Sunuyu indir
Sunum yükleniyor. Lütfen bekleyiniz

1
Recent Developments in Pathological Diagnosis and Classification of Lung Cancer
Serpil Dizbay Sak Ankara ÜTF, Patoloji ABD 15. Toraks Kongresi Nisan 2012/Antalya

2
Conflict of Interest: NONE TO DECLARE

3
Topics “Old” classification Why do we need change?
The new (proposed) classification
 classification.")
4
OLD CLASSIFICATION

5
TC Sağlık Bakanlığı

6
T.C. Sağlık Bakanlığı Kanserle Savaş Dairesi
Yaşa spesifik insidans Erkek Kadın Kaba insidens hızı 74,85 10,68 Yaşa standardize insidens hızı (YSH) 75,80 9,58 Expected number of new cases in Turkey 30.239 Türkiye’nin Akciğer Kanseri Haritası Projesi Türk Toraks Derneği/ Akciğer ve Plevra Maligniteleri Çalışma Grubu T.C. Sağlık Bakanlığı Kanserle Savaş Dairesi
 75,80. 9,58. Expected number of new cases. in Turkey Türkiye’nin Akciğer Kanseri Haritası Projesi. Türk Toraks Derneği/ Akciğer ve Plevra Maligniteleri Çalışma Grubu. T.C. Sağlık Bakanlığı Kanserle Savaş Dairesi.")
7
2004 Written by pathologists for pathologists
Surgical resection specimens

8
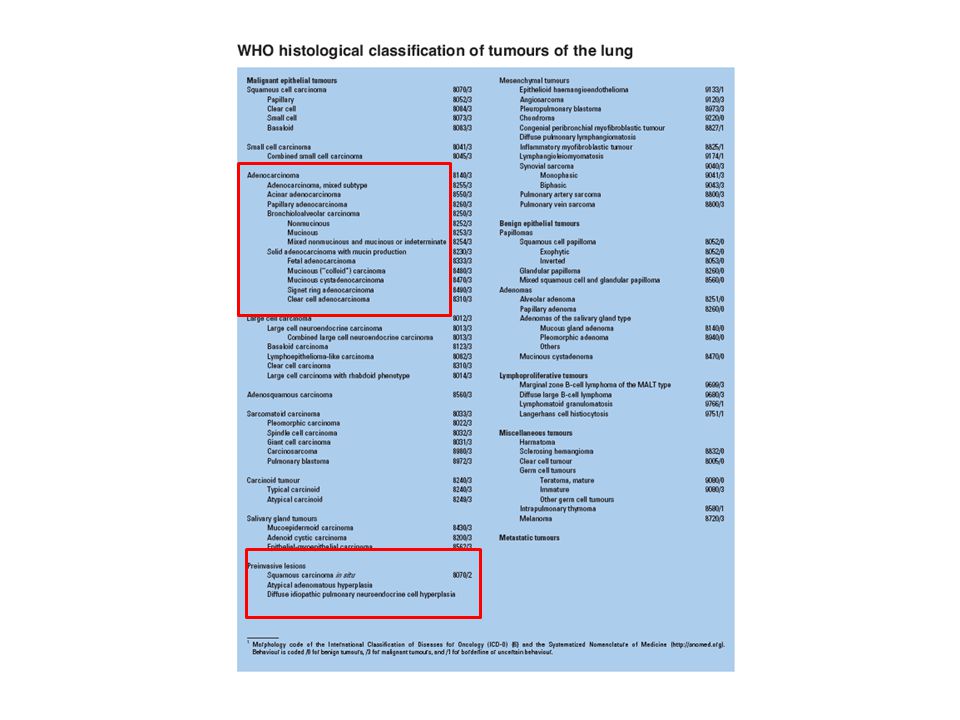
Akciğerin malign epitelyal tümörleri (WHO 2004)
İNVAZİV 1.Yassı hücreli karsinoma 2.Küçük hücreli karsinoma 3. Adenokarsinoma 4. Büyük hücreli karsinoma 5. Adenoskuamöz karsinoma 6. Sarkomatoid karsinoma 7. Karsinoid tümör 8.Tükrük bezi tipi karsinomalar PREKÜRSÖR-ÖNCÜ 9.Preinvaziv lezyonlar Displazi- CIS AAH DIPNECH

9
Adeno carcinoma(25-40%) ↑ SCC (25-40%) ↓ Small cell (20-25%)
WHO 2004 Adeno carcinoma(25-40%) ↑ SCC (25-40%) ↓ Small cell (20-25%) Large cell (%10-25)
 ↑ SCC (25-40%) ↓ Small cell (20-25%) Large cell (%10-25)")
10
Akciğerin malign epitelyal tümörleri Mevcut Sınıflama (WHO2004)
4. Büyük hücreli karsinoma a. Büyük hücreli nöroendokrin karsinoma b.Bazoloid karsinoma c.Lenfoepitelyoma benzeri karsinoma d. Şeffaf (berrak) hücreli karsinoma g. Rabdoid fenotipli büyük hücreli karsinoma 5. Adenoskuamöz karsinoma 6. Sarkomatoid karsinomalar a. Pleomorfik karsinoma b. İğsi hücreli karsinoma c. Dev hücreli karsinoma b. Karsinosarkoma c. Pulmoner blastoma 7. Karsinoid tümör a.Tipik karsinoid b.Atipik karsinoid 8.Tükrük bezi tipi karsinomalar a. Mukoepidermoid karsinoma b. Adenoid kistik karsinoma c. Epitelyal-myoepitelyal 9.Preinvaziv l ezyonlar a.İn situ yassı hücreli karsinoma b.Atipik adenomatöz hiperplazi c. Diffüz idiyopatik pulmoner nöroendokrin hücre hiperplazisi 1.Yassı hücreli karsinoma a. Papiller b. Şeffaf (berrak) hücreli c. Küçük hücreli d. Bazaloid 2.Küçük hücreli karsinoma Kombine küçük hücreli karsinoma 3. Adenokarsinoma a. Asiner b. Papiller c. Bronkioloalveolar karsinoma: müsinöz/nonmüsinöz/mikst d. Müsin bulunduran solid e. Mikst adenokarsinoma Varyantlar: Fetal Müsinöz karsinom Müsinöz kistadeno karsinom Taşlı yüzük hücreli karsinom Berrak hücreli karsinom 3. Adenokarsinoma a. Asiner b. Papiller c. Bronkioloalveolar karsinoma: müsinöz/nonmüsinöz/mikst d. Müsin bulunduran solid e. Mikst adenokarsinoma
 hücreli karsinoma. g. Rabdoid fenotipli büyük hücreli karsinoma. 5. Adenoskuamöz karsinoma. 6. Sarkomatoid karsinomalar. a. Pleomorfik karsinoma. b. İğsi hücreli karsinoma. c. Dev hücreli karsinoma. b. Karsinosarkoma. c. Pulmoner blastoma. 7. Karsinoid tümör. a.Tipik karsinoid. b.Atipik karsinoid. 8.Tükrük bezi tipi karsinomalar. a. Mukoepidermoid karsinoma. b. Adenoid kistik karsinoma. c. Epitelyal-myoepitelyal. 9.Preinvaziv l ezyonlar. a.İn situ yassı hücreli karsinoma. b.Atipik adenomatöz hiperplazi. c. Diffüz idiyopatik pulmoner nöroendokrin hücre hiperplazisi. 1.Yassı hücreli karsinoma. a. Papiller. b. Şeffaf (berrak) hücreli. c. Küçük hücreli. d. Bazaloid. 2.Küçük hücreli karsinoma. Kombine küçük hücreli karsinoma. 3. Adenokarsinoma. a. Asiner. b. Papiller. c. Bronkioloalveolar karsinoma: müsinöz/nonmüsinöz/mikst. d. Müsin bulunduran solid. e. Mikst adenokarsinoma. Varyantlar: Fetal. Müsinöz karsinom. Müsinöz kistadeno karsinom. Taşlı yüzük hücreli karsinom. Berrak hücreli karsinom. 3. Adenokarsinoma. a. Asiner. b. Papiller. c. Bronkioloalveolar karsinoma: müsinöz/nonmüsinöz/mikst. d. Müsin bulunduran solid. e. Mikst adenokarsinoma.")
11
WHO 2004

12
WHO 2004

13
Adenokarsinoma a. Asiner b. Papiller c. Bronkioloalveolar karsinoma d. Müsin bulunduran solid adenokarsinoma e. Mikst adenokarsinoma %90 Mikst tipte (asiner, papiller ve BAK patterni bulunduran) adenokarsinoma
 adenokarsinoma.")
14
Stage of NSCLC by the time of diagnosis
Number (%) IA 72 1.8 IB 336 8.3 IIA 21 0.5 IIB 234 5.8 IIIA 446 11.0 IIIB 1248 30.8 IV 1696 41.8 Total 4053 100.0 72.6 % Türkiye’nin Akciğer Kanseri Haritası Projesi Türk Toraks Derneği/ Akciğer ve Plevra Maligniteleri Çalışma Grubu T.C. Sağlık Bakanlığı Kanserle Savaş Dairesi
 IA IB IIA IIB IIIA IIIB IV Total % Türkiye’nin Akciğer Kanseri Haritası Projesi. Türk Toraks Derneği/ Akciğer ve Plevra Maligniteleri Çalışma Grubu. T.C. Sağlık Bakanlığı Kanserle Savaş Dairesi.")
15
Only small biopsy and cytology specimens are available in advanced disease

16
Classification is difficult in small specimen
Necrosis Artefacts Lack of differantiation Tumor heterogeneity

17
Non-small cell carcinoma
Adenocarcinoma SCC Large cell

18
Simple Reproducable Sufficient for patient management Chemo for small cell Surgery or cytotoxic therapy for NSCLC

19
CHANGE, WHY?

20
NEED FOR NEW PROGNOSTIC CATEGORIES
Why Change? New and Targeted therapies Prognostic information on small BAC’s Molecular characterization of lung cancer New agents for adenocarcinoma Histologic eligibility criteria for some new drugs Excellent prognosis of pure BAC and BAC with minimal invasion DEMISE OF NSCLC NEED FOR NEW PROGNOSTIC CATEGORIES

21
NEED FOR NEW PROGNOSTIC CATEGORIES
Why Change? New and Targeted therapies Prognostic information on small BAC’s Molecular characterization of lung cancer New agents for adenocarcinoma Histologic eligibility criteria for some new drugs Excellent prognosis of pure BAC and BAC with minimal invasion DEMISE OF NSCLC NEED FOR NEW PROGNOSTIC CATEGORIES

22
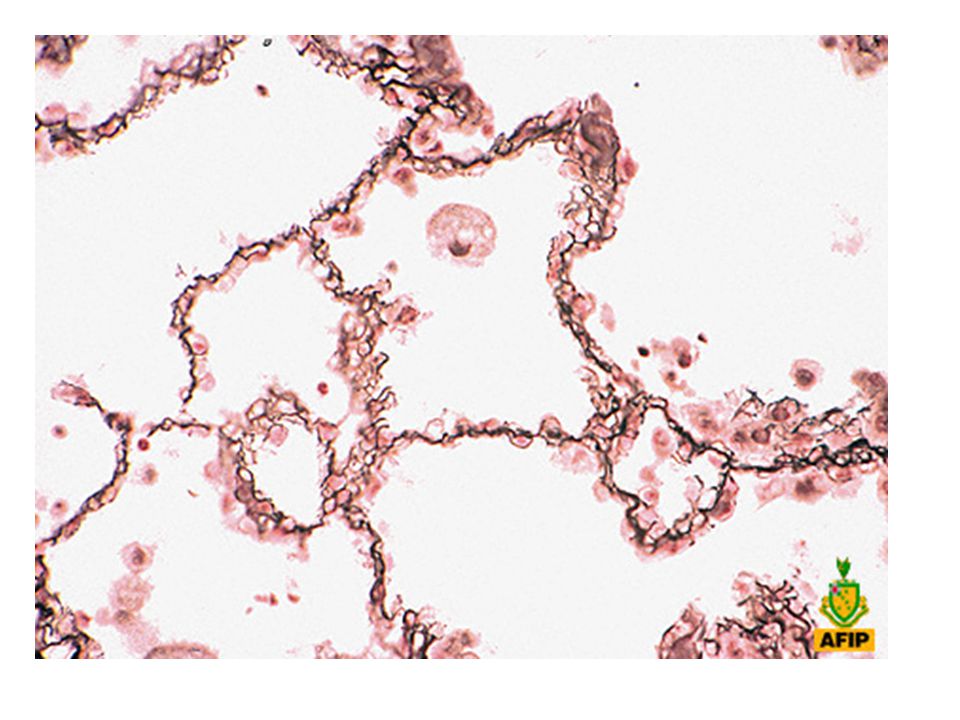
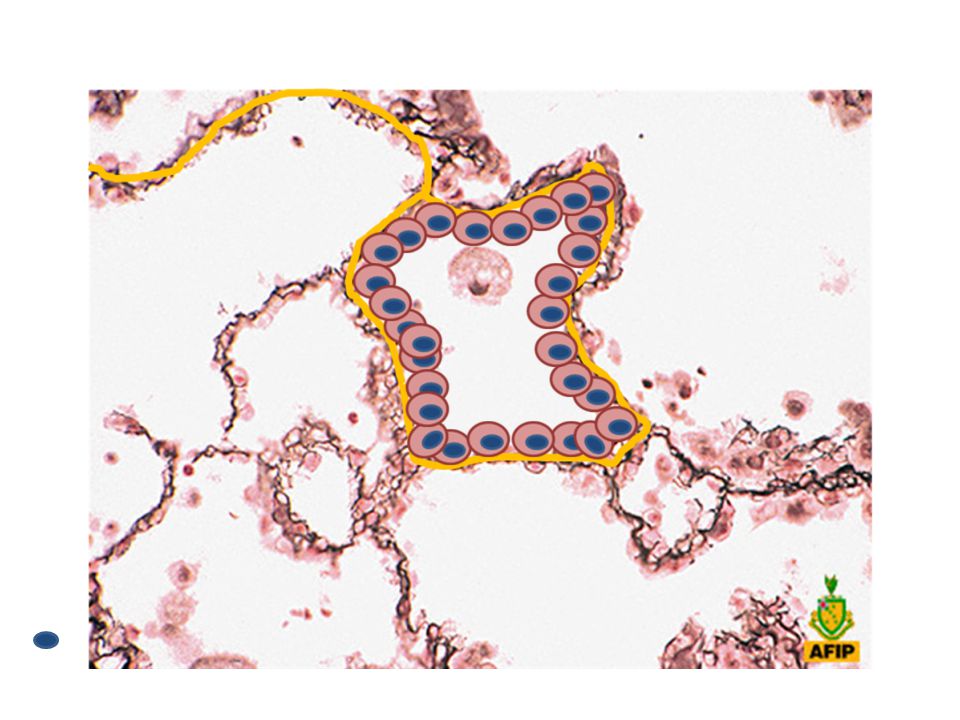
Normal akciğere bi daha bi görelim

29
Lung adenocarcinoma measuring 2 cm or less A Lokalized BAC
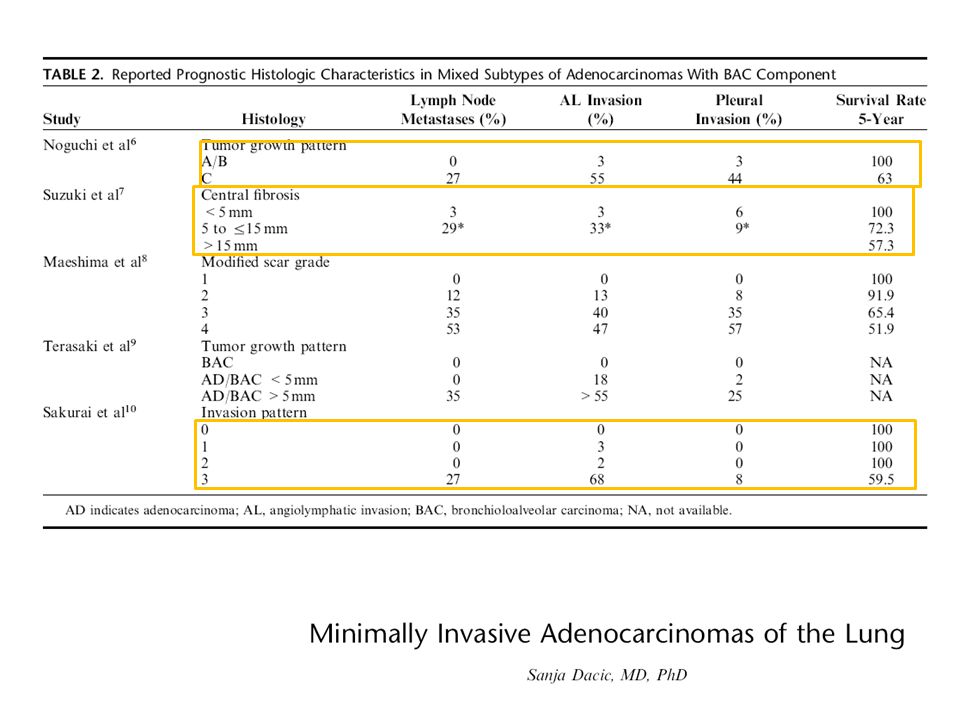
Noguchi M, Morikawa A, Kawasaki M, et al. Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer. 1995;75:2844–2852. Lung adenocarcinoma measuring 2 cm or less A Lokalized BAC B Lokalized BAC-focal alveolar collapse C Lokalized BAC-focal aktve fibroblastic proliferation 4. D Poorly differentiated AC E Tubular adenocarcinoma F Papillary adenocarcinoma with compressive and destructive growth

31
LOH in tumor supressor genes: Noguchi A (BAC): 17%
Aoyagi Y, Yokose T, Minami Y, et al. Accumulation of losses of heterozygosity and multistep carcinogenesis in pulmonary adenocarcinoma. Cancer Res. 2001;61:7950–7954. LOH in tumor supressor genes: Noguchi A (BAC): 17% Noguchi B (BAK-focal alveolar collapse):40% Noguchi C (BAK-focal active fibroblastic proliferation): 96%
: 17% Noguchi B (BAK-focal alveolar collapse):40% Noguchi C (BAK-focal active fibroblastic. proliferation): 96%")
32
In-situ adenocarcinoma: BAC 0 %
Koga T, Hashimoto S, Sugio K, et al. Clinicopathological and molecular evidence indicating the independence of bronchioloalveolar components from other subtypes of human peripheral lung adenocarcinoma. Clin Cancer Res. 2001;7:1730–1738. P53 mutation In-situ adenocarcinoma: BAC 0 % Early invazive adenocarcinoma (Minimally invazive adenocarcinoma) : Mixt type adenocarcinoma with a major BAC component 11% Late adenocarcinoma: Other adenocarcinomas 48%
 : Mixt type adenocarcinoma with a major BAC component 11% Late adenocarcinoma: Other adenocarcinomas 48%")
33
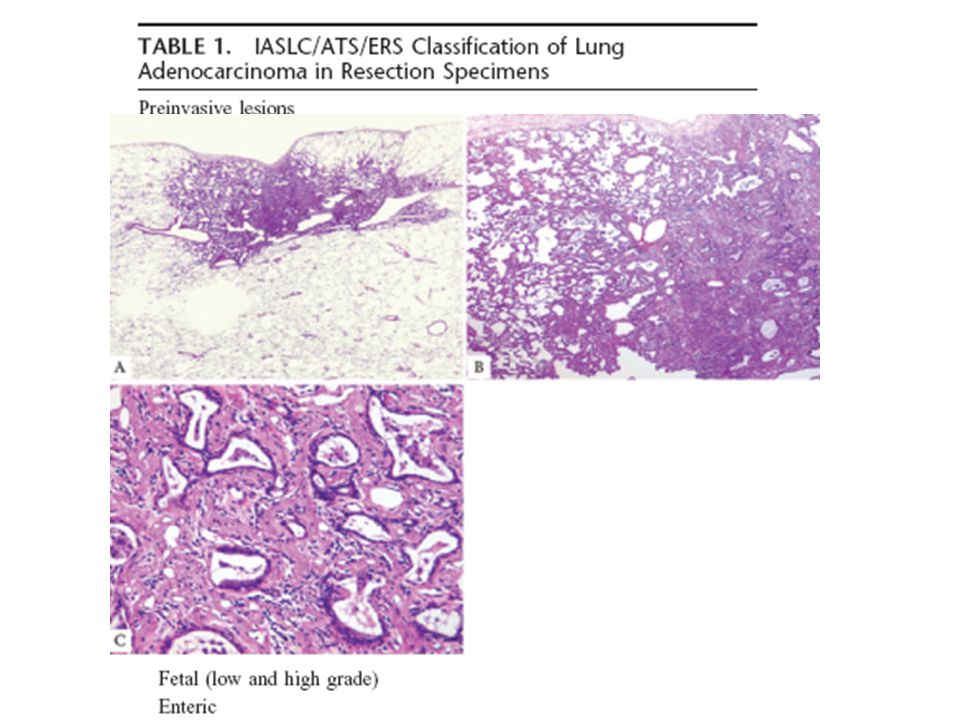
In-situ adenocarcinoma
Early invazive adenocarcinoma (Minimally invazive adenocarcinoma) Late adenocarcinoma
 Late adenocarcinoma.")
34
NEED FOR NEW PROGNOSTIC CATEGORIES
Why Change? New and Targeted therapies Prognostic information on small BAC’s Molecular characterization of lung cancer New agents for adenocarcinoma Histologic eligibility criteria for some new drugs Excellent prognosis of pure BAC and BAC with minimal invasion DEMISE OF NSCLC NEED FOR NEW PROGNOSTIC CATEGORIES

35
New Agents Agent Trade name Type Erlotinib Tarceva Adenocarcinoma
Gefitinib Iressa Bevacizumab Avastin Non-squamous Pemetrexed Alimta Etkinlik Toksisite Etkinlik NSCLC is not enough now

36
NEW (PROPOSED) CLASSIFICATION
 CLASSIFICATION")
37
2011 Multidisciplinary approach Small specimens

38
WHAT İS NEW? ReSECTIONS

39
Strong Recommendations
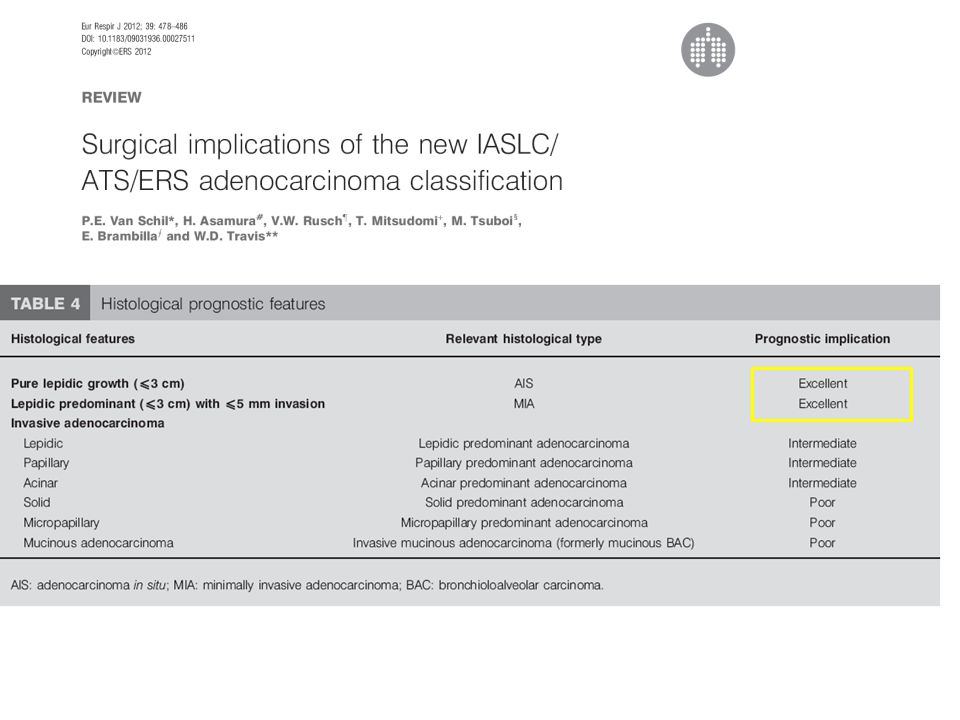
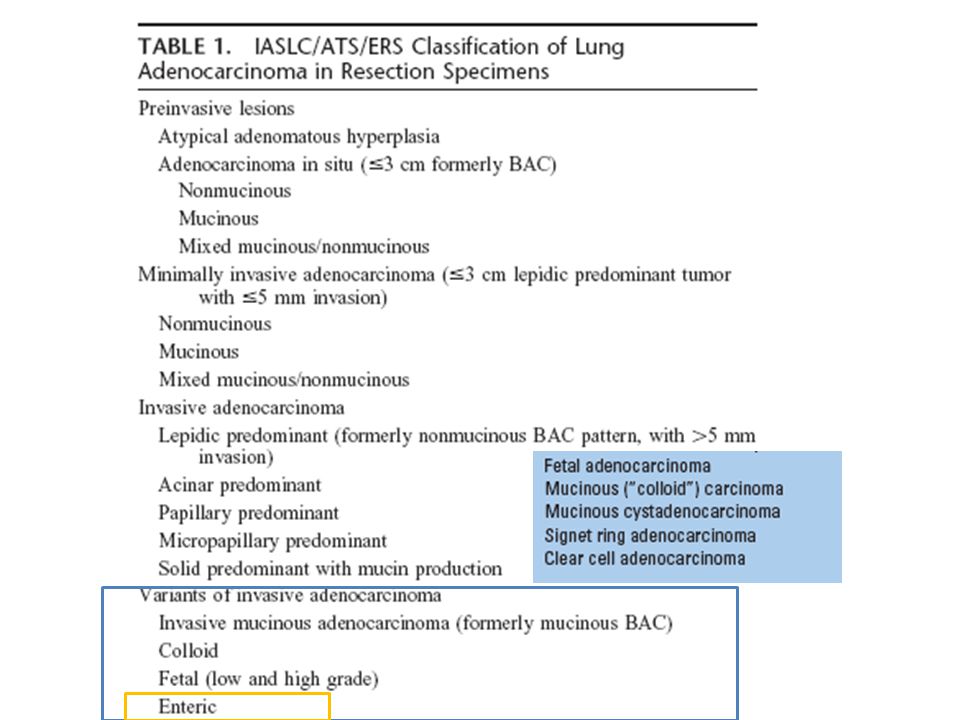
For nonmucinous adenocarcinomas previously classified as mixed subtype where the predominant subtype consists of the former nonmucinous BAC, the use of the term LPA and discontinuing the term “mixed” subtype In patients with early-stage adenocarcinoma, the addition of “micropapillary predominant adenocarcinoma” as a major histologic subtype due to its association with poor prognosis Discontinuing the use of the term “BAC” For small (3 cm), solitary adenocarcinomas with pure lepidic growth, the use of term “Adenocarcinoma in situ” For small (3 cm), solitary, adenocarcinomas with predominant lepidic growth and small foci of invasion measuring 0.5 cm, the use of a new concept: “Minimally invasive adenocarcinoma”
, solitary adenocarcinomas with. pure lepidic growth, the use of term Adenocarcinoma in situ For small (3 cm), solitary, adenocarcinomas with. predominant lepidic growth and small foci of invasion measuring 0.5 cm, the use of a new concept: Minimally invasive adenocarcinoma")
40
Other Recommendations
For invasive adenocarcinomas, comprehensive histologic subtyping be used to assess histologic patterns semiquantitatively in 5% increments, choosing a single predominant pattern. Individual tumors be classified according to the predominant pattern In patients with multiple lung adenocarcinomas, comprehensive histologic subtyping in the comparison of the complex, heterogeneous mixtures of histologic patterns to determine whether the tumors are metastases or separate synchronous or metachronous primaries

42
WHO 2004

44
100 % DFS

46
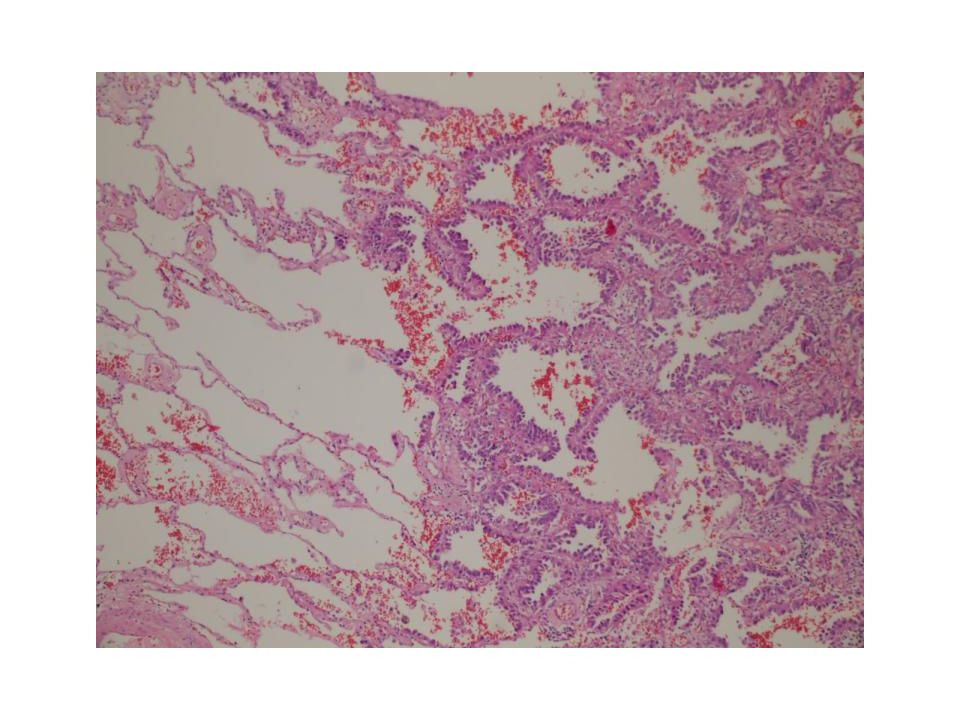
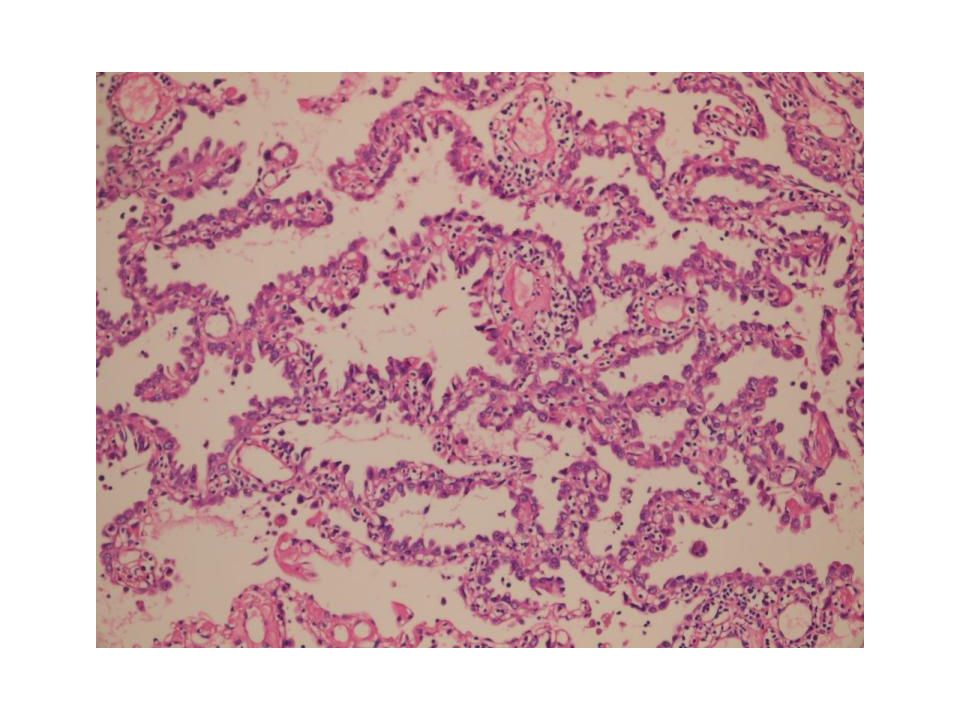
Micropapillary Solid Lepidic Aciner Papillary

47
Micropapillary pattern: Poor prognosis

48
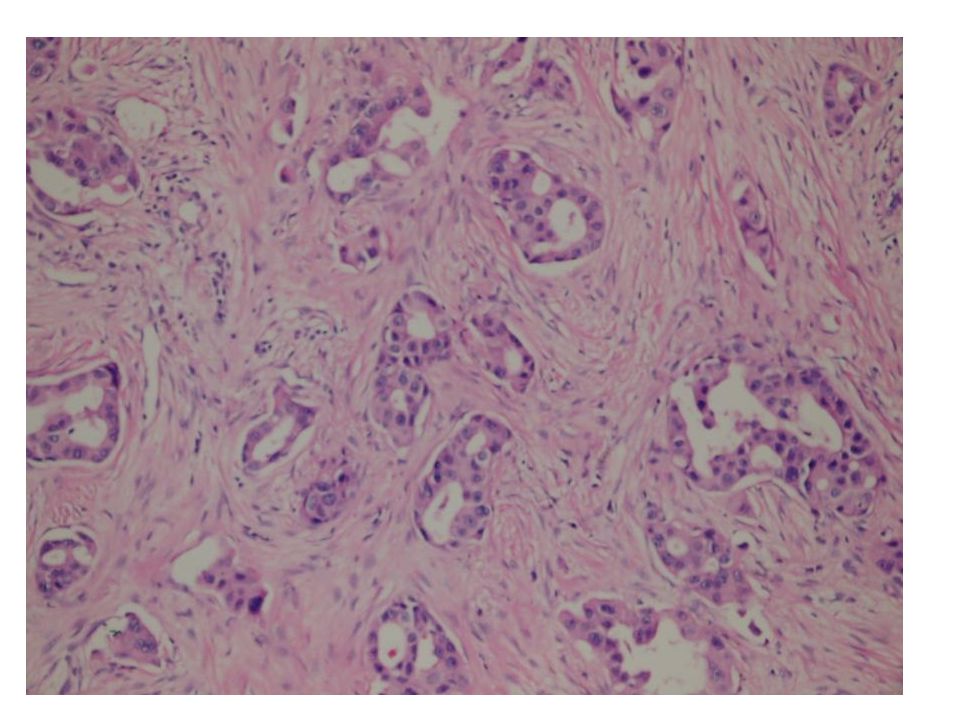
Örnek: İNVAZİV ADENOKARSİNOMA, ASİNER TİP BASKIN
( % 50 ASİNER, %25 PAPİLLER, %25 LEPİDİK TİP) İNVAZİV ADENOKARSİNOMA, MÜSİN OLUŞTURAN SOLİD TİP BASKIN ( % 70 MÜSİN OLUŞTURAN SOLİD , %30 ASİNER TİP) İNVAZİV ADENOKARSİNOMA, MİKROPAPİLLER TİP BASKIN ( % 80 MİKROPAPİLLER, % 15 PAPİLLER, %5 ASİNER TİP)
 İNVAZİV ADENOKARSİNOMA, MÜSİN OLUŞTURAN SOLİD TİP BASKIN. ( % 70 MÜSİN OLUŞTURAN SOLİD , %30 ASİNER TİP) İNVAZİV ADENOKARSİNOMA, MİKROPAPİLLER TİP BASKIN. ( % 80 MİKROPAPİLLER, % 15 PAPİLLER, %5 ASİNER TİP)")
50
Limited (Sublobar) resections
For a limited resection to be adequate: A precise intraoperative diagnosis Evaluation of resection margins Evaluation of lymph nodes FROZEN SECTIONS

52
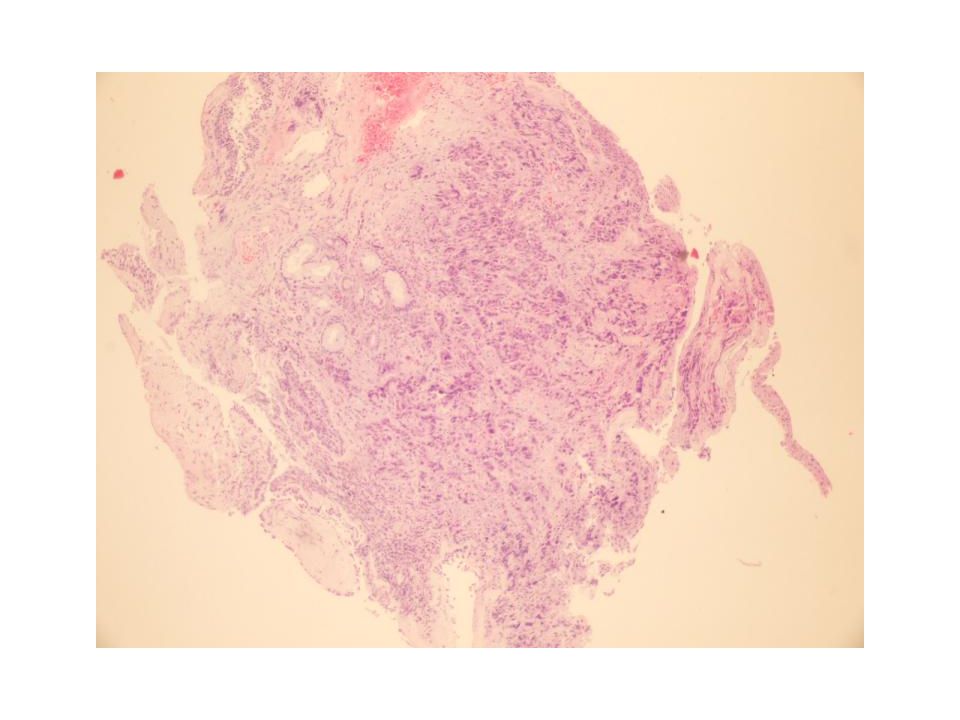
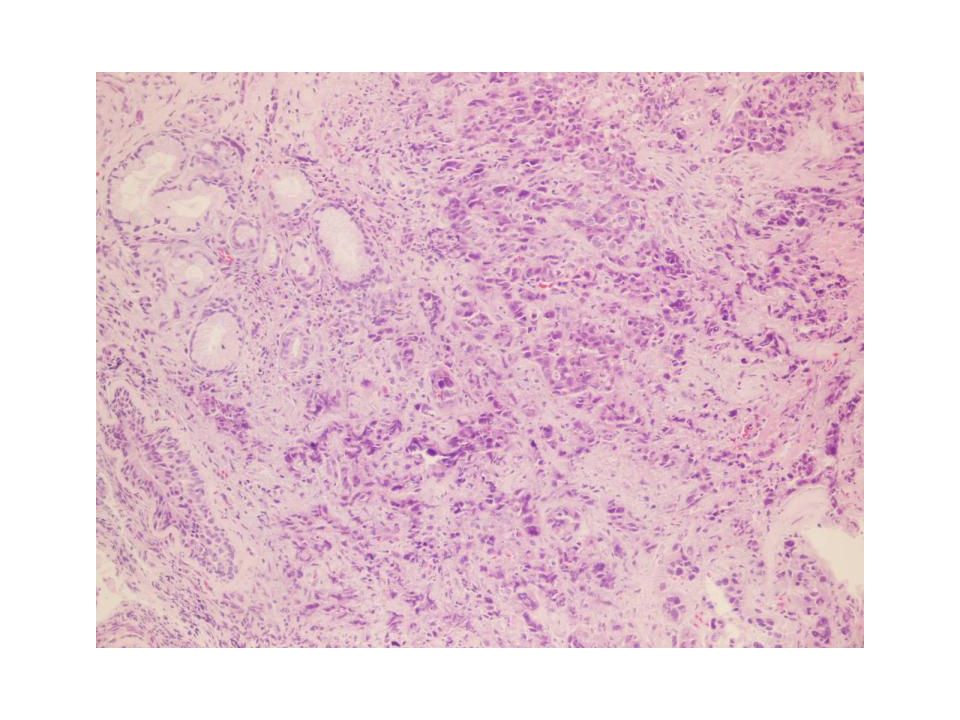
TTF1 SPA CDX2 MUC5A A subset of AC morphologically and immunohistochemically resembling colonic carcinoma

53
WHAT IS NEW? SMALL BIOPSY

54
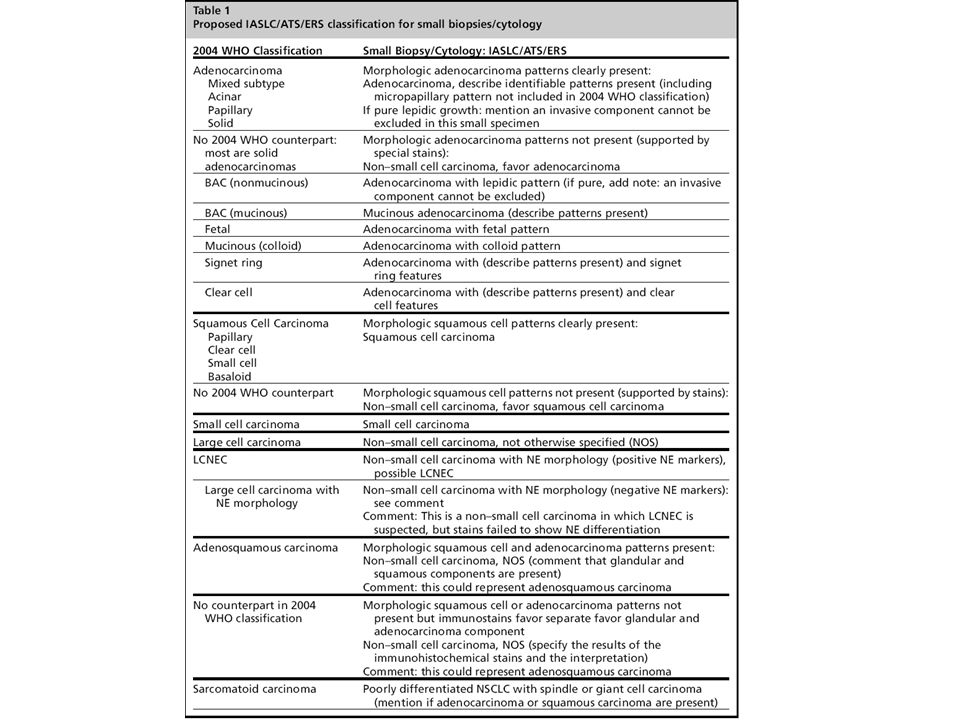
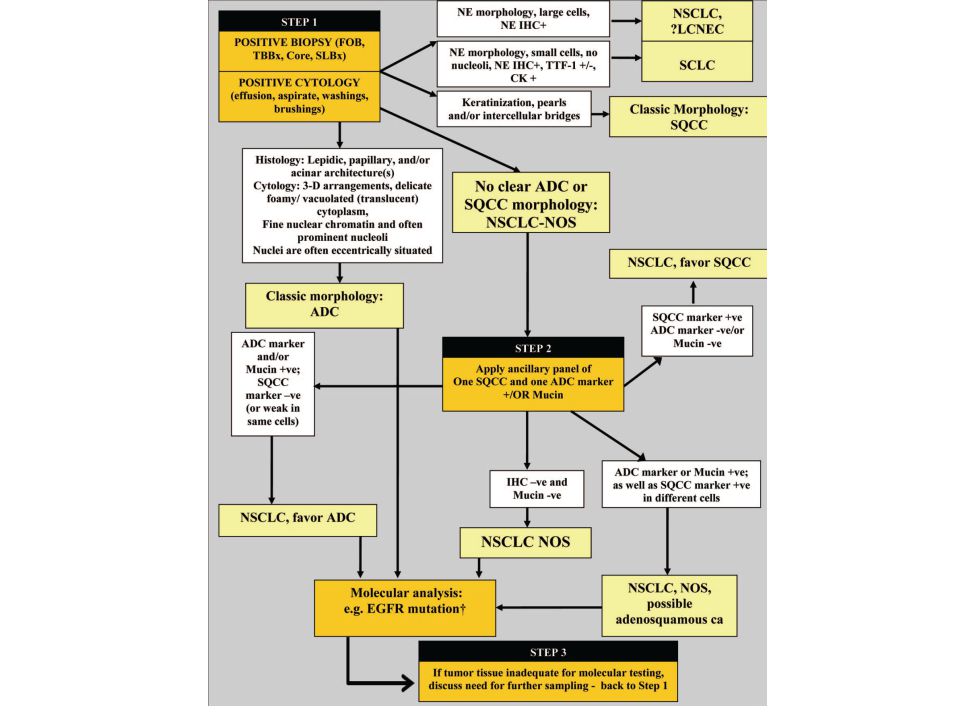
RECOMMENDATION For small biopsies and cytology, NSCLC be further classified into a more specific type, such as adenocarcinoma or squamous cell carcinoma, whenever possible The term NSCLC-NOS be used as little as possible, only when a more specific diagnosis is not possible by morphology and/or special stains

55
Special Stains Adenocarcinoma Squamous Cocktails (nuclear/cytoplasmic)
Mucin TTF1, Napsin, PE10 Squamous P63, CK5/6, 34BE12 Cocktails (nuclear/cytoplasmic) Adeno TTF1/napsin Squamous p63/ck5/6
 Adeno TTF1/napsin. Squamous p63/ck5/6.")
57
Summary Classify by morphology if possible Squamous Adeno
Define patterns

58
Summary If NSCL-NOS by H&E
IHC Squamous markers +, adeno -: NSCL- favor squamous Squamous markers -, adeno +: NSCL- favor adeno If both negative, inconsistent NSCL-NOS

59
Morphology should be adequate for most cases
IHC should be used if necessary Tissue must be used very carefully and saved for molecular studies

62
p63

63
NSCLC Favor adenocarcinoma TTF1

65
Molecular: When? Every case if it is adenocarcinoma; and when adenocarcinoma can not be ruled out safely: Adenocarcinoma NSCLC- favor adenocarcinoma NSCLC-NOS

66
Molecular: What? EGFR (mutation) EML4-ALK translocation (FISH)
K-Ras (mutation)
")
67
Role of Pathology Differentiate cancer from non-cancer
Differentiate viable tissue from non-viable tissue Differentiate adequate sample size from non- adequate sample size Tumor type Suggesting/performing the appropriate molecular test for the tumor type

Benzer bir sunumlar



 A: _____ nerede? B: _____ evde. (…at home) OR: tell the location using.>")

 Test ve Tartışma Varlıklar Bölümler 14 &15.>")
















