Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Tubal Hastalıklarda IVF mi? Cerrahi mi?
Prof. Dr. Hulusi Bülent Zeyneloğlu Başkent Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum AB Üreme Endokrinolojisi ve İnfertilite Ünitesi

3
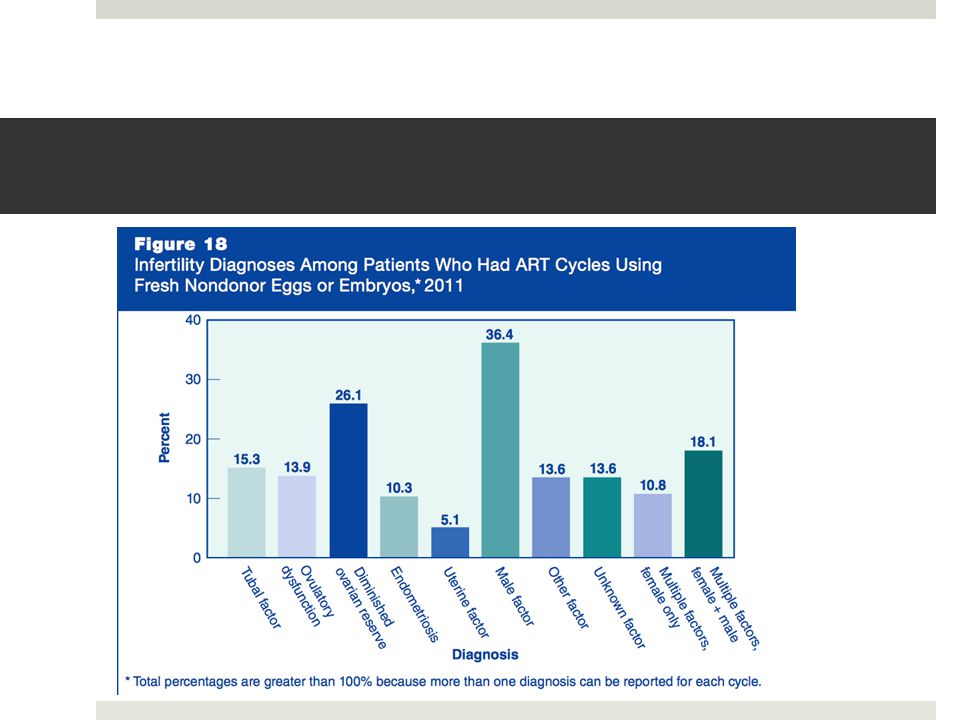
Fallop Tüp Patolojisi Distal tubal hastalık Bipolar hastalık %85;
Pelvik inflamatuvar koşullar sonucu oluşur Enfeksiyon, endometriozis, abdomino-pelvik cerrahi Hidrosalpenks Bipolar hastalık Tüpün hem proksimal, hem de distal ucunun etkilendiği durumdur Distal tubal disease may account for up to 85% of tubal infertility and is the result of any pelvic inflammatory condition including infection, endometriosis and abdomino-pelvic surgery. The endpoint of distal tubal disease is the formation of a hydrosalpinx, which constitutes the collection of fluid in the tube. The term bipolar tubal disease is used when both proximal and distal aspects of a tube are affected.

4
Tanı HSG USG: HyCoSy (HyFoSy) CAT Hidrolaparoskopi
Selektif Salpingografi Selective salpingography is another promising tech- nique that can be used in the assessment of proximal disease. It is based on the direct opacification of the fal- lopian tube with the use of a catheter directly placed in the tubal ostium. It is useful in differentiating tubal spasm from true obstruction and clarifying discrepant findings from other tests. It can be used therapeutically when combined with fallopian tube recanalisation to treat mild obstructions. The recanalisation procedure is simple for interventional radiologists, sometimes alongside gynaecologists and is performed with the use of a catheter and a guide wire system. The success rates reported range between 62% and 90%, and the aver- age pregnancy rates following the procedure are 30% (Thurmond et al., 2000). For patients with no risk factors, a negative chlamydia antibody test indicates that there is less than a 15% likelihood of tubal pathology (6). However, chlamydia antibody test- ing is limited by false positives from cross-reactivity with chlamydia pneu- moniae IgG and does not distinguish between remote and persistent infec- tion nor does it indicate whether the infection resulted in tubal damage (6). Therefore, hysterosalpingography (HSG) is the standard first-line test to evaluate tubal patency (7).
. For patients with no risk factors, a negative chlamydia antibody test indicates that there is less than a 15% likelihood of tubal pathology (6). However, chlamydia antibody test- ing is limited by false positives from cross-reactivity with chlamydia pneu- moniae IgG and does not distinguish between remote and persistent infec- tion nor does it indicate whether the infection resulted in tubal damage (6). Therefore, hysterosalpingography (HSG) is the standard first-line test to evaluate tubal patency (7).")
5
Laparoskopi Altın Standart

6
Tubal Cerrahi Gelişimi
1970’lerdeki mikrocerrahi kuralları başarıyı artırmıştır. The development of microsurgery (minimal tissue trauma, use of fine nonabsorbable sutures and intraoperative magnification, avoidance of tissue dessication, exquisite hemostasis and repair of all peritoneal surfaces) has offered great improvement in the outcome of reconstructive surgery.The residual length, the presence of chronic inflammation or tubal inclusion in the tubal wall and the presence of tubal endometriosis are all factors affecting the outcome of proximal reconstructive surgery that need to be con- sidered. Occasionally, proximal tubal patency can be restored by less invasive means via selective salpingog- raphy and tubal catheterisation (Sacks & Trew, 2004).
 has offered great improvement in the outcome of reconstructive surgery.The residual length, the presence of chronic inflammation or tubal inclusion in the tubal wall and the presence of tubal endometriosis are all factors affecting the outcome of proximal reconstructive surgery that need to be con- sidered. Occasionally, proximal tubal patency can be restored by less invasive means via selective salpingog- raphy and tubal catheterisation (Sacks & Trew, 2004).")
7
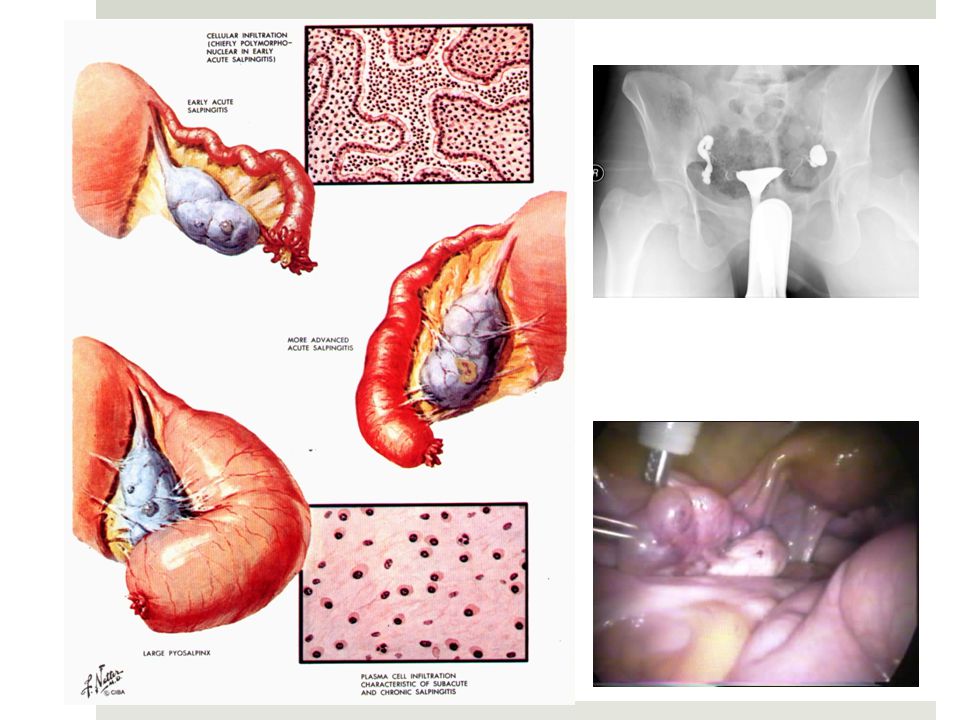
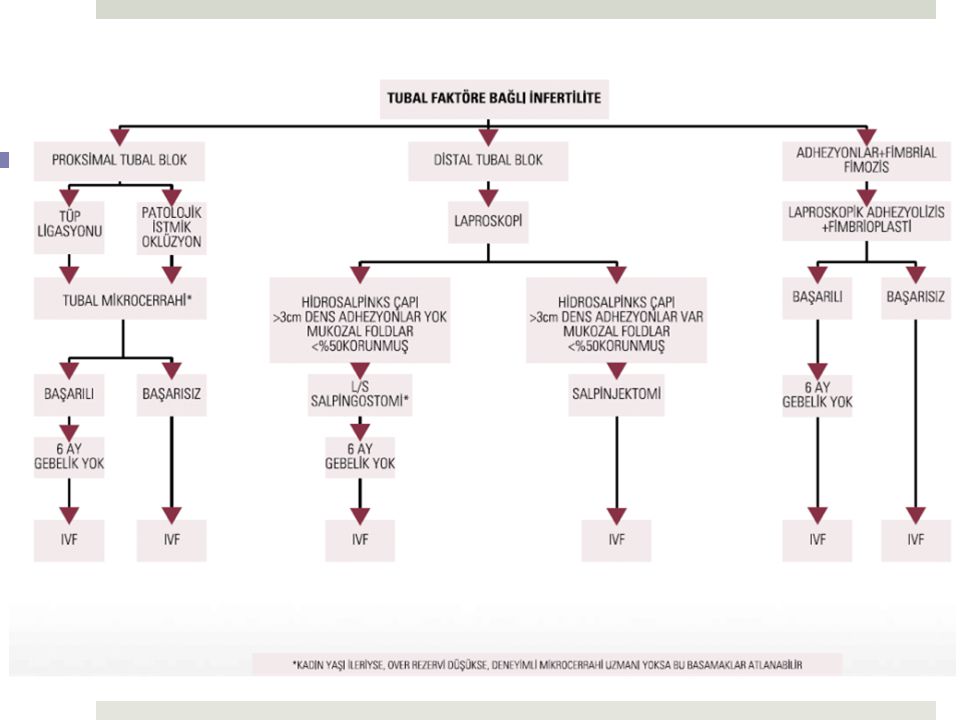
Distal tubal hastalık-Hidrosalpenks
Peritubal adezyonlar değil, tubal mukozal adezyonlar en belirleyici faktördür (Vasquez 1995) Sınırlı filmsel adezyonlar, <3cm dilate ve ince, katmanlı duvarı olan tüpler, İyi korunmuş tubal mukoza varlığında hidrosalpenks için rekonstrüktif cerrahi sonrasında GH %77 ve ektopik GH %4 civarındadır (Boer-Meisel 1986) Tubal mukoza LS ve HSG tarafından değerlendirilebilir. Ancak salpingoskopik değerlendirme daha hassastır. (Déchaud 1998). Sık kullanılmayan bir yöntemdir. The state of the tubal mucosa has attracted significant attention as a strong patient selection criterion. Evidence level A (Puttemans et al., 2000; Strandell & lindhard, 2000). Interestingly mucosal adhesions were shown to be the most important factor in selection of patients, while peritubal adhesions did not seem to influence preg- nancy rates (Vasquez et al., 1995). Pregnancy rates as high as 77% and tubal ectopic rates as low as 4% have been reported following reconstructive surgery for hydrosalpinges with a well-preserved mucosa (Boer-Meisel et al., 1986). The tubal mucosa can be assessed by laparoscopy and indirectly by HSG. Both methods have a widespread use in the fertility work up. It has, however, been suggested that the combina- tion of HSG and laparoscopy is not as accurate in the assessment of the tubal mucosa as is endoscopic inspection (Déchaud et al., 1998). Salpingoscopy is the most accurate method for identifying mucosal ad- hesions, but, although it has been available for many years, it is still not part of normal clinical practice in most centres. A good prognosis is associated with patients who have no more than limited filmy adnexal adhesions, mildly dilated tubes (<3 cm) with thin and pliable walls, and a lush endosal- pinx with preservation of the mucosal folds (26). Peritubal ad- hesions from the above causes or endometriosis may impair the ability of intrinsically normal tubes to capture an oocyte by mechanically interfering with the anatomic relationship between the distal fallopian tube and the ovary. One study of 147 patients reported cumulative pregnancy rates of 40% at 12 months after adhesiolysis by laparotomy, versus 8% in an untreated group (27).
 Sınırlı filmsel adezyonlar, <3cm dilate ve ince, katmanlı duvarı olan tüpler, İyi korunmuş tubal mukoza varlığında hidrosalpenks için rekonstrüktif cerrahi sonrasında GH %77 ve ektopik GH %4 civarındadır (Boer-Meisel 1986) Tubal mukoza LS ve HSG tarafından değerlendirilebilir. Ancak salpingoskopik değerlendirme daha hassastır. (Déchaud 1998). Sık kullanılmayan bir yöntemdir. The state of the tubal mucosa has attracted significant attention as a strong patient selection criterion. Evidence level A (Puttemans et al., 2000; Strandell & lindhard, 2000). Interestingly mucosal adhesions were shown to be the most important factor in selection of patients, while peritubal adhesions did not seem to influence preg- nancy rates (Vasquez et al., 1995). Pregnancy rates as high as 77% and tubal ectopic rates as low as 4% have been reported following reconstructive surgery for hydrosalpinges with a well-preserved mucosa (Boer-Meisel et al., 1986). The tubal mucosa can be assessed by laparoscopy and indirectly by HSG. Both methods have a widespread use in the fertility work up. It has, however, been suggested that the combina- tion of HSG and laparoscopy is not as accurate in the assessment of the tubal mucosa as is endoscopic inspection (Déchaud et al., 1998). Salpingoscopy is the most accurate method for identifying mucosal ad- hesions, but, although it has been available for many years, it is still not part of normal clinical practice in most centres. A good prognosis is associated with patients who have no more than limited filmy adnexal adhesions, mildly dilated tubes (<3 cm) with thin and pliable walls, and a lush endosal- pinx with preservation of the mucosal folds (26). Peritubal ad- hesions from the above causes or endometriosis may impair the ability of intrinsically normal tubes to capture an oocyte by mechanically interfering with the anatomic relationship between the distal fallopian tube and the ovary. One study of 147 patients reported cumulative pregnancy rates of 40% at 12 months after adhesiolysis by laparotomy, versus 8% in an untreated group (27).")
9
Puttemans Salpingoscopy Classification-1987
Grade I normal mucosal folds Grade II Major folds separated and flattened, however, otherwise normal Grade III Focal adhesions throughout the mucosal folds Grade IV Extensive adhesions and/or flattened areas throughout the mucosal folds Grade V Total disappearance of mucosal folds Boer-Meisel classification, 1986 Group 1 mucosa is normal with regular folds. Group 2 moderate alterations to the ampullary mucosa, with areas of normal mucosa interspersed with areas where the mucosal folds are rare or non-existent (atrophic mucosa). Group 3 mucosa has deteriorated considerably with either complete disappearance of the mucosa or the existence of intratubal synechiae (alveolar mucosa).
. Group 3. mucosa has deteriorated considerably with either complete disappearance of the mucosa or the existence of intratubal synechiae (alveolar mucosa).")
10
Salpinkoskopi

11
Salpingoskopi Değeri Marana R, Hum Reprod 1999;14::2072

12
Distal tubal Lezyonlarda Laparoskopi

15
İntraoperatif Hidrotubasyon Fertiliteyi Artırıyor.
Cerrahiden hemen sonra tubal yıkama gebelik oranlarını artırırken, post operatif yıkama veya hiç yıkamama gebelik oranları aynı kalır. 20mm Ringer Laktat IU Gentamisin + 5 mg Dekzametazon Zhengyu, 2013 Arch Gynecol Obstet

17
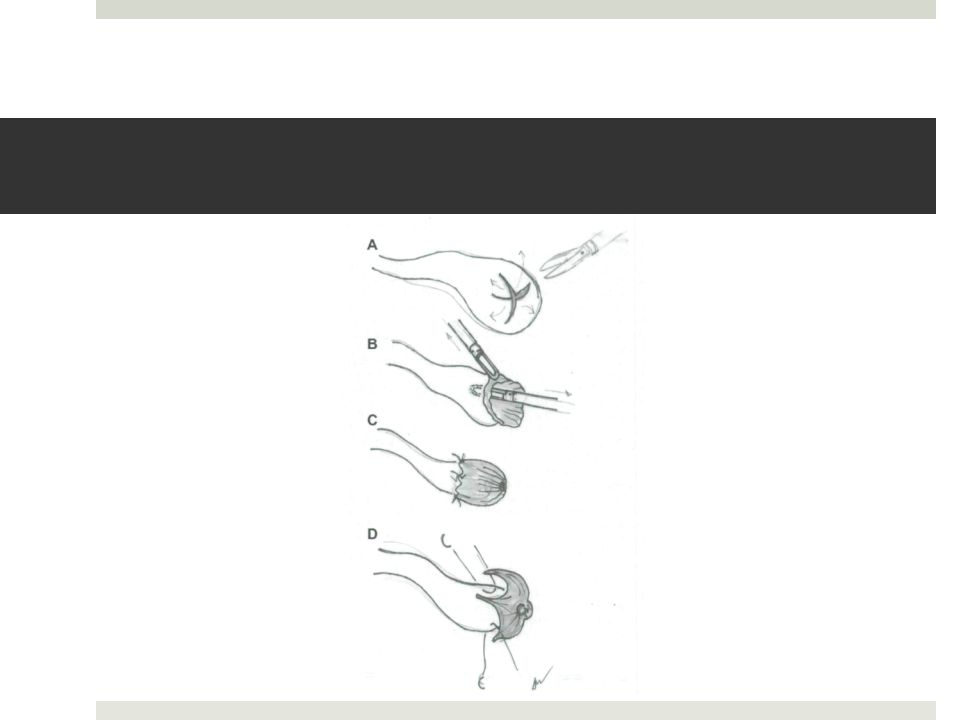
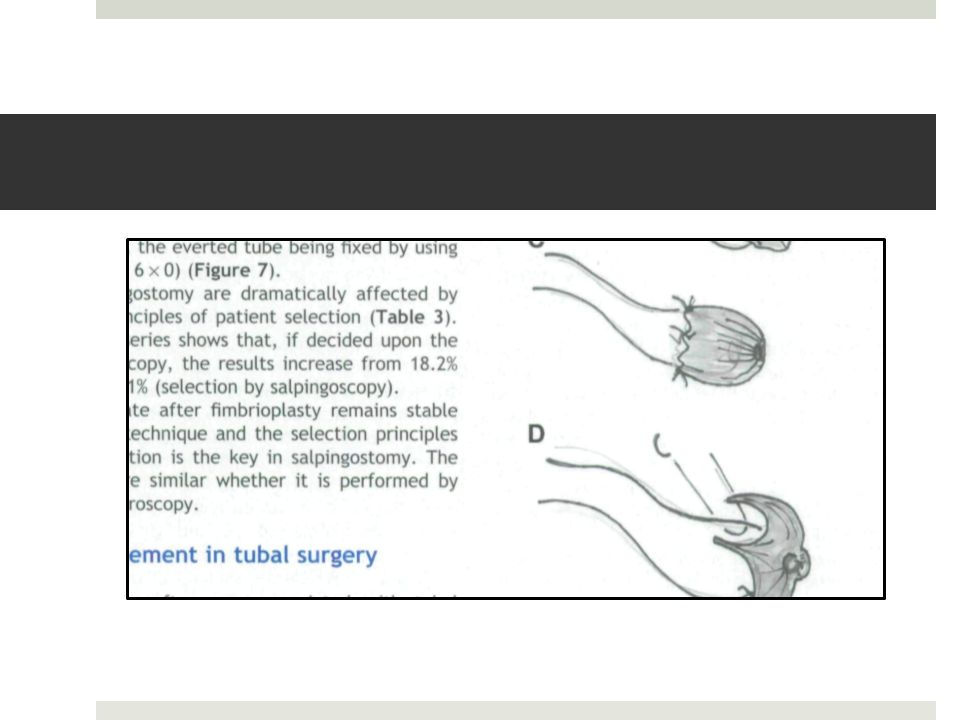
Techniques for pelvic surgery in subfertility

18
Distal tubal lezyonlarda laparoskopi
Yazar # Yapılan Süre IU.GH% Ekt.GH% DH% Fayez, fimbriopl 2y 19 salpingoneos 2y Daniell, salpingost 18ay Dubuisson, fimbriopl 18ay 34 salpingoneos 18ay 29 3 Audebert, fimbriopl 2y 17 4 ? Mc Comb, salpingost >1y ? 5 23 Dubuisson, salpingost 3-60ay Audebert, fimbriopl 2-5y

19
Laparoskopik Adezyolizis
Yazar # Takip IU-GH% Ekt-GH% DH% Bruhat, (orta) >18 ay 55 8 ? 27 (şidd.) ? Fayez, yıl Donnez, (avask) 18 ay ? ? 62 22 (vask) ? ? 50 Gomel, >9 ay
 >18 ay (şidd.) 44 7 Fayez, yıl Donnez, (avask) 18 ay (vask) 50. Gomel, >9 ay")
20
Contraindications to Tubal Surgery
Frozen pelvis Extensive ampullo-infundibular tubal resections for sterilization Extensive intra-ampullary and confirmed during the diagnostic phase of laparoscopy after opening the hydrosalpinx Genital tuberculosis or sequelae Additional infertility factors Age is another contraindication.

21
Cerrahi Ektopik Gebelik Riskini Artırır
Total Ektopik Gebelik Prediktörleri Bilateral Cerrahi Orta derecede hasar görmüş tubal mukoza Daha önceki PID atakları+ FHC Sendromu IUP EP Taylor, Fertil Steril, 2001

22
Unilateral Salpinjektomi veya PTL Gebelik Şansını Artırır
Ortalama gebe kalma süresi 5.6 ay Ektopik gebelik yok Sagoskin, Hum Reprod 2003

23
Konservatif mi, Radikal Cerrahi mi?
ESEP Çalışması Lancet 2014

24
Tubal Hastalık ve IVF İlk insan IVF gebeliği intrauterin olmayıp, ektopik idi. Steptoe PC & Edwards RG, 1976 “Proksimal tubal okluzyon Şiddetli tubal hastalığı olan hastalarda IVF öncesi uygulanmalıdır!” Steptoe PC, 1979 “Tubal faktörü olan hastalar IVF’de daha az gebelik şansı vardır.” Englert Y, 1987

25
Results of 3 Meta-analyses
Strandell A, Hum Reprod Update, 2000

26
Salpenjektomi Gebelik Hızını Artırır mı?
Power=0.43 Zeyneloglu, HB: Current Opinion Obst Gynecol /3

27
Hidrosalpinks: IVF

28
Hidrosalpenks: IVF oklüzyon

29
Salpenjektomi Over Rezervini Azaltır mı?
Grynnerup A: 2013

30
Tubal Ligasyon Over Rezervini Azaltır mı?

31
Cerrahi Başarısız Olduğunda

32
Tubal Cerrahi mi? IVF mi? Şu ana kadar bu iki yöntemi karşılaştırmış randomize kontrollü çalışma bulunmamaktadır.

33
Tubal Anastomoz veya IVF
Cetin, 2013 Laparoendosc Adv Surg Tech A

34
Tubal Anastomoz veya IVF
Kümülatif GH (Boeckxstaens, 2007 Hum Rep) 37y altı : IVF için %52, Cerrahi için %72 37y üstü :IVF için %51, Cerrahi için %36 Mikrocerrahi (Schippert 2011, Fertil Steril) Mikrocerrahi sonrası GH: %43, IVF sonrası GH:%28 Ektopik Gebelik Riski (Schippert, 2012 Arch Gynecol Obstet) Cerrahi sonrası %7.9, IVF sonrası 5.6
 37y altı : IVF için %52, Cerrahi için %72. 37y üstü :IVF için %51, Cerrahi için %36. Mikrocerrahi (Schippert 2011, Fertil Steril) Mikrocerrahi sonrası GH: %43, IVF sonrası GH:%28. Ektopik Gebelik Riski (Schippert, 2012 Arch Gynecol Obstet) Cerrahi sonrası %7.9, IVF sonrası 5.6.")
35
Ektopik Gebelik Riski-IVF

36
Hidrosalpenks: Cerrahi veya IVF
Chanelles, 2011

37
Robotik Cerrahi – Tubal cerrahi
İlk rapor 1999y (Falcone) Laparotomi ile benzer ekonomik, ve daha az hastane süresi (Dharia Patel 2008) Tüm Robotik Cerrahi avantajları geçerli.
 Laparotomi ile benzer ekonomik, ve daha az hastane süresi (Dharia Patel 2008) Tüm Robotik Cerrahi avantajları geçerli.")
39
C. Bonneau , 2012

Benzer bir sunumlar