Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
KOH ve embriyo kalitesi
Dr. Kemal ÖZGÜR

3
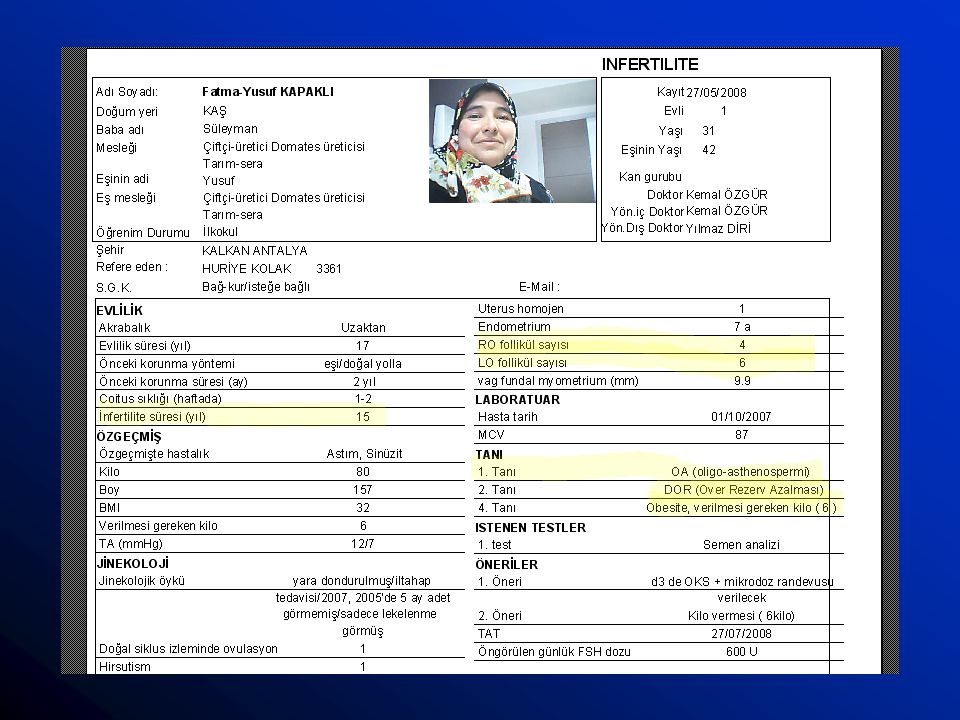
1. KOH: Temmuz 2008

4
Total yumurta 11 M2 8 2PN 3 G2 2 G3 1

5
2. KOH=Kasım 2008

6
Total yumurta 14 M2 9 2PN 8 G1 7 G2 1

7
Plan Embriyo kalitesi tanımı Agonist ve antagonist siklusları
HMG ve FSH siklusları LH katkısı Follikül çaplarının katkısı Coasting katkısı Mild stimulations vs harsh (dozun katkısı)
")
8
EQ; Cleavage stage embryos
Cleavage rate Cell number Cleavage symmetry Cytoplasmic fragmentasyon Multinucleation Zona pellucida structure Cell-cell contact Cytoplasmic organization

9
Cleavage hızı 1st cleavage: hr post insemination: Avantajlı implantasyon. D2-4 cells (Ziebe et al 1997, Giorgetti et al. 1995) D3: 7-9 cells (Gerris et al. 1999, Van Royen et al 1999, 2001) Hızlı cleavage: yüksek mozaisizm ve polyspermic fertilizasyon olabilir ancak data yok. Data olmadığı için yavaş büyüyen embriyo transferi yapılmakta.
 Hızlı cleavage: yüksek mozaisizm ve polyspermic fertilizasyon. olabilir ancak data yok. Data olmadığı için yavaş büyüyen embriyo transferi yapılmakta.")
10
Hücre boyut ve simetrisi
Zayıf foll gelişim=(Goyannes et al(1990) eşit boyutta olmayan blastomerlerde total blastomer volümünün % 8 daha az olduğunu buldu. (Pronucl evredeki volümden farklı olmayacağı için zayıf folliküler gelişimden kaynaklanacağını iddia etmiş) Spindle asimetrisi de yol açabilir. Fragmantasyonla sitoplazma kaybı Cytokynesis-karyokinesis ilişkisinin bozulması-(dominant multinukleate blastomer ve bölünen diğerleri)
 eşit boyutta olmayan blastomerlerde total blastomer volümünün % 8 daha az olduğunu buldu. (Pronucl evredeki volümden farklı olmayacağı için zayıf folliküler gelişimden kaynaklanacağını iddia etmiş) Spindle asimetrisi de yol açabilir. Fragmantasyonla sitoplazma kaybı. Cytokynesis-karyokinesis ilişkisinin bozulması-(dominant multinukleate blastomer ve bölünen diğerleri)")
11
Multinukleasyon Mekanizma: sitokinesis olmadan karyokinesis; nukleus fragmantasyonu; anafaz sırasında kromozomların anormal migrasyonu (Tesarik et al. 1987, Winston et la 1991, Hardy et al.1993) 2 hücreli embriyolarda daha fazla (Blaiker ve Cadesky 1997) D2 ve d3 embriyolarda varlığı ileri derecede mozaisizm ve FISH de polyploidi (Kigman et al 1996) Staessemn ve Van Steirrteghem (1998) 2 cell stage multinukleasyon yarısı normal diploid olup geçici ve reversibl fenomen olabileceğini iddia etmişler.
 2 hücreli embriyolarda daha fazla (Blaiker ve Cadesky 1997) D2 ve d3 embriyolarda varlığı ileri derecede mozaisizm ve FISH de polyploidi (Kigman et al 1996) Staessemn ve Van Steirrteghem (1998) 2 cell stage multinukleasyon yarısı normal diploid olup geçici ve reversibl fenomen olabileceğini iddia etmişler.")
12
Zona Pellucida yapısı ZP embriyo gelişiminde incelme
Kalınlığı embriyo doğal hatching yetisini belirliyor (Cohen et al 1989) Hücre sayısı, embriyo grade, ileri maternal yaş, fragmentasyon oranı ile kalın zona arasında anlamlı korelasyon (Garsida et al 1997).
 Hücre sayısı, embriyo grade, ileri maternal yaş, fragmentasyon oranı ile kalın zona arasında anlamlı korelasyon (Garsida et al 1997).")
13
Cell-cell contact Cell-cell contact hücre adezyon moleküllerinin expresyonuna yol açar Arrest olan fare blastomerlerini arrest olmayanları ile agregasyon yaptırması tekrar gelişme yeteneğini kazanmasına yol açtı. (Neganova et al 2000) Sitoplazmik fragmantasyon interselüler aralıkları doldurarak bozabilir.
 Sitoplazmik fragmantasyon interselüler aralıkları doldurarak bozabilir.")
14
Cytoplasmic integrity
Çok sayıda intrasitoplazmik vakuol veya şiddetli hücre kontraksionu = muhtemel dejenaratif süreç Buna karşın özellikle d3 embriyolardaki veziküler görünüm genomik aktivasyon sinyali? Vezikulasyon ile gebelik pozitif korele (Desai et al 2000)
")
15
Sitoplazmik fragmantasyon
Erken evre embriyolarda sıkça görülen bir durum: Bir cohort grubu içinde bütün embriyoları-bir kısmını alabilir. “cell division without nuclear division” ( Edwards RG, Steptoe PC, Purdy JM. Fertilization and cleavage in vitro of preovulator human oocytes. Nature. 1970) Çoğu ilk cleavage’da. Fragmantasyonun klinik gebelik oranın düşürdüğü ilk olarak 1987 de gösterilmiş. (Puissant F et al. Hum Reprod 1987 Nov;2(8):705-8 Embryo scoring as a prognostic tool in IVF treatment.
 Çoğu ilk cleavage’da. Fragmantasyonun klinik gebelik oranın düşürdüğü ilk olarak 1987 de gösterilmiş. (Puissant F et al. Hum Reprod 1987 Nov;2(8):705-8 Embryo scoring as a prognostic tool in IVF treatment.")
16
Fragmantasyon ve IVF outcome
Saint Barnabas grubu EggCyte database. (1999 Fert& Sterility 2410 hasta retrospective analiz). PATTERN VOLUM W1 % 0-5 W2 %6-15 W3 % 16-25 W4 % 26-35 W5 % >35 Tip I: minimal volüm- fragmanlar tek blastomerle ilişkili Tip II: lokalize fragmanlar ve perivitelline aralığı kaplar Tip III: küçük yayılmış fragmanlar Tip IV: iri fragmanlar-blastomer e yakın boyutta: gnll random ve eşit olmayan blastomerler eşlik eder Tip V: nekrotik görünümde granüler görünüm ve komşu blastomerde kontraksion
. PATTERN. VOLUM. W1. % 0-5. W2. %6-15. W3. % W4. % W5. % >35. Tip I: minimal volüm- fragmanlar tek blastomerle ilişkili. Tip II: lokalize fragmanlar ve perivitelline aralığı kaplar. Tip III: küçük yayılmış fragmanlar. Tip IV: iri fragmanlar-blastomer e yakın boyutta: gnll random ve eşit olmayan blastomerler eşlik eder. Tip V: nekrotik görünümde granüler görünüm ve komşu blastomerde kontraksion.")
17
6,4 31,8 37,9 28,2 33,8 23,4 30,5 18,2 Volume göre IR Group IR(%) W1
PATTERN VOLUM Group Fragmantation range IR(%) W1 % 0-5 31,8 W2 %6-15 28,2 W3 % 16-25 23,4 W4 % 26-35 W5 % >35 6,4 Group Fragmantation range IR(%) T1 minimal volüm- fragmanlar tek blastomerle ilişkili 37,9 T2 lokalize fragmanlar ve perivitelline aralığı kaplar 33,8 T3 küçük yayılmış fragmanlar 30,5 T4 iri fragmanlar-blastomer e yakın boyutta: gnll random ve eşit olmayan blastomerler eşlik eder 18,2
 W1. % ,8. W2. % ,2. W3. % ,4. W4. % W5. % >35. 6,4. Group. Fragmantation range. IR(%) T1. minimal volüm- fragmanlar tek blastomerle ilişkili. 37,9. T2. lokalize fragmanlar ve perivitelline aralığı kaplar. 33,8. T3. küçük yayılmış fragmanlar. 30,5. T4. iri fragmanlar-blastomer e yakın boyutta: gnll random ve eşit olmayan blastomerler eşlik eder. 18,2.")
18
Mekanizma ? Apopitosis (programlı hücre ölümü) ? İskemik nekroz
İzole tek hücre sorunu Enflamasyon yok İskemik nekroz (Oncosis): Hasar—hücresel şişme-membran rüptürü Komşu sağlıklı dokuda Enflamatuar yanıt
: Hasar—hücresel şişme-membran rüptürü. Komşu sağlıklı dokuda Enflamatuar yanıt.")
19
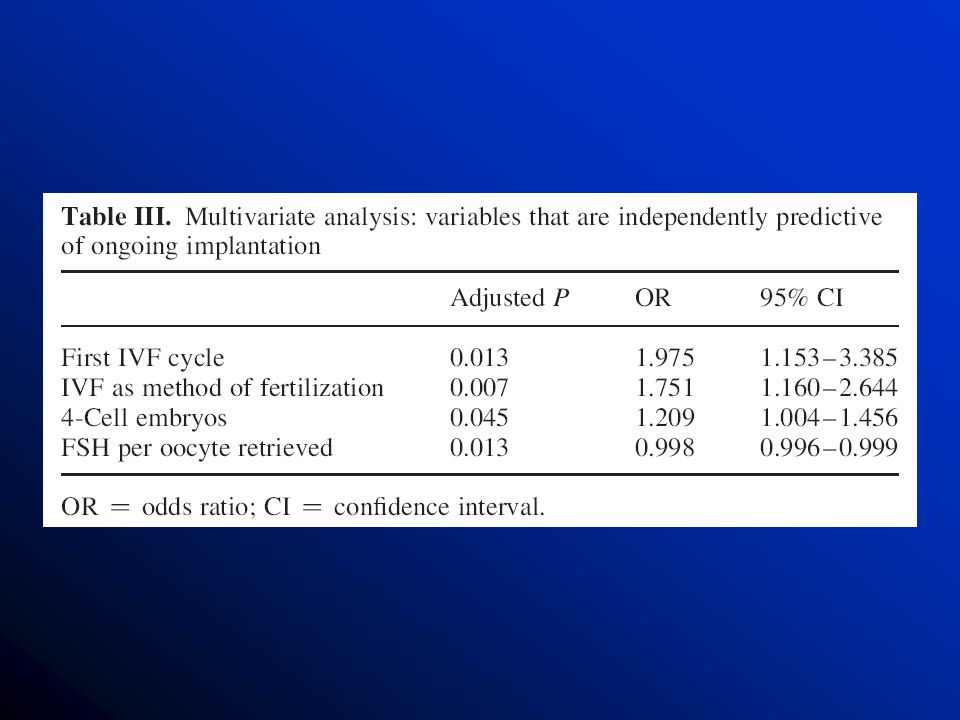
Başarıyı etkileyen parametre?

20
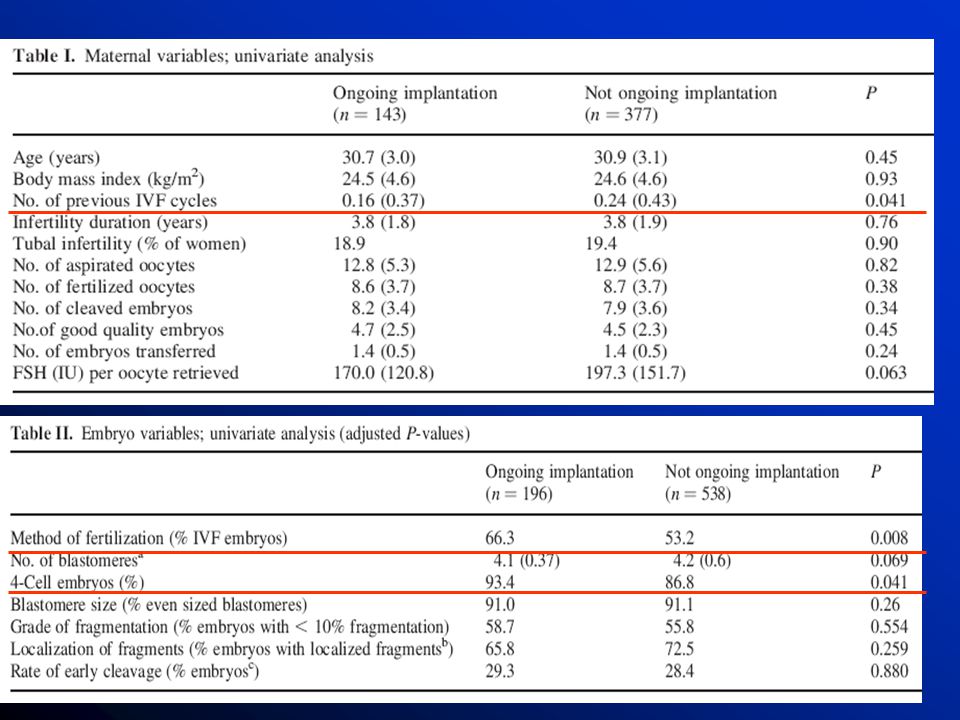
661 women elective single embryo transfer or double embryo transfer cycles with 0 or 100% ongoing implantation (n 5 520) were analysed
 were analysed.")
23
KOH da antagonist kullanımının etkisi?

24
F&S 2005 OBJECTIVE: To compare the effects of oral contraceptive (OC) pill pretreatment in recombinant FSH/GnRH-antagonist versus recombinant FSH/GnRH-agonist stimulation in in vitro fertilization (IVF) patients, and to evaluate optimization of retrieval day. DESIGN: Prospective, randomized, multicenter study. SETTING: Private practice and university centers. PATIENT(S): Eighty patients undergoing IVF who met the appropriate inclusion criteria. INTERVENTION(S): Four study centers recruited 80 patients. The OC regimen began on cycle days 2 to 4 and was discontinued on a Sunday after 14 to 28 days. The recombinant FSH regimen was begun on the following Friday. The GnRH-agonist group was treated with a long protocol; the GnRH-antagonist was initiated when the lead follicle reached 12 to 14 mm. When two follicles had reached 16 to 18 mm, hCG was administered. MAIN OUTCOME MEASURE(S): The primary outcome measures were the number of cumulus-oocyte complexes, day of the week for oocyte retrieval, and total dose and days of stimulation of recombinant FSH. Secondary efficacy variables included pregnancy and implantation rate; serum E(2) levels on stimulation day 1; serum E(2), P, and LH levels on the day of hCG administration; follicle size on day 6 and day of hCG administration; the total days of GnRH-analogue treatment; total days on OC; total days from end of OC to oocyte retrieval; and the cycle cancellation rate. RESULT(S): Patient outcomes were similar for the days of stimulation, total dose of gonadotropin used, two-pronuclei embryos, pregnancy (44.4% GnRH-antagonist vs. 45.0% GnRH-agonist, P=.86) and implantation rates (22.2% GnRH-antagonist vs. 26.4% GnRH-agonist, P=.71). Oral contraceptive cycle scheduling resulted in 78% and 90% of retrievals performed Monday through Friday for GnRH-antagonist and GnRH-agonist. A one day delay in OC discontinuation and recombinant FSH start would result in over 90% of oocyte retrievals occurring Monday through Friday in both groups. CONCLUSION(S): The OC pretreatment in recombinant FSH/GnRH-antagonist protocols provides a patient-friendly regimen and can be optimized for weekday retrievals. No difference was seen in number of 2PN embryos, cryopreserved embryos, embryos transferred, implantation and pregnancy rates between the two stimulation protocols.
 pill pretreatment in recombinant FSH/GnRH-antagonist versus recombinant FSH/GnRH-agonist stimulation in in vitro fertilization (IVF) patients, and to evaluate optimization of retrieval day. DESIGN: Prospective, randomized, multicenter study. SETTING: Private practice and university centers. PATIENT(S): Eighty patients undergoing IVF who met the appropriate inclusion criteria. INTERVENTION(S): Four study centers recruited 80 patients. The OC regimen began on cycle days 2 to 4 and was discontinued on a Sunday after 14 to 28 days. The recombinant FSH regimen was begun on the following Friday. The GnRH-agonist group was treated with a long protocol; the GnRH-antagonist was initiated when the lead follicle reached 12 to 14 mm. When two follicles had reached 16 to 18 mm, hCG was administered. MAIN OUTCOME MEASURE(S): The primary outcome measures were the number of cumulus-oocyte complexes, day of the week for oocyte retrieval, and total dose and days of stimulation of recombinant FSH. Secondary efficacy variables included pregnancy and implantation rate; serum E(2) levels on stimulation day 1; serum E(2), P, and LH levels on the day of hCG administration; follicle size on day 6 and day of hCG administration; the total days of GnRH-analogue treatment; total days on OC; total days from end of OC to oocyte retrieval; and the cycle cancellation rate. RESULT(S): Patient outcomes were similar for the days of stimulation, total dose of gonadotropin used, two-pronuclei embryos, pregnancy (44.4% GnRH-antagonist vs. 45.0% GnRH-agonist, P=.86) and implantation rates (22.2% GnRH-antagonist vs. 26.4% GnRH-agonist, P=.71). Oral contraceptive cycle scheduling resulted in 78% and 90% of retrievals performed Monday through Friday for GnRH-antagonist and GnRH-agonist. A one day delay in OC discontinuation and recombinant FSH start would result in over 90% of oocyte retrievals occurring Monday through Friday in both groups. CONCLUSION(S): The OC pretreatment in recombinant FSH/GnRH-antagonist protocols provides a patient-friendly regimen and can be optimized for weekday retrievals. No difference was seen in number of 2PN embryos, cryopreserved embryos, embryos transferred, implantation and pregnancy rates between the two stimulation protocols.")
25
22 RCTs 3176 subjects live birth between the two GnRH analogues [odds ratio (OR), 0.86; 95% confidence intervals (CI), 0.72 to 1.02]. This systematic review and meta-analysis aimed to answer the following clinical question: among patients treated for IVF with gonadotrophins and GnRH analogues, is the probability of live birth per randomized patient dependent on the type of analogue used? Eligible studies were randomized controlled trials (RCTs), published as a full manuscript in a peer-reviewed journal, that contained sufficient information to allow ascertainment of whether randomization was true and whether equality was present between the groups compared. A literature search identified 22 RCTs comparing GnRH antagonists and GnRH agonists that involved 3176 subjects. Where live birth was not reported in a study that fulfilled the inclusion criteria, an effort was made to contact the corresponding authors to retrieve the missing information. If this was not possible, the reported outcome measure, clinical pregnancy or ongoing pregnancy was converted to live birth in 12 studies using published data (Arce et al., 2005). No significant difference was present in the probability of live birth between the two GnRH analogues [odds ratio (OR), 0.86; 95% confidence intervals (CI), 0.72 to 1.02]. This result remains stable in subgroup analysis that ordered the studies by type of population studied, gonadotrophin type used for stimulation, type of agonist protocol used, type of agonist used, type of antagonist protocol used, type of antagonist used, presence of allocation concealment, presence of co-intervention and the way the information on live birth was retrieved. In conclusion, the probability of live birth after ovarian stimulation for IVF does not depend on the type of analogue used for pituitary suppression.
![22 RCTs 3176 subjects. live birth between the two GnRH analogues [odds ratio (OR), 0.86; 95% confidence intervals (CI), 0.72 to 1.02].](http://slideplayer.biz.tr/slide/2805638/10/images/25/22+RCTs+3176+subjects.+live+birth+between+the+two+GnRH+analogues+%5Bodds+ratio+%28OR%29%2C+0.86%3B+95%25+confidence+intervals+%28CI%29%2C+0.72+to+1.02%5D..jpg "This systematic review and meta-analysis aimed to answer the following clinical question: among patients treated for IVF with gonadotrophins and GnRH analogues, is the probability of live birth per randomized patient dependent on the type of analogue used Eligible studies were randomized controlled trials (RCTs), published as a full manuscript in a peer-reviewed journal, that contained sufficient information to allow ascertainment of whether randomization was true and whether equality was present between the groups compared. A literature search identified 22 RCTs comparing GnRH antagonists and GnRH agonists that involved 3176 subjects. Where live birth was not reported in a study that fulfilled the inclusion criteria, an effort was made to contact the corresponding authors to retrieve the missing information. If this was not possible, the reported outcome measure, clinical pregnancy or ongoing pregnancy was converted to live birth in 12 studies using published data (Arce et al., 2005). No significant difference was present in the probability of live birth between the two GnRH analogues [odds ratio (OR), 0.86; 95% confidence intervals (CI), 0.72 to 1.02]. This result remains stable in subgroup analysis that ordered the studies by type of population studied, gonadotrophin type used for stimulation, type of agonist protocol used, type of agonist used, type of antagonist protocol used, type of antagonist used, presence of allocation concealment, presence of co-intervention and the way the information on live birth was retrieved. In conclusion, the probability of live birth after ovarian stimulation for IVF does not depend on the type of analogue used for pituitary suppression.")
26
HMG vs rec FSH?

27
731 women first attempt to provide a comprehensive and systematic evaluation of embryo quality in patients undergoing ovarian stimulation with two different gonadotrophin preparations, following a similar stimulation protocol and similar pre-randomization and post-randomization procedures. BACKGROUND: There are limited data on the impact of different gonadotrophin preparations on embryo quality. METHODS: This evaluation was part of a randomized, assessor-blind, multinational trial, conducted in 731 women undergoing IVF after stimulation with highly purified human menopausal gonadotropin (HP-hMG; MENOPUR) (n = 363) or recombinant FSH (rFSH; GONAL-F) (n = 368). Ongoing pregnancy was the primary end-point [HP-hMG 27% and rFSH 22%; odds ratio (OR) (95% confidence interval, CI) 1.25 ( )]. All 7535 oocytes retrieved were evaluated daily until day 3 (embryo transfer) in a blinded manner both by local site embryologists and a central panel of three embryologists. RESULTS: The proportion of top-quality embryos per oocyte retrieved was higher with HP-hMG (11.3%) compared with rFSH (9.0%) (P = 0.044) in the local assessment, but comparable in the central assessment (9.5 and 8.0%, respectively). Significant differences in favour of HP-hMG were observed for number of blastomeres and degree of fragmentation, while uniformity of blastomere sizes, localization of fragments, frequency of multinucleation and homogeneous cytoplasm were comparable between HP-hMG and rFSH. The live birth, ongoing pregnancy and ongoing implantation rates for top-quality embryos were higher with HP-hMG than rFSH [48 versus 32% (P = 0.038), 48 versus 32% (P = 0.038), 41 versus 27% (P = 0.032)]. Both the proportion of embryos with at least 50% surviving blastomeres after cryopreservation and embryos resuming mitosis were more frequent with HP-hMG compared with rFSH. CONCLUSIONS: Composition of gonadotrophin preparations used during ovarian stimulation has an impact on some embryo quality parameters. The capacity to implant of the top-quality embryos derived from stimulation with HP-hMG appears to be improved, although the mechanism needs to be elucidated.
 (n = 363) or recombinant FSH (rFSH; GONAL-F) (n = 368). Ongoing pregnancy was the primary end-point [HP-hMG 27% and rFSH 22%; odds ratio (OR) (95% confidence interval, CI) 1.25 ( )]. All 7535 oocytes retrieved were evaluated daily until day 3 (embryo transfer) in a blinded manner both by local site embryologists and a central panel of three embryologists. RESULTS: The proportion of top-quality embryos per oocyte retrieved was higher with HP-hMG (11.3%) compared with rFSH (9.0%) (P = 0.044) in the local assessment, but comparable in the central assessment (9.5 and 8.0%, respectively). Significant differences in favour of HP-hMG were observed for number of blastomeres and degree of fragmentation, while uniformity of blastomere sizes, localization of fragments, frequency of multinucleation and homogeneous cytoplasm were comparable between HP-hMG and rFSH. The live birth, ongoing pregnancy and ongoing implantation rates for top-quality embryos were higher with HP-hMG than rFSH [48 versus 32% (P = 0.038), 48 versus 32% (P = 0.038), 41 versus 27% (P = 0.032)]. Both the proportion of embryos with at least 50% surviving blastomeres after cryopreservation and embryos resuming mitosis were more frequent with HP-hMG compared with rFSH. CONCLUSIONS: Composition of gonadotrophin preparations used during ovarian stimulation has an impact on some embryo quality parameters. The capacity to implant of the top-quality embryos derived from stimulation with HP-hMG appears to be improved, although the mechanism needs to be elucidated.")
28
In the present study, despite the fact that more oocytes were retrieved after stimulation with rFSH, the number of top-quality embryos was the same in the two groups. CRITICS MAIN FLAWS: PRIMARY ENDPOINT NOT MET The study aimed at demonstrating the superiority of Menopur. This endpoint was not met, this is why the authors switched to non-inferiority claims. The study failed to show statistically significant higher pregnancy rates (PR) with Menopur versus GONAL-f. (See back-up information for Statistical analysis.) LOW POWER for the study – 70 %! There is a high probability (30%) that the results are just by chance and not due to true treatment differences. The unusually low power does not provide confidence as to the reliability of the data. For registration trials authorities request usually 90% power for Phase III (ICH guidelines, EMEA, FDA). LOW ONGOING PREGNANCY RATE – 22 % for GONAL-f The ongoing pregnancy rate observed with GONAL-f (22%) is surprisingly low compared to other published studies, which have shown pregnancy rates generally above 30%. (See back-up information for Literature Review.) 225 IU IS OVERDOSING The GONAL-f Package Insert (USA) refers to an initial dosing of 150 IU per day. Only in patients 35 years old or in patients with deeply suppressed endogenous gonadotrophins should GONAL-f be initiated at a dose of 225 IU per day. This also reflects current clinical practice. (See back-up information: Published studies with different starting doses for GONAL-f.) THE PERCENTAGE OF TOP QUALITY EMBRYOS PER OOCYTE RETRIEVED was 11.3% in the Menopur group and 9.0% in the GONAL-f group (p<0.05). It has been shown that – especially in young patients overdosing may lead to low-quality embryos. A difference of 2.3% can not be considered as statistically significant (p<0.05) with an insufficient sample size. RECOMBINANT VERSUS URINARIES Why did Ferring announce investment in recombinant gonadotrophin research if they believe that urinaries are better? Ferring Forum, Hamburg, Germany, 2005. Other important considerations The authors mentioned that the study was stratified by age; however, nothing is said about how this stratification factor was used in the analysis, or about the results obtained in the different age strata. The study reports a higher, though not statistically different rate in early pregnancy loss for the r-hFSH-treated group (32% in the GONAL-f group versus 24% in the Menopur group). Literature data report on a lower abortion rate for r-hFSH or similar/comparable early pregnancy loss for the two compounds (Franco 2000). Safety data associated with both treatments is missing from the abstract. Literature data report on a slightly lower occurrence of OHSS with r-hFSH compared to hMG (Aboulghar 1998, Eur-Israeli Study). STATISTICS The hypotheses presented in the protocol involve a 2-step procedure: step 1, test for superiority but, if superiority is not demonstrated, switch to step 2, test for non-inferiority. Step 1 (superiority objective) is not powered at all; the authors do not mention what difference they expected in order to establish the superiority of Menopur compared to GONAL-f. The minimum rule should be to define an expected difference between the 2 treatments, an alpha level for the statistical significance (generally set at 5%) and a power for this study. Neither are mentioned; therefore, it is impossible to estimate the number of patients, which would have been required to conclude on superiority. Step 2 (non-inferiority objective) is largely underpowered. In fact, the number of patients entered in this study (N = 731 overall) is far below the sample size required (N = 1042 patients) for a power of 80% (the minimum power required by regulatory agencies). Furthermore, the limit margins used for a hypothetical proof of non-inferiority (ranging from –6.5% to –7.8%) are largely outside the clinically relevant window (-3% to-4%). In other words, the rules they used for this study, they could conclude on a relative similarity of the 2 products even if the difference observed was as high as 8% !!, which is completely unrealistic. Overall pregnancy rate with GONAL-f is surprisingly low Clinical pregnancy rates with the use of recombinant h-FSH compared to urinary FSH or u-hMG.
 with Menopur versus GONAL-f. (See back-up information for Statistical analysis.) LOW POWER for the study – 70 %! There is a high probability (30%) that the results are just by chance and not due to true treatment differences. The unusually low power does not provide confidence as to the reliability of the data. For registration trials authorities request usually 90% power for Phase III (ICH guidelines, EMEA, FDA). LOW ONGOING PREGNANCY RATE – 22 % for GONAL-f. The ongoing pregnancy rate observed with GONAL-f (22%) is surprisingly low compared to other published studies, which have shown pregnancy rates generally above 30%. (See back-up information for Literature Review.) 225 IU IS OVERDOSING. The GONAL-f Package Insert (USA) refers to an initial dosing of 150 IU per day. Only in patients 35 years old or in patients with deeply suppressed endogenous gonadotrophins should GONAL-f be initiated at a dose of 225 IU per day. This also reflects current clinical practice. (See back-up information: Published studies with different starting doses for GONAL-f.) THE PERCENTAGE OF TOP QUALITY EMBRYOS PER OOCYTE RETRIEVED was 11.3% in the Menopur group and 9.0% in the GONAL-f group (p<0.05). It has been shown that – especially in young patients overdosing may lead to low-quality embryos. A difference of 2.3% can not be considered as statistically significant (p<0.05) with an insufficient sample size. RECOMBINANT VERSUS URINARIES. Why did Ferring announce investment in recombinant gonadotrophin research if they believe that urinaries are better Ferring Forum, Hamburg, Germany, Other important considerations. The authors mentioned that the study was stratified by age; however, nothing is said about how this stratification factor was used in the analysis, or about the results obtained in the different age strata. The study reports a higher, though not statistically different rate in early pregnancy loss for the r-hFSH-treated group (32% in the GONAL-f group versus 24% in the Menopur group). Literature data report on a lower abortion rate for r-hFSH or similar/comparable early pregnancy loss for the two compounds (Franco 2000). Safety data associated with both treatments is missing from the abstract. Literature data report on a slightly lower occurrence of OHSS with r-hFSH compared to hMG (Aboulghar 1998, Eur-Israeli Study). STATISTICS. The hypotheses presented in the protocol involve a 2-step procedure: step 1, test for superiority but, if superiority is not demonstrated, switch to step 2, test for non-inferiority. Step 1 (superiority objective) is not powered at all; the authors do not mention what difference they expected in order to establish the superiority of Menopur compared to GONAL-f. The minimum rule should be to define an expected difference between the 2 treatments, an alpha level for the statistical significance (generally set at 5%) and a power for this study. Neither are mentioned; therefore, it is impossible to estimate the number of patients, which would have been required to conclude on superiority. Step 2 (non-inferiority objective) is largely underpowered. In fact, the number of patients entered in this study (N = 731 overall) is far below the sample size required (N = 1042 patients) for a power of 80% (the minimum power required by regulatory agencies). Furthermore, the limit margins used for a hypothetical proof of non-inferiority (ranging from –6.5% to –7.8%) are largely outside the clinically relevant window (-3% to-4%). In other words, the rules they used for this study, they could conclude on a relative similarity of the 2 products even if the difference observed was as high as 8% !!, which is completely unrealistic. Overall pregnancy rate with GONAL-f is surprisingly low. Clinical pregnancy rates with the use of recombinant h-FSH compared to urinary FSH or u-hMG.")
29
Ongoing pregnancy was the primary end-point [HPhMG 27% and rFSH 22%; odds ratio (OR) (95% confidence interval, CI) 1.25 ( )]. The live birth,ongoing pregnancy and ongoing implantation rates for top-quality embryos were higher with HP-hMG than rFSH [48 versus 32% (P ), 48 versus 32% (P ), 41 versus 27% (P )]. the proportion of embryos with at least 50% surviving blastomeres after cryopreservation and embryos resuming mitosis were more frequent with HP-hMG compared with rFSH.
![Ongoing pregnancy was the primary end-point [HPhMG 27% and rFSH 22%; odds ratio (OR) (95% confidence interval, CI) 1.25 ( )].](http://slideplayer.biz.tr/slide/2805638/10/images/29/Ongoing+pregnancy+was+the+primary+end-point+%5BHPhMG+27%25+and+rFSH+22%25%3B+odds+ratio+%28OR%29+%2895%25+confidence+interval%2C+CI%29+1.25+%28+%29%5D..jpg "The live birth,ongoing pregnancy and ongoing implantation rates for top-quality embryos were higher with HP-hMG than rFSH [48 versus 32% (P ), 48 versus 32% (P ), 41 versus 27% (P )]. the proportion of embryos with at least 50% surviving blastomeres after cryopreservation and embryos resuming mitosis were more frequent with HP-hMG compared with rFSH.")
30
Serum Follicular fluid
BACKGROUND: Highly purified menotrophin (HP-hMG) has been associated with fewer oocytes retrieved and a higher proportion of top-quality embryos compared with recombinant FSH (rFSH). METHODS: A randomized, assessor-blind, multinational trial in 731 women undergoing IVF after stimulation with HP-hMG (MENOPUR) (n = 363) or rFSH (GONAL-F) (n = 368) following a long GnRH agonist protocol was conducted. Blood was collected before, during and after stimulation. Fluid was collected from follicles > or =17 mm. RESULTS: Serum androstenedione, total testosterone and free androgen index (FAI) were higher (P < 0.001) with HP-hMG than with rFSH after starting stimulation. At the end of stimulation, serum estradiol was higher (P = 0.031) with HP-hMG, whereas progesterone was higher (P < 0.001) with rFSH, even after adjusting for ovarian response. Serum LH was not different between treatments. Mean mid- and end-follicular hCG levels in the HP-hMG group were 2.5 and 2.9 IU/l, respectively. Follicular fluid levels of FSH, LH, hCG, androstenedione, testosterone, FAI and estradiol and ratios of estradiol:androstenedione, estradiol:total testosterone and estradiol:progesterone were higher (P < 0.001) with HP-hMG, whereas progesterone was higher (P < 0.001) with rFSH. CONCLUSION: Major differences in serum and follicular fluid endocrine profile exist after stimulation with HP-hMG or rFSH. Exogenous LH activity induces a differential endocrine environment influencing oocyte quantity and quality, which may be of relevance for clinical outcome.
 has been associated with fewer oocytes retrieved and a higher proportion of top-quality embryos compared with recombinant FSH (rFSH). METHODS: A randomized, assessor-blind, multinational trial in 731 women undergoing IVF after stimulation with HP-hMG (MENOPUR) (n = 363) or rFSH (GONAL-F) (n = 368) following a long GnRH agonist protocol was conducted. Blood was collected before, during and after stimulation. Fluid was collected from follicles > or =17 mm. RESULTS: Serum androstenedione, total testosterone and free androgen index (FAI) were higher (P < 0.001) with HP-hMG than with rFSH after starting stimulation. At the end of stimulation, serum estradiol was higher (P = 0.031) with HP-hMG, whereas progesterone was higher (P < 0.001) with rFSH, even after adjusting for ovarian response. Serum LH was not different between treatments. Mean mid- and end-follicular hCG levels in the HP-hMG group were 2.5 and 2.9 IU/l, respectively. Follicular fluid levels of FSH, LH, hCG, androstenedione, testosterone, FAI and estradiol and ratios of estradiol:androstenedione, estradiol:total testosterone and estradiol:progesterone were higher (P < 0.001) with HP-hMG, whereas progesterone was higher (P < 0.001) with rFSH. CONCLUSION: Major differences in serum and follicular fluid endocrine profile exist after stimulation with HP-hMG or rFSH. Exogenous LH activity induces a differential endocrine environment influencing oocyte quantity and quality, which may be of relevance for clinical outcome.")
31
P-value <0.001 HP-hMG preparation has a longer half-life
It was interesting to observe that progesterone was more elevated with rFSH-alone treatment. presence of LH activity in gonadotrophin preparations has a differential effect on the antral follicle selection process. P-value <0.001

32
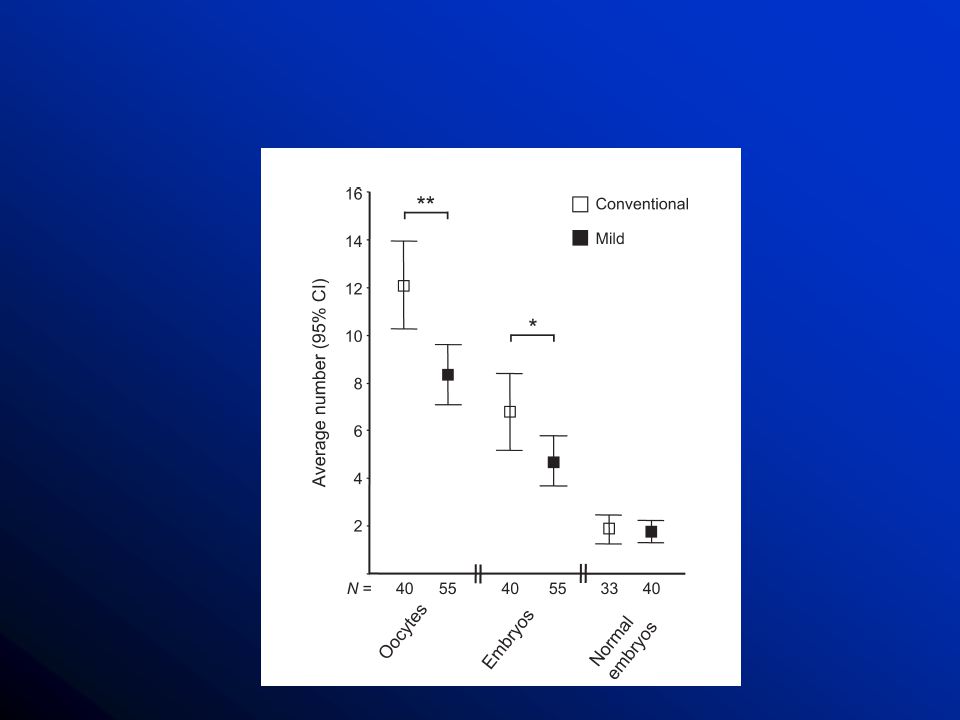
Mild vs harsh stimulasyon?

35
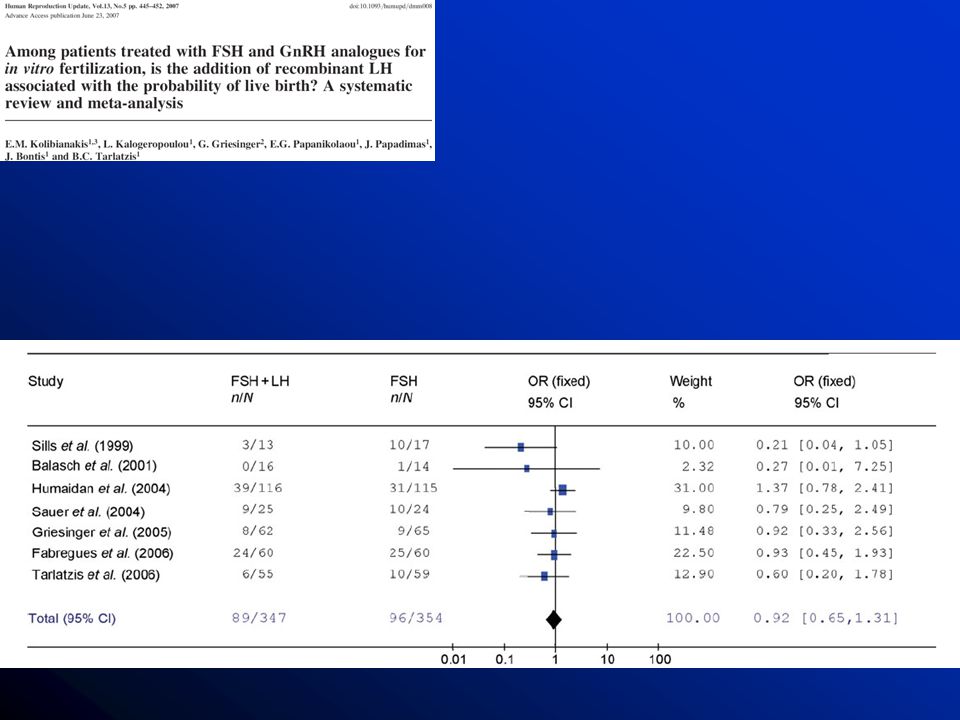
LH eklenmesi?

37
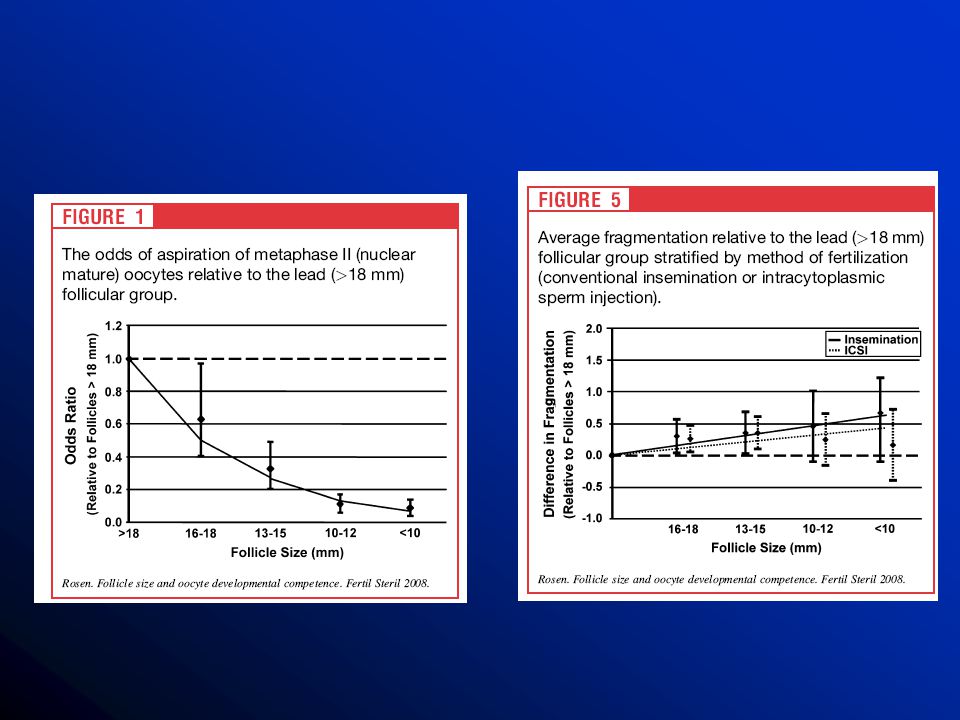
Follikül çapları?

38
F&S 2008

40
F&S 2006 3-4 hrs

41
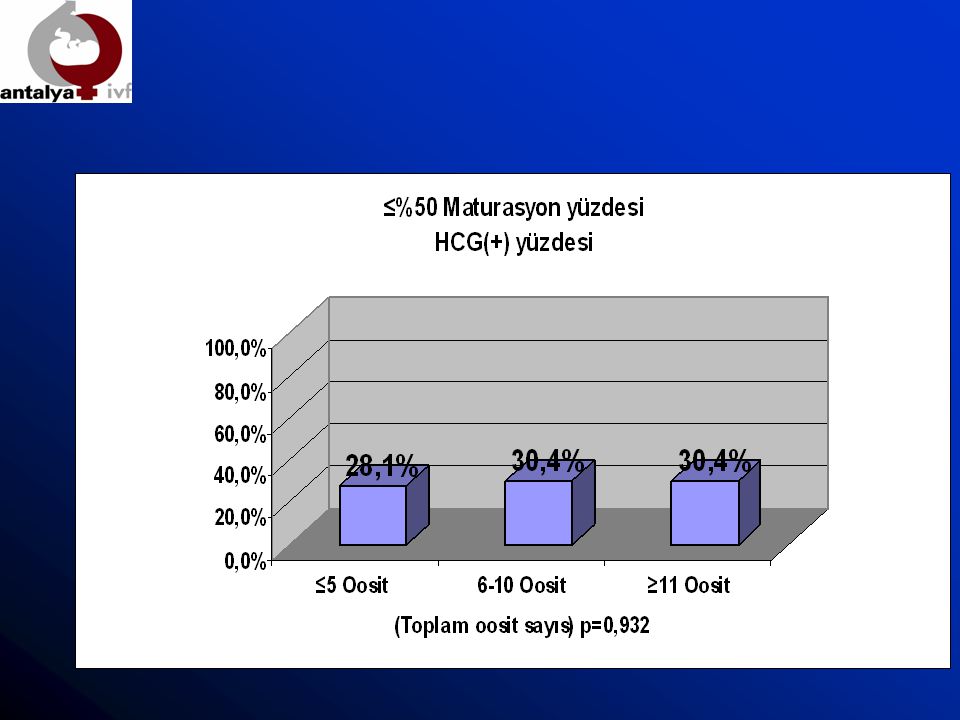
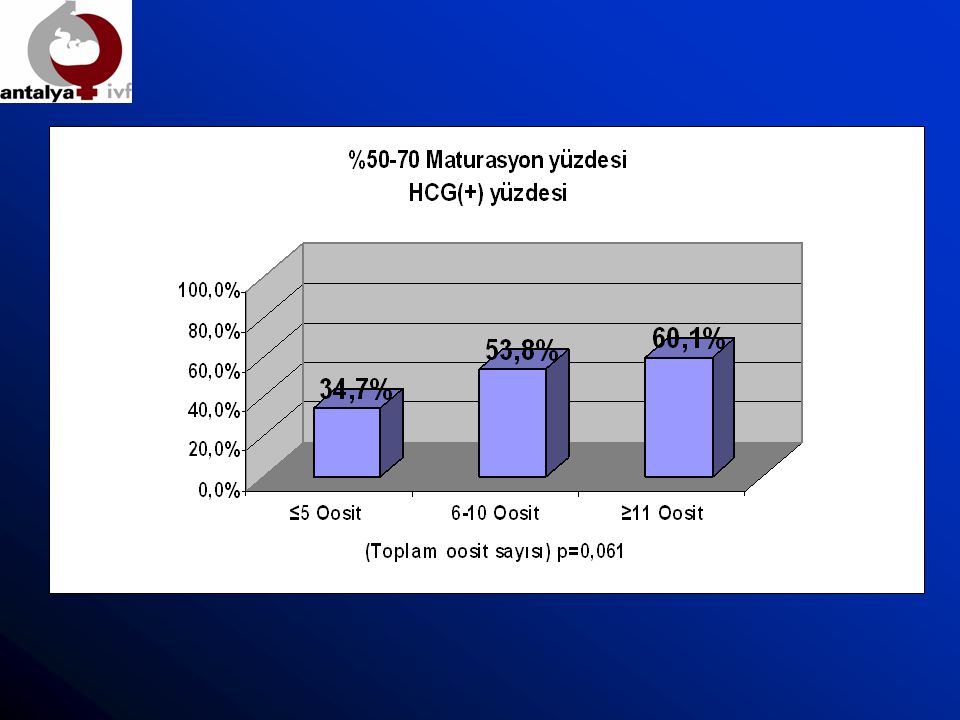
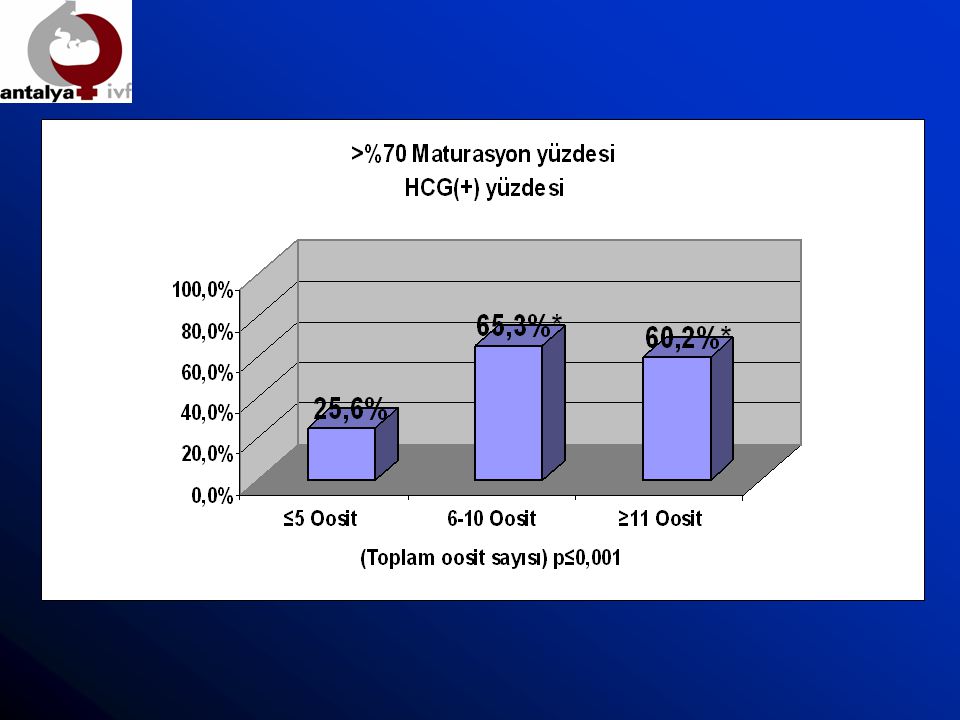
Oosit maturasyonun katkısı?

42
Antalya IVF 740 ICSI-ET yapılan sikluslar ele alındı
Pick-up sonrası denudasyon ve M2, M1, ICSI Day 2 transferi M2 oosit/toplam oosit oranına göre gruplar değerlendirildi

46
Coasting katkısı

47
F&S 2006

48
Sonuçlar Embriyo kalitesini tanımlayan morfolojik özellikler başarıyı etkilemektedir. Agonist - antagonist siklusları – recLH eklenmesi arasında başarıyı etkileyen farklılıklar bulunmamaktadır Coasting süresi uzadıkça outcome olumsuz etkilenmektedir. Mild stimulation ile daha az oosit üretilmektedir. HMG ve FSH sikluslarında farklılık olabileceğini gösteren çalışmanın tek olması sonucu netleştirememektedir. Follikül çapları optimum düzeylerde daha olgun ve muhtemel daha kaliteli embriyo üretmektedir. Oosit olgunlaşma oranı stimulasyon kalitesini yansıtan anlamlı bir parametre olup ilerleyen çalışmalara ihtiyaç vardır.

Benzer bir sunumlar




>")















