Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
POSTMENOPOZAL HORMON TEDAVİSİ VE KANSER
Prof. Dr. Mithat Erenus Marmara Üniversitesi Tıp Fakültesi Kadın Hastalıkları Anabilim Dalı

3
4/11/2017 5:11 AM LMF/FM 2004 Oncology Endometrial Cancer 41,200 new cases of cancer of the uterine corpus expected in 2006 Most of these are of the endometrium (95%) which is the most common reproductive organ cancer in the US Accounts for 6% of all cancers in women in the US Roughly 7350 deaths from endometrial cancer expected in 2006 Represents 3% of cancer deaths in US women Major risk factor is high cumulative exposure to estrogen, e.g., estrogen therapy without adequate progestin, obesity The American Cancer Society estimates that there will be 40,880 new cases of cancer of the uterine corpus diagnosed in The vast majority of these cancers will be endometrial. Cancers of the uterine corpus account for approximately 6% of all new cancers in women in the US and only 3% of cancer deaths in women. An estimated 7350 deaths attributable to cancer of the uterine corpus are expected in In this country, cancer of the endometrium is the most common cancer found in women’s reproductive organs. Diagnosed primarily in postmenopausal women, most endometrial cancer is detected at an early stage because abnormal vaginal bleeding is an early sign of this cancer. The 1-year survival rate for endometrial cancer is 94%. 5-year survival for women with Stage I disease is 90-95%. When endometrial cancer is diagnosed with Stage II, Stage III or Stage IV disease, the 5-year survival rates are 75%, 60% and 15-24%, respectively. High cumulative exposure to estrogen is the primary risk factor for endometrial cancer. Factors that substantially increase a woman’s exposure to estrogen include obesity and estrogen therapy without adequate use of progestin. Other factors that increase risk of endometrial cancer include use of tamoxifen, early menarche, late menopause, nulliparity, and a personal history of polycystic ovary syndrome. Concomitant E+P has not been associated with an increased risk of endometrial cancer; whereas, E alone has. American Cancer Society. Cancer Facts and Figures Available at: American Cancer Society. Cancer Facts and Figures Available at:
 which is the most common reproductive organ cancer in the US. Accounts for 6% of all cancers in women in the US. Roughly 7350 deaths from endometrial cancer expected in Represents 3% of cancer deaths in US women. Major risk factor is high cumulative exposure to estrogen, e.g., estrogen therapy without adequate progestin, obesity. The American Cancer Society estimates that there will be 40,880 new cases of cancer of the uterine corpus diagnosed in The vast majority of these cancers will be endometrial. Cancers of the uterine corpus account for approximately 6% of all new cancers in women in the US and only 3% of cancer deaths in women. An estimated 7350 deaths attributable to cancer of the uterine corpus are expected in In this country, cancer of the endometrium is the most common cancer found in women’s reproductive organs. Diagnosed primarily in postmenopausal women, most endometrial cancer is detected at an early stage because abnormal vaginal bleeding is an early sign of this cancer. The 1-year survival rate for endometrial cancer is 94%. 5-year survival for women with Stage I disease is 90-95%. When endometrial cancer is diagnosed with Stage II, Stage III or Stage IV disease, the 5-year survival rates are 75%, 60% and 15-24%, respectively. High cumulative exposure to estrogen is the primary risk factor for endometrial cancer. Factors that substantially increase a woman’s exposure to estrogen include obesity and estrogen therapy without adequate use of progestin. Other factors that increase risk of endometrial cancer include use of tamoxifen, early menarche, late menopause, nulliparity, and a personal history of polycystic ovary syndrome. Concomitant E+P has not been associated with an increased risk of endometrial cancer; whereas, E alone has. American Cancer Society. Cancer Facts and Figures Available at: American Cancer Society. Cancer Facts and Figures Available at:")
4
IN 1975 ZİEHL AND SMİTH İN TWO CASE CONTROL STUDİES REPORTED AN ASSOCİATON BETWEEN ERT AND AN İNCREASED RİSK OF ENDOMETRİAL CARCİNOMA

5
Relative Risk from Meta-Analysis: Postmenopausal Estrogen therapy and Endometrial Cancer
RR 95%CI # of studies CEE dose 0.3 3.9 3 0.625 3.4 4 >1.25 5.8 9 Duration (yrs) <1 1.4 1-5 2.8 12 5-10 5.9 10 >10 9.5 Regimen Cycic 3.0 8 Continuous 2.9
 < > Regimen. Cycic Continuous")
6
No Increased Risk of Endometrial Cancer With E+P Regimens
4/11/2017 5:11 AM LMF/FM 2004 Oncology No Increased Risk of Endometrial Cancer With E+P Regimens HT Use* Mean Yrs of Use Cases per population Relative Risk (95% CI) Never -- 763/395,800 1.00 (referent) E+P, daily 5.0 73/69,600 0.71 ( ) E+P, cyclic 5.1 242/145,500 1.05 ( ) E only 4.6 33/14,200 1.45 ( ) Tibolone 5.2 86/28,000 1.79 ( ) It is well-established that the use of unopposed estrogen in women with intact uteri is associated with a dose-dependent increased risk for endometrial cancer and that the addition of a progestin reduces this risk. In the Million Women Study, 716,738 postmenopausal women without previous cancer or previous hysterectomy provided information about their use of HT and other personal details at the time they were recruited into the study (between 1996–2001). The women were followed for an average of 3.4 years, during which time 1320 incident endometrial cancers were diagnosed.1 As shown in this slide, compared with never-users, risk of endometrial cancer was: reduced with use of continuous combined HT; increased with use of unopposed estrogen and tibolone; and not significantly altered with use of cyclic combined HT. Interestingly, BMI significantly affected these associations, such that the adverse effects of tibolone and unopposed estrogen were greatest in nonobese women, and the beneficial effects of combined HT were greatest in obese women. (See next slide.) These findings are consistent with earlier meta-analyses and randomized trials A meta-analysis of 29 observational studies of unopposed E and endometrial cancer incidence found a combined RR for unopposed E users compared with nonusers of 2.3 (95% CI, 2.1–2.5).2 A meta-analysis of 7 studies evaluating the effects of E+P on endometrial cancer incidence reported an RR of 0.8 (95% CI, 0.6–1.2).3 Neither WHI4 nor HERS5 reported an increase in endometrial cancer with a daily regimen of E+P. *Type of HT last used, self-reported at recruitment. Million Women Study Collaborators. Lancet. 2005;365: 1Million Women Study Collaborators. Lancet. 2005;365: 2Nelson HD, et al. JAMA. 2002;288: 3Grady D, et al. Obstet Gynecol. 1995;85: 4Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: 5Hulley S, et al. JAMA. 2002;288:58-66.
 Never /395, (referent) E+P, daily /69, ( ) E+P, cyclic /145, ( ) E only /14, ( ) Tibolone /28, ( ) It is well-established that the use of unopposed estrogen in women with intact uteri is associated with a dose-dependent increased risk for endometrial cancer and that the addition of a progestin reduces this risk. In the Million Women Study, 716,738 postmenopausal women without previous cancer or previous hysterectomy provided information about their use of HT and other personal details at the time they were recruited into the study (between 1996–2001). The women were followed for an average of 3.4 years, during which time 1320 incident endometrial cancers were diagnosed.1. As shown in this slide, compared with never-users, risk of endometrial cancer was: reduced with use of continuous combined HT; increased with use of unopposed estrogen and tibolone; and not significantly altered with use of cyclic combined HT. Interestingly, BMI significantly affected these associations, such that the adverse effects of tibolone and unopposed estrogen were greatest in nonobese women, and the beneficial effects of combined HT were greatest in obese women. (See next slide.) These findings are consistent with earlier meta-analyses and randomized trials. A meta-analysis of 29 observational studies of unopposed E and endometrial cancer incidence found a combined RR for unopposed E users compared with nonusers of 2.3 (95% CI, 2.1–2.5).2. A meta-analysis of 7 studies evaluating the effects of E+P on endometrial cancer incidence reported an RR of 0.8 (95% CI, 0.6–1.2).3. Neither WHI4 nor HERS5 reported an increase in endometrial cancer with a daily regimen of E+P. *Type of HT last used, self-reported at recruitment. Million Women Study Collaborators. Lancet. 2005;365: Million Women Study Collaborators. Lancet. 2005;365: Nelson HD, et al. JAMA. 2002;288: Grady D, et al. Obstet Gynecol. 1995;85: Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: Hulley S, et al. JAMA. 2002;288:")
7
WHI Results: Hazard Ratio for Endometrial Cancer with E+P
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI Results: Hazard Ratio for Endometrial Cancer with E+P Placebo E+P 95% nominal CI 95% adjusted CI 0.1 0.5 1.0 5.0 2.0 Recently, the WHI reported a small, nonsignificant reduction in the risk of endometrial cancer in women assigned to receive E+P compared with those assigned to placebo (HR, 0.81; 95% nCI, 0.48–1.36; 95% aCI, 0.40–1.64).1 Average follow-up time for the women included in this analysis was 5.6 years. The annual incidence rate for endometrial cancer observed among the total study population was 62 cases per 100,000 person-years. This rate is lower than the National Cancer Institute’s Surveillance, Epidemiology, and End Results population-based rate of 92 cases per 100,000 person-years in women in the same age range as the WHI participants.2 The WHI investigators found no differences between treatment groups in histology, grade, or stage of disease at diagnosis. In addition, no significant interactions between group assignment and any of the following variables were observed: age, race/ethnicity, BMI, hypertension, smoking status, pack-years of smoking, prior exposure to unopposed E, or prior use of E+P.1 In summary, there was an observed difference in endometrial cancer rates between E+P and placebo, although the difference in incidence rates was not statistically significant. The authors noted that the WHI was the first randomized, double-blind, placebo-controlled trial to demonstrate that endometrial cancer rates among women assigned to continuous E+P are similar to those observed in women assigned to placebo.1 Hazard Ratio Incidence rate of endometrial cancer for the total study population was 62 cases per 100,000 person-years. Anderson GL, et al. JAMA. 2003;290: 1Anderson GL, et al. JAMA. 2003;290: 2Ries LAG, Harkins D, Krapcho M, Mariotto A, Miller BA, Feuer EJ, Clegg L, Eisner MP, Horner MJ, Howlader N, Hayat M, Hankey BF, Edwards BK (eds). SEER Cancer Statistics Review, , National Cancer Institute. Bethesda, MD, based on November 2005 SEER data submission, posted to the SEER web site, Accessed June 7,2006.
.1 Average follow-up time for the women included in this analysis was 5.6 years. The annual incidence rate for endometrial cancer observed among the total study population was 62 cases per 100,000 person-years. This rate is lower than the National Cancer Institute’s Surveillance, Epidemiology, and End Results population-based rate of 92 cases per 100,000 person-years in women in the same age range as the WHI participants.2. The WHI investigators found no differences between treatment groups in histology, grade, or stage of disease at diagnosis. In addition, no significant interactions between group assignment and any of the following variables were observed: age, race/ethnicity, BMI, hypertension, smoking status, pack-years of smoking, prior exposure to unopposed E, or prior use of E+P.1. In summary, there was an observed difference in endometrial cancer rates between E+P and placebo, although the difference in incidence rates was not statistically significant. The authors noted that the WHI was the first randomized, double-blind, placebo-controlled trial to demonstrate that endometrial cancer rates among women assigned to continuous E+P are similar to those observed in women assigned to placebo.1. Hazard Ratio. Incidence rate of endometrial cancer for the total study population was 62 cases per 100,000 person-years. Anderson GL, et al. JAMA. 2003;290: Anderson GL, et al. JAMA. 2003;290: Ries LAG, Harkins D, Krapcho M, Mariotto A, Miller BA, Feuer EJ, Clegg L, Eisner MP, Horner MJ, Howlader N, Hayat M, Hankey BF, Edwards BK (eds). SEER Cancer Statistics Review, , National Cancer Institute. Bethesda, MD, based on November 2005 SEER data submission, posted to the SEER web site, Accessed June 7,2006.")
8
HT and Risk of Endometrial Cancer: Summary
4/11/2017 5:11 AM LMF/FM 2004 Oncology HT and Risk of Endometrial Cancer: Summary Unopposed estrogen increases endometrial cancer risk in postmenopausal women with an intact uterus Estrogen in combination with a progestin has not been associated with increased endometrial cancer risk and some observational studies have noted a potential protective effect. Progestin use must be for >10 days per month WHI did not find a significant reduction in endometrial cancer risk in E+P group Observational studies have shown trends in endometrial cancer incidence in women taking E+P, implying variable effects upon endometrial cancer risk. Possibly related to BMI; progestin provides greatest protection in obese women; on average, subjects in E+P trial were overweight but not obese Progestin has been used in combination with E in HT for several decades to reduce the risk of E associated endometrial cancer, with many studies and meta-analyses supporting its risk reducing role and some observational studies have noted a potential protective effect. In order for the progestin to reduce the E associated risk of endometrial cancer, it must be used for longer than 10 days per cycle. In WHI, there was a decrease in endometrial cancer in the E+P group compared with placebo (HR, 0.81), but the difference was not statistically significant.1 Failure to demonstrate a decreased risk of endometrial cancer among E+P users in the WHI may be related to an effect of BMI. Observational studies have shown trends in endometrial cancer incidence in women taking E+P, implying variable effects upon endometrial cancer risk. Studies suggest that the protective effect of progestin is greatest in obese women. On average, the women in WHI E+P trial were overweight but not obese. 1Anderson GL, et al. JAMA. 2003;290:
, but the difference was not statistically significant.1 Failure to demonstrate a decreased risk of endometrial cancer among E+P users in the WHI may be related to an effect of BMI. Observational studies have shown trends in endometrial cancer incidence in women taking E+P, implying variable effects upon endometrial cancer risk. Studies suggest that the protective effect of progestin is greatest in obese women. On average, the women in WHI E+P trial were overweight but not obese. 1Anderson GL, et al. JAMA. 2003;290:")
9
American Cancer Society. Cancer Facts and Figures 2006. Available at:
LMF/FM 2004 Oncology Colorectal Cancer A woman’s lifetime risk of developing colorectal cancer is 5.5% 3rd most common cancer and 3rd most common cause of cancer death in US women 2006 estimates: 74,746 new cases and 27,300 deaths from colorectal cancer in US women 91% of new cases and 94% of colorectal cancer deaths occur after age 50 years 10-year survival for colorectal cancer is 57% Colorectal cancer is the third most common cancer among women in the US. The American Cancer Society estimates that in 2006: colorectal cancer will be newly diagnosed in an estimated 74,746 women nationwide. 27,300 women in the US are expected to die from colorectal cancer. Colorectal cancer will account for 11% of new cancer cases and 10% of all cancer deaths in US women. Age is a primary risk factor for colorectal cancer, with 91% of new cases and 94% of deaths from colorectal cancer occurring in individuals over the age of 50 years. Family history, obesity, diet and physical inactivity are also primary risk factors for colorectal cancer. 1- and 5-year survival rates for individuals newly diagnosed with colorectal cancer are 83% and 63%, respectively. 10-year survival is 57%. With early detection, 5-year survival is 90%. However, only 39% of colorectal cancers are diagnosed at an early, localized stage (stage 12). When colorectal cancer is diagnosed with regional metastases to adjacent organs or lymph nodes, 5-year survival decreases to 67%. 5-year survival for patients with distant metastases is 10%. American Cancer Society. Cancer Facts and Figures Available at: Accessed 6/5/06. American Cancer Society. Cancer Facts and Figures Available at: and
. When colorectal cancer is diagnosed with regional metastases to adjacent organs or lymph nodes, 5-year survival decreases to 67%. 5-year survival for patients with distant metastases is 10%. American Cancer Society. Cancer Facts and Figures Available at: sitearea= Accessed 6/5/06. American Cancer Society. Cancer Facts and Figures Available at: rnav=criov&dt=10. and sitearea=")
10
WHI E+P Trial: Risk of Colorectal Cancer
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E+P Trial: Risk of Colorectal Cancer Kaplan-Meier Estimate HR = % nCI = 0.38– % aCI = 0.33–0.94 Placebo E+P The WHI E+P trial reported a significant reduction in invasive colorectal cancers in women assigned to E+P compared with placebo (HR, 0.56; 95% nCI, 0.38–0.81; 95% aCI, 0.33–0.94).1 This figure shows the Kaplan-Meier plots of the cumulative hazard of invasive colorectal cancer for both the E+P and placebo groups. As indicated by the plots, the difference in incidence began to emerge early in the first year of follow-up, suggesting an effect of E+P on established cancers. The invasive colorectal cancers in the E+P and placebo groups were similar in location, tumor grade, and histologic features (ie, adenocarcinoma, not otherwise specified; in adenomatous polyp; in tubulovillous adenoma; or in villous adenoma). However, cancers in the E+P group had a greater number of positive lymph nodes (mean ± SD, 3.2 ± 4.1 vs 0.8 ± 1.7; P = .002), compared with placebo, and were more advanced (regional or metastatic disease, 76.2% vs 48.5%; P = .004). The reasons for these differences are unknown. It should be noted that no difference in mortality was observed between the E+P and placebo groups. Exploratory analyses indicated that among those women in the E+P group who were diagnosed with colorectal cancer, those with antecedent vaginal bleeding had cancers with a greater number of positive nodes, compared with those women who did not have vaginal bleeding (3.8 ± 4.3 vs 0.7 ± 1.5, P = .006). Abdominal pain, a change in bowel habits, and rectal bleeding are common symptoms in patients who present with colorectal cancer. The authors speculated that in some women assigned to E+P, perineal bleeding may have been perceived as vaginal bleeding which could have led to a delay in seeking care and a higher rate of advanced cancers in the E+P group. Given this possibility, wider implementation of bowel screening among postmenopausal women using HT was recommended. The American Cancer Society recently reported that the proportion of the US population 50 years and older that has been screened for colorectal cancer remains low (less than 50%).2 Chlebowski RT, et al. N Engl J Med. 2004;350: 1Chlebowski RT, et al. N Engl J Med. 2004;350: 2American Cancer Society. Colorectal Cancer Facts & Figures Special Edition Atlanta: American Cancer Society, 2005.
.1 This figure shows the Kaplan-Meier plots of the cumulative hazard of invasive colorectal cancer for both the E+P and placebo groups. As indicated by the plots, the difference in incidence began to emerge early in the first year of follow-up, suggesting an effect of E+P on established cancers. The invasive colorectal cancers in the E+P and placebo groups were similar in location, tumor grade, and histologic features (ie, adenocarcinoma, not otherwise specified; in adenomatous polyp; in tubulovillous adenoma; or in villous adenoma). However, cancers in the E+P group had a greater number of positive lymph nodes (mean ± SD, 3.2 ± 4.1 vs 0.8 ± 1.7; P = .002), compared with placebo, and were more advanced (regional or metastatic disease, 76.2% vs 48.5%; P = .004). The reasons for these differences are unknown. It should be noted that no difference in mortality was observed between the E+P and placebo groups. Exploratory analyses indicated that among those women in the E+P group who were diagnosed with colorectal cancer, those with antecedent vaginal bleeding had cancers with a greater number of positive nodes, compared with those women who did not have vaginal bleeding (3.8 ± 4.3 vs 0.7 ± 1.5, P = .006). Abdominal pain, a change in bowel habits, and rectal bleeding are common symptoms in patients who present with colorectal cancer. The authors speculated that in some women assigned to E+P, perineal bleeding may have been perceived as vaginal bleeding which could have led to a delay in seeking care and a higher rate of advanced cancers in the E+P group. Given this possibility, wider implementation of bowel screening among postmenopausal women using HT was recommended. The American Cancer Society recently reported that the proportion of the US population 50 years and older that has been screened for colorectal cancer remains low (less than 50%).2. Chlebowski RT, et al. N Engl J Med. 2004;350: Chlebowski RT, et al. N Engl J Med. 2004;350: American Cancer Society. Colorectal Cancer Facts & Figures Special Edition Atlanta: American Cancer Society,")
11
WHI E-Alone Trial: Risk of Colorectal Cancer
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E-Alone Trial: Risk of Colorectal Cancer Kaplan-Meier Estimate HR = % nCI = 0.75– % aCI = 0.63–1.86 E Alone Placebo In the WHI E-alone trial, no significant difference in the rate of colorectal cancer was observed between the conjugated equine estrogens (CEE)-alone and placebo groups. (HR 1.08; 95% nCI 0.75–1.55).1 Thus, in contrast to the results from the WHI E+P trial,2 the overall data from the WHI E-alone trial do not support a benefit of CEE-alone for prevention of colorectal cancer in postmenopausal women who were on average 63 years of age when treatment was initiated. Women’s Health Initiative Steering Committee. JAMA. 2004;291: 1Women’s Health Initiative Steering Committee. JAMA. 2004;291: 2Chlebowski RT, et al. N Engl J Med. 2004;350:
-alone and placebo groups. (HR 1.08; 95% nCI 0.75–1.55).1. Thus, in contrast to the results from the WHI E+P trial,2 the overall data from the WHI E-alone trial do not support a benefit of CEE-alone for prevention of colorectal cancer in postmenopausal women who were on average 63 years of age when treatment was initiated. Women’s Health Initiative Steering Committee. JAMA. 2004;291: Women’s Health Initiative Steering Committee. JAMA. 2004;291: Chlebowski RT, et al. N Engl J Med. 2004;350:")
12
2Chlebowski RT, et al. N Engl J Med. 2004;350:991-1004.
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E+P Trial: What Do the Results Mean for Absolute Risk of Colorectal Cancer? A 50-year-old woman in the US has an approximate 0.5% chance of developing colorectal cancer by age 60 years1 This translates to an absolute risk of 5.0 cases per 1000 women HR for colorectal cancer = 0.56 after 5.6 years of E+P use in the WHI (a 44% reduction in risk)2 This translates into an absolute risk of 2.8 cases per 1000 E+P users The National Cancer Institute estimates that a 50-year-old woman has a 0.5% chance of developing colorectal cancer before she turns 60 years old.1 Therefore, among year-old women, under usual conditions, 5 are at risk for being diagnosed with colorectal cancer over the course of the next 10 years. The WHI E+P results suggest that combination HT may reduce the risk of developing colorectal cancer by 44%,2 which in the example given above, translates to an absolute risk of 2.8 cases of colorectal cancer per 1,000 users (rather than the 5 per 1000 women expected under usual conditions). HR = hazard ratio. 1Available at: Accessed 6/5/2006. 2Chlebowski RT, et al. N Engl J Med. 2004;350: 1Feuer EJ, Wun LM. Available at: Accessed 1/24/04. 2Chlebowski RT, et al. N Engl J Med. 2004;350:
2. This translates into an absolute risk of 2.8 cases per 1000 E+P users. The National Cancer Institute estimates that a 50-year-old woman has a 0.5% chance of developing colorectal cancer before she turns 60 years old.1 Therefore, among year-old women, under usual conditions, 5 are at risk for being diagnosed with colorectal cancer over the course of the next 10 years. The WHI E+P results suggest that combination HT may reduce the risk of developing colorectal cancer by 44%,2 which in the example given above, translates to an absolute risk of 2.8 cases of colorectal cancer per 1,000 users (rather than the 5 per 1000 women expected under usual conditions). HR = hazard ratio. 1Available at: site=Colon%20and%20Rectum%20Cancer&stat=Lifetime%20Risk. Accessed 6/5/ Chlebowski RT, et al. N Engl J Med. 2004;350: Feuer EJ, Wun LM. Available at: Accessed 1/24/04. 2Chlebowski RT, et al. N Engl J Med. 2004;350:")
13
Reduced Risk of Death From Colorectal Cancer in Ever-Users of HT
4/11/2017 5:11 AM LMF/FM 2004 Oncology Reduced Risk of Death From Colorectal Cancer in Ever-Users of HT Calle et al, 1995 Sturgeon et al, 1995 Persson et al, 1996 Meta-analysis: Nanda et al, 1999 Several observational studies and a meta-analysis have examined the relationship between HT and colorectal cancer mortality and incidence.1-4 Calle et al1 investigated 897 colon cancer-related deaths among 422,373 postmenopausal women. Approximately 33% of the women who died had a history of HT use. Ever-use of HT was associated with a decreased risk of fatal colon cancer (RR, 0.71; 95% CI, 0.61–0.83); the effect was strongest among recent and long-term users. Sturgeon et al2 evaluated colon cancer-related deaths among a cohort of 49,000 women. A total of 1,824 deaths occurred among the participants (807 deaths among HT users and 1,017 deaths among never-users); 647 deaths were cancer related. Among HT users, 43 deaths were related to colon cancer versus 46 deaths among never-users (RR, 0.8; 95% CI, 0.6–1.3 compared with never-users). Persson and colleagues3 followed a cohort of 22,597 Swedish HT users for 13 years to evaluate colon cancer incidence and mortality in this population. Eight hundred forty-eight cancer deaths occurred, of which 62 (7.3%) were related to colon cancer. These investigators reported that HT users had a decreased risk of dying from colon cancer compared with nonusers (RR, 0.7; 95% CI, 0.5–0.9). A meta-analysis by Nanda and colleagues4 looked at the association between HT and risk of developing or dying from colorectal cancer. The investigators found that HT users had a reduced risk of dying from colon cancer compared with nonusers (RR, 0.72; 95% CI, 0.64–0.81). They also found that recent HT users had a reduced risk of developing colon cancer (RR, 0.67; 95% CI, 0.59–0.77) compared with never-users. The reduction in risk for ever-users was not statistically significant. Duration of use was also not a significant factor. 0.5 1.0 10 2.0 Relative Risk (95% CI) 1Calle EE, et al. J Natl Cancer Inst. 1995;87: 2Sturgeon SR, et al. Epidemiology. 1995;6: 3Persson I, et al. Int J Cancer. 1996;67: 4Nanda K, et al. Obstet Gynecol. 1999;93:880-8.
; the effect was strongest among recent and long-term users. Sturgeon et al2 evaluated colon cancer-related deaths among a cohort of 49,000 women. A total of 1,824 deaths occurred among the participants (807 deaths among HT users and 1,017 deaths among never-users); 647 deaths were cancer related. Among HT users, 43 deaths were related to colon cancer versus 46 deaths among never-users (RR, 0.8; 95% CI, 0.6–1.3 compared with never-users). Persson and colleagues3 followed a cohort of 22,597 Swedish HT users for 13 years to evaluate colon cancer incidence and mortality in this population. Eight hundred forty-eight cancer deaths occurred, of which 62 (7.3%) were related to colon cancer. These investigators reported that HT users had a decreased risk of dying from colon cancer compared with nonusers (RR, 0.7; 95% CI, 0.5–0.9). A meta-analysis by Nanda and colleagues4 looked at the association between HT and risk of developing or dying from colorectal cancer. The investigators found that HT users had a reduced risk of dying from colon cancer compared with nonusers (RR, 0.72; 95% CI, 0.64–0.81). They also found that recent HT users had a reduced risk of developing colon cancer (RR, 0.67; 95% CI, 0.59–0.77) compared with never-users. The reduction in risk for ever-users was not statistically significant. Duration of use was also not a significant factor Relative Risk (95% CI) 1Calle EE, et al. J Natl Cancer Inst. 1995;87: Sturgeon SR, et al. Epidemiology. 1995;6: Persson I, et al. Int J Cancer. 1996;67: Nanda K, et al. Obstet Gynecol. 1999;93:")
14
HT and Colorectal Cancer Risk: Summary
4/11/2017 5:11 AM LMF/FM 2004 Oncology HT and Colorectal Cancer Risk: Summary WHI E+P Trial Colorectal cancer reduced with E+P vs placebo Results consistent with earlier studies showing protective effect Greater proportion of advanced cancers in E+P users requires further study No difference in mortality, E+P vs placebo WHI E-Alone Trial No significant difference in colorectal cancer rates in E-alone vs placebo E+P users in the WHI had a significantly reduced risk of colorectal cancer—a finding that is consistent with results from several other studies, however there are also epidemiological studies which have not observed an association between E+P and reduced cancer incidence. Findings of greater proportion of advanced cancers in E+P users requires further study and suggests a need for expanded colorectal screening in postmenopausal women. The evidence from the WHI E-alone trial does not support a protective effect of unopposed estrogen in older, hysterectomized, postmenopausal women.

15
Ovarian Cancer 20,180 new cases expected in the US in 2006
4/11/2017 5:11 AM LMF/FM 2004 Oncology Ovarian Cancer 20,180 new cases expected in the US in 2006 Accounts for 3% of all cancers in women 2nd most common gynecologic cancer 15,310 deaths from ovarian cancer expected in 2006 Causes more deaths than cervical and uterine cancer combined; ranks 5th in cancer deaths among women. Risk increases with age; peaks in late 70s ~2/3 of diagnosed women are over age 50 Mutations of BRCA genes increase a woman’s lifetime risk to 26% (BRCA1) and 10% (BRCA2) Use of oral contraceptives reduces risk primarily related to pre-menopausal use According to the American Cancer Society, ovarian cancer is the second most common gynecologic cancer and is expected to account for 3% of new cancer cases in 2006 and 6% of cancer deaths in women.1 An estimated 20,180 new cases of ovarian cancer will be diagnosed in the US in 2006, and 15,310 women are expected to die from the disease this year.1 Risk increases as women approach their late 70s and early 80s, and almost 50% of patients will be 65 years or older. Pregnancy, tubal ligation, and the use of oral contraceptives reduce a woman’s risk of ovarian cancer. 2 Family history is a primary risk factor for ovarian cancer. Women with a first-degree relative (mother, daughter, or sister) with ovarian cancer have an elevated risk of developing the disease themselves. Women with two or more first-degree relatives with ovarian cancer have even higher risk. 3 Mutations of BRCA1 and BRCA2 genes increase a woman’s lifetime risk for ovarian cancer to 26% (BRCA1) and 10% (BRCA2).4 These mutations are also associated with a substantially increased risk for breast cancer. Age at time of diagnosis influences survival. Women younger than 65 years of age have nearly double the 5-year survival rate of women 65 years and older (56% vs 29%). Overall, 1- and 5-year survival rates for newly diagnosed patients are 77% and 44%, respectively.1 When diagnosed at a localized stage IA, 5-year survival is 92.7%. Only 19% of cases are detected at this stage.1 5-year survival rates for women with regional and distant metastases at the time of diagnosis are 69% and 29%, respectively.1 Over the past 20 years, ovarian cancer incidence and mortality has declined for younger generations in most developing countries, particularly those where oral contraceptive use spread earlier. The overall estimated protection from cohort and case control studies is approximately 30% for ever OC users, and increases with duration of use by ~5% per year of use to ~50% for long term use of 10 or more years.5 The favorable effects persists for at least 20 years after OC use has ceased and is not confined to any particular OC formulation. The reduced risk is observed in women with or without family history or genetic predisposition to ovarian cancer.5 American Cancer Society. Cancer Facts and Figures Available at: Accessed 6/5/06. Nelson HD, et al. Ann Intern Med. 2005;143: La Veccia C. Eur J Cancer Prev. 2006;15:117-24 1American Cancer Society. Cancer Facts and Figures revised: 05/22/2006. Available at: and 2Schneider HP. Maturitas. 2002;43:S35-S52. 3Piver MS, et al. Cancer. 1993;71(suppl):582-8. 4Nelson HD, et al. Ann Intern Med. 2005;143: 5La Veccia C. Eur J Cancer Prev. 2006;15:117-24
 and 10% (BRCA2) Use of oral contraceptives reduces risk. primarily related to pre-menopausal use. According to the American Cancer Society, ovarian cancer is the second most common gynecologic cancer and is expected to account for 3% of new cancer cases in 2006 and 6% of cancer deaths in women.1. An estimated 20,180 new cases of ovarian cancer will be diagnosed in the US in 2006, and 15,310 women are expected to die from the disease this year.1. Risk increases as women approach their late 70s and early 80s, and almost 50% of patients will be 65 years or older. Pregnancy, tubal ligation, and the use of oral contraceptives reduce a woman’s risk of ovarian cancer. 2. Family history is a primary risk factor for ovarian cancer. Women with a first-degree relative (mother, daughter, or sister) with ovarian cancer have an elevated risk of developing the disease themselves. Women with two or more first-degree relatives with ovarian cancer have even higher risk. 3. Mutations of BRCA1 and BRCA2 genes increase a woman’s lifetime risk for ovarian cancer to 26% (BRCA1) and 10% (BRCA2).4 These mutations are also associated with a substantially increased risk for breast cancer. Age at time of diagnosis influences survival. Women younger than 65 years of age have nearly double the 5-year survival rate of women 65 years and older (56% vs 29%). Overall, 1- and 5-year survival rates for newly diagnosed patients are 77% and 44%, respectively.1. When diagnosed at a localized stage IA, 5-year survival is 92.7%. Only 19% of cases are detected at this stage.1. 5-year survival rates for women with regional and distant metastases at the time of diagnosis are 69% and 29%, respectively.1. Over the past 20 years, ovarian cancer incidence and mortality has declined for younger generations in most developing countries, particularly those where oral contraceptive use spread earlier. The overall estimated protection from cohort and case control studies is approximately 30% for ever OC users, and increases with duration of use by ~5% per year of use to ~50% for long term use of 10 or more years.5 The favorable effects persists for at least 20 years after OC use has ceased and is not confined to any particular OC formulation. The reduced risk is observed in women with or without family history or genetic predisposition to ovarian cancer.5. American Cancer Society. Cancer Facts and Figures Available at: Accessed 6/5/06. Nelson HD, et al. Ann Intern Med. 2005;143: La Veccia C. Eur J Cancer Prev. 2006;15: American Cancer Society. Cancer Facts and Figures revised: 05/22/2006. Available at: rnav=cri and 2Schneider HP. Maturitas. 2002;43:S35-S52. 3Piver MS, et al. Cancer. 1993;71(suppl): Nelson HD, et al. Ann Intern Med. 2005;143: La Veccia C. Eur J Cancer Prev. 2006;15:")
16
WHI E+P Trial: Effect of HT on Risk of Invasive Ovarian Cancer
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E+P Trial: Effect of HT on Risk of Invasive Ovarian Cancer Placebo E+P 95% nCI 95% aCI 0.1 0.5 1.0 5.0 2.0 The WHI E+P trial reported a small, nonsignificant increase in ovarian cancer risk in women assigned to E+P compared with those assigned to placebo (HR, 1.58; 95% nCI, 0.77–3.24; 95% aCI, 0.59–4.23).1 Average follow-up time for the women included in this analysis was 5.6 years. The annual incidence rate for ovarian cancer observed among the total study population was 34 cases per 100,000 person-years. This rate is lower than the National Cancer Institute’s Surveillance, Epidemiology, and End Results population-based rate of 52 cases per 100,000 person-years in women in the same age range as the WHI participants.2 The WHI investigators found no differences between treatment groups in histology, grade, or stage of disease at diagnosis. In addition, no significant interactions between group assignment and any of the following variables were observed: age, race/ethnicity, body mass index (BMI), family history of breast or ovarian cancer, family history of colorectal cancer, prior use of oral contraceptives, prior exposure to E alone, or prior use of E+P.1 In summary, the incidence of ovarian cancer among E+P users in the WHI was somewhat greater than that observed in the placebo group, although the difference was small and not statistically significant. The authors concluded that continuous combined E+P may increase the risk of ovarian cancer. They added, however, that due to the low rates of ovarian and other gynecologic cancers in the study population and the limited precision of the risk estimates, “the results should not have an appreciable influence on most women’s decision-making when seeking relief for moderate-to-severe vasomotor symptoms.”1 Hazard Ratio Incidence rate of invasive ovarian cancer for the total study population was 34 cases per 100,000 person-years. Anderson GL, et al. JAMA. 2003;290: 1Anderson GL, et al. JAMA. 2003;290: 2National Cancer Institute, Surveillance, Epidemiology and End Results (SEER); Search Cancer Statistics Review, : (XXI:379) Age-Adjusted SEER Incidence Rates and SEER Death Rates by Registry (Ovary) Accessed 6/5/2006.
.1 Average follow-up time for the women included in this analysis was 5.6 years. The annual incidence rate for ovarian cancer observed among the total study population was 34 cases per 100,000 person-years. This rate is lower than the National Cancer Institute’s Surveillance, Epidemiology, and End Results population-based rate of 52 cases per 100,000 person-years in women in the same age range as the WHI participants.2. The WHI investigators found no differences between treatment groups in histology, grade, or stage of disease at diagnosis. In addition, no significant interactions between group assignment and any of the following variables were observed: age, race/ethnicity, body mass index (BMI), family history of breast or ovarian cancer, family history of colorectal cancer, prior use of oral contraceptives, prior exposure to E alone, or prior use of E+P.1. In summary, the incidence of ovarian cancer among E+P users in the WHI was somewhat greater than that observed in the placebo group, although the difference was small and not statistically significant. The authors concluded that continuous combined E+P may increase the risk of ovarian cancer. They added, however, that due to the low rates of ovarian and other gynecologic cancers in the study population and the limited precision of the risk estimates, the results should not have an appreciable influence on most women’s decision-making when seeking relief for moderate-to-severe vasomotor symptoms. 1. Hazard Ratio. Incidence rate of invasive ovarian cancer for the total study population was 34 cases per 100,000 person-years. Anderson GL, et al. JAMA. 2003;290: Anderson GL, et al. JAMA. 2003;290: National Cancer Institute, Surveillance, Epidemiology and End Results (SEER); Search Cancer Statistics Review, : (XXI:379) Age-Adjusted SEER Incidence Rates and SEER Death Rates by Registry (Ovary) Accessed 6/5/2006.")
17
Meta-Analyses Evaluating HT Use and Risk of Ovarian Cancer
4/11/2017 5:11 AM LMF/FM 2004 Oncology Meta-Analyses Evaluating HT Use and Risk of Ovarian Cancer Garg et al, 1998 Coughlin et al, 2000 Relative Risk (95% CI) The overall findings from research evaluating the association between HT and ovarian cancer are equivocal. The two meta-analyses illustrated above reported ovarian cancer risk estimates of 1.15 (95% CI, 1.05–1.27)1 and 1.1 (95% CI, 0.9–1.3)2 for HT ever-users. Available data exclude a strong association between HT and epithelial ovarian cancer, though a moderate association remains open to debate. The US Preventive Services Task Force has concluded that evidence was insufficient to determine the effect of HT on ovarian cancer.3 Garg PP, et al. Obstet Gynecol. 1998;92:472-9. Coughlin SS, et al. J Clin Epidemiol. 2000;53: 1Garg PP, et al. Obstet Gynecol. 1998;92:472-9. 2Coughlin SS, et al. J Clin Epidemiol. 2000;53: 3U.S. Preventive Services Task Force. Ann Intern Med. 2005;142:
 The overall findings from research evaluating the association between HT and ovarian cancer are equivocal. The two meta-analyses illustrated above reported ovarian cancer risk estimates of 1.15 (95% CI, 1.05–1.27)1 and 1.1 (95% CI, 0.9–1.3)2 for HT ever-users. Available data exclude a strong association between HT and epithelial ovarian cancer, though a moderate association remains open to debate. The US Preventive Services Task Force has concluded that evidence was insufficient to determine the effect of HT on ovarian cancer.3. Garg PP, et al. Obstet Gynecol. 1998;92: Coughlin SS, et al. J Clin Epidemiol. 2000;53: Garg PP, et al. Obstet Gynecol. 1998;92: Coughlin SS, et al. J Clin Epidemiol. 2000;53: U.S. Preventive Services Task Force. Ann Intern Med. 2005;142:")
18
Kotsopoulos J et al. Gynecol Oncol. 2006;100:83-8
4/11/2017 5:11 AM LMF/FM 2004 Oncology HT Does Not Increase the Risk of Ovarian Cancer in BRCA1 and BRCA2 Mutation Carriers Group Adjusted Odds Ratio P value Never Users 1.00 [95% CI ( referent )] Ever Users 0.93 [95% CI ( )] 0.79 BRCA1 Ever 1.13 [95% CI ( )] 0.67 BRCA2 Ever 1.08 [95% CI ( )] 0.87 In a first study to specifically address the role of HT use on the risk of hereditary ovarian cancer, HT associated risk of ovarian cancers in BRCA1 and BRCA2 carriers was evaluated in a matched case-control study of 162 matched sets of women . HT did not appear to adversely influence the risk of ovarian cancer in BRCA1 or BRCA2 mutation carriers. Compared to those who never used HT, the odds ratio associated with ever use of HT was 0.93 (95% CI= ) and the odds ratio associated with BRCA1 ever use, or BRCA2 ever use was 1.13 [95% CI ( )] and 1.08 [95% CI ( )] respectively.1 Women who had been diagnosed with ovarian cancer were matched to control subjects by mutation, year of birth, and age at menopause. Information of HT use Was derived from a questionnaire routinely administered to women who were found to be carriers of a mutation in either gene. Only women who reached natural menopause were included in this study. While the possibility of recall bias cannot be excluded in self-reported exclusion data, others have shown a high level of concordance between HT use obtained through a questionnaire and information obtained from prescription forms.2 Adding to its strength, the study was based on known mutation carriers and included patients from numerous participating centers and of different ethnic backgrounds. Kotsopoulos J et al. Gynecol Oncol. 2006;100:83-8 1Kotsopoulos J et al. Gynecol Oncol. 2006;100:83-8 2Persson I, et al. Int J Epidemiol 1987;16(2):222– 8.
] Ever Users 0.93 [95% CI ( )] BRCA1 Ever 1.13 [95% CI ( )] BRCA2 Ever 1.08 [95% CI ( )] In a first study to specifically address the role of HT use on the risk of hereditary ovarian cancer, HT associated risk of ovarian cancers in BRCA1 and BRCA2 carriers was evaluated in a matched case-control study of 162 matched sets of women . HT did not appear to adversely influence the risk of ovarian cancer in BRCA1 or BRCA2 mutation carriers. Compared to those who never used HT, the odds ratio associated with ever use of HT was 0.93 (95% CI= ) and the odds ratio associated with BRCA1 ever use, or BRCA2 ever use was 1.13 [95% CI ( )] and 1.08 [95% CI ( )] respectively.1. Women who had been diagnosed with ovarian cancer were matched to control subjects by mutation, year of birth, and age at menopause. Information of HT use Was derived from a questionnaire routinely administered to women who were found to be carriers of a mutation in either gene. Only women who reached natural menopause were included in this study. While the possibility of recall bias cannot be excluded in self-reported exclusion data, others have shown a high level of concordance between HT use obtained through a questionnaire and information obtained from prescription forms.2 Adding to its strength, the study was based on known mutation carriers and included patients from numerous participating centers and of different ethnic backgrounds. Kotsopoulos J et al. Gynecol Oncol. 2006;100: Kotsopoulos J et al. Gynecol Oncol. 2006;100: Persson I, et al. Int J Epidemiol 1987;16(2):222– 8.")
19
HT and Ovarian Cancer Risk: Summary
4/11/2017 5:11 AM LMF/FM 2004 Oncology HT and Ovarian Cancer Risk: Summary Research findings are inconsistent for post-menopausal use. If increased risk exists, it is small and difficult to demonstrate from study to study Possible weak association with long-term (>10 years) use of unopposed E, but data are inconclusive Overall, data are not sufficient for clinical recommendations1 Due to inconsistencies in the available data, the association between HT use and ovarian cancer outcomes requires further investigation. Small differences in risk from study to study could be explained by varying distribution of other factors that influence the risk of ovarian cancer in the populations under study. Examples of these factors include duration of oral contraceptive use, infertility, fertility drug use, number of pregnancies, and duration of breast feeding . Pre-menopausal use of oral contraceptives (E+P) appears protective and any contradictory findings may possibly be due to differences in the pre- and post-menopausal state. 1 U.S. Preventive Services Task Force. Ann Intern Med May 17;142(10):
 use of unopposed E, but data are inconclusive. Overall, data are not sufficient for clinical recommendations1. Due to inconsistencies in the available data, the association between HT use and ovarian cancer outcomes requires further investigation. Small differences in risk from study to study could be explained by varying distribution of other factors that influence the risk of ovarian cancer in the populations under study. Examples of these factors include duration of oral contraceptive use, infertility, fertility drug use, number of pregnancies, and duration of breast feeding . Pre-menopausal use of oral contraceptives (E+P) appears protective and any contradictory findings may possibly be due to differences in the pre- and post-menopausal state. 1 U.S. Preventive Services Task Force. Ann Intern Med May 17;142(10):")
20
4/11/2017 5:11 AM LMF/FM 2004 Oncology Breast Cancer Among women in the US, breast cancer is the most common diagnosed non-skin cancer and the 2nd leading cause of cancer-related deaths. National Cancer Institute 2006 estimates: 212,920 new cases of breast cancer and 40,970 deaths A woman’s risk of developing breast cancer in her life time is currently estimated to be 1 in 7.56 (1 in 8) irrespective of HT use Among women, breast cancer is the most commonly diagnosed cancer after nonmelanoma skin cancer, and is the second leading cause of cancer deaths after lung cancer. In 2006, an estimated 212,920 new cases will be diagnosed, and 40,970 deaths from breast cancer will occur. The age-adjusted incidence rate was per 100,000 women per year. These rates are based on cases diagnosed in from 17 SEER geographic areas.1-3 Well-established factors for increased risk of breast cancer include: personal history of breast cancer (in situ or invasive), family history and BRCA1 and BRCA2 mutation carrier status, advanced age, nulliparity, late first parity, early menarche, late menopause, ionizing radiation exposure, hormone therapy [HT] (primarily associated with combination estrogen + progestin), obesity in non-HT users, alcohol consumption (dose-dependent increased risk).2 current National Cancer Institute (NCI) statistics show that 1 in 8 women will develop breast cancer in their lifetime regardless of whether HT is used.3 National Cancer Institute: 1Ries LAG, Eisner MP, Kosary CL, et al. (eds). SEER Cancer Statistics Review, 1975–2002, National Cancer Institute. Bethesda, MD, 2005 ( 2National Cancer Institute. Bethesda, MD. Breast Cancer (PDQ®): Prevention Last Modified: 05/23/ Accessed 06/07/06. 3National Cancer Institute: Last accessed June 7,2006.
 irrespective of HT use. Among women, breast cancer is the most commonly diagnosed cancer after nonmelanoma skin cancer, and is the second leading cause of cancer deaths after lung cancer. In 2006, an estimated 212,920 new cases will be diagnosed, and 40,970 deaths from breast cancer will occur. The age-adjusted incidence rate was per 100,000 women per year. These rates are based on cases diagnosed in from 17 SEER geographic areas.1-3. Well-established factors for increased risk of breast cancer include: personal history of breast cancer (in situ or invasive), family history and BRCA1 and BRCA2 mutation carrier status, advanced age, nulliparity, late first parity, early menarche, late menopause, ionizing radiation exposure, hormone therapy [HT] (primarily associated with combination estrogen + progestin), obesity in non-HT users, alcohol consumption (dose-dependent increased risk).2. current National Cancer Institute (NCI) statistics show that 1 in 8 women will develop breast cancer in their lifetime regardless of whether HT is used.3. National Cancer Institute: viewid=6bc9885b-da a-c2c7170fc548&version=1#Section_339. 1Ries LAG, Eisner MP, Kosary CL, et al. (eds). SEER Cancer Statistics Review, 1975–2002, National. Cancer Institute. Bethesda, MD, 2005 ( 2National Cancer Institute. Bethesda, MD. Breast Cancer (PDQ®): Prevention. Last Modified: 05/23/2006. Accessed 06/07/06. 3National Cancer Institute: viewid=6bc9885b-da a-c2c7170fc548&version=1#Section_339. Last accessed June 7,2006.")
21
Meme Kanseri Risk Faktörleri (RR>4)
Yaş BRCA1 ve BRCA2 mutasyonları Postmenopozal dens (yoğun) meme
 meme.")
22
Risk of Breast Cancer Changes With a Woman’s Age
4/11/2017 5:11 AM LMF/FM 2004 Oncology Risk of Breast Cancer Changes With a Woman’s Age Age (years) Probability of Developing Breast Cancer Within 10 Years 20 0.05% (1 in 2044) 30 0.40% (1 in 249) 40 1.49% (1 in 67) 50 2.77% (1 in 36) 60 3.45% (1 in 29) 70 4.16% (1 in 24) A woman’s risk of breast cancer increases with age. As shown, risk of breast cancer is less than one half of 1% for a woman under 30 years of age, but risk increases more than 10-fold for a 70-year-old woman.1 Thus, a 20% to 40% increased risk of breast cancer results in a much different increase in absolute risk in women around age 50 years compared with women around age 70 years or older. NCI Update 2006 shows little change: A woman’s chance of being diagnosed with breast cancer is: from age 30 through age 39, 0.44% (1 in 229);from age 40 through age 49, 1.46% (1 in 68);from age 50 through age 59, 2.73% (1 in 37);from age 60 through age 69, 3.82% (1 in 26).2 From , the median age at diagnosis for cancer of the breast was 61 years of age. Approximately 0.0% were diagnosed under age 20; 1.9% between 20 and 34; 10.6% between 35 and 44; 22.1% between 45 and 54; 22.8% between 55 and 64; 20.4% between 65 and 74; 16.8% between 75 and 84; and 5.4% 85+ years of age.2 American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001– Available at: http// 1American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001–2002. Available at: http// 2National Cancer Institute. SEER Cancer Stat Fact Sheets, Cancer of the breast. Available at: Accessed June 7, Based on: Ries LAG, Harkins D, Krapcho M, Mariotto A, Miller BA, Feuer EJ, Clegg L, Eisner MP, Horner MJ, Howlader N, Hayat M, Hankey BF, Edwards BK (eds). SEER Cancer Statistics Review, , National Cancer Institute. Bethesda, MD, based on November 2005 SEER data submission, posted to the SEER web site Cancer Stat Fact Sheets, Cancer of the breast; Available at:
 Probability of Developing Breast Cancer Within 10 Years % (1 in 2044) % (1 in 249) % (1 in 67) % (1 in 36) % (1 in 29) % (1 in 24) A woman’s risk of breast cancer increases with age. As shown, risk of breast cancer is less than one half of 1% for a woman under 30 years of age, but risk increases more than 10-fold for a 70-year-old woman.1. Thus, a 20% to 40% increased risk of breast cancer results in a much different increase in absolute risk in women around age 50 years compared with women around age 70 years or older. NCI Update 2006 shows little change: A woman’s chance of being diagnosed with breast cancer is: from age 30 through age 39, 0.44% (1 in 229);from age 40 through age 49, 1.46% (1 in 68);from age 50 through age 59, 2.73% (1 in 37);from age 60 through age 69, 3.82% (1 in 26).2. From , the median age at diagnosis for cancer of the breast was 61 years of age. Approximately 0.0% were diagnosed under age 20; 1.9% between 20 and 34; 10.6% between 35 and 44; 22.1% between 45 and 54; 22.8% between 55 and 64; 20.4% between 65 and 74; 16.8% between 75 and 84; and 5.4% 85+ years of age.2. American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001–2002. Available at: http// 1American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001–2002. Available at: http// 2National Cancer Institute. SEER Cancer Stat Fact Sheets, Cancer of the breast. Available at: Accessed June 7, Based on: Ries LAG, Harkins D, Krapcho M, Mariotto A, Miller BA, Feuer EJ, Clegg L, Eisner MP, Horner MJ, Howlader N, Hayat M, Hankey BF, Edwards BK (eds). SEER Cancer Statistics Review, , National Cancer Institute. Bethesda, MD, based on November 2005 SEER data submission, posted to the SEER web site Cancer Stat Fact Sheets, Cancer of the breast; Available at:")
23
Meme Kanseri Risk Faktörleri RR:2.1-4
↑ postmenopozal kemik yoğunluğu, meme biyopsisinde atipik hiperplazi Birinci derece akrabada meme kanseri öyküsü

24
Meme Kanseri Risk Faktörleri RR:1.1-2.0
ilk gebelik>30 menarş <12 yaşından, menopoz yaşı > 55, nulliparite, hiç emzirmemiş olmak, postmenopozal obezite göğüs bölgesine yüksek doz radyasyon, günlük alkol alımı önceden tanı almış endometrium, over veya kolon kanseri

26
Absolute Risk of Breast Cancer in the General Population
4/11/2017 5:11 AM LMF/FM 2004 Oncology Absolute Risk of Breast Cancer in the General Population Each 50-year-old woman has approximately a 2.8% chance of developing breast cancer by age 60 years This translates to an absolute risk of 2.8 per 100 women All Women Aged 50 Years in the General Population— Risk for Breast Cancer by Age 60 Years In 100 women, 2.8 are at risk To address patients’ confusion regarding breast cancer risk, it may be helpful to discuss a woman’s absolute risk of breast cancer, with or without HT. Absolute risk is the overall incidence of a disease in a given population. For example, Feuer and colleagues estimated that a 50-year-old woman has a 2.8% chance of developing breast cancer before she turns 60 years of age. Therefore, among 100 women, 2.8 are at risk for breast cancer. American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001– Available at: http// American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001–2002. Available at: http//

27
Absolute Risk of Breast Cancer After 5 Years of HT
4/11/2017 5:11 AM LMF/FM 2004 Oncology Absolute Risk of Breast Cancer After 5 Years of HT WHI results indicate an HR for breast cancer of 1.24 after 5 years of HT use (a 24% increase in risk)1 This translates into an absolute risk of 3.5 per 100 users Risk of Breast Cancer by Age 60 Years After 5 Years of HT Use (Assuming a 24% Increase in Risk) 3.5 of 100 women who are HT users are at risk (<1 additional woman over baseline risk) Relative risk is different from absolute and attributable risk and should not be interpreted as such. Relative risk is the ratio of the risk of disease among those exposed to a risk factor to the risk among those who were not exposed and is independent of the overall incidence of disease in the population. The WHI reported that HT use was associated with an RR of breast cancer of Women using HT experienced a 24% increase in the risk of breast cancer compared with women taking placebo.1 Therefore, the absolute risk of breast cancer by age 60 years among 50-year-old women taking HT for 5.2 years is 3.5 per 100 HT users.1,2 A discussion of the attributable risk associated with HT also may help patients put breast cancer risk with HT into perspective. Attributable risk refers to the excess risk of disease in patients exposed to a potential risk factor, above and beyond the risk expected in patients not exposed to the potential risk factor. In cohort studies evaluating breast cancer risk and HT use, attributable risk is calculated as the difference in incidence rates between users and nonusers. The attributable risk of breast cancer in HT users, or the excess risk of breast cancer in HT users versus nonusers, is the difference between the incidence rates of HT users compared with nonusers. Therefore, the attributable risk of breast cancer in HT users who are 50 years of age is 0.7 per 100 women. 1Chlebowski RT, et al. JAMA. 2003;289: 1Chlebowski RT, et al. JAMA. 2003;289: 2American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001–2002. Available at: http//
1. This translates into an absolute risk of 3.5 per 100 users. Risk of Breast Cancer by Age 60 Years After 5 Years of HT Use (Assuming a 24% Increase in Risk) 3.5 of 100 women who are HT users are at risk (<1 additional woman over baseline risk) Relative risk is different from absolute and attributable risk and should not be interpreted as such. Relative risk is the ratio of the risk of disease among those exposed to a risk factor to the risk among those who were not exposed and is independent of the overall incidence of disease in the population. The WHI reported that HT use was associated with an RR of breast cancer of Women using HT experienced a 24% increase in the risk of breast cancer compared with women taking placebo.1 Therefore, the absolute risk of breast cancer by age 60 years among 50-year-old women taking HT for 5.2 years is 3.5 per 100 HT users.1,2. A discussion of the attributable risk associated with HT also may help patients put breast cancer risk with HT into perspective. Attributable risk refers to the excess risk of disease in patients exposed to a potential risk factor, above and beyond the risk expected in patients not exposed to the potential risk factor. In cohort studies evaluating breast cancer risk and HT use, attributable risk is calculated as the difference in incidence rates between users and nonusers. The attributable risk of breast cancer in HT users, or the excess risk of breast cancer in HT users versus nonusers, is the difference between the incidence rates of HT users compared with nonusers. Therefore, the attributable risk of breast cancer in HT users who are 50 years of age is 0.7 per 100 women. 1Chlebowski RT, et al. JAMA. 2003;289: Chlebowski RT, et al. JAMA. 2003;289: American Cancer Society, Surveillance Research, Breast Cancer Facts and Figures 2001–2002. Available at: http//")
28
Review of Observational Studies Published From 1975-2000
4/11/2017 5:11 AM LMF/FM 2004 Oncology Review of Observational Studies Published From E Alone (n = 45)* E+P (n = 20) In the past 25 years, more than 50 epidemiologic studies and six meta-analyses have examined the association between HT and breast cancer risk. Bush et al1 compiled the results from these studies and found a lack of consistency among the findings. Among studies that examined use of E-alone, 82% found no effect of E-alone use on breast cancer risk; 13% reported a modest increase in risk (>1.0 but not >2.0); and 2% reported a reduced risk of breast cancer with use of E-alone. The results from the WHI E-alone trial also indicate no increased risk of breast cancer with an average of 7 years of use.2 Results from observational studies on E+P followed a similar pattern: 80% of the studies found no effect of E+P use on breast cancer risk; 10% of the studies reported an elevated risk; and 10% of the studies reported a reduction in breast cancer risk. Preliminary data from the E+P arm of the WHI showed a small increase in risk that was not statistically significant. However, the risk estimate crossed the predetermined stopping boundary for breast cancer and, as a result, the E+P arm of the WHI was stopped.3 In summary, while the large majority of observational studies have failed to show any difference in breast cancer risk between HT users and nonusers, results from the WHI E+P trial indicate a small increase in risk with long-term use (>5 years) of E+P. *Percents do not total 100% because 1 study did not report confidence intervals; NS = not significant. Bush TL, et al. Obstet Gynecol. 2001;98: 1Bush TL, et al. Obstet Gynecol. 2001;98: 2Women's Health Initiative Steering Committee. JAMA. 2004;291: 3Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:
* E+P (n = 20) In the past 25 years, more than 50 epidemiologic studies and six meta-analyses have examined the association between HT and breast cancer risk. Bush et al1 compiled the results from these studies and found a lack of consistency among the findings. Among studies that examined use of E-alone, 82% found no effect of E-alone use on breast cancer risk; 13% reported a modest increase in risk (>1.0 but not >2.0); and 2% reported a reduced risk of breast cancer with use of E-alone. The results from the WHI E-alone trial also indicate no increased risk of breast cancer with an average of 7 years of use.2. Results from observational studies on E+P followed a similar pattern: 80% of the studies found no effect of E+P use on breast cancer risk; 10% of the studies reported an elevated risk; and 10% of the studies reported a reduction in breast cancer risk. Preliminary data from the E+P arm of the WHI showed a small increase in risk that was not statistically significant. However, the risk estimate crossed the predetermined stopping boundary for breast cancer and, as a result, the E+P arm of the WHI was stopped.3. In summary, while the large majority of observational studies have failed to show any difference in breast cancer risk between HT users and nonusers, results from the WHI E+P trial indicate a small increase in risk with long-term use (>5 years) of E+P. *Percents do not total 100% because 1 study did not report confidence intervals; NS = not significant. Bush TL, et al. Obstet Gynecol. 2001;98: Bush TL, et al. Obstet Gynecol. 2001;98: Women s Health Initiative Steering Committee. JAMA. 2004;291: Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:")
29
Yaşamın Bir Döneminde HRT Kullanılmış Olması ve Meme Kanseri Riski
LMF/FM 2004 Oncology Yaşamın Bir Döneminde HRT Kullanılmış Olması ve Meme Kanseri Riski Meta Analizler Armstrong ve ark, 1988 Dupont ve ark, 1991* Steinberg ve ark, 1991 Sillero-Arenas ve ark, 1992 Colditz ve ark, 1993 Grady ve ark, 1992 0,5 1,0 2,0 Rölatif Risk (%95 GA) *0,425 ya da daha az konjüge estrojen almış olan kadınlar.
 *0,425 ya da daha az konjüge estrojen almış olan kadınlar.")
30
Ortaklaşa Grup Analiz Tekrarı
4/11/2017 5:11 AM LMF/FM 2004 Oncology Ortaklaşa Grup Analiz Tekrarı Meme kanseri olan kadın Meme kanseri olmayan kadın 51 çalışma, 21 ülke Ana analizin temel aldığı veriler: Menopoz çağında olduğu bilinen postmenopozal kadın; (%33) HRT kullanıcısı vaka / kontrol Collaborative Group on Hormonal Factors in Breast Cancer. Lancet. 1997;350:
 HRT kullanıcısı vaka / kontrol. Collaborative Group on Hormonal Factors in Breast Cancer. Lancet. 1997;350:")
31
HRT ile Meme Kanseri Riski
4/11/2017 5:11 AM LMF/FM 2004 Oncology HRT ile Meme Kanseri Riski HRT Kullanımı RR Herhangi bir zamanda kullanmış Halen Kullanmakta Halen Kullanan >5 yıl Geçmişte kullanmış 1.14* 1.21* 1.35+ 1.07 *P < 0,01. Collaborative Group on Hormonal Factors in Breast Cancer . Lancet. 1997;350:

32
Ortaklaşa Analizin Tekrarı: Klinik Sonuçlar
4/11/2017 5:11 AM LMF/FM 2004 Oncology Ortaklaşa Analizin Tekrarı: Klinik Sonuçlar Tahmin Edilen Fazla Meme Kanseri Sayısı/1000 Kadın* Etkilenen Kullanıcıların Oranı HRT Süresi 5 yıl 10 yıl 15 yıl 2 6 12 0,2 0,6 1,2 *Her kullanım yılı ile riskte meydana gelen %2,3 artışı temel almaktadır. Collaborative Group on Hormonal Factors in Breast Cancer. Lancet. 1997;350:

33
Women’s Health Initiative (WHI) Clinical Trials of HT
4/11/2017 5:11 AM LMF/FM 2004 Oncology Women’s Health Initiative (WHI) Clinical Trials of HT Over 27,000 postmenopausal women were randomized between 1993 and 1998 Age at baseline ranged from 50 yrs–79 yrs Mean age, ~63 yrs Primary outcomes CHD (nonfatal MI, CHD death) Invasive breast cancer Approximately 8 yrs of follow-up planned Between 1993 and 1998, over 27,000 postmenopausal women between the ages of 50 and 79 years were enrolled in the WHI HT trials at 40 US clinical centers. Mean age at baseline was approximately 63 years. In the E+P trial, a total of 16,608 women without prior hysterectomy were randomly assigned to CEE/MPA or placebo.1 In the E-alone trial, a total of 10,739 women with prior hysterectomy were randomly assigned to CEE alone or placebo.2 The primary outcomes for both HT trials were CHD (acute myocardial infarction [MI], silent MI, or CHD death) and invasive breast cancer. The investigators also designed a “global index” as a summary measure of the overall balance of risks and benefits of HT.1 The global index is an unweighted index defined as the first event for each participant among the following: CHD, invasive breast cancer, stroke, pulmonary embolism, endometrial cancer, colorectal cancer, hip fracture, and death from other causes. The conditions included in the global index were those that the WHI investigators had determined to be important aspects of health benefits/risks that might be affected by long-term use of HT. A variety of other conditions were not part of the global index, including gallbladder disease, diabetes, menopausal symptoms, and cognitive function.. CHD = coronary heart disease; MI = myocardial infarction. Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: Women's Health Initiative Steering Committee. JAMA. 2004;291: 1Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: 2Women’s Health Initiative Steering Committee. JAMA. 2004;291:
 Clinical Trials of HT. Over 27,000 postmenopausal women were randomized between 1993 and Age at baseline ranged from 50 yrs–79 yrs. Mean age, ~63 yrs. Primary outcomes. CHD (nonfatal MI, CHD death) Invasive breast cancer. Approximately 8 yrs of follow-up planned. Between 1993 and 1998, over 27,000 postmenopausal women between the ages of 50 and 79 years were enrolled in the WHI HT trials at 40 US clinical centers. Mean age at baseline was approximately 63 years. In the E+P trial, a total of 16,608 women without prior hysterectomy were randomly assigned to CEE/MPA or placebo.1. In the E-alone trial, a total of 10,739 women with prior hysterectomy were randomly assigned to CEE alone or placebo.2. The primary outcomes for both HT trials were CHD (acute myocardial infarction [MI], silent MI, or CHD death) and invasive breast cancer. The investigators also designed a global index as a summary measure of the overall balance of risks and benefits of HT.1. The global index is an unweighted index defined as the first event for each participant among the following: CHD, invasive breast cancer, stroke, pulmonary embolism, endometrial cancer, colorectal cancer, hip fracture, and death from other causes. The conditions included in the global index were those that the WHI investigators had determined to be important aspects of health benefits/risks that might be affected by long-term use of HT. A variety of other conditions were not part of the global index, including gallbladder disease, diabetes, menopausal symptoms, and cognitive function.. CHD = coronary heart disease; MI = myocardial infarction. Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: Women s Health Initiative Steering Committee. JAMA. 2004;291: Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: Women’s Health Initiative Steering Committee. JAMA. 2004;291:")
34
WHI E and E+P: Baseline Characteristics
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E and E+P: Baseline Characteristics Characteristic E alone 1 n = 5310 E+P n = 8506 Age at screening, years* 63.6 (7.3) 63.2 (7.1) Prior hormone use, % 47.8 26.1 Body mass index, kg/m2* 30.1 (6.1) 28.5 (5.8) Never smokers, % 51.9 49.6 Diabetes, % 7.7 4.4 Hypertension, % 48.0 35.7 Statin use at baseline, % 7.4 6.9 History of MI, %† 3.1 1.6 History of CABG/PTCA, %† 2.3 1.1 Family history of breast cancer, % 18.0 16.0 This table lists baseline characteristics of the WHI E alone and E+P groups.1,2 For the most part, there were no substantive differences between the E alone and placebo or E+P and placebo groups and thus the placebo group comparisons are not shown, allowing for ease in comparing between the two major WHI treatment arms (however see note below**). The mean age of the study participants (63.6 and 63.2 for the E alone and E+P groups) was substantially older than the typical age of most women who present to physicians and clinics seeking relief of menopausal symptoms (51 years of age for nonhysterectomized women).3 Fewer than one third of the participants were younger than 60 years when they entered the study. Nearly a quarter were in their 70s. Average BMI for the E alone group was 30.1 kg/m2, a value that is indicative of obesity (BMI 30.0). In fact, 80% of the women in the WHI E-alone trial were either overweight (~35%) or obese (~45%). Average BMI for the E+P treatment group was 28.5 kg/m2, a value classified as overweight (BMI 25.0–29.9). As a reference, guidelines from the National Heart, Lung, and Blood Institute4 define overweight and obesity as: Underweight: <18.5 kg/m²; normal: 18.5–24.9 kg/m²; overweight: 25.0–29.9 kg/m²; obese: 30.0 kg/m² The study populations for the E-alone and E+P trials differed in several ways: Mean BMI was higher in the E-alone study than in the E+P study (30.1 vs 28.5). Prior hormone use was higher in the E-alone study (48% vs 26%). A greater proportion of women in the E-alone study reported diabetes (~7.7% vs 4.4%) and hypertension (~47.5% vs ~36%) at baseline. Note: **As a result of these and other differences between the two study populations (eg, intact uterus vs hysterectomy), caution is needed in making head-to-head comparisons of the results of the E-alone and E+P studies. *Values are means (SD). †Overall incidence of prior cardiovascular disease = 7.7%. CABG = coronary artery bypass graft; PTCA = percutaneous transluminal coronary angioplasty. 1 Women's Health Initiative Steering Committee. JAMA. 2004;291: 2 Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: 1Women’s Health Initiative Steering Committee. JAMA. 2004;291: 2Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: 3Taylor Nelson Sofres (TNS) Intersearch Corporation. Incidence and Persistency of Estrogen Replacement. May 17, 2000. 4National Institutes of Health National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. Executive Summary. Available at: Accessed January 27, 2003.
 63.2 (7.1) Prior hormone use, % Body mass index, kg/m2* 30.1 (6.1) 28.5 (5.8) Never smokers, % Diabetes, % Hypertension, % Statin use at baseline, % History of MI, %† History of CABG/PTCA, %† Family history of breast cancer, % This table lists baseline characteristics of the WHI E alone and E+P groups.1,2 For the most part, there were no substantive differences between the E alone and placebo or E+P and placebo groups and thus the placebo group comparisons are not shown, allowing for ease in comparing between the two major WHI treatment arms (however see note below**). The mean age of the study participants (63.6 and 63.2 for the E alone and E+P groups) was substantially older than the typical age of most women who present to physicians and clinics seeking relief of menopausal symptoms (51 years of age for nonhysterectomized women).3. Fewer than one third of the participants were younger than 60 years when they entered the study. Nearly a quarter were in their 70s. Average BMI for the E alone group was 30.1 kg/m2, a value that is indicative of obesity (BMI 30.0). In fact, 80% of the women in the WHI E-alone trial were either overweight (~35%) or obese (~45%). Average BMI for the E+P treatment group was 28.5 kg/m2, a value classified as overweight (BMI 25.0–29.9). As a reference, guidelines from the National Heart, Lung, and Blood Institute4 define overweight and obesity as: Underweight: <18.5 kg/m²; normal: 18.5–24.9 kg/m²; overweight: 25.0–29.9 kg/m²; obese: 30.0 kg/m². The study populations for the E-alone and E+P trials differed in several ways: Mean BMI was higher in the E-alone study than in the E+P study (30.1 vs 28.5). Prior hormone use was higher in the E-alone study (48% vs 26%). A greater proportion of women in the E-alone study reported diabetes (~7.7% vs 4.4%) and hypertension (~47.5% vs ~36%) at baseline. Note: **As a result of these and other differences between the two study populations (eg, intact uterus vs hysterectomy), caution is needed in making head-to-head comparisons of the results of the E-alone and E+P studies. *Values are means (SD). †Overall incidence of prior cardiovascular disease = 7.7%. CABG = coronary artery bypass graft; PTCA = percutaneous transluminal coronary angioplasty. 1 Women s Health Initiative Steering Committee. JAMA. 2004;291: Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: Women’s Health Initiative Steering Committee. JAMA. 2004;291: Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288: Taylor Nelson Sofres (TNS) Intersearch Corporation. Incidence and Persistency of Estrogen Replacement. May 17, National Institutes of Health National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. Executive Summary. Available at: Accessed January 27,")
35
Risk of Invasive Breast Cancer in the WHI HT Trials
4/11/2017 5:11 AM LMF/FM 2004 Oncology Risk of Invasive Breast Cancer in the WHI HT Trials HR Placebo 1.00 E+P1 1.24 95% nCI 95% aCI E alone2 0.77 0.5 1.0 5.0 2.0 Among the results reported in April 2004 from the WHI E-alone study was the unexpected finding that invasive breast cancer was diagnosed at a 23% lower rate in women assigned to unopposed E compared with those assigned to placebo.1 The difference in breast cancer risk between the E-alone and placebo groups just failed to meet the criteria for statistical significance, thus, the lower risk may have been due to chance. Nonetheless, the results indicate that the use of unopposed E for an average of 7 years did not increase breast cancer risk in postmenopausal women with prior hysterectomy. In contrast, the WHI E+P study found an increased risk of breast cancer associated with the use of E+P for an average of 5 years compared with placebo, although the increase in risk was small. Hazard Ratio HR = hazard ratio; nCI = nominal confidence interval; aCI = adjusted confidence interval. 1Chlebowski RT, et al. JAMA. 2003;289: 2Women's Health Initiative Steering Committee. JAMA. 2004;291: 1Women’s Health Initiative Steering Committee. JAMA. 2004;291: 2 Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:

36
WHI E+P Trial: No Effect of E+P on Risk of In Situ Breast Cancer
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E+P Trial: No Effect of E+P on Risk of In Situ Breast Cancer HR = 1.18 95% CI = 0.77–1.82 Cumulative Proportion Placebo CEE + MPA Breast cancers often take at least 5 years to progress from inception to the point at which they can be detectable. Mean patient follow-up in this updated analysis was 5.6 years. Whether E+P may have stimulated the growth of early breast cancers that were undetected at enrollment remains unanswered. This slide shows the cumulative proportion of women diagnosed with in situ breast cancer over time in the WHI E+P trial. The results show no difference in risk for in situ breast cancer between the E+P and placebo groups (HR, 1.18; 95% CI, 0.77–1.82).1 The authors noted that the data suggested an increased risk for in situ breast cancers in the women assigned to CEE/MPA compared with those assigned to placebo: CEE/MPA = 47 cases/8,506 women (0.6% over 5.6 years; 10 per 10,000 women/year) Placebo = 37 cases/8,102 women (0.5% over 5.6 years; 8 per 10,000 women/year) For comparison purposes, SEER incidence rates for in situ breast cancer for women 60–64 years old2 are: All races = 9 per 10,000 women/year Whites (84% of study population) = 9 per 10,000 women/year Time (years) Chlebowski RT, et al. JAMA. 2003;289: 1Chlebowski RT, et al. JAMA. 2003;289: 2Ries LAG, et al. SEER Cancer Statistics Review, , National Cancer Institute. Avaliable at:
.1. The authors noted that the data suggested an increased risk for in situ breast cancers in the women assigned to CEE/MPA compared with those assigned to placebo: CEE/MPA = 47 cases/8,506 women (0.6% over 5.6 years; 10 per 10,000 women/year) Placebo = 37 cases/8,102 women (0.5% over 5.6 years; 8 per 10,000 women/year) For comparison purposes, SEER incidence rates for in situ breast cancer for women 60–64 years old2 are: All races = 9 per 10,000 women/year. Whites (84% of study population) = 9 per 10,000 women/year. Time (years) Chlebowski RT, et al. JAMA. 2003;289: Chlebowski RT, et al. JAMA. 2003;289: Ries LAG, et al. SEER Cancer Statistics Review, , National Cancer Institute. Avaliable at:")
38
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E+P Trial: Risk of Invasive Breast Cancer in Women With and Without Prior HT Use Prior HT Use None <5 Years 5 Years Overall % of WHI Population 74.0 14.8 11.2 100 Subgroup analyses in the WHI E+P trial indicated that the increased risk of invasive breast cancer was limited to those women with prior use of postmenopausal HT. Women with no prior HT use comprised a large proportion of the study population (74%). The HR for breast cancer associated with CEE/MPA use in these women was only marginally greater than 1.0 and was not statistically significant. (The table below provides the data shown graphically in the slide.) 0.1 0.5 1.0 2.0 4.0 6.0 Hazard Ratio (95% CI) Chlebowski RT, et al. JAMA. 2003;289: Prior HT Use % of Study Population HR (95% CI) No prior use 74% 1.09 (0.86–1.39) <5 years of prior use 14.8% 1.70 (0.99–2.91) 5 years of prior use 11.2% 2.27 (1.00–5.15) Chlebowski RT, et al. JAMA. 2003;289:
. The HR for breast cancer associated with CEE/MPA use in these women was only marginally greater than 1.0 and was not statistically significant. (The table below provides the data shown graphically in the slide.) Hazard Ratio (95% CI) Chlebowski RT, et al. JAMA. 2003;289: Prior HT Use. % of Study Population. HR (95% CI) No prior use. 74% 1.09 (0.86–1.39) <5 years of prior use. 14.8% 1.70 (0.99–2.91) 5 years of prior use. 11.2% 2.27 (1.00–5.15) Chlebowski RT, et al. JAMA. 2003;289:")
39
Breast Cancer Risk Among E+P Users in Randomized Controlled Trials
LMF/FM 2004 Oncology Breast Cancer Risk Among E+P Users in Randomized Controlled Trials Relative Hazard (95% CI) 0.5 1.0 10 2.0 WHI HERS HERS II Similar to the findings in the WHI E+P trial,1 the Heart and Estrogen/progestin Replacement Study (HERS) found that risk ratio for breast cancer among E+P users compared with placebo was close to unity.2 HERS was a randomized, blinded, placebo-controlled trial evaluating the effect of E+P on subsequent CHD events in postmenopausal women with established coronary disease. At the end of the 4-year HERS, some participants continued open-label use of E+P/placebo for an additional 2.7 years. Data collected from this observational segment of the trial (HERS II) were analyzed and reported separately. At randomization, the mean age of participants was 67 years; 2,763 women participated in HERS and 2,321 in HERS II. Although the occurrence of CHD events was the primary outcome in HERS and HERS II, data were also published on secondary outcomes, including breast cancer. As illustrated above, there was no significant difference in risk of breast cancer between E+P users and the women randomly ssigned to placebo. This finding was consistent for the HERS, HERS II, and overall results. The risk estimates from HERS, although not statistically significant, were similar to the HR reported in the WHI E+P trial. Chlebowski RT, et al. JAMA. 2003;289: Hulley S, et al. JAMA. 2002;288:58-66. 1Chlebowski RT, et al. JAMA. 2003;289: 2Hulley S, et al. JAMA. 2002;288:58-66.
 WHI. HERS. HERS II. Similar to the findings in the WHI E+P trial,1 the Heart and Estrogen/progestin Replacement Study (HERS) found that risk ratio for breast cancer among E+P users compared with placebo was close to unity.2. HERS was a randomized, blinded, placebo-controlled trial evaluating the effect of E+P on subsequent CHD events in postmenopausal women with established coronary disease. At the end of the 4-year HERS, some participants continued open-label use of E+P/placebo for an additional 2.7 years. Data collected from this observational segment of the trial (HERS II) were analyzed and reported separately. At randomization, the mean age of participants was 67 years; 2,763 women participated in HERS and 2,321 in HERS II. Although the occurrence of CHD events was the primary outcome in HERS and HERS II, data were also published on secondary outcomes, including breast cancer. As illustrated above, there was no significant difference in risk of breast cancer between E+P users and the women randomly ssigned to placebo. This finding was consistent for the HERS, HERS II, and overall results. The risk estimates from HERS, although not statistically significant, were similar to the HR reported in the WHI E+P trial. Chlebowski RT, et al. JAMA. 2003;289: Hulley S, et al. JAMA. 2002;288: Chlebowski RT, et al. JAMA. 2003;289: Hulley S, et al. JAMA. 2002;288:")
40
4/11/2017 5:11 AM LMF/FM 2004 Oncology Million Women Study Investigators recruited 1,084,110 women in the UK, aged years, between 1996 and 2001 Questionnaire about lifestyle, SES, medical history, and HT use sent in conjunction with invitation from NHSBSP for screening mammography Mean age, 56 years; 9364 cases of invasive breast cancer and 637 breast cancer deaths identified during follow-up Analysis of HT and breast cancer risk restricted to postmenopausal women (n = 828,923) 50% were ever-users of HT; 33% were current users; mean duration of use was 5.8 years The Million Women Study was an impressively large, observational study conducted in the UK to evaluate the effects of specific types of HT on incident and fatal breast cancer.1 The investigators recruited 1,084,110 women aged 50 to 64 years to participate in the study. Recruitment proceeded as follows: The National Health Service Breast Screening Programme invited all women in the UK aged 50–64 years for routine screening mammography once every 3 years. From May 1996 to March 2001, the National Health Service breast screening centers participating in the study included the study questionnaire together with their letter of invitation for routine mammography. Questionnaires were returned before screening. The questionnaire contained items about sociodemographic and other personal factors, including information about use of HT and menstrual history. Mean age at time of recruitment was 55.9 years. Average follow-up was 2.6 years for analyses of cancer incidence and 4.1 years for analyses of mortality. During the follow-up period, 9,364 cases of invasive breast cancer and 637 deaths from breast cancer were identified by the National Health Service. Analyses evaluating HT use and breast cancer risk were restricted to postmenopausal women (n = 828,923). Approximately half of these women reported ever using HT, and one third were current users. The mean duration of HT use was 5.8 years. For a small sample of the study population (n = 570), validation studies were done, comparing self-reported data with information in family physicians’ records from 2 general practices.2 These studies showed 96% agreement between data from the questionnaires and the prescription record for current HT use, and 95% agreement for any use of HT during the period covered by the prescription record. Agreement on the proprietary preparation was 69%. Agreement was 97% for hormonal constituents used. SES = socioeconomic status; NHSBSP = National Health Service Breast Screening Programme. Million Women Study Collaborators. Lancet. 2003;362: 1Million Women Study Collaborators. Lancet. 2003;362: 2Banks E, et al. J Epidemiol Biostat. 2001;6:
 50% were ever-users of HT; 33% were current users; mean duration of use was 5.8 years. The Million Women Study was an impressively large, observational study conducted in the UK to evaluate the effects of specific types of HT on incident and fatal breast cancer.1 The investigators recruited 1,084,110 women aged 50 to 64 years to participate in the study. Recruitment proceeded as follows: The National Health Service Breast Screening Programme invited all women in the UK aged 50–64 years for routine screening mammography once every 3 years. From May 1996 to March 2001, the National Health Service breast screening centers participating in the study included the study questionnaire together with their letter of invitation for routine mammography. Questionnaires were returned before screening. The questionnaire contained items about sociodemographic and other personal factors, including information about use of HT and menstrual history. Mean age at time of recruitment was 55.9 years. Average follow-up was 2.6 years for analyses of cancer incidence and 4.1 years for analyses of mortality. During the follow-up period, 9,364 cases of invasive breast cancer and 637 deaths from breast cancer were identified by the National Health Service. Analyses evaluating HT use and breast cancer risk were restricted to postmenopausal women (n = 828,923). Approximately half of these women reported ever using HT, and one third were current users. The mean duration of HT use was 5.8 years. For a small sample of the study population (n = 570), validation studies were done, comparing self-reported data with information in family physicians’ records from 2 general practices.2 These studies showed 96% agreement between data from the questionnaires and the prescription record for current HT use, and 95% agreement for any use of HT during the period covered by the prescription record. Agreement on the proprietary preparation was 69%. Agreement was 97% for hormonal constituents used. SES = socioeconomic status; NHSBSP = National Health Service Breast Screening Programme. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362: Banks E, et al. J Epidemiol Biostat. 2001;6:")
41
4/11/2017 5:11 AM LMF/FM 2004 Oncology Incident Invasive Breast Cancer in Relation to Recency and Type of HT Used HT Use at Baseline Relative Risk (95% FCI)* All never-users 1.00 (0.96–1.04) All past users 1.01 (0.95–1.08) Current users E-only 1.30 (1.22–1.38) E+P 2.00 (1.91–2.09) Tibolone 1.45 (1.25–1.67) Other/unknown types 1.44 (1.17–1.76) Among the 828,923 postmenopausal women included in the main analyses, the risk of breast cancer was significantly higher among ever-users of HT at baseline than among never-users (RR, 1.43; 95% CI, 1.36–1.50). This increased risk was largely restricted to current users, rather than past users, regardless of how recently women had ceased HT use (ie, last use <5 years ago, 5–9 years ago, or 10 years ago). Most of the current users of HT reported using E alone (41%) or E+P (50%). RR of breast cancer was significantly increased in current users of E alone (1.30; 95% CI, 1.22–1.38), E+P (2.00; 95% CI, 1.91–2.09), and tibolone (1.45; 95% CI, 1.17–1.76). The magnitude of increased risk varied significantly between these 3 types of HT and was significantly greater in current E+P users (P < .0001) FCI = floated CI. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, body mass index, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:
* All never-users (0.96–1.04) All past users (0.95–1.08) Current users. E-only (1.22–1.38) E+P (1.91–2.09) Tibolone (1.25–1.67) Other/unknown types (1.17–1.76) Among the 828,923 postmenopausal women included in the main analyses, the risk of breast cancer was significantly higher among ever-users of HT at baseline than among never-users (RR, 1.43; 95% CI, 1.36–1.50). This increased risk was largely restricted to current users, rather than past users, regardless of how recently women had ceased HT use (ie, last use <5 years ago, 5–9 years ago, or 10 years ago). Most of the current users of HT reported using E alone (41%) or E+P (50%). RR of breast cancer was significantly increased in current users of E alone (1.30; 95% CI, 1.22–1.38), E+P (2.00; 95% CI, 1.91–2.09), and tibolone (1.45; 95% CI, 1.17–1.76). The magnitude of increased risk varied significantly between these 3 types of HT and was significantly greater in current E+P users (P < .0001) FCI = floated CI. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, body mass index, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:")
42
4/11/2017 5:11 AM LMF/FM 2004 Oncology Incident Invasive Breast Cancer in Relation to Recency and Type of HT Used Total Duration of HT Use by Type of HT Used at Baseline Relative Risk (95% FCI)* Never-users of HT –1.04 Past users of HT <1 year 0.94 (0.84–1.05) 1–4 years 1.01 (0.92–1.12) 5–9 years 1.14 (1.00–1.30) ≥10 years 1.05 (0.84–1.30) Current users of E alone 0.81 (0.55–1.20) 1.25 (1.10–1.41) 1.32 (1.20–1.46) 1.37 (1.22–1.54) Current users of E+P 1.45 (1.19–1.78) 1.74 (1.60–1.89) 2.17 (2.03–2.33) 2.31 (2.08–2.56) These results from the Million Women Study indicate that, in general, the RR of breast cancer in current HT users increased as duration of HT use increased. Past use of HT, regardless of duration, was not associated with an increased risk of breast cancer. FCI = floated CI. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, BMI, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:
* Never-users of HT –1.04. Past users of HT. <1 year (0.84–1.05) 1–4 years (0.92–1.12) 5–9 years (1.00–1.30) ≥10 years (0.84–1.30) Current users of E alone (0.55–1.20) 1.25 (1.10–1.41) 1.32 (1.20–1.46) 1.37 (1.22–1.54) Current users of E+P (1.19–1.78) 1.74 (1.60–1.89) 2.17 (2.03–2.33) 2.31 (2.08–2.56) These results from the Million Women Study indicate that, in general, the RR of breast cancer in current HT users increased as duration of HT use increased. Past use of HT, regardless of duration, was not associated with an increased risk of breast cancer. FCI = floated CI. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, BMI, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:")
43
4/11/2017 5:11 AM LMF/FM 2004 Oncology Incident Invasive Breast Cancer in Current Users of E-only Preparations E-only Formulation Relative Risk (95% CI)* All E-only formulations 1.30 (1.21–1.40) By constituent and dose All equine estrogen 1.29 (1.16–1.43) ≤0.625 mg 1.25 (1.11–1.41) >0.625 mg 1.36 (1.14–1.61) All 17-estradiol 1.24 (1.12–1.37) ≤1 mg 1.25 (1.12–1.40) >1 mg 1.19 (0.89–1.58) By formulation Oral 1.32 (1.21–1.45) Transdermal 1.24 (1.11–1.39) Implanted 1.65 (1.26–2.16) This slide shows the RR of breast cancer in current users of E-only therapy compared with women who never used HT according to specific preparations used. In general, these results show that the risk was similarly increased for equine estrogen formulations and 17- estradiol preparations. As well, use of oral or transdermal E-only formulations was associated with a comparable increase in breast cancer risk. The risk associated with the use of implanted E preparations was somewhat higher, although this difference was not statistically significant. Dotted line represents overall relative risk for current users of estrogen-only preparations compared with never-users at baseline. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, BMI, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:
* All E-only formulations (1.21–1.40) By constituent and dose. All equine estrogen (1.16–1.43) ≤0.625 mg (1.11–1.41) >0.625 mg (1.14–1.61) All 17-estradiol (1.12–1.37) ≤1 mg (1.12–1.40) >1 mg (0.89–1.58) By formulation. Oral (1.21–1.45) Transdermal (1.11–1.39) Implanted (1.26–2.16) This slide shows the RR of breast cancer in current users of E-only therapy compared with women who never used HT according to specific preparations used. In general, these results show that the risk was similarly increased for equine estrogen formulations and 17- estradiol preparations. As well, use of oral or transdermal E-only formulations was associated with a comparable increase in breast cancer risk. The risk associated with the use of implanted E preparations was somewhat higher, although this difference was not statistically significant. Dotted line represents overall relative risk for current users of estrogen-only preparations compared with never-users at baseline. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, BMI, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:")
44
Incident Invasive Breast Cancer in Current Users of E+P Preparations
4/11/2017 5:11 AM LMF/FM 2004 Oncology Incident Invasive Breast Cancer in Current Users of E+P Preparations Duration of Use, <5 Years E+P Formulation Relative Risk (95% CI)* All E+P formulations 1.70 (1.56–1.86) By progestin constituent Medroxyprogesterone acetate 1.60 (1.33–1.93) Norethisterone 1.53 (1.35–1.75) Norgestrel/levonorgestrel 1.97 (1.74–2.33) By type of regimen Sequential 1.77 (1.59–1.97) Continuous 1.57 (1.37–1.79) This slide shows the RR of breast cancer in current E+P users, compared with women who never used HT, according to the specific progestin used and whether progestin was administered sequentially or continuously. These results are for those women who, at the time they enrolled in the study, reported current use of E+P for a duration of <5 years. In general, RR of breast cancer was increased in current E+P users, and this elevation in risk did not differ substantially with use of various progestins or regimens (sequential vs continuous). Dotted line represents overall relative risk for current users of estrogen-progestin preparations compared with never-users at baseline. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, BMI, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:
* All E+P formulations (1.56–1.86) By progestin constituent. Medroxyprogesterone acetate (1.33–1.93) Norethisterone (1.35–1.75) Norgestrel/levonorgestrel (1.74–2.33) By type of regimen. Sequential (1.59–1.97) Continuous (1.37–1.79) This slide shows the RR of breast cancer in current E+P users, compared with women who never used HT, according to the specific progestin used and whether progestin was administered sequentially or continuously. These results are for those women who, at the time they enrolled in the study, reported current use of E+P for a duration of <5 years. In general, RR of breast cancer was increased in current E+P users, and this elevation in risk did not differ substantially with use of various progestins or regimens (sequential vs continuous). Dotted line represents overall relative risk for current users of estrogen-progestin preparations compared with never-users at baseline. *Relative to never-users, stratified by age, time since menopause, parity and age at first birth, family history of breast cancer, BMI, region, and deprivation index. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:")
45
Breast Cancer Mortality Rates in the Million Women Study
4/11/2017 5:11 AM LMF/FM 2004 Oncology Breast Cancer Mortality Rates in the Million Women Study HT Use at Baseline Breast Cancer Deaths/Breast Cancer Cases Mortality Rate (%) Never-users 238/2894 8.2 Current users 191/3202 5.9 Past users 88/1044 8.4 Total breast cancer deaths 517/6961 7.1 The increased risk of fatal breast cancer reported by the Million Women Study appeared to be in direct contrast with the results of numerous previous studies showing similar—or in some cases reduced—breast cancer mortality rates in HT users and nonusers. The discrepancy between findings from previous studies and the Million Women Study results can be resolved, however, by calculating the mortality rate in the Million Women Study in the same manner as it is generally calculated in most studies. This calculation (shown in this slide) involves dividing the number of breast cancer deaths by the number of breast cancer cases. When calculated in this manner, the Million Women Study results for breast cancer mortality rates are consistent with those from previous studies. The next slide graphically shows the results from a number of previous studies. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:
 Never-users. 238/ Current users. 191/ Past users. 88/ Total breast cancer deaths. 517/ The increased risk of fatal breast cancer reported by the Million Women Study appeared to be in direct contrast with the results of numerous previous studies showing similar—or in some cases reduced—breast cancer mortality rates in HT users and nonusers. The discrepancy between findings from previous studies and the Million Women Study results can be resolved, however, by calculating the mortality rate in the Million Women Study in the same manner as it is generally calculated in most studies. This calculation (shown in this slide) involves dividing the number of breast cancer deaths by the number of breast cancer cases. When calculated in this manner, the Million Women Study results for breast cancer mortality rates are consistent with those from previous studies. The next slide graphically shows the results from a number of previous studies. Million Women Study Collaborators. Lancet. 2003;362: Million Women Study Collaborators. Lancet. 2003;362:")
46
WHI E+P Trial: Characteristics of Invasive Breast Cancers
4/11/2017 5:11 AM LMF/FM 2004 Oncology WHI E+P Trial: Characteristics of Invasive Breast Cancers E+P (n = 199) Placebo (n = 150) P-Value Tumor size, mean ± SD (cm) 1.7 ± 1.1 1.5 ± 0.9 .04 Positive lymph nodes, % 25.9 15.8 .03 Morphology, grade, % Well differentiated 25.0 20.3 Moderately differentiated 43.3 47.7 .61 Poorly differentiated/anaplastic 31.7 32.0 ER status, % Positive 86.8 88.2 .72 PR status, % 75.0 69.9 .33 Deaths attributed to breast cancer, n (%) 4 (2.0) 4 (2.7) — Chlebowski and colleagues also compared the characteristics of the breast cancers that developed in the active treatment and placebo groups. These results indicated that tumors diagnosed in women in the E+P group were, on average, 0.2 cm larger than those diagnosed in the placebo group. In addition, 26% of breast cancers in the E+P group were node positive compared with 16% in the placebo group. Differences between groups in the morphology of the cancers were not statistically significant, and the proportion of poorly differentiated or anaplastic cancers was almost identical in both groups (32%). One quarter of the breast cancers in the E+P group were well differentiated compared with on fifth in the placebo group. No differences between groups were observed for tumor histology (data not shown). Points to consider: The standard deviation for tumor size, which indicates the degree of variance observed in tumor size in this study population, was fairly large. Standard deviations in the range of 0.9–1.1 cm suggest a variability in tumor size that is clinically meaningful in terms of differences in patient prognosis. Although statistically significant, the difference in mean tumor size between groups (0.2 cm) was small. In most cases, one would not expect this difference in tumor size to be associated with a difference in cancer stage and/or the proportion of patients with positive lymph nodes. Such differences, however, were observed in this study and additional research is needed to better understand these findings. Decisions regarding the workup of breast findings were directed by community physicians, and data on breast cancer end points was obtained by review of medical records and pathology reports. No information was provided on how lymph nodes were evaluated in the 349 cases for which results were reported. No significant differences between E+P and placebo were observed for the proportion of breast cancers that were estrogen receptor-positive (ER-positive) or progesterone receptor-positive (PR-positive).1 However, the incidence of ER-positive tumors (87% in the E+P group, 88% in the placebo group) is higher than what would be expected in this age group. On average, two thirds to three quarters of women with breast cancer in the US have ER-positive tumors.2 ER-positive tumors are associated with better overall and disease-free survival compared with ER-negative tumors.3 This increase in the incidence of ER-positive breast cancers may be due to the high frequency of obesity in this population (34% had a BMI 30 kg/m2).4 Obese women have a higher risk of ER-positive breast cancer compared with thinner women.5 Mortality from breast cancer was similar among patients receiving E+P compared with those receiving placebo. Four deaths attributed to breast cancer occurred in each group (2.0% of the cases in the E+P group and 2.7% of cases in the placebo group).1 ER = estrogen receptor; PR = progesterone receptor. Chlebowski RT, et al. JAMA. 2003;289: 1Chlebowski RT, et al. JAMA. 2003;289: ; 2Li CI, et al. J Clin Oncol. 2003;21:28-34; 3Bardou VJ, et al. J Clin Oncol. 2003;21:1973-9; 4Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:321-33; 5Morimoto LM, et al. Cancer Causes Control. 2002;13:
 Placebo (n = 150) P-Value. Tumor size, mean ± SD (cm) 1.7 ± ± Positive lymph nodes, % Morphology, grade, % Well differentiated Moderately differentiated Poorly differentiated/anaplastic ER status, % Positive PR status, % Deaths attributed to breast cancer, n (%) 4 (2.0) 4 (2.7) — Chlebowski and colleagues also compared the characteristics of the breast cancers that developed in the active treatment and placebo groups. These results indicated that tumors diagnosed in women in the E+P group were, on average, 0.2 cm larger than those diagnosed in the placebo group. In addition, 26% of breast cancers in the E+P group were node positive compared with 16% in the placebo group. Differences between groups in the morphology of the cancers were not statistically significant, and the proportion of poorly differentiated or anaplastic cancers was almost identical in both groups (32%). One quarter of the breast cancers in the E+P group were well differentiated compared with on fifth in the placebo group. No differences between groups were observed for tumor histology (data not shown). Points to consider: The standard deviation for tumor size, which indicates the degree of variance observed in tumor size in this study population, was fairly large. Standard deviations in the range of 0.9–1.1 cm suggest a variability in tumor size that is clinically meaningful in terms of differences in patient prognosis. Although statistically significant, the difference in mean tumor size between groups (0.2 cm) was small. In most cases, one would not expect this difference in tumor size to be associated with a difference in cancer stage and/or the proportion of patients with positive lymph nodes. Such differences, however, were observed in this study and additional research is needed to better understand these findings. Decisions regarding the workup of breast findings were directed by community physicians, and data on breast cancer end points was obtained by review of medical records and pathology reports. No information was provided on how lymph nodes were evaluated in the 349 cases for which results were reported. No significant differences between E+P and placebo were observed for the proportion of breast cancers that were estrogen receptor-positive (ER-positive) or progesterone receptor-positive (PR-positive).1. However, the incidence of ER-positive tumors (87% in the E+P group, 88% in the placebo group) is higher than what would be expected in this age group. On average, two thirds to three quarters of women with breast cancer in the US have ER-positive tumors.2 ER-positive tumors are associated with better overall and disease-free survival compared with ER-negative tumors.3. This increase in the incidence of ER-positive breast cancers may be due to the high frequency of obesity in this population (34% had a BMI 30 kg/m2).4 Obese women have a higher risk of ER-positive breast cancer compared with thinner women.5. Mortality from breast cancer was similar among patients receiving E+P compared with those receiving placebo. Four deaths attributed to breast cancer occurred in each group (2.0% of the cases in the E+P group and 2.7% of cases in the placebo group).1. ER = estrogen receptor; PR = progesterone receptor. Chlebowski RT, et al. JAMA. 2003;289: Chlebowski RT, et al. JAMA. 2003;289: ; 2Li CI, et al. J Clin Oncol. 2003;21:28-34; 3Bardou VJ, et al. J Clin Oncol. 2003;21:1973-9; 4Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:321-33; 5Morimoto LM, et al. Cancer Causes Control. 2002;13:")
47
Mortaliteye İlişkin Rölatif Risk (%95 GA)
4/11/2017 5:11 AM LMF/FM 2004 Oncology ERT/HRT Kullananlarda Meme Kanseri Nedeniyle Mortalite Sonuçları Tutarlılık Göstermektedir Hunt ve ark, 1990 Henderson ve ark, 1991 Willis ve ark, 1996 Grodstein ve ark, 1997 Kullanmakta olan Geçmişte kullanmış olan Sellers ve ark, 1997 Rodriguez ve ark, 2001 Kullanmakta olan Geçmişte kullanmış olan 0.1 0.5 1.0 10 2.0 Mortaliteye İlişkin Rölatif Risk (%95 GA)
")
48
MEME KANSERİ-PROBLEM Östrojene maruz kalmak meme kanseri için risk faktörü müdür? Östrojenler yeni meme kanserine neden olur mu? Progesteron eklenmesi meme kanseri riskini etkiler mi? HT ile gözlenen meme tümörleri daha az agresif mi?

49
Hormonal risk factors for breast cancer
High risk group Low risk group RR Age at menarche < 12 years > 14 years 1.5 Age at menopause >55 years < 45 years 2.0 Oophorectomy - < 35 years 3.0 Serum E2 High Low BMI > 30 <23 Bone density Breast density 6.0 Modified after Clemons and Goss (2001)
")
50
Hormone dependent carcinogenesis
Tumor initiation mutagens direct DNA damage DNA DNA A Normal cell Cancer cell

51
Hormone dependent carcinogenesis
mitosis Tumor initiation Accumulation of replication damage DNA DNA Normal cell Cancer cell B

52
Hormone dependent carcinogenesis
Tumor growth acceleration mitosis DNA* proliferation DNA* DNA* DNA* DNA* Occult tumor Clinical tumor C

53
MEME KANSERİ GENETİK MUTASYON
Biyolojik kanıtlar meme kanserinin ,çok sayıda genetik mutasyonlar sonucunda meme hücresinin internal sinyal sistemindeki bozulma sonucu oluştuğunu göstermektedir. Wren BG Menopause , 2007

54
Meme kanseri Mutasyon Meme hücre mutasyonları , büyük oranda hızlı kök hücre bölünmesinin yaşandığı adölesan meme gelişimi döneminde gözlenmektedir. Wren BG Menopause , 2007

55
Meme kanseri Mutasyon Eğer aberran mutasyonlar adölesan meme oluşumu sırasında görülmezse daha ileri yıllarda meme kanseri görülme olasılığı çok nadirdir. Wren BG Menopause , 2007

56
MEME KANSERİ HORMONLAR
Endojen veya exojen hormonlar malignant mutasyonları indüklemezler.EPT kök hücre replikasyonunu arttırır. Önceden genetik yapı değişikliklerinin olduğu meme hücrelerinde, hormonlar mitozu arttırabilir.Böylece spontan mutasyonları arttırarak kanser riski oluşturabilir. Wren BG Menopause , 2007

57
MEME KANSERİ HORMONLAR
Adölesan meme oluşumu sırasında genetik olarak değişime uğramış kök hücre kolonileri oluşmamışsa ,daha sonradan uzun süre sex hormonlarına maruz kalmak meme kanseri riskini arttırmayacaktır. Wren BG Menopause , 2007

58
MEME KANSERİ HORMONLAR
Eğer aberran hücre kolonileri adelosan dönemde oluşmuşsa,histolojik olarak benign hipertrofiden,atipik hipertrofi,carcinoma insitu, mikroinvazyon,invazif kanser ve metastas dönüşümü,genetik mutasyondaki artışa bağlı görülebilecektir. Wren BG Menopause , 2007

59
BİR KARŞIT GÖRÜŞ ÖSTROJEN PROGESTERON TEDAVİSİ ÖNCEDEN VAR OLAN MEME TÜMÖRÜNÜN ERKEN TANISI VE DAHA İYİ FARKLILAŞMASINI SAĞLAYARAK BELKİ DE OLUMLU BİR SONUÇ YARATMAKTADIR LEON SPEROFF Menopause 394,2008

60
MEME KANSERİ PR-A PR-A + Meme hücrelerinde agresif büyüme gözlenir.progesterone yokluğunda PR-A isoformları dominanttır.PR-A fazlalığı ile meme kanseri ilişkilidir.ER+ tümörler PR-A isoformlarından zengindir.EPT ER+ tümörlerde PR-B nin olumlu etkilerini promote etmesi mümkündür. LEON SPEROFF Menopause 394,2008

61
VAR OLAN TÜMÖRLERDE HORMONAL ETKİ GÖZLEMLERİ
EPİDEMİYOLOJİK ÇALIŞMALARDA HORMON TEDAVİSİ SONRASINDA HEMEN RİSK ARTIŞI EP İLE İLİŞKİLİ KANSER ER+ DÜŞÜK GRADE DÜŞÜK EVREDE TÜMÖRLER MEME KANSERİ PREVALANSINDAKİ YENİ DÜŞME POSTMENOPOZAL EPT KULLANIMINDAKİ DÜŞME İLE EŞ ZAMANLI. LEON SPEROFF Menopause 394,2008

63
PROGESTİNİN VAR OLAN TÜMÖRLERE OLUMLU ETKİSİNİN KANITLARI
EPT tedavisini takiben ER+ tümörlerin görülmesi. Sürekli tedavide daha sık E ile up regüle genler EPT ile down regüle olur. EPT ile aktive olan genler DNA tamirinde hücre siklus regulasyonunda kullanılır. Progestinler meme dokusu PRA reseptörlerni azaltır.PRA/PRB oranını değiştirerek daha iyi farklılaşmayı sağlar. Meme kanseri mortalitesinde EPT kullanımı ile azalma rapor edilmiştir.

64
BİR KARŞIT GÖRÜŞ Postmenopozal hormon tedavisi yeni meme tümörlerinin gelişimi ni indüklemek yerine var olan tümörlere hormonal cevabı yansıtır. EPT daha iyi farklılaşma ve erken tanıya sebep olarak belkide olumlu bir sonuç yaratmaktadır. LEON SPEROFF Menopause 394,2008

67
NAMS position statement. Menopause 2008.
HT & Breast Cancer Breast cancer risk increases with EPT use beyond 3-5 y Increased absolute risk of EPT in WHI viewed as “rare” (4-6 additional cases/ 10,000 women/y of EPT for ≥ 5 y) Unclear whether EPT risk differs between continuous and sequential progestogen use WHI ET trial showed no increased risk after 7.1 y (6 fewer cases/10,000 women/y of ET use; not statistically significant) ET for <5 y has little impact on breast cancer risk (cont’d) NAMS position statement. Menopause 2008. Copyright 2008
 Unclear whether EPT risk differs between continuous and sequential progestogen use. WHI ET trial showed no increased risk after 7.1 y (6 fewer cases/10,000 women/y of ET use; not statistically significant) ET for <5 y has little impact on breast cancer risk. (cont’d) NAMS position statement. Menopause Copyright")
68
HT & Breast Cancer (cont’d)
EPT and, to a lesser extent, ET, increase breast cell proliferation, breast pain, and mammographic density EPT may impede diagnostic interpretation of mammograms Whether to use HT when history of breast cancer is unresolved (limited epidemiologic evidence mixed; no completed long-term RCTs) NAMS position statement. Menopause 2008. Copyright 2008
 NAMS position statement. Menopause Copyright")
70
PH’si ya da KFA’sı olmayan HRT kullanıcıları (referent)
4/11/2017 5:11 AM LMF/FM 2004 Oncology Selim Meme Kanseri Hikayesi Olan Kadınlarda HRT Kullanımı ve Meme Kanseri 0,5 1,0 5,0 2,0 PH’si ya da KFA’sı olmayan HRT kullanıcıları (referent) HRT kullanıcıları Kullanmayanlar Atipik hiperplazi HRT kullanıcıları Kullanmayanlar Atipisiz PH HRT kullanıcıları Kullanmayanlar Tüm PH’ler Rölatif Risk (%95 GA) PH = proliferatif hastalık. KFA = kompleks fibroadenom. Dupont WD ve ark. Cancer. 1999;85:
 HRT kullanıcıları Kullanmayanlar. Atipik hiperplazi. HRT kullanıcıları Kullanmayanlar. Atipisiz PH. HRT kullanıcıları Kullanmayanlar. Tüm PH’ler. Rölatif Risk (%95 GA) PH = proliferatif hastalık. KFA = kompleks fibroadenom. Dupont WD ve ark. Cancer. 1999;85:")
73
MEME CA VE HT KLİNİK UYGULAMA
Postmenopozal kadınlarda HT başlanması veya tedaviye devam kararı verilmesi sırasında, kadınların kombine HT nin meme kanserini arttırmada küçük ama gerçek bir riski olduğunu bilmesi gerekmektedir.ET ile bu risk daha azdır (beklide hiç yoktur)Bu riskin meme kanserini arttıran diğer risk faktörleri ile karşılaştırılması yararlı olur.
Bu riskin meme kanserini arttıran diğer risk faktörleri ile karşılaştırılması yararlı olur.")
76
HRT in Women with BRCA1 & 2 After Prophylactic BPO
4/11/2017 5:11 AM LMF/FM 2004 Oncology HRT in Women with BRCA1 & 2 After Prophylactic BPO RR BPO, no HRT 0.38 (0.09–1.59) BPO, any HRT 0.37 (0.14–0.96) BPO, E2 0.44 (0.12–1.61) BPO, E+P 0.43 (0.07–2.68) Rebbeck TR et al in a prospective cohort study by of 462 women with BRCA 1/2 mutations evaluated whether the breast cancer risk reduction conferred by bilateral prophylactic oophorectomy (BPO) in BRCA 1/2 mutation carriers is altered by use of post-BPO hormone replacement therapy (HRT) over 3.6 years. Consistent with previous reports, BPO was significantly associated with breast cancer risk reduction overall (hazard ratio [HR] = 0.40; 95%CI, 0.18–0.92). Short-term HRT use does not negate the protective effect of BPO on subsequent breast cancer risk in BRCA1/2 mutation carriers. Using mutation carriers without BPO or HRT as the referent group, HRT of any type after BPO did not significantly alter the reduction in breast cancer risk associated with BPO (HR = 0.37; 95% CI, 0.14– 0.96). This is one of the largest existing cohorts of women with BRCA 1/2 but the usual caveats apply concerning sampling or information biases and the sample provided insufficient power to detect effects for some comparisons.. BPO = Bilateral prophylactic oophorectomy Rebbeck TR, et al. J Clin Oncol. 2005;23(31): Rebbeck TR, et al. J Clin Oncol. 2005;23(31):
 BPO, any HRT (0.14–0.96) BPO, E (0.12–1.61) BPO, E+P (0.07–2.68) Rebbeck TR et al in a prospective cohort study by of 462 women with BRCA 1/2 mutations evaluated whether the breast cancer risk reduction conferred by bilateral prophylactic oophorectomy (BPO) in BRCA 1/2 mutation carriers is altered by use of post-BPO hormone replacement therapy (HRT) over 3.6 years. Consistent with previous reports, BPO was significantly associated with breast cancer risk reduction overall (hazard ratio [HR] = 0.40; 95%CI, 0.18–0.92). Short-term HRT use does not negate the protective effect of BPO on subsequent breast cancer risk in BRCA1/2 mutation carriers. Using mutation carriers without BPO or HRT as the referent group, HRT of any type after BPO did not significantly alter the reduction in breast cancer risk associated with BPO (HR = 0.37; 95% CI, 0.14– 0.96). This is one of the largest existing cohorts of women with BRCA 1/2 but the usual caveats apply concerning sampling or information biases and the sample provided insufficient power to detect effects for some comparisons.. BPO = Bilateral prophylactic oophorectomy. Rebbeck TR, et al. J Clin Oncol. 2005;23(31): Rebbeck TR, et al. J Clin Oncol. 2005;23(31):")
80
Body Mass Index Affects Relationship Between HT and Endometrial Cancer
4/11/2017 5:11 AM LMF/FM 2004 Oncology Body Mass Index Affects Relationship Between HT and Endometrial Cancer Continuous combined 8 Cyclic combined Tibolone Never HRT 6 Incidence of endometrial cancer per 1000 women over 5 years 4 2 Normal weight (BMI <25 kg/m2) Overweight (BMI 25–29) Obese (BMI ≥30) This slide shows the 5-year incidence rates of endometrial cancer for subgroups in the Million Women Study based on type of HT used and by BMI. Among never-users, incidence rates were four times higher in women with a BMI of ≥30 kg/m2 than in those with BMI <25 kg/m2 (6.4 vs 1.6 per 1000). BMI did not, however, have the same pattern of effect in HT users: Among HT users who were not overweight (BMI <25 kg/m2) use of cyclic HT or tibolone significantly increased the incidence of endometrial cancer compared with never-users, and continuous HT conferred no benefit. By contrast, among obese women (BMI ≥30 kg/m2), users of both continuous and cyclic HT had a lower incidence of endometrial cancer than never-users, and tibolone users had similar rates to never-users. These results suggest that the adverse effects of tibolone and unopposed estrogen were greatest in nonobese women, and the beneficial effects of combined HT were greatest in obese women. BMI = body mass index (kg/m2). Million Women Study Collaborators. Lancet. 2005;365: Million Women Study Collaborators. Lancet. 2005;365:
 Overweight. (BMI 25–29) Obese. (BMI ≥30) This slide shows the 5-year incidence rates of endometrial cancer for subgroups in the Million Women Study based on type of HT used and by BMI. Among never-users, incidence rates were four times higher in women with a BMI of ≥30 kg/m2 than in those with BMI <25 kg/m2 (6.4 vs 1.6 per 1000). BMI did not, however, have the same pattern of effect in HT users: Among HT users who were not overweight (BMI <25 kg/m2) use of cyclic HT or tibolone significantly increased the incidence of endometrial cancer compared with never-users, and continuous HT conferred no benefit. By contrast, among obese women (BMI ≥30 kg/m2), users of both continuous and cyclic HT had a lower incidence of endometrial cancer than never-users, and tibolone users had similar rates to never-users. These results suggest that the adverse effects of tibolone and unopposed estrogen were greatest in nonobese women, and the beneficial effects of combined HT were greatest in obese women. BMI = body mass index (kg/m2). Million Women Study Collaborators. Lancet. 2005;365: Million Women Study Collaborators. Lancet. 2005;365:")
81
WHI E+P Trial: Mammography Results
LMF/FM 2004 Oncology WHI E+P Trial: Mammography Results % Abnormal* E Placebo E+P Year 1 9.2 5.5† 9.4 5.4‡ Overall 36.2 28.1† 31.5 21.2‡ In the US, 11% of screening mammograms have abnormal findings *Abnormal mammograms included those that were associated with recommendations for short-term follow-up, showed a suspicious abnormality, or were highly suggestive of malignancy †P < .001 vs E; ‡P < .001 vs E+P. Chlebowski RT, et al. JAMA. 2003;289: Stefanick ML, et al. JAMA. 2006;295: Yearly mammography and clinical breast exams were required in the WHI, and these mammograms were performed at more than 3,000 clinics, hospitals, and practices in the US. Mammography reports from these settings were reviewed locally and coded as: negative, benign finding-negative, short interval follow-up suggested, suspicious abnormality, or highly suggestive of malignancy.1 The WHI investigators evaluated the frequency of abnormal mammograms in the E alone and E+P trial, which they defined as those with either a recommendation for short interval follow-up or a suspicious abnormality, or those highly suggestive of malignancy. After 1 year of follow-up, the proportion of women with abnormal mammograms was greater in the E alone group (9.2%) compared with the placebo group (5.4%). This pattern continued throughout the study. However, the author’s note that the difference was primarily in assessments requiring short interval follow-up but not those with more suspicious findings, which contrasted with the E + P trial results. After 1 year of follow-up, the proportion of women with abnormal mammograms was greater in the E+P group (9.4%) compared with the placebo group (5.4%). This pattern continued throughout the study. In comparison, in a study of screening mammography in 50 community mammography practices that were included in the National Survey of Mammography Facilities, 11% of screening mammograms had abnormal findings and required further diagnostic evaluation.2 One factor to consider in examining these findings is that, with an average age of 63 years at enrollment, some older women who initiated E+P would be expected to experience physiological changes in breast tissue that could have been interpreted as “abnormal,” but are typical of changes seen when women begin HT years after menopause. 1Chlebowski RT, et al. JAMA. 2003;289: 2Brown ML, et al. AJR Am J Roentgenol. 1995;165:
 compared with the placebo group (5.4%). This pattern continued throughout the study. However, the author’s note that the difference was primarily in assessments requiring short interval follow-up but not those with more suspicious findings, which contrasted with the E + P trial results. After 1 year of follow-up, the proportion of women with abnormal mammograms was greater in the E+P group (9.4%) compared with the placebo group (5.4%). This pattern continued throughout the study. In comparison, in a study of screening mammography in 50 community mammography practices that were included in the National Survey of Mammography Facilities, 11% of screening mammograms had abnormal findings and required further diagnostic evaluation.2. One factor to consider in examining these findings is that, with an average age of 63 years at enrollment, some older women who initiated E+P would be expected to experience physiological changes in breast tissue that could have been interpreted as abnormal, but are typical of changes seen when women begin HT years after menopause. 1Chlebowski RT, et al. JAMA. 2003;289: Brown ML, et al. AJR Am J Roentgenol. 1995;165:")
82
HRT’den Kaynaklanan Atfedilebilir Meme Kanseri Riski
4/11/2017 5:11 AM LMF/FM 2004 Oncology HRT’den Kaynaklanan Atfedilebilir Meme Kanseri Riski Kanser Gelişmeme İhtimali 50 yaşında, 10 yıl takip edilmiş, HRT almamış 50 yaşında, 10 yıl takip edilmiş, HRT almış %97,5 %96,8 Santen RJ, Petroni GR. J Clin Endocrinol Metab. 1999;84:

Benzer bir sunumlar

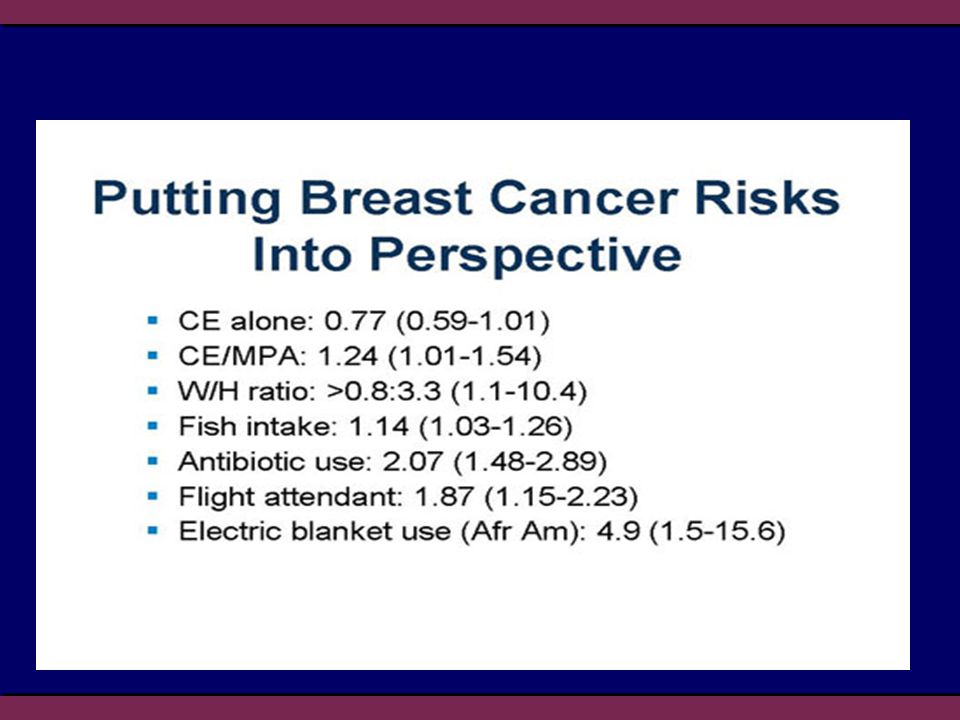
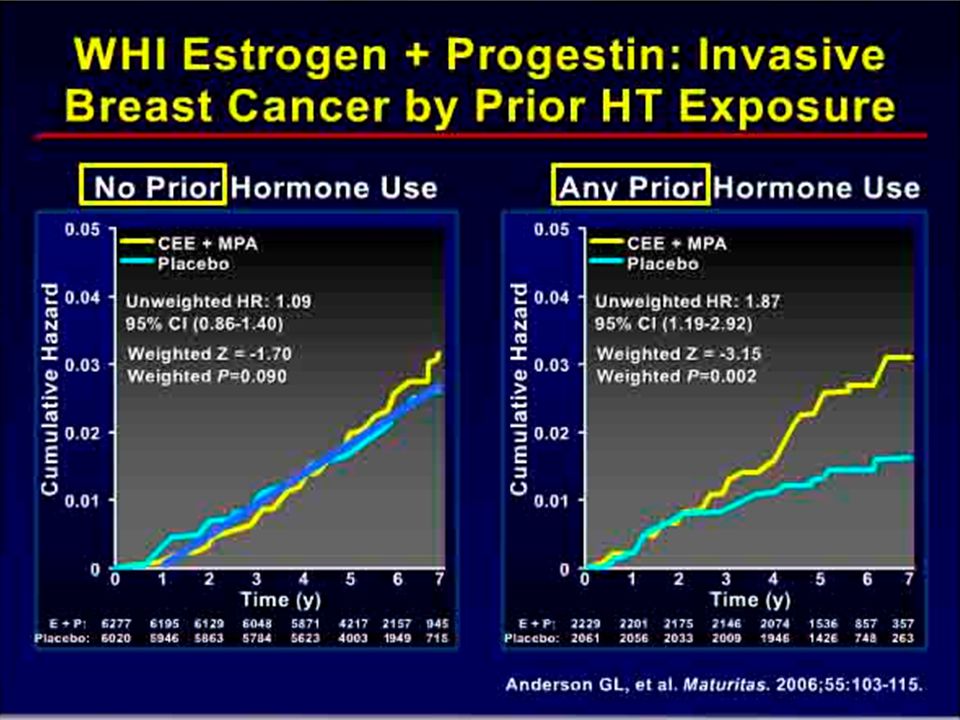




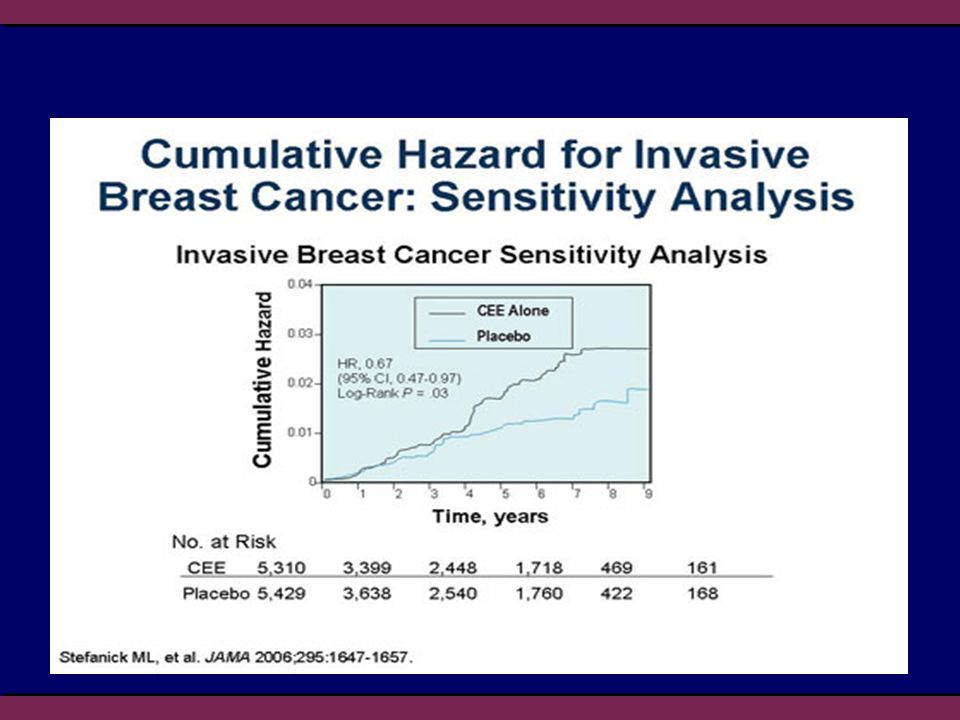
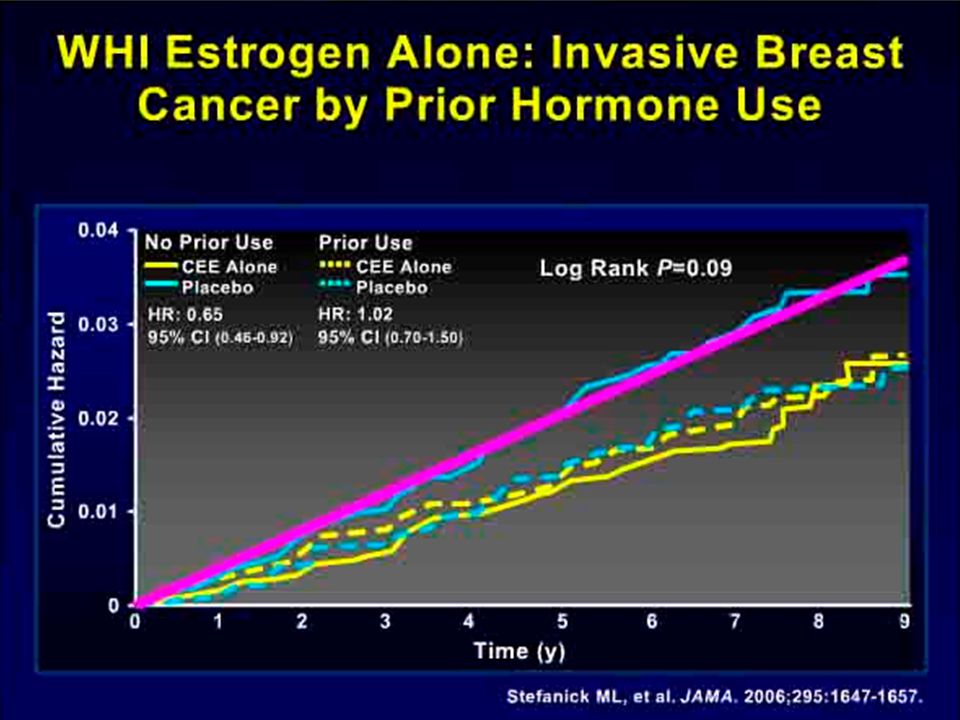
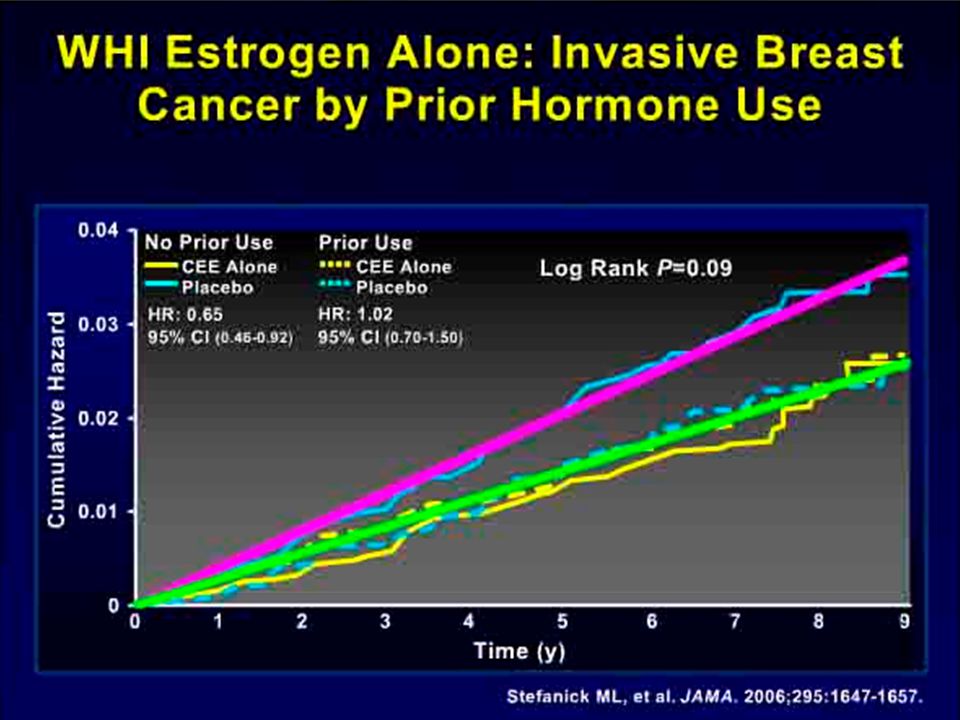
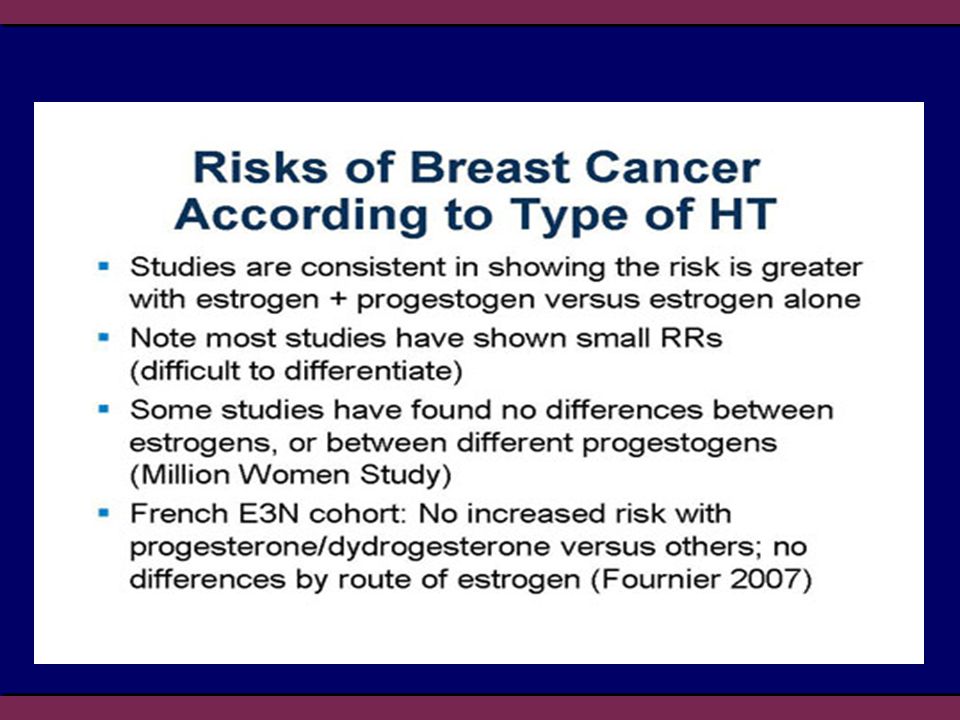
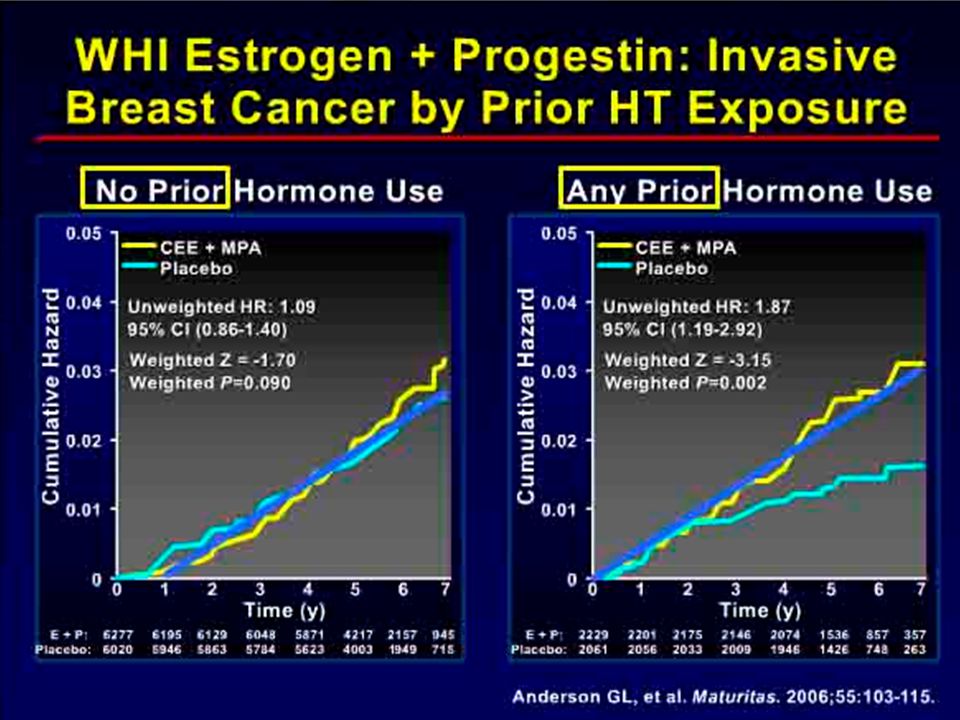
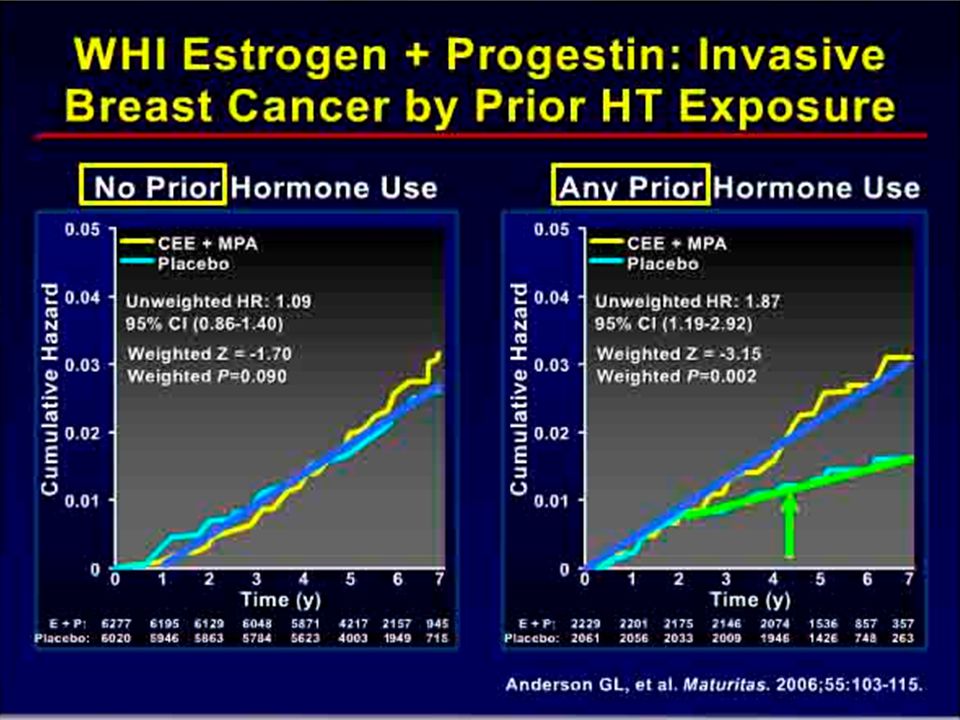
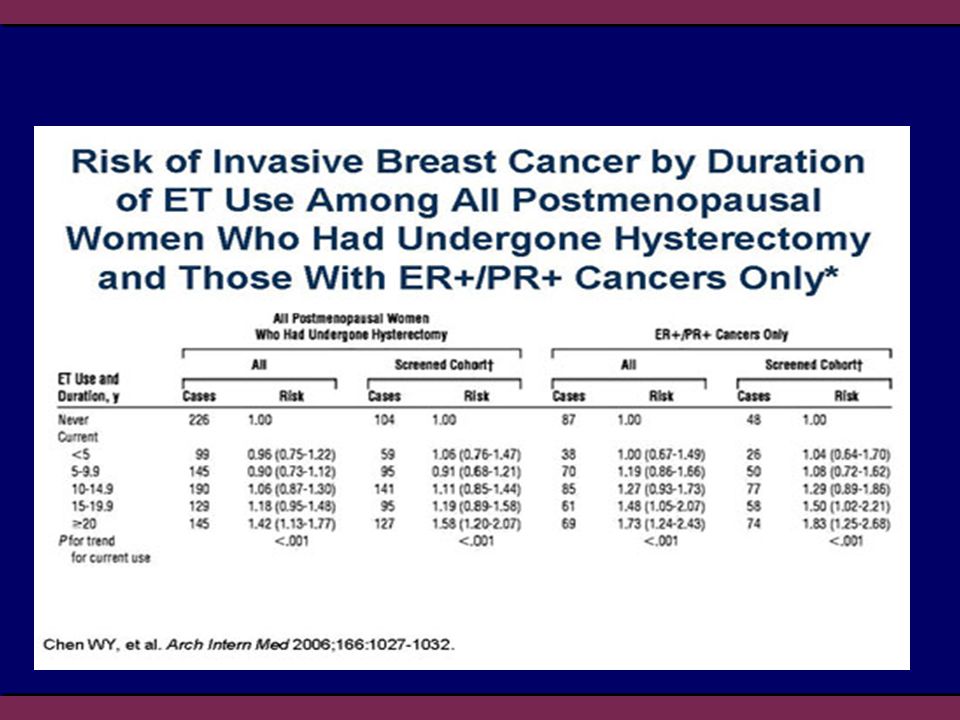

















>")

