joints, positive results for rheumatoid factor or anticitrullinated peptide by serum tests, and the presence of erosions in the hands and feet. Depending on the outcome tested (persistent or erosive disease), different weight factors were assigned to these items and the sum of these weight factors yielded a probability for persistent disease or erosive disease 570 AA 177 ,RA 150 Remisyon 94…Başka hastalık van der Helm-van Mil AH, et al. A prediction rule for disease outcome in patients with recent-onset undifferentiated arthritis: how to guide individual treatment decisions. Arthritis Rheum 2007; 56:433–440. 19
 tahmin kuralı dır. Among the 570 patients with recent-onset undifferentiated arthritis, 177 patients developed RA, 150 achieved remission, and 94 developed another rheumatologic disorder after 1 year of follow-up. Using regression analysis, nine independent clinical parameters could be identified that predict the risk of developing RA within 1 year (sex, age, localization of symptoms,morning stiffness, tender joint count, swollen joint count, C-reactive protein level, rheumatoid factor positivity, and anti-CCP status). These were simplified into a 14-point, easy-to-use, weighted score (Table 1). Usage of this instrument should allow improving individualized treatment decisions for patients suffering from early undifferentiated arthritis. A score of 0 represents the lowest risk of developing RA, and a score of 14 represents the highest risk. The positive predicted value for patients with a prediction score of 8 or greater was 97%; the negative predictive value for patients with a score of 6 or lower was 83% and virtually none of the patientswith a score of 3 or less was ultimately diagnosed with RA [28]. On the basis of these findings, for patients with a score of at least 8, DMARD therapy should be considered, whereas for patients with a score of 6 or less, the risk of progression is low and careful clinical supervision might be enough. …………………………………………………………. Depo. Despite these caveats, J. M. W. Hazes reported an effort to identify determinants of the disease course in patients with early RA, in which 524 consecutive patients with recent-onset arthritis who were referred to Leiden University Medical Center were investigated. This cohort was followed up for 2 years, predict outcome at 2 years. In this model, 7 variables were found to be optimal for the prediction of persistent or erosive disease. These 7 variables were symptom duration at first visit, morning stiffness 1 hour, arthritis in 3 joints, presence of pain bilaterally on compression of metatarsophalangeal joints, positive results for rheumatoid factor or anticitrullinated peptide by serum tests, and the presence of erosions in the hands and feet. Depending on the outcome tested (persistent or erosive disease), different weight factors were assigned to these items and the sum of these weight factors yielded a probability for persistent disease or erosive disease. 570 AA. 177 ,RA. 150 Remisyon. 94…Başka hastalık. van der Helm-van Mil AH, et al. A prediction rule for disease outcome in patients with recent-onset undifferentiated arthritis: how to guide individual treatment decisions. Arthritis Rheum 2007; 56:433–")
20
RA’yı Öngörmek Mümkün mü? Leiden CPR (2007)
Yaşx0.02 Cinsiyet 1 puan Eklem tutulumu El ayakların küçük eklemi tutulumu 0,5 puan Simetrik tutulum 0,5 puan Üst ekstremitede: 1 puan Üst ve alt ekstremitede tutulum 1,5 puan Sabah tutukluğunun 100-mm VAS ile değerlendirilmesi 26-90-mm 1 puan >90-mm 2 puan Hassas eklem sayısı 4-10 0,5 puan 11 ve üstü 1 puan Şiş eklem sayısı ,5 puan 11 ve üstü 1 puan CRP seviyesi 5-50 mg/litre 0,5 puan 51 mg/ litre ve üstü 1,5 puan RF (+ )1 puan anti-CCP (+) 2 puan Total predictionscores range from 0 to14,with higher scores associated with increasing probability of developing RA at 1year [5]. A cutpoint of 6 is used to identify patients who are at a low risk ofdeveloping RA,while a cut point of 8 is applied to identify those who are at a high risk of developing RA Toplam skor: <6düşük risk >8:yüksek risk Pozitif prediksiyon: 8 ve üstü: %97,Negatif prediksiyon 6 ve altı: % 83 20
1 puan. anti-CCP (+) 2 puan. Total predictionscores range from 0 to14,with higher scores associated with increasing probability of developing RA at 1year [5]. A cutpoint of 6 is used to identify patients who are at a low risk ofdeveloping RA,while a cut point of 8 is applied to identify those who are at a high risk of developing RA. Toplam skor:14 <6düşük risk >8:yüksek risk. Pozitif prediksiyon: 8 ve üstü: %97,Negatif prediksiyon 6 ve altı: %")
21
Sistematik derleme ve metaanaliz
1084 hasta (6 veri kaynağı) ≥ 9 optimal kestirim değeri
 ≥ 9 optimal kestirim değeri.")
22
Kalıcı Hastalık Belirteçleri
Kadın cinsiyet Semptom süresi > 12 hafta Yüksek sayıda şiş ve hassas eklem sayısı El eklem tutulumu Sigara Akut faz reaktanları Romatoid faktör ACPA pozitifliği X-ray’de erozyon Romatoid artrit 1987 ACR kriterlerini karşılamak (sensitivite %88, özgüllük %73) 22
 22.")
23
60 dk↑sabah tutukluğu artrit/ artralji Leiden EAC OR 1,55
Groningen EAC OR 1,73 REACH 1,61 Erken artrit Leiden OR 3,07, ESPOIR OR 2,28 Leiden OR 1,75, ESPOIR OR 1,68 (aOR) Sabah tutukluğu süresi 30 dk 2014 EULAR,Paris Yaş, cinsiyet,ACPA, RF, ESH ve şiş eklem sayısına göre uyarlandıktan sonra
 Sabah tutukluğu süresi 30 dk EULAR,Paris. Yaş, cinsiyet,ACPA, RF, ESH ve şiş eklem sayısına göre uyarlandıktan sonra.")
24
hastalık progresyonunu belirler
Erozyon Çok Önemli erozyonların özgüllüğü yüksektir Kendini sınırlayan Kalıcı erozif hastalık progresyonunu belirler

25
Erozyon Bir andiferansiye artrit kohortunda;
başlangıçta ≥2 erozif eklem, kalıcı artrit için %68 pozitif tahmin değeri gösterilmiştir Thabet MM, Huizinga TW, van der Heijde DM, van der Helm,van Mil AH. The prognostic value of baseline erosions undifferentiated arthritis. Arthritis research & therapy. 2009;11(5):R155.
:R155.")
26
USG USG, erozyonları, X-ray’e göre 1.4 kat daha fazla göstermekte
Imaging of the second metacarpophalangeal joint of a patient with rheumatoid arthritis.. A. Conventional radiography shows juxta-articular osteoporosis. B. Ultrasonographic examination, in the longitudinal dorsal scan, reveals proliferative synovitis with marked intra-articular power Doppler signal. m = metacarpal bone; p = proximal phalanx; t = extensor tendon 26

27
Hedef eklemlerde erozyon varlığı (2 ve 5. MKF, 5.MTF ve distal ulna )
(semikantitatif skor ≥2) Özgüllük % 97,9 Duyarlılık % 41,4 Daha büyük erozyonlar daha özgül ve prediktif The presence of erosions with semiquantitative score ≥2 in four target joints (2nd, 5rd MCP, 5th MTP joints and distal ulna) was highly specific for RA (specificity 97.9% and sensitivity 41.4%). Size of erosion was found to be associated with RA. Erosions of any size in the 5th MTP joint were both specific and sensitive for RA (specificity 85.4% and sensitivity 68.6%). sions The presence of US-detected erosions is not specific for RA. However, larger erosions in selected joints, especially 2nd and 5rd MCP, 5th MTP joints and distal ulna, were highly specific for and predictive of RA. 5.MTF %85,4 özgül ve %68,6 duyarlı
 Özgüllük % 97,9. Duyarlılık % 41,4. Daha büyük erozyonlar daha özgül ve prediktif. The presence of erosions with semiquantitative score ≥2 in four target joints (2nd, 5rd MCP, 5th MTP joints and distal ulna) was highly specific for RA (specificity 97.9% and sensitivity 41.4%). Size of erosion was found to be associated with RA. Erosions of any size in the 5th MTP joint were both specific and sensitive for RA (specificity 85.4% and sensitivity 68.6%). sions The presence of US-detected erosions is not specific for RA. However, larger erosions in selected joints, especially 2nd and 5rd MCP, 5th MTP joints and distal ulna, were highly specific for and predictive of RA. 5.MTF %85,4 özgül ve %68,6 duyarlı.")
28
Klinik olarak şüpheli 102 artralji olgusu
MRG’de subklinik inflamasyon oranı %44 Subclinical inflammation as measured by MRI is present in 44% of patients with CSA. A combination of symptoms/characteristics incompletely differentiated patients with and without MRI inflammation

30
30

31
MRG 1.T1FsC Koranal kesit 2-3 mcf eklemde kalınlaşmış sinovya pannus dokusu ile uyumlu 2.T1FsC Aksiyel kesit pannus kalınlaşmış sinovya 2.T2 Fs Koronal el –el bileği Erken RA’da kemik iliği ödemi El bileği, distal ulna, II.MCF, el bileği kemiklerinde kemik iliği ödemi

32
l Erken RA’da, el ve parmaklarda, MRG’de kemik iliği ödemi 2010 kriterlerinin tanısal olasılığını artırır The present findings are the first evidence that the diagnostic probability of early RA using the 2010 RA classification criteria is improved by combining these criteria with MRI-detected bone marrow oedema of the wrist and finger joints. Our study may strengthen the statements of the European League Against Rheumatism recommendations for the use of imaging. Yanıt: First, we have examined both hands though Nieuwenhuis et al scanned only unilateral hand. Our previous data showed that the sensitivity of detection of BME declined by unilateral hand compared with both hands. Our present MRI data are derived from gadolinium-diethylenetriamine pentaacetic acid (Gd-DTPA)-enhanced MRI; however, Nieuwenhuis et al might have used plain MRI. If so, the sensitivity of detection of BME also declines by plain MRI compared with Gd-DTPA-enhanced MRI. The above differences of MRI procedure may affect the difference of MRI results of both groups. In conclusion, the difference of role of MRI-detected BME is found between our cohort and the Leiden Early Arthritis Clinic; however, these might be attributable to the differences of MRI procedure and patient characteristics
-enhanced MRI; however, Nieuwenhuis et al might have used plain MRI. If so, the sensitivity of detection of BME also declines by plain MRI compared with Gd-DTPA-enhanced MRI. The above differences of MRI procedure may affect the difference of MRI results of both groups. In conclusion, the difference of role of MRI-detected BME is found between our cohort and the Leiden Early Arthritis Clinic; however, these might be attributable to the differences of MRI procedure and patient characteristics.")
33
AA’de kriterlerin ayırt ediciliğini artırmaz
Kemik iliği ödemi ve erozyon varlığının 2010 kriterlerine eklenmesi kesinliği artırmaz AA’de kriterlerin ayırt ediciliğini artırmaz MRG işlemi ve hasta özellikleri In conclusion, in line with the findings of Tamai et al, we did observe an increase in sensitivity when adding information on MRI detected BME or MRI detected erosions to the 2010 criteria. However, this was at the cost of a considerable decrease in specificity. The accuracy and discriminative ability (expressed using AUCs) decreased or remained unchanged. Based on these results, we conclude that the addition of MRI detected features to the 2010 classification criteria for RA does not evidently improve the accuracy of these criteria when applied in patients with undifferentiated arthritis according to the 1987 criteria. Wouter P Nieuwenhuis,1 Monique Reijnierse,2 Annette HM van der Helm-van Mil1 Leiden Erken Artrit Kliniği Nieuwenhuis ve ark.
 decreased or remained unchanged. Based on these results, we conclude that the addition of MRI detected features to the 2010 classification criteria for RA does not evidently improve the accuracy of these criteria when applied in patients with undifferentiated arthritis according to the 1987 criteria. Wouter P Nieuwenhuis,1 Monique Reijnierse,2 Annette HM van der Helm-van Mil1. Leiden Erken Artrit Kliniği. Nieuwenhuis ve ark.")
34
Pre-RA olguların belirlenmesi önümüzdeki 10 yılda mümkün olabilir mi ?

36
Preklinik Otoimmünite
Nielen ve ark. saklanmış serumlarda IgM-RF %28 (+ ), tanıdan ~ 2 yıl önce Anti-CCP %41 (+),tanıdan ~ 4,5 yıl önce Anti-CCP/ herhangi bir RF izotip kombinasyonu %99 özgül Popülasyonda anti-CCP / Ig A-RF kombinasyonu PPD %16-22 Yeni biyobelirteçlerin UA’da tanıda sınırlıdır. PPD:Pozitif prediktif değer
, tanıdan ~ 2 yıl önce. Anti-CCP %41 (+),tanıdan ~ 4,5 yıl önce. Anti-CCP/ herhangi bir RF izotip kombinasyonu %99 özgül. Popülasyonda anti-CCP / Ig A-RF kombinasyonu PPD % Yeni biyobelirteçlerin UA’da tanıda sınırlıdır. PPD:Pozitif prediktif değer.")
37
Erken tanı,erken tedavi ve erken tedavi de daha iyi sonuçlar demektir
1.Basamakta AA’nın tanınması ve uzmana gönderilmesi esastır Tarama amacıyla, artraljisi olan hastalarda kullanılan araç ve gereçler: sorgulama formları ve özel kas iskelet sisteminin muayenesidir 37

38
Kimleri Tarayalım? Tüm popülasyonu tarayalım mı?
Yüksek riskli hastaları tarayalım RA hastalarının birinci derece akrabaları veya erken eklem semptomu veren sağlıklı bireyler Sabah tutukluğu, MKF sıkma testi Bugün için ‘tarama’ pre-klinik RA’da popüler bir araştırma alanıdır; kan bankası çalışmaları, prospektif çalışmalar, prediktif biyobelirteçler Maliyet/etkinlik Screening for people at risk of RA remains an area of research at the moment. As early treatment leads to better outcomes, patients’ general physicians should refer them to arthritis specialty care as soon as they have a suspicion of IA. Screening tools in the form of questionnaires as well as MSK screening examination are available to help health professionals in primary care identify patients with IA. The use of referral forms combined with triage or triage clinics are an effective means for rheumatologists to identify patients who are most likely to have IA and thus need to be seen as early as possible. SABAH TUTUKLUĞU, MKF sıkma testi Research agenda Results from blood-bank studies of pre-RA serum have helped identified factors that could be used to identify RA at a preclinical stage, but prospective studies are needed to define which tests will be of most value in which populations. Intervention studies in the preclinical RA group are needed before we can determine the value of screening for preclinical RA in the general population. Although it is agreed that early treatment is more effective, the best initial treatment strategy for RA is still a question of debate and even more so for the management of UA that can have a variable course. Better predictive biomarkers and strategy trials are needed in this scenario.

39
Tedavi Yaklaşımı AA’nın progresyonu önlenebilir mi ?
RA gelişimi önlenebilir mi? En iyi tedavi stratejisi nedir ?

40
Sigaranın erken RA’da radyografik progresyonun güçlü bir bağımsız prediktörü olduğu gösterilmiştir. ACPA üretiminde ortak epitopla özellikle ACPA pozitif hastalarda sigaranın rolü vardır.

41
Diyet Alkol alımı riski azaltır.Uzun süreli uzun zincirli poliansatüre yağ asitlerinin diyetle alımı riski artırır.Omega 3 yağ asiti barındıran yiyecekler alınmalıdır.

42
Peridontal hastalıklar ve Porphyromonas
gingivalis tetikleyici rol oynayabilir Peptidilarginin deaminaz sitruline neoantjenler üretir Oral hijyen, ağız ve diş sağlığı sorunları önemlidir RA’da sitruline proteinlere karşı antikorlar esastır. Porphyromonas gingivalis peptidylarginine deiminase (PPAD) has been implicated in the initiation of RA by generating citrullinated neoantigens and due to its ability to autocitrullinate. Objectives To define the citrullination status and biology
 has been implicated in the initiation of RA by generating citrullinated neoantigens and due to its ability to autocitrullinate. Objectives To define the citrullination status and biology.")
43
PRObable rheumatoid arthritis: Methotrexate versus Placebo Treatment
RKÇ,110 hasta,30 ay izlem RA gelişimi plasebo grubunda %53 MTX grubunda %40

44
PROMPT Çalışması-2007 ACPA(+) grupta AA’nın RA’ya progresyonunu ve radyolojik progresyonu geciktirmektedir,18 ay
 grupta AA’nın RA’ya progresyonunu ve radyolojik progresyonu geciktirmektedir,18 ay.")
45
PROMPT Çalışması-2007 ACPA(+) grupta AA’nın RA’ya progresyonunu ve radyolojik progresyonu geciktirmektedir 18 ay izlem ACPA(+) grupta AA’nın RA’ya progresyonunu ve radyolojik progresyonu geciktirmektedir,18 ay
 grupta AA’nın RA’ya progresyonunu ve radyolojik progresyonu geciktirmektedir,18 ay.")
46
Bu RKÇ’nin 5 yıllık sonuçları. AA’da MTX ve plasebo
Bu RKÇ’nin 5 yıllık sonuçları. AA’da MTX ve plasebo. İlk yıl MTX’in sonlandırıcı etkisi yok. Pozitif ACPA ve radyolojik hasar RA’ya progresyonun bağımsız prediktörleri. Negatif ACPA ilaçsız remisyonun bağımsız belirtecidir. Spontan remisyon oranı, ACR/EULAR kriterlerini tamamlayan herkese MTX başlanmasının %25 over treratment olacağını göstermektedir. Öte yandan çoğu ACPA (+) hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.
 hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.")
47
ACPA (-) ilaçsız remisyon prediktörü
ACPA(+) ve radyografik hasar RA’ya progresyonun bağımsız pozitif prediktörü ACPA (-) ilaçsız remisyon prediktörü Bu RKÇ’nin 5 yıllık sonuçları. AA’da MTX ve plasebo. İlk yıl MTX’in sonlandırıcı etkisi yok. Pozitif ACPA ve radyolojik hasar RA’ya progresyonun bağımsız prediktörleri. Negatif ACPA ilaçsız remisyonun bağımsız belirtecidir. Spontan remisyon oranı, ACR/EULAR kriterlerini tamamlayan herkese MTX başlanmasının %25 over treratment olacağını göstermektedir. Öte yandan çoğu ACPA (+) hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.
 ve radyografik hasar RA’ya progresyonun bağımsız pozitif prediktörü. ACPA (-) ilaçsız remisyon prediktörü. Bu RKÇ’nin 5 yıllık sonuçları. AA’da MTX ve plasebo. İlk yıl MTX’in sonlandırıcı etkisi yok. Pozitif ACPA ve radyolojik hasar RA’ya progresyonun bağımsız prediktörleri. Negatif ACPA ilaçsız remisyonun bağımsız belirtecidir. Spontan remisyon oranı, ACR/EULAR 2010 kriterlerini tamamlayan herkese MTX başlanmasının %25 over treratment olacağını göstermektedir. Öte yandan çoğu ACPA (+) hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.")
48
ACPA (+) hastalarda başlangıç MTX monoterapisi hastalık progresyonunu önlemek için yeterli değildir
Bu RKÇ’nin 5 yıllık sonuçları. AA’da MTX ve plasebo. İlk yıl MTX’in sonlandırıcı etkisi yok. Pozitif ACPA ve radyolojik hasar RA’ya progresyonun bağımsız prediktörleri. Negatif ACPA ilaçsız remisyonun bağımsız belirtecidir. Spontan remisyon oranı, ACR/EULAR kriterlerini tamamlayan herkese MTX başlanmasının %25 over treratment olacağını göstermektedir. Öte yandan çoğu ACPA (+) hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.
 hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.")
49
Spontan remisyon nedeniyle %25 gereksiz tedavi
Bu RKÇ’nin 5 yıllık sonuçları. AA’da MTX ve plasebo. İlk yıl MTX’in sonlandırıcı etkisi yok. Pozitif ACPA ve radyolojik hasar RA’ya progresyonun bağımsız prediktörleri. Negatif ACPA ilaçsız remisyonun bağımsız belirtecidir. Spontan remisyon oranı, ACR/EULAR kriterlerini tamamlayan herkese MTX başlanmasının %25 over treratment olacağını göstermektedir. Öte yandan çoğu ACPA (+) hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.
 hastalarda 1 yıl başlangıç MTX monoterapisinin hastalık progresyonunu önlemek için yeterli olmadığı görülmektedir. Erken ve doğru RA tanısı ve ve hastalık progresyonunu önleyecek doğru tedavi için daha ileri çalışmalar gerekir.")
50
İM 120 mg metilprednizolon 12 ayda
Semptom süresi < 16 hft İM 120 mg metilprednizolon 12 ayda Remisyon veya progresyonda PLB ile fark yok In the Stop Arthritis Very Early (SAVE) trial, patients with IA of <16 weeks duration were given a single intramuscular (IM) dose of 120 mg of methylprednisolone versus placebo,and followed for 12 months for the development of RA by 1987 criteria. This intervention did not result in any decrease in progression to RA between the study groups. Background Glucocorticoids (GCs) are often used as early arthritis treatment and it has been suggested that they induce remission or at least delay the development of rheumatoid arthritis (RA) and the need to start disease modifying antirheumatic drugs (DMARDs). Objective To test the effect of GCs on patients with very early arthritis (symptom duration of <16 weeks) in a randomised controlled trial. Methods Patients received a single intramuscular injection of 120 mg methylprednisolone or placebo (PL) and were followed up for 52 weeks. Primary end point was drug-free clinical remission, both at weeks 12 and 52. Among secondary outcomes were fulfilment of remission criteria at weeks 2, 12 or 52, time course of ‘core set variables’ and proportion of patients starting DMARDs. Results 17.0% of all analysed subjects (65/383) achieved persistent remission: 17.8% (33/185) of the PL group, 16.2% (32/198) of the patients receiving methylprednisolone (OR=1.13, 95% CI 0.66 to 1.92, p=0.6847). Analyses of secondary end points showed significant clinical benefits of the GC only at week 2. These differences subsequently disappeared. DMARDs were started in 162 patients: 50.3% methylprednisolone and 56.7% PL patients had to start DMARD treatment (OR=0.78, 95% CI 0.49 to 1.22, p=0.30). Significantly more patients with polyarthritis than with oligoarthritis received DMARDs (OR=2.84, 95% CI 1.75 to 4.60, p<0.0001). Conclusions Neither remission nor development of RA is delayed by GC treatment. Remission is rare in the first year of very early arthritis, occurring in <20% of the patients. Also, the need to the need to start DMARDs was not influenced by GC treatment 50
 trial, patients with IA of <16 weeks duration were given a single intramuscular (IM) dose of 120 mg of methylprednisolone versus placebo,and followed for 12 months for the development of RA by 1987 criteria. This intervention did not result in any decrease in progression to RA between the study groups. Background Glucocorticoids (GCs) are often used as early arthritis treatment and it has been suggested that they induce remission or at least delay the development of rheumatoid arthritis (RA) and the need to start disease modifying antirheumatic drugs (DMARDs). Objective To test the effect of GCs on patients with very early arthritis (symptom duration of <16 weeks) in a randomised controlled trial. Methods Patients received a single intramuscular injection of 120 mg methylprednisolone or placebo (PL) and were followed up for 52 weeks. Primary end point was drug-free clinical remission, both at weeks 12 and 52. Among secondary outcomes were fulfilment of remission criteria at weeks 2, 12 or 52, time course of ‘core set variables’ and proportion of patients starting. DMARDs. Results 17.0% of all analysed subjects (65/383) achieved persistent remission: 17.8% (33/185) of the PL group, 16.2% (32/198) of the patients receiving methylprednisolone (OR=1.13, 95% CI 0.66 to 1.92, p=0.6847). Analyses of secondary end points showed significant clinical benefits of the GC only at week 2. These differences subsequently disappeared. DMARDs were started in 162 patients: 50.3% methylprednisolone and 56.7% PL patients had to start DMARD treatment (OR=0.78, 95% CI 0.49 to 1.22, p=0.30). Significantly more patients with polyarthritis than with oligoarthritis received DMARDs (OR=2.84, 95% CI 1.75 to 4.60, p<0.0001). Conclusions Neither remission nor development of RA is delayed by GC treatment. Remission is rare in the first year of very early arthritis, occurring in <20% of the patients. Also, the need to the need to start DMARDs was not influenced by GC treatment. 50.")
51
3 hft İM 80 mg/hft metilprednizolonasetat 12 ay izlem
Semptom süresi 4-10 hft 132 H PLB,133 H GK 3 hft İM 80 mg/hft metilprednizolonasetat 12 ay izlem DMARD tedavisini geciktirmede ve RA’ya progresyonda fark var In the STIVEA trial, patients with early IA (4–10 weeks duration) were given 3 weekly IM injections of 80 mg of methylprednisolone versus placebo, and followed for 12 months.This intervention resulted in the delay of prescription of DMARDs, and per the authors, prevented the development of RA (1987 criteria) in 1 of 10 subjects treated. 132 hasta PLB,133 hasta GK 51
 were given 3 weekly IM injections of 80 mg of methylprednisolone versus placebo, and followed for 12 months.This intervention resulted in the delay of prescription of DMARDs, and per the authors, prevented the development of RA (1987 criteria) in 1 of 10 subjects treated. 132 hasta PLB,133 hasta GK. 51.")
52
Tripl DMARD induksiyonu MTX monoterapisinden üstün
Yan etkiye bağlı uyum sorununda fark yok İM ve oral GK’ler köprü tedavisinde eşit derecede etkili, ikisi de kullanılabilir Triple DMARD induction therapy is better than MTX monotherapy in early RA. Furthermore, no differences were seen in medication adjustments due to adverse events after stratifi cation for drug. Intramuscular and oral GCs are equally effective as bridging treatments and both can be used.

53
10INF 10 hasta INF 7 hasta PLS 0,2,6 ve 14.hafta
Patients with UA of ,12 months’ duration and having relapsed after a single parenteral corticosteroid injection were recruited into a double-blind, placebo controlled trial of infliximab or placebo monotherapy administered at weeks 0, 2, 6 and 14. Methotrexate was added at week 14 if no clinical response (raised C-reactive protein (CRP) and clinical synovitis) was achieved. Standard outcomes were collected at baseline, infusion visits and weeks 26 and 52. The primary outcome was clinical remission at week 26. In poor prognosis UA, a short course of TNF antagonist therapy provided modest short-term relief but did not prevent the development of RA. Patients with UA with a poor prognosis relapsing after corticosteroid have a high risk of evolving to RA and are suitable candidates for interventional treatment. 17 hasta ,10 INF,7 PLS 10 hasta INF 7 hasta PLS 0,2,6 ve 14.hafta Yanıt yoksa MTX ilavesi 26 ve 52.hafta
 and clinical synovitis) was achieved. Standard outcomes were collected at baseline, infusion visits and weeks 26 and 52. The primary outcome was clinical remission at week 26. In poor prognosis UA, a short course of TNF antagonist therapy provided modest short-term relief but did not prevent the development of RA. Patients with UA with a poor prognosis relapsing after corticosteroid have a high risk of evolving to RA and are suitable candidates for interventional treatment. 17 hasta ,10 INF,7 PLS. 10 hasta INF. 7 hasta PLS. 0,2,6 ve 14.hafta. Yanıt yoksa MTX ilavesi. 26 ve 52.hafta.")
55
2010 kriterleri değerlendirilmemiş ABA v plasebo 6 ay Primer sonlanım;
50 AA hastası; 2 veya daha fazla şiş eklem, 1987 kriterlerini tamamlamıyor 2010 kriterleri değerlendirilmemiş ABA v plasebo 6 ay Primer sonlanım; 12 ayda RA (1987 kriterleri gelişimi) ABA grubu 12/26 (%46) PLB grubu 16/24 (%67) Ab titresinde azalma Ab titresinde azalma (istatistiksel anlamı olmayan),
 ABA grubu 12/26 (%46) PLB grubu 16/24 (%67) Ab titresinde azalma. Ab titresinde azalma (istatistiksel anlamı olmayan),")
56
ABA hastalık progresyonunu geciktirir
Radyografik ve MRG inhibisyonu tedavi kesildikten 6 sonraya kadar sürer Çok erken evrede T hücre cevabının modülasyonu ile RA progresyonunu değiştirmek mümkün olabilir

57
STIEVA ADJUST SAVE PROMPT
Figure 2 (A) Remission percentages after 1 year (24,20,23) and 30 (16) month follow-up of the four completed placebo controlled trials on temporary treatment of patients with UA. (B) Percentages of patients who progressed to rheumatoid arthritis after 1 year and 30 months follow-up of the four completed placebo controlled trials on temporary treatment of patients with UA * p=0.048; CS, corticosteroids; IM, intra-muscular; RA, Tamamlanmış 4 tane randomize kontrollü çalışma
 Remission percentages after 1 year (24,20,23) and 30 (16) month follow-up of the four completed placebo controlled trials on temporary treatment of patients with UA. (B) Percentages of patients who progressed to rheumatoid arthritis after 1 year and 30 months follow-up of the four completed placebo controlled trials on temporary treatment of patients with UA * p=0.048; CS, corticosteroids; IM, intra-muscular; RA, Tamamlanmış 4 tane randomize kontrollü çalışma.")
58
Sistematik Literatür Taraması Der ki !
AA’da remisyon/progresyonu araştıran çalışma sayısı sınırlıdır ve uzun süreli izlemler henüz yoktur MTX monoterapisi, DMARD kombinasyonu, GK’ler ve biyolojik tedaviler ile inflamasyon ve radyolojik hasar baskılanabilir Erken tedavi özellikle hastalık aktivitesi yüksek olgularda önemlidir Erken tanı stratejisi önemlidir

59
İlacı bıraktıktan en az 1 yıl sonra,
5 yıla kadar izlem, ilaçsız remisyon EAC grubunda %11,5 (n=738) Optimal semptom süresi 14,9 hafta ESPOIR grubunda %5,4 (n=533) Optimal semptom süresi 19,1 hafta
 Optimal semptom süresi 14,9 hafta. ESPOIR grubunda %5,4 (n=533) Optimal semptom süresi 19,1 hafta.")
60
Ne Kadar Erken «Yeterince» Erkendir ?
Semptom süresi yaklaşık ilk 20 hafta içinde ise şans daha fazla EAC ACPA (-) grup remisyon %19,9 ACPA (+) grup %3,5 ESPOIR ACPA (+) grup remisyon %1,1 Karşılaştırmalı çalışma etik açıdan sorunlu In this study, van Nies and colleagues used data obtained from two groups of patients with rheumatoid arthritis (RA), as defined by the 1987 American College of Rheumatology criteria, who were treated with disease-modifying antirheumatic drugs (DMARDs): the Leiden Early Arthritis Cohort (EAC) (n = 738) from The Netherlands, and the Evaluation et Suivi de POlyarthrites Indifférenciées Récentes (ESPOIR) cohort (n = 533) from France. The primary outcome was DMARD-free remission, defined as absence of joint swelling after cessation of DMARDs after at least 1 year and up to 5 years. This was deemed by the authors to be the best proxy for a "cure" of RA. During 5 years of follow-up, 11.5% and 5.4% of patients achieved DMARD-free remission in the EAC and ESPOIR groups, respectively. When anti-citrullinated peptide antibody (ACPA) status was evaluated, 67 (19.9%) ACPA-negative patients in the EAC group achieved DMARD-free remission vs only 13 (3.5%) ACPA-positive patients; in the ESPOIR group, only 3 (1.1%) ACPA-positive patients achieved DMARD-free remission. The duration of symptoms that best predicted DMARD-free remission was 14.9 weeks among the EAC patients and 19.1 weeks among the ESPOIR patients. Beyond these periods, the rates of DMARD-free remission were lower, leading the authors to conclude that there may be a defined period in early RA that is most susceptible to treatment. Viewpoint After many years of struggling to merely control RA, it is exciting see factors being identified that are associated with DMARD-free remission. From van Nies and colleagues' study, it appears that initiating DMARD therapy within about 20 weeks of symptom onset may result in the best chance of DMARD-free remission. Because it now may not be ethical to compare early vs later treatment of RA in randomized controlled trials, important next steps should be to determine the underlying biology of RA that makes it more susceptible to treatment in this early period and to identify the optimal treatment regimens that can improve rates of DMARD-free remission. In addition, we need to develop a healthcare infrastructure that is capable of diagnosing and treating RA in this early time frame. Even though initiating DMARD therapy soon after symptom onset improved rates of DMARD-free remission, it is still disappointing that the rates of DMARD-free remission were quite low overall in this study and were particularly low for patients who were ACPA-positive. As such, for the vast majority of patients (and in particular those with ACPA-positive disease), once RA is diagnosed, it is a lifelong disease—emphasizing that we still need to improve both the timing of treatment initiation and the treatments themselves, in addition to identifying potential preventive strategies. Of note, the symptoms attributable to RA and their duration were identified retrospectively (ie, once patients had developed classifiable disease) in this study. However, in actual clinical practice, symptoms attributable to RA need to be identified prospectively (ie, in advance of classifiable disease). Many factors affect the time between onset of symptoms of RA and initiation of DMARD therapy, including patients' awareness of symptoms, access to healthcare, quality of initial evaluation, and rapidity of referral to a rheumatologist. The wide variety of presentations of RA can also complicate early identification of its symptoms. For example, explosive onset of polyarticular disease may be easy for any provider to identify as RA, whereas palindromic-type onset or gradual accumulation of symptomatic joints may be more difficult to attribute to RA. Certainly, joint symptoms in an ACPA-positive patient, even in the absence of meeting classification criteria for RA, may be easier to attribute to RA and therefore lead to earlier initiation of DMARD therapy; however, ACPA status in such patients is often not known, and it may not be practical to assess ACPA status in all patients with joint symptoms. Developing robust approaches that can accurately identify specific symptoms that warrant more detailed evaluation for RA has been a major challenge.[1,2] While clinicians, researchers, and healthcare delivery systems face these issues, it seems prudent for rheumatologists and other healthcare providers to continue to work to identify and treat patients with RA in a timely fashion, with the hope of improving rates of DMARD-free remission.
 grup remisyon %19,9 ACPA (+) grup %3,5. ESPOIR ACPA (+) grup remisyon %1,1. Karşılaştırmalı çalışma etik açıdan sorunlu. In this study, van Nies and colleagues used data obtained from two groups of patients with rheumatoid arthritis (RA), as defined by the 1987 American College of Rheumatology criteria, who were treated with disease-modifying antirheumatic drugs (DMARDs): the Leiden Early Arthritis Cohort (EAC) (n = 738) from The Netherlands, and the Evaluation et Suivi de POlyarthrites Indifférenciées Récentes (ESPOIR) cohort (n = 533) from France. The primary outcome was DMARD-free remission, defined as absence of joint swelling after cessation of DMARDs after at least 1 year and up to 5 years. This was deemed by the authors to be the best proxy for a cure of RA. During 5 years of follow-up, 11.5% and 5.4% of patients achieved DMARD-free remission in the EAC and ESPOIR groups, respectively. When anti-citrullinated peptide antibody (ACPA) status was evaluated, 67 (19.9%) ACPA-negative patients in the EAC group achieved DMARD-free remission vs only 13 (3.5%) ACPA-positive patients; in the ESPOIR group, only 3 (1.1%) ACPA-positive patients achieved DMARD-free remission. The duration of symptoms that best predicted DMARD-free remission was 14.9 weeks among the EAC patients and 19.1 weeks among the ESPOIR patients. Beyond these periods, the rates of DMARD-free remission were lower, leading the authors to conclude that there may be a defined period in early RA that is most susceptible to treatment. Viewpoint. After many years of struggling to merely control RA, it is exciting see factors being identified that are associated with DMARD-free remission. From van Nies and colleagues study, it appears that initiating DMARD therapy within about 20 weeks of symptom onset may result in the best chance of DMARD-free remission. Because it now may not be ethical to compare early vs later treatment of RA in randomized controlled trials, important next steps should be to determine the underlying biology of RA that makes it more susceptible to treatment in this early period and to identify the optimal treatment regimens that can improve rates of DMARD-free remission. In addition, we need to develop a healthcare infrastructure that is capable of diagnosing and treating RA in this early time frame. Even though initiating DMARD therapy soon after symptom onset improved rates of DMARD-free remission, it is still disappointing that the rates of DMARD-free remission were quite low overall in this study and were particularly low for patients who were ACPA-positive. As such, for the vast majority of patients (and in particular those with ACPA-positive disease), once RA is diagnosed, it is a lifelong disease—emphasizing that we still need to improve both the timing of treatment initiation and the treatments themselves, in addition to identifying potential preventive strategies. Of note, the symptoms attributable to RA and their duration were identified retrospectively (ie, once patients had developed classifiable disease) in this study. However, in actual clinical practice, symptoms attributable to RA need to be identified prospectively (ie, in advance of classifiable disease). Many factors affect the time between onset of symptoms of RA and initiation of DMARD therapy, including patients awareness of symptoms, access to healthcare, quality of initial evaluation, and rapidity of referral to a rheumatologist. The wide variety of presentations of RA can also complicate early identification of its symptoms. For example, explosive onset of polyarticular disease may be easy for any provider to identify as RA, whereas palindromic-type onset or gradual accumulation of symptomatic joints may be more difficult to attribute to RA. Certainly, joint symptoms in an ACPA-positive patient, even in the absence of meeting classification criteria for RA, may be easier to attribute to RA and therefore lead to earlier initiation of DMARD therapy; however, ACPA status in such patients is often not known, and it may not be practical to assess ACPA status in all patients with joint symptoms. Developing robust approaches that can accurately identify specific symptoms that warrant more detailed evaluation for RA has been a major challenge.[1,2] While clinicians, researchers, and healthcare delivery systems face these issues, it seems prudent for rheumatologists and other healthcare providers to continue to work to identify and treat patients with RA in a timely fashion, with the hope of improving rates of DMARD-free remission.")
61
Erken Tanı/Tedavi Farkındalık düzeyi, hekime ulaşabilme olanakları
RA’nın başlangıç tablosu önemlidir; ani poliartiküler başlangıçta RA daha çok akla gelir Palindromik/tedrici başlangıçta DMARD başlanması daha gecikebilir Zamanında tanı ve tedavi ile ilaçsız remisyon hedeflenmelidir Araştırmacılar ve sağlık çalışanları hedefi

62
Artılar/Eksiler Fırsat penceresi giderek daraltılmaktadır
« Ne kadar erken,o kadar iyi» MTX güvenlik profili iyi bir ilaçtır EAA’da %40-50 spontan remisyon olabilir Kabul gören prensip Norfolk kayıt sistemine göre remisyon prediktörleri 1) RF (-) , 2) 6’dan az eklemde hassasiyet 3) Ayak bileğinde şişlik olmayışı
 RF (-) , 2) 6’dan az eklemde hassasiyet 3) Ayak bileğinde şişlik olmayışı.")
Benzer bir sunumlar