Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Sedatif Hipnotik İlaçlar
Benzodiazepinler Buspiron Zopiklon Zolpidem Barbitüratlar Diğer Hipnotikler

2
GABAA Reseptörü Çeşitli alt birimlerin birleşmesinden oluşan pentamerik (veya tetramerik) yapıda iyonotropik bir reseptördür. Farklı alt birimlerin birleşmesi ile çok sayıda GABAA reseptör alt tipi oluşabilir. Alt birimler a1-6 b1-3 g1-3 d r1-2 g-Aminobutyric acid (GABA) is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. Katzung 11th ed. A major isoform of the GABAA receptor that is found in many regions of the brain consists of two a1 and two b2 subunits and one g2 subunit. In this isoform, the binding sites for GABA are located between adjacent a1 and b2 subunits, and the binding pocket for benzodiazepines (the BZ site of the GABAA receptor) is between an a1 and the g2 subunit. However, GABAA receptors in different areas of the central nervous system consist of various combinations of the essential subunits, and the benzodiazepines bind to many of these, including receptor isoforms containing a2, a3, and a5 subunits. Barbiturates also bind to multiple isoforms of the GABAA receptor but at different sites from those with which benzodiazepines interact. In contrast to benzodiazepines, zolpidem, zaleplon, and eszopiclone bind more selectively because these drugs interact only with GABAA-receptor isoforms that contain a1 subunits. The heterogeneity of GABAA receptors may constitute the molecular basis for the varied pharmacologic actions of benzodiazepines and related drugs (see Box: GABA Receptor Heterogeneity & Pharmacologic Selectivity).
 is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. Katzung 11th ed. A major isoform of the GABAA receptor that is found in many regions of the brain consists of two a1 and two b2 subunits and one g2 subunit. In this isoform, the binding sites for GABA are located between adjacent a1 and b2 subunits, and the binding pocket for benzodiazepines (the BZ site of the GABAA receptor) is between an a1 and the g2 subunit. However, GABAA receptors in different areas of the central nervous system consist of various combinations of the essential subunits, and the benzodiazepines bind to many of these, including receptor isoforms containing a2, a3, and a5 subunits. Barbiturates also bind to multiple isoforms of the GABAA receptor but at different sites from those with which benzodiazepines interact. In contrast to benzodiazepines, zolpidem, zaleplon, and eszopiclone bind more selectively because these drugs interact only with GABAA-receptor isoforms that contain a1 subunits. The heterogeneity of GABAA receptors may constitute the molecular basis for the varied pharmacologic actions of benzodiazepines and related drugs (see Box: GABA Receptor Heterogeneity & Pharmacologic Selectivity).")
3
GABAA Reseptörü Beynin bir çok bölgesinde bulunan ana GABAA reseptör izoformu iki a1 iki b2 ve bir g2 alt birimi içerir. Bu izoformda GABA bağlanma yerleri komşu a1 ve b2 altbirimler arasında , benzodiazepin bağlanma cebi ise a1 ve g2 altbirimler arasındadır. Beynin farklı bölgelerindeki GABAA reseptörleri temel altbirimlerin çeşitli kombinasyonlarından ibaret olduğu oluşmaktadır. g-Aminobutyric acid (GABA) is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. Katzung 11th ed. A major isoform of the GABAA receptor that is found in many regions of the brain consists of two a1 and two b2 subunits and one g2 subunit. In this isoform, the binding sites for GABA are located between adjacent a1 and b2 subunits, and the binding pocket for benzodiazepines (the BZ site of the GABAA receptor) is between an a1 and the g2 subunit. However, GABAA receptors in different areas of the central nervous system consist of various combinations of the essential subunits, and the benzodiazepines bind to many of these, including receptor isoforms containing a2, a3, and a5 subunits. Barbiturates also bind to multiple isoforms of the GABAA receptor but at different sites from those with which benzodiazepines interact. In contrast to benzodiazepines, zolpidem, zaleplon, and eszopiclone bind more selectively because these drugs interact only with GABAA-receptor isoforms that contain a1 subunits. The heterogeneity of GABAA receptors may constitute the molecular basis for the varied pharmacologic actions of benzodiazepines and related drugs (see Box: GABA Receptor Heterogeneity & Pharmacologic Selectivity). Studies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.
 is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. Katzung 11th ed. A major isoform of the GABAA receptor that is found in many regions of the brain consists of two a1 and two b2 subunits and one g2 subunit. In this isoform, the binding sites for GABA are located between adjacent a1 and b2 subunits, and the binding pocket for benzodiazepines (the BZ site of the GABAA receptor) is between an a1 and the g2 subunit. However, GABAA receptors in different areas of the central nervous system consist of various combinations of the essential subunits, and the benzodiazepines bind to many of these, including receptor isoforms containing a2, a3, and a5 subunits. Barbiturates also bind to multiple isoforms of the GABAA receptor but at different sites from those with which benzodiazepines interact. In contrast to benzodiazepines, zolpidem, zaleplon, and eszopiclone bind more selectively because these drugs interact only with GABAA-receptor isoforms that contain a1 subunits. The heterogeneity of GABAA receptors may constitute the molecular basis for the varied pharmacologic actions of benzodiazepines and related drugs (see Box: GABA Receptor Heterogeneity & Pharmacologic Selectivity). Studies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.")
4
GABAA Reseptörü Benzodiazepinler, yalnızca N-ucunda histidin kalıntısı içeren a altbirimleri (1, 2, 3 ve 5) olan GABAA reseptörleri ile etkileşmektedirler. a alt biriminin ucundaki histidin yerine arginin sokulmuş mutant fareler, benzodiazepinlerin sedatif ve amnezik etkilerine karşı direnç gösterirler; ancak, anksiyolitik ve kas gevşetici etkiler fazla etkilenmez. Bu hayvanlar GABAA reseptörlerindeki a1 altbirimlere spesifik olarak bağlanan zolpidem ve zaleplonun hipnotik etkilerine karşı da direnç gösterirler. Bu tip çalışmalara dayanarak GABAA reseptörlerindeki a1 altbirimlerin, benzodiazepinlerin sedasyon, amnezi ve muhtemelen antiepileptik etkilerine aracılık ettiği; buna karşılık a1 altbirimlerin anksiyolitk ve kas-gevşetici etkilerine aracılık ettiği öne sürülmüştür. Diğer mutasyon çalışmalarına dayanak a5 altbirimin benzodiazepinlerin bellek bozucu etkilerinde rol oynadığı iddia edilmiştir.
 olan GABAA reseptörleri ile etkileşmektedirler. a alt biriminin ucundaki histidin yerine arginin sokulmuş mutant fareler, benzodiazepinlerin sedatif ve amnezik etkilerine karşı direnç gösterirler; ancak, anksiyolitik ve kas gevşetici etkiler fazla etkilenmez. Bu hayvanlar GABAA reseptörlerindeki a1 altbirimlere spesifik olarak bağlanan zolpidem ve zaleplonun hipnotik etkilerine karşı da direnç gösterirler. Bu tip çalışmalara dayanarak GABAA reseptörlerindeki a1 altbirimlerin, benzodiazepinlerin sedasyon, amnezi ve muhtemelen antiepileptik etkilerine aracılık ettiği; buna karşılık a1 altbirimlerin anksiyolitk ve kas-gevşetici etkilerine aracılık ettiği öne sürülmüştür. Diğer mutasyon çalışmalarına dayanak a5 altbirimin benzodiazepinlerin bellek bozucu etkilerinde rol oynadığı iddia edilmiştir.")
5
FIGURE 1 Schematic of GABAA Receptors. The protein is shown as
a pseudo-symmetric membrane-spanning ion channel protein made of five homologous subunits, each of which has four membrane-spanning regions as shown in the pull-out subunit. The view from outside the cell (plan view) shows the arrangement around the central core, the chloride ion channel. Also indicated are the subunit families that can be utilized in composing each receptor, and the ligand-binding sites present on the receptor. The neurosteroids are hormone metabolites that have rapid and direct effects on neurons, such as modulation of GABAR. Metabolites of the female sex hormone progesterone (allopregnanolone), corticosteroids (tetrahydrocorticosterone), and possibly androgens, enhance GABAR currents and appear to reach effective concentrations during certain physiological and pathological conditions. This field of research is just in its infancy.
 shows the arrangement around the central core, the. chloride ion channel. Also indicated are the subunit families that can be. utilized in composing each receptor, and the ligand-binding sites. present on the receptor. The neurosteroids are hormone metabolites that have. rapid and direct effects on neurons, such as modulation. of GABAR. Metabolites of the female sex hormone. progesterone (allopregnanolone), corticosteroids (tetrahydrocorticosterone), and possibly androgens, enhance. GABAR currents and appear to reach effective concentrations. during certain physiological and pathological. conditions. This field of research is just in its infancy.")
7
Inhibitory synapses employing GABA as their transmitter can exhibit three types of postsynaptic receptors, called GABAA, GABAB, and GABAC. GABAA and GABAC receptors are ionotropic receptors, while GABAB receptors are metabotropic. GABA-C receptors have only recently been identified and their function is still uncertain. There is evidence that, besides GABA, the GABA receptor agonists muscimol and isogucacine have a high affinity for these receptors. A high density of GABA-C receptors has been detected in the retina where they appear to be involved in the development of retinal rod cells. In the brain, there is evidence that GABA-C receptors are concentrated in the superior colliculus where they have a disinhibitory role. There is also evidence that they play an important role in some aspects of neuroendocrine regulation both in the gastrointestinal tract and in the secretion of thyroid stimulating hormone.

8
Figure 2.12. Diagrammatic representation of the GABA-benzodiazepine supramolecular
complex. Compounds that increase inhibitory transmission may do so either by directly activating the GABA receptor site (e.g. muscimol) or by acting directly on the chloride ionophore (e.g. barbiturates). Benzodiazepines (e.g. diazepam) enhance the sensitivity of the GABA-A receptor to GABA. Compounds that decrease inhibitory transmission may do so by activating the picrotoxin site, which closes the chloride ionophore, or by blocking the GABA-A receptor.
 or by acting. directly on the chloride ionophore (e.g. barbiturates). Benzodiazepines (e.g. diazepam) enhance the sensitivity of the GABA-A receptor to GABA. Compounds. that decrease inhibitory transmission may do so by activating the picrotoxin site, which closes the chloride ionophore, or by blocking the GABA-A receptor.")
9
GABAA Reseptörü Kesiti
Fig. 2. Hypothetical model of the GABAA receptor with the agonist and modulatory sites at subunit interfaces. Five subunits are arranged around a central Cl– ion-selective pore, that opens as a consequence of agonist (GABA) binding. The numbers indicate amino acid residues of the corresponding mature rat subunit isoform. Amino acid residues of agonist and modulatory sites identical or directly homologous to each other are shown in the same colour. A, agonist (GABA) binding site; M, modulatory site for benzodiazepine-type ligands. As two subunits contribute to each, the agonist and to the modulatory binding site, they must be located at subunit interfaces. If the modulatory site is occupied, this fact is allosterically communicated to the agonist binding site whose function is altered as a consequence.
 binding. The numbers indicate amino acid residues of the corresponding mature rat subunit isoform. Amino acid residues of agonist and modulatory sites identical or directly homologous to each other are shown in the same colour. A, agonist (GABA) binding site; M, modulatory site for benzodiazepine-type ligands. As two subunits contribute to each, the agonist and to the modulatory binding site, they must be located at subunit interfaces. If the modulatory site is occupied, this fact is allosterically communicated to the agonist binding site whose function is altered as a consequence.")
10
GABAA Reseptör Kompleksi
GABA bağlanma yeri (+) Agonist: GABA, musimol Antagonist: bikukulin Barbitürat bağlanma yeri (+) Agonist: barbitüratlar Benzodiazepin bağlanma yeri (+) Agonist: benzodiazepinler Ters agonist: b-CCE, b-CCM Antagonist: flumazenil Benzodiazepin bağlanma yerinin en az 2 alt tipi olduğu saptanmıştır: BZ1 (w1) ve BZ2 (w2) Pikrotoksin bağlanma yeri (-) Agonist: pikrotoksinin, pentilentetrazol Alkol bağlanma yeri (+) Agonist: alkol g-Aminobutyric acid (GABA) is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. For this reason it is referred to as a GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. You should refer to pages 220 to 226 of the text for a discussion of the GABAergic synapse as the primary site of action of benzodiazepines and also refer to pages 194 to 197 for a brief discussion of how some anticonvulsants work via activation of GABAergic receptors. Objectives A student should be able to: 1. Reproduce the biosynthetic and metabolic pathways of GABA. 2. Identify the step at which sodium valproate exerts its anticonvulsant response in the above pathways. 3. Reproduce the model of the GABAA Receptor-Benzodiazepine Receptor-Chloride Channel Complex and explain the effect on the receptor and the biological response of each type of drug or endogenous compound, which interacts with the receptor complex. 4. Explain the location and function of GABA’s presynaptic receptor. 5. Account for the mechanism of action of baclofen and its structural relationship to GABA and its structural differences from the more classical muscle relaxants. 6. Account for the mechanism of action of irreversible GABA transaminase (GABA-T) inhibitors. 7. Identify the receptor bound conformation of GABA. 8. Explain why GABA must be present in order for barbiturates or benzodiazepines to exert their pharmacological activity.
 Agonist: GABA, musimol. Antagonist: bikukulin. Barbitürat bağlanma yeri (+) Agonist: barbitüratlar. Benzodiazepin bağlanma yeri (+) Agonist: benzodiazepinler. Ters agonist: b-CCE, b-CCM. Antagonist: flumazenil. Benzodiazepin bağlanma yerinin en az 2 alt tipi olduğu saptanmıştır: BZ1 (w1) ve BZ2 (w2) Pikrotoksin bağlanma yeri (-) Agonist: pikrotoksinin, pentilentetrazol. Alkol bağlanma yeri (+) Agonist: alkol. g-Aminobutyric acid (GABA) is perhaps the most comprehensively studied inhibitory neurotransmitter in the mammalian central nervous system (CNS). It has been estimated that about 40% of synapses in the brain are GABAergic. It is now well recognized that cellular excitability leading to convulsive seizures can be attenuated by GABAergic stimulation in the CNS. Current evidence also indicates that most anxiolytics and hypnotic-sedative drugs such as benzodiazepines and barbiturates exert their pharmacological actions via interactions with a discrete neuronal site on the GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. Unlike other neurotransmitter receptors such as DA and 5-HT discussed earlier, the model of the GABA receptor consists of a multiple receptor complex which provides binding sites for a variety of drugs and/or endogenous biologically active compounds. Stimulation of these binding sites contributes to the responses related to the GABAergic system itself. For this reason it is referred to as a GABAA Receptor-Benzodiazepine Receptor-Chloride Ion Channel Complex. You should refer to pages 220 to 226 of the text for a discussion of the GABAergic synapse as the primary site of action of benzodiazepines and also refer to pages 194 to 197 for a brief discussion of how some anticonvulsants work via activation of GABAergic receptors. Objectives. A student should be able to: 1. Reproduce the biosynthetic and metabolic pathways of GABA. 2. Identify the step at which sodium valproate exerts its anticonvulsant response in the above pathways. 3. Reproduce the model of the GABAA Receptor-Benzodiazepine Receptor-Chloride Channel Complex and explain the effect on the receptor and the biological response of each type of drug or endogenous compound, which interacts with the receptor complex. 4. Explain the location and function of GABA’s presynaptic receptor. 5. Account for the mechanism of action of baclofen and its structural relationship to GABA and its structural differences from the more classical muscle relaxants. 6. Account for the mechanism of action of irreversible GABA transaminase (GABA-T) inhibitors. 7. Identify the receptor bound conformation of GABA. 8. Explain why GABA must be present in order for barbiturates or benzodiazepines to exert their pharmacological activity.")
11
The inhibitory effect of GABA is mediated by the chloride ion channel
(Figure 2.12). When the GABA-A receptor is activated by GABA or a specific agonist such as muscimol, the frequency of opening of the channel is increased and the cell is hyperpolarized. Barbiturates, such as phenobarbitone, and possibly alcohol, also facilitate the chloride ion influx, but these drugs increase the duration, rather than the frequency, of the channel opening. Recently, novel benzodiazepine receptor ligands have been produced which, like the typical benzodiazepines, increase the frequency of chloride channel opening. The cyclopyrrolone sedative/ hypnotic zopiclone is an example of such a ligand. Some glucocorticoids are also known to have sedative effects which may be ascribed to their ability to activate specific steroid receptor facilitatory sites on the GABA-A receptor.
. When the GABA-A receptor is activated by GABA or a. specific agonist such as muscimol, the frequency of opening of the channel. is increased and the cell is hyperpolarized. Barbiturates, such as. phenobarbitone, and possibly alcohol, also facilitate the chloride ion influx, but these drugs increase the duration, rather than the frequency, of the. channel opening. Recently, novel benzodiazepine receptor ligands have. been produced which, like the typical benzodiazepines, increase the. frequency of chloride channel opening. The cyclopyrrolone sedative/ hypnotic zopiclone is an example of such a ligand. Some glucocorticoids are. also known to have sedative effects which may be ascribed to their ability to. activate specific steroid receptor facilitatory sites on the GABA-A receptor.")
12
GABAA Reseptörü Üzerinde GABA-Barbitürat-Benzodiazepin Etkileşmesi
Kanalı açar. BZ’lere afiniteyi artırır. Barbitüratlara afiniteyi artırır. Barbitürat Düşük konsantrasyonlarda kanalı açamaz, yüksek konsantrasyonlarda açar. BZ’lere afiniteyi artırır. GABA’ya afiniteyi artırır. Kanalın açık kalma süresini uzatır, açılma frekansını değiştirmez. GABA’nın doz yanıt eğrisini (benzodiazepinden daha fazla) sola kaydırır; Emax’ını artırır. Benzodiazepin Yüksek konsantrasyonlarda bile kanalı açamaz. GABA’ya afiniteyi artırır. Kanalın açılma frekansını artırır, açık kalma süresini değiştirmez. GABA’nın doz yanıt eğrisini sola kaydırır; ancak Emax’ını artırmaz.
 sola kaydırır; Emax’ını artırır. Benzodiazepin. Yüksek konsantrasyonlarda bile kanalı açamaz. GABA’ya afiniteyi artırır. Kanalın açılma frekansını artırır, açık kalma süresini değiştirmez. GABA’nın doz yanıt eğrisini sola kaydırır; ancak Emax’ını artırmaz.")
15
Types of benzodiazepine receptors
Two types of receptor have been identified, termed Bz1 and Bz2. These receptors occupy different sub-units of the GABA-A receptor and therefore have different affinities for the benzodiazepine ligands. For example, the potent hypnotic zolpidem binds to the Bz1 receptor that is linked to the alpha-1 site on the GABA-A receptor while the hypnotic zopiclone binds to the Bz2 receptor which occupies both the alpha-2 and 3 sites on the GABA receptor. This selectivity for the Bz1 receptor may account for the fewer side effects of zolpiden in comparison to other hypnotic benzodiazepines. The third type of benzodiazepine receptor is the so-called peripheral benzodiazepine receptor (pBz). This was first discovered in the rat adrenal gland, hence the term ‘‘peripheral’’. However, it is now known to occur on the platelet membrane, on immune cells and also in the mammalian brain. The pBz receptor is distinct from the Bz1 and 2 receptors and does not activate GABA-A receptors. It is occupied by the isoquinoline PK and the benzodiazepine Ro 4864, neither of which has affinity for the brain Bz1 or 2 receptors. In the brain the pBz receptor is associated with the outer membrane of the mitochondria and with the glia cells. The primary function of the pBz receptor is in the regulation of cholesterol uptake and the synthesis of neurosteroids. The latter compounds have an affinity for the GABA-A receptors which provide an indirect coupling between the pBz and the GABA receptors in the brain. Most of the benzodiazepines that are currently available are full agonists occupying the Bz1 and 2 receptors. However, several drugs have been developed which act as partial agonists (for example, bretazenil which is a non-sedative anxiolytic) and partial inverse agonists such as sarmazenil. The beta carboline abercarnil is in development as a partial agonist. Types of benzodiazepine receptors Two types of receptor have been identified, termed Bz1 and Bz2. These receptors occupy different sub-units of the GABA-A receptor and therefore have different affinities for the benzodiazepine ligands. For example, the potent hypnotic zolpidem binds to the Bz1 receptor that is linked to the alpha-1 site on the GABA-A receptor while the hypnotic zopiclone binds to the Bz2 receptor which occupies both the alpha-2 and 3 sites on the GABA receptor. This selectivity for the Bz1 receptor may account for the fewer side effects of zolpiden in comparison to other hypnotic benzodiazepines. GABA RECEPTOR HETEROGENEITY & PHARMACOLOGIC SELECTIVITYStudies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.
. This was first discovered in the rat adrenal gland, hence the term ‘‘peripheral’’. However, it is now known to occur on the platelet membrane, on immune cells and also in the mammalian brain. The pBz receptor is distinct from the Bz1 and 2 receptors and does not activate GABA-A receptors. It is occupied by the isoquinoline PK and the benzodiazepine Ro 4864, neither of which has affinity for the brain Bz1 or 2 receptors. In the brain the pBz receptor is associated with the outer membrane of the mitochondria and with the glia cells. The primary function of the pBz receptor is in the regulation of cholesterol uptake and the synthesis of neurosteroids. The latter compounds have an affinity for the GABA-A receptors which provide an indirect coupling between the pBz and the GABA receptors in the brain. Most of the benzodiazepines that are currently available are full agonists occupying the Bz1 and 2 receptors. However, several drugs have been developed which act as partial agonists (for example, bretazenil which is a non-sedative anxiolytic) and partial inverse agonists such as sarmazenil. The beta carboline abercarnil is in development as a partial agonist. Types of benzodiazepine receptors. Two types of receptor have been identified, termed Bz1 and Bz2. These. receptors occupy different sub-units of the GABA-A receptor and therefore. have different affinities for the benzodiazepine ligands. For example, the. potent hypnotic zolpidem binds to the Bz1 receptor that is linked to the. alpha-1 site on the GABA-A receptor while the hypnotic zopiclone binds to. the Bz2 receptor which occupies both the alpha-2 and 3 sites on the GABA. receptor. This selectivity for the Bz1 receptor may account for the fewer side. effects of zolpiden in comparison to other hypnotic benzodiazepines. GABA RECEPTOR HETEROGENEITY & PHARMACOLOGIC SELECTIVITYStudies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.")
17
Benzodiazepinler İlk kez 1960’da pazarlanmışlardır.
Terapötik indeksi en yüksek hipnosedatif ilaçlardır. Karaciğer mikrozomal enzimlerini indüklemezler. Bağımlılık oluşturma potansiyelleri barbitüratlara göre daha düşüktür. Yeşil reçeteye yazılırlar. Diazepam

19
Uzun etki süreli Diazepam Ank., Ak. Prototip BZ'dir, en hızlı absorbe edilen BDZ Klordiazepoksid Ank. Prazepam Halazepam Klorazepat Ank. Hpn. Ön ilaçtır, nordazepam'a dönüşür. Anksiyeteli uykusuzlukta yararlı Klonazepam Ak. Antikonvülsan olarak kullanılır Flurazepam Hpn. Kronik kullanımda aktif metabolileri birikir Kuvazepam Orta etki süreli Lorazepam Amnezi yapıcı etkisi diğerlerinden daha fazladır, antipanik etkilidir Oksazepam Alprazolam Ank., Ad Antidepresan etkili BZ, antipanik etkilidir Flunitrazepam Hpn., Ans. Türkiye'deki suistimalinin fazlalığı nedeniyle diğer BDZ'ler gibi yeşil reçeteye değil, kırmızı reçeteye yazılması gerekir. Bir reçetede en fazla toplam 20 mg'lık dozda yazılır (ampul şekli için en fazla 10 mg toplam doz). Belirgin amnezi yapar. Nitrazepam Temazepam Estazolam Kısa etki süreli Midazolam Hpn., Ans Triazolam Hpn Belirgin amnezi yapar. Fiziksel bağımlılık yapma eğilimi yüksektir.
. Belirgin amnezi yapar. Nitrazepam. Temazepam. Estazolam. Kısa etki süreli. Midazolam. Hpn., Ans. Triazolam. Hpn. Belirgin amnezi yapar. Fiziksel bağımlılık yapma eğilimi yüksektir.")
20
Benzodiazepinlerin Etkileri
Normal dozlarda Anksiyolitik etki Sedatif etki Hipnotik etki Antikonvülsan etki Çizgili kas tonusu (rijidite varsa özellikle) Yüksek dozlarda Motor koordinasyonu bozarlar Anterograd belleği bozarlar Psikomotor reaksiyon hızını
 Yüksek dozlarda. Motor koordinasyonu bozarlar. Anterograd belleği bozarlar. Psikomotor reaksiyon hızını ")
21
Benzodiazepin Preparatları
Diazepam DİAZEM 2 mg, 5 mg ve 10 mg, 25 kapsül 10 mg, 10 ampul DİAPAM 10 mg/2ml, 10 ve 100 ampul LİZAN 2 mg ve 5 mg, 25 kapsül NERVİUM 5 mg, 50 tablet Klorazepat ANKSEN 5 mg ve 10 mg, 30 kapsül TRANXİLENE Klordiazepoksit LİBKOL 5 mg, 50 kapsül LİBRAX 5 mg, 40 ve 100 draje KLİPAKS Alprazolam XANAX 0,5 ve 1 mg, 30 tablet Lorazepam ATİVAN EXPİDET 1 ve 2.5 mg, 20 tablet

22
Benzodiazepinlerin Yan Etkileri
SSS depresyonu Anterograd amnezi Artık etki Rebound uykusuzluk Bağımlılık

23
Flumazenil Benzodiazepin antagonistidir
Hem benzodiazepinleri hem de ters agonistleri antagonize eder. Benzodiazepin aşırı dozajına bağlı belirtilerin giderilmesinde kullanılır. Benzodiazepin bağımlılarına verildiğinde yoksunluk sendromuna neden olur. ANEXATE 0,5 mg/5 ml, 5x5 ml ampul 1 mg/10 ml, 5x10 ml ampul

24
Atipik Benzodiazepin Reseptör Agonistleri
Zopiklon Zolpidem Zaleplon

25
Zopiklon GABAA reseptör kompleksini etkileyerek klorür kondüktansını artırır. (BZ1 selektif) Hipnotik olarak kullanılır. Anksiyolitik etkisi zayıftır; antikonvülsan ve santral kas gevşetici etkisi de vardır. Suistimal potansiyeli ve artık etkisinin BZ'lere göre daha az olması avantajlarıdır. Alkolle birlikte alınması SSS depresyonu yapıcı etkisini aşırı derecede artırır. Doz: mg En sık görülen yan etkisi ağızda acı bir tad (% 4) yapmasıdır. GABA RECEPTOR HETEROGENEITY & PHARMACOLOGIC SELECTIVITYStudies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs. IMOVANE 5 mg ve 7,5 mg, 5 ve 20 tablet
 yapmasıdır. GABA RECEPTOR HETEROGENEITY & PHARMACOLOGIC SELECTIVITYStudies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs. IMOVANE. 5 mg ve 7,5 mg, 5 ve 20 tablet.")
26
Zolpidem GABAA reseptör kompleksini etkileyerek klorür kondüktansını artırır. (BZ1 selektif) Hipnotik olarak kullanılır. Antikonvülsan ve santral kas gevşetici etkisi yoktur. Suistimal potansiyeli, belleği bozucu etki ve artık etkisinin BZ'lere göre daha az olması avantajlarıdır. Alkolle birlikte alınması SSS depresyonu yapıcı etkisini artırır. Doz: 10 mg yatarken (hipnotik olarak) Seyrek olarak diplopi ve mesane inkontinensi yapar. GABA RECEPTOR HETEROGENEITY & PHARMACOLOGIC SELECTIVITYStudies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.
 Seyrek olarak diplopi ve mesane inkontinensi yapar. GABA RECEPTOR HETEROGENEITY & PHARMACOLOGIC SELECTIVITYStudies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.")
27
Zaleplon GABAA reseptör kompleksini etkileyerek klorür kondüktansını artırır. (BZ1 selektif) Hipnotik olarak kullanılır. Antikonvülsan ve santral kas gevşetici etkisi yoktur. Suistimal potansiyeli, belleği bozucu etki ve artık etkisinin BZ'lere göre daha az olması avantajlarıdır. Alkolle birlikte alınması SSS depresyonu yapıcı etkisini artırır. GABA RECEPTOR HETEROGENEITY & PHARMACOLOGIC SELECTIVITYStudies involving genetically engineered mice have demonstrated that the specific pharmacologic actions elicited by benzodiazepines and other drugs that modulate GABA actions are influenced by the composition of the subunits assembled to form the GABAA receptor. Benzodiazepines interact only with brain GABAA receptors in which the a subunits (1,2,3, and 5) have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.
 have a conserved histidine residue in the N-terminal domain. Strains of mice, in which a point mutation has been inserted converting histidine to arginine in the a1 subunit, show resistance to both the sedative and amnestic effects of benzodiazepines, but anxiolytic and muscle-relaxing effects are largely unchanged. These animals are also unresponsive to the hypnotic actions of zolpidem and zaleplon, drugs that bind selectively to GABAA receptors containing a1 subunits. In contrast, mice with selective histidine-arginine mutations in the a2 subunit of GABAA receptors show selective resistance to the antianxiety effects of benzodiazepines. Based on studies of this type, it has been suggested that a1 subunits in GABAA receptors mediate sedation, amnesia, and possibly antiseizure effects of benzodiazepines, whereas a2 subunits are involved in their anxiolytic and muscle-relaxing actions. Other mutation studies have led to suggestions that an a5 subtype is involved in at least some of the memory impairment caused by benzodiazepines. It should be noted that these studies involving genetic manipulations of the GABAA receptor utilize rodent models of the anxiolytic and amnestic actions of drugs.")
28
Barbitüratlar Barbitürik asit türevidirler. Bağımlılık yaparlar.
Yeşil reçeteye yazılırlar. Karaciğer mikrozomal enzimlerini indüklerler. Fenobarbital

29
Barbitüratların Dozları
Doz (mg) Sedatif* Hipnotik Uzun etki süreli (> 6 saat) Fenobarbital 15-30 Barbital 65-130 Orta etki süreli (3 - 6 saat) Pentobarbital 15-40 60-125 Allobarbital 32-64 Amobarbital 20-60 Butalbital Siklobarbital 50-100 Butabarbital 10-60 Kısa etki süreli (< 3 saat) Sekobarbital - Heksobarbital Tetrabarbital Çok kısa etki süreli (birkaç dakika) Tiopental Tiamilal Metoheksital Barbitüratların Dozları * Bir kezlik dozu gösterir. Bu doz günde 3-4 kez verilir.
 Sedatif* Hipnotik. Uzun etki süreli (> 6 saat) Fenobarbital Barbital Orta etki süreli (3 - 6 saat) Pentobarbital Allobarbital Amobarbital Butalbital Siklobarbital Butabarbital Kısa etki süreli (< 3 saat) Sekobarbital. - Heksobarbital Tetrabarbital. Çok kısa etki süreli (birkaç dakika) Tiopental. Tiamilal. Metoheksital. Barbitüratların Dozları. * Bir kezlik dozu gösterir. Bu doz günde 3-4 kez verilir.")
30
Barbitüratların Etkileri
Sedatif ve hipnotik etki Antikonvülsan etki Bu etki sedatif etki ile ilişkili değildir; sedatif etkiye tolerans oluştuğunda antiepileptik etkide azalma olmaz. Anestezi Barbitüratların analjezik etkisi yoktur. Solunum merkezinin depresyonu Kardiyovasküler etkiler Karaciğer mikrozomal enzimlerinin indüksiyonu CYP2A, CYP2B ve CYP2C, CYP3A4 glukuronil transferaz Diğer etkiler d-aminolevülinik asit (d-ALA) sentetaz indüksiyonu Safra oluşumu ve safra akımında artış (sadece fenobarbital) Tolerans gelişmesi ve bağımlılık Çapraz tolerans diğer hipnosedatiflere karşı etil alkole karşı genel anesteziklere karşı Sedatif ve hipnotik etki: Oluşturdukları uyku doğal uykuya çok benzer; fakat REM döneminin süresi kısalmıştır. Kişi barbitüratların oluşturduğu uykudan kolaylıkla uyandırılabilir. Barbitürat alıp uyuyan kimse sabah kalktığında normal uykudan kalkan kişi kadar zinde değildir. Bu ilaçlar uykudan sonra en az birkaç saat devam eden bir uyuşukluk haline neden olurlar (artık etki). Uzun ve orta etki süreli barbitüratlarda artık etki daha belirgindir. Antikonvülsan etki: SSS'de depresyon yapan diğer ilaçlar gibi barbitüratlar da bilinci ileri derecede bozan dozlarda verildiklerinde, antikonvülsan etki oluştururlar. Fenobarbital ve vücutta buna dönüşen mefobarbital belirgin sedasyon yapmayan dozlarda antiepileptik etki gösterirler. Bu etki sedatif etki ile ilişkili değildir; sedatif etkiye tolerans oluştuğunda antiepileptik etkide azalma olmaz. Anestezi: Bu etki yüksek dozlarda tüm barbitüratlarla oluşturulabilir; ancak bu amaçla sadece çok kısa etki süreli olanlar kullanılmaktadır. Barbitüratların analjezik etkisi yoktur. Solunum merkezinin depresyonu: Solunum merkezinin otomatizmasını sağlayan pontobulber retiküler formasyondaki nöron grupları barbitüratlar arafından inhibe edilir. Barbitüratlar kan CO2 ve pH'ının uyarıcı etkisine karşı solunum merkezini baskılar.; solunumu sürdüren uyarı hipoksiye bağlı olarak kemoreseptörlerden gelen uyarılar ile sağlanır (barbitürat intoksikasyonunda bu nedenle hipoksi tedavisi yapılmaz). Barbitüratlar sedatif ve hipnotik dozlarda öksürük merkezini inhibe etmezler. EEG üzerine etki: Düşük dozda İ.V. verildiklerinde EEG'de paradoksik aktivasyona neden olurlar (düşük amplitüdlü, yüksek frekanslı dalgalar). Daha yüksek dozlarda NREM döneminde görülen dalgalara benzeyen yüksek amplitüdlü yavaş (5-12 Hz) dalgalar ortaya çıkar. Kardiyovasküler etkiler: Sedatif ve hipnotik dozlarda KVS'yi pek etkilemezler. Genel anestezi yapan dozlarda kan basıncında belirgin düşme yaparlar. bunun nedenleri: 1. bulbustaki vazomotor merkezin depresyonu 2. Miyokard depresyonu 3. Damar düz kaslarının direkt olarak gevşetilmesi ve histamin salıverilmesine bağlı vazodilatasyon Düz kaslı organlar üzerine etki: Devamlı barbitürat kullananlarda kabızlık gelişebilir. Hipnotik dozda uterusu etkilemez; ancak, genel anestezi yapan dozlarda i.v. verildiğinde kontraksiyon gücü ve sıklığını azaltırlar. Doğum eylemi sırasında verilen barbitüratların en önemli yan tesiri yenidoğanda solunumu deprese etmesidir. Karaciğer mikrozomal enzimlerinin indüksiyonu: Barbitüratlar (özellikle fenobarbital) CYP2A, CYP2B ve CYP2C alt-familyasındaki enzimleri indüklerler. Fenobarbital karaciğerde glukuronil transferaz enzimini indükleyerek bilirubinin konjügasyonunu ve atılımını artırır, ayrıca bilirubin bağlayan Y proteini düzeyini yükseltir. Bu etkilerinden dolayı yenidoğanlarda hiperbilirubinemi ve kernikterus'a karşı kullanılabilir. Diğer etkileri: Barbitüratlar mitokondriyel bir enzim olan d-aminolevülinik asit (d-ALA) sentetaz enzimini indüklerler. Fenobarbital karaciğerde safra oluşumunu ve safra akımını artırır (kolerezis). Diğer barbitüratlar bu özelliği göstermezler. Tolerans gelişmesi ve bağımlılık: Tolerans hem farmakokinetik, hem de ilaca karşı duyarlılık azalmasına (reseptör desensitizasyonu ve/veya down-regulation) bağlıdır. Çapraz tolerans diğer hipnosedatiflere karşı etil alkole karşı genel anesteziklere karşı Barbitüratlar pozitif pekiştiri yapıcı maddelerdir. Bu nedenle suistimal edilirler. En fazla suistimal edilenler kısa etki süreli sekobarbital ve pentobarbitaldir. Kısa ve orta etki süreli olanların suistimal edilme ve bağımlılık yapma potansiyelleri uzun etki sürelilerden daha fazladır.
 sentetaz indüksiyonu. Safra oluşumu ve safra akımında artış (sadece fenobarbital) Tolerans gelişmesi ve bağımlılık. Çapraz tolerans. diğer hipnosedatiflere karşı. etil alkole karşı. genel anesteziklere karşı. Sedatif ve hipnotik etki: Oluşturdukları uyku doğal uykuya çok benzer; fakat REM döneminin süresi kısalmıştır. Kişi barbitüratların oluşturduğu uykudan kolaylıkla uyandırılabilir. Barbitürat alıp uyuyan kimse sabah kalktığında normal uykudan kalkan kişi kadar zinde değildir. Bu ilaçlar uykudan sonra en az birkaç saat devam eden bir uyuşukluk haline neden olurlar (artık etki). Uzun ve orta etki süreli barbitüratlarda artık etki daha belirgindir. Antikonvülsan etki: SSS de depresyon yapan diğer ilaçlar gibi barbitüratlar da bilinci ileri derecede bozan dozlarda verildiklerinde, antikonvülsan etki oluştururlar. Fenobarbital ve vücutta buna dönüşen mefobarbital belirgin sedasyon yapmayan dozlarda antiepileptik etki gösterirler. Bu etki sedatif etki ile ilişkili değildir; sedatif etkiye tolerans oluştuğunda antiepileptik etkide azalma olmaz. Anestezi: Bu etki yüksek dozlarda tüm barbitüratlarla oluşturulabilir; ancak bu amaçla sadece çok kısa etki süreli olanlar kullanılmaktadır. Barbitüratların analjezik etkisi yoktur. Solunum merkezinin depresyonu: Solunum merkezinin otomatizmasını sağlayan pontobulber retiküler formasyondaki nöron grupları barbitüratlar arafından inhibe edilir. Barbitüratlar kan CO2 ve pH ının uyarıcı etkisine karşı solunum merkezini baskılar.; solunumu sürdüren uyarı hipoksiye bağlı olarak kemoreseptörlerden gelen uyarılar ile sağlanır (barbitürat intoksikasyonunda bu nedenle hipoksi tedavisi yapılmaz). Barbitüratlar sedatif ve hipnotik dozlarda öksürük merkezini inhibe etmezler. EEG üzerine etki: Düşük dozda İ.V. verildiklerinde EEG de paradoksik aktivasyona neden olurlar (düşük amplitüdlü, yüksek frekanslı dalgalar). Daha yüksek dozlarda NREM döneminde görülen dalgalara benzeyen yüksek amplitüdlü yavaş (5-12 Hz) dalgalar ortaya çıkar. Kardiyovasküler etkiler: Sedatif ve hipnotik dozlarda KVS yi pek etkilemezler. Genel anestezi yapan dozlarda kan basıncında belirgin düşme yaparlar. bunun nedenleri: 1. bulbustaki vazomotor merkezin depresyonu 2. Miyokard depresyonu 3. Damar düz kaslarının direkt olarak gevşetilmesi ve histamin salıverilmesine bağlı vazodilatasyon. Düz kaslı organlar üzerine etki: Devamlı barbitürat kullananlarda kabızlık gelişebilir. Hipnotik dozda uterusu etkilemez; ancak, genel anestezi yapan dozlarda i.v. verildiğinde kontraksiyon gücü ve sıklığını azaltırlar. Doğum eylemi sırasında verilen barbitüratların en önemli yan tesiri yenidoğanda solunumu deprese etmesidir. Karaciğer mikrozomal enzimlerinin indüksiyonu: Barbitüratlar (özellikle fenobarbital) CYP2A, CYP2B ve CYP2C alt-familyasındaki enzimleri indüklerler. Fenobarbital karaciğerde glukuronil transferaz enzimini indükleyerek bilirubinin konjügasyonunu ve atılımını artırır, ayrıca bilirubin bağlayan Y proteini düzeyini yükseltir. Bu etkilerinden dolayı yenidoğanlarda hiperbilirubinemi ve kernikterus a karşı kullanılabilir. Diğer etkileri: Barbitüratlar mitokondriyel bir enzim olan d-aminolevülinik asit (d-ALA) sentetaz enzimini indüklerler. Fenobarbital karaciğerde safra oluşumunu ve safra akımını artırır (kolerezis). Diğer barbitüratlar bu özelliği göstermezler. Tolerans gelişmesi ve bağımlılık: Tolerans hem farmakokinetik, hem de ilaca karşı duyarlılık azalmasına (reseptör desensitizasyonu ve/veya down-regulation) bağlıdır. Çapraz tolerans diğer hipnosedatiflere karşı etil alkole karşı genel anesteziklere karşı Barbitüratlar pozitif pekiştiri yapıcı maddelerdir. Bu nedenle suistimal edilirler. En fazla suistimal edilenler kısa etki süreli sekobarbital ve pentobarbitaldir. Kısa ve orta etki süreli olanların suistimal edilme ve bağımlılık yapma potansiyelleri uzun etki sürelilerden daha fazladır.")
31
Barbitüratların Yan Etkileri
Uyuşukluk hali ve artık etki Bağımlılık Rebound uykusuzluk Alerjik reaksiyonlar Solunum depresyonu Paradoksik eksitasyon Porfiria'nın şiddetlenmesi Uyuşukluk hali ve artık etki: Bağımlılık Rebound uykusuzluk: Barbitüratların REM dönemini kısaltmaları nedeniyle bu ilaçları hipnotik dozda bir süre alan hastalarda ilaç kesildiğinde REM'in rebound uzamasına bağlı olarak eskisinden daha şiddetli uykusuzluk oluşur. Rebound uykusuzluk hafif bir fiziksel bağımlılık gelişmiş olmasının bir belirtisi olarak kabul edilir. Fenobarbital gibi uzun etki süreli olanlar böyle bir sorun oluşturmazlar. Alerjik reaksiyonlar: Çeşitli tipte cilt döküntüleri ve anjiyoödem (özellikle göz kapakları, yanak ve dudaklarda şişme) şeklinde ortaya çıkar. Fenobarbital nadir olarak fatal eksfoliyatif dermatit ve megaloblastik anemi yapabilir. Solunum depresyonu Paradoksik eksitasyon: Nadir görülür. Porfiria'nın şiddetlenmesi
 şeklinde ortaya çıkar. Fenobarbital nadir olarak fatal eksfoliyatif dermatit ve megaloblastik anemi yapabilir. Solunum depresyonu. Paradoksik eksitasyon: Nadir görülür. Porfiria nın şiddetlenmesi.")
32
Barbitüratların İlaç Etkileşimleri
Birlikte kullanıldıklarında etki artar! Anksiyolitik ilaçlar (aditif) Diğer uyku ilaçları (aditif) Alkol (potansiyalizasyon) Barbitürat kullananlarda karaciğer mikrozomal enzim indüksiyonu nedeniyle metabolizmaları hızlanmış, etkileri azalmıştır! Kumarin türevi oral antikoagülanlar Steroidler Fenitoin Griseofulvin Rifampisin Fenotiazinler Trisiklik antidepresanlar
 Diğer uyku ilaçları (aditif) Alkol (potansiyalizasyon) Barbitürat kullananlarda karaciğer mikrozomal enzim indüksiyonu nedeniyle metabolizmaları hızlanmış, etkileri azalmıştır! Kumarin türevi oral antikoagülanlar. Steroidler. Fenitoin. Griseofulvin. Rifampisin. Fenotiazinler. Trisiklik antidepresanlar.")
33
Buspiron 5-HT1A reseptörlerinin parsiyel agonistidir. GABA ve BZ reseptörlerini etkilemez. Anksiyolitik etkisi 1-3 haftalık bir uygulamadan sonra (latent dönem) ortaya çıkar. Antidepresan etkinlik de gösterir. Avantajları Anksiyolitik etkisine daha az psikomotor bozukluk eşlik eder. Sedasyon ve amnezi oluşturmaz veya çok hafif oluşturur. Tolerans ve bağımlılık gelişmez; kesilme sendromu oluşturmaz. Yeşil reçeteye yazılması gerekmez. Alkol ve diğer sedatif ilaçlarla birlikte alındığında onların depresif etkilerini artırmaz. Kısmen karaciğerde metabolize edilir; kısmen de değişmeden böbreklerden atılır. İleri derecede karaciğer veya böbrek yetmezliği olanlarda kontrendikedir. Doz: 5 mg x 3 kez/gün ile başlanır. Günlük doz 2-3 günde bir yeterli bir cevap alınana kadar 5 mg artırılır. Optimal günlük doz mg'dır. Diğer türevler: ipsapiron, gepiron BUSPON 5 mg, 50 kapsül
 ortaya çıkar. Antidepresan etkinlik de gösterir. Avantajları. Anksiyolitik etkisine daha az psikomotor bozukluk eşlik eder. Sedasyon ve amnezi oluşturmaz veya çok hafif oluşturur. Tolerans ve bağımlılık gelişmez; kesilme sendromu oluşturmaz. Yeşil reçeteye yazılması gerekmez. Alkol ve diğer sedatif ilaçlarla birlikte alındığında onların depresif etkilerini artırmaz. Kısmen karaciğerde metabolize edilir; kısmen de değişmeden böbreklerden atılır. İleri derecede karaciğer veya böbrek yetmezliği olanlarda kontrendikedir. Doz: 5 mg x 3 kez/gün ile başlanır. Günlük doz 2-3 günde bir yeterli bir cevap alınana kadar 5 mg artırılır. Optimal günlük doz mg dır. Diğer türevler: ipsapiron, gepiron. BUSPON. 5 mg, 50 kapsül.")
34
Ramelteon Suprakiazmatik nükleusta yer alan MT1 ve MT2 melatonin reseptörlerinin agonistidir. İlacın, santral sinir sistemindeki GABAerjik ileti üzerinde herhangi bir etkisi yoktur. Kronik insomnialı hastalarda yapılan polisomnografi çalışmalarında, ramelteon’un uykuya dalma süresini kısalttığı, rebound uykusuzluk veya yoksunluk sendromu oluşturmadığı saptanmıştır. Oral verilişten sonra hızlı bir şekilde emilir ve önemli ölçüde ilk geçiş etkisine uğrar, ana bileşikten daha uzun yarılanma ömrüne sahip (2-5 saat) bir aktif metabolite dönüşür. Metabolizması CYP1A2 ile gerçekleştirilir. Fluvoksamin ile beraber (CYP1A2 inhibitörü) birlikte kullanılmamalıdır. Karaciğer fonksiyon bozukluğu olanlarda dikkatli kullanılmalıdır. Başlıca yan etkileri baş dönmesi, uyku hali, yorgunluk ve endokrin değişikliklerdir (testosteronu azaltır, prolaktini artırır). RAMELTEONMelatonin receptors are thought to be involved in maintaining circadian rhythms underlying the sleep-wake cycle (Chapter 16). Ramelteon, a novel hypnotic drug prescribed specifically for patients who have difficulty in falling asleep, is an agonist at MT1 and MT2 melatonin receptors located in the suprachiasmatic nuclei of the brain. The drug has no direct effects on GABAergic neurotransmission in the central nervous system. In polysomnography studies of patients with chronic insomnia, ramelteon reportedly reduced the latency to persistent sleep with no rebound insomnia or withdrawal symptoms. The drug is rapidly absorbed after oral administration and undergoes extensive first-pass metabolism, forming an active metabolite with longer half-life (2-5 hours) than the parent drug. The CYP1A2 isoform of cytochrome P450 is mainly responsible for the metabolism of ramelteon; the drug should not be used with fluvoxamine (an inhibitor of CYP1A2) and should be used with caution in patients with liver dysfunction. Adverse effects of ramelteon include dizziness, somnolence, fatigue, and endocrine changes as well as decreases in testosterone and increases in prolactin. Ramelteon is not a controlled substance.
 bir aktif metabolite dönüşür. Metabolizması CYP1A2 ile gerçekleştirilir. Fluvoksamin ile beraber (CYP1A2 inhibitörü) birlikte kullanılmamalıdır. Karaciğer fonksiyon bozukluğu olanlarda dikkatli kullanılmalıdır. Başlıca yan etkileri baş dönmesi, uyku hali, yorgunluk ve endokrin değişikliklerdir (testosteronu azaltır, prolaktini artırır). RAMELTEONMelatonin receptors are thought to be involved in maintaining circadian rhythms underlying the sleep-wake cycle (Chapter 16). Ramelteon, a novel hypnotic drug prescribed specifically for patients who have difficulty in falling asleep, is an agonist at MT1 and MT2 melatonin receptors located in the suprachiasmatic nuclei of the brain. The drug has no direct effects on GABAergic neurotransmission in the central nervous system. In polysomnography studies of patients with chronic insomnia, ramelteon reportedly reduced the latency to persistent sleep with no rebound insomnia or withdrawal symptoms. The drug is rapidly absorbed after oral administration and undergoes extensive first-pass metabolism, forming an active metabolite with longer half-life (2-5 hours) than the parent drug. The CYP1A2 isoform of cytochrome P450 is mainly responsible for the metabolism of ramelteon; the drug should not be used with fluvoxamine (an inhibitor of CYP1A2) and should be used with caution in patients with liver dysfunction. Adverse effects of ramelteon include dizziness, somnolence, fatigue, and endocrine changes as well as decreases in testosterone and increases in prolactin. Ramelteon is not a controlled substance.")
35
Anksiyete Bozukluklarının Tedavisi
Jeneralize anksiyete bozukluğu: Benzodiazepinler ve Buspiron Panik bozukluğu: Antipanik etkili BZ'ler: Alprazolam ve Lorazepam SSRİ'ler: Fluoksetin, Paroksetin, Sertralin, Trazodon Antipanik etkileri antidepresan etkilerinden bağımsızdır. Trisiklik antidepresanlar: Antipanik etkileri antidepresan etkilerinden bağımsızdır.

36
Diğer Hipnotikler t1/2 Doz (mg) (PO) İstenmeyen etkiler Kloral hidrat
7-10 Mideyi tahriş eder, tadı kötüdür. Halojenli bir bileşiktir (hepatotoksisite, aritmi riski) Paraldehid - 5-10 ml (sıvıdır) Nefeste kokma (% 10-30'u akciğerlerden atıldığı için) Etklorvinol 10-20 Tolerans-bağımlılık Porfirialılarda KE, Etinamat 2.5 Bağımlılık GİS iritasyonu, ciltte kızarıklık, alerji, trombositopenik purpura Hidroksizin 3 50-100 Uyuşukluk, atropin benzeri etkiler Meprobamat 6-17 YR SSS depresyonu, paradoksik eksitasyon, alerji, KcME İndüksiyonu Metiprilon 3-6 50-400 Porfirialılarda KE, SSS depresyonu, paradoksik eksitasyon, GİS iritasyonu, KcME İndüksiyonu
 Paraldehid ml (sıvıdır) Nefeste kokma (% u akciğerlerden atıldığı için) Etklorvinol Tolerans-bağımlılık. Porfirialılarda KE, Etinamat Bağımlılık. GİS iritasyonu, ciltte kızarıklık, alerji, trombositopenik purpura. Hidroksizin Uyuşukluk, atropin benzeri etkiler. Meprobamat YR. SSS depresyonu, paradoksik eksitasyon, alerji, KcME İndüksiyonu. Metiprilon Porfirialılarda KE, SSS depresyonu, paradoksik eksitasyon, GİS iritasyonu, KcME İndüksiyonu.")
37
Barbituratlarla additif etkileşme ile toksisiteyi arttıran ilaç hangisidir? (Nisan 1999) a. Trankilizanlar b. Antikoagulanlar c. Glukokortikoitler d. Trisiklikler e. Rifampisin (Cevap D) Aşağıdaki benzodirazepinlerin en uzun plazma ömre sahip olanı hangisidir? (Nisan 1999) a. Diazepam b. Lorazepam c. Oksazepam d. Tenazepam e. Flurazepam (Cevap A) Benzodiazepinlerin etkisini geri çeviren hangisidir? (Eylül 2000) a. Nalokson b. Flumazenil c. Klordiazepoksid d. Thiopental e. Metadion (Cevap B) Aşağıdakilerden hangisi bir benzodiazepin olmamasına karşılık BZ1 (omega1, w1) reseptör agonistidir? (Eylül 2002) a. Alprazolam b. Klorazepat c. Zolpidem d. Flurazepam e. Klordiazepoksit (Cevap C) Oral alındığında aktif metabolit olan desmetildiazepam’a dönüşmeyen benzodiazepin hangisidir? (Nisan 1995) a. Klorazepat b. Diazepam c. Halazepam d. Oksazepam e. Prazepam (Cevap D) Aşağıdakilerden hangisi diazepamın endikasyonu değildir? (Nisan 1988) a. Alkol yoksunluk sendromu b. Status epilepticus c. Anksiyete d. Anestezi premedikasyonu e. majör depresyon (Cevap E) TUS Soruları
 a. Diazepam b. Lorazepam c. Oksazepam d. Tenazepam e. Flurazepam (Cevap A) Benzodiazepinlerin etkisini geri çeviren hangisidir (Eylül 2000) a. Nalokson. b. Flumazenil. c. Klordiazepoksid. d. Thiopental. e. Metadion. (Cevap B) Aşağıdakilerden hangisi bir benzodiazepin olmamasına karşılık BZ1 (omega1, w1) reseptör agonistidir (Eylül 2002) a. Alprazolam b. Klorazepat c. Zolpidem d. Flurazepam e. Klordiazepoksit (Cevap C) Oral alındığında aktif metabolit olan desmetildiazepam’a dönüşmeyen benzodiazepin hangisidir (Nisan 1995) a. Klorazepat b. Diazepam c. Halazepam d. Oksazepam e. Prazepam (Cevap D) Aşağıdakilerden hangisi diazepamın endikasyonu değildir (Nisan 1988) a. Alkol yoksunluk sendromu b. Status epilepticus c. Anksiyete d. Anestezi premedikasyonu e. majör depresyon (Cevap E) TUS Soruları.")
38
Aşağıdakilerden hangisi barbituratların etkilerinden değildir
Aşağıdakilerden hangisi barbituratların etkilerinden değildir? (Eylül 1987) a. Solunum depresyonu b. Kas gevşemesi c. Analjezi d. Sedasyon e. Kc mikrozomal enz. indüksiyonu (Cevap C) Aşağıdakilerden hangisi barbituratların etkisi değildir? (Nisan 1990) a. Analjezi b. Bağımlılık c. Solunum depresyonu d. Sedasyon e. Kc mikrozomal enz. indüksiyonu (Cevap A) Etki süresi en uzun barbiturat hangisidir? (Nisan 1991) a. Tiobarbital b. Fenobarbital c. Sekobarbital d. Amobarbital e. Pentobarbital (Cevap B) En uzun etki süreli barbiturat aşağıdakilerden hangisidir? (Nisan 1995) a. Fenobarbital b. Sekobarbital c. Pentobarbital d. Tiopental e. Amobarnital (Cevap A) Etki süresi en kısa hipnotik hangisidir? (Eylül 1991) a. Diazepam b. Klorazepam c. Triazolam d. Nitrazepam e. Klorazepam (Cevap C) Aşağıdaki benzodiazepinlerden etki süresi en kısa olan hangisidir? (Eylül 1995) a. Halazepam b. Triazolam c. Diazepam d. Flurazepam e. Klordiazepoksit (Cevap B) TUS Soruları
 a. Solunum depresyonu b. Kas gevşemesi c. Analjezi d. Sedasyon e. Kc mikrozomal enz. indüksiyonu (Cevap C) Aşağıdakilerden hangisi barbituratların etkisi değildir (Nisan 1990) a. Analjezi b. Bağımlılık c. Solunum depresyonu d. Sedasyon e. Kc mikrozomal enz. indüksiyonu (Cevap A) Etki süresi en uzun barbiturat hangisidir (Nisan 1991) a. Tiobarbital b. Fenobarbital c. Sekobarbital d. Amobarbital e. Pentobarbital (Cevap B) En uzun etki süreli barbiturat aşağıdakilerden hangisidir (Nisan 1995) a. Fenobarbital b. Sekobarbital c. Pentobarbital d. Tiopental e. Amobarnital (Cevap A) Etki süresi en kısa hipnotik hangisidir (Eylül 1991) a. Diazepam b. Klorazepam c. Triazolam d. Nitrazepam e. Klorazepam (Cevap C) Aşağıdaki benzodiazepinlerden etki süresi en kısa olan hangisidir (Eylül 1995) a. Halazepam b. Triazolam c. Diazepam d. Flurazepam e. Klordiazepoksit (Cevap B) TUS Soruları.")
39
Benzodiazepinler etkilerini hangi yolla gerçekleştirirler
Benzodiazepinler etkilerini hangi yolla gerçekleştirirler? (Eylül 1987) a. Gangliyon blokajı yaparak b. Enkefalinlerin etkilerini artırarak c. GABA’nın etkisini artırarak d. İyon pompasını inhibe edek e. Depolarizasyon blokajı yaparak (Cevap C) Benzodiazepinlerin trankilizan ve hipnotik etkinliğinin meydana gelmesinde en fazla rol oynayan nöromediyatör aşağıdakilerden hangisidir? (Eylül 1991) a. Asetilkolin b. Enkefalin c. Adrenalin d. Serotonin e. GABA (Cevap E) Fenobarbital zehirlenmesinde hangisi kullanılır? (Nisan 2001) a. Diazepam b. Klorpromazin c. Amonyum klorür d. Sodyum bikarbonat e. Askorbik asit (Cevap D) Aşağıdaki benzodiazepinlerden hangisi aktif metabolitine dönüşerek etki göstermez? (Eylül 2003) a. oksazepam b. flurazepam c. prazepam d. kuazepam e. klordiazepoksid (Cevap A) Aşağıdaki benzodiazepinlerden hangisinin insan plazmasında eliminasyon yarı ömrü en kısadır? (Nisan 2003) a. flurazepam b. kuazepam c. klordiazepoksid d. …… e. triazolam (Cevap E) TUS Soruları
 a. Gangliyon blokajı yaparak b. Enkefalinlerin etkilerini artırarak c. GABA’nın etkisini artırarak d. İyon pompasını inhibe edek e. Depolarizasyon blokajı yaparak (Cevap C) Benzodiazepinlerin trankilizan ve hipnotik etkinliğinin meydana gelmesinde en fazla rol oynayan nöromediyatör aşağıdakilerden hangisidir (Eylül 1991) a. Asetilkolin b. Enkefalin c. Adrenalin d. Serotonin e. GABA (Cevap E) Fenobarbital zehirlenmesinde hangisi kullanılır (Nisan 2001) a. Diazepam b. Klorpromazin c. Amonyum klorür d. Sodyum bikarbonat e. Askorbik asit (Cevap D) Aşağıdaki benzodiazepinlerden hangisi aktif metabolitine dönüşerek etki göstermez (Eylül 2003) a. oksazepam b. flurazepam c. prazepam d. kuazepam e. klordiazepoksid (Cevap A) Aşağıdaki benzodiazepinlerden hangisinin insan plazmasında eliminasyon yarı ömrü en kısadır (Nisan 2003) a. flurazepam b. kuazepam c. klordiazepoksid d. …… e. triazolam (Cevap E) TUS Soruları.")
40
(A) Phenobarbital (B) Alprazolam (C) Zolpidem (D) Hydroxyzine
1. A 21-year-old man is a full-time college student who also works 25 hours per week. Over the past 3 months he has become increasingly anxious. He says he is tired most of the time and has trouble concentrating on his studies. Which of the following drugs would be the most appropriate initial pharmacologic treatment for his anxiety? B. The young man’s anxiety is probably caused by the stress induced by a full college curriculum along with working 25 hours per week. A benzodiazepine antianxiety agent would help relieve his symptoms. (A) Phenobarbital (B) Alprazolam (C) Zolpidem (D) Hydroxyzine (E) Propranolol
 Phenobarbital. (B) Alprazolam. (C) Zolpidem. (D) Hydroxyzine. (E) Propranolol.")
41
2. A 33-year-old woman has recently undergone a divorce
2. A 33-year-old woman has recently undergone a divorce. She reports that although she is exhausted, it usually takes her 2 or more hours to fall asleep at night.Which of the following drugs would help relieve her sleep disturbance while being least disruptive to REM sleep? C. Zolpidem is effective at relieving sleep-onset insomnia. The other agents listed could also induce sleep, although each would be expected to produce more disruption of sleep rhythm than would zolpidem. (A) Triazolam (B) Chloral hydrate (C) Zolpidem (D) Amobarbital (E) Hydroxyzine
 Triazolam. (B) Chloral hydrate. (C) Zolpidem. (D) Amobarbital. (E) Hydroxyzine.")
42
3. A 54-year-old man is scheduled for an elective colonoscopy that will take approximately 20 minutes. Which of the following drugs would be most likely to produce the desired anesthesia and anterograde amnesia? C. Midazolam, like all benzodiazepines given in sufficient dose, has the capacity to produce anterograde amnesia. It is also available in an injectable form and frequently is used as an anesthetic agent during short procedures. (A) Buspirone (B) Zephalon (C) Midazolam (D) Chlordiazepoxide (E) Hydroxyzine
 Buspirone. (B) Zephalon. (C) Midazolam. (D) Chlordiazepoxide. (E) Hydroxyzine.")
43
4. A 33-year-old woman has a 15-year history of alcohol abuse
4. A 33-year-old woman has a 15-year history of alcohol abuse. She comes to the emergency department for treatment of injuries received in a fall. She says she has been drinking heavily and almost continuously for 2 weeks, and she wants to stop. Which of the following drugs would most effectively and safely lessen the intensity of her withdrawal syndrome? B. Chlordiazepoxide, through its metabolites, has a relatively long biological half-life. It will prevent many of the severe symptoms of acute alcohol withdrawal. Buspirone is not a sedative and will not suppress alcohol withdrawal.The other agents have sedative properties and could potentially suppress alcohol withdrawal but each has a much shorter biological half-life than chlordiazepoxide. (A) Buspirone (B) Chlordiazepoxide (C) Chloral hydrate (D) Midazolam (E) Zolpidem
 Buspirone. (B) Chlordiazepoxide. (C) Chloral hydrate. (D) Midazolam. (E) Zolpidem.")
44
(A) Alprazolam (B) Zephalon (C) Chloral hydrate (D) Propranolol
5. A 23-year-old medical student has to make a presentation before his classmates. He is very anxious about this presentation and reports that on one previous occasion the sweating and palpitations that accompany his stage fright were so intense that he was unable to complete his presentation. Pretreatment with which of the following drugs would relieve his symptoms without making him drowsy? D. As a -adrenoceptor blocker, propranolol can relieve many of the symptoms of stage fright. For this use it can be taken once a few hours before the performance. Chronic dosing is usually not necessary. The other agents produce sedation. (A) Alprazolam (B) Zephalon (C) Chloral hydrate (D) Propranolol (E) Diazepam
 Alprazolam. (B) Zephalon. (C) Chloral hydrate. (D) Propranolol. (E) Diazepam.")
45
these definitions have now been appended to the DSM–IV.
The Association of Sleep Disorders Centres has classified sleep disorders into two broad classes disorders of initiating and maintaining sleep (DIMS) and disorders of excessive somnolence (DOES); these definitions have now been appended to the DSM–IV.
 and. disorders of excessive somnolence (DOES); these definitions have now been appended to the DSM–IV.")
46
Insomnia may be classified into three major types
Transient insomnia. This occurs in normal sleepers who experience an acute stress or stressful situation lasting for a few days, for example, air travel to a different time zone or hospitalization. Short-term insomnia. This is usually associated with situational stress caused, for example, by bereavement or which may be related to conflict at work or in the family. Long-term insomnia. Studies suggest that insomnia in up to 50% of patients in this category is related to an underlying psychiatric illness. Of the remainder of the patients in this category, chronic alcohol or drug abuse may be the cause of the sleep disruption.

47
Plasma elimination half-lives of hypnotic benzodiazepines and their active metabolites
For all practical purposes, the benzodiazepines are the group of drugs most widely used to treat insomnia. These may be divided into three classes based on their pharmacokinetic characteristics: 1. Short half-life drugs, such as triazolam, midazolam and brotizolam, with elimination half-lives of about 6 hours. 2. Intermediate half-life drugs, such as temazepam, lormetazepam and loprazolam, with half-lives of 6–12 hours. 3. Long half-life drugs, such as nitrazepam, flurazepam and flunitrazepam, with half-lives over 12 hours.

48
Summary of the drugs used to treat insominia
1. Benzodiazepine receptor agonists Benzodiazepines (triazolam, temazepam, midazolam, lorazepam, estazolam). Non-benzodiazepines (imidazopyridines, e.g. zolpidem; pyrazopyrimidines, e.g. zaleplon; cyclopyrolones, e.g. zopiclone). 2. Pharmacological effects Benzodiazepines – shorter latency to sleep, longer duration of sleep, decreased REM sleep, increased slow-wave sleep. Zopiclone – similar to benzodiazepines. Zaleplon and zolpidem – stated to have little adverse effect on sleep profile. There is evidence that the therapeutic efficacy is maintained even after several months of treatment. 3. Main side effects Long half-life benzodiazepines cause day-time sedation. Dose-related anterograde amnesia. Impaired reaction time and vigilance. In elderly, cognitive impairment; falls causing fractures. Rebound insomnia can occur after withdrawal of short half-life drugs. Recurrence of original symptoms can occur when drug is stopped. Withdrawal effects on abrupt discontinuation of drug. These include: dizziness, confusion and dysphoria. Because of the frequency of side effects, benzodiazepine ligands are only recommended for the short-term (4 weeks) treatment of insomnia. 4. Other treatments include: Sedative antidepressants (venlafaxine, trazodone, nefazodone, TCAs, mianserin, mirtazepine). Antihistamines (diphenhydramine, doxylamine). Melatonin (may shorten sleep latency but little effect on sleep time). Valerian extract (evidence of efficacy in double-blind studies). It should be noted that all these alternative treatments for insomnia also have side effects, some of which (e.g. TCAs) are potentially more serious than those occurring with the benzodiazepine group. Summary of the drugs used to treat insominia 1. Benzodiazepine receptor agonists Benzodiazepines (triazolam, temazepam, midazolam, lorazepam, estazolam). Non-benzodiazepines (imidazopyridines, e.g. zolpidem; pyrazopyrimidines, e.g. zaleplon; cyclopyrolones, e.g. zopiclone). 2. Pharmacological effects Benzodiazepines – shorter latency to sleep, longer duration of sleep, decreased REM sleep, increased slow-wave sleep. Zopiclone – similar to benzodiazepines. Zaleplon and zolpidem – stated to have little adverse effect on sleep profile. There is evidence that the therapeutic efficacy is maintained even after several months of treatment. 3. Main side effects Long half-life benzodiazepines cause day-time sedation. Dose-related anterograde amnesia. Impaired reaction time and vigilance. In elderly, cognitive impairment; falls causing fractures. Rebound insomnia can occur after withdrawal of short half-life drugs. Recurrence of original symptoms can occur when drug is stopped. Withdrawal effects on abrupt discontinuation of drug. These include: dizziness, confusion and dysphoria. Because of the frequency of side effects, benzodiazepine ligands are only recommended for the short-term (4 weeks) treatment of insomnia. 4. Other treatments include: Sedative antidepressants (venlafaxine, trazodone, nefazodone, TCAs, mianserin, mirtazepine). Antihistamines (diphenhydramine, doxylamine). Melatonin (may shorten sleep latency but little effect on sleep time). Valerian extract (evidence of efficacy in double-blind studies). It should be noted that all these alternative treatments for insomnia also have side effects, some of which (e.g. TCAs) are potentially more serious than those occurring with the benzodiazepine group.
. Non-benzodiazepines (imidazopyridines, e.g. zolpidem; pyrazopyrimidines, e.g. zaleplon; cyclopyrolones, e.g. zopiclone). 2. Pharmacological effects. Benzodiazepines – shorter latency to sleep, longer duration of sleep, decreased REM sleep, increased slow-wave sleep. Zopiclone – similar to benzodiazepines. Zaleplon and zolpidem – stated to have little adverse effect on sleep profile. There is evidence that the therapeutic efficacy is maintained even after several months of treatment. 3. Main side effects. Long half-life benzodiazepines cause day-time sedation. Dose-related anterograde amnesia. Impaired reaction time and vigilance. In elderly, cognitive impairment; falls causing fractures. Rebound insomnia can occur after withdrawal of short half-life drugs. Recurrence of original symptoms can occur when drug is stopped. Withdrawal effects on abrupt discontinuation of drug. These include: dizziness, confusion and dysphoria. Because of the frequency of side effects, benzodiazepine ligands are only recommended for the short-term (4 weeks) treatment of insomnia. 4. Other treatments include: Sedative antidepressants (venlafaxine, trazodone, nefazodone, TCAs, mianserin, mirtazepine). Antihistamines (diphenhydramine, doxylamine). Melatonin (may shorten sleep latency but little effect on sleep time). Valerian extract (evidence of efficacy in double-blind studies). It should be noted that all these alternative treatments for insomnia also have side effects, some of which (e.g. TCAs) are potentially more serious than those occurring with the benzodiazepine group. Summary of the drugs used to treat insominia. 1. Benzodiazepine receptor agonists. Benzodiazepines (triazolam, temazepam, midazolam, lorazepam, estazolam). Non-benzodiazepines (imidazopyridines, e.g. zolpidem; pyrazopyrimidines, e.g. zaleplon; cyclopyrolones, e.g. zopiclone). 2. Pharmacological effects. Benzodiazepines – shorter latency to sleep, longer duration of sleep, decreased REM sleep, increased slow-wave sleep. Zopiclone – similar to benzodiazepines. Zaleplon and zolpidem – stated to have little adverse effect on sleep profile. There is evidence that the therapeutic efficacy is maintained even after several months of treatment. 3. Main side effects. Long half-life benzodiazepines cause day-time sedation. Dose-related anterograde amnesia. Impaired reaction time and vigilance. In elderly, cognitive impairment; falls causing fractures. Rebound insomnia can occur after withdrawal of short half-life drugs. Recurrence of original symptoms can occur when drug is stopped. Withdrawal effects on abrupt discontinuation of drug. These include: dizziness, confusion and dysphoria. Because of the frequency of side effects, benzodiazepine ligands are only recommended for the short-term (4 weeks) treatment of insomnia. 4. Other treatments include: Sedative antidepressants (venlafaxine, trazodone, nefazodone, TCAs, mianserin, mirtazepine). Antihistamines (diphenhydramine, doxylamine). Melatonin (may shorten sleep latency but little effect on sleep time). Valerian extract (evidence of efficacy in double-blind studies). It should be noted that all these alternative treatments for insomnia also have side effects, some of which (e.g. TCAs) are potentially more serious than those occurring with the benzodiazepine group.")
62
İnsomnia Tedavisi Non-farmakolojik Kognitif-davranış tedavisi Sleep restriction ve stimulus control therapy Farmakolojik temazepam Her 2 tedavi de yaklaşık eşit etkinlikte. Yeni yaklaşım 2 tedaviyi birlikte uygulamak yönünde TREATMENT OF IDIOPATHIC INSOMNIA – Because insomnia is a syndrome rather than a specific disorder, treatment is dependent upon the underlying cause. Treatment of secondary insomnia is unlikely to be successful unless the primary cause of the disturbance is diagnosed and properly remedied. (See "Epidemiology and causes of insomnia"). Pharmacologic therapy – Hypnotic medications alone may not be the treatment of first choice for chronic insomnia. When they are prescribed, they should be combined with nonpharmacologic therapies, such as improvements in sleep hygiene [12-16,24-29]. Judicious use of hypnotics may be helpful when treating transient or short-term idiopathic or psychophysiologic insomnia. Some patients with insomnia benefit from long term hypnotics without evidence of tolerance or abuse. Contraindications – Hypnotic medications are contraindicated in pregnancy because of data showing an increased risk of fetal malformations when diazepam or chlordiazepoxide is used during the first trimester. The drugs should also be avoided or used judiciously in patients with alcoholism or renal, hepatic, or pulmonary disease. The combination of alcohol and hypnotics is absolutely contraindicated. The drugs should also be avoided in patients with sleep apnea syndrome. Because all hypnotics produce sedation, they should not be taken by individuals who may be called upon to make important decisions in the night (ie, physicians "on call" and single parents responsible for the care of young children). Benzodiazepines and related hypnotics – Six benzodiazepine drugs (temazepam, flurazepam, triazolam, estazolam, lorazepam, and clonazepam) are commonly used as hypnotics in the United States. Three nonbenzodiazepine drugs, which appear to interact with the benzodiazepine receptor, are also available. These include zolpidem, zaleplon, and eszopiclone (Lunesta, previously Estorra) [30,31]. Eszopiclone was approved by the Food and Drug Administration for prolonged use in December 2004; the use of the other agents is restricted to 35 days [31]. The mechanism of action of these drugs in insomnia is not clear. They often produce subjective improvement in the quality and quantity of sleep rather than appreciable objective improvement. (See "The effect of drugs on sleep quality and architecture"). The selection of a specific hypnotic agent should be based primarily upon the elimination half-life. Short acting drugs such as temazepam, estazolam, triazolam, zaleplon, and zolpidem are generally preferable because they produce less residual somnolence the morning following their use. Adjustments in dosage may be necessary in patients who have prolonged drug elimination half-lives due to age or impaired renal or hepatic function. The incidence of tolerance, abuse, addiction, or rebound insomnia upon discontinuation in the insomnia population has been overrated. The fear of drug abuse results in patient abuse. For patients treated with benzodiazepines on a chronic basis to manage insomnia, the combination of cognitive behavioral therapy and a tapered reduction in benzodiazepine dosage is superior to dosage tapering alone. This was demonstrated in a randomized trial comparing these approaches in 65 adult patients who had used benzodiazepines for at least three months to manage primary insomnia [29]. Patients in the dual modality group were more likely to wean completely from benzodiazepines over the 8-week course of the study than patients treated with dose reduction alone (77 versus 38 percent respectively). These benefits were maintained at follow-up one year after completion of the initial intervention. Other hypnotics – A number of nonbenzodiazepine hypnotic medications may also be employed in the short-term treatment of insomnia. Zolpidem and related compounds have been included in the preceding discussion, because they activate the benzodiazepine receptor, although they do not have a benzodiazepine structure. • Antidepressants – A number of antidepressants (eg, amitriptyline, trazodone) have sedative properties because of central anticholinergic or antihistaminergic activities. Sedating antidepressants are most useful in the management of patients in whom depression and insomnia coexist, but have not been shown to be effective in the treatment of insomnia not associated with depression. • Antihistamines – Many over-the-counter sleep aids contain the sedating antihistamines diphenhydramine or doxylamine. These drugs have half-lives of 8.5 to 10 hours and may therefore result in decreased alertness, daytime sedation, and prolonged reaction times on the day following use. Dizziness, dryness of the mouth, constipation, and blurring of vision also may occur. These medications make people feel sleepy, but do not improve sleep, and are not helpful in the management of chronic insomnia. • Melatonin – Melatonin is a normal product of the pineal gland, and is sold as a food supplement and an orphan drug for use in correcting circadian rhythm sleep disorders in blind persons with no light perception [32]. Over-the-counter sales have been banned in Great Britain. Data regarding the efficacy and safety of melatonin are minimal, but the hormone does not appear to be a potent hypnotic for most patients with chronic insomnia [33-35]. However, a subgroup of patients with low melatonin levels have benefited from melatonin supplementation [36-38], and the treatment may be useful in patients with delayed sleep phase syndrome [33]. (See "Epidemiology and causes of insomnia" and see "Physiology and clinical use of melatonin"). Both nonpharmacologic and pharmacologic therapies may be useful in the management of idiopathic insomnia. As an example, one trial randomized 78 patients with idiopathic insomnia to treatment with cognitive-behavior therapy (including sleep restriction and stimulus control therapy), pharmacotherapy with temazepam, both interventions, or neither intervention [11]. The three active treatment arms had better results than the placebo arm after 3 months of therapy, and there was a trend toward better outcomes with the use of the combination of cognitive-behavior and pharmacologic therapies. The use of cognitive-behavior therapy was associated with more sustained improvements in sleep over the 24 month follow-up period. The mainstay of treatment for patients with idiopathic chronic insomnia consists of nonpharmacologic measures in conjunction with the judicious use of hypnotics [12-17]. Nonpharmacologic therapy – Nonpharmacologic interventions include sleep hygiene measures, relaxation therapy and biofeedback, stimulus control therapy, sleep restriction, and cognitive behaviorial therapy. Sleep hygiene measures – Sleep hygiene measures are listed in Table 3 (show table 3). These are simple, common sense actions that address sleep habits, attitudes, and other factors that are potentially detrimental to good sleep. Relaxation therapy – Relaxation therapy involves progressive muscle relaxation and biofeedback to reduce somatic arousal. One small study of several different relaxation procedures found a 42 percent improvement in self-reported sleep complaints after one year of relaxation therapy [18]. Stimulus control therapy – Stimulus control therapy may also be beneficial in patients with chronic idiopathic insomnia. Bootzin's stimulus control technique is directed at discouraging the learned association between the bedroom and wakefulness, and reestablishing the bedroom as the major stimulus for sleep (show table 4). These techniques have been reported to improve insomnia complaints in approximately 50 percent of individuals after one year [18]. Stimulus control therapy is based on the assumption that patients with insomnia have learned to associate the bed with the fear of not sleeping, rather than with the pleasurable anticipation of sleep. The longer one spends in bed trying to sleep, the stronger this subconscious association becomes. Patients should not spend more than 15 minutes in bed awake. If they are awake for 15 minutes, they should leave the bed and engage in a relaxing activity (reading, watching television, etc), and not engage in activities which subconsciously reward them for being awake in the middle of the night (such as balancing the checkbook, doing housework, or studying for a test). They can return to bed only when tired. If they still cannot sleep within 15 minutes, the process is repeated (show table 4). Sleep restriction therapy – Sleep restriction therapy may improve sleep efficiency by restricting the total time in bed for sleep. Once this has occurred, gradually increasing the time allotted to sleep may improve the level of daytime functioning and the overall quality of sleep. Roughly one-quarter of patients with insomnia may benefit from such a regimen [18]. Sleep restriction is accomplished by determining the average total sleep time (not time in bed). The patient is instructed to spend only that amount of time in bed, with a rigid bed and rise time. This will serve to sleep deprive the patient, increasing the pressure to sleep the next night. Cognitive behavioral therapy – Cognitive behavioral therapy (CBT), using a combination of the techniques described above, has been assessed in several small studies of patients with chronic insomnia [19-22]. Most of these trials suggest that CBT is associated with significant improvement in daytime and nocturnal symptoms with one randomized controlled trial of 63 adults with chronic sleep-onset insomnia that found CBT was superior to pharmacologic management with zolpidem [21]. Despite the promise of CBT, the relative efficacy of these various nonpharmacologic approaches has not been well established. One meta-analysis involving 2102 patients in 59 trials found that sleep restriction and stimulus control therapies were more effective than relaxation techniques when used alone; sleep hygiene measures alone did not show evidence of efficacy [23]. The extent to which the concomitant use of nonpharmacologic therapy augments the performance of pharmacologic treatments is also unclear [20].
. Pharmacologic therapy – Hypnotic medications alone may not be the treatment of first choice for chronic insomnia. When they are prescribed, they should be combined with nonpharmacologic therapies, such as improvements in sleep hygiene [12-16,24-29]. Judicious use of hypnotics may be helpful when treating transient or short-term idiopathic or psychophysiologic insomnia. Some patients with insomnia benefit from long term hypnotics without evidence of tolerance or abuse. Contraindications – Hypnotic medications are contraindicated in pregnancy because of data showing an increased risk of fetal malformations when diazepam or chlordiazepoxide is used during the first trimester. The drugs should also be avoided or used judiciously in patients with alcoholism or renal, hepatic, or pulmonary disease. The combination of alcohol and hypnotics is absolutely contraindicated. The drugs should also be avoided in patients with sleep apnea syndrome. Because all hypnotics produce sedation, they should not be taken by individuals who may be called upon to make important decisions in the night (ie, physicians on call and single parents responsible for the care of young children). Benzodiazepines and related hypnotics – Six benzodiazepine drugs (temazepam, flurazepam, triazolam, estazolam, lorazepam, and clonazepam) are commonly used as hypnotics in the United States. Three nonbenzodiazepine drugs, which appear to interact with the benzodiazepine receptor, are also available. These include zolpidem, zaleplon, and eszopiclone (Lunesta, previously Estorra) [30,31]. Eszopiclone was approved by the Food and Drug Administration for prolonged use in December 2004; the use of the other agents is restricted to 35 days [31]. The mechanism of action of these drugs in insomnia is not clear. They often produce subjective improvement in the quality and quantity of sleep rather than appreciable objective improvement. (See The effect of drugs on sleep quality and architecture ). The selection of a specific hypnotic agent should be based primarily upon the elimination half-life. Short acting drugs such as temazepam, estazolam, triazolam, zaleplon, and zolpidem are generally preferable because they produce less residual somnolence the morning following their use. Adjustments in dosage may be necessary in patients who have prolonged drug elimination half-lives due to age or impaired renal or hepatic function. The incidence of tolerance, abuse, addiction, or rebound insomnia upon discontinuation in the insomnia population has been overrated. The fear of drug abuse results in patient abuse. For patients treated with benzodiazepines on a chronic basis to manage insomnia, the combination of cognitive behavioral therapy and a tapered reduction in benzodiazepine dosage is superior to dosage tapering alone. This was demonstrated in a randomized trial comparing these approaches in 65 adult patients who had used benzodiazepines for at least three months to manage primary insomnia [29]. Patients in the dual modality group were more likely to wean completely from benzodiazepines over the 8-week course of the study than patients treated with dose reduction alone (77 versus 38 percent respectively). These benefits were maintained at follow-up one year after completion of the initial intervention. Other hypnotics – A number of nonbenzodiazepine hypnotic medications may also be employed in the short-term treatment of insomnia. Zolpidem and related compounds have been included in the preceding discussion, because they activate the benzodiazepine receptor, although they do not have a benzodiazepine structure. • Antidepressants – A number of antidepressants (eg, amitriptyline, trazodone) have sedative properties because of central anticholinergic or antihistaminergic activities. Sedating antidepressants are most useful in the management of patients in whom depression and insomnia coexist, but have not been shown to be effective in the treatment of insomnia not associated with depression. • Antihistamines – Many over-the-counter sleep aids contain the sedating antihistamines diphenhydramine or doxylamine. These drugs have half-lives of 8.5 to 10 hours and may therefore result in decreased alertness, daytime sedation, and prolonged reaction times on the day following use. Dizziness, dryness of the mouth, constipation, and blurring of vision also may occur. These medications make people feel sleepy, but do not improve sleep, and are not helpful in the management of chronic insomnia. • Melatonin – Melatonin is a normal product of the pineal gland, and is sold as a food supplement and an orphan drug for use in correcting circadian rhythm sleep disorders in blind persons with no light perception [32]. Over-the-counter sales have been banned in Great Britain. Data regarding the efficacy and safety of melatonin are minimal, but the hormone does not appear to be a potent hypnotic for most patients with chronic insomnia [33-35]. However, a subgroup of patients with low melatonin levels have benefited from melatonin supplementation [36-38], and the treatment may be useful in patients with delayed sleep phase syndrome [33]. (See Epidemiology and causes of insomnia and see Physiology and clinical use of melatonin ). Both nonpharmacologic and pharmacologic therapies may be useful in the management of idiopathic insomnia. As an example, one trial randomized 78 patients with idiopathic insomnia to treatment with cognitive-behavior therapy (including sleep restriction and stimulus control therapy), pharmacotherapy with temazepam, both interventions, or neither intervention [11]. The three active treatment arms had better results than the placebo arm after 3 months of therapy, and there was a trend toward better outcomes with the use of the combination of cognitive-behavior and pharmacologic therapies. The use of cognitive-behavior therapy was associated with more sustained improvements in sleep over the 24 month follow-up period. The mainstay of treatment for patients with idiopathic chronic insomnia consists of nonpharmacologic measures in conjunction with the judicious use of hypnotics [12-17]. Nonpharmacologic therapy – Nonpharmacologic interventions include sleep hygiene measures, relaxation therapy and biofeedback, stimulus control therapy, sleep restriction, and cognitive behaviorial therapy. Sleep hygiene measures – Sleep hygiene measures are listed in Table 3 (show table 3). These are simple, common sense actions that address sleep habits, attitudes, and other factors that are potentially detrimental to good sleep. Relaxation therapy – Relaxation therapy involves progressive muscle relaxation and biofeedback to reduce somatic arousal. One small study of several different relaxation procedures found a 42 percent improvement in self-reported sleep complaints after one year of relaxation therapy [18]. Stimulus control therapy – Stimulus control therapy may also be beneficial in patients with chronic idiopathic insomnia. Bootzin s stimulus control technique is directed at discouraging the learned association between the bedroom and wakefulness, and reestablishing the bedroom as the major stimulus for sleep (show table 4). These techniques have been reported to improve insomnia complaints in approximately 50 percent of individuals after one year [18]. Stimulus control therapy is based on the assumption that patients with insomnia have learned to associate the bed with the fear of not sleeping, rather than with the pleasurable anticipation of sleep. The longer one spends in bed trying to sleep, the stronger this subconscious association becomes. Patients should not spend more than 15 minutes in bed awake. If they are awake for 15 minutes, they should leave the bed and engage in a relaxing activity (reading, watching television, etc), and not engage in activities which subconsciously reward them for being awake in the middle of the night (such as balancing the checkbook, doing housework, or studying for a test). They can return to bed only when tired. If they still cannot sleep within 15 minutes, the process is repeated (show table 4). Sleep restriction therapy – Sleep restriction therapy may improve sleep efficiency by restricting the total time in bed for sleep. Once this has occurred, gradually increasing the time allotted to sleep may improve the level of daytime functioning and the overall quality of sleep. Roughly one-quarter of patients with insomnia may benefit from such a regimen [18]. Sleep restriction is accomplished by determining the average total sleep time (not time in bed). The patient is instructed to spend only that amount of time in bed, with a rigid bed and rise time. This will serve to sleep deprive the patient, increasing the pressure to sleep the next night. Cognitive behavioral therapy – Cognitive behavioral therapy (CBT), using a combination of the techniques described above, has been assessed in several small studies of patients with chronic insomnia [19-22]. Most of these trials suggest that CBT is associated with significant improvement in daytime and nocturnal symptoms with one randomized controlled trial of 63 adults with chronic sleep-onset insomnia that found CBT was superior to pharmacologic management with zolpidem [21]. Despite the promise of CBT, the relative efficacy of these various nonpharmacologic approaches has not been well established. One meta-analysis involving 2102 patients in 59 trials found that sleep restriction and stimulus control therapies were more effective than relaxation techniques when used alone; sleep hygiene measures alone did not show evidence of efficacy [23]. The extent to which the concomitant use of nonpharmacologic therapy augments the performance of pharmacologic treatments is also unclear [20].")
67
Binding sites for GABA, barbiturates,
steroids, and picrotoxin are all located within the pore domain of the channel (Figure 6.9B). Another site, called the benzodiazepine binding site, lies outside the pore and modulates channel activity.
. Another site, called the benzodiazepine binding site, lies. outside the pore and modulates channel activity.")
69
Figure 6.9 Ionotropic GABA receptors. (A) Stimulation of a
presynaptic GABAergic interneuron, at the time indicated by the arrow, causes a transient inhibition of action potential firing in its postynaptic target. This inhibitory response is caused by activation of postsynaptic GABAA receptors. (B) Ionotropic GABA receptors contain two binding sites for GABA and numerous sites at which drugs bind to and modulate these receptors. (A after Chavas and Marty, 2003).
 Ionotropic. GABA receptors contain two binding sites for GABA and. numerous sites at which drugs bind to and modulate these. receptors. (A after Chavas and Marty, 2003).")
71
FIGURE 1 Structure and function of the GABAB receptor
FIGURE 1 Structure and function of the GABAB receptor. Attachment of GABA to the receptor recognition site located on the GABAB(1) component causes dissociation of the a- and bg-subunits from the G protein affiliated with the GABAB(2) component of the receptor dimer. The liberated G-protein subunits influence cellular activity by regulating Ca2ş and Kş flux, adenylyl cyclase activity, and transcription factors. (Modified from Enna, S. (2001). A GABAB mystery: The search for pharmacologically distinct GABAB receptors. Mol. Interventions 1, 208–218.)
 component causes dissociation of the a- and bg-subunits from the G protein affiliated with the GABAB(2) component of the receptor dimer. The. liberated G-protein subunits influence cellular activity by regulating Ca2ş and Kş flux, adenylyl cyclase activity, and transcription factors. (Modified from Enna, S. (2001). A GABAB mystery: The search for pharmacologically distinct GABAB receptors. Mol. Interventions 1, 208–218.)")
72
FIGURE 2 Donut model of GABAA receptor heteropentamer showing ligand-binding and subunit interaction domains. (A) The 5 subunits (-b–g–a–b–a-) and 5 subunit interfaces (1–5) are shown, indicating the two different subunit interfaces for each subunit ((2) and (ş)), the ligandbinding pockets for GABA and benzodiazepines (BZ), and the various peptide loops (A–I) involved in ligand-binding or subunit interfaces. The pore in the center represents the chloride channel. (B) The sequences represent the loopsA–I within the N-terminal extracellular domain of thea1,b2, and g2 subunits (numbering corresponds to mature subunits from rat). Circles: GABA site; squares: BZ site; diamonds (a1): photoaffinity label sites identified by sequencing: F64 (Muscimol);H101 (Flunitrazepam); Y209 (Ro ). Underlines: subunit interaction loops, indicated under the line.
 and 5 subunit interfaces (1–5) are shown, indicating the two different subunit interfaces for each subunit ((2) and (ş)), the ligandbinding. pockets for GABA and benzodiazepines (BZ), and the various peptide loops (A–I) involved in ligand-binding or subunit interfaces. The pore. in the center represents the chloride channel. (B) The sequences represent the loopsA–I within the N-terminal extracellular domain of thea1,b2, and. g2 subunits (numbering corresponds to mature subunits from rat). Circles: GABA site; squares: BZ site; diamonds (a1): photoaffinity label sites. identified by sequencing: F64 (Muscimol);H101 (Flunitrazepam); Y209 (Ro ). Underlines: subunit interaction loops, indicated under the line.")
Benzer bir sunumlar

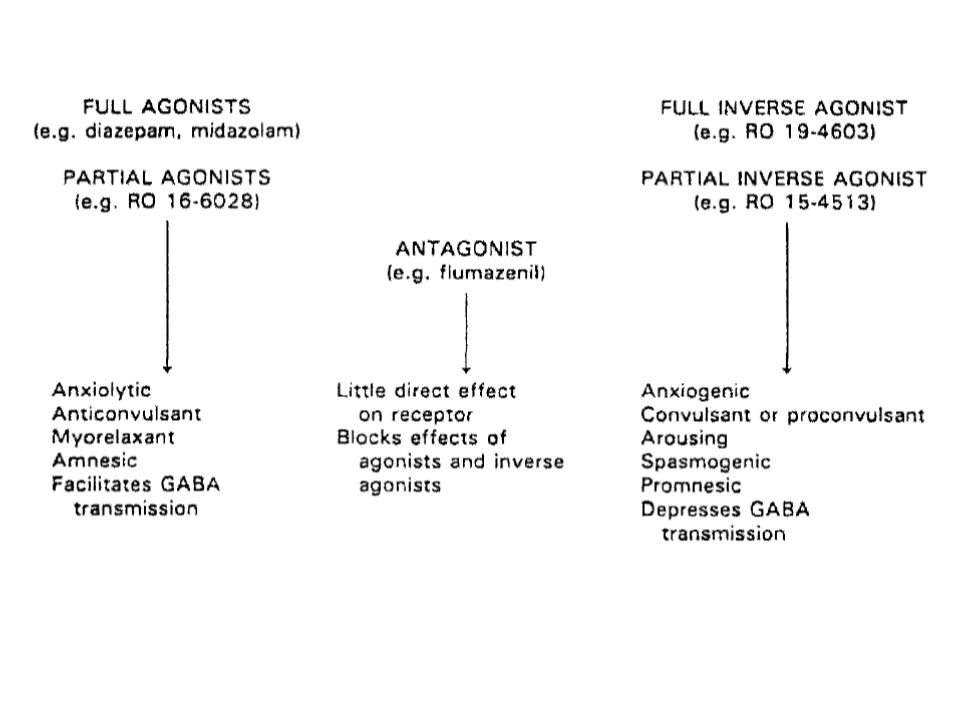
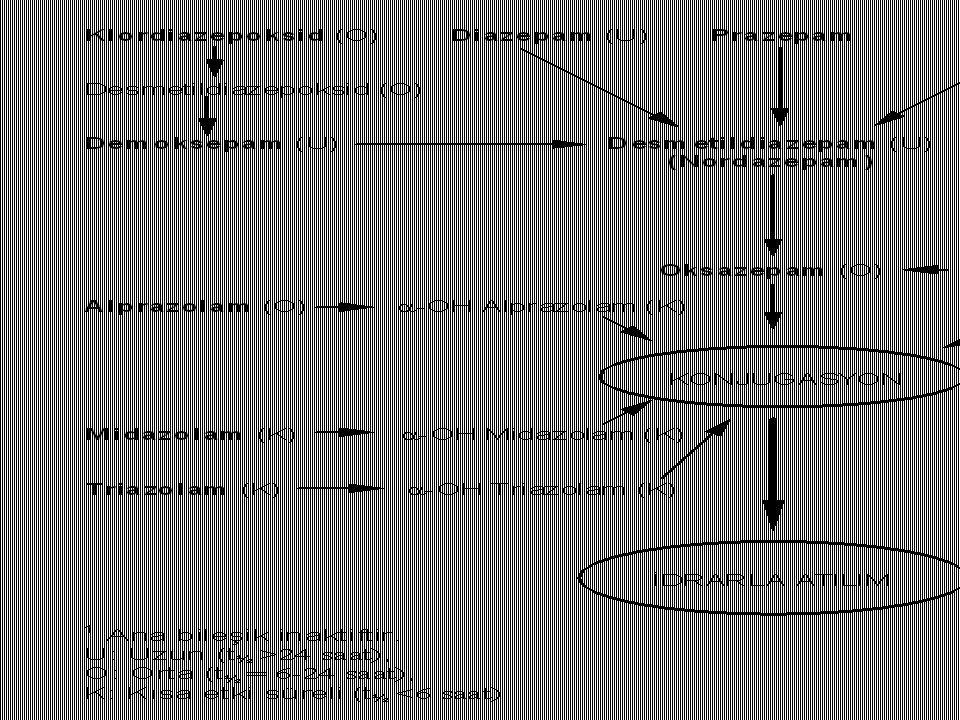
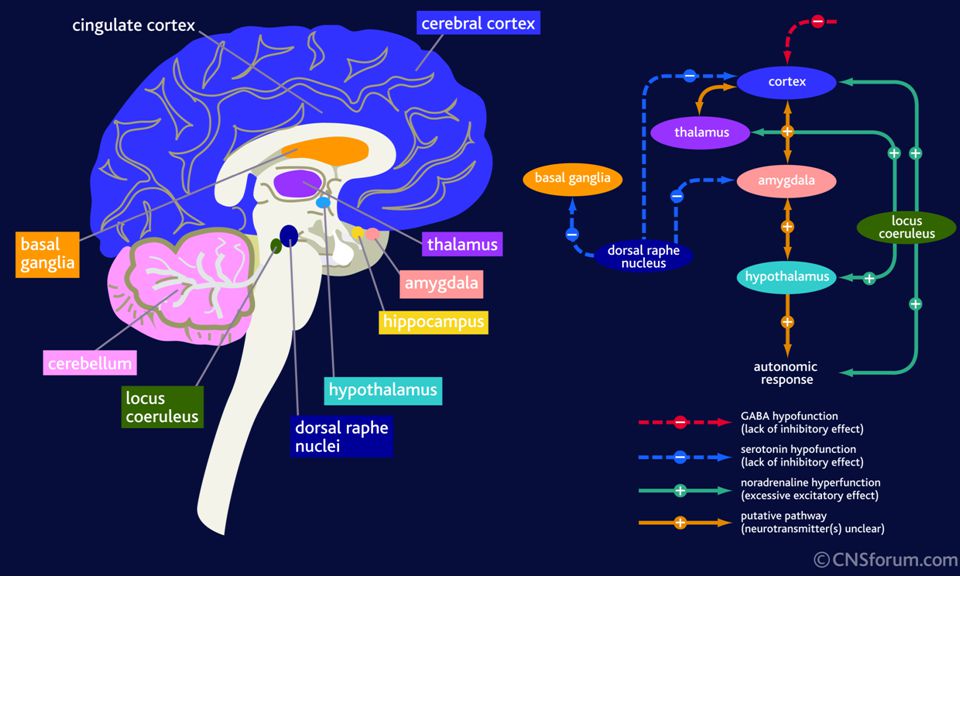
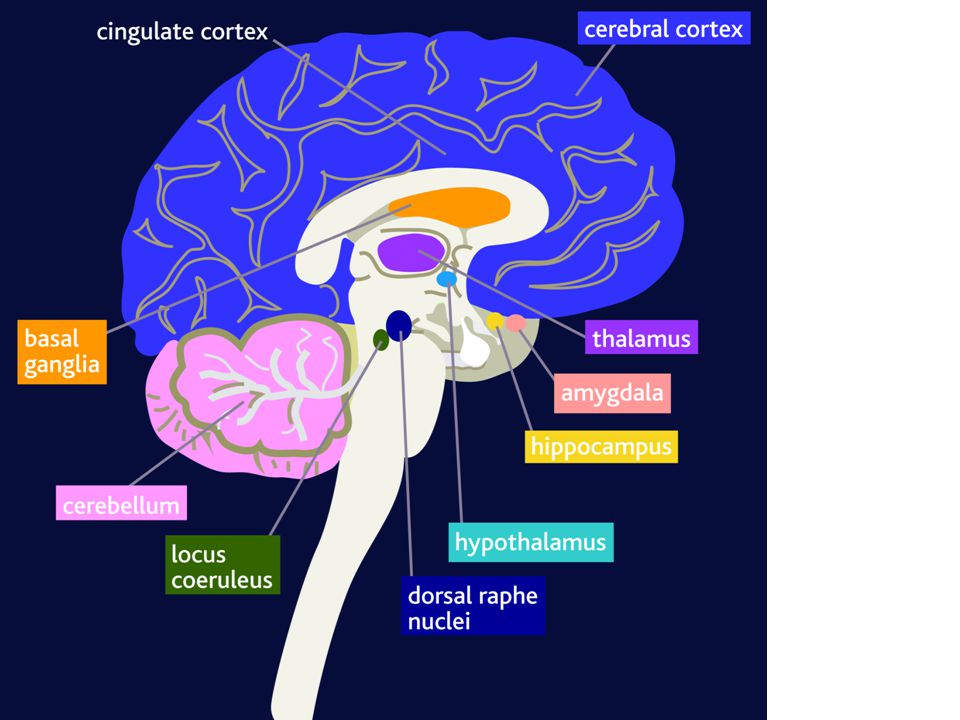

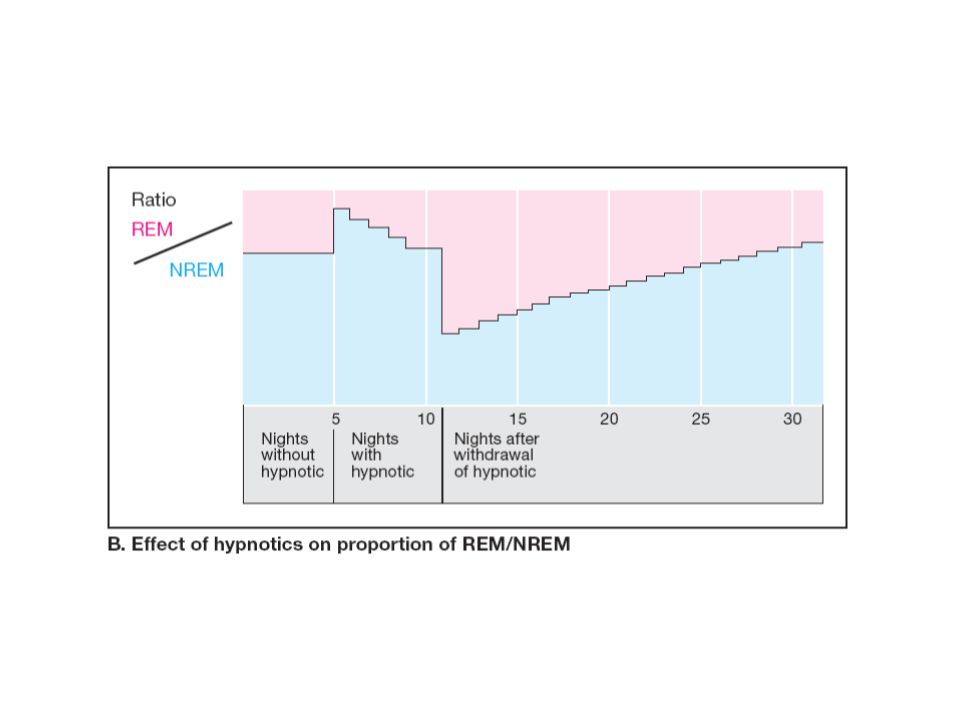
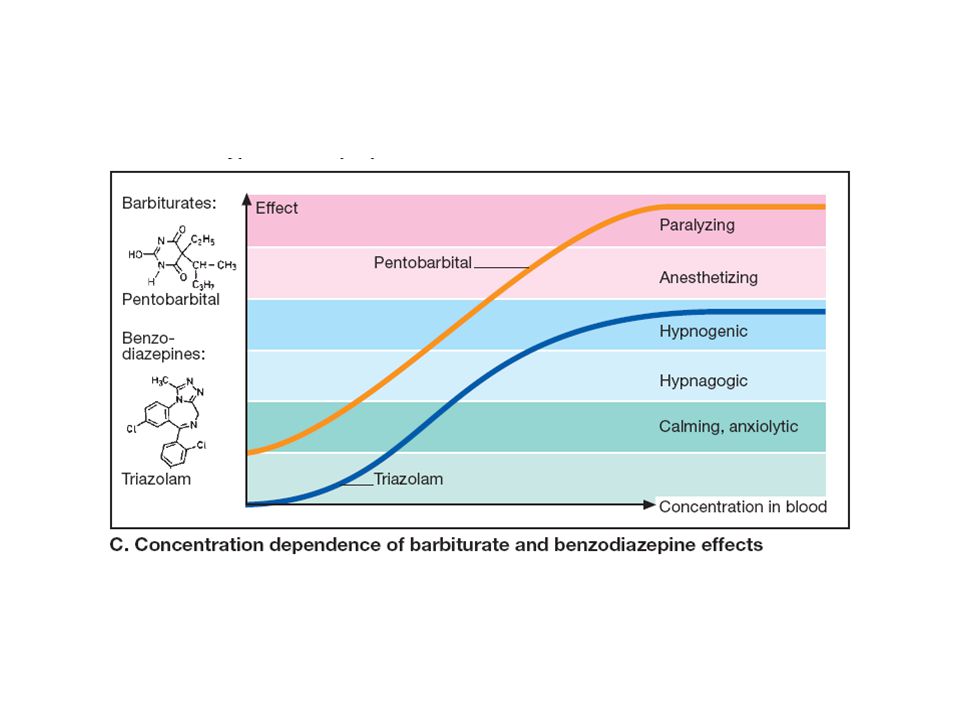
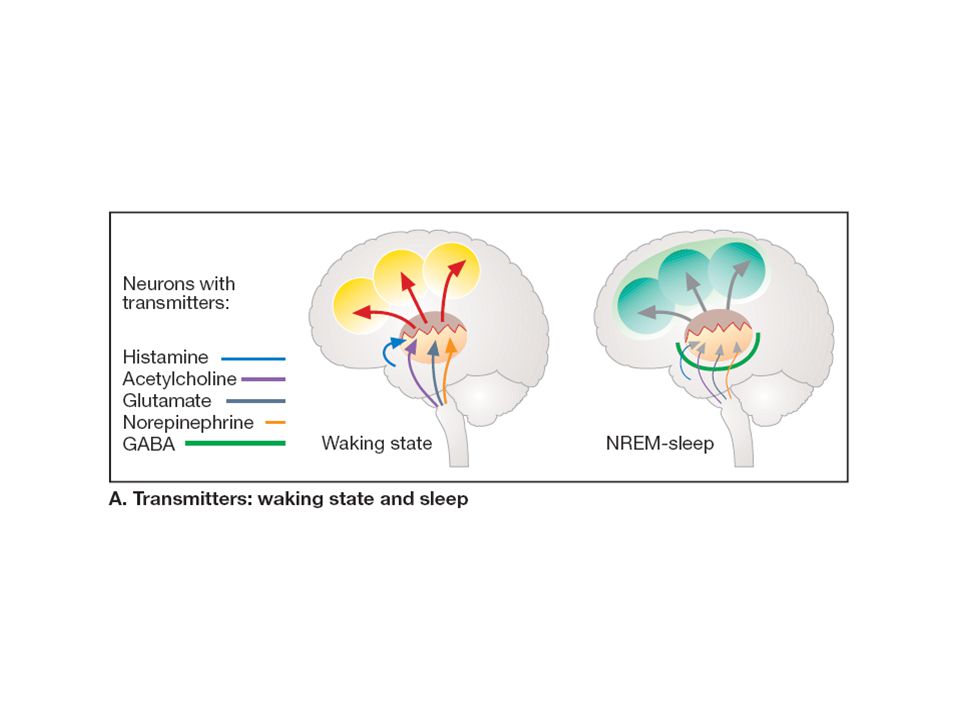
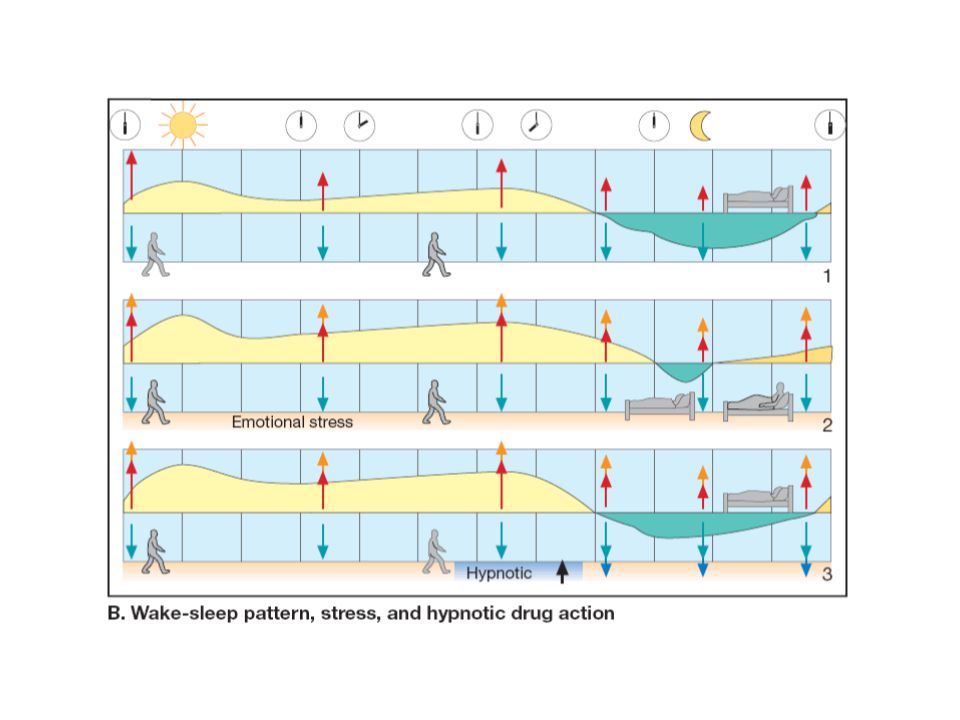
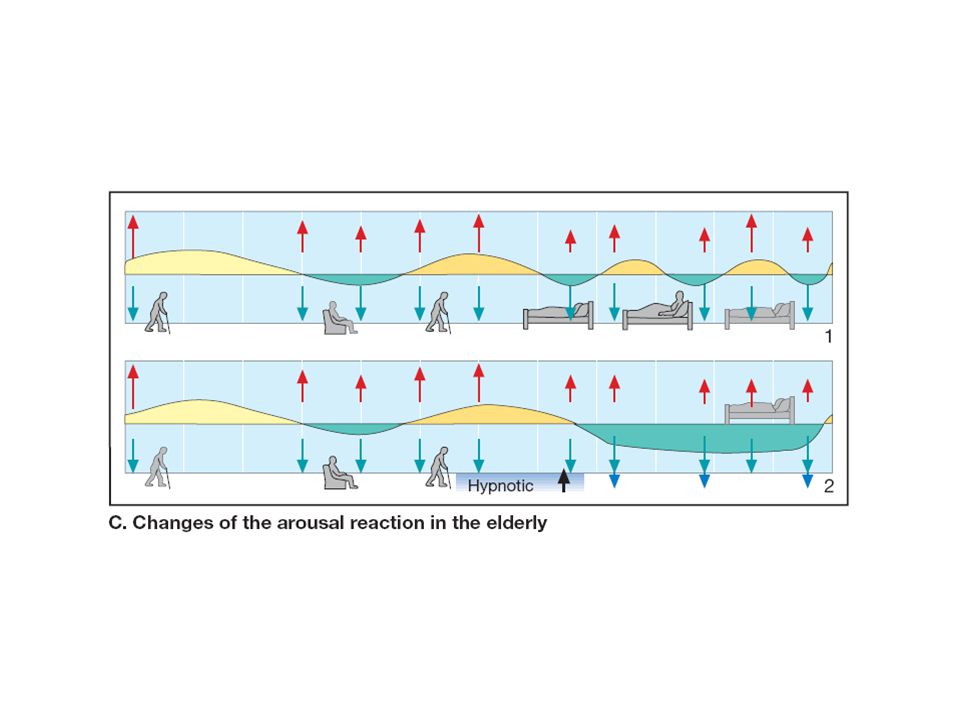
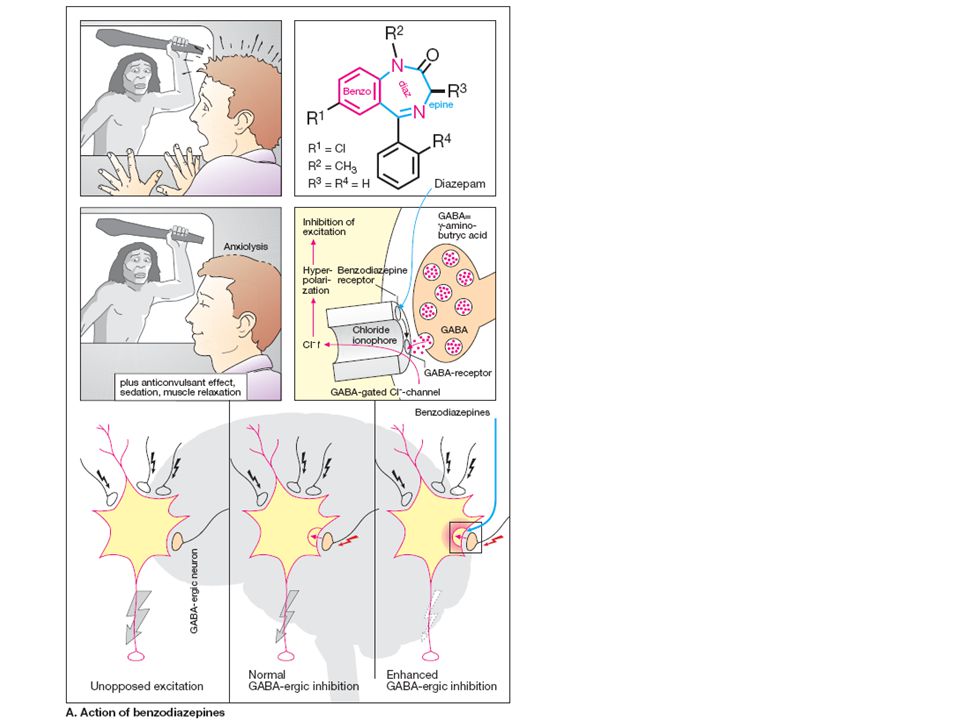

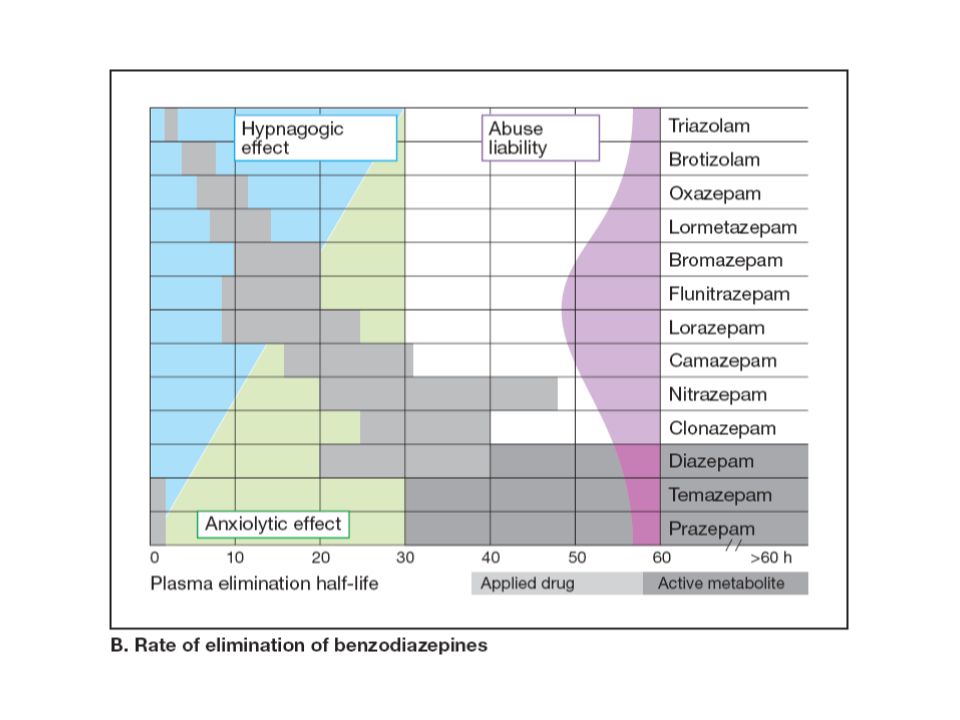
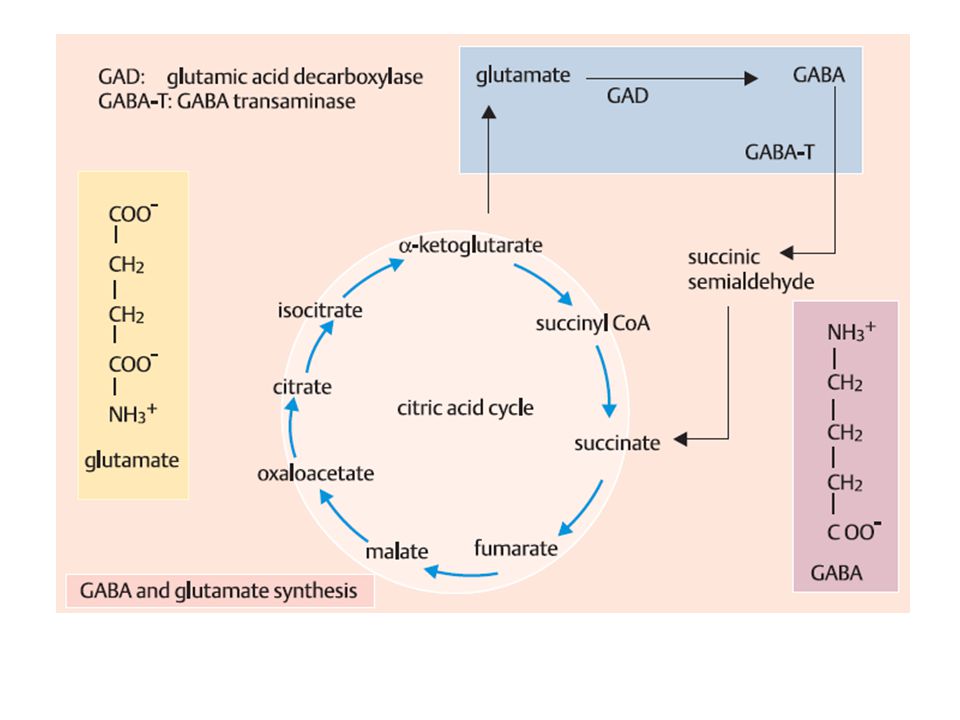
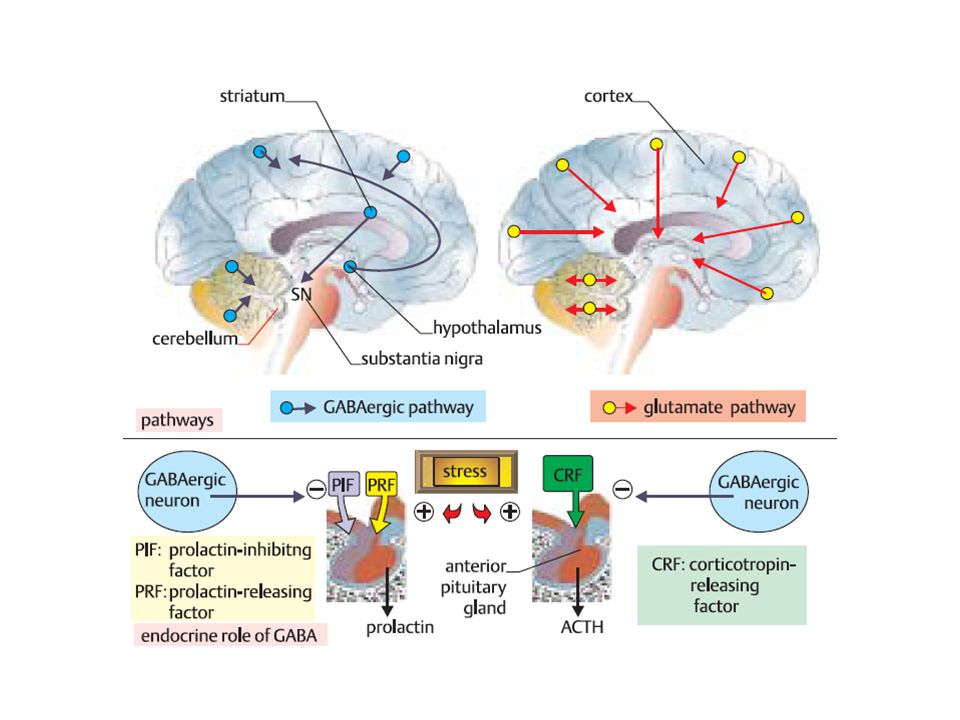
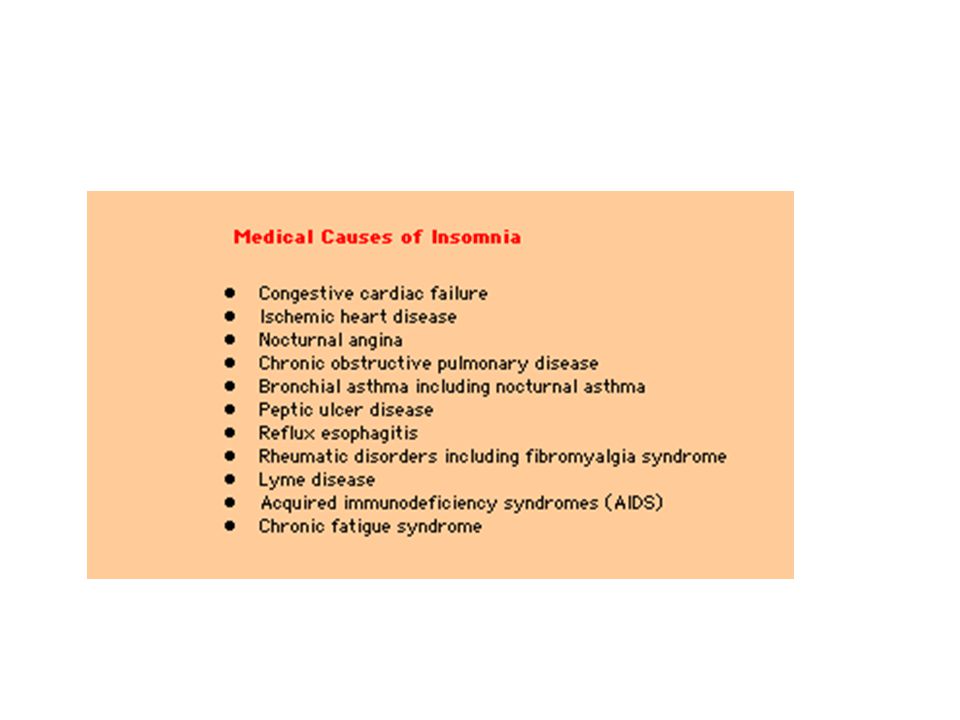

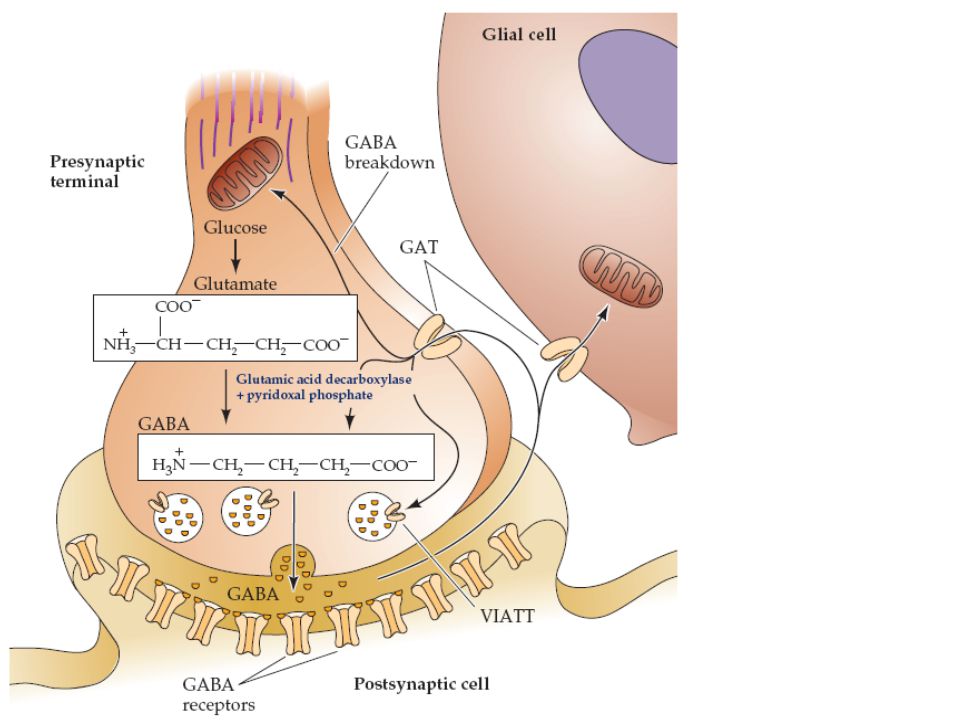
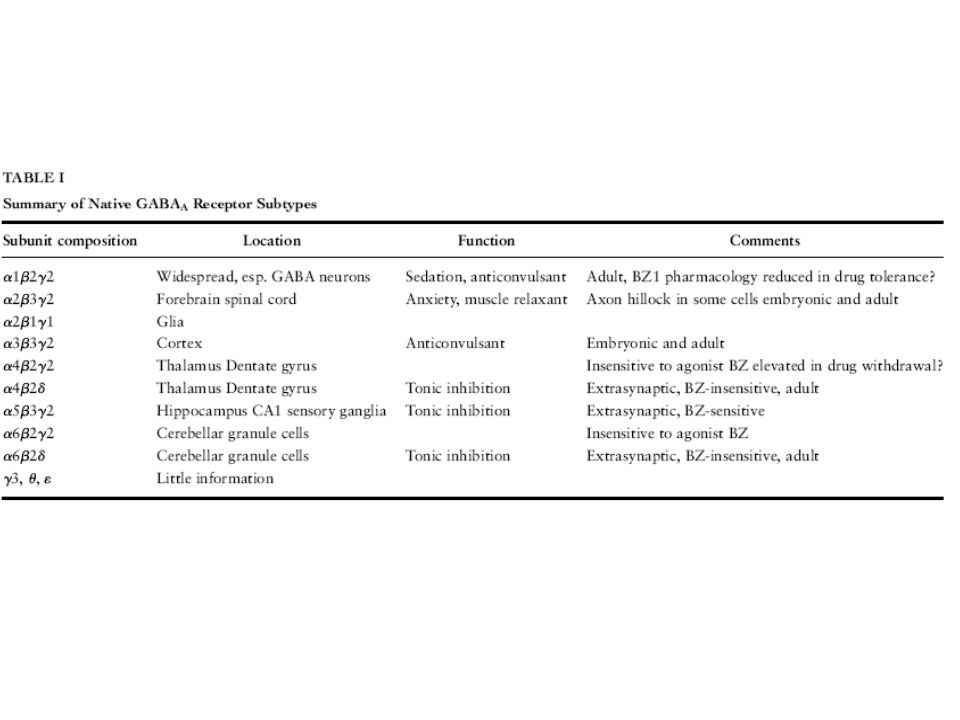
Bu tense ile temel olarak içinde bulunduğumuz anda yapmakta olduğumuz eylemleri anlatırız. Zamanı.>")














 2 friends... you'll have 3 years of good luck!!!>")



